Pearls and Pitfalls in Neuroradiology of Cerebrovascular Disease The Essentials with MR and CT
|
|
|
- Meredith Sabrina French
- 6 years ago
- Views:
Transcription


1 Pearls and Pitfalls in Neuroradiology of Cerebrovascular Disease The Essentials with MR and CT Val M. Runge, MD Wendy R. K. Smoker, MD Anton Valavanis, MD Control # 823
2 Purpose The focus of this educational exhibit, presenting pearls and pitfalls in imaging of the brain, is also in a more broad sense that of clinical Neuroradiology itself. Recognition of characteristic findings on both MR and CT of the disease processes we are likely to encounter in clinical practice is key. The basis for this presentation is clinical case material, specifically excellent images and characteristic findings, demonstrating the points in question, from both modalities.
3 Approach/Methods Of the four major disease categories (neoplastic, vascular, inflammatory, and congenital), vascular disease is the most common. Vascular disease itself is divided into two major subgroups, ischemia and structural vascular anomalies (aneurysms and vascular malformations). Cerebrovascular disease is often accompanied by intracranial hemorrhage, with the imaging appearance of the latter thus also important to understand. This exhibit presents 18 carefully chosen vascular disease imaging 'cases', focusing on less common presentations, the pitfalls in recognition and dating of hemorrhage, and important "Aunt Minnie" findings involving the vessels themselves and lesions therein.
4 Cerebral Ischemia With regard to ischemia, several of the less commonly involved arterial territories are illustrated, specifically including the PCA, ACA, PICA and SCA. The spectrum of lacunar infarcts is then presented, along with the imaging appearance of intraparenchymal hemorrhage (including pitfalls in terms of temporal evolution, on both CT and MR). This section concludes with an illustration of the sometimes confusing appearance of late subacute infarction on MR, together with an illustration of extension of an infarct in the setting of a prior chronic infarct.
, which is supplied by the posterior thalamoperforators.")
5 PCA infarction, early subacute There is both vasogenic edema and cytotoxic edema, as demonstrated by respectively high signal intensity on the T2- and the diffusion-weighted scans, in the entirety of the left PCA distribution. In this instance, infarcts of the same time frame are also seen in the left thalamus (white arrow), which is supplied by the posterior thalamoperforators. There is also hemorrhage (black arrow) within the lesion, seen with low signal intensity due to a T2* effect. Cases courtesy of Neuroradiology: The Essentials with MR and CT (Thieme 2015)
.")
6 ACA infarction, early subacute On FLAIR, there is abnormal high signal intensity in the medial frontal lobe (ACA territory) on the right, involving both gray and white matter, with mild mass effect upon the frontal horn of the lateral ventricle. There is corresponding abnormal hyperintensity on DWI, reflecting cytotoxic edema (confirmed to be restricted diffusion on the ADC map). This anatomic distribution lies within, and forms part of, the ACA territory.

7 Subacute PICA infarct There is abnormal high signal intensity on T2- and diffusion-weighted axial scans in the left PICA territory. The ADC map however does not demonstrate restricted diffusion, thus identifying the findings on DWI to represent T2 shine through. The absence of a true diffusion change dates the infarct to be more than 1 week old, thus late subacute in time frame.
 - consistent with")
8 A portion of the superior cerebellar artery territory is noted to be involved on the left, with abnormal high signal intensity on both T2- and diffusion weighted scans. The high signal intensity on T2- weighted scans denotes vasogenic edema, with the findings on DWI specifically restricted diffusion, confirmed on the ADC map (low signal intensity) - consistent with cytotoxic edema. TOF MRA reveals the left SCA to be small in caliber and truncated. Early subacute SCA infarct
9 In the first patient, on DWI, high signal intensity is seen both in the lentiform nucleus (globus pallidus and putamen) and the caudate head, a common imaging appearance. The caudate head lesion is also shown on FLAIR to be high signal intensity, dating this lesion as acute to subacute in time frame. The caudate infarct, however, cannot be differentiated on the basis of signal intensity on the FLAIR scan from the marked accompanying periventricular white matter gliosis. The anatomic spectrum of lacunar infarction In the second and third patients, respectively, thalamic (white arrow) and pontine lacunar infarcts are seen with high signal intensity on DWI. Note the sharp demarcation, vertically along the median raphe, of the pontine infarct, a common imaging appearance. In the fourth patient, a lateral medullary infarct (white arrow) is seen with hyper- intensity on both DWI and T2-weighted scans.
10 In the first patient, on DWI, high signal intensity is seen both in the lentiform nucleus (globus pallidus and putamen) and the caudate head, a common imaging appearance. The caudate head lesion is also shown on FLAIR to be high signal intensity, dating this lesion as acute to subacute in time frame. The caudate infarct, however, cannot be differentiated on the basis of signal intensity on the FLAIR scan from the marked accompanying periventricular white matter gliosis. In the second and third patients, respectively, thalamic (white arrow) and pontine lacunar infarcts are seen with high signal intensity on DWI. Note the sharp demarcation, vertically along the median raphe, of the pontine infarct, a common imaging appearance. In the fourth patient, a lateral medullary infarct (white arrow) is seen with hyper- intensity on both DWI and T2-weighted scans.

11 Early subacute infarction of the caudate head and lentiform nucleus Both structures are supplied by the lateral lenticulostriate arteries, which originate from the MCA. The caudate nucleus is also supplied by the medial lenticulostriate arteries, which arise from the ACA. The recurrent artery of Heubner, which supplies the anteromedial caudate nucleus and the anteroinferior internal capsule, is the largest of the medial lenticulostriate arteries, and originates near the anterior communicating artery. This early subacute lacunar infarct is better visualized, in terms of the specific region involved, on MR. The infarct manifests both vasogenic and cytotoxic edema.

12 Hypertensive hemorrhage A large acute parenchymal hematoma is seen on the initial CT in this patient (left upper image), with its epicenter in the right putamen. There has also been extravasation of blood into the ventricular system, with hemorrhage seen in the frontal horns, third ventricle, and atria of the lateral ventricles. On the follow-up CT 3 weeks later, the hematoma is smaller and is in transition from hyperdense to isodense to brain. On the MR obtained after an additional 3 weeks, the hematoma is high SI on both T2- and T1-weighted scans (consistent with methemoglobin), with a hemosiderin rim seen on the T2- weighted scan and a thin peripheral rim of enhancement (black arrow) post-contrast. Both are characteristic features on MR in a subacute hematoma, with the enhancement blending into the margin of the high signal intensity hemorrhage.
13 Parenchymal hemorrhage on MR, the spectrum of appearance Initially, but for a very short time, a parenchymal hemorrhage contains oxygenated hemoglobin and is seen as a fluid collection, with slight hyperintensity on a T2-weighted scan. A large, basal ganglia, hyperacute hemorrhage (black asterisk) illustrates this appearance. There is a small amount of associated vasogenic edema and marked mass effect upon the right lateral ventricle. In the next patient, FLAIR scans are shown both on presentation and long term follow-up. This large, acute, left external capsule hematoma evolves from a fluid collection containing deoxyhemoglobin (white asterisk, with low signal intensity on T2-weighted scans), to a hemosiderin lined cleft (also low signal intensity). Note the associated vasogenic edema and mass effect in the acute stage.

14 Parenchymal hemorrhage on MR, the spectrum of appearance The third patient illustrates a subacute, extracellular methemoglobin hematoma, with high signal intensity on both T2- and T1- weighted scans, in the left parietal region. Note the peripheral hemosiderin rim, with low signal intensity, already present on the T2- weighted scan. The fourth patient illustrates on an unenhanced T1- weighted scan a methemoglobin hematoma in the right occipital lobe. This case emphasizes the importance of looking for the cause of a hemorrhage, as the post-contrast scan reveals the associated enhancing metastasis (black arrows).

15 Late subacute, enhancing, PICA infarct There is slight hyperintensity on DWI, which proved to be T2-shine through (not true restricted diffusion) in a portion of the arterial territory of PICA on the right. Hyperintensity is noted on the axial FSE T2-weighted scan in this region, with only subtle increased signal intensity on the coronal FLAIR. On the postcontrast coronal scan there is enhancement of the associated gyri, somewhat wedge shaped in appearance and predominantly involving gray matter.

