Anaesthesia for spine surgery
|
|
|
- Joseph Brendan Robinson
- 5 years ago
- Views:
Transcription
1 Anaesthesia for spine surgery Dr. Patricia Kan Associate Consultant Department of Anaesthesia and Intensive Care Prince of Wales Hospital Feb 2014
2 Spinal trauma Goals: To prevent secondary injury to spine Ischaemia, hypoxia, inflammation, etc. Cord oedema, Cell death To provide other organ support
3 Focus 1. Airway management 2. Intraoperative measures to prevent secondary injury 3. Positioning 4. Neurophysiological monitoring
4 1. Airway Management Primary survey in ATLS guideline A- Airway maintenance with cervical spine protection B- Breathing and ventilation C- Circulation with hemorrhage control D- Disability (Neurological evaluation) E- Exposure and Environment (Temperature) SCI in up to 2-5% of all major trauma cases Cervical SCI in 10% of head injured patients Level of injury? Neck stable or unstable? Urgency of intubation?



5 Airway management Neck immobilization Neck Collars



6 Spinal board with head restraints

7 Halo Brace


8 How to intubate?
")

9 Neck extension and head elevation (pillow) Greatest motion in occiput-c1 and C1-2 Minimal motion below C4

10
11 Minimize neck movement during intubation Manual in-line stabilization Awake fibreoptic intubation Videolaryngoscope


12 Manual in-line stabilization Head and neck in neutral position Assistant Head of bed: Grasp the mastoid process with the fingertips and cradle the occiput in the palms of their hands Side of bed: Cradle the mastoids and grasp the occiput When MILS is in place, the anterior portion of the cervical collar can be removed. Reapplication of neck collar when airway interventions are complete.





13 Awake fibreoptic intubation
14 Advantages: Minimal neck movement For patients wearing stabilization devices such as halo vests Difficult airway Allows post-intubation neurological assessment Disadvantages Blood in airway Uncooperative/ combative patient Requires expertise/ equipment Time constraints Increase ICP if gag or cough
15 Topicalization of airway LA Regional block +/- Sedation




16 Videolaryngoscope

17 Improved laryngeal visualization Less force used ; Less cervical spine movement


18 Cricoid pressure To prevent aspiration Efficacy controversial In cadavers with C-spine injuries, cricoid pressure did not distract the injured segment.
19 Choice of muscle relaxant Succinlycholine/ Suxamethonium Avoid if spine injury >48 hours Hyperkalaemia
20 Extubation/ Post-op placement Individualized decision Level of injury/ surgical intervention C3-5 diaphragm innervation Difficult airway Prone position facial oedema Type of operation/ intraoperative events Anterior spinal fusion risk of recurrent laryngeal nerve injury, neck haematoma Long operating time Massive blood loss Other co-morbidities/ pre-op status


21
22 2. Secondary injuries Hypoxia Oxygenation, Haemoglobin Ischaemia BP control Hyperglycaemia Hypothermia, Hyperthermia
23 BP control Spinal cord perfusion pressure = Mean arterial pressure cerebrospinal fluid pressure (SCPP=MAP-CSFP) MAP 85mmHg Spinal shock (Acute phase, 4-6weeks) Flaccid paralysis, loss of reflexes below the level of lesion, paralytic ileus, loss of visceral and somatic sensation, vascular tone and vasopressor reflex Neurogenic shock: Bradycardia, Hypotension High cervical lesion First 2 weeks Medication (fluid, vasopressor/inotrope)
24 Autonomic hyperreflexia (chronic phase) Appear 1-3 weeks after injury Stimulation from bladder, bowel, surgical stimulation massive sympathetic response Vasoconstriction below lesion, Hypertension Vasodilatation above lesion, bradycardia, ventricular dysrhythmia, heart block 85% of patient with spinal cord transections above T6 Medications, Arterial line



25 Blood loss
26 Risk factors Procedure characteristics Patient characteristics Surgery for tumour excision Surgery for trauma of spine Surgery for infection (TB, osteomyelitis, etc.) Revision surgery 3 vertebral segments fusion instrumentation Age >70 years old Obesis Patients with known clotting defects Children with neuromuscular scoliosis
27 Minimizing blood loss/ blood transfusion Medication history: Aspirin, NSAID, Plavix, LMWH, Chinese medicine (ginkgo, ginseng, etc.) Careful positioning to avoid impediment of venous drainage and engorgement of the epidural veins Staged operation, pre-op embolization, meticulous haemostasis, etc. Transamine (Tranexamic acid), NovoSeven (recombinant activated factor VII) Rarely: Controlled hypotension, acute normovolemic haemodilution, erythropoietin

28 Cell Saver Collection of blood shed Anticoagulated Filtered for debris and clots Centrifuged Re-suspended in saline

29 3. Positioning
30 Supine, prone, lateral Can be accomplished in different ways Different surgery/ Adequate surgical exposure Level of intervention Different tables/ support devices Intraoperative X-ray Safe!
31 Principles Head and neck support




32 Head and neck support devices
33 Space for endotracheal tube Avoid pressure on eyes Postoperative visual loss Spine, cardiac, head and neck surgeries Uncommon (0.3% in spine surgery)/rare Increased intraocular pressure from prone position, hypotension, anaemia, blood loss >1 L, duration >6 hours Frequent checking, Head up 10 Avoid pinching of the ears Headrest may cause pressure injury of supraorbital nerve Lack of lubrication or coverage of eyes: corneal abrasion
34 Post-operative visual loss Etiology Mechanism Clinical Features Ischemic Optic Neuropathy (ION) Intraop BP Prolonged surgery Blood loss Crystalloid infusion Ischemia Orbital edema stretch and compression of ON Painless Bilateral Light perception Visual fields Central Retinal Artery Occlusion (CRAO) Direct external pressure Emboli Ocular perfusion pressure Painless Unilateral Periorbital swelling or ecchymosis
35 Thoracic compression Increase airway pressure, affect ventilation Decrease venous return, decrease cardiac output
36 Abdominal compression Vertebral venous engorgement More bleeding
37 Nerve injury Brachial plexus stretch or compression the arms at the shoulders must be in 90 degrees or less abduction the elbow in 90 degrees flexion the forearms pronated Ulnar nerve compression: pressure to the olecranon Peroneal nerve compression: pressure over the head of the fibula Lateral femoral cutaneous nerve trauma: pressure over the iliac crest Soft tissue compression injury face, breasts, and genitalia
38 4. Neurophysiological monitoring SSEP (Somatosensory evoked potential) MEP (Motor evoked potential) Wake up test

