HANDBOOK FOR JUNIOR RESIDENTS AND MEDICAL STUDENTS LEARNING EMERGENCY OPHTHALMOLOGY
|
|
|
- Cecil Shepherd
- 5 years ago
- Views:
Transcription

1 HANDBOOK FOR JUNIOR RESIDENTS AND MEDICAL STUDENTS LEARNING EMERGENCY OPHTHALMOLOGY Compiled by The Task Force on Undergraduate Teaching in Ophthalmology of the International Council of Ophthalmology and based on their curriculum
2 In this booklet we have put together common ophthalmic emergency conditions that we think you need to know and key ophthalmic disorders we think you need to have seen. There are descriptions and colour pictures of these conditions. This pocket sized book summaries the key points in the ophthalmology curriculum complied by the Task Force of the International Council of Ophthalmology and is a format that is very portable! Sue Lightman, Do Nhu Hon and Peter McCluskey On behalf of the International Council of Ophthalmology and Vietnam National Institute of Ophthalmology, Hanoi Medical University 2010 Other Contributing Authors with thanks Anh Dinh Kim, Anh Nguyen Quoc, Chau Hoang Thi Minh, Dong Pham Ngoc, Ha Tran Minh, Hon Do Nhu, Ngoc Do Quang, Quan Bui Dao, Richard Andrews, Thang Nguyen Canh, Thanh Pham Thi Kim, Thuy Nguyen Thi Thu, Thuy Vu Thi Bich, Tung Mai Quoc, Van Pham Thi Khanh, Van Pham Trong, Yen Nguyen Thu, Simon Taylor 2
3 Have you seen? Trauma Tick if yes Do you know how it is caused and treated? Tick if yes Note for you: Remember to look it up Periorbital haematoma Orbital blowout Lid laceration Subconjunctival Haemorrhage Chemical burns cornea and conjunctiva Foreign body Corneal abrasion Hyphema Iridodialysis Cataract Lens subluxation /dislocation Intraocular foreign body Scleral rupture 3
4 Painful Red Eye Chalazion Dacryocystitis Orbital cellulitis Conjunctivitis Scleritis Episcleritis Viral keratitis Bacterial keratitis Shingles Uveitis Acute angle-closure glaucoma Endophthalmitis Sudden Painless Loss of Vision Vitreous haemorrhage Retinal tear/detachment Central retinal artery occlusion Central retinal vein occlusion Others 4
5 Proptosis VII nerve palsy TRAUMA Ocular trauma is very common, especially in developing countries. It can involve any part of the ocular system, including the eyelids, globe and visual pathways. All patients with a history of trauma must have a full ophthalmic examination. Periorbital haematoma 5


6 Haematoma (black eye) is the most common result of blunt injury to the eyelid. Signs: Ecchymosis, sub-conjunctival haemorrhage Management: This will resolve on its own and treatment is aimed at patient comfort. Cool compresses can be useful. In cases with bilateral involvement, a skull-base fracture needs to be excluded. Orbital blowout 6


7 A blowout fracture of the orbital floor is usually the result of a sudden increase in the orbital pressure caused by a striking object, such as a fist or tennis ball. Signs: These include enophthalmos (sinking of the eye ball into the orbit), diplopia (double vision), infraorbital nerve anaesthesia and limitation of upgaze limitation. A CT scan helps to evaluate the fracture. Management: Surgical repair is often required. 7


8 Lid laceration Lid lacerations must be explored thoroughly to ensure the lacrimal system is intact. Improper eyelid closure can cause exposure keratopathy. Management: minor lid lacerations should be repaired by direct horizontal closure whenever possible, in order to archive the best functional and cosmetic results. Accurate apposition of the eyelid margins is critical. Major tissue loss needs oculoplastic surgery. Lacerated lacrimal ducts should be repaired to maintain normal tear drainage. 8



9 Subconjunctival haemorrhage 9


10 This is Blood under the conjunctiva, and is usually unilateral, localised and sharply circumscribed; the underlying sclera is often not visible. There is no inflammation, pain or discharge, and the visual acuity is unchanged. Sometimes, there can be an association with minor injuries, including eyerubbing, and it is more common with use of anti-platelet agents and anticoagulants. Management: This is mostly reassururance, but checking blood pressure and coagulation may be indicated. Chemical burns of cornea and conjunctiva Mild Moderate 10

11 Severe 11


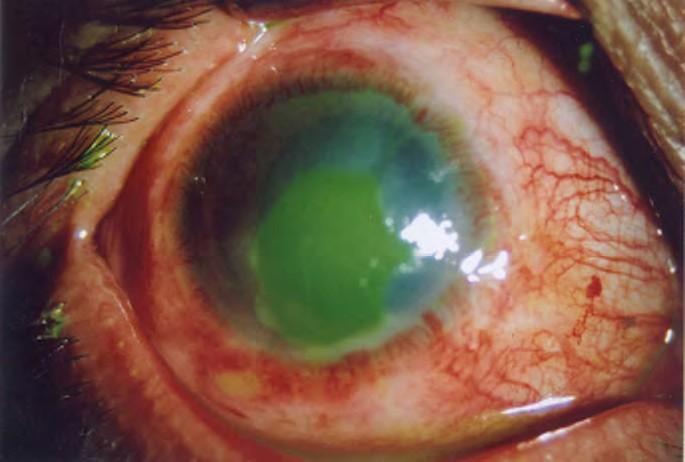
12 Alkalis (bleach, cement) tend to penetrate deeper into the ocular structures than acids. This is an ocular emergency, and the initial management consists of copious irrigation of the eyes under topical anaesthetic. Signs include corneal haze, limbal ischaemia and loss of epithelium. Management: An acute ocular emergency. Immediate, prolonged and copious irrigation with normal saline until the ocular ph remains normal. Intensive topical steroids, antibiotics and Lubricants are given. Later management may include limbal stem cell grafting for limbal stem cell loss, but keratoplasty or keratoprothesis (artifical cornea) surgery may be required for dense corneal scarring. 12

13 Superficial foreign Body Cornea 13


14 Bulbar conjunctiva Signs: foreign body on corneal surface or bulbar conjunctiva. If the foreign body is not visible, evert the eyelids to expose a possiblesubtarsal foreign body. Management: topical antibiotics after removal of the foreign body. Corneal abrasion Corneal epithelium is scraped and lost after eye trauma. Symptoms: sore, watery eye with blurred vision. Signs: red and watery eye. Fluorescein staining in area where corneal epithelium is lost. Management: topical antibiotics and eye pad for symptomatic relief. 14


15 Eye globe perforation Scleral rupture Corneal rupture 15


16 This results from severe blunt trauma and perforating ocular trauma. Signs: soft eye, protruding iris, irregular pupil. The perforated eye is prone to infection (endophthalmitis). Late complications include sympathetic ophthalmia (inflammation of the uvea of the normal fellow eye that occurs late after perforating injury) Management: Surgical primary repair. 16


17 Hyphaema Mild Severe Blood in the anterior chamber following blunt trauma to the eye. Symptoms: red eye and severe loss of vision following trauma. Signs: visible blood in anterior chamber and cornea may also be stained. Eye may be very sore if intraocular pressure is raised. Haematocornea causes cloudy vision. Management: Bed rest And topical atropine to reduce the risk of rebleeding. Urgent assessment by ophthalmologist is required, as treatment of raised intraocular pressure or anterior chamber irrigation may be required. 17


18 Iridodialysis A dehiscence of the iris from the ciliary body at its root. Symptoms: This may be asymptomatic, or it may cause monocular diplopia and glare. Signs: misshapen pupil. Management: surgical iridoplasty may be required 18


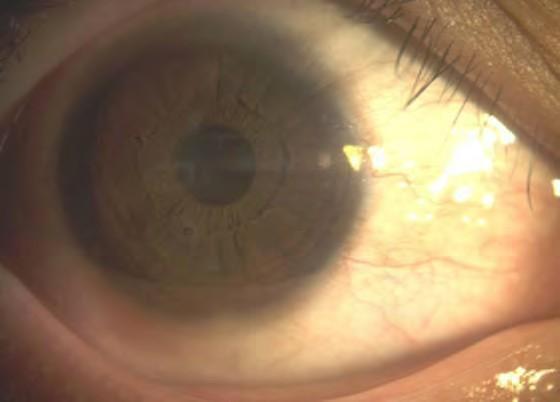
19 Cataract Traumatic cataract may arise from direct penetrating injury to the lens. Concussion may cause an imprinting of iris pigment onto the anterior lens capsule and a rosette-shaped cortical opacity. Management: cataract extraction and intraocular lens implantation 19

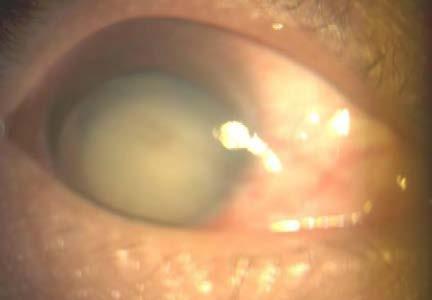

20 Lens subluxation/dislocation Lens subluxation Lens dislocated into the anterior chamber Lens dislocated out from the globe 20


21 Direct trauma to the eye may result in lens subluxation or total dislocation. Victims may experience reduced vision, monocular diplopia and intraocular hypertension. Management: lens removal with (usually) intraocular lens implantation. Intraocular foreign body (IOFB) Anterior chamber Lens 21
.")