16 New infarction bordering a chronic infarct The axial FLAIR and FSE T2-weighted scans reveal extensive chronic deep white matter ischemia, together with generalized cortical atrophy and more focal atrophy in the left MCA posterior division, reflecting a prior chronic infarct. There is also abnormal high SI adjacent to the largest area of cystic change, which could simply reflect gliosis due to this old infarct. However, the diffusion-weighted image demonstrates prominent abnormal high SI (confirmed on the ADC map to be restricted diffusion) circumferential and medial to this region, consistent with an early subacute infarct (representing extension of the prior infarct).
17 Aneurysms, Vascular Malformations, and Other Lesions Transitioning to the topic of vessel abnormalities, characteristic imaging findings including pulsation artifacts and flow voids are illustrated, together with partial thrombosis. The exhibit concludes with discussion of several less common entities, all with characteristic and easily recognizable imaging presentations, including specifically myxomatous emboli, carotid cavernous fistula, and venous thrombosis with venous infarction.
, the aneurysm is well depicted, other than partial volume effects (due to the 4 mm slice thickness).")
18 ACA aneurysm Note the prominent pulsation artifact in the first image (a FSE T1-weighted scan at 3 T), seen propagating in the left-right dimension. On the postcontrast image (a short TE GRE scan), the aneurysm is well depicted, other than partial volume effects (due to the 4 mm slice thickness). This 2D scan is relatively immune to pulsation artifacts due to the short TE (2.9 msec in this instance). Thick MIP axial and coronal sections from a 3D TOF exam depict the aneurysm well, with both A2 segments originating from the aneurysm, and absence of the left A1 segment.

19 ACOM aneurysm A flow void is noted in the region of the anterior communicating artery (ACOM) on an axial T2-weighted image, with signal intensity corresponding to arterial flow on an axial source image from a 3D TOF MRA. CE MRA images further confirm the aneurysm, with the right A1 segment of the ACA noted to be very small in diameter. DSA confirms that the aneurysm has a wide neck, an important finding for treatment planning.
.")
20 Superior cerebellar artery aneurysm A predominantly hyperintense lesion is noted on the right, anterior to the pons, causing mild adjacent deformity. Additional scans identify the abnormal high SI to represent methemoglobin in a SCA aneurysm that is predominantly thrombosed and has only a small, residual patent component (medially). The TOF exams, with thick coronal and axial MIPs illustrated, visualize both the methemoglobin (with slight hyperintensity) and the small patent portion of the aneurysm. DSA identifies the patent lumen of the aneurysm, but not the much larger thrombosed component.

21 Multiple cerebral aneurysms Several small lesions with peripheral hemosiderin are noted on the axial T2- weighted scan, one with marked associated vasogenic edema. Comparison of axial source images from a TOF exam, both prior to and with contrast enhancement, reveals a small focus of enhancement within one of the previously noted lesions. A lateral projection from DSA confirms multiple peripheral cerebral aneurysms due to myxomatous emboli, with several visualized in the presented thick section, coronal MIP images from an enhanced TOF MRA.
22 Carotid cavernous fistula, traumatic The images are all from a single patient. In part 1, the axial CT reconstructed with a bone algorithm reveals complete opacification of the sphenoid sinus (by blood in this instance) in this trauma patient, together with a fracture of the wall of the sinus on the left (white arrow). Fractures were also noted of the left occipital bone and petrous apex (not shown). The axial CT and MR through the orbits demonstrate an enlarged superior ophthalmic vein (white asterisk) on the left. This is seen as a flow void (dark) on the MR.
.")

23 Carotid cavernous fistula, traumatic In part 2, prominent flow voids are seen within, together with engorgement of, both cavernous sinuses (white arrows). The frontal DSA projection from a left internal carotid artery injection reveals the shunt into the left cavernous sinus, with filling as well of the contralateral cavernous sinus and retrograde filling of the left superior ophthalmic vein (black arrow). There is prominent filling of the inferior petrosal sinuses bilaterally (black asterisks).

24 Venous thrombosis with venous infarction Vasogenic edema is noted in the right temporal lobe (arrow), but specifically not in an arterial vascular distribution. There is a small parenchymal hemorrhage, with low signal intensity on the T2-weighted scan, seen within the infarct on the axial image. This venous infarct was the result of dural sinus thrombosis, with clot (asterisk) well depicted on multiple images, including specifically within the superior sagittal sinus on coronal images and the right transverse sinus on the axial T1- weighted scan.

25 Quiz case (presentation)
26 Quiz case (additional imaging)
27 Recurrent MCA aneurysm following surgical clipping. On the unenhanced CT, there is a question of a focal abnormal high-density lesion adjacent and just lateral to the surgical clip, placed 13 years earlier for a proximal MCA aneurysm. Post-contrast, a round 16 mm diameter, enhancing lesion is noted, consistent with a recurrent aneurysm. A second aneurysm is identified on DSA, a 4 mm multi-lobulated aneurysm of the left PCOM. The latter is best depicted (arrow) on the volume rendered projection. Both aneurysms were occluded with platinum microcoils, with DSA presented both prior to and following coiling.
28 Some other problems today Time pressures image acquisition scan interpretation Proliferation of imaging techniques Increasing scanner complexity Need for standardization imaging plane acquired scans Decrease in reimbursement


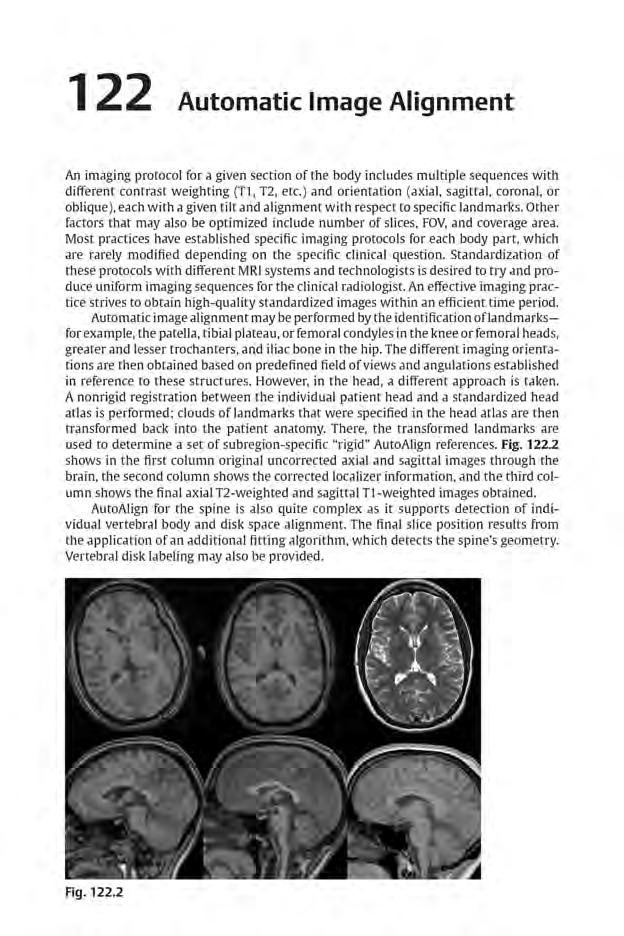
29 Use of automatic image alignment prospectively is strongly recommended Standardization of imaging plane

30 Standardization of the axial imaging plane, enabling improved evaluation of follow-up exams. Watershed infarcts are presented on FLAIR the week following clinical presentation, and at 3 months. The upper row of images are the original axial images, and the lower row reformatted to match imaging plane. By standardization of the displayed imaging plane the larger deep white matter infarct on the right (white arrow) can now be easily identified on the follow-up exam, and its evolution assessed. Comparison of a cortical lesion in the superior parietal gyrus on the left (black arrow), with standardization of the presented plane, reveals extensive resolution of edema with only a pinpoint area of gliosis remaining.