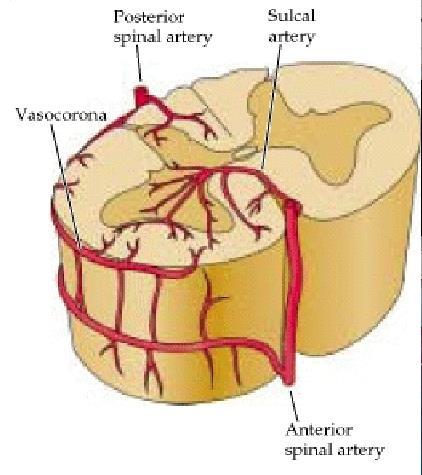
39 Anatomy and Blood Flow
40 SSEP Electrophysiologic response to stimulation 1µV Amplification α N

41 MEP
42 Anaesthetic implications Maintain perfusion pressure Stable physiology Avoid Hypothermia Hypotension Hyperventilation Hypoxia SSEP Propofol Inhalational agents (< 1MAC) MEP Avoid inhalational agents; no muscle relaxation Bite block


43 Bite Block

44 Wake up test Preoperative counseling Careful titration of anaesthetics Bite block
45 Summary 1. Airway management Different ways to perform intubation 2. Intraoperative measures to prevent secondary injury BP, O2, H stix, Temp, Hb 3. Positioning Prone 4. Neurophysiological monitoring May affect choice of anaesthetics

