Eculizumab in an anephric patient with atypical haemolytic uraemic syndrome and advanced vascular lesions.
|
|
|
- Junior Gaines
- 5 years ago
- Views:
Transcription

1 Eculizumab in an anephric patient with atypical haemolytic uraemic syndrome and advanced vascular lesions. Bekassy, Zivile; Kristoffersson, Ann-Charlotte; Cronqvist, Mats; Roumenina, Lubka T; Rybkine, Tania; Vergoz, Laura; Hue, Christophe; Fremeaux-Bacchi, Veronique; Karpman, Diana Published in: Nephrology Dialysis Transplantation DOI: /ndt/gft Link to publication Citation for published version (APA): Békassy, Z., Kristoffersson, A-C., Cronqvist, M., Roumenina, L. T., Rybkine, T., Vergoz, L.,... Karpman, D. (2013). Eculizumab in an anephric patient with atypical haemolytic uraemic syndrome and advanced vascular lesions. Nephrology Dialysis Transplantation, 28(11), DOI: /ndt/gft340 General rights Copyright and moral rights for the publications made accessible in the public portal are retained by the authors and/or other copyright owners and it is a condition of accessing publications that users recognise and abide by the legal requirements associated with these rights. Users may download and print one copy of any publication from the public portal for the purpose of private study or research. You may not further distribute the material or use it for any profit-making activity or commercial gain You may freely distribute the URL identifying the publication in the public portal Take down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. L UNDUNI VERS I TY PO Box L und
2 Eculizumab in an anephric patient with atypical hemolytic uremic syndrome and advanced vascular lesions Zivile D. Békássy 1, Ann-Charlotte Kristoffersson 1, Mats Cronqvist 2, Lubka T. Roumenina 3,4,5, Tania Rybkine 3,4,5, Laura Vergoz 3,5, Christophe Hue 3,4,5, Veronique Fremeaux-Bacchi 3,6, Diana Karpman 1 1 Department of Pediatrics, Clinical Sciences Lund, Lund University, Lund, Sweden 2 Department of Radiology, Skåne University Hospital, Lund, Sweden 3 INSERM UMRS 872, Cordeliers Research Center, Paris, France 4 Université Paris Descartes Sorbonne Paris-Cité, Paris, France 5 Université Pierre et Marie Curie (UPMC-Paris-6), Paris, France 6 Assistance Publique-Hopitaux de Paris, Hopital Européen Georges-Pompidou, Service d Immunologie Biologique, Paris, France Corresponding author: Diana Karpman, Department of Pediatrics, Lund University, Lund, Sweden Telephone number: , Fax number: address: diana.karpman@med.lu.se 1
3 Abstract Background Atypical hemolytic uremic syndrome (ahus) is associated with dysfunction of the alternative pathway of complement. Disease activity subsides as renal failure progresses but recurs upon renal transplantation, indicating that viable renal tissue contributes to disease activity. We present evidence of cerebrovascular occlusive disease indicating that vascular injury may occur in the absence of kidneys. Methods A currently 12-year-old girl developed renal failure at the age of 20 months, underwent bilateral nephrectomy and renal transplantation but lost the transplant due to recurrences. She was on hemodialysis for 7 years. At 10 years of age she developed a transient ischemic attack. Imaging, genetic investigation and mutation characterization were performed. Results Imaging demonstrated occlusion and stenosis of the carotid arteries. Two complement mutations, a novel mutation in factor B and a previously described mutation in factor I, and the H3-factor H haplotype, were identified. The factor B mutation, L433S, did not induce excessive complement activation in vitro. Measurement of C3 degradation products indicated ongoing complement activation. In spite of the patient s being anephric treatment was initiated with Eculizumab, humanized anti-c5 antibody that blocks terminal complement activation. She underwent a successful kidney transplant nine months later and has not developed a recurrence or progression of vascular stenosis one year later. Conclusions The course of disease in this patient with ahus suggests that complement-mediated vascular injury may occur in the total absence of renal tissue and overt recurrences. To our knowledge this is the first description of Eculizumab treatment in an anephric ahus patient. 2
4 Keywords: complement, eculizumab, factor B, factor I, hemolytic uremic syndrome, transient ischemic attack Short summary This study describes the clinical course of a child with recurrent episodes of atypical HUS and complement mutations in factor B and factor I. Her native kidneys and kidney transplant were removed and she was on dialysis for 7 years at which point she developed a transient ischemic attack. Imaging demonstrated advanced carotid artery lesions bilaterally. Evidence of ongoing complement activation led to the initiation of eculizumab (anti-c5) treatment while the patient was anephric, and on this treatment the patient was successfully transplanted and did not exhibit progression of arterial lesions. 3
5 Introduction Patients with atypical hemolytic uremic syndrome (ahus) develop symptomatic disease and recurrences (defined as acute episodes of non-immune hemolytic anemia, thrombocytopenia and acute renal failure) as long as there is residual renal function and after renal transplantation, indicating that viable renal tissue triggers disease activity. ahus is, in most cases, associated with mutations or complex rearrangements in complement regulators and factors such as factor H (CFH), factor I (CFI), membrane-cofactor protein (MCP), C3, factor B (CFB) and thrombomodulin, as reviewed in [1, 2]. Certain patients have circulating anti-factor H antibodies [3] often associated with deletions in factor H-related proteins (CFHRs) 3/1 [4]. Treatment with the inhibitor of the terminal pathway of complement Eculizumab blocks disease progression and enables transplantation without recurrence in the majority of ahus patients with terminal renal failure [5, 6]. It has previously been assumed that patients with ahus will not have evidence of disease progression or hematological recurrence when kidneys are removed or severely dysfunctional resulting in terminal renal failure. One previous report showed, however, that vascular stenosis might occur even in the absence of viable renal tissue [7]. We will describe the investigation and treatment of a child with ahus, and several complement mutations, with a clinical course indicating advanced vascular stenosis years after nephrectomy. This case demonstrates that patients may develop severe systemic vascular damage even in the absence of recurrences of disease. 4
6 Subject and Methods Patient A currently 12 year-old girl presented at 17 months of age with a transient episode of anemia associated with infection. One month later she developed HUS and after a second recurrence within 3 months, in spite of weekly plasma exchange, developed end-stage renal failure treated with peritoneal dialysis and weekly plasma exchange. A renal biopsy showed glomerular endothelial cell swelling, arteriolar intimal thickening and mesangial proliferation. Immunofluorescence exhibited deposits of IgM, fibrinogen and C3 in glomerular capillaries. She underwent deceased-donor renal transplant and nephrectomy of her native kidneys at the age of 3 years, before the advent of Eculizumab treatment. She was treated with plasma infusions once weekly and plasma exchange also once weekly but, in spite of these treatments, developed three HUS recurrences related to septic episodes caused by Staphylococcus aureus. The HUS episodes were associated with malignant hypertension leading to generalized seizures with transient focal neurological symptoms including increased right-sided muscle tone. Computed tomography of the brain was normal at that time. The hypertensive crisis resulted in removal of the transplant at 4 years of age. She was thereafter treated with hemodialysis through an arteriovenous fistula five days a week for 7 years. Treatment with plasma exchange and infusions was terminated after transplant nephrectomy and no hematological recurrences of HUS (hemolytic anemia and thrombocytopenia) occurred during this period. 5
7 At the age of 10 years she developed a transient ischemic attack (TIA) with severe neurological symptoms including sudden onset of headache and vomiting followed by aphasia, salivation, ataxia, weakness in both arms and confusion. These neurological symptoms resolved within a few hours. Imaging of her carotid arteries demonstrated total occlusion of the right carotid artery and near-occlusion of the left carotid artery (see detailed description below). Echocardiography ruled out left ventricular hypertrophy. Ophthalmological examination was normal. Measurement of C3 and the C3 degradation product C3dg indicated that there was ongoing complement activation (Table 1). Eculizumab (Alexion, Cheshire, Conn) treatment was initiated in the absence of HUS manifestations and viable renal tissue. Doses were 600 mg per week for three weeks followed by 600 mg every other week. On this treatment the patient underwent a successful deceased-donor kidney transplant eleven months after the TIA without recurrence of HUS one year later. The current Eculizumab dose is 900 mg every other week adjusted for the patient s weight. No progression of vascular occlusion was noted within one year after the TIA by repeated imaging. The glomerular filtration rate was 79 ml/min/1.73 m 2 one year post-transplant. She developed transient mild proteinuria eight months post-transplant with urinary albumin/creatinine ratio of 30 g/mol (reference value <3.8 g/mol), which normalized afterwards. Protocol renal biopsy was not performed. ADAMTS13 activity was measured twice and found to be normal, once at presentation, assayed by the collagen binding assay [8] and the second time by the FRETS-VWF73 assay [9] one year after the second transplantation. The homocysteine level, assayed twice, was 12 µmol/l (reference <10 µmol/l) while on hemodialysis, before the start of eculizumab treatment, and one year after the second transplantation. This study was performed 6
8 with the approval of the Ethics Committee of the Medical Faculty at Lund University and the informed consent of the patient s parents. Mutation analysis DNA was extracted from whole blood using the QIAamp DNA Blood Mini Kit (Qiagen GmbH, Hilden, Germany) [10] and exons of CFI [11], CFB [12], C3 [13], CFH [14] and MCP [15] were sequenced. The presence or deletion of the CFHR3/1 genes was analyzed as described [16]. Sequencing of the thrombomodulin gene was not performed. CFH antibody analysis Analysis of anti-cfh antibodies was performed by ELISA according to a previously described method [3]. In silico analysis of CFB and C3b The atomic coordinates of the C3 convertase C3bBb [17] were used to visualize ahus-associated mutations using PyMol software. In this study amino acid residue numbering of CFB included the 25-residue leader peptide. Recombinant CFB constructs The CFB mutation L433S was introduced into a CFB-containing plasmid by sitedirected mutagenesis, as previously described [18]. The construct was completely sequenced to assure the introduction of the mutation and the lack of additional genetic changes. The recombinant wild-type or mutant (L433S) and previously published ahus gain-of-function mutation D279G [18] CFB proteins were transiently expressed in human embryonic kidney (HEK-293T) cells (ATCC). The cells were 7
