SUDDEN CARDIAC DEATH IN ATHLETES
|
|
|
- Darcy Johnston
- 5 years ago
- Views:
Transcription
1 SUDDEN CARDIAC DEATH IN ATHLETES Alix Dufresne, MD, FACP, FACC, FESC Cardiology Division Chief, Interfaith Medical Center Director Cardiology Clinic, Kingsbrook Jewish Center
2 PURPOSE AND OBJECTIVES PURPOSE The goal of the presentation is to review the most common pathologies seen in the USA that can lead to sudden death and consider the necessary steps to prevent such a bleak outcome OBJECTIVES Identify normal EKG variants in young athletes Be able to stratify patients at high risk of sudden death Be familiar with the latest available tools to present sudden cardiac death FINANCIAL DISCLOSURE None
3 EPIDEMIOLOGY College and Professional Athletes 500,000 participants each year Competitive Athletics: Several million high school students participate in competitive athletics each year in the United States Organized Sports Participation 25 million children and young adults
4 SUDDEN DEATH IN ATHLETES In the United States, the incidence of SCD averages 0.5 per 100, 000 athletes a year Similar to the current incidence in Italy This incidence has been relatively stable over time in the United States but has decreased in Italy. The incidence of SCD increases as people age due to the expanding prevalence of CAD.

5 Number of cardiovascular (CV), trauma-related, and other sudden death events in 1866 young competitive athletes, tabulated by year Maron, B. J. et al. Circulation 2009;119: Copyright 2009 American Heart Association
6 Basketball Football Track Soccer Baseball Swimming SCD BY SPORTS No of athletes 0 Maron BJ et al, JAMA 1996 ; 276 :
7 INCIDENCE OF NCAA SCD BY SPORT Harmon, K. G. et al. Circulation 2011;123:
8 CAUSES OF SCD IN ATHLETES In athletes with SCD, most patients have underlying structural heart disease The most common cause in the US is hypertrophic cardiomyopathy (HCM). Commotio cordis is the second most common etiology in the United States. accounts for nearly 20% of SCD in athletes LQTS, coronary artery anomalies, myocarditis, Marfan syndrome, arrhythmogenic right ventricular cardiomyopathy (ARVC), valvular disease, and dilated cardiomyopathies account for most of the remaining underlying heart disease.
9 Table 1. Cardiovascular causes of exercise-related SCD in young athletes. Van Camp et al.[8] (n = 100), % Maron et al.[9] (n = 134), % Corrado et al. (25) (n = 55), % Hypertrophic cardiomyopathy Probable hypertrophic cardiomyopathy 5 10 Coronary anomalies Valvular and subvalvular aortic stenosis 8 4 Possible myocarditis Dilated and nonspecific cardiomyopathy Atherosclerotic CAD Aortic dissection/rupture Arrhythmogenic right ventricular cardiomyopathy Myocardial scarring 3 Mitral valve prolapse Other congenital abnormalities 1.5 Long-QT syndrome Wolff-Parkinson-White syndrome 1 1 Cardiac conduction disease 3 Cardiac sarcoidosis 0.5 Coronary artery aneurysm 1 Normal heart at necropsy Pulmonary thromboembolism 1

10 Table 1. Causes of Sudden Cardiac Death in the Young

11 Table 2. Genetic Causes of Sudden Cardiac Death in the Young

12 Flow diagram summarizing causes of death in 1866 young competitive athletes Maron, B. J. et al. Circulation 2009;119: Copyright 2009 American Heart Association

13 Causes of sudden death in National Collegiate Athletic Association athletes, 2004 to 2008 Harmon, K. G. et al. Circulation 2011;123: Copyright 2011 American Heart Association
14 RELATIVE INCIDENCE OF UNDERLYING DISEASES IN SUDDEN CARDIAC DEATH OF ATHLETES In Italian series of SCD in athletes, ARVC is the most common underlying heart disease. HCM accounts for a much lower percentage perhaps related to the screening process, a lower underlying genetic penetration, or less-lethal forms of the gene or disease.
15 RELATIVE INCIDENCE OF UNDERLYING DISEASES IN SUDDEN CARDIAC DEATH OF ATHLETES In non-athletic populations such as the military and general public, the causes of SCD in the young are less commonly cardiomyopathies and more commonly myocarditis, anomalous coronary arteries, and CAD.
16 Gray Area of Overlap between Athlete's Heart and Cardiomyopathies, Including Myocarditis, Hypertrophic Cardiomyopathy, and Arrhythmogenic Right Ventricular Cardiomyopathy. Maron BJ. N Engl J Med 2003;349:
17

18 HCM VS. ATHLETE S HEART Circulation 1995;91.

19
20 ABNORMALITIES POINTING TO POSSIBLY INCREASED SUDDEN-DEATH RISK IN THE SEATTLE CRITERIA INCLUDE: T-wave inversion (defined as >1 mm in depth in two or more of leads V2-V6, II and avf, or I and avl). Long QT interval (corrected QT [QTc] >470 ms in men, >480 ms in women ). Short QT interval (QTc <320 ms). ST-segment depression (>0.5 mm in two or more leads). Pathologic Q waves (>3 mm in depth or >40 ms in duration in two or more leads, excluding III and avr). Left atrial enlargement (P-wave duration >120 ms in leads I or II with negative portion of the P wave >1 mm in depth and >40 ms in duration in lead V1). Right ventricular hypertrophy (R-V1 + S-V5 >10.5 mm plus right axis deviation >120 )..
21 Compete left bundle branch block (LBBB) or any QRS >140ms Mobitz type II 2 AV block or complete heart block. Ventricular preexcitation (PR interval <120 ms with a delta wave and QRS >120 ms). Profound sinus bradycardia defined as <30 beats per minute or sinus pauses >3 s. Atrial tachyarrhythmias (supraventricular tachycardia or atrial fibrillation or flutter). Premature ventricular contractions (>2 per 10 second tracing), ventricular arrhythmias (couplets, nonsustained VT). Type 1 Brugada pattern.
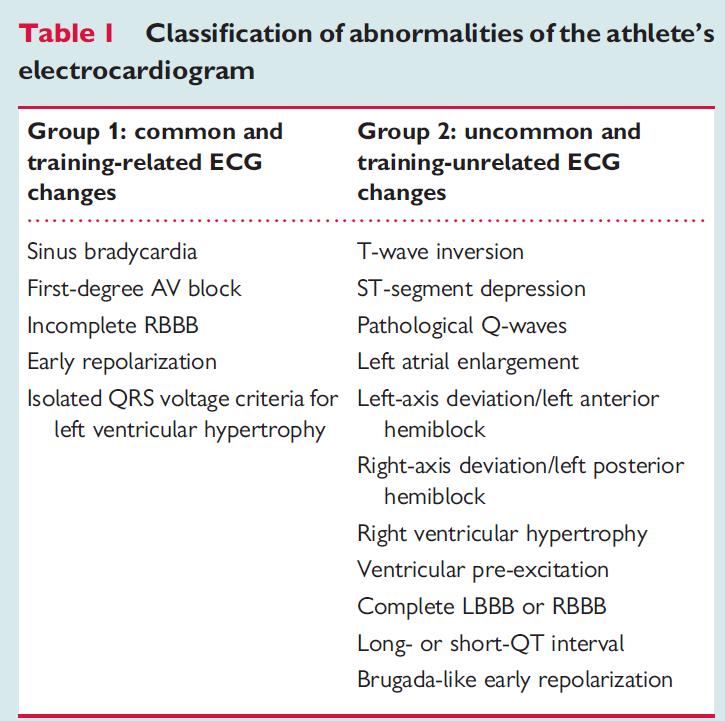
22 ELECTROCARDIOGRAM IN ATHLETES Abnormalities in ECGs of athletes are common. In the Corrado screening series published in 1998, nearly 10% of their subjects who wished to begin an athletic program or who were involved in an athletic program had abnormal ECGs. Sinus bradycardia, first-degree heart block, and second-degree heart block are common, as are early repolarization and isolated voltage criteria for left ventricular hypertrophy.
23 ELECTROCARDIOGRAM IN ATHLETES Abnormal vs normal variant Distinguishing the atypical ECG of a young athlete from truly abnormal ECG results is very important Complete evaluation of the heart (echocardiography, MRI, CT, stress test,etc) in every one of these athletes could not be justified on the basis of cost
24
25 ELECTROCARDIOGRAM IN ATHLETES Atrioventricular block First-degree AV block and Mobitz Type I (Wenkebach) second degree AV block are common in trained athletes, being present 35 and 10% of athlete s ECGs, respectively. AV conduction slowing and block are mediated by increased parasympathetic tone and/or decreased resting sympathetic tone. Second-degree Mobitz Type II and third-degree heart block are rare in the athlete and caution should be used in accepting these findings as normal adaptive changes to training.
26 ELECTROCARDIOGRAM IN ATHLETES Isolated increase of QRS voltages Physiological LV hypertrophy in trained athletes usually manifests as an isolated increase of QRS amplitude, with normal QRS axis, normal atrial and ventricular activation patterns, and normal ST-segment T-wave repolarization. A high prevalence of ECGs that fulfill Sokolow Lyon voltage criteria for LV hypertrophy has been consistently reported in trained athletes. Non-voltage ECG criteria for LV hypertrophy such as atrial enlargement, left-axis deviation, a strain pattern of repolarization, and delayed intrinsicoid deflection are not usually seen in athletes.
27 ELECTROCARDIOGRAM IN ATHLETES The prevalence of incomplete RBBB has been estimated to range from 35 to 50% in athletes compared with less than 10% in young, healthy controls. The ECG pattern is more often noted in athletes engaged in endurance sports, with a male preponderance. Right ventricular conduction delay is most likely not within the conduction system, but as a result of increased conduction time across the RV due to the physiologically enlarged RV cavity size/increased cardiac muscle mass The RBBB morphology has been shown to be reversible with deconditioning
28 ELECTROCARDIOGRAM IN ATHLETES Incomplete RBBB should be differentiated from ARVC and Brugada ECG ARVC should be suspected when the pattern of incomplete RBBB is associated with T-wave inversion extending beyond V2 to include leads V3 and V4 or in the presence of premature ventricular beats with a left bundle branch block (LBBB) morphology. Brugada-ECG is characterized by a slow, positive deflection at the R-ST junction ( J-wave ), which is most evident in leads V1 and V2, with minimal or no reciprocal changes in other leads Unlike the R -wave seen in RBBB, the J-wave seen in Brugada syndrome does not indicate delayed RV activation, but reflects early repolarization with J-point elevation and a high take-off ST-segment. The down-sloping ST-segment is followed by a negative ( coved type) or a positive ( saddle-back type) T-wave.

