DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
|
|
|
- Sabrina Fleming
- 5 years ago
- Views:
Transcription

1 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this photo and/or video. If you don t want your photo taken, please let us know. Thank you! ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.

2 Approach to dizziness in older adults MOHAMED ELNAGGAR, MD GERIATRIC MEDICINE FELLOW, UNIVERSITY OF NEVADA, RENO FEBRUARY 21, 2018
3 Objectives How to define and describe dizziness. Discuss different categories of dizziness. Demonstrate how to approach a patient with dizziness. Review most common causes of each category and its treatment.

4 Introduction Dizziness in general is a false sense of motion One of the most common symptoms of older adults Its prevalence reaches 30% beyond 60 years of age, while rising to 50% beyond 85 years. Dizziness is more common in women than in men. Dizziness in the elderly is a strong predictor of falls. One of the strongest contributors to disability burden after age 65.
5 Introduction Manifest differently as more of non-specific dizziness and instability than younger patients, making diagnosis more complex. Associated with increased fear of falling, functional disability and depressive symptoms. The most common causes of acute dizziness are acute vestibular neuritis, cerebrovascular ischemia and cardiovascular disorders resulting in hypotension.
6 Pathophysiology of Balance 1-The brain receives sensory information from three sources: A-Vestibular part of the inner ear B- Vision. C- Proprioceptors of the muscles, joints, and tendons. 2-The brain integrates these sensory information and sends motor orders to two groups of muscles: The extra-ocular muscles to keep the eyes stable and The spinal muscles to keep the limbs and trunk stable. Age-related degeneration of different neural structures affects balance

7 Main categories of Dizziness Patients sometimes have difficulty describing it >> Physicians should focus more on timing and triggers! Mixed dizziness: results from combination of two or more of the above and is the most common type of dizziness reported by older adults. (Combination of vestibular, CNS, visual or proprioceptive system, anemia, H.F, DM and hypothyroidism) therefore it requires multifactorial assessment and intervention.

8 Case based question GRS 9th edition An 81 year-old woman comes to the office, because she has episodes of dizziness in which the room spins intensely when she tries to get out of bed. The episodes last up to 1 minute. The first few times they were associated with intense nausea. She feels better when she doesn t move her head. O/E: External auditory canals and T.M appear normal. Results of Weber and Rinne tests are normal. What other questions you shall ask and physical exam you can do?
9 History alone can reveal diagnosis in ¾ of cases How patients describe it Onset (sudden or slow) Course (episodic or continuous) Associated symptoms (CNS symptoms, hearing symptoms) Associated nausea/vomiting Hearing loss or tinnitus Risk factors for cardiovascular disease Duration (seconds, minutes or hours) Drug history Severity Past history medical problems Recurrence (Meniere, BPPV) Recent viral illness, fever, systemic symptoms Family history New medications, OTC meds Impact on life Provoking, aggravating factors Triggering factors



10 History taking Duration Meniere's Disease, Migraine Seconds BPPV Hours BPPV Minutes Perilymphatic fistula Migraine, early Vestibular Neuritis Days TIA, Meniere's >Hour Perilymphatic fistula Acoustic Neuroma Weeks MS, Stroke Psychogenic


11 TITRATE approach for Dizziness AAFP 2017 The approach to management in older adults has similarities to that in younger patients

12 Physical examination PHYSICAL EXAMINATION: Vital Signs: -Blood pressure (sitting & lying) - pulse CNS exam : -Cranial nerves - gait - Romberg sign - proprioception & vibration. Head & Neck: -Auscultate for carotid bruits, Nystagmus Heart : - Auscultation for A.S. Ear exam: - Rinne test -Weber s test - TM - Valsalva
13 Physical examination Timed Up and Go test for gait and balance problems. Dix-Hallpike maneuver. HINTS exam: (head impulse, nystagmus, test of skew) examination can help distinguish a possible stroke (central cause) from acute vestibular syndrome (peripheral cause).

14 Acute vestibular syndrome Acute, continuous vertigo lasting days to weeks with nausea or vomiting with nystagmus even if the patient gets worse with changes in position 2 forms: Post-Exposure: anti-epileptic drugs, etc, Spontaneous: vestibular neuritis, stroke, MS HINTS required! ruling out stroke is critical, particularly in the elderly The HINTS assessment protocol can be performed at the bedside, with high sensitivity and specificity to diagnose stroke in an acute vestibular syndrome with better sensitivity than early (MRI).

15 Acute vestibular syndrome

16 Missed Stroke and Dizziness


17 Peripheral causes of Dizziness Peripheral causes of dizziness arise from abnormalities in the peripheral vestibular system: semicircular canals, the saccule, the utricle, and the vestibular nerve. Common peripheral causes of dizziness/vertigo include: - BPPV - Vestibular neuritis (i.e., vestibular neuronitis) - Meniere s disease 7% 93%
18 Benign Paroxysmal Positional Vertigo Benign Paroxysmal Positional Vertigo (Most common!) - Common between 50 and 70 years. - Etiology: -Head trauma -Intoxication alcohol, Canelithiasis - No obvious cause is found in 50% to 70% of older patients - Precipitated by movement or position change in the head or body - Dx: Dix-Hallpike maneuver - Contraindication: Severe carotid stenosis, unstable heart disease, severe neck disease
19 Treatment of BPPV Treatment of BPPV consists of a canalith repositioning procedure such as the Epley maneuver, LI maneuvers which repositions the canalith from the semicircular canal into the vestibule. The success rate is approximately 70% on the first attempt, and nearly 100% on successive maneuvers. Home treatment with BrandtDaroff exercises (
20 Treatment of BPPV If there is no improvement with repeated repositioning maneuvers, or if atypical or ongoing nystagmus with nausea is present, another cause should be considered. Pharmacologic treatment :(Meclizine (Antivert), 25 to 50 mg orally every four to six hours) has no role in the treatment of BPPV. Vestibular suppressant medications should be avoided Surgical treatment: Post. Canal occlusion in refractory BPPV.
21 Vestibular neuritis Vestibular neuritis: Cause unknown, viral Clinical features: - Sudden prolonged attack of vertigo Nausea, vomiting, disequilibrium and apprehension Positional - Tinnitus and a sensation of fullness in the ear Audiology tests are normal No neurological signs Usually resolves spontaneously but may recur
22 Treatment of Vestibular neuritis - Vestibular neuritis is treated with medications and vestibular rehabilitation. - Vertigo and associated nausea or vomiting can be treated with a combination of antihistamine and antiemetic. - Systemic corticosteroids have been recommended as a treatment for vestibular neuritis. Methylprednisolone (Depo-Medrol), initially 100 mg orally daily then tapered to 10 mg orally daily over three weeks - Antiviral medications are ineffective.
23 Meniere's disease Meniere s disease: Pathophysiology :The underlying pathology is excess endo-lymphatic fluid pressure leading to inner ear dysfunction; however, the exact cause is unknown. Any age, it is more common between 20 and 60 years Bouts of intense vertigo minutes to hours Fullness or pressure in the ear Tinnitus Fluctuating unilateral hearing loss (SNHL low more than high frequency)
24 Treatment of Meniere's disease 1st line Treatment of Meniere s disease: - limiting dietary salt intake to less than 2,000 mg per day - reducing caffeine intake - limiting alcohol to one drink per day 2nd line treatment: - Daily thiazide diuretic hydrochlorothiazide/ triamterene [Dyazide]. - Intratympanic injections of Dexamethasone and gentamicin can improve vertigo.

