Neurological examination of the neurosurgical patient. Dániel Bereczki SU Department of Neurology
|
|
|
- Audrey Short
- 5 years ago
- Views:
Transcription
1 Neurological examination of the neurosurgical patient Dániel Bereczki SU Department of Neurology


2 E-learning Indivudual study Interactive learning Self assessment at the end of chapters

3 E-learning Indivudual study Interactive learning Self assessment at the end of chapters
4

5

6

7
8 The 4 questions to answer 1. Is there a neurological disease? 2. If yes, where is the lesion? 3. What pathological conditions may cause a lesion at this site? 4. In this patient which of these conditions is the most likely to be present?
9 Case y/o man Car accident years before, with fracture of left scapula Abstinent to alcohol Quitted smoking 1 month ago (before that he smoked 2 packs per day) Clonisation in his left arm started during conversation No loss of consciousness
10 RR: 205/120 mm Hg On admission No other signs of internal disease R. decreased visual acuity R. larger pupil L. central (upper motor neuron) facial laesion L. severe paresis of upper extremity, with exaggerated deep tendon reflexes, Trömner and Hoffmann signs. No other signs
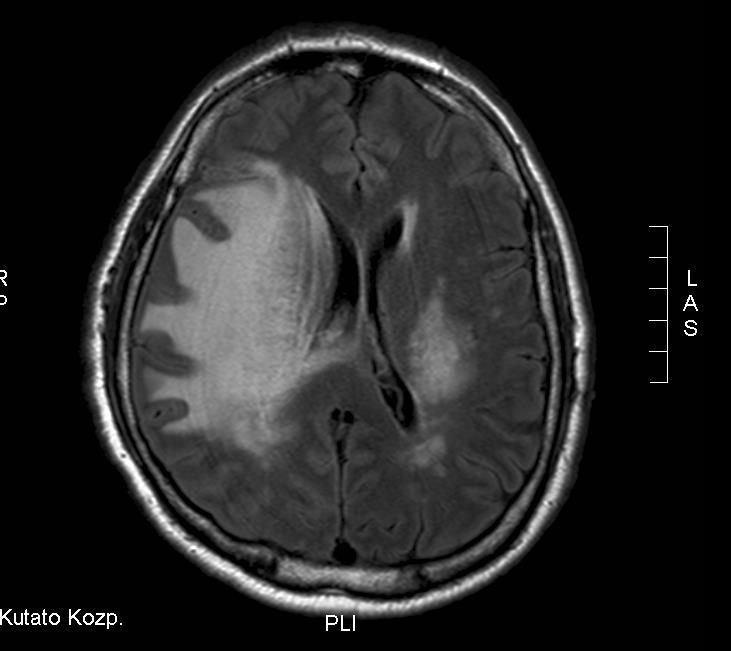
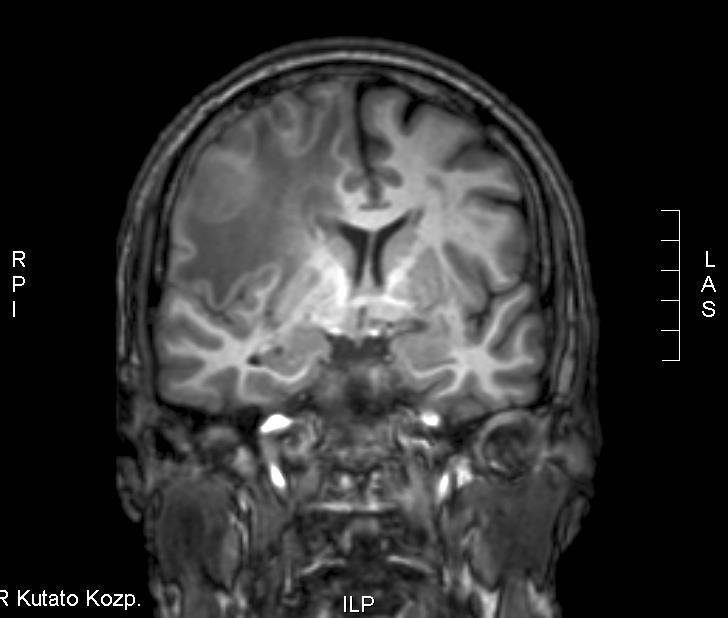
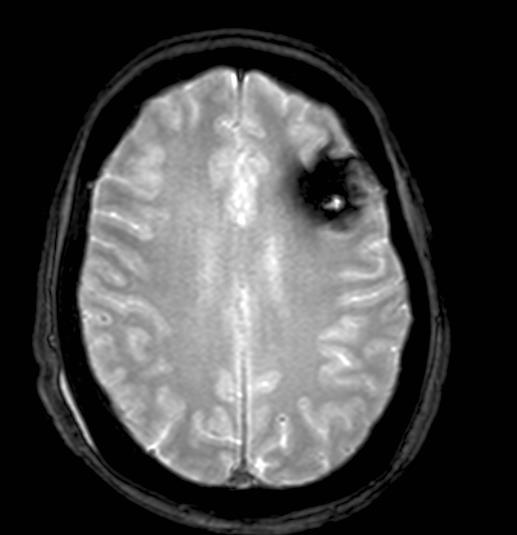
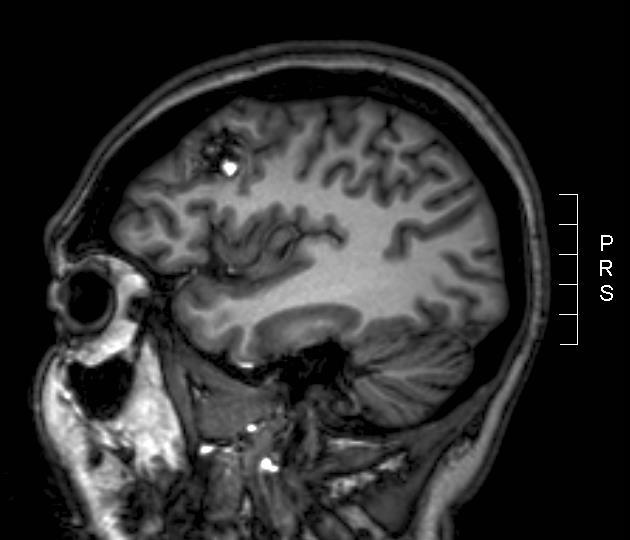
11 MRI
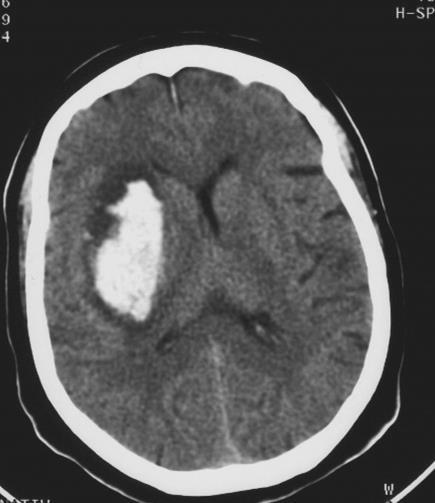
12 61 y/o woman Case years ago ovariectomy due to benign tu 10 y hypertension 3 y surgery for duodenal ulcer 1 y planocellular lung cancer discovered at screening - surgery, chemoth. CT control no recidival tumor One week ago left extremities became weak, weakness worsened 2 days ago
13 On admission RR: 165/90 mm Hg Alopecia (chemoth) Cushingoid face Scar of chest surgery Left central facial paresis Left sided faciobrachial mild hemiparesis Normal reflexes Alert, oriented
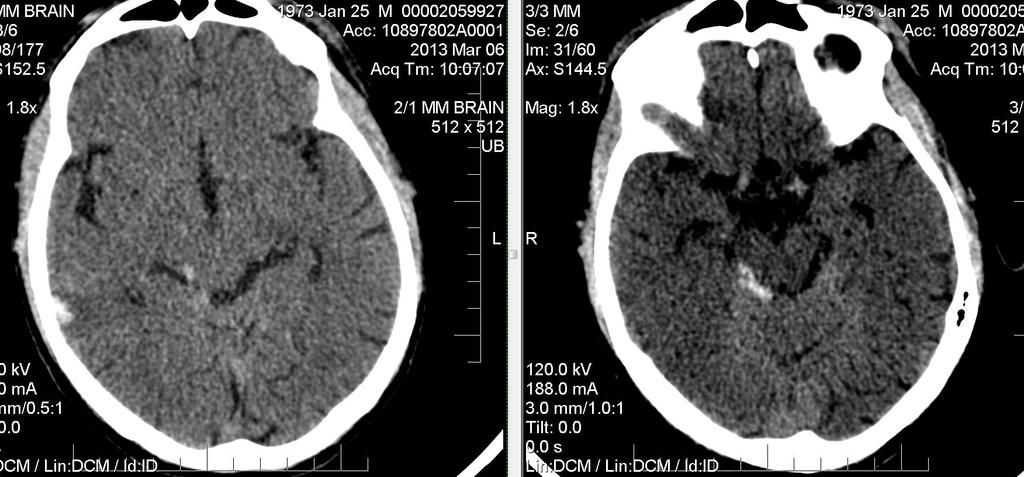
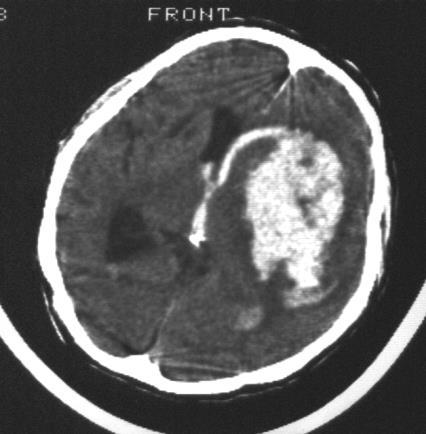
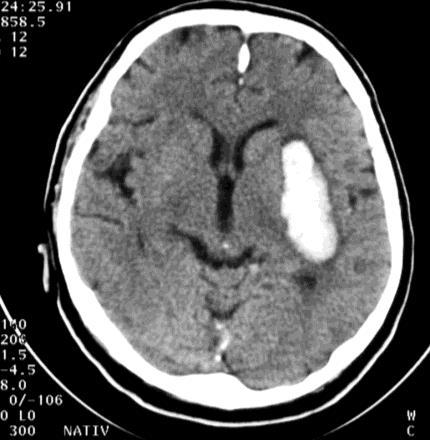
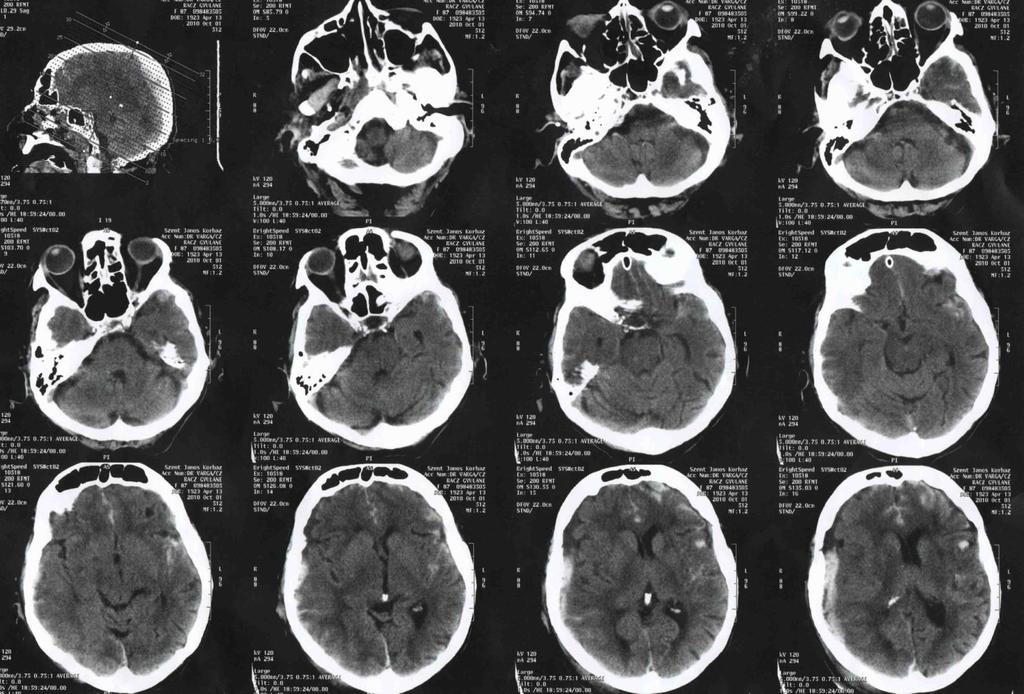
14 Non-contrast CT

