Normal ECG And ECHO Findings in Athletes
|
|
|
- Helen Ashlie Burke
- 6 years ago
- Views:
Transcription
1 Normal ECG And ECHO Findings in Athletes Dr.Yahya Kiwan Consultant Interventional Cardiologist Head Of Departement Of Cardiology Canadian Specialist Hospital
2 Sinus Bradycardia The normal heartbeat is initiated by the sinus node which is located high in the right atrium near the junction of the superior vena cava and the right atrial appendage. To be classified as sinus rhythm, three criteria must be met: There must be a P wave before every QRS complex There must be a QRS complex after every P wave the P wave must have a normal axis in the frontal plane (0 90 s) Assuming an intact sinus node, the heart rate is set by the balance between the sympathetic and parasympathetic nervous systems. In healthy adults, sinus rhythm < 60 beats/min is considered as 'sinus bradycardia.
3 In well-trained athletes, resting sinus bradycardia is a common finding due to increased vagal tone. In endurance athletes, aerobic training also may induce intrinsic adaptations in the sinus node with decreased automaticity resulting in a high prevalence of sinus bradycardia. In the absence of symptoms such as fatigue, dizziness or syncope, a heart rate 30 beats/min should be considered normal in a well-trained athlete. Sinus bradycardia disappears with an increase in heart rate during physical activity.
 P wave before every QRS complex, (2) QRS after every P")
4 ECG demonstrates sinus bradycardia with a heart rate of 40 bpm. The three required features of sinus bradycardia include: (1) P wave before every QRS complex, (2) QRS after every P wave and (3) normal P wave axis (frontal plane 0 90 s
5 Sinus Arrhythmia The heart rate usually increases slightly during inspiration and decreases slightly during expiration. This response called sinus arrhythmia can be quite exaggerated in children and in well-trained athletes resulting in an irregular heart rhythm which originates from the sinus node. It has been estimated that up to 55% of well-trained athletes have sinus arrhythmia. This should not be confused with sinus node dysfunction (sick sinus syndrome).
6 Differentiating features that suggest sinus node dysfunction include lack of rhythmic changes in the heart rate, abrupt sustained rate increases and decreases and an inappropriate rate response to exercise (both a slowed acceleration and an inappropriately rapid deceleration), as well as any association with clinical symptoms such as exercise intolerance, presyncope and syncope. While the heart rhythm is quite irregular in sinus arrhythmia, the P wave axis remains normal in the frontal plane. Accelerating the heart rate with physical activity normalises the heart rhythm. Sinus arrhythmia is considered as a normal finding in an athlete.
 suggesting a sinus origin.")
7 ECG demonstrates sinus arrhythmia. Note the irregular heart rate that varies with respiration. The P waves are upright in leads I and avf (frontal plane) suggesting a sinus origin. This figure is only reproduced in colour in the online version
8 Junctional Escape Rhythm A junctional or nodal rhythm occurs when the QRS rate is faster than the resting P wave or sinus rate which is slowed in athletes due to increased vagal tone. The QRS rate for junctional rhythms is typically less than 100 beats/min, and the QRS complex usually narrow unless the baseline QRS has a bundle branch block. Sinus rhythm resumes with increased heart rates during exercise

9 ECG of a 28-year-old asymptomatic Caucasian handball player demonstrating a junctional escape rhythm. Note the constant RR interval between beats. This figure is only reproduced in colour in the online version.
10 Ectopic Atrial Rhythm In an ectopic atrial rhythm, P waves are present but are a different morphology compared to the sinus P wave. Ectopic P waves are most easily seen when the P waves are negative in the inferior leads. The atrial rate is typically less than 100 beats/min. There also may be more than two different P wave morphologies known as a wandering atrial pacemaker. Ectopic atrial rhythms occur due to a slowed resting sinus rate from increased vagal tone in athletes, and sinus rhythm replaces the ectopic atrial rhythm when the heart rate is increased during exercise.
, also known as")
11 ECG shows an ectopic atrial rhythm. The atrial rate is 63 beats/min and the P wave morphology is negative in leads II, III and avf (arrows), also known as a low atrial rhythm. This figure is only reproduced in colour in the online version.
12 First-degree AV Block In first-degree AV block, the PR interval is prolonged (>200 ms) but is the same duration on every beat This represents a delay in AV nodal conduction in athletes, due to increased vagal activity or intrinsic AV node changes, and typically resolves with faster heart rates during exercise.

13 ECG shows first-degree AV block (PR interval >200 ms). The PR interval is measured from the beginning of the P wave to the beginning of the QRS complex. This figure is only reproduced in colour in the online version.
14 Mobitz Type I (Wenckebach) Second-degree AV Block In Mobitz type I second-degree AV block, the PR interval progressively lengthens from beat to beat, until there is a non-conducted P wave with no QRS complex The first PR interval after the dropped beat is shorter than the last conducted PR interval before the dropped beat. This represents a greater disturbance of AV nodal conduction than firstdegree AV block, but with exercise there should be a return of 1:1 conduction.

15 ECG shows Mobitz type I (Wenckebach) second-degree AV block demonstrated by progressively longer PR intervals until there is a non-conducted P wave (arrows) and no QRS complex. Note the first PR interval after the dropped beat is shorter than the last conducted PR interval prior to the dropped beat. This figure is only reproduced in colour in the online version
16 Incomplete Right Bundle Branch Block IRBBB is defined by a QRS duration <120 ms with an RBBB pattern: terminal R wave in lead V1 (rsr') and wide terminal S wave in leads I and V6 IRBBB is seen in less than 10% of the general population but is observed in up to 40% of highly trained athletes, particularly those engaged in endurance training and mixed sport disciplines that include both aerobic and anaerobic components It has been suggested that the mildly delayed RV conduction is caused by RV remodelling, with increased cavity size and resultant increased conduction time, rather than an intrinsic delay within the His-Purkinje system itself

17 ECG demonstrates incomplete right bundle branch block (IRBBB) with rsr' pattern in V1 and QRS duration of <120 ms. IRBBB is a common and normal finding in athletes and does not require additional evaluation. This figure is only reproduced in colour in the online version.
18 The occurrence of IRBBB in an asymptomatic athlete with a negative family history and physical examination does not require further evaluation. During the physical examination, particular care should be devoted to the auscultation of a fixed splitting of the second heart sound because IRBBB can be an associated ECG finding in patients with an atrial septal defect. IRBBB may be seen in patients with arrhythmogenic RV cardiomyopathy (ARVC). However, in ARVC, the IRBBB pattern is usually associated with other ECG abnormalities, such as T wave inversion involving the mid-precordial leads beyond V2, low limb-lead voltages, prolonged S wave upstroke and/or premature ventricular beats with a left bundle branch block (LBBB) morphology
19 ECG from a patient with arrhythmogenic right ventricular cardiomyopathy showing delayed S wave upstroke in V1 (arrow), low voltages in limb leads < 5 mm (circles) and inverted T waves in anterior precordial leads (V1 V4) and inferior leads (III and avf). This figure is only reproduced in colour in the online version.
20 In some cases, IRBBB may be confused with a Brugada-ECG pattern, which is characterised by a high take-off and downsloping ST segment elevation followed by a negative T wave in 2 leads in V1 V3. Unlike the R' wave in IRBBB, the 'J wave' seen in a Brugada-ECG pattern does not indicate delayed RV activation, but reflects early repolarisation with J point elevation and a high take-off with downsloping ST segment followed by a negative T wave
 of Brugada-ECG is confined to right precordial leads (V1 and V2) without reciprocal 's wave' (of comparable voltage and duration) in leads I and V6 (arrowheads).")
21 (A) Brugada-ECG pattern mimicking IRBBB. The 'J wave' (arrows) of Brugada-ECG is confined to right precordial leads (V1 and V2) without reciprocal 's wave' (of comparable voltage and duration) in leads I and V6 (arrowheads). (B) IRBBB in a trained athlete. The RV conduction interval is mildly prolonged (QRS duration=115 ms) with a typical rsr' pattern in V1 (arrow). Note also the reciprocal 's wave' in V6 (arrow).
22 Early Repolarisation Early repolarisation is an ECG pattern consisting of ST elevation and/or a J wave (distinct notch) or slur on the downslope of the R wave Traditional examples of early repolarisation referred to ST elevation, but newer definitions also include J waves or terminal QRS slurring
. These are common, training-related findings in athletes and do not require more evaluation.")