9 cultured for 3 days in DMEM+glutaMAXTM-I with 4.5g/l D-glucose and pyruvate (Gibco, Paisley, UK) without fetal calf serum. The integrity of the proteins was verified by immunoblotting and quantified by ELISA, as previously described [19]. CFB binding to C3b Enzyme-linked immunosorbent assay (ELISA) CFB binding to C3b was measured by ELISA as described previously [18]. Plates were coated with C3b (CompTech, Tylor, TX) and various concentrations of recombinant wild-type or mutant CFB were added in the fluid phase. The binding of the mutant protein was expressed as percent of the wild-type CFB binding in the plateau. Surface plasmon resonance The interaction of wild-type and mutant CFB with C3b was also analyzed in real-time using surface plasmon resonance technology on ProteOn XPR36 equipment (BioRad, Hercules, CA). C3b was coupled to the GLC biosensor chip, using standard amidecoupling technology, according to the manufacturer s instructions. Recombinant CFB were injected as an analyte at concentrations , 81.25, 162.5, 325, 650 pm at a flow of 50 μl/min in Mg 2+ - containing Hepes buffer (10mM Hepes ph 7.4, 50mM NaCl, 10mM MgCl 2 ). A blank activated/deactivated flowcell served as a control with and without injected CFB. Data were analyzed using ProteOn Manager software and the data from the blank flowcell were subtracted. 8
10 Endothelial cell assay Primary human umbilical cord veins cells (HUVEC) in the third passage were activated overnight with tumor necrosis factor-alpha (TNFα, 10 ng/ml) and interferon-gamma (IF γ, 10 3 U/ml, both from Peprotech, Rockyhill NJ), as described [18, 20]. After washing with PBS, adherent cells were incubated with 50 μl CFBdepleted serum (CompTech), and with 100 µl recombinant wild-type or mutant CFB supernatants, containing an equal amount (10 μg/ml) of CFB. Alternatively, the cells were incubated with sera of normal anonymous blood donors (n=55, obtained with INSERM IRB authorization for research purposes) or sera from the patient s mother or father. Sera were diluted to 33% in M199 medium (Gibco) as described [18, 20]. After a 30-minute incubation at 37 C and washing, the cells were detached labeled with monoclonal anti-c3c (Quidel, San Diego, CA) or control mouse IgG1, followed by phycoerythrin (PE)-labeled secondary antibody (Beckman Coulter, Roissy, France). Cells were analyzed by flow cytometry using Becton Dickinson Facs-calibur (Mountain View, CA), and CellQuest and FCS express software (for acquisition and analysis, respectively). 9
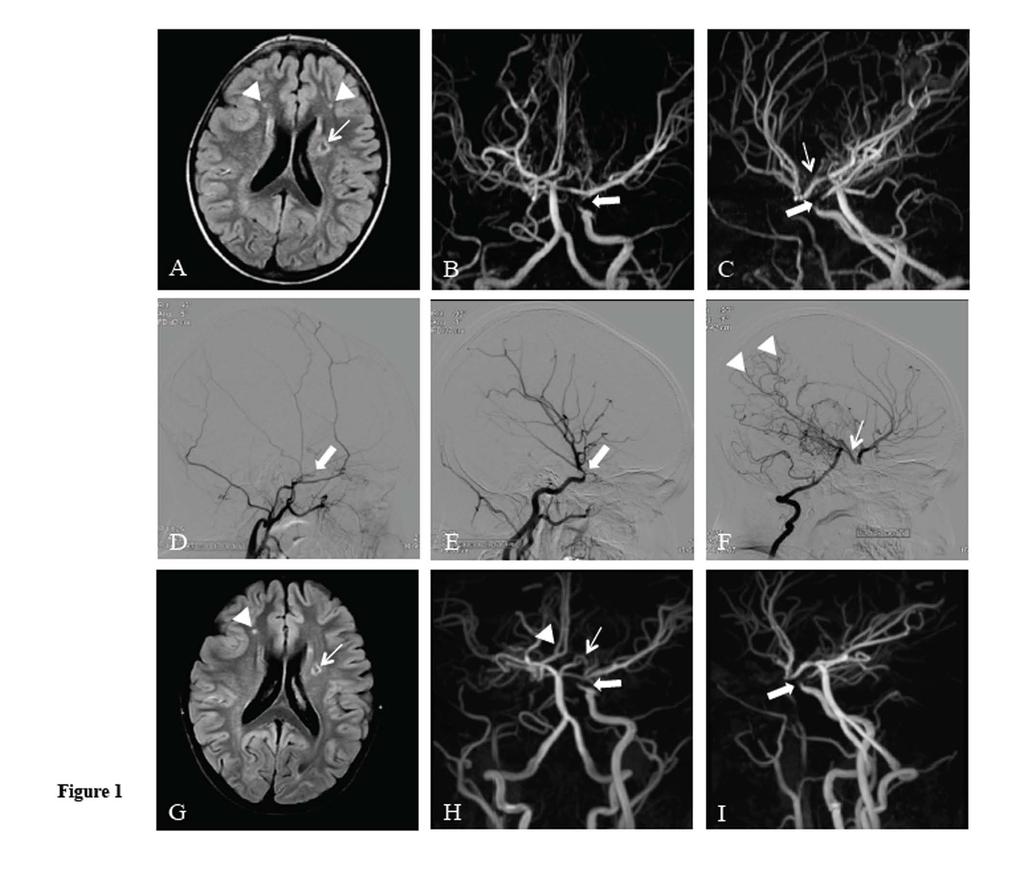
11 Results Imaging of the vascular lesions At the time of the TIA magnetic resonance imaging and angiography (MRI/MRA) as well as digital subtraction angiography (DSA) were carried out. MRI demonstrated an older frontal infarct in the left hemisphere as well as small frontal nodular and subcortical vascular lesions bilaterally (Figure 1A). More recent ischemic lesions were not present. MRA of the cervical and intracranial arteries revealed total occlusion of the right carotid artery (the artery is therefore not visible in Figure 1B) and near-occlusion of the left carotid artery (Figure 1B and 1C). This was confirmed by DSA (Figure 1D-F). Collateral flow to the right hemisphere from the right posterior communicating artery (Figure 1C and 1F) and retrograde supply through an organized pial network (Figure 1F) were noted. The following MRI and MRAs two and 16 months after the TIA (the latter six months after the renal transplantation) showed no change (Figure 1G-I). Complement analysis Complement analyses carried out on samples from the patient and her parents are summarized in Table 1. C3 was low and C3dg was elevated at debut suggesting complement consumption. Low C3 and elevated C3dg were also detected after removal of all renal tissue, before and during eculizumab treatment while the patient was on hemodialysis. After the 2 nd transplantation C3 levels increased initially to normal range but later fell to below the normal range with subsequent C3dg elevation. Quantitative complement function via the alternative pathway was totally blocked during eculizumab treatment, as expected. The CFI concentration was normal during the entire follow-up. Increased levels of C3dg indicated adequate degradation of C3 10
12 by functionally active CFI. The CFB concentration was normal at debut but was decreased or in the lower normal range during hemodialysis and after the 2 nd transplantation. CFH and C4 levels were normal at all times. Genetic investigation of the patient Two complement mutations, in the genes encoding CFI and CFB, as well as the CFH H3 disease-associated haplotype, were found (Table 2). The heterozygous G261D mutation in the CFI gene was found before removal of the first graft but no functional defect of CFI was demonstrated, as previously reported [21, 22]. A novel heterozygous mutation in CFB, L433S, was found, as characterized below. The CFB mutation was not found in the normal population ( The finding of normal CFB levels in certain samples indicated that the mutated protein was normally secreted. In addition to the mutation a rare polymorphism was found in exon 13 (E566A), and at amino acid position 7 (exon 2) the patient was homozygous for the R7 polymorphism, which was previously shown to exhibit better binding capacity to C3 than other allele variants [23]. No mutations in the genes encoding CFH, C3 or MCP and no deletion of the CFHR3/1 genes were detected. Serum antibodies to CFH were not detected. Characterization of the CFB mutation A novel heterozygous mutation was found in the CFB gene four years after the CFI mutation was detected and before the second transplantation. This mutation is located in the von Willebrand factor-like A domain, near the Mg 2+ metal-ion adhesion site (MIDAS) and in proximity to, but not directly in the area that binds C3b to form the 11
13 C3bBb convertase (Figure 2A). It is close to three other previously published ahus CFB mutations [12, 18]. To characterize the secretion and function of the CFB mutation, recombinant wildtype CFB, L433S and D279G mutations (the latter is a gain-of-function ahus mutation in CFB used as a positive control[18, 19]) were expressed in HEK293T cells. The level of CFB secreted in the supernatant was similar between the wild-type and the two mutants tested. No CFB was detected in the supernatant of the mocktransfected cells (SN0) (Figure 2B). The interaction of C3b with the wild-type or mutant CFB variants was tested by ELISA and surface plasmon resonance as previously described [18, 20]. Increased binding was observed for the positive control, D279G, but binding of the L433S mutant was similar to, or even weaker than, the wild-type CFB (Figure 2C,D). The capacity of the different CFB variants to induce C3 deposition was tested using TNF IFN -activated HUVEC. D279G, the gain-of-function CFB mutant, showed increased C3 deposition compared to the wild-type but no increase was detected for L433S (Figure 2E). To further address the role of the mutations in CFB and CFI for complement activation, sera from the patient s parents were applied to TNF /IFN -activated HUVECs and tested for C3 deposition as described for other complement mutations [18, 20]. The serum from the patient was obtained when she was on dialysis and had low C3 and CFB levels, and could therefore not be reliably used in this assay. The unaffected parents carried the same CFI and CFB mutations (father) and CFH haplotype (mother) but had normal complement levels at the time of sampling, thus 12
14 their samples were used. Results from this assay are presented in Figure 2F and show that serum from both the father and the mother exhibited increased C3 deposition on the cytokine-activated endothelial cells compared to sera from 55 normal donors. 13
15 Discussion We describe a patient with ahus and mutations in CFB and CFI as well as a riskassociated CFH haplotype in whom we found evidence for complement activation after all renal tissue was removed and no overt hematological recurrences of ahus occurred. We suggest that the advanced occlusion and stenosis in the patient s carotid arteries was due to ongoing complement-induced vascular injury. This provided the rationale for treatment with eculizumab in the absence of renal function. Treatment was efficient in blocking complement activation via the alternative pathway although other endpoints indicating the prevention of ahus activity, such as maintaining a normal platelet count and preventing hemolysis, were not deranged even before the initiation of treatment. No further progression of vascular injury occurred during an 18-month period from when treatment with eculizumab commenced and the patient was successfully transplanted during this time. Hematological recurrences of ahus cease to occur when renal function is very low. This clinical observation has led to the notion that viable renal tissue is required for overt relapses to occur. The kidney is the major organ affected during ahus although the central nervous system may be involved [24]. It is, as yet, unclear how the disease is activated in the kidney. However, limited evidence suggests that low-grade disease activity can proceed even when renal function diminishes or, as in this and one other case [7] is absent. This low-grade complement activation would be expected to progressively damage the endothelium consequently leading to vascular stenosis. Thus even patients with reduced, or lack of, renal function could benefit from complement inhibition. 14
16 Eculizumab inhibits C5 and thereby the terminal complement pathway. Complement activity proximal to C5 remains functional. This may explain why the patient exhibited low levels of C3 even after treatment with eculizumab was initiated. The CFI mutation was not shown to promote complement activation via the alternative pathway [21, 22]. Surprisingly, the novel CFB mutation described here did not exhibit enhanced C3b binding and complement activation on endothelial cells, despite its close proximity to other previously described gain of-function CFB mutations [12, 18]. This is not the only case of complement mutations with no associated functional change. Recently other ahus-associated genetic changes, CFH variants I890 and L1007, were found to lack functional significance, despite strong association with ahus [25]. Nevertheless, the finding that the patient had complement consumption and that both parents sera induced excessive C3 deposition on endothelial cells indicates a clear role for complement in the disease process of this patient. When the mutations in CFB, CFI as well as the CFH risk-associated haplotype, and possibly as yet unidentified factors, are combined in vivo the effect may lead to an overactivation of the alternative pathway that cannot be accounted for by each mutation alone. The beneficial effect of eculizumab in preventing disease recurrence after the second transplant is the ultimate evidence for the role of complement activation in this patient. In addition to vascular damage induced by complement activation, other factors may also contribute to the development of vascular stenosis in our patient, such as a prolonged period of dialysis and elevated homocysteine levels. Children on hemodialysis are at higher risk for developing cardiovascular disease due to uremia- 15