22 Vitreous/ retina An IOFB may lodge in any of the ocular structures it passes through, so may be located anywhere from the anterior chamber, lens to the retina and choroid. Foreign bodies are prone to result in infection (endophthalmitis). Management: immediate referral to ophthalmologist for removal of foreign body. Siderosis Retinal toxicity can be caused by an iron IOFB remaining in the eye for a long time. Symptoms: reduced vision Signs: dilated pupil, rust-brown or yellow lens opacity and abolised electro-retinogram (ERG).Management: late IOFB removal may not help visual recovery. 22

23 PAINFUL RED EYE Chalazion 23

 of the 5 th (trigeminal) cranial nerve is affected, extremely painful,")
24 Inflammation of the meibomian glands causes lumps in the eyelids. Signs: eyelid swelling, redness and pain. Management: self-limited, topical antibiotics and surgical removal if necessary. Ophthalmic zoster (shingles) A painful condition caused by Herpes zoster infection. Signs: when the 1 st division (ophthalmic nerve) of the 5 th (trigeminal) cranial nerve is affected, extremely painful, blister-like lesions appear on the face. Sometimes, the cornea, uvea can get inflammed. Management: anti-viral drugs and analgesics. 24


25 Dacryocystitis Infection of the lacrimal sac usually secondary to obstruction of the lacrimal duct. Signs: a tender, red, tense swelling at the medial canthus. May be associated with preseptal cellulitis. Management: initial warm compresses and oral antibiotics. Sometimes, draining and tear sac removal may be necessary. 25


26 Orbital cellulitis 26


27 This is a life-threatening infection of the soft tissues behind the orbital septum. It is more common in children. Symptoms: fever, pain and visual impairment. Signs: unilateral, tender, warm and red periorbital lid oedema, proptosis, painful ophthalmoplegia and optic nerve dysfunction. CT scan shows thickened periocular tissues. Management: admission and intravenous antibiotic therapy. 27


28 Rhabdomyosarcoma Highly malignant orbital tumor of striated muscles in children Symptoms: unilateral eye pain. Signs: reduced vision. Extremely progressive exophthalmos or proptosis (buldging or protrusion of the eye ball), red eye. Management: referral to oncologists for exenteration, radiotherapy and chemotherapy. Conjunctivitis Inflammation of the conjunctiva (a mucous membrane that covers white of the eye and inner surface of the eyelids) Bacterial conjunctivitis 28

29 Symptoms: Red sticky eyes, usually bilaterally. Signs: red eyes with purulent discharge. No corneal or anterior chamber involvement. Systemically well. Management: regular hygiene to minimise secretion buildup, topical antibiotics for 5 days. Viral conjunctivitis 29
.")

30 Contact history with recent eye or upper respiratory tract infection symptoms (especially children). Highly contagious. Symptoms: burning sensation and watery discharge (different from purulent exudate in bacterial infections). Classically begins in one eye with rapid spread to the other, often pre-auricular lymphadenopathy. Signs: eye red and watery. Swollen conjunctiva particularly in lids. Management: will resolve on own and treatment aimed at comfort. Cool compresses, regular lubricants (without preservative). Antibiotic drops if indicated. Resolution may take weeks. Allergic conjunctivitis 30


31 Symptoms: eyes itch (++) and are red and sore. Signs: eyelid swelling and. papillae (tiny elevation on the palpebral conjunctiva). History of atopy e.g asthma, eczema. Management: remove allergens where possible, topical anti-histamines, cool compresses. Episcleritis Sectoral episcleritis 31


32 Diffuse episcleritis Inflammation of episclera, the outmost layer of the sclera. Symptoms: mild discomfort, tenderness and watering. Signs: sectoral or diffuse redness. Management: topical steroid. Self-limiting. Scleritis 32


33 This is inflammation of the sclera. In the most severe form scleral necrosis can occur. Symptoms: Eye pain which radiates to head and wakes patient at night. Signs: The eye is red and may have visible sclera nodules or a necrotic patch. The sclera may be discolored and is tender to palpation. There is often an associated history of rheumatoid arthritis, vascular or connective tissue disease. Management: Urgent (same day) referral to an ophthalmologist. Topical and /or systemic corticotherapy may be required. Keratitis Viral keratitis 33



34 Bacterial keratitis Fungal keratitis 34

 referral to ophthalmologist for corneal scrape and intensive topical antibiotic/ antiviral/")
35 Parasitic keratitis Corneal inflammation from various agents such as virus, bacteria, fungi and parasite (acanthamoeba). Symptoms: A sore, red eye, often in contact lens wearer or following trauma. Signs: White area on cornea, may be peripheral or central. Management: Urgent (same day) referral to ophthalmologist for corneal scrape and intensive topical antibiotic/ antiviral/ antifungal therapy. Keratoplasty (corneal graft) may be required especially when the cornea is perforated. 35


36 Uveitis 36

 referral to ophthalmologist for mydriasis, intensive steroid therapy and")
37 Inflammation of any part of the uveal tract (iris, ciliary body and choroid). Symptoms: photophobia, eye red and sore, vision may or may not be affected. Signs: red eye with ciliary injection around iris, anterior chamber appears cloudy from cells and flare. Management: urgent (same day) referral to ophthalmologist for mydriasis, intensive steroid therapy and aetiological workup. Acute angle-closure glaucoma 37

38 A sudden increase in intraocular pressure occurs owing to to a closed anterior chamber angle which prevents aqueous drainage. Symptoms: Painful eye with systemic symptoms including headache, nausea and vomiting. Signs: More common in Asian races. The eye is red, very tender and feels hard on palpation; the cornea usually has hazy appearance. The anterior chamber is shallow with irregular semi-dilated pupil. Management: urgent (same day) referral to ophthalmologist. Topical pilocarpine, Aqueous inhibitors and beta blockers may help to lower the intraocular pressure. Laser iridotomy or trabeculectomy is indicated according to intraocular pressure level and whether the angle is open. Additional cataract extraction may help to open the angle and normalize the pressure. Endophthalmitis 38


39 Most commonly seen after trauma or intraocular surgery. Symptoms: painful eye with loss of vision. Signs: lid swelling, discharge, red eye, hypopyon, reduced vision. Management: urgent referral to ophthalmologist for vitreous sampling, intravitreal antibiotics and vitrectomy. 39


40 Vitreous haemorrhage SUDDEN PAINLESS LOSS OF VISION Bleeding in the vitreous cavity seen in individuals with diabetes mellitus, cardio-vascular diseases and retinal detachment. Symptoms: Sudden loss of vision often with floaters. Signs: Reduced or absent red reflex. Limited or no fundal view. Management: Refer to ophthalmologist for ultrasound scan to ensure that there is no underlying retinal detachment. A vitrectomy may be required for nonclearing haemorrhage. 40


41 Retinal tear/detachment Retinal tear/ detachment occurs when there is separation of sensory retina from the retinal pigment epithelium. Most common aetiology is a predisposing retinal hole tear often associated with myopia but may follow trauma Symptoms: Painless loss of vision. The patient may have encountered a recent history of increased number of visual floaters and/ or visual flashes. There may be a dark shadow in the vision of the affected eye. Signs: Grey area of raised retina at site of detachment. The vision will be reduced if macula becomes detached. Management: urgent (same day) referral to ophthalmologist for surgical repair (cryotherapy with gas tamponade and/or scleral buckle). 41

. Fundus examination: Pale retina (abnormal and asymmetrical red reflex), cherry-red spot at macula due to cilioretinal sparing.")
42 Central retinal artery occlusion Blocked blood flow in the central retinal artery, which often occurs in one eye. Symptoms: Sudden and painless loss of vision. Signs: The visual acuity is very poor, at best perception of light or hand movements, together with a Relative Afferent Pupillary Defect (RAPD). Fundus examination: Pale retina (abnormal and asymmetrical red reflex), cherry-red spot at macula due to cilioretinal sparing. Delayed arterial filling on fluorescein angiogram. Investigation: urgent (same day) ESR and CRP to exclude giant cell arteritis. 42
 may help in some cases.")