29 BRUGADA ECG PATTERN
30 EPSILON WAVE
31 EARLY REPOLARIZATION Traditionally been regarded as an idiopathic and benign ECG phenomenon, with an estimated prevalence in healthy young individuals of 1 2%, and a clear male preponderance. The early repolarization ECG pattern is observed in 50 80% of resting ECGs among highly trained athletes The early repolarization ECG shows elevation of J-point of at least 0.1 mv from baseline, associated with notching or slurring of the terminal QRS complex which may vary in location, morphology, and degree
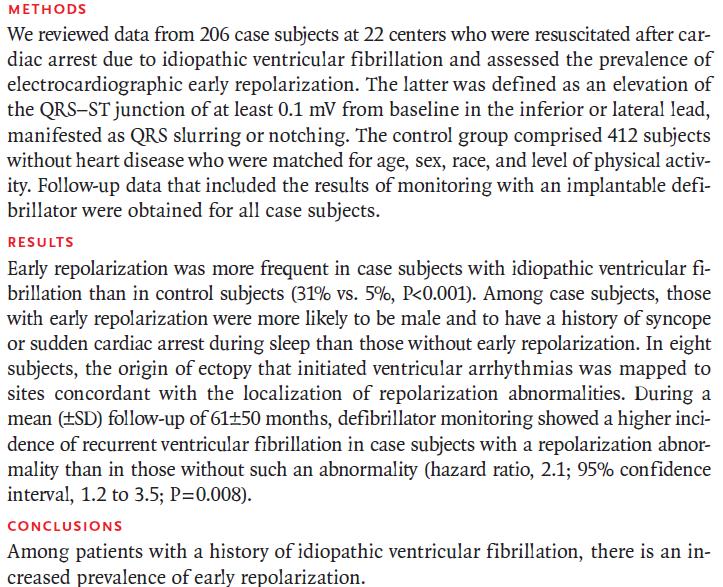
32 EARLY REPOLARIZATION Recently, isolated changes of early repolarization in inferior and/ or lateral leads with terminal QRS slurring has been reported in patients with idiopathic ventricular fibrillation. The study was a retrospective analysis of a selected cohort with episodes of short coupled rapid/polymorphic ventricular tachycardia or ventricular fibrillation leading to syncope or cardiac arrest. Haıssaguerre et al. Sudden cardiac arrest associated with early repolarization. N Engl J Med 2008;358:
33
34
 preceded by STsegment")
35 EARLY REPOLARIZATION PATTERN Early repolarization pattern in a healthy black athlete characterized by right precordial T- wave inversion (arrowhead) preceded by STsegment elevation (arrow)

36

37 ARVC Right precordial T-wave inversion in a patient with ARVC Note that unlike early repolarization, in the ARVC the right precordial leads do not demonstrate any elevation of the ST-segment.
38

39

40
41
42 ECHOCARDIOGRAPHIC CHANGES IN ATHLETES Competitive athletes have myocardial remodeling, including left ventricular dilation and hypertrophy Left ventricular wall dimensions have been shown to increase to up to 14 mm in Italian and British athletes American football players have been demonstrated to have even more marked myocardial hypertrophy of up to 16 mm In a cohort of 156 asymptomatic National Football League players, 23% had evidence of left ventricular hypertrophy, including 6% with wall thicknesses greater than 14 mm.

43 INCIDENCE OF PROFESSIONAL ATHLETES IN ITALY, BRITAIN, AND UNITED STATES WITH ECHOCARDIOGRAPHIC DEFINED LV WALL THICKNESS 12 MM
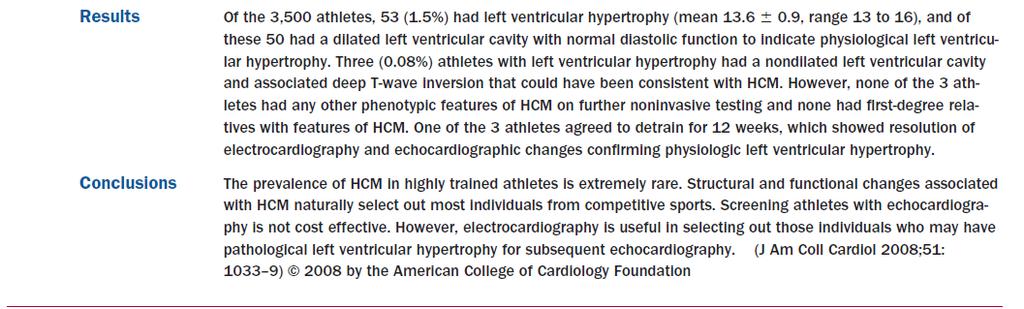
44 Distribution of LVWT in 3,500 Elite Athletes Basavarajaiah, S. et al. J Am Coll Cardiol 2008;51: Copyright 2008 American College of Cardiology Foundation. Restrictions may apply.
45 ECHOCARDIOGRAPHIC CHANGES IN ATHLETES Differentiation of physiologic hypertrophy from HCM can be difficult. In general, physiologic hypertrophy is marked by left ventricular dilatation and excellent exercise tolerance, whereas patients with HCM more commonly demonstrate marked abnormal ECGs, bizarre patterns of hypertrophy, and left atrial enlargement. The changes in athletes are ADAPTIVE and REVERSIBLE.

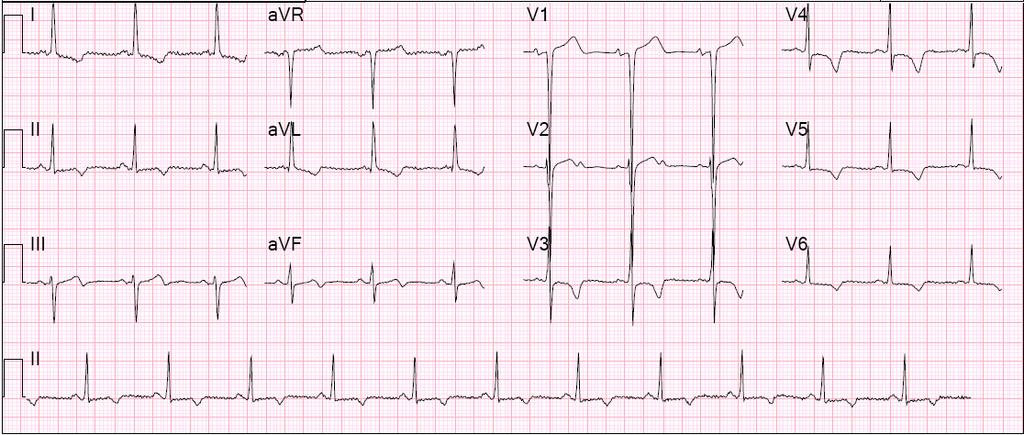
46 Electrocardiograms of a Swimmer With LVH and Inferolateral T-Wave Inversions Before and After Detraining for 12 Weeks Basavarajaiah, S. et al. J Am Coll Cardiol 2008;51: Copyright 2008 American College of Cardiology Foundation. Restrictions may apply.
47

48 CAUSES OF SCD IN ATHLETES
49 COMMOTIO CORDIS Commotio Cordis sudden death with relatively innocent chest wall impact first described in the 19th century The second leading cause of sudden death in young athletes in the United States The median age of commotio cordis victims is 14 years Nearly two thirds of the deaths are in competitive sports, and the others are during recreational sports and routine daily activities. Impacts occur directly over the cardiac silhouette and are thought to be of routine velocity for the age and sex of the person struck by the ball.
50 DISTRIBUTION OF COMMOTIO CORDIS EVENTS ACCORDING TO AGE AND ACTIVITY Maron BJ, Estes N III. N Engl J Med 2010;362:

51 SPORTS DURING WHICH A COMMOTIO CORDIS EVENT OCCURRED

52 Pathophysiology of Commotio Cordis Maron BJ, Estes N III. N Engl J Med 2010;362:
53 T WO-LEAD ECG AND RIGHT ATRIAL AND LEFT VENTRICULAR PRESSURE TRACINGS OF A 16 -KG SWINE UNDERGOING CHEST WALL IMPACT WITH A 40-MPH LACROSSE BALL
54 COMMOTIO CORDIS Commotio cordis has occurred despite the use of safety baseballs and chest wall protection. In nearly one third of the players who underwent a commotio cordis event during competitive sports, a chest protector was worn. There are cases during lacrosse and baseball where the ball struck the chest protector, which was directly over the heart, and commotio cordis still resulted.
55 HYPERTROPHIC CARDIOMYOPATHY

56 HYPERTROPHIC CARDIOMYOPATHY Occurs in 1 of 500 in general population Men and African-Americans affected by almost 2:1 ratio over women and Caucasians Most common cause of sudden death in young athletes Mutation in genes encoding sarcomeric proteins Histological examination reveals myocyte disarray and myocyte loss with fibrosis Variable clinical symptomology Watkins H et al. N Engl J Med 2011;364:

57 The principal pathways of disease progression in hypertrophic cardiomyopathy (HCM) Maron, B. J. et al. J Am Coll Cardiol 2003;42: Copyright 2003 American College of Cardiology Foundation. Restrictions may apply.