25 Vestibular Suppressant Meds Effective in vertigo but generally don t provide benefit in chronic dizziness or disequilibrium Vestibular suppressants should be tapered quickly >> inhibitory effect on vestibular and central compensation
 - MRI brain (Diagnostic) - Treatment:")
26 Other Peripheral causes of Dizziness Acoustic neuroma: - Slow growing tumor - Patients often experience mild vertigo or no vertiginous symptoms at all - Unilateral tinnitus - Unilateral SNHL (high frequencies) - MRI brain (Diagnostic) - Treatment: Surgery

27 Other Peripheral causes of Dizziness Peripheral neuropathy: - DM, Vit B12 def., Idiopathic, Cervical spine DJD - Decreased vibration and position sense, gait abnormality - Signs of radiculopathy or mylopathy - Cervical or vestibular rehabilitation, cervical collar, surgery if needed

28 D.D of central causes of Dizziness 25% Pathology at the following sites: - The vestibular nuclei - Cerebellum - Brainstem - Spinal cord - Potentially deadly central causes of acute vestibular syndrome may mimic a more benign peripheral disorder, and a stroke may present with no focal neurologic signs.
29 Vertebrobasilar ischemia Diagnosis usually relies on a history of brainstem symptoms, such as diplopia, dysarthria, weakness, Gait or truncal ataxia, hypertonia and hyperreflexia. clumsiness of the limbs. MRI/MRA may be helpful - Treatment includes antiplatelet therapy and reduction of risk factors for cerebrovascular disease. - Warfarin (Coumadin) has been used in cases of significant vertebral or basilar artery stenos
30 Cerebellar infarction/hemorrhage Sudden intense persistent vertigo with nausea and vomiting. Pronounced gait abnormalities Pt falls toward the side of the lesion Typically older pts (>60 y/o) with CV risk factors
31 Chronic dizziness Dizziness for more than 1-2 months More common in older adults, has a larger variety of contributing causes. Risk factors: Angina, MI, stroke, arthritis, diabetes, syncope, anxiety, depressive symptoms, impaired hearing, use of medications in several classes, > 5 medications. Given the multifactorial etiology >> Geriatric syndrome. Therefore, multifaceted approach to interventions
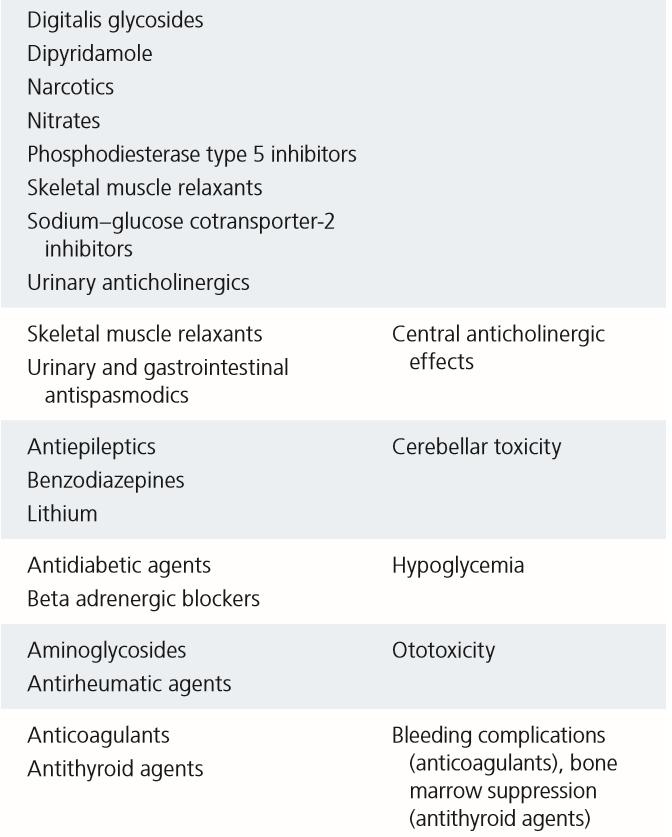
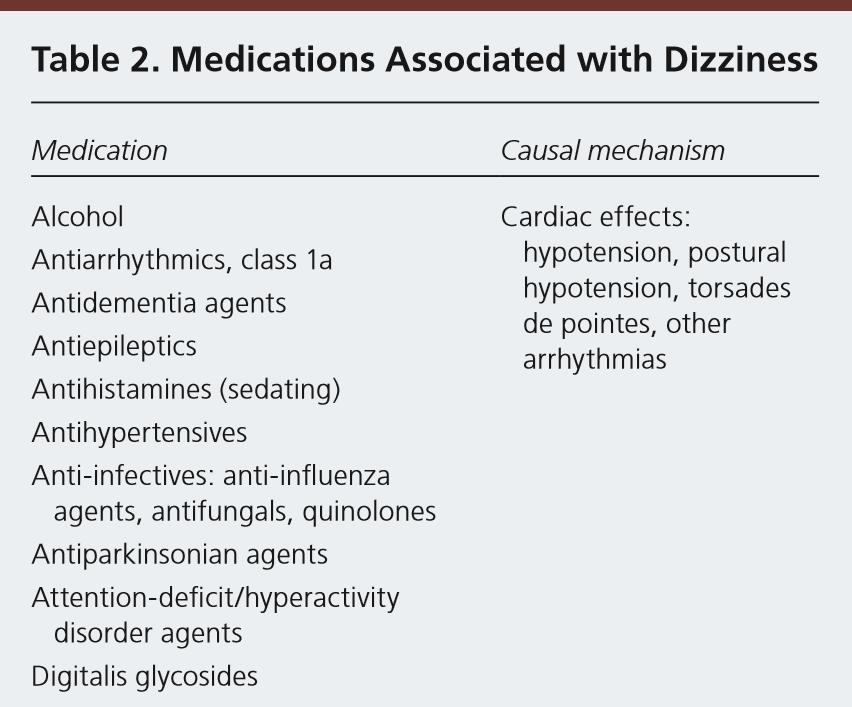

32 Medications associated with Dizziness
33 Laboratory evaluation Most patients presenting with dizziness DON T require laboratory testing. Laboratory tests includes hematocrit, glucose, electrolytes, BUN, Vitamin B12, folic acid and TSH should be performed on all patient with chronic dizziness.

34 When to order imaging studies Neurological Risk factors for cerebrovascular disease. Progressive MRI sign and symptoms. unilateral hearing loss. more appropriate than CT.
35 When to order imaging studies Expensive tests like electronystagmography, rotational chair testing, postugraphy and not often needed in the evaluation of dizziness. ECG: If cardiac cause is suspected, Holter and event monitor only if suspicious of arrhythmia is strong. Audiometry: in Tinnitus and hearing loss to differentiate between Meniere disease and Acoustic neuroma.

36 Case based question A 67-Year-old woman c/o dizziness and generalized weakness. She recently had a prosthetic heart valve placed. She describes her dizziness as gradually over the past few days, at a bearable, constant level of intensity. She reports no nausea, vomiting, or ringing in her ears. O/E: There is a vertical nystagmus. Dix-Hallpike test is inconclusive. Which one of the following is the most likely diagnosis: - Vestibular neuritis - Central vertigo probably due to stroke - Meniere s disease - BPPV - Perilymph fistula

37 Case based question An 85-year-old woman comes to the office because she has had a recent episode of dizziness in which she senses the room spinning around her, feels her right ear is blocked, and hears a roaring sensation. The symptoms improve gradually until she returns to baseline over few hours. She has no associated headaches. History includes diabetes and hypertension. Which one of the following is the most likely diagnosis: - BPPV - Acute labrynthitis - Arrhythmia - Meniere's disease - Migraine-associated vertigo.
38 Take home message TITRATE approach + History (important) Dizziness.. Vertigo/Presyncope / disequilibrium / Lightheadedness Seconds = Dix The longer symptoms >> Central cause >> urgent treatment Laboratory testing and imaging are not required and are usually not helpful. VRT includes different exercises such as vestibule-ocular reflex adaptation exercises and habituation exercises Days = HINTS

39 Take home message
40 References Am Fam Physician. 2017;95(3): Copyright 2017 American Academy of Family Physicians. ECHO Dizziness in Older Adults - Final PPT Elnaggar.pptx Geriatrics Review Syllabus 9th Edition.


