Nephrotic Syndrome -membranous nephropathy-
|
|
|
- Trevor Matthews
- 5 years ago
- Views:
Transcription
1 Nephrotic Syndrome -membranous nephropathy- APSN Continuing Medical Education (CME) course July 2 nd, 2014 Yokohama, Japan Shoichi Maruyama, M.D. Nagoya University Graduate School of Medicine
2 This presentation is constructed in reference to the educational course entitled MEMBRANOUS NEPHROPATHY: Treatment in the Modern Era. presented by Dr. Richard Glassock, in KDIGO- Mumbai Nephrology Summit, Mumbai, India I tried to review the evidence from Asian countries, including China, Korea, India and Japan. The management can be different in different regions.
3 APSN CME 2014 YOKOHAMA Case 1 (1). A 80-year-old man visits our hospital because of persistent ankle edema for 4 months. His urine protein excretion is 7.89 g/day and urine sediments show RBC/hpf. His serum albumin is 2.0 gms/dl, and serum creatinine is 0.8 mg/dl. He has been treated with CCB for ten years. He has past history of early gastric cancer which was cured by endoscopic mucosal resection 6 years ago. Upper gastrointestinal endoscopy performed last year showed no malignancy. Blood pressure is 150/75mmHg. 2+ pitting edema of ankles is present. Abdominal CT shows no abnormality.
4 Q1. Which kind of renal pathology would you expect? Q2. Would you perform renal biopsy?


5 Clin Exp Nephrol Dec;16(6): J-KDR/J-RBR

6 Nephrotic Syndrome in Japan Glomerular lesions of nephrotic syndrome patients in Japan. J-RBR registry: 2066 cases in total; 1203 cases of primary glomerular disease. Membranous nephropathy accounted for 37% of the idiopathic nephrotic syndrome cases in Japan. Clin Exp Nephrol (2012) 16:

7 Idiopathic nephrotic syndrome patients in Japan Glomerular lesions of idiopathic nephrotic syndrome patients in Japan according to age. J-RBR registry: 1203 cases of primary glomerular disease excluding IgA nephropathy. Clin Exp Nephrol (2012) 16:
 16:903")
8 Clin Exp Nephrol (2012) 16:
9 Clin Exp Nephrol (2012) 16:
10 Clin Exp Nephrol (2012) 16:
11 Q1. Which kind of renal pathology would you expect? 1. Membranous nephropathy 2. MCD 3. FSGS 4. MPGN 5. IgA-N 6. Amyloidosis 7. Infection related GN 8. Lupus Nephritis 9. Others Q2. Would you perform renal biopsy? Yes
12 Q3 Before performing renal biopsy, which of the following would you request? A. Anti-nuclear antibody and anti-dsdna assay B. Serum Hepatitis B surface antigen C. HCV Ab D. Serum Protein Electrophoresis E. Complement C3 and C4 Answer. I would order all of the above. The test results are all negative or normal.
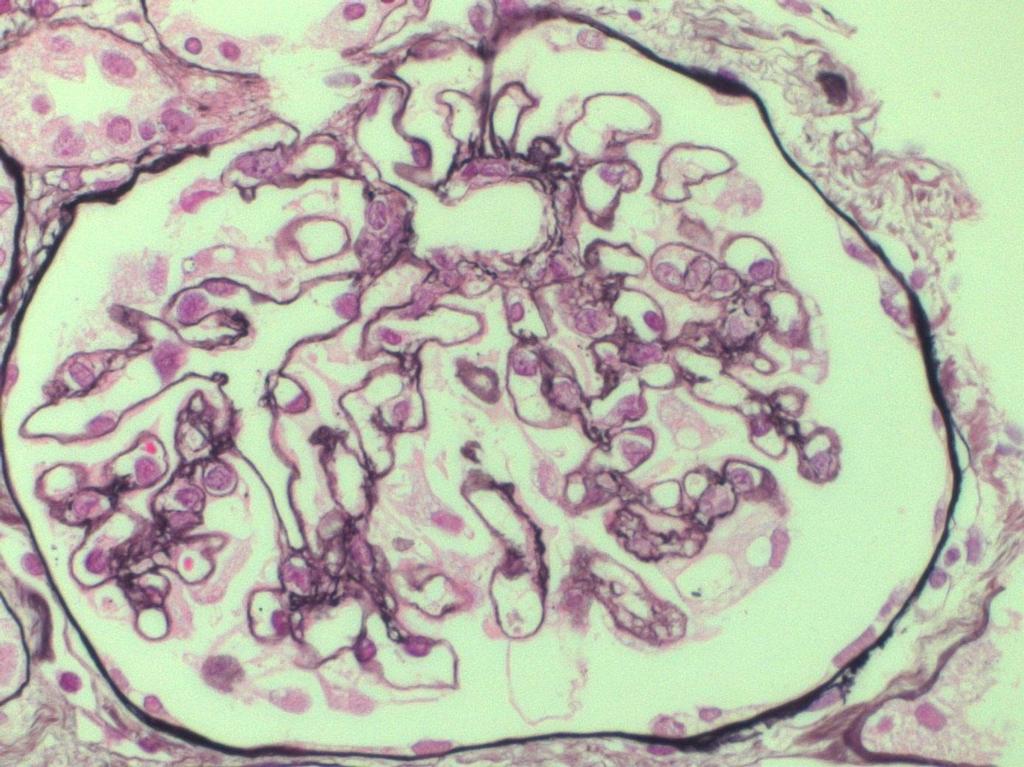
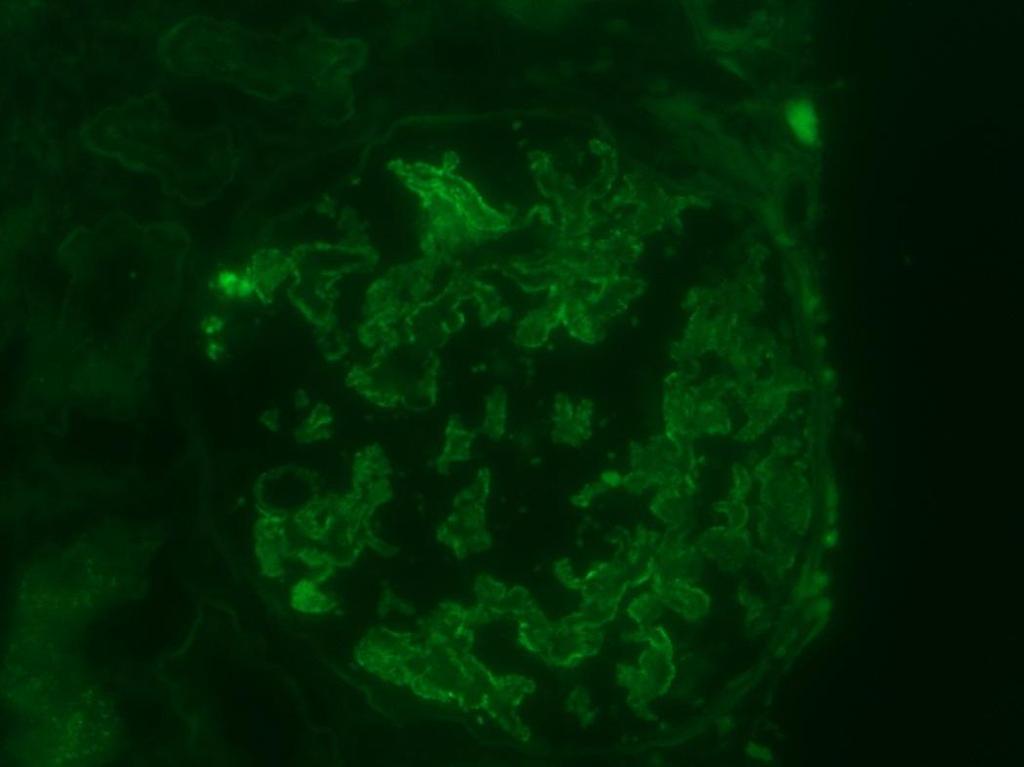
13 Case 1(2) A renal biopsy was performed. Light microscopy reveals slightly thickened capillary walls, without proliferation. IF shows 3+ granular IgG and 2+ granular C3 along the glomerular capillary wall. No mesangial deposits is seen. IgA and C4 are weakly positive (+). IgM and C1q are negative. EM shows thickened basement membrane, spikes and electron dense deposits along the subepithelium.