17 related risk factors, dysregulated calcium/phosphate and parathyroid hormone, dyslipidemia, hypertension and chronic inflammation associated with protein-energy malnutrition [26]. Furthermore, pediatric patients with chronic kidney disease were shown to have increased carotid intima-media thickness [27]. High levels of homocysteine are frequently detected in children with chronic renal failure [26] and correlate to arterial stiffness [28]. Accumulation of homocysteine in patients with inborn cobalamin defects may trigger HUS [29]. Although the patient described in this study did not have particularly high homocysteine levels the mild elevation, together with other risk factors, could enhance a prothrombotic propensity. Stenosis and occlusion of large arteries has not been reported as a complication in pediatric dialysis patients suggesting that renal replacement therapy and chronic kidney failure per se could not account for the findings. Complement can be activated during hemodialysis. Several reports have demonstrated generation of activation products C3a and C5a after exposure of plasma or whole blood to hemodialysis filters, both in vitro and vivo (reviewed in [30]). C3 is adsorbed to the biomaterial surface upon contact with blood and can thus trigger the alternative pathway [31, 32]. Dialysis-related complement activation could possibly contribute to advanced vascular injury in the setting of ahus and uninhibited complement activation due to mutations. Stenosis of large arteries has been described in ahus patients on longterm dialysis. One child with a CFH mutation (Ser1191Leu) who was on long-term dialysis after loss of two renal grafts developed stenosis of the middle and anterior cerebral arteries [33, 34]. Her younger monozygous twin sisters, bore the same CFH mutation and also developed ahus. One was dialyzed for two years after which she underwent renal transplantation and both were treated with continuous prophylactic 16
18 plasma exchange for 7 and 9 years, respectively, and exhibited normal cerebral vasculature. Another child with ahus and a CFB mutation (Lys350Asp) developed progressive stenosis of multiple large arteries including thoracic and abdominal aorta branches as well as pulmonary and coronary arteries [7] after several years of dialysis. These cases together with our case suggest that both large and small vessel wall injury is inherent to the course of disease and that progression of extra-renal vascular lesions occurs even in the absence of overt recurrences, a process that may be exacerbated by long-term dialysis. Increasing evidence indicates that activation of the alternative pathway of complement may be proatherogenic within the vessel wall (reviewed in [35]). Early atherosclerotic changes have been demonstrated in internal iliac artery samples obtained during kidney transplantation of pediatric hemodialysis patients [36]. In a patient with multiple complement mutations, such as described here, complement activation in atherosclerotic lesions could be enhanced. Our patient exhibited continuous complement activation as indicated by increased complement degradation products in the circulation. This suggests a pathogenetic mechanism whereby lowgrade constant complement activation will lead to vascular occlusion. We therefore propose that extra-renal vascular lesions may progress even during symptom-free intervals and that imaging for vascular changes, particularly cerebral, should be monitored. For this reason transplantation should be considered as early as possible in ahus patients with end-stage renal failure. Eculizumab protection, during periods of dialysis and after renal transplantation, might prevent serious vascular damage in patients with ahus. 17
19 Financial support and acknowledgements This study was supported by grants from The Swedish Research Council (K X-14008), The Torsten Söderberg Foundation, Crown Princess Lovisa s Society for Child Care and The Konung Gustaf V:s 80-årsfond (to DK). Agence Nationale de la Recherche (ANR Genopath geno03101I) and by EU FP7 grant (EURenOmics) to VFB. The authors thank Fanny Tabarin (INSERM U872, Paris, France) for excellent technical assistance. This study was presented in poster form at the 4 th International Conference HUS- MPGN-TTP & related disorders Innsbruck, Austria, June 9-11, 2013 Transparency declaration VFB is a member of the Alexion Pharmaceuticals (Cheshire, Conn) national advisory board in France. DK was the national coordinator of the Eculizumab multi-center trial in Sweden during The other authors have no disclosures and no competing financial interests. 18
20 References 1. Loirat C, Fremeaux-Bacchi V. Atypical hemolytic uremic syndrome. Orphanet J Rare Dis 2011;6:60 2. Roumenina LT, Loirat C, Dragon-Durey MA, et al. Alternative complement pathway assessment in patients with atypical HUS. J Immunol Methods 2011;365: Dragon-Durey MA, Loirat C, Cloarec S, et al. Anti-Factor H autoantibodies associated with atypical hemolytic uremic syndrome. J Am Soc Nephrol 2005;16: Zipfel PF, Mache C, Muller D, et al. DEAP-HUS: deficiency of CFHR plasma proteins and autoantibody-positive form of hemolytic uremic syndrome. Pediatr Nephrol 2010;25: Zuber J, Le Quintrec M, Krid S, et al. Eculizumab for atypical hemolytic uremic syndrome recurrence in renal transplantation. Am J Transplant 2012;12: Legendre CM, Licht C, Muus P, et al. Terminal complement inhibitor eculizumab in atypical hemolytic-uremic syndrome. N Engl J Med 2013;368: Loirat C, Macher MA, Elmaleh-Berges M, et al. Non-atheromatous arterial stenoses in atypical haemolytic uraemic syndrome associated with complement dysregulation. Nephrol Dial Transplant 2010;25: Gerritsen HE, Turecek PL, Schwarz HP, et al. Assay of von Willebrand factor (vwf)-cleaving protease based on decreased collagen binding affinity of degraded vwf: a tool for the diagnosis of thrombotic thrombocytopenic purpura (TTP). Thromb Haemost 1999;82:
21 9. Kokame K, Nobe Y, Kokubo Y, et al. FRETS-VWF73, a first fluorogenic substrate for ADAMTS13 assay. Br J Haematol 2005;129: Vaziri-Sani F, Holmberg L, Sjöholm AG, et al. Phenotypic expression of factor H mutations in patients with atypical hemolytic uremic syndrome. Kidney Int 2006;69: Fremeaux-Bacchi V, Dragon-Durey MA, Blouin J, et al. Complement factor I: a susceptibility gene for atypical haemolytic uraemic syndrome. J Med Genet 2004;41:e Goicoechea de Jorge E, Harris CL, Esparza-Gordillo J, et al. Gain-of-function mutations in complement factor B are associated with atypical hemolytic uremic syndrome. Proc Natl Acad Sci U S A 2007;104: Sartz L, Olin AI, Kristoffersson AC, et al. A novel C3 mutation causing increased formation of the C3 convertase in familial atypical hemolytic uremic syndrome. J Immunol 2012;188: Richards A, Buddles MR, Donne RL, et al. Factor H mutations in hemolytic uremic syndrome cluster in exons 18-20, a domain important for host cell recognition. Am J Hum Genet 2001;68: Fremeaux-Bacchi V, Moulton EA, Kavanagh D, et al. Genetic and functional analyses of membrane cofactor protein (CD46) mutations in atypical hemolytic uremic syndrome. J Am Soc Nephrol 2006;17: Zipfel PF, Edey M, Heinen S, et al. Deletion of complement factor H-related genes CFHR1 and CFHR3 is associated with atypical hemolytic uremic syndrome. PLoS Genet 2007;3:e41 20
22 17. Rooijakkers SH, Wu J, Ruyken M, et al. Structural and functional implications of the alternative complement pathway C3 convertase stabilized by a staphylococcal inhibitor. Nat Immunol 2009;10: Roumenina LT, Jablonski M, Hue C, et al. Hyperfunctional C3 convertase leads to complement deposition on endothelial cells and contributes to atypical hemolytic uremic syndrome. Blood 2009;114: Frimat M, Tabarin F, Dimitrov JD, et al. Complement activation by heme as a secondary hit for atypical hemolytic uremic syndrome. Blood 2013: in press 20. Roumenina LT, Frimat M, Miller EC, et al. A prevalent C3 mutation in ahus patients causes a direct C3 convertase gain of function. Blood 2012;119: Nilsson SC, Karpman D, Vaziri-Sani F, et al. A mutation in factor I that is associated with atypical hemolytic uremic syndrome does not affect the function of factor I in complement regulation. Mol Immunol 2007;44: Kavanagh D, Richards A, Noris M, et al. Characterization of mutations in complement factor I (CFI) associated with hemolytic uremic syndrome. Mol Immunol 2008;45: Montes T, Tortajada A, Morgan BP, et al. Functional basis of protection against age-related macular degeneration conferred by a common polymorphism in complement factor B. Proc Natl Acad Sci U S A 2009;106: Gulleroglu K, Fidan K, Hancer VS, et al. Neurologic involvement in atypical hemolytic uremic syndrome and successful treatment with eculizumab. Pediatr Nephrol 2013;28:
23 25. Tortajada A, Pinto S, Martinez-Ara J, et al. Complement factor H variants I890 and L1007 while commonly associated with atypical hemolytic uremic syndrome are polymorphisms with no functional significance. Kidney Int 2012;81: Shroff R, Weaver DJ, Jr., Mitsnefes MM. Cardiovascular complications in children with chronic kidney disease. Nat Rev Nephrol 2011;7: Brady TM, Schneider MF, Flynn JT, et al. Carotid intima-media thickness in children with CKD: results from the CKiD study. Clin J Am Soc Nephrol 2012;7: Rinat C, Becker-Cohen R, Nir A, et al. A comprehensive study of cardiovascular risk factors, cardiac function and vascular disease in children with chronic renal failure. Nephrol Dial Transplant 2010;25: Sharma AP, Greenberg CR, Prasad AN, et al. Hemolytic uremic syndrome (HUS) secondary to cobalamin C (cblc) disorder. Pediatr Nephrol 2007;22: Nilsson B, Ekdahl KN, Mollnes TE, et al. The role of complement in biomaterialinduced inflammation. Mol Immunol 2007;44: Andersson J, Ekdahl KN, Larsson R, et al. C3 adsorbed to a polymer surface can form an initiating alternative pathway convertase. J Immunol 2002;168: Nilsson B, Nilsson Ekdahl K. The tick-over theory revisited: is C3 a contactactivated protein? Immunobiology 2012;217: Davin JC, Majoie C, Groothoff J, et al. Prevention of large-vessel stenoses in atypical hemolytic uremic syndrome associated with complement dysregulation. Pediatr Nephrol 2011;26: Vergouwen MD, Adriani KS, Roos YB, et al. Proximal cerebral artery stenosis in a patient with hemolytic uremic syndrome. AJNR Am J Neuroradiol 2008;29:e34 22
24 35. Speidl WS, Kastl SP, Huber K, et al. Complement in atherosclerosis: friend or foe? J Thromb Haemost 2011;9: Nayir A, Bilge I, Kilicaslan I, et al. Arterial changes in paediatric haemodialysis patients undergoing renal transplantation. Nephrol Dial Transplant 2001;16:
25 Table 1: Complement levels in the patient and her parents Complement assay During HD Patient During (reference value) At dialysis presentation 2002 Mother Father During dialysis After 2 nd on transplant on before eculizumab eculizumab eculizumab C3 ( g /L) c c, C3dg (< 5 mg/l) Quantitative complement function via the alternative pathway a ( %) Factor H ( %) Factor I ( %) , <1 < , Factor B ( % 44, 60 % 118 % 90 % 59 % or mg/l) b mg/l HD: hemodialysis. a, Assayed by ELISA (Wieslab, Euro Diagnostica, Malmö Sweden). b, Factor B analyzed in Lund is given in %, and in Paris given in mg/l. c, These values were obtained within 6 weeks after removal of the transplant (on HD) or after transplantation.