31 Conclusion Pearls and pitfalls regarding the interpretation of MR and CT in patients with cerebrovascular disease are presented, focusing on entities seen in clinical practice, but occurring less frequently and thus often leading to confusion. This selected group of cases covers the less commonly involved arterial territories (for ischemia), the varied appearance of hemorrhage, and key imaging findings in aneurysms and vascular malformations.
Essentials of Clinical MR, 2 nd edition. 14. Ischemia and Infarction II
 14. Ischemia and Infarction II Lacunar infarcts are small deep parenchymal lesions involving the basal ganglia, internal capsule, thalamus, and brainstem. The vascular supply of these areas includes the
14. Ischemia and Infarction II Lacunar infarcts are small deep parenchymal lesions involving the basal ganglia, internal capsule, thalamus, and brainstem. The vascular supply of these areas includes the
Cerebro-vascular stroke
 Cerebro-vascular stroke CT Terminology Hypodense lesion = lesion of lower density than the normal brain tissue Hyperdense lesion = lesion of higher density than normal brain tissue Isodense lesion = lesion
Cerebro-vascular stroke CT Terminology Hypodense lesion = lesion of lower density than the normal brain tissue Hyperdense lesion = lesion of higher density than normal brain tissue Isodense lesion = lesion
NEURO IMAGING 2. Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity
 NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
Blood Supply of the CNS
 Blood Supply of the CNS Lecture Objectives Describe the four arteries supplying the CNS. Follow up each artery to its destination. Describe the circle of Willis and its branches. Discuss the principle
Blood Supply of the CNS Lecture Objectives Describe the four arteries supplying the CNS. Follow up each artery to its destination. Describe the circle of Willis and its branches. Discuss the principle
NEURO IMAGING OF ACUTE STROKE
 1 1 NEURO IMAGING OF ACUTE STROKE ALICIA RICHARDSON, MSN, RN, ACCNS-AG, ANVP-BC WENDY SMITH, MA, RN, MBA, SCRN, FAHA LYNN HUNDLEY, APRN, CNRN, CCNS, ANVP-BC 2 2 1 DISCLOSURES Alicia Richardson: Stryker
1 1 NEURO IMAGING OF ACUTE STROKE ALICIA RICHARDSON, MSN, RN, ACCNS-AG, ANVP-BC WENDY SMITH, MA, RN, MBA, SCRN, FAHA LYNN HUNDLEY, APRN, CNRN, CCNS, ANVP-BC 2 2 1 DISCLOSURES Alicia Richardson: Stryker
OBJECTIVES. At the end of the lecture, students should be able to: List the cerebral arteries.
 DR JAMILA EL MEDANY OBJECTIVES At the end of the lecture, students should be able to: List the cerebral arteries. Describe the cerebral arterial supply regarding the origin, distribution and branches.
DR JAMILA EL MEDANY OBJECTIVES At the end of the lecture, students should be able to: List the cerebral arteries. Describe the cerebral arterial supply regarding the origin, distribution and branches.
Medical Neuroscience Tutorial Notes
 Medical Neuroscience Tutorial Notes Blood Supply to the Brain MAP TO NEUROSCIENCE CORE CONCEPTS 1 NCC1. The brain is the body's most complex organ. LEARNING OBJECTIVES After study of the assigned learning
Medical Neuroscience Tutorial Notes Blood Supply to the Brain MAP TO NEUROSCIENCE CORE CONCEPTS 1 NCC1. The brain is the body's most complex organ. LEARNING OBJECTIVES After study of the assigned learning
Principles Arteries & Veins of the CNS LO14
 Principles Arteries & Veins of the CNS LO14 14. Identify (on cadaver specimens, models and diagrams) and name the principal arteries and veins of the CNS: Why is it important to understand blood supply
Principles Arteries & Veins of the CNS LO14 14. Identify (on cadaver specimens, models and diagrams) and name the principal arteries and veins of the CNS: Why is it important to understand blood supply
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
ISCHEMIC STROKE IMAGING
 ISCHEMIC STROKE IMAGING ผศ.พญ พญ.จ ร ร ตน ธรรมโรจน ภาคว ชาร งส ว ทยา คณะแพทยศาสตร มหาว ทยาล ยขอนแก น A case of acute hemiplegia Which side is the abnormality, right or left? Early Right MCA infarction
ISCHEMIC STROKE IMAGING ผศ.พญ พญ.จ ร ร ตน ธรรมโรจน ภาคว ชาร งส ว ทยา คณะแพทยศาสตร มหาว ทยาล ยขอนแก น A case of acute hemiplegia Which side is the abnormality, right or left? Early Right MCA infarction
Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD
 Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD Five Step Approach 1. Adequate study 2. Bone windows 3. Ventricles 4. Quadrigeminal cistern 5. Parenchyma
Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD Five Step Approach 1. Adequate study 2. Bone windows 3. Ventricles 4. Quadrigeminal cistern 5. Parenchyma
brain MRI for neuropsychiatrists: what do you need to know
 brain MRI for neuropsychiatrists: what do you need to know Christoforos Stoupis, MD, PhD Department of Radiology, Spital Maennedorf, Zurich & Inselspital, University of Bern, Switzerland c.stoupis@spitalmaennedorf.ch
brain MRI for neuropsychiatrists: what do you need to know Christoforos Stoupis, MD, PhD Department of Radiology, Spital Maennedorf, Zurich & Inselspital, University of Bern, Switzerland c.stoupis@spitalmaennedorf.ch
SWI including phase and magnitude images
 On-line Table: MRI imaging recommendation and summary of key features Sequence Pathologies Visible Key Features T1 volumetric high-resolution whole-brain reformatted in axial, coronal, and sagittal planes
On-line Table: MRI imaging recommendation and summary of key features Sequence Pathologies Visible Key Features T1 volumetric high-resolution whole-brain reformatted in axial, coronal, and sagittal planes
Attenuation value in HU From -500 To HU From -10 To HU From 60 To 90 HU. From 200 HU and above
 Brain Imaging Common CT attenuation values Structure Air Fat Water Brain tissue Recent hematoma Calcifications Bone Brain edema and infarction Normal liver parenchyma Attenuation value in HU From -500
Brain Imaging Common CT attenuation values Structure Air Fat Water Brain tissue Recent hematoma Calcifications Bone Brain edema and infarction Normal liver parenchyma Attenuation value in HU From -500
STROKE - IMAGING. Dr RAJASEKHAR REDDY 2nd Yr P.G. RADIODIAGNOSIS KIMS,Narkatpalli.
 STROKE - IMAGING Dr RAJASEKHAR REDDY 2nd Yr P.G. RADIODIAGNOSIS KIMS,Narkatpalli. STROKE Describes a clinical event that consists of sudden onset of neurological symptoms Types Infarction - occlusion of
STROKE - IMAGING Dr RAJASEKHAR REDDY 2nd Yr P.G. RADIODIAGNOSIS KIMS,Narkatpalli. STROKE Describes a clinical event that consists of sudden onset of neurological symptoms Types Infarction - occlusion of
Blood Supply. Allen Chung, class of 2013
 Blood Supply Allen Chung, class of 2013 Objectives Understand the importance of the cerebral circulation. Understand stroke and the types of vascular problems that cause it. Understand ischemic penumbra
Blood Supply Allen Chung, class of 2013 Objectives Understand the importance of the cerebral circulation. Understand stroke and the types of vascular problems that cause it. Understand ischemic penumbra
41 year old female with headache. Elena G. Violari MD and Leo Wolansky MD
 41 year old female with headache Elena G. Violari MD and Leo Wolansky MD ? Dural Venous Sinus Thrombosis with Hemorrhagic Venous Infarct Acute intraparenchymal hematoma measuring ~3 cm in diameter centered
41 year old female with headache Elena G. Violari MD and Leo Wolansky MD ? Dural Venous Sinus Thrombosis with Hemorrhagic Venous Infarct Acute intraparenchymal hematoma measuring ~3 cm in diameter centered
