Neuroradiology: Imaging and Stroke
|
|
|
- Stanley Hudson
- 6 years ago
- Views:
Transcription
1 Neuroradiology: Imaging and Stroke Stroke 2017 William Gallmann January 28, 2017
2 Stroke Arterial ischemia/infarct accounts for ~85% Cerebral venous occlusions % Spontaneous intracranial hemorrhage (ICH)~15% Hypertension (50%) Amyloid angiopathy (20%) Others (tumor, vascular malformation, coagulopathy) (30%)
3 Arterial Ischemic Stroke Etiology Atherosclerotic vascular disease (ASVD) (40-45%) Most infarcts are embolic, arising from an at risk plaque. Carotid bifurcation > cavernous ICA segment. Most frequently occluded intracranial vessel is the MCA. Small vessel disease (15-30%) Small artery occlusions (lacunar infarcts) Occlusion of perforating branches, most commonly in the basal ganglia, thalami, deep white matter, and brainstem. Cardioembolic disease (15-20%) Common risk factors include MI and arrhythmia Craniocervical artery dissection (~2%) Important cause of ischemic stroke in young and middle-aged adults
4 Acute Ischemic Stroke Terminology Cerebral ischemia- Affected tissue remains viable although blood flow is inadequate to sustain normal function. Cerebral infarction- Frank cell death occurs with loss of neurons, glia, or both. Infarct core- Center of affected parenchyma. Typically has a cerebral blood flow (CBF) <6-8 cm 3 100g/min. Ischemic penumbra- Less ischemic brain surrounding the infarct core with CBF cm 3 100g/min. Present in ~1/2 of patients. At risk but potentially salvageable tissue.
5 Imaging in Acute Stroke Clinical presentation is misleading in 15-20% of presumed strokes. Imaging has become essential in rapid stroke assessment
6 The 4 Must Know Acute Stroke Questions Is there intracranial hemorrhage (or a stroke mimic )? Is a large vessel occluded? Is part of the brain irreversibly injured? Is an ischemic penumbra present?
7 Time is Brain ~ 2 million neurons lost each minute when a major vessel such as the MCA is occluded. It is essential to initiate a CT scan within 25 minutes of arrival - Code Stroke Complete interpretation of the CT scan within 45minutes
8 The 4 Must Know Acute Stroke Questions Is there intracranial hemorrhage (or a stroke mimic )? CT Is a large vessel occluded? CTA Is part of the brain irreversibly injured? CT/MRI(DWI) Is an ischemic penumbra present? CT or MR Perfusion
9
10 CT vs MR CT Faster Cheaper More readily available More appropriate in most hospitals in the acute setting. Good at detecting acute hemorrhage Limited sensitivity in detection of hyeracute/acute infarcts MR Used at some centers as the workhorse in acute stroke workup. Far superior to CT in detecting small vessel and brainstem ischemia. Slower, but can be expedited with selection of only a few key sequences. Contraindications More expensive
11 Imaging in Acute Ischemic Stroke Relevant Pathophysiology As oxygen is depleted, cellular energy production fails, and ion homeostasis is lost. ATP dependent Na + /K + membrane pumps fail Na + accumulates in the cell, producing swelling and reduction in extracellular volume. Cytotoxic edema.
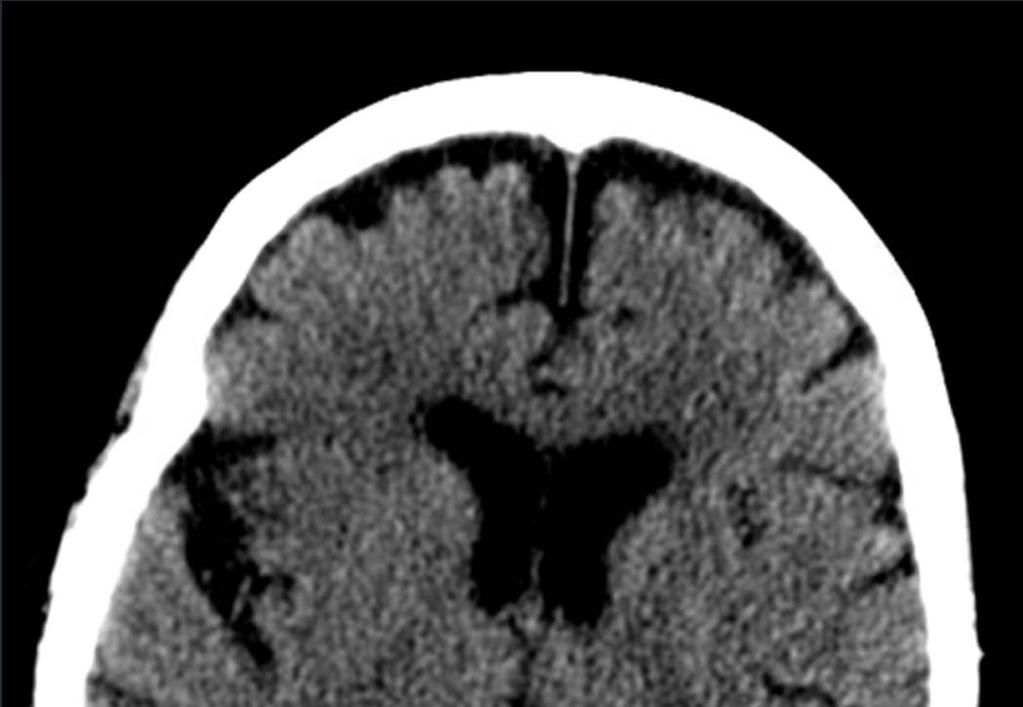
12 CT in acute infarct Initial non-enhanced CT (NECT) are abnormal in 50-60% of acute ischemic strokes. Hyperdense MCA Insular ribbon sign Disappearing basal ganglia sign Wedge shaped hypoattenuation
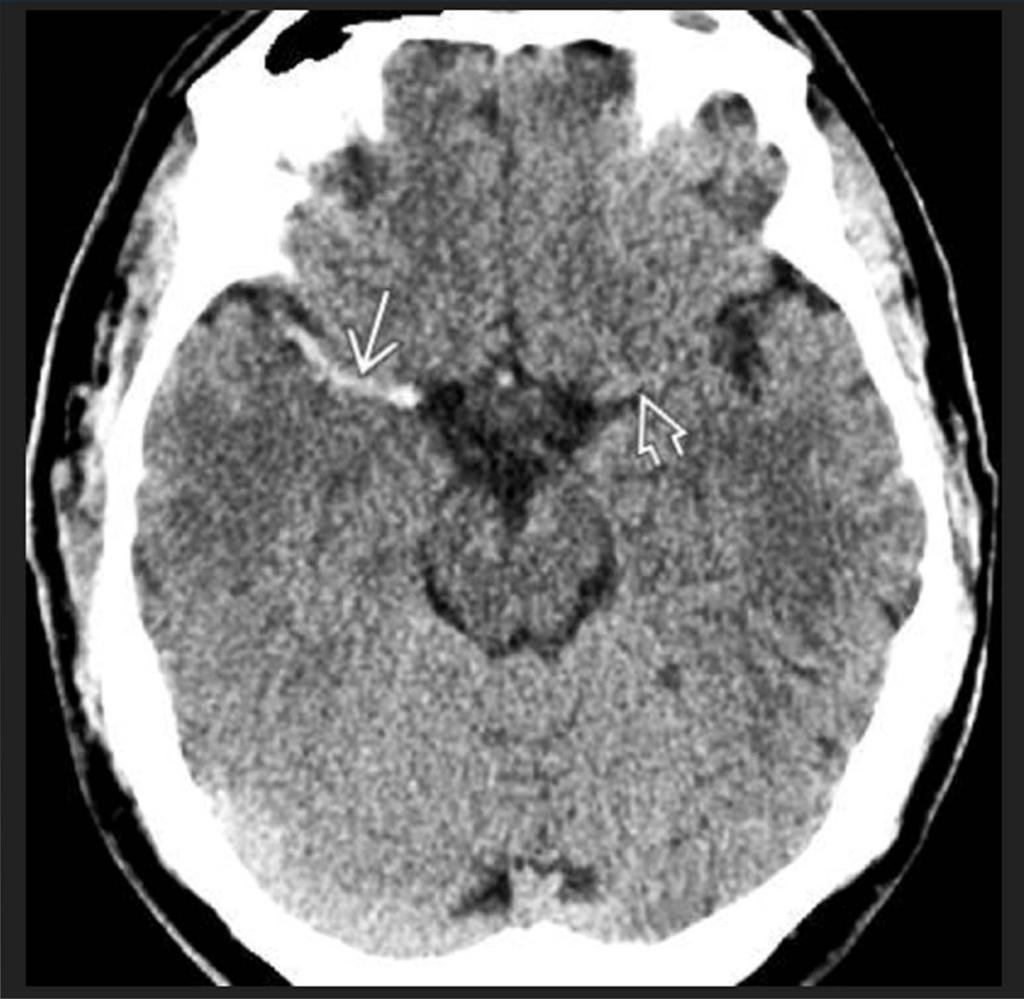
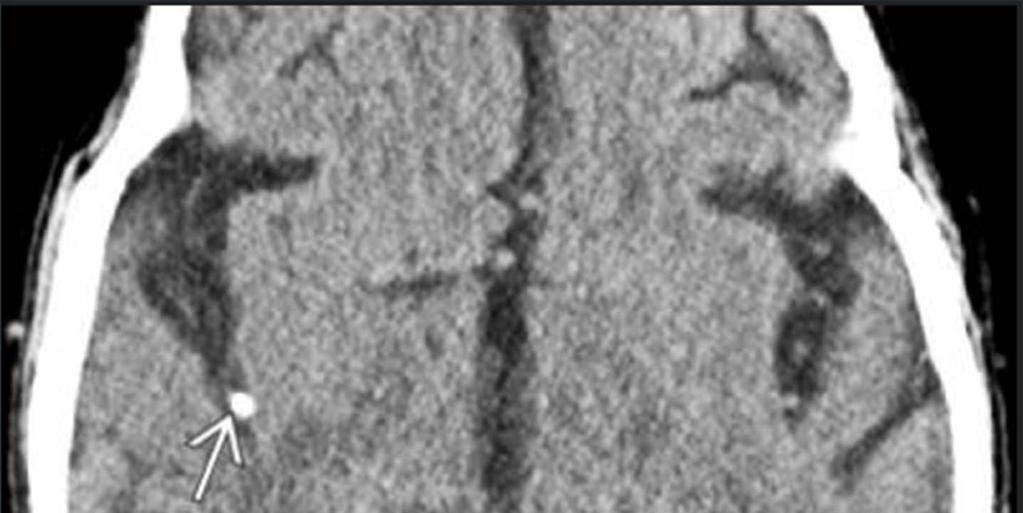
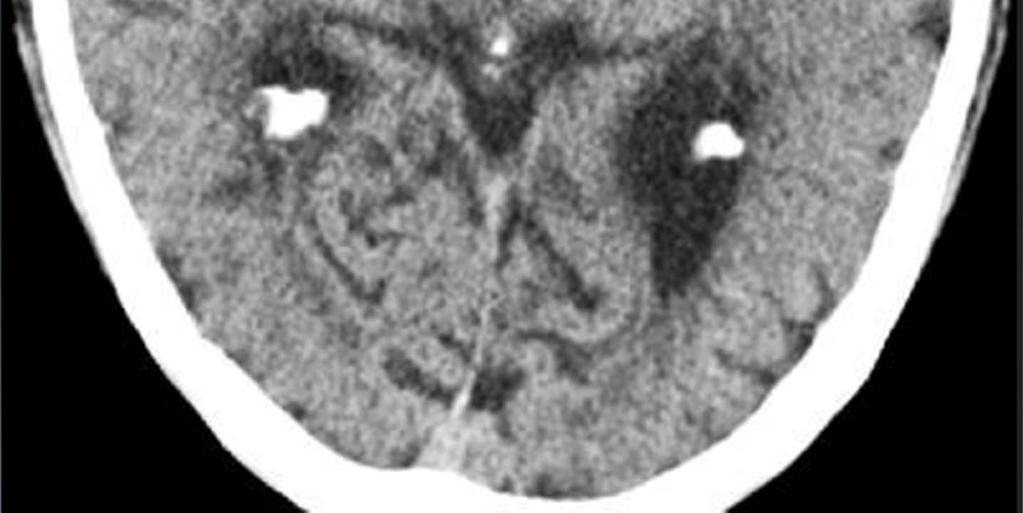
13 Hyperdense MCA Seen in 30% of cases with documented proximal MCA occlusion. Most specific but least sensitive sign of early ischemic stroke. Less common sites for a hyperdense vessel are the intracranial ICA, basilar artery, and deeper MCA branches in the sylvian fissure ( dot sign ). Remains hyperdense until the clot is lysed
14

15
16
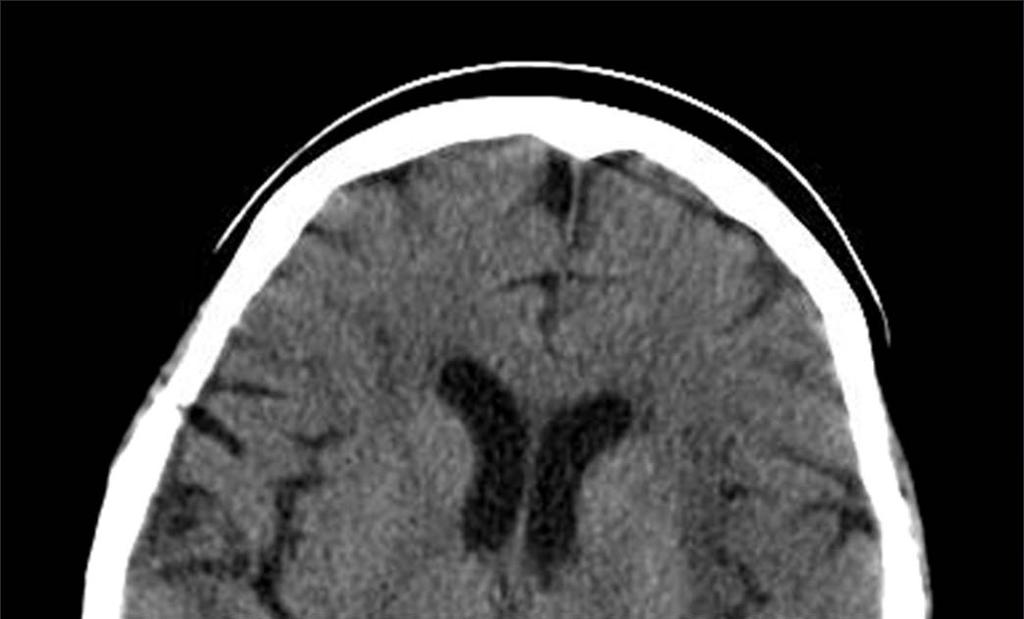
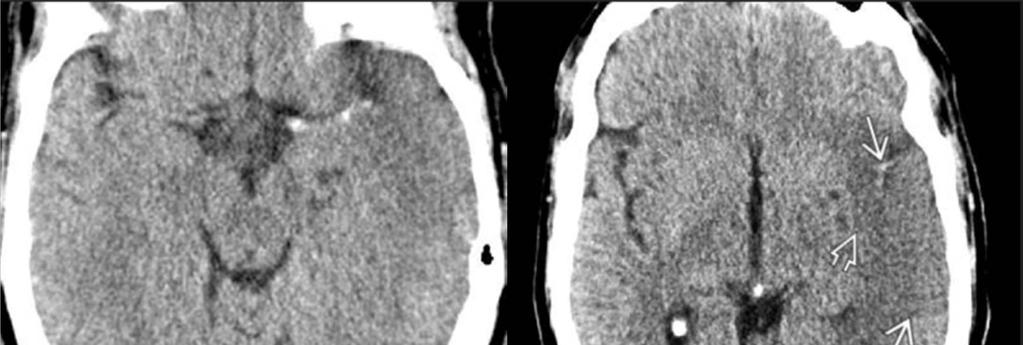
17 Early Ischemic Changes by CT Blurring and indistinctness of gray-white matter interfaces can be seen in 50-70% of cases within the first 3 hrs Insular ribbon sign- Blurring of the insular cortex and adjacent white matter. Disappearing basal ganglia sign- Edema of the basal ganglia and loss of differentiation with the internal capsule. Wedge shaped parenchymal hypodensity and cortical sulcal effacement.