58 INTEGRATED PATHOPHYSIOLOGY Braunwald. Atlas of Heart Diseases: Cardiomyopathies, Myocarditis, and Pericardial Disease

59 Incidence of SCD of 1% per year Selected patients treated with an ICD receive appropriate shocks in up to 10% per year SCD occurs more often in younger patients, but does take place in the elderly. The treatment of choice for patients at higher risk for SCD is the ICD. About half of the SCD cases occur during strenuous exercise and competitive sports should therefore be avoided. No evidence that medical Rx (β-blockers, amiodarone) reduces the risk of SCD and prevention should therefore not rely on medical treatment alone. SCD IN HCM

60 Intracardiac Electrogram Showing the Mechanism of Sudden Death in Hypertrophic Cardiomyopathy. Maron BJ. N Engl J Med 2003;349:
. ten Berg J et al.")
61 Septal hypertrophy (arrow) demonstrated on four chamber MRI (A) and on four chamber two dimensional (2D) echocardiography (B). ten Berg J et al. Heart 2010;96: by BMJ Publishing Group Ltd and British Cardiovascular Society

62 Systolic anterior movement (SAM; arrow) of the anterior mitral valve leaflet in a patient with hypertrophic obstructive cardiomyopathy demonstrated with 2D echocardiography in parasternal long axis view. ten Berg J et al. Heart 2010;96: by BMJ Publishing Group Ltd and British Cardiovascular Society
. ten Berg J et al.")
63 Apical hypertrophy (arrow) demonstrated with four chamber MRI (A) and with four chamber 2D echocardiography (B and C). ten Berg J et al. Heart 2010;96: by BMJ Publishing Group Ltd and British Cardiovascular Society

64 Angiogram of the left ventricle in the right oblique view. 1, small end-systolic left ventricular cavity; 2, septal bulge impinging on left ventricular cavity; 3, severe eccentric mitral regurgitation. ten Berg J et al. Heart 2010;96: by BMJ Publishing Group Ltd and British Cardiovascular Society
65
66

67 Electrocardiograms and Parasternal Short-Axis Views of the LV at the Level of Papillary Muscle of the 3 Athletes With LVH and a Nondilated LV Cavity Basavarajaiah, S. et al. J Am Coll Cardiol 2008;51: Copyright 2008 American College of Cardiology Foundation. Restrictions may apply.
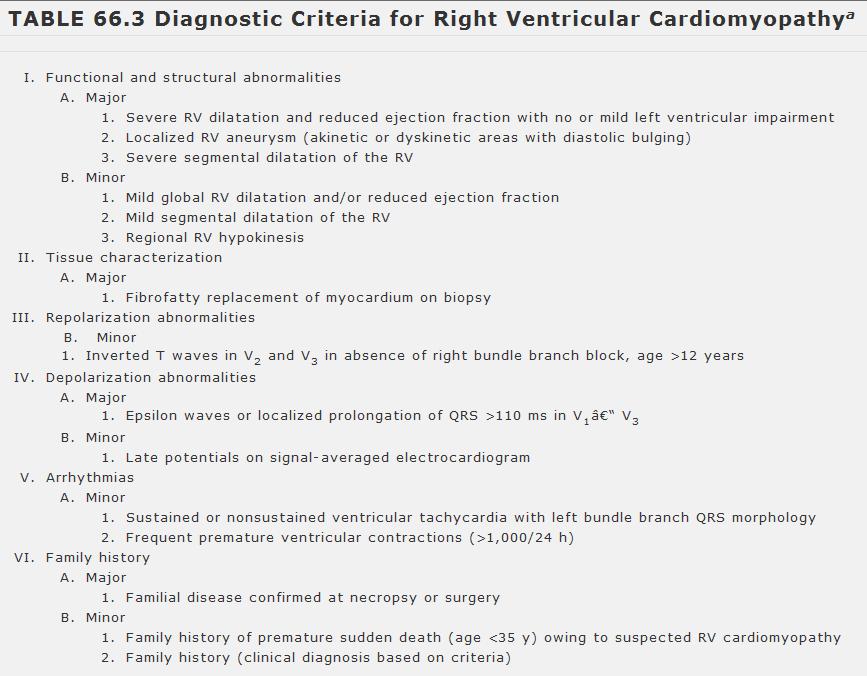
68 RIGHT VENTRICULAR CARDIOMYOPATHY The term "ARVC" was first proposed by Fontaine et al. in a 1977 report describing six patients with sustained ventricular tachycardia Prevalence estimated at 1:5000 Incidence: 6/10,000 up to 44/10,000 Inherited as an autosomal dominant trait with variable penetrance and incomplete expression

69 PATHOGENESIS OF ARRHYTHMOGENIC RIGHT VENTRICULAR CARDIOMYOPATHY The main feature of ARVC is fibrofatty replacement of the myocardium, mainly in the right ventricle but also in the left ventricle This change results in the predominant clinical feature of susceptibility to ventricular arrhythmias The disease is familial, and typically autosomal dominant, in about half the cases. Watkins H et al. N Engl J Med 2011;364:

70 ARVC Mallat Z et al. N Engl J Med 1996;335:


71 ARVD Epsilon wave a late positive deflection in the terminal QRS complex Triangle of dysplasia. Anderson EL. Arrhythmogenic Right Ventricular Dysplasia Am Fam Physician. 2006;73:1391-8

72 EPSILON WAVE

73 Figure 2. Conventional angiogram of the right ventricle in a patient with ARVD shows heavy trabeculation and aneurysmal bulges of the right ventricular outflow tract. Kayser H W M et al. Radiographics 2002;22: by Radiological Society of North America
74 SCD IN ARVC In the US ARVC accounts for approximately 5% of SCD in individuals under the age of 65 Responsible for at least 3% to 4% of deaths associated with physical activity in young athletes In the Veneto region of Italy, ARVC is the most common cause of sudden arrhythmic deaths in individuals under the age of 35 years and the overwhelming cause of sudden death associated with exertion in young athletes in The annual mortality rate of ARVC has been estimated at 3% without treatment and at 1% with pharmacologic medical treatment not including ICD
75 SCD IN ARVC The mechanism of sudden death in ARVC is, in most cases, acceleration of VT with degeneration into ventricular fibrillation. VT in ARVC is due to sympathetic stimulation. accounting for the high prevalence of this condition in individuals who die during exertion. Ambulatory ECG recordings of patients developing sustained VT demonstrate a progressive increase in the sinus rate before the onset of the arrhythmia, suggesting progressive sympathetic stimulation
76
77 SCREENING Screening programs are not widely adopted in the United States. High false positive rates High cost-to-benefit ratio Low rate of sports-related sudden death
78 SCREENING In Italy and most other countries of Europe, in addition to the history and examination, a resting ECG is mandated by law. a decline in sports-related sudden death after ECG screening was instituted in 1982 (Corrado et al). In 1982 the incidence of SCD in Italy was 4.2/100,000 athletes In 2004 the incidence of SCD decreased markedly to 0.9/100,000 In Israel, both a resting ECG and a symptom-limited stress test are mandated
79 NUMBERS AND MONEY HCM 1:500 incidence $500/ECHO $250,000 to detect 1 case 1 death 1000 at risk of sudden cardiac death 200,000 Athletes
80 AHA CONSENSUS PANEL

81 Classification of sports Mitchell, J. H. et al. J Am Coll Cardiol 2005;45: Copyright 2005 American College of Cardiology Foundation. Restrictions may apply.
82
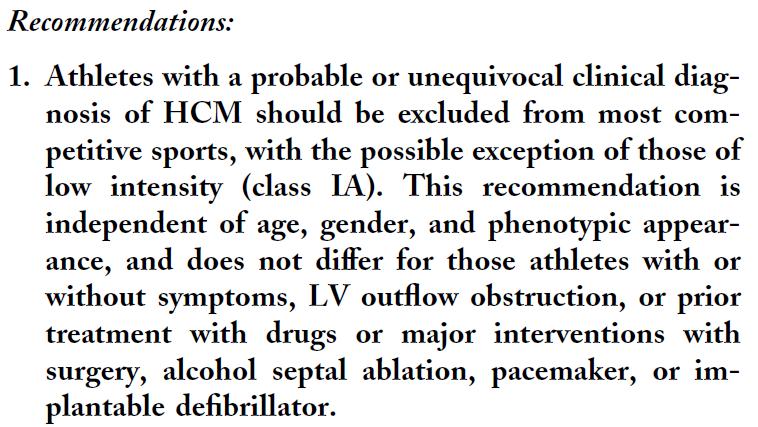
83 HCM
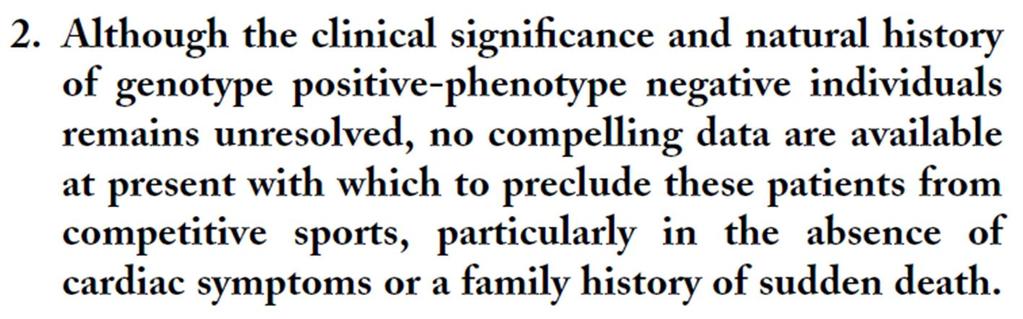
84 HCM
85 ARVC