For Emergency Doctors. Dr Suzanne Smallbane November 2011
 For Emergency Doctors Dr Suzanne Smallbane November 2011 A: Orbit B: Sphenoid Sinus C: Temporal Lobe D: EAC E: Mastoid air cells F: Cerebellar hemisphere A: Frontal lobe B: Frontal bone C: Dorsum sellae
For Emergency Doctors Dr Suzanne Smallbane November 2011 A: Orbit B: Sphenoid Sinus C: Temporal Lobe D: EAC E: Mastoid air cells F: Cerebellar hemisphere A: Frontal lobe B: Frontal bone C: Dorsum sellae
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Acute stroke. Ischaemic stroke. Characteristics. Temporal classification. Clinical features. Interpretation of Emergency Head CT
 Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Enhancement of Cranial US: Utility of Supplementary Acoustic Windows and Doppler Harriet J. Paltiel, MD
 Enhancement of Cranial US: Utility of Supplementary Acoustic Windows and Doppler Harriet J. Paltiel, MD Boston Children s Hospital Harvard Medical School None Disclosures Conventional US Anterior fontanelle
Enhancement of Cranial US: Utility of Supplementary Acoustic Windows and Doppler Harriet J. Paltiel, MD Boston Children s Hospital Harvard Medical School None Disclosures Conventional US Anterior fontanelle
Neuroradiology MR Protocols
 Neuroradiology MR Protocols Brain protocols N 1: Brain MRI without contrast N 2: Pre- and post-contrast brain MRI N 3 is deleted N 4: Brain MRI without or pre-/post-contrast (seizure protocol) N 5: Pre-
Neuroradiology MR Protocols Brain protocols N 1: Brain MRI without contrast N 2: Pre- and post-contrast brain MRI N 3 is deleted N 4: Brain MRI without or pre-/post-contrast (seizure protocol) N 5: Pre-
NEURORADIOLOGY Part I
 NEURORADIOLOGY Part I Vörös Erika University of Szeged Department of Radiology SZEGED BRAIN IMAGING METHODS Plain film radiography Ultrasonography (US) Computer tomography (CT) Magnetic resonance imaging
NEURORADIOLOGY Part I Vörös Erika University of Szeged Department of Radiology SZEGED BRAIN IMAGING METHODS Plain film radiography Ultrasonography (US) Computer tomography (CT) Magnetic resonance imaging
Essentials of Clinical MR, 2 nd edition. 99. MRA Principles and Carotid MRA
 99. MRA Principles and Carotid MRA As described in Chapter 12, time of flight (TOF) magnetic resonance angiography (MRA) is commonly utilized in the evaluation of the circle of Willis. TOF MRA allows depiction
99. MRA Principles and Carotid MRA As described in Chapter 12, time of flight (TOF) magnetic resonance angiography (MRA) is commonly utilized in the evaluation of the circle of Willis. TOF MRA allows depiction
Imaging of Cerebrovascular Disease
 Imaging of Cerebrovascular Disease A Practical Guide Val M. Runge, MD Editor-in-Chief of Investigative Radiology Institute for Diagnostic, Interventional, and Pediatric Radiology Inselspital, University
Imaging of Cerebrovascular Disease A Practical Guide Val M. Runge, MD Editor-in-Chief of Investigative Radiology Institute for Diagnostic, Interventional, and Pediatric Radiology Inselspital, University
C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical College NewYork-Presbyterian Hospital
 C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical College NewYork-Presbyterian Hospital I have no financial disclosures Understand range of pathology that may present
C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical College NewYork-Presbyterian Hospital I have no financial disclosures Understand range of pathology that may present
PRESERVE: How intensively should we treat blood pressure in established cerebral small vessel disease? Guide to assessing MRI scans
 PRESERVE: How intensively should we treat blood pressure in established cerebral small vessel disease? Guide to assessing MRI scans Inclusion Criteria Clinical syndrome Patients must have clinical evidence
PRESERVE: How intensively should we treat blood pressure in established cerebral small vessel disease? Guide to assessing MRI scans Inclusion Criteria Clinical syndrome Patients must have clinical evidence
MR Imaging with the CCSVI or Haacke protocol
 MR Imaging with the CCSVI or Haacke protocol Reports from the Haacke protocol are often made available to the patients. The report consists of four major components: 1. anatomical images of major neck
MR Imaging with the CCSVI or Haacke protocol Reports from the Haacke protocol are often made available to the patients. The report consists of four major components: 1. anatomical images of major neck
HEAD AND NECK IMAGING. James Chen (MS IV)
") HEAD AND NECK IMAGING James Chen (MS IV) Anatomy Course Johns Hopkins School of Medicine Sept. 27, 2011 OBJECTIVES Introduce cross sectional imaging of head and neck Computed tomography (CT) Review head
HEAD AND NECK IMAGING James Chen (MS IV) Anatomy Course Johns Hopkins School of Medicine Sept. 27, 2011 OBJECTIVES Introduce cross sectional imaging of head and neck Computed tomography (CT) Review head
How to interpret an unenhanced CT brain scan. Part 2: Clinical cases
 How to interpret an unenhanced CT brain scan. Part 2: Clinical cases Thomas Osborne a, Christine Tang a, Kivraj Sabarwal b and Vineet Prakash c a Radiology Registrar; b Radiology Foundation Year 1 Doctor;
How to interpret an unenhanced CT brain scan. Part 2: Clinical cases Thomas Osborne a, Christine Tang a, Kivraj Sabarwal b and Vineet Prakash c a Radiology Registrar; b Radiology Foundation Year 1 Doctor;
A Case of Carotid-Cavernous Fistula
 A Case of Carotid-Cavernous Fistula By : Mohamed Elkhawaga 2 nd Year Resident of Ophthalmology Alexandria University A 19 year old male patient came to our outpatient clinic, complaining of : -Severe conjunctival
A Case of Carotid-Cavernous Fistula By : Mohamed Elkhawaga 2 nd Year Resident of Ophthalmology Alexandria University A 19 year old male patient came to our outpatient clinic, complaining of : -Severe conjunctival
NEURORADIOLOGY DIL part 4
 NEURORADIOLOGY DIL part 4 Strokes and infarcts K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
NEURORADIOLOGY DIL part 4 Strokes and infarcts K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage
 Cronicon OPEN ACCESS EC PAEDIATRICS Case Report Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage Dimitrios Panagopoulos* Neurosurgical Department, University
Cronicon OPEN ACCESS EC PAEDIATRICS Case Report Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage Dimitrios Panagopoulos* Neurosurgical Department, University
Index. aneurysm, 92 carotid occlusion, 94 ICA stenosis, 95 intracranial, 92 MCA, 94
 A ADC. See Apparent diffusion coefficient (ADC) Aneurysm cerebral artery aneurysm, 93 CT scan, 93 gadolinium, 93 Angiography, 13 Anoxic brain injury, 25 Apparent diffusion coefficient (ADC), 7 Arachnoid
A ADC. See Apparent diffusion coefficient (ADC) Aneurysm cerebral artery aneurysm, 93 CT scan, 93 gadolinium, 93 Angiography, 13 Anoxic brain injury, 25 Apparent diffusion coefficient (ADC), 7 Arachnoid
Applicable Neuroradiology
 For the Clinical Neurology Clerkship LSU Medical School New Orleans Amy W Voigt, MD Clerkship Director Introduction The field of Radiology first developed following the discovery of X-Rays by Wilhelm Roentgen
For the Clinical Neurology Clerkship LSU Medical School New Orleans Amy W Voigt, MD Clerkship Director Introduction The field of Radiology first developed following the discovery of X-Rays by Wilhelm Roentgen
Pediatric MS MRI Study Methodology