18
19

20
21 Contraindications to IV-TPA on initial NECT Hemorrhage Cytotoxic edema involving greater than 1/3 of the MCA territory (~70mL). Stroke mimicker (neoplasm).
22

23


24 Alberta Stroke Program Early CT Score (ASPECTS)
25

26

27

28 Differentiating acute from chronic infarct
29 Vascular imaging in acute stroke Goal of imaging Is a large vessel occluded? Is there a critical stenosis? Degree of collateral supply? Role for endovascular therapy?
30
31 CT Angiography (CTA) Pros Faster and more readily available Very accurate in detecting thrombus and degree of stenosis Less prone to motion artifact in an uncooperative patient Less contraindications Reveal access limitations for endovascular treatment Assess collaterals Cons IV contrast Radiation *NECT should always accompany CTA head + neck

32

33
34
35
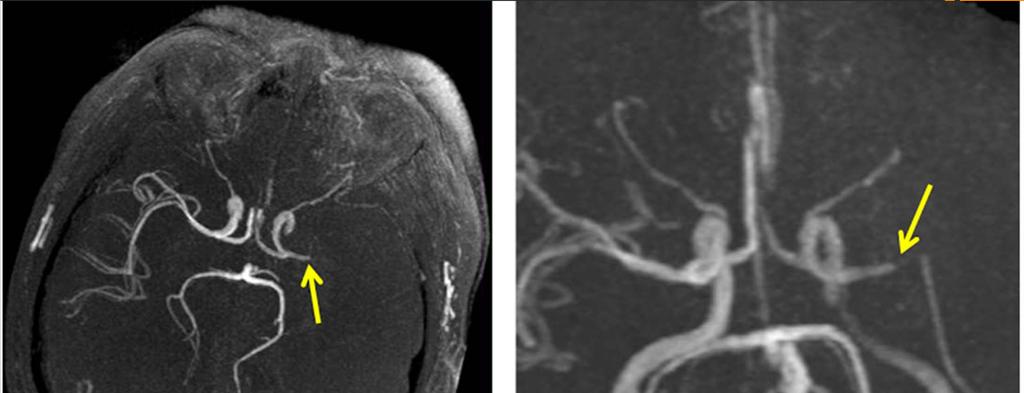
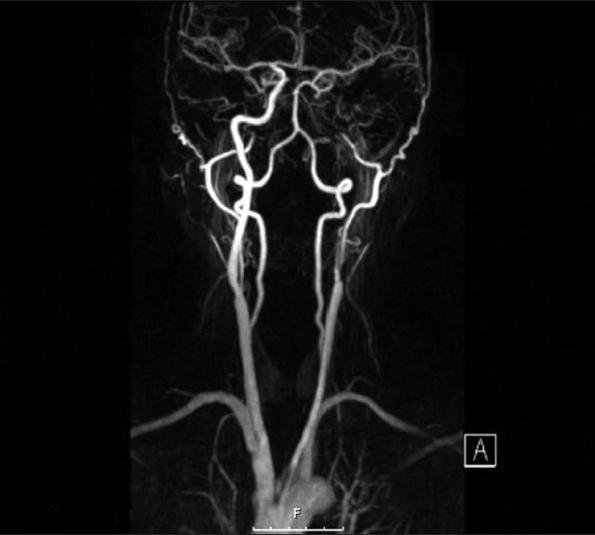
36 MR Angiography Pros Time of Flight allows for dynamic vessel assessment without contrast Better at diagnosing dissection No radiation Cons Time Contraindications Motion artifact *can do MRA neck with and without contrast *MRA head w/o only.

37
38
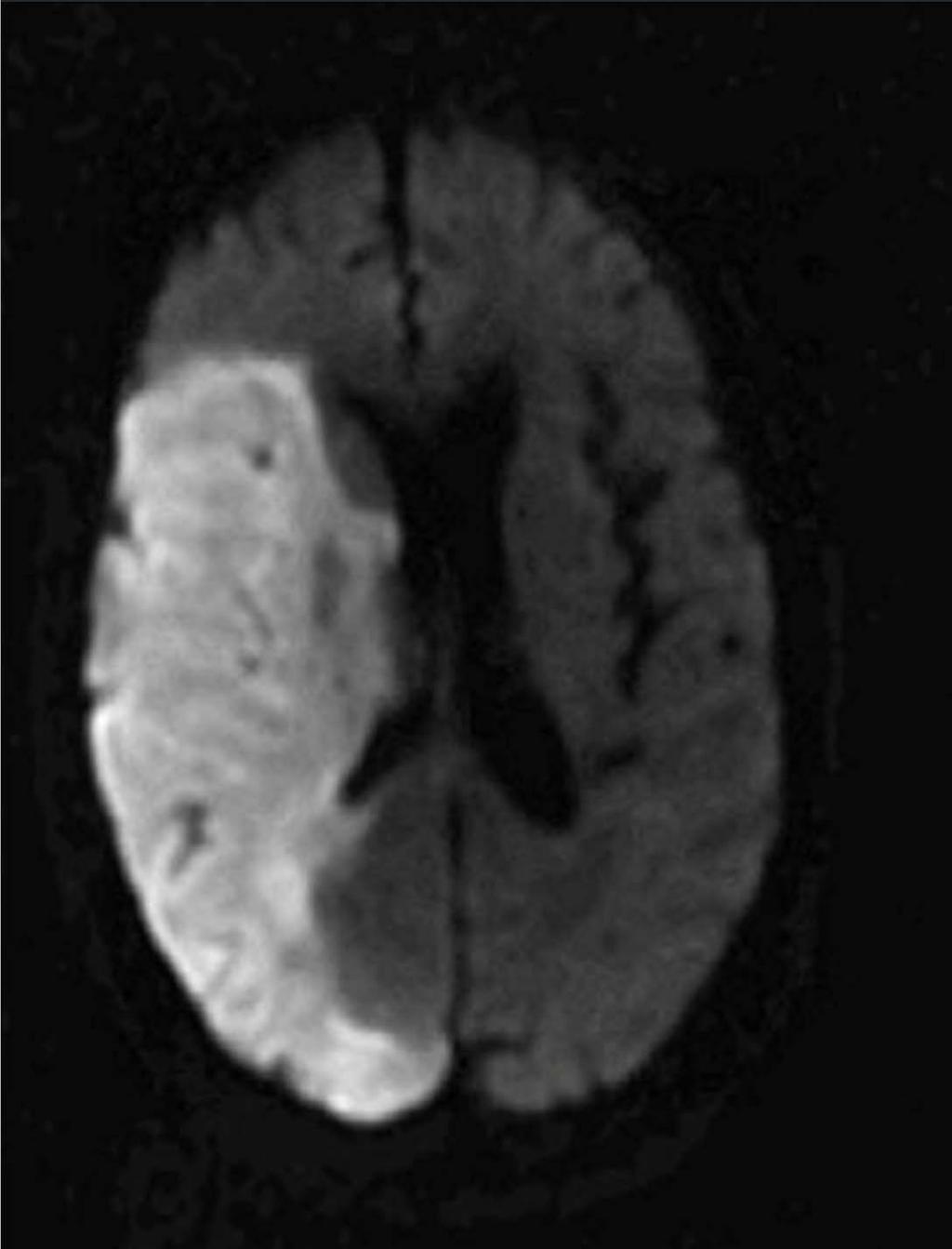
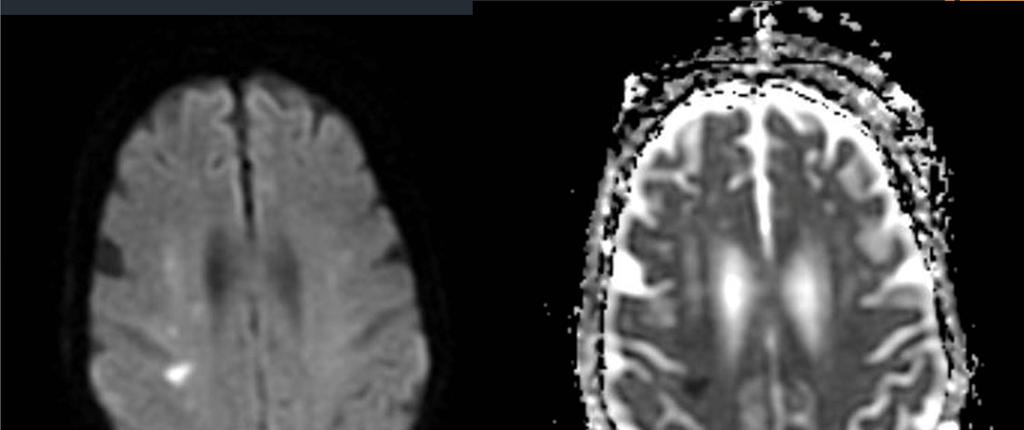
39 MRI in Acute Stroke Diffusion Weighted Imaging (DWI) Gold standard in assessing infarct core. Positive within minutes of ischemic insult. High signal on DWI. Low signal on ADC % sensitive for detection of acute/hyperacute infarcts
40
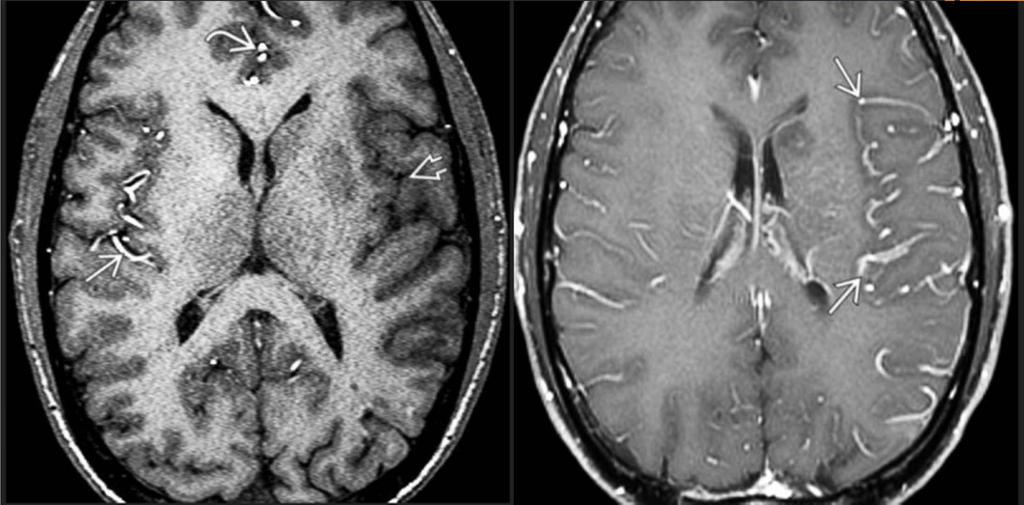
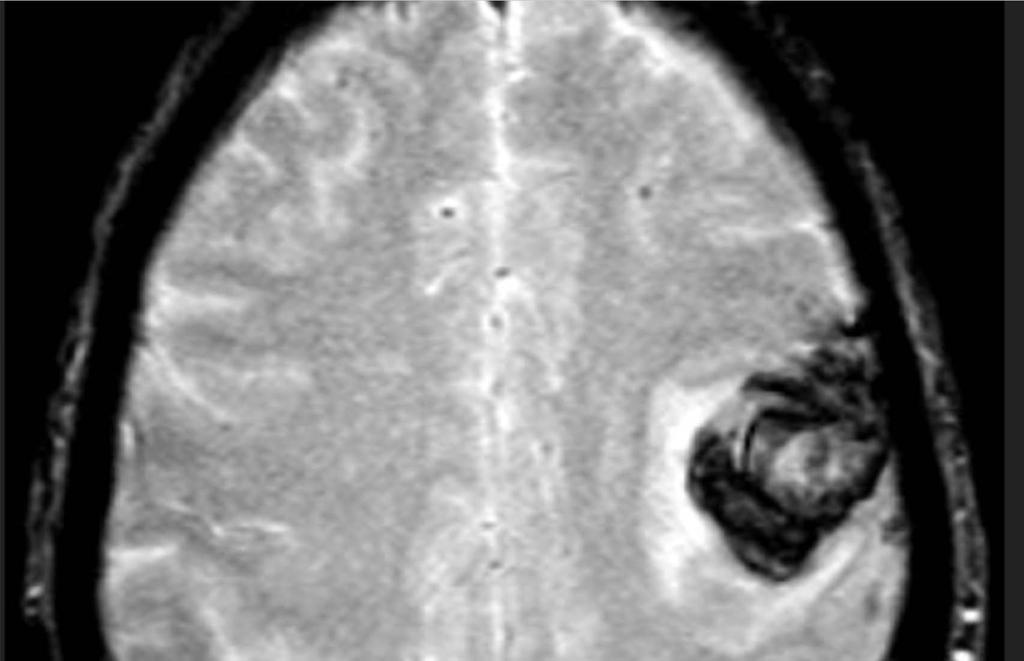
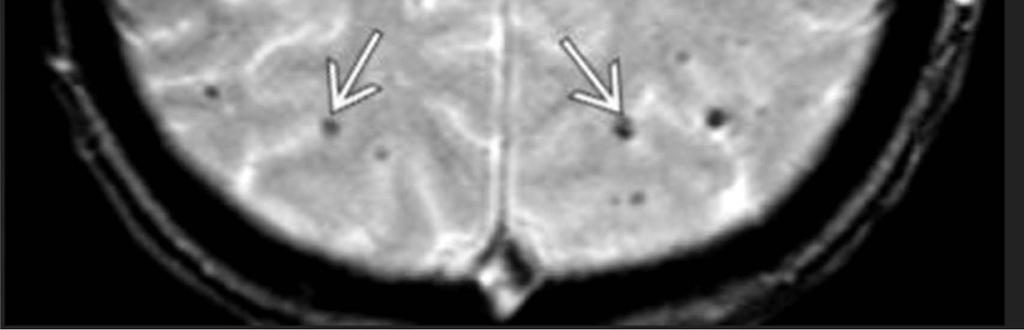
41 MRI in Acute Stroke T1WI Usually normal in first 3-6hr Subtle gyral swelling/edema (low signal) within 12-24hr. T2/FLAIR Increased signal and swelling % of acute strokes visible on FLAIR within first 4 hrs. Nearly all are positive on FLAIR by 7 hrs. Loss of flow void due to slow flow or occlusion. T2* Intra-arterial thrombus blooming. Can identify petechial hemorrhage T1C+ Intravascular enhancement due to slow flow.