23 ECG from a 29-year-old asymptomatic soccer player demonstrating early repolarisation (J-point and ST elevation) in I, II, avf, V2 V6 (arrows) and tall, peaked T waves (circles). These are common, training-related findings in athletes and do not require more evaluation. This figure is only reproduced in color in the online version.
 and with (B) a J wave.")
24 (A and B) Classic definition of early repolarisation based on ST elevation at QRS end (Jpoint). Examples without (A) and with (B) a J wave. (C and D) New definitions of early repolarisation showing slurred QRS downstroke (C) and J-wave (D) without ST elevation.
25 Early repolarisation is a common finding in trained athletes and considered a benign ECG pattern in apparently healthy, asymptomatic individuals. Depending on how it is defined, early repolarisation is reported in up to 35 91% of trained athletes and is more prevalent in young males and black/africans. Early repolarisation is most common in the precordial leads but can be present in any lead. Commercially available computer diagnostic ECG programmes commonly misreport early repolarisation patterns in athletes as acute ischaemia/myocardial infarction or pericarditis.
26 The early repolarisation pattern in athletes typically involves a concave and ascending/upward ST segment elevation. Late QRS slurring or notching with horizontal ST segment elevation in the inferolateral leads has been associated with an increased risk of arrhythmic death in one study of middle-aged, non-athletic Finnish citizens. However, a significant percentage of young competitive athletes (25 30%) show early repolarisation with similar morphological features in either the inferior or lateral leads. These findings are more common in athletes at times of peak fitness, suggesting early repolarisation is a dynamic process and is at least in part a direct result of exercise training.
27 To date, no data support the presence of an association between early repolarisation and SCD in athletes. Although further investigation is warranted to fully characterise the prognostic implications of early repolarisation in competitive athletes, all patterns of early repolarisation, including inferolateral subtypes, should be considered normal variants in athletes.
28 QRS Voltage Criteria for LVH The most commonly used voltage criterion for LVH is the Sokolow-Lyon index. However, ECG QRS voltage may not be a reliable predictor of LVH. The limitation of the ECG in identifying ventricular hypertrophy is due to the reliance of measuring the electrical activity of the heart by electrodes on the surface of the body. Consequently, anything between the left ventricular myocardium and the surface electrodes will affect the voltage. ECG QRS voltage, therefore, can be influenced by a variety of factors other than LV size or mass. Males, athletes and black/african individuals have higher QRS voltage, while obesity, older age and pulmonary disease may cause lower voltage
29 The goal of identifying clinically relevant LVH by voltage criteria alone is particularly problematic in children. The standards for QRS voltage have been derived from studies of populations of clinically normal children. Furthermore, the limited studies do not consistently include referencing to body size, gender or ethnicity. Lastly, correlation with echocardiography is limited, and reference standards from autopsy or MRI are not available. In athletes, intensive conditioning is also associated with morphological cardiac changes of increased cavity dimensions and wall thickness that are reflected on the ECG.
30 These changes constitute physiological LVH in trained athletes and usually manifests as an isolated increase in QRS amplitude ECGs with increased QRS amplitudes meeting ECG voltage criteria for LVH are prevalent and present in up to 45% of athletes and 25% of sedentary young adults. As a result, the accuracy of increased QRS voltage as an indicator of pathological LVH is poor.

31 ECG from a 19-year-old asymptomatic soccer player demonstrating voltage criteria for left ventricular hypertrophy (S-V1+R-V5>35 mm). Note the absence of left atrial enlargement, left axis deviation, ST depression, T wave inversion, or pathological Q waves. Increased QRS amplitude without other ECG abnormalities is a common finding in trained athletes and does not require additional testing. This figure is only reproduced in colour in the online version.
32 Increased QRS Voltage and HCM Several studies have evaluated athletes and young adults with isolated increased QRS voltage using echocardiography or cardiac MRI and none had hypertrophic cardiomyopathy (HCM) Furthermore, increased QRS voltage in the absence of other ECG abnormalities is uncommon in subjects with HCM being present in less than 2% of individuals with the disease. However, when other ECG abnormalities such as ST depression, T wave inversion, pathological Q waves, left axis deviation or left atrial abnormalities are present, the possibility of HCM should be investigated by additional testing

33 Therefore, isolated increased QRS voltage on the ECG in the absence of other abnormalities in an asymptomatic athlete with a negative family history is not a reliable indicator of LVH or HCM and does not require further evaluation. Abnormal ECG from a patient with hypertrophic cardiomyopathy. In addition to voltage criteria for left ventricular hypertrophy, note the deep T wave inversions extending to the lateral leads (I and avl, V5 V6). These findings are abnormal, not related to regular training and require additional evaluation. This figure is only reproduced in colour in the online version.
34 Repolarisation Findings in Black/African Athletes Growing attention has been paid to ethnic-related differences in morphological and ECG features of the athlete's heart. Notably, there are specific repolarisation patterns in black/african athletes that are normal variants and should be distinguished from abnormal findings suggestive of a pathological cardiac disorder. As aforementioned, early repolarisation is common in athletes and usually characterised by an elevated ST segment with upward concavity, ending in a positive (upright 'peaked') T wave There is also a normal variant early repolarisation pattern found in some black/african athletes, characterised by an elevated ST segment with upward convexity ('dome' shaped), followed by a negative T wave confined to leads V1 V4
.")
35 The presence of either repolarisation pattern in an asymptomatic black/african athlete does not require additional testing. ECG from a 24-year-old asymptomatic black/african soccer player demonstrating 'domed' ST elevation followed by T wave inversion in leads V1 V4 (circles). This is a normal repolarisation pattern in black/african athletes. This figure is only reproduced in colour in the online version.
36 Differentiating Normal Repolarisation Variants From Pathological Findings The presence of early repolarisation and T wave inversion in the anterior leads in black/african athletes probably represents a specific, ethnically dependent adaption to regular exercise. More than two-thirds of black athletes exhibit ST segment elevation and up to 25% show T wave inversions However, normal repolarisation changes in black/african athletes do not extend beyond V4. Thus, T wave inversion in the lateral leads (V5 V6) is always considered as an abnormal finding and requires additional testing to rule out HCM or other cardiomyopathies
 Pathological T wave inversion and ST depression in the lateral leads. T wave inversion in V5 V6 is always an abnormal finding and requires additional testing to rule out cardiomyopathy.")
37 (A) Normal variant repolarisation changes in a black/african athlete characterised by domed ST segment elevation and T wave inversion in V1 V4. (B) Pathological T wave inversion and ST depression in the lateral leads. T wave inversion in V5 V6 is always an abnormal finding and requires additional testing to rule out cardiomyopathy. This figure is only reproduced in colour in the online version.
38 Repolarisation variants in black/african athletes also must be distinguished from pathological repolarisation changes in the anterior precordial leads found in ARVC and Brugada-pattern ECGs. In ARVC, the ST segment is usually isoelectric prior to T wave inversion, in contrast to the 'domed' ST segment elevation which is the hallmark feature of the normal repolarisation variant in black/african athletes In Brugada-pattern ECGs, the high take-off and downsloping ST segment prior to T wave inversion distinguishes this from the 'domed' ST segment elevation preceding the negative T wave in black/african athletes Pathological repolarisation changes in the anterior precordial leads suggesting either ARVC or Brugada-pattern require additional testing.

39 (A) Normal variant repolarisation changes in a black/african athlete characterised by domed ST segment elevation and T wave inversion in V1 V4. (B) Pathological T wave inversion in V1 V3. Note the isoelectric ST segment. The absence of ST segment elevation prior to T wave inversion makes this ECG abnormal. Additional testing is required to rule out arrhythmogenic right ventricular cardiomyopathy. This figure is only reproduced in colour in the online version.
 A downsloping ST segment elevation followed by T wave inversion in V1 V2 suggestive of a Brugadapattern ECG.")
40 (A) Normal variant repolarisation changes in a black/african athlete characterised by domed ST segment elevation and T wave inversion in V1 V4. (B) A downsloping ST segment elevation followed by T wave inversion in V1 V2 suggestive of a Brugadapattern ECG. Note the high-take off and absence of upward convexity ('dome' shape) of the ST segment distinguishing this from the repolarisation variant in black/african athletes. This figure is only reproduced in colour in the online version.
41 Conclusions Fundamental to the cardiovascular care of athletes is an understanding of the physiological cardiac adaptations in athletes that are manifested on the ECG. The ECG can provide valuable information when interpreted properly, accounting for the electrical and structural changes that are a common result of regular training. Distinguishing ECG findings related to athlete's heart from changes suggestive of an underlying pathological disorder is critical to the identification of athletes at risk of SCD.