 General Pediatric MS MRI Study Methodology SCAN PREPARATION axial T2-weighted scans and/or axial FLAIR scans were obtained for all subjects when available, both T2 and FLAIR scans were scored. In order
General Pediatric MS MRI Study Methodology SCAN PREPARATION axial T2-weighted scans and/or axial FLAIR scans were obtained for all subjects when available, both T2 and FLAIR scans were scored. In order
Vascular Malformations
 Vascular Malformations LTC Robert Shih Chief of Neuroradiology Walter Reed Medical Center Special thanks to LTC Alice Smith (retired) Disclosures: None. This presentation reflects the personal views of
Vascular Malformations LTC Robert Shih Chief of Neuroradiology Walter Reed Medical Center Special thanks to LTC Alice Smith (retired) Disclosures: None. This presentation reflects the personal views of
Benign brain lesions
 Benign brain lesions Diagnostic and Interventional Radiology Hung-Wen Kao Department of Radiology, Tri-Service General Hospital, National Defense Medical Center Computed tomography Hounsfield unit (HU)
Benign brain lesions Diagnostic and Interventional Radiology Hung-Wen Kao Department of Radiology, Tri-Service General Hospital, National Defense Medical Center Computed tomography Hounsfield unit (HU)
Acute stroke imaging
 Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Department of Radiology University of California San Diego. MR Angiography. Techniques & Applications. John R. Hesselink, M.D.
 Department of Radiology University of California San Diego MR Angiography Techniques & Applications John R. Hesselink, M.D. Vascular Imaging Arterial flow void Flow enhancement Gadolinium enhancement Vascular
Department of Radiology University of California San Diego MR Angiography Techniques & Applications John R. Hesselink, M.D. Vascular Imaging Arterial flow void Flow enhancement Gadolinium enhancement Vascular
Case Report 1. CTA head. (c) Tele3D Advantage, LLC
 Tele3D Advantage, LLC") Case Report 1 CTA head 1 History 82 YEAR OLD woman with signs and symptoms of increased intra cranial pressure in setting of SAH. CT Brain was performed followed by CT Angiography of head. 2 CT brain Extensive
Case Report 1 CTA head 1 History 82 YEAR OLD woman with signs and symptoms of increased intra cranial pressure in setting of SAH. CT Brain was performed followed by CT Angiography of head. 2 CT brain Extensive
Cerebrovascular diseases-2
 Cerebrovascular diseases-2 Primary angiitis of CNS - Other causes of infarction i. Hypercoagulable states ii. Drug-abuse such as amphetamine, heroin and cocain Note - The venous side of the circulation
Cerebrovascular diseases-2 Primary angiitis of CNS - Other causes of infarction i. Hypercoagulable states ii. Drug-abuse such as amphetamine, heroin and cocain Note - The venous side of the circulation
An Introduction to Imaging the Brain. Dr Amy Davis
 An Introduction to Imaging the Brain Dr Amy Davis Common reasons for imaging: Clinical scenarios: - Trauma (NICE guidelines) - Stroke - Tumours - Seizure - Neurological degeneration memory, motor dysfunction,
An Introduction to Imaging the Brain Dr Amy Davis Common reasons for imaging: Clinical scenarios: - Trauma (NICE guidelines) - Stroke - Tumours - Seizure - Neurological degeneration memory, motor dysfunction,
Neuroradiology. of Stroke and Headaches
 Neuroradiology of Stroke and Headaches Learning Objec:ves 1. Iden:fy T1 and T2 sequences 2. Recall the normal anatomy of the intracranial circula:on 3. Apply appropriate CT and MR imaging of the brain
Neuroradiology of Stroke and Headaches Learning Objec:ves 1. Iden:fy T1 and T2 sequences 2. Recall the normal anatomy of the intracranial circula:on 3. Apply appropriate CT and MR imaging of the brain
CNS Imaging. Dr Amir Monir, MD. Lecturer of radiodiagnosis.
 CNS Imaging Dr Amir Monir, MD Lecturer of radiodiagnosis www.dramir.net Types of radiological examinations you know Plain X ray X ray with contrast GIT : barium (swallow, meal, follow through, enema) ERCP
CNS Imaging Dr Amir Monir, MD Lecturer of radiodiagnosis www.dramir.net Types of radiological examinations you know Plain X ray X ray with contrast GIT : barium (swallow, meal, follow through, enema) ERCP
Intracranial spontaneous hemorrhage mechanisms, imaging and management
 Intracranial spontaneous hemorrhage mechanisms, imaging and management Dora Zlatareva Department of Diagnostic Imaging Medical University, Sofia, Bulgaria Intracranial hemorrhage (ICH) ICH 15% of strokes
Intracranial spontaneous hemorrhage mechanisms, imaging and management Dora Zlatareva Department of Diagnostic Imaging Medical University, Sofia, Bulgaria Intracranial hemorrhage (ICH) ICH 15% of strokes
Magnetic Resonance Imaging. Basics of MRI in practice. Generation of MR signal. Generation of MR signal. Spin echo imaging. Generation of MR signal
 Magnetic Resonance Imaging Protons aligned with B0 magnetic filed Longitudinal magnetization - T1 relaxation Transverse magnetization - T2 relaxation Signal measured in the transverse plane Basics of MRI
Magnetic Resonance Imaging Protons aligned with B0 magnetic filed Longitudinal magnetization - T1 relaxation Transverse magnetization - T2 relaxation Signal measured in the transverse plane Basics of MRI
CT and MR findings of systemic lupus erythematosus involving the brain: Differential diagnosis based on lesion distribution
 CT and MR findings of systemic lupus erythematosus involving the brain: Differential diagnosis based on lesion distribution Poster No.: C-2723 Congress: ECR 2010 Type: Educational Exhibit Topic: Neuro
CT and MR findings of systemic lupus erythematosus involving the brain: Differential diagnosis based on lesion distribution Poster No.: C-2723 Congress: ECR 2010 Type: Educational Exhibit Topic: Neuro
TRANSVERSE SECTION PLANE Scalp 2. Cranium. 13. Superior sagittal sinus
 TRANSVERSE SECTION PLANE 1 1. Scalp 2. Cranium 3. Superior sagittal sinus 4. Dura mater 5. Falx cerebri 6. Frontal lobes of the cerebrum 7. Middle meningeal artery 8. Cortex, grey matter 9. Cerebral vessels
TRANSVERSE SECTION PLANE 1 1. Scalp 2. Cranium 3. Superior sagittal sinus 4. Dura mater 5. Falx cerebri 6. Frontal lobes of the cerebrum 7. Middle meningeal artery 8. Cortex, grey matter 9. Cerebral vessels
A New Trend in Vascular Imaging: the Arterial Spin Labeling (ASL) Sequence
 Sequence") A New Trend in Vascular Imaging: the Arterial Spin Labeling (ASL) Sequence Poster No.: C-1347 Congress: ECR 2013 Type: Educational Exhibit Authors: J. Hodel, A. GUILLONNET, M. Rodallec, S. GERBER, R. 1
A New Trend in Vascular Imaging: the Arterial Spin Labeling (ASL) Sequence Poster No.: C-1347 Congress: ECR 2013 Type: Educational Exhibit Authors: J. Hodel, A. GUILLONNET, M. Rodallec, S. GERBER, R. 1
Stroke imaging. Why image stroke patients? Stroke. Treatment of infarct. Methods for infarct diagnosis. Treatment of infarct.
 Stroke imaging Stroke Infarct: -Arterial thrombosis/embolus -Hypoxic/ischemic -Venous thrombosis Non-traumatic hemorrhage: -Intracerebral -Subarachnoid Johan Wikström MD PhD Associate Professor of Radiology
Stroke imaging Stroke Infarct: -Arterial thrombosis/embolus -Hypoxic/ischemic -Venous thrombosis Non-traumatic hemorrhage: -Intracerebral -Subarachnoid Johan Wikström MD PhD Associate Professor of Radiology
Announcement. Danny to schedule a time if you are interested.
 Announcement If you need more experiments to participate in, contact Danny Sanchez (dsanchez@ucsd.edu) make sure to tell him that you are from LIGN171, so he will let me know about your credit (1 point).