41

42
Sasan Dabiri, MD, Assistant Professor
 Sasan Dabiri, MD, Assistant Professor Department of Otorhinolaryngology Head & Neck Surgery Amir A lam hospital Tehran University of Medical Sciences October 2015 Outlines Anatomy of Vestibular System
Sasan Dabiri, MD, Assistant Professor Department of Otorhinolaryngology Head & Neck Surgery Amir A lam hospital Tehran University of Medical Sciences October 2015 Outlines Anatomy of Vestibular System
What could be reffered to as dizziness by the patient?
 What could be reffered to as dizziness by the patient? Rotational vertigo Sense of instability Ataxia of gait Disturbance of vision Loss of contact with surroundings Nausea Loss of memory Loss of confidence
What could be reffered to as dizziness by the patient? Rotational vertigo Sense of instability Ataxia of gait Disturbance of vision Loss of contact with surroundings Nausea Loss of memory Loss of confidence
Vertigo. Tunde Magyar MD, PhD
 Vertigo Tunde Magyar MD, PhD What could be reffered to as dizziness by the patient? Rotational vertigo Sense of instability Ataxia of gait Disturbance of vision Loss of contact with surroundings Nausea
Vertigo Tunde Magyar MD, PhD What could be reffered to as dizziness by the patient? Rotational vertigo Sense of instability Ataxia of gait Disturbance of vision Loss of contact with surroundings Nausea
Dizziness: Neurological Aspect
 Dizziness: Neurological Aspect..! E-mail: somtia@kku.ac.th http://epilepsy.kku.ac.th Features between peripheral and central vertigo 1. Peripheral Central 2.! " # $ " Imbalance Mild-moderate Severe 3.!
Dizziness: Neurological Aspect..! E-mail: somtia@kku.ac.th http://epilepsy.kku.ac.th Features between peripheral and central vertigo 1. Peripheral Central 2.! " # $ " Imbalance Mild-moderate Severe 3.!
CITY & HACKNEY PATHFINDER CLINICAL COMMISSIONING GROUP. Vertigo. (1) Vertigo. (4) Provisional Diagnosis. (5) Investigations. lasting days or weeks
 Vertigo. (4) Provisional Diagnosis. (5) Investigations. lasting days or weeks") Authors: Dr Lucy O'Rouke and Mr N Eynon-Lewis Review date: January 2017 Vertigo (1) Vertigo (2) History (3) Examination (4) Provisional Diagnosis (5) Investigations (6) Medical Cause (7) Psychiatric Cause
Authors: Dr Lucy O'Rouke and Mr N Eynon-Lewis Review date: January 2017 Vertigo (1) Vertigo (2) History (3) Examination (4) Provisional Diagnosis (5) Investigations (6) Medical Cause (7) Psychiatric Cause
Vertigo. David Clark, DO Oregon Neurology Associates Springfield, OR
 Vertigo David Clark, DO Oregon Neurology Associates Springfield, OR 44F vertigo, nausea & vomiting Unidirectional Nystagmus 44F vertigo, nausea & vomiting Impaired VOR Gain to the right Vertigo History
Vertigo David Clark, DO Oregon Neurology Associates Springfield, OR 44F vertigo, nausea & vomiting Unidirectional Nystagmus 44F vertigo, nausea & vomiting Impaired VOR Gain to the right Vertigo History
Evaluation of the Dizzy Patient
 Evaluation of the Dizzy Patient S. Andrew Josephson, MD Department of Neurology University of California San Francisco October 1, 2007 Who Sees Dizzy Patients? ED physicians Internists Neurologists ENT
Evaluation of the Dizzy Patient S. Andrew Josephson, MD Department of Neurology University of California San Francisco October 1, 2007 Who Sees Dizzy Patients? ED physicians Internists Neurologists ENT
Acoustic neuroma s/p removal BPPV (Crystals)- 50% of people over 65 y/ o with dizziness will have this as main reason for dizziness
- 50% of people over 65 y/ o with dizziness will have this as main reason for dizziness") Dizziness and the Heart Mended Hearts Inservice Karen Hansen, PT, DPT, Cert Vestibular Rehab, CEAS Tennessee Therapy & Balance Center, LLC July 21, 2016 Balance We maintain balance with input from our
Dizziness and the Heart Mended Hearts Inservice Karen Hansen, PT, DPT, Cert Vestibular Rehab, CEAS Tennessee Therapy & Balance Center, LLC July 21, 2016 Balance We maintain balance with input from our
Because dizziness is an imprecise term, a major role of the clinician is to sort patients out into categories
 Dizziness and Imbalance Timothy C. Hain, MD Clinical Professor of Neurology, Otolaryngology, Physical Therapy Chicago Dizziness and Hearing 645 N. Michigan, Suite 410 312-274-0197 Lecture Goals 1. What
Dizziness and Imbalance Timothy C. Hain, MD Clinical Professor of Neurology, Otolaryngology, Physical Therapy Chicago Dizziness and Hearing 645 N. Michigan, Suite 410 312-274-0197 Lecture Goals 1. What
Vertigo: A practical approach to diagnosis and treatment. John Waterston
 Vertigo: A practical approach to diagnosis and treatment John Waterston Background. Vertigo is a symptom that has diverse causes. The diagnosis may remain elusive even after exhaustive clinical enquiry
Vertigo: A practical approach to diagnosis and treatment John Waterston Background. Vertigo is a symptom that has diverse causes. The diagnosis may remain elusive even after exhaustive clinical enquiry
Vertigo. Definition Important history questions Examination Common vertigo cases and management Summary
 Vertigo Vertigo Definition Important history questions Examination Common vertigo cases and management Summary Cases 1) 46 year old man presents two weeks after knocking his head with recurrent episodes
Vertigo Vertigo Definition Important history questions Examination Common vertigo cases and management Summary Cases 1) 46 year old man presents two weeks after knocking his head with recurrent episodes
An Introduction to Dizziness and Vertigo
 An Introduction to Dizziness and Vertigo Tamara Mijovic MD CM FRCSC Clinical Assistant Professor Department of Otolaryngology Head and Neck Surgery Otology, Neurotology & Skull Base Surgery McGill University
An Introduction to Dizziness and Vertigo Tamara Mijovic MD CM FRCSC Clinical Assistant Professor Department of Otolaryngology Head and Neck Surgery Otology, Neurotology & Skull Base Surgery McGill University
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 04/26/2014 Radiology Quiz of the Week # 108 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 04/26/2014 Radiology Quiz of the Week # 108 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Vertigo. Definition. Causes. (Dizziness) Benign Paroxysmal Positional Vertigo (BPPV) Labyrinthitis. by Karen Schroeder, MS, RD
 Benign Paroxysmal Positional Vertigo (BPPV) Labyrinthitis. by Karen Schroeder, MS, RD") Vertigo (Dizziness) by Karen Schroeder, MS, RD En Español (Spanish Version) Definition Vertigo is a feeling of spinning or whirling when you are not moving. It can also be an exaggerated feeling of motion
Vertigo (Dizziness) by Karen Schroeder, MS, RD En Español (Spanish Version) Definition Vertigo is a feeling of spinning or whirling when you are not moving. It can also be an exaggerated feeling of motion
OBJECTIVES TYPES OF DIZZINESS TYPES OF DIZZINESS. Type III Disequilibrium. Classifying Common Position Sense Disturbances
 OBJECTIVES Define four major types of dizziness Emphasizing vertigo Describe pathophysiology of dizziness Emphasizing BPPV Review how to cure BPPV How do you know where you are in 3-dimensional space?
OBJECTIVES Define four major types of dizziness Emphasizing vertigo Describe pathophysiology of dizziness Emphasizing BPPV Review how to cure BPPV How do you know where you are in 3-dimensional space?
Workshop: The Assessment of Patients with Dizziness and Vertigo
 Workshop: The Assessment of Patients with Dizziness and Vertigo Tamara Mijovic MD CM FRCSC Clinical Assistant Professor Department of Otolaryngology Head and Neck Surgery Otology, Neurotology & Skull Base
Workshop: The Assessment of Patients with Dizziness and Vertigo Tamara Mijovic MD CM FRCSC Clinical Assistant Professor Department of Otolaryngology Head and Neck Surgery Otology, Neurotology & Skull Base
The Big 3 of Vertigo