43 Management: Urgent (same day) referral to ophthalmologist to see whether any immediate treatment is possible. Intensive intraocular pressure lowering (AC inhibitors and paracenthesis) may help in some cases. A work-up for causes of Transient Ischaemic Attacks will need to be arranged. Central retinal vein occlusion Blocked blood flow through the central retinal vein. Symptoms: Sudden and painless loss of vision. Signs: Dilated tortuous veins, cotton wool spots, optic disc swelling, retinal haemorrhage visible in all four quadrants which may obscure much of fundus 43


44 detail. Predisposing factors include increasing age, hypertension and diabetes, as well as raised intraocular pressure. Investigation and Management : Screen for diabetes and hypertension, exclude glaucoma. Routine referral for an ophthalmological opinion. Fluorescein angiography is often performed to investigate how ischaemic the fundus is, and laser can be indicated to prevent neovascular glaucoma and recurrent vitreous haemorrhage. Papillitis 44
. Management: exclude multiple sclerosis, infection of meninges, orbital tissues or paranasal sinuses.")
45 Acute inflammation of optic nerve is associated with moderate to severe vision loss. Long lasting papillitis leads to optic atrophy. Symptoms: sudden reduced vision, discomfort upon eye movement. Signs: central visual field defect, optic disc swelling, Relative Afferent Pupillary Defect (RAPD). Management: exclude multiple sclerosis, infection of meninges, orbital tissues or paranasal sinuses. Intensive systemic corticotherapy may help. Proptosis Acute or chronic expansion of globe contents which may be unilateral or bilateral Signs: may have corneal exposure, displacement of globe, vision may or may not be affected, eye movements may be affected, RAPD if optic nerve involved 45