86 Table 3. Triggers and Drug Responses in Familial LQTS Types 1 3
 ST-segment elevation with upward concavity (arrows), followed by a positive T-wave (arrowheads).")
87 Figure 2. Different patterns of precordial early repolarization in two healthy athletes. (A) ST-segment elevation with upward concavity (arrows), followed by a positive T-wave (arrowheads). (B) ST-segment elevation with upward convexity (arrows), followed by a negative T-wave (arrowheads).
 Right precordial T-wave inversion in a patient with ARVC.")
88 Figure 3. (A) Early repolarization pattern in a healthy black athlete characterized by right precordial T-wave inversion (arrowhead) preceded by ST-segment elevation (arrow). (B) Right precordial T-wave inversion in a patient with ARVC. Note that unlike early repolarization, in the ARVC the right precordial leads do not demonstrate any elevation of the ST-segment.
89 SUDDEN DEATH IN ATHLETES WITH SICKLE CELL TRAIT
90 The majority of individuals who have sickle cell trait have no personal medical problems related to their carrier status, and there are no significant differences in performance between athletes who have SCT versus those who do not have SCT.
91 Since 2013, NCAA, incorporated SCT screening for all athletes from Division I to Division III One in 12 African Americans has SCT Epidemiologic studies suggest a greater relative risks of sudden cardiac death during basic training in army recruits Recent study shows that out 247 cases of sudden death, only 5 (2%) were associated with SCT All cases occur in football players, none during the games but most of them during pre-season conditioning practice Rhabdomyolysis _ as an inciting event due to muscle Hypoxia and sickling_ has been studied
92 PROPOSED UNIVERSAL PRECAUTIONS Managing heat exposure, including the implementation of, and adherence to, established acclimatization protocols. Heat, dehydration, altitude and asthma can increase the risk for and worsen complications associated with SCT, even when exercise is not intense. Supporting adequate nutrition and hydration, especially in hot and humid climates. Studentathletes should refrain from consuming high-caffeine energy drinks and supplements, or other stimulants, as they may contribute to dehydration.
93 Understanding the impact of exercise intensity, especially in the untrained or undertrained student-athlete, and implementation of progressively intense exercise in the first few weeks of the season. Providing adequate time for rest and recovery both during an exercise session and after intense and/or extended periods of physical activity. Development, implementation and adherence to site -specific emergency action plans with appropriate medical equipment and staff to intervene during an emergency situation. Education and counseling are essential for helping student - athletes with SCT understand the potential risks associated with SCT and intense physical activity.
94 CONTACT Alix Dufresne, MD, FACP, FACC, FESC Cardiology Division Chief, Interfaith Medical Center Director Cardiology Clinic, Kingsbrook Jewish Center Fellow American College of Physicians, American College of Cardiology, European Society of Cardiology
at least 4 8 hours per week
 ECG IN ATHLETS An athlete is defined as an individual who engages in regular exercise or training for sport or general fitness, typically with a premium on performance, and often engaged in individual
ECG IN ATHLETS An athlete is defined as an individual who engages in regular exercise or training for sport or general fitness, typically with a premium on performance, and often engaged in individual
Current ECG interpretation guidelines in the screening of athletes
 REVIEW ARTICLE 7 How to differentiate physiological adaptation to intensive physical exercise from pathologies Current ECG interpretation guidelines in the screening of athletes Gemma Parry-Williams, Sanjay
REVIEW ARTICLE 7 How to differentiate physiological adaptation to intensive physical exercise from pathologies Current ECG interpretation guidelines in the screening of athletes Gemma Parry-Williams, Sanjay
ECG Underwriting Puzzler Dr. Regina Rosace AVP & Medical Director
 December 2018 ECG Underwriting Puzzler Dr. Regina Rosace AVP & Medical Director To obtain best results Select Slide Show from the ribbon at the top of your PowerPoint screen Select From Beginning on the
December 2018 ECG Underwriting Puzzler Dr. Regina Rosace AVP & Medical Director To obtain best results Select Slide Show from the ribbon at the top of your PowerPoint screen Select From Beginning on the
Study methodology for screening candidates to athletes risk
 1. Periodical Evaluations: each 2 years. Study methodology for screening candidates to athletes risk 2. Personal history: Personal history of murmur in childhood; dizziness, syncope, palpitations, intolerance
1. Periodical Evaluations: each 2 years. Study methodology for screening candidates to athletes risk 2. Personal history: Personal history of murmur in childhood; dizziness, syncope, palpitations, intolerance
La valutazione dell atleta: è una strategia salva-vita e costo-efficace?
 La valutazione dell atleta: è una strategia salva-vita e costo-efficace? Primo trattato di Medicina Wilson and Jungner s criteria In the 1960s the World Health Organization adopted the Wilson and Jungner
La valutazione dell atleta: è una strategia salva-vita e costo-efficace? Primo trattato di Medicina Wilson and Jungner s criteria In the 1960s the World Health Organization adopted the Wilson and Jungner
6/19/2018. Background Athlete s heart. Ultimate question. Applying the International Criteria for ECG
 Applying the International Criteria for ECG Interpretation in Athletes to a preparticipation screening program DAVE SIEBERT, MD, CAQSM ASSISTANT PROFESSOR DEPARTMENT OF FAMILY MEDICINE UNIVERSITY OF WASHINGTON
Applying the International Criteria for ECG Interpretation in Athletes to a preparticipation screening program DAVE SIEBERT, MD, CAQSM ASSISTANT PROFESSOR DEPARTMENT OF FAMILY MEDICINE UNIVERSITY OF WASHINGTON
Risk Factors for Sudden cardiac Death
 Risk Factors for Sudden cardiac Death A. Arenal Arrhythmias in competitive sports Disclosure Conflict of interest Advisory board: Medtronic, Boston Scientific Research grants: Medtronic, Boston Scientific,
Risk Factors for Sudden cardiac Death A. Arenal Arrhythmias in competitive sports Disclosure Conflict of interest Advisory board: Medtronic, Boston Scientific Research grants: Medtronic, Boston Scientific,
EKG screening in athletics
 Use of PPE EKG screening in athletics Stefan Montgomery MD, ATC 4/27/18 The overall role of the preparticipation physical evaluation (PPE) is to evaluate the health of the athlete to optimize safe sports
Use of PPE EKG screening in athletics Stefan Montgomery MD, ATC 4/27/18 The overall role of the preparticipation physical evaluation (PPE) is to evaluate the health of the athlete to optimize safe sports
Interpretation and Consequences of Repolarisation Changes in Athletes
 Interpretation and Consequences of Repolarisation Changes in Athletes Professor Sanjay Sharma E-mail sasharma@sgul.ac.uk @SSharmacardio Disclosures: None Athlete s ECG Vagotonia Sinus bradycardia Sinus
Interpretation and Consequences of Repolarisation Changes in Athletes Professor Sanjay Sharma E-mail sasharma@sgul.ac.uk @SSharmacardio Disclosures: None Athlete s ECG Vagotonia Sinus bradycardia Sinus
How to Read an Athlete s ECG. Sanjay Sharma BSc (Hons), MD, FRCP, FESC
, MD, FRCP, FESC") How to Read an Athlete s ECG Sanjay Sharma BSc (Hons), MD, FRCP, FESC Athlete s EKG Vagotonia Sinus bradycardia Sinus arrhythmia First degree AVB ST-elevation Tall T waves Increased chamber size Left ventricular
How to Read an Athlete s ECG Sanjay Sharma BSc (Hons), MD, FRCP, FESC Athlete s EKG Vagotonia Sinus bradycardia Sinus arrhythmia First degree AVB ST-elevation Tall T waves Increased chamber size Left ventricular
Sudden cardiac death: Primary and secondary prevention
 Sudden cardiac death: Primary and secondary prevention By Kai Chi Chan Penultimate Year Medical Student St George s University of London at UNic Sheba Medical Centre Definition Sudden cardiac arrest (SCA)
Sudden cardiac death: Primary and secondary prevention By Kai Chi Chan Penultimate Year Medical Student St George s University of London at UNic Sheba Medical Centre Definition Sudden cardiac arrest (SCA)
SABIHA GATI AND SANJAY SHARMA
 9 The athlete s heart SABIHA GATI AND SANJAY SHARMA Pasieka/Science Photo Library In this article, the authors highlight the spectrum, magnitude and determinants of the athlete s heart and provide a practical
9 The athlete s heart SABIHA GATI AND SANJAY SHARMA Pasieka/Science Photo Library In this article, the authors highlight the spectrum, magnitude and determinants of the athlete s heart and provide a practical
EVALUATION OF ELECTROCARDIOGRAPHIC FINDINGS IN ATHLETES
 EVALUATION OF ELECTROCARDIOGRAPHIC FINDINGS IN ATHLETES UNIT OF INHERITED CV DISEASES HEART CENTER OF THE YOUNG AND ATHLETES A DPT OF CARDIOLOGY UNIVERSITY OF ATHENS EVALUATION OF ELECTROCARDIOGRAPHIC
EVALUATION OF ELECTROCARDIOGRAPHIC FINDINGS IN ATHLETES UNIT OF INHERITED CV DISEASES HEART CENTER OF THE YOUNG AND ATHLETES A DPT OF CARDIOLOGY UNIVERSITY OF ATHENS EVALUATION OF ELECTROCARDIOGRAPHIC
Sudden Cardiac Death in Sports: Causes and Current Screening Recommendations
 Sports Cardiology Sudden Cardiac Death in Sports: Causes and Current Screening Recommendations Domenico Corrado, MD, PhD Inherited Arrhytmogenic Cardiomyopathy Unit Department of Cardiac, Thoracic and
Sports Cardiology Sudden Cardiac Death in Sports: Causes and Current Screening Recommendations Domenico Corrado, MD, PhD Inherited Arrhytmogenic Cardiomyopathy Unit Department of Cardiac, Thoracic and