Announcement If you need more experiments to participate in, contact Danny Sanchez (dsanchez@ucsd.edu) make sure to tell him that you are from LIGN171, so he will let me know about your credit (1 point).
CT - Brain Examination
 CT - Brain Examination Submitted by: Felemban 1 CT - Brain Examination The clinical indication of CT brain are: a) Chronic cases (e.g. headache - tumor - abscess) b) ER cases (e.g. trauma - RTA - child
CT - Brain Examination Submitted by: Felemban 1 CT - Brain Examination The clinical indication of CT brain are: a) Chronic cases (e.g. headache - tumor - abscess) b) ER cases (e.g. trauma - RTA - child
Vascular Malformations of the Brain: A Review of Imaging Features and Risks
 Vascular Malformations of the Brain: A Review of Imaging Features and Risks Comprehensive Neuroradiology: Best Practices October 27-30, 2016 Sudhakar R. Satti, MD Associate Director Neurointerventional
Vascular Malformations of the Brain: A Review of Imaging Features and Risks Comprehensive Neuroradiology: Best Practices October 27-30, 2016 Sudhakar R. Satti, MD Associate Director Neurointerventional
Marc Norman, Ph.D. - Do Not Use without Permission 1. Cerebrovascular Accidents. Marc Norman, Ph.D. Department of Psychiatry
 Cerebrovascular Accidents Marc Norman, Ph.D. Department of Psychiatry Neuropsychiatry and Behavioral Medicine Neuropsychology Clinical Training Seminar 1 5 http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/18009.jpg
Cerebrovascular Accidents Marc Norman, Ph.D. Department of Psychiatry Neuropsychiatry and Behavioral Medicine Neuropsychology Clinical Training Seminar 1 5 http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/18009.jpg
The central nervous system
 Sectc.qxd 29/06/99 09:42 Page 81 Section C The central nervous system CNS haemorrhage Subarachnoid haemorrhage Cerebral infarction Brain atrophy Ring enhancing lesions MRI of the pituitary Multiple sclerosis
Sectc.qxd 29/06/99 09:42 Page 81 Section C The central nervous system CNS haemorrhage Subarachnoid haemorrhage Cerebral infarction Brain atrophy Ring enhancing lesions MRI of the pituitary Multiple sclerosis
Methods. Yahya Paksoy, Bülent Oğuz Genç, and Emine Genç. AJNR Am J Neuroradiol 24: , August 2003
 AJNR Am J Neuroradiol 24:1364 1368, August 2003 Retrograde Flow in the Left Inferior Petrosal Sinus and Blood Steal of the Cavernous Sinus Associated with Central Vein Stenosis: MR Angiographic Findings
AJNR Am J Neuroradiol 24:1364 1368, August 2003 Retrograde Flow in the Left Inferior Petrosal Sinus and Blood Steal of the Cavernous Sinus Associated with Central Vein Stenosis: MR Angiographic Findings
Neuroanatomy Dr. Maha ELBeltagy Assistant Professor of Anatomy Faculty of Medicine The University of Jordan 2018
 Neuroanatomy Dr. Maha ELBeltagy Assistant Professor of Anatomy Faculty of Medicine The University of Jordan 2018 Blood Supply of Brain and Spinal Cord Arterial Supply of Brain The brain receives blood
Neuroanatomy Dr. Maha ELBeltagy Assistant Professor of Anatomy Faculty of Medicine The University of Jordan 2018 Blood Supply of Brain and Spinal Cord Arterial Supply of Brain The brain receives blood
Review Article Differentiating between Hemorrhagic Infarct and Parenchymal Intracerebral Hemorrhage
 Hindawi Publishing Corporation Radiology Research and Practice Volume 2012, Article ID 475497, 11 pages doi:10.1155/2012/475497 Review Article Differentiating between Hemorrhagic Infarct and Parenchymal
Hindawi Publishing Corporation Radiology Research and Practice Volume 2012, Article ID 475497, 11 pages doi:10.1155/2012/475497 Review Article Differentiating between Hemorrhagic Infarct and Parenchymal
Slide 1. Slide 2. Slide 3. Tomography vs Topography. Computed Tomography (CT): A simplified Topographical review of the Brain. Learning Objective
: A simplified Topographical review of the Brain. Learning Objective") Slide 1 Computed Tomography (CT): A simplified Topographical review of the Brain Jon Wheiler, ACNP-BC Slide 2 Tomography vs Topography Tomography: A technique for displaying a representation of a cross
Slide 1 Computed Tomography (CT): A simplified Topographical review of the Brain Jon Wheiler, ACNP-BC Slide 2 Tomography vs Topography Tomography: A technique for displaying a representation of a cross
Neuroradiology: Imaging and Stroke
 Neuroradiology: Imaging and Stroke Stroke 2017 William Gallmann January 28, 2017 Stroke Arterial ischemia/infarct accounts for ~85% Cerebral venous occlusions - 0.5-1% Spontaneous intracranial hemorrhage
Neuroradiology: Imaging and Stroke Stroke 2017 William Gallmann January 28, 2017 Stroke Arterial ischemia/infarct accounts for ~85% Cerebral venous occlusions - 0.5-1% Spontaneous intracranial hemorrhage
Keep Imaging Simple: An Introduction To Neuroimaging
 Keep Imaging Simple: An Introduction To Neuroimaging Meghan Elkins, OD, FAAO Please silence all mobile devices and remove items from chairs so others can sit. Unauthorized recording of this session is
Keep Imaging Simple: An Introduction To Neuroimaging Meghan Elkins, OD, FAAO Please silence all mobile devices and remove items from chairs so others can sit. Unauthorized recording of this session is
Classical CNS Disease Patterns
 Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
Module 3. The Blood Supply of the Brain
 Module 3. The Blood Supply of the Brain Relating Vascular and Functional Anatomy Objectives for Module 3 Knowledge! Describe or sketch the course of the major arteries and their branches that comprise
Module 3. The Blood Supply of the Brain Relating Vascular and Functional Anatomy Objectives for Module 3 Knowledge! Describe or sketch the course of the major arteries and their branches that comprise
MRI OF THE THALAMUS. Mohammed J. Zafar, MD, FAAN Kalamazoo, MI
 1 MRI OF THE THALAMUS Mohammed J. Zafar, MD, FAAN Kalamazoo, MI Objectives: The thalamic nuclei can be involved in a wide variety of conditions. A systematic imaging approach would be useful for narrowing
1 MRI OF THE THALAMUS Mohammed J. Zafar, MD, FAAN Kalamazoo, MI Objectives: The thalamic nuclei can be involved in a wide variety of conditions. A systematic imaging approach would be useful for narrowing
RADIOLOGY TEACHING CONFERENCE
 RADIOLOGY TEACHING CONFERENCE John Athas, MD Monica Tadros, MD Columbia University, College of Physicians & Surgeons Department of Otolaryngology- Head & Neck Surgery September 27, 2007 CT SCAN IMAGING
RADIOLOGY TEACHING CONFERENCE John Athas, MD Monica Tadros, MD Columbia University, College of Physicians & Surgeons Department of Otolaryngology- Head & Neck Surgery September 27, 2007 CT SCAN IMAGING
L M Thornton, MD; L Lanier, MD; C L Sistrom, MD; D Rajderkar, MD; A Mancuso, MD; IM Schmalfuss, MD University of Florida, Gainesville Department of
 L M Thornton, MD; L Lanier, MD; C L Sistrom, MD; D Rajderkar, MD; A Mancuso, MD; IM Schmalfuss, MD University of Florida, Gainesville Department of Radiology RSNA Annual Meeting 2016 Trainee call readiness
L M Thornton, MD; L Lanier, MD; C L Sistrom, MD; D Rajderkar, MD; A Mancuso, MD; IM Schmalfuss, MD University of Florida, Gainesville Department of Radiology RSNA Annual Meeting 2016 Trainee call readiness
Journal of Radiology Case Reports
 Pediatric Holohemispheric Developmental Venous Anomaly: Definitive characterization by 3D Susceptibility Weighted Magnetic Resonance Angiography Michael A. Casey 1, Sourabh Lahoti 2, Ajeet Gordhan 2* 1.
