CARDIAC CHEST PAIN. 1. ST Elevation MI
|
|
|
- August Leonard
- 5 years ago
- Views:
Transcription
1 CARDIAC CHEST PAIN ACUTE ST ELEVATION MYOCARDIAL INFARCTION* and ACUTE CORONARY SYNDROME (ACS) are caused by instability/rupture of atheromatous plaques in the coronary circulation. Identifying ST Elevation MI rapidly is the first goal so that definitive treatment can be achieved as early as possible to limit myocardial damage. The ACS spectrum ranges from unstable angina (USA) to non-st elevation myocardial infarction (NSTEMI). ACS is extremely common amongst ED patients and it is associated with high risk of cardiac arrest, peri-arrest arrhythmias, acute ST elevation myocardial infarction and acute LVF. *Rarely acute MI may be caused by another cause such as cocaine abuse 1. ST Elevation MI All patients with a STEMI should be referred to RVH for consideration of primary PCI. NIAS have a bypass protocol so most patients that they attend who have a STEMI will go directly to RVH. Suspected STEMI less than 12 hours from onset of maximum pain ST elevation: 1mm or more in at least 2 contigious limb leads or 2mm or more in at least 2 contiguous chest leads Diagnostic uncertainty Discuss with on cardiology on call team FAX ECG to and then PHONE the PCI co-ordinator Accepted for PCI: Give aspirin 300mg only IV access minimum 20G (pink) Do ABG unless clear clinical indication Continuous cardiac monitor Arrange immediate transfer to RVH cath lab or CCU Not accepted for PCI: Discuss with local cardiology on call team 68
2 2. Non- ST Elevation MI and other Acute Coronary Syndromes History: Cardiac sounding chest pain Atypical pain especially females and diabetic Cardiac risk factors Previous MI / IHD Examination: CVS and RS examination BP in both arms and peripheral pulses if possibility of dissection thoracic aorta Ischaemic ECG changes: (repeat ECG in 30 mins if suggestive history but normal initial ECG) 1. LBBB = assume anterior myocardial infarction if new 2. Profound ST depression V1-3 +/- Tall R-wave in V1 = posterior myocardial infarction 3. Tall peaked T-waves with early slurring of ST segment=?hyperacute ischaemic ECG: GET ADVICE 4. Any other ST segment depression( NSSTTW ) = assume Acute Coronary Syndrome unless present on old ECGs Management: All patients with suspected ACS should receive the following treatment (unless contra-indicated e.g. on warfarin). 100 % oxygen NRRM Continuous ECG monitor, SaO2, NIBP GTN spray Pain relief as required e.g. diamorphine +/- metoclopramide Chewable Aspirin 300 mgs orally Enoxaparin (Clexane) 1mg/kg subcutaneously bd. Admit under cardiology 3. Low Risk Cardiac Chest Pain Patients with history suggestive of cardiac chest pain but who are low risk (TIMI score 2 or less) who are pain free are suitable for ED / Observation Ward management. See flow diagram on next page for appropriate management. 69
3 Assessment of low risk patients with cardiac sounding chest pain presenting to Antrim ED Chest pain suggestive of cardiac origin Pain free ECG no acute changes TIMI score 2 Troponin at triage or initial doctor assessment TIMI Score 1 One point for each; Age 65 years 3 CAD risk factors Prior stenosis >50% ST deviation 2 anginal events in 24 hours Aspirin in last 7 days Elevated troponin Initial troponin 14 or less and 4 hours or more from onset of pain Initial troponin 14 or less and less than 4 hours from onset of pain Initial troponin greater than 14 (unless at baseline) Repeat ECG no acute changes* Repeat troponin in 3 hours. Admit to Observation Ward on pathway Possible AMI, refer to cardiology # Not consistent with AMI. Consider discharge and outpatient follow-up # Absolute $ troponin change 9 ng/l and no evolving changes* on ECG Not consistent with AMI. Consider discharge and outpatient follow-up # Absolute $ troponin change of > 9 ng/l Possible AMI, refer to cardiology # References 1. Antman EM, Cohen M, Bernink PM, et al. The TIMI Risk Score for Unstable Angina/Non ST Elevation MI: A Method for Prognostication and Therapeutic Decision Making. JAMA. 2000;284(7): Notes * if acute ischaemic changes refer to cardiology $ Absolute change equates to difference between the original and second troponin results, this may be positive or negative. Absolute change of 9 ng/l is considered clinically significant # it is the responsibility of the discharging doctor to follow-up results and complete discharge letter 70
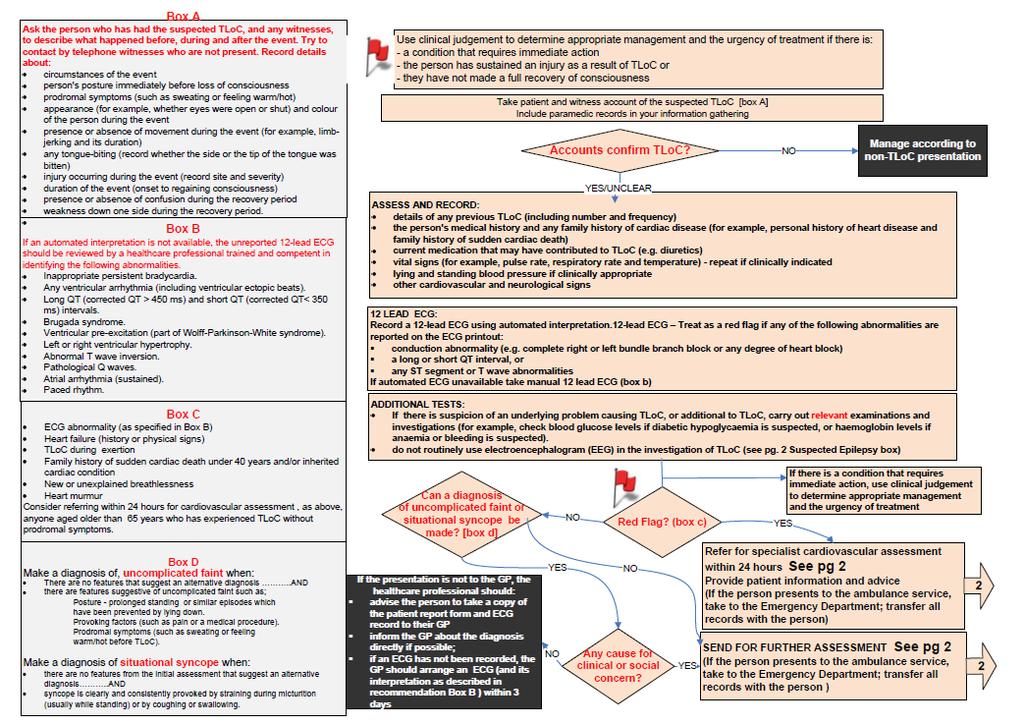
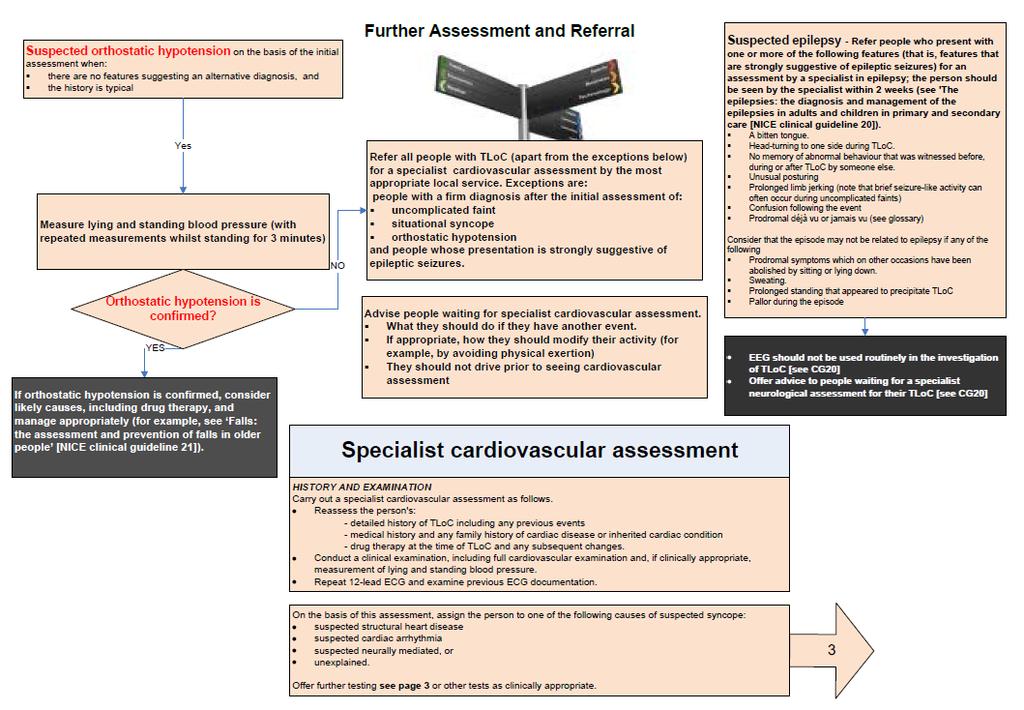
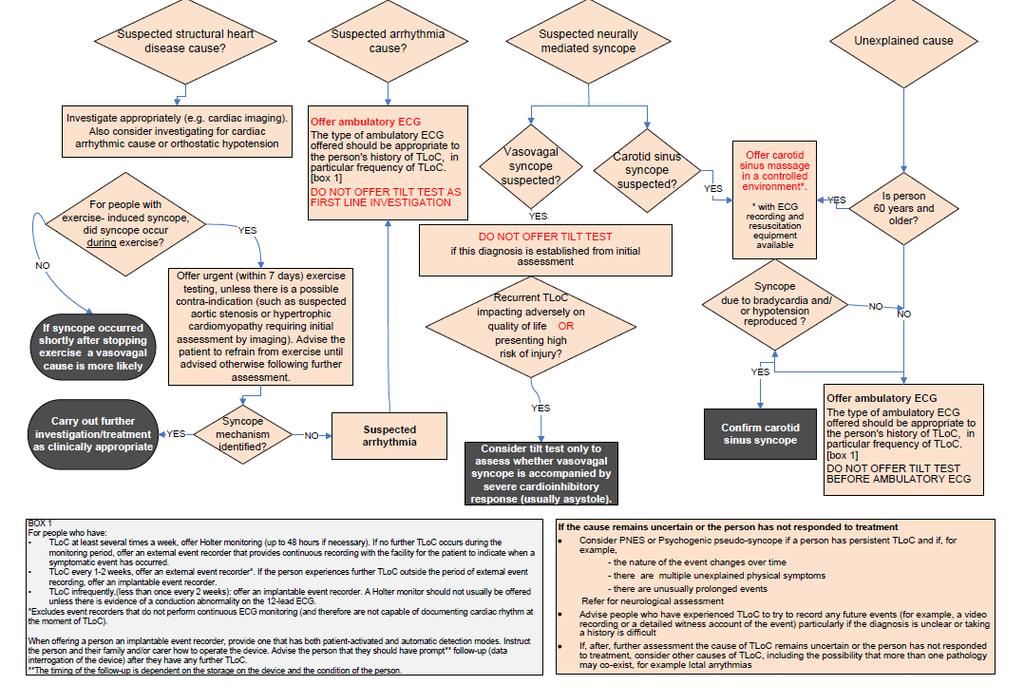
4 4. Rapid Access Chest Pain Clinic CARDIOVASCULAR The Rapid Access Chest Pain Clinic is designed to provide a one stop service for patients presenting with a recent onset of chest pain thought to be stable angina or very low risk unstable angina. ED doctors on the advice of the ED consultant can refer patients directly to RACPC. 5. Not all Chest Pain is Cardiac You will see many other types of chest pain. Common causes of chest pain include: Musculoskeletal pain is the commonest take a good history!--did the patient undertake strenuous activity e.g. gardening?, do certain movements hurt? Is there a tender costo vertebral junction suggesting an acutely subluxed rib at the back (common and self limiting) but remember that ~15% of patients with acute MI have marked chest wall tenderness! Upper GI GORD, Acute Cholecystitis, Pancreatitis PE (use Canada Score) Stress, Hyperventilation Chest infection Rib fractures e.g. cough fracture Herpes zoster (dermatomal) TRANSIENT LOSS OF CONSCIOUSNESS (TLOC) Significant causes of TLOC must be excluded before patients can be safely discharged home. The following is a summary of the NICE 2010 Clinical Guidelines for the Management of TLOC in adults and young people. 71