46 Management: imaging to define cause of propotosis. Investigations as appropriate depending on which orbital structures are involved which may include thyroid function tests and orbital biopsy VII nerve palsy Main problem for eye is failure of eyeid closure so corneal exposure. May be idiopathic (Bell s palsy) or caused by trauma, tumour, infection, inflammation Signs: Vary in severity but failure to close eyelid is the key sign, may be other signs of VII th nerve palsy Management: ensure eye closure and lubricate. May recover. If not may require procedures to help with this eg tarrsorraphy, weights on upper lid. 46
Acute Eyes for ED. Enis Kocak. The Alfred Ophthalmology
 Acute Eyes for ED Enis Kocak The Alfred Ophthalmology The problem with eyes Things to cover Ocular anatomy Basic assessment Common presentations Eye first aid and procedures Ophthalmic emergencies What
Acute Eyes for ED Enis Kocak The Alfred Ophthalmology The problem with eyes Things to cover Ocular anatomy Basic assessment Common presentations Eye first aid and procedures Ophthalmic emergencies What
EYE TRAUMA: INCIDENCE
 Introduction EYE TRAUMA: INCIDENCE 2.5 million eye injuries per year in U.S. 40,000 60,000 of eye injuries lead to visual loss Introduction Final visual outcome of many ocular emergencies depends on prompt,
Introduction EYE TRAUMA: INCIDENCE 2.5 million eye injuries per year in U.S. 40,000 60,000 of eye injuries lead to visual loss Introduction Final visual outcome of many ocular emergencies depends on prompt,
PAINFUL PAINLESS Contact lens user BOV
 Common Causes Allergies Infections Ocular Cornea, uveitis, endophthalmitis Orbital Orbital cellulitis Inflammation Uveitis Scleritis / episcleritis Glaucomas Trauma Foreign bodies Chemical injuries History
Common Causes Allergies Infections Ocular Cornea, uveitis, endophthalmitis Orbital Orbital cellulitis Inflammation Uveitis Scleritis / episcleritis Glaucomas Trauma Foreign bodies Chemical injuries History
OPHTHALMOLOGY REFERRAL GUIDE FOR GPS
 OPHTHALMOLOGY REFERRAL GUIDE FOR GPS A guidebook to support general practitioners in the management and referral of a range of common eye problems. Contents 3 Introduction 4 Ophthalmic Workup 6 Acute Visual
OPHTHALMOLOGY REFERRAL GUIDE FOR GPS A guidebook to support general practitioners in the management and referral of a range of common eye problems. Contents 3 Introduction 4 Ophthalmic Workup 6 Acute Visual
Ocular Urgencies and Emergencies
 Ocular Urgencies and Emergencies Pam Boyce, O.D., F.A.A.O. Boyce Family Eye Care, Ltd. 528 Devon Ave. Park Ridge, IL 60068 847-518-0303 Somebody s going to lose an eye Epidemiology 2.4 million ocular and
Ocular Urgencies and Emergencies Pam Boyce, O.D., F.A.A.O. Boyce Family Eye Care, Ltd. 528 Devon Ave. Park Ridge, IL 60068 847-518-0303 Somebody s going to lose an eye Epidemiology 2.4 million ocular and
Handbook for Medical Students Learning Ophthalmology
 International Council of Ophthalmology Handbook for Medical Students Learning Ophthalmology 2009 Compiled by the Task Force on Undergraduate Teaching in Ophthalmology of the International Council of Ophthalmology
International Council of Ophthalmology Handbook for Medical Students Learning Ophthalmology 2009 Compiled by the Task Force on Undergraduate Teaching in Ophthalmology of the International Council of Ophthalmology
Ocular Lecture. Sue Bednar NP Ali Atwater PA-C
 Ocular Lecture Sue Bednar NP Ali Atwater PA-C Triaging Ocular Complaints Painful Eye/Red eye +/-blurry vision +/-visual loss +/-floaters +/-fevers If any of the above findings exist, pt is likely to have
Ocular Lecture Sue Bednar NP Ali Atwater PA-C Triaging Ocular Complaints Painful Eye/Red eye +/-blurry vision +/-visual loss +/-floaters +/-fevers If any of the above findings exist, pt is likely to have
Paediatric acute ophthalmology. Harry Bradshaw
 Paediatric acute ophthalmology Harry Bradshaw Approach Red eye Leukocoria Neurological Trauma Visual loss Red eye Orbital Eyelid Conjunctiva Cornea Uvea Orbital Orbit fixed volume Contiguous with sinuses,
Paediatric acute ophthalmology Harry Bradshaw Approach Red eye Leukocoria Neurological Trauma Visual loss Red eye Orbital Eyelid Conjunctiva Cornea Uvea Orbital Orbit fixed volume Contiguous with sinuses,
Dr Jo-Anne Pon. Dr Sean Every. 8:30-9:25 WS #70: Eye Essentials for GPs 9:35-10:30 WS #80: Eye Essentials for GPs (Repeated)
") Dr Sean Every Ophthalmologist Southern Eye Specialists Christchurch Dr Jo-Anne Pon Ophthalmologist Southern Eye Specialists, Christchurch Hospital, Christchurch 8:30-9:25 WS #70: Eye Essentials for GPs
Dr Sean Every Ophthalmologist Southern Eye Specialists Christchurch Dr Jo-Anne Pon Ophthalmologist Southern Eye Specialists, Christchurch Hospital, Christchurch 8:30-9:25 WS #70: Eye Essentials for GPs
Management of specific eye problems in the ED
 of specific eye problems in the ED CORNEAL ABRASION Causes Foreign bodies Tangential shearing injuries, e.g. poking finger into eye Exact cause of injury (Remember to exclude possibility of intraocular
of specific eye problems in the ED CORNEAL ABRASION Causes Foreign bodies Tangential shearing injuries, e.g. poking finger into eye Exact cause of injury (Remember to exclude possibility of intraocular
Mild NPDR. Moderate NPDR. Severe NPDR
 Diabetic retinopathy Diabetic retinopathy is the most common cause of blindness in adults aged 35-65 years-old. Hyperglycaemia is thought to cause increased retinal blood flow and abnormal metabolism in
Diabetic retinopathy Diabetic retinopathy is the most common cause of blindness in adults aged 35-65 years-old. Hyperglycaemia is thought to cause increased retinal blood flow and abnormal metabolism in
Differential diagnosis of the red eye. Carol Slight Nurse Practitioner Ophthalmology
 Differential diagnosis of the red eye Carol Slight Nurse Practitioner Ophthalmology The red eye Conjunctivitis HSV Keratitis Acute angle closure glaucoma Anterior Uveitis Red eye Scleritis Subconjunctival
Differential diagnosis of the red eye Carol Slight Nurse Practitioner Ophthalmology The red eye Conjunctivitis HSV Keratitis Acute angle closure glaucoma Anterior Uveitis Red eye Scleritis Subconjunctival
Work Sheet And Course Hand Out
 Work Sheet And Course Hand Out This course provides the primary care health professional with a basic understanding of the eye, its function and the assessment of common sight- and non-sight threatening
Work Sheet And Course Hand Out This course provides the primary care health professional with a basic understanding of the eye, its function and the assessment of common sight- and non-sight threatening
THE 35 GOLDEN EYE RULES
 THE 35 GOLDEN EYE RULES The Sense of Sight, from La Dame a la Licorne, The Lady and the Unicorn Tapestries, Late 15th Century Flemish Tapestry in wool and silk, Musée Nationale du Moyen Age, Paris. 1.
THE 35 GOLDEN EYE RULES The Sense of Sight, from La Dame a la Licorne, The Lady and the Unicorn Tapestries, Late 15th Century Flemish Tapestry in wool and silk, Musée Nationale du Moyen Age, Paris. 1.
Ocular and Periocular Trauma. Tina Rutar, MD. Assistant Professor of Ophthalmology and Pediatrics. Director, Visual Center for the Child
 Ocular and Periocular Trauma Tina Rutar, MD Assistant Professor of Ophthalmology and Pediatrics Director, Visual Center for the Child University of California, San Francisco Phone: 415-353-2560 Fax: 415-353-2468
Ocular and Periocular Trauma Tina Rutar, MD Assistant Professor of Ophthalmology and Pediatrics Director, Visual Center for the Child University of California, San Francisco Phone: 415-353-2560 Fax: 415-353-2468
Examining Children s Eyes
 Paediatric Ophthalmology What to refer & when? Aims Tips for assessing a child s eyes in general practice Common paediatric ophthalmology symptoms and signs What needs to be referred and when? MISS FARIHA
Paediatric Ophthalmology What to refer & when? Aims Tips for assessing a child s eyes in general practice Common paediatric ophthalmology symptoms and signs What needs to be referred and when? MISS FARIHA
Assessment and Management of Ocular Trauma. Disclosure I have no direct financial interests in today s subject matter. 3/25/2019. Normal Eye Anatomy
 Assessment and Management of Ocular Trauma Samiksha Fouzdar Jain, MD,FRCS Department of Ophthalmology & Visual Sciences Truhlsen Eye Institute Disclosure I have no direct financial interests in today s
Assessment and Management of Ocular Trauma Samiksha Fouzdar Jain, MD,FRCS Department of Ophthalmology & Visual Sciences Truhlsen Eye Institute Disclosure I have no direct financial interests in today s
Eye Trauma. Lid Laceration. Orbital Fracture
 Eye Trauma Lid Laceration The presence of a lid laceration, however insignificant, mandates careful exploration of the wound and examination of the globe. 1. Superficial lacerations parallel to the lid
Eye Trauma Lid Laceration The presence of a lid laceration, however insignificant, mandates careful exploration of the wound and examination of the globe. 1. Superficial lacerations parallel to the lid
Ocular and periocular trauma
 Ocular and periocular trauma No financial disclosures. Tina Rutar M.D. Assistant Professor of Clinical Ophthalmology and Pediatrics Director, Visual Center for the Child University of California San Francisco
Ocular and periocular trauma No financial disclosures. Tina Rutar M.D. Assistant Professor of Clinical Ophthalmology and Pediatrics Director, Visual Center for the Child University of California San Francisco