 They feel it, you see it, few know it: Common vertigo conditions seen, but rarely diagnosed Peter Johns MD, FRCPC University of Ottawa pjohns@toh.ca Twitter @peterjohns84 The Big 3 of Vertigo BPPV Vestibular
They feel it, you see it, few know it: Common vertigo conditions seen, but rarely diagnosed Peter Johns MD, FRCPC University of Ottawa pjohns@toh.ca Twitter @peterjohns84 The Big 3 of Vertigo BPPV Vestibular
EMU 2017 DIZZINESS AND VERTIGO Walter Himmel MD
 EMU 2017 DIZZINESS AND VERTIGO Walter Himmel MD There is only one essential challenge in the world of dizziness and vertigo: Don t miss a posterior circulation stroke (vertebral/basilar artery) or TIA.
EMU 2017 DIZZINESS AND VERTIGO Walter Himmel MD There is only one essential challenge in the world of dizziness and vertigo: Don t miss a posterior circulation stroke (vertebral/basilar artery) or TIA.
Differential Diagnosis: Vestibular Pathology. Causes of Dizziness. Benign Paroxysmal Positional Vertigo
 Differential Diagnosis: Vestibular Learning objective: The participant will identify the pathologies associated with complaints of imbalance and dizziness Anne K Galgon PT, PhD, NCS Vestibular and Related
Differential Diagnosis: Vestibular Learning objective: The participant will identify the pathologies associated with complaints of imbalance and dizziness Anne K Galgon PT, PhD, NCS Vestibular and Related
Acute Vestibular Syndrome (AVS) 12/5/2017
 12/5/2017") Sharon Hartman Polensek, MD, PhD Dept of Neurology, Emory University Atlanta VA Medical Center DIAGNOSTIC GROUPS FOR PATIENTS PRESENTING WITH DIZZINESS TO EMERGENCY DEPARTMENTS Infectious 2.9% Genitourinary
Sharon Hartman Polensek, MD, PhD Dept of Neurology, Emory University Atlanta VA Medical Center DIAGNOSTIC GROUPS FOR PATIENTS PRESENTING WITH DIZZINESS TO EMERGENCY DEPARTMENTS Infectious 2.9% Genitourinary
VERTIGO. Tuesday 20 th February 2018 Dr Rukhsana Hussain. Disclaimers apply:
 VERTIGO Tuesday 20 th February 2018 Dr Rukhsana Hussain WHAT IS VERTIGO? 4 Vertigo is defined as an illusory sensation of motion of either the self or the surroundings in the absence of true motion. Explaining
VERTIGO Tuesday 20 th February 2018 Dr Rukhsana Hussain WHAT IS VERTIGO? 4 Vertigo is defined as an illusory sensation of motion of either the self or the surroundings in the absence of true motion. Explaining
Chapter 19 Dizziness and Vertigo
 Chapter 19 Dizziness and Vertigo Episode overview: 1) Compare characteristics of peripheral and central vertigo 2) What are risk factors for central causes of vertigo? 3) List 4 vestibulotoxic drugs. 4)
Chapter 19 Dizziness and Vertigo Episode overview: 1) Compare characteristics of peripheral and central vertigo 2) What are risk factors for central causes of vertigo? 3) List 4 vestibulotoxic drugs. 4)
I m dizzy-what can I expect at my doctor visit? Dennis M. Moore, M.D. Lutheral General
 I m dizzy-what can I expect at my doctor visit? Dennis M. Moore, M.D. Lutheral General Dizziness and Balance is a broad area encompassing multiple fields: primary care (internal medicine, pediatrics),
I m dizzy-what can I expect at my doctor visit? Dennis M. Moore, M.D. Lutheral General Dizziness and Balance is a broad area encompassing multiple fields: primary care (internal medicine, pediatrics),
Dizziness Cases. Martin A. Samuels Chair, Department of Neurology Brigham and Women s Hospital Boston
 Dizziness Cases Martin A. Samuels Chair, Department of Neurology Brigham and Women s Hospital Boston Basic Principles Take an open ended history Know the synonyms for dizziness A patient can have more
Dizziness Cases Martin A. Samuels Chair, Department of Neurology Brigham and Women s Hospital Boston Basic Principles Take an open ended history Know the synonyms for dizziness A patient can have more
Dominic J Mort 23/03/17 Spire Bushey Hospital
 Dominic J Mort 23/03/17 Spire Bushey Hospital Dizziness Good grief! Hx: Pre-syncope Dizziness As if you might faint? Vertigo Mostly about this As if on a merry-go-round? Non-rotational commoner than spinning
Dominic J Mort 23/03/17 Spire Bushey Hospital Dizziness Good grief! Hx: Pre-syncope Dizziness As if you might faint? Vertigo Mostly about this As if on a merry-go-round? Non-rotational commoner than spinning
what is the permanent impact of loss of the vestibular sense? for balance, vision and spatial orientation)
") what is the permanent impact of loss of the vestibular sense? for balance, vision and spatial orientation) loss of speed - poor dynamic vision (daily life) - fear to fall and falls loss of automatisation
what is the permanent impact of loss of the vestibular sense? for balance, vision and spatial orientation) loss of speed - poor dynamic vision (daily life) - fear to fall and falls loss of automatisation
2/8/2017 WHERE ARE WE? East Amherst East Aurora Hamburg West Seneca Williamsville Boulevard
 2/8/2017 WHERE ARE WE? East Amherst East Aurora Hamburg West Seneca Williamsville Boulevard 1 2/8/2017 MY GOAL TODAY. 1. Provide a quick overview on falls 2. How our balance systems work 3. What treatments
2/8/2017 WHERE ARE WE? East Amherst East Aurora Hamburg West Seneca Williamsville Boulevard 1 2/8/2017 MY GOAL TODAY. 1. Provide a quick overview on falls 2. How our balance systems work 3. What treatments
Inner Ear Disorders. Information for patients and families
 Inner Ear Disorders Information for patients and families Read this booklet to learn about: What are inner ear disorders Symptoms Tests you may need Treatment options Please visit the UHN Patient Education
Inner Ear Disorders Information for patients and families Read this booklet to learn about: What are inner ear disorders Symptoms Tests you may need Treatment options Please visit the UHN Patient Education
Physical Therapy Examination of the Acutely Vertiginous Patient. Objectives. Prevalence/Incidence of Dizziness 3/20/2018
 Physical Therapy Examination of the Acutely Vertiginous Patient Andrew Wagner, PT, DPT, NCS Jennifer Williams, PT, DPT, NCS April 13, 2018 Objectives The learner will integrate basic examination principles
Physical Therapy Examination of the Acutely Vertiginous Patient Andrew Wagner, PT, DPT, NCS Jennifer Williams, PT, DPT, NCS April 13, 2018 Objectives The learner will integrate basic examination principles
Control of eye movement
 Control of eye movement Third Nerve Palsy Eye down and out Trochlear Nerve Palsy Note: Right eye Instead of intorsion and depression action of superior oblique See extorsion and elevation Observe how
Control of eye movement Third Nerve Palsy Eye down and out Trochlear Nerve Palsy Note: Right eye Instead of intorsion and depression action of superior oblique See extorsion and elevation Observe how
Benign Paroxysmal Positional Vertigo
 Benign Paroxysmal Positional Vertigo Information for patients and families Read this booklet to learn about: What Benign Paroxysmal Positional Vertigo (BPPV) is Symptoms How your doctor will diagnose it
Benign Paroxysmal Positional Vertigo Information for patients and families Read this booklet to learn about: What Benign Paroxysmal Positional Vertigo (BPPV) is Symptoms How your doctor will diagnose it
Vestibular System. Dian Yu, class of 2016
 Vestibular System Dian Yu, class of 2016 Objectives 1. Describe the functions of the vestibular system: What is it? How do you stimulate it? What are the consequences of stimulation? 2. Describe the vestibular
Vestibular System Dian Yu, class of 2016 Objectives 1. Describe the functions of the vestibular system: What is it? How do you stimulate it? What are the consequences of stimulation? 2. Describe the vestibular
Otologic (Ear) Dizziness Fistula SCD Bilateral. Other. Neuritis BPPV. Menieres
 Dizziness Fistula SCD Bilateral. Other. Neuritis BPPV. Menieres") Otologic Dizziness (Dizziness from Ear) Ear Structures of importance Timothy C. Hain, MD Northwestern University, Chicago t-hain@northwestern.edu The ear is an inertial navigation device Semicircular Canals