26 Table 2: Genetic work-up of the patient Complement factor Genetic analysis Inheritance CFI G261D (Gly261Asp), c.782g>a, exon 6 mutation [21] Paternal CFB L433S (Leu433Ser), c. 1298T>C, exon 10 mutation E566A (Glu433Ala), exon 13, rare polymorphism R7 Arg exon 2, polymorphism Paternal CFH H3 haplotype (tgtgt) [20] Maternal 25
27 Legends to figures Figure 1. Imaging of the brain, cerebral and carotid vasculature. A-C: Magnetic resonance imaging and angiography MR/MRA at the time of the transient ischemic attack (TIA). A) MR, T2-Flair imaging showing an old infarct in the frontal corona radiate area of the left hemisphere (arrow) and two small subcortical vascular lesions (arrowheads). MRA frontal (B) and lateral (C) projection illustrates a tight stenosis of the left internal carotid artery ICA (thick arrow). The large right posterior communicating artery (PComA) supplying the right hemisphere (arrow) is visible. The right internal carotid artery (ICA) is occluded and therefore not visible. D-F: Digital subtraction angiography DSA at time of TIA presentation. D) Injection via the right common carotid artery (CCA) exhibits good filling of the external carotid artery and occlusion of ICA at the level of the dural entrance (arrow). E) Injection via the left CCA exhibited moderate stenosis of the left ICA at the dural level (arrow). No filling of the anterior cerebral arteries was noted. F) Injection via the left vertebral artery demonstrated good collateral filling to the right anterior circulation from the right PComA (arrow). A pial vascular network was established giving retrograde supply to parieto-occipital and deep vessels (arrowheads). G-I: MR and MRA carried out 16 months after TIA presentation and 6 months after renal transplantation. G) T2- Flair imaging did not exhibit new lesions. The previously noted infarct (arrow) and small vascular lesions (arrowhead) were unchanged. In this image only the right-sided lesion is demonstrated. H-I, MRA of the right ICA that was still occluded (not visible) demonstrating the stenosis of the left ICA (thick arrow) with no progression. The arrow points to the agenesis of the left ACA (this is a normal variant), and to both pericallosal arteries (arrowhead) that are supplied from the right side.
28 Figure 2. Characterization of the factor B mutation. A) The position of the ahus CFB mutations in proximity to the MIDAS and C3b binding region. C3b is presented in surface, CFB in cartoon. The residues affected by the ahusassociated mutation presented here, L433S, as well as the previously published CFB mutations in this region D279G, F286L and K350N [12, 18] (are indicated by dark spheres). B) The secretion level of the L433S mutant compared to the wild-type (WT) CFB, SN0 (supernatant from mock-transfected cells as the negative control) and D279G (positive control), as analysed by ELISA. Results are presented as % of the wild-type in mean ± SD of three independent experiments. C) C3b binding tested by ELISA. The interaction of wild-type or mutant CFB to plate-coated C3b was measured by ELISA. The results are presented as % of the binding of the wild-type in the plateau of the dose response curve, mean ± SD from 5 different experiments. D) C3b binding tested by SPR. The interaction of biosensor chipimmobilized C3b with CFB as an analyte was studied in real time. One representative sensorogram out of 3 independent experiments is presented. E) C3 deposition on cytokineactivated HUVECs in CFB-depleted serum reconstituted with recombinant wild-type CFB, L433S or D279G mutants evaluated by flow cytometry. The results are presented as fold difference of the relative fluorescence intensity (RFI) of the C3 deposition in the presence of a mutant CFB, compared to the wild-type (mean ± SD from 3 experiments) F). Cytokineactivated HUVECs were incubated with sera from 55 normal donors, CFH-depleted serum (as a positive control), and serum from the patient s parents, and tested for C3 deposition by flow cytometry. The results are expressed as RFI. The normal range was determined as the average of the C3 deposition from the normal donors ± 2SD, depicted as the horizontal dashed bar. Patient serum had low C3 and CFB levels and could not be used in this test, as it requires normal C3 and CFB levels. 27
29
30
M.Weitz has documented that he has no relevant financial relationships to disclose or conflict of interest to resolve.
 M.Weitz has documented that he has no relevant financial relationships to disclose or conflict of interest to resolve. Prophylactic eculizumab prior to kidney transplantation for atypical hemolytic uremic
M.Weitz has documented that he has no relevant financial relationships to disclose or conflict of interest to resolve. Prophylactic eculizumab prior to kidney transplantation for atypical hemolytic uremic
New insights in thrombotic microangiopathies : TTP and ahus
 New insights in thrombotic microangiopathies : TTP and ahus Dr Catherine LAMBERT Hematology Cliniques universitaires Saint-Luc Catherine.lambert@uclouvain.be New insights in thrombotic microangiopathies
New insights in thrombotic microangiopathies : TTP and ahus Dr Catherine LAMBERT Hematology Cliniques universitaires Saint-Luc Catherine.lambert@uclouvain.be New insights in thrombotic microangiopathies
Acquired Drivers of Disaese ahus and autoantibodies: their role in disease and their impact on patient management
 Acquired Drivers of Disaese ahus and autoantibodies: their role in disease and their impact on patient management Veronique Fremeaux-Bacchi Cordeliers Research Center and Européen Georges Pompidou Hospital,
Acquired Drivers of Disaese ahus and autoantibodies: their role in disease and their impact on patient management Veronique Fremeaux-Bacchi Cordeliers Research Center and Européen Georges Pompidou Hospital,
Recent advances in pathogenesis & treatment of ahus
 Recent advances in pathogenesis & treatment of ahus Miquel Blasco Pelicano Nephrology and Kidney Transplant Unit Hospital Clínic, Barcelona Atypical Hemolytic Uremic Syndrome (ahus) Ultra-rare disease:
Recent advances in pathogenesis & treatment of ahus Miquel Blasco Pelicano Nephrology and Kidney Transplant Unit Hospital Clínic, Barcelona Atypical Hemolytic Uremic Syndrome (ahus) Ultra-rare disease:
Safety and Efficacy of Eculizumab in Pediatric Patients With ahus, With or Without Baseline Dialysis
 SP281 Safety and Efficacy of Eculizumab in Pediatric Patients With ahus, With or Without Baseline Johan Vande Walle, 1 Larry A. Greenbaum, 2 Camille L. Bedrosian, 3 Masayo Ogawa, 3 John F. Kincaid, 3 Chantal
SP281 Safety and Efficacy of Eculizumab in Pediatric Patients With ahus, With or Without Baseline Johan Vande Walle, 1 Larry A. Greenbaum, 2 Camille L. Bedrosian, 3 Masayo Ogawa, 3 John F. Kincaid, 3 Chantal
Safety and Efficacy of Eculizumab in Pediatric Patients With ahus, With or Without Baseline Dialysis
 SA-PO546 Safety and Efficacy of Eculizumab in Pediatric Patients With ahus, With or Without Baseline Johan Vande Walle, 1 Larry A. Greenbaum, 2 Camille L. Bedrosian, 3 Masayo Ogawa, 3 John F. Kincaid,
SA-PO546 Safety and Efficacy of Eculizumab in Pediatric Patients With ahus, With or Without Baseline Johan Vande Walle, 1 Larry A. Greenbaum, 2 Camille L. Bedrosian, 3 Masayo Ogawa, 3 John F. Kincaid,
Atypical Hemolytic Uremic Syndrome: When the Environment and Mutations Affect Organ Systems. A Case Report with Review of Literature
 Atypical Hemolytic Uremic Syndrome: When the Environment and Mutations Affect Organ Systems. A Case Report with Review of Literature Mouhanna Abu Ghanimeh 1, Omar Abughanimeh 1, Ayman Qasrawi 1, Abdulraheem
Atypical Hemolytic Uremic Syndrome: When the Environment and Mutations Affect Organ Systems. A Case Report with Review of Literature Mouhanna Abu Ghanimeh 1, Omar Abughanimeh 1, Ayman Qasrawi 1, Abdulraheem
Risk factors of chronic renal failure after atypical Hemolytic Uremic Syndrome under plasmatherapy
 Risk factors of chronic renal failure after atypical Hemolytic Uremic Syndrome under plasmatherapy Professeur Eric Rondeau Urgences néphrologiques et Transplantation rénale Hôpital Tenon, Paris WWA SFH
Risk factors of chronic renal failure after atypical Hemolytic Uremic Syndrome under plasmatherapy Professeur Eric Rondeau Urgences néphrologiques et Transplantation rénale Hôpital Tenon, Paris WWA SFH
C3 Glomerulopathy. Jun-Ki Park
 C3 Glomerulopathy Jun-Ki Park 03.08.11 For the last 30 years classification MPGN is based on glomerular findings by light microscopy with further specification on EM and staining for Ig and complement
C3 Glomerulopathy Jun-Ki Park 03.08.11 For the last 30 years classification MPGN is based on glomerular findings by light microscopy with further specification on EM and staining for Ig and complement
DRUG NAME: Eculizumab Brand(s): Soliris DOSAGE FORM/ STRENGTH: 10 mg/ml (300 mg per vial)
: Soliris DOSAGE FORM/ STRENGTH: 10 mg/ml (300 mg per vial)") Preamble: A confirmed diagnosis of atypical hemolytic uremic syndrome (ahus) is required for eculizumab funding. The information below is to provide clinicians with context for how a diagnosis of ahus
Preamble: A confirmed diagnosis of atypical hemolytic uremic syndrome (ahus) is required for eculizumab funding. The information below is to provide clinicians with context for how a diagnosis of ahus
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Lapeyraque A-L, Malina M, Fremeaux-Bacchi V, et al. Eculizumab
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Lapeyraque A-L, Malina M, Fremeaux-Bacchi V, et al. Eculizumab
ahus A PATIENT S GUIDE To learn more about ahus, visit Copyright 2011, Alexion Pharmaceuticals, Inc. All rights reserved.
 To learn more about ahus, visit www.ahussource.com ahus A PATIENT S GUIDE Copyright 2011, Alexion Pharmaceuticals, Inc. All rights reserved. SOL 1169 BECOME EMPOWERED By learning more and taking control
To learn more about ahus, visit www.ahussource.com ahus A PATIENT S GUIDE Copyright 2011, Alexion Pharmaceuticals, Inc. All rights reserved. SOL 1169 BECOME EMPOWERED By learning more and taking control
TMA CASE STUDY. Pamela Harmon, RN & Keturah Tomlin, RN Toronto General Hospital Apheresis Unit
 TMA CASE STUDY Pamela Harmon, RN & Keturah Tomlin, RN Toronto General Hospital Apheresis Unit Cumulative fraction of patients free of events ahus is a catastrophic disease that can result in sudden & progressive
TMA CASE STUDY Pamela Harmon, RN & Keturah Tomlin, RN Toronto General Hospital Apheresis Unit Cumulative fraction of patients free of events ahus is a catastrophic disease that can result in sudden & progressive
Thrombocytopenia is not mandatory to diagnose haemolytic and uremic syndrome
 Sallée et al. BMC Nephrology 2013, 14:3 RESEARCH ARTICLE Open Access Thrombocytopenia is not mandatory to diagnose haemolytic and uremic syndrome Marion Sallée 1, Khalil Ismail 1, Fadi Fakhouri 2, Henri
Sallée et al. BMC Nephrology 2013, 14:3 RESEARCH ARTICLE Open Access Thrombocytopenia is not mandatory to diagnose haemolytic and uremic syndrome Marion Sallée 1, Khalil Ismail 1, Fadi Fakhouri 2, Henri
Spectrum of complement-mediated thrombotic microangiopathies after kidney transplantation
 Spectrum of complement-mediated thrombotic microangiopathies after kidney transplantation Marius Miglinas Vilnius university hospital: Nephrology center, Center of Rare Kidney Diseases Vilnius university
Spectrum of complement-mediated thrombotic microangiopathies after kidney transplantation Marius Miglinas Vilnius university hospital: Nephrology center, Center of Rare Kidney Diseases Vilnius university
R. Coward has documented that he has received cooperative grants from Takeda and Novo Nordisk
 R. Coward has documented that he has received cooperative grants from Takeda and Novo Nordisk Advances in our understanding of the pathogenesis of glomerular thrombotic microangiopathy Lindsay Keir Richard
R. Coward has documented that he has received cooperative grants from Takeda and Novo Nordisk Advances in our understanding of the pathogenesis of glomerular thrombotic microangiopathy Lindsay Keir Richard
When a patient presents with TMA, identify the underlying cause for the appropriate diagnosis... IS IT TTP OR IS IT ahus?