5 72
6 73
7 74
8 ACUTE LEFT VENTRICULAR FAILURE CARDIOVASCULAR Recognition: Sudden onset of dyspnoea or sudden deterioration? Previous cardiac history? Pallor/sweating? Pulmonary crepitations? Hypotension/ clammy? Treatment Inform senior ED doctor immediately Consider arrhythmia or MI as cause monitor, 12-lead ECG Give oxygen 100%* Diamorphine 2.5-5mg iv +/- metoclopramide 10mg iv Administer Furosemide mg iv (repeat if necessary) Consider iv GTN (only if SBP >110) Consider CPAP if respiratory distress Notify Cardiac doctor ASAP +/- ICU THROMBO-EMBOLIC DISEASE IT IS ESSENTIAL TO UNDERSTAND THE DIFFERENCES IN APPLICATION AND NORMAL RANGE BETWEEN D-DIMER TESTING FOR PULMONARY EMBOLISM AND DVT 1. Pulmonary Embolism MASSIVE PULMONARY EMBOLISM IS A CLINICAL DIAGNOSIS MADE IN THE PRESENCE OF SHOCK, RIGHT HEART STRAIN AND SEVERE HYPOXIA WITH RISK FACTORS FOR THROMBOEMBOLIC DISEASE AND NO OBVIOUS ALTERNATIVE DIAGNOSIS (EG MI). GIVE 0 2 via NRRM and CONSIDER IMMEDIATE LYSIS (PREFERABLY AFTER CARDIAC ECHO IN RESUS) SEEK SENIOR ADVICE Assessment for acute sub-massive pulmonary embolus follows the rule inrule out method outlined below. A scoring system devised by a team of Canadian physicians forms the basis for our assessment. Although this system incorporates D-dimer testing and is supported by diagnostic imaging, your clinical assessment of the likelihood of PE as opposed to some other diagnosis is crucial. 75
9 a) Step One: Clinical Assessment History: Acute pulmonary embolus is often a difficult diagnosis as signs are often non-specific or unreliable. Patients often complain of dypsnoea, pleuritic chest pain or collapse with shock in the absence of other causes. 97% of patients have one of the following 1. Dypsnoea 2. Tachypnoea (Respiratory rate >29/min) 3. Pleuritic chest pain But you must consider if another diagnosis is more likely. Examination: of the cardiovascular system, chest and legs may confirm your suspicion of PE but physical findings are more often useful in suggesting an alternative diagnosis (see below). Investigations: ECG: should be taken, mainly to exclude acute MI or pericarditis. In PE tachycardia is the most common finding, non-specific ST-T wave abnormality is common, S1Q3T3 is rare. PACXR: should be also requested. Once again, it is often more helpful in identifying an alternative diagnosis such as pneumothorax, LVF or chest infection. It is normal in 10-20% of patients with PE (note that a normal CXR with hypoxia and significant dyspnoea supports a diagnosis of PE). Most of the remaining patients have non-specific findings like atelectatsis / small effusion / elevated diaphragm, cardiomegaly. Occasionally, specific findings like a pulmonary infarct will be seen (wedge shaped, Hampton s hump) or an area of oligaemia identified distal to a dilated vessel (Westermark sign). ABG / 0 2 sat: should always be measured. Low 0 2 saturation or P0 2 increases suspicion in the absence of alternative diagnosis but normal oxygenation does not exclude PE. Comparing ABGs with and without 0 2 mask is not helpful. b) Step Two: Measure Canadian Score Clinical features of DVT 3.0 Recent immobility or surgery 1.5 Active cancer 1.0 Hx of DVT / PE 1.5 Haemoptysis 1.0 Resting heart rate >100/min 1.5 PE as likely as or more likely 3.0 than an alternative diagnosis 76
10 SCORE Pre-test Probability of PE <2 low 6 Medium to high risk c) Step Three: Investigation to Rule In or Rule Out PE RULE OUT: Patients with a low pre-test probability score can have a d-dimer test to rule out PE. IF their D-Dimer is < 250ng/ml, PE can be excluded and an alternative diagnosis should be sought. RULE IN: Patients with a medium or high pre-test probability OR a D-dimer > 250mg/ml will probably require radio-isotope scan or CTPA scan to rule in PE irrespective of D-dimer result. Stable patients with a low PESI score may be investigated in the Observation Ward. Patients with a high PESI score are high risk and should be admitted for investigation and management under the medical inpatient team. d) Management All patients suspected of having a PE after the above assessment should be treated with enoxaparin 1.5 mk/kg SC (reduced in renal impairment as per BNF). Next their PESI score should be calculated as an indication of risk of complications. Those patients with a PESI score of 85 or less can be investigated through the Observation Ward Pathway. Those with a PESI score higher than 85, a confirmed diagnosis of PE or clinical picture suggestive of a massive PE should be admitted under the respiratory team. PESI Score Clinical indicator Points Age + age (in years) Male sex + 10 Cancer + 30 Heart failure + 10 Chronic lung disease + 10 Pulse > 110 bpm + 20 Systolic BP < 100 mmhg + 30 Respiratory rate 30 breaths/min + 20 Temperature < Altered mental state + 60 Arterial saturation < 90%