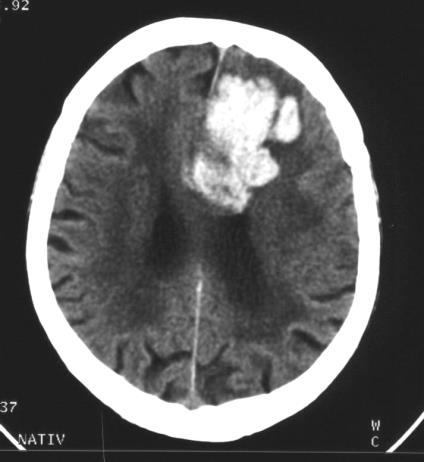
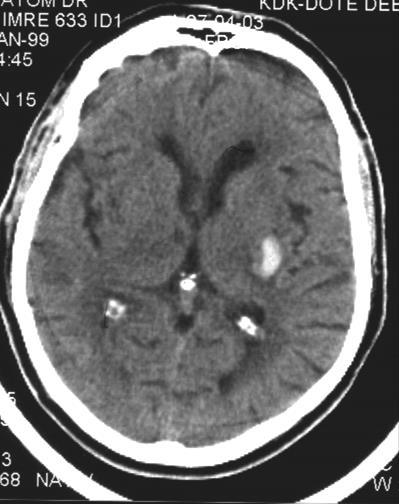
15 Postcontrast and native CT


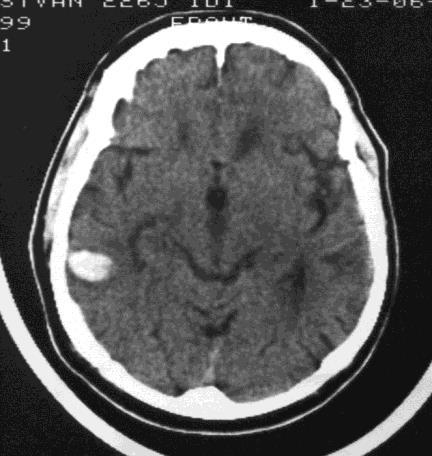
16 Other patient. Primary lung cancer. Neurosurgery indicated??
17 Case y/o woman History unknown Found in the morning comatose in her bed Does not communciate RR: 116/78 T: 38 o C Periodical nystagmus to the left Repeated epileptic seizures (status epilepticus) No other focal signs
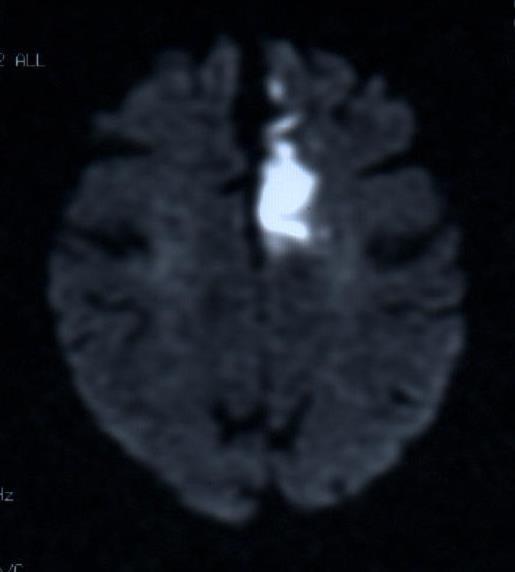
18 MRI

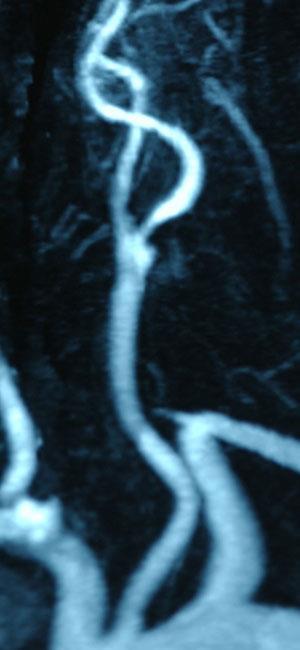
19 MRI and MRA

20 Angioma known since 40 years. Neurosurgery indicated?
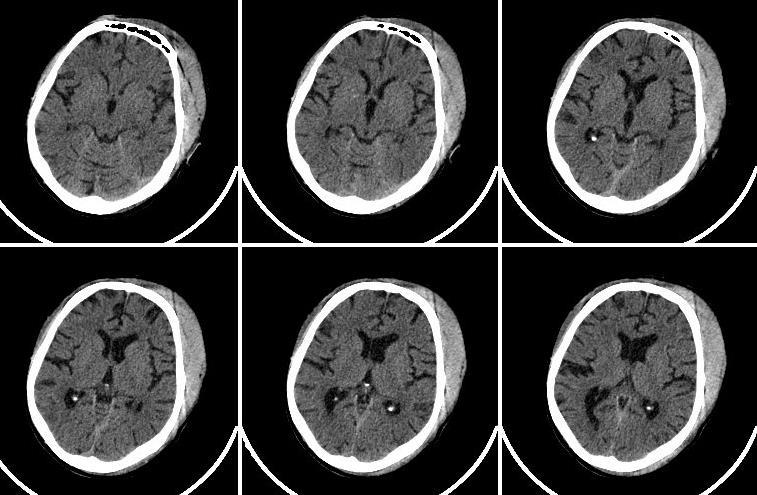
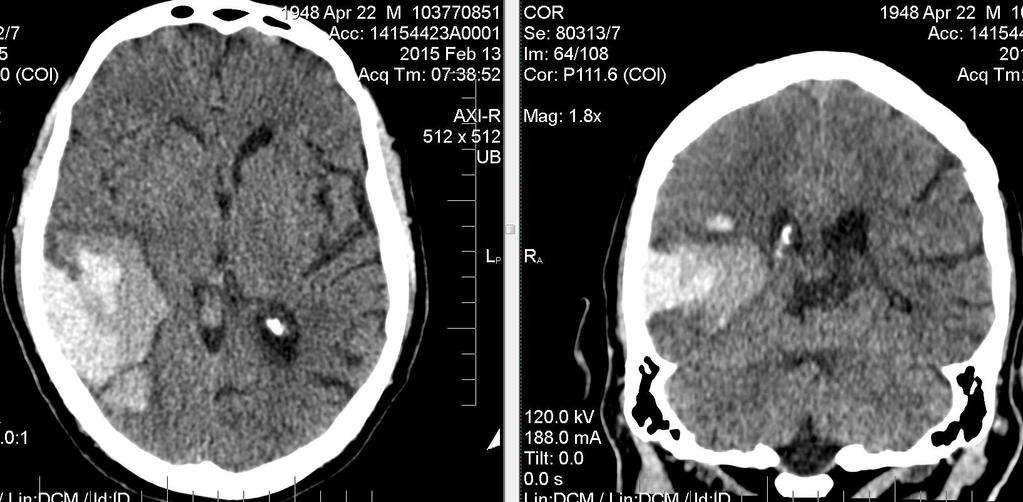
21 Patient history Chronic alcohol consumption Epileptic seizure Head injury CT
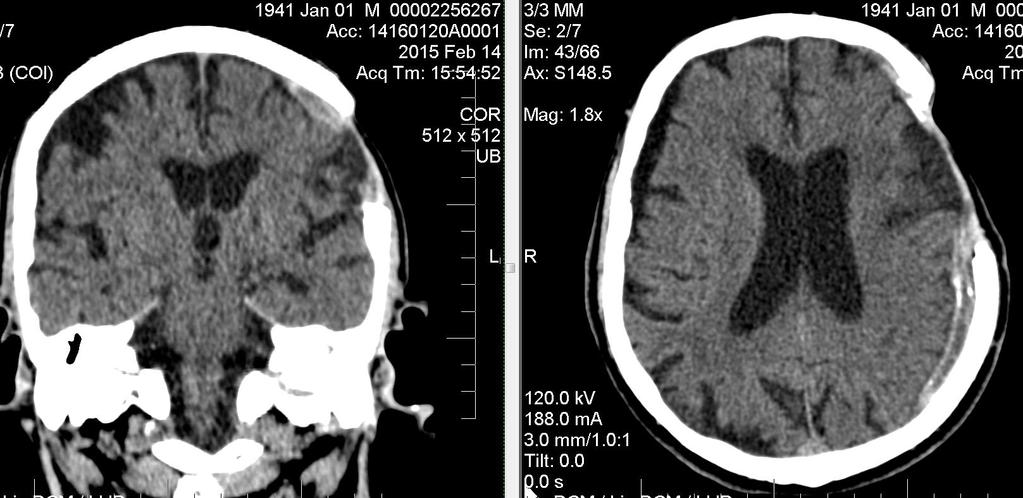
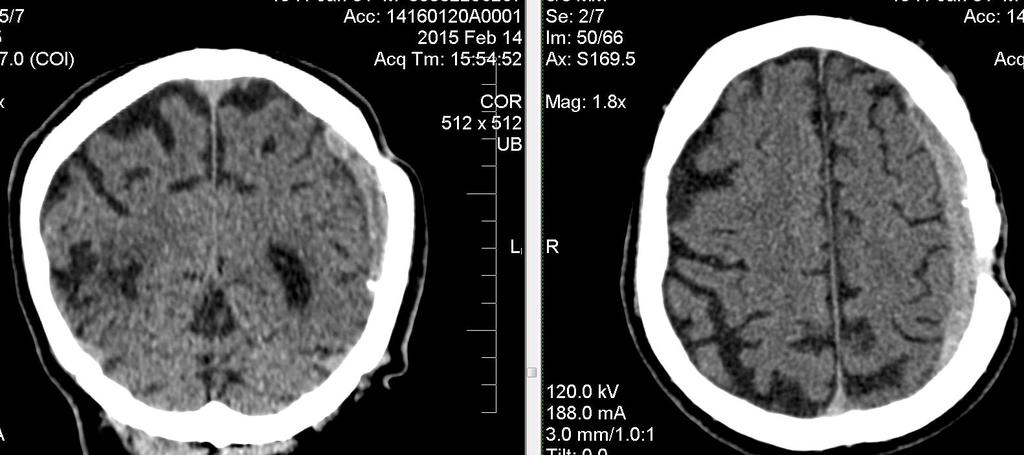
22 CT examination Any pathological?
23 CT examination
, to")
24 neuro- = nervelogia = knowledge of soemthing, λέγω (lego), to speak




