Practical Emergency Medicine Dizziness and vertigo. Dr. H K Tong Consultant A&E Dept Queen Mary Hospital Hon Associate Prof. HKU
|
|
|
- Beatrice Horton
- 5 years ago
- Views:
Transcription
1 Practical Emergency Medicine Dizziness and vertigo Dr. H K Tong Consultant A&E Dept Queen Mary Hospital Hon Associate Prof. HKU

2 Introduction Dizziness Common And Challenging: Too many possible diagnoses Too difficult to get a clear history Physical exam is often non-contributory Too many pitfalls
3 Many causes:- 15% Spectrum of Dizziness Visits to US Emergency Departments Mayo Clin Proc. 2008;83(7):


4 Case scenario Triage F 65 dizziness today vomited once PH-- HT, DM FU GOPD BP 150/90 P 65/min Temp 37 C Category III (Stretcher case)
5 Dizziness Targeted history Nature Duration and previous episode Provoking factors associated symptoms PMH, Drug, Allergy
6 What do you understand by the term : dizziness? Vertigo? Disequilibrium (tend to fall)? Lightheadedness? (pre-syncope) Blackout? (syncope) Unwell? Headache? Weakness? Unhappy..??
7 Some more history... Need to clarify dizziness your understanding on dizziness may not be the same as the patient s.
8 Try not to use the word 暈 to describe your feeling 天旋地轉 睜不開眼 好想睏 暈船浪 想暈倒 Vertigo Dysequilibrium Lightheadedness Near syncope
9 Martin A. Samuels THE DIZZY PATIENT: A CLEAR-HEADED APPROACH
10 Pitfall Rely too much on assigning a dizziness category in limiting the DDx.
11 Symptom description is not precise
12 Common DDx of Vertigo CNS problem Cerebellar stroke Brain stem stroke TIA (vertebro-basilar insufficiency) CP angle tumor Demyelination disease Vestibular migraine Peripheral Labyrinthitis Vestibular neuronitis BPPV (otoconia) Meniere s disease Concussion (labyrinthine) Acoustic neuroma Drugs can cause both types of vertigo
13 Central Peripheral Vertigo less intense Constant symptom Imbalance: severe Hearing loss and tinnitus less common CNS / Cerebellar sign +ve More intense Paroxysmal acute relapse Imbalance: milder Hearing loss and tinnitus more common No cerebellar sign These are NOT INVARIABLE!!!
14 Otogenic vertigo: DDx matrix
15 Duration of illness Long history Really? Or just recurrent episodes Persisting e.g. multiple sensory deficits Recurrent e.g. Menieres BPPV Short history 1-2 days Never before Implication: look for acute sinister problem
 Long (hours) BPPV")


16 Duration of symptoms Short (minutes) Long (hours) BPPV Near-syncope TIA Vestibular neuronitis Menieres Ds Initial Evaluation of Vertigo. Am Fam Physician 2006;73:
17 Provoking/Precipitating factors Triggered by certain head position e.g. looking up Positional vertigo (e.g.bppv) Triggered by change in head position Likely peripheral vestibular Worsen while getting up and lying down Equivalent to change head position Worsen while getting up only Think orthostatic hypotension, autonomic neuropathy Only while walking Likely neurological deficit During exercise Perfusion problem due to CV causes

18 Vertigo provoked or aggravated by head motion? Overreliance on symptom quality in diagnosing dizziness: Stanton VA - Mayo Clin Proc ; 82(11):
19 Pitfall Vertigo aggravated (NOT triggered) by head movement may still be due to CENTRAL causes
20 Associated symptoms are useful in pointing to other DDx General Fever (URI) Nausea Depression / anxiety CNS headache diplopia weakness/numbness unsteady gait CVS/Resp palpitation chest pain SOB, cough ENT earache, fullness hearing loss tinnitis GI Vomiting/ Diarrhea Abd pain tarry stool
21 Drug related dizziness Hypotension All anti HT drugs (especially recently added) postural hypotension: alpha-blockers Hypoglycemia: Long acting DM drug: Daonil for age>70 Toxic action at reticular activating system Anticonvulsant e.g. phenytoin + nystagmus Drugs that disturb electrolytes: Natrilix Ototoxic drugs: lasix, salicylates
22
23 Physical exam may help in pin pointing the cause. CNS? Peripheral vestibular? Perfusion problems?
24 Focus your exam GC--pallor CNS cranial N nystagmus cerebellar signs limb: motor, sensory ENT hearing T M Neck rigidity bruit CVS/Resp GI BP/P; Postural BP JVP; HS; M AE, added sounds abdomen PR tarry stool Test Gait at some point
25 Investigation Unnecessary if diagnosis is obvious from history or physical exam: Peripheral vertigo due to BPPV, Meniere s disease, vasovagal attack No routine set of Ix for dizziness
26 Useful investigations for dizziness ECG: suspected silent MI ( usually in diabetic and old female ) or arrhythmia Blood glucose: hyper/hypo in DM patients CBP: suspected anemia Electrolytes: maybe useful in pt with nonspecific dizziness and risk factors e.g. on diuretics CT brain
27 Consider urgent CT Age >50 Abrupt onset of symptoms Prior history of stroke/tia Risk factors for stroke Head/ Neck injury (MVC, neck manipulation? Dissection) Headache (sudden, severe, persistent) Nausea/vomiting disproportionate to dizziness
28 Wait h before CT Isolated vertigo Nystagmus of peripheral type Can still walk though unstable If symptoms improve over time vestibular disease and no need for CT
29 Three categories of ED dizzy pt Acute severe dizziness Recurrent attacks of dizziness Recurrent positional dizziness


30 Acute severe dizziness (not near syncope pattern) Kerber. Emerg Med Clin N Am 27 (2009) 39 50
")
31 Recurrent dizziness Kerber. Emerg Med Clin N Am 27 (2009) 39 50
 39")
32 Emerg Med Clin N Am 27 (2009) 39 50
33 Scenario A--F/65, DM, HT Onset Provoke Today, gradual Hx of URI recently Quality Spinning sensation + Relief Severity Time Better with eyes closed, worse with neck movement Cannot get up for a few hours already Associated symptoms: Nausea + vomiting; no tinnitus/hearing loss Exam: essentially normal
34 Vestibular sedatives Prochlorperazine (Stemetil) Anti-emetic, phenothiazine group CNS acting Not for children Caution in young adults (dyskinesia) Dimenhydrinate (Gravol) First generation antihistamine Anti-motion sickness (unknown mechanism) Betahistine(Merislon) antivertigo/selective vasodilator Diazepam (Valium) BZD Not For Brief Episodes Beware: not useful if not vestibular ds.
35 Any special test for vestibular ds? Hallpike test (For BPPV only) Head Thrust Test
36 Hallpike test positional testing using the head-hanging technique sit patient up head turn to one side lower body and head to a level lower than bed patients with benign positional vertigo will show a burst of upbeating nystagmus after a delay of 5 to 10 seconds, the nystagmus lasts about 30 seconds
37



38 Dix Hallpike: Traditional and Sideway Position Barraclough, Kevin; Bronstein, Adolfo. Vertigo. BMJ. 339:b3493, September 26, 2009
39 Hallpike test & Epley manoevre
40 Nystagmus? Central Central Horizontal; vertical Change direction with gaze No fatigue Peripheral Horizontal Fixed direction Fatiguable Fixation has no effect Disappear with fixation
41 Effect of fixation Hotson et al. Acute Vestibular Sx. NEJM 1998;339 (10)

42 Alexander law Nystagmus due to peripheral vestibular disease increases in intensity when the eyes are turned in the direction of the saccade (fast phase)

43 Down beating nystagmus


44 Vertical nystagmus Pitfall Overreliance on symptom quality in diagnosing dizziness: Stanton VA - Mayo Clin Proc ; 82(11):
45 Bidirectional nystagmus
46 Any other features to suggest central origin? Vascular risk factors e.g. HT, smoker Headache, neck rigidity Focal signs e.g. double vision Cerebellar sign e.g. truncal ataxia < 50% pts with cerebellar infarct have nystagmus
47 Stroke e.g. cerebellar should be suspected CT scan Consult Neuro PRN
48 Any other specific points you want to ascertain in the history and physical? LMP in younger patient Drugs e.g. NSAID, Po Chai pill Omit meal (other features of hypoglycemia) Palpitation (arrhythmia) BP postural changes Tarry stool (melena PR)
49 How do you check postural BP BP lying repeat BP after patient stands for ~ 1min SBP > 20 mmhg is significant may reproduce dizziness This patient has SBP drop ~ 20 mmhg + recurrence of dizziness on standing up