11 2. Acute Life Threatening Pulmonary Embolism CARDIOVASCULAR RESUSCITATION When a patient presents with suspected PE, the initial focus is on stabilizing the patient. Respiratory support Supplemental oxygen should be administered if hypoxemia exists. Severe hypoxemia or respiratory failure should prompt consideration of intubation and mechanical ventilation. Hemodynamic support Hemodynamic support should be instituted promptly when a patient presents with PE and hypotension, defined as a systolic blood pressure <90 mmhg or a drop in systolic blood pressure of 40 mmhg from baseline. Intravenous fluid administration is first-line therapy. Clinicians should be wary of administering more than 500 to 1000 ml of normal saline during the initial resuscitation period. If the patient's hypotension does not resolve with intravenous fluids, intravenous vasopressor therapy should promptly follow. THROMBOLYSIS Thrombolytic therapy accelerates the lysis of acute PE and improves important physiologic parameters, such as RV function and pulmonary perfusion. However, no clinical trial has been large enough to conclusively demonstrate a mortality benefit. Thrombolytic therapy is associated with an increased risk of major hemorrhage, defined as intracranial hemorrhage, retroperitoneal hemorrhage, or bleeding leading directly to death, hospitalization, or transfusion. Persistent hypotension due to PE (ie, massive PE) is the most widely accepted indication for thrombolytic therapy. A 50 mg bolus of alteplase is recommended. 78
CARDIAC CHEST PAIN. 1. ST Elevation MI
 CARDIAC CHEST PAIN ACUTE ST ELEVATION MYOCARDIAL INFARCTION* and ACUTE CORONARY SYNDROME (ACS) are caused by instability/rupture of atheromatous plaques in the coronary circulation. Identifying ST Elevation
CARDIAC CHEST PAIN ACUTE ST ELEVATION MYOCARDIAL INFARCTION* and ACUTE CORONARY SYNDROME (ACS) are caused by instability/rupture of atheromatous plaques in the coronary circulation. Identifying ST Elevation
RESUSCITATION - ABC. Advanced Adult Algorithms Cardiac Arrest
 RESUSCITATION - ABC Advanced Adult Algorithms Cardiac Arrest 60 61 RESUSCITATION ABC 62 RESUSCITATION ABC 63 RESUSCITATION - ABC 64 RESUSCITATION ABC 65 CARDIOVASCULAR Shock inadequate tissue perfusion
RESUSCITATION - ABC Advanced Adult Algorithms Cardiac Arrest 60 61 RESUSCITATION ABC 62 RESUSCITATION ABC 63 RESUSCITATION - ABC 64 RESUSCITATION ABC 65 CARDIOVASCULAR Shock inadequate tissue perfusion
Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine
 Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine Venous thromboembolism: pulmonary embolism (PE) deep vein thrombosis (DVT) 1% of all patients admitted to hospital 5% of in-hospital mortality
Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine Venous thromboembolism: pulmonary embolism (PE) deep vein thrombosis (DVT) 1% of all patients admitted to hospital 5% of in-hospital mortality
PE Pathway. The charts are listed as follows:
 PE Pathway This document comprises 6 simple flow charts to assist clinicians in the investigation and treatment of suspected or confirmed Acute Pulmonary Emboli. The pathway has been put together using
PE Pathway This document comprises 6 simple flow charts to assist clinicians in the investigation and treatment of suspected or confirmed Acute Pulmonary Emboli. The pathway has been put together using
OVERVIEW ACUTE CORONARY SYNDROME SYMPTOMS 9/30/14 TYPICAL WHAT IS ACUTE CORONARY SYNDROME? SYMPTOMS, IDENTIFICATION, MANAGEMENT
 OVERVIEW ACUTE CORONARY SYNDROME SYMPTOMS, IDENTIFICATION, MANAGEMENT OCTOBER 7, 2014 PETE PERAUD, MD SYMPTOMS TYPICAL ATYPICAL IDENTIFICATION EKG CARDIAC BIOMARKERS STEMI VS NON-STEMI VS USA MANAGEMENT
OVERVIEW ACUTE CORONARY SYNDROME SYMPTOMS, IDENTIFICATION, MANAGEMENT OCTOBER 7, 2014 PETE PERAUD, MD SYMPTOMS TYPICAL ATYPICAL IDENTIFICATION EKG CARDIAC BIOMARKERS STEMI VS NON-STEMI VS USA MANAGEMENT
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT
: DIAGNOSIS AND TREATMENT") PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
Pulmonary Embolism. Pulmonary Embolism. Pulmonary Embolism. PE - Clinical
 Pulmonary embolus - a practical approach to investigation and treatment Sam Janes Wellcome Senior Fellow and Respiratory Physician, University College London Background Diagnosis Treatment Common: 50 cases
Pulmonary embolus - a practical approach to investigation and treatment Sam Janes Wellcome Senior Fellow and Respiratory Physician, University College London Background Diagnosis Treatment Common: 50 cases
A Diagnostic Dilemma saved by sound
 A Diagnostic Dilemma saved by sound Dr Syam Ravindranath MBBS DNB, Dr Ash Mukherjee FCEM FACEM We p r e s e n t a d i a g n o s t i c a l l y c h a l l e n g i n g s c e n a r i o in a 59 y e a r old f
A Diagnostic Dilemma saved by sound Dr Syam Ravindranath MBBS DNB, Dr Ash Mukherjee FCEM FACEM We p r e s e n t a d i a g n o s t i c a l l y c h a l l e n g i n g s c e n a r i o in a 59 y e a r old f
AIMS: CHEST PAIN. Causes of chest pain. Causes of chest pain: Cardiac causes: Acute coronary syndromes pericarditis thoracic aortic dissection
 CHEST PAIN Dr Susan Hertzberg Emergency Department Prince of Wales Hospital AIMS: To identify causes of chest pain in patients presenting to the ED. To identify and risk stratify patients presenting with
CHEST PAIN Dr Susan Hertzberg Emergency Department Prince of Wales Hospital AIMS: To identify causes of chest pain in patients presenting to the ED. To identify and risk stratify patients presenting with
Management of Acute Pulmonary Embolism. Judith Hurdman Consultant Respiratory Physician
 Management of Acute Pulmonary Embolism Judith Hurdman Consultant Respiratory Physician Judith.hurdman@sth.nhs.uk Overview Risk Stratification Who can be managed as an outpatient? To thrombolyse or not
Management of Acute Pulmonary Embolism Judith Hurdman Consultant Respiratory Physician Judith.hurdman@sth.nhs.uk Overview Risk Stratification Who can be managed as an outpatient? To thrombolyse or not
Practitioner Education Course
 2015 Practitioner Education Course ST Elevation Myocardial Infarction 2 Pathology Concept of vulnerable plaque Mild Atheroma Diagnosis IVUS OCT 3 Diagnosis This is based on : Clinical History ECG Changes.
