ACUTE CORONARY SYNDROME
|
|
|
- Nancy Lynch
- 5 years ago
- Views:
Transcription




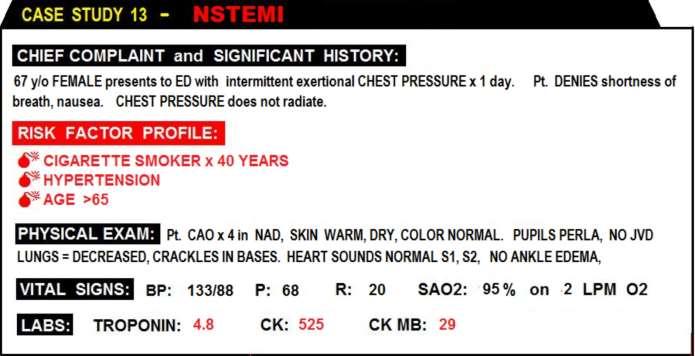
1 12 LEAD ECG INTERPRETATION in ACUTE CORONARY SYNDROME WAYNE W RUPPERT, CVT, CCCC, NREMT-P Cardiovascular Clinical Coordinator Bayfront Health Seven Rivers Crystal River, FL Education Specialist St. Joseph s Hospital Tampa, FL Copyright, 2010, 2015 Wayne W Ruppert
2
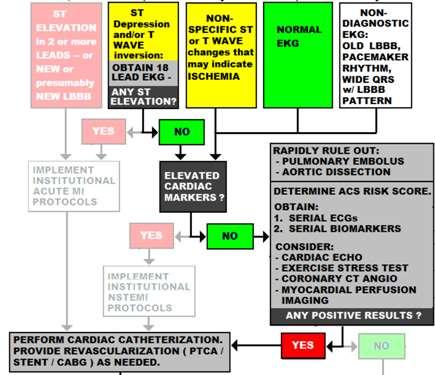
3 IDENTIFY and MANAGE ACUTE CORONARY SYNDROMES: STEMI NON-STEMI UNSTABLE ANGINA CP-LOW RISK

4
5
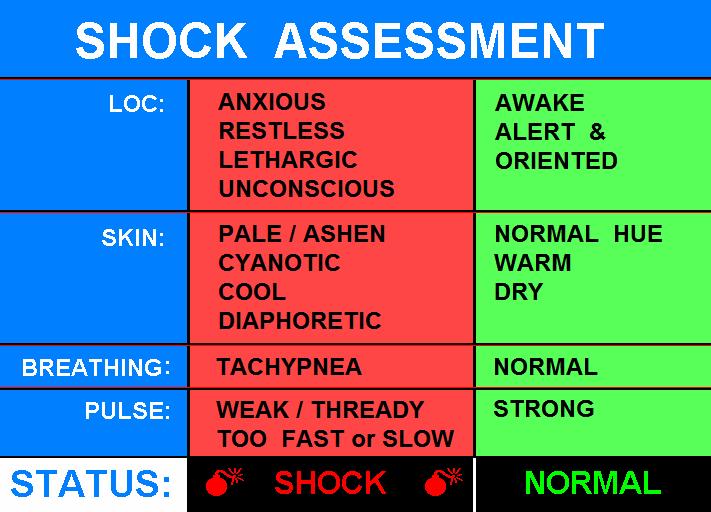
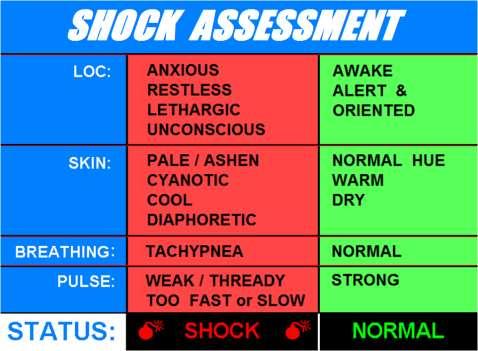
6 PATIENT EVALUATION INITIAL APPROACH (SHOCK SURVEY) ABCs CHIEF COMPLAINT SECONDARY EVALUATION RAPID, FOCUSED ASSESSMENT PAIN / PRESSURE / BREATHING / SYMPTOMS?
7
8
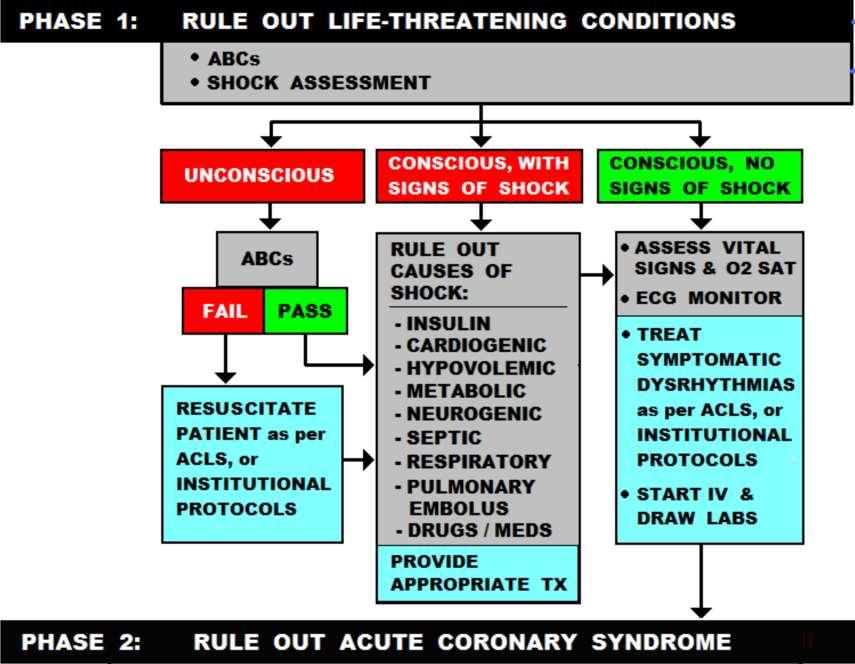
9 FAIL the SHOCK SURVEY? F RAPIDLY FIND AND TREAT THE ROOT CAUSE... WORK TO RAPIDLY IDENTIFY THE CAUSE OF SHOCK.
10

11 PASSED SHOCK SURVEY:..... Move on to RULING OUT ACS By conducting the... INITIAL EVALUATION: 1. ASSESSMENT 2. RISK STRATIFICATION 3. ECG 4. CARDIAC MARKERS ON-GOING E.D. EVALUATION -REPEAT EKGs -REPEAT CARDIAC MARKERS BOOK PAGE: 68
12
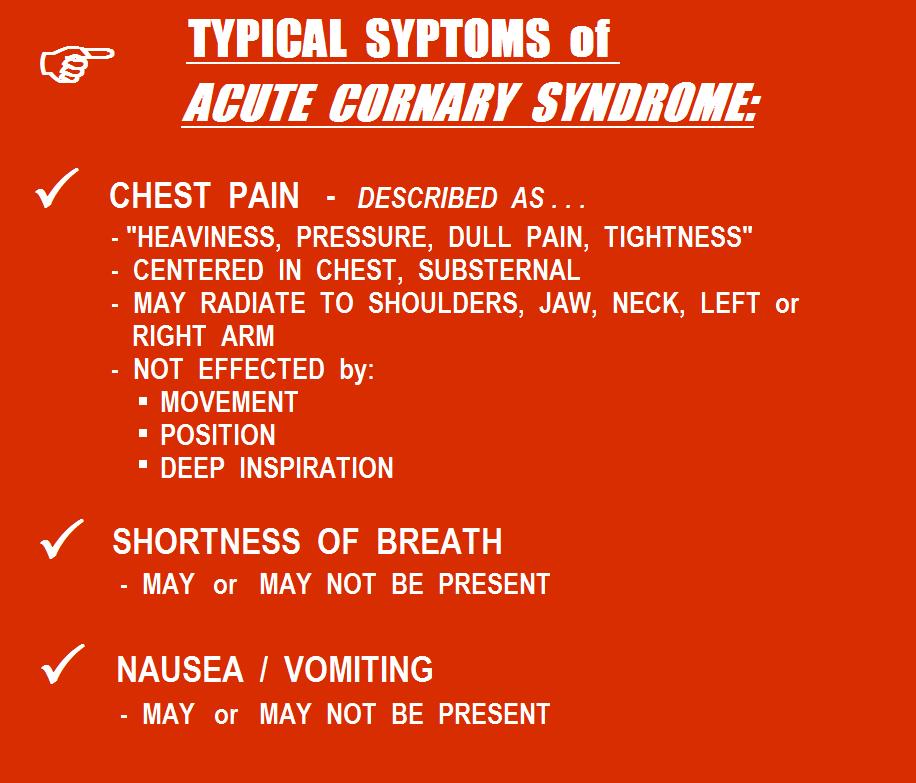
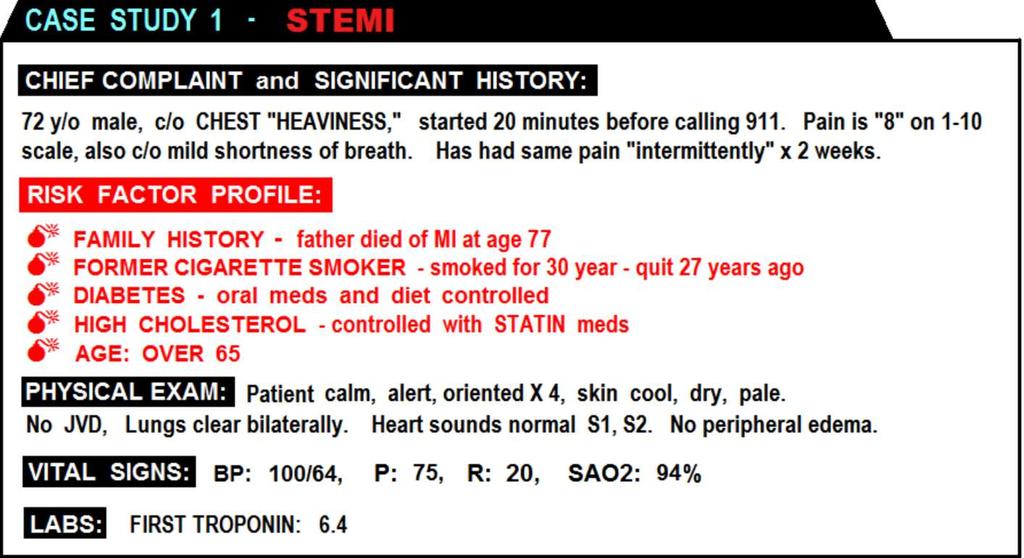
13 CHIEF COMPLAINT KEY WORDS: CHEST: PAIN / HEAVINESS / PRESSURE/ FUNNY FEELING IN, etc. SHORTNESS BREATH DIZZINESS / LIGHTHEADEDNESS ETC. ETC. ETC.
14
15

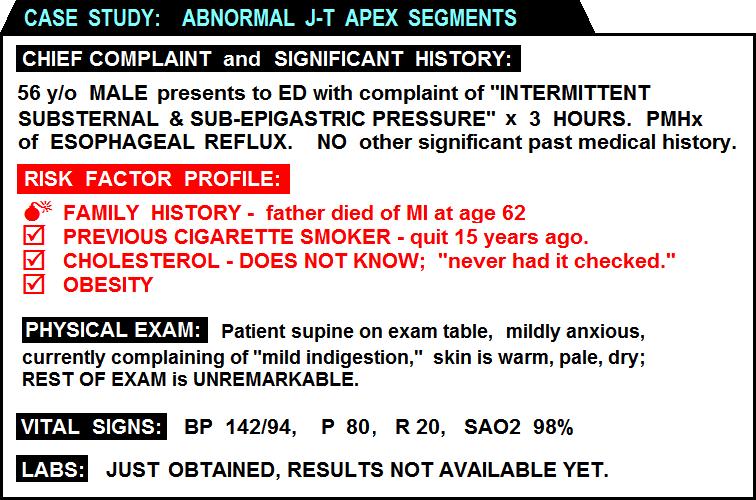
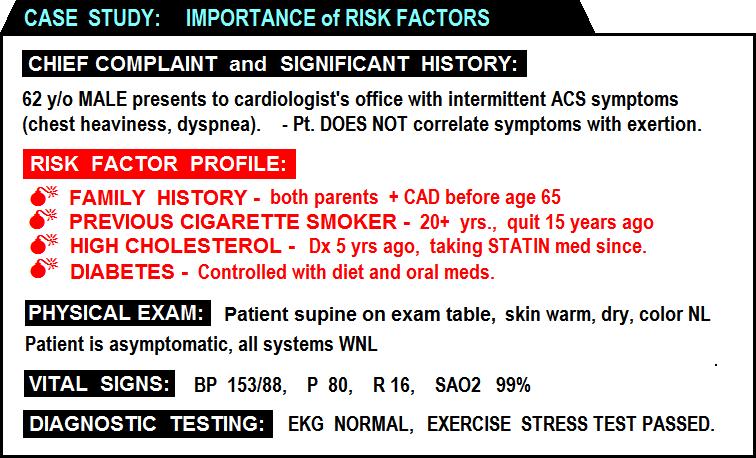
16 BEWARE of the patient with INTERMITTENT CHEST PAIN.... M
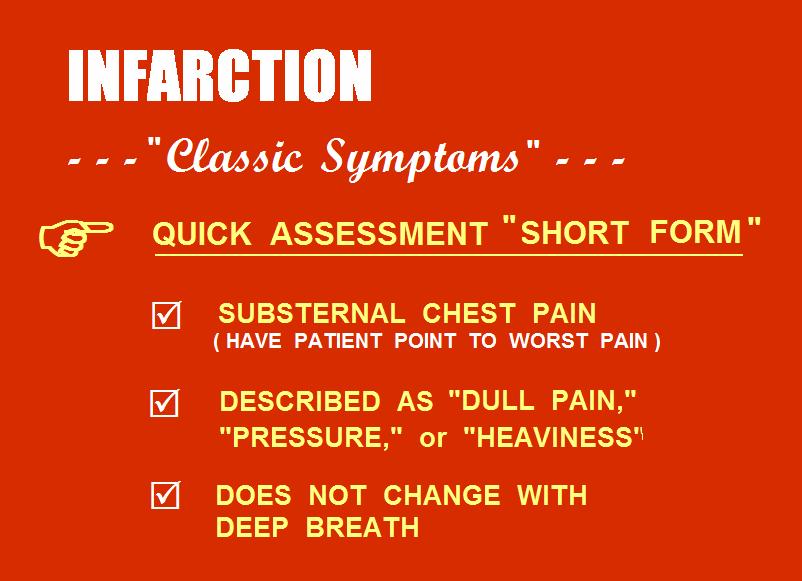
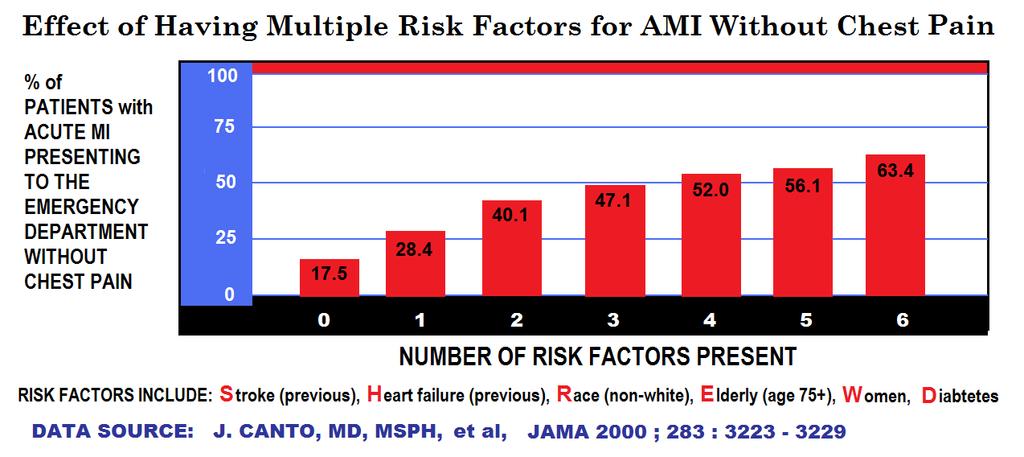
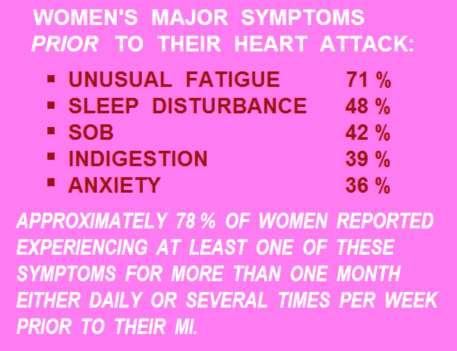
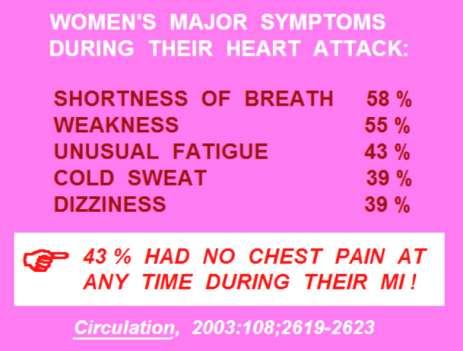
17 ATYPICAL SYMPTOMS of ACS???
18 BOOK PAGE: 70
19
20
21
22