46 The End Thank You
ESCOME Pre-Course Outline (v1.09)
") ESCOME Pre-Course Outline (v1.09) 1. Basics of Spinal Disorders Introduction to Spinal Surgery Spinal Anatomy Introduction to Vertebral Anatomical Concepts Anatomy and Function of Joints and Ligaments
ESCOME Pre-Course Outline (v1.09) 1. Basics of Spinal Disorders Introduction to Spinal Surgery Spinal Anatomy Introduction to Vertebral Anatomical Concepts Anatomy and Function of Joints and Ligaments
Introduction to Emergency Medical Care 1
 Introduction to Emergency Medical Care 1 OBJECTIVES 31.1 Define key terms introduced in this chapter. Slides 13 15, 17, 19, 28 31.2 Describe the components and function of the nervous system and the anatomy
Introduction to Emergency Medical Care 1 OBJECTIVES 31.1 Define key terms introduced in this chapter. Slides 13 15, 17, 19, 28 31.2 Describe the components and function of the nervous system and the anatomy
Disclosures. Closed Claims Reports: Review of Anesthetic Complications. ASA Closed Claims Database. Outline
 Closed Claims Reports: Review of Anesthetic Complications Disclosures Funded by NHLBI & Hamilton Endowment Funds (UCSF Department of Anesthesia). Jae-Woo Lee, MD Associate Professor in Residence University
Closed Claims Reports: Review of Anesthetic Complications Disclosures Funded by NHLBI & Hamilton Endowment Funds (UCSF Department of Anesthesia). Jae-Woo Lee, MD Associate Professor in Residence University
ANESTHESIA EXAM (four week rotation)
") SPARROW HEALTH SYSTEM ANESTHESIA SERVICES ANESTHESIA EXAM (four week rotation) Circle the best answer 1. During spontaneous breathing, volatile anesthetics A. Increase tidal volume and decrease respiratory
SPARROW HEALTH SYSTEM ANESTHESIA SERVICES ANESTHESIA EXAM (four week rotation) Circle the best answer 1. During spontaneous breathing, volatile anesthetics A. Increase tidal volume and decrease respiratory
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
General OR Rotations GOALS & OBJECTIVES
 General OR Rotations GOALS & OBJECTIVES Goals At the end of the CA 1 year General OR rotations, the resident should competently manage uncomplicated ambulatory, orthopedic, maxillo-facial, ENT, gynecologic,
General OR Rotations GOALS & OBJECTIVES Goals At the end of the CA 1 year General OR rotations, the resident should competently manage uncomplicated ambulatory, orthopedic, maxillo-facial, ENT, gynecologic,
1- Prone position implications: Most spine cases are performed with the patient in the
 April 14, 2017 Division of Orthopedic Anesthesia Stony Brook University Medical Center Peri-Operative Anesthesia Protocol for Spine Surgery. Most Commonly performed spine procedures that include SSEP/MEP
April 14, 2017 Division of Orthopedic Anesthesia Stony Brook University Medical Center Peri-Operative Anesthesia Protocol for Spine Surgery. Most Commonly performed spine procedures that include SSEP/MEP
Post-Anesthesia Care In the ICU
 Post-Anesthesia Care In the ICU The following is based on current research and regional standards of care. At completion you will be able to identify Basic equipment needed at the bedside. Aldrete scoring
Post-Anesthesia Care In the ICU The following is based on current research and regional standards of care. At completion you will be able to identify Basic equipment needed at the bedside. Aldrete scoring
11. Spinal cord injury
 11. Spinal cord injury Introduction Always think spinal (vertebral) and/or spinal cord injury (SCI) in children with trauma. Remember SCIWORA cord injury may be present without abnormalities on routine
11. Spinal cord injury Introduction Always think spinal (vertebral) and/or spinal cord injury (SCI) in children with trauma. Remember SCIWORA cord injury may be present without abnormalities on routine
Anaesthetic Plan And The Practical Conduct Of Anaesthesia. Dr.S.Vashisht Hillingdon Hospital
 Anaesthetic Plan And The Practical Conduct Of Anaesthesia Dr.S.Vashisht Hillingdon Hospital Anaesthetic Plan Is based on Age / physiological status of the patient (ASA) Co-morbid conditions that may be
Anaesthetic Plan And The Practical Conduct Of Anaesthesia Dr.S.Vashisht Hillingdon Hospital Anaesthetic Plan Is based on Age / physiological status of the patient (ASA) Co-morbid conditions that may be
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Spinal Cord Injury Transection Injury, Spinal Shock, and Hermiated Disc. Copyright 2014, 2011, 2006 by Saunders, an imprint of Elsevier, Inc.
 Spinal Cord Injury Transection Injury, Spinal Shock, and Hermiated Disc 1 Spinal Cord Injury Results from fracture and/or dislocation of vertebrae // Compresses, stretches, or tears spinal cord Cervical
Spinal Cord Injury Transection Injury, Spinal Shock, and Hermiated Disc 1 Spinal Cord Injury Results from fracture and/or dislocation of vertebrae // Compresses, stretches, or tears spinal cord Cervical
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Profession experiences
 WACHARIN SRISUK Bangkok Hospital Udon,HOD Education :2000 Bachelor of Nursing science, Thai Red Cross College of Nursing Profession experiences :2000-2014 @Professional Orthopaedic OR Nurse at King Chulalongkorn
WACHARIN SRISUK Bangkok Hospital Udon,HOD Education :2000 Bachelor of Nursing science, Thai Red Cross College of Nursing Profession experiences :2000-2014 @Professional Orthopaedic OR Nurse at King Chulalongkorn
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours
 Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
Chapter 26 Head and Spine Trauma The Nervous System The nervous system controls virtually all of our body activities including reflex, voluntary and
 1 2 3 4 5 Chapter 26 Head and Spine Trauma The Nervous System The nervous system controls virtually all of our body activities including reflex, voluntary and involuntary activities Voluntary activities
1 2 3 4 5 Chapter 26 Head and Spine Trauma The Nervous System The nervous system controls virtually all of our body activities including reflex, voluntary and involuntary activities Voluntary activities
American Board of Physical Medicine & Rehabilitation. Part I Curriculum & Weights
 American Board of Physical Medicine & Rehabilitation Part I Curriculum & Weights Neurologic Disorders 30% Stroke Spinal Cord Injury Traumatic Brain Injury Neuropathies a) Mononeuropathies b) Polyneuropathies
American Board of Physical Medicine & Rehabilitation Part I Curriculum & Weights Neurologic Disorders 30% Stroke Spinal Cord Injury Traumatic Brain Injury Neuropathies a) Mononeuropathies b) Polyneuropathies
10. Severe traumatic brain injury also see flow chart Appendix 5
 10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
