Neuroimaging of TBI: Current Clinical Guidelines and Future Direction Brain Injury Alliance of Colorado 2017
|
|
|
- Patience Burke
- 6 years ago
- Views:
Transcription


1 Neuroimaging of TBI: Current Clinical Guidelines and Future Direction Brain Injury Alliance of Colorado 2017 Peter E. Ricci, M.D. Staff Neuroradiologist Radiology Imaging Associates
2 OBJECTIVES 1. Understand when CT is appropriate for imaging patients with traumatic brain injury (TBI) 2. Understand how and when conventional MR imaging is used to evaluate TBI patients 3. Understand how some of the newer imaging techniques are being applied to the evaluation of the TBI patient, particularly in the setting of mild TBI (MTBI)
3 IMAGING MODALITIES Diagnostic X-ray Computed tomography (CT) Including CT angiography Magnetic resonance (MR) imaging Including MR angiography Positron Emission Tomography (PET) Single photon emission computed tomography (SPECT) In-111 DTPA cisternography suspected CSF leak Ultrasound (transcranial doppler) Magnetoencephalography
4 THE MAIN ISSUE? CT OR MR
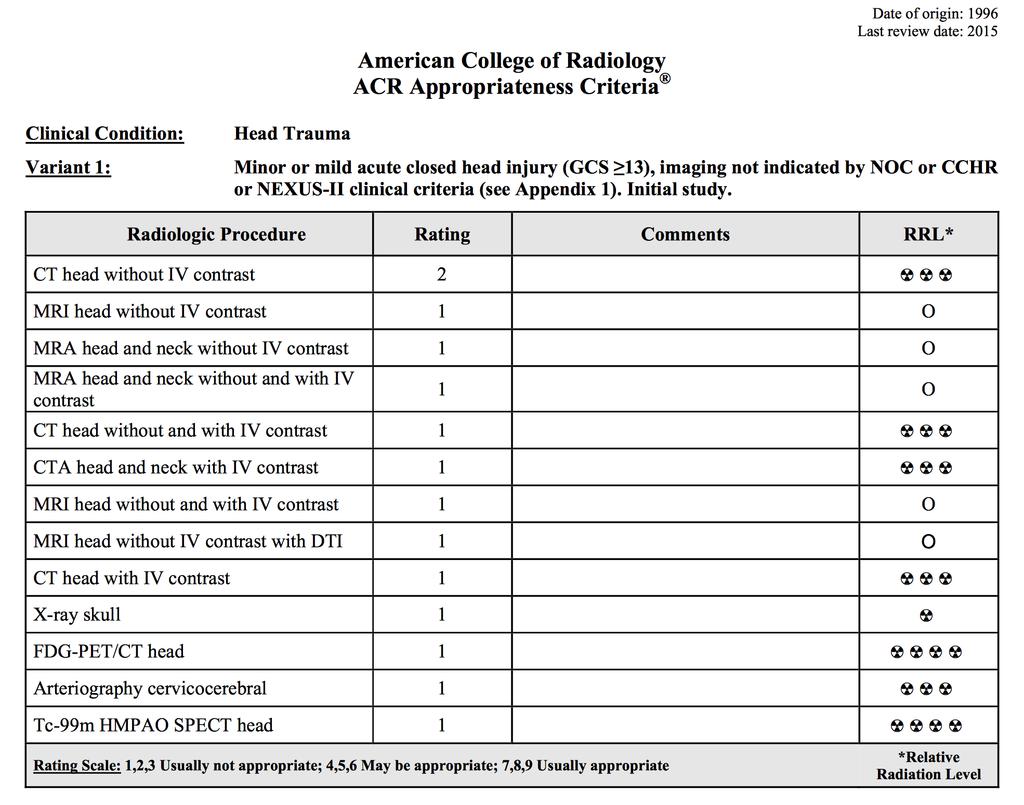
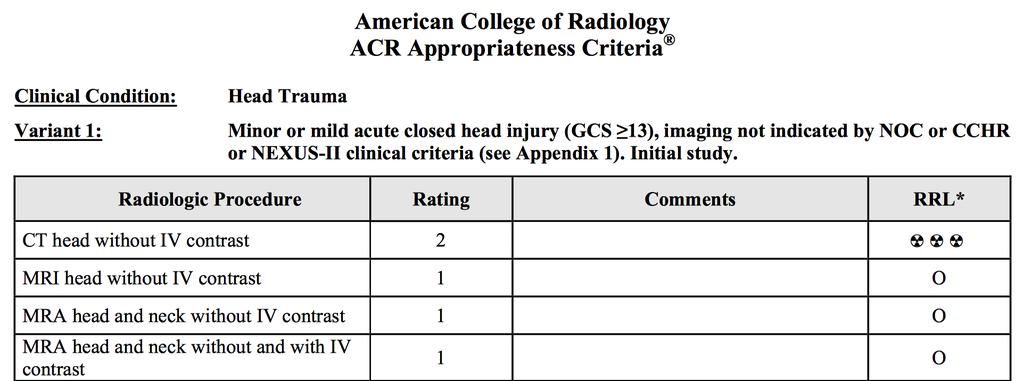
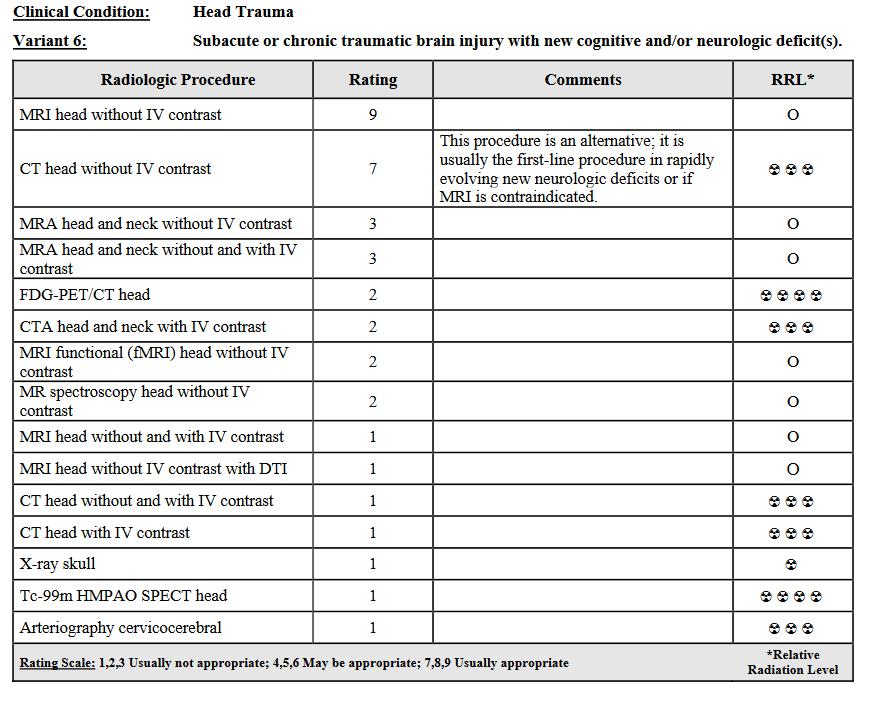
5 A NOTE ABOUT UTILIZATION Knowing when not to image is as important as knowing when to image and with what test ACR Appropriateness Criteria: guidelines designed to help providers select the best imaging test for a specific clinical condition grades imaging studies from 1 > 9 (not > usually appropriate) based on a thorough literature review which is updated periodically Literature cited in 2015 head trauma review included 61 level 1-4 studies published in the literature from Shetty VS, et al. ACR Appropriateness Criteria Head Trauma. Available at American College of Radiology. Accessed Apr 28, 2017.

6
7 UTILIZATION NOC, CCHR, NEXUS II: clinical guidelines used to identify patients with mild acute CHI who can safely avoid imaging CCHR - CT is not required if ALL of the following are met: GCS >15 at 2 hours post-injury No suspected open or depressed skull fracture No sign of basilar skull fracture (hemotympanum, raccoon eye, CSF otorrhea or rhinorrhea, Battle sign) Less than two episodes of vomiting Age <65 years No amnesia before impact 30 minutes, No dangerous mechanism (pedestrian struck by MV, ejection from MV, fall from elevation <3 feet or <5 steps)
8 UTILIZATION Prospective multicenter study comparing the Canadian CT Head Rule (CCHR) and the New Orleans Criteria (NOC) 1,822 patients with GCS of 15; 8 (0.4%) required neurosurgical intervention and 97 (5.3%) had a clinically important brain injury. Both the NOC and the CCHR were 100% sensitive CCHR was more specific for predicting both the need for neurosurgical intervention (76.3% vs 12.1%) and the presence of clinically important brain injury (50.6% vs 12.7%) CCHR would have resulted in lower CT rates (52% vs 88%) Stiell IG, et al. JAMA 2005; 294(12):
9 CT
10 ADVANTAGES OF CT Readily available at virtually all acute care facilities. Extremely fast (< 5s for 16/32/64/128/256 slice scanners). Highly sensitive and specific for identifying actionable lesions: Intracranial hemorrhage (epidural, subdural, subarachnoid, parenchymal, and intraventicular) Intracranial mass effect & herniation Depressed skull fractures And, a negative head CT effectively excludes the likelihood of significant injury that would require early intervention
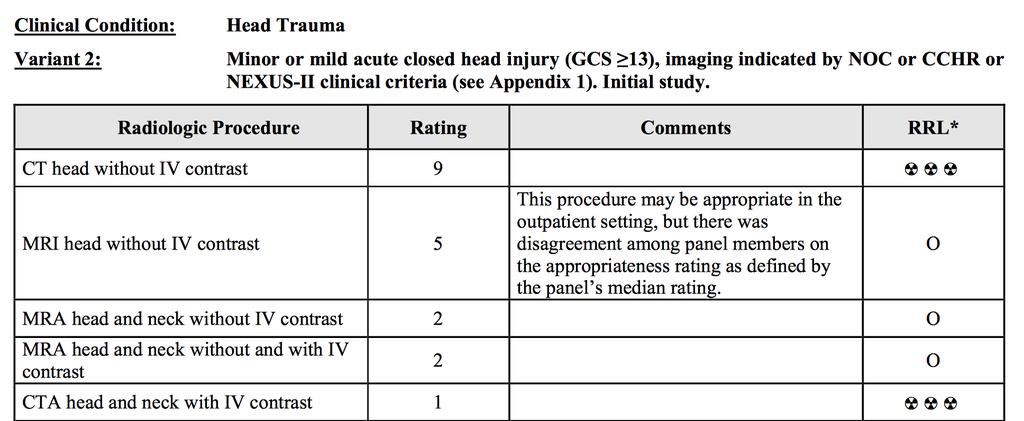
11 IMAGING OF ACUTE TBI CT is appropriate for acute TBI evaluation in the following situations: Mild closed head injury in which imaging is indicated by NOC or CCHR or NEXUS-II criteria Any moderate or severe acute closed head injury (GCS <13) Any penetrating injury, but stable and neurologically intact A known or suspected skull fracture For suspected vascular injury: CTA and MRA (in combo with CT or MR) are equally efficacious we typically use CTA due to 24/7 availability, speed, cost Shetty VS, et al. ACR Appropriateness Criteria Head Trauma. Available at American College of Radiology. Accessed Apr 28, 2017.