23
24
25 TROPONIN IS NEGATIVE.
26
27
28
29
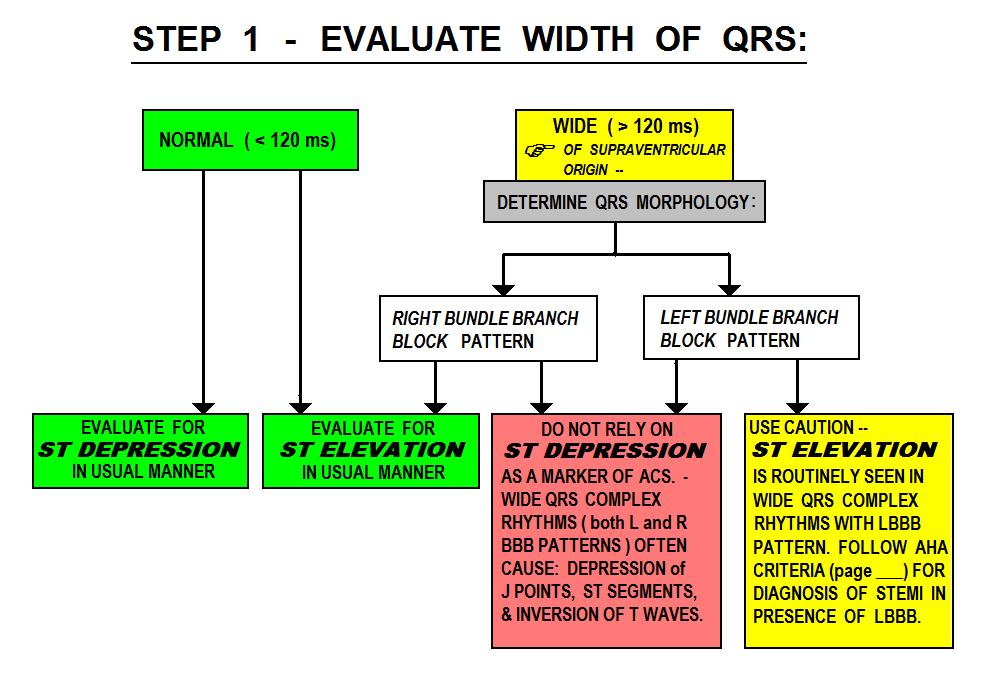
30 ECG EVALUATION for ACS: STEP 1: EVALUATE WIDTH of QRS BOOK PAGE: 73
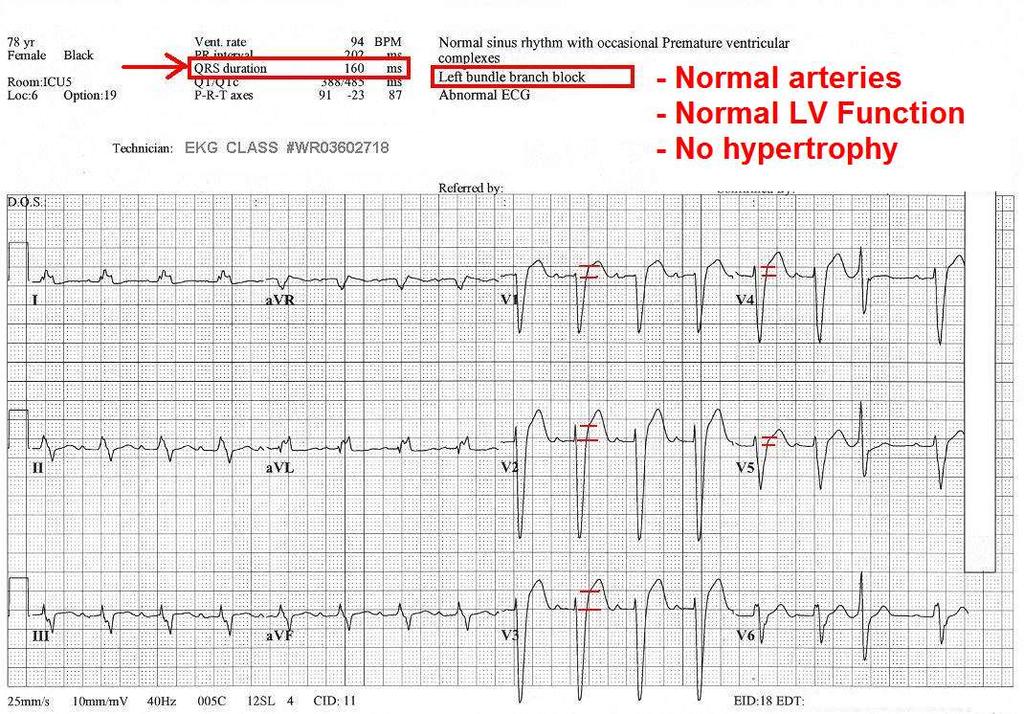
31 IF THE QRS IS TOO WIDE ( GREATER THAN 120 ms ).... IS the QRS morphology: LEFT BUNDLE BRANCH BLOCK - OR - RIGHT BUNDLE BRANCH BLOCK?????

32 WIDE QRS COMPLEXES ALTER THE -J POINTS -ST SEGMENTS -T WAVES Of the ECG... BOOK PAGE: 74
33
34
35
36
37
38
39
40
41
42
43 IF THE QRS COMPLEXES ON THE EKG ARE OF NORMAL WIDTH (<120 ms) : BOOK PAGE: 80
44

45 ALL KINDS of WEIRD ST SEGMENT and T WAVE VARIATIONS.... ALL CAN SPELL T-R-O-U-B-L-E. IF IT S NOT NORMAL, it s ABNORMAL! BOOK PAGE: 83
46
47
48
49
50


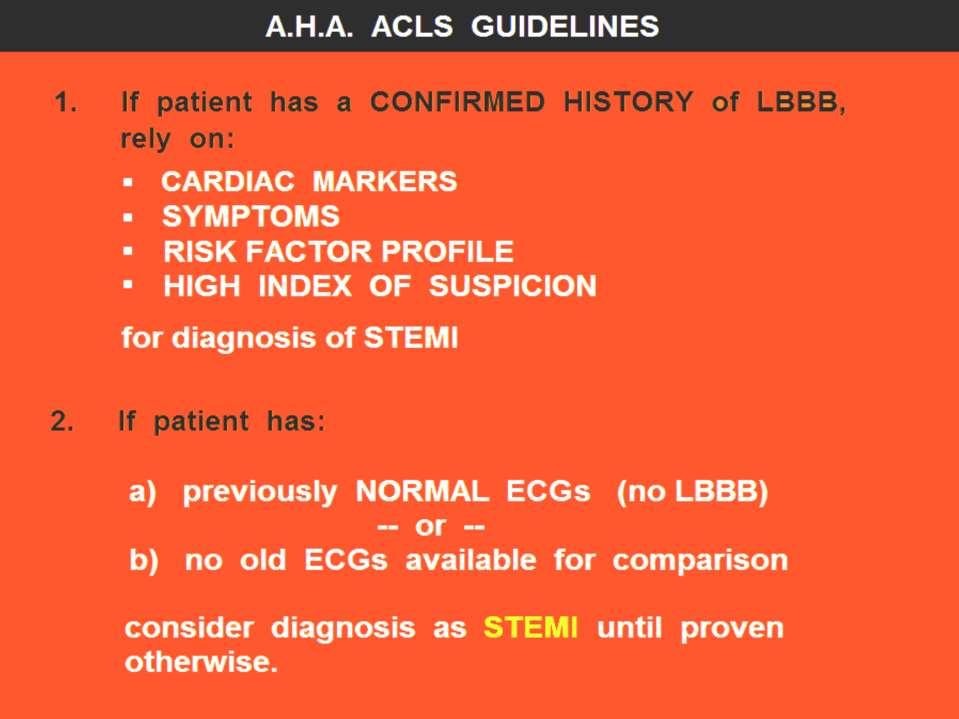
51 WHEN EVALUATING for ST SEGMENT ELEVATION From: AMERICAN HEART ASSOCIATION ACLS 2005 REVISIONS
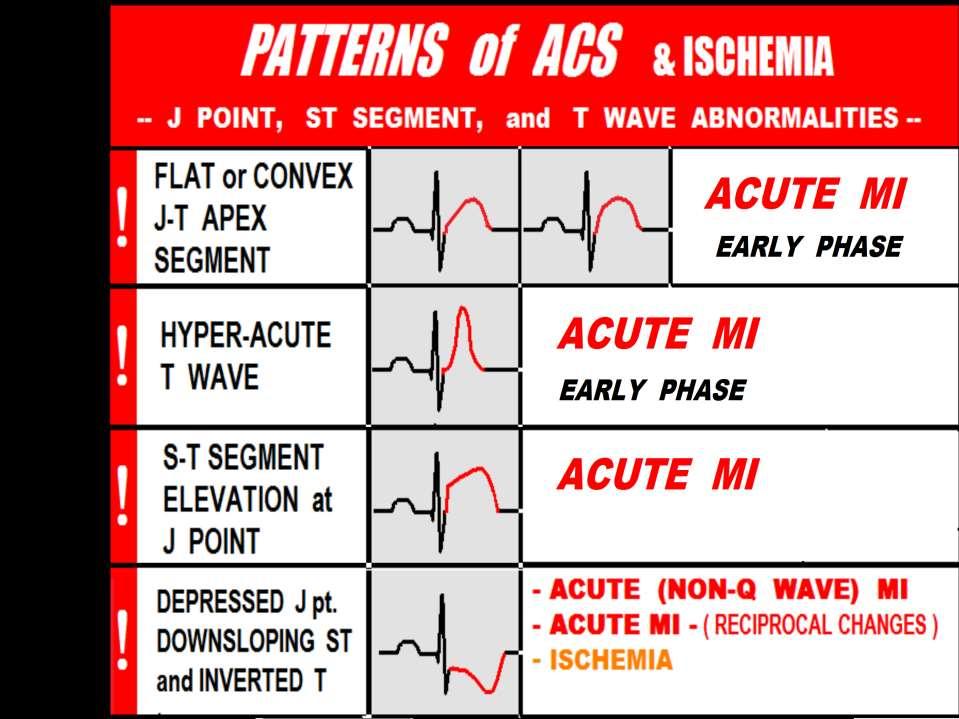
52


53
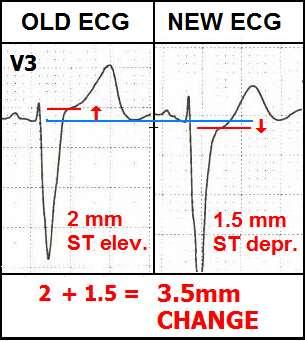
54

55 ECG COMPUTER DOES NOT NOTICE THE CONVEX J-T APEX SEGMENTS!
56
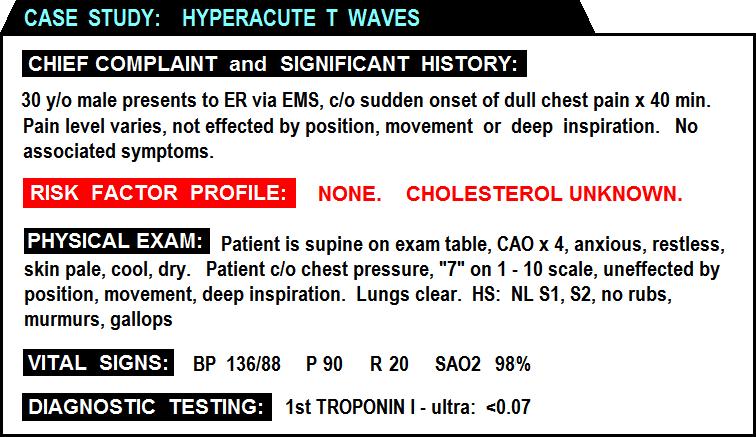
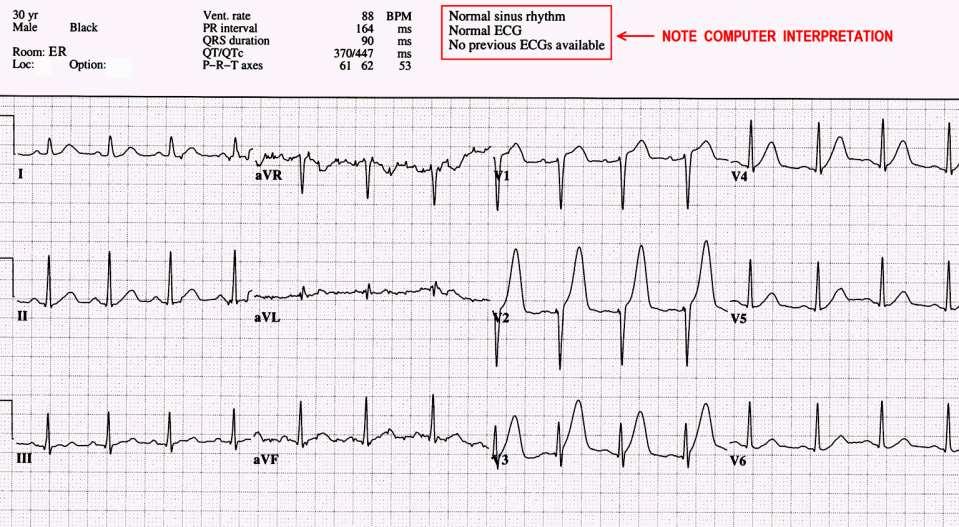
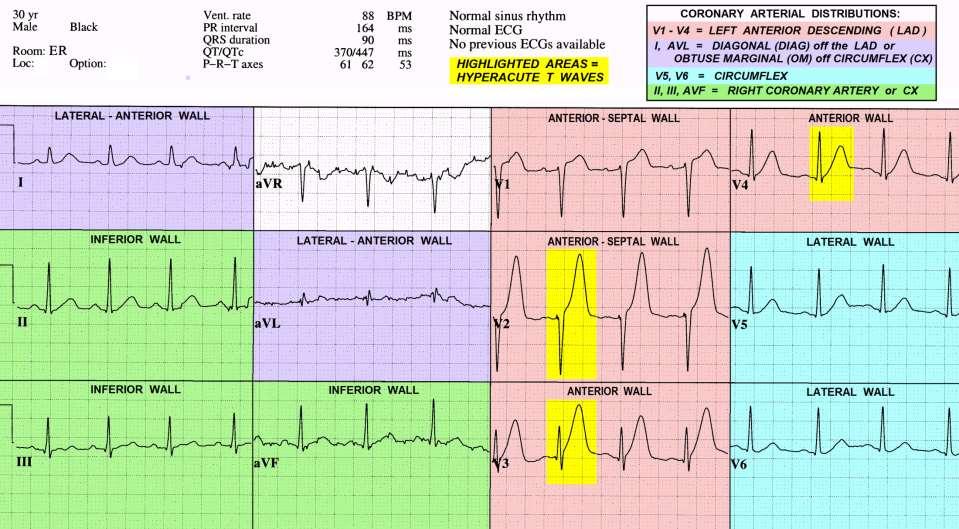
57
58
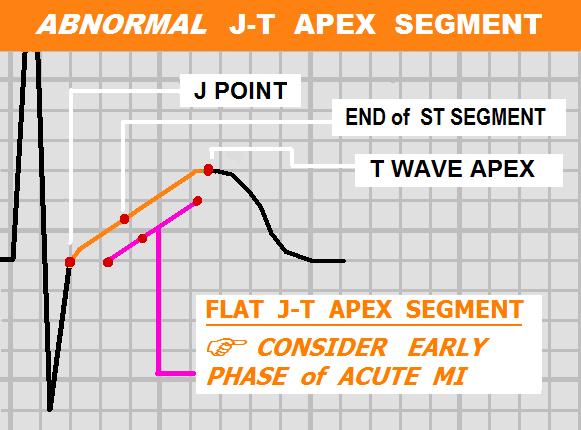
59 ECG Patterns associated with EARLY PHASE MI: J-T Apex abnormalities Dynamic ST-T Wave Changes on Serial ECGs
60