42
43
44
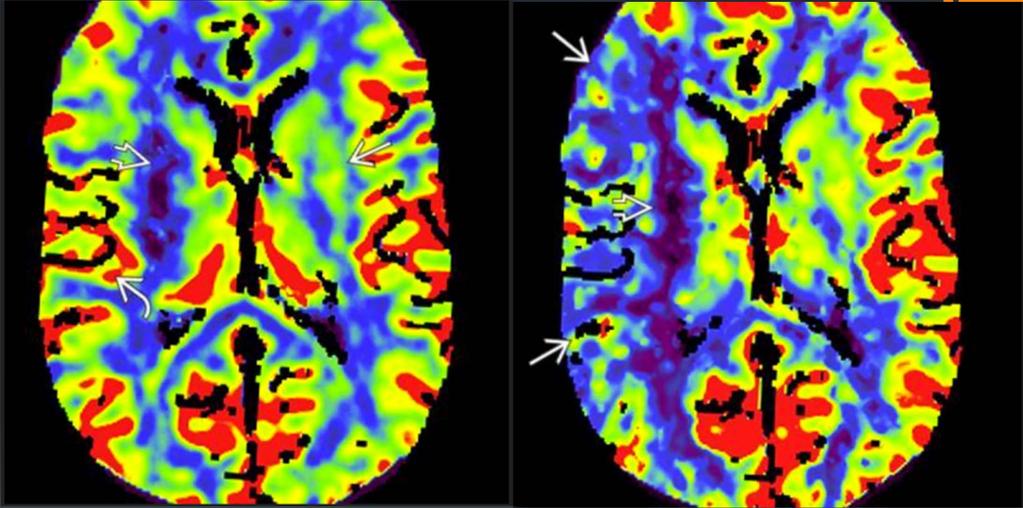
45 Perfusion Imaging Can be performed with CT or MR Rapid dynamic imaging of the brain following contrast administration allows for quantification of cerebral blood volume (CBV), flow (CBF), and mean transit time (MTT) Infarct core - CBV and CBF are decreased. MTT is prolonged. Ischemic penumbra CBF decreased, CBV normal or increased. MTT prolonged. Potentially salvageable brain tissue is equivalent to CBF - CBV
46 CBV CBF
47 Perfusion Imaging Pros and Cons Pros Identifies core infarct Identifies penumbra Cons Time (~25-30min) Limited brain coverage Very susceptible to motion Contrast required High radiation dose
48 Imaging in subacute stroke Generally refers to 2 days-2weeks Edema and mass effect peak at 3-4 days Hemorrhagic transformation (HT) occurs in 20-25% of cases Ischemia damaged endothelium becomes leaky CT Wedge-shaped area more sharply defined Mass effect increases with herniation in some cases HT seen as gyriform or basal ganglia hyperdensity MR Increased T2/FLAIR signal and swelling Enhancement typical (2-2-2 rule). DWI remains bright, though ADC gradually becomes less dark


49


50
51

52
53 Know when to consult Neurosurgery Complications from stroke usually occur in the subacute setting Mass effect, herniation decompressive craniectomy Hydrocephalus ventriculostomy Hemorrhagic transformation larger than 30cc decompression

54
55 Imaging in Chronic infarct Beyond 2-3 weeks Progressive volume loss and gliosis (scar) CT Sharply delineated wedge-shaped hypodense area in a vascular territory. Adjacent sulci are ventricle enlarged. MR Near CSF equivalent signal intensity. Peripheral rim of increased FLAIR signal (gliosis) Wallerian degeneration with an ipsilateral small cerebral peduncle. No restricted diffusion.
56
57
58 Miscellaneous Stroke Subtypes Cardiac and atheromatous emboli Lacunar infarcts Watershed
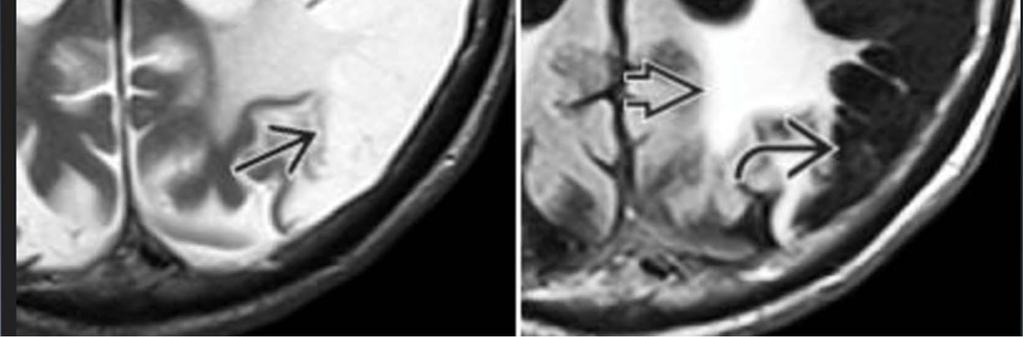
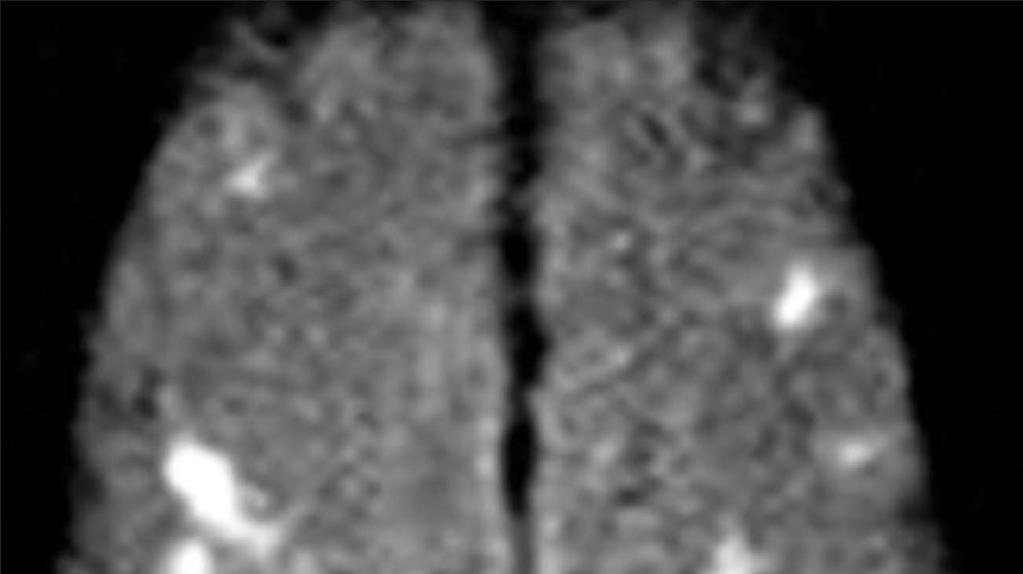
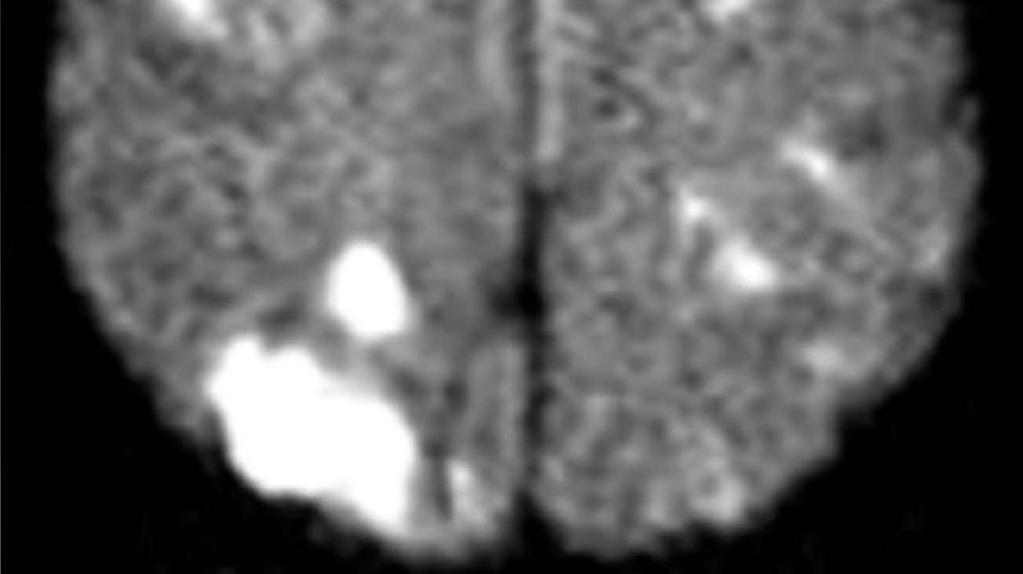
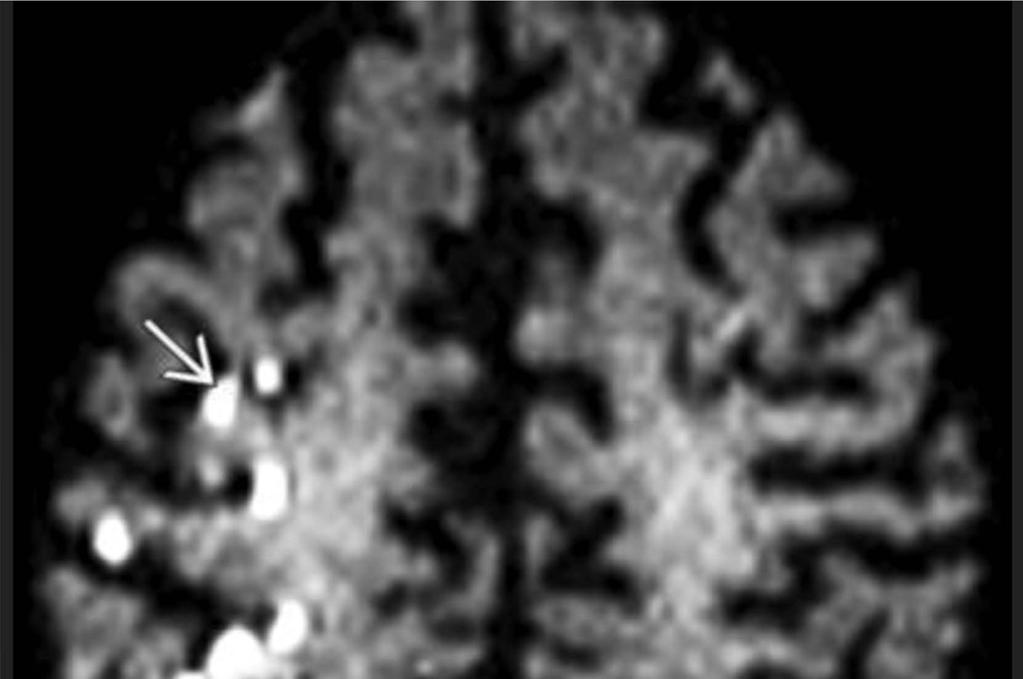
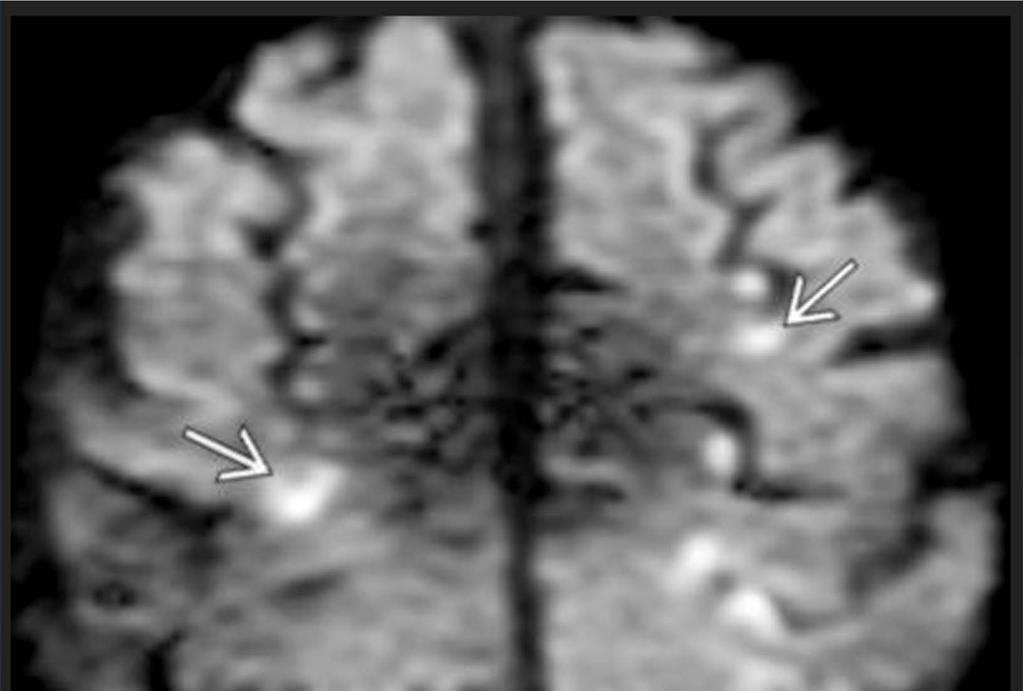
59 Cardiac and atheromatous emboli Simultaneous small infarcts in multiple different vascular distributions. Heart is most common source. Ipsilateral hemispheric emboli most commonly due to ICA Fat emboli rare but can occur following long bone fracture Emboli usually land near the gray/white junction
60
61
62 Lacunar Infarcts 25% of all ischemic strokes 15mm or less Atherosclerotic occlusion of tiny perforating branches Very small end arteries with few collaterals May or may not be symptomatic CT Usually not visible acutely. Chronic small holes in the deep gray or central white matter MR T1 dark and T2 bright holes Periphery is bright on FLAIR Restricted diffusion acutely
63
64
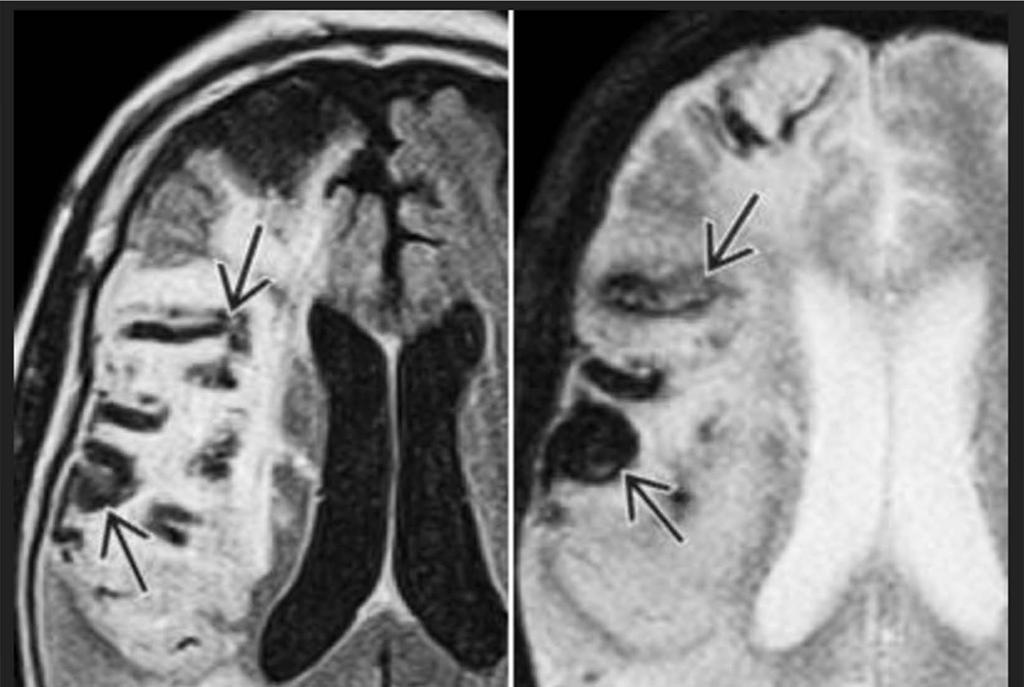
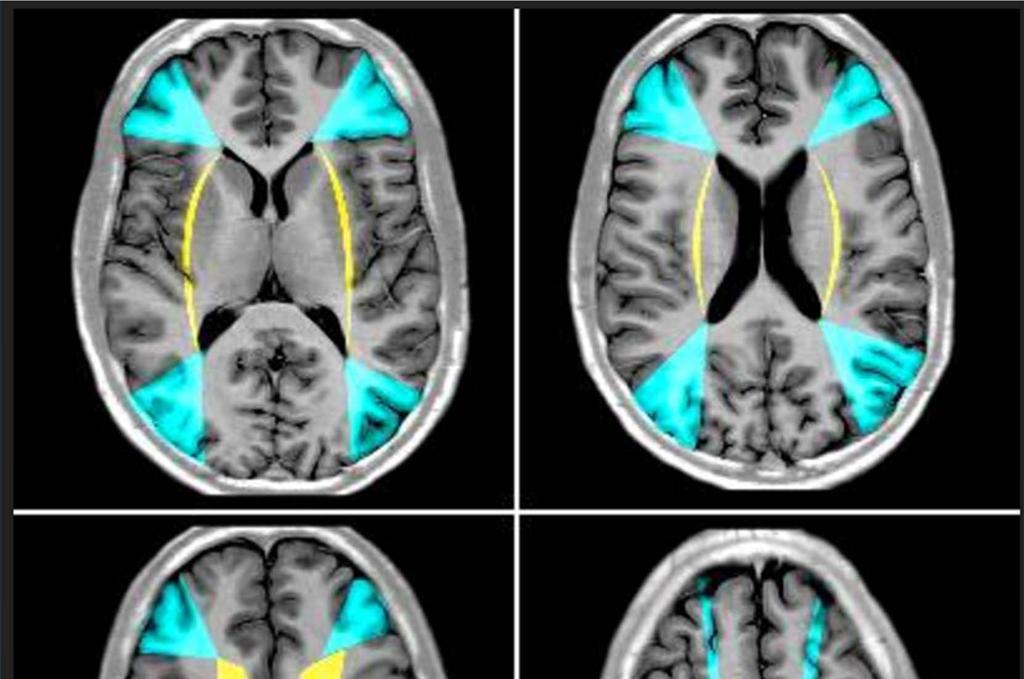
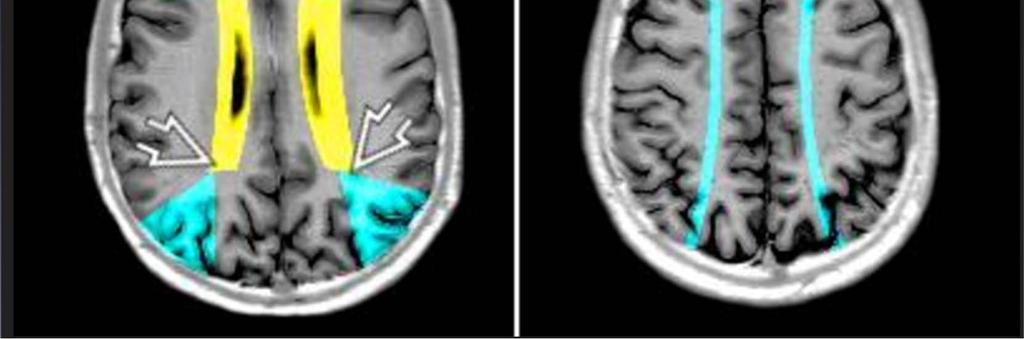
65 Watershed Infarct Occur at the junction between 2 arterial distributions 10-12% of infarcts Secondary to hypotension and/or severe proximal stenosis, most commonly the ICA Hypoperfusion and microemboli both proposed etiologies Imaging Internal border zone- Several small infarcts in a linear fashion parallel to the lateral ventricle in the periventricular white matter. External border zone- Small or confluent infarcts at the junction of the ACA/MCA or MCA/PCA
66