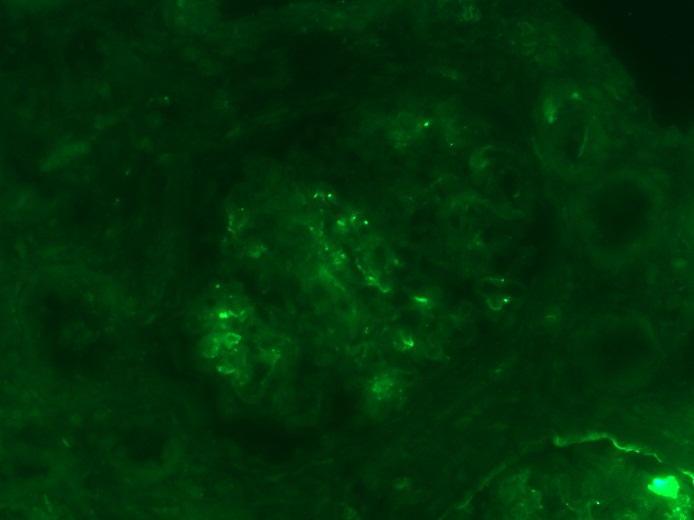
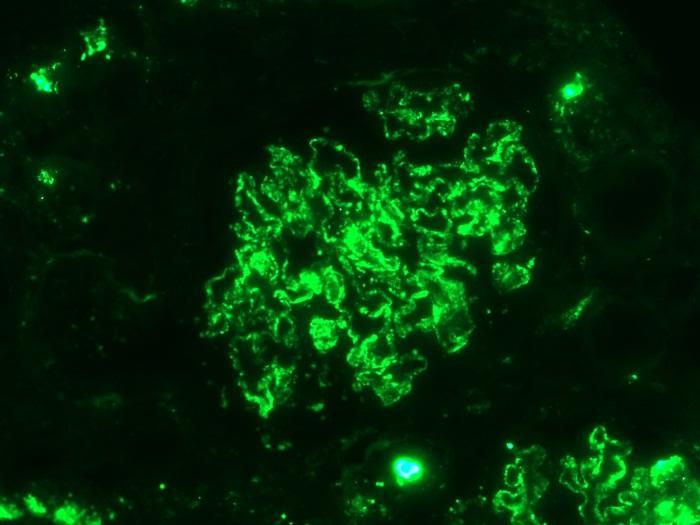
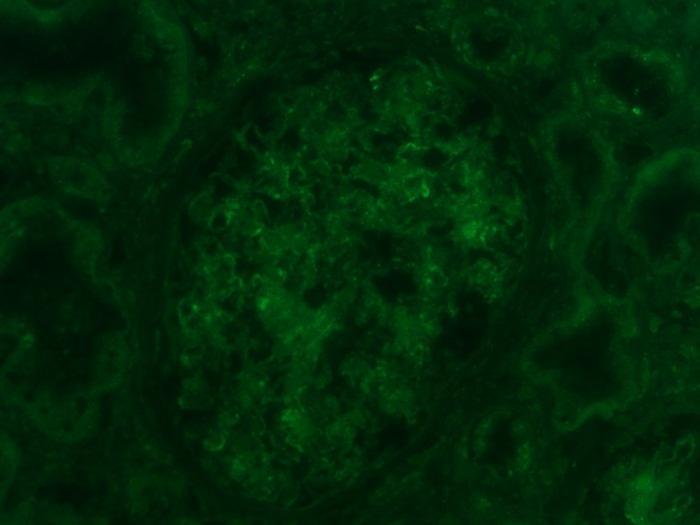
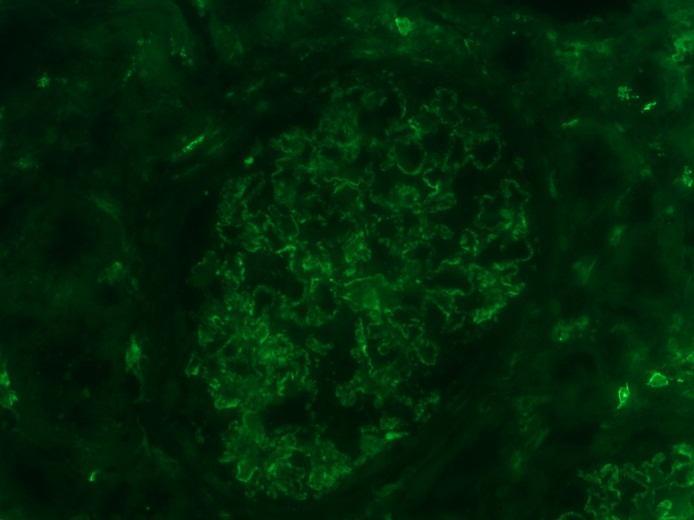
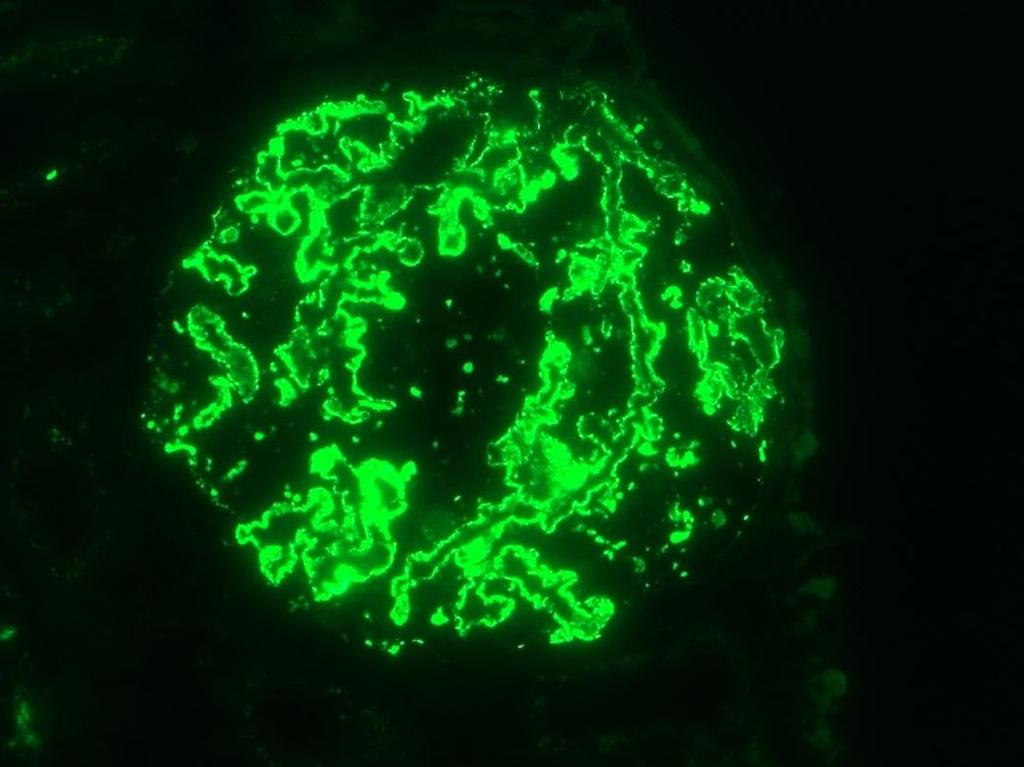
14 IgG IgA IgM C3 C1q C4

15 IgG
16
17
18 Q4. Which of the following would you now request? A. IgG subclass staining B. Congo Red Staining C. PLA2R Ab measurement D. IgG k and IgG l staining E. Additional sections stained with PAM
19 KDIGO Clinical Practice Guideline for Glomerulonephritis
20 KDIGO Clinical Practice Guideline for Glomerulonephritis 7.1: Evaluation of MN 7.1.1: Perform appropriate investigations to exclude secondary causes in all cases of biopsy-proven MN. (Not Graded)
21 KDIGO Clinical Practice Guideline for Glomerulonephritis
22 KDIGO Clinical Practice Guideline for Glomerulonephritis
23 Etiology and Clinical Characteristics of China Membranous Nephropathy in Chinese Patients Study Design Case series. Setting & Participants Patients with biopsy-proven MN at the Research Institute of Nephrology, Jinling Hospital, Nanjing University School of Medicine, Nanjing, China. Results 390 patients with MN were identified from 1985 to Of 390 patients with MN, 124 (31.8%) had idiopathic MN and 266 had secondary MN (68.2%). Of patients with idiopathic MN. Common presentations of idiopathic MN were 60.5% with proteinuria (39.5% of whom presented with nephrotic syndrome), 29.8% with hypertension, 17.7% with hematuria, and 0.8% with decreased kidney function. In patients with secondary MN, causes were autoimmune diseases (73.3%), infections (17.7%), tumors (4.5%), and drugs or toxins (4.5%). Systemic lupus erythematosus was the most common autoimmune disease (predominately in younger women). Hepatitis B predominated in younger men. Greater levels of proteinuria were found in patients who presented with drugs or toxins compared with patients with other secondary MNs (P < 0.05). Am J Kidney Dis 2008; 52:
24 KDIGO Clinical Practice Guideline for Glomerulonephritis
25 KDIGO Clinical Practice Guideline for Glomerulonephritis

26 China Clin J Am Soc Nephrol 5: , 2010.
27 Mercury-Induced Membranous Nephropathy China 1. History of mercury exposure 2. Urine test for mercury excretion 3. IgG1>IgG4>IgG3 Patients should abstain from the mercury exposure, and immune suppression should be carefully avoided. Clin J Am Soc Nephrol 5: , 2010.

28 KDIGO Clinical Practice Guideline for Glomerulonephritis
29 Major Causes of Secondary MN 1. Infection hepatitis B and hepatitis C malaria, schistosomiasis, TB, leprosy Syphilis 2. Diseases associated with MN Autoimmune Lupus Nephritis Rheumatoid arthritis Sjogren's syndrome Diabetes mellitus sickle cell disease. 3. Drugs gold, bucillamine, penicillamine, NSAIDs, captopril 4. Malignancy
30 Japan Nephrol Dial Transplant (2004) 19:
31 Japan Nephrol Dial Transplant (2004) 19:
32 IgG Subclass Distribution in Membranous Nephropathy IgG1 IgG2 IgG3 IgG4 Idiopathic Lupus Neoplasia ~- Am J Kidney Dis.1994 Mar;23(3): Clin Exp Immunol Oct;58(1): Clin Nephrol Apr;19(4): Nephrol. Dial. Transplant. (2004) 19 (3): Kidney International (1997) 51,
33 Pathological findings suggesting secondary MN 20 1.LM 2.IF 3.EM 4.IHC Proliferative lesion SLE, MPGN? Full house (including C1q) SLE? Vascular and TBM staining SLE? IgG1, 3 > IgG4 SLE? IgG1, 2 > IgG4 malignancy? Subendothelial deposits Mesangial deposits No granular staining for PLA2R Ag along GBM
 patients with MN had a malignancy at the time of renal biopsy or within a year thereafter.")
34 Glomerular Diseases: Membranous Nephropathy A Modern View Claudio Ponticelli* and Richard J. Glassock The association of MN with cancer is frequent, although not always clear cut. A French review showed that 24 of 240 (10%) patients with MN had a malignancy at the time of renal biopsy or within a year thereafter. The frequency of malignancy in MN increased with age up to 20% 25% after age 60 years. The solid organ cancers are particularly frequent, mainly in the lung, colon, breast, prostate, oruterus. An evaluation for underlying cancer is recommended for patients with MN, particularly for older individuals (Table 1). Clin J Am Soc Nephrol 9: , 2014
35 Case 1 In the mean time Abdominal CT: normal Chest CT: normal PSA: normal Urinary cytodiagnosis: no malignancy Fecal occult blood: negative
36 Q4. Which of the following would you now request? A. IgG subclass staining B. Congo Red Staining C. PLA2R Ab measurement D. IgG k and IgG l staining E. Additional sections stained with PAM Answer. I would order A (and C).
37 Case 1 (2) A renal biopsy was performed. Light microscopy reveals slightly thickened capillary walls, without proliferation. IF shows 4+ granular IgG and 3+ granular C3 along the glomerular capillary wall. No mesangial deposits is seen. IgA and IgM are weakly positive (+). C1q and C4 are negative. EM shows thickened basement membrane, spikes and electron dense deposits along the subepithelium. IgG subclass shows IgG4>>IgG1> IgG2. IgG3 is negative.

38 IgG1 IgG2 IgG3 IgG4
39 Target antigens in Membranous Nephropathy 1. a-enolase Circulating antibodies against a-enolase in patients with primary membranous nephropathy (MN). Wakui H, Imai A. et al. Clin Exp Immunol 1999; 118: NEP: neutral endopeptidase Alloantigen involved in neonatal cases of membranous nephropathy that occur in newborns from neutral endopeptidase-deficient mothers. Debiec H, Ronco P. N. Engl J Med 2002, Lancet PLA2R: M-type phospholipase A2 receptor The first autoantigen identified in idiopathic MN in the adult. Beck and Salant. N Engl J Med 2009;361: Cationic BSA 5. AR and SOD2: 6. Others: Target Antigen in Early childhood MN. Debiec H, Ronco P. N. N Engl J Med 2011;364: Specific anti aldose reductase (AR) and anti manganese superoxide dismutase (SOD2) IgG4 were detected in sera of MN patients. J Am Soc Nephrol 21: , 2010