61 3. Dynmamic ST-T Wave Changes in Serial ECGs. Recorded at SRRMC 1 st ECG 2 nd ECG 1 st ECG 2 nd ECG

62 Acute In-Stent Thrombus Proximal LAD
63
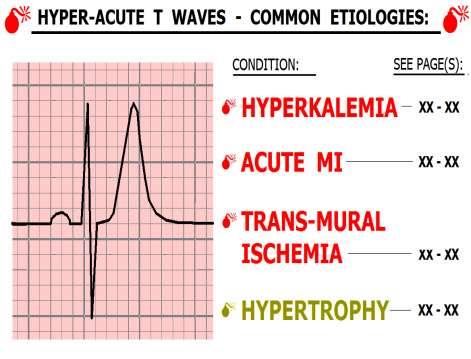
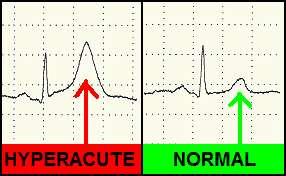
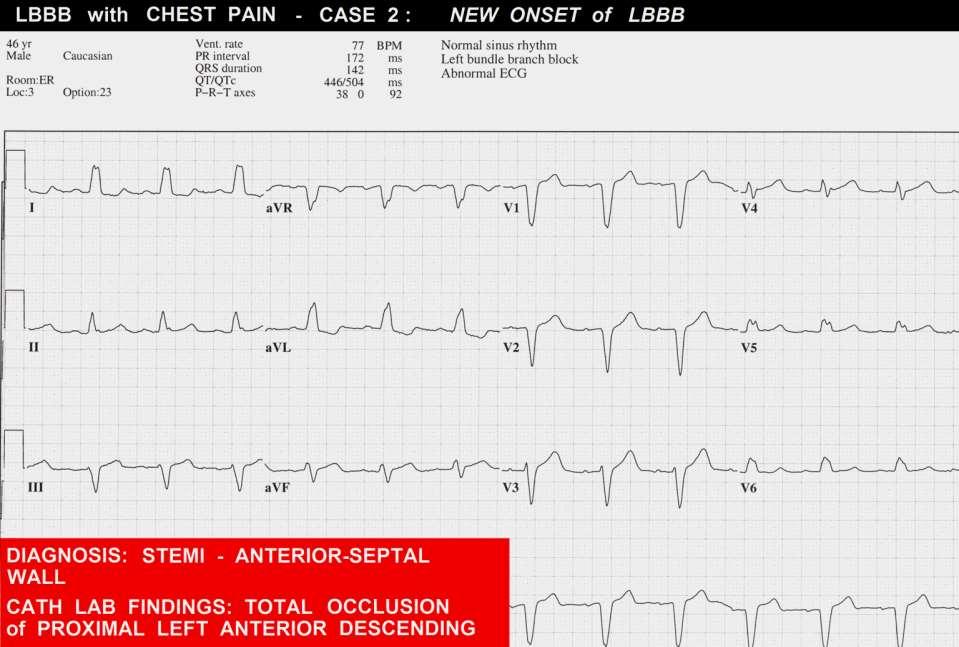
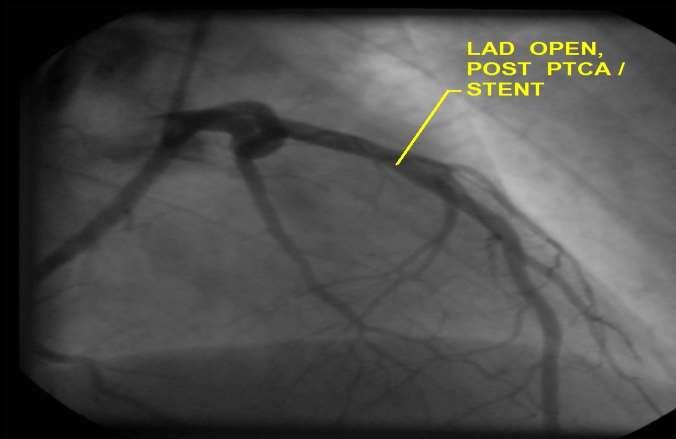
64 HYPERACUTE T WAVES BOOK PAGE: 88
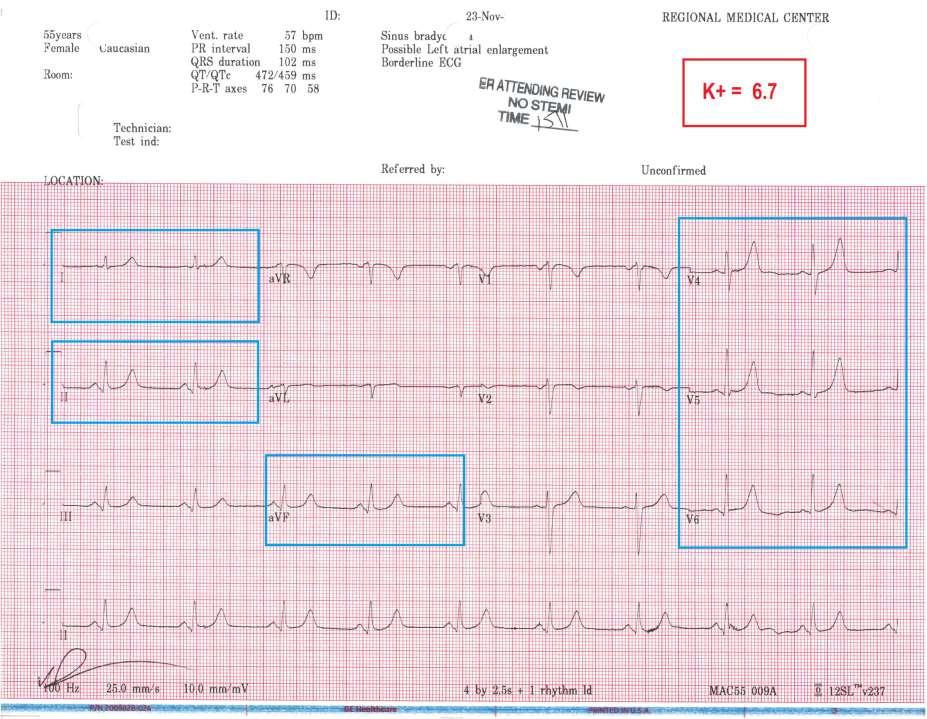
65 Helpful Clue: Hyper-Acute T Waves GLOBAL Hyper-acute T Waves (in leads viewing multiple myocardial regions / arterial distributions) favors HYPERKALEMIA
66
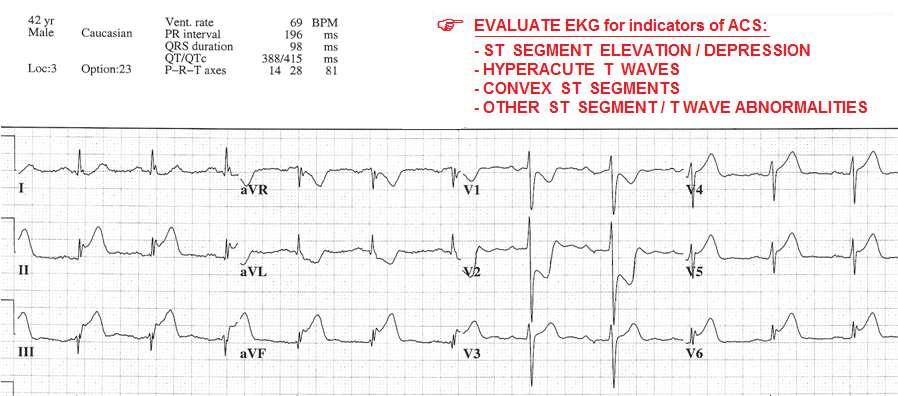
67 Helpful Clue: Hyper-Acute T Waves GLOBAL Hyper-acute T Waves (in leads viewing multiple myocardial regions / arterial distributions) favors HYPERKALEMIA Hyper-acute T Wave noted in ONE ARTERIAL DISTRIBUTION ( Anterior / Lateral / Inferior ) favors TRANSMURAL ISCHEMIA / Early Phase Acute MI
68
69
70

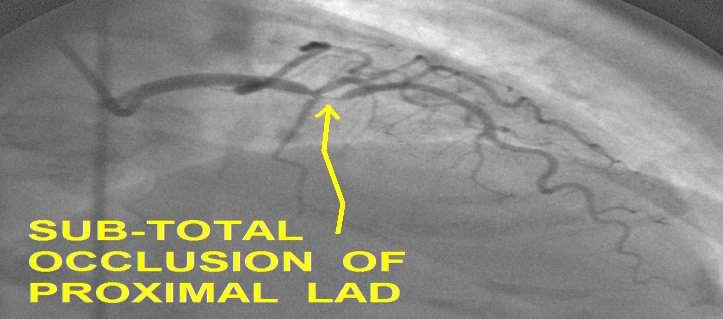
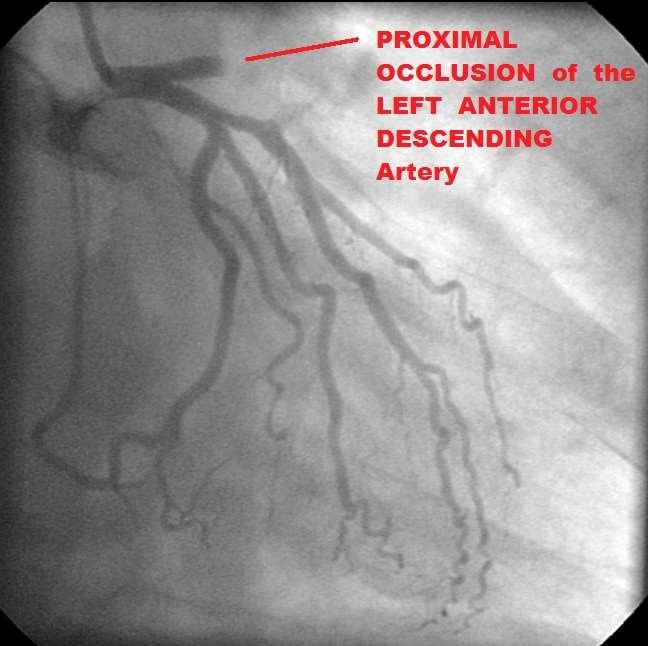
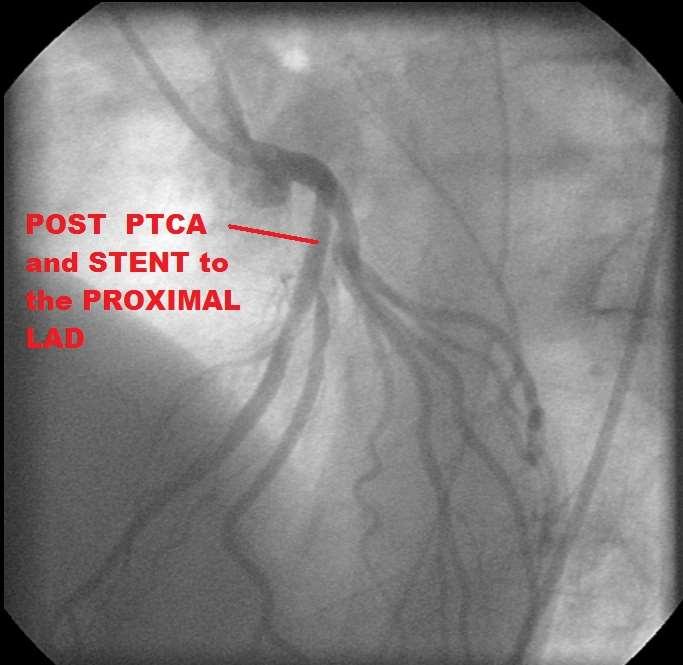
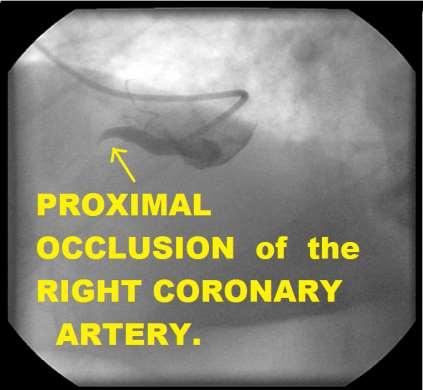
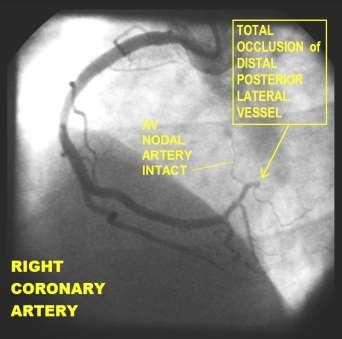
71 Cath Lab findings:
72
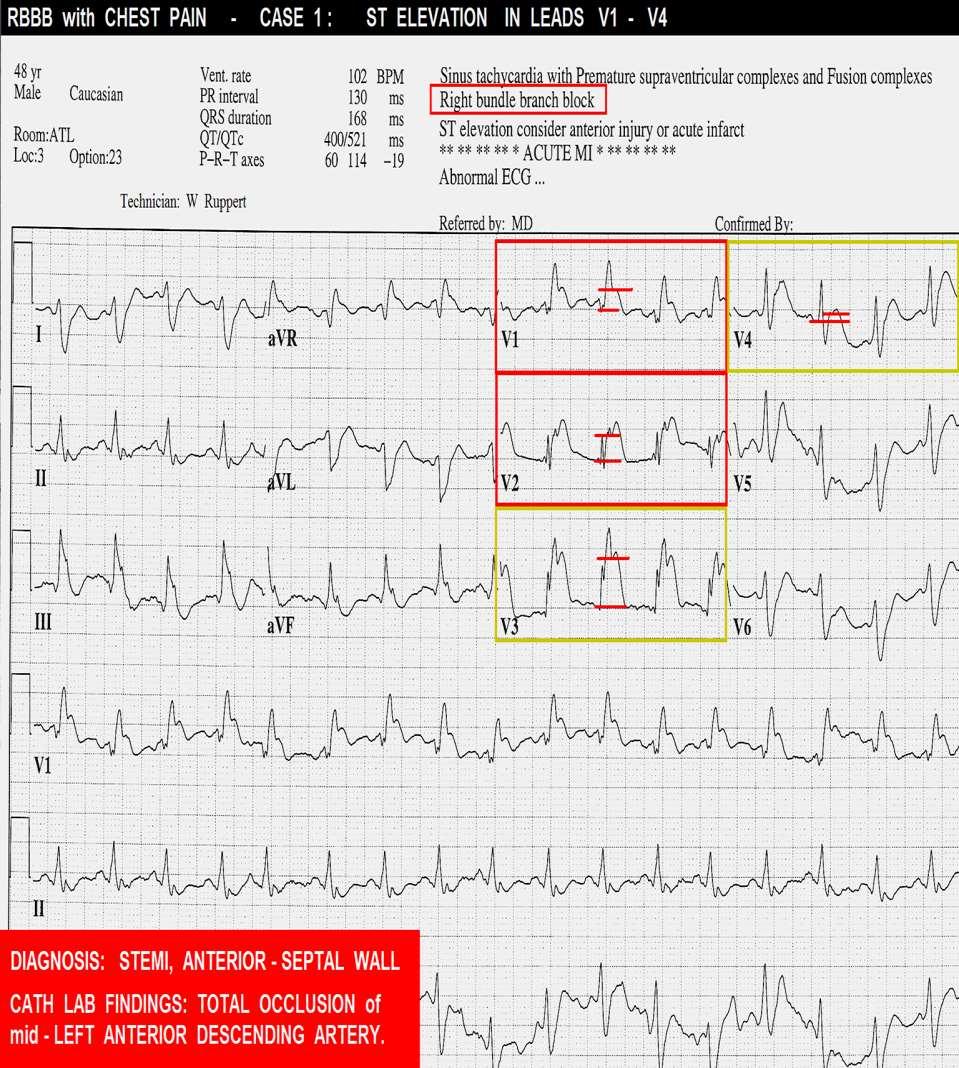
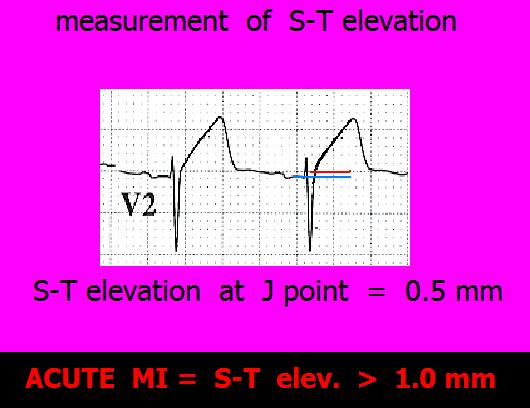
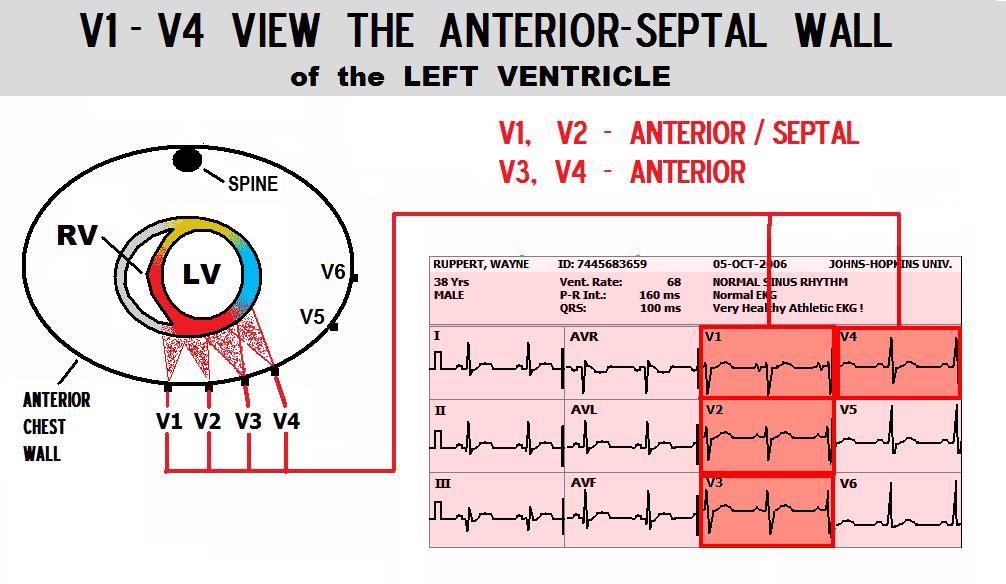
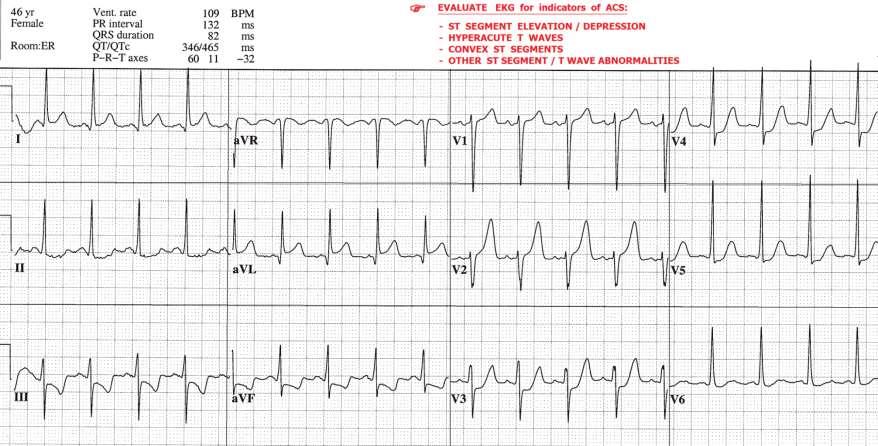
73 ECG CRITERIA for DIAGNOSIS of STEMI: (ST J POINT) *LEADS V2 and V3: MALES AGE 40 and up mm (MALES LESS THAN mm) FEMALES mm ALL OTHER LEADS: 1.0 mm or more, in TWO or more CONTIGUOUS LEADS * P. Rautaharju et al, Standardization and Interpretation of the ECG, JACC 2009;(53)No.11:

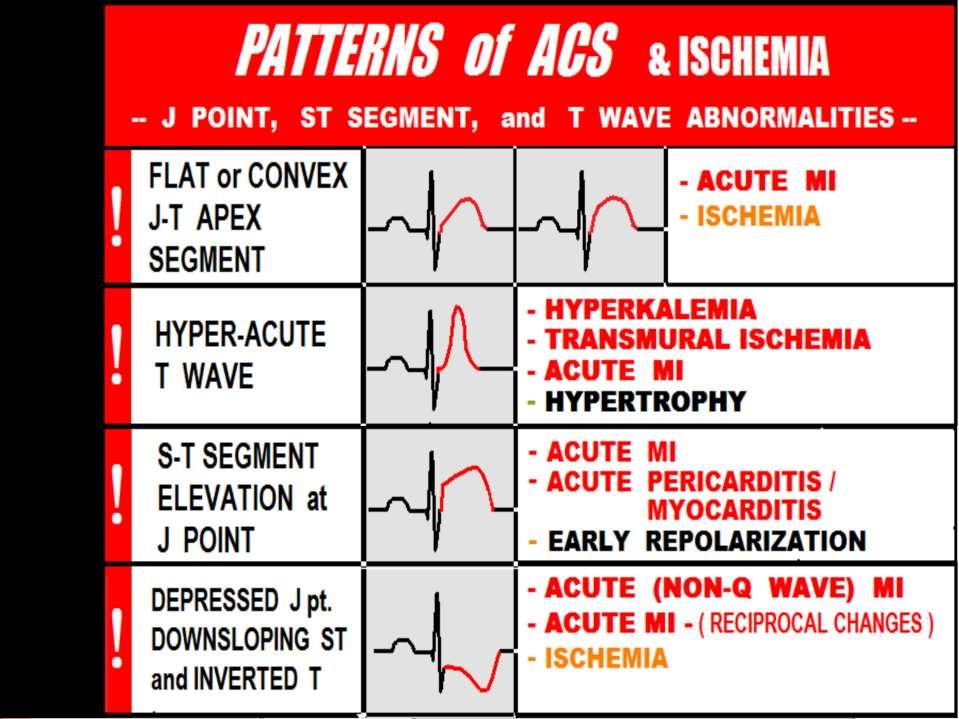
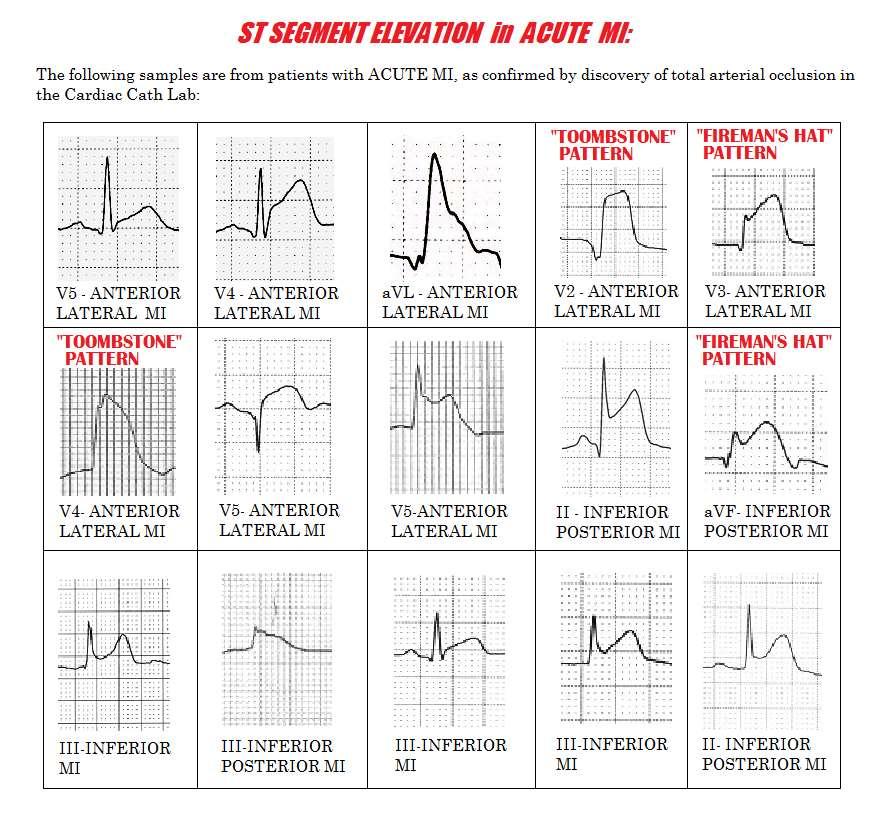
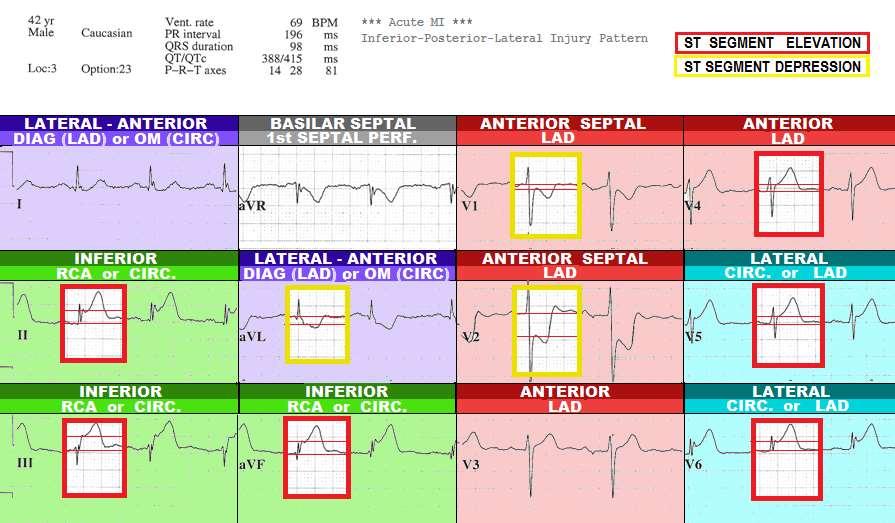
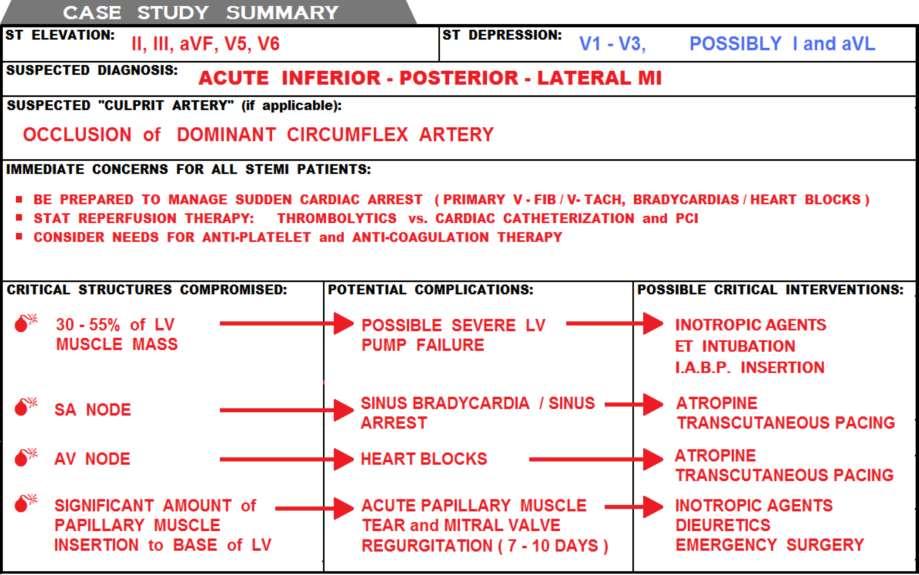
74 ST SEGMENT ELEVATION: 3 COMMON PATTERNS of ST SEGMENT ELEVATION From ACUTE MI:
75
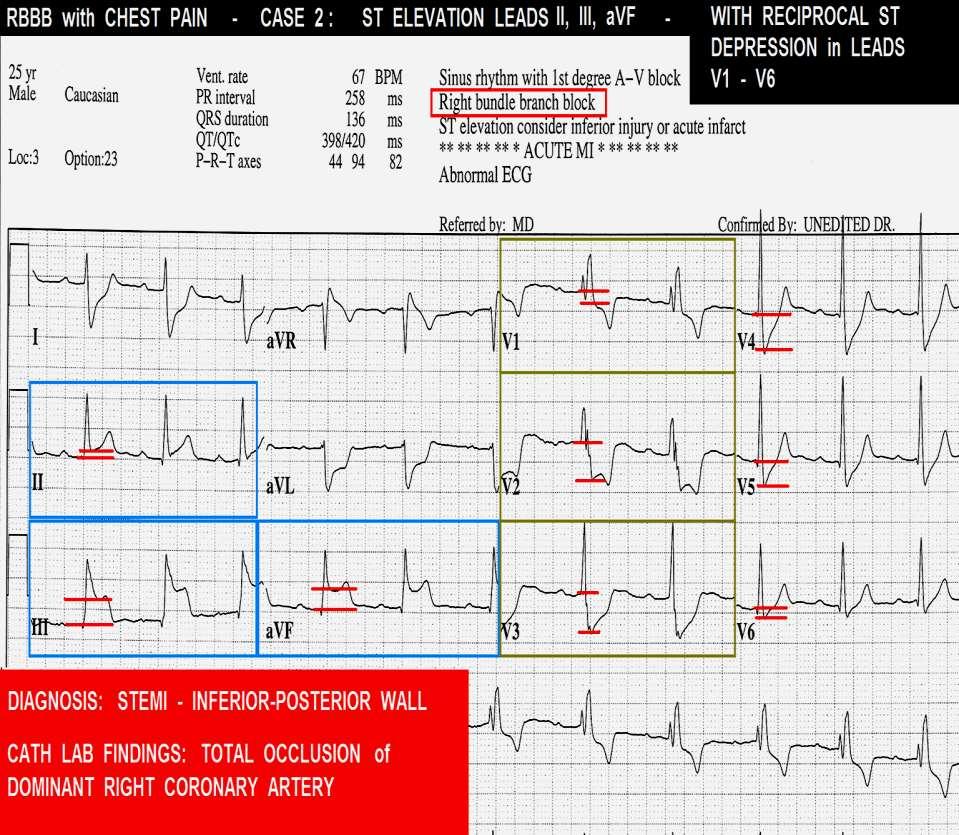
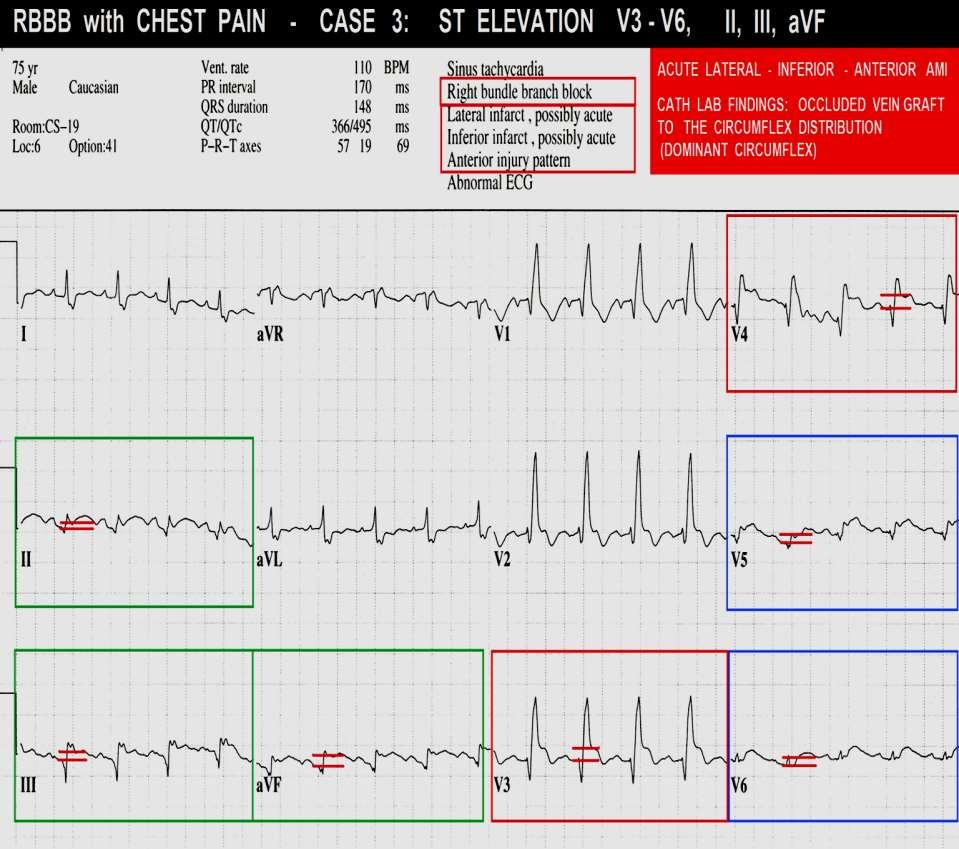
76 Reciprocal S-T Segment Depression may or may not be present during AMI. The presence of S-T Depression on an EKG which exhibits significant S-T elevation is a fairly reliable indicator that AMI is the diagnosis. However the lack of Reciprocal S-T Depression DOES NOT rule out AMI.
77
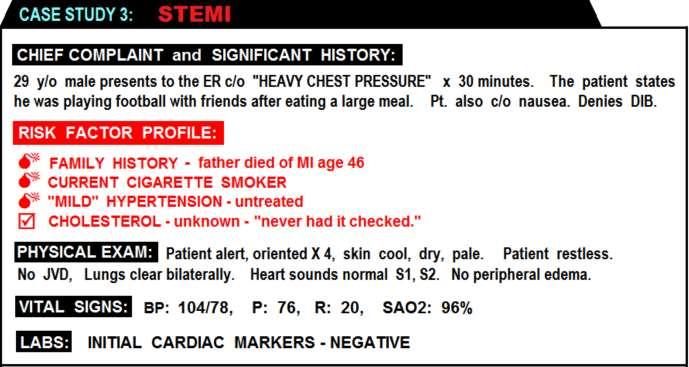
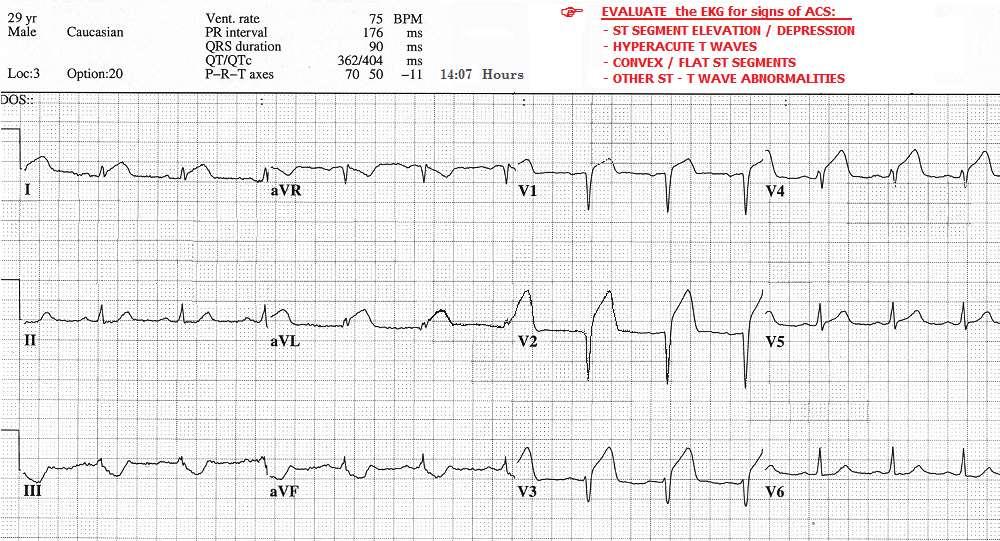
78 STEMI CASE STUDIES
79
80
81
82
83