ANAESTHESIA FOR BLEEDING TONSIL
 ANAESTHESIA FOR BLEEDING TONSIL BY Dr.S.C.Ganeshprabu, MD., D.A., Professor of Anaesthesiology, Madurai Medical College & Govt. Rajaji Hospital, Madurai -652 020. A 5-year-old child who had tonsillectomy
ANAESTHESIA FOR BLEEDING TONSIL BY Dr.S.C.Ganeshprabu, MD., D.A., Professor of Anaesthesiology, Madurai Medical College & Govt. Rajaji Hospital, Madurai -652 020. A 5-year-old child who had tonsillectomy
1. Spinal cord injury mild flexion-extension whiplash ~ complete transection with permanent quadriplegia
 Wk 5. Management of Clients with Neurologic Trauma 1. Spinal cord injury mild flexion-extension whiplash ~ complete transection with permanent quadriplegia most common in cervical, lower thoracic-upper
Wk 5. Management of Clients with Neurologic Trauma 1. Spinal cord injury mild flexion-extension whiplash ~ complete transection with permanent quadriplegia most common in cervical, lower thoracic-upper
Management of Bone and Spinal Cord in Spinal Surgery.
 Management of Bone and Spinal Cord in Spinal Surgery. G. Saló, PhD, MD. Senior Consultant Spine Unit. Hospital del Mar. Barcelona. Ass. Prof. Universitat Autònoma de Barcelona. Introduction The management
Management of Bone and Spinal Cord in Spinal Surgery. G. Saló, PhD, MD. Senior Consultant Spine Unit. Hospital del Mar. Barcelona. Ass. Prof. Universitat Autònoma de Barcelona. Introduction The management
Traumatic Brain Injury
 Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Dr Kelly Jones Anesthesiologist at Northwest Orthopedics
 Dr Kelly Jones Anesthesiologist at Northwest Orthopedics Decrease narcotic use in the immediate post operative period. Better Pain Control Less side effects then General Anesthesia Sedation Post operative
Dr Kelly Jones Anesthesiologist at Northwest Orthopedics Decrease narcotic use in the immediate post operative period. Better Pain Control Less side effects then General Anesthesia Sedation Post operative
Emergency Room Resuscitation of the Unstable Trauma Patient
 Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
Chapter 32. Injuries to the Spine by Pearson Education, Inc. Upper Saddle River, New Jersey
 Chapter Injuries to the Spine Topics Anatomy and physiology of the spine Spinal injuries Guidelines for immobilization Special considerations Enrichment Introduction Injuries to the spine are among the
Chapter Injuries to the Spine Topics Anatomy and physiology of the spine Spinal injuries Guidelines for immobilization Special considerations Enrichment Introduction Injuries to the spine are among the
Chapter 32. Objectives. Objectives 01/09/2013. Spinal Column and Spinal Cord Trauma
 Chapter 32 Spinal Column and Spinal Cord Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1.
Chapter 32 Spinal Column and Spinal Cord Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1.
Trauma Echo PVA. Improving Spinal Cord Injury Acute Management
 Improving Spinal Cord Injury Acute Management William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies Trauma Echo PVA 86 yo PVA
Improving Spinal Cord Injury Acute Management William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies Trauma Echo PVA 86 yo PVA
SPINE EVALUATION AND CLEARANCE Basic Principles
 SPINE EVALUATION AND CLEARANCE Basic Principles General 1. Entire spine is immobilized during primary survey. 2. Radiographic clearance of the spine is not required before emergent surgical procedures.
SPINE EVALUATION AND CLEARANCE Basic Principles General 1. Entire spine is immobilized during primary survey. 2. Radiographic clearance of the spine is not required before emergent surgical procedures.
Intra-operative neurologic injuries: Avoidance and prompt response
 Intra-operative neurologic injuries: Avoidance and prompt response James S. Harrop MD, FACS Professor Neurological and Orthopedic Surgery Director, Division of Spine and Peripheral Nerve Surgery Nsurg
Intra-operative neurologic injuries: Avoidance and prompt response James S. Harrop MD, FACS Professor Neurological and Orthopedic Surgery Director, Division of Spine and Peripheral Nerve Surgery Nsurg
The Case: A 64 yo man with chronic back pain has elective multilevel lumbar spinal surgery
 The Case: A 64 yo man with chronic back pain has elective multilevel lumbar spinal surgery The Case: Upon awakening from anesthesia, he is blind in both eyes After Non-Ocular Surgeries Nancy J. Newman,
The Case: A 64 yo man with chronic back pain has elective multilevel lumbar spinal surgery The Case: Upon awakening from anesthesia, he is blind in both eyes After Non-Ocular Surgeries Nancy J. Newman,
General surgery. Thyroid surgery. Physiological response to pneumoperitoneum. Bowel resection
 General surgery Thyroid surgery Physiological response to pneumoperitoneum Bowel resection General surgery 3.D.9.1 James Mitchell (December 24, 2003) Thyroid surgery Preoperative Assessment Routine, plus
General surgery Thyroid surgery Physiological response to pneumoperitoneum Bowel resection General surgery 3.D.9.1 James Mitchell (December 24, 2003) Thyroid surgery Preoperative Assessment Routine, plus
Chapter 24 Spinal Trauma Introduction to Spinal Injuries (1 of 2) Annually 15,000 permanent spinal cord injuries Commonly men years old
 Annually 15,000 permanent spinal cord injuries Commonly men years old") 1 2 3 4 5 6 7 Chapter 24 Spinal Trauma Introduction to Spinal Injuries (1 of 2) Annually 15,000 permanent spinal cord injuries Commonly men 16-30 years old Mechanism of Injury: Vehicle crashes: 48% : 21%
1 2 3 4 5 6 7 Chapter 24 Spinal Trauma Introduction to Spinal Injuries (1 of 2) Annually 15,000 permanent spinal cord injuries Commonly men 16-30 years old Mechanism of Injury: Vehicle crashes: 48% : 21%
Anaesthesia for major spinal surgery
 Robert WA Nowicki FRCA Matrix reference 2A01, 2A07,3F00 Key points Major spinal surgery is commonly associated with massive haemorrhage. Airway compromise has been reported to occur in up to 1.9% of patients
Robert WA Nowicki FRCA Matrix reference 2A01, 2A07,3F00 Key points Major spinal surgery is commonly associated with massive haemorrhage. Airway compromise has been reported to occur in up to 1.9% of patients
Airway Management. Key points. Rapid Sequence Intubation. Rapid Sequence Intubation Recognizing difficult airway Managing difficult airway
 Airway Management Prasha Ramanujam and Guy Shochat Department of Emergency Medicine UCSF Medical Center Key points Rapid Sequence Intubation Recognizing difficult airway Managing difficult airway Rapid
Airway Management Prasha Ramanujam and Guy Shochat Department of Emergency Medicine UCSF Medical Center Key points Rapid Sequence Intubation Recognizing difficult airway Managing difficult airway Rapid