Otologic Dizziness (Dizziness from Ear) Ear Structures of importance Timothy C. Hain, MD Northwestern University, Chicago t-hain@northwestern.edu The ear is an inertial navigation device Semicircular Canals
Vestibular Differential Diagnosis
 Vestibular Differential Diagnosis P R E S E N T E D B Y : S H A R I K I C K E R, P T, M P T C E R T I F I C A T E I N V E S T I B U L A R R E H A B I L I T A T I O N 2 0 1 7 L A C E Y H A L E, P T, D P
Vestibular Differential Diagnosis P R E S E N T E D B Y : S H A R I K I C K E R, P T, M P T C E R T I F I C A T E I N V E S T I B U L A R R E H A B I L I T A T I O N 2 0 1 7 L A C E Y H A L E, P T, D P
Benign Paroxysmal Positional Vertigo (BPPV) Structures of importance. The ear is an inertial navigation device. Vestibular Reflexes
 Structures of importance. The ear is an inertial navigation device. Vestibular Reflexes") Otologic Dizziness (Dizziness from Ear) Structures of importance Timothy C. Hain, MD Northwestern University, Chicago t-hain@northwestern.edu The ear is an inertial navigation device Semicircular Canals
Otologic Dizziness (Dizziness from Ear) Structures of importance Timothy C. Hain, MD Northwestern University, Chicago t-hain@northwestern.edu The ear is an inertial navigation device Semicircular Canals
Predictors of Protracted Recovery
 CONCUSSION MANAGEMENT SPECIALIST ON LINE CURRICULUM Protracted Recovery and Clinical Rehabilitation All rights reserved. Sports Medicine Concepts Concussion Management Specialist Program 1 Predictors of
CONCUSSION MANAGEMENT SPECIALIST ON LINE CURRICULUM Protracted Recovery and Clinical Rehabilitation All rights reserved. Sports Medicine Concepts Concussion Management Specialist Program 1 Predictors of
THE STATS KEEPING YOUR BALANCE THE PROFESSIONALS 2/23/2018 THE STATS QUALITY OF LIFE QUALITY OF LIFE - FALLS
 KEEPING YOUR BALANCE EVAL & MANAGEMENT OF INNER EAR BALANCE DISORDERS Dr. Lily V. Hughes, Audiologist Fairbanks Hearing & Balance Center at the ENT Clinic THE STATS THE STATS QUALITY OF LIFE Vestibular
KEEPING YOUR BALANCE EVAL & MANAGEMENT OF INNER EAR BALANCE DISORDERS Dr. Lily V. Hughes, Audiologist Fairbanks Hearing & Balance Center at the ENT Clinic THE STATS THE STATS QUALITY OF LIFE Vestibular
VESTIBULAR SYSTEM. Deficits cause: Vertigo. Falling Tilting Nystagmus Nausea, vomiting
 VESTIBULAR SYSTEM Objectives: Understand the functions of the vestibular system: What is it? How do you stimulate it? What are the consequences of stimulation? Describe the vestibular apparatus, the 2
VESTIBULAR SYSTEM Objectives: Understand the functions of the vestibular system: What is it? How do you stimulate it? What are the consequences of stimulation? Describe the vestibular apparatus, the 2
Dizziness and Vertigo: A Step wise Approach to Evaluation and Management
 Dizziness and Vertigo: A Step wise Approach to Evaluation and Management Jennifer Wipperman, MD, MPH Via Christi Family Medicine Residency University of Kansas School of Medicine Wichita 1 Speaker Disclosure
Dizziness and Vertigo: A Step wise Approach to Evaluation and Management Jennifer Wipperman, MD, MPH Via Christi Family Medicine Residency University of Kansas School of Medicine Wichita 1 Speaker Disclosure
Chapter 12 Dizziness and Vertigo
 Chapter 12 Dizziness and Vertigo Jonathan S. Olshaker PERSPECTIVE An estimated 7.5 million patients with dizziness are seen each year in ambulatory care settings. It is one of the most common principal
Chapter 12 Dizziness and Vertigo Jonathan S. Olshaker PERSPECTIVE An estimated 7.5 million patients with dizziness are seen each year in ambulatory care settings. It is one of the most common principal
Dizziness, Vertigo, and Syncope: Assessment and treatment
 Dizziness, Vertigo, and Syncope: Assessment and treatment Sally K. Miller, PhD, APRN FNP-BC, AGACNP-BC, AGPCNP-BC Associate Professor University of Nevada Las Vegas School of Nursing Nurse Practitioner
Dizziness, Vertigo, and Syncope: Assessment and treatment Sally K. Miller, PhD, APRN FNP-BC, AGACNP-BC, AGPCNP-BC Associate Professor University of Nevada Las Vegas School of Nursing Nurse Practitioner
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: vestibular_function_testing 5/2017 N/A 10/2017 5/2017 Description of Procedure or Service Dizziness, vertigo,
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: vestibular_function_testing 5/2017 N/A 10/2017 5/2017 Description of Procedure or Service Dizziness, vertigo,
DIZZINESS & VERTIGO A MULTIDISCIPLINARY APPROACH
 DIZZINESS & VERTIGO A MULTIDISCIPLINARY APPROACH Dr DOSH SANDOORAM MB ChB, MD, FRCS Consultant ENT Surgeon, City Clinic Group Labyrinthine disturbance may make one feel like the end of the world has arrived...
DIZZINESS & VERTIGO A MULTIDISCIPLINARY APPROACH Dr DOSH SANDOORAM MB ChB, MD, FRCS Consultant ENT Surgeon, City Clinic Group Labyrinthine disturbance may make one feel like the end of the world has arrived...
International Journal of Medical and Exercise Science (Multidisciplinary, Peer Reviewed and Indexed Journal)
") ORIGINAL ARTICLE International Journal of Medical and Exercise Science (Multidisciplinary, Peer Reviewed and Indexed Journal) PHYSICAL THERAPY MANAGEMENT IN PATIENTS WITH CERVICOGENIC DIZZINESS-A CASE
ORIGINAL ARTICLE International Journal of Medical and Exercise Science (Multidisciplinary, Peer Reviewed and Indexed Journal) PHYSICAL THERAPY MANAGEMENT IN PATIENTS WITH CERVICOGENIC DIZZINESS-A CASE
UNDERSTANDING VERTIGO
 Backgrounder UNDERSTANDING VERTIGO Vertigo is a false sensation of movement, either of one s self or one s surroundings. It may exist as an isolated symptom or it may be associated with other conditions
Backgrounder UNDERSTANDING VERTIGO Vertigo is a false sensation of movement, either of one s self or one s surroundings. It may exist as an isolated symptom or it may be associated with other conditions
BPPV and Pitfalls in its Management. Reza Golrokhian Sani MD, Otolaryngologist- Head & Neck Surgeon Otologist & Neurotologist
 BPPV and Pitfalls in its Management Reza Golrokhian Sani MD, Otolaryngologist- Head & Neck Surgeon Otologist & Neurotologist Objectives 1-The best methods of diagnosis of BPV 2-How to differentiate between
BPPV and Pitfalls in its Management Reza Golrokhian Sani MD, Otolaryngologist- Head & Neck Surgeon Otologist & Neurotologist Objectives 1-The best methods of diagnosis of BPV 2-How to differentiate between
Nicolas Bianchi M.D. May 15th, 2012
 Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Evaluation & Management of Vestibular Disorders
 Evaluation & Management of Vestibular Disorders Richard A. Roberts, Ph.D., FAAA Alabama Hearing & Balance Associates, Inc. Disclosure and Copyright Statements Richard Roberts has no financial or nonfinancial
Evaluation & Management of Vestibular Disorders Richard A. Roberts, Ph.D., FAAA Alabama Hearing & Balance Associates, Inc. Disclosure and Copyright Statements Richard Roberts has no financial or nonfinancial
Peripheral vestibular disorders will affect 1 of 13 people in their lifetime
 Peripheral vestibular disorders will affect 1 of 13 people in their lifetime 80% of affected persons seek medical consultation Unclear how many of these are for peripheral vs central disorders Generally:
Peripheral vestibular disorders will affect 1 of 13 people in their lifetime 80% of affected persons seek medical consultation Unclear how many of these are for peripheral vs central disorders Generally:
Dizziness: Natural Treatment for Vertigo and BPPV
 Wellness and WBV Studio Home» Bodywork» Massage» CranioSacral Therapy» Dizziness: Natural Treatment for Vertigo and BPPV CRANIOSACRAL THERAPY HOLISTIC HEALING Dizziness: Natural Treatment for Vertigo and
Wellness and WBV Studio Home» Bodywork» Massage» CranioSacral Therapy» Dizziness: Natural Treatment for Vertigo and BPPV CRANIOSACRAL THERAPY HOLISTIC HEALING Dizziness: Natural Treatment for Vertigo and
Vestibular Symptoms in Concussion: Medical/Surgical Perspective. Jacob R. Brodsky, MD Boston Children s Hospital