42 Echo indication in Athletes Family history of exertional syncope. Family history of sudden Cardiac Death. Those with Cardiac Symptoms
43 Athletes Doppler Many studies have shown cardiac changes that are induced by intense and regular physical activity. A study was conducted to evaluate cardiac structures and function in soccer players, cyclists and long-distance runners, and compare them with non-athlete controls. Cardiac structural, systolic, and diastolic function parameters in 53 athletes and 36 non-athlete controls were evaluated by Doppler echocardiography. Results of the study indicated that : Athletes presented higher left atrial volume, left ventricular (LV) thickness, and LV and right ventricular (RV) diastolic diameters (LVDD and RVDD, respectively) compared to non-athletes.
44 Left atrium and LVDD were higher in cyclists than runners, and RVDD was higher in cyclists than soccer players. LV mass index was higher in athletes, and cyclists had higher values than runners and soccer players. LV systolic function did not differ significantly between groups. The only altered index of LV diastolic function was a higher E/A ratio in cyclists compared to controls. There was no difference in LV E/E' ratio. RV systolic function evaluated by tissue Doppler imaging was higher in cyclists and soccer players than runners. There were no conclusive differences in RV diastolic function.
45 Conclusion From this study it was concluded that : Soccer players, runners and cyclists had remodeling of left and right ventricular structures compared to controls. Cardiac remodeling was more intense in cyclists than runners and soccer players.
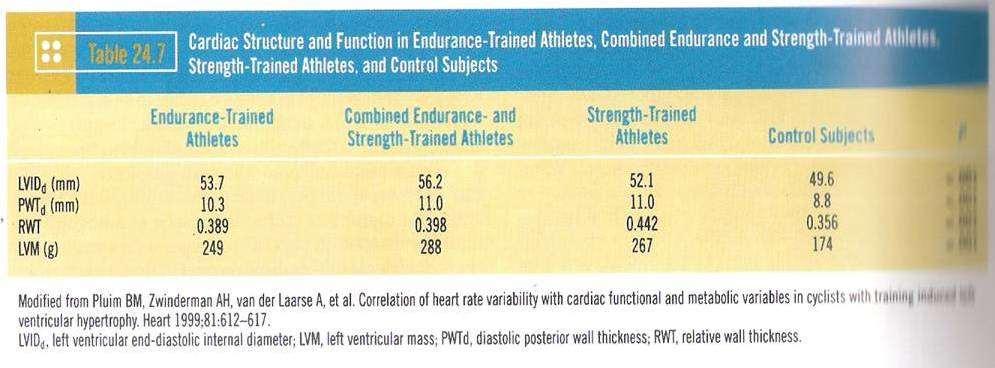
46 Structural features of the athlete heart as defined by echocardiography The morphologic concepts of the "athlete heart" have been enhanced and clarified over the last 10 years by virtue of M-mode echocardiographic studies performed on more than 1,000 competitive athletes. Long-term athletic training produces relatively mild but predictable alterations in cardiac structure that result in an increase in calculated left ventricular mass. This increase in mass observed in highly trained athletes is due to a mild increase in either transverse end-diastolic dimension of the left ventricle or left ventricular wall thickness, or both. Cardiac dimensions in athletes compared with matched control subjects show increases of about 10% for left ventricular enddiastolic dimension, about 15 to 20% for wall thickness and about 45% for calculated left ventricular mass.
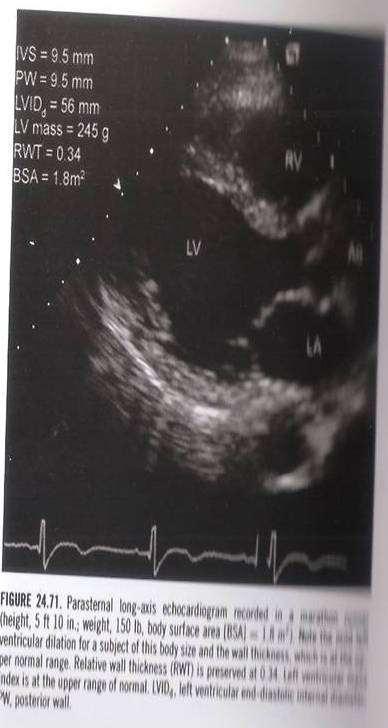
47 Furthermore, there is evidence that the modest degree of "physiologic" left ventricular hypertrophy (both the cavity dilation and wall thickening) observed in athletes is dynamic in nature, that is, it may develop rapidly within weeks or months after the initiation of vigorous conditioning and may be reversed in a similar time period after the cessation of training. Several echocardiographic studies also suggest that the precise alterations in cardiac structure associated with training may differ depending on the type of athletic activity undertaken (that is, whether training is primarily dynamic [isotonic] or static [isometric]). Although the ventricular septal to free wall thickness ratio (on M- mode echocardiogram) is almost always within normal limits (<1.3), occasionally an athlete will show mild asymmetric thickening of the anterior basal septum (usually 13 to 15 mm). This circumstance may mimic certain pathologic conditions characterized by primary left ventricular hypertrophy such as nonobstructive hypertrophic cardiomyopathy.
48 The long-term significance of increased left ventricular mass in trained athletes has not been conclusively defined. However, there is no evidence at this time suggesting that this form of hypertrophy is itself deleterious to the athlete or predisposes to (or prevents) the natural occurrence of cardiovascular disease later in life.
49
50

51
6/19/2018. Background Athlete s heart. Ultimate question. Applying the International Criteria for ECG
 Applying the International Criteria for ECG Interpretation in Athletes to a preparticipation screening program DAVE SIEBERT, MD, CAQSM ASSISTANT PROFESSOR DEPARTMENT OF FAMILY MEDICINE UNIVERSITY OF WASHINGTON
Applying the International Criteria for ECG Interpretation in Athletes to a preparticipation screening program DAVE SIEBERT, MD, CAQSM ASSISTANT PROFESSOR DEPARTMENT OF FAMILY MEDICINE UNIVERSITY OF WASHINGTON
at least 4 8 hours per week
 ECG IN ATHLETS An athlete is defined as an individual who engages in regular exercise or training for sport or general fitness, typically with a premium on performance, and often engaged in individual
ECG IN ATHLETS An athlete is defined as an individual who engages in regular exercise or training for sport or general fitness, typically with a premium on performance, and often engaged in individual
Study methodology for screening candidates to athletes risk
 1. Periodical Evaluations: each 2 years. Study methodology for screening candidates to athletes risk 2. Personal history: Personal history of murmur in childhood; dizziness, syncope, palpitations, intolerance
1. Periodical Evaluations: each 2 years. Study methodology for screening candidates to athletes risk 2. Personal history: Personal history of murmur in childhood; dizziness, syncope, palpitations, intolerance
ECG Underwriting Puzzler Dr. Regina Rosace AVP & Medical Director
 December 2018 ECG Underwriting Puzzler Dr. Regina Rosace AVP & Medical Director To obtain best results Select Slide Show from the ribbon at the top of your PowerPoint screen Select From Beginning on the
December 2018 ECG Underwriting Puzzler Dr. Regina Rosace AVP & Medical Director To obtain best results Select Slide Show from the ribbon at the top of your PowerPoint screen Select From Beginning on the
Current ECG interpretation guidelines in the screening of athletes
 REVIEW ARTICLE 7 How to differentiate physiological adaptation to intensive physical exercise from pathologies Current ECG interpretation guidelines in the screening of athletes Gemma Parry-Williams, Sanjay
REVIEW ARTICLE 7 How to differentiate physiological adaptation to intensive physical exercise from pathologies Current ECG interpretation guidelines in the screening of athletes Gemma Parry-Williams, Sanjay
How to Read an Athlete s ECG. Sanjay Sharma BSc (Hons), MD, FRCP, FESC
, MD, FRCP, FESC") How to Read an Athlete s ECG Sanjay Sharma BSc (Hons), MD, FRCP, FESC Athlete s EKG Vagotonia Sinus bradycardia Sinus arrhythmia First degree AVB ST-elevation Tall T waves Increased chamber size Left ventricular
How to Read an Athlete s ECG Sanjay Sharma BSc (Hons), MD, FRCP, FESC Athlete s EKG Vagotonia Sinus bradycardia Sinus arrhythmia First degree AVB ST-elevation Tall T waves Increased chamber size Left ventricular
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH
 ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
Cardiovascular Impacts of long-term endurance exercise: Implications of athlete s heart
 Cardiovascular Impacts of long-term endurance exercise: Implications of athlete s heart Dr. Gary Mak 麥耀光心臟科專科醫生 IPP of HK Associa4on of Sports Medicine and Sports Science Director of Pro-Cardio Heart Disease