40
41
42
43

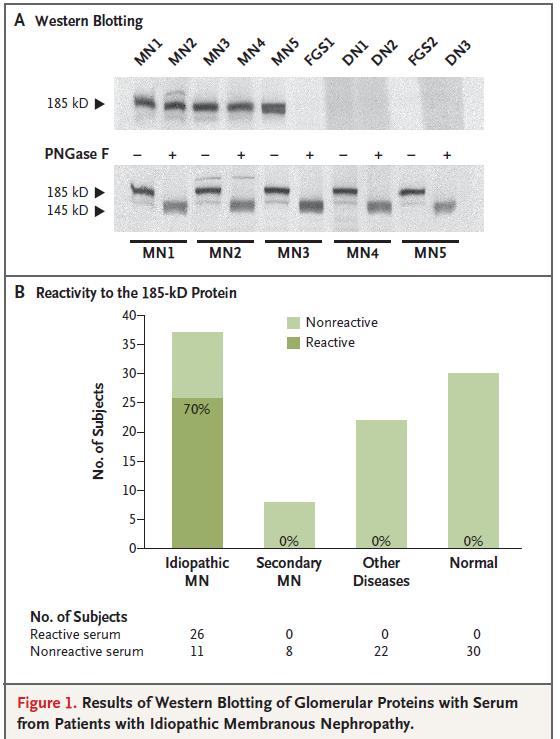
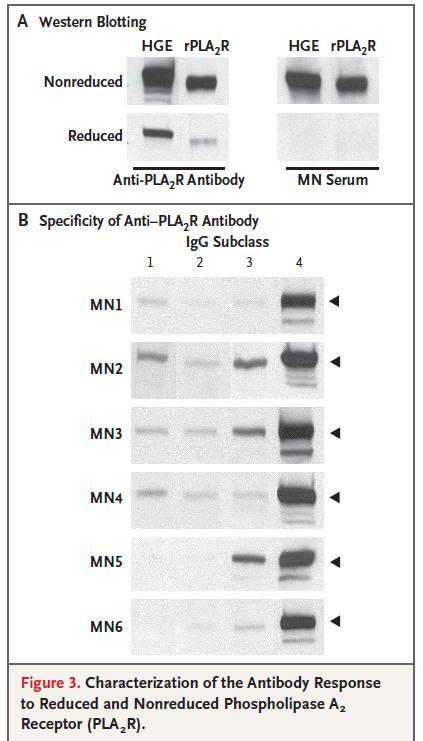
44 Beck and Salant
 and outcomes (n=79-")

45 Anti-PLA2R auto-antibody (ELISA) and outcomes (n=79- all PLA2R1 +) Low middle High Hofstra JM, et al JASN 23: , 2012
46 Anti-PLA2R auto-antibody (ELISA) and outcomes (n=79- all PLA2R1 +) Figure 2. Correlation between anti-pla2r levels measured with an ELISA technique and proteinuria in patients of the Dutch cohort. (A) Unadjusted analysis. (B) Anti- PLA2R levels adjusted for fractional excretion of IgG. Hofstra JM, et al JASN 23: , 2012
47 China
: e62151.")
48 Korea PLoS ONE 8(4): e
: e62151.")
49 Positive Negative Korea PLoS ONE 8(4): e

50 Korea Negative Low middle High No relationship was observed between anti-pla1r titer and remission rate. PLoS ONE 8(4): e
51 Nephrol Dial Transplant Jul;28(7):

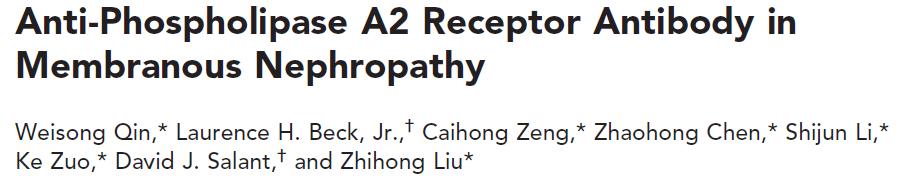
52 Membranous Nephropathy: PLA2R antibody and PLA2R antigen Normal imn imn Lupus HBV Sarcoidosis Nephrol Dial Transplant Jul;28(7):
53 Membranous Nephropathy: PLA2R antibody and PLA2R antigen Nephrol Dial Transplant Jul;28(7):
54 Membranous Nephropathy: PLA2R antibody and PLA2R antigen Nephrol Dial Transplant Jul;28(7):
55
56
57 Case 1 (2) A renal biopsy was performed. Light microscopy reveals slightly thickened capillary walls, without proliferation. IF shows 4+ granular IgG and 3+ granular C3 along the glomerular capillary wall. No mesangial deposits is seen. IgA and IgM are weakly positive (+). C1q and C4 are negative. EM shows thickened basement membrane, spikes and electron dense deposits along the subepithelium. IgG subclass shows IgG4>IgG1> IgG2. IgG3 is negative. Western blotting revealed that anti-pla2r1 Ab is present in his serum.
58 Primary ( Idiopathic ) Membranous Nephropathy: Diagnostic Criteria-2014 A renal biopsy lesion showing exclusively epimembranous deposits by EM, predominantly containing IgG4 and lesser amount of IgG1,2,3. PLA2R1 Antigen, C4d, C3 and MBL commonly present in deposits in active disease, C1q always negative by IF. No recognizable underlying disease (especially SLE, HBV, drugs, heavy metal exposure and neoplasia). PLA2R1 auto-antibody + in 80%. Normal serum C3 and C4 concentration. Glassock R, KDIGO- Mumbai Nephrology Summit, Mumbai, India 2014
59 Standard Evaluation for Secondary MN PLA2R Ag Negative ANA, anti-dsdna antibody, C3 level in subjects <40 years Hepatitis B surface antigen, Hepatitis B core antibody in all. Careful history for drug use (including skin lightening creams containing Hg). Careful history and physical exam for signs of neoplasia + stool for occult blood, spiral CT of chest, mammogram (female), PSA (male), colonoscopy (if not done recently as a part of routine surveillance). Glassock R, KDIGO- Mumbai Nephrology Summit, Mumbai, India 2014
60 PLA2R Ab With a combination of anti-pla2r autoantibody testing, and examination of the renal biopsy for dominant deposits of IgG4, C1q and PLA2R1 antigen it should be possible to diagnose primary MN with an accuracy of over 95% Glassock R, KDIGO- Mumbai Nephrology Summit, Mumbai, India 2014
61 Q5. Serum creatinine has gradually increased from 0.8mg/dL to 1.1 mg/dl.which ONE of the following treatments would you recommend? A. Observe for up to 6 more months while receiving an angiotensin converting enzyme inhibitor and diuretic B. Give Cyclosporine 2~4mg/kg/d plus 30mg/d of prednisone C. Give cyclical oral cyclophosphamide at 1-1.5mg/Kg alternating with IV methyl prednisolone and oral prednisone D. Give 40mg of prednisone E. Give 1000mg of Rituximab twice at an interval of two weeks F. Give MMF 1.0gm twice daily

62 KDIGO Clinical Practice Guideline for Glomerulonephritis
63 KDIGO Clinical Practice Guideline for Glomerulonephritis Recommendation We recommend that initial therapy be started ONLY in patients with Nephrotic Syndrome (NS) AND when at least ONE of the following conditions are met: 1. Urine protein excretion persistently exceeds 4g/d AND remains over 50% of the baseline value AND does not show a progressive decline during an observation period of at least 6 months 2. Presence of severe, disabling or life-threatening symptoms related to the NS 3. Scr has risen by 30% or more within 6-12 months from the time of diagnosis but is not less than 25ml/min/1.73m2 AND this change is not explained by superimposed complications
64 A large cohort of patients with idiopathic membranous nephropathy treated according to a restrictive treatment policy. Participants are 254 patients who visited our outpatient clinic between 1995 and J Am Soc Nephrol 25: , 2014
65 Restrictive Treatment Strategy for Primary MN 254 patients with primary MN initially treated according the strategy similar to that advocated by KDIGO were examined for long-term outcomes (median 57 months) 96% of patients received RAS inhibiting therapy. Oral anti-coagulation was given to 36% of patients. 130 (51%) received conservative therapy only, while 124 (49%) eventually received immunosuppressive therapy. 91/124 (73%) were given oral CYC + Prednisone and 33/124 (27%) others. J Am Soc Nephrol 25: , 2014
66 Restrictive Treatment Strategy for Primary MN Mortality among IS Pt PR CR Con IS Con IS Figure 2. Renal replacement and all-cause mortality rates were higher in the treated patients (top panel). Partial remission rates were similar. However, complete remission rate was lower in the treated patients (bottom panel). The thick lines represent patients treated with immunosuppressive drugs, and the thin lines represent patients treated conservatively. The top panel shows survival until renal replacement therapy (solid lines) and mortality (dotted lines). Death was considered competing for renal replacement therapy in the analyses. The bottom panel shows the cumulative incidence of partial (solid lines) and complete remission (dotted lines). Severe kidney failure was considered competing for remission. J Am Soc Nephrol 25: , 2014
67 Restrictive Treatment Strategy for Primary MN Conservative: Deaths- 4/130 Any Scr >3.0mg/dL 13/130 PR 90/130, CR 60/130 ESRD- 1/130 Immunosuppressive: Deaths- 15/124 Any Scr >3.0mg/dL- 20/124 PR 88/130, CR 45/130 ESRD- 6/124 J Am Soc Nephrol 25: , 2014
68 Restrictive Treatment Strategy for Primary MN In conclusion, a restrictive therapeutic regimen yields favorable long-term outcomes. Additionally, it results in half of the patients not requiring toxic drugs. Shortterm and long-term adverse effects remain an important issue, and risks of adverse effects should be balanced against the potential benefits of treatment. Overall, our study supports the recommendations in the recently published KDIGO guideline. J Am Soc Nephrol 25: , 2014
69 KDIGO Clinical Practice Guideline for Glomerulonephritis 7.3: Initial therapy of IMN 7.3.1: We recommend that initial therapy consist of a 6-month course of alternating monthly cycles of oral and i.v. corticosteroids, and oral alkylating agents (see Table 15). (1B) 7.3.2: We suggest using cyclophosphamide rather than chlorambucil for initial therapy. (2B) 7.3.5: Adjust the dose of cyclophosphamide or chlorambucil according to the age of the patient and egfr. (Not Graded)

70 KDIGO Clinical Practice Guideline for Glomerulonephritis

71 KDIGO Clinical Practice Guideline for Glomerulonephritis
72 Kidney International, Vol. 48 (1995), pp
73 treated Renal survival untreated Kidney International, Vol. 48 (1995), pp
74 CR or PR untreated treated Kidney International, Vol. 48 (1995), pp
75 A randomized, controlled trial of steroids and India cyclophosphamide in adults with nephrotic syndrome caused by idiopathic membranous nephropathy. Patients: biopsy-proven IMN of at least 6 mo duration. Intervention: Group2(n=47): a 6-mo course of alternate months of steroid and cyclophosphamide. Control: Group1(N=46): supportive therapy Outcomes: doubling of serum cre, development of ESRD, or patient death. (PR, CR, Quality of life) Jha V, Ganguli A, Saha TK et al. J Am Soc Nephrol 2007; 18:
76 A randomized, controlled trial of steroids and India cyclophosphamide in adults with nephrotic syndrome caused by idiopathic membranous nephropathy. dialysis-free survival IS cont Renal survival IS cont CR PR + CR IS IS cont cont 35 Jha V, Ganguli A, Saha TK et al. J Am Soc Nephrol 2007; 18:
77 35 CKD, chronic kidney disease; ESRD, end-stage renal disease; MN, membranous nephropathy. KDIGO Clinical Practice Guideline for Glomerulonephritis
78 KDIGO Clinical Practice Guideline for Glomerulonephritis 7.4: Alternative regimens for the initial therapy of IMN: CNI therapy 7.4.1: We recommend that cyclosporine or tacrolimus be used for a period of at least 6 months in patients who meet the criteria for initial therapy (as described in Recommendation 7.2.1), but who choose not to receive the cyclical corticosteroid/alkylating-agent regimen or who have contraindications to this regimen. (1C)