 Vestibular Symptoms in Concussion: Medical/Surgical Perspective Jacob R. Brodsky, MD Boston Children s Hospital jacob.brodsky@childrens.harvard.edu On Field Symptoms Headache Dizziness Confusion Fatigue
Vestibular Symptoms in Concussion: Medical/Surgical Perspective Jacob R. Brodsky, MD Boston Children s Hospital jacob.brodsky@childrens.harvard.edu On Field Symptoms Headache Dizziness Confusion Fatigue
Dizziness and Vertigo: A Step wise Approach to Evaluation and Management
 Saturday CME Lunch Dizziness and Vertigo: A Step wise Approach to Evaluation and Management Jennifer Wipperman, MD, MPH Associate Director, Via Christi Family Medicine Residency Assistant Professor of
Saturday CME Lunch Dizziness and Vertigo: A Step wise Approach to Evaluation and Management Jennifer Wipperman, MD, MPH Associate Director, Via Christi Family Medicine Residency Assistant Professor of
Dizziness and Vertigo: A Step-wise Approach to Evaluation and Management
 Dizziness and Vertigo: A Step-wise Approach to Evaluation and Management Jennifer Wipperman, MD, MPH Via Christi Family Medicine Residency University of Kansas School of Medicine Wichita Objectives Narrow
Dizziness and Vertigo: A Step-wise Approach to Evaluation and Management Jennifer Wipperman, MD, MPH Via Christi Family Medicine Residency University of Kansas School of Medicine Wichita Objectives Narrow
The Geriatric Patient The EM Perspective. Advice from a neophyte
 The Geriatric Patient The EM Perspective Advice from a neophyte Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any
The Geriatric Patient The EM Perspective Advice from a neophyte Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any
ACTIVITY DISCLAIMER. Jennifer Wipperman, MD
 Dizziness and Vertigo: A Step-Wise Approach to Evaluation and Management Jennifer Wipperman, MD ACTIVITY DISCLAIMER The material presented here is being made available by the American Academy of Family
Dizziness and Vertigo: A Step-Wise Approach to Evaluation and Management Jennifer Wipperman, MD ACTIVITY DISCLAIMER The material presented here is being made available by the American Academy of Family
LA CLINICA E LA DIAGNOSI DELLA VERTIGINE VASCOLARE
 LA CLINICA E LA DIAGNOSI DELLA VERTIGINE VASCOLARE M. Mandalà Azienda Ospedaliera Universitaria Senese WHY ARE WE SCARED? NEED TO BETTER UNDERSTAND PATHOPHYSIOLOGY WHAT IS KNOWN WHAT IS EFFECTIVE and SIMPLE
LA CLINICA E LA DIAGNOSI DELLA VERTIGINE VASCOLARE M. Mandalà Azienda Ospedaliera Universitaria Senese WHY ARE WE SCARED? NEED TO BETTER UNDERSTAND PATHOPHYSIOLOGY WHAT IS KNOWN WHAT IS EFFECTIVE and SIMPLE
What is the effect on the hair cell if the stereocilia are bent away from the kinocilium?
 CASE 44 A 53-year-old man presents to his primary care physician with complaints of feeling like the room is spinning, dizziness, decreased hearing, ringing in the ears, and fullness in both ears. He states
CASE 44 A 53-year-old man presents to his primary care physician with complaints of feeling like the room is spinning, dizziness, decreased hearing, ringing in the ears, and fullness in both ears. He states
Suspected neurological conditions: clinical questions
 Suspected neurological clinical questions For questions on signs and symptoms, the committee wanted to consider any studies that determine whether a certain sign or symptom accompanying a main presenting
Suspected neurological clinical questions For questions on signs and symptoms, the committee wanted to consider any studies that determine whether a certain sign or symptom accompanying a main presenting
VESTIBULAR FUNCTION TESTING
 VESTIBULAR FUNCTION TESTING Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices
VESTIBULAR FUNCTION TESTING Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices
High Yield Neurological Examination
 High Yield Neurological Examination Vanja Douglas, MD Sara & Evan Williams Foundation Endowed Neurohospitalist Chair Director, Neurohospitalist Division Associate Professor of Clinical Neurology UCSF Department
High Yield Neurological Examination Vanja Douglas, MD Sara & Evan Williams Foundation Endowed Neurohospitalist Chair Director, Neurohospitalist Division Associate Professor of Clinical Neurology UCSF Department
Problem based review: the patient with dizziness on the AMU
 240 Acute Medicine 2012 11(4): 240-245 Trainee Section Problem based review: the patient with dizziness on the AMU A Kennedy & N Cooper Abstract Unsteadiness, balance disturbance, and dizziness are common
240 Acute Medicine 2012 11(4): 240-245 Trainee Section Problem based review: the patient with dizziness on the AMU A Kennedy & N Cooper Abstract Unsteadiness, balance disturbance, and dizziness are common
Vertigo. Done by : Njoud Alrasheed. Reviewed by :Hadeel B. Alsulami. Correction File
 Vertigo Objectives: To know anatomy of balance organs Physiology of balance Relevant history in dizzy patients Classification of vertigo Common peripheral causes of vertigo, clinical features, investigation
Vertigo Objectives: To know anatomy of balance organs Physiology of balance Relevant history in dizzy patients Classification of vertigo Common peripheral causes of vertigo, clinical features, investigation
Assessing the Deaf & the Dizzy. Phil Bird Senior Lecturer University of Otago, Christchurch Consultant Otolaryngologist CPH & Private
 Assessing the Deaf & the Dizzy Phil Bird Senior Lecturer University of Otago, Christchurch Consultant Otolaryngologist CPH & Private Overview Severe & profoundly deaf children & adults Neonatal screening
Assessing the Deaf & the Dizzy Phil Bird Senior Lecturer University of Otago, Christchurch Consultant Otolaryngologist CPH & Private Overview Severe & profoundly deaf children & adults Neonatal screening
OBJECTIVES BALANCE EVALUATION COMMON CAUSES OF BALANCE DEFICITS POST TBI BRAIN INJURY BALANCE RELATIONSHIP
 OBJECTIVES Understand variables that contribute to balance deficits Understand the relationship between a brain injury and balance Become familiar with the components of a vestibular/balance assessment
OBJECTIVES Understand variables that contribute to balance deficits Understand the relationship between a brain injury and balance Become familiar with the components of a vestibular/balance assessment
BENIGN PAROXYSMAL POSITIONAL VERTIGO (BPPV)
") 5018 NE 15 TH AVE PORTLAND, OR 97211 FAX: (503) 229-8064 (800) 837-8428 INFO@VESTIBULAR.ORG VESTIBULAR.ORG BENIGN PAROXYSMAL POSITIONAL VERTIGO (BPPV) By Sheelah Woodhouse, BScPT WHAT IS BPPV? Benign Paroxysmal
5018 NE 15 TH AVE PORTLAND, OR 97211 FAX: (503) 229-8064 (800) 837-8428 INFO@VESTIBULAR.ORG VESTIBULAR.ORG BENIGN PAROXYSMAL POSITIONAL VERTIGO (BPPV) By Sheelah Woodhouse, BScPT WHAT IS BPPV? Benign Paroxysmal
Dizziness, postural hypotension and postural blackouts: Two cases suggesting multiple system atrophy
 Dizziness, postural hypotension and postural blackouts: Two cases suggesting multiple system atrophy Dr Rahul Chakor, Associate Prof and Head Dept of Neurology, Dr Anand Soni, Senior Resident, T N Medical
Dizziness, postural hypotension and postural blackouts: Two cases suggesting multiple system atrophy Dr Rahul Chakor, Associate Prof and Head Dept of Neurology, Dr Anand Soni, Senior Resident, T N Medical
Update '08: Vestibular and Balance Rehabilitation Therapy
 Update '08: Vestibular and Balance Rehabilitation Therapy In Context with Surgery Medicine & Diet Symptoms of Dizziness Dizziness non-specific term; encompasses any and all of the specific symptoms: Vertigo
Update '08: Vestibular and Balance Rehabilitation Therapy In Context with Surgery Medicine & Diet Symptoms of Dizziness Dizziness non-specific term; encompasses any and all of the specific symptoms: Vertigo
Balance Assessment and Rehabilitation in Audiology. Andy Phillips Director of Therapies and Health Science ABMU Health Board