50 PR shows no melena. Is GIB ruled out? It takes hours for melena to reach rectum.
51 Sources of bleeding/anemia Gut bleeding peptic ulcer bleeding colon cancer Bleeding hemorrhoid GU tract menorrhagia ectopic pregnancy hematuria Concealed bleeding AAA Blood disorders hemolysis e.g. drug induced leukemia Hemodilution takes time.
52 Summary We have covered: Different types of dizziness Important causes of dizziness Vertigo: stroke, vestibular ds non-vertigo: inadequate CNS perfusion, anemia Evaluation of dizzy patients
53 Evaluation of dizziness History O Onset P Provoking factor Q Quality or nature R Relief/Aggravate Factor S Severity T Time Course/ Duration Associated symptoms Physical Exam Cranial N Nystagmus Cerebellar signs Gait/Balance ENT (Head Thrust ) CVS (postural BP) GI (tarry stool) Neuro
54 Diagnosis not to miss: Stroke (cerebellar) GIB Cardiac causes
55 Safe management of dizziness Precise history Repeated physical exam Choice of investigation Reassessment Discharge only if: symptom free while walking +/- referral
56 End
57 Psychiatric dizziness Definition: a subjective sensation of dizziness associated with other anxiety / depression / obsession symptom Non-vertigo Persistent or frequent relapsing Presence of dizziness despites normal neurology and gait Can happen in relative young patients

58 Head Thrust Test Test vestibulo-occular reflex Abnormal eye movements associated with unilateral loss of vestibular function. N Engl J Med 2006;355(24):e26.


59 Initial Evaluation of Vertigo. Am Fam Physician 2006;73:



60 Initial Evaluation of Vertigo. Am Fam Physician 2006;73:


61 Initial Evaluation of Vertigo. Am Fam Physician 2006;73:
Dizziness: Neurological Aspect
 Dizziness: Neurological Aspect..! E-mail: somtia@kku.ac.th http://epilepsy.kku.ac.th Features between peripheral and central vertigo 1. Peripheral Central 2.! " # $ " Imbalance Mild-moderate Severe 3.!
Dizziness: Neurological Aspect..! E-mail: somtia@kku.ac.th http://epilepsy.kku.ac.th Features between peripheral and central vertigo 1. Peripheral Central 2.! " # $ " Imbalance Mild-moderate Severe 3.!
What could be reffered to as dizziness by the patient?
 What could be reffered to as dizziness by the patient? Rotational vertigo Sense of instability Ataxia of gait Disturbance of vision Loss of contact with surroundings Nausea Loss of memory Loss of confidence
What could be reffered to as dizziness by the patient? Rotational vertigo Sense of instability Ataxia of gait Disturbance of vision Loss of contact with surroundings Nausea Loss of memory Loss of confidence
Vertigo. Tunde Magyar MD, PhD
 Vertigo Tunde Magyar MD, PhD What could be reffered to as dizziness by the patient? Rotational vertigo Sense of instability Ataxia of gait Disturbance of vision Loss of contact with surroundings Nausea
Vertigo Tunde Magyar MD, PhD What could be reffered to as dizziness by the patient? Rotational vertigo Sense of instability Ataxia of gait Disturbance of vision Loss of contact with surroundings Nausea
Evaluation of the Dizzy Patient
 Evaluation of the Dizzy Patient S. Andrew Josephson, MD Department of Neurology University of California San Francisco October 1, 2007 Who Sees Dizzy Patients? ED physicians Internists Neurologists ENT
Evaluation of the Dizzy Patient S. Andrew Josephson, MD Department of Neurology University of California San Francisco October 1, 2007 Who Sees Dizzy Patients? ED physicians Internists Neurologists ENT
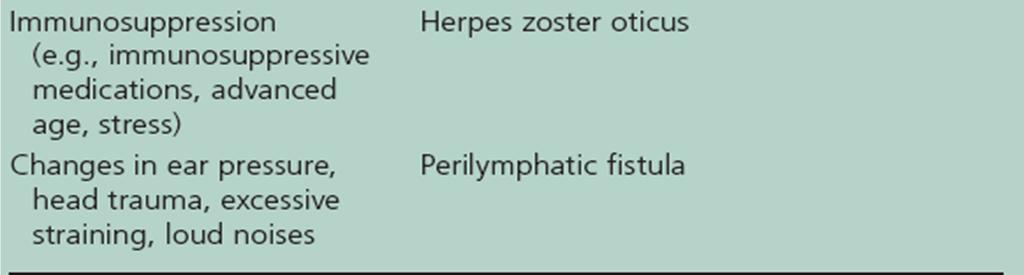
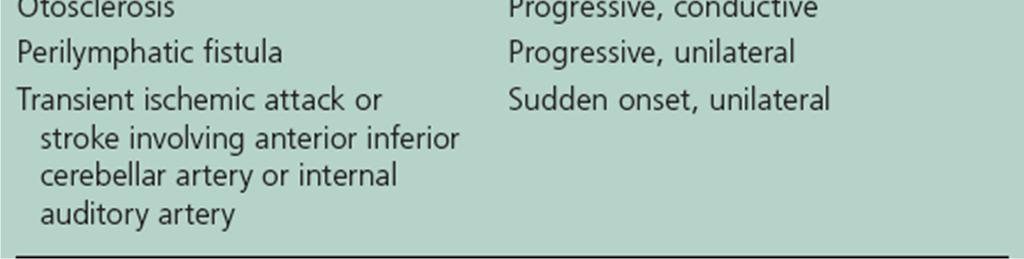
CITY & HACKNEY PATHFINDER CLINICAL COMMISSIONING GROUP. Vertigo. (1) Vertigo. (4) Provisional Diagnosis. (5) Investigations. lasting days or weeks
 Vertigo. (4) Provisional Diagnosis. (5) Investigations. lasting days or weeks") Authors: Dr Lucy O'Rouke and Mr N Eynon-Lewis Review date: January 2017 Vertigo (1) Vertigo (2) History (3) Examination (4) Provisional Diagnosis (5) Investigations (6) Medical Cause (7) Psychiatric Cause
Authors: Dr Lucy O'Rouke and Mr N Eynon-Lewis Review date: January 2017 Vertigo (1) Vertigo (2) History (3) Examination (4) Provisional Diagnosis (5) Investigations (6) Medical Cause (7) Psychiatric Cause
Acute Vestibular Syndrome (AVS) 12/5/2017
 12/5/2017") Sharon Hartman Polensek, MD, PhD Dept of Neurology, Emory University Atlanta VA Medical Center DIAGNOSTIC GROUPS FOR PATIENTS PRESENTING WITH DIZZINESS TO EMERGENCY DEPARTMENTS Infectious 2.9% Genitourinary
Sharon Hartman Polensek, MD, PhD Dept of Neurology, Emory University Atlanta VA Medical Center DIAGNOSTIC GROUPS FOR PATIENTS PRESENTING WITH DIZZINESS TO EMERGENCY DEPARTMENTS Infectious 2.9% Genitourinary
Vertigo: A practical approach to diagnosis and treatment. John Waterston
 Vertigo: A practical approach to diagnosis and treatment John Waterston Background. Vertigo is a symptom that has diverse causes. The diagnosis may remain elusive even after exhaustive clinical enquiry
Vertigo: A practical approach to diagnosis and treatment John Waterston Background. Vertigo is a symptom that has diverse causes. The diagnosis may remain elusive even after exhaustive clinical enquiry
Acoustic neuroma s/p removal BPPV (Crystals)- 50% of people over 65 y/ o with dizziness will have this as main reason for dizziness
- 50% of people over 65 y/ o with dizziness will have this as main reason for dizziness") Dizziness and the Heart Mended Hearts Inservice Karen Hansen, PT, DPT, Cert Vestibular Rehab, CEAS Tennessee Therapy & Balance Center, LLC July 21, 2016 Balance We maintain balance with input from our
Dizziness and the Heart Mended Hearts Inservice Karen Hansen, PT, DPT, Cert Vestibular Rehab, CEAS Tennessee Therapy & Balance Center, LLC July 21, 2016 Balance We maintain balance with input from our
Vertigo. David Clark, DO Oregon Neurology Associates Springfield, OR
 Vertigo David Clark, DO Oregon Neurology Associates Springfield, OR 44F vertigo, nausea & vomiting Unidirectional Nystagmus 44F vertigo, nausea & vomiting Impaired VOR Gain to the right Vertigo History
Vertigo David Clark, DO Oregon Neurology Associates Springfield, OR 44F vertigo, nausea & vomiting Unidirectional Nystagmus 44F vertigo, nausea & vomiting Impaired VOR Gain to the right Vertigo History
The Big 3 of Vertigo
 They feel it, you see it, few know it: Common vertigo conditions seen, but rarely diagnosed Peter Johns MD, FRCPC University of Ottawa pjohns@toh.ca Twitter @peterjohns84 The Big 3 of Vertigo BPPV Vestibular
They feel it, you see it, few know it: Common vertigo conditions seen, but rarely diagnosed Peter Johns MD, FRCPC University of Ottawa pjohns@toh.ca Twitter @peterjohns84 The Big 3 of Vertigo BPPV Vestibular