Normal ECG And ECHO Findings in Athletes
 Normal ECG And ECHO Findings in Athletes Dr.Yahya Kiwan Consultant Interventional Cardiologist Head Of Departement Of Cardiology Canadian Specialist Hospital Sinus Bradycardia The normal heartbeat is initiated
Normal ECG And ECHO Findings in Athletes Dr.Yahya Kiwan Consultant Interventional Cardiologist Head Of Departement Of Cardiology Canadian Specialist Hospital Sinus Bradycardia The normal heartbeat is initiated
Historical Notes: Clinical Exercise Testing in the Athlete. An Efficient Heart. Structural Changes, Cont. Coronary Arteries
 Clinical Exercise Testing in the Athlete The athlete s heart Sudden cardiac death in athletes Screening athletes for cardiovascular disease Historical Notes: Giovanni Lancisi (father of cardiology), 17
Clinical Exercise Testing in the Athlete The athlete s heart Sudden cardiac death in athletes Screening athletes for cardiovascular disease Historical Notes: Giovanni Lancisi (father of cardiology), 17
Index. cardiacep.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A AEDs. See Automated external defibrillators (AEDs) AF. See Atrial fibrillation (AF) Age as factor in SD in marathon runners, 45 Antiarrhythmic
Note: Page numbers of article titles are in boldface type. A AEDs. See Automated external defibrillators (AEDs) AF. See Atrial fibrillation (AF) Age as factor in SD in marathon runners, 45 Antiarrhythmic
Slide 1. Slide 2. Slide 3. Sudden Cardiac Death In Athletes. Epidemiology. Epidemiology. Shaun McMurtry, MD Primary Care Sports Medicine
 Slide 1 Sudden Cardiac Death In Athletes Shaun McMurtry, MD Primary Care Sports Medicine Slide 2 Epidemiology College and Professional Athletes 500,000 participants each year Competitive Athletics Estimated
Slide 1 Sudden Cardiac Death In Athletes Shaun McMurtry, MD Primary Care Sports Medicine Slide 2 Epidemiology College and Professional Athletes 500,000 participants each year Competitive Athletics Estimated
Jonathan Kim MD, FACC
 Jonathan Kim MD, FACC Assistant Professor, Division of Cardiology, Emory University Adjunct Assistant Professor, School of Applied Physiology, Georgia Tech Team Cardiologist, Sports Medicine, Emory University
Jonathan Kim MD, FACC Assistant Professor, Division of Cardiology, Emory University Adjunct Assistant Professor, School of Applied Physiology, Georgia Tech Team Cardiologist, Sports Medicine, Emory University
EVALUATION OF THE ATHLETE. Karen Stout, MD Professor, Medicine and Pediatrics University of Washington
 EVALUATION OF THE 12 ATHLETE Karen Stout, MD Professor, Medicine and Pediatrics University of Washington NO DISCLOSURES OUTLINE Why evaluate athletes? What s the problem? What evaluation should be done?
EVALUATION OF THE 12 ATHLETE Karen Stout, MD Professor, Medicine and Pediatrics University of Washington NO DISCLOSURES OUTLINE Why evaluate athletes? What s the problem? What evaluation should be done?
Managing Hypertrophic Cardiomyopathy with Imaging. Gisela C. Mueller University of Michigan Department of Radiology
 Managing Hypertrophic Cardiomyopathy with Imaging Gisela C. Mueller University of Michigan Department of Radiology Disclosures Gadolinium contrast material for cardiac MRI Acronyms Afib CAD Atrial fibrillation
Managing Hypertrophic Cardiomyopathy with Imaging Gisela C. Mueller University of Michigan Department of Radiology Disclosures Gadolinium contrast material for cardiac MRI Acronyms Afib CAD Atrial fibrillation
Ablative Therapy for Ventricular Tachycardia
 Ablative Therapy for Ventricular Tachycardia Nitish Badhwar, MD, FACC, FHRS 2 nd Annual UC Davis Heart and Vascular Center Cardiovascular Nurse / Technologist Symposium May 5, 2012 Disclosures Research
Ablative Therapy for Ventricular Tachycardia Nitish Badhwar, MD, FACC, FHRS 2 nd Annual UC Davis Heart and Vascular Center Cardiovascular Nurse / Technologist Symposium May 5, 2012 Disclosures Research
REtrive. REpeat. RElearn Design by. Test-Enhanced Learning based ECG practice E-book
 Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Sudden Death in Athletes: What is the role of ECG Screening?
 Sudden Death in Athletes: What is the role of ECG Screening? Byron K. Lee MD Professor of Medicine Director of EP Laboratory leeb@medicine.ucsf.edu Division of Cardiology Cardiac Electrophysiology Arrhythmias,
Sudden Death in Athletes: What is the role of ECG Screening? Byron K. Lee MD Professor of Medicine Director of EP Laboratory leeb@medicine.ucsf.edu Division of Cardiology Cardiac Electrophysiology Arrhythmias,
Acute Coronary Syndromes Unstable Angina Non ST segment Elevation MI (NSTEMI) ST segment Elevation MI (STEMI)
 ST segment Elevation MI (STEMI)") Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Evaluate common abnormalities that mimic myocardial infarction. Identify
Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Evaluate common abnormalities that mimic myocardial infarction. Identify
Athlete s Heart vs. Cardiomyopathy
 Athlete s Heart vs. Cardiomyopathy Linda D. Gillam, MD, MPH, FASE Chair, Department of Cardiovascular Medicine Medical Director, Cardiovascular Service Line Former Team Cardiologist to the New York Jets
Athlete s Heart vs. Cardiomyopathy Linda D. Gillam, MD, MPH, FASE Chair, Department of Cardiovascular Medicine Medical Director, Cardiovascular Service Line Former Team Cardiologist to the New York Jets
Office ECG Interpretation
 Office ECG Interpretation Jason Evanchan, DO Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center Outline of topics High risk ischemia T wave
Office ECG Interpretation Jason Evanchan, DO Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center Outline of topics High risk ischemia T wave
Electrical System Overview Electrocardiograms Action Potentials 12-Lead Positioning Values To Memorize Calculating Rates
 Electrocardiograms Electrical System Overview James Lamberg 2/ 74 Action Potentials 12-Lead Positioning 3/ 74 4/ 74 Values To Memorize Inherent Rates SA: 60 to 100 AV: 40 to 60 Ventricles: 20 to 40 Normal
Electrocardiograms Electrical System Overview James Lamberg 2/ 74 Action Potentials 12-Lead Positioning 3/ 74 4/ 74 Values To Memorize Inherent Rates SA: 60 to 100 AV: 40 to 60 Ventricles: 20 to 40 Normal
François Carré Hôpital Pontchaillou -INSERM UMR1099-Université Rennes 1
 Normal electrocardiogram variants in Athletes François Carré Hôpital Pontchaillou -INSERM UMR1099-Université Rennes 1 Disclosures No disclosure of interest concerning this lecture The cardiovascular sport
Normal electrocardiogram variants in Athletes François Carré Hôpital Pontchaillou -INSERM UMR1099-Université Rennes 1 Disclosures No disclosure of interest concerning this lecture The cardiovascular sport
Professor Sanjay Sharma St George s University of London
 How to Evaluate an Athlete of Afro- Caribbean Origin. Professor Sanjay Sharma St George s University of London Background: Causes of SCD in Sport Young competitive athlete Personal and family history Physical
How to Evaluate an Athlete of Afro- Caribbean Origin. Professor Sanjay Sharma St George s University of London Background: Causes of SCD in Sport Young competitive athlete Personal and family history Physical
Echo Evaluation of the Heart of an Athlete
 Echo Evaluation of the Heart of an Athlete 18 th SA Heart Congress, 2017 Johannesburg, South Africa November 9-12, 2017 Naser Ammash. MD Professor of Medicine Practice Chair, Cardiovascular Department
Echo Evaluation of the Heart of an Athlete 18 th SA Heart Congress, 2017 Johannesburg, South Africa November 9-12, 2017 Naser Ammash. MD Professor of Medicine Practice Chair, Cardiovascular Department
Please check your answers with correct statements in answer pages after the ECG cases.
 ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
I have nothing to disclose. Research support from: Cardiac Risk in The Young
 I have nothing to disclose. Research support from: Cardiac Risk in The Young Pre-participation screening of Young Athletes: Current Perspective Professor Sanjay Sharma Disclosures: None SCD in Young Athletes
I have nothing to disclose. Research support from: Cardiac Risk in The Young Pre-participation screening of Young Athletes: Current Perspective Professor Sanjay Sharma Disclosures: None SCD in Young Athletes
Athletes with cardiac disease; dead and buried or chance for resurrection?
 Athletes with cardiac disease; dead and buried or chance for resurrection? EuroPRevent 2011 Geneva F. Carré University Rennes 1-Pontchaillou Hospital Inserm U642, Rennes - F-35000 Risk of physical activity
Athletes with cardiac disease; dead and buried or chance for resurrection? EuroPRevent 2011 Geneva F. Carré University Rennes 1-Pontchaillou Hospital Inserm U642, Rennes - F-35000 Risk of physical activity
Cardiovascular Impacts of long-term endurance exercise: Implications of athlete s heart
 Cardiovascular Impacts of long-term endurance exercise: Implications of athlete s heart Dr. Gary Mak 麥耀光心臟科專科醫生 IPP of HK Associa4on of Sports Medicine and Sports Science Director of Pro-Cardio Heart Disease
Cardiovascular Impacts of long-term endurance exercise: Implications of athlete s heart Dr. Gary Mak 麥耀光心臟科專科醫生 IPP of HK Associa4on of Sports Medicine and Sports Science Director of Pro-Cardio Heart Disease
DEPARTMENT NAME PRE-PARTICIPATION SCREENING THE SPORTS PHYSICAL
 PRE-PARTICIPATION SCREENING THE SPORTS PHYSICAL Michele Krenek, MSN, RN, FNP-C TCHAPP Conference, Houston, TX April 4, 2019 PRE-PARTICIPATION SPORTS SCREENING According to the AHA the definition of the
PRE-PARTICIPATION SCREENING THE SPORTS PHYSICAL Michele Krenek, MSN, RN, FNP-C TCHAPP Conference, Houston, TX April 4, 2019 PRE-PARTICIPATION SPORTS SCREENING According to the AHA the definition of the
Athlete s Heart vs. Cardiomyopathy