67

68
69 Craniocervical Artery Dissection Vessel wall tear permitting blood to penetrate into the wall layers, causing luminal narrowing/occlusion. Often associated with thrombosis, embolism, and pseudoaneurysm Cause 2% of ischemic strokes 60% are spontaneous, others post-traumatic Underlying collagen vascular disease predisposes Extracranial ICA most common followed by vertebral artery


70
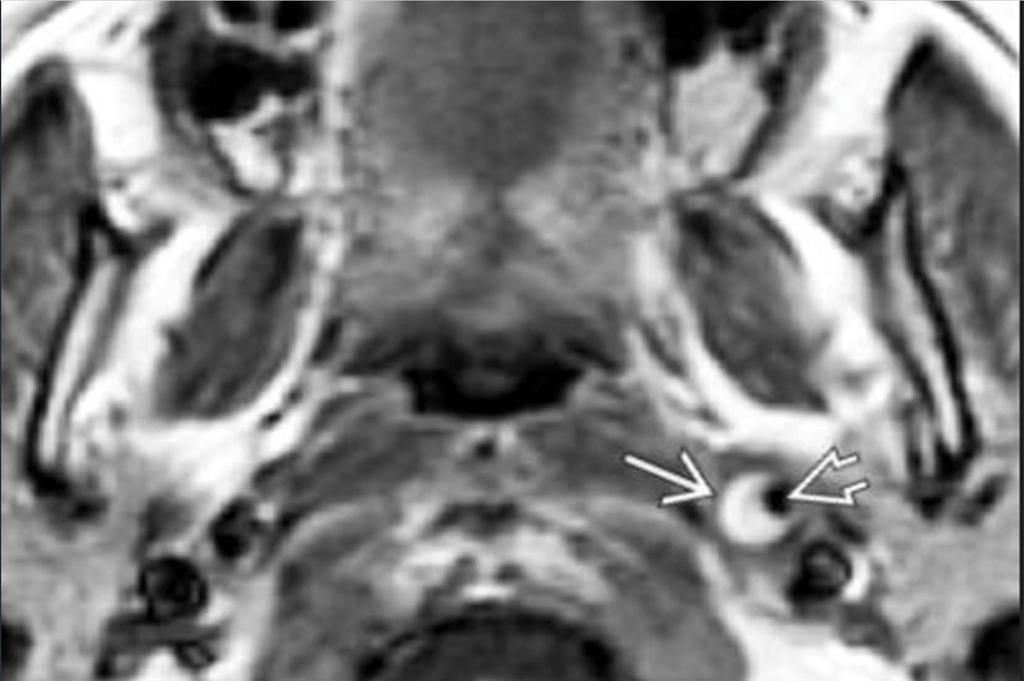
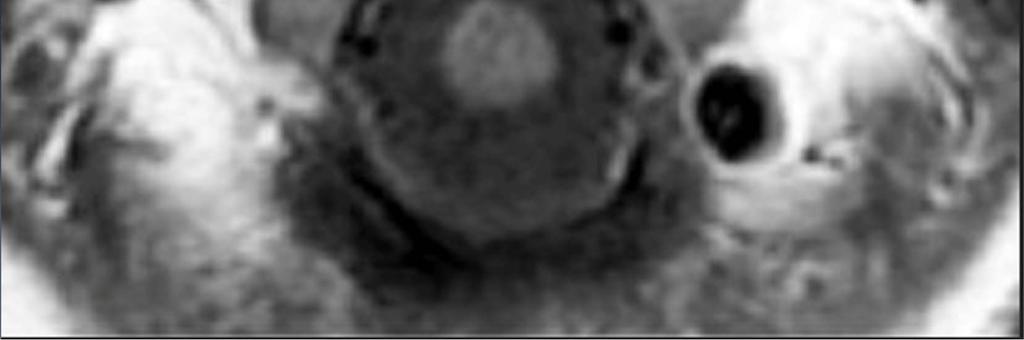
71
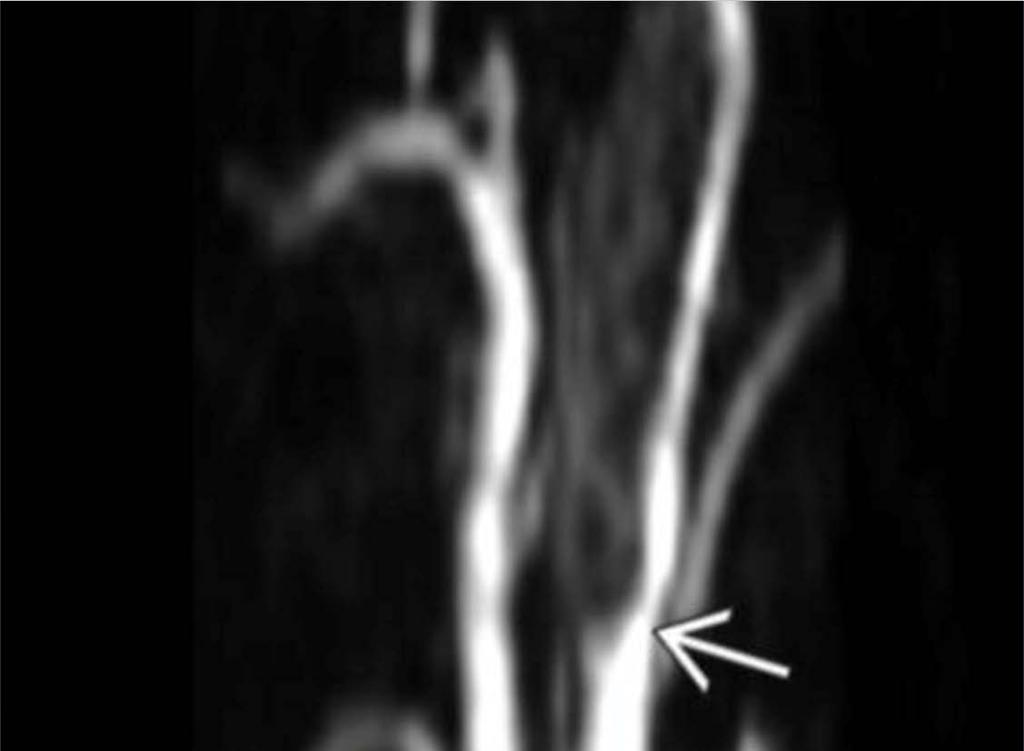
72
73 Cerebral Venous Thrombosis 0.5-1% of all acute strokes OCPs, hypercoagulable state, pregnancy, dehydration, infection Transverse sinus most common, followed by SSS Most common in young women Imaging Hyperdense vein on NECT Filling defect on CTA/CTV Loss of flow void on MRI Infarct in venous, not arterial territory More vasogenic, less cytotoxic edema More prone to hemorrhage.

74

75

76
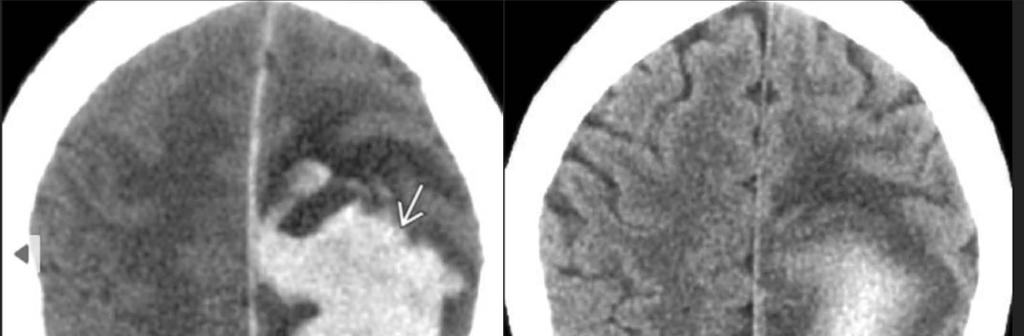
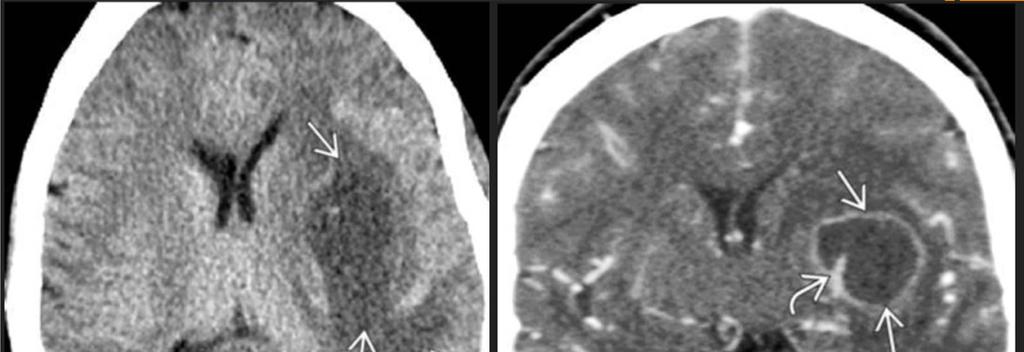
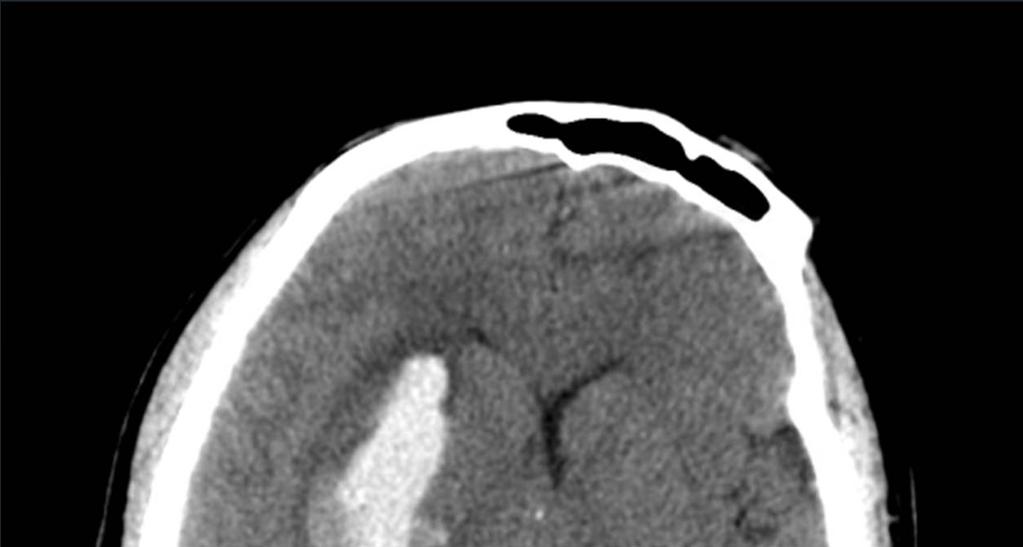
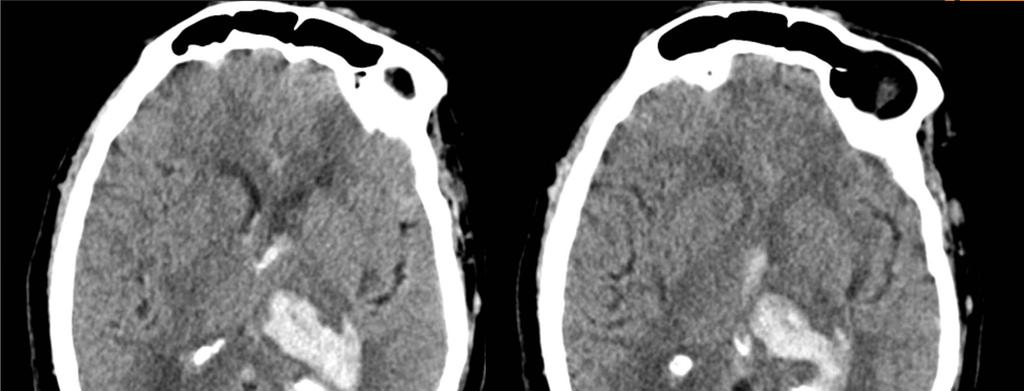
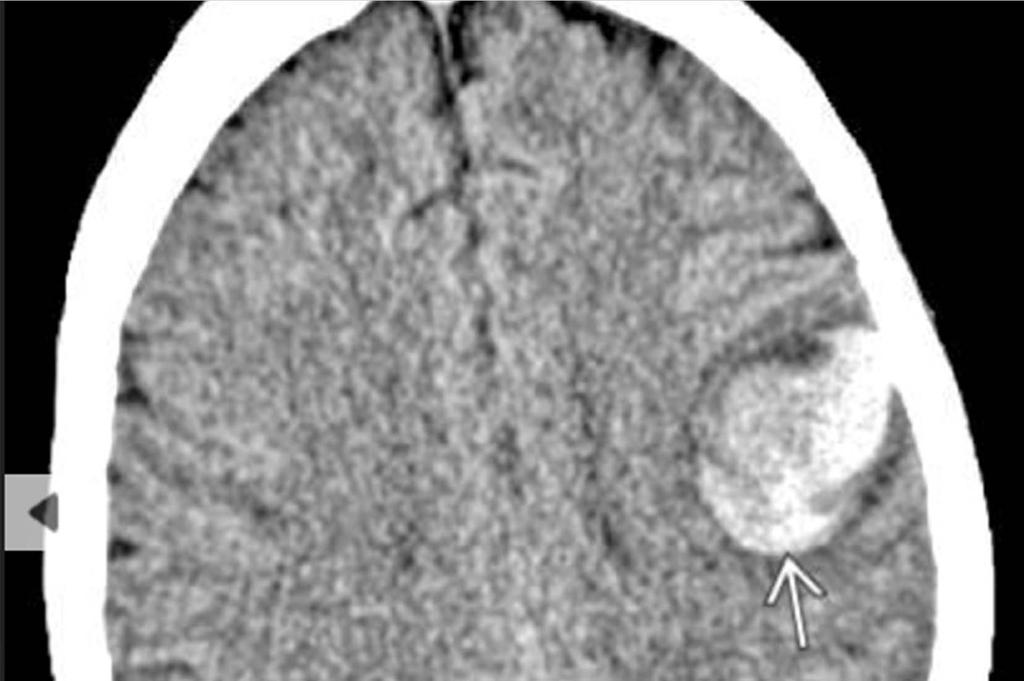
77 Spontaneous Intracranial Hemorrhage (sich) 15% of all strokes 70-80,000 /yr Common etiologies vary based on age Young adults Vascular malformation Drug abuse Middle aged and elderly Hypertension Amyloid angiopathy Neoplasm Coagulopathy
78 Role of Imaging in sich Identify presence and location of a clot Age the clot Identify mass effect and hydrocephalus Detect other findings that may be clues to its etiology If hemorrhage etiology is not clear by location/morphology, secondary imaging (MRI/CTA) necessary. Know when to consult neurosurgery
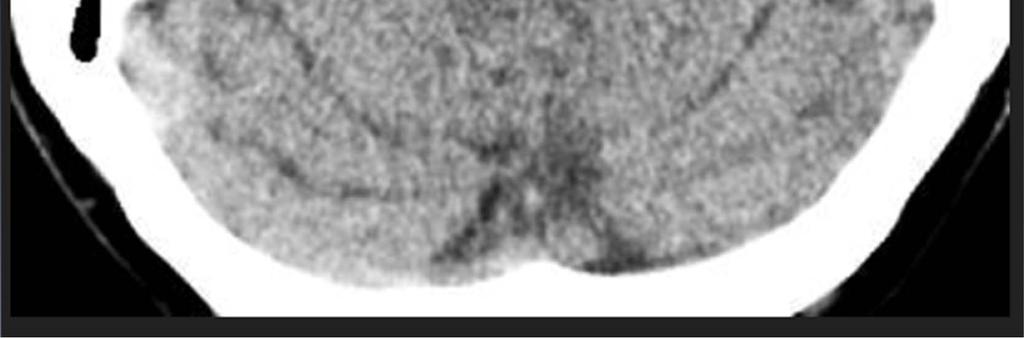
79 CT Hyperacute (Minutes to Hours) iso or even hypodense to brain Acute (Hours-days) Hyperdense Subacute (Days-weeks) Gradually becomes less dense. After days, the hematoma will become similar in density to brain. Can get ring enhancement Chronic- Small hemorrhages may become invisible. Larger ones leav a slit-like defect.