Cardiovascular Impacts of long-term endurance exercise: Implications of athlete s heart Dr. Gary Mak 麥耀光心臟科專科醫生 IPP of HK Associa4on of Sports Medicine and Sports Science Director of Pro-Cardio Heart Disease
Historical Notes: Clinical Exercise Testing in the Athlete. An Efficient Heart. Structural Changes, Cont. Coronary Arteries
 Clinical Exercise Testing in the Athlete The athlete s heart Sudden cardiac death in athletes Screening athletes for cardiovascular disease Historical Notes: Giovanni Lancisi (father of cardiology), 17
Clinical Exercise Testing in the Athlete The athlete s heart Sudden cardiac death in athletes Screening athletes for cardiovascular disease Historical Notes: Giovanni Lancisi (father of cardiology), 17
Normal electrocardiographic findings: recognising physiological adaptations in athletes
 Scan to access more free content For numbered affiliations see end of article. Correspondence to Jonathan A Drezner, Department of Family Medicine, University of Washington, 1959 NE Pacific Street, Box
Scan to access more free content For numbered affiliations see end of article. Correspondence to Jonathan A Drezner, Department of Family Medicine, University of Washington, 1959 NE Pacific Street, Box
Interpretation and Consequences of Repolarisation Changes in Athletes
 Interpretation and Consequences of Repolarisation Changes in Athletes Professor Sanjay Sharma E-mail sasharma@sgul.ac.uk @SSharmacardio Disclosures: None Athlete s ECG Vagotonia Sinus bradycardia Sinus
Interpretation and Consequences of Repolarisation Changes in Athletes Professor Sanjay Sharma E-mail sasharma@sgul.ac.uk @SSharmacardio Disclosures: None Athlete s ECG Vagotonia Sinus bradycardia Sinus
Blocks & Dissociations. Reading Assignment (p47-52 in Outline )
") Blocks & Dissociations Reading Assignment (p47-52 in Outline ) Objectives Who are Wenckebach and Mobitz? Review SA and AV Blocks AV Dissociations: learning who s the boss and why 2 nd degree SA Block:
Blocks & Dissociations Reading Assignment (p47-52 in Outline ) Objectives Who are Wenckebach and Mobitz? Review SA and AV Blocks AV Dissociations: learning who s the boss and why 2 nd degree SA Block:
Paediatric ECG Interpretation
 Paediatric ECG Interpretation Dr Sanj Fernando (thanks to http://lifeinthefastlane.com/ecg-library/paediatric-ecginterpretation/) 3 yo boy complaining of abdominal pain and chest pain Child ECG vs Adult
Paediatric ECG Interpretation Dr Sanj Fernando (thanks to http://lifeinthefastlane.com/ecg-library/paediatric-ecginterpretation/) 3 yo boy complaining of abdominal pain and chest pain Child ECG vs Adult
François Carré Hôpital Pontchaillou -INSERM UMR1099-Université Rennes 1
 Normal electrocardiogram variants in Athletes François Carré Hôpital Pontchaillou -INSERM UMR1099-Université Rennes 1 Disclosures No disclosure of interest concerning this lecture The cardiovascular sport
Normal electrocardiogram variants in Athletes François Carré Hôpital Pontchaillou -INSERM UMR1099-Université Rennes 1 Disclosures No disclosure of interest concerning this lecture The cardiovascular sport
UNDERSTANDING YOUR ECG: A REVIEW
 UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
The Electrocardiogram part II. Dr. Adelina Vlad, MD PhD
 The Electrocardiogram part II Dr. Adelina Vlad, MD PhD Basic Interpretation of the ECG 1) Evaluate calibration 2) Calculate rate 3) Determine rhythm 4) Determine QRS axis 5) Measure intervals 6) Analyze
The Electrocardiogram part II Dr. Adelina Vlad, MD PhD Basic Interpretation of the ECG 1) Evaluate calibration 2) Calculate rate 3) Determine rhythm 4) Determine QRS axis 5) Measure intervals 6) Analyze
REtrive. REpeat. RElearn Design by. Test-Enhanced Learning based ECG practice E-book
 Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Dr. Schroeder has no financial relationships to disclose
 Valerie A Schroeder MD MS Assistant Professor University of Kansas Medical Center READING THE WAVES- THE HEART S ELECTRICAL MESSAGE FINANCIAL DISCLOSURE Dr. Schroeder has no financial relationships to
Valerie A Schroeder MD MS Assistant Professor University of Kansas Medical Center READING THE WAVES- THE HEART S ELECTRICAL MESSAGE FINANCIAL DISCLOSURE Dr. Schroeder has no financial relationships to
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016
 Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
Electrocardiography Abnormalities (Arrhythmias) 7. Faisal I. Mohammed, MD, PhD
 7. Faisal I. Mohammed, MD, PhD") Electrocardiography Abnormalities (Arrhythmias) 7 Faisal I. Mohammed, MD, PhD 1 Causes of Cardiac Arrythmias Abnormal rhythmicity of the pacemaker Shift of pacemaker from sinus node Blocks at different
Electrocardiography Abnormalities (Arrhythmias) 7 Faisal I. Mohammed, MD, PhD 1 Causes of Cardiac Arrythmias Abnormal rhythmicity of the pacemaker Shift of pacemaker from sinus node Blocks at different
General Introduction to ECG. Reading Assignment (p2-16 in PDF Outline )
") General Introduction to ECG Reading Assignment (p2-16 in PDF Outline ) Objectives 1. Practice the 5-step Method 2. Differential Diagnosis: R & L axis deviation 3. Differential Diagnosis: Poor R-wave progression
General Introduction to ECG Reading Assignment (p2-16 in PDF Outline ) Objectives 1. Practice the 5-step Method 2. Differential Diagnosis: R & L axis deviation 3. Differential Diagnosis: Poor R-wave progression
ECG Interpretation Made Easy
 ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School 2007-2008 ECG Interpretation Made Easy Synopsis Benefits Objectives Process
ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School 2007-2008 ECG Interpretation Made Easy Synopsis Benefits Objectives Process
Appendix D Output Code and Interpretation of Analysis
 Appendix D Output Code and Interpretation of Analysis 8 Arrhythmia Code No. Description 8002 Marked rhythm irregularity 8110 Sinus rhythm 8102 Sinus arrhythmia 8108 Marked sinus arrhythmia 8120 Sinus tachycardia
Appendix D Output Code and Interpretation of Analysis 8 Arrhythmia Code No. Description 8002 Marked rhythm irregularity 8110 Sinus rhythm 8102 Sinus arrhythmia 8108 Marked sinus arrhythmia 8120 Sinus tachycardia
By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG
 By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG recording Identify the ECG changes that occur in the presence
By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG recording Identify the ECG changes that occur in the presence
CLINICAL RESEARCH ON CARDIOVASCULAR ALTERATION ON 86 S PROFESSIONAL ATHLETES IN IRAN
 CLINICAL RESEARCH ON CARDIOVASCULAR ALTERATION ON 86 S PROFESSIONAL ATHLETES IN IRAN Lotfali Pourkazemi 1 * and Roghieh Razeghi Jadid 2 1 Sports Medicine Federation of Iran 2 Department of Herbal Sciences,
CLINICAL RESEARCH ON CARDIOVASCULAR ALTERATION ON 86 S PROFESSIONAL ATHLETES IN IRAN Lotfali Pourkazemi 1 * and Roghieh Razeghi Jadid 2 1 Sports Medicine Federation of Iran 2 Department of Herbal Sciences,
Introduction to ECG Gary Martin, M.D.
 Brief review of basic concepts Introduction to ECG Gary Martin, M.D. The electrical activity of the heart is caused by a sequence of rapid ionic movements across cell membranes resulting first in depolarization
Brief review of basic concepts Introduction to ECG Gary Martin, M.D. The electrical activity of the heart is caused by a sequence of rapid ionic movements across cell membranes resulting first in depolarization
Please check your answers with correct statements in answer pages after the ECG cases.
 ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
Case 1. Case 2. Case 3
 Case 1 The correct answer is D. Occasionally, the Brugada syndrome can present similar morphologies to A and also change depending on the lead position but in the Brugada pattern the r is wider and ST
Case 1 The correct answer is D. Occasionally, the Brugada syndrome can present similar morphologies to A and also change depending on the lead position but in the Brugada pattern the r is wider and ST
Basic electrocardiography reading. R3 lee wei-chieh
 Basic electrocardiography reading R3 lee wei-chieh The Normal Conduction System Lead Placement avf Limb Leads Precordial Leads Interpretation Rate Rhythm Interval Axis Chamber abnormality QRST change What
Basic electrocardiography reading R3 lee wei-chieh The Normal Conduction System Lead Placement avf Limb Leads Precordial Leads Interpretation Rate Rhythm Interval Axis Chamber abnormality QRST change What
Diploma in Electrocardiography
 The Society for Cardiological Science and Technology Diploma in Electrocardiography The Society makes this award to candidates who can demonstrate the ability to accurately record a resting 12-lead electrocardiogram
The Society for Cardiological Science and Technology Diploma in Electrocardiography The Society makes this award to candidates who can demonstrate the ability to accurately record a resting 12-lead electrocardiogram
SABIHA GATI AND SANJAY SHARMA
 9 The athlete s heart SABIHA GATI AND SANJAY SHARMA Pasieka/Science Photo Library In this article, the authors highlight the spectrum, magnitude and determinants of the athlete s heart and provide a practical
9 The athlete s heart SABIHA GATI AND SANJAY SHARMA Pasieka/Science Photo Library In this article, the authors highlight the spectrum, magnitude and determinants of the athlete s heart and provide a practical
PAEDIATRIC ECG Dimosthenis Avramidis, MD.
 PAEDIATRIC ECG Dimosthenis Avramidis, MD. Consultant Mitera Children s Hospital Athens Greece S. Associate 1st Cardiology Dpt Evangelismos Hospital Athens Greece 5 y/o with sinus tach Background ECG changes
PAEDIATRIC ECG Dimosthenis Avramidis, MD. Consultant Mitera Children s Hospital Athens Greece S. Associate 1st Cardiology Dpt Evangelismos Hospital Athens Greece 5 y/o with sinus tach Background ECG changes
Step by step approach to EKG rhythm interpretation:
 Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
EVALUATION OF ELECTROCARDIOGRAPHIC FINDINGS IN ATHLETES
 EVALUATION OF ELECTROCARDIOGRAPHIC FINDINGS IN ATHLETES UNIT OF INHERITED CV DISEASES HEART CENTER OF THE YOUNG AND ATHLETES A DPT OF CARDIOLOGY UNIVERSITY OF ATHENS EVALUATION OF ELECTROCARDIOGRAPHIC
EVALUATION OF ELECTROCARDIOGRAPHIC FINDINGS IN ATHLETES UNIT OF INHERITED CV DISEASES HEART CENTER OF THE YOUNG AND ATHLETES A DPT OF CARDIOLOGY UNIVERSITY OF ATHENS EVALUATION OF ELECTROCARDIOGRAPHIC
Miscellaneous Stuff Keep reading the Outline
 Miscellaneous Stuff Keep reading the Outline Welcome to the 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis= 1. Compute the 5 basic measurements:
Miscellaneous Stuff Keep reading the Outline Welcome to the 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis= 1. Compute the 5 basic measurements:
EKG screening in athletics
 Use of PPE EKG screening in athletics Stefan Montgomery MD, ATC 4/27/18 The overall role of the preparticipation physical evaluation (PPE) is to evaluate the health of the athlete to optimize safe sports
Use of PPE EKG screening in athletics Stefan Montgomery MD, ATC 4/27/18 The overall role of the preparticipation physical evaluation (PPE) is to evaluate the health of the athlete to optimize safe sports
SIMPLY ECGs. Dr William Dooley
 SIMPLY ECGs Dr William Dooley Content Basic ECG interpretation pattern Some common (examined) abnormalities Presenting ECGs in context Setting up an ECG Setting up an ECG 1 V1-4 th Right intercostal space
SIMPLY ECGs Dr William Dooley Content Basic ECG interpretation pattern Some common (examined) abnormalities Presenting ECGs in context Setting up an ECG Setting up an ECG 1 V1-4 th Right intercostal space
Myocardial Infarction. Reading Assignment (p66-78 in Outline )
") Myocardial Infarction Reading Assignment (p66-78 in Outline ) Objectives 1. Why do ST segments go up or down in ischemia? 2. STEMI locations and culprit vessels 3. Why 15-lead ECGs? 4. What s up with avr?
Myocardial Infarction Reading Assignment (p66-78 in Outline ) Objectives 1. Why do ST segments go up or down in ischemia? 2. STEMI locations and culprit vessels 3. Why 15-lead ECGs? 4. What s up with avr?
If the P wave > 0.12 sec( 3 mm) usually in any lead. Notched P wave usually in lead I,aVl may be lead II Negative terminal portion of P wave in V1, 1
 usually in any lead. Notched P wave usually in lead I,aVl may be lead II Negative terminal portion of P wave in V1, 1") If the P wave > 0.12 sec( 3 mm) usually in any lead. Notched P wave usually in lead I,aVl may be lead II Negative terminal portion of P wave in V1, 1 mm depth and 3 mm width( most specific) Since Mitral
If the P wave > 0.12 sec( 3 mm) usually in any lead. Notched P wave usually in lead I,aVl may be lead II Negative terminal portion of P wave in V1, 1 mm depth and 3 mm width( most specific) Since Mitral
FLB s What Are Those Funny-Looking Beats?
 FLB s What Are Those Funny-Looking Beats? Reading Assignment (pages 27-45 in Outline ) The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis=
FLB s What Are Those Funny-Looking Beats? Reading Assignment (pages 27-45 in Outline ) The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis=
ECG. Prepared by: Dr.Fatima Daoud Reference: Guyton and Hall Textbook of Medical Physiology,12 th edition Chapters: 11,12,13
 ECG Prepared by: Dr.Fatima Daoud Reference: Guyton and Hall Textbook of Medical Physiology,12 th edition Chapters: 11,12,13 The Concept When the cardiac impulse passes through the heart, electrical current
ECG Prepared by: Dr.Fatima Daoud Reference: Guyton and Hall Textbook of Medical Physiology,12 th edition Chapters: 11,12,13 The Concept When the cardiac impulse passes through the heart, electrical current
2017 EKG Workshop Advanced. Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA
 2017 EKG Workshop Advanced Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part II - Objective Describe a useful approach to interpreting
2017 EKG Workshop Advanced Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part II - Objective Describe a useful approach to interpreting
ECG Interpretation Cat Williams, DVM DACVIM (Cardiology)
") ECG Interpretation Cat Williams, DVM DACVIM (Cardiology) Providing the best quality care and service for the patient, the client, and the referring veterinarian. GOAL: Reduce Anxiety about ECGs Back to
ECG Interpretation Cat Williams, DVM DACVIM (Cardiology) Providing the best quality care and service for the patient, the client, and the referring veterinarian. GOAL: Reduce Anxiety about ECGs Back to
1 st Degree Block Prolonged P-R interval caused by first degree heart block (lead II)
") AV Heart Blocks 1 st degree A condition of a rhythm, not a true rhythm Need to always state underlying rhythm 2 nd degree Type I - Wenckebach Type II Classic dangerous to the patient Can be variable (periodic)
AV Heart Blocks 1 st degree A condition of a rhythm, not a true rhythm Need to always state underlying rhythm 2 nd degree Type I - Wenckebach Type II Classic dangerous to the patient Can be variable (periodic)
Reading Assignment (p1-91 in Outline ) Objectives What s in an ECG?
 Objectives What s in an ECG?") Reading Assignment (p1-91 in Outline ) Objectives What s in an ECG? The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis= 1. Compute the 5 basic
Reading Assignment (p1-91 in Outline ) Objectives What s in an ECG? The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis= 1. Compute the 5 basic
DEPARTMENT NAME PRE-PARTICIPATION SCREENING THE SPORTS PHYSICAL
 PRE-PARTICIPATION SCREENING THE SPORTS PHYSICAL Michele Krenek, MSN, RN, FNP-C TCHAPP Conference, Houston, TX April 4, 2019 PRE-PARTICIPATION SPORTS SCREENING According to the AHA the definition of the
PRE-PARTICIPATION SCREENING THE SPORTS PHYSICAL Michele Krenek, MSN, RN, FNP-C TCHAPP Conference, Houston, TX April 4, 2019 PRE-PARTICIPATION SPORTS SCREENING According to the AHA the definition of the
Electrocardiography for Healthcare Professionals. Chapter 14 Basic 12-Lead ECG Interpretation
 Electrocardiography for Healthcare Professionals Chapter 14 Basic 12-Lead ECG Interpretation 2012 The Companies, Inc. All rights reserved. Learning Outcomes 14.1 Discuss the anatomic views seen on a 12-lead
Electrocardiography for Healthcare Professionals Chapter 14 Basic 12-Lead ECG Interpretation 2012 The Companies, Inc. All rights reserved. Learning Outcomes 14.1 Discuss the anatomic views seen on a 12-lead
Supraventricular Arrhythmias. Reading Assignment. Chapter 5 (p17-30)
") Supraventricular Arrhythmias Reading Assignment Chapter 5 (p17-30) The Supraventricular Rhythms In Our Lives Site of Origin Single Events Slow Rates Intermediate Rates Fast Rates (>100 bpm) Sinus Sinus
Supraventricular Arrhythmias Reading Assignment Chapter 5 (p17-30) The Supraventricular Rhythms In Our Lives Site of Origin Single Events Slow Rates Intermediate Rates Fast Rates (>100 bpm) Sinus Sinus
ECG CONVENTIONS AND INTERVALS
 1 ECG Waveforms and Intervals ECG waveforms labeled alphabetically P wave== represents atrial depolarization QRS complex=ventricular depolarization ST-T-U complex (ST segment, T wave, and U wave)== V repolarization.