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 04/26/2014 Radiology Quiz of the Week # 108 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 04/26/2014 Radiology Quiz of the Week # 108 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Speaker Disclosures: 12/4/2015 DIZZINESS AND NEAR SYNCOPE. I have no relevant commercial relationships to disclose
 DIZZINESS AND NEAR SYNCOPE Bernard Gran, M.D. Neurologist, Co-Chief, Department of Neuroscience Baptist Health Neuroscience Center Speaker Disclosures: I have no relevant commercial relationships to disclose
DIZZINESS AND NEAR SYNCOPE Bernard Gran, M.D. Neurologist, Co-Chief, Department of Neuroscience Baptist Health Neuroscience Center Speaker Disclosures: I have no relevant commercial relationships to disclose
Dominic J Mort 23/03/17 Spire Bushey Hospital
 Dominic J Mort 23/03/17 Spire Bushey Hospital Dizziness Good grief! Hx: Pre-syncope Dizziness As if you might faint? Vertigo Mostly about this As if on a merry-go-round? Non-rotational commoner than spinning
Dominic J Mort 23/03/17 Spire Bushey Hospital Dizziness Good grief! Hx: Pre-syncope Dizziness As if you might faint? Vertigo Mostly about this As if on a merry-go-round? Non-rotational commoner than spinning
An Introduction to Dizziness and Vertigo
 An Introduction to Dizziness and Vertigo Tamara Mijovic MD CM FRCSC Clinical Assistant Professor Department of Otolaryngology Head and Neck Surgery Otology, Neurotology & Skull Base Surgery McGill University
An Introduction to Dizziness and Vertigo Tamara Mijovic MD CM FRCSC Clinical Assistant Professor Department of Otolaryngology Head and Neck Surgery Otology, Neurotology & Skull Base Surgery McGill University
Vertigo. Definition Important history questions Examination Common vertigo cases and management Summary
 Vertigo Vertigo Definition Important history questions Examination Common vertigo cases and management Summary Cases 1) 46 year old man presents two weeks after knocking his head with recurrent episodes
Vertigo Vertigo Definition Important history questions Examination Common vertigo cases and management Summary Cases 1) 46 year old man presents two weeks after knocking his head with recurrent episodes
Dizziness Cases. Martin A. Samuels Chair, Department of Neurology Brigham and Women s Hospital Boston
 Dizziness Cases Martin A. Samuels Chair, Department of Neurology Brigham and Women s Hospital Boston Basic Principles Take an open ended history Know the synonyms for dizziness A patient can have more
Dizziness Cases Martin A. Samuels Chair, Department of Neurology Brigham and Women s Hospital Boston Basic Principles Take an open ended history Know the synonyms for dizziness A patient can have more
EMU 2017 DIZZINESS AND VERTIGO Walter Himmel MD
 EMU 2017 DIZZINESS AND VERTIGO Walter Himmel MD There is only one essential challenge in the world of dizziness and vertigo: Don t miss a posterior circulation stroke (vertebral/basilar artery) or TIA.
EMU 2017 DIZZINESS AND VERTIGO Walter Himmel MD There is only one essential challenge in the world of dizziness and vertigo: Don t miss a posterior circulation stroke (vertebral/basilar artery) or TIA.
what is the permanent impact of loss of the vestibular sense? for balance, vision and spatial orientation)
") what is the permanent impact of loss of the vestibular sense? for balance, vision and spatial orientation) loss of speed - poor dynamic vision (daily life) - fear to fall and falls loss of automatisation
what is the permanent impact of loss of the vestibular sense? for balance, vision and spatial orientation) loss of speed - poor dynamic vision (daily life) - fear to fall and falls loss of automatisation
Vestibular Differential Diagnosis
 Vestibular Differential Diagnosis P R E S E N T E D B Y : S H A R I K I C K E R, P T, M P T C E R T I F I C A T E I N V E S T I B U L A R R E H A B I L I T A T I O N 2 0 1 7 L A C E Y H A L E, P T, D P
Vestibular Differential Diagnosis P R E S E N T E D B Y : S H A R I K I C K E R, P T, M P T C E R T I F I C A T E I N V E S T I B U L A R R E H A B I L I T A T I O N 2 0 1 7 L A C E Y H A L E, P T, D P
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Workshop: The Assessment of Patients with Dizziness and Vertigo
 Workshop: The Assessment of Patients with Dizziness and Vertigo Tamara Mijovic MD CM FRCSC Clinical Assistant Professor Department of Otolaryngology Head and Neck Surgery Otology, Neurotology & Skull Base
Workshop: The Assessment of Patients with Dizziness and Vertigo Tamara Mijovic MD CM FRCSC Clinical Assistant Professor Department of Otolaryngology Head and Neck Surgery Otology, Neurotology & Skull Base
The Geriatric Patient The EM Perspective. Advice from a neophyte
 The Geriatric Patient The EM Perspective Advice from a neophyte Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any
The Geriatric Patient The EM Perspective Advice from a neophyte Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any
Vertigo. Definition. Causes. (Dizziness) Benign Paroxysmal Positional Vertigo (BPPV) Labyrinthitis. by Karen Schroeder, MS, RD
 Benign Paroxysmal Positional Vertigo (BPPV) Labyrinthitis. by Karen Schroeder, MS, RD") Vertigo (Dizziness) by Karen Schroeder, MS, RD En Español (Spanish Version) Definition Vertigo is a feeling of spinning or whirling when you are not moving. It can also be an exaggerated feeling of motion
Vertigo (Dizziness) by Karen Schroeder, MS, RD En Español (Spanish Version) Definition Vertigo is a feeling of spinning or whirling when you are not moving. It can also be an exaggerated feeling of motion
Chapter 19 Dizziness and Vertigo
 Chapter 19 Dizziness and Vertigo Episode overview: 1) Compare characteristics of peripheral and central vertigo 2) What are risk factors for central causes of vertigo? 3) List 4 vestibulotoxic drugs. 4)
Chapter 19 Dizziness and Vertigo Episode overview: 1) Compare characteristics of peripheral and central vertigo 2) What are risk factors for central causes of vertigo? 3) List 4 vestibulotoxic drugs. 4)
Because dizziness is an imprecise term, a major role of the clinician is to sort patients out into categories
 Dizziness and Imbalance Timothy C. Hain, MD Clinical Professor of Neurology, Otolaryngology, Physical Therapy Chicago Dizziness and Hearing 645 N. Michigan, Suite 410 312-274-0197 Lecture Goals 1. What
Dizziness and Imbalance Timothy C. Hain, MD Clinical Professor of Neurology, Otolaryngology, Physical Therapy Chicago Dizziness and Hearing 645 N. Michigan, Suite 410 312-274-0197 Lecture Goals 1. What
Differential Diagnosis: Vestibular Pathology. Causes of Dizziness. Benign Paroxysmal Positional Vertigo