80

81
82 Hypertensive Hemorrhage Accounts for ~50% of sich in adults Accelerated atherosclerosis formation of small pseduoaneurysm ( Charcot-Bouchard aneurysms ). Rupture hemorrhage Location Putamen/External capsule (striatocapsular) (50-60%) Thalamus (15-25%) Pons (10%) Cerebellum (dentate nucleus) (10%) Lobar hemorrhage (5%) Microbleeds tend to cluster in the basal ganglia and cerebellum

83

84

85
86
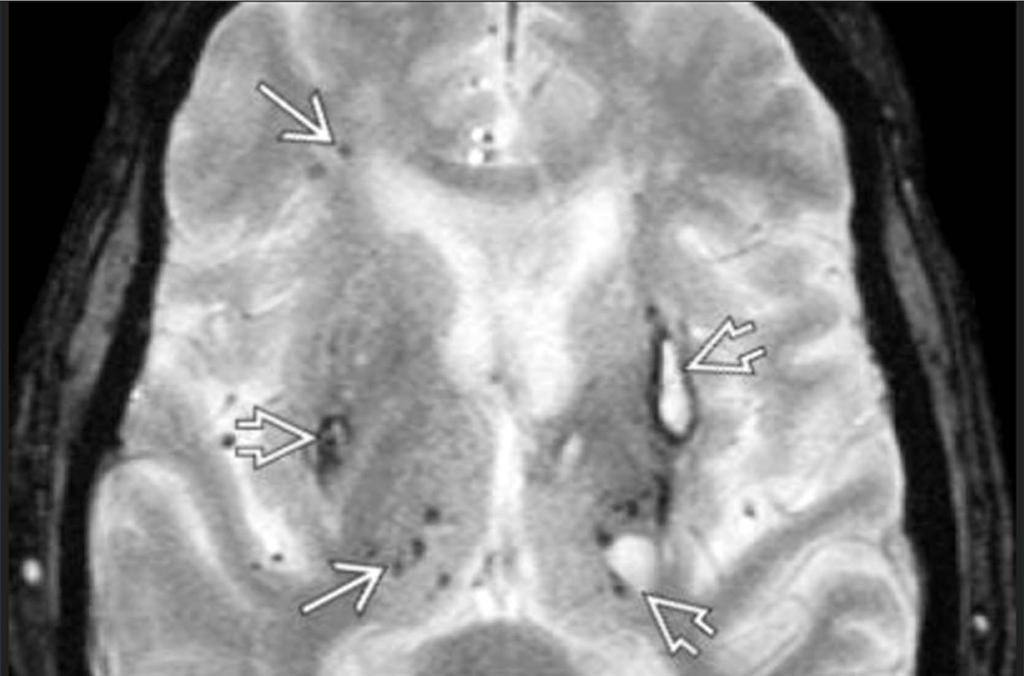
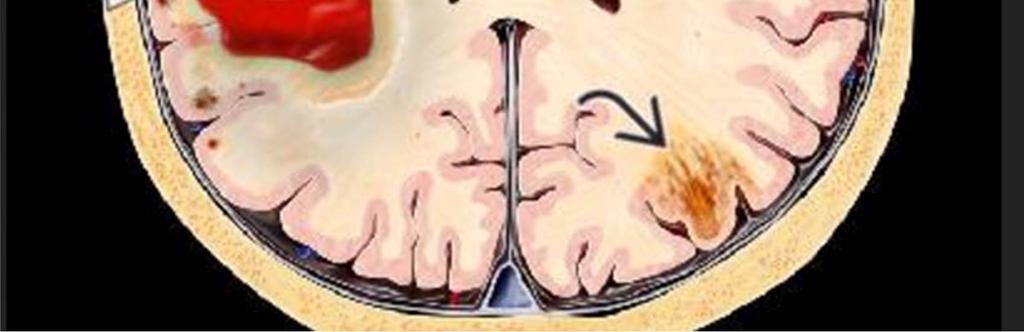
87 Amyloid Angiopathy 20% of hemorrhages in patients >60 Mean age 73 The most common of 3 varieties of cerebral amyloid deposition disease Amyloid beta accumulates in small vessels Imaging Lobar hemorrhage Multiple white matter lesions Multiple punctate microhemorrhage, more peripheral than in hypertension

88
89
90
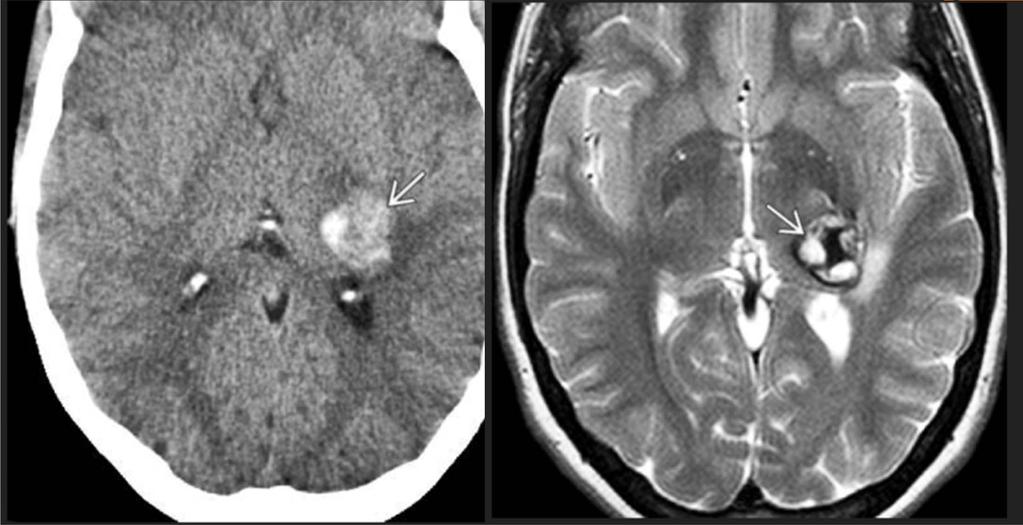
91 Vascular Malformations Diverse group of lesions, some of which are prone to rupture Types associated with hemorrhage Arteriovenous malformation (AVM) Dural AV fistula Cerebral Cavernous malformation

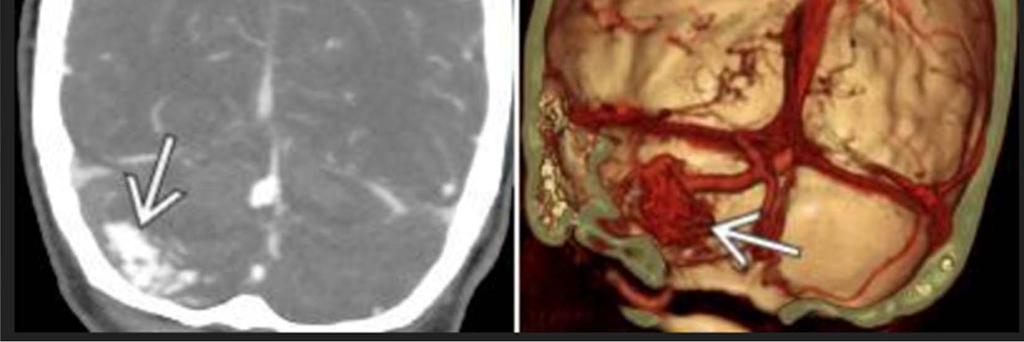
92
93
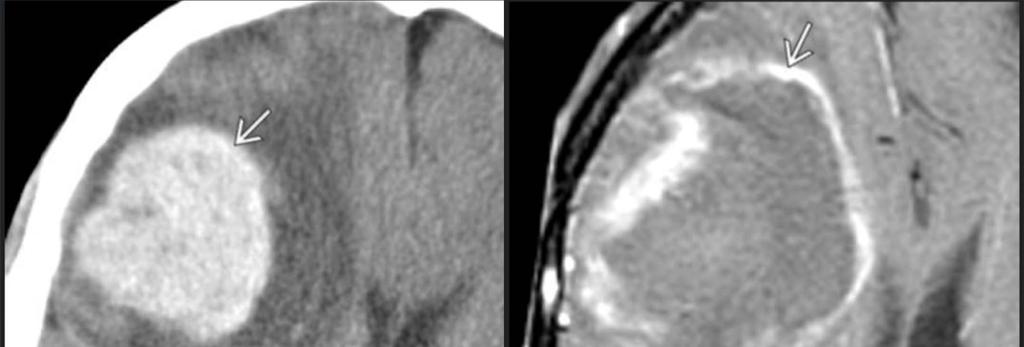
94 Hemorrhagic Neoplasm 10% of sich Usually a high-grade GBM or hemorrhagic mets from an extracranial primary such as renal cell carcinoma.