84
85
86
87
88
89
90
91
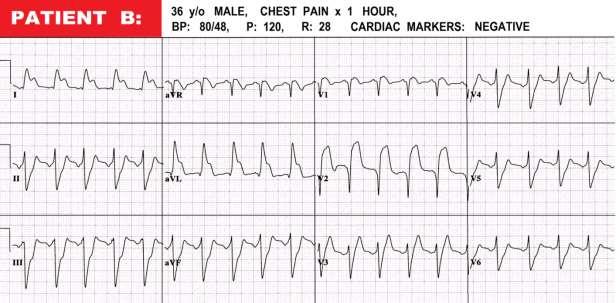
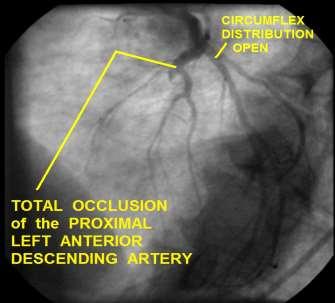
92
93




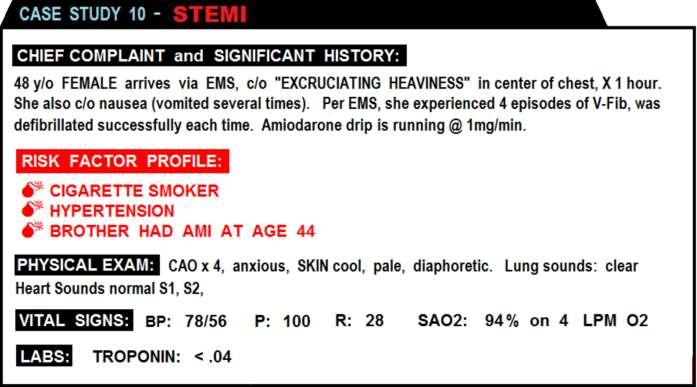
94 CASE PROGRESSION: As the patient was being prepared for transport to the Cardiac Cath Lab, she experienced an episode of Ventricular Fibrillation.
95
96
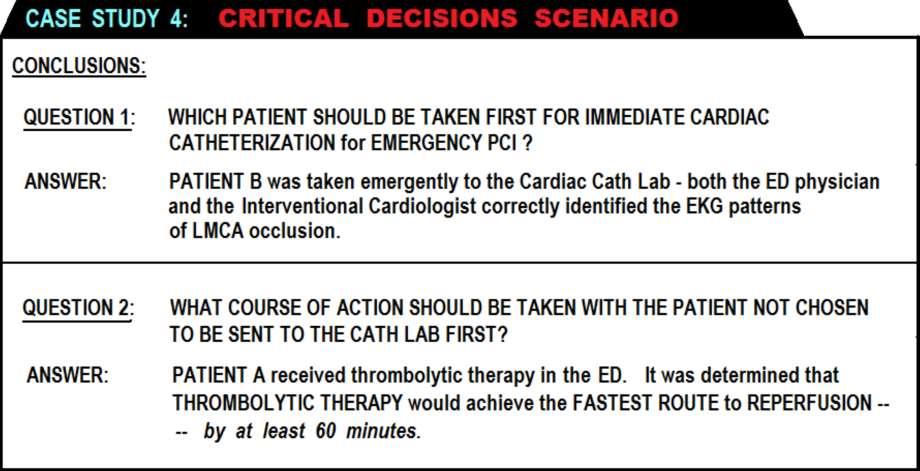
97
98

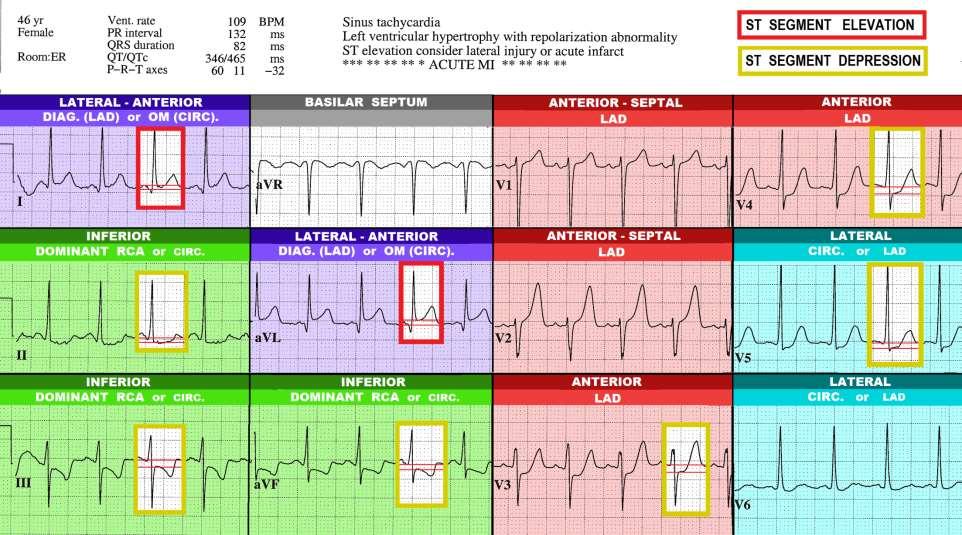
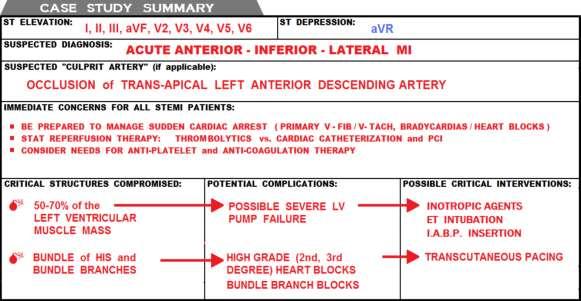
99 F THERE ARE TWO IMPORTANT CLUES that the patient s BLOCKAGE is in the PROXIMAL LEFT ANTERIOR DESCENDING ARTERY: 1. When ST elevation is noted in leads I and avl in cases of ANTERIOR WALL STEMI, it is a good indicator that the FIRST DIAGONAL BRANCH is included in the zone of infarction. RECIPROCAL ST DEPRESSION in the INFERIOR LEADS (II, III, and/or avf) is an indication that the LAD is blocked proximal to the FIRST DIAGONAL BRANCH. [1] [1] Use of the Electrocardiogram in Acute Myocardial Infarction, Zimetbaum, et al, NEJM 348:

100 WHILE WAITING FOR THE RETEVASE TO WORK, THE PATIENT BEGAN VOMITING. SKIN BECAME ASHEN & DIAPHORETIC. REPEAT BP = 50/30. -WHAT THERAPEUTIC INTERVENTIONS SHOULD BE IMPLMENTED AT THIS POINT?
101

102 PLUS: EXTENSION OF THROMBUS LOAD INTO THE LEFT MAIN CORONARY ARTERY....
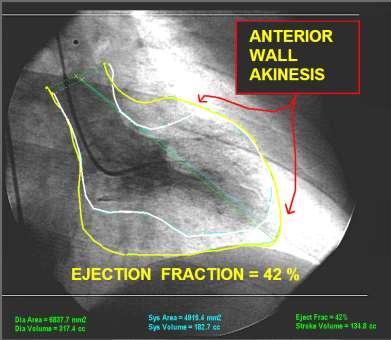
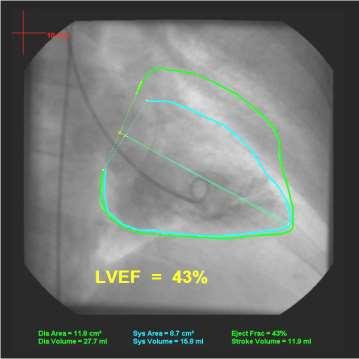
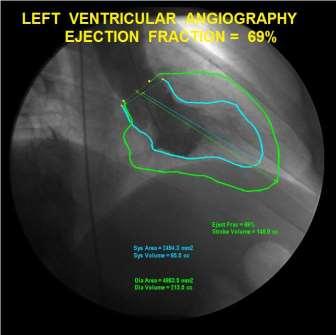
103

104 WHO SHOULD GO TO THE CATH LAB FIRST? And.... WHAT WOULD YOU DO WITH THE PATIENT WHO DID NOT GO TO THE CATH LAB?
105

106 PATIENT A: PATIENT B:

107
108
109



110 Despite the dismal mortality rate associated with STEMI from total LMCA occlusion, this patient survived and was later discharged. His EF is estimated at approximately 30%. He received an ICD, and is currently stable.
111
112
113
114
115
116
117 TEST QUESTION # 27
118
119
120
121
122
123