UC SF. g h. Eye Trauma. Martha Neighbor, MD Emergency Services San Francisco General Hospital University of California
 UC SF Eye Trauma sf g h Martha Neighbor, MD Emergency Services San Francisco General Hospital University of California Goals Recognize vision threatening eye emergencies Treat them when we can Know when
UC SF Eye Trauma sf g h Martha Neighbor, MD Emergency Services San Francisco General Hospital University of California Goals Recognize vision threatening eye emergencies Treat them when we can Know when
Sepideh Tara Rousta, MD FAAO Robert Wood Johnson University Hospital Saint Peter s University Hospital Wills Eye Hospital
 Sepideh Tara Rousta, MD FAAO Robert Wood Johnson University Hospital Saint Peter s University Hospital Wills Eye Hospital 14 mo old w R eye cross (parents) 9 mo old R eye crossing getting worse for past
Sepideh Tara Rousta, MD FAAO Robert Wood Johnson University Hospital Saint Peter s University Hospital Wills Eye Hospital 14 mo old w R eye cross (parents) 9 mo old R eye crossing getting worse for past
5/2/2016 EYE EMERGENCIES. Nathaniel Pelsor, O.D., FAAO Talley Medical-Surgical Eye Care Associates. Anatomy. Tools
 EYE EMERGENCIES Nathaniel Pelsor, O.D., FAAO Talley Medical-Surgical Eye Care Associates Anatomy Tools 1 Contact dermatitis Blepharitis HSV Preseptal Cellulitis Anterior Chamber Subconjunctival hemorrhage
EYE EMERGENCIES Nathaniel Pelsor, O.D., FAAO Talley Medical-Surgical Eye Care Associates Anatomy Tools 1 Contact dermatitis Blepharitis HSV Preseptal Cellulitis Anterior Chamber Subconjunctival hemorrhage
Ophthalmic Trauma Update
 Ophthalmic Trauma Update Richard S. Davidson, M.D. Professor of Ophthalmology Vice Chair for Quality and Clinical Affairs UCHealth Eye Center University of Colorado School of Medicine August 5, 2017 Financial
Ophthalmic Trauma Update Richard S. Davidson, M.D. Professor of Ophthalmology Vice Chair for Quality and Clinical Affairs UCHealth Eye Center University of Colorado School of Medicine August 5, 2017 Financial
Ophthalmology. Corneal Abrasion. History
 Ophthalmology Corneal Abrasion - Usually clear history of very recent trauma - Foreign Body Sensation - Pain +++ - Lacrimation - Photophobia Fig. 1 Corneal Abrasion - Abrasion stains yellow / green with
Ophthalmology Corneal Abrasion - Usually clear history of very recent trauma - Foreign Body Sensation - Pain +++ - Lacrimation - Photophobia Fig. 1 Corneal Abrasion - Abrasion stains yellow / green with
Focusing on A&E. By Sandy Cooper, (Ophthalmic Nurse Practitioner), Tel
, Tel") Focusing on A&E By Sandy Cooper, (Ophthalmic Nurse Practitioner), Tel 01752 439331 Email sandra.cooper5@nhs.net sandracooper041@btinternet.com THINGS TO WORRY ABOUT WITH ANY EYE PROBLEM CHANGES IN VISION
Focusing on A&E By Sandy Cooper, (Ophthalmic Nurse Practitioner), Tel 01752 439331 Email sandra.cooper5@nhs.net sandracooper041@btinternet.com THINGS TO WORRY ABOUT WITH ANY EYE PROBLEM CHANGES IN VISION
REFERRAL GUIDELINES: OPHTHALMOLOGY
 Outpatient Referral Guidelines Page 1 1 REFERRAL GUIDELINES: OPHTHALMOLOGY Date of birth Demographic Contact details (including mobile phone) Clinical Reason for referral Duration of symptoms Essential
Outpatient Referral Guidelines Page 1 1 REFERRAL GUIDELINES: OPHTHALMOLOGY Date of birth Demographic Contact details (including mobile phone) Clinical Reason for referral Duration of symptoms Essential
Phone Triage for Optometric Staff ???????? CHEMICAL BURN CHEMICAL BURN
 Phone Triage for Optometric Staff There are very few ocular emergencies that you will have to deal with in practice, but it is imperative that you be able to Michelle Welch, O.D. NSU Oklahoma College of
Phone Triage for Optometric Staff There are very few ocular emergencies that you will have to deal with in practice, but it is imperative that you be able to Michelle Welch, O.D. NSU Oklahoma College of
MRI masterfile Part 5 WM Heme Strokes.ppt 1
 Ocular and Orbital Trauma Eye Trauma: Incidence 1.3 million eye injuries in the US per year. 40,000 of these injuries lead to blindness in the US. Patrick Sibony, MD March 23, 2013 Ophthalmic Emergencies
Ocular and Orbital Trauma Eye Trauma: Incidence 1.3 million eye injuries in the US per year. 40,000 of these injuries lead to blindness in the US. Patrick Sibony, MD March 23, 2013 Ophthalmic Emergencies
By Darlene Jones, Nurse. May 2017
 By Darlene Jones, Nurse May 2017 Disclosure of potential conflict of interest Darlene Jones, Nurse I have no conflict of interest Course objectives Become familiar with the different pathologies in ophthalmology
By Darlene Jones, Nurse May 2017 Disclosure of potential conflict of interest Darlene Jones, Nurse I have no conflict of interest Course objectives Become familiar with the different pathologies in ophthalmology
10/4/2013. Bruce K.Williams, MSN, RN,ACNP-BC Sisters of Charity Providence Hospitals. What is the worst thing that can go wrong with an eye?
 Red Eyes, Red Alert! Bruce K.Williams, MSN, RN,ACNP-BC Sisters of Charity Providence Hospitals Red Eyes, Red Alert! Red Eyes, Red Alert! What is the worst thing that can go wrong with an eye? 1 Red Eyes,
Red Eyes, Red Alert! Bruce K.Williams, MSN, RN,ACNP-BC Sisters of Charity Providence Hospitals Red Eyes, Red Alert! Red Eyes, Red Alert! What is the worst thing that can go wrong with an eye? 1 Red Eyes,
THE RED EYE Cynthia McNamara, MD Week 25
 THE RED EYE Cynthia McNamara, MD Week 25 Educational Objectives: 1. Know the differential diagnosis and presentation of specific etiologies of the red eye 2. Be able to evaluate patients presenting with
THE RED EYE Cynthia McNamara, MD Week 25 Educational Objectives: 1. Know the differential diagnosis and presentation of specific etiologies of the red eye 2. Be able to evaluate patients presenting with
Test Bank for Medical Surgical Nursing An Integrated Approach 3rd Edition by White
 Test Bank for Medical Surgical Nursing An Integrated Approach 3rd Edition by White Link full download : http://testbankair.com/download/test-bank-for-medical-surgical-nursing-anintegrated-approach-3rd-edition-by-white/
Test Bank for Medical Surgical Nursing An Integrated Approach 3rd Edition by White Link full download : http://testbankair.com/download/test-bank-for-medical-surgical-nursing-anintegrated-approach-3rd-edition-by-white/
Eyes, ears, teeth and everything in between
 Eyes, ears, teeth and everything in between E M E R G E N C Y D E P A R T M E N T J U N I O R T E A C H created 14/11/10 by S.R. Bruijns, version 1.0 Objectives Eyes Ears Teeth Maxilla- facial EYES Approaching
Eyes, ears, teeth and everything in between E M E R G E N C Y D E P A R T M E N T J U N I O R T E A C H created 14/11/10 by S.R. Bruijns, version 1.0 Objectives Eyes Ears Teeth Maxilla- facial EYES Approaching
A Case of Carotid-Cavernous Fistula
 A Case of Carotid-Cavernous Fistula By : Mohamed Elkhawaga 2 nd Year Resident of Ophthalmology Alexandria University A 19 year old male patient came to our outpatient clinic, complaining of : -Severe conjunctival
A Case of Carotid-Cavernous Fistula By : Mohamed Elkhawaga 2 nd Year Resident of Ophthalmology Alexandria University A 19 year old male patient came to our outpatient clinic, complaining of : -Severe conjunctival
Faculty Financial Disclosure. Learning Objectives: Office Ophthalmology. Basic Eye Exam: What s in your pocket/office? Office Ophthalmology
 Faculty Financial Disclosure Office Ophthalmology Lynn K. Gordon, MD, PhD, has no financial relationships to disclose. Lynn K. Gordon, MD, PhD Professor and Vernon O Underwood Family Chair Department of
Faculty Financial Disclosure Office Ophthalmology Lynn K. Gordon, MD, PhD, has no financial relationships to disclose. Lynn K. Gordon, MD, PhD Professor and Vernon O Underwood Family Chair Department of
Identify the choice that best completes the statement or answers the question.
 Chapter 5. The Eye Multiple Choice Identify the choice that best completes the statement or answers the question. 1. The most common type of eye disorder is: A. Refractive errors B. Macular conditions
Chapter 5. The Eye Multiple Choice Identify the choice that best completes the statement or answers the question. 1. The most common type of eye disorder is: A. Refractive errors B. Macular conditions
SILA THONGLAI MD. Bangkok Eye center Bangkok Hospital Thailand
 SILA THONGLAI MD. Bangkok Eye center Bangkok Hospital Thailand Ocular Anatomy Bony Components of Orbit 1 1. Frontal bone 4 5 7 6 2. Zygomatic bone 3. Maxillary bone 4. Sphenoid bone 5. Ethmoid bone 2 3
SILA THONGLAI MD. Bangkok Eye center Bangkok Hospital Thailand Ocular Anatomy Bony Components of Orbit 1 1. Frontal bone 4 5 7 6 2. Zygomatic bone 3. Maxillary bone 4. Sphenoid bone 5. Ethmoid bone 2 3
CORNEAL CONDITIONS CORNEAL TRANSPLANTATION
 GENERAL INFORMATION CORNEAL CONDITIONS CORNEAL TRANSPLANTATION WHAT ARE CORNEAL CONDITIONS? The cornea is the clear outer layer of the eye. Shaped like a dome, it helps to protect the eye from foreign
GENERAL INFORMATION CORNEAL CONDITIONS CORNEAL TRANSPLANTATION WHAT ARE CORNEAL CONDITIONS? The cornea is the clear outer layer of the eye. Shaped like a dome, it helps to protect the eye from foreign
EYE INJURIES OBJECTIVES COMMON EYE EMERGENCIES 7/19/2017 IMPROVE ASSESSMENT OF EYE INJURIES
 EYE INJURIES BRITTA ANDERSON D.O. DMC PRIMARY CARE SPORTS MEDICINE ASSOCIATE TEAM PHYSICIAN DETROIT TIGERS OBJECTIVES IMPROVE ASSESSMENT OF EYE INJURIES UNDERSTAND WHAT IS CONSIDERED AN EMERGENCY DEVELOP
EYE INJURIES BRITTA ANDERSON D.O. DMC PRIMARY CARE SPORTS MEDICINE ASSOCIATE TEAM PHYSICIAN DETROIT TIGERS OBJECTIVES IMPROVE ASSESSMENT OF EYE INJURIES UNDERSTAND WHAT IS CONSIDERED AN EMERGENCY DEVELOP