79 KDIGO Clinical Practice Guideline for Glomerulonephritis
, pp. 1484 1490")
80 Kidney International, Vol. 59 (2001), pp
81 Cyclosporin in MN: Complete and Partial Remssions Kidney International, Vol. 59 (2001), pp
82 Cyclosporin in MN: Complete and Partial Remssions Fig. 2. Remission and relapses in the two groups over the study and follow-up period. Abbreviations are: CR, complete remission; PR, partial remission; NR, no remission; R, relapse. Kidney International, Vol. 59 (2001), pp

83 Patients: biopsy-proven idiopathic membranous nephropathy Intervention: Patients were randomly assigned (1:1:1) by a random number table to receive supportive treatment only, supportive treatment plus 6 months of alternating cycles of prednisolone and chlorambucil, or supportive treatment plus 12 months of ciclosporin. The primary outcome: a further 20% decline in renal function from baseline, analysed by intention to treat. Lancet Mar 2;381(9868):
84 20% decline in renal function Patients treated with PSL and chlorambucil showed better survival than those with ciclosporin or supportive therapy. Is 20% decline appropriate outcome? Lancet Mar 2;381(9868):

85 Lancet Mar 2;381(9868):
86 A large cohort of patients with idiopathic membranous nephropathy treated according to a restrictive treatment policy. Participants are 254 patients who visited our outpatient clinic between 1995 and J Am Soc Nephrol 25: , 2014

87 Malignancies occurred more frequently in cyclophosphamide-treated patients. J Am Soc Nephrol 25: , 2014
88 Cohort Study Ninety-five consecutive adult patients attending two centres in the UK between 1997 and Nephrol Dial Transplant (2012) 27:
89 MN Cohort Study in the UK Treatment: IS is considered for patients with prolonged nephrotic syndrome (>6months), serious complications of nephrotic syndrome including venous thromboemboli and intractable oedema or rapidly deteriorating renal function. Choice of immunosuppressive regime has been physician led, with no fixed unit policy but treatment adhered to published protocols. (Cattran or ponticelli) Nephrol Dial Transplant (2012) 27:
90 MN Cohort Study in the UK PR CR Pont Cattran Cattran Pont Fig. 3. Kaplan Meier one-survival plots of outcomes by type of IS. (A) Cattran regimen (cyclosporine) (interrupted line); (B) Ponticelli regimen (solid line). Comparison by log-rank test. Nephrol Dial Transplant (2012) 27:
91 MN Cohort Study in the UK Type of IS used did not have an impact on outcome but the Ponticelli regimen was associated with a higher incidence of side effects than the Cattran regimen. These findings should help inform physician and patient treatment choice while awaiting the results of the ongoing UK MRC randomized controlled trial of immunosuppressive regimens in patients with IMN. Nephrol Dial Transplant (2012) 27:
92 7.5: Regimens not recommended or suggested for initial therapy of IMN 7.5.1: We recommend that corticosteroid monotherapy not be used for initial therapy of IMN. (1B) 7.5.2: We suggest that monotherapy with MMF not be used for initial therapy of IMN. (2C) Nevertheless, retrospective studies conducted in subjects of Asian (Japanese) ancestry have suggested possible benefits for steroid monotherapy. KDIGO Clinical Practice Guideline for Glomerulonephritis
, pp.")
93 Japan Kidney International, Vol. 65 (2004), pp
94 Japan Kidney International, Vol. 65 (2004), pp
95 Japan Conclusion. IMNis a disease with a comparatively good prognosis in Japan even when it is associated with nephrotic syndrome. Steroid therapy, which has not been recommended for IMN in most review articles, seems to be useful at least for Japanese patients. In particular, a remission from heavy proteinuria likely results in a favorable outcome. Kidney International, Vol. 65 (2004), pp
96 Korea Yonsei Med J Jul;54(4):

97 Korea Yonsei Med J Jul;54(4):
98 Korea Yonsei Med J Jul;54(4):

99 Korea Yonsei Med J Jul;54(4):
100 EVENTS: a decline in egfr >50% or initiation of dialysis, and all-cause mortality. Korea 40 Yonsei Med J Jul;54(4):



101 JNSCS as a secondary study of J-KDR JNSCS: Japan Nephrotic Syndrome Cohort Study JNSCS Primary nephrotic syndrome J-IGACS Patietns with IgA nephropathy JRPGN-CS J-KDR/J-RBR Rapidly progressive glomerulonephritis JDNCS Diabetic nephropathy J-PKD Polycystic kidney disease 40 Dialysis J-IDCS
102 Study Design of JNSCS Purpose To disclose the outcomes and practice patterns in patients with primary nephrotic syndrome in Japan Design Multicenter prospective cohort study Participants Patients diagnosed histologically by renal biopsy with primary nephrotic syndrome between Jan 2008 and Dec 2010 Definition of nephrotic syndrome: (1) Urinary protein 3.5 g/day (2) Serum protein <3.0 g/dl
 Kyusyu U East Fukuoka MC Kurume U Fukuoka U Miyazaki U Nagasaki U Chubu Area 129 cases (31%) Niigata")
 Osaka U Osaka City U Munincipal Toyonaka Hospital Kitano Hospital Osaka Prefectural Hospital Kobe U Wakayama")
 Tsukuba U Saitama Med U Saitama Med U General Hosp Gunma U Tokyo Women s Med U Juntendo U Teikyo U St.")
103 396 cases from 56 medical centers Chugoku Shikoku area 26 cases (6%) Kawasaki MU Okayama U Shimane U Kagawa U Tokushima UJ Kochi U Kyusyu area 42 cases (10%) Kyusyu U East Fukuoka MC Kurume U Fukuoka U Miyazaki U Nagasaki U Chubu Area 129 cases (31%) Niigata U Kanazawa Med Univ Kanazawa U Hamamatsu Med U Shizuoka General Hosp Nagoya U+15 Fujita Health U Nagoya Daini Red Cross Kinki Area 83 cases (20%) Osaka U Osaka City U Munincipal Toyonaka Hospital Kitano Hospital Osaka Prefectural Hospital Kobe U Wakayama Med Univ Nara Medical U Hokkaido Tohoku 66 cases (16%) Hokkaido U Tohoku U Sendai Shakaihpoken H Yamagata U Fukushima M U Kanto Area 66cases (18%) Tsukuba U Saitama Med U Saitama Med U General Hosp Gunma U Tokyo Women s Med U Juntendo U Teikyo U St. Mariana Med U
104 Baseline Characteristics MCD N = 165 MN N = 158 FSGS N = 38 Others N = 35 Age (year) 42 (26-61) 66 (59-75) 62 (29-73) 58 (45-71) Male gender (N (%)) 95 (57.6) 85 (53.8) 25 (65.8) 20 (57.1) Edema (N (%)) 153 (92.7) 132 (85.2) 36 (94.7) 25 (71.4) BMI (kg/m 2 ) 23.9± ± ± ±3.5 Systolic blood pressure (mmhg) 120±16 128±19 134±17 135±15 Diastolic blood pressure (mmhg) 73±11 75±13 80±13 78±11 Serum creatinine (mg/dl) 0.87 ( ) 0.86 ( ) 1.17 ( ) 1.06 ( ) Serum albumin (g/dl) 1.7± ± ± ±0.4 Total cholesterol (mg/dl) 405± ± ± ±78 HDL-cholesterol (mg/dl) 75±27 63±23 61±20 58±25 Triglyceride (mg/dl) 194 ( ) 186 ( ) 224 ( ) 147 ( ) Hemoglobin A1c (%) 5.5± ± ± ±0.5 Urinary protein (g/day) 6.3 ( ) 4.6 ( ) 6.0 ( ) 5.1 ( ) UPCR 7.1 ( ) 4.6 ( ) 6.0 ( ) 5.1 ( ) Mean±SD, or Median (25% - 75%)
105 Treatment for NS MCD n MN n FSGS n Observation period (year) 2.3 ( ) ( ) ( ) 38 Immunosuppressive therapy 162 (98.2) 136 (86.1) 35 (92.1) The 1 st month oral glucocorticoids 158 (95.8) 127 (80.9) 35 (92.1) methyl predonisolone IV 47 (28.5) 25 (15.9) 10 (26.3) Cyclosporine 24 (14.6) 61 (38.9) 15 (39.5) Cyclophosphamide 1 (0.6) 6 (3.8) 0 (0.0) Mizoribine 3 (1.8) 10 (6.4) 0 (0.0) ACEI/ARB 41 (24.9) 119 (75.8) 20 (52.6) 2-12 months oral glucocorticoids 157 (96.9) 125 (82.8) 35 (92.1) methyl predonisolone IV 8 (4.9) 2 (1.3) 1 (2.6) Cyclosporine 46 (28.4) 70 (46.4) 20 (52.6) Cyclophosphamide 0 (0.0) 3 (2.0) 1 (2.6) Mizoribine 7 (4.3) 20 (13.3) 0 (0.0) ACEI/ARB 50 (30.9) 125 (82.8) 28 (82.4)
106 In this annual meeting of JSN, we are publishing an Evidence Based Guideline for Nephrotic Syndrome MN Initial treatment Oral predonisolone is administered at single daily dose starting at 0.6~0.8 mg/kg/day and continued for 4 weeks. Instead of oral steroid alone, predonisolone and cyclophosphamide 50~ 100 mg/day is administered as starting doses. Lower oral steroid and cyclosporine as initial treatment is considered for the cases that are skeptical about steroid adverse effects, such as diabetic patients.
107 Initial immunosuppressive treatment for idiopathic membranous nephropathy KDIGO GL JSN GL 1. Ponticelli treatment 2. Cyclosporin or Tacrolimus Steroid monotherapy Cyclophosphamide + PSL Cyclosporin + PSL
 Baseline 24 hour protein= 9.1gms (5.8-12.")
108 A retrospective stay of 100 consecutive patients with IMN and NS treatment with Rituximab (68 as initial first-line therapy; 32 as second line therapy after failure of another regimen) Baseline Scr= 1.2mg/dL ( mg/dL-44 patients had an elevated Scr.) Baseline 24 hour protein= 9.1gms ( gm/d) RTX given as 4 weekly 375mg/m2 doses IV or B-cell count modified dosage regimen J Am Soc Nephrol 23: , 2012
109 RITUXIMAB in Primary MN J Am Soc Nephrol 23: , 2012