 Balance Assessment and Rehabilitation in Audiology Andy Phillips Director of Therapies and Health Science ABMU Health Board Balance Mechanism This has 3 components -Sensory Input -Central Processing -Motor
Balance Assessment and Rehabilitation in Audiology Andy Phillips Director of Therapies and Health Science ABMU Health Board Balance Mechanism This has 3 components -Sensory Input -Central Processing -Motor
Acute Dizziness: Is It a Stroke? Gordon Kelley MD November 2017
 Acute Dizziness: Is It a Stroke? Gordon Kelley MD November 2017 No Disclosures Dizziness Occurs in nearly ¾ of cerebellar strokes 4 categories in classic teaching*: Vertigo Presyncope Imbalance Non-specific
Acute Dizziness: Is It a Stroke? Gordon Kelley MD November 2017 No Disclosures Dizziness Occurs in nearly ¾ of cerebellar strokes 4 categories in classic teaching*: Vertigo Presyncope Imbalance Non-specific
V e r t i g o. T ü n d e. M a g y a r
 V e r t i g o T ü n d e M a g y a r Dizziness Vestibular Proprioception Optic input (afferentation) carries not Optic input (afferentation) carries not synchronizated information to the CNS, but contradictory
V e r t i g o T ü n d e M a g y a r Dizziness Vestibular Proprioception Optic input (afferentation) carries not Optic input (afferentation) carries not synchronizated information to the CNS, but contradictory
Cross Country Education Leading the Way in Continuing Education and Professional Development.
 To comply with professional boards/associations standards: I declare that I or my family do not have any financial relationship in any amount, occurring in the last 12 months with a commercial interest
To comply with professional boards/associations standards: I declare that I or my family do not have any financial relationship in any amount, occurring in the last 12 months with a commercial interest
Vestibular service (balance)
") The vestibular service at Addenbrooke s Hospital works closely with the Ear Nose and Throat (ENT), Neurology consultants and physiotherapists to help manage patients with dizziness/balance problems. The
The vestibular service at Addenbrooke s Hospital works closely with the Ear Nose and Throat (ENT), Neurology consultants and physiotherapists to help manage patients with dizziness/balance problems. The
Clinical Recommendation: Assessment and Management of Dizziness Associated with Mild TBI
 Clinical Recommendation: Assessment and Management of Dizziness Associated with Mild TBI Learning Objectives Understand an overview of dizziness response following mild TBI Differentiate between three
Clinical Recommendation: Assessment and Management of Dizziness Associated with Mild TBI Learning Objectives Understand an overview of dizziness response following mild TBI Differentiate between three
Speaker Disclosures: 12/4/2015 DIZZINESS AND NEAR SYNCOPE. I have no relevant commercial relationships to disclose
 DIZZINESS AND NEAR SYNCOPE Bernard Gran, M.D. Neurologist, Co-Chief, Department of Neuroscience Baptist Health Neuroscience Center Speaker Disclosures: I have no relevant commercial relationships to disclose
DIZZINESS AND NEAR SYNCOPE Bernard Gran, M.D. Neurologist, Co-Chief, Department of Neuroscience Baptist Health Neuroscience Center Speaker Disclosures: I have no relevant commercial relationships to disclose
The evaluation of a patient with dizziness
 The evaluation of a patient with dizziness Kevin A. Kerber and Robert W. Baloh Neurol Clin Pract 2011;1;24 DOI 10.1212/CPJ.0b013e31823d07b6 This information is current as of December 28, 2011 The online
The evaluation of a patient with dizziness Kevin A. Kerber and Robert W. Baloh Neurol Clin Pract 2011;1;24 DOI 10.1212/CPJ.0b013e31823d07b6 This information is current as of December 28, 2011 The online
It s Always a Stroke; Except For When It s Not..
 It s Always a Stroke; Except For When It s Not.. TREVOR PHINNEY, D.O. Disclosures No Relevant Disclosures 1 Objectives Discuss variables of differential diagnosis for stroke Review when to TPA and when
It s Always a Stroke; Except For When It s Not.. TREVOR PHINNEY, D.O. Disclosures No Relevant Disclosures 1 Objectives Discuss variables of differential diagnosis for stroke Review when to TPA and when
Monitoring of Caloric Response and Outcome in Patients With Benign Paroxysmal Positional Vertigo
 Otology & Neurotology 28:798Y800 Ó 2007, Otology & Neurotology, Inc. Monitoring of Caloric Response and Outcome in Patients With Benign Paroxysmal Positional Vertigo *Maria I. Molina, *Jose A. López-Escámez,
Otology & Neurotology 28:798Y800 Ó 2007, Otology & Neurotology, Inc. Monitoring of Caloric Response and Outcome in Patients With Benign Paroxysmal Positional Vertigo *Maria I. Molina, *Jose A. López-Escámez,
Labyrinthitis and Vestibular Neuritis
 Labyrinthitis and Vestibular Neuritis http://www.patient.co.uk/health/labyrinthitis-and-vestibular-neuritis.htm Labyrinthitis and vestibular neuritis are most commonly caused by a viral infection that
Labyrinthitis and Vestibular Neuritis http://www.patient.co.uk/health/labyrinthitis-and-vestibular-neuritis.htm Labyrinthitis and vestibular neuritis are most commonly caused by a viral infection that
Management of Ear, Hearing and Balance Disorders: Fact, Fiction, and Future
 Management of Ear, Hearing and Balance Disorders: Fact, Fiction, and Future George W. Hicks, M,D. 7440 N. Shadeland Avenue, Suite 150 Indianapolis, IN 46250 904 N. Samuel Moore Parkway Mooresville, IN
Management of Ear, Hearing and Balance Disorders: Fact, Fiction, and Future George W. Hicks, M,D. 7440 N. Shadeland Avenue, Suite 150 Indianapolis, IN 46250 904 N. Samuel Moore Parkway Mooresville, IN
Paediatric Balance Assessment
 BAA regional meeting 11 th March 2016 Paediatric Balance Assessment Samantha Lear, Lead Clinical Scientist, Hearing Services, SCH overview The balance system Vestibular disorders referrals Vestibular assessment
BAA regional meeting 11 th March 2016 Paediatric Balance Assessment Samantha Lear, Lead Clinical Scientist, Hearing Services, SCH overview The balance system Vestibular disorders referrals Vestibular assessment
An approach to vertigo in general practice
 CLINICAL An approach to vertigo in general practice Sindhu Dommaraju, Eshini Perera Background Dizziness is a common and very distressing presentation in general practice. In more than half of these cases,
CLINICAL An approach to vertigo in general practice Sindhu Dommaraju, Eshini Perera Background Dizziness is a common and very distressing presentation in general practice. In more than half of these cases,
Balance Disorders in Adolescents (and Young Adults)
") Balance Disorders in Adolescents (and Young Adults) RCP Conference 18 January 2016 Katherine Harrop-Griffiths Consultant in Audiovestibular Medicine (Paediatric) Royal National Throat, Nose & Ear Hospital
Balance Disorders in Adolescents (and Young Adults) RCP Conference 18 January 2016 Katherine Harrop-Griffiths Consultant in Audiovestibular Medicine (Paediatric) Royal National Throat, Nose & Ear Hospital
Dizziness is VERY Common. Dizziness is an imprecise term. Diagnostic Categories. Question. Answer 1. The Dizzy Patient Recent advances (2007)
") The Dizzy Patient Recent advances (2007) Timothy C. Hain, MD Chicago Dizziness and Hearing Neurology, Otolaryngology, Physical Therapy Northwestern University, Chicago t-hain@northwestern.edu Dizziness
The Dizzy Patient Recent advances (2007) Timothy C. Hain, MD Chicago Dizziness and Hearing Neurology, Otolaryngology, Physical Therapy Northwestern University, Chicago t-hain@northwestern.edu Dizziness
Very few dizzy conditions have a surgical treatment SURGICAL MANAGEMENT OF THE DIZZY PATIENT. Surgical Treatments for. Shunts and Sac Surgery
 SURGICAL MANAGEMENT OF THE DIZZY PATIENT Very few dizzy conditions have a surgical treatment Timothy C. Hain, M.D. Meniere s Disease Perilymphatic Fistula (PLF) Superior Canal Dehiscence (SSD) Benign Paroxysmal