OOGZIEKTEN VOOR DE HUISARTS F. GOES, JR.
 OOGZIEKTEN VOOR DE HUISARTS F. GOES, JR. HET RODE OOG F. GOES, JR. Condition Signs Symptoms Causes Conjunctivitis Viral Normal vision, normal pupil size Mild to no pain, diffuse Adenovirus (most common),
OOGZIEKTEN VOOR DE HUISARTS F. GOES, JR. HET RODE OOG F. GOES, JR. Condition Signs Symptoms Causes Conjunctivitis Viral Normal vision, normal pupil size Mild to no pain, diffuse Adenovirus (most common),
Clinical Practice Guide for the Diagnosis, Treatment and Management of Anterior Eye Conditions. April 2018
 Clinical Practice Guide for the Diagnosis, Treatment and Management of Anterior Eye Conditions This Clinical Practice Guide provides evidence-based information about current best practice in the management
Clinical Practice Guide for the Diagnosis, Treatment and Management of Anterior Eye Conditions This Clinical Practice Guide provides evidence-based information about current best practice in the management
Ocular Emergencies. Pisit Preechawat, MD Department of Ophthalmology, Ramathibodi Hospital
 Ocular Emergencies Pisit Preechawat, MD Department of Ophthalmology, Ramathibodi Hospital Ocular Anatomy Bony Components of Orbit 1 1. Frontal bone 4 5 7 6 2. Zygomatic bone 3. Maxillary bone 4. Sphenoid
Ocular Emergencies Pisit Preechawat, MD Department of Ophthalmology, Ramathibodi Hospital Ocular Anatomy Bony Components of Orbit 1 1. Frontal bone 4 5 7 6 2. Zygomatic bone 3. Maxillary bone 4. Sphenoid
LECTURE # 7 EYECARE REVIEW: PART III
 LECTURE # 7 EYECARE REVIEW: PART III HOW TO TRIAGE EYE EMERGENCIES STEVE BUTZON, O.D. EYECARE REVIEW: HOW TO TRIAGE EYE EMERGENCIES FOR PRIMARY CARE PHYSICIANS Steve Butzon, O.D. Member Director IDOC President
LECTURE # 7 EYECARE REVIEW: PART III HOW TO TRIAGE EYE EMERGENCIES STEVE BUTZON, O.D. EYECARE REVIEW: HOW TO TRIAGE EYE EMERGENCIES FOR PRIMARY CARE PHYSICIANS Steve Butzon, O.D. Member Director IDOC President
Professor Helen Danesh-Meyer. Eye Institute Auckland
 Professor Helen Danesh-Meyer Eye Institute Auckland Bitten by Ophthalmology Emergencies Helen Danesh-Meyer, MBChB, MD, FRANZCO Sir William and Lady Stevenson Professor of Ophthalmology Head of Glaucoma
Professor Helen Danesh-Meyer Eye Institute Auckland Bitten by Ophthalmology Emergencies Helen Danesh-Meyer, MBChB, MD, FRANZCO Sir William and Lady Stevenson Professor of Ophthalmology Head of Glaucoma
The Emergent Eye in the Acute Setting
 The Emergent Eye in the Acute Setting Todd P. Margolis MD, PhD Professor of Ophthalmology & Director of the F.I. Proctor Foundation UCSF Physical Exam-- Visual Acuity Essential Corrected visual acuity
The Emergent Eye in the Acute Setting Todd P. Margolis MD, PhD Professor of Ophthalmology & Director of the F.I. Proctor Foundation UCSF Physical Exam-- Visual Acuity Essential Corrected visual acuity
10 EYE EMERGENCIES. Who goes, who you better not send! Brant Slomovic, MD, FRCPC University Health Network
 10 EYE EMERGENCIES Who goes, who you better not send! Brant Slomovic, MD, FRCPC University Health Network DISCLOSURES I have none PVD CASE 1 WHAT IS A PVD? a process of aging (45-55) liquefaction of vitreous
10 EYE EMERGENCIES Who goes, who you better not send! Brant Slomovic, MD, FRCPC University Health Network DISCLOSURES I have none PVD CASE 1 WHAT IS A PVD? a process of aging (45-55) liquefaction of vitreous
9/23/2014. Emily Thomas, O.D. MOA Paraoptometric Education October 5, 2014
 Emily Thomas, O.D. MOA Paraoptometric Education October 5, 2014 Anterior toward the front of the body Posterior toward the rear of the body Unilateral only one eye involved Bilateral both eyes involved
Emily Thomas, O.D. MOA Paraoptometric Education October 5, 2014 Anterior toward the front of the body Posterior toward the rear of the body Unilateral only one eye involved Bilateral both eyes involved
OPHTHALMOLOGIC PEARLS FOR THE NON- OPHTHALMOLOGIST. David G. Gross D.O. Deen-Gross Eye Centers Merrillville-Hobart Deengrosseye.
 OPHTHALMOLOGIC PEARLS FOR THE NON- OPHTHALMOLOGIST David G. Gross D.O. Deen-Gross Eye Centers Merrillville-Hobart Deengrosseye.com A FEW OF THE AREAS WE WILL DISCUSS Red Eye Glaucoma Neuro ophthalmic tid
OPHTHALMOLOGIC PEARLS FOR THE NON- OPHTHALMOLOGIST David G. Gross D.O. Deen-Gross Eye Centers Merrillville-Hobart Deengrosseye.com A FEW OF THE AREAS WE WILL DISCUSS Red Eye Glaucoma Neuro ophthalmic tid
Around The Globe in 60 Minutes
 Around The Globe in 60 Minutes Around the GLOBE in Sixty Minutes Basic Ocular Anatomy, Examination, and Diagnostic Techniques Introduction Focusing on canine and feline ocular anatomy and basic examination
Around The Globe in 60 Minutes Around the GLOBE in Sixty Minutes Basic Ocular Anatomy, Examination, and Diagnostic Techniques Introduction Focusing on canine and feline ocular anatomy and basic examination
Index. C Canalicular system, 4 Carbonic anhydrase inhibitors, 29 30
 A Acanthamoeba keratitis (AK), 82, 83 Acute angle-closure crisis, 156 Acute angle-closure glaucoma (AACG), 121, 141, 284 causes of, 122 clinical presentation, 153 evaluation, 156 157 management/treatment,
A Acanthamoeba keratitis (AK), 82, 83 Acute angle-closure crisis, 156 Acute angle-closure glaucoma (AACG), 121, 141, 284 causes of, 122 clinical presentation, 153 evaluation, 156 157 management/treatment,
MRI masterfile Part 5 WM Heme Strokes.ppt 2
 Imaging of Orbital Trauma Corneal Abrasion CT scan is preferable to MRI Bone, Rapid, Easy to monitor patient Foreign bodies, air, hemorrhage Fractures Cost Needed for an MRI MRI Globe and intraocular injuries
Imaging of Orbital Trauma Corneal Abrasion CT scan is preferable to MRI Bone, Rapid, Easy to monitor patient Foreign bodies, air, hemorrhage Fractures Cost Needed for an MRI MRI Globe and intraocular injuries
OCCLUSIVE VASCULAR DISORDERS OF THE RETINA
 OCCLUSIVE VASCULAR DISORDERS OF THE RETINA Learning outcomes By the end of this lecture the students would be able to Classify occlusive vascular disorders (OVD) of the retina. Correlate the clinical features
OCCLUSIVE VASCULAR DISORDERS OF THE RETINA Learning outcomes By the end of this lecture the students would be able to Classify occlusive vascular disorders (OVD) of the retina. Correlate the clinical features
Injury. Contusion Lamellar Laceration Laceration Rupture. Penetrating IOFB. Perforating
 Mechanical Ocular Trauma Došková Hana, MD. Department of Ophthalmology Medicine Faculty of Masaryk University Brno General Considerations Ocular trauma constitude about 6% of all injuries, but eyes set
Mechanical Ocular Trauma Došková Hana, MD. Department of Ophthalmology Medicine Faculty of Masaryk University Brno General Considerations Ocular trauma constitude about 6% of all injuries, but eyes set
Andrew J. Hendershot, MD Havener Eye Institute The Ohio State University s Wexner Medical Center
 Ocular Trauma for the Primary Care Physician Andrew J. Hendershot, MD Havener Eye Institute The Ohio State University s Wexner Medical Center Relevance Often those with minor eye injuries will first seek
Ocular Trauma for the Primary Care Physician Andrew J. Hendershot, MD Havener Eye Institute The Ohio State University s Wexner Medical Center Relevance Often those with minor eye injuries will first seek
Ocular warning signs in GP practice: Paediatric Eye Pointers
 Ocular warning signs in GP practice: Paediatric Eye Pointers Dr Benjamin Chang MB, BCh, BAO, MMedSci, FRCS(Irel), FRCS(Edin), FRCOphth(Lond) Senior Consultant Ophthalmology and Visual Sciences Khoo Teck
Ocular warning signs in GP practice: Paediatric Eye Pointers Dr Benjamin Chang MB, BCh, BAO, MMedSci, FRCS(Irel), FRCS(Edin), FRCOphth(Lond) Senior Consultant Ophthalmology and Visual Sciences Khoo Teck
Scrub In. What is the function of vitreous humor? What does the pupil do when exposed to bright light? a. Maintain eye shape and provide color vision
 Scrub In What is the function of vitreous humor? a. Maintain eye shape and provide color vision b. Maintain eye shape and refract light rays c. Provide night vision and color vision d. Provide night vision
Scrub In What is the function of vitreous humor? a. Maintain eye shape and provide color vision b. Maintain eye shape and refract light rays c. Provide night vision and color vision d. Provide night vision
Ophthalmology Unit Referral Guidelines
 Ophthalmology Unit Referral Guidelines Austin Health Ophthalmology Unit holds sub-specialty sessions to discuss and plan the treatment of patients with specific ocular conditions. General including cataract
Ophthalmology Unit Referral Guidelines Austin Health Ophthalmology Unit holds sub-specialty sessions to discuss and plan the treatment of patients with specific ocular conditions. General including cataract
Ocular Emergencies. What is an emergency to the patient is not necessarily an emergency to the staff
 OCULAR EMERGENCIES Ophthalmic Photographers Society November 15, 2013 Michael A. DellaVecchia MD PhD FACS Wills Eye Emergency Department Philadelphia PA Ocular Emergencies What is an emergency to the patient
OCULAR EMERGENCIES Ophthalmic Photographers Society November 15, 2013 Michael A. DellaVecchia MD PhD FACS Wills Eye Emergency Department Philadelphia PA Ocular Emergencies What is an emergency to the patient
For further reading we recommend the following excellent textbooks:
 FURTHER READING Intravitreal Injections Downloaded from www.worldscientific.com For further reading we recommend the following excellent textbooks: Clinical Anatomy of the Eye by Richard S Snell and Michael