110 RITUXIMAB in Primary MN J Am Soc Nephrol 23: , 2012
111 Q5. Serum creatinine has gradually increased to 1.2 mg/dl. Which ONE of the following treatments would you recommend? A. Observe for up to 6 more months while receiving an angiotensin converting enzyme inhibitor and diuretic B. Give Cyclosporine 2~4mg/kg/d plus 30mg/d of prednisone C. Give cyclical oral cyclophosphamide at 1-1.5mg/Kg alternating with IV methyl prednisolone and oral prednisone D. Give 40mg of prednisone E. Give 1000mg of Rituximab twice at an interval of two weeks F. Give MMF 1.0gm twice daily According to the KDIGO GL, the answer is C. According to the Japanese GL, the answer is either B, C, or D. I would choose B.
MEMBRANOUS NEPHROPATHY: Treatment in the Modern Era
 MEMBRANOUS NEPHROPATHY: Treatment in the Modern Era Richard Glassock, MD, MACP Geffen School of Medicine at UCLA KDIGO- Mumbai Nephrology Summit Mumbai, India February 6-9, 2014 QUESTION #1A A 71 year
MEMBRANOUS NEPHROPATHY: Treatment in the Modern Era Richard Glassock, MD, MACP Geffen School of Medicine at UCLA KDIGO- Mumbai Nephrology Summit Mumbai, India February 6-9, 2014 QUESTION #1A A 71 year
Membranous nephropathy. By Mohammed Kamal Nassar, MD Lecturer of Nephrology Mansoura University
 Membranous nephropathy By Mohammed Kamal Nassar, MD Lecturer of Nephrology Mansoura University Membranous nephropathy Definition: Immune complex glomerular disease in which immune deposits of IgG and complement
Membranous nephropathy By Mohammed Kamal Nassar, MD Lecturer of Nephrology Mansoura University Membranous nephropathy Definition: Immune complex glomerular disease in which immune deposits of IgG and complement
Nephrotic syndrome minimal change disease vs. IgA nephropathy. Hadar Meringer Internal medicine B Sheba
 Nephrotic syndrome minimal change disease vs. IgA nephropathy Hadar Meringer Internal medicine B Sheba The Case 29 year old man diagnosed with nephrotic syndrome 2 weeks ago and complaining now about Lt.flank
Nephrotic syndrome minimal change disease vs. IgA nephropathy Hadar Meringer Internal medicine B Sheba The Case 29 year old man diagnosed with nephrotic syndrome 2 weeks ago and complaining now about Lt.flank
Glomerular Pathology- 1 Nephrotic Syndrome. Dr. Nisreen Abu Shahin
 Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
C1q nephropathy the Diverse Disease
 C1q nephropathy the Diverse Disease Danica Galešić Ljubanović School of Medicine, University of Zagreb Dubrava University Hospital Zagreb, Croatia Definition Dominant or codominant ( 2+), mesangial staining
C1q nephropathy the Diverse Disease Danica Galešić Ljubanović School of Medicine, University of Zagreb Dubrava University Hospital Zagreb, Croatia Definition Dominant or codominant ( 2+), mesangial staining
Chapter 4: Steroid-resistant nephrotic syndrome in children Kidney International Supplements (2012) 2, ; doi: /kisup.2012.
 2, ; doi: /kisup.2012.") http://www.kidney-international.org & 2012 KDIGO Chapter 4: Steroid-resistant nephrotic syndrome in children Kidney International Supplements (2012) 2, 172 176; doi:10.1038/kisup.2012.17 INTRODUCTION This
http://www.kidney-international.org & 2012 KDIGO Chapter 4: Steroid-resistant nephrotic syndrome in children Kidney International Supplements (2012) 2, 172 176; doi:10.1038/kisup.2012.17 INTRODUCTION This
Case 3. ACCME/Disclosure. Laboratory results. Clinical history 4/13/2016
 Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
Membranous nephropathy
 TURKISH SOCIETY of PEDIATRIC NEPHROLOGY Membranous nephropathy Elena Levtchenko Leuven, Belgium Antalya, November 27, 2016 Lecture overview Definition Epidemiology Clinical features Histopathology Pathogenesis
TURKISH SOCIETY of PEDIATRIC NEPHROLOGY Membranous nephropathy Elena Levtchenko Leuven, Belgium Antalya, November 27, 2016 Lecture overview Definition Epidemiology Clinical features Histopathology Pathogenesis
Lupus Related Kidney Diseases. Jason Cobb MD Assistant Professor Renal Division Emory University School of Medicine October 14, 2017
 Lupus Related Kidney Diseases Jason Cobb MD Assistant Professor Renal Division Emory University School of Medicine October 14, 2017 Financial Disclosures MedImmune Lupus Nephritis Kidney Biopsy Biomarkers
Lupus Related Kidney Diseases Jason Cobb MD Assistant Professor Renal Division Emory University School of Medicine October 14, 2017 Financial Disclosures MedImmune Lupus Nephritis Kidney Biopsy Biomarkers
Management and treatment of glomerular diseases KDIGO Controversies Conference Part 1
 Management and treatment of glomerular diseases KDIGO Controversies Conference Part 1 Dr.M.Matinfar Assistant Professor of Internal Medicine & Nephrology IUMS -IKRC GENERAL PRINCIPLES IN THE MANAGEMENT
Management and treatment of glomerular diseases KDIGO Controversies Conference Part 1 Dr.M.Matinfar Assistant Professor of Internal Medicine & Nephrology IUMS -IKRC GENERAL PRINCIPLES IN THE MANAGEMENT
Nephrotic Syndrome NS
 Nephrotic Syndrome NS By : Dr. Iman.M. Mudawi Pediatric Nephrology Unit Gaafar Ibn Auf Hospital Definitions: In children NS is applied to any condition with a triad of: Heavy proteinuria (UACR ratio >200
Nephrotic Syndrome NS By : Dr. Iman.M. Mudawi Pediatric Nephrology Unit Gaafar Ibn Auf Hospital Definitions: In children NS is applied to any condition with a triad of: Heavy proteinuria (UACR ratio >200
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Clinical Commissioning Policy: Rituximab for the treatment of idiopathic membranous nephropathy in adults
 Clinical Commissioning Policy: Rituximab for the treatment of idiopathic membranous nephropathy in adults Reference: NHS England: 16047/P NHS England INFORMATION READER BOX Directorate Medical Operations
Clinical Commissioning Policy: Rituximab for the treatment of idiopathic membranous nephropathy in adults Reference: NHS England: 16047/P NHS England INFORMATION READER BOX Directorate Medical Operations
Atypical IgA Nephropathy
 Atypical IgA Nephropathy Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA XXXIII Chilean Congress of Nephrology, Hypertension and Transplantation Puerto Varas, Chile October 6, 2016 IgA
Atypical IgA Nephropathy Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA XXXIII Chilean Congress of Nephrology, Hypertension and Transplantation Puerto Varas, Chile October 6, 2016 IgA
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
The CARI Guidelines Caring for Australasians with Renal Impairment. Membranous nephropathy role of steroids GUIDELINES
 Membranous nephropathy role of steroids Date written: July 2005 Final submission: September 2005 Author: Merlin Thomas GUIDELINES There is currently no data to support the use of short-term courses of
Membranous nephropathy role of steroids Date written: July 2005 Final submission: September 2005 Author: Merlin Thomas GUIDELINES There is currently no data to support the use of short-term courses of
CHAPTER 2. Primary Glomerulonephritis
 2nd Report of the PRIMARY GLOMERULONEPHRITIS CHAPTER 2 Primary Glomerulonephritis Sunita Bavanandan Lee Han Wei Lim Soo Kun 21 PRIMARY GLOMERULONEPHRITIS 2nd Report of the 2.1 Introduction This chapter
2nd Report of the PRIMARY GLOMERULONEPHRITIS CHAPTER 2 Primary Glomerulonephritis Sunita Bavanandan Lee Han Wei Lim Soo Kun 21 PRIMARY GLOMERULONEPHRITIS 2nd Report of the 2.1 Introduction This chapter
How I Treat Membranous Nephropathy
 How I Treat Membranous Nephropathy Patrick H. Nachman, MD, FASN Marion Stedman Covington Professor May 20, 2017 Treating Membranous Nephropathy: after changes upon changes we are more or less the same
How I Treat Membranous Nephropathy Patrick H. Nachman, MD, FASN Marion Stedman Covington Professor May 20, 2017 Treating Membranous Nephropathy: after changes upon changes we are more or less the same
Focal Segmental Glomerulosclerosis and the Nephro6c Syndrome Dr. A. Gangji Dr. P. Marge>s. Part 1: Clinical
 Focal Segmental Glomerulosclerosis and the Nephro6c Syndrome Dr. A. Gangji Dr. P. Marge>s Part 1: Clinical Pa#ent DM 18 year old McMaster student Back pain, severe fa#gue Oct 2006 Leg swelling to ER Nov
Focal Segmental Glomerulosclerosis and the Nephro6c Syndrome Dr. A. Gangji Dr. P. Marge>s Part 1: Clinical Pa#ent DM 18 year old McMaster student Back pain, severe fa#gue Oct 2006 Leg swelling to ER Nov
CHAPTER 2 PRIMARY GLOMERULONEPHRITIS
 CHAPTER 2 Sunita Bavanandan Lim Soo Kun 19 5th Report of the 2.1: Introduction This chapter covers the main primary glomerulonephritis that were reported to the MRRB from the years 2005-2012. Minimal change
CHAPTER 2 Sunita Bavanandan Lim Soo Kun 19 5th Report of the 2.1: Introduction This chapter covers the main primary glomerulonephritis that were reported to the MRRB from the years 2005-2012. Minimal change
Monoclonal Gammopathies and the Kidney. Tibor Nádasdy, MD The Ohio State University, Columbus, OH
 Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Administration of low-dose cyclosporine alone for the treatment of elderly patients with membranous nephropathy
 Administration of low-dose cyclosporine alone for the treatment of elderly patients with membranous nephropathy M.X. Li, Y.W. Yu, Z.Y. Zhang, H.D. Zhao and F.L. Xiao Department of Nephrology, The Navy
Administration of low-dose cyclosporine alone for the treatment of elderly patients with membranous nephropathy M.X. Li, Y.W. Yu, Z.Y. Zhang, H.D. Zhao and F.L. Xiao Department of Nephrology, The Navy
Idiopathic Membranous Nephropathy: Diagnosis and Treatment
 Clinical Conference Idiopathic Membranous Nephropathy: Diagnosis and Treatment Fernando C. Fervenza,* Sanjeev Sethi, and Ulrich Specks *Division of Nephrology and Hypertension, Department of Pathology,
Clinical Conference Idiopathic Membranous Nephropathy: Diagnosis and Treatment Fernando C. Fervenza,* Sanjeev Sethi, and Ulrich Specks *Division of Nephrology and Hypertension, Department of Pathology,
Minimal change nephropathy: an update (for adults) Dr. CC Szeto Department of Medicine & Therapeutics The Chinese University of Hong Kong
 Dr. CC Szeto Department of Medicine & Therapeutics The Chinese University of Hong Kong") Minimal change nephropathy: an update (for adults) Dr. CC Szeto Department of Medicine & Therapeutics The Chinese University of Hong Kong First, it is not uncommon Cameron JS. Am J Kidney Dis 10: 157 171,
Minimal change nephropathy: an update (for adults) Dr. CC Szeto Department of Medicine & Therapeutics The Chinese University of Hong Kong First, it is not uncommon Cameron JS. Am J Kidney Dis 10: 157 171,
Dense deposit disease with steroid pulse therapy