25 Neurology Central nervous system Brain Spinal cord Radices, plexus, nerves Neuromuscular junction Muscles
26 Neurology and neurosurgery Dsieases of the central nervous system Tumors Cerebral abscess Cerebrovascular disorders Cerebellar hemorrhage Cerebellar infarct Intracerebral hemorrhage AVM Aneurysm Traumatic lesions Subdural and epidural hemorrhage Other central nervous system trauma (commotion, etc) Spinal cord compression Peripheral nervous system disorders Acustic neurinoma Carpal tunnel syndrome (and other peripheral compression syndromes) Some cases of radicular compression caused by intervertebral disk herniation
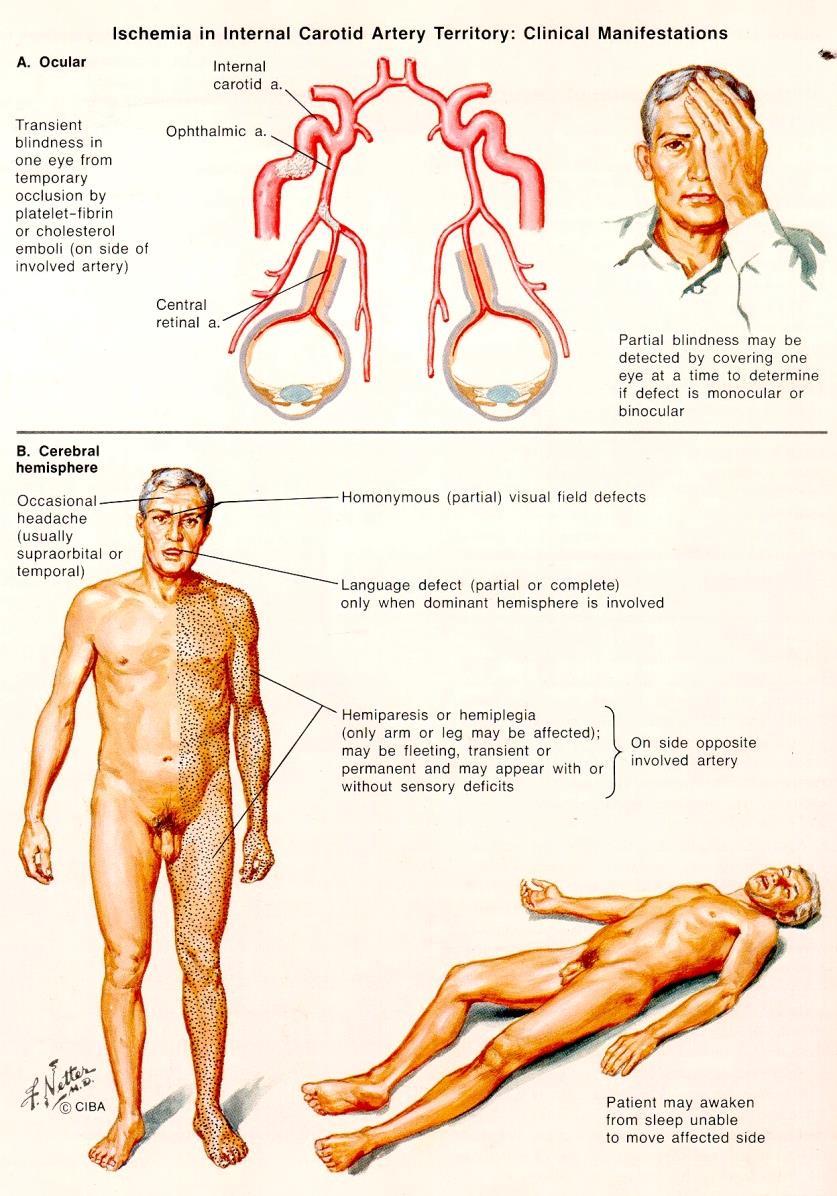
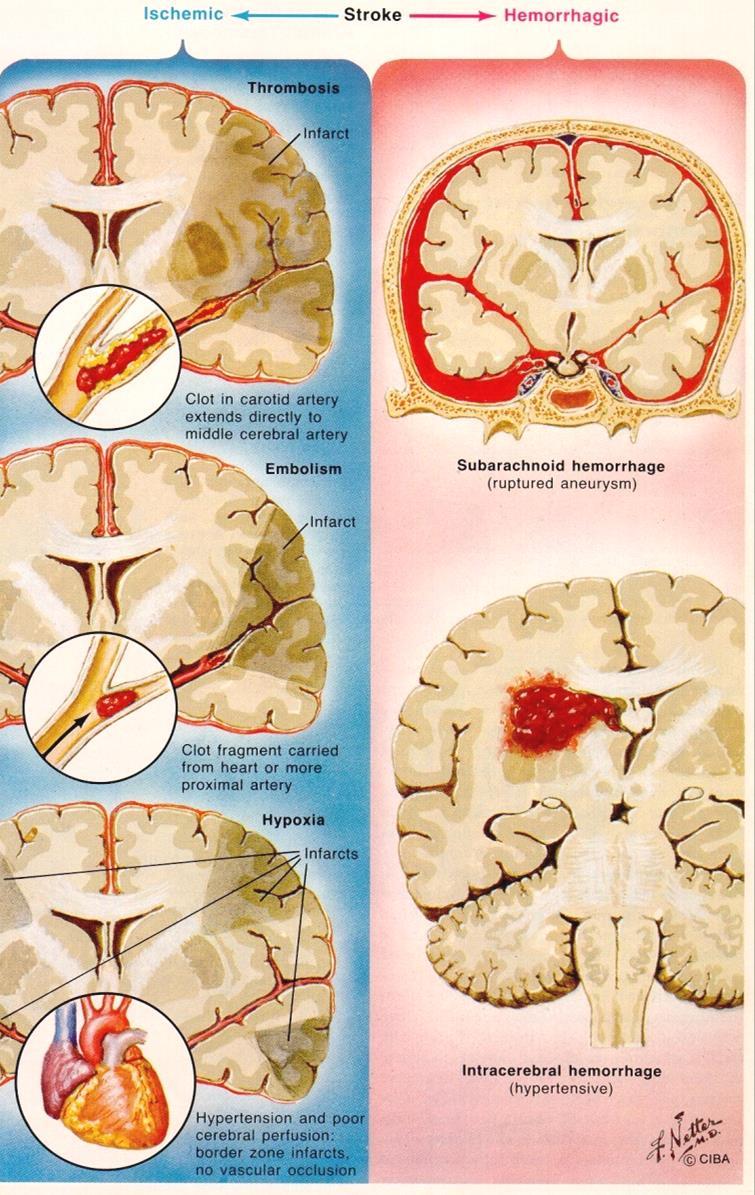
27 Cerebrovascular disorders