Pediatric Holohemispheric Developmental Venous Anomaly: Definitive characterization by 3D Susceptibility Weighted Magnetic Resonance Angiography Michael A. Casey 1, Sourabh Lahoti 2, Ajeet Gordhan 2* 1.
Radiologic diagnosis of cerebral venous thrombosis and its differential diagnosis
 Radiologic diagnosis of cerebral venous thrombosis and its differential diagnosis Poster No.: C-0628 Congress: ECR 2014 Type: Educational Exhibit Authors: A. M. Vargas Díaz, C. Fernández Rey, D. Garcia
Radiologic diagnosis of cerebral venous thrombosis and its differential diagnosis Poster No.: C-0628 Congress: ECR 2014 Type: Educational Exhibit Authors: A. M. Vargas Díaz, C. Fernández Rey, D. Garcia
What Is an Arteriovenous malformation (AVM)?
?") American Society of Neuroradiology What Is an Arteriovenous malformation (AVM)? From the Cerebrovascular Imaging and Intervention Committee of the American Heart Association Cardiovascular Council Randall
American Society of Neuroradiology What Is an Arteriovenous malformation (AVM)? From the Cerebrovascular Imaging and Intervention Committee of the American Heart Association Cardiovascular Council Randall
Magnetic Resonance Imaging for Neurological Conditions. Lawrance Yip Department of Radiology Queen Mary Hospital
 Magnetic Resonance Imaging for Neurological Conditions Lawrance Yip Department of Radiology Queen Mary Hospital Outline Strength and limitations of MRI for neurological conditions MR Imaging techniques
Magnetic Resonance Imaging for Neurological Conditions Lawrance Yip Department of Radiology Queen Mary Hospital Outline Strength and limitations of MRI for neurological conditions MR Imaging techniques
Multidetector computed tomographic (CT) angiography : FREQUENTLY ANATOMICAL VARIATIONS OF THE CIRCLE WILLIS ICONOGRAPHIC REVIEW
 angiography : FREQUENTLY ANATOMICAL VARIATIONS OF THE CIRCLE WILLIS ICONOGRAPHIC REVIEW") Multidetector computed tomographic (CT) angiography : FREQUENTLY ANATOMICAL VARIATIONS OF THE CIRCLE WILLIS ICONOGRAPHIC REVIEW Dra. Ximena González Larramendi Dr. Fernando Landó Baison ABSTRACT: Objetives:
Multidetector computed tomographic (CT) angiography : FREQUENTLY ANATOMICAL VARIATIONS OF THE CIRCLE WILLIS ICONOGRAPHIC REVIEW Dra. Ximena González Larramendi Dr. Fernando Landó Baison ABSTRACT: Objetives:
HEAD/NECK VESSELS. Objectives
 Objectives Arterial Supply to Head and Neck Arteries to Head Surrounding Brain Common carotid arteries Arteries to Head Surrounding Brain External carotid arteries Arteries to Head Surrounding Brain External
Objectives Arterial Supply to Head and Neck Arteries to Head Surrounding Brain Common carotid arteries Arteries to Head Surrounding Brain External carotid arteries Arteries to Head Surrounding Brain External
Non-Traumatic Neuro Emergencies
 Department of Radiology University of California San Diego Non-Traumatic Neuro Emergencies John R. Hesselink, M.D. Nontraumatic Neuroemergencies 1. Acute focal neurological deficit 2. Worst headache of
Department of Radiology University of California San Diego Non-Traumatic Neuro Emergencies John R. Hesselink, M.D. Nontraumatic Neuroemergencies 1. Acute focal neurological deficit 2. Worst headache of
V. CENTRAL NERVOUS SYSTEM TRAUMA
 V. CENTRAL NERVOUS SYSTEM TRAUMA I. Concussion - Is a clinical syndrome of altered consiousness secondary to head injury - Brought by a change in the momentum of the head when a moving head suddenly arrested
V. CENTRAL NERVOUS SYSTEM TRAUMA I. Concussion - Is a clinical syndrome of altered consiousness secondary to head injury - Brought by a change in the momentum of the head when a moving head suddenly arrested
Cerebral malaria: MR imaging spectrum
 Cerebral malaria: MR imaging spectrum Poster No.: C-2705 Congress: ECR 2010 Type: Educational Exhibit Topic: Neuro Authors: P. S. Naphade, M. D. Agrawal, S. S. Sankhe, K. M. Siva, B. K. Jain; Mumbai/IN
Cerebral malaria: MR imaging spectrum Poster No.: C-2705 Congress: ECR 2010 Type: Educational Exhibit Topic: Neuro Authors: P. S. Naphade, M. D. Agrawal, S. S. Sankhe, K. M. Siva, B. K. Jain; Mumbai/IN
CEREBROVASCULAR DISEASES. By: Shifaa AlQa qa
 CEREBROVASCULAR DISEASES By: Shifaa AlQa qa Cerebrovascular diseases Brain disorders caused by pathologic processes involving blood vessels 3 pathogenic mechanisms (1) thrombotic occlusion, (2) embolic
CEREBROVASCULAR DISEASES By: Shifaa AlQa qa Cerebrovascular diseases Brain disorders caused by pathologic processes involving blood vessels 3 pathogenic mechanisms (1) thrombotic occlusion, (2) embolic
CT of the Head, Spine, and Cerebral Vessels
 CT of the Head, Spine, and Cerebral Vessels Objectives Determine specific imaging plane used to acquire or reformat CT scan, i.e. sagittal, coronal, transverse, and offaxis or oblique. Assess and evaluate
CT of the Head, Spine, and Cerebral Vessels Objectives Determine specific imaging plane used to acquire or reformat CT scan, i.e. sagittal, coronal, transverse, and offaxis or oblique. Assess and evaluate
Magnetic Resonance Angiography
 Magnetic Resonance Angiography 1 Magnetic Resonance Angiography exploits flow enhancement of GR sequences saturation of venous flow allows arterial visualization saturation of arterial flow allows venous
Magnetic Resonance Angiography 1 Magnetic Resonance Angiography exploits flow enhancement of GR sequences saturation of venous flow allows arterial visualization saturation of arterial flow allows venous
IMAGING IN ACUTE ISCHEMIC STROKE
 IMAGING IN ACUTE ISCHEMIC STROKE Timo Krings MD, PhD, FRCP (C) Professor of Radiology & Surgery Braley Chair of Neuroradiology, Chief and Program Director of Diagnostic and Interventional Neuroradiology;
IMAGING IN ACUTE ISCHEMIC STROKE Timo Krings MD, PhD, FRCP (C) Professor of Radiology & Surgery Braley Chair of Neuroradiology, Chief and Program Director of Diagnostic and Interventional Neuroradiology;
TABLES. Table 1 Terminal vessel aneurysms. Table. Aneurysm location. Bypass flow** Symptoms Strategy Bypass recipient. Age/ Sex.
 Table TABLES Table 1 Terminal vessel aneurysms Age/ Sex Aneurysm location Symptoms Strategy Bypass recipient Recipient territory Recipient territory flow* Cut flow Bypass flow** Graft Patent postop F/U
Table TABLES Table 1 Terminal vessel aneurysms Age/ Sex Aneurysm location Symptoms Strategy Bypass recipient Recipient territory Recipient territory flow* Cut flow Bypass flow** Graft Patent postop F/U
North Oaks Trauma Symposium Friday, November 3, 2017
 Traumatic Intracranial Hemorrhage Aaron C. Sigler, DO, MS Neurosurgery Tulane Neurosciences None Disclosures Overview Anatomy Epidural hematoma Subdural hematoma Cerebral contusions Outline Traumatic ICH
Traumatic Intracranial Hemorrhage Aaron C. Sigler, DO, MS Neurosurgery Tulane Neurosciences None Disclosures Overview Anatomy Epidural hematoma Subdural hematoma Cerebral contusions Outline Traumatic ICH
Sectional Anatomy Head Practice Problems
 1. Which of the following is illustrated by #3? (Fig. 5-42) A) maxillary sinus B) vomer C) septal cartilage D) perpendicular plate of ethmoid bone 2. What number illustrates the cornea? (Fig. 5-42) A)
1. Which of the following is illustrated by #3? (Fig. 5-42) A) maxillary sinus B) vomer C) septal cartilage D) perpendicular plate of ethmoid bone 2. What number illustrates the cornea? (Fig. 5-42) A)
Acute Ischaemic Stroke
 Acute Ischaemic Stroke CT or MR SCA READIG FORM SCA ID: DATE OF READIG: SCA QUALIT: Good Moderate Poor Comment: READER ID: TPE OF SCA: CT: Without contrast: With contrast: MR: Diffusion: Perfusion ote