 Case Report Dense deposit disease with steroid pulse therapy Jun Odaka, Takahiro Kanai, Takane Ito, Takashi Saito, Jun Aoyagi, and Mariko Y Momoi Abstract Treatment of dense deposit disease DDD has not
Case Report Dense deposit disease with steroid pulse therapy Jun Odaka, Takahiro Kanai, Takane Ito, Takashi Saito, Jun Aoyagi, and Mariko Y Momoi Abstract Treatment of dense deposit disease DDD has not
THE KIDNEY AND SLE LUPUS NEPHRITIS
 THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
Current treatment recommendations in children with IgA nephropathy Selçuk Yüksel
 Current treatment recommendations in children with IgA nephropathy Selçuk Yüksel Department of Pediatric Nephrology Pamukkale University School of Medicine IgA Nephropathy The most common cause of primary
Current treatment recommendations in children with IgA nephropathy Selçuk Yüksel Department of Pediatric Nephrology Pamukkale University School of Medicine IgA Nephropathy The most common cause of primary
The CARI Guidelines Caring for Australasians with Renal Impairment. Idiopathic membranous nephropathy: use of other therapies GUIDELINES
 Idiopathic membranous nephropathy: use of other therapies Date written: July 2005 Final submission: September 2005 Author: Merlin Thomas GUIDELINES No recommendations possible based on Level I or II evidence
Idiopathic membranous nephropathy: use of other therapies Date written: July 2005 Final submission: September 2005 Author: Merlin Thomas GUIDELINES No recommendations possible based on Level I or II evidence
Experimental and human models of membranous nephropathy : the story goes on. Pierre Ronco, Hanna Debiec Unité UMPC/IMSERM 702 HôpitalTenon
 Experimental and human models of membranous nephropathy : the story goes on Pierre Ronco, Hanna Debiec Unité UMPC/IMSERM 702 HôpitalTenon Actualités Néphrologiques 19/04/2011 Membranous Nephropathy Major
Experimental and human models of membranous nephropathy : the story goes on Pierre Ronco, Hanna Debiec Unité UMPC/IMSERM 702 HôpitalTenon Actualités Néphrologiques 19/04/2011 Membranous Nephropathy Major
A clinical syndrome, composed mainly of:
 Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
IgA-Nephropathy: an update on treatment Jürgen Floege
 IgA-Nephropathy: an update on treatment Jürgen Floege Division of Nephrology & Immunology juergen.floege@rwth-aachen.de Floege & Feehally, Nat Rev Nephrol 2013 Floege & Eitner, J Am Soc Nephrol. 2011 If
IgA-Nephropathy: an update on treatment Jürgen Floege Division of Nephrology & Immunology juergen.floege@rwth-aachen.de Floege & Feehally, Nat Rev Nephrol 2013 Floege & Eitner, J Am Soc Nephrol. 2011 If
Elevated Serum Creatinine, a simplified approach
 Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
An unusual association between focal segmental sclerosis and lupus nephritis: a distinct concept from lupus podocytopathy?
 CEN Case Rep (2015) 4:70 75 DOI 10.1007/s13730-014-0142-1 CASE REPORT An unusual association between focal segmental sclerosis and lupus nephritis: a distinct concept from lupus podocytopathy? Hironari
CEN Case Rep (2015) 4:70 75 DOI 10.1007/s13730-014-0142-1 CASE REPORT An unusual association between focal segmental sclerosis and lupus nephritis: a distinct concept from lupus podocytopathy? Hironari
Additional file 2: Details of cohort studies and randomised trials
 Reference Randomised trials Ye et al. 2001 Abstract 274 R=1 WD=0 Design, numbers, treatments, duration Randomised open comparison of: (45 patients) 1.5 g for 3, 1 g for 3, then 0.5 to 0.75 g IV cyclophosphamide
Reference Randomised trials Ye et al. 2001 Abstract 274 R=1 WD=0 Design, numbers, treatments, duration Randomised open comparison of: (45 patients) 1.5 g for 3, 1 g for 3, then 0.5 to 0.75 g IV cyclophosphamide
Steroid Resistant Nephrotic Syndrome. Sanjeev Gulati, Debashish Sengupta, Raj K. Sharma, Ajay Sharma, Ramesh K. Gupta*, Uttam Singh** and Amit Gupta
 Steroid Resistant Nephrotic Syndrome Sanjeev Gulati, Debashish Sengupta, Raj K. Sharma, Ajay Sharma, Ramesh K. Gupta*, Uttam Singh** and Amit Gupta From the Departments of Nephrology, Pathology* and Biostatistics**,
Steroid Resistant Nephrotic Syndrome Sanjeev Gulati, Debashish Sengupta, Raj K. Sharma, Ajay Sharma, Ramesh K. Gupta*, Uttam Singh** and Amit Gupta From the Departments of Nephrology, Pathology* and Biostatistics**,
Rituximab Treatment for Membranous Nephropathy: A French Clinical and Serological Retrospective Study of 28 Patients
 Original Paper This is an Open Access article licensed under the terms of the Creative Commons Attribution- NonCommercial-NoDerivs.0 License (www.karger.com/oa-license), applicable to the online version
Original Paper This is an Open Access article licensed under the terms of the Creative Commons Attribution- NonCommercial-NoDerivs.0 License (www.karger.com/oa-license), applicable to the online version
Nephrotic syndrome in children. Bashir Admani KPA Nephrology Precongress 24/4/2018
 Nephrotic syndrome in children Bashir Admani KPA Nephrology Precongress 24/4/2018 What is Nephrotic syndrome?? Nephrotic syndrome is caused by renal diseases that increase the permeability across the glomerular
Nephrotic syndrome in children Bashir Admani KPA Nephrology Precongress 24/4/2018 What is Nephrotic syndrome?? Nephrotic syndrome is caused by renal diseases that increase the permeability across the glomerular
Rejection or Not? Interhospital Renal Meeting 10 Oct Desmond Yap & Sydney Tang Queen Mary Hospital
 Rejection or Not? Interhospital Renal Meeting 10 Oct 2007 Desmond Yap & Sydney Tang Queen Mary Hospital Case Presentation F/61 End stage renal failure due to unknown cause Received HD in private hospital
Rejection or Not? Interhospital Renal Meeting 10 Oct 2007 Desmond Yap & Sydney Tang Queen Mary Hospital Case Presentation F/61 End stage renal failure due to unknown cause Received HD in private hospital
GOODPASTURE'S SYNDROME WITH CONCOMITANT IMMUNE COMPLEX MIXED MEMBRANOUS AND PROLIFERATIVE GLOMERULONEFRITIS
 GOODPASTURE'S SYNDROME WITH CONCOMITANT IMMUNE COMPLEX MIXED MEMBRANOUS AND PROLIFERATIVE GLOMERULONEFRITIS VESNA JURČIĆ 1, ANDREJA ALEŠ RIGLER 2, INSTITUTE OF PATHOLOGY, FACULTY OF MEDICINE, UNIVERSITY
GOODPASTURE'S SYNDROME WITH CONCOMITANT IMMUNE COMPLEX MIXED MEMBRANOUS AND PROLIFERATIVE GLOMERULONEFRITIS VESNA JURČIĆ 1, ANDREJA ALEŠ RIGLER 2, INSTITUTE OF PATHOLOGY, FACULTY OF MEDICINE, UNIVERSITY
Clots and Foamy Urine: Thrombotic Complications of Nephrotic Syndrome. Prayus Tailor, MD October 5, 2013 Renal and Hypertension Symposium
 Clots and Foamy Urine: Thrombotic Complications of Nephrotic Syndrome Prayus Tailor, MD October 5, 2013 Renal and Hypertension Symposium Objectives Discuss the pathophysiology of thrombosis in nephrotic
Clots and Foamy Urine: Thrombotic Complications of Nephrotic Syndrome Prayus Tailor, MD October 5, 2013 Renal and Hypertension Symposium Objectives Discuss the pathophysiology of thrombosis in nephrotic
Stepwise Treatment Using Corticosteroids Alone and in Combination with Cyclosporine in Korean Patients with Idiopathic Membranous Nephropathy
 Original Article http://dx.doi.org/1.3349/ymj.213.54.4.973 pissn: 513-5796, eissn: 1976-2437 Yonsei Med J 54(4):973-982, 213 Stepwise Treatment Using Corticosteroids Alone and in Combination with Cyclosporine
Original Article http://dx.doi.org/1.3349/ymj.213.54.4.973 pissn: 513-5796, eissn: 1976-2437 Yonsei Med J 54(4):973-982, 213 Stepwise Treatment Using Corticosteroids Alone and in Combination with Cyclosporine
IRACON Management of Lupus Nephritis: Old is gold, New is Trendy
 IRACON 2016 Management of Lupus Nephritis: Old is gold, New is Trendy First episode of LN (III/IV): Induction Low dose is equally considerable as high dose CYC Switch to the other agent if no improvement
IRACON 2016 Management of Lupus Nephritis: Old is gold, New is Trendy First episode of LN (III/IV): Induction Low dose is equally considerable as high dose CYC Switch to the other agent if no improvement
The CARI Guidelines Caring for Australasians with Renal Impairment
 Specific management of IgA nephropathy: role of triple therapy and cytotoxic therapy Date written: July 2005 Final submission: September 2005 Author: Merlin Thomas GUIDELINES a. Triple therapy with cyclophosphamide,
Specific management of IgA nephropathy: role of triple therapy and cytotoxic therapy Date written: July 2005 Final submission: September 2005 Author: Merlin Thomas GUIDELINES a. Triple therapy with cyclophosphamide,
Case # 2 3/27/2017. Disclosure of Relevant Financial Relationships. Clinical history. Clinical history. Laboratory findings
 Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Kidney disease associated with autoimmune disease
 Kidney disease associated with autoimmune disease Masaomi Nangaku Division of Nephrology and Endocrinology the University of Tokyo Graduate School of Medicine, Japan M-type Phospholipase A2 Receptor as
Kidney disease associated with autoimmune disease Masaomi Nangaku Division of Nephrology and Endocrinology the University of Tokyo Graduate School of Medicine, Japan M-type Phospholipase A2 Receptor as
Treatment of MGN A roundtable discussion based on best evidence Drs Cattran Expert Panel Dr Ruggenenti,Falk,Ponticelli,Fervenza,Remuzzi
 Treatment of MGN A roundtable discussion based on best evidence Drs Cattran Expert Panel Dr Ruggenenti,Falk,Ponticelli,Fervenza,Remuzzi Level 1 2 3 4 5 6 Definition of evidence Randomized, controlled trial
Treatment of MGN A roundtable discussion based on best evidence Drs Cattran Expert Panel Dr Ruggenenti,Falk,Ponticelli,Fervenza,Remuzzi Level 1 2 3 4 5 6 Definition of evidence Randomized, controlled trial
Mr. I.K 58 years old
 Mr. I.K 58 years old Hospitalized because of marked pitting peripheral edema (bilateral crural and perimalleolar edema) and uncontrolled blood pressure (BP 150/100 mmhg under treatment). since age 54 years
Mr. I.K 58 years old Hospitalized because of marked pitting peripheral edema (bilateral crural and perimalleolar edema) and uncontrolled blood pressure (BP 150/100 mmhg under treatment). since age 54 years
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT. J. H. Helderman,MD,FACP,FAST
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
The CARI Guidelines Caring for Australasians with Renal Impairment. Specific management of IgA nephropathy: role of steroid therapy GUIDELINES
 Specific management of IgA nephropathy: role of steroid therapy Date written: July 2005 Final submission: September 2005 Author: Merlin Thomas GUIDELINES Steroid therapy may protect against progressive