1 ECG Waveforms and Intervals ECG waveforms labeled alphabetically P wave== represents atrial depolarization QRS complex=ventricular depolarization ST-T-U complex (ST segment, T wave, and U wave)== V repolarization.
All About STEMIs. Presented By: Brittney Urvand, RN, BSN, CCCC. Essentia Health Fargo Cardiovascular Program Manager.
 All About STEMIs Presented By: Brittney Urvand, RN, BSN, CCCC Essentia Health Fargo Cardiovascular Program Manager Updated 10/2/2018 None Disclosures Objectives Identify signs and symptoms of a heart attack
All About STEMIs Presented By: Brittney Urvand, RN, BSN, CCCC Essentia Health Fargo Cardiovascular Program Manager Updated 10/2/2018 None Disclosures Objectives Identify signs and symptoms of a heart attack
Abnormal ECG patterns and significance in a group of mountaineers
 Original Article Abnormal ECG patterns and significance in a group of mountaineers Wg Cdr V Vasdev*, Wg Cdr DS Chadha +, Gp Capt P Kharbanda #, Lt Col SK Datta**, Air Cmde RK Ganjoo AVSM VSM ++ ABSTRACT
Original Article Abnormal ECG patterns and significance in a group of mountaineers Wg Cdr V Vasdev*, Wg Cdr DS Chadha +, Gp Capt P Kharbanda #, Lt Col SK Datta**, Air Cmde RK Ganjoo AVSM VSM ++ ABSTRACT
Introduction to Electrocardiography
 Introduction to Electrocardiography Class Objectives: Introduction to ECG monitoring Discuss principles of interpretation Identify the components and measurements of the ECG ECG analysis ECG Monitoring
Introduction to Electrocardiography Class Objectives: Introduction to ECG monitoring Discuss principles of interpretation Identify the components and measurements of the ECG ECG analysis ECG Monitoring
Degrees AV blocks in athletes
 Degrees AV blocks in athletes Name: BCA Age: 22yo Sex: Male Race: Black Weight: 82 kg Height: 1.96m Biotype: Athletic rofession: professional basketball player Date: 2/09/2001 Clinical diagnosis: athlete
Degrees AV blocks in athletes Name: BCA Age: 22yo Sex: Male Race: Black Weight: 82 kg Height: 1.96m Biotype: Athletic rofession: professional basketball player Date: 2/09/2001 Clinical diagnosis: athlete
ECG Interpretation. Best to have a system to methodically evaluate ECG (from Dubin) * Rate * Rhythm * Axis * Intervals * Hypertrophy * Infarction
 * Rate * Rhythm * Axis * Intervals * Hypertrophy * Infarction") ECG to save Babies ECG Interpretation Best to have a system to methodically evaluate ECG (from Dubin) * Rate * Rhythm * Axis * Intervals * Hypertrophy * Infarction Electrical Activity in the heart 5 events
ECG to save Babies ECG Interpretation Best to have a system to methodically evaluate ECG (from Dubin) * Rate * Rhythm * Axis * Intervals * Hypertrophy * Infarction Electrical Activity in the heart 5 events
Conduction Problems / Arrhythmias. Conduction
 Conduction Problems / Arrhythmias Conduction Wolf-Parkinson White Syndrome (WPW) and Lown-Ganong-Levine (LGL): Atrial impulses bypass the AV node through an accessory pathway or bypass tract (bundle of
Conduction Problems / Arrhythmias Conduction Wolf-Parkinson White Syndrome (WPW) and Lown-Ganong-Levine (LGL): Atrial impulses bypass the AV node through an accessory pathway or bypass tract (bundle of
12 LEAD EKG BASICS. By: Steven Jones, NREMT P CLEMC
 12 LEAD EKG BASICS By: Steven Jones, NREMT P CLEMC ECG Review Waves and Intervals P wave: the sequential activation (depolarization) of the right and left atria QRS complex: right and left ventricular
12 LEAD EKG BASICS By: Steven Jones, NREMT P CLEMC ECG Review Waves and Intervals P wave: the sequential activation (depolarization) of the right and left atria QRS complex: right and left ventricular
12-Lead ECG Interpretation. Kathy Kuznar, RN, ANP
 12-Lead ECG Interpretation Kathy Kuznar, RN, ANP The 12-Lead ECG Objectives Identify the normal morphology and features of the 12- lead ECG. Perform systematic analysis of the 12-lead ECG. Recognize abnormalities
12-Lead ECG Interpretation Kathy Kuznar, RN, ANP The 12-Lead ECG Objectives Identify the normal morphology and features of the 12- lead ECG. Perform systematic analysis of the 12-lead ECG. Recognize abnormalities
HR: 50 bpm (Sinus) PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70. Sinus bradycardia with one ventricular escape (*)
 PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70. Sinus bradycardia with one ventricular escape (*)") 1? HR: 50 bpm (Sinus) PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70 1 Sinus P waves? 2 sinus cycles The pause (2 sinus cycles) suggests that the sinus fired (?) but did not conduct to the atria (i.e., missing
1? HR: 50 bpm (Sinus) PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70 1 Sinus P waves? 2 sinus cycles The pause (2 sinus cycles) suggests that the sinus fired (?) but did not conduct to the atria (i.e., missing
Professor Sanjay Sharma St George s University of London
 How to Evaluate an Athlete of Afro- Caribbean Origin. Professor Sanjay Sharma St George s University of London Background: Causes of SCD in Sport Young competitive athlete Personal and family history Physical
How to Evaluate an Athlete of Afro- Caribbean Origin. Professor Sanjay Sharma St George s University of London Background: Causes of SCD in Sport Young competitive athlete Personal and family history Physical
Abnormal electrocardiographic findings in athletes: recognising changes suggestive of cardiomyopathy
 Scan to access more free content For numbered affiliations see end of article Correspondence to Jonathan A Drezner, Department of Family Medicine, University of Washington, 1959 NE Pacific Street, Box
Scan to access more free content For numbered affiliations see end of article Correspondence to Jonathan A Drezner, Department of Family Medicine, University of Washington, 1959 NE Pacific Street, Box
International Criteria for Electrocardiographic Interpretation in Athletes
 International Criteria for Electrocardiographic Interpretation in Athletes Jonathan A. Drezner, MD* 1, Sanjay Sharma, MD* 2, Aaron Baggish, MD 3, Michael Papadakis, MD 2, Mathew G. Wilson, PhD 4, Jordan
International Criteria for Electrocardiographic Interpretation in Athletes Jonathan A. Drezner, MD* 1, Sanjay Sharma, MD* 2, Aaron Baggish, MD 3, Michael Papadakis, MD 2, Mathew G. Wilson, PhD 4, Jordan
ELECTROCARDIOGRAPH. General. Heart Rate. Starship Children s Health Clinical Guideline
 General Heart Rate QRS Axis T Wave Axis PR Interval according to Heart Rate & Age P Wave Duration and Amplitude QRS Duration according to Age QT Interval R & S voltages according to Lead & Age R/S ratio