28 Carotis endarterectomy


29 Intracerebral hemorrhages: where is the limit? - -?+ +?? +? +? -
 Litvania: out of 89 certain indication - 80%")
30 STICH trial Debrecen: out of 55 certain indication - 54 conservative - 1 surgery (2%) Litvania: out of 89 certain indication - 80% surgery
31 A STICH RESULTS(Lancet 2005;365: ) Good outcome: Early surgery: 26,1% Early medical treatment: 23,8 % NS

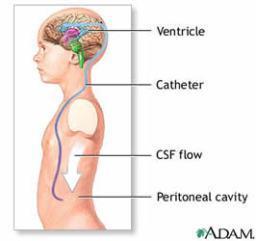
32 Surgery for NPH
33 Tasks in general practice Take the history and perform exam. Consider a neurological disease. Answer the 4 questions. Organize diagnostic procedures. Decide on treatment. Educate and help relatives of patient
34 Taking the hisory Not enough time. What exactly mean the patient and the relative on the complaint? Do you suspect a neurological disease? Is there an emergency?
35 What to consider at history Age Clarifying the symptoms Mode of onset and progression Chronological sequence of events Value of negative information Exclude irrelevancies Drugs Heteroanamnesis (interviewing relatives)
36 The 4 questions to answer 1. Is there a neurological disease? 2. If yes, where is the lesion? 3. What pathological conditions may cause a lesion at this site? 4. In this patient which of these conditions is the most likely to be present?
37 If you suspect a neurological disease Think over what to do with the patient. Can you take the responsibility to treat this patient? Is it necessary to send the patient to a neurologist? How urgent it is?
38 Organizing the diagnostic procedures Is it an emergency? If yes, where to send the patient? If not, how far can I get in the diagnostic process? What ancillary investigations to ask for, and from whom? Where do they perfom these investigations? If the appointment is at a distant time, is it safe to wait?
39 Ancillary invstigations to confirm or refute the suspected diagnosis Methods examining structure X-ray, CT, MRI, ultrasound Imaging methods examining function fmri, SPECT, PET, ultrasound Electrophysiological methods EEG, ENG, EMG, evoked responses Examination of the cerebrospinal fluid Immunological, genetic and molecular biological investigations Cytology and pathological investigations Consultations with other specialities



40 Previous practice (until the 1980-ies) 1. day: cisternal CSF 2. day: percutan carotid angiography
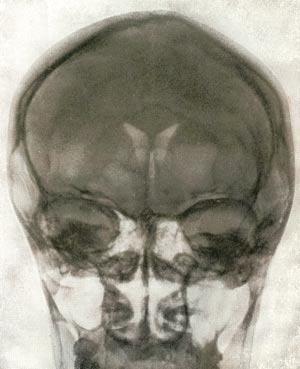
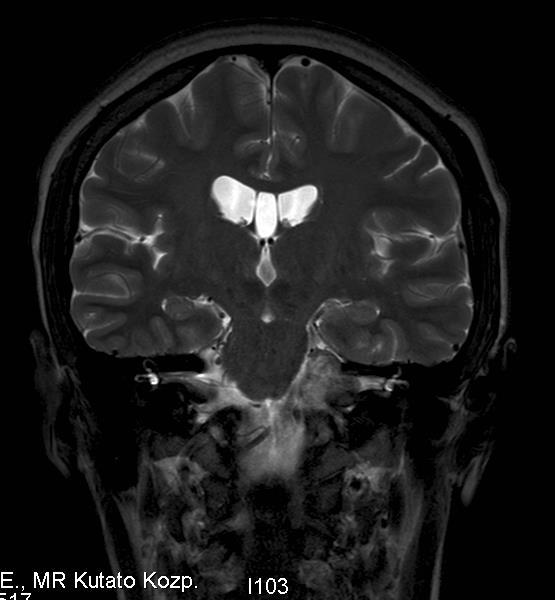
41 PNEUMOENCEPHALOGRAM MR IMAGING
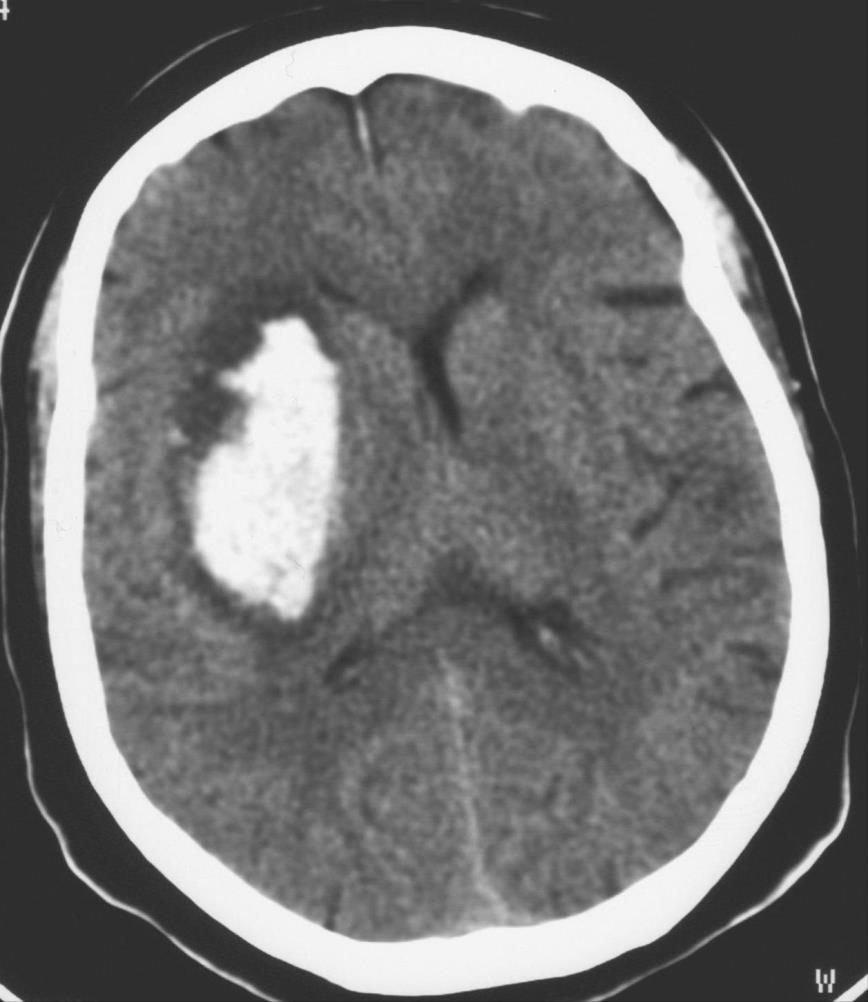
42 ICH


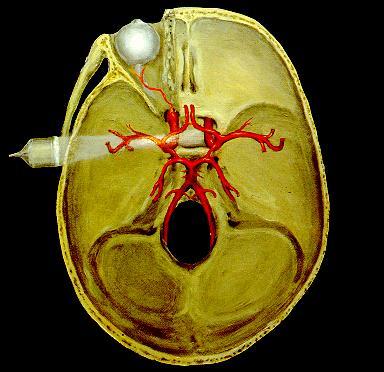
43 Arteria cerebri anterior
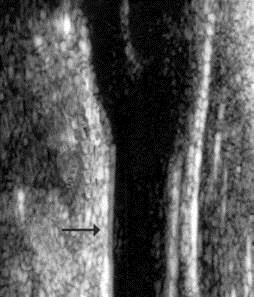
44 Carotid Ultrasound
45 Transcranial Doppler

46 Visual evoked response
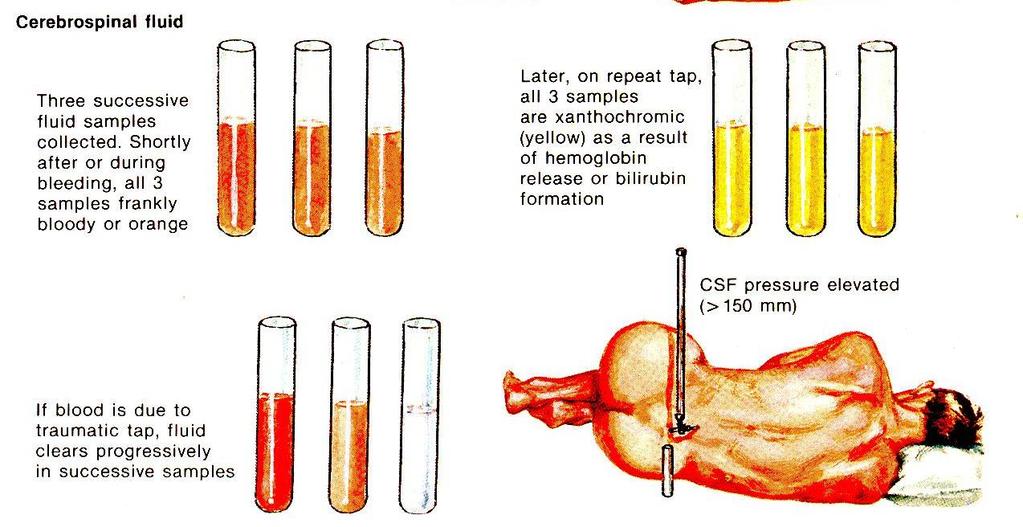
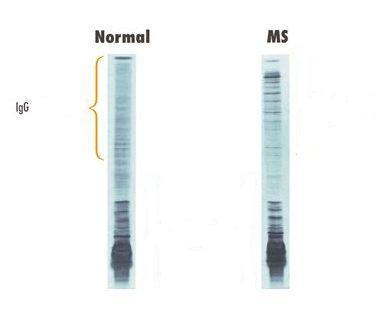
47 CSF examination


48 Pathology ISCHEMIC STROKE INTRACEREBRAL HEMORRHAGE Hegedűs, 2001
49 EMERGENCY IN NEUROLOGICAL DISEASES Unexpected (street, home, workplace), sudden onset conditions Expected (inhospital, dg known) emergency situations stroke epileptic seizure head injury loss of consciousness due to unknown cause etc repeated epileptic seizures breathing disorder in myasthenia breathing disorder in ALS breathing disorder in periphreal disorders (Guillain-Barré) etc Admit to general emergency unit Directly admit to specialized unit: STROKE NEUROTRAUMATOLOGY Etc Transfer to specialized/ intensive unit
50 What is pathological?