12
13 EFFICACY OF SCREENING CT 2766 pts with isolated mild head injury 1170 pts had normal CT; none required craniotomy 2112 pts had normal neuro exam; 59 (~3%) required surgery CT sensitivity was 100%; NPV 100% CT alone would have saved 3924 hospital days, 814 ICU days, and $1.5M in hospital charges Shackford SR, et al. J Trauma 1992 Sep;33(3):385-94
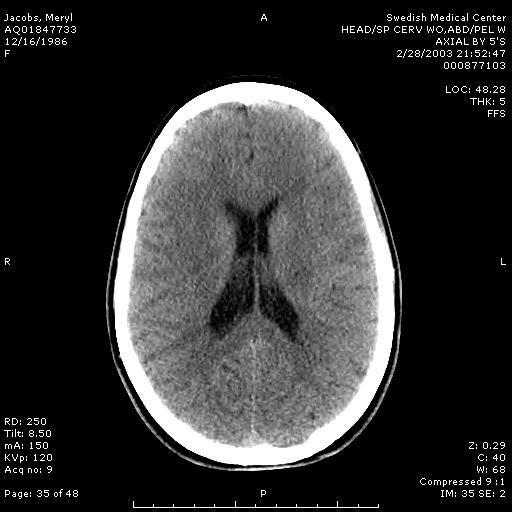
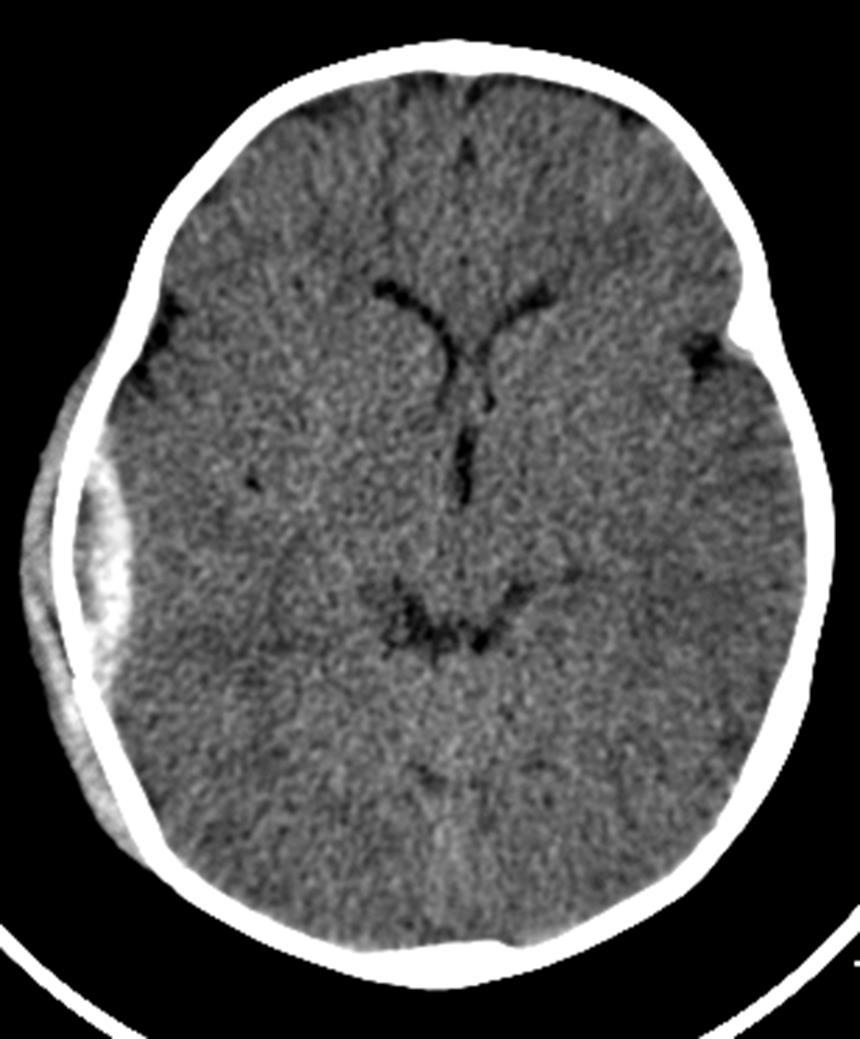
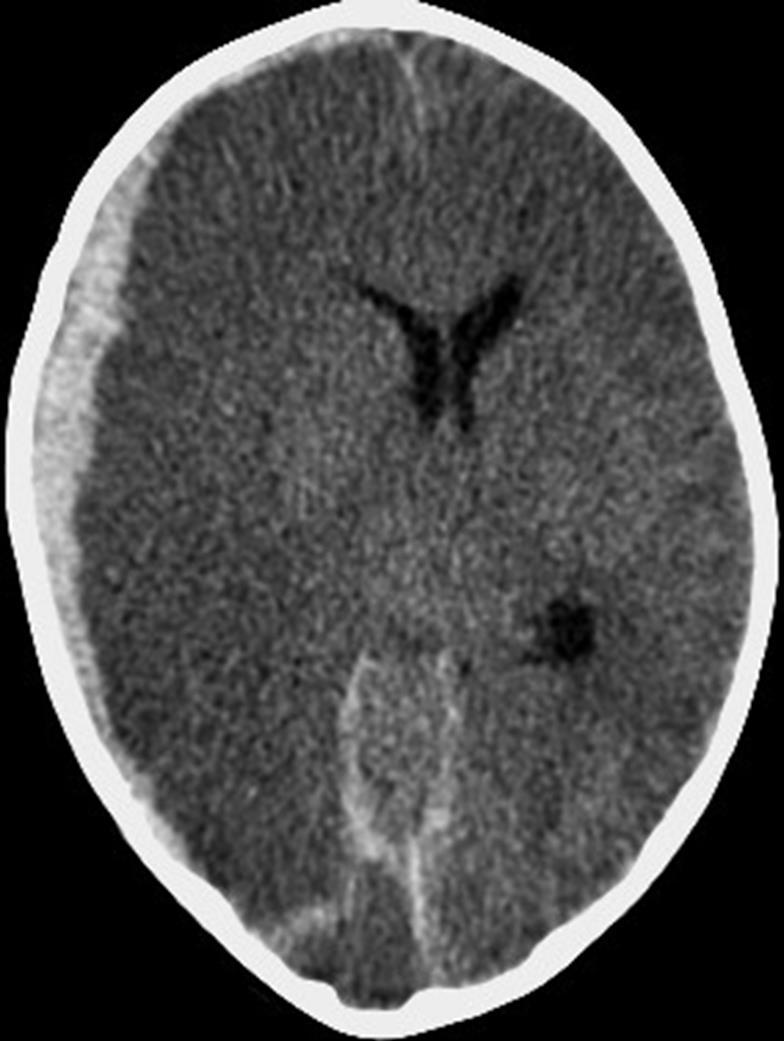
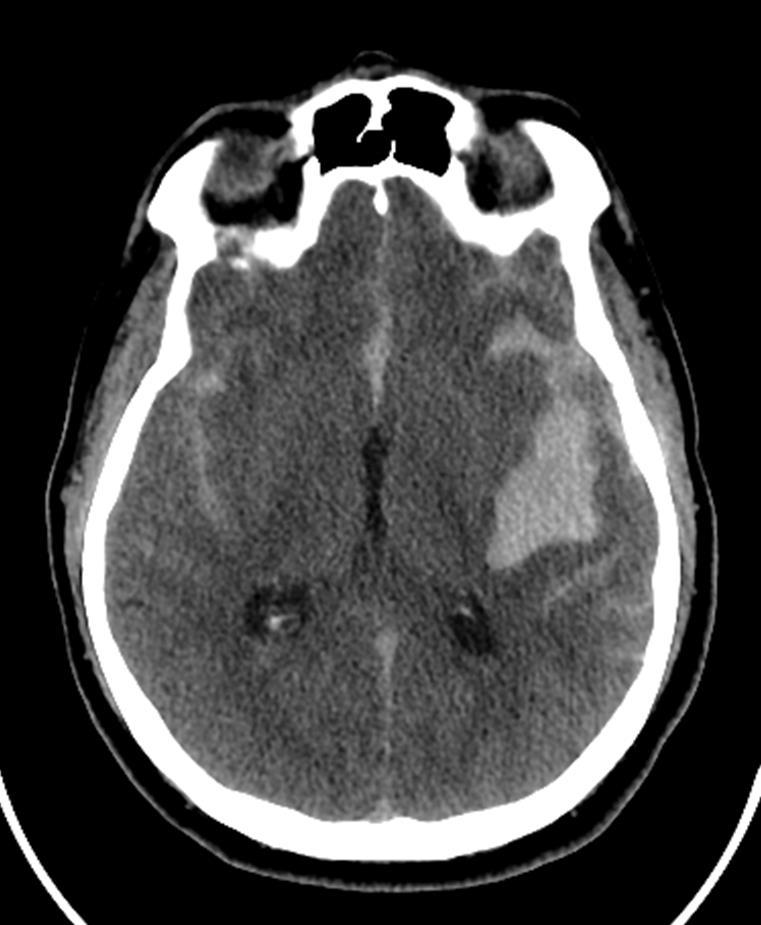
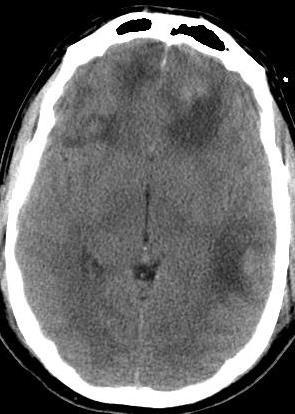
14 WHAT DO WE LOOK FOR 4 key things: blood, contusions, mass effect, fractures Findings that correlate with poor outcome: Traumatic subarachnoid hemorrhage Large and/or multiple hematomas Diffuse hemispheric swelling Effacement of the basilar cisterns Midline shift Brainstem injury d'avella D, et al. Neurosurgery 2002 Jan;50(1):16-25 Firsching R, et al. Acta Neurochir (Wien) 2001;143(3): Eisenberg HM, et al. J Neurosurg 1990 Nov;73(5):688-98
15

16
17
18


19

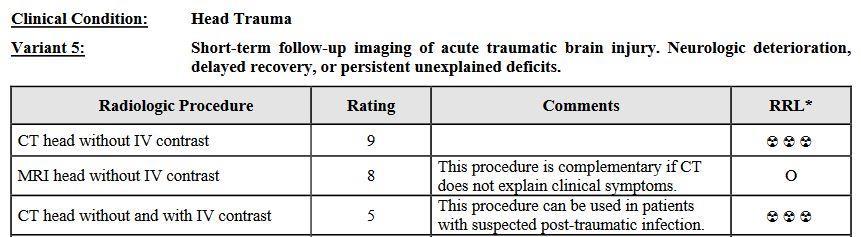
20 SHORT TERM FOLLOW-UP


21
22 TAKE HOME POINTS 1 1. CCHR and NOC can be used to reduce inappropriate use of head CT's in the setting of acute trauma. 2. CT remains the preferred imaging test for the initial evaluation of acute TBI because its fast & it readily identifies abnormalities that require urgent medical attention or surgical intervention. 3. A negative head CT effectively rules out an injury that needs surgical intervention

23 MR IMAGING
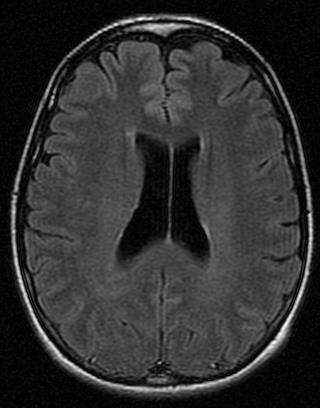
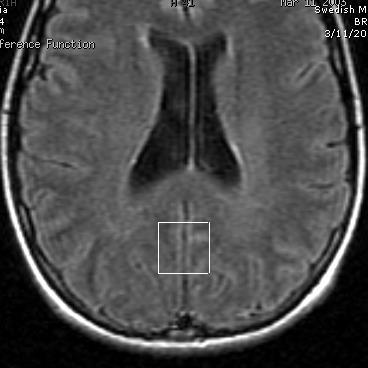
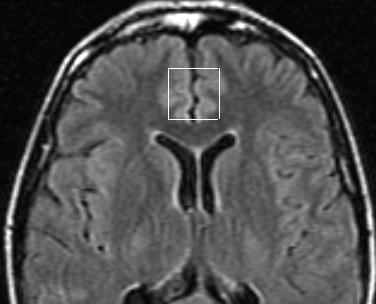
24 MR IMAGING MR s superior soft-tissue contrast makes it better for detecting: non-hemorrhagic lesions (contusions) hemorrhagic lesions (including DAI) any secondary effects of trauma (such as edema and HIE) Also better for frontal lobe, temporal lobe & brainstem injuries 2015 ACR Appropriateness Criteria MR is the study of choice in the subacute or chronic phase of closed head injury with new or persistent cognitive and/or neurologic deficit(s) not explained by CT Shetty VS, et al. ACR Appropriateness Criteria Head Trauma. Available at American College of Radiology. Accessed Apr 28, 2017.

25 CT FSE T2 FLAIR

26 CT FSE T2 FLAIR
27
28
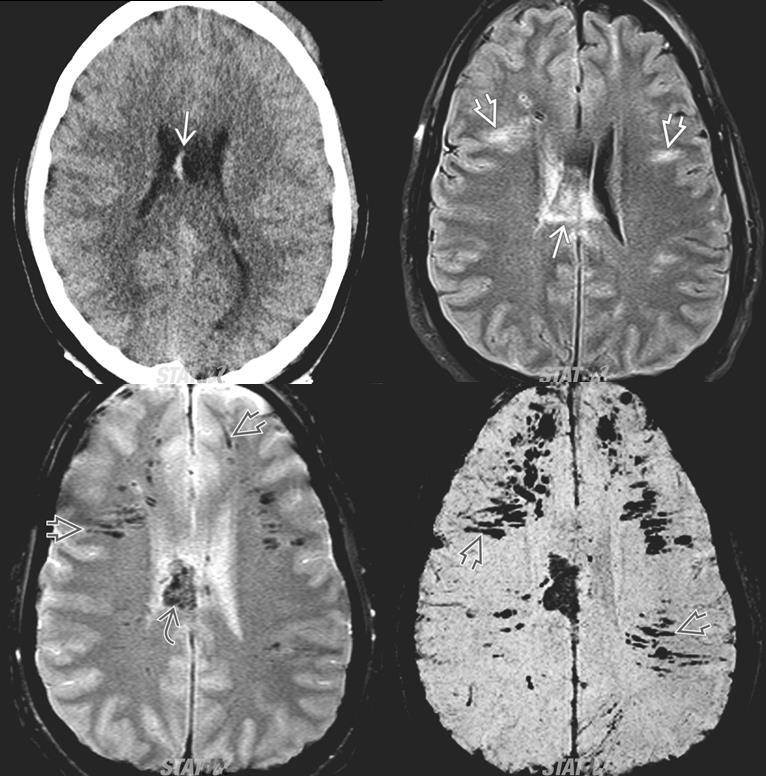
29 C T FSE T2 T2* GRE 27 y M. skier hit tree
30 T2W T2* GE
31 MR CORRELATION WITH SEVERITY T2* GE findings correlate with GCS and PTA; T2 SE findings better predicts TFC Lesion depth on MR correlates with degree/duration of impaired consciousness and initial GCS Lesions on T2* gradient-echo images correlate with duration of impaired consciousness Significant differences have been found on neuropsych testing in mild TBI between pts with traumatic MR lesions and those without Levin HS, et al. Neurosurgery 1997 Mar;40(3): Grados MA, et al. J Neurol Neurosurg Psychiatry 2001 Mar;70(3):350-8 Yanagawa Y, et al. J Trauma 2000 Aug;49(2):272-7 Kurca E, et al. Neuroradiology 2006, 48:
32 MR CORRELATION WITH OUTCOME Lesion depth correlates with disability at discharge from rehab and with outcome at 1y and 3y. Lesions on T2* gradient-echo images correlate w/ GOS at 3 mo. Traumatic callosal and dorsolateral brainstem lesions predict poor recovery. Kampfl A, et al. Lancet 1998 Jun 13; 351(9118): MacKenzie JD, et al. AJNR 2002 Oct; 23:
33 TAKE HOME POINTS 2 Superior contrast resolution makes MR the preferred imaging tool for identifying the extent of TBI and its complications (shear injury, ischemia, etc). MR imaging of TBI must include GRE or SWI to optimally detect shear injury
34 ANATOMIC IMAGING PROBLEM Based on animal studies, we know that pathologic/metabolic changes occur even in mild TBI, and those with persistent metabolic changes are at risk for second impact syndrome 1 Despite that, 43% to 68% of MTBI patients have normal conventional MR scans despite neuropsychological or clinical impairment (the post-concussive syndrome ) 2,3 Annually, mild TBI represents 75-90% of all head injuries, and accounts for ~ 44% of the $56B cost of TBI in the US 4,5 1. Longhi L, et al. Neurosurgery 2005 Feb;56(2): Hofman PA, et al: Am J Neuroradiol 2001; 22: Hughes DG, et al: Neuroradiology 2004; 46: Signoretti S, et al. Neurosurg Focus. 2010;29(5): Thurman DJ. Head Trauma: Basic, Preclinical, and Clinical Directions. Edited by Miller L, Hayes R. New York, John Wiley & Sons, 2001, pp
35 ANATOMIC IMAGING PROBLEM TBI is not a single pathophysiological process. There are: Subcellular events: calcium-mediated excitotoxicity, mitochondrial dysfunction, apoptotic cell death Cellular level events: breakdown of the axonal cytoskeleton, cytotoxic edema Macroscopic events: mass effect related to intra- or extra-axial hematomas, vascular compromise leading to ischemia Psychological issues Expecting a macroscopic anatomic imaging technique to sort all this out isn t realistic
36
37
38 TOOLS MR Techniques Diffusion-weighted imaging evaluates cellular swelling Diffusion tensor imaging evaluates tissue microstructure Spectroscopy evaluates physiology (chemistry) Functional MR evaluates blood flow as a surrogate for neuronal function SPECT imaging evaluates physiology (blood flow) PET imaging evaluates physiology (metabolism), function US Transcranial doppler evaluates blood flow
39 ACR APPROPRIATENESS CRITERIA Advanced imaging techniques (perfusion CT, perfusion MRI, SPECT, and PET) may be appropriate in selected cases Those techniques are not considered routine clinical practice at this time
40 DIFFUSION TENSOR IMAGING (DTI) DTI evaluates the directional diffusion of water molecules along the structural cytoskeleton (axolemma, microtubules, neurofilaments, and myelin sheaths). Diseases which disrupt axons or the cytoskeleton alter the pattern of diffusivity (water motion becomes less restricted) As a result, DTI allows us to assess changes in microstructural integrity (including injury related to diffuse axonal injury).