95
96 In Summary Time is brain Know and utilize the new stroke imaging algorithm Identify early signs of stroke Know the contraindications to TPA Hemorrhage Large amount of edema Stroke mimicker Understand strengths/weaknesses of CT/MR and appropriate ordering practices Know when to consult neurosurgery.
97 References Osborn, Anne. Osborn s Brain:Imaging, Pathology, and Anatomy Amirsys Jan 2013 Goyal M, Menon BK, Derdeyn CP (2013) Perfusion imaging in acute ischemic stroke: let us improve the science before changing clinical practice. Radiology 266:16 de Lucas EM et al: CT protocol for acute stroke: tips and tricks for general radiologists. Radiographics. 28(6): , 2008
STROKE - IMAGING. Dr RAJASEKHAR REDDY 2nd Yr P.G. RADIODIAGNOSIS KIMS,Narkatpalli.
 STROKE - IMAGING Dr RAJASEKHAR REDDY 2nd Yr P.G. RADIODIAGNOSIS KIMS,Narkatpalli. STROKE Describes a clinical event that consists of sudden onset of neurological symptoms Types Infarction - occlusion of
STROKE - IMAGING Dr RAJASEKHAR REDDY 2nd Yr P.G. RADIODIAGNOSIS KIMS,Narkatpalli. STROKE Describes a clinical event that consists of sudden onset of neurological symptoms Types Infarction - occlusion of
ISCHEMIC STROKE IMAGING
 ISCHEMIC STROKE IMAGING ผศ.พญ พญ.จ ร ร ตน ธรรมโรจน ภาคว ชาร งส ว ทยา คณะแพทยศาสตร มหาว ทยาล ยขอนแก น A case of acute hemiplegia Which side is the abnormality, right or left? Early Right MCA infarction
ISCHEMIC STROKE IMAGING ผศ.พญ พญ.จ ร ร ตน ธรรมโรจน ภาคว ชาร งส ว ทยา คณะแพทยศาสตร มหาว ทยาล ยขอนแก น A case of acute hemiplegia Which side is the abnormality, right or left? Early Right MCA infarction
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
NEURO IMAGING 2. Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity
 NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
Essentials of Clinical MR, 2 nd edition. 14. Ischemia and Infarction II
 14. Ischemia and Infarction II Lacunar infarcts are small deep parenchymal lesions involving the basal ganglia, internal capsule, thalamus, and brainstem. The vascular supply of these areas includes the
14. Ischemia and Infarction II Lacunar infarcts are small deep parenchymal lesions involving the basal ganglia, internal capsule, thalamus, and brainstem. The vascular supply of these areas includes the
UPSTATE Comprehensive Stroke Center. Neurosurgical Interventions Satish Krishnamurthy MD, MCh
 UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
Intracranial spontaneous hemorrhage mechanisms, imaging and management
 Intracranial spontaneous hemorrhage mechanisms, imaging and management Dora Zlatareva Department of Diagnostic Imaging Medical University, Sofia, Bulgaria Intracranial hemorrhage (ICH) ICH 15% of strokes
Intracranial spontaneous hemorrhage mechanisms, imaging and management Dora Zlatareva Department of Diagnostic Imaging Medical University, Sofia, Bulgaria Intracranial hemorrhage (ICH) ICH 15% of strokes
NEURO IMAGING OF ACUTE STROKE
 1 1 NEURO IMAGING OF ACUTE STROKE ALICIA RICHARDSON, MSN, RN, ACCNS-AG, ANVP-BC WENDY SMITH, MA, RN, MBA, SCRN, FAHA LYNN HUNDLEY, APRN, CNRN, CCNS, ANVP-BC 2 2 1 DISCLOSURES Alicia Richardson: Stryker
1 1 NEURO IMAGING OF ACUTE STROKE ALICIA RICHARDSON, MSN, RN, ACCNS-AG, ANVP-BC WENDY SMITH, MA, RN, MBA, SCRN, FAHA LYNN HUNDLEY, APRN, CNRN, CCNS, ANVP-BC 2 2 1 DISCLOSURES Alicia Richardson: Stryker
An Introduction to Imaging the Brain. Dr Amy Davis
 An Introduction to Imaging the Brain Dr Amy Davis Common reasons for imaging: Clinical scenarios: - Trauma (NICE guidelines) - Stroke - Tumours - Seizure - Neurological degeneration memory, motor dysfunction,
An Introduction to Imaging the Brain Dr Amy Davis Common reasons for imaging: Clinical scenarios: - Trauma (NICE guidelines) - Stroke - Tumours - Seizure - Neurological degeneration memory, motor dysfunction,
IV. Cerebrovascular diseases
 IV. Cerebrovascular diseases - Cerebrovascular disease denotes brain disorders caused by pathologic processes involving the blood vessels. - The three main pathogenic mechanisms are: 1. Thrombotic occlusion
IV. Cerebrovascular diseases - Cerebrovascular disease denotes brain disorders caused by pathologic processes involving the blood vessels. - The three main pathogenic mechanisms are: 1. Thrombotic occlusion
CT INTERPRETATION COURSE
 CT INTERPRETATION COURSE Refresher Course ASTRACAT October 2012 Stroke is a Clinical Diagnosis A clinical syndrome characterised by rapidly developing clinical symptoms and/or signs of focal loss of cerebral
CT INTERPRETATION COURSE Refresher Course ASTRACAT October 2012 Stroke is a Clinical Diagnosis A clinical syndrome characterised by rapidly developing clinical symptoms and/or signs of focal loss of cerebral
CEREBROVASCULAR DISEASES. By: Shifaa AlQa qa
 CEREBROVASCULAR DISEASES By: Shifaa AlQa qa Cerebrovascular diseases Brain disorders caused by pathologic processes involving blood vessels 3 pathogenic mechanisms (1) thrombotic occlusion, (2) embolic
CEREBROVASCULAR DISEASES By: Shifaa AlQa qa Cerebrovascular diseases Brain disorders caused by pathologic processes involving blood vessels 3 pathogenic mechanisms (1) thrombotic occlusion, (2) embolic
Acute stroke. Ischaemic stroke. Characteristics. Temporal classification. Clinical features. Interpretation of Emergency Head CT
 Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Imaging in Stroke. D Nagaraja, N Karthik
 Imaging in Stroke D Nagaraja, N Karthik Cerebro-vascular disease (stroke) is the second leading cause of death. Prior to CT era, diagnosis was essentially clinical supported by angio and lumbar puncture.
Imaging in Stroke D Nagaraja, N Karthik Cerebro-vascular disease (stroke) is the second leading cause of death. Prior to CT era, diagnosis was essentially clinical supported by angio and lumbar puncture.
On Call Guide to CT Perfusion. Updated: March 2011
 On Call Guide to CT Perfusion Updated: March 2011 CT Stroke Protocol 1. Non contrast CT brain 2. CT perfusion: contrast 40cc bolus dynamic imaging at 8 slice levels ~ 60 sec creates perfusion color maps
On Call Guide to CT Perfusion Updated: March 2011 CT Stroke Protocol 1. Non contrast CT brain 2. CT perfusion: contrast 40cc bolus dynamic imaging at 8 slice levels ~ 60 sec creates perfusion color maps
Place for Interventional Radiology in Acute Stroke
 Place for Interventional Radiology in Acute Stroke Dr Lakmalie Paranahewa MBBS, MD(Radiology), FRCR Consultant Interventional Radiologist Asiri Group of Hospitals Objectives Imaging in Stroke Neurovascular
Place for Interventional Radiology in Acute Stroke Dr Lakmalie Paranahewa MBBS, MD(Radiology), FRCR Consultant Interventional Radiologist Asiri Group of Hospitals Objectives Imaging in Stroke Neurovascular
C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical College NewYork-Presbyterian Hospital
 C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical College NewYork-Presbyterian Hospital I have no financial disclosures Understand range of pathology that may present
C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical College NewYork-Presbyterian Hospital I have no financial disclosures Understand range of pathology that may present
Disclosure. + Outline. What is a stroke? Role of imaging in stroke Ischemic stroke Venous infarct Current topics
 + Kathleen R. Fink, MD University of Washington 5 th Nordic Emergency Radiology Course May 21, 2015 + Disclosure My spouse receives research salary support from: Bracco BayerHealthcare Guerbet Thank you
+ Kathleen R. Fink, MD University of Washington 5 th Nordic Emergency Radiology Course May 21, 2015 + Disclosure My spouse receives research salary support from: Bracco BayerHealthcare Guerbet Thank you
11/1/2018. Disclosure. Imaging in Acute Ischemic Stroke 2018 Neuro Symposium. Is NCCT good enough? Keystone Heart Consultant, Stock Options
 Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
AMSER Case of the Month: March 2019
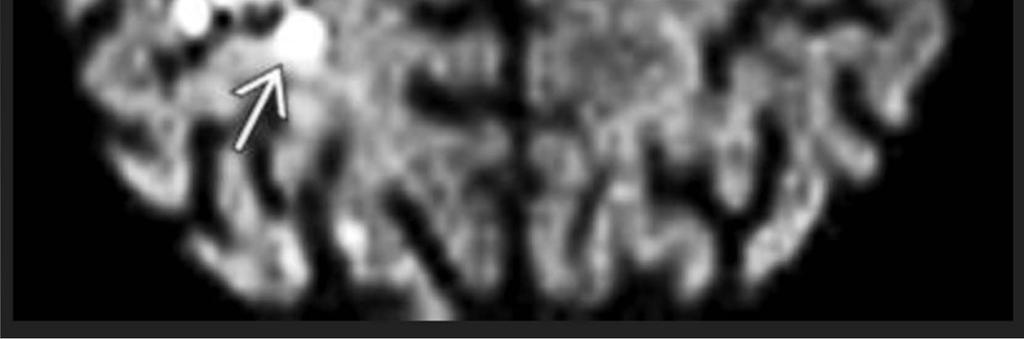
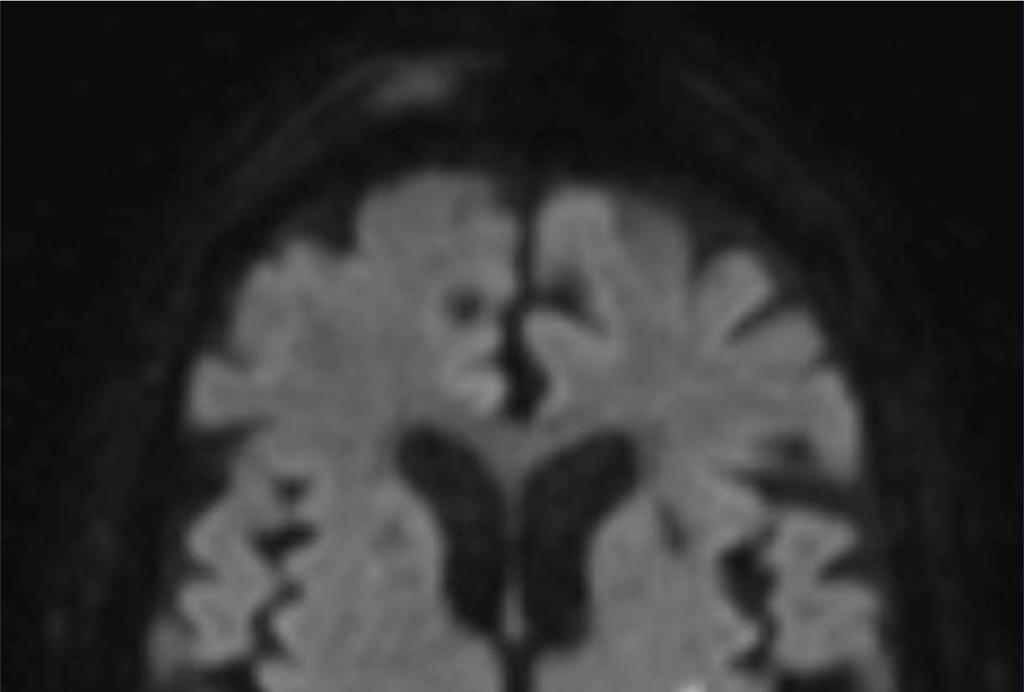
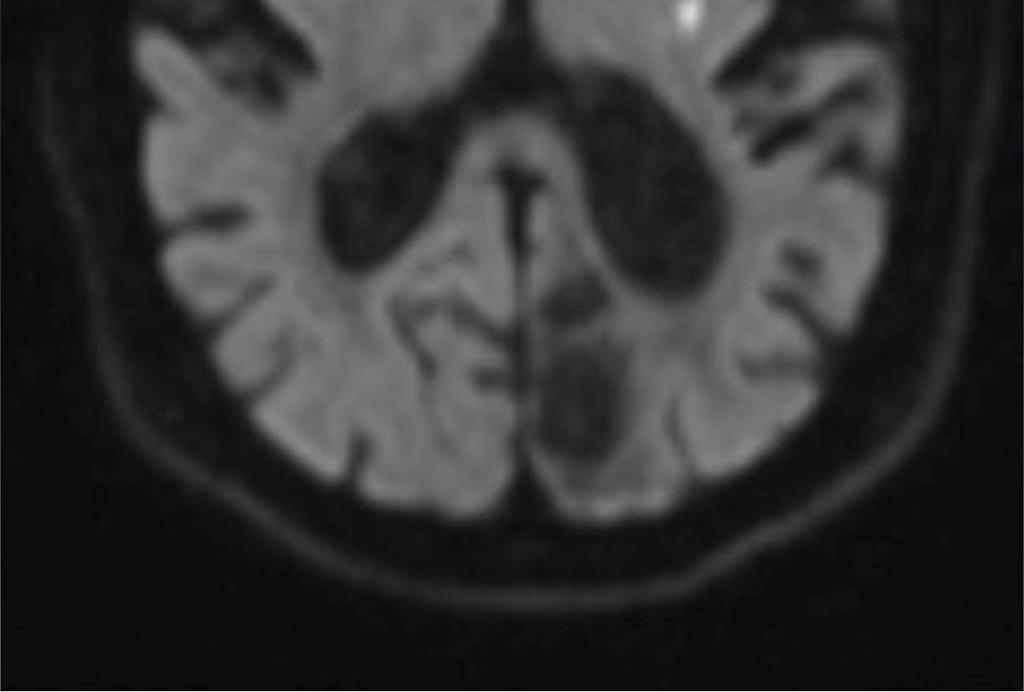
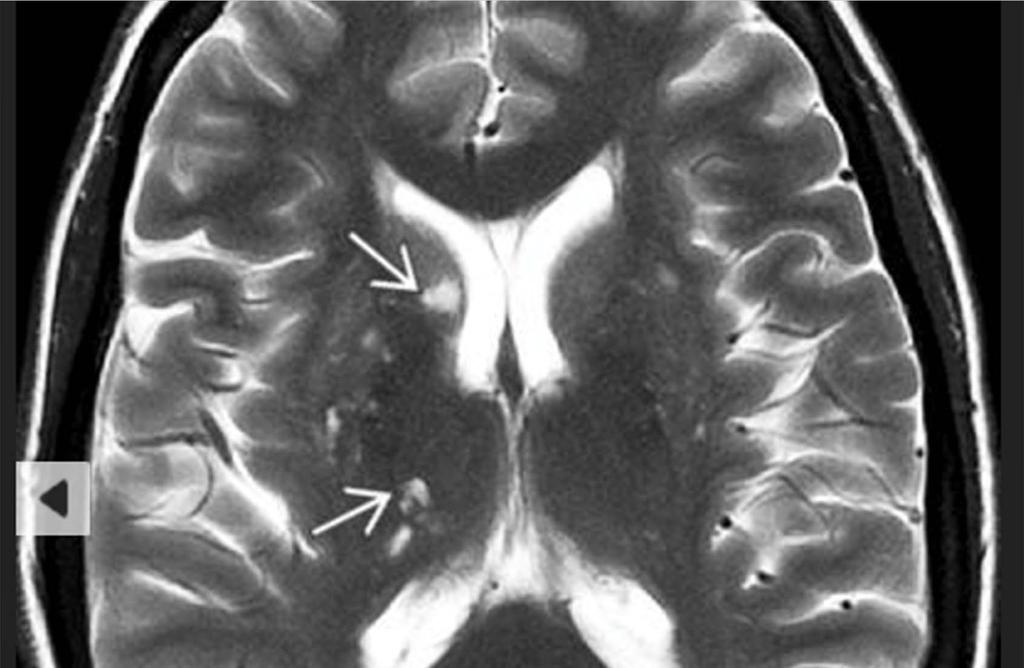
 AMSER Case of the Month: March 2019 62 year-old male with left-sided weakness Ashley Graziano OMS IV, Lake Erie College of Osteopathic Medicine Erik Yannone MD, Charles Q. Li MD, Warren Chang MD, Matthew
AMSER Case of the Month: March 2019 62 year-old male with left-sided weakness Ashley Graziano OMS IV, Lake Erie College of Osteopathic Medicine Erik Yannone MD, Charles Q. Li MD, Warren Chang MD, Matthew
Cerebrovascular diseases-2
 Cerebrovascular diseases-2 Primary angiitis of CNS - Other causes of infarction i. Hypercoagulable states ii. Drug-abuse such as amphetamine, heroin and cocain Note - The venous side of the circulation
Cerebrovascular diseases-2 Primary angiitis of CNS - Other causes of infarction i. Hypercoagulable states ii. Drug-abuse such as amphetamine, heroin and cocain Note - The venous side of the circulation
Imaging Acute Stroke and Cerebral Ischemia
 Department of Radiology University of California San Diego Imaging Acute Stroke and Cerebral Ischemia John R. Hesselink, M.D. Causes of Stroke Arterial stenosis Thrombosis Embolism Dissection Hypotension
Department of Radiology University of California San Diego Imaging Acute Stroke and Cerebral Ischemia John R. Hesselink, M.D. Causes of Stroke Arterial stenosis Thrombosis Embolism Dissection Hypotension
IMAGING IN ACUTE ISCHEMIC STROKE
 IMAGING IN ACUTE ISCHEMIC STROKE Timo Krings MD, PhD, FRCP (C) Professor of Radiology & Surgery Braley Chair of Neuroradiology, Chief and Program Director of Diagnostic and Interventional Neuroradiology;
IMAGING IN ACUTE ISCHEMIC STROKE Timo Krings MD, PhD, FRCP (C) Professor of Radiology & Surgery Braley Chair of Neuroradiology, Chief and Program Director of Diagnostic and Interventional Neuroradiology;
Acute stroke imaging
 Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Cerebro-vascular stroke
 Cerebro-vascular stroke CT Terminology Hypodense lesion = lesion of lower density than the normal brain tissue Hyperdense lesion = lesion of higher density than normal brain tissue Isodense lesion = lesion
Cerebro-vascular stroke CT Terminology Hypodense lesion = lesion of lower density than the normal brain tissue Hyperdense lesion = lesion of higher density than normal brain tissue Isodense lesion = lesion
Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD
 Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD Five Step Approach 1. Adequate study 2. Bone windows 3. Ventricles 4. Quadrigeminal cistern 5. Parenchyma
Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD Five Step Approach 1. Adequate study 2. Bone windows 3. Ventricles 4. Quadrigeminal cistern 5. Parenchyma
Advanced Neuroimaging for Acute Stroke
 Advanced Neuroimaging for Acute Stroke E. Bradshaw Bunney, MD, FACEP Professor Department Of Emergency Medicine University of Illinois at Chicago Swedish American Belvidere Hospital Disclosures FERNE Board
Advanced Neuroimaging for Acute Stroke E. Bradshaw Bunney, MD, FACEP Professor Department Of Emergency Medicine University of Illinois at Chicago Swedish American Belvidere Hospital Disclosures FERNE Board
NEURORADIOLOGY Part I
 NEURORADIOLOGY Part I Vörös Erika University of Szeged Department of Radiology SZEGED BRAIN IMAGING METHODS Plain film radiography Ultrasonography (US) Computer tomography (CT) Magnetic resonance imaging
NEURORADIOLOGY Part I Vörös Erika University of Szeged Department of Radiology SZEGED BRAIN IMAGING METHODS Plain film radiography Ultrasonography (US) Computer tomography (CT) Magnetic resonance imaging
ACUTE STROKE IMAGING
 ACUTE STROKE IMAGING Mahesh V. Jayaraman M.D. Director, Inter ventional Neuroradiology Associate Professor Depar tments of Diagnostic Imaging and Neurosurger y Alper t Medical School at Brown University
ACUTE STROKE IMAGING Mahesh V. Jayaraman M.D. Director, Inter ventional Neuroradiology Associate Professor Depar tments of Diagnostic Imaging and Neurosurger y Alper t Medical School at Brown University
Pearls and Pitfalls in Neuroradiology of Cerebrovascular Disease The Essentials with MR and CT
 Pearls and Pitfalls in Neuroradiology of Cerebrovascular Disease The Essentials with MR and CT Val M. Runge, MD Wendy R. K. Smoker, MD Anton Valavanis, MD Control # 823 Purpose The focus of this educational
Pearls and Pitfalls in Neuroradiology of Cerebrovascular Disease The Essentials with MR and CT Val M. Runge, MD Wendy R. K. Smoker, MD Anton Valavanis, MD Control # 823 Purpose The focus of this educational
IMAGING IN ACUTE ISCHEMIC STROKE
 IMAGING IN ACUTE ISCHEMIC STROKE Timo Krings MD, PhD, FRCP (C) Professor of Radiology & Surgery Braley Chair of Neuroradiology, Chief and Program Director of Diagnostic and Interventional Neuroradiology;
IMAGING IN ACUTE ISCHEMIC STROKE Timo Krings MD, PhD, FRCP (C) Professor of Radiology & Surgery Braley Chair of Neuroradiology, Chief and Program Director of Diagnostic and Interventional Neuroradiology;
CT INTERPRETATION COURSE
 CT INTERPRETATION COURSE Introductory Lecture on Basic Principles ASTRACAT 2012 Part One Stroke is a Clinical Diagnosis A clinical syndrome characterised by rapidly developing clinical symptoms and/or
CT INTERPRETATION COURSE Introductory Lecture on Basic Principles ASTRACAT 2012 Part One Stroke is a Clinical Diagnosis A clinical syndrome characterised by rapidly developing clinical symptoms and/or
Background. Recommendations for Imaging of Acute Ischemic Stroke: A Scientific Statement From the American Heart Association
 for Imaging of Acute Ischemic Stroke: A Scientific Statement From the American Heart Association An Scientific Statement from the Stroke Council, American Heart Association and American Stroke Association
for Imaging of Acute Ischemic Stroke: A Scientific Statement From the American Heart Association An Scientific Statement from the Stroke Council, American Heart Association and American Stroke Association
Stroke imaging. Why image stroke patients? Stroke. Treatment of infarct. Methods for infarct diagnosis. Treatment of infarct.