2015 Practitioner Education Course ST Elevation Myocardial Infarction 2 Pathology Concept of vulnerable plaque Mild Atheroma Diagnosis IVUS OCT 3 Diagnosis This is based on : Clinical History ECG Changes.
An Approach to Chest Pain
 Oesophageal Spasm Acute Coronary Syndrome Pneumothorax An Approach to Chest Pain Musculoskeletal Pulmonary Embolism Aortic Dissection Ema Pitts Cardiology Registrar Basic Trainee Pain S Site O Onset C
Oesophageal Spasm Acute Coronary Syndrome Pneumothorax An Approach to Chest Pain Musculoskeletal Pulmonary Embolism Aortic Dissection Ema Pitts Cardiology Registrar Basic Trainee Pain S Site O Onset C
Results of Ischemic Heart Disease
 Ischemic Heart Disease: Angina and Myocardial Infarction Ischemic heart disease; syndromes causing an imbalance between myocardial oxygen demand and supply (inadequate myocardial blood flow) related to
Ischemic Heart Disease: Angina and Myocardial Infarction Ischemic heart disease; syndromes causing an imbalance between myocardial oxygen demand and supply (inadequate myocardial blood flow) related to
ECG Workshop. Nezar Amir
 ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
Acute Coronary Syndromes Unstable Angina Non ST segment Elevation MI (NSTEMI) ST segment Elevation MI (STEMI)
 ST segment Elevation MI (STEMI)") Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Evaluate common abnormalities that mimic myocardial infarction. Identify
Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Evaluate common abnormalities that mimic myocardial infarction. Identify
ST Elevation Myocardial Infarction (STEMI) Reperfusion Order Set
 Reperfusion Order Set") Form Title Form Number CH-0454 2018, Alberta Health Services, CKCM This work is licensed under the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License. The license does not
Form Title Form Number CH-0454 2018, Alberta Health Services, CKCM This work is licensed under the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License. The license does not
Acute Coronary Syndrome
 Acute Coronary Syndrome Clinical Manifestation of CAD Silent Ischemia/asymptomatic Stable Angina Acute Coronary Syndrome (Non- STEMI/UA and STEMI) Arrhythmias Heart Failure Sudden Death Pain patterns with
Acute Coronary Syndrome Clinical Manifestation of CAD Silent Ischemia/asymptomatic Stable Angina Acute Coronary Syndrome (Non- STEMI/UA and STEMI) Arrhythmias Heart Failure Sudden Death Pain patterns with
CLINICIAN INTERVIEW RECOGNIZING ACS AND STRATIFYING RISK IN PRIMARY CARE. An interview with A. Michael Lincoff, MD, and Eric R. Bates, MD, FACC, FAHA
 RECOGNIZING ACS AND STRATIFYING RISK IN PRIMARY CARE An interview with A. Michael Lincoff, MD, and Eric R. Bates, MD, FACC, FAHA Dr Lincoff is an interventional cardiologist and the Vice Chairman for Research
RECOGNIZING ACS AND STRATIFYING RISK IN PRIMARY CARE An interview with A. Michael Lincoff, MD, and Eric R. Bates, MD, FACC, FAHA Dr Lincoff is an interventional cardiologist and the Vice Chairman for Research
Cardiovascular emergencies. 05/March/2014 László Rudas Szeged
 Cardiovascular emergencies 05/March/2014 László Rudas Szeged Acute chest pain Acute heart failure Sudden cardiac death Acute chest pain What is the etiology? Chest pain signals emergency: - ACS - Pulmonary
Cardiovascular emergencies 05/March/2014 László Rudas Szeged Acute chest pain Acute heart failure Sudden cardiac death Acute chest pain What is the etiology? Chest pain signals emergency: - ACS - Pulmonary
Acute coronary syndromes
 Acute coronary syndromes 1 Acute coronary syndromes Acute coronary syndromes results primarily from diminished myocardial blood flow secondary to an occlusive or partially occlusive coronary artery thrombus.
Acute coronary syndromes 1 Acute coronary syndromes Acute coronary syndromes results primarily from diminished myocardial blood flow secondary to an occlusive or partially occlusive coronary artery thrombus.
Acute Coronary Syndrome
 ACUTE CORONOARY SYNDROME, ANGINA & ACUTE MYOCARDIAL INFARCTION Administrative Consultant Service 3/17 Acute Coronary Syndrome Acute Coronary Syndrome has evolved as a useful operational term to refer to
ACUTE CORONOARY SYNDROME, ANGINA & ACUTE MYOCARDIAL INFARCTION Administrative Consultant Service 3/17 Acute Coronary Syndrome Acute Coronary Syndrome has evolved as a useful operational term to refer to
Characteristics of Transient ST-Elevation versus ST-Elevation and Non-ST-Elevation Myocardial Infarction
 Characteristics of Transient ST-Elevation versus ST-Elevation and Non-ST-Elevation Myocardial Infarction Blondheim DS, Shochat M, Asif A, Kazatsker M, Frimerman A, Vassilenko L, Abu Fane R, Neiman E, Barel
Characteristics of Transient ST-Elevation versus ST-Elevation and Non-ST-Elevation Myocardial Infarction Blondheim DS, Shochat M, Asif A, Kazatsker M, Frimerman A, Vassilenko L, Abu Fane R, Neiman E, Barel
Prehospital Resuscitation for the 21 st Century Simulation Case. VF/Asystole
 Prehospital Resuscitation for the 21 st Century Simulation Case VF/Asystole Case History 1 (hypovolemic cardiac arrest secondary to massive upper GI bleed) 56 year-old male patient who fainted in the presence
Prehospital Resuscitation for the 21 st Century Simulation Case VF/Asystole Case History 1 (hypovolemic cardiac arrest secondary to massive upper GI bleed) 56 year-old male patient who fainted in the presence
Pulmonary Embolism Pathway
 Pulmonary Embolism Pathway Ambulatory Care Pathway Dr. A. Zafar, Dr. A. Rehman, Dr. T. Malik September, 2011. Patient Identification Label Pulmonary Embolism Pathway Clinical History Comments Hospital
Pulmonary Embolism Pathway Ambulatory Care Pathway Dr. A. Zafar, Dr. A. Rehman, Dr. T. Malik September, 2011. Patient Identification Label Pulmonary Embolism Pathway Clinical History Comments Hospital
What is Your Diagnosis?