 Athlete s Heart vs. Cardiomyopathy Linda D. Gillam, MD, MPH, FASE Chair, Department of Cardiovascular Medicine Medical Director, Cardiovascular Service Line Former Team Cardiologist to the New York Jets
Athlete s Heart vs. Cardiomyopathy Linda D. Gillam, MD, MPH, FASE Chair, Department of Cardiovascular Medicine Medical Director, Cardiovascular Service Line Former Team Cardiologist to the New York Jets
Exercise guidelines in athletes with isolated repolarisation abnormalities and structurally normal heart.
 Exercise guidelines in athletes with isolated repolarisation abnormalities and structurally normal heart. Hanne Rasmusen Consultant cardiologist, PhD Dept. of Cardiology Bispebjerg University Hospital
Exercise guidelines in athletes with isolated repolarisation abnormalities and structurally normal heart. Hanne Rasmusen Consultant cardiologist, PhD Dept. of Cardiology Bispebjerg University Hospital
Advances in Ablation Therapy for Ventricular Tachycardia
 Advances in Ablation Therapy for Ventricular Tachycardia Nitish Badhwar, MD, FACC, FHRS Director, Cardiac Electrophysiology Training Program University of California, San Francisco For those of you who
Advances in Ablation Therapy for Ventricular Tachycardia Nitish Badhwar, MD, FACC, FHRS Director, Cardiac Electrophysiology Training Program University of California, San Francisco For those of you who
All About STEMIs. Presented By: Brittney Urvand, RN, BSN, CCCC. Essentia Health Fargo Cardiovascular Program Manager.
 All About STEMIs Presented By: Brittney Urvand, RN, BSN, CCCC Essentia Health Fargo Cardiovascular Program Manager Updated 10/2/2018 None Disclosures Objectives Identify signs and symptoms of a heart attack
All About STEMIs Presented By: Brittney Urvand, RN, BSN, CCCC Essentia Health Fargo Cardiovascular Program Manager Updated 10/2/2018 None Disclosures Objectives Identify signs and symptoms of a heart attack
Arrhythmias (II) Ventricular Arrhythmias. Disclosures
 Ventricular Arrhythmias. Disclosures") Arrhythmias (II) Ventricular Arrhythmias Amy Leigh Miller, MD, PhD Cardiovascular Electrophysiology, Brigham & Women s Hospital Disclosures None Rhythms and Mortality Implantable loop recorder post-mi
Arrhythmias (II) Ventricular Arrhythmias Amy Leigh Miller, MD, PhD Cardiovascular Electrophysiology, Brigham & Women s Hospital Disclosures None Rhythms and Mortality Implantable loop recorder post-mi
9/17/2010. Phidippides. Phidippides. Sudden Death in the Young Athlete. What is the extent of the problem? Can we prevent it?
 Phidippides Phidippides Sudden Death in the Young Athlete What is the extent of the problem? Can we prevent it? 1 Number of cardiovascular (CV), trauma-related, and other sudden death events in 1866 young
Phidippides Phidippides Sudden Death in the Young Athlete What is the extent of the problem? Can we prevent it? 1 Number of cardiovascular (CV), trauma-related, and other sudden death events in 1866 young
ECG Cases and Questions. Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology
 ECG Cases and Questions Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology 32 yo female Life Insurance Physical 56 yo male with chest pain Terminology Injury ST elevation Ischemia T wave inversion
ECG Cases and Questions Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology 32 yo female Life Insurance Physical 56 yo male with chest pain Terminology Injury ST elevation Ischemia T wave inversion
Cardiomyopathy. Jeff Grubbe MD FACP, Chief Medical Director, Allstate Life & Retirement
 Cardiomyopathy Jeff Grubbe MD FACP, Chief Medical Director, Allstate Life & Retirement Nebraska Home Office Life Underwriters Association March 20, 2018 1 Cardiomyopathy A myocardial disorder in which
Cardiomyopathy Jeff Grubbe MD FACP, Chief Medical Director, Allstate Life & Retirement Nebraska Home Office Life Underwriters Association March 20, 2018 1 Cardiomyopathy A myocardial disorder in which
Sudden Cardiac Arrest in Athletes Capital City Sports Summit June 7, 2012
 Sudden Cardiac Arrest in Athletes Capital City Sports Summit June 7, 2012 John Katopodis, MD, FACC Southern Medical Group Cardiology Tallahassee, Florida Scope of the Problem Relating to Screening and
Sudden Cardiac Arrest in Athletes Capital City Sports Summit June 7, 2012 John Katopodis, MD, FACC Southern Medical Group Cardiology Tallahassee, Florida Scope of the Problem Relating to Screening and
How NOT to miss Hypertrophic Cardiomyopathy? Adaya Weissler-Snir, MD University Health Network, University of Toronto
 How NOT to miss Hypertrophic Cardiomyopathy? Adaya Weissler-Snir, MD University Health Network, University of Toronto Introduction Hypertrophic cardiomyopathy is the most common genetic cardiomyopathy,
How NOT to miss Hypertrophic Cardiomyopathy? Adaya Weissler-Snir, MD University Health Network, University of Toronto Introduction Hypertrophic cardiomyopathy is the most common genetic cardiomyopathy,
Abnormal electrocardiographic findings in athletes: recognising changes suggestive of cardiomyopathy
 Scan to access more free content For numbered affiliations see end of article Correspondence to Jonathan A Drezner, Department of Family Medicine, University of Washington, 1959 NE Pacific Street, Box
Scan to access more free content For numbered affiliations see end of article Correspondence to Jonathan A Drezner, Department of Family Medicine, University of Washington, 1959 NE Pacific Street, Box
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016
 Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
DIAGNOSIS AND MANAGEMENT OF ARRHYTHMOGENIC CARDIOMYOPATHY. David SIU MD ( 蕭頌華醫生 ) Division of Cardiology The University of Hong Kong
 Division of Cardiology The University of Hong Kong") APHRS Summit 2018 in conjunction with HKCC Heart Rhythm Refresher Course DIAGNOSIS AND MANAGEMENT OF ARRHYTHMOGENIC CARDIOMYOPATHY David SIU MD ( 蕭頌華醫生 ) Division of Cardiology The University of Hong Kong
APHRS Summit 2018 in conjunction with HKCC Heart Rhythm Refresher Course DIAGNOSIS AND MANAGEMENT OF ARRHYTHMOGENIC CARDIOMYOPATHY David SIU MD ( 蕭頌華醫生 ) Division of Cardiology The University of Hong Kong
Nancy Goldman Cutler, MD Beaumont Children s Hospital Royal Oak, Mi
 Nancy Goldman Cutler, MD Beaumont Children s Hospital Royal Oak, Mi Identify increased LV wall thickness (WT) Understand increased WT in athletes Understand hypertrophic cardiomyopathy (HCM) Enhance understanding
Nancy Goldman Cutler, MD Beaumont Children s Hospital Royal Oak, Mi Identify increased LV wall thickness (WT) Understand increased WT in athletes Understand hypertrophic cardiomyopathy (HCM) Enhance understanding
Case 1. Case 2. Case 3
 Case 1 The correct answer is D. Occasionally, the Brugada syndrome can present similar morphologies to A and also change depending on the lead position but in the Brugada pattern the r is wider and ST
Case 1 The correct answer is D. Occasionally, the Brugada syndrome can present similar morphologies to A and also change depending on the lead position but in the Brugada pattern the r is wider and ST
Dr. Schroeder has no financial relationships to disclose
 Valerie A Schroeder MD MS Assistant Professor University of Kansas Medical Center READING THE WAVES- THE HEART S ELECTRICAL MESSAGE FINANCIAL DISCLOSURE Dr. Schroeder has no financial relationships to
Valerie A Schroeder MD MS Assistant Professor University of Kansas Medical Center READING THE WAVES- THE HEART S ELECTRICAL MESSAGE FINANCIAL DISCLOSURE Dr. Schroeder has no financial relationships to
FANS ARVC (Arrhythmogenic Right Ventricular Cardiomyopathy) Investigation Protocol
 Investigation Protocol") Clinical Features FANS ARVC (Arrhythmogenic Right Ventricular Cardiomyopathy) Investigation Protocol History: Progressive disease, characterised by the following clinical stages: o Early concealed phase
Clinical Features FANS ARVC (Arrhythmogenic Right Ventricular Cardiomyopathy) Investigation Protocol History: Progressive disease, characterised by the following clinical stages: o Early concealed phase
The Athlete s Heart. Role of Echo. Neil J. Weissman, MD MedStar Health Research Institute & Professor of Medicine Georgetown University
 The Athlete s Heart Role of Echo Neil J. Weissman, MD MedStar Health Research Institute & Professor of Medicine Georgetown University Washington, D.C. Disclosures Grant support (to institution) for Core
The Athlete s Heart Role of Echo Neil J. Weissman, MD MedStar Health Research Institute & Professor of Medicine Georgetown University Washington, D.C. Disclosures Grant support (to institution) for Core
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH
 ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
Ronald J. Kanter, MD Director, Electrophysiology Miami Children s Hospital Professor Emeritus, Duke University Miami, Florida
 S306- Pediatric Electrocardiography: A Potpourri Ronald J. Kanter, MD Director, Electrophysiology Miami Children s Hospital Professor Emeritus, Duke University Miami, Florida Disclosure of Relevant Relationship
S306- Pediatric Electrocardiography: A Potpourri Ronald J. Kanter, MD Director, Electrophysiology Miami Children s Hospital Professor Emeritus, Duke University Miami, Florida Disclosure of Relevant Relationship
Cardiac Conditions in Sport & Exercise. Cardiac Conditions in Sport. USA - Sudden Cardiac Death (SCD) Dr Anita Green. Sudden Cardiac Death
 Dr Anita Green. Sudden Cardiac Death") Cardiac Conditions in Sport & Exercise Dr Anita Green Cardiac Conditions in Sport Sudden Cardiac Death USA - Sudden Cardiac Death (SCD)
Cardiac Conditions in Sport & Exercise Dr Anita Green Cardiac Conditions in Sport Sudden Cardiac Death USA - Sudden Cardiac Death (SCD)
The Athlete s Heart. Critical Role of Echo. Neil J. Weissman, MD MedStar Health Research Institute & Professor of Medicine Georgetown University