 Stroke imaging Stroke Infarct: -Arterial thrombosis/embolus -Hypoxic/ischemic -Venous thrombosis Non-traumatic hemorrhage: -Intracerebral -Subarachnoid Johan Wikström MD PhD Associate Professor of Radiology
Stroke imaging Stroke Infarct: -Arterial thrombosis/embolus -Hypoxic/ischemic -Venous thrombosis Non-traumatic hemorrhage: -Intracerebral -Subarachnoid Johan Wikström MD PhD Associate Professor of Radiology
Imaging Stroke: Is There a Stroke Equivalent of the ECG? Albert J. Yoo, MD Director of Acute Stroke Intervention Massachusetts General Hospital
 Imaging Stroke: Is There a Stroke Equivalent of the ECG? Albert J. Yoo, MD Director of Acute Stroke Intervention Massachusetts General Hospital Disclosures Penumbra, Inc. research grant (significant) for
Imaging Stroke: Is There a Stroke Equivalent of the ECG? Albert J. Yoo, MD Director of Acute Stroke Intervention Massachusetts General Hospital Disclosures Penumbra, Inc. research grant (significant) for
Case Conference: Neuroradiology. Case 1: Tumor Case 1: 22yo F w/ HA and prior Seizures
 Case Conference: Neuroradiology Case 1: 22yo F w/ HA and prior Seizures David E. Rex, MD, PhD Stanford University Hospital Department of Radiology Case 1: Tumor Most likely gangiloglioma, oligodendroglioma,
Case Conference: Neuroradiology Case 1: 22yo F w/ HA and prior Seizures David E. Rex, MD, PhD Stanford University Hospital Department of Radiology Case 1: Tumor Most likely gangiloglioma, oligodendroglioma,
How to interpret an unenhanced CT brain scan. Part 2: Clinical cases
 How to interpret an unenhanced CT brain scan. Part 2: Clinical cases Thomas Osborne a, Christine Tang a, Kivraj Sabarwal b and Vineet Prakash c a Radiology Registrar; b Radiology Foundation Year 1 Doctor;
How to interpret an unenhanced CT brain scan. Part 2: Clinical cases Thomas Osborne a, Christine Tang a, Kivraj Sabarwal b and Vineet Prakash c a Radiology Registrar; b Radiology Foundation Year 1 Doctor;
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
For Emergency Doctors. Dr Suzanne Smallbane November 2011
 For Emergency Doctors Dr Suzanne Smallbane November 2011 A: Orbit B: Sphenoid Sinus C: Temporal Lobe D: EAC E: Mastoid air cells F: Cerebellar hemisphere A: Frontal lobe B: Frontal bone C: Dorsum sellae
For Emergency Doctors Dr Suzanne Smallbane November 2011 A: Orbit B: Sphenoid Sinus C: Temporal Lobe D: EAC E: Mastoid air cells F: Cerebellar hemisphere A: Frontal lobe B: Frontal bone C: Dorsum sellae
Marc Norman, Ph.D. - Do Not Use without Permission 1. Cerebrovascular Accidents. Marc Norman, Ph.D. Department of Psychiatry
 Cerebrovascular Accidents Marc Norman, Ph.D. Department of Psychiatry Neuropsychiatry and Behavioral Medicine Neuropsychology Clinical Training Seminar 1 5 http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/18009.jpg
Cerebrovascular Accidents Marc Norman, Ph.D. Department of Psychiatry Neuropsychiatry and Behavioral Medicine Neuropsychology Clinical Training Seminar 1 5 http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/18009.jpg
41 year old female with headache. Elena G. Violari MD and Leo Wolansky MD
 41 year old female with headache Elena G. Violari MD and Leo Wolansky MD ? Dural Venous Sinus Thrombosis with Hemorrhagic Venous Infarct Acute intraparenchymal hematoma measuring ~3 cm in diameter centered
41 year old female with headache Elena G. Violari MD and Leo Wolansky MD ? Dural Venous Sinus Thrombosis with Hemorrhagic Venous Infarct Acute intraparenchymal hematoma measuring ~3 cm in diameter centered
Interventions in the Management of Acute Stroke. Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital
 Interventions in the Management of Acute Stroke Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital Acute stroke intervention Number of stroke patients increasing day by
Interventions in the Management of Acute Stroke Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital Acute stroke intervention Number of stroke patients increasing day by
RINGS N THINGS: Imaging Patterns in Differential Diagnosis. Anne G. Osborn, M.D.
 RINGS N THINGS: Imaging Patterns in Differential Diagnosis Anne G. Osborn, M.D. ExpDDxs: Intra-axial (Parenchymal) Lesions Ring-enhancing lesions, solitary 1 Ring-enhancing lesion crossing corpus callosum
RINGS N THINGS: Imaging Patterns in Differential Diagnosis Anne G. Osborn, M.D. ExpDDxs: Intra-axial (Parenchymal) Lesions Ring-enhancing lesions, solitary 1 Ring-enhancing lesion crossing corpus callosum
Acute Ischemic Stroke Imaging. Ronald L. Wolf, MD, PhD Associate Professor of Radiology
 Acute Ischemic Stroke Imaging Ronald L. Wolf, MD, PhD Associate Professor of Radiology Title of First Slide of Substance An Illustrative Case 2 Disclosures No financial disclosures Off-label uses of some
Acute Ischemic Stroke Imaging Ronald L. Wolf, MD, PhD Associate Professor of Radiology Title of First Slide of Substance An Illustrative Case 2 Disclosures No financial disclosures Off-label uses of some
L M Thornton, MD; L Lanier, MD; C L Sistrom, MD; D Rajderkar, MD; A Mancuso, MD; IM Schmalfuss, MD University of Florida, Gainesville Department of
 L M Thornton, MD; L Lanier, MD; C L Sistrom, MD; D Rajderkar, MD; A Mancuso, MD; IM Schmalfuss, MD University of Florida, Gainesville Department of Radiology RSNA Annual Meeting 2016 Trainee call readiness
L M Thornton, MD; L Lanier, MD; C L Sistrom, MD; D Rajderkar, MD; A Mancuso, MD; IM Schmalfuss, MD University of Florida, Gainesville Department of Radiology RSNA Annual Meeting 2016 Trainee call readiness
brain MRI for neuropsychiatrists: what do you need to know
 brain MRI for neuropsychiatrists: what do you need to know Christoforos Stoupis, MD, PhD Department of Radiology, Spital Maennedorf, Zurich & Inselspital, University of Bern, Switzerland c.stoupis@spitalmaennedorf.ch
brain MRI for neuropsychiatrists: what do you need to know Christoforos Stoupis, MD, PhD Department of Radiology, Spital Maennedorf, Zurich & Inselspital, University of Bern, Switzerland c.stoupis@spitalmaennedorf.ch
Acute Ischemic Stroke Imaging Innovations
 Acute Ischemic Stroke Imaging Innovations Guilherme Dabus, MD, FAHA Director, Fellowship NeuroInterventional Surgery Miami Cardiac & Vascular Institute Baptist Neuroscience Center Baptist Neuroscience
Acute Ischemic Stroke Imaging Innovations Guilherme Dabus, MD, FAHA Director, Fellowship NeuroInterventional Surgery Miami Cardiac & Vascular Institute Baptist Neuroscience Center Baptist Neuroscience
CEREBROVASCULAR DISEASES. By: Shifaa AlQa qa
 CEREBROVASCULAR DISEASES By: Shifaa AlQa qa Cerebrovascular diseases Brain disorders caused by pathologic processes involving blood vessels 3 pathogenic mechanisms (1) thrombotic occlusion, (2) embolic
CEREBROVASCULAR DISEASES By: Shifaa AlQa qa Cerebrovascular diseases Brain disorders caused by pathologic processes involving blood vessels 3 pathogenic mechanisms (1) thrombotic occlusion, (2) embolic
HYPERTENSIVE ENCEPHALOPATHY
 HYPERTENSIVE ENCEPHALOPATHY Reversible posterior leukoencephalopathy syndrome Cause Renal disease Pheochromocytoma Disseminated vasculitis Eclampsia Acute toxemia Medications & illicit drugs (cocaine)
HYPERTENSIVE ENCEPHALOPATHY Reversible posterior leukoencephalopathy syndrome Cause Renal disease Pheochromocytoma Disseminated vasculitis Eclampsia Acute toxemia Medications & illicit drugs (cocaine)
Cerebral Vascular Diseases. Nabila Hamdi MD, PhD
 Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
A New Trend in Vascular Imaging: the Arterial Spin Labeling (ASL) Sequence
 Sequence") A New Trend in Vascular Imaging: the Arterial Spin Labeling (ASL) Sequence Poster No.: C-1347 Congress: ECR 2013 Type: Educational Exhibit Authors: J. Hodel, A. GUILLONNET, M. Rodallec, S. GERBER, R. 1
A New Trend in Vascular Imaging: the Arterial Spin Labeling (ASL) Sequence Poster No.: C-1347 Congress: ECR 2013 Type: Educational Exhibit Authors: J. Hodel, A. GUILLONNET, M. Rodallec, S. GERBER, R. 1
Attenuation value in HU From -500 To HU From -10 To HU From 60 To 90 HU. From 200 HU and above
 Brain Imaging Common CT attenuation values Structure Air Fat Water Brain tissue Recent hematoma Calcifications Bone Brain edema and infarction Normal liver parenchyma Attenuation value in HU From -500
Brain Imaging Common CT attenuation values Structure Air Fat Water Brain tissue Recent hematoma Calcifications Bone Brain edema and infarction Normal liver parenchyma Attenuation value in HU From -500
Vascular Malformations of the Brain: A Review of Imaging Features and Risks
 Vascular Malformations of the Brain: A Review of Imaging Features and Risks Comprehensive Neuroradiology: Best Practices October 27-30, 2016 Sudhakar R. Satti, MD Associate Director Neurointerventional
Vascular Malformations of the Brain: A Review of Imaging Features and Risks Comprehensive Neuroradiology: Best Practices October 27-30, 2016 Sudhakar R. Satti, MD Associate Director Neurointerventional
Review Article Differentiating between Hemorrhagic Infarct and Parenchymal Intracerebral Hemorrhage
 Hindawi Publishing Corporation Radiology Research and Practice Volume 2012, Article ID 475497, 11 pages doi:10.1155/2012/475497 Review Article Differentiating between Hemorrhagic Infarct and Parenchymal
Hindawi Publishing Corporation Radiology Research and Practice Volume 2012, Article ID 475497, 11 pages doi:10.1155/2012/475497 Review Article Differentiating between Hemorrhagic Infarct and Parenchymal
Debbie Summers, MSN, RN, ACNS-BC, CNRN, SCRN. Debbie Summers, MSN, ACNS-BC Nothing
 Debbie Summers, MSN, RN, ACNS-BC, CNRN, SCRN Debbie Summers, MSN, ACNS-BC Nothing Identify anatomical location of stroke on CT, MRI, and perfusion scans and angiography. Relate underlying pathology to
Debbie Summers, MSN, RN, ACNS-BC, CNRN, SCRN Debbie Summers, MSN, ACNS-BC Nothing Identify anatomical location of stroke on CT, MRI, and perfusion scans and angiography. Relate underlying pathology to
Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage
 Cronicon OPEN ACCESS EC PAEDIATRICS Case Report Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage Dimitrios Panagopoulos* Neurosurgical Department, University
Cronicon OPEN ACCESS EC PAEDIATRICS Case Report Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage Dimitrios Panagopoulos* Neurosurgical Department, University
Discovering the hippocampus with cranial-ct.
 Discovering the hippocampus with cranial-ct. Poster No.: C-0378 Congress: ECR 2018 Type: Educational Exhibit Authors: F. Pozo Piñon, A. B. Barba Arce, E. herrera romero, V. 1 2 3 1 3 3 Fernández Lobo,
Discovering the hippocampus with cranial-ct. Poster No.: C-0378 Congress: ECR 2018 Type: Educational Exhibit Authors: F. Pozo Piñon, A. B. Barba Arce, E. herrera romero, V. 1 2 3 1 3 3 Fernández Lobo,
Vascular Malformations
 Vascular Malformations LTC Robert Shih Chief of Neuroradiology Walter Reed Medical Center Special thanks to LTC Alice Smith (retired) Disclosures: None. This presentation reflects the personal views of
Vascular Malformations LTC Robert Shih Chief of Neuroradiology Walter Reed Medical Center Special thanks to LTC Alice Smith (retired) Disclosures: None. This presentation reflects the personal views of
Anoxic brain injury CT and MRI patterns - quick pictoral quide for junior radiologists.
 Anoxic brain injury CT and MRI patterns - quick pictoral quide for junior radiologists. Poster No.: C-1844 Congress: ECR 2017 Type: Educational Exhibit Authors: A. Kecler - Pietrzyk, W. Torreggiani ; Dublin/IE,
Anoxic brain injury CT and MRI patterns - quick pictoral quide for junior radiologists. Poster No.: C-1844 Congress: ECR 2017 Type: Educational Exhibit Authors: A. Kecler - Pietrzyk, W. Torreggiani ; Dublin/IE,
Neuroradiology. of Stroke and Headaches
 Neuroradiology of Stroke and Headaches Learning Objec:ves 1. Iden:fy T1 and T2 sequences 2. Recall the normal anatomy of the intracranial circula:on 3. Apply appropriate CT and MR imaging of the brain
Neuroradiology of Stroke and Headaches Learning Objec:ves 1. Iden:fy T1 and T2 sequences 2. Recall the normal anatomy of the intracranial circula:on 3. Apply appropriate CT and MR imaging of the brain
NEURORADIOLOGY DIL part 4
 NEURORADIOLOGY DIL part 4 Strokes and infarcts K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
NEURORADIOLOGY DIL part 4 Strokes and infarcts K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
Blood Supply. Allen Chung, class of 2013
 Blood Supply Allen Chung, class of 2013 Objectives Understand the importance of the cerebral circulation. Understand stroke and the types of vascular problems that cause it. Understand ischemic penumbra
Blood Supply Allen Chung, class of 2013 Objectives Understand the importance of the cerebral circulation. Understand stroke and the types of vascular problems that cause it. Understand ischemic penumbra
Non-Traumatic Neuro Emergencies
 Department of Radiology University of California San Diego Non-Traumatic Neuro Emergencies John R. Hesselink, M.D. Nontraumatic Neuroemergencies 1. Acute focal neurological deficit 2. Worst headache of
Department of Radiology University of California San Diego Non-Traumatic Neuro Emergencies John R. Hesselink, M.D. Nontraumatic Neuroemergencies 1. Acute focal neurological deficit 2. Worst headache of
What Are We Going to Do? Fourth Year Meds Clinical Neuroanatomy. Hydrocephalus and Effects of Interruption of CSF Flow. Tube Blockage Doctrine
 Fourth Year Meds Clinical Neuroanatomy Ventricles, CSF, Brain Swelling etc. David A. Ramsay, Neuropathologist, LHSC What Are We Going to Do? Hydrocephalus and some effects of the interruption of CSF flow
Fourth Year Meds Clinical Neuroanatomy Ventricles, CSF, Brain Swelling etc. David A. Ramsay, Neuropathologist, LHSC What Are We Going to Do? Hydrocephalus and some effects of the interruption of CSF flow
Index. aneurysm, 92 carotid occlusion, 94 ICA stenosis, 95 intracranial, 92 MCA, 94
 A ADC. See Apparent diffusion coefficient (ADC) Aneurysm cerebral artery aneurysm, 93 CT scan, 93 gadolinium, 93 Angiography, 13 Anoxic brain injury, 25 Apparent diffusion coefficient (ADC), 7 Arachnoid