41
42
43 43yo M with traumatic brain injury
44 Predominant regions of DTI injury include: inferior longitudinal fasciculus (21%), uncinate fasciculus (29%), genu of the corpus callosum (21%), anterior corona radiata (41%), and cingulum bundle (18%). Niogi S et al. AJNR Am J Neuroradiol 2008; 29:
45 MR SPECTROSCOPY MR imaging technique that produces a map of cerebral metabolites Metabolite Evaluates Change in MTBI NAA Neuronal integrity decr Cr Cellular energy metabolism decr Cho Cellular turnover incr Lactate Anaerobic glycolysis present Myo-Inositol Astroglial proliferation incr

46 Hunter s line Normal MR Spectrum

47 MR Spectrum in TBI
48

49

50
51
52 TAKE HOME POINTS 3 Physiologic/functional techniques can provide insight into brain microstructure and function. They detect changes not demonstrated on conventional MR and CT and thus show promise as more sensitive tools for the detection of TBI. However, research data to date are insufficient to draw widespread conclusions, so more research is needed.
53 CONCLUSIONS CT: preferred imaging tool in the acute setting to triage TBI patients and identify lesions that require urgent surgery. MRI: preferred imaging tool to define the extent of TBI and identify shear injury, contusion, etc. Functional/physiologic techniques: provide insight into brain microstructure / function and may ultimately improve our ability to better characterize the extent of injury and predict outcome

54
Laura Tormoehlen, M.D. Neurology and EM-Toxicology Indiana University
 Laura Tormoehlen, M.D. Neurology and EM-Toxicology Indiana University Disclosures! No conflicts of interest to disclose Neuroimaging 101! Plain films! Computed tomography " Angiography " Perfusion! Magnetic
Laura Tormoehlen, M.D. Neurology and EM-Toxicology Indiana University Disclosures! No conflicts of interest to disclose Neuroimaging 101! Plain films! Computed tomography " Angiography " Perfusion! Magnetic
Head Injury: Classification Most Severe to Least Severe
 Head Injury: Classification Most Severe to Least Severe Douglas I. Katz, MD Professor, Dept. Neurology, Boston University School of Medicine, Boston MA Medical Director Brain Injury Program, HealthSouth
Head Injury: Classification Most Severe to Least Severe Douglas I. Katz, MD Professor, Dept. Neurology, Boston University School of Medicine, Boston MA Medical Director Brain Injury Program, HealthSouth
Functional Neuroanatomy and Traumatic Brain Injury The Frontal Lobes
 Functional Neuroanatomy and Traumatic Brain Injury The Frontal Lobes Jessica Matthes, Ph.D., ABN Barrow TBI Symposium March 23, 2019 jessica.matthes@dignityhealth.org Outline TBI Mechanisms of Injury Types
Functional Neuroanatomy and Traumatic Brain Injury The Frontal Lobes Jessica Matthes, Ph.D., ABN Barrow TBI Symposium March 23, 2019 jessica.matthes@dignityhealth.org Outline TBI Mechanisms of Injury Types
Index. aneurysm, 92 carotid occlusion, 94 ICA stenosis, 95 intracranial, 92 MCA, 94
 A ADC. See Apparent diffusion coefficient (ADC) Aneurysm cerebral artery aneurysm, 93 CT scan, 93 gadolinium, 93 Angiography, 13 Anoxic brain injury, 25 Apparent diffusion coefficient (ADC), 7 Arachnoid
A ADC. See Apparent diffusion coefficient (ADC) Aneurysm cerebral artery aneurysm, 93 CT scan, 93 gadolinium, 93 Angiography, 13 Anoxic brain injury, 25 Apparent diffusion coefficient (ADC), 7 Arachnoid
A Guide to the Radiologic Evaluation of Extra-Axial Hemorrhage
 July 2013 A Guide to the Radiologic Evaluation of Extra-Axial Hemorrhage John Dickson, Harvard Medical School Year III Agenda 1. Define extra-axial hemorrhage and introduce its subtypes 2. Review coup
July 2013 A Guide to the Radiologic Evaluation of Extra-Axial Hemorrhage John Dickson, Harvard Medical School Year III Agenda 1. Define extra-axial hemorrhage and introduce its subtypes 2. Review coup
Pre-hospital Response to Trauma and Brain Injury. Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center
 Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Web Training Modules Module 13: MR Imaging for Brain Injuries
 Web Training Modules Module 13: MR Imaging for Brain Injuries 1 Introduction... 4 Mild Traumatic Brain Injuries... 5 Structural MRI... 5 Diffusion Tensor Imaging... 6 Diffusion Kurtosis Imaging... 11 Functional
Web Training Modules Module 13: MR Imaging for Brain Injuries 1 Introduction... 4 Mild Traumatic Brain Injuries... 5 Structural MRI... 5 Diffusion Tensor Imaging... 6 Diffusion Kurtosis Imaging... 11 Functional
Head injury in children
 Head injury in children Michael Kim, MD Department of Emergency Medicine University of Wisconsin- Madison #1 cause of death and disability Bimodal distribution 62,000 hospitalization 564,000 ED visits
Head injury in children Michael Kim, MD Department of Emergency Medicine University of Wisconsin- Madison #1 cause of death and disability Bimodal distribution 62,000 hospitalization 564,000 ED visits
MEDICAL POLICY EFFECTIVE DATE: 12/18/08 REVISED DATE: 12/17/09, 03/17/11, 05/19/11, 05/24/12, 05/23/13, 05/22/14
 MEDICAL POLICY SUBJECT: CT (COMPUTED TOMOGRAPHY) PAGE: 1 OF: 5 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical
MEDICAL POLICY SUBJECT: CT (COMPUTED TOMOGRAPHY) PAGE: 1 OF: 5 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical
Applicable Neuroradiology
 For the Clinical Neurology Clerkship LSU Medical School New Orleans Amy W Voigt, MD Clerkship Director Introduction The field of Radiology first developed following the discovery of X-Rays by Wilhelm Roentgen
For the Clinical Neurology Clerkship LSU Medical School New Orleans Amy W Voigt, MD Clerkship Director Introduction The field of Radiology first developed following the discovery of X-Rays by Wilhelm Roentgen
Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD
 Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD Five Step Approach 1. Adequate study 2. Bone windows 3. Ventricles 4. Quadrigeminal cistern 5. Parenchyma
Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD Five Step Approach 1. Adequate study 2. Bone windows 3. Ventricles 4. Quadrigeminal cistern 5. Parenchyma
SUPPLEMENTARY FIG. S2. (A) Risk of bias and applicability concerns graph by marker. Review authors judgments about each domain presented as
 Risk of bias and applicability concerns graph by marker. Review authors judgments about each domain presented as") Supplementary Data SUPPLEMENTARY FIG. S1. Graphical depiction of (A) influence and (B) outlier detection analyses of S100 calcium binding protein B (S100B) 0.10 0.11lg/L cutoff value studies. (C) Summary
Supplementary Data SUPPLEMENTARY FIG. S1. Graphical depiction of (A) influence and (B) outlier detection analyses of S100 calcium binding protein B (S100B) 0.10 0.11lg/L cutoff value studies. (C) Summary
USASOC Neurocognitive Testing and Post Injury Evaluation and Treatment Clinical Practice Guideline (CPG)
") USASOC Neurocognitive Testing and Post Injury Evaluation and Treatment Clinical Practice Guideline (CPG) Note: The intent of this CPG is to serve as general guidance for medics and medical officers. It
USASOC Neurocognitive Testing and Post Injury Evaluation and Treatment Clinical Practice Guideline (CPG) Note: The intent of this CPG is to serve as general guidance for medics and medical officers. It
Avoidable Imaging Learning Collaborative: 2008 Mild Traumatic Brain Injury Clinical Policy Success Story BWH Head and PE CTs with Clinical Decision
 Avoidable Imaging Learning Collaborative: 2008 Mild Traumatic Brain Injury Clinical Policy Success Story BWH Head and PE CTs with Clinical Decision Support Using the Canadian CT Head Rule to Reduce Unnecessary
Avoidable Imaging Learning Collaborative: 2008 Mild Traumatic Brain Injury Clinical Policy Success Story BWH Head and PE CTs with Clinical Decision Support Using the Canadian CT Head Rule to Reduce Unnecessary
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Marshall Scale for Head Trauma Mark C. Oswood, MD PhD Department of Radiology Hennepin County Medical Center, Minneapolis, MN
 Marshall Scale for Head Trauma Mark C. Oswood, MD PhD Department of Radiology Hennepin County Medical Center, Minneapolis, MN History of Marshall scale Proposed by Marshall, et al in 1991 to classify head
Marshall Scale for Head Trauma Mark C. Oswood, MD PhD Department of Radiology Hennepin County Medical Center, Minneapolis, MN History of Marshall scale Proposed by Marshall, et al in 1991 to classify head
TBI are twice as common in males High potential for poor outcome Deaths occur at three points in time after injury
 Head Injury Any trauma to (closed vs. open) Skull Scalp Brain Traumatic brain injury (TBI) High incidence Most common causes Falls Motor vehicle accidents Other causes Firearm- related injuries Assaults
Head Injury Any trauma to (closed vs. open) Skull Scalp Brain Traumatic brain injury (TBI) High incidence Most common causes Falls Motor vehicle accidents Other causes Firearm- related injuries Assaults
GUIDELINES FOR THE MANAGEMENT OF HEAD INJURIES IN REMOTE AND RURAL ALASKA
 GUIDELINES FOR THE MANAGEMENT OF HEAD INJURIES IN REMOTE AND RURAL ALASKA Approximately 800 patients with head injuries die or are hospitalized in the state of Alaska each year 1. In addition, thousands
GUIDELINES FOR THE MANAGEMENT OF HEAD INJURIES IN REMOTE AND RURAL ALASKA Approximately 800 patients with head injuries die or are hospitalized in the state of Alaska each year 1. In addition, thousands
FORENSIC SCIENCE NEWSLETTER Forensic Pathology and Neuropathology. William A. Cox, M.D., FCAP.