 What is Your Diagnosis? A STORM R Dulgheru, Liege, Belgium Faculty disclosure Raluca Dulgheru I have no financial relationships to disclose. Case presentation 52 years old male Ongoing oppressive chest
What is Your Diagnosis? A STORM R Dulgheru, Liege, Belgium Faculty disclosure Raluca Dulgheru I have no financial relationships to disclose. Case presentation 52 years old male Ongoing oppressive chest
Cardiology. Self Learning Package. Module 5: Pharmacology: Treatment of Acute Coronary. Prevention
 Cardiology Self Learning Package Module 5: Pharmacology: Treatment of Acute Coronary Syndromes, Module 5: Pharmacology: Hyperlipidaemia, Treatment of Acute Coronary Hypertension, Symdrome, Hyperlipidaemia,
Cardiology Self Learning Package Module 5: Pharmacology: Treatment of Acute Coronary Syndromes, Module 5: Pharmacology: Hyperlipidaemia, Treatment of Acute Coronary Hypertension, Symdrome, Hyperlipidaemia,
Acute Coronary Syndromes
 Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
What is a myocardial infarction and how do we treat it? Paul Das Consultant Cardiologist North Wales Cardiac Centre Glan Clwyd Hospital
 What is a myocardial infarction and how do we treat it? Paul Das Consultant Cardiologist North Wales Cardiac Centre Glan Clwyd Hospital What is a myocardial infarction? THEY AINT WHAT THEY USED TO BE Case
What is a myocardial infarction and how do we treat it? Paul Das Consultant Cardiologist North Wales Cardiac Centre Glan Clwyd Hospital What is a myocardial infarction? THEY AINT WHAT THEY USED TO BE Case
Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism A pulmonary embolism (PE) is
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism A pulmonary embolism (PE) is
UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME. DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18
 Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18") UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18 INTRODUCTION The clinical entities that comprise acute coronary syndromes (ACS)-ST-segment
UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18 INTRODUCTION The clinical entities that comprise acute coronary syndromes (ACS)-ST-segment
Management of Acute Myocardial Infarction
 Management of Acute Myocardial Infarction Prof. Hossam Kandil Professor of Cardiology Cairo University ST Elevation Acute Myocardial Infarction Aims Of Management Emergency care (Pre-hospital) Early care
Management of Acute Myocardial Infarction Prof. Hossam Kandil Professor of Cardiology Cairo University ST Elevation Acute Myocardial Infarction Aims Of Management Emergency care (Pre-hospital) Early care
Chest Pain. Dr Robert Huggett Consultant Cardiologist
 Chest Pain Dr Robert Huggett Consultant Cardiologist Outline Diagnosis of cardiac chest pain 2016 NICE update on stable chest pain Assessment of unstable chest pain/acs and MI definition Scope of the
Chest Pain Dr Robert Huggett Consultant Cardiologist Outline Diagnosis of cardiac chest pain 2016 NICE update on stable chest pain Assessment of unstable chest pain/acs and MI definition Scope of the
APPENDIX F: CASE REPORT FORM
 APPENDIX F: CASE REPORT FORM Instruction: Complete this form to notify all ACS admissions at your centre to National Cardiovascular Disease Registry. Where check boxes are provided, check ( ) one or more
APPENDIX F: CASE REPORT FORM Instruction: Complete this form to notify all ACS admissions at your centre to National Cardiovascular Disease Registry. Where check boxes are provided, check ( ) one or more
CURRENT & FUTURE THERAPEUTIC MANAGEMENT OF VENOUS THROMBOEMBOLISM. Gordon Lowe Professor of Vascular Medicine University of Glasgow
 CURRENT & FUTURE THERAPEUTIC MANAGEMENT OF VENOUS THROMBOEMBOLISM Gordon Lowe Professor of Vascular Medicine University of Glasgow VENOUS THROMBOEMBOLISM Common cause of death and disability 50% hospital-acquired
CURRENT & FUTURE THERAPEUTIC MANAGEMENT OF VENOUS THROMBOEMBOLISM Gordon Lowe Professor of Vascular Medicine University of Glasgow VENOUS THROMBOEMBOLISM Common cause of death and disability 50% hospital-acquired
A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD
 A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD NAVAL HOSPITAL OF ATHENS case presentation Female, 81yo Hx: diabetes mellitus, hypertension, chronic anaemia presented
A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD NAVAL HOSPITAL OF ATHENS case presentation Female, 81yo Hx: diabetes mellitus, hypertension, chronic anaemia presented
Essam Mahfouz, MD. Professor of Cardiology, Mansoura University
 By Essam Mahfouz, MD. Professor of Cardiology, Mansoura University Agenda Definitions Classifications Epidemiology Risk stratification What is new? What is MI? Myocardial infarction is the death of part
By Essam Mahfouz, MD. Professor of Cardiology, Mansoura University Agenda Definitions Classifications Epidemiology Risk stratification What is new? What is MI? Myocardial infarction is the death of part
Acute Coronary Syndrome. Emergency Department Updated Jan. 2017
 Acute Coronary Syndrome Emergency Department Updated Jan. 2017 Goals and Objectives To reduce mortality and morbidity for people who have cardiovascular disease, with a focus on those who experience an
Acute Coronary Syndrome Emergency Department Updated Jan. 2017 Goals and Objectives To reduce mortality and morbidity for people who have cardiovascular disease, with a focus on those who experience an
NUH Emergency Department. Guideline for Diagnosis & Treatment of PE (Massive and Non-Massive) in Adults only
 in Adults only") NUH Emergency Department Guideline for Diagnosis & Treatment of PE (Massive and n-massive) in Adults only Contents Suspected Pulmonary Embolus in the ED Flow Chart Page 1 Administration of Thrombolysis
NUH Emergency Department Guideline for Diagnosis & Treatment of PE (Massive and n-massive) in Adults only Contents Suspected Pulmonary Embolus in the ED Flow Chart Page 1 Administration of Thrombolysis
Case Study 50 YEAR OLD MALE WITH UNSTABLE ANGINA
 Case Study 50 YEAR OLD MALE WITH UNSTABLE ANGINA Case History A 50-year-old man with type 1 diabetes mellitus and hypertension presents after experiencing 1 hour of midsternal chest pain that began after
Case Study 50 YEAR OLD MALE WITH UNSTABLE ANGINA Case History A 50-year-old man with type 1 diabetes mellitus and hypertension presents after experiencing 1 hour of midsternal chest pain that began after
Acute Management of Pulmonary Embolism
 Acute Management of Pulmonary Embolism Dr Alex West Respiratory Consultant Guy s and St Thomas Hospital London Declarations - none Order of Play Up date in Diagnostic Imaging - CTPA and V:Q SPECT Sub-massive
Acute Management of Pulmonary Embolism Dr Alex West Respiratory Consultant Guy s and St Thomas Hospital London Declarations - none Order of Play Up date in Diagnostic Imaging - CTPA and V:Q SPECT Sub-massive
How to give thrombolysis in acute myocardial infarction
 Page 1 of 6 How to give thrombolysis in acute myocardial infarction Original article: Michael Tam In the major urban hospitals, there will be little place for thrombolysis in acute STEMI (STelevation myocardial
Page 1 of 6 How to give thrombolysis in acute myocardial infarction Original article: Michael Tam In the major urban hospitals, there will be little place for thrombolysis in acute STEMI (STelevation myocardial
RISK STRATIFICATION OF PATIENTS WITH ACUTE SYMPTOMATIC PULMONARY EMBOLISM. David Jiménez, MD, PhD, FCCP Ramón y Cajal Hospital, IRYCIS Madrid, Spain
 RISK STRATIFICATION OF PATIENTS WITH ACUTE SYMPTOMATIC PULMONARY EMBOLISM David Jiménez, MD, PhD, FCCP Ramón y Cajal Hospital, IRYCIS Madrid, Spain Potential Conflicts of Interest Financial conflicts of
RISK STRATIFICATION OF PATIENTS WITH ACUTE SYMPTOMATIC PULMONARY EMBOLISM David Jiménez, MD, PhD, FCCP Ramón y Cajal Hospital, IRYCIS Madrid, Spain Potential Conflicts of Interest Financial conflicts of
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 Assessment and immediate management of suspected acute coronary syndrome bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They
Assessment and immediate management of suspected acute coronary syndrome bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They
ST SEGMENT ELEVATION MYOCARDIAL INFARCTION
 ST SEGMENT ELEVATION MYOCARDIAL INFARCTION John Harrison, (1693-1776) H4 (1760) H1 (1737) H2 (1741) H3 (1759) In the wake of Harrison s success with H-4, legions of watch makers took up the special calling
ST SEGMENT ELEVATION MYOCARDIAL INFARCTION John Harrison, (1693-1776) H4 (1760) H1 (1737) H2 (1741) H3 (1759) In the wake of Harrison s success with H-4, legions of watch makers took up the special calling
Risk Stratification of ACS Patients. Frans Van de Werf, MD, PhD University of Leuven, Belgium
 Risk Stratification of ACS Patients Frans Van de Werf, MD, PhD University of Leuven, Belgium Which type of ACS patients are we talking about to day? 4/14/2011 STEMI and NSTEMI in the NRMI registry from
Risk Stratification of ACS Patients Frans Van de Werf, MD, PhD University of Leuven, Belgium Which type of ACS patients are we talking about to day? 4/14/2011 STEMI and NSTEMI in the NRMI registry from
Reporting SPECT-VQ. Alp Notghi
 Reporting SPECT-VQ Alp Notghi 20 year old female 24 weeks pregnant Clinical History : SOB and chest pain for past 3 days.?pe Doppler USS excluded DVT Case 4413041 Normal Case 4413041 CXR report: The heart
Reporting SPECT-VQ Alp Notghi 20 year old female 24 weeks pregnant Clinical History : SOB and chest pain for past 3 days.?pe Doppler USS excluded DVT Case 4413041 Normal Case 4413041 CXR report: The heart
Nitroglycerin and Heparin Drip Interfacility Protocols
 Nitroglycerin and Heparin Drip Interfacility Protocols EMS Protocol This protocol applies to nitroglycerin and Heparin drips that are initiated at the transferring facility prior to transport and are not
Nitroglycerin and Heparin Drip Interfacility Protocols EMS Protocol This protocol applies to nitroglycerin and Heparin drips that are initiated at the transferring facility prior to transport and are not
STANDARDIZED PROCEDURE CARDIAC STRESS TESTING-EXERCISE TESTING (Adult)
") 1 I. Definition: During the exercise test, the patient exercises on a bike or treadmill while being monitored with a 12 lead ECG, blood pressure device, pulse oximetry oxygen consumption, and perhaps imaging
1 I. Definition: During the exercise test, the patient exercises on a bike or treadmill while being monitored with a 12 lead ECG, blood pressure device, pulse oximetry oxygen consumption, and perhaps imaging
The PAIN Pathway for the Management of Acute Coronary Syndrome
 2 The PAIN Pathway for the Management of Acute Coronary Syndrome Eyal Herzog, Emad Aziz, and Mun K. Hong Acute coronary syndrome (ACS) subsumes a spectrum of clinical entities, ranging from unstable angina
2 The PAIN Pathway for the Management of Acute Coronary Syndrome Eyal Herzog, Emad Aziz, and Mun K. Hong Acute coronary syndrome (ACS) subsumes a spectrum of clinical entities, ranging from unstable angina
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist. Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI
 Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
Acute Coronary Syndromes: Challenges to Management. Claire Williams November 2017
 Acute Coronary Syndromes: Challenges to Management Claire Williams November 2017 Challenge 1: Diagnosis Chest pain >20 minutes ECG Challenge 1: Diagnosis Treat as STEMI Chest pain >20 minutes ECG STEMI
Acute Coronary Syndromes: Challenges to Management Claire Williams November 2017 Challenge 1: Diagnosis Chest pain >20 minutes ECG Challenge 1: Diagnosis Treat as STEMI Chest pain >20 minutes ECG STEMI
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases
 Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Acute Coronary Syndrome. Sonny Achtchi, DO
 Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Goals: Widen Your Understanding of the Wide QRS!