Anesthesia for Total Hip and Knee Arthroplasty
 Anesthesia for Total Hip and Knee Arthroplasty Typical approach Describe anesthesia technique Rather Describe issues with THA and TKA How anesthesia can modify Issues Total Hip Total Knee Blood Loss ++
Anesthesia for Total Hip and Knee Arthroplasty Typical approach Describe anesthesia technique Rather Describe issues with THA and TKA How anesthesia can modify Issues Total Hip Total Knee Blood Loss ++
1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D.
 1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D. Sacral-coccygeal 2. A 36-year-old male sustains blunt force thoracic
1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D. Sacral-coccygeal 2. A 36-year-old male sustains blunt force thoracic
Thoracic anaesthesia. Simon May
 Thoracic anaesthesia Simon May Contents Indications for lung isolation Ways of isolating lungs Placing a DLT Hypoxia on OLV Suitability for surgery Analgesia Key procedures Indications for lung isolation
Thoracic anaesthesia Simon May Contents Indications for lung isolation Ways of isolating lungs Placing a DLT Hypoxia on OLV Suitability for surgery Analgesia Key procedures Indications for lung isolation
Dr Brigitta Brandner UCLH
 Dr Brigitta Brandner UCLH 2.5% paraplegia/paraparesis (EUROSTAR) Some studies up to 8% Immediate, recurrent and delayed 37% deficits are delayed: present 13 hours 91 days post op >50% will resolve with
Dr Brigitta Brandner UCLH 2.5% paraplegia/paraparesis (EUROSTAR) Some studies up to 8% Immediate, recurrent and delayed 37% deficits are delayed: present 13 hours 91 days post op >50% will resolve with
Shepherd Center: A Catastrophic Care Hospital. The Jane Woodruff Pavilion
 Shepherd Center: A Catastrophic Care Hospital The Jane Woodruff Pavilion Acute Management of SCI & Prevention of Secondary Complications Joycelyn Craig, BSN, RN, CRRN SCI Nurse Education Manager FACTS
Shepherd Center: A Catastrophic Care Hospital The Jane Woodruff Pavilion Acute Management of SCI & Prevention of Secondary Complications Joycelyn Craig, BSN, RN, CRRN SCI Nurse Education Manager FACTS
SHOCK AETIOLOGY OF SHOCK (1) Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function
 Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function") SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT
 PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT Board Approved June 2007 Revised December 2009 Revised July 2011 Revised June 2015 435 Hunter Street Fredericksburg, VA 22401
PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT Board Approved June 2007 Revised December 2009 Revised July 2011 Revised June 2015 435 Hunter Street Fredericksburg, VA 22401
ITLS Pediatric Provider Course Advanced Pre-Test
 ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
MULTIPLE CHOICE. Choose the one alternative that best completes the statement or answers the question.
 EPC Ch 24 Quiz w-key Name MULTIPLE CHOICE. Choose the one alternative that best completes the statement or answers the question. 1) Which of the following best explains the presentation and prognosis of
EPC Ch 24 Quiz w-key Name MULTIPLE CHOICE. Choose the one alternative that best completes the statement or answers the question. 1) Which of the following best explains the presentation and prognosis of
All bedside percutaneously placed tracheostomies
 Page 1 of 5 Scope: All bedside percutaneously placed tracheostomies Population: All ICU personnel Outcomes: To standardize and outline the steps necessary to safely perform a percutaneous tracheostomy
Page 1 of 5 Scope: All bedside percutaneously placed tracheostomies Population: All ICU personnel Outcomes: To standardize and outline the steps necessary to safely perform a percutaneous tracheostomy
European Resuscitation Council
 European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
Slide 1. Slide 2. Slide 3. The Role Of Plastic Surgery In Reducing A Patient s Disability Score A Reconstructive Approach. Peripheral Nerve Surgery
 Slide 1 The Role Of Plastic Surgery In Reducing A Patient s Disability Score A Reconstructive Approach Andrew I. Elkwood MD FACS Director of the Center for Treatment of Paralysis and Reconstructive Nerve
Slide 1 The Role Of Plastic Surgery In Reducing A Patient s Disability Score A Reconstructive Approach Andrew I. Elkwood MD FACS Director of the Center for Treatment of Paralysis and Reconstructive Nerve
EVALUATION OF SELF LEARNING BASED ON WHO MANUAL SURGICAL CARE AT THE DISTRICT HOSPITAL (SCDH)
") EVALUATION OF SELF LEARNING BASED ON WHO MANUAL SURGICAL CARE AT THE DISTRICT HOSPITAL (SCDH) Note: For the answers, refer to the SCDH Manual. The pages listed below each question will contain the answers,
EVALUATION OF SELF LEARNING BASED ON WHO MANUAL SURGICAL CARE AT THE DISTRICT HOSPITAL (SCDH) Note: For the answers, refer to the SCDH Manual. The pages listed below each question will contain the answers,
Anesthetic Techniques in Endoscopic Sinus and Skull Base Surgery
 Anesthetic Techniques in Endoscopic Sinus and Skull Base Surgery Martha Cordoba Amorocho, MD Iuliu Fat, MD Supplement to Cordoba Amorocho M, Fat I. Anesthetic techniques in endoscopic sinus and skull base
Anesthetic Techniques in Endoscopic Sinus and Skull Base Surgery Martha Cordoba Amorocho, MD Iuliu Fat, MD Supplement to Cordoba Amorocho M, Fat I. Anesthetic techniques in endoscopic sinus and skull base
DOCUMENT CONTROL PAGE
 DOCUMENT CONTROL PAGE Title Title: UNDERGOING SPINAL DEFORMITY SURGERY Version: 2 Reference Number: Supersedes Supersedes: all other versions Description of Amendment(s): Revision of analgesia requirements
DOCUMENT CONTROL PAGE Title Title: UNDERGOING SPINAL DEFORMITY SURGERY Version: 2 Reference Number: Supersedes Supersedes: all other versions Description of Amendment(s): Revision of analgesia requirements
Role of IONM in reducing the incidence and severity in pediatric patients with AIS
 Role of IONM in reducing the incidence and severity in pediatric patients with AIS Mohamed Nassef M.D PGY 2 ANESTHESIA McMaster University DEC 9, 2015 Objectives: Literature Review on neurological complications
Role of IONM in reducing the incidence and severity in pediatric patients with AIS Mohamed Nassef M.D PGY 2 ANESTHESIA McMaster University DEC 9, 2015 Objectives: Literature Review on neurological complications
A Patient s Guide to Ulnar Nerve Entrapment at the Wrist (Guyon s Canal Syndrome)
") A Patient s Guide to Ulnar Nerve Entrapment at the Wrist (Guyon s Canal Syndrome) Introduction The ulnar nerve is often called the funny bone at the elbow. However, there is little funny about injury to