General Heart Rate QRS Axis T Wave Axis PR Interval according to Heart Rate & Age P Wave Duration and Amplitude QRS Duration according to Age QT Interval R & S voltages according to Lead & Age R/S ratio
Family Medicine for English language students of Medical University of Lodz ECG. Jakub Dorożyński
 Family Medicine for English language students of Medical University of Lodz ECG Jakub Dorożyński Parts of an ECG The standard ECG has 12 leads: six of them are considered limb leads because they are placed
Family Medicine for English language students of Medical University of Lodz ECG Jakub Dorożyński Parts of an ECG The standard ECG has 12 leads: six of them are considered limb leads because they are placed
ECGs: Everything a finalist needs to know. Dr Amy Coulden As part of the Simply Finals series
 ECGs: Everything a finalist needs to know Dr Amy Coulden As part of the Simply Finals series Aims and objectives To be able to interpret basic ECG abnormalities To be able to recognise commonly tested
ECGs: Everything a finalist needs to know Dr Amy Coulden As part of the Simply Finals series Aims and objectives To be able to interpret basic ECG abnormalities To be able to recognise commonly tested
The frontier between normal and abnormal electrocardiogram in athletes
 The frontier between normal and abnormal electrocardiogram in athletes ESC Congress 2011 Paris F. Carré University Rennes 1-Pontchaillou Hospital Inserm U642, Rennes - F-35000 Cardiovascular preparticipation
The frontier between normal and abnormal electrocardiogram in athletes ESC Congress 2011 Paris F. Carré University Rennes 1-Pontchaillou Hospital Inserm U642, Rennes - F-35000 Cardiovascular preparticipation
Section V. Objectives
 Section V Landscape of an MI Objectives At the conclusion of this presentation the participant will be able to Outline a systematic approach to 12 lead ECG interpretation Demonstrate the process for determining
Section V Landscape of an MI Objectives At the conclusion of this presentation the participant will be able to Outline a systematic approach to 12 lead ECG interpretation Demonstrate the process for determining
12 Lead ECG Skills: Building Confidence for Clinical Practice. Presented By: Cynthia Webner, BSN, RN, CCRN-CMC. Karen Marzlin, BSN, RN,CCRN-CMC
 12 Lead ECG Skills: Building Confidence for Clinical Practice NTI 2009 Preconference Session 803 Presented By: Karen Marzlin, BSN, RN,CCRN-CMC 1 12 Lead ECG Fundamentals: The Starting Place for Linking
12 Lead ECG Skills: Building Confidence for Clinical Practice NTI 2009 Preconference Session 803 Presented By: Karen Marzlin, BSN, RN,CCRN-CMC 1 12 Lead ECG Fundamentals: The Starting Place for Linking
2017 EKG Workshop Basic. Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA
 2017 EKG Workshop Basic Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part I - Objectives Discuss a systematic approach to EKG interpretation
2017 EKG Workshop Basic Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part I - Objectives Discuss a systematic approach to EKG interpretation
Understanding the 12-lead ECG, part II
 Bundle-branch blocks Understanding the 12-lead ECG, part II Most common electrocardiogram (ECG) abnormality Appears as a wider than normal S complex Occurs when one of the two bundle branches can t conduct
Bundle-branch blocks Understanding the 12-lead ECG, part II Most common electrocardiogram (ECG) abnormality Appears as a wider than normal S complex Occurs when one of the two bundle branches can t conduct
SIMPLY ECGs. Dr William Dooley
 SIMPLY ECGs Dr William Dooley 1 No anatomy just interpretation 2 Setting up an ECG 3 Setting up an ECG 1 V1-4 th Right intercostal space at sternal border 2 V2-4 th Left intercostal space at sternal border
SIMPLY ECGs Dr William Dooley 1 No anatomy just interpretation 2 Setting up an ECG 3 Setting up an ECG 1 V1-4 th Right intercostal space at sternal border 2 V2-4 th Left intercostal space at sternal border
Relax and Learn At the Farm 2012
 Relax and Learn At the Farm 2012 Session 2: 12 Lead ECG Fundamentals 101 Cynthia Webner DNP, RN, CCNS, CCRN-CMC, CHFN Though for Today Mastery is not something that strikes in an instant, like a thunderbolt,
Relax and Learn At the Farm 2012 Session 2: 12 Lead ECG Fundamentals 101 Cynthia Webner DNP, RN, CCNS, CCRN-CMC, CHFN Though for Today Mastery is not something that strikes in an instant, like a thunderbolt,
10 ECGs No Practitioner Can Afford to Miss. Objectives
 10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
Bundle Branch & Fascicular Blocks. Reading Assignment (p53-58 in Outline )
") Bundle Branch & Fascicular Blocks Reading Assignment (p53-58 in Outline ) Objectives 1. QRS analysis of Right and Left BBB 2. Uncomplicated vs complicated BBB 3. Diagnosis of RBBB with LAFB and LPFB 4.
Bundle Branch & Fascicular Blocks Reading Assignment (p53-58 in Outline ) Objectives 1. QRS analysis of Right and Left BBB 2. Uncomplicated vs complicated BBB 3. Diagnosis of RBBB with LAFB and LPFB 4.
ECG (MCQs) In the fundamental rules of the ECG all the following are right EXCEP:
 In the fundamental rules of the ECG all the following are right EXCEP:") ECG (MCQs) 2010 1- In the fundamental rules of the ECG all the following are right EXCEP: a- It is a biphasic record of myocardial action potential fluctuations. b- Deflection record occurs only during
ECG (MCQs) 2010 1- In the fundamental rules of the ECG all the following are right EXCEP: a- It is a biphasic record of myocardial action potential fluctuations. b- Deflection record occurs only during
Dr Navin Chandra Clinical Research Fellow in Cardiology St George s University of London
 Dr Navin Chandra Clinical Research Fellow in Cardiology St George s University of London Cardiac Adaptation in Athletes Athletic training for prolonged periods may result in physiological adaptations of
Dr Navin Chandra Clinical Research Fellow in Cardiology St George s University of London Cardiac Adaptation in Athletes Athletic training for prolonged periods may result in physiological adaptations of
Cardiology Flash Cards
 Cardiology Flash Cards EKG in a nut shell www.brain101.info Conduction System www.brain101.info 2 Analyzing EKG Step by step Steps in Analyzing ECG'S 1. Rhythm: - Regular _ Sinus, Junctional or Ventricular.
Cardiology Flash Cards EKG in a nut shell www.brain101.info Conduction System www.brain101.info 2 Analyzing EKG Step by step Steps in Analyzing ECG'S 1. Rhythm: - Regular _ Sinus, Junctional or Ventricular.