 Differential Diagnosis: Vestibular Learning objective: The participant will identify the pathologies associated with complaints of imbalance and dizziness Anne K Galgon PT, PhD, NCS Vestibular and Related
Differential Diagnosis: Vestibular Learning objective: The participant will identify the pathologies associated with complaints of imbalance and dizziness Anne K Galgon PT, PhD, NCS Vestibular and Related
Physical Therapy Examination of the Acutely Vertiginous Patient. Objectives. Prevalence/Incidence of Dizziness 3/20/2018
 Physical Therapy Examination of the Acutely Vertiginous Patient Andrew Wagner, PT, DPT, NCS Jennifer Williams, PT, DPT, NCS April 13, 2018 Objectives The learner will integrate basic examination principles
Physical Therapy Examination of the Acutely Vertiginous Patient Andrew Wagner, PT, DPT, NCS Jennifer Williams, PT, DPT, NCS April 13, 2018 Objectives The learner will integrate basic examination principles
Problem based review: the patient with dizziness on the AMU
 240 Acute Medicine 2012 11(4): 240-245 Trainee Section Problem based review: the patient with dizziness on the AMU A Kennedy & N Cooper Abstract Unsteadiness, balance disturbance, and dizziness are common
240 Acute Medicine 2012 11(4): 240-245 Trainee Section Problem based review: the patient with dizziness on the AMU A Kennedy & N Cooper Abstract Unsteadiness, balance disturbance, and dizziness are common
I m Weak and Dizzy. Dr. Peter J. Lin Director Primary Care Initiative Canadian Heart Research Centre
 I m Weak and Dizzy Dr. Peter J. Lin Director Primary Care Initiative Canadian Heart Research Centre Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied,
I m Weak and Dizzy Dr. Peter J. Lin Director Primary Care Initiative Canadian Heart Research Centre Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied,
VERTIGO. Tuesday 20 th February 2018 Dr Rukhsana Hussain. Disclaimers apply:
 VERTIGO Tuesday 20 th February 2018 Dr Rukhsana Hussain WHAT IS VERTIGO? 4 Vertigo is defined as an illusory sensation of motion of either the self or the surroundings in the absence of true motion. Explaining
VERTIGO Tuesday 20 th February 2018 Dr Rukhsana Hussain WHAT IS VERTIGO? 4 Vertigo is defined as an illusory sensation of motion of either the self or the surroundings in the absence of true motion. Explaining
Sasan Dabiri, MD, Assistant Professor
 Sasan Dabiri, MD, Assistant Professor Department of Otorhinolaryngology Head & Neck Surgery Amir A lam hospital Tehran University of Medical Sciences October 2015 Outlines Anatomy of Vestibular System
Sasan Dabiri, MD, Assistant Professor Department of Otorhinolaryngology Head & Neck Surgery Amir A lam hospital Tehran University of Medical Sciences October 2015 Outlines Anatomy of Vestibular System
Adequacy of Initial History and Physical Examination
 October 13 th 2015 I am an Associate Professor in the Department of Emergency Medicine, University of Ottawa. I have expertise in Emergency Medicine and hold a certificate of special competency with the
October 13 th 2015 I am an Associate Professor in the Department of Emergency Medicine, University of Ottawa. I have expertise in Emergency Medicine and hold a certificate of special competency with the
Update '08: Vestibular and Balance Rehabilitation Therapy
 Update '08: Vestibular and Balance Rehabilitation Therapy In Context with Surgery Medicine & Diet Symptoms of Dizziness Dizziness non-specific term; encompasses any and all of the specific symptoms: Vertigo
Update '08: Vestibular and Balance Rehabilitation Therapy In Context with Surgery Medicine & Diet Symptoms of Dizziness Dizziness non-specific term; encompasses any and all of the specific symptoms: Vertigo
OBJECTIVES BALANCE EVALUATION COMMON CAUSES OF BALANCE DEFICITS POST TBI BRAIN INJURY BALANCE RELATIONSHIP
 OBJECTIVES Understand variables that contribute to balance deficits Understand the relationship between a brain injury and balance Become familiar with the components of a vestibular/balance assessment
OBJECTIVES Understand variables that contribute to balance deficits Understand the relationship between a brain injury and balance Become familiar with the components of a vestibular/balance assessment
OBJECTIVES TYPES OF DIZZINESS TYPES OF DIZZINESS. Type III Disequilibrium. Classifying Common Position Sense Disturbances
 OBJECTIVES Define four major types of dizziness Emphasizing vertigo Describe pathophysiology of dizziness Emphasizing BPPV Review how to cure BPPV How do you know where you are in 3-dimensional space?
OBJECTIVES Define four major types of dizziness Emphasizing vertigo Describe pathophysiology of dizziness Emphasizing BPPV Review how to cure BPPV How do you know where you are in 3-dimensional space?
What Do You Think of My Posterior?
 What Do You Think of My Posterior? Posterior Stroke and Stroke Mimics Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School of Medicine Disclosures
What Do You Think of My Posterior? Posterior Stroke and Stroke Mimics Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School of Medicine Disclosures
Vague Neurological Conditions
 Vague Neurological Conditions Dr. John Lefebre, MD, FRCPC Chief Regional Medical Director Europe, India, South Africa, Middle East and Turkey Canada 2014 2 3 4 Agenda Dr. John Lefebre, M.D., FRCPC 1. TIA
Vague Neurological Conditions Dr. John Lefebre, MD, FRCPC Chief Regional Medical Director Europe, India, South Africa, Middle East and Turkey Canada 2014 2 3 4 Agenda Dr. John Lefebre, M.D., FRCPC 1. TIA
V e r t i g o. T ü n d e. M a g y a r
 V e r t i g o T ü n d e M a g y a r Dizziness Vestibular Proprioception Optic input (afferentation) carries not Optic input (afferentation) carries not synchronizated information to the CNS, but contradictory
V e r t i g o T ü n d e M a g y a r Dizziness Vestibular Proprioception Optic input (afferentation) carries not Optic input (afferentation) carries not synchronizated information to the CNS, but contradictory
Paediatric Balance Assessment
 BAA regional meeting 11 th March 2016 Paediatric Balance Assessment Samantha Lear, Lead Clinical Scientist, Hearing Services, SCH overview The balance system Vestibular disorders referrals Vestibular assessment
BAA regional meeting 11 th March 2016 Paediatric Balance Assessment Samantha Lear, Lead Clinical Scientist, Hearing Services, SCH overview The balance system Vestibular disorders referrals Vestibular assessment
DIZZINESS & VERTIGO A MULTIDISCIPLINARY APPROACH
 DIZZINESS & VERTIGO A MULTIDISCIPLINARY APPROACH Dr DOSH SANDOORAM MB ChB, MD, FRCS Consultant ENT Surgeon, City Clinic Group Labyrinthine disturbance may make one feel like the end of the world has arrived...