A ADC. See Apparent diffusion coefficient (ADC) Aneurysm cerebral artery aneurysm, 93 CT scan, 93 gadolinium, 93 Angiography, 13 Anoxic brain injury, 25 Apparent diffusion coefficient (ADC), 7 Arachnoid
Disclosures. CREST Trial: Summary. Lecture Outline 4/16/2015. Cervical Atherosclerotic Disease
 Disclosures Your Patient Has Carotid Bulb Stenosis and a Tandem Intracranial Stenosis: How Do SAMMPRIS and Other Evidence Inform Your Treatment? UCSF Vascular Symposium 2015 Steven W. Hetts, MD Associate
Disclosures Your Patient Has Carotid Bulb Stenosis and a Tandem Intracranial Stenosis: How Do SAMMPRIS and Other Evidence Inform Your Treatment? UCSF Vascular Symposium 2015 Steven W. Hetts, MD Associate
Brain Attack. Strategies in the Management of Acute Ischemic Stroke: Neuroscience Clerkship. Case Medical Center
 Brain Attack Strategies in the Management of Acute Ischemic Stroke: Neuroscience Clerkship Stroke is a common and devastating disorder Third leading antecedent of death in American men, and second among
Brain Attack Strategies in the Management of Acute Ischemic Stroke: Neuroscience Clerkship Stroke is a common and devastating disorder Third leading antecedent of death in American men, and second among
Principles Arteries & Veins of the CNS LO14
 Principles Arteries & Veins of the CNS LO14 14. Identify (on cadaver specimens, models and diagrams) and name the principal arteries and veins of the CNS: Why is it important to understand blood supply
Principles Arteries & Veins of the CNS LO14 14. Identify (on cadaver specimens, models and diagrams) and name the principal arteries and veins of the CNS: Why is it important to understand blood supply
10 May Disclosure. + Outline. Case-based approach to nontraumatic intracranial hemorrhage. Kathleen R. Fink, MD University of Washington
 Kathleen R. Fink, MD University of Washington 5 th Nordic Emergency Radiology Course May 21, 2015 Disclosure My spouse receives research salary support from: Bracco BayerHealthcare Guerbet Outline Case-based
Kathleen R. Fink, MD University of Washington 5 th Nordic Emergency Radiology Course May 21, 2015 Disclosure My spouse receives research salary support from: Bracco BayerHealthcare Guerbet Outline Case-based
Case 9511 Hypertensive microangiopathy
 Case 9511 Hypertensive microangiopathy Schepers S, Barthels C Section: Neuroradiology Published: 2011, Nov. 3 Patient: 67 year(s), male Authors' Institution Department of Radiology, Jessa ziekenhuis campus
Case 9511 Hypertensive microangiopathy Schepers S, Barthels C Section: Neuroradiology Published: 2011, Nov. 3 Patient: 67 year(s), male Authors' Institution Department of Radiology, Jessa ziekenhuis campus
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective
 Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
Imaging Modalities in Acute Stroke: Time is Brain
 April 2001 Imaging Modalities in Acute Stroke: Time is Brain Jeremiah Scharf, Harvard Medical School, MS IV Beth Israel-Deaconess Medical Center Department of Radiology Stroke - Definition and Statistics
April 2001 Imaging Modalities in Acute Stroke: Time is Brain Jeremiah Scharf, Harvard Medical School, MS IV Beth Israel-Deaconess Medical Center Department of Radiology Stroke - Definition and Statistics
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes
 and Non- Aneurysmal Causes") Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
Stroke/TIA. Tom Bedwell
 Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
secondary effects and sequelae of head trauma.
 Neuroimaging of vascular/secondary secondary effects and sequelae of head trauma. Andrès Server Alonso Department of Neuroradiology Division of Radiology Ullevål University Hospital Oslo, Norway. Guidelines
Neuroimaging of vascular/secondary secondary effects and sequelae of head trauma. Andrès Server Alonso Department of Neuroradiology Division of Radiology Ullevål University Hospital Oslo, Norway. Guidelines
Acute Ischaemic Stroke
 Acute Ischaemic Stroke CT or MR SCA READIG FORM SCA ID: DATE OF READIG: SCA QUALIT: Good Moderate Poor Comment: READER ID: TPE OF SCA: CT: Without contrast: With contrast: MR: Diffusion: Perfusion ote
Acute Ischaemic Stroke CT or MR SCA READIG FORM SCA ID: DATE OF READIG: SCA QUALIT: Good Moderate Poor Comment: READER ID: TPE OF SCA: CT: Without contrast: With contrast: MR: Diffusion: Perfusion ote
Update on Emergency Imaging of Acute Ischemic Stroke
 Update on Emergency Imaging of Acute Ischemic Stroke Daniel Kawakyu-O Connor, M.D. Division of Emergency Imaging, University of Rochester Medical Center, Rochester, NY Introduction The term acute stroke
Update on Emergency Imaging of Acute Ischemic Stroke Daniel Kawakyu-O Connor, M.D. Division of Emergency Imaging, University of Rochester Medical Center, Rochester, NY Introduction The term acute stroke
CNS pathology Third year medical students. Dr Heyam Awad 2018 Lecture 7: Non traumatic brain haemorrhage
 CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 7: Non traumatic brain haemorrhage ILOS To list the causes of intracranial haemorrhage. To understand the pathogenesis of each cause.
CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 7: Non traumatic brain haemorrhage ILOS To list the causes of intracranial haemorrhage. To understand the pathogenesis of each cause.
Imaging ischemic strokes: Correlating radiological findings with the pathophysiological evolution of an infarct
 Imaging ischemic strokes: Correlating radiological findings with the pathophysiological evolution of an infarct Jay Chyung,, PhD, HMS III Patient A: history 91 y.o. woman Acute onset R sided weakness and
Imaging ischemic strokes: Correlating radiological findings with the pathophysiological evolution of an infarct Jay Chyung,, PhD, HMS III Patient A: history 91 y.o. woman Acute onset R sided weakness and
Stroke Imaging Basics. Jeremy Hopkin M.D.
 Stroke Imaging Basics Jeremy Hopkin M.D. Goals Introduce the basic physical properties of imaging used in stroke. Understand why each modality is used in the setting of stroke. Understand some strengths
Stroke Imaging Basics Jeremy Hopkin M.D. Goals Introduce the basic physical properties of imaging used in stroke. Understand why each modality is used in the setting of stroke. Understand some strengths
North Oaks Trauma Symposium Friday, November 3, 2017
 Traumatic Intracranial Hemorrhage Aaron C. Sigler, DO, MS Neurosurgery Tulane Neurosciences None Disclosures Overview Anatomy Epidural hematoma Subdural hematoma Cerebral contusions Outline Traumatic ICH
Traumatic Intracranial Hemorrhage Aaron C. Sigler, DO, MS Neurosurgery Tulane Neurosciences None Disclosures Overview Anatomy Epidural hematoma Subdural hematoma Cerebral contusions Outline Traumatic ICH
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
CLEAR III TRIAL : UPDATE ON SURGICAL MATTERS THAT MATTER
 CLEAR III TRIAL : UPDATE ON SURGICAL MATTERS THAT MATTER CLEAR Surgical Center Team July 2011 Trial Enrollment Status Updates Insert latest enrollment update chart from most recent CLEAR newsletter Imaging
CLEAR III TRIAL : UPDATE ON SURGICAL MATTERS THAT MATTER CLEAR Surgical Center Team July 2011 Trial Enrollment Status Updates Insert latest enrollment update chart from most recent CLEAR newsletter Imaging
ACUTE ISCHEMIC STROKE. Current Treatment Approaches for Acute Ischemic Stroke
 ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
The Epidemiology of Stroke and Vascular Risk Factors in Cognitive Aging
 The Epidemiology of Stroke and Vascular Risk Factors in Cognitive Aging REBECCA F. GOTTESMAN, MD PHD ASSOCIATE PROFESSOR OF NEUROLOGY AND EPIDEMIOLOGY JOHNS HOPKINS UNIVERSITY OCTOBER 20, 2014 Outline
The Epidemiology of Stroke and Vascular Risk Factors in Cognitive Aging REBECCA F. GOTTESMAN, MD PHD ASSOCIATE PROFESSOR OF NEUROLOGY AND EPIDEMIOLOGY JOHNS HOPKINS UNIVERSITY OCTOBER 20, 2014 Outline
DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service
 M AY. 6. 2011 10:37 A M F D A - C D R H - O D E - P M O N O. 4147 P. 1 DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Food and Drug Administration 10903 New Hampshire Avenue Document Control
M AY. 6. 2011 10:37 A M F D A - C D R H - O D E - P M O N O. 4147 P. 1 DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Food and Drug Administration 10903 New Hampshire Avenue Document Control
Identifying Cerebrovascular Disorders. Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine
 Identifying Cerebrovascular Disorders Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine Objectives Review different types of cerebrovascular disorders. Briefly discuss etiology,
Identifying Cerebrovascular Disorders Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine Objectives Review different types of cerebrovascular disorders. Briefly discuss etiology,
Management of cervicocephalic arterial dissection. Ciro G. Randazzo, MD, MPH Thomas Jefferson University Hospital, Department of Neurosurgery
 Management of cervicocephalic arterial dissection Ciro G. Randazzo, MD, MPH Thomas Jefferson University Hospital, Department of Neurosurgery Definition Disruption of arterial wall, either at level of intima-media
Management of cervicocephalic arterial dissection Ciro G. Randazzo, MD, MPH Thomas Jefferson University Hospital, Department of Neurosurgery Definition Disruption of arterial wall, either at level of intima-media
Case Report 1. CTA head. (c) Tele3D Advantage, LLC
 Tele3D Advantage, LLC") Case Report 1 CTA head 1 History 82 YEAR OLD woman with signs and symptoms of increased intra cranial pressure in setting of SAH. CT Brain was performed followed by CT Angiography of head. 2 CT brain Extensive
Case Report 1 CTA head 1 History 82 YEAR OLD woman with signs and symptoms of increased intra cranial pressure in setting of SAH. CT Brain was performed followed by CT Angiography of head. 2 CT brain Extensive
UC Irvine Western Journal of Emergency Medicine: Integrating Emergency Care with Population Health
 UC Irvine Western Journal of Emergency Medicine: Integrating Emergency Care with Population Health Title Permalink https://escholarship.org/uc/item/4bb0x2v1 Journal Western Journal of Emergency Medicine:
UC Irvine Western Journal of Emergency Medicine: Integrating Emergency Care with Population Health Title Permalink https://escholarship.org/uc/item/4bb0x2v1 Journal Western Journal of Emergency Medicine:
Imaging of Cerebrovascular Disease
 Imaging of Cerebrovascular Disease A Practical Guide Val M. Runge, MD Editor-in-Chief of Investigative Radiology Institute for Diagnostic, Interventional, and Pediatric Radiology Inselspital, University
Imaging of Cerebrovascular Disease A Practical Guide Val M. Runge, MD Editor-in-Chief of Investigative Radiology Institute for Diagnostic, Interventional, and Pediatric Radiology Inselspital, University
HEAD AND NECK IMAGING. James Chen (MS IV)
") HEAD AND NECK IMAGING James Chen (MS IV) Anatomy Course Johns Hopkins School of Medicine Sept. 27, 2011 OBJECTIVES Introduce cross sectional imaging of head and neck Computed tomography (CT) Review head
HEAD AND NECK IMAGING James Chen (MS IV) Anatomy Course Johns Hopkins School of Medicine Sept. 27, 2011 OBJECTIVES Introduce cross sectional imaging of head and neck Computed tomography (CT) Review head
Hypertensive Haemorrhagic Stroke. Dr Philip Lam Thuon Mine
 Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage. By: Shifaa AlQa qa
 CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage By: Shifaa AlQa qa Subarachnoid Hemorrhage Causes: Rupture of a saccular (berry) aneurysm Vascular malformation Trauma Hematologic disturbances
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage By: Shifaa AlQa qa Subarachnoid Hemorrhage Causes: Rupture of a saccular (berry) aneurysm Vascular malformation Trauma Hematologic disturbances
UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015
 UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015 NEW STUDIES FOR 2015 MR CLEAN ESCAPE EXTEND-IA REVASCAT SWIFT PRIME RECOGNIZED LIMITATIONS IV Alteplase proven benefit
UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015 NEW STUDIES FOR 2015 MR CLEAN ESCAPE EXTEND-IA REVASCAT SWIFT PRIME RECOGNIZED LIMITATIONS IV Alteplase proven benefit
9/18/16. Setting: Community ED, 30k admissions per year Time: Friday night, 11pm. CC: Syncope
 William A. Knight IV MD, FACEP Associate Professor Emergency Medicine & Neurosurgery University of Cincinnati September 21, 2016 (William.knight@uc.edu) ED as the Front Door Spectrum of care with Endovascular
William A. Knight IV MD, FACEP Associate Professor Emergency Medicine & Neurosurgery University of Cincinnati September 21, 2016 (William.knight@uc.edu) ED as the Front Door Spectrum of care with Endovascular
The central nervous system
 Sectc.qxd 29/06/99 09:42 Page 81 Section C The central nervous system CNS haemorrhage Subarachnoid haemorrhage Cerebral infarction Brain atrophy Ring enhancing lesions MRI of the pituitary Multiple sclerosis
Sectc.qxd 29/06/99 09:42 Page 81 Section C The central nervous system CNS haemorrhage Subarachnoid haemorrhage Cerebral infarction Brain atrophy Ring enhancing lesions MRI of the pituitary Multiple sclerosis
MD SUBTYPE ADJUDICATION VARIABLE DEFINITIONS MANUAL The following is a list of variables and how to complete each one:
 MD SUBTYPE ADJUDICATION VARIABLE DEFINITIONS MANUAL 2014-15 The following is a list of variables and how to complete each one: (PHY-1) Case, per physician review: The most important task for the physicians
MD SUBTYPE ADJUDICATION VARIABLE DEFINITIONS MANUAL 2014-15 The following is a list of variables and how to complete each one: (PHY-1) Case, per physician review: The most important task for the physicians
Quality Metrics. Stroke Related Procedure Outcomes
 Quality Metrics Stroke Related Procedure Outcomes Below is a description of some of the stroke-related procedures performed at St. Dominic Hospital in Jackson, with quality information on the complication
Quality Metrics Stroke Related Procedure Outcomes Below is a description of some of the stroke-related procedures performed at St. Dominic Hospital in Jackson, with quality information on the complication