51 Milyen kóros eltérés látszik? What is pathological?
52 What is pathological?
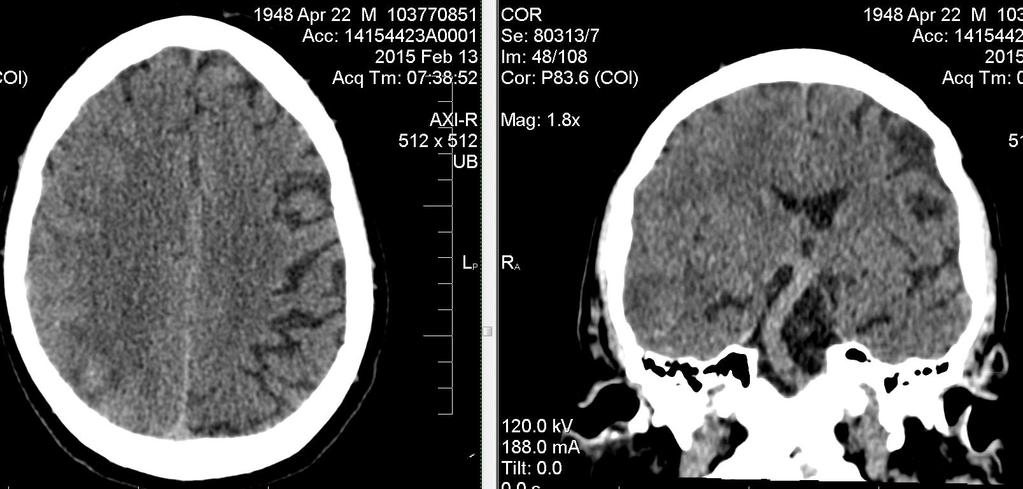
53 What is pathological?
54 What is pathological?
55 What is pathological?
56 What is pathological?

57
58 Mild traumatic brain injury 1./ Characteristic history? 2. / When to perform neuroimaging (CT or MRI) and when is it not necessary? 3. / What are the criteria to decide on hospitalization or discharge home? 4./ What are the late consequences of MTBI?
59 Mild traumatic brain injury Blunted force, closed skull injury Associated with LOC < 20 min and/or retrograde amnesia Glasgow Coma Scale between 13-15, No focal neurological signs, No signs of intracranial damage (eg. epileptic signs), and Nothing pathological can be seen by CT
60 Commotio cerebri (cerebral concussion ) Relatively short (max 1 h) LOC after skull injury with amnesia (retreograde or anterograde) but without other signs of brain injury and neuroimaging (CT, MRI) reveals no pathological findings, there is no blood in the CSF.
61 Contusio cerebri (cerebral contusion): Skull taruma is usually (but not always) assocaited with longer LOC (sometimes days), cerebral lesions refelected by appropriate focal neurological signs, neuroimaging reveals focal hemorrhages in the brain tissue and the CSF is usually stained with blood
62 Compressio cerebri (cerebral compression) Compression on the brain caused by a consequence of injury (subdural or epidural haematoma, contusion hemorrhage and edema) LOC associated with the injury might be followed by a transient period with alert state ( lucidum intervallum ), The increasing intracranial pressure due to the increasing space occupation might result in cerebral herniation.
63
64 Indications of neuroimaging (CT or MRI) after head injury Always if GCS 13, If GCS 14 and during injury amnesia LOC vomiting suspected cranial fracture coagulation disorder in history with concomittant anticoagulant treatment if focal signs are seen if post traumatic epileptic seizure occurs severe or increasing headache anisocoria multiple trauma
65 Conditions of discharge in patients with low risk normal CT, GCS = 15, at most only very mild complaints (headache or dizziness), no LOC, no amnesia, no neurological or cognitive signs, no any other significant complaint or sign, supervision at home can be organized.