Acute Ischaemic Stroke CT or MR SCA READIG FORM SCA ID: DATE OF READIG: SCA QUALIT: Good Moderate Poor Comment: READER ID: TPE OF SCA: CT: Without contrast: With contrast: MR: Diffusion: Perfusion ote
Cryptogenic Enlargement Of Bilateral Superior Ophthalmic Veins
 ISPUB.COM The Internet Journal of Radiology Volume 18 Number 1 Cryptogenic Enlargement Of Bilateral Superior Ophthalmic Veins K Kragha Citation K Kragha. Cryptogenic Enlargement Of Bilateral Superior Ophthalmic
ISPUB.COM The Internet Journal of Radiology Volume 18 Number 1 Cryptogenic Enlargement Of Bilateral Superior Ophthalmic Veins K Kragha Citation K Kragha. Cryptogenic Enlargement Of Bilateral Superior Ophthalmic
NACC Vascular Consortium. NACC Vascular Consortium. NACC Vascular Consortium
 NACC Vascular Consortium NACC Vascular Consortium Participating centers: Oregon Health and Science University ADC Rush University ADC Mount Sinai School of Medicine ADC Boston University ADC In consultation
NACC Vascular Consortium NACC Vascular Consortium Participating centers: Oregon Health and Science University ADC Rush University ADC Mount Sinai School of Medicine ADC Boston University ADC In consultation
Essentials of Clinical MR, 2 nd edition. 73. Urinary Bladder and Male Pelvis
 73. Urinary Bladder and Male Pelvis Urinary bladder carcinoma is best locally staged with MRI. It is important however to note that a thickened wall (> 5 mm) is a non-specific finding seen in an underfilled
73. Urinary Bladder and Male Pelvis Urinary bladder carcinoma is best locally staged with MRI. It is important however to note that a thickened wall (> 5 mm) is a non-specific finding seen in an underfilled
IV. Cerebrovascular diseases
 IV. Cerebrovascular diseases - Cerebrovascular disease denotes brain disorders caused by pathologic processes involving the blood vessels. - The three main pathogenic mechanisms are: 1. Thrombotic occlusion
IV. Cerebrovascular diseases - Cerebrovascular disease denotes brain disorders caused by pathologic processes involving the blood vessels. - The three main pathogenic mechanisms are: 1. Thrombotic occlusion
Regional and Lobe Parcellation Rhesus Monkey Brain Atlas. Manual Tracing for Parcellation Template
 Regional and Lobe Parcellation Rhesus Monkey Brain Atlas Manual Tracing for Parcellation Template Overview of Tracing Guidelines A) Traces are performed in a systematic order they, allowing the more easily
Regional and Lobe Parcellation Rhesus Monkey Brain Atlas Manual Tracing for Parcellation Template Overview of Tracing Guidelines A) Traces are performed in a systematic order they, allowing the more easily
On Call Guide to CT Perfusion. Updated: March 2011
 On Call Guide to CT Perfusion Updated: March 2011 CT Stroke Protocol 1. Non contrast CT brain 2. CT perfusion: contrast 40cc bolus dynamic imaging at 8 slice levels ~ 60 sec creates perfusion color maps
On Call Guide to CT Perfusion Updated: March 2011 CT Stroke Protocol 1. Non contrast CT brain 2. CT perfusion: contrast 40cc bolus dynamic imaging at 8 slice levels ~ 60 sec creates perfusion color maps
General Imaging. Imaging modalities. Incremental CT. Multislice CT Multislice CT [ MDCT ]
![General Imaging. Imaging modalities. Incremental CT. Multislice CT Multislice CT [ MDCT ]](/thumbs/76/74079340.jpg "General Imaging. Imaging modalities. Incremental CT. Multislice CT Multislice CT [ MDCT ]") General Imaging Imaging modalities Conventional X-rays Ultrasonography [ US ] Computed tomography [ CT ] Radionuclide imaging Magnetic resonance imaging [ MRI ] Angiography conventional, CT,MRI Interventional
General Imaging Imaging modalities Conventional X-rays Ultrasonography [ US ] Computed tomography [ CT ] Radionuclide imaging Magnetic resonance imaging [ MRI ] Angiography conventional, CT,MRI Interventional
Clinical Applications
 C H A P T E R 16 Clinical Applications In selecting pulse sequences and measurement parameters for a specific application, MRI allows the user tremendous flexibility to produce variations in contrast between
C H A P T E R 16 Clinical Applications In selecting pulse sequences and measurement parameters for a specific application, MRI allows the user tremendous flexibility to produce variations in contrast between
Anoxic brain injury CT and MRI patterns - quick pictoral quide for junior radiologists.
 Anoxic brain injury CT and MRI patterns - quick pictoral quide for junior radiologists. Poster No.: C-1844 Congress: ECR 2017 Type: Educational Exhibit Authors: A. Kecler - Pietrzyk, W. Torreggiani ; Dublin/IE,
Anoxic brain injury CT and MRI patterns - quick pictoral quide for junior radiologists. Poster No.: C-1844 Congress: ECR 2017 Type: Educational Exhibit Authors: A. Kecler - Pietrzyk, W. Torreggiani ; Dublin/IE,
BRAIN STEM AND CEREBELLUM..
 Lecture Title: BRAIN STEM AND CEREBELLUM.. (CNS Block, Radiology) Dr. Hamdy Hassan Ass.Prof. Consultant Radiology Department KKHU King Saud University Lecture Objectives.. Students at the end of the lecture
Lecture Title: BRAIN STEM AND CEREBELLUM.. (CNS Block, Radiology) Dr. Hamdy Hassan Ass.Prof. Consultant Radiology Department KKHU King Saud University Lecture Objectives.. Students at the end of the lecture
Professor Dr.Muhammad Ajmal Dr.Tehmina Nazir. HOLY FAMILY HOSPITAL Rawalpindi
 Professor Dr.Muhammad Ajmal Dr.Tehmina Nazir HOLY FAMILY HOSPITAL Rawalpindi SCHEME OF PRESENTATION PLAIN X-RAYS CT SCAN MRI CONCLUSION IMAGING MODALITIES PLAIN X-RAYS CT SCAN MRI OCCIPITOMENTAL/WATER
Professor Dr.Muhammad Ajmal Dr.Tehmina Nazir HOLY FAMILY HOSPITAL Rawalpindi SCHEME OF PRESENTATION PLAIN X-RAYS CT SCAN MRI CONCLUSION IMAGING MODALITIES PLAIN X-RAYS CT SCAN MRI OCCIPITOMENTAL/WATER
NEURORADIOLOGY DIL part 3
 NEURORADIOLOGY DIL part 3 Bleeds and hemorrhages K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
NEURORADIOLOGY DIL part 3 Bleeds and hemorrhages K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
Imaging of Hearing Loss
 Contemporary Imaging of Sensorineural Hearing Loss Imaging of Hearing Loss Discussion Outline (SNHL) Imaging Approaches Anatomic Relationships Lesions: SNHL KL Salzman, MD University of Utah School of
Contemporary Imaging of Sensorineural Hearing Loss Imaging of Hearing Loss Discussion Outline (SNHL) Imaging Approaches Anatomic Relationships Lesions: SNHL KL Salzman, MD University of Utah School of
A pictorial review of neurological complications of systemic lupus erythematosus and antiphospholipid syndrome
 A pictorial review of neurological complications of systemic lupus erythematosus and antiphospholipid syndrome Poster No.: C-2780 Congress: ECR 2010 Type: Educational Exhibit Topic: Neuro Authors: E. Tavernaraki,
A pictorial review of neurological complications of systemic lupus erythematosus and antiphospholipid syndrome Poster No.: C-2780 Congress: ECR 2010 Type: Educational Exhibit Topic: Neuro Authors: E. Tavernaraki,
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage. By: Shifaa AlQa qa
 CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage By: Shifaa AlQa qa Subarachnoid Hemorrhage Causes: Rupture of a saccular (berry) aneurysm Vascular malformation Trauma Hematologic disturbances
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage By: Shifaa AlQa qa Subarachnoid Hemorrhage Causes: Rupture of a saccular (berry) aneurysm Vascular malformation Trauma Hematologic disturbances