 Goals: Widen Your Understanding of the Wide QRS! 1. Describe an approach to diagnosis of LBBB 2. Describe the predictive value of New LBBB 3. Describe the ST segment changes that are diagnostic of AMI
Goals: Widen Your Understanding of the Wide QRS! 1. Describe an approach to diagnosis of LBBB 2. Describe the predictive value of New LBBB 3. Describe the ST segment changes that are diagnostic of AMI
Acute Coronary Syndrome (ACS) Initial Evaluation and Management
 Initial Evaluation and Management") Acute Coronary Syndrome (ACS) Initial Evaluation and Management Symptoms of Possible ACS Chest discomfort with or without radiation to the arm(s), jaw, or epigastrium Short of breath Weakness Diaphoresis
Acute Coronary Syndrome (ACS) Initial Evaluation and Management Symptoms of Possible ACS Chest discomfort with or without radiation to the arm(s), jaw, or epigastrium Short of breath Weakness Diaphoresis
Richard Grocott Mason
 Richard Grocott Mason What to do with a 50 year old man with chest pain? Does the pain sound cardiac? Is this a possible acute coronary syndrome? Does patient have a previous cardiac history? Natural history
Richard Grocott Mason What to do with a 50 year old man with chest pain? Does the pain sound cardiac? Is this a possible acute coronary syndrome? Does patient have a previous cardiac history? Natural history
DISCUSSION QUESTION - 1
 CASE PRESENTATION 87 year old male No past history of diabetes, HTN, dyslipidemia or smoking Very active Medications: omeprazole for heart burn Admitted because of increasing retrosternal chest pressure
CASE PRESENTATION 87 year old male No past history of diabetes, HTN, dyslipidemia or smoking Very active Medications: omeprazole for heart burn Admitted because of increasing retrosternal chest pressure
Troponin = 35. Objectives. Low Risk Chest Pain. Does this patient have ACS? Does this patient have ACS? Objectives
 Objectives Low Risk Chest Pain Jeffrey Tabas, MD Professor of Emergency Medicine Office of CME UCSF School of Medicine Improve speed and accuracy in assessing patients with possible ACS! Avoid pitfalls
Objectives Low Risk Chest Pain Jeffrey Tabas, MD Professor of Emergency Medicine Office of CME UCSF School of Medicine Improve speed and accuracy in assessing patients with possible ACS! Avoid pitfalls
Is it safe to manage pulmonary embolism in Primary Care? Roopen Arya King s College Hospital
 Is it safe to manage pulmonary embolism in Primary Care? Roopen Arya King s College Hospital A few definitions Safe Avoid death, recurrent thrombosis, bleeding Manage Diagnosis + treatment Pulmonary embolism
Is it safe to manage pulmonary embolism in Primary Care? Roopen Arya King s College Hospital A few definitions Safe Avoid death, recurrent thrombosis, bleeding Manage Diagnosis + treatment Pulmonary embolism
Tissue Plasminogen Activator in In-Hospital Cardiac Arrest with Pulseless Electrical Activity
 Tissue Plasminogen Activator in In-Hospital Cardiac Arrest with Pulseless Electrical Activity Hannah Jordan A. Study Purpose and Rationale Pulseless electrical activity during cardiac arrest carries a
Tissue Plasminogen Activator in In-Hospital Cardiac Arrest with Pulseless Electrical Activity Hannah Jordan A. Study Purpose and Rationale Pulseless electrical activity during cardiac arrest carries a
Name Authentication Date (Position or Committee) Quality & Patient Safety Steering. Meeting Minutes & 08/14 Committee
 Quality & Patient Safety Steering. Meeting Minutes & 08/14 Committee") Title: Document Number: Document Type: Affected Departments: Review Bodies: Revision/(Review) Dates: (Dates that included only a review, but no content 07/14 revision, are in parentheses) Effective Date:
Title: Document Number: Document Type: Affected Departments: Review Bodies: Revision/(Review) Dates: (Dates that included only a review, but no content 07/14 revision, are in parentheses) Effective Date:
Difficult Data Definitions and Scenario s
 Difficult Data Definitions and Scenario s Presenter Disclosure Information Cornelia Anderson BSN, RN To following relationships exist related to this presentation: No Disclosures Objectives Discuss key
Difficult Data Definitions and Scenario s Presenter Disclosure Information Cornelia Anderson BSN, RN To following relationships exist related to this presentation: No Disclosures Objectives Discuss key
Hot Topics in Cardiac Arrest. Should the patient go To the Cath Lab?