66
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
LOSS OF CONSCIOUSNESS & ASSESSMENT. Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT
 LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
Brain Injuries. Presented By Dr. Said Said Elshama
 Brain Injuries Presented By Dr. Said Said Elshama Types of head injuries 1- Scalp injuries 2- Skull injuries 3- Intra Cranial injuries ( Brain ) Anatomical structure of meninges Intra- Cranial Injuries
Brain Injuries Presented By Dr. Said Said Elshama Types of head injuries 1- Scalp injuries 2- Skull injuries 3- Intra Cranial injuries ( Brain ) Anatomical structure of meninges Intra- Cranial Injuries
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
PA SYLLABUS. Syllabus for students of the FACULTY OF MEDICINE No.2
 Approved At the meeting of the Faculty Council Medicine No. of Approved At the meeting of the chair of Neurosurgery No. of Dean of the Faculty Medicine No.2 PhD, associate professor M. Betiu Head of the
Approved At the meeting of the Faculty Council Medicine No. of Approved At the meeting of the chair of Neurosurgery No. of Dean of the Faculty Medicine No.2 PhD, associate professor M. Betiu Head of the
Neurotrauma. Béla Faludi Dept.. of Neurology University of PécsP
 Neurotrauma Béla Faludi Dept.. of Neurology University of PécsP Emergency!!! Why here? Opened cranial injury visible: neurosurgery Closed injuries sometimes diagnosed by neurologist Masking situation:
Neurotrauma Béla Faludi Dept.. of Neurology University of PécsP Emergency!!! Why here? Opened cranial injury visible: neurosurgery Closed injuries sometimes diagnosed by neurologist Masking situation:
Louisiana State University Health Sciences Center
 Louisiana State University Health Sciences Center Department of Neurosurgery Student Clerkship Guide 2017 2018 Introduction Welcome to LSUHSC New Orleans neurosurgery rotation. Our department is dedicated
Louisiana State University Health Sciences Center Department of Neurosurgery Student Clerkship Guide 2017 2018 Introduction Welcome to LSUHSC New Orleans neurosurgery rotation. Our department is dedicated
Vascular Disorders. Nervous System Disorders (Part B-1) Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013
 Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013") Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
A Hypothesis Driven Approach to the Neurological Exam
 A Hypothesis Driven Approach to the Neurological Exam Vanja Douglas, MD Assistant Clinical Professor UCSF Department of Neurology Disclosures None 1 Purpose of Neuro Exam Screen asymptomatic patients Screen
A Hypothesis Driven Approach to the Neurological Exam Vanja Douglas, MD Assistant Clinical Professor UCSF Department of Neurology Disclosures None 1 Purpose of Neuro Exam Screen asymptomatic patients Screen
Traumatic brain injuries are caused by external mechanical forces such as: - Falls - Transport-related accidents - Assault
 PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
SUPPLEMENTARY FIG. S2. (A) Risk of bias and applicability concerns graph by marker. Review authors judgments about each domain presented as
 Risk of bias and applicability concerns graph by marker. Review authors judgments about each domain presented as") Supplementary Data SUPPLEMENTARY FIG. S1. Graphical depiction of (A) influence and (B) outlier detection analyses of S100 calcium binding protein B (S100B) 0.10 0.11lg/L cutoff value studies. (C) Summary
Supplementary Data SUPPLEMENTARY FIG. S1. Graphical depiction of (A) influence and (B) outlier detection analyses of S100 calcium binding protein B (S100B) 0.10 0.11lg/L cutoff value studies. (C) Summary
Virtual Mentor American Medical Association Journal of Ethics August 2008, Volume 10, Number 8:
 Virtual Mentor American Medical Association Journal of Ethics August 2008, Volume 10, Number 8: 516-520. CLINICAL PEARL The Hazards of Stopping a Brain in Motion: Evaluation and Classification of Traumatic
Virtual Mentor American Medical Association Journal of Ethics August 2008, Volume 10, Number 8: 516-520. CLINICAL PEARL The Hazards of Stopping a Brain in Motion: Evaluation and Classification of Traumatic
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Pre-hospital Response to Trauma and Brain Injury. Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center
 Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Head, Face, Eyes, Ears, Nose and Throat. Neurological Exam. Eye Function 12/11/2017. Oak Ridge High School Conroe, Texas
 Head, Face, Eyes, Ears, Nose and Throat Oak Ridge High School Conroe, Texas Neurological Exam Consists of Five Major Areas: 1. cerebral testing cognitive functioning 2. Cranial nerve testing 3. Cerebellar
Head, Face, Eyes, Ears, Nose and Throat Oak Ridge High School Conroe, Texas Neurological Exam Consists of Five Major Areas: 1. cerebral testing cognitive functioning 2. Cranial nerve testing 3. Cerebellar
TBI are twice as common in males High potential for poor outcome Deaths occur at three points in time after injury
 Head Injury Any trauma to (closed vs. open) Skull Scalp Brain Traumatic brain injury (TBI) High incidence Most common causes Falls Motor vehicle accidents Other causes Firearm- related injuries Assaults
Head Injury Any trauma to (closed vs. open) Skull Scalp Brain Traumatic brain injury (TBI) High incidence Most common causes Falls Motor vehicle accidents Other causes Firearm- related injuries Assaults
UPSTATE Comprehensive Stroke Center. Neurosurgical Interventions Satish Krishnamurthy MD, MCh
 UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
Chapter 57: Nursing Management: Acute Intracranial Problems
 Chapter 57: Nursing Management: Acute Intracranial Problems NORMAL INTRACRANIAL PRESSURE Intracranial pressure (ICP) is the hydrostatic force measured in the brain CSF compartment. Normal ICP is the total
Chapter 57: Nursing Management: Acute Intracranial Problems NORMAL INTRACRANIAL PRESSURE Intracranial pressure (ICP) is the hydrostatic force measured in the brain CSF compartment. Normal ICP is the total
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Imaging Biomarkers Significance S100B NSE. Admitted within 6 hours of injury and CT scan occurred after initial examination. N = 1,064 CT+ N = 50 4.
 Concussion Guidelines Step 1: Systematic Review of Prevalent Indicators Supplemental Content 7 Evidence Table. Included Studies For Key Question 4 Imaging and Biomarker Publications Medium Potential for
Concussion Guidelines Step 1: Systematic Review of Prevalent Indicators Supplemental Content 7 Evidence Table. Included Studies For Key Question 4 Imaging and Biomarker Publications Medium Potential for
Kristin s Head Trauma Board Questions 11/07/14
 Kristin s Head Trauma Board Questions { 11/07/14 A healthy 15 y/o boy was playing football at a park near his home with a group of friends when he tripped over a friend s leg while trying to catch a pass.
Kristin s Head Trauma Board Questions { 11/07/14 A healthy 15 y/o boy was playing football at a park near his home with a group of friends when he tripped over a friend s leg while trying to catch a pass.
Reviewing the recent literature to answer clinical questions: Should I change my practice?
 Reviewing the recent literature to answer clinical questions: Should I change my practice? JILL MILLER, MD PEM ATTENDING CHKD ASSISTANT PROFESSOR PEDIATRICS, EVMS Objectives Review the literature to answer
Reviewing the recent literature to answer clinical questions: Should I change my practice? JILL MILLER, MD PEM ATTENDING CHKD ASSISTANT PROFESSOR PEDIATRICS, EVMS Objectives Review the literature to answer
UHSM ED Pathway ELDERLY FALL / COLLAPSE
 UHSM ED Pathway ELDERLY FALL / COLLAPSE Patient name / Pathway for patients who require assessment in ED after a fall or collapse Note: - It can be used if the patient has also sustained a minor head injury
UHSM ED Pathway ELDERLY FALL / COLLAPSE Patient name / Pathway for patients who require assessment in ED after a fall or collapse Note: - It can be used if the patient has also sustained a minor head injury
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth. Objectives 11/7/2017
 Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE
 WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
Diagnostic modalities of the Central Nervous System
 NEURORADIOLOGY Kinga Karlinger, MD, PhD Associate Professor Semmelweis University, Budapest Diagnostic modalities of the Central Nervous System X-ray: screening is not used any more, x-ray images instead
NEURORADIOLOGY Kinga Karlinger, MD, PhD Associate Professor Semmelweis University, Budapest Diagnostic modalities of the Central Nervous System X-ray: screening is not used any more, x-ray images instead
Use of CT in minor traumatic brain injury. Lisa Ayoub-Rodriguez, MD Bert Johansson, MD Michael Lee, MD
 Use of CT in minor traumatic brain injury Lisa Ayoub-Rodriguez, MD Bert Johansson, MD Michael Lee, MD No financial or other conflicts of interest Epidemiology of traumatic brain injury (TBI) Risks associated
Use of CT in minor traumatic brain injury Lisa Ayoub-Rodriguez, MD Bert Johansson, MD Michael Lee, MD No financial or other conflicts of interest Epidemiology of traumatic brain injury (TBI) Risks associated
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
10/6/2017. Notice. Traumatic Brain Injury & Head Trauma
 Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
Neurology Clerkship Learning Objectives
 Neurology Clerkship Learning Objectives Clinical skills Perform a neurological screening examination of the cranial nerves, motor system, reflexes, and sensory system under the observation and guidance
Neurology Clerkship Learning Objectives Clinical skills Perform a neurological screening examination of the cranial nerves, motor system, reflexes, and sensory system under the observation and guidance
Workbook Answers Chapter 13. Neurologic Diseases and Conditions
 Workbook Answers Chapter 13 Neurologic Diseases and Conditions Short Answer 1. Afferent nerves transmit impulses from parts of the body to the spinal cord; efferent nerves transmit impulses away from the
Workbook Answers Chapter 13 Neurologic Diseases and Conditions Short Answer 1. Afferent nerves transmit impulses from parts of the body to the spinal cord; efferent nerves transmit impulses away from the
Brain and Central Nervous System Cancers
 Brain and Central Nervous System Cancers NICE guidance link: https://www.nice.org.uk/guidance/ta121 Clinical presentation of brain tumours History and Examination Consider immediate referral Management
Brain and Central Nervous System Cancers NICE guidance link: https://www.nice.org.uk/guidance/ta121 Clinical presentation of brain tumours History and Examination Consider immediate referral Management
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES
 TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
USASOC Neurocognitive Testing and Post Injury Evaluation and Treatment Clinical Practice Guideline (CPG)
") USASOC Neurocognitive Testing and Post Injury Evaluation and Treatment Clinical Practice Guideline (CPG) Note: The intent of this CPG is to serve as general guidance for medics and medical officers. It
USASOC Neurocognitive Testing and Post Injury Evaluation and Treatment Clinical Practice Guideline (CPG) Note: The intent of this CPG is to serve as general guidance for medics and medical officers. It
Marc Norman, Ph.D. - Do Not Use without Permission 1. Cerebrovascular Accidents. Marc Norman, Ph.D. Department of Psychiatry
 Cerebrovascular Accidents Marc Norman, Ph.D. Department of Psychiatry Neuropsychiatry and Behavioral Medicine Neuropsychology Clinical Training Seminar 1 5 http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/18009.jpg
Cerebrovascular Accidents Marc Norman, Ph.D. Department of Psychiatry Neuropsychiatry and Behavioral Medicine Neuropsychology Clinical Training Seminar 1 5 http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/18009.jpg
Management of Severe Traumatic Brain Injury
 Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Neurology. Access Center 24/7 access for referring physicians (866) 353-KIDS (5437)
 353-KIDS (5437)") Neurology The Neurology practice at Valley Children s provides diagnostic services, medical treatment, and followup care to infants, children, and adolescents who have suspected or confirmed neurological
Neurology The Neurology practice at Valley Children s provides diagnostic services, medical treatment, and followup care to infants, children, and adolescents who have suspected or confirmed neurological
Neurology Goals: Knowledge:
 Neurology Goals: A solid understanding of normal neurological development, anatomy and neurophysiology is imperative to the treatment of neurological pathology. The goal is to sensitize the family medicine
Neurology Goals: A solid understanding of normal neurological development, anatomy and neurophysiology is imperative to the treatment of neurological pathology. The goal is to sensitize the family medicine
North Oaks Trauma Symposium Friday, November 3, 2017
 Traumatic Intracranial Hemorrhage Aaron C. Sigler, DO, MS Neurosurgery Tulane Neurosciences None Disclosures Overview Anatomy Epidural hematoma Subdural hematoma Cerebral contusions Outline Traumatic ICH
Traumatic Intracranial Hemorrhage Aaron C. Sigler, DO, MS Neurosurgery Tulane Neurosciences None Disclosures Overview Anatomy Epidural hematoma Subdural hematoma Cerebral contusions Outline Traumatic ICH
The University of Arizona Pediatric Residency Program. Primary Goals for Rotation. Neurology
 The University of Arizona Pediatric Residency Program Primary Goals for Rotation Neurology 1. GOAL: Understand the role of the pediatrician in preventing neurological diseases, and in counseling and screening
The University of Arizona Pediatric Residency Program Primary Goals for Rotation Neurology 1. GOAL: Understand the role of the pediatrician in preventing neurological diseases, and in counseling and screening
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage. By: Shifaa AlQa qa
 CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage By: Shifaa AlQa qa Subarachnoid Hemorrhage Causes: Rupture of a saccular (berry) aneurysm Vascular malformation Trauma Hematologic disturbances
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage By: Shifaa AlQa qa Subarachnoid Hemorrhage Causes: Rupture of a saccular (berry) aneurysm Vascular malformation Trauma Hematologic disturbances
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Provide specific counseling to parents and patients with neurological disorders, addressing:
 Neurology Description: The Pediatric Neurology elective will give the resident the opportunity to learn how to obtain an appropriate history and perform a complete neurologic exam. Four to five half days
Neurology Description: The Pediatric Neurology elective will give the resident the opportunity to learn how to obtain an appropriate history and perform a complete neurologic exam. Four to five half days
Avoidable Imaging Learning Collaborative: 2008 Mild Traumatic Brain Injury Clinical Policy Success Story BWH Head and PE CTs with Clinical Decision
 Avoidable Imaging Learning Collaborative: 2008 Mild Traumatic Brain Injury Clinical Policy Success Story BWH Head and PE CTs with Clinical Decision Support Using the Canadian CT Head Rule to Reduce Unnecessary
Avoidable Imaging Learning Collaborative: 2008 Mild Traumatic Brain Injury Clinical Policy Success Story BWH Head and PE CTs with Clinical Decision Support Using the Canadian CT Head Rule to Reduce Unnecessary
Brief Clinical Report: Recognizing Subdural Hemorrhage in Older Adults
 Research Brief Clinical Report: Recognizing Subdural Hemorrhage in Older Adults Mark T. Pfefer, RN, MS, DC *1 ; Richard Strunk MS, DC 2 Address: 1 Professor and Director of Research, Cleveland Chiropractic
Research Brief Clinical Report: Recognizing Subdural Hemorrhage in Older Adults Mark T. Pfefer, RN, MS, DC *1 ; Richard Strunk MS, DC 2 Address: 1 Professor and Director of Research, Cleveland Chiropractic
Classical CNS Disease Patterns
 Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
5. Headache. and/or neck trauma. attributed to moderate. head injury. Glasgow Coma Scale x/15. ICHD II- Chaps 5&6 Posttraumatic and Vascular Headaches
 Diagnosis and Classification of Secondary Headaches Part 1 Posttraumatic and Vascular Morris Levin, MD Associate Professor of Medicine (Neurology) Associate Professor of Psychiatry Dartmouth Medical School
Diagnosis and Classification of Secondary Headaches Part 1 Posttraumatic and Vascular Morris Levin, MD Associate Professor of Medicine (Neurology) Associate Professor of Psychiatry Dartmouth Medical School
Traumatic Brain Injury Pathway, GCS 15 Closed head injury
 Traumatic Brain Injury Pathway, GCS 15 Closed head injury Plus Any One of the Following Mild TBI 2010 Consensus Definition of TBI from CDC, NINDS, NIDDR, VA, DVBIC, DCoE Plus Any One of the Following New
Traumatic Brain Injury Pathway, GCS 15 Closed head injury Plus Any One of the Following Mild TBI 2010 Consensus Definition of TBI from CDC, NINDS, NIDDR, VA, DVBIC, DCoE Plus Any One of the Following New
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Learning Objectives for Rotations in Vascular Surgery Year 3 Basic Clerkship
 Learning Objectives for Rotations in Vascular Surgery Year 3 Basic Clerkship CLINICAL PROBLEMS IN VASCULAR SURGERY 1. ABDOMINAL AORTIC ANEURYSM A 70 year old man presents in the emergency department with
Learning Objectives for Rotations in Vascular Surgery Year 3 Basic Clerkship CLINICAL PROBLEMS IN VASCULAR SURGERY 1. ABDOMINAL AORTIC ANEURYSM A 70 year old man presents in the emergency department with
8th Annual NKY TBI Conference 3/28/2014
 Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
CNS pathology Third year medical students. Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure
 CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
Neurosurgery. Neurosurgery
 Neurosurgery Neurosurgery Neurosurgery Telephone Numbers: Appointment: 202-476-3020 Fax: 202-476-3091 Administration: 202-476-3020 Evenings and Weekends: 202-476-5000 Robert Keating, MD, Chief The Division
Neurosurgery Neurosurgery Neurosurgery Telephone Numbers: Appointment: 202-476-3020 Fax: 202-476-3091 Administration: 202-476-3020 Evenings and Weekends: 202-476-5000 Robert Keating, MD, Chief The Division
Adult Neurology Residency Training Program McGill University Objectives of Training and Training Requirements. For Outpatient Neurology Clinics
 Neurology Residency Program Department of Neurology & Neurosurgery Postal address: Montreal Neurological Institute 3801 University Street Montreal, PQ, Canada H3A 2B4 Tel.: (514) 398-1904 Fax: (514) 398-4621
Neurology Residency Program Department of Neurology & Neurosurgery Postal address: Montreal Neurological Institute 3801 University Street Montreal, PQ, Canada H3A 2B4 Tel.: (514) 398-1904 Fax: (514) 398-4621
Nicolas Bianchi M.D. May 15th, 2012
 Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Chapter 15. Neurologic Emergencies
 Chapter 15 Neurologic Emergencies Introduction (1 of 4) Stroke is the third leading cause of death in the United States. After heart disease and cancer It is common in geriatric patients. More men than
Chapter 15 Neurologic Emergencies Introduction (1 of 4) Stroke is the third leading cause of death in the United States. After heart disease and cancer It is common in geriatric patients. More men than
Spasm of the extracranial internal carotid artery resulting from blunt trauma demonstrated by angiography
 Spasm of the extracranial internal carotid artery resulting from blunt trauma demonstrated by angiography Case report ELISHA S. GURDJIAN, M.D., BLAISE AUDET, M.D., RENATO W. SIBAYAN, M.D., AND LLYWELLYN
Spasm of the extracranial internal carotid artery resulting from blunt trauma demonstrated by angiography Case report ELISHA S. GURDJIAN, M.D., BLAISE AUDET, M.D., RENATO W. SIBAYAN, M.D., AND LLYWELLYN
Subarachnoid Hemorrhage (SAH) Disclosures/Relationships. Click to edit Master title style. Click to edit Master title style.
 Disclosures/Relationships. Click to edit Master title style. Click to edit Master title style.") Subarachnoid Hemorrhage (SAH) William J. Jones, M.D. Assistant Professor of Neurology Co-Director, UCH Stroke Program Click to edit Master title style Disclosures/Relationships No conflicts of interest
Subarachnoid Hemorrhage (SAH) William J. Jones, M.D. Assistant Professor of Neurology Co-Director, UCH Stroke Program Click to edit Master title style Disclosures/Relationships No conflicts of interest
Neurosurgical Management of Stroke
 Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
It s Always a Stroke; Except For When It s Not..
 It s Always a Stroke; Except For When It s Not.. TREVOR PHINNEY, D.O. Disclosures No Relevant Disclosures 1 Objectives Discuss variables of differential diagnosis for stroke Review when to TPA and when
It s Always a Stroke; Except For When It s Not.. TREVOR PHINNEY, D.O. Disclosures No Relevant Disclosures 1 Objectives Discuss variables of differential diagnosis for stroke Review when to TPA and when
PEDIATRIC BRAIN CARE
 PEDIATRIC BRAIN CARE The brain matters most! OVERVIEW OF NEURO ASSESSMENT 1. Overall responsiveness/activity 2. The eyes 3.? Increased ICP 4. Movements 5.? Seizures 6. Other OVERALL RESPONSIVENESS/ ACTIVITY
PEDIATRIC BRAIN CARE The brain matters most! OVERVIEW OF NEURO ASSESSMENT 1. Overall responsiveness/activity 2. The eyes 3.? Increased ICP 4. Movements 5.? Seizures 6. Other OVERALL RESPONSIVENESS/ ACTIVITY
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 04/26/2014 Radiology Quiz of the Week # 108 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 04/26/2014 Radiology Quiz of the Week # 108 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Subspecialty Rotation: Child Neurology at SUNY (KCHC and UHB) Residents: Pediatric residents at the PL1, PL2, PL3 level
 Residents: Pediatric residents at the PL1, PL2, PL3 level") Subspecialty Rotation: Child Neurology at SUNY (KCHC and UHB) Residents: Pediatric residents at the PL1, PL2, PL3 level Prerequisites: Any prior pediatric rotations and experience Primary Goals for this
Subspecialty Rotation: Child Neurology at SUNY (KCHC and UHB) Residents: Pediatric residents at the PL1, PL2, PL3 level Prerequisites: Any prior pediatric rotations and experience Primary Goals for this
PEDIATRIC MILD TRAUMATIC HEAD INJURY
 PEDIATRIC MILD TRAUMATIC HEAD INJURY October 2011 Quality Improvement Resources Illinois Emergency Medical Services for Children is a collaborative program between the Illinois Department of Public Health
PEDIATRIC MILD TRAUMATIC HEAD INJURY October 2011 Quality Improvement Resources Illinois Emergency Medical Services for Children is a collaborative program between the Illinois Department of Public Health
Cerebral Vascular Diseases. Nabila Hamdi MD, PhD
 Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
Stroke Transfer Checklist
 Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes
 and Non- Aneurysmal Causes") Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
High Yield Neurological Examination
 High Yield Neurological Examination Vanja Douglas, MD Sara & Evan Williams Foundation Endowed Neurohospitalist Chair Director, Neurohospitalist Division Associate Professor of Clinical Neurology UCSF Department
High Yield Neurological Examination Vanja Douglas, MD Sara & Evan Williams Foundation Endowed Neurohospitalist Chair Director, Neurohospitalist Division Associate Professor of Clinical Neurology UCSF Department
NEUROSURGICAL EMERGENCY GUIDELINE DEVELOPMENT GROUP P3 NEURO CENTER OF NEUROSCIENCE RESEARCH AND SERVICE USM
 NEUROSURGICAL EMERGENCY GUIDELINE DEVELOPMENT GROUP P3 NEURO CENTER OF NEUROSCIENCE RESEARCH AND SERVICE USM Chairperson Professor Dr Zamzuri Idris Head of Department Members Associate Professor Dato Dr
NEUROSURGICAL EMERGENCY GUIDELINE DEVELOPMENT GROUP P3 NEURO CENTER OF NEUROSCIENCE RESEARCH AND SERVICE USM Chairperson Professor Dr Zamzuri Idris Head of Department Members Associate Professor Dato Dr