 The Athlete s Heart Critical Role of Echo Neil J. Weissman, MD MedStar Health Research Institute & Professor of Medicine Georgetown University Washington, D.C. Disclosures Grant support (to institution)
The Athlete s Heart Critical Role of Echo Neil J. Weissman, MD MedStar Health Research Institute & Professor of Medicine Georgetown University Washington, D.C. Disclosures Grant support (to institution)
Το ΗΚΓ στις Μυοκαρδιοπάθειες και στην Περικαρδίτιδα
 4 ο ΠΑΝΕΛΛΗΝΙΟ ΑΡΡΥΘΜΙΟΛΟΓΙΚΟ ΣΥΝΕΔΡΙΟ Φροντιστηριακό Μάθημα ΗΚΓ Το ΗΚΓ στις Μυοκαρδιοπάθειες και στην Περικαρδίτιδα Γ.Ν.Α. «Ο Ευαγγελισμός» Ξυδώνας Σωτήριος, MD, PhD, FESC Εργαστήριο Ηλεκτροφυσιολογίας
4 ο ΠΑΝΕΛΛΗΝΙΟ ΑΡΡΥΘΜΙΟΛΟΓΙΚΟ ΣΥΝΕΔΡΙΟ Φροντιστηριακό Μάθημα ΗΚΓ Το ΗΚΓ στις Μυοκαρδιοπάθειες και στην Περικαρδίτιδα Γ.Ν.Α. «Ο Ευαγγελισμός» Ξυδώνας Σωτήριος, MD, PhD, FESC Εργαστήριο Ηλεκτροφυσιολογίας
Basic electrocardiography reading. R3 lee wei-chieh
 Basic electrocardiography reading R3 lee wei-chieh The Normal Conduction System Lead Placement avf Limb Leads Precordial Leads Interpretation Rate Rhythm Interval Axis Chamber abnormality QRST change What
Basic electrocardiography reading R3 lee wei-chieh The Normal Conduction System Lead Placement avf Limb Leads Precordial Leads Interpretation Rate Rhythm Interval Axis Chamber abnormality QRST change What
402 Index. B β-blockers, 4, 5 Bradyarrhythmias, 76 77
 Index A Acquired immunodeficiency syndrome (AIDS), 126, 163 Action potentials, 1, 5, 27 Acute coronary syndromes, 123t, 129 Adenosine, intravenous, 277 Alcohol abuse, as T wave inversion cause, 199 Aneurysm,
Index A Acquired immunodeficiency syndrome (AIDS), 126, 163 Action potentials, 1, 5, 27 Acute coronary syndromes, 123t, 129 Adenosine, intravenous, 277 Alcohol abuse, as T wave inversion cause, 199 Aneurysm,
December 2018 Tracings
 Tracings Tracing 1 Tracing 4 Tracing 1 Answer Tracing 4 Answer Tracing 2 Tracing 5 Tracing 2 Answer Tracing 5 Answer Tracing 3 Tracing 6 Tracing 3 Answer Tracing 6 Answer Questions? Contact Dr. Nelson
Tracings Tracing 1 Tracing 4 Tracing 1 Answer Tracing 4 Answer Tracing 2 Tracing 5 Tracing 2 Answer Tracing 5 Answer Tracing 3 Tracing 6 Tracing 3 Answer Tracing 6 Answer Questions? Contact Dr. Nelson
Name of Presenter: Marwan Refaat, MD
 NAAMA s 24 th International Medical Convention Medicine in the Next Decade: Challenges and Opportunities Beirut, Lebanon June 26 July 2, 2010 I have no actual or potential conflict of interest in relation
NAAMA s 24 th International Medical Convention Medicine in the Next Decade: Challenges and Opportunities Beirut, Lebanon June 26 July 2, 2010 I have no actual or potential conflict of interest in relation
Cardiac hypertrophy and how it may break an athlete s heart e the Cypriot case
 Eur J Echocardiography (2005) 6, 301e307 Cardiac hypertrophy and how it may break an athlete s heart e the Cypriot case C.E. Chee a,1, C.P. Anastassiades a,1, A.G. Antonopoulos b, A.A. Petsas b, L.C. Anastassiades
Eur J Echocardiography (2005) 6, 301e307 Cardiac hypertrophy and how it may break an athlete s heart e the Cypriot case C.E. Chee a,1, C.P. Anastassiades a,1, A.G. Antonopoulos b, A.A. Petsas b, L.C. Anastassiades
Preventing Sudden Death in Young Athletes. Outline. Scope of the Problem. Causes of SCD in Young Athletes. Sudden death in the young athlete
 Preventing Sudden Death in Young Athletes Ronn E. Tanel, MD Director, Pediatric Arrhythmia Service UCSF Children s Hospital Associate Professor of Pediatrics UCSF School of Medicine Outline Sudden death
Preventing Sudden Death in Young Athletes Ronn E. Tanel, MD Director, Pediatric Arrhythmia Service UCSF Children s Hospital Associate Professor of Pediatrics UCSF School of Medicine Outline Sudden death
Echocardiographic Evaluation of the Cardiomyopathies. Stephanie Coulter, MD, FACC, FASE April, 2016
 Echocardiographic Evaluation of the Cardiomyopathies Stephanie Coulter, MD, FACC, FASE April, 2016 Cardiomyopathies (CMP) primary disease intrinsic to cardiac muscle Dilated CMP Hypertrophic CMP Infiltrative
Echocardiographic Evaluation of the Cardiomyopathies Stephanie Coulter, MD, FACC, FASE April, 2016 Cardiomyopathies (CMP) primary disease intrinsic to cardiac muscle Dilated CMP Hypertrophic CMP Infiltrative
2/26/2015.
 Gerry Keenan MMS PA-C Associate Professor -Physician Assistant Studies Arizona School of Health Sciences A T Still University Event Medical Director-USA/Karate- Arizona Clinical Director-MEDfest/Healthy
Gerry Keenan MMS PA-C Associate Professor -Physician Assistant Studies Arizona School of Health Sciences A T Still University Event Medical Director-USA/Karate- Arizona Clinical Director-MEDfest/Healthy
My Patient Needs a Stress Test
 My Patient Needs a Stress Test Amy S. Burhanna,, MD, FACC Coastal Cardiology Cape May Court House, New Jersey Absolute and relative contraindications to exercise testing Absolute Acute myocardial infarction
My Patient Needs a Stress Test Amy S. Burhanna,, MD, FACC Coastal Cardiology Cape May Court House, New Jersey Absolute and relative contraindications to exercise testing Absolute Acute myocardial infarction
Key wards: PR Interval, QT interval, bradycardia.
 bü z ÇtÄ TÜà väx : A Pilot Study Eman Abdo Elaziz Ahmed 1 and Amal Mahmoud Saied 2 Abstract Background: Sudden deaths of young competitive athletes are tragic events that continue to have a considerable
bü z ÇtÄ TÜà väx : A Pilot Study Eman Abdo Elaziz Ahmed 1 and Amal Mahmoud Saied 2 Abstract Background: Sudden deaths of young competitive athletes are tragic events that continue to have a considerable
Relax and Learn at the FARM 2012: Session 8: 12 Lead ECG 401: ECG Variants
 Relax and Learn at the FARM 2012: Session 8: 12 Lead ECG 401: ECG Variants A Ship in the Harbor is Safe But that is not what ships are built for. Karen Marzlin DNP, RN, CCNS, CCRN-CMC, CHFN Cardiovascular
Relax and Learn at the FARM 2012: Session 8: 12 Lead ECG 401: ECG Variants A Ship in the Harbor is Safe But that is not what ships are built for. Karen Marzlin DNP, RN, CCNS, CCRN-CMC, CHFN Cardiovascular
The frontier between normal and abnormal electrocardiogram in athletes
 The frontier between normal and abnormal electrocardiogram in athletes ESC Congress 2011 Paris F. Carré University Rennes 1-Pontchaillou Hospital Inserm U642, Rennes - F-35000 Cardiovascular preparticipation
The frontier between normal and abnormal electrocardiogram in athletes ESC Congress 2011 Paris F. Carré University Rennes 1-Pontchaillou Hospital Inserm U642, Rennes - F-35000 Cardiovascular preparticipation
Tachycardias II. Štěpán Havránek
 Tachycardias II Štěpán Havránek Summary 1) Supraventricular (supraventricular rhythms) Atrial fibrillation and flutter Atrial ectopic tachycardia / extrabeats AV nodal reentrant a AV reentrant tachycardia
Tachycardias II Štěpán Havránek Summary 1) Supraventricular (supraventricular rhythms) Atrial fibrillation and flutter Atrial ectopic tachycardia / extrabeats AV nodal reentrant a AV reentrant tachycardia
ECG Interpretation Made Easy
 ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School 2007-2008 ECG Interpretation Made Easy Synopsis Benefits Objectives Process
ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School 2007-2008 ECG Interpretation Made Easy Synopsis Benefits Objectives Process
12-Lead ECG Interpretation. Kathy Kuznar, RN, ANP
 12-Lead ECG Interpretation Kathy Kuznar, RN, ANP The 12-Lead ECG Objectives Identify the normal morphology and features of the 12- lead ECG. Perform systematic analysis of the 12-lead ECG. Recognize abnormalities
12-Lead ECG Interpretation Kathy Kuznar, RN, ANP The 12-Lead ECG Objectives Identify the normal morphology and features of the 12- lead ECG. Perform systematic analysis of the 12-lead ECG. Recognize abnormalities
Family Medicine for English language students of Medical University of Lodz ECG. Jakub Dorożyński
 Family Medicine for English language students of Medical University of Lodz ECG Jakub Dorożyński Parts of an ECG The standard ECG has 12 leads: six of them are considered limb leads because they are placed
Family Medicine for English language students of Medical University of Lodz ECG Jakub Dorożyński Parts of an ECG The standard ECG has 12 leads: six of them are considered limb leads because they are placed
ECG Workshop. Nezar Amir
 ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
Endurance Exercise and Cardiovascular Health
 Endurance Exercise and Cardiovascular Health Professor Sanjay Sharma St George s University of London St George s Hospital NHS Trust sasharma@sgul.ac.uk @SSharmacardio Conflicts/Disclosures: None Objectives
Endurance Exercise and Cardiovascular Health Professor Sanjay Sharma St George s University of London St George s Hospital NHS Trust sasharma@sgul.ac.uk @SSharmacardio Conflicts/Disclosures: None Objectives
General Introduction to ECG. Reading Assignment (p2-16 in PDF Outline )
") General Introduction to ECG Reading Assignment (p2-16 in PDF Outline ) Objectives 1. Practice the 5-step Method 2. Differential Diagnosis: R & L axis deviation 3. Differential Diagnosis: Poor R-wave progression
General Introduction to ECG Reading Assignment (p2-16 in PDF Outline ) Objectives 1. Practice the 5-step Method 2. Differential Diagnosis: R & L axis deviation 3. Differential Diagnosis: Poor R-wave progression
Investigating the family after a sudden cardiac death. Dr Catherine Mercer Consultant Clinical Geneticist, Wessex
 Investigating the family after a sudden cardiac death Dr Catherine Mercer Consultant Clinical Geneticist, Wessex Sudden adult deaths subdivided Sudden Adult Death Sudden Cardiac Death Sudden Arrhythmic
Investigating the family after a sudden cardiac death Dr Catherine Mercer Consultant Clinical Geneticist, Wessex Sudden adult deaths subdivided Sudden Adult Death Sudden Cardiac Death Sudden Arrhythmic