 NEUROPATHOLOGY FORENSIC SCIENCE NEWSLETTER Forensic Pathology and Neuropathology William A. Cox, M.D., FCAP www.forensicjournals.cm May 15, 2016 This issue of the Forensic Science Newsletter will address
NEUROPATHOLOGY FORENSIC SCIENCE NEWSLETTER Forensic Pathology and Neuropathology William A. Cox, M.D., FCAP www.forensicjournals.cm May 15, 2016 This issue of the Forensic Science Newsletter will address
PEDIATRIC MILD TRAUMATIC HEAD INJURY
 PEDIATRIC MILD TRAUMATIC HEAD INJURY October 2011 Quality Improvement Resources Illinois Emergency Medical Services for Children is a collaborative program between the Illinois Department of Public Health
PEDIATRIC MILD TRAUMATIC HEAD INJURY October 2011 Quality Improvement Resources Illinois Emergency Medical Services for Children is a collaborative program between the Illinois Department of Public Health
DIAGNOSTIC PROCEDURES IN MILD TRAUMATIC BRAIN INJURY: RESULTS OF THE WHO COLLABORATING CENTRE TASK FORCE ON MILD TRAUMATIC BRAIN INJURY
 J Rehabil Med 2004; Suppl. 43: 61 75 DIAGNOSTIC PROCEDURES IN MILD TRAUMATIC BRAIN INJURY: RESULTS OF THE WHO COLLABORATING CENTRE TASK FORCE ON MILD TRAUMATIC BRAIN INJURY Jörgen Borg, 1 Lena Holm, 2
J Rehabil Med 2004; Suppl. 43: 61 75 DIAGNOSTIC PROCEDURES IN MILD TRAUMATIC BRAIN INJURY: RESULTS OF THE WHO COLLABORATING CENTRE TASK FORCE ON MILD TRAUMATIC BRAIN INJURY Jörgen Borg, 1 Lena Holm, 2
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Traumatic Brain Injury
 General Information Traumatic Brain Injury What you need to know Complicated condition with high variability in etiology, severity, distribution of injury, and pattern of functional impairment (Klyce,
General Information Traumatic Brain Injury What you need to know Complicated condition with high variability in etiology, severity, distribution of injury, and pattern of functional impairment (Klyce,
Screening and Management of Blunt Cereberovascular Injuries (BCVI)
") Grady Memorial Hospital Trauma Service Guidelines Screening and Management of Blunt Cereberovascular Injuries (BCVI) BACKGROUND Blunt injury to the carotid or vertebral vessels (blunt cerebrovascular injury
Grady Memorial Hospital Trauma Service Guidelines Screening and Management of Blunt Cereberovascular Injuries (BCVI) BACKGROUND Blunt injury to the carotid or vertebral vessels (blunt cerebrovascular injury
Leah Militello, class of 2018
 Leah Militello, class of 2018 Objectives 1. Describe the general organization of cerebral hemispheres. 2. Describe the locations and features of the different functional areas of cortex. 3. Understand
Leah Militello, class of 2018 Objectives 1. Describe the general organization of cerebral hemispheres. 2. Describe the locations and features of the different functional areas of cortex. 3. Understand
Use of CT in minor traumatic brain injury. Lisa Ayoub-Rodriguez, MD Bert Johansson, MD Michael Lee, MD
 Use of CT in minor traumatic brain injury Lisa Ayoub-Rodriguez, MD Bert Johansson, MD Michael Lee, MD No financial or other conflicts of interest Epidemiology of traumatic brain injury (TBI) Risks associated
Use of CT in minor traumatic brain injury Lisa Ayoub-Rodriguez, MD Bert Johansson, MD Michael Lee, MD No financial or other conflicts of interest Epidemiology of traumatic brain injury (TBI) Risks associated
V. CENTRAL NERVOUS SYSTEM TRAUMA
 V. CENTRAL NERVOUS SYSTEM TRAUMA I. Concussion - Is a clinical syndrome of altered consiousness secondary to head injury - Brought by a change in the momentum of the head when a moving head suddenly arrested
V. CENTRAL NERVOUS SYSTEM TRAUMA I. Concussion - Is a clinical syndrome of altered consiousness secondary to head injury - Brought by a change in the momentum of the head when a moving head suddenly arrested
Traumatic Head Injury
 Traumatic Head Injury Liu Yi, MD. PhD, associate professor Dept. Neurosurgery Conception Any injury to the skull, or brain, caused by external physical forces, in stead of degenerative or congenital nature
Traumatic Head Injury Liu Yi, MD. PhD, associate professor Dept. Neurosurgery Conception Any injury to the skull, or brain, caused by external physical forces, in stead of degenerative or congenital nature
Canadian CT head rule and New Orleans Criteria in mild traumatic brain injury: comparison at a tertiary referral hospital in Japan
 DOI 10.1186/s40064-016-1781-9 RESEARCH Open Access Canadian CT head rule and New Orleans Criteria in mild traumatic brain injury: comparison at a tertiary referral hospital in Japan Daddy Mata Mbemba 1,2,
DOI 10.1186/s40064-016-1781-9 RESEARCH Open Access Canadian CT head rule and New Orleans Criteria in mild traumatic brain injury: comparison at a tertiary referral hospital in Japan Daddy Mata Mbemba 1,2,
Evaluation of Craniocerebral Trauma Using Computed Tomography
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 13, Issue 9 Ver. IV (Sep. 2014), PP 57-62 Evaluation of Craniocerebral Trauma Using Computed Tomography
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 13, Issue 9 Ver. IV (Sep. 2014), PP 57-62 Evaluation of Craniocerebral Trauma Using Computed Tomography
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
The Central Nervous System
 The Central Nervous System Cellular Basis. Neural Communication. Major Structures. Principles & Methods. Principles of Neural Organization Big Question #1: Representation. How is the external world coded
The Central Nervous System Cellular Basis. Neural Communication. Major Structures. Principles & Methods. Principles of Neural Organization Big Question #1: Representation. How is the external world coded
Neurological examination of the neurosurgical patient. Dániel Bereczki SU Department of Neurology
 Neurological examination of the neurosurgical patient Dániel Bereczki SU Department of Neurology E-learning Indivudual study Interactive learning Self assessment at the end of chapters E-learning Indivudual
Neurological examination of the neurosurgical patient Dániel Bereczki SU Department of Neurology E-learning Indivudual study Interactive learning Self assessment at the end of chapters E-learning Indivudual
Mild Traumatic Brain Injury
 Mild Traumatic Brain Injury Concussions This presentation is for information purposes only, not for any commercial purpose, and may not be sold or redistributed. David Wesley, M.D. Outline Epidemiology
Mild Traumatic Brain Injury Concussions This presentation is for information purposes only, not for any commercial purpose, and may not be sold or redistributed. David Wesley, M.D. Outline Epidemiology
Virtual Mentor American Medical Association Journal of Ethics August 2008, Volume 10, Number 8:
 Virtual Mentor American Medical Association Journal of Ethics August 2008, Volume 10, Number 8: 516-520. CLINICAL PEARL The Hazards of Stopping a Brain in Motion: Evaluation and Classification of Traumatic
Virtual Mentor American Medical Association Journal of Ethics August 2008, Volume 10, Number 8: 516-520. CLINICAL PEARL The Hazards of Stopping a Brain in Motion: Evaluation and Classification of Traumatic
Tips and tricks for detecting diffuse axonal injury on CT and MR neuroimaging
 Tips and tricks for detecting diffuse axonal injury on CT and MR neuroimaging Poster No.: C-3080 Congress: ECR 2018 Type: Educational Exhibit Authors: M. Marinkic, D. Zadravec ; Zagreb/HR, Zageb/HR Keywords:
Tips and tricks for detecting diffuse axonal injury on CT and MR neuroimaging Poster No.: C-3080 Congress: ECR 2018 Type: Educational Exhibit Authors: M. Marinkic, D. Zadravec ; Zagreb/HR, Zageb/HR Keywords:
Concussion: Research Overview
 Concussion: Research Overview September 30, 2013 Hugh J.L. Garton, M.D.,M.HSc. Dept. of Neurosurgery University of Michigan No Disclosures Overview Anatomy / Definitions Biomechanics Cerebral Blood Flow
Concussion: Research Overview September 30, 2013 Hugh J.L. Garton, M.D.,M.HSc. Dept. of Neurosurgery University of Michigan No Disclosures Overview Anatomy / Definitions Biomechanics Cerebral Blood Flow
Traumatic Brain Injury TBI Presented by Bill Masten
 1 2 Cerebrum two hemispheres and four lobes. Cerebellum (little brain) coordinates the back and forth ballet of motion. It judges the timing of every movement precisely. Brainstem coordinates the bodies
1 2 Cerebrum two hemispheres and four lobes. Cerebellum (little brain) coordinates the back and forth ballet of motion. It judges the timing of every movement precisely. Brainstem coordinates the bodies
HEAD AND NECK IMAGING. James Chen (MS IV)
") HEAD AND NECK IMAGING James Chen (MS IV) Anatomy Course Johns Hopkins School of Medicine Sept. 27, 2011 OBJECTIVES Introduce cross sectional imaging of head and neck Computed tomography (CT) Review head
HEAD AND NECK IMAGING James Chen (MS IV) Anatomy Course Johns Hopkins School of Medicine Sept. 27, 2011 OBJECTIVES Introduce cross sectional imaging of head and neck Computed tomography (CT) Review head
Post-concussion syndrome: Correlation of neuropsychological deficits, structural lesions on magnetic resonance imaging and symptoms
 Original Article Post-concussion syndrome: Correlation of neuropsychological deficits, structural lesions on magnetic resonance imaging and symptoms S. G. S. Datta, S. V. Pillai, S. L. Rao 1, J. M. E.