 When a patient presents with TMA, identify the underlying cause for the appropriate diagnosis... IS IT TTP OR IS IT ahus? ADAMTS13 activity >5% RULES OUT a diagnosis of severe ADAMTS13 deficiency (TTP)
When a patient presents with TMA, identify the underlying cause for the appropriate diagnosis... IS IT TTP OR IS IT ahus? ADAMTS13 activity >5% RULES OUT a diagnosis of severe ADAMTS13 deficiency (TTP)
TMA in HUS and TTP: new insights
 TMA in HUS and TTP: new insights Daan Dierickx University Hospitals Leuven, Department of Hematology, Belgium 20th Annual Meeting Belgian Society on Thrombosis and Haemostatis Antwerpen, 22 th November
TMA in HUS and TTP: new insights Daan Dierickx University Hospitals Leuven, Department of Hematology, Belgium 20th Annual Meeting Belgian Society on Thrombosis and Haemostatis Antwerpen, 22 th November
Beyond Plasma Exchange: Targeted Therapy for Thrombotic Thrombocytopenic Purpura
 Beyond Plasma Exchange: Targeted Therapy for Thrombotic Thrombocytopenic Purpura Kristen Knoph, PharmD, BCPS PGY2 Pharmacotherapy Resident Pharmacy Grand Rounds April 25, 2017 2016 MFMER slide-1 Objectives
Beyond Plasma Exchange: Targeted Therapy for Thrombotic Thrombocytopenic Purpura Kristen Knoph, PharmD, BCPS PGY2 Pharmacotherapy Resident Pharmacy Grand Rounds April 25, 2017 2016 MFMER slide-1 Objectives
Hemolytic uremic syndrome: Investigations and management
 Hemolytic uremic syndrome: Investigations and management SAWAI Toshihiro M.D., Ph.D. Department of Pediatrics, Shiga University of Medical Science Otsu, JAPAN AGENDA TMA; Thrombotic micro angiopathy STEC-HUS;
Hemolytic uremic syndrome: Investigations and management SAWAI Toshihiro M.D., Ph.D. Department of Pediatrics, Shiga University of Medical Science Otsu, JAPAN AGENDA TMA; Thrombotic micro angiopathy STEC-HUS;
Atypical hemolytic uremic syndrome. Diana Karpman Department of Pediatrics Lund University
 Atypical hemolytic uremic syndrome Diana Karpman Department of Pediatrics Lund University Image courtesy of Dr. Sabine Leh, Haukeland University Hospital, Bergen Norway Hemolytic Uremic Syndrome Non-immune
Atypical hemolytic uremic syndrome Diana Karpman Department of Pediatrics Lund University Image courtesy of Dr. Sabine Leh, Haukeland University Hospital, Bergen Norway Hemolytic Uremic Syndrome Non-immune
Accepted Manuscript. No more thrombotic thrombocytopenic purpura/hemolytic uremic syndrome please. Yeong-Hau H. Lien MD, PhD S (18)
") Accepted Manuscript No more thrombotic thrombocytopenic purpura/hemolytic uremic syndrome please Yeong-Hau H. Lien MD, PhD PII: S0002-9343(18)30965-3 DOI: https://doi.org/10.1016/j.amjmed.2018.10.009 Reference:
Accepted Manuscript No more thrombotic thrombocytopenic purpura/hemolytic uremic syndrome please Yeong-Hau H. Lien MD, PhD PII: S0002-9343(18)30965-3 DOI: https://doi.org/10.1016/j.amjmed.2018.10.009 Reference:
C3 Glomerulonephritis versus C3 Glomerulopathies?
 Washington University School of Medicine Digital Commons@Becker Kidneycentric Kidneycentric 2016 C3 Glomerulonephritis versus C3 Glomerulopathies? T. Keefe Davis Washington University School of Medicine
Washington University School of Medicine Digital Commons@Becker Kidneycentric Kidneycentric 2016 C3 Glomerulonephritis versus C3 Glomerulopathies? T. Keefe Davis Washington University School of Medicine
Eculizumab as Prophylactic Therapy in Atypical Hemolytic Uremic Syndrome in Adult Living-Related Kidney Transplantation
 Anti-C5 as Prophylactic Therapy in Atypical Hemolytic Uremic Syndrome in Living- Related Kidney Transplantation Authors: Miquel Blasco 1, Santiago Rodríguez de Córdoba 2, Fritz Diekmann 1, Mercedes Saiz
Anti-C5 as Prophylactic Therapy in Atypical Hemolytic Uremic Syndrome in Living- Related Kidney Transplantation Authors: Miquel Blasco 1, Santiago Rodríguez de Córdoba 2, Fritz Diekmann 1, Mercedes Saiz
Soliris and You. Your Guide To Living With ahus. INDICATION & IMPORTANT SAFETY INFORMATION FOR SOLIRIS (eculizumab)
") INDICATION & IMPORTANT SAFETY INFORMATION FOR SOLIRIS (eculizumab) INDICATION What is SOLIRIS? SOLIRIS is a prescription medicine called a monoclonal antibody. SOLIRIS is used to treat: adults and children
INDICATION & IMPORTANT SAFETY INFORMATION FOR SOLIRIS (eculizumab) INDICATION What is SOLIRIS? SOLIRIS is a prescription medicine called a monoclonal antibody. SOLIRIS is used to treat: adults and children
Recurrence of C3G after renal transplantation. Moglie Le Quintrec Service de Néphrologie, Hôpital Foch CRC, UMRS 1138, Equipe complement and diseases
 Recurrence of C3G after renal transplantation Moglie Le Quintrec Service de Néphrologie, Hôpital Foch CRC, UMRS 1138, Equipe complement and diseases New MPGN classification C3G MPGN I DDD C3GN IF C3 deposits
Recurrence of C3G after renal transplantation Moglie Le Quintrec Service de Néphrologie, Hôpital Foch CRC, UMRS 1138, Equipe complement and diseases New MPGN classification C3G MPGN I DDD C3GN IF C3 deposits
Specialised Services Policy: CP98 Eculizumab for Atypical Haemolytic Uraemic Syndrome (ahus)
") Specialised Services Policy: CP98 Eculizumab for Atypical Haemolytic Uraemic Syndrome (ahus) Document Author: Assistant Director for Evidence, Evaluation and Effectiveness Executive Lead: Medical Director
Specialised Services Policy: CP98 Eculizumab for Atypical Haemolytic Uraemic Syndrome (ahus) Document Author: Assistant Director for Evidence, Evaluation and Effectiveness Executive Lead: Medical Director
Familial DDD associated with a gain-of-function mutation in complement C3.
 Familial DDD associated with a gain-of-function mutation in complement C3. Santiago Rodríguez de Córdoba, Centro de investigaciones Biológicas, Madrid Valdés Cañedo F. and Vázquez- Martul E., Complejo
Familial DDD associated with a gain-of-function mutation in complement C3. Santiago Rodríguez de Córdoba, Centro de investigaciones Biológicas, Madrid Valdés Cañedo F. and Vázquez- Martul E., Complejo
Clinical Study Eculizumab Therapy Leads to Rapid Resolution of Thrombocytopenia in Atypical Hemolytic Uremic Syndrome
 Hindawi Publishing Corporation Advances in Hematology Volume 214, Article ID 295323, 7 pages http://dx.doi.org/1.1155/214/295323 Clinical Study Therapy Leads to Rapid Resolution of Thrombocytopenia in
Hindawi Publishing Corporation Advances in Hematology Volume 214, Article ID 295323, 7 pages http://dx.doi.org/1.1155/214/295323 Clinical Study Therapy Leads to Rapid Resolution of Thrombocytopenia in
What is meant by Thrombotic Microangiopathy (TMA)?
?") What is meant by Thrombotic Microangiopathy (TMA)? Thrombotic Microangiopathy (TMA) is a group of disorders characterized by injured endothelial cells, microangiopathic hemolytic anemia (MAHA), with its
What is meant by Thrombotic Microangiopathy (TMA)? Thrombotic Microangiopathy (TMA) is a group of disorders characterized by injured endothelial cells, microangiopathic hemolytic anemia (MAHA), with its
THE MULTIPLE FACETS OF THROMBOTIC MICROANGIOPATHIES
 THE MULTIPLE FACETS OF THROMBOTIC MICROANGIOPATHIES Summary of Presentations from the Alexion-Sponsored Symposium, held at the 19 th EHA Congress, Milan, Italy, on 12 th June 2014 Chairperson Pier Mannuccio
THE MULTIPLE FACETS OF THROMBOTIC MICROANGIOPATHIES Summary of Presentations from the Alexion-Sponsored Symposium, held at the 19 th EHA Congress, Milan, Italy, on 12 th June 2014 Chairperson Pier Mannuccio
Pathology of Complement Mediated Renal Disease
 Pathology of Complement Mediated Renal Disease Mariam Priya Alexander, MD Associate Professor of Pathology GN Symposium Hong Kong Society of Nephrology July 8 th, 2017 2017 MFMER slide-1 The complement
Pathology of Complement Mediated Renal Disease Mariam Priya Alexander, MD Associate Professor of Pathology GN Symposium Hong Kong Society of Nephrology July 8 th, 2017 2017 MFMER slide-1 The complement
Hemolytic uremic syndrome
 Hemolytic uremic syndrome Doyeun Oh Department of Internal Medicine CHA University School of Medicine Disclosures for Doyeun Oh Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau
Hemolytic uremic syndrome Doyeun Oh Department of Internal Medicine CHA University School of Medicine Disclosures for Doyeun Oh Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau
FLT3 mutations in patients with childhood acute lymphoblastic leukemia (ALL)
") FLT3 mutations in patients with childhood acute lymphoblastic leukemia (ALL) Kabir, Nuzhat N.; Rönnstrand, Lars; Uddin, Kazi Published in: Medical Oncology DOI: 10.1007/s12032-013-0462-6 Published: 2013-01-01
FLT3 mutations in patients with childhood acute lymphoblastic leukemia (ALL) Kabir, Nuzhat N.; Rönnstrand, Lars; Uddin, Kazi Published in: Medical Oncology DOI: 10.1007/s12032-013-0462-6 Published: 2013-01-01
Novel aspects of atypical haemolytic uraemic syndrome and the role of eculizumab
 Nephrol Dial Transplant (2014) 29: iv131 iv141 doi: 10.1093/ndt/gfu235 Full Review Novel aspects of atypical haemolytic uraemic syndrome and the role of eculizumab Jacobien C. Verhave 1, Jack F.M. Wetzels
Nephrol Dial Transplant (2014) 29: iv131 iv141 doi: 10.1093/ndt/gfu235 Full Review Novel aspects of atypical haemolytic uraemic syndrome and the role of eculizumab Jacobien C. Verhave 1, Jack F.M. Wetzels
THROMBOTIC MICROANGIOPATHY. Jun-Ki Park 7/19/11
 THROMBOTIC MICROANGIOPATHY Jun-Ki Park 7/19/11 TMAs are microvascular occlusive disorders characterized by systemic or intrarenal aggregation of platelets, thrombocytopenia, and mechanical injury to erythrocytes.