Specific management of IgA nephropathy: role of steroid therapy Date written: July 2005 Final submission: September 2005 Author: Merlin Thomas GUIDELINES Steroid therapy may protect against progressive
reported, these are perhaps surprisingly rare given the role immunogenetics is now Table 1. Secondary membranous nephropathy (MN).
.") CME RENAL MEDICINE Clinical Medicine 2012, Vol 12, No 5: 461 6 CME Renal medicine Edited by Simon C Satchell, consultant senior lecturer in renal medicine, Richard Bright Renal Unit, Southmead Hospital
CME RENAL MEDICINE Clinical Medicine 2012, Vol 12, No 5: 461 6 CME Renal medicine Edited by Simon C Satchell, consultant senior lecturer in renal medicine, Richard Bright Renal Unit, Southmead Hospital
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Clinical pathological correlations in AKI
 Clinical pathological correlations in AKI Dr. Rajasekara chakravarthi Director - Nephrology Star Kidney Center, Star Hospitals Renown clinical services India Introduction AKI is common entity Community
Clinical pathological correlations in AKI Dr. Rajasekara chakravarthi Director - Nephrology Star Kidney Center, Star Hospitals Renown clinical services India Introduction AKI is common entity Community
Glomerular diseases with organized deposits
 Glomerular diseases with organized deposits Banu Sis, MD, FRCPC University of Alberta, Edmonton, AB, Canada Ulusal Patoloji Kongresi, Manavgat, Antalya 8/11/2012 What is an organized deposit? A number
Glomerular diseases with organized deposits Banu Sis, MD, FRCPC University of Alberta, Edmonton, AB, Canada Ulusal Patoloji Kongresi, Manavgat, Antalya 8/11/2012 What is an organized deposit? A number
The CARI Guidelines Caring for Australians with Renal Impairment. Membranous nephropathy Role of alkylating agents GUIDELINES
 Membranous nephropathy Role of alkylating agents Date written: July 2005 Final submission: September 2005 Author: Merlin Thomas GUIDELINES a. Treatment with alkylating agents is associated with an increased
Membranous nephropathy Role of alkylating agents Date written: July 2005 Final submission: September 2005 Author: Merlin Thomas GUIDELINES a. Treatment with alkylating agents is associated with an increased
Factors affecting the long-term outcomes of idiopathic membranous nephropathy
 Huh et al. BMC Nephrology (2017) 18:104 DOI 10.1186/s12882-017-0525-6 RESEARCH ARTICLE Factors affecting the long-term outcomes of idiopathic membranous nephropathy Hyuk Huh 1, Hajeong Lee 1, Jung Pyo
Huh et al. BMC Nephrology (2017) 18:104 DOI 10.1186/s12882-017-0525-6 RESEARCH ARTICLE Factors affecting the long-term outcomes of idiopathic membranous nephropathy Hyuk Huh 1, Hajeong Lee 1, Jung Pyo
Clinicopathologic Characteristics of IgA Nephropathy with Steroid-responsive Nephrotic Syndrome
 J Korean Med Sci 2009; 24 (Suppl 1): S44-9 ISSN 1011-8934 DOI: 10.3346/jkms.2009.24.S1.S44 Copyright The Korean Academy of Medical Sciences Clinicopathologic Characteristics of IgA Nephropathy with Steroid-responsive
J Korean Med Sci 2009; 24 (Suppl 1): S44-9 ISSN 1011-8934 DOI: 10.3346/jkms.2009.24.S1.S44 Copyright The Korean Academy of Medical Sciences Clinicopathologic Characteristics of IgA Nephropathy with Steroid-responsive
Do Anti Phospholipase A2 Receptor Antibodies Predict Recurrence of Membranous Nephropathy After Transplantation?
 Do Anti Phospholipase A2 Receptor Antibodies Predict Recurrence of Membranous Nephropathy After Transplantation? Rivka Ayalon MD Boston University Medical Center Idiopathic Membranous Nephropathy One of
Do Anti Phospholipase A2 Receptor Antibodies Predict Recurrence of Membranous Nephropathy After Transplantation? Rivka Ayalon MD Boston University Medical Center Idiopathic Membranous Nephropathy One of
PRIMARY GLOMERULAR DISEASES
 University of Sydney PRIMARY GLOMERULAR DISEASES David Harris 8/2015 Westmead Hospital KDIGO GUIDELINES Steroid-sensitive & resistant nephrotic syndrome in children Minimal-change disease and FSGS in children
University of Sydney PRIMARY GLOMERULAR DISEASES David Harris 8/2015 Westmead Hospital KDIGO GUIDELINES Steroid-sensitive & resistant nephrotic syndrome in children Minimal-change disease and FSGS in children
Secondary IgA Nephropathy & HSP
 Secondary IgA Nephropathy & HSP Anjali Gupta, MD 1/11/11 AKI sec to Hematuria? 65 cases of ARF after an episode of macroscopic hematuria have been reported in the literature in patients with GN. The main
Secondary IgA Nephropathy & HSP Anjali Gupta, MD 1/11/11 AKI sec to Hematuria? 65 cases of ARF after an episode of macroscopic hematuria have been reported in the literature in patients with GN. The main
Chapter 6: Idiopathic focal segmental glomerulosclerosis in adults Kidney International Supplements (2012) 2, ; doi: /kisup.2012.
 2, ; doi: /kisup.2012.") http://www.kidney-international.org chapter 6 & 2012 KDIGO Chapter 6: Idiopathic focal segmental glomerulosclerosis in adults Kidney International Supplements (2012) 2, 181 185; doi:10.1038/kisup.2012.19
http://www.kidney-international.org chapter 6 & 2012 KDIGO Chapter 6: Idiopathic focal segmental glomerulosclerosis in adults Kidney International Supplements (2012) 2, 181 185; doi:10.1038/kisup.2012.19
Types Pathophysiology Clinical manifestations D.Dx. Investigations. Treatment. Complications.
 Types Pathophysiology Clinical manifestations D.Dx. Investigations. Treatment. Complications. Nephrotic syndrome affects 1-3 per 100,000 children
Types Pathophysiology Clinical manifestations D.Dx. Investigations. Treatment. Complications. Nephrotic syndrome affects 1-3 per 100,000 children
Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis
 GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
Out of date SUGGESTIONS FOR CLINICAL CARE (Suggestions are based on level III and IV evidence)
") Membranous nephropathy role of cyclosporine therapy Date written: July 2005 Final submission: September 2005 Author: Merlin Thomas GUIDELINES a. The use of cyclosporine therapy alone to prevent progressive
Membranous nephropathy role of cyclosporine therapy Date written: July 2005 Final submission: September 2005 Author: Merlin Thomas GUIDELINES a. The use of cyclosporine therapy alone to prevent progressive
GOOD MORNING. Welcome Applicants! Friday, October 31, (Happy Halloween!)
") GOOD MORNING Welcome Applicants! Friday, October 31, 2014 (Happy Halloween!) PREP QUESTION A 14-year-old girl has had 3 days of new, unremitting headache associated with vomiting and awakening from sleep
GOOD MORNING Welcome Applicants! Friday, October 31, 2014 (Happy Halloween!) PREP QUESTION A 14-year-old girl has had 3 days of new, unremitting headache associated with vomiting and awakening from sleep
Use of mycophenolate mofetil in steroid-dependent and -resistant nephrotic syndrome
 Pediatr Nephrol (2003) 18:833 837 DOI 10.1007/s00467-003-1175-4 BRIEF REPORT Gina-Marie Barletta William E. Smoyer Timothy E. Bunchman Joseph T. Flynn David B. Kershaw Use of mycophenolate mofetil in steroid-dependent
Pediatr Nephrol (2003) 18:833 837 DOI 10.1007/s00467-003-1175-4 BRIEF REPORT Gina-Marie Barletta William E. Smoyer Timothy E. Bunchman Joseph T. Flynn David B. Kershaw Use of mycophenolate mofetil in steroid-dependent
Nephrology Grand Rounds. Mansi Mehta November 24, 2015
 Nephrology Grand Rounds Mansi Mehta November 24, 2015 Case 51yo F with PMH significant for Hypertension referred to renal clinic for evaluation of elevated Cr. no known history of CKD; baseline creatinine
Nephrology Grand Rounds Mansi Mehta November 24, 2015 Case 51yo F with PMH significant for Hypertension referred to renal clinic for evaluation of elevated Cr. no known history of CKD; baseline creatinine
Glomerular pathology-2 Nephritic syndrome. Dr. Nisreen Abu Shahin
 Glomerular pathology-2 Nephritic syndrome Dr. Nisreen Abu Shahin 1 The Nephritic Syndrome Pathogenesis: inflammation proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls
Glomerular pathology-2 Nephritic syndrome Dr. Nisreen Abu Shahin 1 The Nephritic Syndrome Pathogenesis: inflammation proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls
ANCA associated vasculitis in China
 ANCA associated vasculitis in China Min Chen Renal Division, Peking University First Hospital, Beijing 100034, P. R. China 1 General introduction of AAV in China Disease spectrum and ANCA type Clinical
ANCA associated vasculitis in China Min Chen Renal Division, Peking University First Hospital, Beijing 100034, P. R. China 1 General introduction of AAV in China Disease spectrum and ANCA type Clinical
Russia Dialysis Society Peterhof, Russia June 8, 2016
 Russia Dialysis Society Peterhof, Russia June 8, 2016 TREATMENT OF GLOMERULONEPHRITIS XV Северо-Западная ( AAV, SLE, Нефрологическая Membranous) Школа What s changed in the past decade? William Couser,
Russia Dialysis Society Peterhof, Russia June 8, 2016 TREATMENT OF GLOMERULONEPHRITIS XV Северо-Западная ( AAV, SLE, Нефрологическая Membranous) Школа What s changed in the past decade? William Couser,
Treatment of Idiopathic Membranous Nephropathy
 Treatment of Idiopathic Membranous Nephropathy Meryl Waldman and Howard A. Austin III Kidney Disease Section, National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health,
Treatment of Idiopathic Membranous Nephropathy Meryl Waldman and Howard A. Austin III Kidney Disease Section, National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health,
LONG-TERM OUTCOME OF PATIENTS WITH LUPUS NEPHRITIS: A SINGLE CENTER EXPERIENCE
 & LONG-TERM OUTCOME OF PATIENTS WITH LUPUS NEPHRITIS: A SINGLE CENTER EXPERIENCE Senija Rašić 1 *, Amira Srna 1, Snežana Unčanin 1, Jasminka Džemidžić 1, Damir Rebić 1, Alma Muslimović 1, Maida Rakanović-Todić
& LONG-TERM OUTCOME OF PATIENTS WITH LUPUS NEPHRITIS: A SINGLE CENTER EXPERIENCE Senija Rašić 1 *, Amira Srna 1, Snežana Unčanin 1, Jasminka Džemidžić 1, Damir Rebić 1, Alma Muslimović 1, Maida Rakanović-Todić
Evidence review: Rituximab for Membranous Glomerular Nephritis
 NHS England Evidence review: Rituximab for Membranous Glomerular Nephritis 1 NHS England Evidence review: Rituximab for Membranous Glomerular Nephritis First published: March 2013 Updated: March 2016 Prepared
NHS England Evidence review: Rituximab for Membranous Glomerular Nephritis 1 NHS England Evidence review: Rituximab for Membranous Glomerular Nephritis First published: March 2013 Updated: March 2016 Prepared
Primary Glomerulonephritides
 Primary Glomerulonephritides Idiopathic Nephrotic Syndrome in Adults Stephen M. Korbet, M.D. Rush University Medical Center Chicago, Illinois 40% 35% 30% 34% 35% 33% 33% Korbet Haas 25% 20% 15% 10% 5%