Original Article Post-concussion syndrome: Correlation of neuropsychological deficits, structural lesions on magnetic resonance imaging and symptoms S. G. S. Datta, S. V. Pillai, S. L. Rao 1, J. M. E.
NEURO IMAGING OF ACUTE STROKE
 1 1 NEURO IMAGING OF ACUTE STROKE ALICIA RICHARDSON, MSN, RN, ACCNS-AG, ANVP-BC WENDY SMITH, MA, RN, MBA, SCRN, FAHA LYNN HUNDLEY, APRN, CNRN, CCNS, ANVP-BC 2 2 1 DISCLOSURES Alicia Richardson: Stryker
1 1 NEURO IMAGING OF ACUTE STROKE ALICIA RICHARDSON, MSN, RN, ACCNS-AG, ANVP-BC WENDY SMITH, MA, RN, MBA, SCRN, FAHA LYNN HUNDLEY, APRN, CNRN, CCNS, ANVP-BC 2 2 1 DISCLOSURES Alicia Richardson: Stryker
Dr Chris Milne. Dr Michael Kahan. Sports Physician Anglesea Clinic Hamilton. Occupational Specialist Waikato Occupational Services, Hamilton
 Dr Michael Kahan Occupational Specialist Waikato Occupational Services, Hamilton Dr Chris Milne Sports Physician Anglesea Clinic Hamilton 16:30-17:25 WS #71: Concussion - Clinical Considerations, Cares
Dr Michael Kahan Occupational Specialist Waikato Occupational Services, Hamilton Dr Chris Milne Sports Physician Anglesea Clinic Hamilton 16:30-17:25 WS #71: Concussion - Clinical Considerations, Cares
Do Prognostic Models Matter in Neurocritical Care?
 Do Prognostic Models Matter in Neurocritical Care? Alexis F. Turgeon MD MSc FRCPC Associate Professor and Director of Research Department of Anesthesiology and Critical Care Medicine Division of Critical
Do Prognostic Models Matter in Neurocritical Care? Alexis F. Turgeon MD MSc FRCPC Associate Professor and Director of Research Department of Anesthesiology and Critical Care Medicine Division of Critical
Stroke & Neurovascular Center of New Jersey. Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center
 Stroke & Neurovascular Center of New Jersey Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center Past, present and future Past, present and future Cerebral Blood Flow Past, present and future
Stroke & Neurovascular Center of New Jersey Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center Past, present and future Past, present and future Cerebral Blood Flow Past, present and future
Head injuries in children. Dr Jason Hort Paediatrician Paediatric Emergency Physician, June 2017 Children s Hospital Westmead
 Head injuries in children Dr Jason Hort Paediatrician Paediatric Emergency Physician, June 2017 Children s Hospital Westmead Objectives Approach to minor head injury Child protection issues Concussion
Head injuries in children Dr Jason Hort Paediatrician Paediatric Emergency Physician, June 2017 Children s Hospital Westmead Objectives Approach to minor head injury Child protection issues Concussion
NEURO IMAGING 2. Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity
 NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
State of the Art Multimodal Monitoring
 State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
Case Report. Annals of Rehabilitation Medicine INTRODUCTION
 Case Report Ann Rehabil Med 2017;41(1):153-157 pissn: 2234-0645 eissn: 2234-0653 https://doi.org/10.5535/arm.2017.41.1.153 Annals of Rehabilitation Medicine Diagnostic Challenge of Diffusion Tensor Imaging
Case Report Ann Rehabil Med 2017;41(1):153-157 pissn: 2234-0645 eissn: 2234-0653 https://doi.org/10.5535/arm.2017.41.1.153 Annals of Rehabilitation Medicine Diagnostic Challenge of Diffusion Tensor Imaging
Introduction, use of imaging and current guidelines. John O Brien Professor of Old Age Psychiatry University of Cambridge
 Introduction, use of imaging and current guidelines John O Brien Professor of Old Age Psychiatry University of Cambridge Why do we undertake brain imaging in AD and other dementias? Exclude other causes
Introduction, use of imaging and current guidelines John O Brien Professor of Old Age Psychiatry University of Cambridge Why do we undertake brain imaging in AD and other dementias? Exclude other causes
MRI and CT of the CNS
 MRI and CT of the CNS Dr.Maha ELBeltagy Assistant Professor of Anatomy Faculty of Medicine The University of Jordan 2018 Computed Tomography CT is used for the detection of intracranial lesions. CT relies
MRI and CT of the CNS Dr.Maha ELBeltagy Assistant Professor of Anatomy Faculty of Medicine The University of Jordan 2018 Computed Tomography CT is used for the detection of intracranial lesions. CT relies
Clinical Outcome of Borderline Subdural Hematoma with 5-9 mm Thickness and/or Midline Shift 2-5 mm
 Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/300 Clinical Outcome of Borderline Subdural Hematoma with 5-9 mm Thickness and/or Midline Shift 2-5 mm Raja S Vignesh
Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/300 Clinical Outcome of Borderline Subdural Hematoma with 5-9 mm Thickness and/or Midline Shift 2-5 mm Raja S Vignesh
The risk of a bleed after delayed head injury presentation to the ED: systematic review protocol. Correspondence to:
 The risk of a bleed after delayed head injury presentation to the ED: systematic review protocol. Carl Marincowitz, Christopher M. Smith, William Townend Emergency Department, Hull Royal, Hull, UK Correspondence
The risk of a bleed after delayed head injury presentation to the ED: systematic review protocol. Carl Marincowitz, Christopher M. Smith, William Townend Emergency Department, Hull Royal, Hull, UK Correspondence
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
THE ESSENTIAL BRAIN INJURY GUIDE
 THE ESSENTIAL BRAIN INJURY GUIDE Neuroanatomy & Neuroplasticity Section 2 Contributors Erin D. Bigler, PhD Michael R. Hoane, PhD Stephanie Kolakowsky-Hayner, PhD, CBIST, FACRM Dorothy A. Kozlowski, PhD
THE ESSENTIAL BRAIN INJURY GUIDE Neuroanatomy & Neuroplasticity Section 2 Contributors Erin D. Bigler, PhD Michael R. Hoane, PhD Stephanie Kolakowsky-Hayner, PhD, CBIST, FACRM Dorothy A. Kozlowski, PhD
Hit head, on blood thinner-wife wants CT. Will Davies June 2014
 Hit head, on blood thinner-wife wants CT Will Davies June 2014 Selection of Adults with Head Injury for CT Scan Early management of head injury: summary of updated NICE guidance. Hodgkinson S, Pollit V,
Hit head, on blood thinner-wife wants CT Will Davies June 2014 Selection of Adults with Head Injury for CT Scan Early management of head injury: summary of updated NICE guidance. Hodgkinson S, Pollit V,
Neuroimaging 101. Amy Shatila, LSSP/NCSP Kelsey Theis, LSSP/NCSP. TASP Convention November 4, 2017
 Neuroimaging 101 Amy Shatila, LSSP/NCSP Kelsey Theis, LSSP/NCSP TASP Convention November 4, 2017 A bit-o-trivia: Gray matter in a live brain is actually more of a pink color But Gray matter is the cell
Neuroimaging 101 Amy Shatila, LSSP/NCSP Kelsey Theis, LSSP/NCSP TASP Convention November 4, 2017 A bit-o-trivia: Gray matter in a live brain is actually more of a pink color But Gray matter is the cell
Outline. Neuroradiology. Diffusion Imaging in. Clinical Applications of. Basics of Diffusion Imaging. Basics of Diffusion Imaging
 Clinical Applications of Diffusion Imaging in Neuroradiology No disclosures Stephen F. Kralik Assistant Professor of Radiology Indiana University School of Medicine Department of Radiology and Imaging
Clinical Applications of Diffusion Imaging in Neuroradiology No disclosures Stephen F. Kralik Assistant Professor of Radiology Indiana University School of Medicine Department of Radiology and Imaging
Evaluation and Stabilization of the Athlete with Possible Spine Injury
 Evaluation and Stabilization of the Athlete with Possible Spine Injury Jeffrey H. Bohmer, MD, FACEP Emergency Physician Northwestern Medicine Central DuPage Hospital June 12, 2015 Introduction Goals: 1.
Evaluation and Stabilization of the Athlete with Possible Spine Injury Jeffrey H. Bohmer, MD, FACEP Emergency Physician Northwestern Medicine Central DuPage Hospital June 12, 2015 Introduction Goals: 1.