DIZZINESS & VERTIGO A MULTIDISCIPLINARY APPROACH Dr DOSH SANDOORAM MB ChB, MD, FRCS Consultant ENT Surgeon, City Clinic Group Labyrinthine disturbance may make one feel like the end of the world has arrived...
Department of Paediatrics Clinical Guideline. Syncope Guideline
 Department of Paediatrics Clinical Guideline Syncope Guideline Definition Transient, self-limited loss of consciousness (TLOC), usually leading to falling. Onset is relatively rapid. Recovery is spontaneous,
Department of Paediatrics Clinical Guideline Syncope Guideline Definition Transient, self-limited loss of consciousness (TLOC), usually leading to falling. Onset is relatively rapid. Recovery is spontaneous,
Predictors of Protracted Recovery
 CONCUSSION MANAGEMENT SPECIALIST ON LINE CURRICULUM Protracted Recovery and Clinical Rehabilitation All rights reserved. Sports Medicine Concepts Concussion Management Specialist Program 1 Predictors of
CONCUSSION MANAGEMENT SPECIALIST ON LINE CURRICULUM Protracted Recovery and Clinical Rehabilitation All rights reserved. Sports Medicine Concepts Concussion Management Specialist Program 1 Predictors of
Control of eye movement
 Control of eye movement Third Nerve Palsy Eye down and out Trochlear Nerve Palsy Note: Right eye Instead of intorsion and depression action of superior oblique See extorsion and elevation Observe how
Control of eye movement Third Nerve Palsy Eye down and out Trochlear Nerve Palsy Note: Right eye Instead of intorsion and depression action of superior oblique See extorsion and elevation Observe how
The evaluation of a patient with dizziness
 The evaluation of a patient with dizziness Kevin A. Kerber and Robert W. Baloh Neurol Clin Pract 2011;1;24 DOI 10.1212/CPJ.0b013e31823d07b6 This information is current as of December 28, 2011 The online
The evaluation of a patient with dizziness Kevin A. Kerber and Robert W. Baloh Neurol Clin Pract 2011;1;24 DOI 10.1212/CPJ.0b013e31823d07b6 This information is current as of December 28, 2011 The online
I m dizzy-what can I expect at my doctor visit? Dennis M. Moore, M.D. Lutheral General
 I m dizzy-what can I expect at my doctor visit? Dennis M. Moore, M.D. Lutheral General Dizziness and Balance is a broad area encompassing multiple fields: primary care (internal medicine, pediatrics),
I m dizzy-what can I expect at my doctor visit? Dennis M. Moore, M.D. Lutheral General Dizziness and Balance is a broad area encompassing multiple fields: primary care (internal medicine, pediatrics),
Nicolas Bianchi M.D. May 15th, 2012
 Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST The Management of Syncope remains a challenge: Clues from the History Richard Sutton, DSc Emeritus Professor of Cardiology Imperial College, St Mary s Hospital, London,
DECLARATION OF CONFLICT OF INTEREST The Management of Syncope remains a challenge: Clues from the History Richard Sutton, DSc Emeritus Professor of Cardiology Imperial College, St Mary s Hospital, London,
Acute Dizziness: Is It a Stroke? Gordon Kelley MD November 2017
 Acute Dizziness: Is It a Stroke? Gordon Kelley MD November 2017 No Disclosures Dizziness Occurs in nearly ¾ of cerebellar strokes 4 categories in classic teaching*: Vertigo Presyncope Imbalance Non-specific
Acute Dizziness: Is It a Stroke? Gordon Kelley MD November 2017 No Disclosures Dizziness Occurs in nearly ¾ of cerebellar strokes 4 categories in classic teaching*: Vertigo Presyncope Imbalance Non-specific
JULY 6 TH GOLDEN PARKK, KOLKATA
 JULY 6 TH 2014- GOLDEN PARKK, KOLKATA ESP - 2014 : INSIGHT "Insight- Connect with the Experts was held at Golden Parkk, Kolkata. It was organized by of Asian Society of Continuing Medical Education collaborating
JULY 6 TH 2014- GOLDEN PARKK, KOLKATA ESP - 2014 : INSIGHT "Insight- Connect with the Experts was held at Golden Parkk, Kolkata. It was organized by of Asian Society of Continuing Medical Education collaborating
MIGRAINE A MYSTERY HEADACHE
 MIGRAINE A MYSTERY HEADACHE The migraine is a chronic neurological disease that is characterized by moderate to severe episodes of headache that is mostly associated with other central nervous system (CNS)
MIGRAINE A MYSTERY HEADACHE The migraine is a chronic neurological disease that is characterized by moderate to severe episodes of headache that is mostly associated with other central nervous system (CNS)
Concurrent Admission Reviews Milliman and Second Level Physician Review Criteria
 Concurrent Admission Reviews Milliman and Second Level Physician Review Criteria Patient Status: Understanding Inpatient and Outpatient Observation Focusing on Chest Pain, TIAs, Syncope and Dizziness Which
Concurrent Admission Reviews Milliman and Second Level Physician Review Criteria Patient Status: Understanding Inpatient and Outpatient Observation Focusing on Chest Pain, TIAs, Syncope and Dizziness Which
Clinical Recommendation: Assessment and Management of Dizziness Associated with Mild TBI
 Clinical Recommendation: Assessment and Management of Dizziness Associated with Mild TBI Learning Objectives Understand an overview of dizziness response following mild TBI Differentiate between three
Clinical Recommendation: Assessment and Management of Dizziness Associated with Mild TBI Learning Objectives Understand an overview of dizziness response following mild TBI Differentiate between three
SIGNS AND SYMPTOMS OF CENTRAL VESTIBULAR DISORDERS
 SIGNS AND SYMPTOMS OF CENTRAL VESTIBULAR DISORDERS By Neil T. Shepard, PhD, CCC-A - Mayo Clinic Emeritus With contributions from Jordan Tucker, PT, DPT [Note: A version of this article was originally published
SIGNS AND SYMPTOMS OF CENTRAL VESTIBULAR DISORDERS By Neil T. Shepard, PhD, CCC-A - Mayo Clinic Emeritus With contributions from Jordan Tucker, PT, DPT [Note: A version of this article was originally published
Dizziness, postural hypotension and postural blackouts: Two cases suggesting multiple system atrophy
 Dizziness, postural hypotension and postural blackouts: Two cases suggesting multiple system atrophy Dr Rahul Chakor, Associate Prof and Head Dept of Neurology, Dr Anand Soni, Senior Resident, T N Medical
Dizziness, postural hypotension and postural blackouts: Two cases suggesting multiple system atrophy Dr Rahul Chakor, Associate Prof and Head Dept of Neurology, Dr Anand Soni, Senior Resident, T N Medical
Suspected neurological conditions: clinical questions
 Suspected neurological clinical questions For questions on signs and symptoms, the committee wanted to consider any studies that determine whether a certain sign or symptom accompanying a main presenting
Suspected neurological clinical questions For questions on signs and symptoms, the committee wanted to consider any studies that determine whether a certain sign or symptom accompanying a main presenting
Difficult Diagnosis: An Interactive Session
 Difficult Diagnosis: An Interactive Session W A D E S M I T H, M. D. D E P T. O F N E U R O L O G Y, U C S F F E B R U A R Y 1 5, 2 0 1 3 58-year-old man with HTN and HLD Recurrent episodes of dizziness
Difficult Diagnosis: An Interactive Session W A D E S M I T H, M. D. D E P T. O F N E U R O L O G Y, U C S F F E B R U A R Y 1 5, 2 0 1 3 58-year-old man with HTN and HLD Recurrent episodes of dizziness
International Journal of Medical and Exercise Science (Multidisciplinary, Peer Reviewed and Indexed Journal)
") ORIGINAL ARTICLE International Journal of Medical and Exercise Science (Multidisciplinary, Peer Reviewed and Indexed Journal) PHYSICAL THERAPY MANAGEMENT IN PATIENTS WITH CERVICOGENIC DIZZINESS-A CASE
ORIGINAL ARTICLE International Journal of Medical and Exercise Science (Multidisciplinary, Peer Reviewed and Indexed Journal) PHYSICAL THERAPY MANAGEMENT IN PATIENTS WITH CERVICOGENIC DIZZINESS-A CASE
Defining Dizziness: An Acute Approach to Vestibular Dysfunction in the Hospital Setting Friday, February 17, :00 AM-10:00 AM
 Defining Dizziness: An Acute Approach to Vestibular Dysfunction in the Hospital Setting Friday, February 17, 2017 8:00 AM-10:00 AM Kerry Lammers, PT, DPT Gabrielle Steinhorn, PT, DPT, NCS Vestibular dysfunction
Defining Dizziness: An Acute Approach to Vestibular Dysfunction in the Hospital Setting Friday, February 17, 2017 8:00 AM-10:00 AM Kerry Lammers, PT, DPT Gabrielle Steinhorn, PT, DPT, NCS Vestibular dysfunction
NIH Public Access Author Manuscript Emerg Med Clin North Am. Author manuscript; available in PMC 2010 February 1.