THROMBOTIC MICROANGIOPATHY Jun-Ki Park 7/19/11 TMAs are microvascular occlusive disorders characterized by systemic or intrarenal aggregation of platelets, thrombocytopenia, and mechanical injury to erythrocytes.
Thrombotic Microangiopathies (TMA) / TTP/HUS/αHUS Pathology & Molecular. Genetics
 / TTP/HUS/αHUS Pathology & Molecular. Genetics") Thrombotic Microangiopathies (TMA) / TTP/HUS/αHUS Pathology & Molecular Genetics Helen Liapis, M.D. Senior Consultant Arkana Labs Professor of Pathology & Immunology. retired Washington University School
Thrombotic Microangiopathies (TMA) / TTP/HUS/αHUS Pathology & Molecular Genetics Helen Liapis, M.D. Senior Consultant Arkana Labs Professor of Pathology & Immunology. retired Washington University School
Some renal vascular disorders
 Some renal vascular disorders Introduction Nearly all diseases of the kidney involve the renal blood vessels secondarily We will discuss: -Hypertension (arterionephrosclerosis in benign HTN & hyperplastic
Some renal vascular disorders Introduction Nearly all diseases of the kidney involve the renal blood vessels secondarily We will discuss: -Hypertension (arterionephrosclerosis in benign HTN & hyperplastic
Hemolytic Uremic Syndrome
 Hemolytic Uremic Syndrome Francesco Emma Division of Nephrology and Dialysis Bambino Gesù Children s Hospital, IRCCS Rome, Italy Hemolytic Uremic Syndrome (HUS) microangiopathic hemolytic anemia thrombocytopenia
Hemolytic Uremic Syndrome Francesco Emma Division of Nephrology and Dialysis Bambino Gesù Children s Hospital, IRCCS Rome, Italy Hemolytic Uremic Syndrome (HUS) microangiopathic hemolytic anemia thrombocytopenia
Thrombotic Microangiopathy (TMA) The Clinical Facets of TMA
 The Clinical Facets of TMA") International Consensus on Management Atypical Hemolytic Uremic Syndrome in Children Loirat C. et al. Pediatr Nephrol 31: 15-39, 2016 Ruth A. McDonald, MD Professor and Vice Chair Clinical Affairs Department
International Consensus on Management Atypical Hemolytic Uremic Syndrome in Children Loirat C. et al. Pediatr Nephrol 31: 15-39, 2016 Ruth A. McDonald, MD Professor and Vice Chair Clinical Affairs Department
Introduction to pathogenesis and treatment of thrombotic microangiopathies (TMA)
") Introduction to pathogenesis and treatment of thrombotic microangiopathies (TMA) JM.Campistol, Nephrology and Renal Transplant Department, Hospital Clinic, University of Barcelona, Barcelona, Spain. jmcampis@clinic.cat
Introduction to pathogenesis and treatment of thrombotic microangiopathies (TMA) JM.Campistol, Nephrology and Renal Transplant Department, Hospital Clinic, University of Barcelona, Barcelona, Spain. jmcampis@clinic.cat
Can eculizumab be discontinued in ahus? Case report and review of the literature
 Clinical Case Report Medicine Can eculizumab be discontinued in ahus? Case report and review of the literature Tuncay Sahutoglu, MD a,, Taner Basturk, MD a, Tamer Sakaci, MD a, Yener Koc, MD a, Elbis Ahbap,
Clinical Case Report Medicine Can eculizumab be discontinued in ahus? Case report and review of the literature Tuncay Sahutoglu, MD a,, Taner Basturk, MD a, Tamer Sakaci, MD a, Yener Koc, MD a, Elbis Ahbap,
To cite this version: HAL Id: hal
 The high frequency of Complement Factor H-Related CFHR1 Gene Deletion is restricted to specific subgroups of patients with atypical Haemolytic Uraemic Syndrome Marie-Agnès Dragon-Durey, Caroline Blanc,
The high frequency of Complement Factor H-Related CFHR1 Gene Deletion is restricted to specific subgroups of patients with atypical Haemolytic Uraemic Syndrome Marie-Agnès Dragon-Durey, Caroline Blanc,
An international consensus approach to the management of atypical hemolytic uremic syndrome in children
 DOI 10.1007/s00467-015-3076-8 REVIEW An international consensus approach to the management of atypical hemolytic uremic syndrome in children Chantal Loirat & Fadi Fakhouri & Gema Ariceta & Nesrin Besbas
DOI 10.1007/s00467-015-3076-8 REVIEW An international consensus approach to the management of atypical hemolytic uremic syndrome in children Chantal Loirat & Fadi Fakhouri & Gema Ariceta & Nesrin Besbas
Initial management of TMA syndromes
 Initial management of TMA syndromes Elie Azoulay, Saint-Louis Hospital, Medical Intensive Care Unit Paris Diderot Sorbonne University Groupe de Recherche Respiratoire en Réanimation Onco-Hématologique
Initial management of TMA syndromes Elie Azoulay, Saint-Louis Hospital, Medical Intensive Care Unit Paris Diderot Sorbonne University Groupe de Recherche Respiratoire en Réanimation Onco-Hématologique
ECULIZUMAB LONG-TERM THERAPY FOR PEDIATRIC RENAL. Centro de Investigaciones Biológicas - Consejo Superior de Investigaciones
 TITLE PAGE ECULIZUMAB LONG-TERM THERAPY FOR PEDIATRIC RENAL TRANSPLANT IN ahus WITH CFH/CFHR1 HYBRID GENE. Román-Ortiz E a *, Mendizabal Oteiza S a, Pinto S b, López-Trascasa M c, Sánchez- Corral P c and
TITLE PAGE ECULIZUMAB LONG-TERM THERAPY FOR PEDIATRIC RENAL TRANSPLANT IN ahus WITH CFH/CFHR1 HYBRID GENE. Román-Ortiz E a *, Mendizabal Oteiza S a, Pinto S b, López-Trascasa M c, Sánchez- Corral P c and
Soliris (eculizumab) DRUG.00050
 DRUG.00050") Market DC Soliris (eculizumab) DRUG.00050 Override(s) Prior Authorization Approval Duration 1 year Medications Soliris (eculizumab) APPROVAL CRITERIA Paroxysmal Nocturnal Hemoglobinuria I. Initiation of
Market DC Soliris (eculizumab) DRUG.00050 Override(s) Prior Authorization Approval Duration 1 year Medications Soliris (eculizumab) APPROVAL CRITERIA Paroxysmal Nocturnal Hemoglobinuria I. Initiation of
Soliris Medical Policy Prior Authorization Program Summary
 Soliris Medical Policy Prior Authorization Program Summary Precertification/Prior Authorization may be required under certain plans. Please verify each member s benefits. OBJECTIVE The intent of the Soliris
Soliris Medical Policy Prior Authorization Program Summary Precertification/Prior Authorization may be required under certain plans. Please verify each member s benefits. OBJECTIVE The intent of the Soliris
A 60 year old woman with altered mental status and thrombotic microangiopathy. Josh Veatch
 A 60 year old woman with altered mental status and thrombotic microangiopathy Josh Veatch Previously healthy 60 year old woman 2 3 months of fatigue following a URI, transient episodes being out of it
A 60 year old woman with altered mental status and thrombotic microangiopathy Josh Veatch Previously healthy 60 year old woman 2 3 months of fatigue following a URI, transient episodes being out of it
Thrombotic Thrombocytopenic Purpura and the Role of ADAMTS-13
 Thrombotic Thrombocytopenic Purpura and the Role of ADAMTS-13 Mark Cunningham,MD Director, Hematology Laboratory Department of Pathology University of Kansas Medical Center College of American Pathologists
Thrombotic Thrombocytopenic Purpura and the Role of ADAMTS-13 Mark Cunningham,MD Director, Hematology Laboratory Department of Pathology University of Kansas Medical Center College of American Pathologists
Year 2004 Paper one: Questions supplied by Megan
 QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
Complement and the atypical hemolytic uremic syndrome in children
 Pediatr Nephrol (2008) 23:1957 1972 DOI 10.1007/s00467-008-0872-4 EDUCATIONAL REVIEW Complement and the atypical hemolytic uremic syndrome in children Chantal Loirat & Marina Noris & Véronique Fremeaux-Bacchi
Pediatr Nephrol (2008) 23:1957 1972 DOI 10.1007/s00467-008-0872-4 EDUCATIONAL REVIEW Complement and the atypical hemolytic uremic syndrome in children Chantal Loirat & Marina Noris & Véronique Fremeaux-Bacchi
Challenges in Renal Apheresis. Mark E. Williams MD, FACP, FASN Director, Renal Apheresis Beth Israel Deaconess Medical Center Harvard Medical School
 Challenges in Renal Apheresis Mark E. Williams MD, FACP, FASN Director, Renal Apheresis Beth Israel Deaconess Medical Center Harvard Medical School Outline Principles of Separation ASFA Guidelines Renal
Challenges in Renal Apheresis Mark E. Williams MD, FACP, FASN Director, Renal Apheresis Beth Israel Deaconess Medical Center Harvard Medical School Outline Principles of Separation ASFA Guidelines Renal
Current evidence on the discontinuation of eculizumab in patients with atypical haemolytic uraemic syndrome
 Clinical Kidney Journal, 2016, 1 10 doi: 10.1093/ckj/sfw115 Original Article ORIGINAL ARTICLE Current evidence on the discontinuation of eculizumab in patients with atypical haemolytic uraemic syndrome
Clinical Kidney Journal, 2016, 1 10 doi: 10.1093/ckj/sfw115 Original Article ORIGINAL ARTICLE Current evidence on the discontinuation of eculizumab in patients with atypical haemolytic uraemic syndrome
Medical Review Guidelines Magnetic Resonance Angiography
 Medical Review Guidelines Magnetic Resonance Angiography Medical Guideline Number: MRG2001-05 Effective Date: 2/13/01 Revised Date: 2/14/2006 OHCA Reference OAC 317:30-5-24. Radiology. (f) Magnetic Resonance
Medical Review Guidelines Magnetic Resonance Angiography Medical Guideline Number: MRG2001-05 Effective Date: 2/13/01 Revised Date: 2/14/2006 OHCA Reference OAC 317:30-5-24. Radiology. (f) Magnetic Resonance
A PATIENT S JOURNEY. Learning about atypical hemolytic uremic syndrome (ahus)