A new consensus document on electrocardiographic interpretation in athletes: does it help to prevent sudden cardiac death in athletes?
 Neth Heart J (2018) 26:127 132 https://doi.org/10.1007/s12471-018-1076-6 POINT OF VIEW A new consensus document on electrocardiographic interpretation in athletes: does it help to prevent sudden cardiac
Neth Heart J (2018) 26:127 132 https://doi.org/10.1007/s12471-018-1076-6 POINT OF VIEW A new consensus document on electrocardiographic interpretation in athletes: does it help to prevent sudden cardiac
Section V. Objectives
 Section V Landscape of an MI Objectives At the conclusion of this presentation the participant will be able to Outline a systematic approach to 12 lead ECG interpretation Demonstrate the process for determining
Section V Landscape of an MI Objectives At the conclusion of this presentation the participant will be able to Outline a systematic approach to 12 lead ECG interpretation Demonstrate the process for determining
Dr Navin Chandra Clinical Research Fellow in Cardiology St George s University of London
 Dr Navin Chandra Clinical Research Fellow in Cardiology St George s University of London Cardiac Adaptation in Athletes Athletic training for prolonged periods may result in physiological adaptations of
Dr Navin Chandra Clinical Research Fellow in Cardiology St George s University of London Cardiac Adaptation in Athletes Athletic training for prolonged periods may result in physiological adaptations of
Pre-Participation Athletic Cardiac Screening
 Pre-Participation Athletic Cardiac Screening Kimberly A Krabill, MD Pediatric and Fetal Cardiologist Northwest Congenital Heart Care, Division of MedNax Cardiology Update for Primary Care Symposium July
Pre-Participation Athletic Cardiac Screening Kimberly A Krabill, MD Pediatric and Fetal Cardiologist Northwest Congenital Heart Care, Division of MedNax Cardiology Update for Primary Care Symposium July
Cardiac Evaluation of the Adolescent. Indications for ordering an ECG 3/18/2010. Cardiac Evaluation of the Adolescent W.
 Cardiac Evaluation of the Adolescent W. Reid Thompson, M.D. The Helen B. Taussig Children s Heart Center Johns Hopkins University School of Medicine Goals for talk By the end of the session you should
Cardiac Evaluation of the Adolescent W. Reid Thompson, M.D. The Helen B. Taussig Children s Heart Center Johns Hopkins University School of Medicine Goals for talk By the end of the session you should
Masqueraders of STEMI
 Masqueraders of STEMI Steven M. Costa, M.D. Assistant Professor Department of Medicine Division of Cardiology Scott & White Memorial Hospital and Clinic Texas A&M University Health Science Center Disclosures
Masqueraders of STEMI Steven M. Costa, M.D. Assistant Professor Department of Medicine Division of Cardiology Scott & White Memorial Hospital and Clinic Texas A&M University Health Science Center Disclosures
THE PRE-PARTICIPATION EXAM (A.K.A. THE PPE)
") THE PRE-PARTICIPATION EXAM (A.K.A. THE PPE) Peter Hoth, MD Clinical Assistant Professor UI Sports Medicine Department of Family Medicine 45 th Annual Refresher Course for the Family Physician April 5,
THE PRE-PARTICIPATION EXAM (A.K.A. THE PPE) Peter Hoth, MD Clinical Assistant Professor UI Sports Medicine Department of Family Medicine 45 th Annual Refresher Course for the Family Physician April 5,
Paroxysmal Supraventricular Tachycardia PSVT.
 Atrial Tachycardia; is the name for an arrhythmia caused by a disorder of the impulse generation in the atrium or the AV node. An area in the atrium sends out rapid signals, which are faster than those
Atrial Tachycardia; is the name for an arrhythmia caused by a disorder of the impulse generation in the atrium or the AV node. An area in the atrium sends out rapid signals, which are faster than those
ECG Interpretation Cat Williams, DVM DACVIM (Cardiology)
") ECG Interpretation Cat Williams, DVM DACVIM (Cardiology) Providing the best quality care and service for the patient, the client, and the referring veterinarian. GOAL: Reduce Anxiety about ECGs Back to
ECG Interpretation Cat Williams, DVM DACVIM (Cardiology) Providing the best quality care and service for the patient, the client, and the referring veterinarian. GOAL: Reduce Anxiety about ECGs Back to
CLINICAL RESEARCH ON CARDIOVASCULAR ALTERATION ON 86 S PROFESSIONAL ATHLETES IN IRAN
 CLINICAL RESEARCH ON CARDIOVASCULAR ALTERATION ON 86 S PROFESSIONAL ATHLETES IN IRAN Lotfali Pourkazemi 1 * and Roghieh Razeghi Jadid 2 1 Sports Medicine Federation of Iran 2 Department of Herbal Sciences,
CLINICAL RESEARCH ON CARDIOVASCULAR ALTERATION ON 86 S PROFESSIONAL ATHLETES IN IRAN Lotfali Pourkazemi 1 * and Roghieh Razeghi Jadid 2 1 Sports Medicine Federation of Iran 2 Department of Herbal Sciences,
Chapter 2 Practical Approach
 Chapter 2 Practical Approach There are beginners in electrocardiogram (ECG) analysis who are fascinated by a special pattern (e.g., a bundle-branch block or a striking Q wave) and thereby overlook other
Chapter 2 Practical Approach There are beginners in electrocardiogram (ECG) analysis who are fascinated by a special pattern (e.g., a bundle-branch block or a striking Q wave) and thereby overlook other
Recommendations for interpretation of 12-lead electrocardiogram in the athlete
 European Heart Journal (2010) 31, 243 259 doi:10.1093/eurheartj/ehp473 ESC REPORT s for interpretation of 12-lead electrocardiogram in the athlete Domenico Corrado 1 *, Antonio Pelliccia 2, Hein Heidbuchel
European Heart Journal (2010) 31, 243 259 doi:10.1093/eurheartj/ehp473 ESC REPORT s for interpretation of 12-lead electrocardiogram in the athlete Domenico Corrado 1 *, Antonio Pelliccia 2, Hein Heidbuchel
SIMPLY ECGs. Dr William Dooley
 SIMPLY ECGs Dr William Dooley Content Basic ECG interpretation pattern Some common (examined) abnormalities Presenting ECGs in context Setting up an ECG Setting up an ECG 1 V1-4 th Right intercostal space
SIMPLY ECGs Dr William Dooley Content Basic ECG interpretation pattern Some common (examined) abnormalities Presenting ECGs in context Setting up an ECG Setting up an ECG 1 V1-4 th Right intercostal space
Reading Assignment (p1-91 in Outline ) Objectives What s in an ECG?
 Objectives What s in an ECG?") Reading Assignment (p1-91 in Outline ) Objectives What s in an ECG? The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis= 1. Compute the 5 basic
Reading Assignment (p1-91 in Outline ) Objectives What s in an ECG? The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis= 1. Compute the 5 basic
Myocardial Infarction. Reading Assignment (p66-78 in Outline )
") Myocardial Infarction Reading Assignment (p66-78 in Outline ) Objectives 1. Why do ST segments go up or down in ischemia? 2. STEMI locations and culprit vessels 3. Why 15-lead ECGs? 4. What s up with avr?
Myocardial Infarction Reading Assignment (p66-78 in Outline ) Objectives 1. Why do ST segments go up or down in ischemia? 2. STEMI locations and culprit vessels 3. Why 15-lead ECGs? 4. What s up with avr?
27-year-old professionnal rugby player: asymptomatic
 27-year-old professionnal rugby player: asymptomatic Benefits and limits of cardiac MRI in the young athlete with a suspected heart disease. Philippe PAULE Service de Cardiologie, HIA Clermont Tonnerre,
27-year-old professionnal rugby player: asymptomatic Benefits and limits of cardiac MRI in the young athlete with a suspected heart disease. Philippe PAULE Service de Cardiologie, HIA Clermont Tonnerre,
ELECTROCARDIOGRAPH. General. Heart Rate. Starship Children s Health Clinical Guideline
 General Heart Rate QRS Axis T Wave Axis PR Interval according to Heart Rate & Age P Wave Duration and Amplitude QRS Duration according to Age QT Interval R & S voltages according to Lead & Age R/S ratio
General Heart Rate QRS Axis T Wave Axis PR Interval according to Heart Rate & Age P Wave Duration and Amplitude QRS Duration according to Age QT Interval R & S voltages according to Lead & Age R/S ratio
Electrocardiography Abnormalities (Arrhythmias) 7. Faisal I. Mohammed, MD, PhD
 7. Faisal I. Mohammed, MD, PhD") Electrocardiography Abnormalities (Arrhythmias) 7 Faisal I. Mohammed, MD, PhD 1 Causes of Cardiac Arrythmias Abnormal rhythmicity of the pacemaker Shift of pacemaker from sinus node Blocks at different
Electrocardiography Abnormalities (Arrhythmias) 7 Faisal I. Mohammed, MD, PhD 1 Causes of Cardiac Arrythmias Abnormal rhythmicity of the pacemaker Shift of pacemaker from sinus node Blocks at different
INTRODUCTION. left ventricular non-compaction is a sporadic or familial cardiomyopathy characterized by
 A Rare Case of Arrhythmogenic Right Ventricular Cardiomyopathy Co-existing with Isolated Left Ventricular Non-compaction NS Yelgeç, AT Alper, Aİ Tekkeşin, C Türkkan INTRODUCTION Arrhythmogenic right ventricular
A Rare Case of Arrhythmogenic Right Ventricular Cardiomyopathy Co-existing with Isolated Left Ventricular Non-compaction NS Yelgeç, AT Alper, Aİ Tekkeşin, C Türkkan INTRODUCTION Arrhythmogenic right ventricular
2017 EKG Workshop Advanced. Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA
 2017 EKG Workshop Advanced Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part II - Objective Describe a useful approach to interpreting
2017 EKG Workshop Advanced Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part II - Objective Describe a useful approach to interpreting
International recommendations for electrocardiographic interpretation in athletes
 European Heart Journal (2017) 00, 1 19 doi:101093/eurheartj/ehw631 CURRENT OPINION International recommendations for electrocardiographic interpretation in athletes Sanjay Sharma 1 *, Jonathan A Drezner
European Heart Journal (2017) 00, 1 19 doi:101093/eurheartj/ehw631 CURRENT OPINION International recommendations for electrocardiographic interpretation in athletes Sanjay Sharma 1 *, Jonathan A Drezner