 NIH Public Access Author Manuscript Published in final edited form as: Emerg Med Clin North Am. 2009 February ; 27(1): 39 viii. doi:10.1016/j.emc.2008.09.002. Vertigo and Dizziness in the Emergency Department
NIH Public Access Author Manuscript Published in final edited form as: Emerg Med Clin North Am. 2009 February ; 27(1): 39 viii. doi:10.1016/j.emc.2008.09.002. Vertigo and Dizziness in the Emergency Department
First a caution. Processes we might NOT try to treat with medications. Processes we might try to treat. Main drug categories.
 Pharmacological Interventions for dizziness Timothy C. Hain, MD Northwestern University Medical School Chicago, Illinois, USA First a caution Torok N. Old and new in Meniere's disease. Laryngoscope 87:1870-1877,
Pharmacological Interventions for dizziness Timothy C. Hain, MD Northwestern University Medical School Chicago, Illinois, USA First a caution Torok N. Old and new in Meniere's disease. Laryngoscope 87:1870-1877,
2/8/2017 WHERE ARE WE? East Amherst East Aurora Hamburg West Seneca Williamsville Boulevard
 2/8/2017 WHERE ARE WE? East Amherst East Aurora Hamburg West Seneca Williamsville Boulevard 1 2/8/2017 MY GOAL TODAY. 1. Provide a quick overview on falls 2. How our balance systems work 3. What treatments
2/8/2017 WHERE ARE WE? East Amherst East Aurora Hamburg West Seneca Williamsville Boulevard 1 2/8/2017 MY GOAL TODAY. 1. Provide a quick overview on falls 2. How our balance systems work 3. What treatments
Labyrinthitis and Vestibular Neuritis
 Labyrinthitis and Vestibular Neuritis http://www.patient.co.uk/health/labyrinthitis-and-vestibular-neuritis.htm Labyrinthitis and vestibular neuritis are most commonly caused by a viral infection that
Labyrinthitis and Vestibular Neuritis http://www.patient.co.uk/health/labyrinthitis-and-vestibular-neuritis.htm Labyrinthitis and vestibular neuritis are most commonly caused by a viral infection that
Dizziness and Vertigo: A Step wise Approach to Evaluation and Management
 Dizziness and Vertigo: A Step wise Approach to Evaluation and Management Jennifer Wipperman, MD, MPH Via Christi Family Medicine Residency University of Kansas School of Medicine Wichita 1 Speaker Disclosure
Dizziness and Vertigo: A Step wise Approach to Evaluation and Management Jennifer Wipperman, MD, MPH Via Christi Family Medicine Residency University of Kansas School of Medicine Wichita 1 Speaker Disclosure
Dizziness, Vertigo, and Syncope: Assessment and treatment
 Dizziness, Vertigo, and Syncope: Assessment and treatment Sally K. Miller, PhD, APRN FNP-BC, AGACNP-BC, AGPCNP-BC Associate Professor University of Nevada Las Vegas School of Nursing Nurse Practitioner
Dizziness, Vertigo, and Syncope: Assessment and treatment Sally K. Miller, PhD, APRN FNP-BC, AGACNP-BC, AGPCNP-BC Associate Professor University of Nevada Las Vegas School of Nursing Nurse Practitioner
Brain and Central Nervous System Cancers
 Brain and Central Nervous System Cancers NICE guidance link: https://www.nice.org.uk/guidance/ta121 Clinical presentation of brain tumours History and Examination Consider immediate referral Management
Brain and Central Nervous System Cancers NICE guidance link: https://www.nice.org.uk/guidance/ta121 Clinical presentation of brain tumours History and Examination Consider immediate referral Management
Understanding Inpatient and Outpatient Observation Status Determination. Focusing on Chest Pain, TIAs, Syncope and Dizziness
 Understanding Inpatient and Outpatient Observation Status Determination Focusing on Chest Pain, TIAs, Syncope and Dizziness Medicare Compliance Inpatient Admissions & Outpatient Observation Monitoring
Understanding Inpatient and Outpatient Observation Status Determination Focusing on Chest Pain, TIAs, Syncope and Dizziness Medicare Compliance Inpatient Admissions & Outpatient Observation Monitoring
First a caution. Processes we might NOT try to treat with medications. Processes we might try to treat. Main drug categories.
 Pharmacological Interventions for dizziness Timothy C. Hain, MD Northwestern University Medical School Chicago, Illinois, USA First a caution Torok N. Old and new in Meniere's disease. Laryngoscope 87:1870-1877,
Pharmacological Interventions for dizziness Timothy C. Hain, MD Northwestern University Medical School Chicago, Illinois, USA First a caution Torok N. Old and new in Meniere's disease. Laryngoscope 87:1870-1877,
Vestibular Symptoms in Concussion: Medical/Surgical Perspective. Jacob R. Brodsky, MD Boston Children s Hospital
 Vestibular Symptoms in Concussion: Medical/Surgical Perspective Jacob R. Brodsky, MD Boston Children s Hospital jacob.brodsky@childrens.harvard.edu On Field Symptoms Headache Dizziness Confusion Fatigue
Vestibular Symptoms in Concussion: Medical/Surgical Perspective Jacob R. Brodsky, MD Boston Children s Hospital jacob.brodsky@childrens.harvard.edu On Field Symptoms Headache Dizziness Confusion Fatigue
Inner Ear Disorders. Information for patients and families
 Inner Ear Disorders Information for patients and families Read this booklet to learn about: What are inner ear disorders Symptoms Tests you may need Treatment options Please visit the UHN Patient Education
Inner Ear Disorders Information for patients and families Read this booklet to learn about: What are inner ear disorders Symptoms Tests you may need Treatment options Please visit the UHN Patient Education
Dizziness: Natural Treatment for Vertigo and BPPV
 Wellness and WBV Studio Home» Bodywork» Massage» CranioSacral Therapy» Dizziness: Natural Treatment for Vertigo and BPPV CRANIOSACRAL THERAPY HOLISTIC HEALING Dizziness: Natural Treatment for Vertigo and
Wellness and WBV Studio Home» Bodywork» Massage» CranioSacral Therapy» Dizziness: Natural Treatment for Vertigo and BPPV CRANIOSACRAL THERAPY HOLISTIC HEALING Dizziness: Natural Treatment for Vertigo and
Medicine Dr. Aso Lecture 9 Syncope and Pre-syncope
 Medicine Dr. Aso Lecture 9 Syncope and Pre-syncope SYNCOPE AND PRE-SYNCOPE Syncope:- sudden, transient loss of consciousness, due to reduced cerebral perfusion. The patient is unresponsive with loss of
Medicine Dr. Aso Lecture 9 Syncope and Pre-syncope SYNCOPE AND PRE-SYNCOPE Syncope:- sudden, transient loss of consciousness, due to reduced cerebral perfusion. The patient is unresponsive with loss of
Steady the dizzy child. Louis M Hofmeyr. (CME, Nov/Dec 2003, Vol 21, No 11.)