124
125
126
127
128
129
130

131
132

133
134
135
136
137
138
139
140
141
142

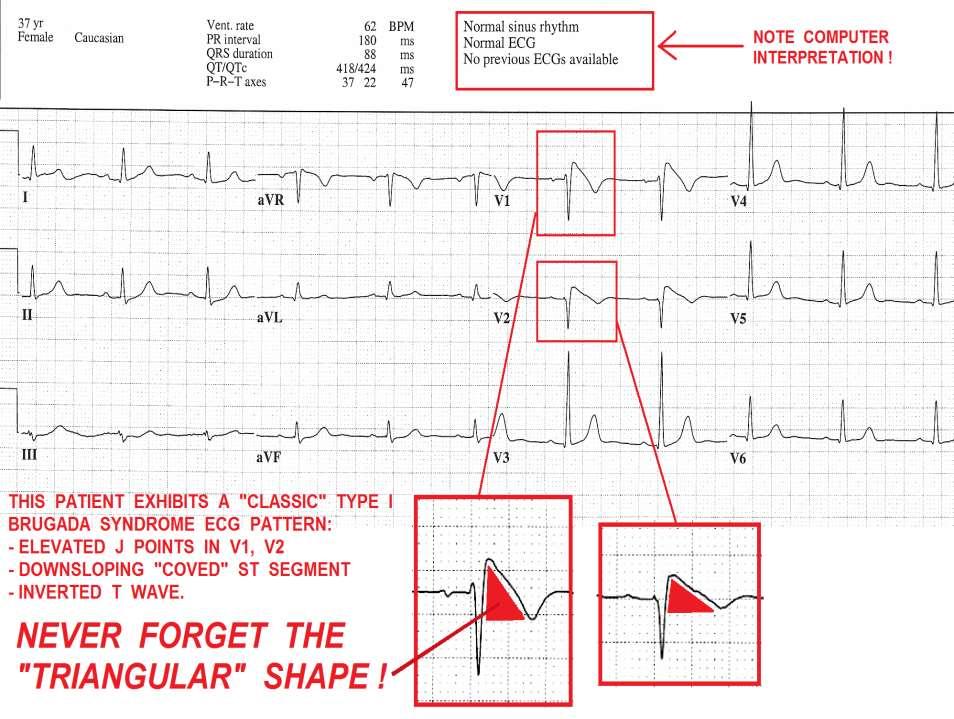
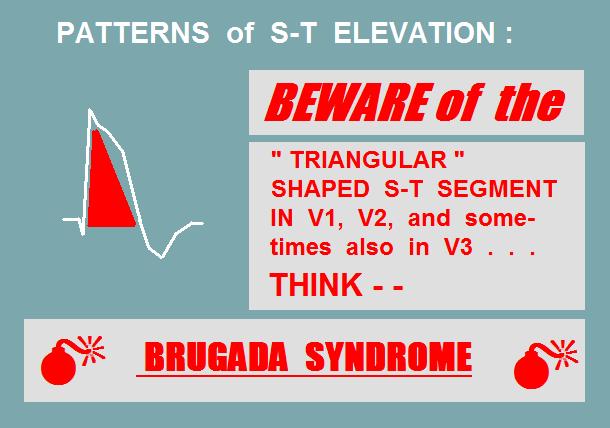
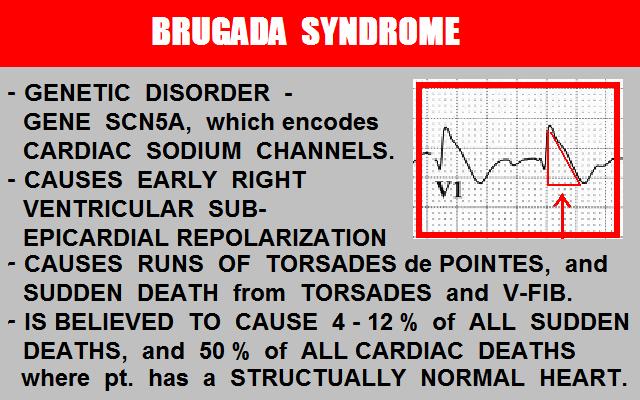
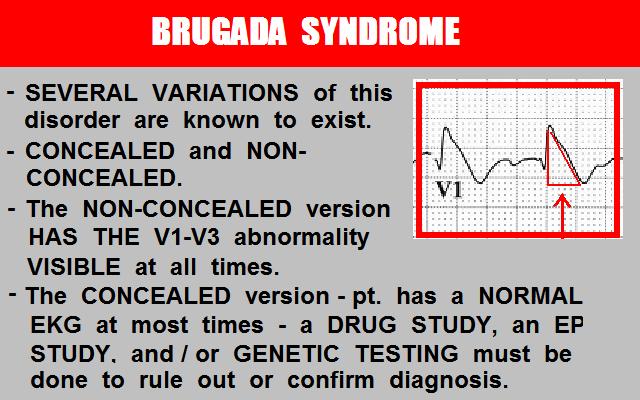
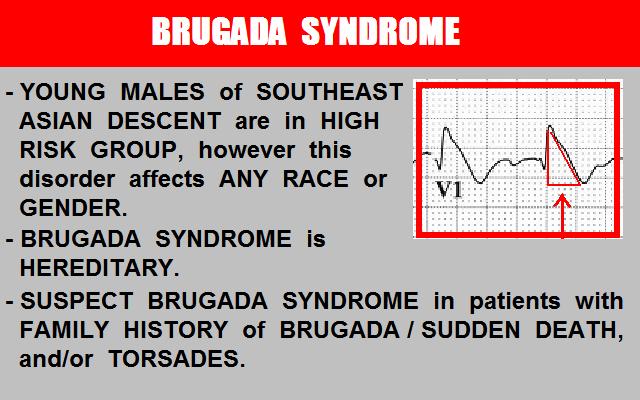
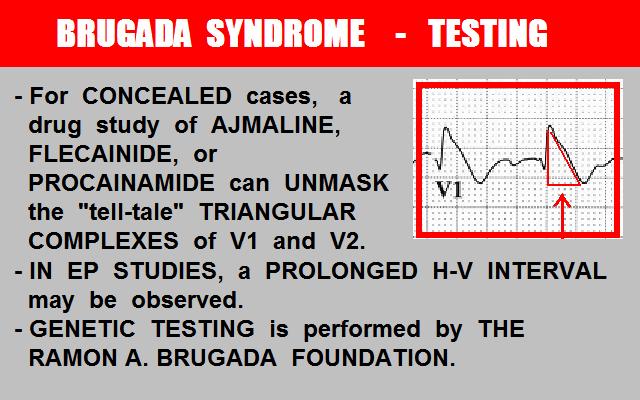
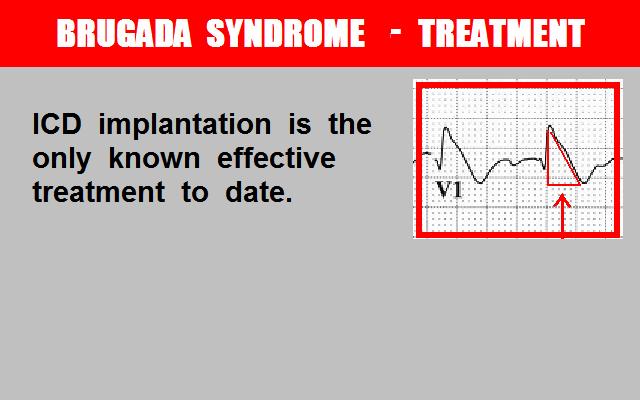
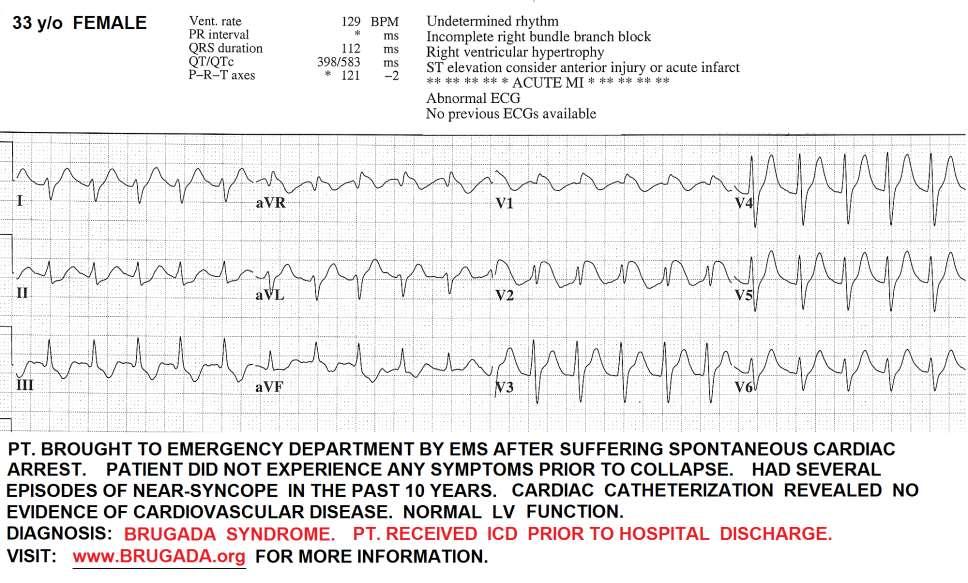
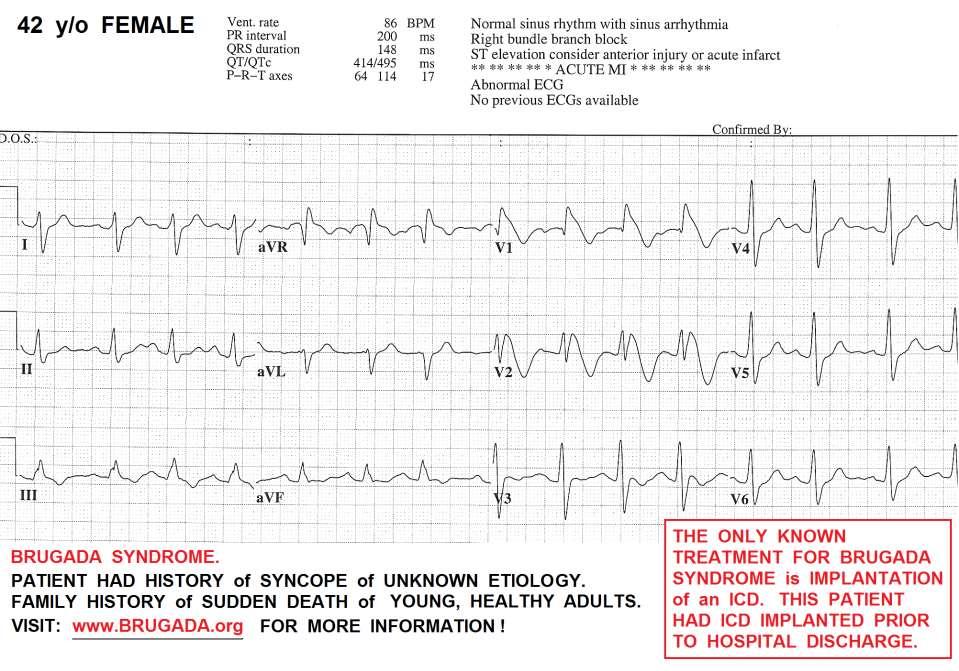
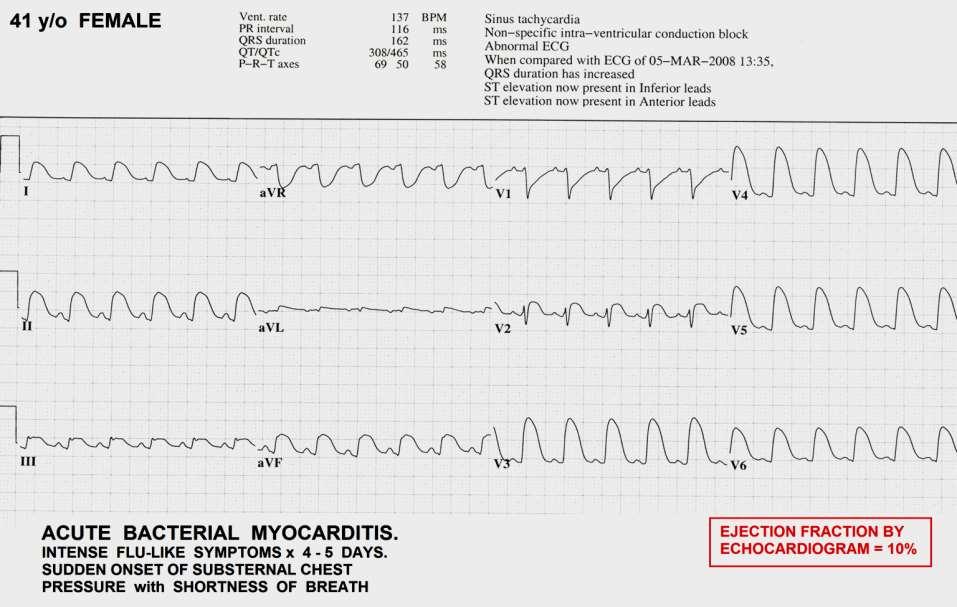
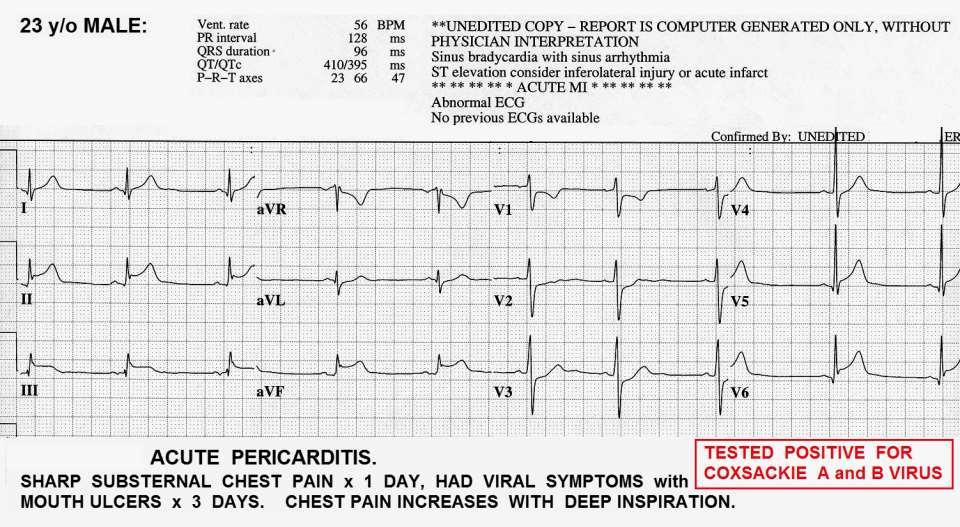
143
144
145 EVOLVING STEMI: -ST SEGMENTS DROP -Q WAVES FORM -R WAVE PROGRESSION CHANGES IN PRECORDIAL LEADS.

146 ACUTE ANTERIOR WALL STEMI

147 EVOLVING ANTERIOR WALL STEMI

148 FULLY EVOLVED ANTERIOR WALL MI

149 NOWHERE, NEW MEXICO, 1994

150 BRUGADA SYNDROME and Other Infarction Mimics
151
152
153

154 TEST QUESTION # 32
155
156
157
158
159
160
161
162
163
164
165
166
167
168

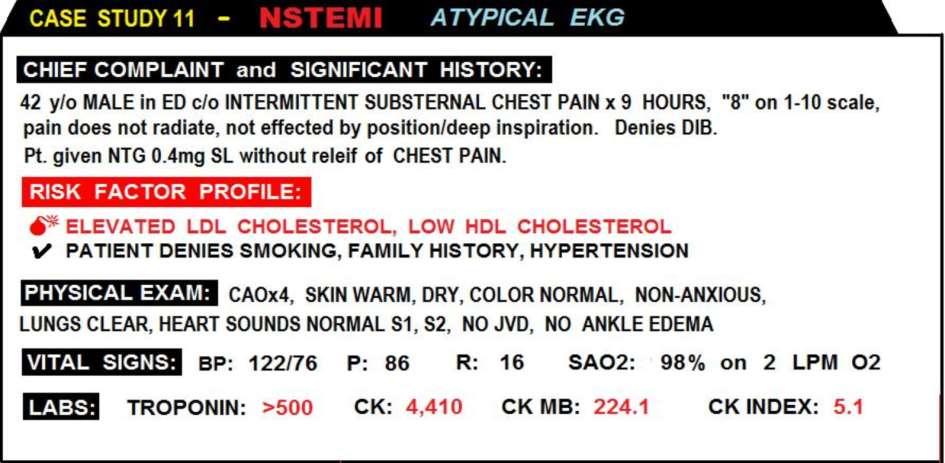
169 NSTEMI CASE STUDIES Book Page: 186
170

171 BOOK PAGE: 108
172
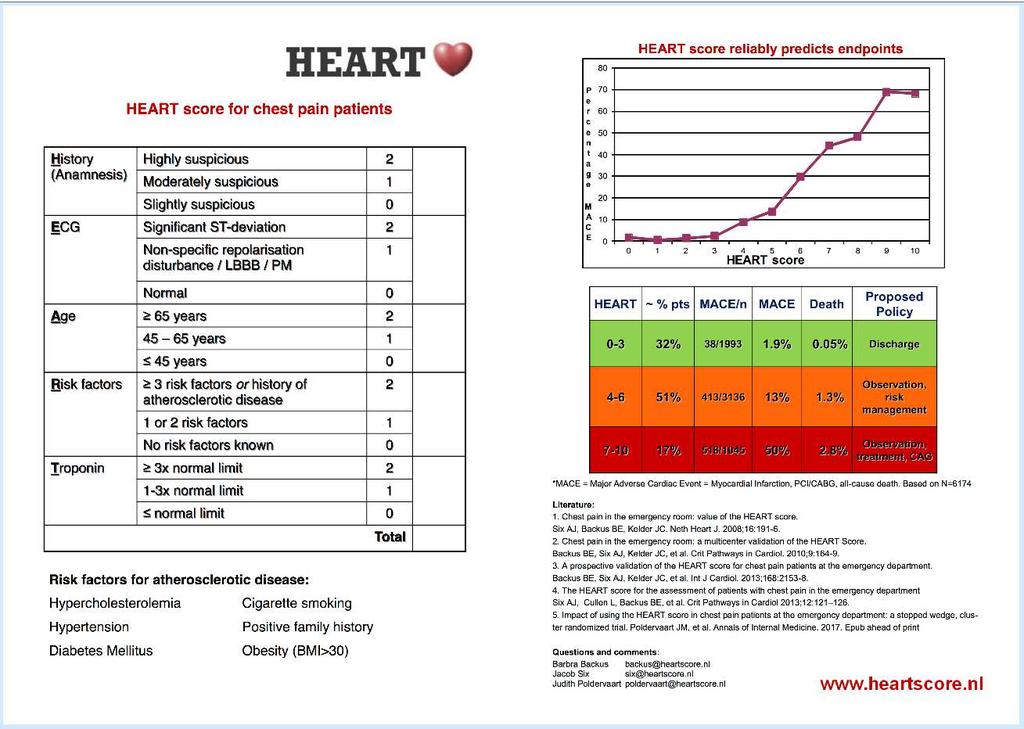
173 HEART Score -vs- TIMI Score

174 63 y/o male patient s TMI Score is a TWO, which means He s only a LOW RISK patient.....
175
176 62 y/o male patient s TMI Score is a TWO, which means He s only a LOW RISK patient.....
177 62 y/o male patient s TMI Score is a TWO, which means He s only a LOW RISK patient..... The Interventional Cardiologist was very suspicious of the man s Risk Factors and Symptoms, and convinced the man to consent to a Cardiac Catheterization..
178 62 y/o male patient s TMI Score is a TWO, which means He s only a LOW RISK patient..... The Interventional Cardiologist was very suspicious of the man s Risk Factors and Symptoms, and convinced the man to consent to a Cardiac Catheterization..