Introduction to Modern Imaging Physics and Techniques used in Clinical Neurology
 Introduction to Modern Imaging Physics and Techniques used in Clinical Neurology Benjamin M. Ellingson, Ph.D., M.S. Associate Professor of Radiology, Biomedical Physics, Bioengineering, and Psychiatry
Introduction to Modern Imaging Physics and Techniques used in Clinical Neurology Benjamin M. Ellingson, Ph.D., M.S. Associate Professor of Radiology, Biomedical Physics, Bioengineering, and Psychiatry
Traumatic brain injuries are caused by external mechanical forces such as: - Falls - Transport-related accidents - Assault
 PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
General Identification. Name: 江 X X Age: 29 y/o Gender: Male Height:172cm, Weight: 65kg Date of admission:95/09/27
 General Identification Name: 江 X X Age: 29 y/o Gender: Male Height:172cm, Weight: 65kg Date of admission:95/09/27 Chief Complaint Sudden onset of seizure for several minutes Present illness This 29-year
General Identification Name: 江 X X Age: 29 y/o Gender: Male Height:172cm, Weight: 65kg Date of admission:95/09/27 Chief Complaint Sudden onset of seizure for several minutes Present illness This 29-year
NEURORADIOLOGY Part I
 NEURORADIOLOGY Part I Vörös Erika University of Szeged Department of Radiology SZEGED BRAIN IMAGING METHODS Plain film radiography Ultrasonography (US) Computer tomography (CT) Magnetic resonance imaging
NEURORADIOLOGY Part I Vörös Erika University of Szeged Department of Radiology SZEGED BRAIN IMAGING METHODS Plain film radiography Ultrasonography (US) Computer tomography (CT) Magnetic resonance imaging
Course objectives. Head Ultrasound. Introduction
 Disclosure Information AACPDM 68 th Annual Meeting September 10-13, 2014 Imaging of the pediatric brain, spinal cord and muscle: Tools and clinical applications Andrea Poretti, MD Research Associate Section
Disclosure Information AACPDM 68 th Annual Meeting September 10-13, 2014 Imaging of the pediatric brain, spinal cord and muscle: Tools and clinical applications Andrea Poretti, MD Research Associate Section
2. Subarachnoid Hemorrhage
 Causes: 2. Subarachnoid Hemorrhage A. Saccular (berry) aneurysm - Is the most frequent cause of clinically significant subarachnoid hemorrhage is rupture of a saccular (berry) aneurysm. B. Vascular malformation
Causes: 2. Subarachnoid Hemorrhage A. Saccular (berry) aneurysm - Is the most frequent cause of clinically significant subarachnoid hemorrhage is rupture of a saccular (berry) aneurysm. B. Vascular malformation
Disclosure Statement. Dr. Kadish has no relevant financial relationships with any commercial interests mentioned in this talk.
 Disclosure Statement Dr. Kadish has no relevant financial relationships with any commercial interests mentioned in this talk. Head Trauma Evaluation Primary and secondary injury Disposition Sports related
Disclosure Statement Dr. Kadish has no relevant financial relationships with any commercial interests mentioned in this talk. Head Trauma Evaluation Primary and secondary injury Disposition Sports related
How to interpret an unenhanced CT brain scan. Part 2: Clinical cases
 How to interpret an unenhanced CT brain scan. Part 2: Clinical cases Thomas Osborne a, Christine Tang a, Kivraj Sabarwal b and Vineet Prakash c a Radiology Registrar; b Radiology Foundation Year 1 Doctor;
How to interpret an unenhanced CT brain scan. Part 2: Clinical cases Thomas Osborne a, Christine Tang a, Kivraj Sabarwal b and Vineet Prakash c a Radiology Registrar; b Radiology Foundation Year 1 Doctor;
ORIGINAL ARTICLE. Temporal Lobe Injury in Temporal Bone Fractures. imaging (MRI) to evaluate lesions of the temporal
 to evaluate lesions of the temporal") ORIGINAL ARTICLE Temporal Lobe Injury in Temporal Bone Fractures Richard M. Jones, MD; Michael I. Rothman, MD; William C. Gray, MD; Gregg H. Zoarski, MD; Douglas E. Mattox, MD Objective: To determine the
ORIGINAL ARTICLE Temporal Lobe Injury in Temporal Bone Fractures Richard M. Jones, MD; Michael I. Rothman, MD; William C. Gray, MD; Gregg H. Zoarski, MD; Douglas E. Mattox, MD Objective: To determine the
Benign brain lesions
 Benign brain lesions Diagnostic and Interventional Radiology Hung-Wen Kao Department of Radiology, Tri-Service General Hospital, National Defense Medical Center Computed tomography Hounsfield unit (HU)
Benign brain lesions Diagnostic and Interventional Radiology Hung-Wen Kao Department of Radiology, Tri-Service General Hospital, National Defense Medical Center Computed tomography Hounsfield unit (HU)
Concussion. Concussion is a disturbance of brain function caused by a direct or indirect force to the head.
 Concussion Concussion is a disturbance of brain function caused by a direct or indirect force to the head. Disturbances of brain tissue is largely related to neurometabolic dysfunction rather then structural
Concussion Concussion is a disturbance of brain function caused by a direct or indirect force to the head. Disturbances of brain tissue is largely related to neurometabolic dysfunction rather then structural
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth. Objectives 11/7/2017
 Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
MR imaging as predictor of delayed posttraumatic cerebral hemorrhage
 J Neurosurg 69:203-209, 1988 MR imaging as predictor of delayed posttraumatic cerebral hemorrhage TOKUTARO TANAKA, M.D., TSUNEO SAKAI, M.D., KENICHI UEMURA, M.D., ATSUSHI TERAMURA, M.D., ICHIRO FUJISHIMA,
J Neurosurg 69:203-209, 1988 MR imaging as predictor of delayed posttraumatic cerebral hemorrhage TOKUTARO TANAKA, M.D., TSUNEO SAKAI, M.D., KENICHI UEMURA, M.D., ATSUSHI TERAMURA, M.D., ICHIRO FUJISHIMA,
PA SYLLABUS. Syllabus for students of the FACULTY OF MEDICINE No.2
 Approved At the meeting of the Faculty Council Medicine No. of Approved At the meeting of the chair of Neurosurgery No. of Dean of the Faculty Medicine No.2 PhD, associate professor M. Betiu Head of the
Approved At the meeting of the Faculty Council Medicine No. of Approved At the meeting of the chair of Neurosurgery No. of Dean of the Faculty Medicine No.2 PhD, associate professor M. Betiu Head of the
Cerebral Cortex 1. Sarah Heilbronner
 Cerebral Cortex 1 Sarah Heilbronner heilb028@umn.edu Want to meet? Coffee hour 10-11am Tuesday 11/27 Surdyk s Overview and organization of the cerebral cortex What is the cerebral cortex? Where is each
Cerebral Cortex 1 Sarah Heilbronner heilb028@umn.edu Want to meet? Coffee hour 10-11am Tuesday 11/27 Surdyk s Overview and organization of the cerebral cortex What is the cerebral cortex? Where is each
Prof. Greg Francis 1/2/19
 Brain scans PSY 200 Greg Francis Lecture 03 How to study the brain without killing someone. Scanning Technology provides insight into brain processes w EEG recordings w MRI w Non-invasive Maps of brain
Brain scans PSY 200 Greg Francis Lecture 03 How to study the brain without killing someone. Scanning Technology provides insight into brain processes w EEG recordings w MRI w Non-invasive Maps of brain
Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage
 Cronicon OPEN ACCESS EC PAEDIATRICS Case Report Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage Dimitrios Panagopoulos* Neurosurgical Department, University
Cronicon OPEN ACCESS EC PAEDIATRICS Case Report Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage Dimitrios Panagopoulos* Neurosurgical Department, University
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE
 WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
Pediatric Trauma Initial Evaluation and management
 Pediatric Trauma Initial Evaluation and management Head Injury Closed head injury Penetrating head injury Closed Head Injury without Fractures Head injury is the most common cause of death and disability
Pediatric Trauma Initial Evaluation and management Head Injury Closed head injury Penetrating head injury Closed Head Injury without Fractures Head injury is the most common cause of death and disability
Neuroradiological Findings in Non- Accidental Trauma Educational Pictorial Review
 Neuroradiological Findings in Non- Accidental Trauma Educational Pictorial Review M B Moss, MD; L Lanier, MD; R Slater; C L Sistrom, MD; R G Quisling, MD; I M Schmalfuss, MD; and D Rajderkar, MD Contact:
Neuroradiological Findings in Non- Accidental Trauma Educational Pictorial Review M B Moss, MD; L Lanier, MD; R Slater; C L Sistrom, MD; R G Quisling, MD; I M Schmalfuss, MD; and D Rajderkar, MD Contact:
Traumatic Brain Injury. Epidemiology and Pathophysiology
 Traumatic Brain Injury Epidemiology and Pathophysiology March 10, 2017 Cherry Junn, M.D. Pinella Holder, D.O. University of Washington Disclosures None Objectives Able to define TBI using CDC criteria
Traumatic Brain Injury Epidemiology and Pathophysiology March 10, 2017 Cherry Junn, M.D. Pinella Holder, D.O. University of Washington Disclosures None Objectives Able to define TBI using CDC criteria
Is DTI Increasing the Connectivity Between the Magnet Suite and the Clinic?
 Current Literature In Clinical Science Is DTI Increasing the Connectivity Between the Magnet Suite and the Clinic? Spatial Patterns of Water Diffusion Along White Matter Tracts in Temporal Lobe Epilepsy.
Current Literature In Clinical Science Is DTI Increasing the Connectivity Between the Magnet Suite and the Clinic? Spatial Patterns of Water Diffusion Along White Matter Tracts in Temporal Lobe Epilepsy.