") Steady the dizzy child Louis M Hofmeyr (CME, Nov/Dec 2003, Vol 21, No 11.) Dizziness in children can be caused by a variety of peripheral and central vestibular disorders. Although less frequent in children
Steady the dizzy child Louis M Hofmeyr (CME, Nov/Dec 2003, Vol 21, No 11.) Dizziness in children can be caused by a variety of peripheral and central vestibular disorders. Although less frequent in children
Balance Disorders in Adolescents (and Young Adults)
") Balance Disorders in Adolescents (and Young Adults) RCP Conference 18 January 2016 Katherine Harrop-Griffiths Consultant in Audiovestibular Medicine (Paediatric) Royal National Throat, Nose & Ear Hospital
Balance Disorders in Adolescents (and Young Adults) RCP Conference 18 January 2016 Katherine Harrop-Griffiths Consultant in Audiovestibular Medicine (Paediatric) Royal National Throat, Nose & Ear Hospital
Peripheral vestibular disorders will affect 1 of 13 people in their lifetime
 Peripheral vestibular disorders will affect 1 of 13 people in their lifetime 80% of affected persons seek medical consultation Unclear how many of these are for peripheral vs central disorders Generally:
Peripheral vestibular disorders will affect 1 of 13 people in their lifetime 80% of affected persons seek medical consultation Unclear how many of these are for peripheral vs central disorders Generally:
Vestibular System. Dian Yu, class of 2016
 Vestibular System Dian Yu, class of 2016 Objectives 1. Describe the functions of the vestibular system: What is it? How do you stimulate it? What are the consequences of stimulation? 2. Describe the vestibular
Vestibular System Dian Yu, class of 2016 Objectives 1. Describe the functions of the vestibular system: What is it? How do you stimulate it? What are the consequences of stimulation? 2. Describe the vestibular
Syncope By Remus Popa
 Syncope By Remus Popa A 66 years old male is brought to the ED from a restaurant where he fainted while dining out with his family. He complained of nausea and stood up to go to the restroom but immediately
Syncope By Remus Popa A 66 years old male is brought to the ED from a restaurant where he fainted while dining out with his family. He complained of nausea and stood up to go to the restroom but immediately
Dizziness 101 E-Class TAKE HOME POINTS
 Dizziness 101 E-Class Dizziness is one of the most common reasons people seek medical care Important to consider the inner ear as a cause 5.5: Average number of providers seen if the inner ear wasn t considered
Dizziness 101 E-Class Dizziness is one of the most common reasons people seek medical care Important to consider the inner ear as a cause 5.5: Average number of providers seen if the inner ear wasn t considered
Chapter 12 Dizziness and Vertigo
 Chapter 12 Dizziness and Vertigo Jonathan S. Olshaker PERSPECTIVE An estimated 7.5 million patients with dizziness are seen each year in ambulatory care settings. It is one of the most common principal
Chapter 12 Dizziness and Vertigo Jonathan S. Olshaker PERSPECTIVE An estimated 7.5 million patients with dizziness are seen each year in ambulatory care settings. It is one of the most common principal
ETHICAL & RATIONAL MANAGEMENT OF VERTIGO
 ...Pharma Company ETHICAL & RATIONAL MANAGEMENT OF VERTIGO -drugs & other modalities Drugs Maneuvers Physical Therapy Non specific Symptomatic therapy Specific therapy to treat the underlying disorder
...Pharma Company ETHICAL & RATIONAL MANAGEMENT OF VERTIGO -drugs & other modalities Drugs Maneuvers Physical Therapy Non specific Symptomatic therapy Specific therapy to treat the underlying disorder
Acute Vestibular Syndrome (VS or Stroke?) Three-step H.I.N.T.S. eye examination
 Three-step H.I.N.T.S. eye examination") Acute Vestibular Syndrome (VS or Stroke?) Three-step H.I.N.T.S. eye examination Head Impulse (right- and leftward) Nystagmus type Test of Skew (cover test for skew deviation) Stroke findings: I.N.F.A.R.C.T.
Acute Vestibular Syndrome (VS or Stroke?) Three-step H.I.N.T.S. eye examination Head Impulse (right- and leftward) Nystagmus type Test of Skew (cover test for skew deviation) Stroke findings: I.N.F.A.R.C.T.
DOWNLOAD OR READ : VERTIGO AND DIZZINESS REHABILITATION THE MCS METHOD PDF EBOOK EPUB MOBI
 DOWNLOAD OR READ : VERTIGO AND DIZZINESS REHABILITATION THE MCS METHOD PDF EBOOK EPUB MOBI Page 1 Page 2 vertigo and dizziness rehabilitation the mcs method vertigo and dizziness rehabilitation pdf vertigo
DOWNLOAD OR READ : VERTIGO AND DIZZINESS REHABILITATION THE MCS METHOD PDF EBOOK EPUB MOBI Page 1 Page 2 vertigo and dizziness rehabilitation the mcs method vertigo and dizziness rehabilitation pdf vertigo
VESTIBULAR SYSTEM. Deficits cause: Vertigo. Falling Tilting Nystagmus Nausea, vomiting
 VESTIBULAR SYSTEM Objectives: Understand the functions of the vestibular system: What is it? How do you stimulate it? What are the consequences of stimulation? Describe the vestibular apparatus, the 2
VESTIBULAR SYSTEM Objectives: Understand the functions of the vestibular system: What is it? How do you stimulate it? What are the consequences of stimulation? Describe the vestibular apparatus, the 2
LA CLINICA E LA DIAGNOSI DELLA VERTIGINE VASCOLARE
 LA CLINICA E LA DIAGNOSI DELLA VERTIGINE VASCOLARE M. Mandalà Azienda Ospedaliera Universitaria Senese WHY ARE WE SCARED? NEED TO BETTER UNDERSTAND PATHOPHYSIOLOGY WHAT IS KNOWN WHAT IS EFFECTIVE and SIMPLE
LA CLINICA E LA DIAGNOSI DELLA VERTIGINE VASCOLARE M. Mandalà Azienda Ospedaliera Universitaria Senese WHY ARE WE SCARED? NEED TO BETTER UNDERSTAND PATHOPHYSIOLOGY WHAT IS KNOWN WHAT IS EFFECTIVE and SIMPLE
Management of TIA. Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital
 Management of TIA Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital Objectives Definition TIA and stroke TIA: Diagnosis & mimics Risk assessment Referral and emergency management Secondary
Management of TIA Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital Objectives Definition TIA and stroke TIA: Diagnosis & mimics Risk assessment Referral and emergency management Secondary
INCIDENCE OF SUSPECTED OTOLITHIC ABNORMALITIES IN MILD TRAUMATIC BRAIN INJURED VETERANS OBSERVATIONS FROM A LARGE VA POLYTRAUMA NETWORK SITE
 INCIDENCE OF SUSPECTED OTOLITHIC ABNORMALITIES IN MILD TRAUMATIC BRAIN INJURED VETERANS OBSERVATIONS FROM A LARGE VA POLYTRAUMA NETWORK SITE David Domoracki Ph.D. Cleveland VAMC Audiology Service Jennifer
INCIDENCE OF SUSPECTED OTOLITHIC ABNORMALITIES IN MILD TRAUMATIC BRAIN INJURED VETERANS OBSERVATIONS FROM A LARGE VA POLYTRAUMA NETWORK SITE David Domoracki Ph.D. Cleveland VAMC Audiology Service Jennifer
A synopsis of: Diagnosis and Management of Headaches in Adults: A national clinical guideline. Scottish intercollegiate Guidelines Network SIGN
 A synopsis of: Diagnosis and Management of Headaches in Adults: A national clinical guideline Scottish intercollegiate Guidelines Network SIGN November 2008. PETER FRAMPTON MSc MCOptom BAppSc (Optom)(AUS)
A synopsis of: Diagnosis and Management of Headaches in Adults: A national clinical guideline Scottish intercollegiate Guidelines Network SIGN November 2008. PETER FRAMPTON MSc MCOptom BAppSc (Optom)(AUS)
Balance Disorder Spectrum
 Balance Disorder Spectrum Technical Report: January 2018 Professor Andrew Hugill College of Science and Engineering University of Leicester Leicester, UK andrew.hugill@leicester.ac.uk Professor Peter Rea
Balance Disorder Spectrum Technical Report: January 2018 Professor Andrew Hugill College of Science and Engineering University of Leicester Leicester, UK andrew.hugill@leicester.ac.uk Professor Peter Rea
Balance Assessment and Rehabilitation in Audiology. Andy Phillips Director of Therapies and Health Science ABMU Health Board
 Balance Assessment and Rehabilitation in Audiology Andy Phillips Director of Therapies and Health Science ABMU Health Board Balance Mechanism This has 3 components -Sensory Input -Central Processing -Motor
Balance Assessment and Rehabilitation in Audiology Andy Phillips Director of Therapies and Health Science ABMU Health Board Balance Mechanism This has 3 components -Sensory Input -Central Processing -Motor
Development of an RANP role, Acute Medicine. Emily Bury RANP, Acute Medicine
 Development of an RANP role, Acute Medicine Emily Bury RANP, Acute Medicine Background 2010 National Acute Medicine Programme NAMP recommends established the in development of ANP Ireland. posts with emphasis
Development of an RANP role, Acute Medicine Emily Bury RANP, Acute Medicine Background 2010 National Acute Medicine Programme NAMP recommends established the in development of ANP Ireland. posts with emphasis
TIA Transient Ischaemic Attack?