") A PATIENT S JOURNEY Learning about atypical hemolytic uremic syndrome (ahus) Begin your path to empowerment Being diagnosed with ahus can be overwhelming. You may have many questions: What is ahus? How
A PATIENT S JOURNEY Learning about atypical hemolytic uremic syndrome (ahus) Begin your path to empowerment Being diagnosed with ahus can be overwhelming. You may have many questions: What is ahus? How
Atypical hemolytic uremic syndrome (ahus) is a progressive
 is a progressive") www.kidney-international.org Eculizumab is a safe and effective treatment in pediatric patients with atypical hemolytic uremic syndrome OPEN Larry A. Greenbaum 1, Marc Fila 2, Gianluigi Ardissino 3, Samhar
www.kidney-international.org Eculizumab is a safe and effective treatment in pediatric patients with atypical hemolytic uremic syndrome OPEN Larry A. Greenbaum 1, Marc Fila 2, Gianluigi Ardissino 3, Samhar
Untying the Knot of Thrombotic Thrombocytopenic Purpura and Atypical Hemolytic Uremic Syndrome
 REVIEW Untying the Knot of Thrombotic Thrombocytopenic Purpura and Atypical Hemolytic Uremic Syndrome Han-Mou Tsai, MD imah Hematology Associates, New Hyde Park, NY. ABSTRACT Patients presenting with microangiopathic
REVIEW Untying the Knot of Thrombotic Thrombocytopenic Purpura and Atypical Hemolytic Uremic Syndrome Han-Mou Tsai, MD imah Hematology Associates, New Hyde Park, NY. ABSTRACT Patients presenting with microangiopathic
C3 GLOMERULOPATHIES. Budapest Nephrology School Zoltan Laszik
 C3 GLOMERULOPATHIES Budapest Nephrology School 8.30.2018. Zoltan Laszik 1 Learning Objectives Familiarize with the pathogenetic mechanisms of glomerular diseases Learn the pathologic landscape and clinical
C3 GLOMERULOPATHIES Budapest Nephrology School 8.30.2018. Zoltan Laszik 1 Learning Objectives Familiarize with the pathogenetic mechanisms of glomerular diseases Learn the pathologic landscape and clinical
HUS and TTP Testing. Kenneth D. Friedman, M.D. Director, Hemostasis Reference Lab BloodCenter of Wisconsin, Milwaukee WI
 HUS and TTP Testing Kenneth D. Friedman, M.D. Director, Hemostasis Reference Lab BloodCenter of Wisconsin, Milwaukee WI Disclosures Relevant Financial Relationships Consultant: Ablynx, Bayer, CSL Behring,
HUS and TTP Testing Kenneth D. Friedman, M.D. Director, Hemostasis Reference Lab BloodCenter of Wisconsin, Milwaukee WI Disclosures Relevant Financial Relationships Consultant: Ablynx, Bayer, CSL Behring,
ahus: recent insights and management
 ahus: recent insights and management Steven Van Laecke MD, PhD Renal Division, Ghent University Hospital, Belgium 13 th BANTAO Sarajevo October 8 2017 The complement is everywhere I could benefit from
ahus: recent insights and management Steven Van Laecke MD, PhD Renal Division, Ghent University Hospital, Belgium 13 th BANTAO Sarajevo October 8 2017 The complement is everywhere I could benefit from
Two Patients With History of STEC-HUS, Posttransplant Recurrence and Complement Gene Mutations
 American Journal of Transplantation 2013; 13: 2201 2206 Wiley Periodicals Inc. Case Report C Copyright 2013 The American Society of Transplantation and the American Society of Transplant Surgeons doi:
American Journal of Transplantation 2013; 13: 2201 2206 Wiley Periodicals Inc. Case Report C Copyright 2013 The American Society of Transplantation and the American Society of Transplant Surgeons doi:
Soliris (eculizumab) Inhibits TMA and Improves Renal Function in Pediatric and Adult Patients with atypical Hemolytic Uremic Syndrome (ahus)
 Inhibits TMA and Improves Renal Function in Pediatric and Adult Patients with atypical Hemolytic Uremic Syndrome (ahus)") Soliris (eculizumab) Inhibits TMA and Improves Renal Function in Pediatric and Adult Patients with atypical Hemolytic Uremic Syndrome (ahus) New Data from the Largest Prospective Trial of Adult Patients
Soliris (eculizumab) Inhibits TMA and Improves Renal Function in Pediatric and Adult Patients with atypical Hemolytic Uremic Syndrome (ahus) New Data from the Largest Prospective Trial of Adult Patients
HEME 10 Bleeding Disorders
 HEME 10 Bleeding Disorders When injury occurs, three mechanisms occur Blood vessels Primary hemostasis Secondary hemostasis Diseases of the blood vessels Platelet disorders Thrombocytopenia Functional
HEME 10 Bleeding Disorders When injury occurs, three mechanisms occur Blood vessels Primary hemostasis Secondary hemostasis Diseases of the blood vessels Platelet disorders Thrombocytopenia Functional
Fibromuscular Dysplasia (FMD) of the renal arteries Angiographic features and therapeutic options
 of the renal arteries Angiographic features and therapeutic options") Fibromuscular Dysplasia (FMD) of the renal arteries Angiographic features and therapeutic options Poster No.: C-0630 Congress: ECR 2012 Type: Educational Exhibit Authors: K. I. Ringe, B. Meyer, F. Wacker,
Fibromuscular Dysplasia (FMD) of the renal arteries Angiographic features and therapeutic options Poster No.: C-0630 Congress: ECR 2012 Type: Educational Exhibit Authors: K. I. Ringe, B. Meyer, F. Wacker,
A CAREGIVER S JOURNEY
 A CAREGIVER S JOURNEY Learning about atypical hemolytic uremic syndrome (ahus) Begin your path to effective advocacy and support Caring for someone who is diagnosed with ahus can be overwhelming. You may
A CAREGIVER S JOURNEY Learning about atypical hemolytic uremic syndrome (ahus) Begin your path to effective advocacy and support Caring for someone who is diagnosed with ahus can be overwhelming. You may
Genetics of Atypical Hemolytic Uremic Syndrome (ahus)
") Genetics of Atypical Hemolytic Uremic Syndrome (ahus) Santiago Rodríguez de Córdoba, PhD 1 Marta Subías Hidalgo, MSc 1 Sheila Pinto, BTec 1 Agustín Tortajada, PhD 1 1 Centro de Investigaciones Biológicas,
Genetics of Atypical Hemolytic Uremic Syndrome (ahus) Santiago Rodríguez de Córdoba, PhD 1 Marta Subías Hidalgo, MSc 1 Sheila Pinto, BTec 1 Agustín Tortajada, PhD 1 1 Centro de Investigaciones Biológicas,
Medical Policy. MP Eculizumab (Soliris) Related Policies None. Last Review: 01/24/2019 Effective Date: 04/25/2019 Section: Prescription Drug
 Related Policies None. Last Review: 01/24/2019 Effective Date: 04/25/2019 Section: Prescription Drug") Medical Policy Last Review: 01/24/2019 Effective Date: 04/25/2019 Section: Prescription Drug Related Policies None DISCLAIMER Our medical policies are designed for informational purposes only and are not
Medical Policy Last Review: 01/24/2019 Effective Date: 04/25/2019 Section: Prescription Drug Related Policies None DISCLAIMER Our medical policies are designed for informational purposes only and are not
A 23 year old Caucasian male presented with shortness of breath, hypertension, bloody sputum, and a history of drug abuse (confirmed by urinalysis).
.") A 23 year old Caucasian male presented with shortness of breath, hypertension, bloody sputum, and a history of drug abuse (confirmed by urinalysis). He was found to have severe kidney injury requiring
A 23 year old Caucasian male presented with shortness of breath, hypertension, bloody sputum, and a history of drug abuse (confirmed by urinalysis). He was found to have severe kidney injury requiring
Subclavian artery Stenting
 Subclavian artery Stenting Etiology Atherosclerosis Takayasu s arteritis Fibromuscular dysplasia Giant Cell Arteritis Radiation-induced Vascular Injury Thoracic Outlet Syndrome Neurofibromatosis Incidence
Subclavian artery Stenting Etiology Atherosclerosis Takayasu s arteritis Fibromuscular dysplasia Giant Cell Arteritis Radiation-induced Vascular Injury Thoracic Outlet Syndrome Neurofibromatosis Incidence
Pregnancy-Associated Hemolytic Uremic Syndrome Revisited in the Era of Complement Gene Mutations
 Pregnancy-Associated Hemolytic Uremic Syndrome Revisited in the Era of Complement Gene Mutations Fadi Fakhouri,* Lubka Roumenina, François Provot, Marion Sallée, Sophie Caillard, Lionel Couzi, Marie Essig,**
Pregnancy-Associated Hemolytic Uremic Syndrome Revisited in the Era of Complement Gene Mutations Fadi Fakhouri,* Lubka Roumenina, François Provot, Marion Sallée, Sophie Caillard, Lionel Couzi, Marie Essig,**
Schematic Of Heparin Induced Thrombocytopenia Platelet Count
 Schematic Of Heparin Induced Thrombocytopenia Platelet Count Normal IgG and IgG2 differentially inhibit HIT antibody-dependent platelet activation that platelet counts were lower in FcγRIIA 131RR patients
Schematic Of Heparin Induced Thrombocytopenia Platelet Count Normal IgG and IgG2 differentially inhibit HIT antibody-dependent platelet activation that platelet counts were lower in FcγRIIA 131RR patients
From MPGN to C3G. F Fakhouri, Nantes, France. «Membranoproliferative» is a pathological feature. Mesangial expansion «Doubles contours»
 From MPGN to C3G F Fakhouri, Nantes, France Conflits d intérêt: consultant auprès d Alexion Pharmaceuticals «Membranoproliferative» is a pathological feature Mesangial expansion «Doubles contours» Immune
From MPGN to C3G F Fakhouri, Nantes, France Conflits d intérêt: consultant auprès d Alexion Pharmaceuticals «Membranoproliferative» is a pathological feature Mesangial expansion «Doubles contours» Immune
Ten recommendations for Osteoarthritis and Cartilage (OAC) manuscript preparation, common for all types of studies.