FURTHER READING Intravitreal Injections Downloaded from www.worldscientific.com For further reading we recommend the following excellent textbooks: Clinical Anatomy of the Eye by Richard S Snell and Michael
An Injector s Guide to OZURDEX (dexamethasone intravitreal implant) 0.7 mg
 0.7 mg") An Injector s Guide to OZURDEX (dexamethasone intravitreal implant) 0.7 mg This guide is intended to provide injectors with information on the recommended injection technique and the important risks related
An Injector s Guide to OZURDEX (dexamethasone intravitreal implant) 0.7 mg This guide is intended to provide injectors with information on the recommended injection technique and the important risks related
Primary Angle Closure Glaucoma
 www.eyesurgeonlondon.co.uk Primary Angle Closure Glaucoma What is Glaucoma? Glaucoma is a condition in which there is damage to the optic nerve. This nerve carries visual signals from the eye to the brain.
www.eyesurgeonlondon.co.uk Primary Angle Closure Glaucoma What is Glaucoma? Glaucoma is a condition in which there is damage to the optic nerve. This nerve carries visual signals from the eye to the brain.
2/5/2018. Trauma. Subdivided into two main categories: Closed globe Open Globe
 1 2 3 4 5 Ocular Trauma Guide for Eye Care Office Staff Winter Thaw 2018 Aaron Yatskevich OD Definition A broad term used to describe a physical or chemical wound to the eye or eye socket. Ocular trauma
1 2 3 4 5 Ocular Trauma Guide for Eye Care Office Staff Winter Thaw 2018 Aaron Yatskevich OD Definition A broad term used to describe a physical or chemical wound to the eye or eye socket. Ocular trauma
Ocular Injuries in Sports. Rance McClain, D.O. Associate Dean, Clinical Sciences William Carey University FM/NMM-OMM/Sports Medicine
 Ocular Injuries in Sports Rance McClain, D.O. Associate Dean, Clinical Sciences William Carey University FM/NMM-OMM/Sports Medicine http://sudc.org/vienna/ Learning Objectives 1. Know the sport classification
Ocular Injuries in Sports Rance McClain, D.O. Associate Dean, Clinical Sciences William Carey University FM/NMM-OMM/Sports Medicine http://sudc.org/vienna/ Learning Objectives 1. Know the sport classification
Department of Ophthalmology
 Department of Ophthalmology Period : 02/July/18 to 30/August/18 Semester : 7 th Semester Lecture Lesson Plan Sr. Date Topic Lesson plan Name of Faculty No. 1 02.07.18 Lens- Lens-Anatomy, Classification
Department of Ophthalmology Period : 02/July/18 to 30/August/18 Semester : 7 th Semester Lecture Lesson Plan Sr. Date Topic Lesson plan Name of Faculty No. 1 02.07.18 Lens- Lens-Anatomy, Classification
Ophthalmology PANRE Review. Brock Phillips, PA-C
 Ophthalmology PANRE Review Brock Phillips, PA-C I am not an ophthalmologist, optometrist or certified eye guy of any sort - I am a practicing UC/EM PA-C who frequently evaluates eye/vision complaints,
Ophthalmology PANRE Review Brock Phillips, PA-C I am not an ophthalmologist, optometrist or certified eye guy of any sort - I am a practicing UC/EM PA-C who frequently evaluates eye/vision complaints,
OPHTHALMOLOGY DEPARTMENT Primary care referral guidelines
 OPHTHALMOLOGY DEPARTMENT Primary care referral guidelines Contents REFERRAL CATEGIES... 2 Emergency... 2 Urgent... 2 Semi urgent/routine... 2 Not accepted... 2 OPHTHALMOLOGY CONDITIONS NOT ACCEPTED...
OPHTHALMOLOGY DEPARTMENT Primary care referral guidelines Contents REFERRAL CATEGIES... 2 Emergency... 2 Urgent... 2 Semi urgent/routine... 2 Not accepted... 2 OPHTHALMOLOGY CONDITIONS NOT ACCEPTED...
The Red Eye: Conjunctivitis, Iritis, or Worse? Sean P. Donahue, MD, PhD
 The Red Eye: Conjunctivitis, Iritis, or Worse? Sean P. Donahue, MD, PhD Sam and Darthea Coleman Chair Vice Chair of Clinical Affairs, Department of Ophthalmology Professor of Pediatrics, Ophthalmology,
The Red Eye: Conjunctivitis, Iritis, or Worse? Sean P. Donahue, MD, PhD Sam and Darthea Coleman Chair Vice Chair of Clinical Affairs, Department of Ophthalmology Professor of Pediatrics, Ophthalmology,
Department of Ophthalmology
 Period : 03/July/17 to 07/September/17 Semester : 7 th Semester Department of Ophthalmology Lecture Lesson Plan Sr 1 03.07.17 Uvea-Anatomy, Uvea-Anatomy, Classification of Uveitis Dr R Paranjpe Classification
Period : 03/July/17 to 07/September/17 Semester : 7 th Semester Department of Ophthalmology Lecture Lesson Plan Sr 1 03.07.17 Uvea-Anatomy, Uvea-Anatomy, Classification of Uveitis Dr R Paranjpe Classification
Recurrent intraocular hemorrhage secondary to cataract wound neovascularization (Swan Syndrome)
") Recurrent intraocular hemorrhage secondary to cataract wound neovascularization (Swan Syndrome) John J. Chen MD, PhD; Young H. Kwon MD, PhD August 6, 2012 Chief complaint: Recurrent vitreous hemorrhage,
Recurrent intraocular hemorrhage secondary to cataract wound neovascularization (Swan Syndrome) John J. Chen MD, PhD; Young H. Kwon MD, PhD August 6, 2012 Chief complaint: Recurrent vitreous hemorrhage,
Dr. D. Y. Patil Medical College, Pimpri, Pune
 Dr. D. Y. Patil Medical College, Pimpri, Pune - 411 018 Period : 04/July/16 to 22/September/16 Semester : 7 th Semester Department : Ophthalmology Lecture Lesson Plan Sr No Date Topic Learning objectives
Dr. D. Y. Patil Medical College, Pimpri, Pune - 411 018 Period : 04/July/16 to 22/September/16 Semester : 7 th Semester Department : Ophthalmology Lecture Lesson Plan Sr No Date Topic Learning objectives
Page 1 RED EYES. conjunctivitis keratitis episcleritis / scleritis. Frank Larkin Moorfields Eye Hospital. acute glaucoma anterior uveitis
 The RED EYE and ALLERGIC EYE DISEASE DIAGNOSIS & MANAGEMENT Frank Larkin Moorfields Eye Hospital RED EYES conjunctivitis keratitis episcleritis / scleritis acute glaucoma anterior uveitis post-op. / trauma
The RED EYE and ALLERGIC EYE DISEASE DIAGNOSIS & MANAGEMENT Frank Larkin Moorfields Eye Hospital RED EYES conjunctivitis keratitis episcleritis / scleritis acute glaucoma anterior uveitis post-op. / trauma
Aristotle University Thessaloniki Medical School I. & II. Departments of Ophthalmology 90 DIAGNOSTIC & THERAPEUTIC APPROACHES IN OPHTHALMOLOGY
 Aristotle University Thessaloniki Medical School I. & II. Departments of Ophthalmology 90 DIAGNOSTIC & THERAPEUTIC APPROACHES IN OPHTHALMOLOGY The medical student should be able to... I. Pathophysiology
Aristotle University Thessaloniki Medical School I. & II. Departments of Ophthalmology 90 DIAGNOSTIC & THERAPEUTIC APPROACHES IN OPHTHALMOLOGY The medical student should be able to... I. Pathophysiology
CASE PRESENTATION. DR.Sravani 1 st yr PG Dept of Ophthalmology
 CASE PRESENTATION DR.Sravani 1 st yr PG Dept of Ophthalmology Name : X X X X X Age : 50yrs Sex : male Occupation : Farmer Residence : Mothkur CHIEF COMPLAINTS : - Diminision of vision in Right Eye since
CASE PRESENTATION DR.Sravani 1 st yr PG Dept of Ophthalmology Name : X X X X X Age : 50yrs Sex : male Occupation : Farmer Residence : Mothkur CHIEF COMPLAINTS : - Diminision of vision in Right Eye since
PRECISION PROGRAM. Injection Technique Quick-Reference Guide. Companion booklet for the Video Guide to Injection Technique
 Injection Technique Quick-Reference Guide PRECISION PROGRAM Companion booklet for the Video Guide to Injection Technique Available at www.ozurdexprecisionprogram.com Provides step-by-step directions with
Injection Technique Quick-Reference Guide PRECISION PROGRAM Companion booklet for the Video Guide to Injection Technique Available at www.ozurdexprecisionprogram.com Provides step-by-step directions with
What are some common conditions that affect the cornea?
 What are some common conditions that affect the cornea? Injuries After minor injuries or scratches, the cornea usually heals on its own. Deeper injuries can cause corneal scarring, resulting in a haze
What are some common conditions that affect the cornea? Injuries After minor injuries or scratches, the cornea usually heals on its own. Deeper injuries can cause corneal scarring, resulting in a haze
Ophthalmology. Juliette Stenz, MD
 Ophthalmology Juliette Stenz, MD Required Slide Disclosures NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT Required Slide At the end of this session, students will be able to: 1.
Ophthalmology Juliette Stenz, MD Required Slide Disclosures NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT Required Slide At the end of this session, students will be able to: 1.
JINNAH SINDH MEDICAL UNIVERSITY STUDY GUIDE- OPHTHALMOLOGY YEAR 4,
 INTRODUCTION Pakistan, the 7th most populous country in the world, has an urban population of 38.8% and rural dwellers of 61.2%. The country has faced challenges with vision impairment and blindness as
INTRODUCTION Pakistan, the 7th most populous country in the world, has an urban population of 38.8% and rural dwellers of 61.2%. The country has faced challenges with vision impairment and blindness as
NEW YORK UNIVERSITY SCHOOL OF MEDICINE DEPARTMENT OF OPHTHALMOLOGY EDUCATIONAL OBJECTIVES AND GOALS
 NEW YORK UNIVERSITY SCHOOL OF MEDICINE DEPARTMENT OF OPHTHALMOLOGY EDUCATIONAL OBJECTIVES AND GOALS Revision Date: 6/30/06 Distribution Date: 7/6/06 The Department of Ophthalmology at the NYU Medical Center
NEW YORK UNIVERSITY SCHOOL OF MEDICINE DEPARTMENT OF OPHTHALMOLOGY EDUCATIONAL OBJECTIVES AND GOALS Revision Date: 6/30/06 Distribution Date: 7/6/06 The Department of Ophthalmology at the NYU Medical Center
CENTRAL MERSEY LOCAL OPTICAL COMMITTEE