A Patient s Guide to Ulnar Nerve Entrapment at the Wrist (Guyon s Canal Syndrome) Introduction The ulnar nerve is often called the funny bone at the elbow. However, there is little funny about injury to
Index. Note: Page numbers of article titles are in bold face type.
 Neurosurg Clin N Am 13 (2002) 259 264 Index Note: Page numbers of article titles are in bold face type. A Abdominal injuries, in child abuse, 150, 159 Abrasions, in child abuse, 157 Abuse, child. See Child
Neurosurg Clin N Am 13 (2002) 259 264 Index Note: Page numbers of article titles are in bold face type. A Abdominal injuries, in child abuse, 150, 159 Abrasions, in child abuse, 157 Abuse, child. See Child
Human Anatomy and Physiology I Laboratory Spinal and Peripheral Nerves and Reflexes
 Human Anatomy and Physiology I Laboratory Spinal and Peripheral Nerves and Reflexes 1 This lab involves the second section of the exercise Spinal Cord, Spinal Nerves, and the Autonomic Nervous System,
Human Anatomy and Physiology I Laboratory Spinal and Peripheral Nerves and Reflexes 1 This lab involves the second section of the exercise Spinal Cord, Spinal Nerves, and the Autonomic Nervous System,
Acute spinal cord injury
 Acute spinal cord injury Thakul Oearsakul Songklanagarind hospital Hat Yai Songkhla Introduction New SCI 10000-12000 cases Approximately 4.0-5.3 per 100000 population Common causes of traumatic SCI :Motor
Acute spinal cord injury Thakul Oearsakul Songklanagarind hospital Hat Yai Songkhla Introduction New SCI 10000-12000 cases Approximately 4.0-5.3 per 100000 population Common causes of traumatic SCI :Motor
OBJECTIVES OF TRAINING FOR THE ANAESTHESIA TERM
 College of Intensive Care Medicine of Australia and New Zealand ABN: 16 134 292 103 Document type: Training Date established: 2007 Date last reviewed: 2014 OBJECTIVES OF TRAINING FOR THE ANAESTHESIA TERM
College of Intensive Care Medicine of Australia and New Zealand ABN: 16 134 292 103 Document type: Training Date established: 2007 Date last reviewed: 2014 OBJECTIVES OF TRAINING FOR THE ANAESTHESIA TERM
Spinal Cord Injuries: The Basics. Kadre Sneddon POS Rounds October 1, 2003
 Spinal Cord Injuries: The Basics Kadre Sneddon POS Rounds October 1, 2003 Anatomy Dorsal columntouch, vibration Corticospinal tract- UMN Anterior horn-lmn Spinothalamic tractpain, temperature (contralateral)
Spinal Cord Injuries: The Basics Kadre Sneddon POS Rounds October 1, 2003 Anatomy Dorsal columntouch, vibration Corticospinal tract- UMN Anterior horn-lmn Spinothalamic tractpain, temperature (contralateral)
Overview. Overview. Chapter 30. Injuries to the Head and Spine 9/11/2012. Review of the Nervous and Skeletal Systems. Devices for Immobilization
 Chapter 30 Injuries to the Head and Spine Slide 1 Overview Review of the Nervous and Skeletal Systems The Nervous System The Skeletal System Devices for Immobilization Cervical Spine Short Backboards Long
Chapter 30 Injuries to the Head and Spine Slide 1 Overview Review of the Nervous and Skeletal Systems The Nervous System The Skeletal System Devices for Immobilization Cervical Spine Short Backboards Long
A Patient s Guide to Intraoperative Monitoring
 A Patient s Guide to Intraoperative Monitoring 228 West Main, Suite C Missoula, MT 59802 Phone: info@spineuniversity.com DISCLAIMER: The information in this booklet is compiled from a variety of sources.
A Patient s Guide to Intraoperative Monitoring 228 West Main, Suite C Missoula, MT 59802 Phone: info@spineuniversity.com DISCLAIMER: The information in this booklet is compiled from a variety of sources.
CARDIAC ARREST IN SPECIAL CIRCUMSTANCES 2
 CARDIAC ARREST IN SPECIAL CIRCUMSTANCES 2 M1 Objectives To understand how resuscitation techniques should be modified in the special circumstances of: Hypothermia Immersion and submersion Poisoning Pregnancy
CARDIAC ARREST IN SPECIAL CIRCUMSTANCES 2 M1 Objectives To understand how resuscitation techniques should be modified in the special circumstances of: Hypothermia Immersion and submersion Poisoning Pregnancy
POSTERIOR CERVICAL FUSION
 AN INTRODUCTION TO PCF POSTERIOR CERVICAL FUSION This booklet provides general information on the Posterior Cervical Fusion (PCF) surgical procedure for you to discuss with your physician. It is not meant
AN INTRODUCTION TO PCF POSTERIOR CERVICAL FUSION This booklet provides general information on the Posterior Cervical Fusion (PCF) surgical procedure for you to discuss with your physician. It is not meant
MD (Anaesthesiology) Title (Plan of Thesis) (Session )
 Title (Plan of Thesis) (Session )") S.No. 1. Comparative Assessment of Sequential organ failure Assessment (SOFA) score and Multiple Organ Dysfunction Score (Mode) in Outcome Prediction among ICU Patients. 2. Comparison of Backpain after
S.No. 1. Comparative Assessment of Sequential organ failure Assessment (SOFA) score and Multiple Organ Dysfunction Score (Mode) in Outcome Prediction among ICU Patients. 2. Comparison of Backpain after
Spinal Column. Anatomy Of The Spine
 Anatomy Of The Spine The spine is a flexible column, composed of a stack of individual bones. Each bone is called a vertebra. There are seven vertebrae in the neck (cervical vertebrae) twelve in the thoracic
Anatomy Of The Spine The spine is a flexible column, composed of a stack of individual bones. Each bone is called a vertebra. There are seven vertebrae in the neck (cervical vertebrae) twelve in the thoracic
Section 11: Nerve damage associated with an operation under general anaesthetic
 Risks associated with your anaesthetic Section 11: Nerve damage associated with an operation under Summary This leaflet explains why it is possible that some nerve damage may occur during your. This is
Risks associated with your anaesthetic Section 11: Nerve damage associated with an operation under Summary This leaflet explains why it is possible that some nerve damage may occur during your. This is
Perioperative Visual Loss
 Perioperative Visual Loss Associated with Spine Surgery Agina M. Kempen, CRNA Chief Nurse Anesthetist St. Clair Hospital Pittsburgh, PA Website/Resources: www.asaclosedclaims.org Miller s s Anesthesia
Perioperative Visual Loss Associated with Spine Surgery Agina M. Kempen, CRNA Chief Nurse Anesthetist St. Clair Hospital Pittsburgh, PA Website/Resources: www.asaclosedclaims.org Miller s s Anesthesia
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #3 Penetrating Neck Trauma
 McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #3 Penetrating Neck Trauma Penetrating neck injury (PNI) comprises 5 to 10 percent of traumatic injuries
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #3 Penetrating Neck Trauma Penetrating neck injury (PNI) comprises 5 to 10 percent of traumatic injuries