ECG Workshop. Nezar Amir
 ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
15 16 September Seminar W10O. ECG for General Practice
 15 16 September 2012 Seminar W10O ECG for General Practice Speaker: Ms Natasha Eaton ECG for General Practice Speaker: Natasha Eaton Cardiac CNC Executive Representative Electrocardiography The graphic
15 16 September 2012 Seminar W10O ECG for General Practice Speaker: Ms Natasha Eaton ECG for General Practice Speaker: Natasha Eaton Cardiac CNC Executive Representative Electrocardiography The graphic
DR QAZI IMTIAZ RASOOL OBJECTIVES
 PRACTICAL ELECTROCARDIOGRAPHY DR QAZI IMTIAZ RASOOL OBJECTIVES Recording of electrical events in heart Established electrode pattern results in specific tracing pattern Health of heart i. e. Anatomical
PRACTICAL ELECTROCARDIOGRAPHY DR QAZI IMTIAZ RASOOL OBJECTIVES Recording of electrical events in heart Established electrode pattern results in specific tracing pattern Health of heart i. e. Anatomical
The ECG in healthy people
 The ECG in healthy people The normal cardiac rhythm 3 The heart rate 3 Extrasystoles 7 The P wave 7 The PR interval The QRS complex 3 The ST segment 29 The T wave 33 The QT interval 42 The ECG in athletes
The ECG in healthy people The normal cardiac rhythm 3 The heart rate 3 Extrasystoles 7 The P wave 7 The PR interval The QRS complex 3 The ST segment 29 The T wave 33 The QT interval 42 The ECG in athletes
ECGs and Arrhythmias: Family Medicine Board Review 2009
 Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
Bradydysrhythmias and Atrioventricular Conduction Blocks
 Emerg Med Clin N Am 24 (2006) 1 9 Bradydysrhythmias and Atrioventricular Conduction Blocks Jacob W. Ufberg, MD*, Jennifer S. Clark, MD Department of Emergency Medicine, Temple University School of Medicine,
Emerg Med Clin N Am 24 (2006) 1 9 Bradydysrhythmias and Atrioventricular Conduction Blocks Jacob W. Ufberg, MD*, Jennifer S. Clark, MD Department of Emergency Medicine, Temple University School of Medicine,
Understanding basics of EKG
 Understanding basics of EKG By Alula A.(R III) www.le.ac.uk Topic for discussion Understanding of cellular electrophysiology Basics Rate Rhythm Axis Intervals P wave QRS ST/T wave Abnormal EKGs Understanding
Understanding basics of EKG By Alula A.(R III) www.le.ac.uk Topic for discussion Understanding of cellular electrophysiology Basics Rate Rhythm Axis Intervals P wave QRS ST/T wave Abnormal EKGs Understanding
ECG Practice Strips Discussion part 1:
 ECG Practice Strips Discussion part 1: The first 20 strips are for teaching various abnormalities of the morphology of the waves of the ECG. Strips 21 and following are for teaching some abnormalities
ECG Practice Strips Discussion part 1: The first 20 strips are for teaching various abnormalities of the morphology of the waves of the ECG. Strips 21 and following are for teaching some abnormalities
Return to Basics. ECG Rate and Rhythm. Management of the Hospitalized Patient September 25, 2009
 Management of the Hospitalized Patient September 25, 2009 ECG Refresher and Update 2009 Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Management of the Hospitalized Patient September 25, 2009 ECG Refresher and Update 2009 Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
This presentation will deal with the basics of ECG description as well as the physiological basics of
 Snímka 1 Electrocardiography basics This presentation will deal with the basics of ECG description as well as the physiological basics of Snímka 2 Lecture overview 1. Cardiac conduction system functional
Snímka 1 Electrocardiography basics This presentation will deal with the basics of ECG description as well as the physiological basics of Snímka 2 Lecture overview 1. Cardiac conduction system functional
Office ECG Interpretation
 Office ECG Interpretation Jason Evanchan, DO Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center Outline of topics High risk ischemia T wave
Office ECG Interpretation Jason Evanchan, DO Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center Outline of topics High risk ischemia T wave
Pathologic ECG. Adelina Vlad, MD PhD
 Pathologic ECG Adelina Vlad, MD PhD Basic Interpretation of the ECG 1) Evaluate calibration 2) Calculate rate 3) Determine rhythm 4) Determine QRS axis 5) Measure intervals 6) Analyze the morphology and
Pathologic ECG Adelina Vlad, MD PhD Basic Interpretation of the ECG 1) Evaluate calibration 2) Calculate rate 3) Determine rhythm 4) Determine QRS axis 5) Measure intervals 6) Analyze the morphology and
12 Lead ECG Interpretation
 12 Lead ECG Interpretation Julie Zimmerman, MSN, RN, CNS, CCRN Significant increase in mortality for every 15 minutes of delay! N Engl J Med 2007;357:1631-1638 Who should get a 12-lead ECG? Also include
12 Lead ECG Interpretation Julie Zimmerman, MSN, RN, CNS, CCRN Significant increase in mortality for every 15 minutes of delay! N Engl J Med 2007;357:1631-1638 Who should get a 12-lead ECG? Also include
International recommendations for electrocardiographic interpretation in athletes
 European Heart Journal (2017) 00, 1 19 doi:101093/eurheartj/ehw631 CURRENT OPINION International recommendations for electrocardiographic interpretation in athletes Sanjay Sharma 1 *, Jonathan A Drezner
European Heart Journal (2017) 00, 1 19 doi:101093/eurheartj/ehw631 CURRENT OPINION International recommendations for electrocardiographic interpretation in athletes Sanjay Sharma 1 *, Jonathan A Drezner
EKG Abnormalities. Adapted from:
 EKG Abnormalities Adapted from: http://www.bem.fi/book/19/19.htm Some key terms: Arrhythmia-an abnormal rhythm or sequence of events in the EKG Flutter-rapid depolarizations (and therefore contractions)
EKG Abnormalities Adapted from: http://www.bem.fi/book/19/19.htm Some key terms: Arrhythmia-an abnormal rhythm or sequence of events in the EKG Flutter-rapid depolarizations (and therefore contractions)
Cardiac hypertrophy and how it may break an athlete s heart e the Cypriot case
 Eur J Echocardiography (2005) 6, 301e307 Cardiac hypertrophy and how it may break an athlete s heart e the Cypriot case C.E. Chee a,1, C.P. Anastassiades a,1, A.G. Antonopoulos b, A.A. Petsas b, L.C. Anastassiades
Eur J Echocardiography (2005) 6, 301e307 Cardiac hypertrophy and how it may break an athlete s heart e the Cypriot case C.E. Chee a,1, C.P. Anastassiades a,1, A.G. Antonopoulos b, A.A. Petsas b, L.C. Anastassiades
Acute Coronary Syndromes Unstable Angina Non ST segment Elevation MI (NSTEMI) ST segment Elevation MI (STEMI)
 ST segment Elevation MI (STEMI)") Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Evaluate common abnormalities that mimic myocardial infarction. Identify
Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Evaluate common abnormalities that mimic myocardial infarction. Identify
PECTUS EXCAVATUM WITH SPONTANEOUS TYPE 1 ECG BRUGADA PATTERN OR BRUGADA LIKE PHENOTYPE: ANOTHER BRUGADA ECG PHENOCOPY
 PECTUS EXCAVATUM WITH SPONTANEOUS TYPE 1 ECG BRUGADA PATTERN OR BRUGADA LIKE PHENOTYPE: ANOTHER BRUGADA ECG PHENOCOPY ANDRÉS RICARDO PÉREZ RIERA MD Chief of the Sector of Electro-Vectocardiography of the
PECTUS EXCAVATUM WITH SPONTANEOUS TYPE 1 ECG BRUGADA PATTERN OR BRUGADA LIKE PHENOTYPE: ANOTHER BRUGADA ECG PHENOCOPY ANDRÉS RICARDO PÉREZ RIERA MD Chief of the Sector of Electro-Vectocardiography of the
TEST BANK FOR ECGS MADE EASY 5TH EDITION BY AEHLERT
 Link download full: http://testbankair.com/download/test-bank-for-ecgs-made-easy-5thedition-by-aehlert/ TEST BANK FOR ECGS MADE EASY 5TH EDITION BY AEHLERT Chapter 5 TRUE/FALSE 1. The AV junction consists
Link download full: http://testbankair.com/download/test-bank-for-ecgs-made-easy-5thedition-by-aehlert/ TEST BANK FOR ECGS MADE EASY 5TH EDITION BY AEHLERT Chapter 5 TRUE/FALSE 1. The AV junction consists
Return to Basics. Normal Intervals & Axes. ECG Rate and Rhythm
 Return to Basics Management of the Hospitalized Patient October 15, 2010 ECG Refresher and Update 2010 Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Return to Basics Management of the Hospitalized Patient October 15, 2010 ECG Refresher and Update 2010 Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
ECG interpretation basics
 ECG interpretation basics Michał Walczewski, MD Krzysztof Ozierański, MD 21.03.18 Electrical conduction system of the heart Limb leads Precordial leads 21.03.18 Precordial leads Precordial leads 21.03.18
ECG interpretation basics Michał Walczewski, MD Krzysztof Ozierański, MD 21.03.18 Electrical conduction system of the heart Limb leads Precordial leads 21.03.18 Precordial leads Precordial leads 21.03.18
La valutazione dell atleta: è una strategia salva-vita e costo-efficace?
 La valutazione dell atleta: è una strategia salva-vita e costo-efficace? Primo trattato di Medicina Wilson and Jungner s criteria In the 1960s the World Health Organization adopted the Wilson and Jungner
La valutazione dell atleta: è una strategia salva-vita e costo-efficace? Primo trattato di Medicina Wilson and Jungner s criteria In the 1960s the World Health Organization adopted the Wilson and Jungner
3/4/2018. March Martina Frost, PA C Desert Cardiology. Electricity moving towards/away from electrode create downward/upward directions of waves
 March 2018 Martina Frost, PA C Desert Cardiology Electricity moving towards/away from electrode create downward/upward directions of waves Frontal view Limb leads: I, II, III, avl, avf, (avr) Horizontal
March 2018 Martina Frost, PA C Desert Cardiology Electricity moving towards/away from electrode create downward/upward directions of waves Frontal view Limb leads: I, II, III, avl, avf, (avr) Horizontal
Lecture outline. Electrical properties of the heart. Automaticity. Excitability. Refractoriness. The ABCs of ECGs Back to Basics Part I
 Lecture outline The ABCs of ECGs Back to Basics Part I Meg Sleeper VMD, DACVIM (cardiology) University of Florida Veterinary School Electrical properties of the heart Action potentials Normal intracardiac
Lecture outline The ABCs of ECGs Back to Basics Part I Meg Sleeper VMD, DACVIM (cardiology) University of Florida Veterinary School Electrical properties of the heart Action potentials Normal intracardiac