Primary Glomerulonephritides Idiopathic Nephrotic Syndrome in Adults Stephen M. Korbet, M.D. Rush University Medical Center Chicago, Illinois 40% 35% 30% 34% 35% 33% 33% Korbet Haas 25% 20% 15% 10% 5%
Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009
 Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009 DR. KERRY COOPER IS ON THE SPEAKER BUREAU OF AMGEN, ABBOTT, GENZYME, SHIRE, AND BMS DR. COOPER IS ALSO INVOLVED IN CLINICAL
Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009 DR. KERRY COOPER IS ON THE SPEAKER BUREAU OF AMGEN, ABBOTT, GENZYME, SHIRE, AND BMS DR. COOPER IS ALSO INVOLVED IN CLINICAL
Glomerular diseases mostly presenting with Nephritic syndrome
 Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis
 Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
Recurrent Idiopathic Membranous Glomerulonephritis After Kidney Transplantation and Successful Treatment With Rituximab
 TRANSPLANTATION Recurrent Idiopathic Membranous Glomerulonephritis After Kidney Transplantation and Successful Treatment With Rituximab Khadijeh Makhdoomi, 1,2 Saeed Abkhiz, 1,2 Farahnaz Noroozinia, 1,3
TRANSPLANTATION Recurrent Idiopathic Membranous Glomerulonephritis After Kidney Transplantation and Successful Treatment With Rituximab Khadijeh Makhdoomi, 1,2 Saeed Abkhiz, 1,2 Farahnaz Noroozinia, 1,3
FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS
 FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS Guillermo A. Herrera MD Louisiana State University, Shreveport Fibrils in bundles 10-20 nm d Diabetic fibrillosis
FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS Guillermo A. Herrera MD Louisiana State University, Shreveport Fibrils in bundles 10-20 nm d Diabetic fibrillosis
IgA Nephropathy - «Maladie de Berger»
 IgA Nephropathy - «Maladie de Berger» B. Vogt, Division de Néphrologie/Consultation d Hypertension CHUV, Lausanne 2011 Montreux CME SGN-SSN IgA Nephropathy 1. Introduction 2. Etiology and Pathogenesis
IgA Nephropathy - «Maladie de Berger» B. Vogt, Division de Néphrologie/Consultation d Hypertension CHUV, Lausanne 2011 Montreux CME SGN-SSN IgA Nephropathy 1. Introduction 2. Etiology and Pathogenesis
Nephrotic syndrome Dr.Basma Adel FIFTH GRADE
 Nephrotic syndrome Dr.Basma Adel FIFTH GRADE 2017-2018 At the end of this lecture you should know: Types Pathophysiology Clinical manifestations D.Dx. Investigations. Treatment. Complications. 12/3/2017
Nephrotic syndrome Dr.Basma Adel FIFTH GRADE 2017-2018 At the end of this lecture you should know: Types Pathophysiology Clinical manifestations D.Dx. Investigations. Treatment. Complications. 12/3/2017
Renal Pathology Case Conference. Case 2
 Renal Pathology Case Conference Case 2 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN cornell.lynn@mayo.edu March 2, 2008 Clinical presentation 68 year old woman, initially with normal renal function
Renal Pathology Case Conference Case 2 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN cornell.lynn@mayo.edu March 2, 2008 Clinical presentation 68 year old woman, initially with normal renal function
Interesting case seminar: Native kidneys Case Report:
 Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Efficacy and safety of long course tacrolimus treatment for idiopathic membranous nephropathy
 EXPERIMENTAL AND THERAPEUTIC MEDICINE 16: 979-984, 2018 Efficacy and safety of long course tacrolimus treatment for idiopathic membranous nephropathy JIA DI 1*, QING QIAN 2*, MIN YANG 1, YAPING JIANG 1,
EXPERIMENTAL AND THERAPEUTIC MEDICINE 16: 979-984, 2018 Efficacy and safety of long course tacrolimus treatment for idiopathic membranous nephropathy JIA DI 1*, QING QIAN 2*, MIN YANG 1, YAPING JIANG 1,
Considering the early proactive switch from a CNI to an mtor-inhibitor (Case: Male, age 34) Josep M. Campistol
 Josep M. Campistol") Considering the early proactive switch from a CNI to an mtor-inhibitor (Case: Male, age 34) Josep M. Campistol Patient details Name DOB ESRD Other history Mr. B.I.B. 12 January 1975 (34yo) Membranous GN
Considering the early proactive switch from a CNI to an mtor-inhibitor (Case: Male, age 34) Josep M. Campistol Patient details Name DOB ESRD Other history Mr. B.I.B. 12 January 1975 (34yo) Membranous GN
CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS
 CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS DR ANNIE JOJO, Dr Seethalekshmy N V, Dr Nanda Kachare DEPARTMENT OF PATHOLOGY, AMRITA INSTITUTE OF MEDICAL SCIENCES, KOCHI. 54 yrs female,
CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS DR ANNIE JOJO, Dr Seethalekshmy N V, Dr Nanda Kachare DEPARTMENT OF PATHOLOGY, AMRITA INSTITUTE OF MEDICAL SCIENCES, KOCHI. 54 yrs female,
Review Article Recent Progress in Deciphering the Etiopathogenesis of Primary Membranous Nephropathy
 Hindawi BioMed Research International Volume 2017, Article ID 1936372, 14 pages https://doi.org/10.1155/2017/1936372 Review Article Recent Progress in Deciphering the Etiopathogenesis of Primary Membranous
Hindawi BioMed Research International Volume 2017, Article ID 1936372, 14 pages https://doi.org/10.1155/2017/1936372 Review Article Recent Progress in Deciphering the Etiopathogenesis of Primary Membranous
Proteinuria DR. SANJAY PANDEYA MD. FRCPC.
 Proteinuria DR. SANJAY PANDEYA MD. FRCPC. Objectives Define normal and abnormal range(s) of proteinuria Evaluation of proteinuria Be aware of complications of proteinuria When to refer and when not to
Proteinuria DR. SANJAY PANDEYA MD. FRCPC. Objectives Define normal and abnormal range(s) of proteinuria Evaluation of proteinuria Be aware of complications of proteinuria When to refer and when not to
Low-Density Lipoprotein Apheresis Therapy for Steroid- and Cyclosporine-Resistant Idiopathic Membranous Nephropathy
 CASE REPORT Low-Density Lipoprotein Apheresis Therapy for Steroid- and Cyclosporine-Resistant Idiopathic Membranous Nephropathy Yoshinori Sato,3, Shinichiro Tsunoda 2,3, Tsuyoshi Nozue 3,QinyaPan 3, Harue
CASE REPORT Low-Density Lipoprotein Apheresis Therapy for Steroid- and Cyclosporine-Resistant Idiopathic Membranous Nephropathy Yoshinori Sato,3, Shinichiro Tsunoda 2,3, Tsuyoshi Nozue 3,QinyaPan 3, Harue
Histopathology: Glomerulonephritis and other renal pathology
 Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That Showed Predominantly Membranous Features
 Hindawi Case Reports in Nephrology Volume 2017, Article ID 1027376, 5 pages https://doi.org/10.1155/2017/1027376 Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That
Hindawi Case Reports in Nephrology Volume 2017, Article ID 1027376, 5 pages https://doi.org/10.1155/2017/1027376 Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That
7-2 Transplantation Case-Based Discussion
 The 58 th JSN 2015/6/4@Nagoya APSN Continuing Medical Education Course 2015 7-2 Transplantation Case-Based Discussion Tadashi Sofue, MD, PhD Division of Nephrology and Dialysis, Department of Internal
The 58 th JSN 2015/6/4@Nagoya APSN Continuing Medical Education Course 2015 7-2 Transplantation Case-Based Discussion Tadashi Sofue, MD, PhD Division of Nephrology and Dialysis, Department of Internal
Familial DDD associated with a gain-of-function mutation in complement C3.
 Familial DDD associated with a gain-of-function mutation in complement C3. Santiago Rodríguez de Córdoba, Centro de investigaciones Biológicas, Madrid Valdés Cañedo F. and Vázquez- Martul E., Complejo
Familial DDD associated with a gain-of-function mutation in complement C3. Santiago Rodríguez de Córdoba, Centro de investigaciones Biológicas, Madrid Valdés Cañedo F. and Vázquez- Martul E., Complejo
Glomerular pathology in systemic disease
 Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
RENAL HISTOPATHOLOGY
 RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
Primary Membranous Nephropathy
 Primary Membranous Nephropathy William G. Couser Abstract Membranous nephropathy (MN) is a unique glomerular lesion that is the most common cause of idiopathic nephrotic syndrome in nondiabetic white adults.
Primary Membranous Nephropathy William G. Couser Abstract Membranous nephropathy (MN) is a unique glomerular lesion that is the most common cause of idiopathic nephrotic syndrome in nondiabetic white adults.
Original. IgAN. Key words : IgA nephropathy, IgM deposition, proteinuria, tonsillectomy, steroid pulse therapy. Introduction
 Showa Univ J Med Sci 27 3, 167 174, September 2015 Original Prominent IgM Deposition in Glomerulus Is Associated with Severe Proteinuria and Reduced after Combined Treatment of Tonsillectomy with Steroid
Showa Univ J Med Sci 27 3, 167 174, September 2015 Original Prominent IgM Deposition in Glomerulus Is Associated with Severe Proteinuria and Reduced after Combined Treatment of Tonsillectomy with Steroid
Oral mizoribine pulse therapy for patients with steroid-resistant and frequently relapsing steroid-dependent nephrotic syndrome
 Nephrol Dial Transplant (2005) 20: 2243 2247 doi:10.1093/ndt/gfh996 Advance Access publication 19 July 2005 Brief Report Oral mizoribine pulse therapy for patients with steroid-resistant and frequently
Nephrol Dial Transplant (2005) 20: 2243 2247 doi:10.1093/ndt/gfh996 Advance Access publication 19 July 2005 Brief Report Oral mizoribine pulse therapy for patients with steroid-resistant and frequently
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Debiec H, Lefeu F, Kemper MJ, et al. Early-childhood membranous
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Debiec H, Lefeu F, Kemper MJ, et al. Early-childhood membranous
Lupus nephritis. Vladimir Tesar Department of Nephrology, General University Hospital, Prague, Czech Republic
 Lupus nephritis Vladimir Tesar Department of Nephrology, General University Hospital, Prague, Czech Republic Disclosure of Interests Abbvie, Amgen, Baxter, Bayer, Boehringer-Ingelheim, Calliditas, Chemocentryx,
Lupus nephritis Vladimir Tesar Department of Nephrology, General University Hospital, Prague, Czech Republic Disclosure of Interests Abbvie, Amgen, Baxter, Bayer, Boehringer-Ingelheim, Calliditas, Chemocentryx,
29th Annual Meeting of the Glomerular Disease Collaborative Network
 29th Annual Meeting of the Glomerular Disease Collaborative Network Updates on the Pathogenesis IgA Nephropathy and IgA Vasculitis (HSP) J. Charles Jennette, M.D. Brinkhous Distinguished Professor and
29th Annual Meeting of the Glomerular Disease Collaborative Network Updates on the Pathogenesis IgA Nephropathy and IgA Vasculitis (HSP) J. Charles Jennette, M.D. Brinkhous Distinguished Professor and