SCIENTIFIC PROGRAMME
 SCIENTIFIC PROGRAMME LEARNING OUTCOMES: SESSION 1 PRINCIPLES OF SPINAL DEFORMITY Scoliosis: Aetiology & Prognostic Factors Describe the aetiology and prognostic factors associated with o idiopathic scoliosis
SCIENTIFIC PROGRAMME LEARNING OUTCOMES: SESSION 1 PRINCIPLES OF SPINAL DEFORMITY Scoliosis: Aetiology & Prognostic Factors Describe the aetiology and prognostic factors associated with o idiopathic scoliosis
CrackCast Episode 8 Brain Resuscitation
 CrackCast Episode 8 Brain Resuscitation Episode Overview: 1) Describe 6 therapeutic interventions for the post-arrest brain 2) List 5 techniques for initiating therapeutic hypothermia 3) List 4 mechanisms
CrackCast Episode 8 Brain Resuscitation Episode Overview: 1) Describe 6 therapeutic interventions for the post-arrest brain 2) List 5 techniques for initiating therapeutic hypothermia 3) List 4 mechanisms
LABETTE COMMUNITY COLLEGE BRIEF SYLLABUS. Please check with the LCC bookstore for the required texts for this class.
 LABETTE COMMUNITY COLLEGE BRIEF SYLLABUS SPECIAL NOTE: This brief syllabus is not intended to be a legal contract. A full syllabus will be distributed to students at the first class session. TEXT AND SUPPLEMENTARY
LABETTE COMMUNITY COLLEGE BRIEF SYLLABUS SPECIAL NOTE: This brief syllabus is not intended to be a legal contract. A full syllabus will be distributed to students at the first class session. TEXT AND SUPPLEMENTARY
The Upper Limb III. The Brachial Plexus. Anatomy RHS 241 Lecture 12 Dr. Einas Al-Eisa
 The Upper Limb III The Brachial Plexus Anatomy RHS 241 Lecture 12 Dr. Einas Al-Eisa Brachial plexus Network of nerves supplying the upper limb Compression of the plexus results in motor & sensory changes
The Upper Limb III The Brachial Plexus Anatomy RHS 241 Lecture 12 Dr. Einas Al-Eisa Brachial plexus Network of nerves supplying the upper limb Compression of the plexus results in motor & sensory changes
Regional Anesthesia. Fatiş Altındaş Dept. of Anesthesiology
 Regional Anesthesia Fatiş Altındaş Dept. of Anesthesiology Regional anesthesia - Definition Renders a specific area of the body, e.g. foot, arm, lower extremities insensating to stimulus of surgery or
Regional Anesthesia Fatiş Altındaş Dept. of Anesthesiology Regional anesthesia - Definition Renders a specific area of the body, e.g. foot, arm, lower extremities insensating to stimulus of surgery or
MD (Anaesthesiology) Title (Plan of Thesis) (Session )
 Title (Plan of Thesis) (Session )") S.No. 1. To study the occurrence of postoperative hyponatremia in paediatric patients under 2 years of age 2. Influence of timing of intravenous fluid therapy on maternal hemodynamics in patients undergoing
S.No. 1. To study the occurrence of postoperative hyponatremia in paediatric patients under 2 years of age 2. Influence of timing of intravenous fluid therapy on maternal hemodynamics in patients undergoing
Milestone Guide. CBD Anesthesia
 Table of Contents Department of Anesthesiology Foundations 1 Airway 1 Pharmacology 1 Physiology 1 Common Uncomplicated Anesthetics Practice 2 Obstetrics 2 Pain 2 Core 3 Perioperative Medicine 3 Complex
Table of Contents Department of Anesthesiology Foundations 1 Airway 1 Pharmacology 1 Physiology 1 Common Uncomplicated Anesthetics Practice 2 Obstetrics 2 Pain 2 Core 3 Perioperative Medicine 3 Complex
NVM5 NERVE MONITORING SYSTEM AN INTRODUCTION TO
 AN INTRODUCTION TO NVM5 NERVE MONITORING SYSTEM This booklet is designed to inform you about the use of NVM5 nerve monitoring in the course of your surgery. It is not meant to replace any personal conversations
AN INTRODUCTION TO NVM5 NERVE MONITORING SYSTEM This booklet is designed to inform you about the use of NVM5 nerve monitoring in the course of your surgery. It is not meant to replace any personal conversations
Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH
 Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH Intended learning outcomes Describe the components of a comprehensive clinician
Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH Intended learning outcomes Describe the components of a comprehensive clinician
DISCLOSURE. A Closed Claims Search. Positioning is Important! Occult Risk of Perioperative Injury to The Cervical Spinal Cord
 Bleeding Is Not The Only Complication What Other Minefields are Out There? Degenerative Disease of the Spine May Place Patients at Risk in Absence of Instability DANIEL JANIK, MD ASSOCIATE PROFESSOR UNIVERSITY
Bleeding Is Not The Only Complication What Other Minefields are Out There? Degenerative Disease of the Spine May Place Patients at Risk in Absence of Instability DANIEL JANIK, MD ASSOCIATE PROFESSOR UNIVERSITY
Shenandoah Co. Fire & Rescue. Injuries to. and Spine. December EMS Training Bill Streett Training Section Chief
 Shenandoah Co. Fire & Rescue Injuries to the Head and Spine December EMS Training Bill Streett Training Section Chief C.E. Card Information BLS Providers 2 Cards / Provider Category 1 Course # Blank Topic#
Shenandoah Co. Fire & Rescue Injuries to the Head and Spine December EMS Training Bill Streett Training Section Chief C.E. Card Information BLS Providers 2 Cards / Provider Category 1 Course # Blank Topic#
Med 536 Communicating About Prognosis Workshop. Case 1
 Med 536 Communicating About Prognosis Workshop Case 1 ID / CC: 39 year-old woman status-post motor-vehicle collision History of the Presenting Illness Previously healthy 39 year-old woman was found in
Med 536 Communicating About Prognosis Workshop Case 1 ID / CC: 39 year-old woman status-post motor-vehicle collision History of the Presenting Illness Previously healthy 39 year-old woman was found in
ANAESTHESIA EDY SUWARSO
 ANAESTHESIA EDY SUWARSO GENERAL REGIONAL LOCAL ANAESTHESIA WHAT DOES ANESTHESIA MEAN? The word anaesthesia is derived from the Greek: meaning insensible or without feeling. The adjective will be ANAESTHETIC.
ANAESTHESIA EDY SUWARSO GENERAL REGIONAL LOCAL ANAESTHESIA WHAT DOES ANESTHESIA MEAN? The word anaesthesia is derived from the Greek: meaning insensible or without feeling. The adjective will be ANAESTHETIC.
8th Annual NKY TBI Conference 3/28/2014
 Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services OBJECTIVES DEFINITION 11/8/2017. Identify SCIWORA.
 SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services Identify SCIWORA. OBJECTIVES Identify the population at risk. To identify anatomic and physiologic reasons for SCIWORA. To
SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services Identify SCIWORA. OBJECTIVES Identify the population at risk. To identify anatomic and physiologic reasons for SCIWORA. To