Objectives. Incidence TBI: Leading cause of death & disability due to trauma. 9th Annual NKY TBI Conference 3/27/2015
 Mild Traumatic Brain Injury & Symptom Assessment in Children Becky Cook, DNP, APRN Trauma Nurse Practitioner Objectives Discuss the incidence and mechanisms of injury of mild traumatic brain injury (mtbi)
Mild Traumatic Brain Injury & Symptom Assessment in Children Becky Cook, DNP, APRN Trauma Nurse Practitioner Objectives Discuss the incidence and mechanisms of injury of mild traumatic brain injury (mtbi)
Attenuation value in HU From -500 To HU From -10 To HU From 60 To 90 HU. From 200 HU and above
 Brain Imaging Common CT attenuation values Structure Air Fat Water Brain tissue Recent hematoma Calcifications Bone Brain edema and infarction Normal liver parenchyma Attenuation value in HU From -500
Brain Imaging Common CT attenuation values Structure Air Fat Water Brain tissue Recent hematoma Calcifications Bone Brain edema and infarction Normal liver parenchyma Attenuation value in HU From -500
7 TI - Epidemiology of intracerebral hemorrhage.
 1 TI - Multiple postoperative intracerebral haematomas remote from the site of craniotomy. AU - Rapana A, et al. SO - Br J Neurosurg. 1998 Aug;1():-8. Review. IDS - PMID: 1000 UI: 991958 TI - Cerebral
1 TI - Multiple postoperative intracerebral haematomas remote from the site of craniotomy. AU - Rapana A, et al. SO - Br J Neurosurg. 1998 Aug;1():-8. Review. IDS - PMID: 1000 UI: 991958 TI - Cerebral
Learning Objectives 1. TBI Severity & Evaluation Tools. Clinical Diagnosis of TBI. Learning Objectives 2 3/3/2015. Define TBI severity using GCS
 Learning Objectives 1 TBI Severity & Evaluation Tools Define TBI severity using GCS and PTA Describe functional prognosis after moderate to severe TBI using trends and threshold values Jennifer M Zumsteg,
Learning Objectives 1 TBI Severity & Evaluation Tools Define TBI severity using GCS and PTA Describe functional prognosis after moderate to severe TBI using trends and threshold values Jennifer M Zumsteg,
Cerebro-vascular stroke
 Cerebro-vascular stroke CT Terminology Hypodense lesion = lesion of lower density than the normal brain tissue Hyperdense lesion = lesion of higher density than normal brain tissue Isodense lesion = lesion
Cerebro-vascular stroke CT Terminology Hypodense lesion = lesion of lower density than the normal brain tissue Hyperdense lesion = lesion of higher density than normal brain tissue Isodense lesion = lesion
Hemodynamic patterns of status epilepticus detected by susceptibility weighted imaging (SWI)
") Hemodynamic patterns of status epilepticus detected by susceptibility weighted imaging (SWI) Poster No.: C-1086 Congress: ECR 014 Type: Scientific Exhibit Authors: J. AELLEN, E. Abela, R. Kottke, E. Springer,
Hemodynamic patterns of status epilepticus detected by susceptibility weighted imaging (SWI) Poster No.: C-1086 Congress: ECR 014 Type: Scientific Exhibit Authors: J. AELLEN, E. Abela, R. Kottke, E. Springer,
Overview of Abusive Head Trauma: What Everyone Needs to Know. 11 th Annual Keeping Children Safe Conference Boise, ID October 17, 2012
 Overview of Abusive Head Trauma: What Everyone Needs to Know 11 th Annual Keeping Children Safe Conference Boise, ID October 17, 2012 Deborah Lowen, MD Associate Professor Pediatrics Director, Child Abuse
Overview of Abusive Head Trauma: What Everyone Needs to Know 11 th Annual Keeping Children Safe Conference Boise, ID October 17, 2012 Deborah Lowen, MD Associate Professor Pediatrics Director, Child Abuse
secondary effects and sequelae of head trauma.
 Neuroimaging of vascular/secondary secondary effects and sequelae of head trauma. Andrès Server Alonso Department of Neuroradiology Division of Radiology Ullevål University Hospital Oslo, Norway. Guidelines
Neuroimaging of vascular/secondary secondary effects and sequelae of head trauma. Andrès Server Alonso Department of Neuroradiology Division of Radiology Ullevål University Hospital Oslo, Norway. Guidelines
CNS Imaging. Dr Amir Monir, MD. Lecturer of radiodiagnosis.
 CNS Imaging Dr Amir Monir, MD Lecturer of radiodiagnosis www.dramir.net Types of radiological examinations you know Plain X ray X ray with contrast GIT : barium (swallow, meal, follow through, enema) ERCP
CNS Imaging Dr Amir Monir, MD Lecturer of radiodiagnosis www.dramir.net Types of radiological examinations you know Plain X ray X ray with contrast GIT : barium (swallow, meal, follow through, enema) ERCP
Trauma Overview. Chapter 1. Introduction. Epidemiology of Head Trauma. Etiology and Mechanisms of Injury
 Chapter 1 5 Overview is one of the most frequent indications for emergent neuroimaging. Because imaging plays such a key role in patient triage and management, we begin this book by discussing skull and
Chapter 1 5 Overview is one of the most frequent indications for emergent neuroimaging. Because imaging plays such a key role in patient triage and management, we begin this book by discussing skull and
Mild traumatic brain injury (mtbi) comprises 75% of the. Original Articles
 comprises 75% of the. Original Articles") JOURNAL OF NEUROTRAUMA 31:1457 1477 (September 1, 2014) ª Mary Ann Liebert, Inc. DOI: 10.1089/neu.2013.3171 Original Articles Diffusion Tensor Imaging for Outcome Prediction in Mild Traumatic Brain Injury:
JOURNAL OF NEUROTRAUMA 31:1457 1477 (September 1, 2014) ª Mary Ann Liebert, Inc. DOI: 10.1089/neu.2013.3171 Original Articles Diffusion Tensor Imaging for Outcome Prediction in Mild Traumatic Brain Injury:
Classical CNS Disease Patterns
 Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
Acute stroke imaging
 Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
The United States and its health care system are in a financial
 Overuse CT Overuse for Mild Traumatic Brain Injury Edward R. Melnick, MD; Christopher M. Szlezak, MD; Suzanne K. Bentley, MD; James D. Dziura, PhD; Simon Kotlyar, MD, MSc; Lori A. Post, PhD The United
Overuse CT Overuse for Mild Traumatic Brain Injury Edward R. Melnick, MD; Christopher M. Szlezak, MD; Suzanne K. Bentley, MD; James D. Dziura, PhD; Simon Kotlyar, MD, MSc; Lori A. Post, PhD The United
Correlation of Computed Tomography findings with Glassgow Coma Scale in patients with acute traumatic brain injury
 Journal of College of Medical Sciences-Nepal, 2014, Vol-10, No-2 ABSTRACT OBJECTIVE To correlate Computed Tomography (CT) findings with Glasgow Coma Scale (GCS) in patients with acute traumatic brain injury
Journal of College of Medical Sciences-Nepal, 2014, Vol-10, No-2 ABSTRACT OBJECTIVE To correlate Computed Tomography (CT) findings with Glasgow Coma Scale (GCS) in patients with acute traumatic brain injury
A bout million patients present to UK hospitals
 420 ORIGINAL ARTICLE Application of the Canadian CT head rules in managing minor head injuries in a UK emergency department: implications for the implementation of the NICE guidelines H Y Sultan, A Boyle,
420 ORIGINAL ARTICLE Application of the Canadian CT head rules in managing minor head injuries in a UK emergency department: implications for the implementation of the NICE guidelines H Y Sultan, A Boyle,
CASE 1. Female 21 years old DOL: November 28, 2016
 CASE 1 Female 21 years old DOL: November 28, 2016 Injuries and Sequelae: GCS: 4 / 15 and coma for 3 weeks Multifocal intracranial hemorrhage at right thalamus and left frontal and temporal lobe Diffuse
CASE 1 Female 21 years old DOL: November 28, 2016 Injuries and Sequelae: GCS: 4 / 15 and coma for 3 weeks Multifocal intracranial hemorrhage at right thalamus and left frontal and temporal lobe Diffuse
Author Manuscript. Received Date : 27-Oct Revised Date : 09-Jan-2017 Accepted Date : 31-Jan-2017
 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 Received Date : 27-Oct-2016 Revised Date : 09-Jan-2017 Accepted Date : 31-Jan-2017 Article type ABSTRACT : Original Contribution
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 Received Date : 27-Oct-2016 Revised Date : 09-Jan-2017 Accepted Date : 31-Jan-2017 Article type ABSTRACT : Original Contribution
The Role of Neuroimaging in Sport-Related Concussion
 The Role of Neuroimaging in Sport-Related Concussion Sanjay P. Prabhu, MBBS, FRCR a,b, * KEYWORDS Concussion Neuroimaging Sport-related Individuals engaged in various sports and recreational physical activities
The Role of Neuroimaging in Sport-Related Concussion Sanjay P. Prabhu, MBBS, FRCR a,b, * KEYWORDS Concussion Neuroimaging Sport-related Individuals engaged in various sports and recreational physical activities
THE ROLE OF IMAGING IN DIAGNOSIS OF SUBDURAL HEMATOMA: REVIEW ARTICLE
 THE ROLE OF IMAGING IN DIAGNOSIS OF SUBDURAL HEMATOMA: REVIEW ARTICLE * Dr. Sumendra Raj Pandey, Prof. Dr. Liu Pei WU, Dr. Sohan Kumar Sah, Dr. Lalu Yadav, Md. Sadam Husen Haque and Rajan KR. Chaurasiya
THE ROLE OF IMAGING IN DIAGNOSIS OF SUBDURAL HEMATOMA: REVIEW ARTICLE * Dr. Sumendra Raj Pandey, Prof. Dr. Liu Pei WU, Dr. Sohan Kumar Sah, Dr. Lalu Yadav, Md. Sadam Husen Haque and Rajan KR. Chaurasiya