 TIA Transient Ischaemic Attack? OR Transient loss of function (TLOF) Tal Anjum Consultant Stroke Physician, Morriston Hospital Training & education lead, WASP (Welsh Association of Stroke Physicians) Qs.
TIA Transient Ischaemic Attack? OR Transient loss of function (TLOF) Tal Anjum Consultant Stroke Physician, Morriston Hospital Training & education lead, WASP (Welsh Association of Stroke Physicians) Qs.
BPPV and Pitfalls in its Management. Reza Golrokhian Sani MD, Otolaryngologist- Head & Neck Surgeon Otologist & Neurotologist
 BPPV and Pitfalls in its Management Reza Golrokhian Sani MD, Otolaryngologist- Head & Neck Surgeon Otologist & Neurotologist Objectives 1-The best methods of diagnosis of BPV 2-How to differentiate between
BPPV and Pitfalls in its Management Reza Golrokhian Sani MD, Otolaryngologist- Head & Neck Surgeon Otologist & Neurotologist Objectives 1-The best methods of diagnosis of BPV 2-How to differentiate between
ENT in General Practice. Dr Nicky Jacobsen Salaried GP, Cogges Surgery, Witney April 2013
 ENT in General Practice Dr Nicky Jacobsen Salaried GP, Cogges Surgery, Witney April 2013 Clinical Tips Audiology When is it best to refer just for audiology? Reported hearing loss History: no other ass
ENT in General Practice Dr Nicky Jacobsen Salaried GP, Cogges Surgery, Witney April 2013 Clinical Tips Audiology When is it best to refer just for audiology? Reported hearing loss History: no other ass
Management Of Medical Emergencies
 Management Of Medical Emergencies U.S. Aging Population 35 million people (12%) 65 years or older Number will increase by nearly 75% by year 2030 The number of people more than 85 years old will approach
Management Of Medical Emergencies U.S. Aging Population 35 million people (12%) 65 years or older Number will increase by nearly 75% by year 2030 The number of people more than 85 years old will approach
Evaluation of Dizziness and Fainting in Children and Adolescents
 Evaluation of Dizziness and Fainting in Children and Adolescents Collin Cowley, MD - Pediatric Cardiology Lynne Kerr, MD, PhD Pediatric Neurology Chuck Norlin, MD General Pediatrics Bettina Smith Edmondson,
Evaluation of Dizziness and Fainting in Children and Adolescents Collin Cowley, MD - Pediatric Cardiology Lynne Kerr, MD, PhD Pediatric Neurology Chuck Norlin, MD General Pediatrics Bettina Smith Edmondson,
Dizziness and Vertigo: A Step wise Approach to Evaluation and Management
 Saturday CME Lunch Dizziness and Vertigo: A Step wise Approach to Evaluation and Management Jennifer Wipperman, MD, MPH Associate Director, Via Christi Family Medicine Residency Assistant Professor of
Saturday CME Lunch Dizziness and Vertigo: A Step wise Approach to Evaluation and Management Jennifer Wipperman, MD, MPH Associate Director, Via Christi Family Medicine Residency Assistant Professor of
Associated Audiologists, Inc Patient History
 Associated Audiologists, Inc Patient History Patient Name: DOB: Date: Primary Concern: When did your symptoms begin: List the outcomes you hope to achieve from today s appointment: Review of Systems &
Associated Audiologists, Inc Patient History Patient Name: DOB: Date: Primary Concern: When did your symptoms begin: List the outcomes you hope to achieve from today s appointment: Review of Systems &
The Clinical Differentiation of Cerebellar Infarction from Common Vertigo Syndromes
 REVIEW ARTICLE The Clinical Differentiation of from Common Vertigo Syndromes James A. Nelson, MD* Erik Viirre MD, PhD * University of California at San Diego, Department of Emergency Medicine University
REVIEW ARTICLE The Clinical Differentiation of from Common Vertigo Syndromes James A. Nelson, MD* Erik Viirre MD, PhD * University of California at San Diego, Department of Emergency Medicine University
Vestibular Migraine Panel Session. Panelists. Learner Objectives 7/31/2017. Steven Harvey MD. Fallon Schloemer MD.
 Vestibular Migraine Panel Session David R. Friedland MD, PhD Professor and Vice-Chair Chief, Division of Otology and Neuro- Otologic Skull Base Surgery Panelists Steven Harvey MD Neuro-otologist Fallon
Vestibular Migraine Panel Session David R. Friedland MD, PhD Professor and Vice-Chair Chief, Division of Otology and Neuro- Otologic Skull Base Surgery Panelists Steven Harvey MD Neuro-otologist Fallon
9/6/2017. Physical Therapist Role in Management of Concussions. Areas where Physical Therapy Can Help. What is the Vestibular System?
 Physical Therapist Role in Management of Concussions The APTA recognizes that physical therapists are part of the multidisciplinary team of licensed healthcare providers that assist in concussion management,
Physical Therapist Role in Management of Concussions The APTA recognizes that physical therapists are part of the multidisciplinary team of licensed healthcare providers that assist in concussion management,
DIZZINESS Varieties. : Fainting, hypotension : Rotatory, spinning. : Muscular incoordination : Collapse without LOC: ELH : Disturbed awareness
 DIZZINESS Varieties head Syncope Vertigo Dysequilibrium Ataxia Drop attacks Confusion Panic Attacks Non-organic : Fainting, hypotension : Rotatory, spinning : Unsteadiness on moving : Muscular incoordination
DIZZINESS Varieties head Syncope Vertigo Dysequilibrium Ataxia Drop attacks Confusion Panic Attacks Non-organic : Fainting, hypotension : Rotatory, spinning : Unsteadiness on moving : Muscular incoordination