Head Trauma Protocol
 Injuries to the head may cause underlying brain tissue damage. Increased intracranial pressure from bleeding or swelling tissue is a common threat after head trauma. Common signs and symptoms of increased
Injuries to the head may cause underlying brain tissue damage. Increased intracranial pressure from bleeding or swelling tissue is a common threat after head trauma. Common signs and symptoms of increased
SPINAL IMMOBILIZATION
 Spinal Immobilization Decision Assessment Recent studies have shown an increase in mortality for patients with isolated penetrating trauma who are spinally immobilized. Therefore spinal immobilization
Spinal Immobilization Decision Assessment Recent studies have shown an increase in mortality for patients with isolated penetrating trauma who are spinally immobilized. Therefore spinal immobilization
Index. Note: Page numbers of article titles are in boldface type
 Index Note: Page numbers of article titles are in boldface type A Acute coronary syndrome, perioperative oxygen in, 599 600 Acute lung injury (ALI). See Lung injury and Acute respiratory distress syndrome.
Index Note: Page numbers of article titles are in boldface type A Acute coronary syndrome, perioperative oxygen in, 599 600 Acute lung injury (ALI). See Lung injury and Acute respiratory distress syndrome.
Injuries to the Head and Spine
 Injuries to the Head and Spine Anatomy Review Skull Protects the brain Made up of several bones with seam like sutures Regions of the scalp-frontal, occipital, parietal, temporal Bones of face Orbits Mandible
Injuries to the Head and Spine Anatomy Review Skull Protects the brain Made up of several bones with seam like sutures Regions of the scalp-frontal, occipital, parietal, temporal Bones of face Orbits Mandible
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials
 Preparatory Materials") Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
PNS and ANS Flashcards
 1. Name several SOMATIC SENSES Light touch (being touched by a feather), heat, cold, vibration, pressure, pain are SOMATIC SENSES. 2. What are proprioceptors; and how is proprioception tested? PROPRIOCEPTORS
1. Name several SOMATIC SENSES Light touch (being touched by a feather), heat, cold, vibration, pressure, pain are SOMATIC SENSES. 2. What are proprioceptors; and how is proprioception tested? PROPRIOCEPTORS
SUBJECT: Clinical Practice Guideline for the Management of Severe Traumatic Brain Injury
 ASPIRUS WAUSAU HOSPITAL, INC. Passion for excellence. Compassion for people. Effective Date: December 1, 2005 Proposed By: Samuel Picone III, MD, Trauma Medical Director Approval and Dates: Dr. Bunch,
ASPIRUS WAUSAU HOSPITAL, INC. Passion for excellence. Compassion for people. Effective Date: December 1, 2005 Proposed By: Samuel Picone III, MD, Trauma Medical Director Approval and Dates: Dr. Bunch,
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Case 1. Case 5/30/2013. Traumatic Brain Injury : Review, Update, and Controversies
 Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Spinal nerves. Aygul Shafigullina. Department of Morphology and General Pathology
 Spinal nerves Aygul Shafigullina Department of Morphology and General Pathology Spinal nerve a mixed nerve, formed in the vicinity of an intervertebral foramen, where fuse a dorsal root and a ventral root,
Spinal nerves Aygul Shafigullina Department of Morphology and General Pathology Spinal nerve a mixed nerve, formed in the vicinity of an intervertebral foramen, where fuse a dorsal root and a ventral root,
A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH)
") A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH) 6565 Fannin Street Houston, TX 77030 Phone: 713-790-3333 DISCLAIMER: The information in this booklet is compiled from a variety of sources.
A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH) 6565 Fannin Street Houston, TX 77030 Phone: 713-790-3333 DISCLAIMER: The information in this booklet is compiled from a variety of sources.
R Adams Cowley Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland.
 R Adams Cowley 1917 -- 1991 Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland. ...That the primary purpose of medicine was to save lives, that every critically
R Adams Cowley 1917 -- 1991 Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland. ...That the primary purpose of medicine was to save lives, that every critically
Prehospital Care Bundles
 Prehospital s The MLREMS Prehospital s have been created to provide a simple framework to help EMS providers identify the most critical elements when caring for a patient. These bundles do not replace
Prehospital s The MLREMS Prehospital s have been created to provide a simple framework to help EMS providers identify the most critical elements when caring for a patient. These bundles do not replace
PATIENT: DOB: TODAY S DATE:
 1. I have been strongly advised to carefully read and consider this operative permit. I realize that it is important that I understand this material. I also understand that if certain sections are not
1. I have been strongly advised to carefully read and consider this operative permit. I realize that it is important that I understand this material. I also understand that if certain sections are not
Subaxial Cervical Spine Trauma Dr Hesarikia BUMS
 Subaxial Cervical Spine Trauma Dr. Hesarikia BUMS Subaxial Cervical Spine From C3-C7 ROM Majority of cervical flexion Lateral bending Approximately 50% rotation Ligamentous Anatomy Anterior ALL, PLL, intervertebral
Subaxial Cervical Spine Trauma Dr. Hesarikia BUMS Subaxial Cervical Spine From C3-C7 ROM Majority of cervical flexion Lateral bending Approximately 50% rotation Ligamentous Anatomy Anterior ALL, PLL, intervertebral
Preoperative assessment of a patient for carotid endarterectomy
 Vascular Carotid endarterectomy Preoperative assessment of a patient for carotid endarterectomy Abdominal aortic aneuysm Thoracic aortic aneurysms Vascular 3.D.2.1 James Mitchell (December 24, 2003) Carotid
Vascular Carotid endarterectomy Preoperative assessment of a patient for carotid endarterectomy Abdominal aortic aneuysm Thoracic aortic aneurysms Vascular 3.D.2.1 James Mitchell (December 24, 2003) Carotid
Injuries to the head and spine
 Injuries to the head and spine Aaron J. Katz, AEMT-P, CIC www.es26medic.net 2013 Nervous System Two sub-systems Central Nervous System ( CNS ) Brain and spinal cord Peripheral Nervous System 12 cranial
Injuries to the head and spine Aaron J. Katz, AEMT-P, CIC www.es26medic.net 2013 Nervous System Two sub-systems Central Nervous System ( CNS ) Brain and spinal cord Peripheral Nervous System 12 cranial