 Hot Topics in Cardiac Arrest Should the patient go To the Cath Lab? Tim Russert 1950-2008 Host of NBC s Meet the Press Sudden Cardiac Arrest : Autopsy showed plaque rupture in his LAD ( per LA Times,
Hot Topics in Cardiac Arrest Should the patient go To the Cath Lab? Tim Russert 1950-2008 Host of NBC s Meet the Press Sudden Cardiac Arrest : Autopsy showed plaque rupture in his LAD ( per LA Times,
CARDIAC PROBLEMS IN PREGNANCY
 CARDIAC PROBLEMS IN PREGNANCY LAS VEGAS, NEVADA, USA 27 February 1 March 2016 SUCCESSFUL TREATMENT WITH RECOMBINANT TISSUE PLASMINOGEN ACTIVATOR OF MASSIVE PULMONARY EMBOLISM IN THE 16 TH WEEK OF PREGNANCY
CARDIAC PROBLEMS IN PREGNANCY LAS VEGAS, NEVADA, USA 27 February 1 March 2016 SUCCESSFUL TREATMENT WITH RECOMBINANT TISSUE PLASMINOGEN ACTIVATOR OF MASSIVE PULMONARY EMBOLISM IN THE 16 TH WEEK OF PREGNANCY
QUESTION EXAMPLES ECG
 ACEM Fellowship VAQ Examination QUESTION EXAMPLES ECG ECG 1: A 16 year old boy with a congenital heart problem presents to your ED with syncopal episodes. An ECG is taken. Describe and interpret his ECG
ACEM Fellowship VAQ Examination QUESTION EXAMPLES ECG ECG 1: A 16 year old boy with a congenital heart problem presents to your ED with syncopal episodes. An ECG is taken. Describe and interpret his ECG
Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies)
") SLO County Emergency Medical Services Agency Bulletin 2012-09 PLEASE POST Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies) July
SLO County Emergency Medical Services Agency Bulletin 2012-09 PLEASE POST Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies) July
2010 ACLS Guidelines. Primary goals of therapy for patients
 2010 ACLS Guidelines Part 10: Acute Coronary Syndrome Present : 內科 R1 鍾伯欣 Supervisor: F1 吳亮廷 991110 Primary goals of therapy for patients of ACS Reduce the amount of myocardial necrosis that occurs in
2010 ACLS Guidelines Part 10: Acute Coronary Syndrome Present : 內科 R1 鍾伯欣 Supervisor: F1 吳亮廷 991110 Primary goals of therapy for patients of ACS Reduce the amount of myocardial necrosis that occurs in
A walk through a STEMI
 A walk through a STEMI M.M. s Story Kim Robison Ashley Corcoran Situation M.M. is an 82 year old male brought in by private vehicle on 10/22/17 to the Emergency Department Pt. c/o left arm numbness, pain
A walk through a STEMI M.M. s Story Kim Robison Ashley Corcoran Situation M.M. is an 82 year old male brought in by private vehicle on 10/22/17 to the Emergency Department Pt. c/o left arm numbness, pain
PAEDIATRIC ACUTE CARE GUIDELINE. Chest Pain
 Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should be read in conjunction
Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should be read in conjunction
Medicine Dr. Omed Lecture 2 Stable and Unstable Angina
 Medicine Dr. Omed Lecture 2 Stable and Unstable Angina Risk stratification in stable angina. High Risk; *post infarct angina, *poor effort tolerance, *ischemia at low workload, *left main or three vessel
Medicine Dr. Omed Lecture 2 Stable and Unstable Angina Risk stratification in stable angina. High Risk; *post infarct angina, *poor effort tolerance, *ischemia at low workload, *left main or three vessel
Exhibit EP16.h University of Virginia Medical Center Clinical Decision Tool
 TITLE: Emergency Management for Suspicion of Cardiac Event PURPOSE: Increasingly, patients have multiple morbidities and are at risk of adverse events related or unrelated to the condition for which they
TITLE: Emergency Management for Suspicion of Cardiac Event PURPOSE: Increasingly, patients have multiple morbidities and are at risk of adverse events related or unrelated to the condition for which they
ACUTE CORONARY SYNDROME
 12 LEAD ECG INTERPRETATION in ACUTE CORONARY SYNDROME WAYNE W RUPPERT, CVT, CCCC, NREMT-P Cardiovascular Clinical Coordinator Bayfront Health Seven Rivers Crystal River, FL Education Specialist St. Joseph
12 LEAD ECG INTERPRETATION in ACUTE CORONARY SYNDROME WAYNE W RUPPERT, CVT, CCCC, NREMT-P Cardiovascular Clinical Coordinator Bayfront Health Seven Rivers Crystal River, FL Education Specialist St. Joseph
URN: Family name: Given name(s): Address: Initial Signature Print Name Role
: Address: Initial Signature Print Name Role") Do Not Write in this binding margin v5.00-02/2012 Mat. No.: 10206019 SW030b The State of Queensland (Queensland Health) 2012 Contact CIM@health.qld.gov.au ÌSW030bIÎ Facility: s Never Replace Clinical Judgement
Do Not Write in this binding margin v5.00-02/2012 Mat. No.: 10206019 SW030b The State of Queensland (Queensland Health) 2012 Contact CIM@health.qld.gov.au ÌSW030bIÎ Facility: s Never Replace Clinical Judgement
Case. Case. Management of Pulmonary Embolism in the ICU
 Management of Pulmonary Embolism in the ICU Todd M Bull, M.D. Associate Professor of Medicine Division of Pulmonary Sciences and Critical Care Medicine Pulmonary Hypertension Center University of Colorado
Management of Pulmonary Embolism in the ICU Todd M Bull, M.D. Associate Professor of Medicine Division of Pulmonary Sciences and Critical Care Medicine Pulmonary Hypertension Center University of Colorado
HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM
 REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
Cardiac Emergencies. Jim Bennett Paramedic and Clinical Education Coordinator American Medical Response Spokane, Washington
 Cardiac Emergencies Jim Bennett Paramedic and Clinical Education Coordinator American Medical Response Spokane, Washington The Heart -------Aorta Pulmonary Veins---- Superior Vena Cava------ Right Atrium-----
Cardiac Emergencies Jim Bennett Paramedic and Clinical Education Coordinator American Medical Response Spokane, Washington The Heart -------Aorta Pulmonary Veins---- Superior Vena Cava------ Right Atrium-----
Echocardiography as a diagnostic and management tool in medical emergencies
 Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Acute heart failure in a patient with lower urinary tract infection Case report of an infection-induced Reverse Takotsubo syndrome
 Acute heart failure in a patient with lower urinary tract infection Case report of an infection-induced Reverse Takotsubo syndrome N.Μoschos, A.Dimitra, E.Tsakiri, D.Stavrianakis, A.Nouli CARDIOLOGY DEPARTMENT
Acute heart failure in a patient with lower urinary tract infection Case report of an infection-induced Reverse Takotsubo syndrome N.Μoschos, A.Dimitra, E.Tsakiri, D.Stavrianakis, A.Nouli CARDIOLOGY DEPARTMENT
October 2017 Pulmonary Embolism
 October 2017 Pulmonary Embolism Prof. Ahmed BaHammam, FRCP, FCCP Professor of Medicine College of Medicine King Saud University 1 Objectives Epidemiology Pathophysiology Diagnosis Massive PE Treatment
October 2017 Pulmonary Embolism Prof. Ahmed BaHammam, FRCP, FCCP Professor of Medicine College of Medicine King Saud University 1 Objectives Epidemiology Pathophysiology Diagnosis Massive PE Treatment
A 50-year-old woman with syncope
 Hira Shahzad 1, Ali Bin Sarwar Zubairi 2 1 Medical College, Aga Khan University Hospital, Karachi 2 Department of Medicine, Aga Khan University Hospital, Karachi, Pakistan Ali Bin Sarwar Zubairi Associate
Hira Shahzad 1, Ali Bin Sarwar Zubairi 2 1 Medical College, Aga Khan University Hospital, Karachi 2 Department of Medicine, Aga Khan University Hospital, Karachi, Pakistan Ali Bin Sarwar Zubairi Associate
STEMI and Cardiogenic Shock. The rules and solution. Dave Kettles St Dominics and Frere Hospitals East London ZA
 STEMI and Cardiogenic Shock. The rules and solution Dave Kettles St Dominics and Frere Hospitals East London ZA Definitions: Shock is a life threatening, but initially reversible state of cellular and
STEMI and Cardiogenic Shock. The rules and solution Dave Kettles St Dominics and Frere Hospitals East London ZA Definitions: Shock is a life threatening, but initially reversible state of cellular and
TROPONIN POSITIVE 2/20/2015 WHAT DOES IT MEAN? When should a troponin level be obtained?