 manuscript preparation, common for all types of studies.") Ten recommendations for Osteoarthritis and Cartilage (OAC) manuscript preparation, common for all types of studies. Ranstam, Jonas; Lohmander, L Stefan Published in: Osteoarthritis and Cartilage DOI: 10.1016/j.joca.2011.07.007
Ten recommendations for Osteoarthritis and Cartilage (OAC) manuscript preparation, common for all types of studies. Ranstam, Jonas; Lohmander, L Stefan Published in: Osteoarthritis and Cartilage DOI: 10.1016/j.joca.2011.07.007
List of authors and affiliations :
 List of authors and affiliations : Fadi Fakhouri 1, Marc Fila 2, François Provot 3, Yahsou Delmas 2, Christelle Barbet 5, Valérie Châtelet 6, Cédric afat 7, Mathilde Cailliez 8, Julien Hogan 9, Aude Servais
List of authors and affiliations : Fadi Fakhouri 1, Marc Fila 2, François Provot 3, Yahsou Delmas 2, Christelle Barbet 5, Valérie Châtelet 6, Cédric afat 7, Mathilde Cailliez 8, Julien Hogan 9, Aude Servais
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT. J. H. Helderman,MD,FACP,FAST
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
1. INSTRUCTIONS 2. DEFINITION OF HUS
 CQ_IBK_aHUS_01 / version 25/11/09 European Paediatric Research Group for HUS and related disorders Case questionnaire for diarrhoea negative/vtec (STEC) negative cases acute phase 1. INSTRUCTIONS Please
CQ_IBK_aHUS_01 / version 25/11/09 European Paediatric Research Group for HUS and related disorders Case questionnaire for diarrhoea negative/vtec (STEC) negative cases acute phase 1. INSTRUCTIONS Please
SUPPLEMENTARY INFORMATION
 SUPPLEMENTARY INFORMATION Supplementary Figure 1. Long-term protection studies. 45 minutes of ischemia was induced in wild type (S1pr2 +/+ ) and S1pr2 -/- by MCAO. A) 5 days later brains were harvested
SUPPLEMENTARY INFORMATION Supplementary Figure 1. Long-term protection studies. 45 minutes of ischemia was induced in wild type (S1pr2 +/+ ) and S1pr2 -/- by MCAO. A) 5 days later brains were harvested
Not So Benign Hematology Aplastic anemia, Paroxysmal Nocturnal Hemoglobinuria, atypical Hemolytic Uremic Syndrome, Thrombotic Thrombocytopenic Purpura
 Not So Benign Hematology Aplastic anemia, Paroxysmal Nocturnal Hemoglobinuria, atypical Hemolytic Uremic Syndrome, Thrombotic Thrombocytopenic Purpura Robert A. Brodsky, MD Johns Hopkins Family Professor
Not So Benign Hematology Aplastic anemia, Paroxysmal Nocturnal Hemoglobinuria, atypical Hemolytic Uremic Syndrome, Thrombotic Thrombocytopenic Purpura Robert A. Brodsky, MD Johns Hopkins Family Professor
1Pulse sequences for non CE MRA
 MRI: Principles and Applications, Friday, 8.30 9.20 am Pulse sequences for non CE MRA S. I. Gonçalves, PhD Radiology Department University Hospital Coimbra Autumn Semester, 2011 1 Magnetic resonance angiography
MRI: Principles and Applications, Friday, 8.30 9.20 am Pulse sequences for non CE MRA S. I. Gonçalves, PhD Radiology Department University Hospital Coimbra Autumn Semester, 2011 1 Magnetic resonance angiography
Case # 2 3/27/2017. Disclosure of Relevant Financial Relationships. Clinical history. Clinical history. Laboratory findings
 Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
3/6/2017. Prevention of Complement Activation and Antibody Development: Results from the Duet Trial
 Prevention of Complement Activation and Antibody Development: Results from the Duet Trial Jignesh Patel MD PhD FACC FRCP Medical Director, Heart Transplant Cedars-Sinai Heart Institute Disclosures Name:
Prevention of Complement Activation and Antibody Development: Results from the Duet Trial Jignesh Patel MD PhD FACC FRCP Medical Director, Heart Transplant Cedars-Sinai Heart Institute Disclosures Name:
Haemolytic uraemic syndrome the story of a whodunit
 Haemolytic uraemic syndrome the story of a whodunit Paul Warwicker Lancashire Teaching Hospitals NHS Trust RCP Kidney for the General Physician Conference Nov 17 Renal thrombotic microangiopathy (TMA)
Haemolytic uraemic syndrome the story of a whodunit Paul Warwicker Lancashire Teaching Hospitals NHS Trust RCP Kidney for the General Physician Conference Nov 17 Renal thrombotic microangiopathy (TMA)
Unravelling the pathophysiology of HUS in light of recent discoveries on complement activation
 Unravelling the pathophysiology of HUS in light of recent discoveries on complement activation Marina Noris November 13, 2018 1 THROMBOTIC MICROANGIOPATHY Histology lesions: Swelling and detachment of
Unravelling the pathophysiology of HUS in light of recent discoveries on complement activation Marina Noris November 13, 2018 1 THROMBOTIC MICROANGIOPATHY Histology lesions: Swelling and detachment of
ahus: Facts, Controversies & Treatment Updates Patrick D. Brophy MD Pediatric Nephrology, Dialysis & Transplant University of Iowa
 ahus: Facts, Controversies & Treatment Updates Patrick D. Brophy MD Pediatric Nephrology, Dialysis & Transplant University of Iowa DISCLOSURE STATEMENT I, Patrick Brophy disclose the following relationships.
ahus: Facts, Controversies & Treatment Updates Patrick D. Brophy MD Pediatric Nephrology, Dialysis & Transplant University of Iowa DISCLOSURE STATEMENT I, Patrick Brophy disclose the following relationships.
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS. 73 year old NS right-handed male applicant for $1 Million life insurance
 MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
Anastasios E. Germenis
 Anastasios E. Germenis Professor and Chairman Department of Immunology & Histocompatibility School of Medicine University of Thessaly University Hospital of Larissa Greece agermen@med.uth.gr The Complement
Anastasios E. Germenis Professor and Chairman Department of Immunology & Histocompatibility School of Medicine University of Thessaly University Hospital of Larissa Greece agermen@med.uth.gr The Complement
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: eculizumab_soliris 8/2014 4/2018 4/2019 4/2018 Description of Procedure or Service Paroxysmal nocturnal hemoglobinuria
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: eculizumab_soliris 8/2014 4/2018 4/2019 4/2018 Description of Procedure or Service Paroxysmal nocturnal hemoglobinuria
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License
 Licht C, Greenbaum LA, Muus P, Babu S, Bedrosian CL, Cohen D, Delmas Y, Douglas K, Furman R, Gaber O, Goodship T, Herthelius M, Hourmant M, Legendre C, Remuzzi G, Sheerin N, Trivelli A, Loirat C. Efficacy
Licht C, Greenbaum LA, Muus P, Babu S, Bedrosian CL, Cohen D, Delmas Y, Douglas K, Furman R, Gaber O, Goodship T, Herthelius M, Hourmant M, Legendre C, Remuzzi G, Sheerin N, Trivelli A, Loirat C. Efficacy
DIAGNOSTIC CHALLENGES IN THROMBOTIC MICROANGIOPATHIES
 DIAGNOSTIC CHALLENGES IN THROMBOTIC MICROANGIOPATHIES Summary of Presentations from the Alexion-Sponsored Symposium, held at the 51 st ERA EDTA Congress, Amsterdam, the Netherlands, on 1 st June 2014 Chairperson
DIAGNOSTIC CHALLENGES IN THROMBOTIC MICROANGIOPATHIES Summary of Presentations from the Alexion-Sponsored Symposium, held at the 51 st ERA EDTA Congress, Amsterdam, the Netherlands, on 1 st June 2014 Chairperson
Core Curriculum in Nephrology
 Core Curriculum in Nephrology Glomerular Diseases Dependent on Complement Activation, Including Atypical Hemolytic Uremic Syndrome, Membranoproliferative Glomerulonephritis, and C3 Glomerulopathy: Core
Core Curriculum in Nephrology Glomerular Diseases Dependent on Complement Activation, Including Atypical Hemolytic Uremic Syndrome, Membranoproliferative Glomerulonephritis, and C3 Glomerulopathy: Core
ISTITUTO DI RICERCHE FARMACOLOGICHE MARIO NEGRI CLINICAL RESEARCH CENTER ALDO E FOR CELE RARE DACCO DISEASES ALDO E CELE DACCO
 ISTITUTO DI RICERCHE FARMACOLOGICHE MARIO NEGRI CENTRO MARIO DI NEGRI RICERCHE INSTITUTE CLINICHE FOR PHARMACOLOGICAL PER LE MALATTIE RESEARCH RARE CLINICAL RESEARCH CENTER ALDO E FOR CELE RARE DACCO DISEASES
ISTITUTO DI RICERCHE FARMACOLOGICHE MARIO NEGRI CENTRO MARIO DI NEGRI RICERCHE INSTITUTE CLINICHE FOR PHARMACOLOGICAL PER LE MALATTIE RESEARCH RARE CLINICAL RESEARCH CENTER ALDO E FOR CELE RARE DACCO DISEASES
Lnformation Coverage Guidance
 Lnformation Coverage Guidance Coverage Indications, Limitations, and/or Medical Necessity Abstract: B-type natriuretic peptide (BNP) is a cardiac neurohormone produced mainly in the left ventricle. It
Lnformation Coverage Guidance Coverage Indications, Limitations, and/or Medical Necessity Abstract: B-type natriuretic peptide (BNP) is a cardiac neurohormone produced mainly in the left ventricle. It
Increased mortality after fracture of the surgical neck of the humerus: a case-control study of 253 patients with a 12-year follow-up.
 Increased mortality after fracture of the surgical neck of the humerus: a case-control study of 253 patients with a 12-year follow-up. Olsson, Christian; Petersson, Claes; Nordquist, Anders Published in:
Increased mortality after fracture of the surgical neck of the humerus: a case-control study of 253 patients with a 12-year follow-up. Olsson, Christian; Petersson, Claes; Nordquist, Anders Published in:
Gene Polymorphism of Complement Factor H in a Turkish Patient With Membranoproliferative Glomerulonephritis Type II
 Kidney Diseases Gene Polymorphism of Complement Factor H in a Turkish Patient With Membranoproliferative Glomerulonephritis Type II Betul Sozeri, 1 Sevgi Mir, 1 Afig Berdeli, 2 Nida Dincel, 1 Banu Sarsik
Kidney Diseases Gene Polymorphism of Complement Factor H in a Turkish Patient With Membranoproliferative Glomerulonephritis Type II Betul Sozeri, 1 Sevgi Mir, 1 Afig Berdeli, 2 Nida Dincel, 1 Banu Sarsik
HUS-MPGN-TTP. & related disorders
 ES-PCR 4 th International Conference HUS-MPGN-TTP & related disorders Current diagnosis and therapy of hemolytic uremic syndrome (HUS), membranoproliferative glomerulonephritis (MPGN), thrombotic thrombocytopenic
ES-PCR 4 th International Conference HUS-MPGN-TTP & related disorders Current diagnosis and therapy of hemolytic uremic syndrome (HUS), membranoproliferative glomerulonephritis (MPGN), thrombotic thrombocytopenic
w ahus pathology is linked to dysregulation of the alternative complement pathway.
 ahus - Pathogenesis, Etiology, and Clinical Advances Craig B. Langman MD The Isaac A Abt MD Professor of Kidney Diseases Feinberg School of Medicine, Northwestern University Head, Kidney Diseases The Ann
ahus - Pathogenesis, Etiology, and Clinical Advances Craig B. Langman MD The Isaac A Abt MD Professor of Kidney Diseases Feinberg School of Medicine, Northwestern University Head, Kidney Diseases The Ann
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS. 73 year old NS right-handed male applicant for $1 Million Life Insurance
 MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
Puschmann, Andreas; Dickson, Dennis W; Englund, Elisabet; Wszolek, Zbigniew K; Ross, Owen A
 CHCHD2 and Parkinson's disease Puschmann, Andreas; Dickson, Dennis W; Englund, Elisabet; Wszolek, Zbigniew K; Ross, Owen A Published in: Lancet Neurology DOI: 10.1016/S1474-4422(15)00095-2 2015 Link to
CHCHD2 and Parkinson's disease Puschmann, Andreas; Dickson, Dennis W; Englund, Elisabet; Wszolek, Zbigniew K; Ross, Owen A Published in: Lancet Neurology DOI: 10.1016/S1474-4422(15)00095-2 2015 Link to
Therapeutic Complement Intervention Michael Kirschfink, Institute of Immunology, University of Heidelberg, Germany
 Therapeutic Complement Intervention Michael Kirschfink, Institute of Immunology, University of Heidelberg, Germany Complement-mediated diseases Therapeutic intervention The complement system is involved
Therapeutic Complement Intervention Michael Kirschfink, Institute of Immunology, University of Heidelberg, Germany Complement-mediated diseases Therapeutic intervention The complement system is involved