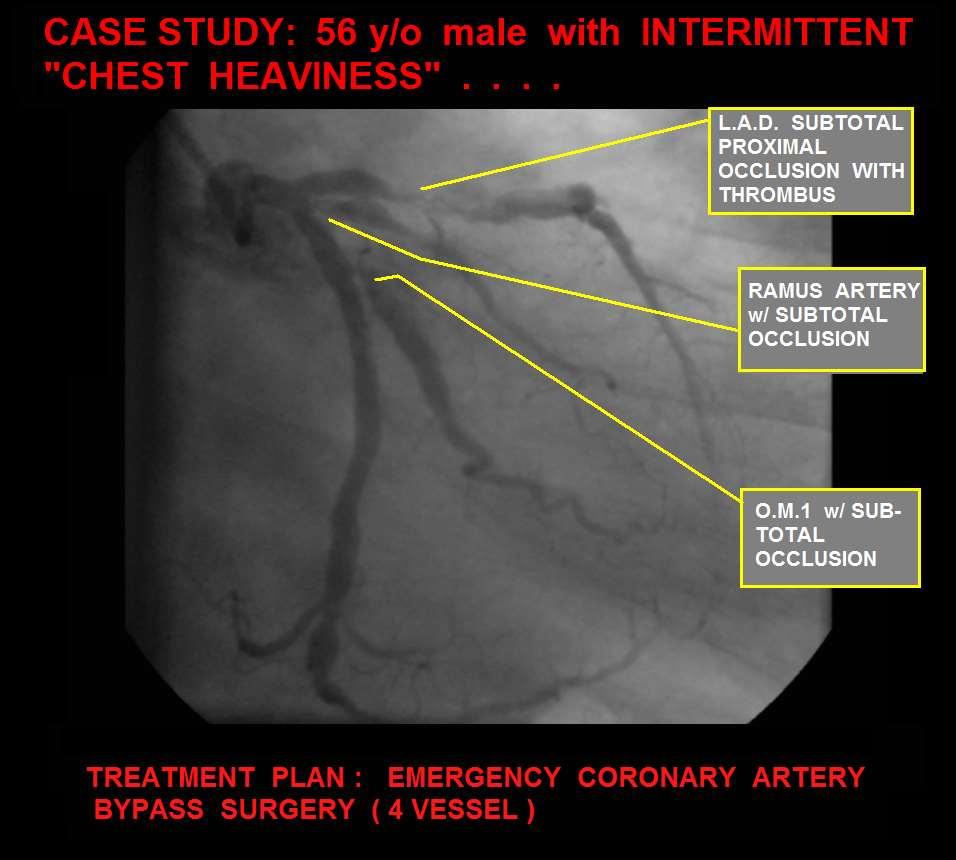
179 62 y/o male patient s TMI Score is a TWO, which means He s only a LOW RISK patient..... The Interventional Cardiologist was very suspicious of the man s Risk Factors and Symptoms, and convinced the man to consent to a Cardiac Catheterization.. It s a good thing the Doctor didn t include the TIMI Score in his clinical decision-making. The patient was directly for emergency bypass surgery.
180
181
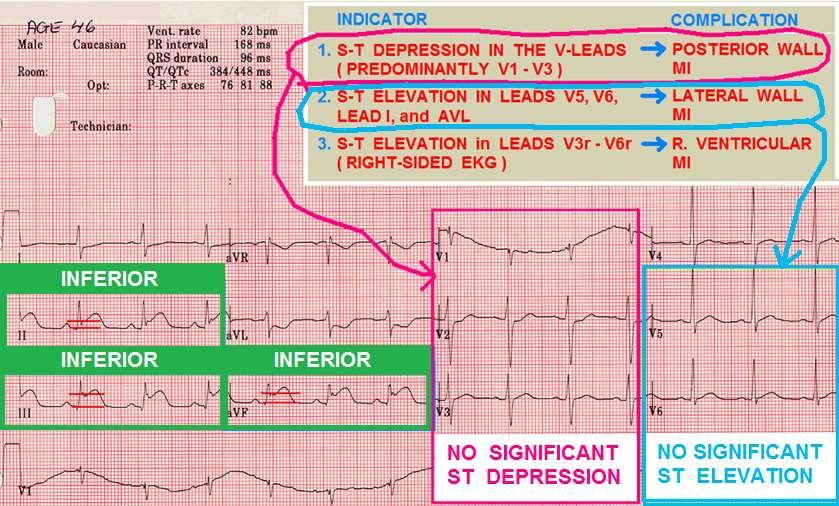
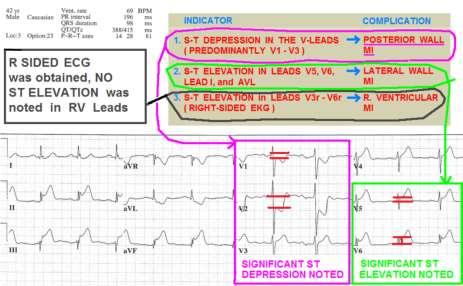
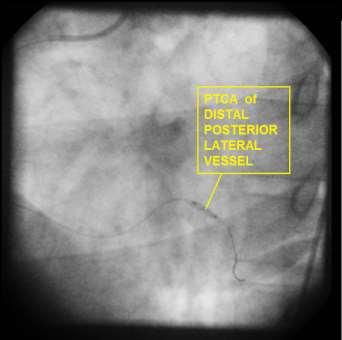
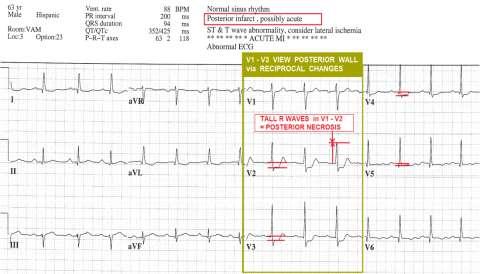
182
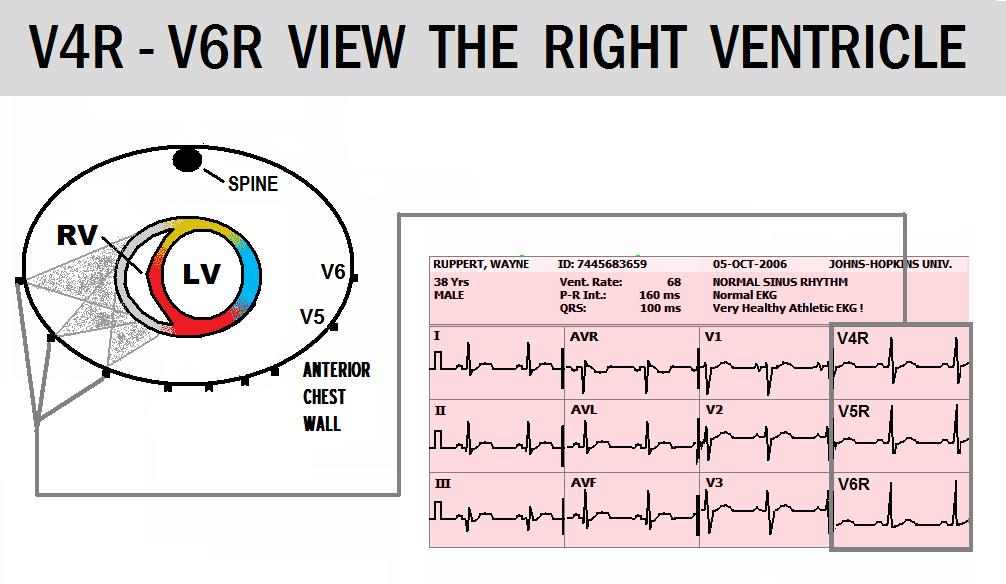
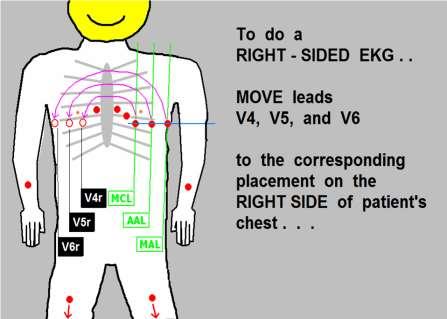
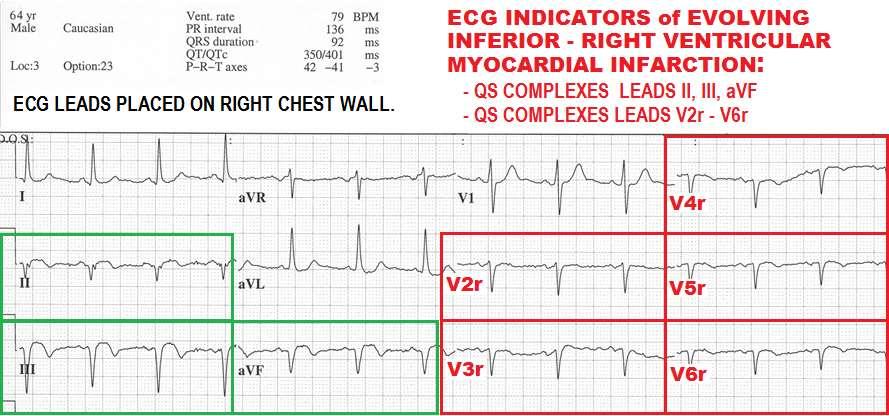
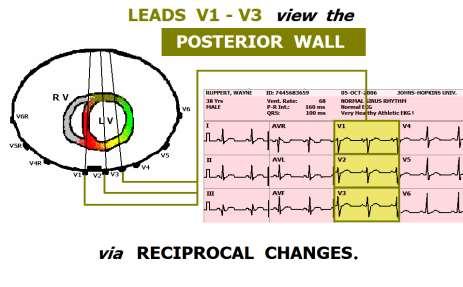
183
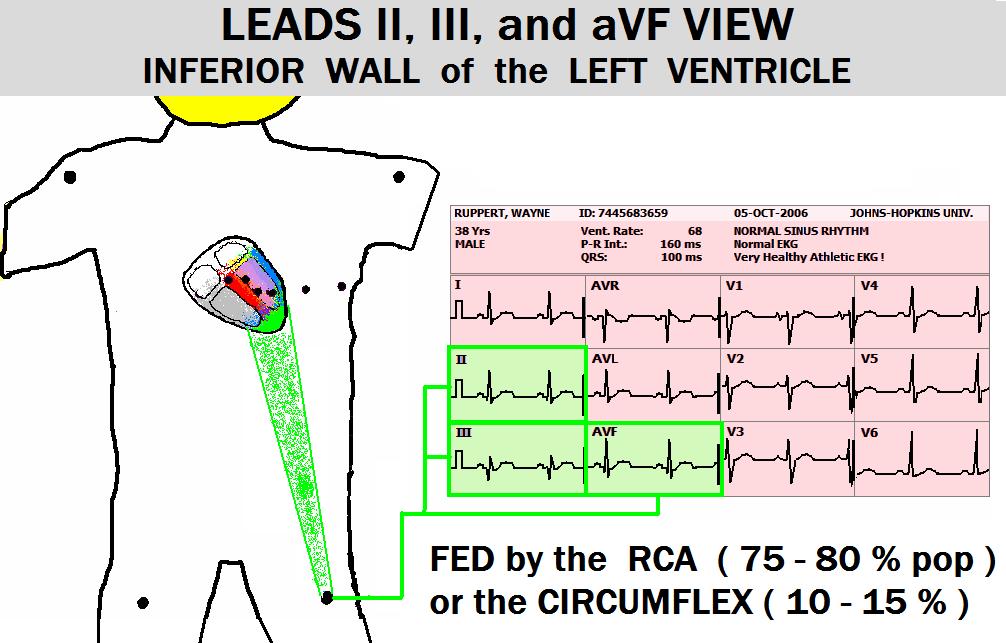
184
185

186 BOOK PAGE: 70
187

188

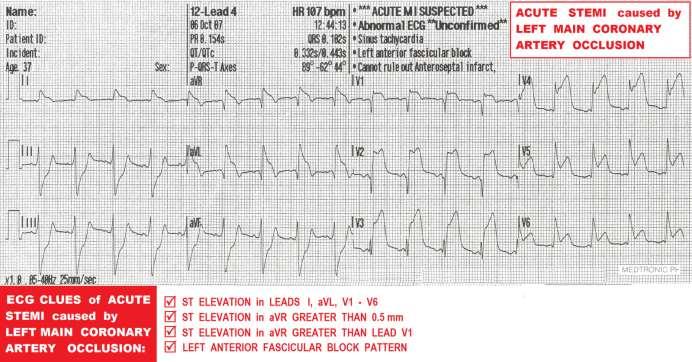
189 REMEMBER IT S POSSIBLE TO HAVE A STEMI... WHEN THERE S NO ST ELEV. ON THE 12 LEAD!!


190 THE 12 LEAD EKG HAS TWO MAJOR BLIND SPOTS: - POSTERIOR WALL - R VENTRICLE THE 18 LEAD EKG ADDS COVERAGE OF THE -POSTERIOR WALL -R VENTRICLE
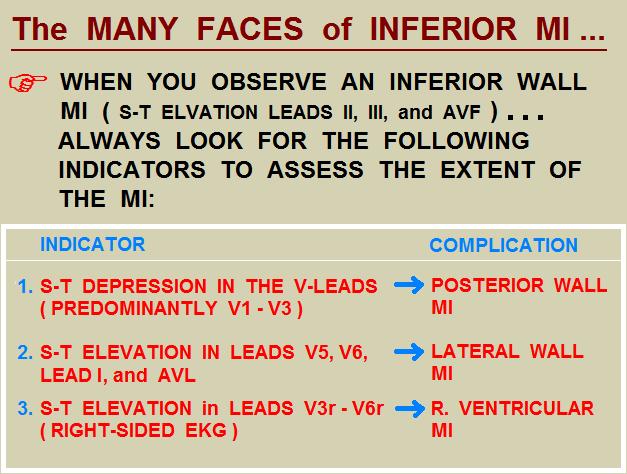
191 INDICATIONS FOR OBTAINING AN 18 LEAD EKG: 1. INFERIOR WALL MIs (ST ELEV II, III, avf) 2. SUSPECTED POSTERIOR WALL MI (ST DEPR V1, V2, and/or V3, V4)
192
193
194
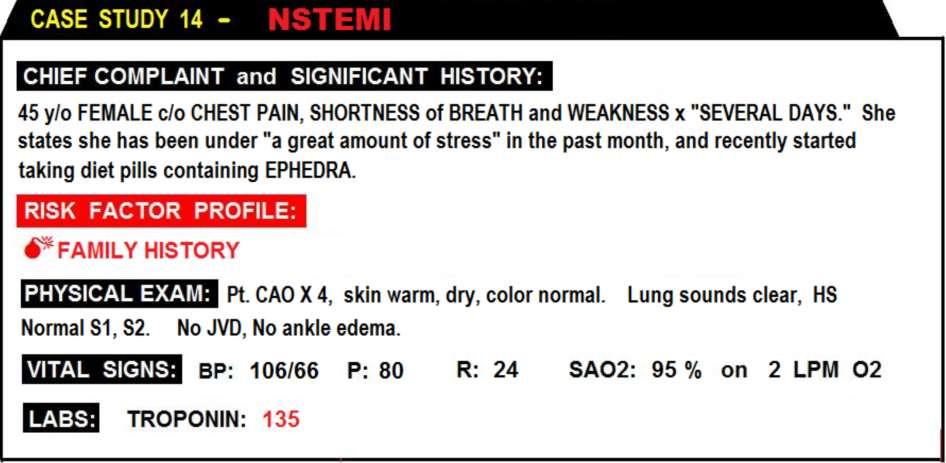
195

196 F LEAD avr sometimes referred to as the forgotten 12 th lead can be a source of valuable information. In this case study, lead avr is the only lead with ST elevation. - In cases of myocardial ischemia and NSTEMI, ST segment elevation of lead avr has been associated with a high incidence of triple vessel disease, [1] which is true in this case study. - In cases of anterior wall STEMI, elevation of lead avr indicates the patient s lesion is proximal to the origin of the first septal perforator. [2] - When the ST elevation of lead avr is higher than that of V1, it is considered an indicator that the left main coronary artery is obstructed. [3] Please review Case Study 4 (p 183), STEMI, and involving occlusion of Left Main Coronary Artery. While reviewing ECGs for inclusion in this curriculum, we noticed the correlation between J point elevation in lead avr and the incidence of severe multivessel disease.
197
198
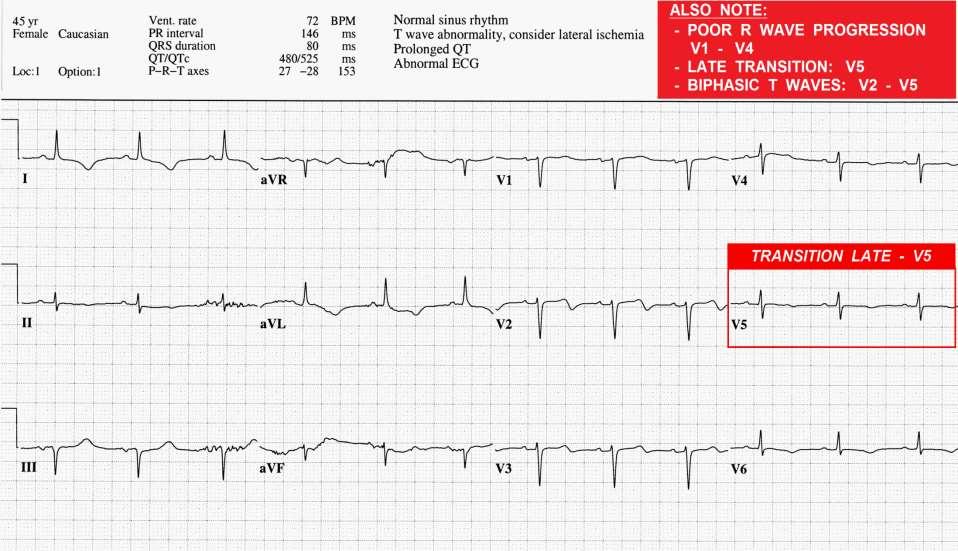
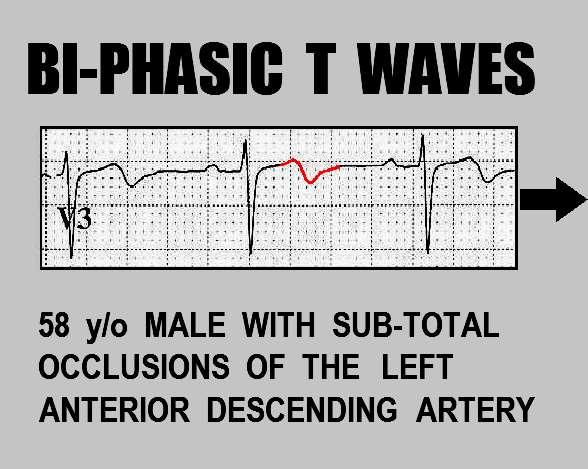
199
200
201