SURGICAL MANAGEMENT OF THE DIZZY PATIENT Very few dizzy conditions have a surgical treatment Timothy C. Hain, M.D. Meniere s Disease Perilymphatic Fistula (PLF) Superior Canal Dehiscence (SSD) Benign Paroxysmal
INCIDENCE OF SUSPECTED OTOLITHIC ABNORMALITIES IN MILD TRAUMATIC BRAIN INJURED VETERANS OBSERVATIONS FROM A LARGE VA POLYTRAUMA NETWORK SITE
 INCIDENCE OF SUSPECTED OTOLITHIC ABNORMALITIES IN MILD TRAUMATIC BRAIN INJURED VETERANS OBSERVATIONS FROM A LARGE VA POLYTRAUMA NETWORK SITE David Domoracki Ph.D. Cleveland VAMC Audiology Service Jennifer
INCIDENCE OF SUSPECTED OTOLITHIC ABNORMALITIES IN MILD TRAUMATIC BRAIN INJURED VETERANS OBSERVATIONS FROM A LARGE VA POLYTRAUMA NETWORK SITE David Domoracki Ph.D. Cleveland VAMC Audiology Service Jennifer
The Dizzy Patient: How You Can Help
 MICHAEL J. RUCKENSTEIN, MD, MSc, FACS University of Pennsylvania LINDSAY A. GOODSTEIN University of Maryland The Dizzy Patient: Dr Ruckenstein is professor of otorhinolaryngology, head and neck surgery,
MICHAEL J. RUCKENSTEIN, MD, MSc, FACS University of Pennsylvania LINDSAY A. GOODSTEIN University of Maryland The Dizzy Patient: Dr Ruckenstein is professor of otorhinolaryngology, head and neck surgery,
What Do You Think of My Posterior?
 What Do You Think of My Posterior? Posterior Stroke and Stroke Mimics Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School of Medicine Disclosures
What Do You Think of My Posterior? Posterior Stroke and Stroke Mimics Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School of Medicine Disclosures
ASAMS Panel Sort n out Vertigo in Pilots
 ASAMS Panel Sort n out Vertigo in Pilots Dave Schall, MD MPH FACPM FACS Great Lakes Regional Flight Surgeon Aerospace Neurotologist May 2013 Disclosure Information 84th Annual AsMA Scientific Meeting David
ASAMS Panel Sort n out Vertigo in Pilots Dave Schall, MD MPH FACPM FACS Great Lakes Regional Flight Surgeon Aerospace Neurotologist May 2013 Disclosure Information 84th Annual AsMA Scientific Meeting David
Vestibular physiology
 Vestibular physiology 2017 Utricle A flat epithelium: horizontal in the upright head Utricle Hair cells: no axons hair cells Utricle Hair cells synapse onto 8th nerve afferents. 8th nerve afferents Hair
Vestibular physiology 2017 Utricle A flat epithelium: horizontal in the upright head Utricle Hair cells: no axons hair cells Utricle Hair cells synapse onto 8th nerve afferents. 8th nerve afferents Hair
Practical Emergency Medicine Dizziness and vertigo. Dr. H K Tong Consultant A&E Dept Queen Mary Hospital Hon Associate Prof. HKU
 Practical Emergency Medicine Dizziness and vertigo Dr. H K Tong Consultant A&E Dept Queen Mary Hospital Hon Associate Prof. HKU Introduction Dizziness Common And Challenging: Too many possible diagnoses
Practical Emergency Medicine Dizziness and vertigo Dr. H K Tong Consultant A&E Dept Queen Mary Hospital Hon Associate Prof. HKU Introduction Dizziness Common And Challenging: Too many possible diagnoses
JULY 6 TH GOLDEN PARKK, KOLKATA
 JULY 6 TH 2014- GOLDEN PARKK, KOLKATA ESP - 2014 : INSIGHT "Insight- Connect with the Experts was held at Golden Parkk, Kolkata. It was organized by of Asian Society of Continuing Medical Education collaborating
JULY 6 TH 2014- GOLDEN PARKK, KOLKATA ESP - 2014 : INSIGHT "Insight- Connect with the Experts was held at Golden Parkk, Kolkata. It was organized by of Asian Society of Continuing Medical Education collaborating
Vague Neurological Conditions
 Vague Neurological Conditions Dr. John Lefebre, MD, FRCPC Chief Regional Medical Director Europe, India, South Africa, Middle East and Turkey Canada 2014 2 3 4 Agenda Dr. John Lefebre, M.D., FRCPC 1. TIA
Vague Neurological Conditions Dr. John Lefebre, MD, FRCPC Chief Regional Medical Director Europe, India, South Africa, Middle East and Turkey Canada 2014 2 3 4 Agenda Dr. John Lefebre, M.D., FRCPC 1. TIA
Defining Dizziness: An Acute Approach to Vestibular Dysfunction in the Hospital Setting Friday, February 17, :00 AM-10:00 AM
 Defining Dizziness: An Acute Approach to Vestibular Dysfunction in the Hospital Setting Friday, February 17, 2017 8:00 AM-10:00 AM Kerry Lammers, PT, DPT Gabrielle Steinhorn, PT, DPT, NCS Vestibular dysfunction
Defining Dizziness: An Acute Approach to Vestibular Dysfunction in the Hospital Setting Friday, February 17, 2017 8:00 AM-10:00 AM Kerry Lammers, PT, DPT Gabrielle Steinhorn, PT, DPT, NCS Vestibular dysfunction
Normal membranous labyrinth. Dilated membranous labyrinth in Meniere's disease (Hydrops)
") Meniere s Disease Normal membranous labyrinth Dilated membranous labyrinth in Meniere's disease (Hydrops) Normal membranous labyrinth Dilated membranous labyrinth in Meniere's disease (Hydrops) DEFINITION
Meniere s Disease Normal membranous labyrinth Dilated membranous labyrinth in Meniere's disease (Hydrops) Normal membranous labyrinth Dilated membranous labyrinth in Meniere's disease (Hydrops) DEFINITION
Classic Cases. Interesting Dizzy Cases. Case 1. Case 2. Case 3. Case 4. Timothy C. Hain, MD
 Interesting Dizzy Cases Classic Cases Timothy C. Hain, MD Case 1 A 30 year old Chicago Park District Worker came in because of dizziness. He fell off of a truck two years ago, hit his head, and now he
Interesting Dizzy Cases Classic Cases Timothy C. Hain, MD Case 1 A 30 year old Chicago Park District Worker came in because of dizziness. He fell off of a truck two years ago, hit his head, and now he
DIZZINESS Varieties. : Fainting, hypotension : Rotatory, spinning. : Muscular incoordination : Collapse without LOC: ELH : Disturbed awareness
 DIZZINESS Varieties head Syncope Vertigo Dysequilibrium Ataxia Drop attacks Confusion Panic Attacks Non-organic : Fainting, hypotension : Rotatory, spinning : Unsteadiness on moving : Muscular incoordination
DIZZINESS Varieties head Syncope Vertigo Dysequilibrium Ataxia Drop attacks Confusion Panic Attacks Non-organic : Fainting, hypotension : Rotatory, spinning : Unsteadiness on moving : Muscular incoordination
Angus Waddell. Basic Structure. When to examine the ear. Knowledge Base. Ear Examination. Ear Examination. How do we Teach ENT in UoB 2014
 How do we Teach ENT in UoB 2014 Angus Waddell Undergraduate Lead for ENT. University of Bristol Consultant ENT Surgeon Great Western Hospital, Swindon Basic Structure Junior Medicine and Surgery 1 Week
How do we Teach ENT in UoB 2014 Angus Waddell Undergraduate Lead for ENT. University of Bristol Consultant ENT Surgeon Great Western Hospital, Swindon Basic Structure Junior Medicine and Surgery 1 Week
7. Anatomy and physiology of the vestibular system. Harmonic and disharmonic vestibular syndrome.
 7. Anatomy and physiology of the vestibular system. Harmonic and disharmonic vestibular syndrome. 8. Fundamental examination tools of otoneurology. 20. Ménière s syndrome and Ménière s disease. Therapeutic
7. Anatomy and physiology of the vestibular system. Harmonic and disharmonic vestibular syndrome. 8. Fundamental examination tools of otoneurology. 20. Ménière s syndrome and Ménière s disease. Therapeutic
DOWNLOAD OR READ : VERTIGO AND DIZZINESS REHABILITATION THE MCS METHOD PDF EBOOK EPUB MOBI
 DOWNLOAD OR READ : VERTIGO AND DIZZINESS REHABILITATION THE MCS METHOD PDF EBOOK EPUB MOBI Page 1 Page 2 vertigo and dizziness rehabilitation the mcs method vertigo and dizziness rehabilitation pdf vertigo
DOWNLOAD OR READ : VERTIGO AND DIZZINESS REHABILITATION THE MCS METHOD PDF EBOOK EPUB MOBI Page 1 Page 2 vertigo and dizziness rehabilitation the mcs method vertigo and dizziness rehabilitation pdf vertigo
A&P 1. Ear, Hearing & Equilibrium Lab. Basic Concepts. Pre-lab Exercises
 A&P 1 Ear, Hearing & Equilibrium Lab Basic Concepts Pre-lab Exercises In this "Lab Exercise Guide", we will be looking at the basics of hearing and equilibrium. NOTE: these notes do not follow the order
A&P 1 Ear, Hearing & Equilibrium Lab Basic Concepts Pre-lab Exercises In this "Lab Exercise Guide", we will be looking at the basics of hearing and equilibrium. NOTE: these notes do not follow the order