 CENTRAL MERSEY LOCAL OPTICAL COMMITTEE OPTOMETRIC REFERRAL GUIDELINES The ocular conditions listed in this document are intended to reflect those that might be encountered in optometric practice and this
CENTRAL MERSEY LOCAL OPTICAL COMMITTEE OPTOMETRIC REFERRAL GUIDELINES The ocular conditions listed in this document are intended to reflect those that might be encountered in optometric practice and this
Table of Contents 1 Orbit 3 2 Eyelids 7
 Table of Contents Preface, x List of abbreviations xi Glossary xii Section I Atlas 1 1 Orbit 3 Clinical signs associated with orbital neoplasia 3 Clinical signs associated with orbital cellulitis 3 Enophthalmos
Table of Contents Preface, x List of abbreviations xi Glossary xii Section I Atlas 1 1 Orbit 3 Clinical signs associated with orbital neoplasia 3 Clinical signs associated with orbital cellulitis 3 Enophthalmos
Ocular Trauma. Breaking Down Blunt. Blunt ocular trauma occurs frequently in sporting
 Focus on CME at the University of Saskatchewan Breaking Down Blunt Ocular Trauma By Dan Ash, MD, BA, FRCSC, FACS, FAAO Blunt ocular trauma occurs frequently in sporting activities, as well as in industrial
Focus on CME at the University of Saskatchewan Breaking Down Blunt Ocular Trauma By Dan Ash, MD, BA, FRCSC, FACS, FAAO Blunt ocular trauma occurs frequently in sporting activities, as well as in industrial
EYE ASSESSMENT - ADULT
 For more information or to provide feedback on this or any other decision support tool, email certifiedpractice@crnbc.ca EYE ASSESSMENT - ADULT Nurses with RN First Call Certified Practice designation
For more information or to provide feedback on this or any other decision support tool, email certifiedpractice@crnbc.ca EYE ASSESSMENT - ADULT Nurses with RN First Call Certified Practice designation
HealthHarmonie Limited Minor Eye Conditions Services Guide
 HealthHarmonie Limited Minor Eye Conditions Services Guide 2017 Contents Introduction... 3 Experience, Qualifications and Competencies... 3 Required Equipment... 3 Clinical assessment... 3 Management of
HealthHarmonie Limited Minor Eye Conditions Services Guide 2017 Contents Introduction... 3 Experience, Qualifications and Competencies... 3 Required Equipment... 3 Clinical assessment... 3 Management of
UNDERSTAND MORE ABOUT UVEITIS UVEITIS
 UNDERSTAND MORE ABOUT UVEITIS UVEITIS Uveitis What is uveitis? Uveitis is inflammation of the uvea, the middle layer of your eye. The eye is shaped much like a tennis ball, with three different layers
UNDERSTAND MORE ABOUT UVEITIS UVEITIS Uveitis What is uveitis? Uveitis is inflammation of the uvea, the middle layer of your eye. The eye is shaped much like a tennis ball, with three different layers
Telephone Triage Urgency or Emergency? Mary E. Schmidt, ABOC, CPO
 Telephone Triage Urgency or Emergency? www.eyesystems.info Mary E. Schmidt, ABOC, CPO mary@eyesystems.info Definition of Triage The sorting of patient and allocation of care or treatment according to the
Telephone Triage Urgency or Emergency? www.eyesystems.info Mary E. Schmidt, ABOC, CPO mary@eyesystems.info Definition of Triage The sorting of patient and allocation of care or treatment according to the
Uveitis. Pt Info Brochure. Q: What is Uvea?
 Pt Info Brochure Uveitis Q: What is Uvea? A: Uvea is the middle layer of the eye. It is the most vascular structure of the eye. It provides nutrition to the other parts of the eye. The uvea is made up
Pt Info Brochure Uveitis Q: What is Uvea? A: Uvea is the middle layer of the eye. It is the most vascular structure of the eye. It provides nutrition to the other parts of the eye. The uvea is made up
Eye Emergencies. David Pendergrast Auckland Eye
 Eye Emergencies David Pendergrast Auckland Eye No financial disclosures Ophthalmic Emergencies Patients with ophthalmic symptoms and signs will often present to the GP and these may indicate normal visual
Eye Emergencies David Pendergrast Auckland Eye No financial disclosures Ophthalmic Emergencies Patients with ophthalmic symptoms and signs will often present to the GP and these may indicate normal visual
Orbital and Ocular Adnexal Disorders with Red Eyes
 Orbital and Ocular Adnexal Disorders with Red Eyes Jason Lee Associate Consultant Department of Ophthalmology and Visual Sciences Practical Ophthalmology for the Family Physician 21 Jan 2017 No financial
Orbital and Ocular Adnexal Disorders with Red Eyes Jason Lee Associate Consultant Department of Ophthalmology and Visual Sciences Practical Ophthalmology for the Family Physician 21 Jan 2017 No financial
Common eye emergencies
 Common eye emergencies The acute red eye, sudden visual loss or trauma are the most common eye emergencies. KAVITHA NAIDU, MB ChB, FCOpth Consultant, Department of Ophthalmology, Nelson Mandela School
Common eye emergencies The acute red eye, sudden visual loss or trauma are the most common eye emergencies. KAVITHA NAIDU, MB ChB, FCOpth Consultant, Department of Ophthalmology, Nelson Mandela School
THE CHRONIC GLAUCOMAS
 THE CHRONIC GLAUCOMAS WHAT IS GLAUCOMA? People with glaucoma have lost some of their field of all round vision. It is often the edge or periphery that is lost. That is why the condition can be missed until
THE CHRONIC GLAUCOMAS WHAT IS GLAUCOMA? People with glaucoma have lost some of their field of all round vision. It is often the edge or periphery that is lost. That is why the condition can be missed until
Information for Patients. Retinal Detachment
 Information for Patients Retinal Detachment Manchester Royal Eye Hospital Retinal services Your eye doctor has told you that you have a retinal detachment. This leaflet will help you understand your condition
Information for Patients Retinal Detachment Manchester Royal Eye Hospital Retinal services Your eye doctor has told you that you have a retinal detachment. This leaflet will help you understand your condition
a.superficial (adenoid layer).contain lymphoid tissue.
.contain lymphoid tissue.") Conjunctiva Dr. saifalshamarti Anatomy Microscopic: 1.Epithelium (non keratinized,includes goblet cell). 2.Epithelial basement membrane. 3.Stroma : a.superficial (adenoid layer).contain lymphoid tissue.
Conjunctiva Dr. saifalshamarti Anatomy Microscopic: 1.Epithelium (non keratinized,includes goblet cell). 2.Epithelial basement membrane. 3.Stroma : a.superficial (adenoid layer).contain lymphoid tissue.
Aging & Ophthalmology
 Aging & Ophthalmology Pr Jean-Marie Rakic Dr Denis Malaise January 2018 Major ocular diseases 1. Cataract 2. Age-related macular degeneration 3. Ischemic optic neuropathy 4. Horton arteritis 5. Glaucoma
Aging & Ophthalmology Pr Jean-Marie Rakic Dr Denis Malaise January 2018 Major ocular diseases 1. Cataract 2. Age-related macular degeneration 3. Ischemic optic neuropathy 4. Horton arteritis 5. Glaucoma
Everyday Practice. Eye trauma: Primary care for general physicians
 VOL.. 15, NO.2, 85 2002 Everyday Practice Eye trauma: Primary care for general physicians H. K. TEWARI, ATUL KUMAR, GUNJAN PRAKASH INTRODUCTION The understanding of ocular trauma is important for the primary
VOL.. 15, NO.2, 85 2002 Everyday Practice Eye trauma: Primary care for general physicians H. K. TEWARI, ATUL KUMAR, GUNJAN PRAKASH INTRODUCTION The understanding of ocular trauma is important for the primary
Rafik Girgis. Consultant Ophthalmic Surgeon ( Cataract & Primary Care)
") Rafik Girgis Consultant Ophthalmic Surgeon ( Cataract & Primary Care) Blepharitis Is a very common condition which usually bilateral & symmetrical. The main types are: Anterior, posterior or mixed Complications:
Rafik Girgis Consultant Ophthalmic Surgeon ( Cataract & Primary Care) Blepharitis Is a very common condition which usually bilateral & symmetrical. The main types are: Anterior, posterior or mixed Complications:
Conjunctival Hemorrhage
 IN THE NAME OF GOD Lid Laceration Conjunctival Hemorrhage a) No therapy is necessary b) Usually resolve in 7-12 days. Subconjunctival Hemorrhage Corneal Abrasion Abrasions Many small abrasions can
IN THE NAME OF GOD Lid Laceration Conjunctival Hemorrhage a) No therapy is necessary b) Usually resolve in 7-12 days. Subconjunctival Hemorrhage Corneal Abrasion Abrasions Many small abrasions can
For details on measurement and recording of visual acuity, refer to Annex 1. VISION INTERPRETING RESULTS ABSTRACT
 management update on functional decline in older adults 2012 Unit No. 5 VISION Dr Au Eong Kah Guan, Ms Yulianti, Ms Fifiana ABSTRACT Among Singaporean adults of Chinese origin aged 40 to 79 years old,
management update on functional decline in older adults 2012 Unit No. 5 VISION Dr Au Eong Kah Guan, Ms Yulianti, Ms Fifiana ABSTRACT Among Singaporean adults of Chinese origin aged 40 to 79 years old,
Ocular Anatomy for the Paraoptometric
 Ocular Anatomy for the Paraoptometric Minnesota Optometric Association Paraoptometric CE Friday September 30, 2016 Lindsay A. Sicks, OD, FAAO Assistant Professor, Illinois College of Optometry lsicks@ico.edu
Ocular Anatomy for the Paraoptometric Minnesota Optometric Association Paraoptometric CE Friday September 30, 2016 Lindsay A. Sicks, OD, FAAO Assistant Professor, Illinois College of Optometry lsicks@ico.edu
Ophthalmology for Primary Care Providers
 Ophthalmology for Primary Care Providers Bob Avery, MD, PhD Ophthalmology/Surgery University of New Mexico School of Medicine bavery@salud.unm.edu Preview How the eye works Basic eye exam The red eye Acute
Ophthalmology for Primary Care Providers Bob Avery, MD, PhD Ophthalmology/Surgery University of New Mexico School of Medicine bavery@salud.unm.edu Preview How the eye works Basic eye exam The red eye Acute