 TROPONIN POSITIVE WHAT DOES IT MEAN? Frequently Asked Questions Regarding the Use of Troponin in the Clinical Setting What does an elevated troponin level mean? Elevated troponin is a sensitive and specific
TROPONIN POSITIVE WHAT DOES IT MEAN? Frequently Asked Questions Regarding the Use of Troponin in the Clinical Setting What does an elevated troponin level mean? Elevated troponin is a sensitive and specific
Chest pain investigation, diagnosis and treatment How to manage a patient presenting with chest pain This page explains how to approach a patient
 Chest pain investigation, diagnosis and treatment How to manage a patient presenting with chest pain This page explains how to approach a patient with chest pain, focusing on the immediate investigations,
Chest pain investigation, diagnosis and treatment How to manage a patient presenting with chest pain This page explains how to approach a patient with chest pain, focusing on the immediate investigations,
IFT1 Interfacility Transfer of STEMI Patients. IFT2 Interfacility Transfer of Intubated Patients. IFT3 Interfacility Transfer of Stroke Patients
 IFT1 Interfacility Transfer of STEMI Patients IFT2 Interfacility Transfer of Intubated Patients IFT3 Interfacility Transfer of Stroke Patients Interfacility Transfer Guidelines IFT 1 TRANSFER INTERFACILITY
IFT1 Interfacility Transfer of STEMI Patients IFT2 Interfacility Transfer of Intubated Patients IFT3 Interfacility Transfer of Stroke Patients Interfacility Transfer Guidelines IFT 1 TRANSFER INTERFACILITY
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014
 Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
HEART CONDITIONS IN SPORT
 HEART CONDITIONS IN SPORT Dr. Anita Green CHD Risk Factors Smoking Hyperlipidaemia Hypertension Obesity Physical Inactivity Diabetes Risks are cumulative (multiplicative) Lifestyles predispose to RF One
HEART CONDITIONS IN SPORT Dr. Anita Green CHD Risk Factors Smoking Hyperlipidaemia Hypertension Obesity Physical Inactivity Diabetes Risks are cumulative (multiplicative) Lifestyles predispose to RF One
Epidemiology. Update on Pulmonary Embolism. Keys to PE Management 5/5/2014. Diagnosis. Risk stratification. Treatment
 Update on Pulmonary Embolism Steven M. Dean, DO, FACP, RPVI Program Director- Vascular Medicine Associate Professor of Internal Medicine Division of Cardiovascular Medicine The Ohio State University Keys
Update on Pulmonary Embolism Steven M. Dean, DO, FACP, RPVI Program Director- Vascular Medicine Associate Professor of Internal Medicine Division of Cardiovascular Medicine The Ohio State University Keys
Objectives. Identify early signs and symptoms of Acute Coronary Syndrome Initiate proper protocol for ACS patient 10/2013 2
 10/2013 1 Objectives Identify early signs and symptoms of Acute Coronary Syndrome Initiate proper protocol for ACS patient 10/2013 2 Purpose of this Education Module: Chest Pain Center Accreditation involves
10/2013 1 Objectives Identify early signs and symptoms of Acute Coronary Syndrome Initiate proper protocol for ACS patient 10/2013 2 Purpose of this Education Module: Chest Pain Center Accreditation involves
CABG Surgery following STEMI
 CABG Surgery following STEMI Susana Harrington, MS,APRN-NP Cardio-Thoracic Surgery Nebraska Methodist Hospital February 15, 2018 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction:
CABG Surgery following STEMI Susana Harrington, MS,APRN-NP Cardio-Thoracic Surgery Nebraska Methodist Hospital February 15, 2018 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction:
Venous Thromboembolism (VTE)
") Venous Thromboembolism (VTE) Nursing A guide for patients and carers Contents Why do blood clots form in veins?... 1 How common is a deep vein thrombosis (DVT) or pulmonary embolus (PE)?... 2 How are DVTs/
Venous Thromboembolism (VTE) Nursing A guide for patients and carers Contents Why do blood clots form in veins?... 1 How common is a deep vein thrombosis (DVT) or pulmonary embolus (PE)?... 2 How are DVTs/
Policy Register No: Status: Public. Contributes to Care Quality Commission Outcome 4
 Operational Policy for Transfer of ST Elevation MI (STEMI) patients to Essex Cardiothoracic Centre (ECTC) for Primary Percutaneous Coronary Intervention Policy Register No: 09122 Status: Public Developed
Operational Policy for Transfer of ST Elevation MI (STEMI) patients to Essex Cardiothoracic Centre (ECTC) for Primary Percutaneous Coronary Intervention Policy Register No: 09122 Status: Public Developed
TOPICS IN EMERGENCY MEDICINE SEMI-FINAL
 RISK ASSESSMENT IN PATIENTS WITH CHEST PAIN Nora Goldschlager, M.D. FACP, FACC, FAHA, FHRS Cardiology - San Francisco General Hospital UCSF Disclosures: None 1 CHEST PAIN NOT DUE TO MYOCARDIAL ISCHEMIA
RISK ASSESSMENT IN PATIENTS WITH CHEST PAIN Nora Goldschlager, M.D. FACP, FACC, FAHA, FHRS Cardiology - San Francisco General Hospital UCSF Disclosures: None 1 CHEST PAIN NOT DUE TO MYOCARDIAL ISCHEMIA
Avoiding Pitfalls In PE
 UC SF Avoiding Pitfalls In PE Jeffrey Tabas, MD Professor UCSF School of Medicine Emergency Department San Francisco General Hospital sf g h Disclosure No Financial Relationships to Disclose No significant
UC SF Avoiding Pitfalls In PE Jeffrey Tabas, MD Professor UCSF School of Medicine Emergency Department San Francisco General Hospital sf g h Disclosure No Financial Relationships to Disclose No significant
Chest pain management. Ruvin Gabriel and Niels van Pelt August 2011
 Chest pain management Ruvin Gabriel and Niels van Pelt August 2011 Introduction Initial assessment Case 1 Case 2 and 3 Comparison of various diagnostic techniques Summary 1-2 % of GP consultations are
Chest pain management Ruvin Gabriel and Niels van Pelt August 2011 Introduction Initial assessment Case 1 Case 2 and 3 Comparison of various diagnostic techniques Summary 1-2 % of GP consultations are
Myocardial Infarction In Dr.Yahya Kiwan
 Myocardial Infarction In 2007 Dr.Yahya Kiwan New Definition Of Acute Myocardial Infarction The term of myocardial infarction should be used when there is evidence of myocardial necrosis in a clinical setting
Myocardial Infarction In 2007 Dr.Yahya Kiwan New Definition Of Acute Myocardial Infarction The term of myocardial infarction should be used when there is evidence of myocardial necrosis in a clinical setting
Diagnosis and Treatment of Pulmonary Embolism: High-Tech versus Low- Tech, which way to go?
 Diagnosis and Treatment of Pulmonary Embolism: High-Tech versus Low- Tech, which way to go? Philip S. Wells MD, FRCPC, MSc Professor Chair and Chief, Department of Medicine, University of Ottawa DISCLOSURE
Diagnosis and Treatment of Pulmonary Embolism: High-Tech versus Low- Tech, which way to go? Philip S. Wells MD, FRCPC, MSc Professor Chair and Chief, Department of Medicine, University of Ottawa DISCLOSURE
Acute coronary syndrome (ACS) is a potentially
 is a potentially") DIAGNOSING ACUTE CORONARY SYNDROME AND DETERMINING PATIENT RISK Edith A. Nutescu, PharmD* ABSTRACT Acute coronary syndrome is a form of coronary artery disease and has a broad range of clinical presentations.
DIAGNOSING ACUTE CORONARY SYNDROME AND DETERMINING PATIENT RISK Edith A. Nutescu, PharmD* ABSTRACT Acute coronary syndrome is a form of coronary artery disease and has a broad range of clinical presentations.
Cardiovascular Emergencies: Diagnosis and Immediate Management
 Cardiovascular Emergencies: Diagnosis and Immediate Management Royal College of Psychiatrists 11 th September 2017 Dr Rob Hatrick Consultant Cardiologist Western Sussex Hospitals NHS Foundation Trust Mental
Cardiovascular Emergencies: Diagnosis and Immediate Management Royal College of Psychiatrists 11 th September 2017 Dr Rob Hatrick Consultant Cardiologist Western Sussex Hospitals NHS Foundation Trust Mental
The spectrum of clinical outcome of PE
 Practical treatment approach for patients with PE Cecilia Becattini University of Perugia The spectrum of clinical presentation of PE PE-related shock Mild clinical symptoms The spectrum of clinical outcome
Practical treatment approach for patients with PE Cecilia Becattini University of Perugia The spectrum of clinical presentation of PE PE-related shock Mild clinical symptoms The spectrum of clinical outcome
STAT 12 Lead ECG Workshop: Basics & ACS
 STAT 12 Lead ECG Workshop: Basics & ACS Part 2: Acute Coronary Syndrome WAYNE W RUPPERT, CVT, CCCC, NREMT-P Cardiovascular Coordinator Bayfront Health Seven Rivers Crystal River, Florida Interventional
STAT 12 Lead ECG Workshop: Basics & ACS Part 2: Acute Coronary Syndrome WAYNE W RUPPERT, CVT, CCCC, NREMT-P Cardiovascular Coordinator Bayfront Health Seven Rivers Crystal River, Florida Interventional