TIA: Updates and Management 2008
 TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
Imaging of Acute Cerebral Trauma
 July, 2005 Imaging of Acute Cerebral Trauma Louis Rivera, Harvard Medical School, Year III 46 y/o Female s/p Trauma - Unrestrained? MVC requiring Med Flight - Facial bruising/swelling - DEEP COMA - SEIZURES
July, 2005 Imaging of Acute Cerebral Trauma Louis Rivera, Harvard Medical School, Year III 46 y/o Female s/p Trauma - Unrestrained? MVC requiring Med Flight - Facial bruising/swelling - DEEP COMA - SEIZURES
Single Seizure of Unknown Cause
 S1: Medical Standards for Safety Critical Workers with Seizures of Unknown Cause 1. Seizure or Epilepsy of Unknown Cause are the classifications used in these medical standards for a probable seizure(s),
S1: Medical Standards for Safety Critical Workers with Seizures of Unknown Cause 1. Seizure or Epilepsy of Unknown Cause are the classifications used in these medical standards for a probable seizure(s),
Pediatric Head Trauma August 2016
 PEDIATRIC HEAD TRAUMA AUGUST 2016 Pediatric Head Trauma August 2016 EDUCATION COMMITTEE PEER EDUCATION Quick Review of Pathophysiology of TBI Nuggets of knowledge to keep in mind with TBI Intracranial
PEDIATRIC HEAD TRAUMA AUGUST 2016 Pediatric Head Trauma August 2016 EDUCATION COMMITTEE PEER EDUCATION Quick Review of Pathophysiology of TBI Nuggets of knowledge to keep in mind with TBI Intracranial
Anticoagulants and Head Injuries. Asaad Shujaa,MD,FRCPC,FAAEM Assistant Professor,weill Corneal Medicne Senior Consultant,HMC Qatar
 Anticoagulants and Head Injuries Asaad Shujaa,MD,FRCPC,FAAEM Assistant Professor,weill Corneal Medicne Senior Consultant,HMC Qatar Common Anticoagulants and Indications Coumadin (warfarin) indicated for
Anticoagulants and Head Injuries Asaad Shujaa,MD,FRCPC,FAAEM Assistant Professor,weill Corneal Medicne Senior Consultant,HMC Qatar Common Anticoagulants and Indications Coumadin (warfarin) indicated for
What Do You Think of My Posterior?
 What Do You Think of My Posterior? Posterior Stroke and Stroke Mimics Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School of Medicine Disclosures
What Do You Think of My Posterior? Posterior Stroke and Stroke Mimics Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School of Medicine Disclosures
Acute stroke imaging
 Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Med 536 Communicating About Prognosis Workshop. Case 1
 Med 536 Communicating About Prognosis Workshop Case 1 ID / CC: 39 year-old woman status-post motor-vehicle collision History of the Presenting Illness Previously healthy 39 year-old woman was found in
Med 536 Communicating About Prognosis Workshop Case 1 ID / CC: 39 year-old woman status-post motor-vehicle collision History of the Presenting Illness Previously healthy 39 year-old woman was found in
Stroke Workshop. Pre-Workshop Handout. With Walter Himmel, Meeta Patel & Anton Helman
 2018 Stroke Workshop Pre-Workshop Handout With Walter Himmel, Meeta Patel & Anton Helman Instructions for Getting the Most Out of The EMU Stroke Workshop Handout This workshop has been designed around
2018 Stroke Workshop Pre-Workshop Handout With Walter Himmel, Meeta Patel & Anton Helman Instructions for Getting the Most Out of The EMU Stroke Workshop Handout This workshop has been designed around
FORM ID. Patient's Personal Details. SECTION A : Medical Record of the Patient. Name. Policy Number. NRIC/Old IC/Passport/Birth Cert/Others
 CRITICAL ILLNESS CLAIM - DOCTOR'S STATEMENT Brain and Nerve Related Conditions Note: This form is to be completed at the Patient s expense by the Attending Physician/ Surgeon who treated the patient. Patient's
CRITICAL ILLNESS CLAIM - DOCTOR'S STATEMENT Brain and Nerve Related Conditions Note: This form is to be completed at the Patient s expense by the Attending Physician/ Surgeon who treated the patient. Patient's
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Coastal Carolina University Athletic Training Department Policy and Procedure Manual Concussion Management Revised/Reviewed 6/2012
 Coastal Carolina University Athletic Training Department Policy and Procedure Manual Concussion Management Revised/Reviewed 6/2012 INTRODUCTION: Concussion classification, management, and protocols have
Coastal Carolina University Athletic Training Department Policy and Procedure Manual Concussion Management Revised/Reviewed 6/2012 INTRODUCTION: Concussion classification, management, and protocols have
Central nervous system
 Central nervous system By Dr. Mohsen Dashti Clinical Medicine & Pathology 316 7 th Lecture Lecture outline Review of structure & function. Symptoms, signs & tests. Specific diseases. Review of structure
Central nervous system By Dr. Mohsen Dashti Clinical Medicine & Pathology 316 7 th Lecture Lecture outline Review of structure & function. Symptoms, signs & tests. Specific diseases. Review of structure
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Introduction to Emergency Medical Care 1
 Introduction to Emergency Medical Care 1 OBJECTIVES 31.1 Define key terms introduced in this chapter. Slides 13 15, 17, 19, 28 31.2 Describe the components and function of the nervous system and the anatomy
Introduction to Emergency Medical Care 1 OBJECTIVES 31.1 Define key terms introduced in this chapter. Slides 13 15, 17, 19, 28 31.2 Describe the components and function of the nervous system and the anatomy
TIAs and posterior circulation problems
 TIAs and posterior circulation problems A/Professor Helen Dewey Head, Stroke Service Austin Health Austin Health How many strokes and TIAs are out there? depends on the definition! ~60,000 strokes in
TIAs and posterior circulation problems A/Professor Helen Dewey Head, Stroke Service Austin Health Austin Health How many strokes and TIAs are out there? depends on the definition! ~60,000 strokes in
Integrated University Study, Medicine. Credits (ECTS) : 7 Semester VII Number of hours per semester (l+e+s) Passed all exams of the 3 rd year
 : 7 Semester VII Number of hours per semester (l+e+s) Passed all exams of the 3 rd year") Name of the course Neurology Code Type of study program Cycle Integrated University Study, Medicine Year of study IV Credits (ECTS) : 7 Semester VII Number of hours per semester (l+e+s) 100 (27+25+48)
Name of the course Neurology Code Type of study program Cycle Integrated University Study, Medicine Year of study IV Credits (ECTS) : 7 Semester VII Number of hours per semester (l+e+s) 100 (27+25+48)
Neuroimaging of TBI: Current Clinical Guidelines and Future Direction Brain Injury Alliance of Colorado 2017
 Neuroimaging of TBI: Current Clinical Guidelines and Future Direction Brain Injury Alliance of Colorado 2017 Peter E. Ricci, M.D. Staff Neuroradiologist Radiology Imaging Associates OBJECTIVES 1. Understand
Neuroimaging of TBI: Current Clinical Guidelines and Future Direction Brain Injury Alliance of Colorado 2017 Peter E. Ricci, M.D. Staff Neuroradiologist Radiology Imaging Associates OBJECTIVES 1. Understand
Pre-Hospital Stroke Care: Bringing It To The Street. by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center
 Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
McCance: Pathophysiology, 6th Edition
 McCance: Pathophysiology, 6th Edition Chapter 17: Disorders of the Central and Peripheral Nervous Systems and the Neuromuscular Junction Key Points Print SUMMARY REVIEW Central Nervous System Disorders
McCance: Pathophysiology, 6th Edition Chapter 17: Disorders of the Central and Peripheral Nervous Systems and the Neuromuscular Junction Key Points Print SUMMARY REVIEW Central Nervous System Disorders
Injuries to the head and spine
 Injuries to the head and spine Aaron J. Katz, AEMT-P, CIC www.es26medic.net 2013 Nervous System Two sub-systems Central Nervous System ( CNS ) Brain and spinal cord Peripheral Nervous System 12 cranial
Injuries to the head and spine Aaron J. Katz, AEMT-P, CIC www.es26medic.net 2013 Nervous System Two sub-systems Central Nervous System ( CNS ) Brain and spinal cord Peripheral Nervous System 12 cranial
Traumatic Brain Injury
 General Information Traumatic Brain Injury What you need to know Complicated condition with high variability in etiology, severity, distribution of injury, and pattern of functional impairment (Klyce,
General Information Traumatic Brain Injury What you need to know Complicated condition with high variability in etiology, severity, distribution of injury, and pattern of functional impairment (Klyce,
InterQual Level of Care 2018 Index
 InterQual Level of Care 2018 Index Rehabilitation Criteria Index Words by Subset The Index is an alphabetical listing of conditions and/or diagnoses designed to guide the user to the criteria subset where
InterQual Level of Care 2018 Index Rehabilitation Criteria Index Words by Subset The Index is an alphabetical listing of conditions and/or diagnoses designed to guide the user to the criteria subset where
Date of Admission: [DATE]. Date of Discharge:
![Date of Admission: [DATE]. Date of Discharge:](/thumbs/74/71277118.jpg "Date of Admission: [DATE]. Date of Discharge:") Date of Admission: [DATE]. Date of Discharge: History of Present Illness: Mr. [NAME] AKA [NAME] is a 31-year-old male who presents to the [PLACE] Trauma Surgery Service as a moderate trauma on [DATE] following
Date of Admission: [DATE]. Date of Discharge: History of Present Illness: Mr. [NAME] AKA [NAME] is a 31-year-old male who presents to the [PLACE] Trauma Surgery Service as a moderate trauma on [DATE] following
Instructional Course #34. Review of Neuropharmacology in Pediatric Brain Injury. John Pelegano MD Jilda Vargus-Adams MD, MSc Micah Baird MD
 Instructional Course #34 Review of Neuropharmacology in Pediatric Brain Injury John Pelegano MD Jilda Vargus-Adams MD, MSc Micah Baird MD Outline of Course 1. Introduction John Pelegano MD 2. Neuropharmocologic
Instructional Course #34 Review of Neuropharmacology in Pediatric Brain Injury John Pelegano MD Jilda Vargus-Adams MD, MSc Micah Baird MD Outline of Course 1. Introduction John Pelegano MD 2. Neuropharmocologic
Head injuries in children. Dr Jason Hort Paediatrician Paediatric Emergency Physician, June 2017 Children s Hospital Westmead
 Head injuries in children Dr Jason Hort Paediatrician Paediatric Emergency Physician, June 2017 Children s Hospital Westmead Objectives Approach to minor head injury Child protection issues Concussion
Head injuries in children Dr Jason Hort Paediatrician Paediatric Emergency Physician, June 2017 Children s Hospital Westmead Objectives Approach to minor head injury Child protection issues Concussion
Clinical Policy: Evoked Potential Testing
 Clinical Policy: Evoked Potential Testing Reference Number: PA.CP.MP.134 Last Review Date: 09/18 Effective Date: 09/18 Coding Implications Revision Log Description Evoked potentials evaluate electrical
Clinical Policy: Evoked Potential Testing Reference Number: PA.CP.MP.134 Last Review Date: 09/18 Effective Date: 09/18 Coding Implications Revision Log Description Evoked potentials evaluate electrical
The central nervous system
 Sectc.qxd 29/06/99 09:42 Page 81 Section C The central nervous system CNS haemorrhage Subarachnoid haemorrhage Cerebral infarction Brain atrophy Ring enhancing lesions MRI of the pituitary Multiple sclerosis
Sectc.qxd 29/06/99 09:42 Page 81 Section C The central nervous system CNS haemorrhage Subarachnoid haemorrhage Cerebral infarction Brain atrophy Ring enhancing lesions MRI of the pituitary Multiple sclerosis
PROPOSAL FOR MULTI-INSTITUTIONAL IMPLEMENTATION OF THE BRAIN INJURY GUIDELINES
 PROPOSAL FOR MULTI-INSTITUTIONAL IMPLEMENTATION OF THE BRAIN INJURY GUIDELINES INTRODUCTION: Traumatic Brain Injury (TBI) is an important clinical entity in acute care surgery without well-defined guidelines
PROPOSAL FOR MULTI-INSTITUTIONAL IMPLEMENTATION OF THE BRAIN INJURY GUIDELINES INTRODUCTION: Traumatic Brain Injury (TBI) is an important clinical entity in acute care surgery without well-defined guidelines