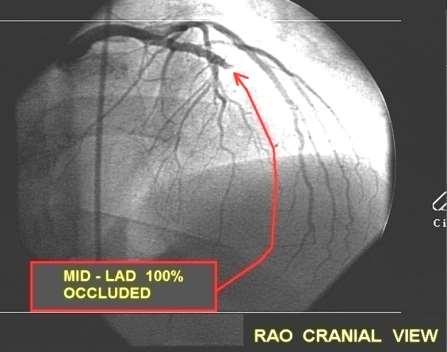
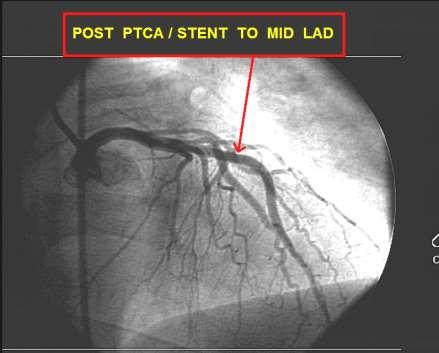
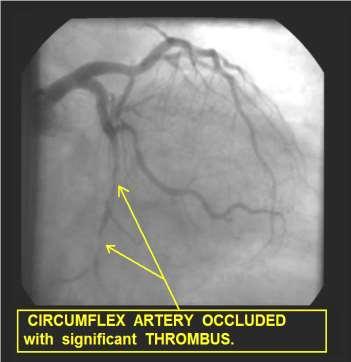
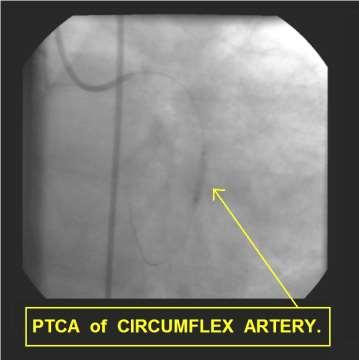
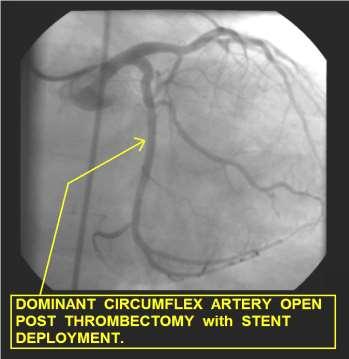
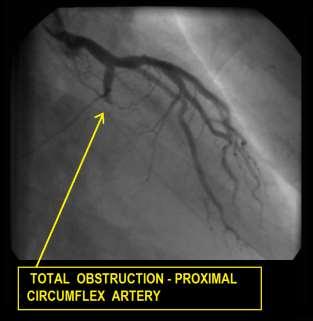
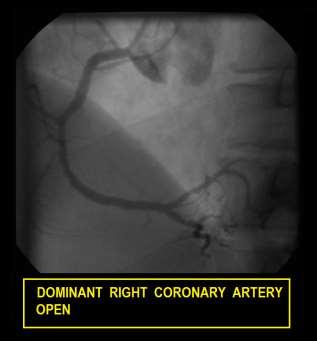
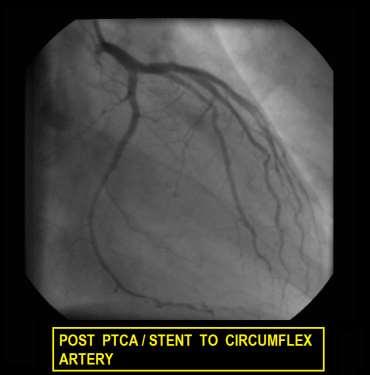
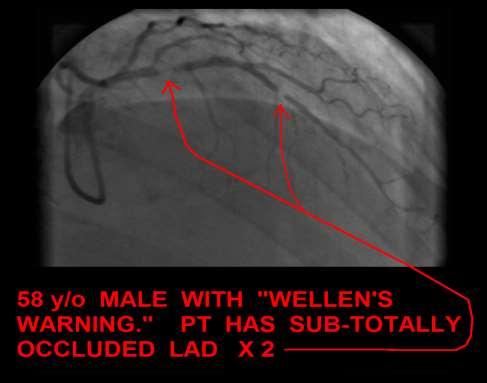
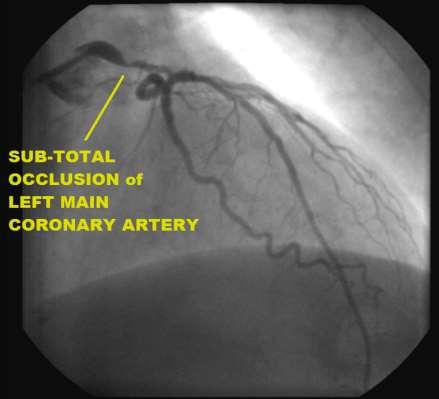
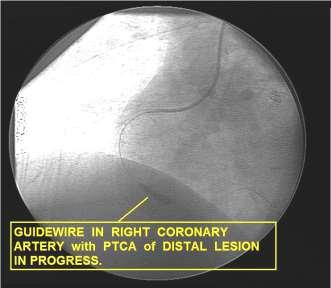
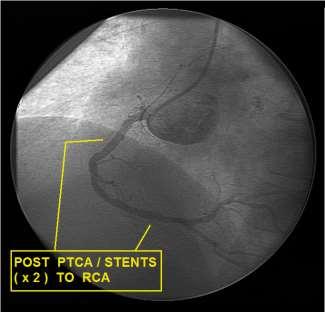
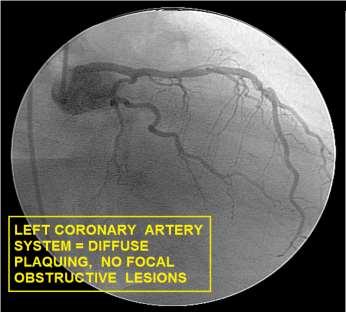
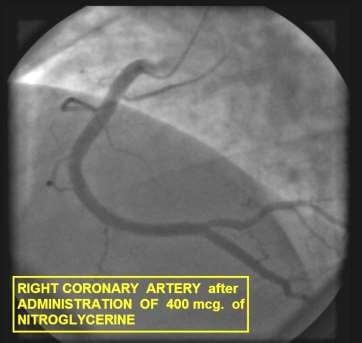
. [1] A.")
202 Apical ballooning syndrome, also known as broken heart syndrome and acute stress induced cardiomyopathy, may account for up to 2% of all incidents of acute myocardial infarction. [1] This condition is uncommon but often life-threatening. ABS can be provoked by extreme emotional distress and a- adrenergic substances (including ephedrine alkaloids). [1] A. Prasad MD, Circulation 2007;115;e56-e59


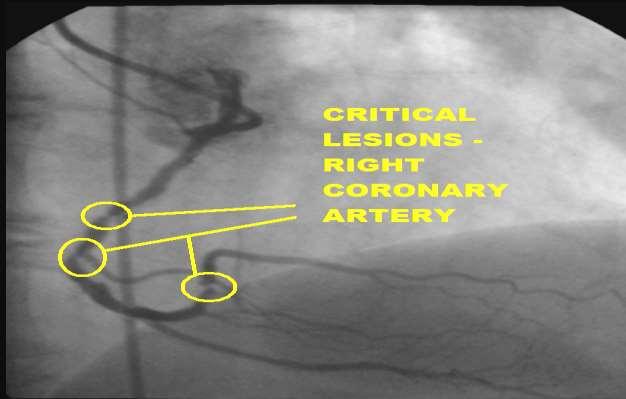
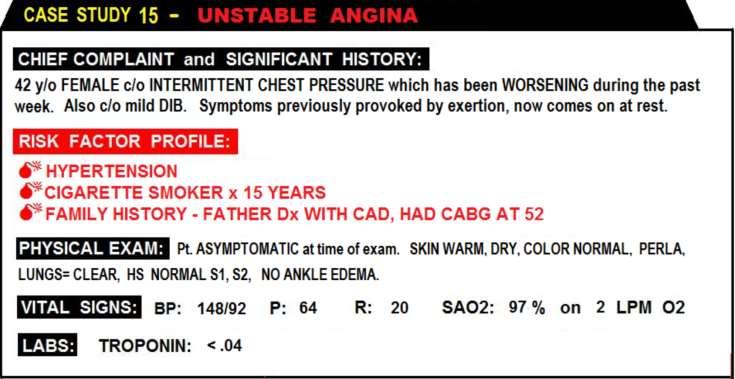
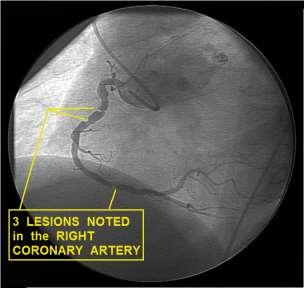
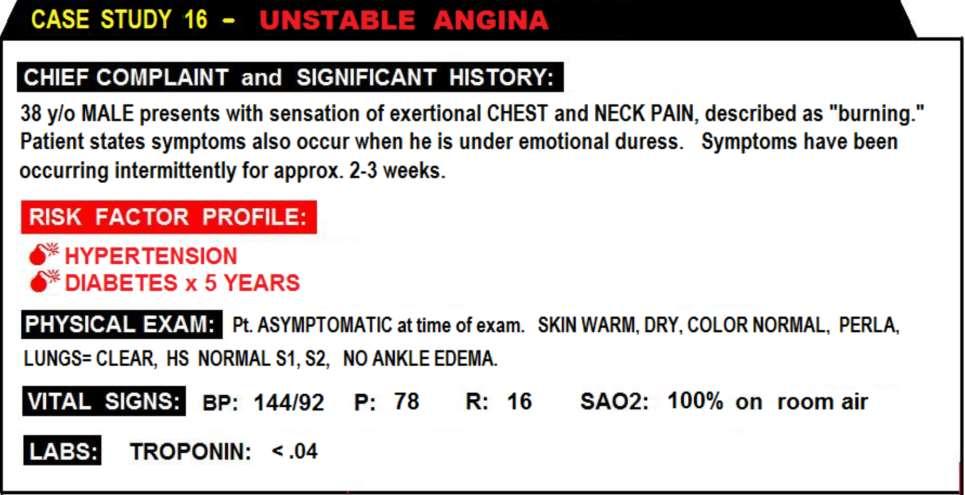
203 UNSTABLE ANGINA CASE STUDIES
204

205 CASE STUDY: SERIAL ECGs. 33 y/o MALE, C/O COUGHING WITH CHEST PAIN. ST ELEVATION BELIEVED TO BE EARLY REPOLARIZATION. A VETERAN ED PHYSICIAN DISCERNED THAT THE PATIENT S CHEST PAIN STARTED BEFORE THE COUGHING, AND ORDERED SERIAL ECGs.

206 APPROX. 3 hrs LATER: BI-PHASIC T WAVES V2, V3; INVERTED Ts V4 V6

207 APPROX 6 hrs AFTER 1 ST ECG: BIPHASIC Ts V1, V2; INVERTED T WAVES V3 - V6

208 APPROX 9 hrs AFTER 1 ST ECG: BIPHASIC Ts V1, V2; INVERTED T WAVES V3 - V6



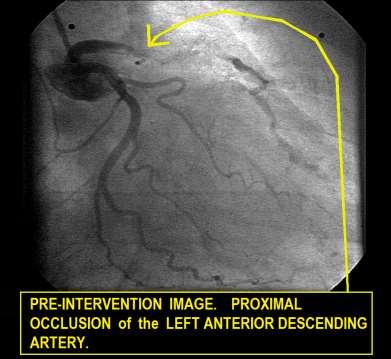
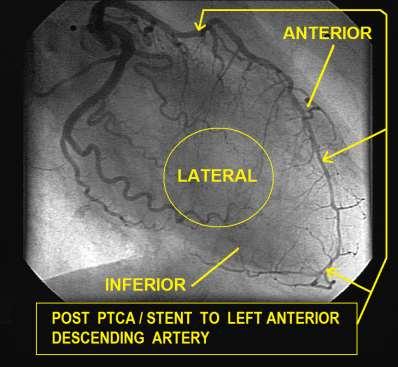
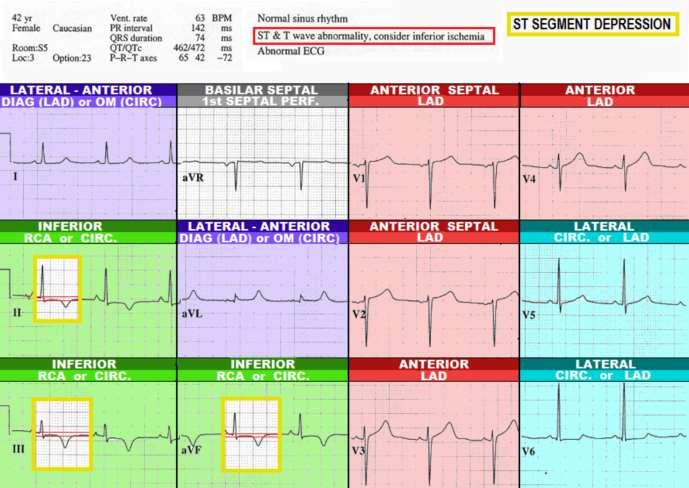
209 PATIENT TAKEN TO THE CARDIAC CATH LAB, WHERE A SUB-TOTALLY OCCLUDED PROXIMAL L.A.D. WAS DISCOVERED (left). BOTTOM LEFT: PTCA/STENT TO L.A.D. BOTTOM RIGHT: POST STENT TO L.A.D.
210
211 Classic Wellen s Syndrome: Characteristic T wave changes Biphasic T waves Inverted T waves History of anginal chest pain Normal or minimally elevated cardiac markers ECG without Q waves, without significant ST-segment elevation, and with normal precordial R-wave progression
212 Wellen s Syndrome ETIOLOGY: Critical Lesion, Proximal LAD Coronary Artery Vasospasm Cocaine use (vasospasm) Increased myocardial oxygen demand Generalized Hypoxia / anemia / low H&H
213 Wellen s Syndrome EPIDEMIOLOGY & PROGNOSIS: Present in 14-18% of patients admitted with unstable angina 75% patients not treated developed extensive Anterior MI within 3 weeks. Median Average time from presentation to Acute Myocardial Infarction 8 days Sources: H Wellens et. Al, Am Heart J 1982; v103(4)
214

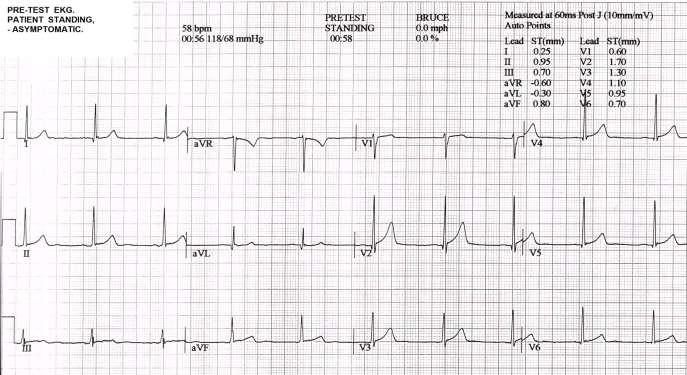
215 VALUE OF STRESS TESTING..
216


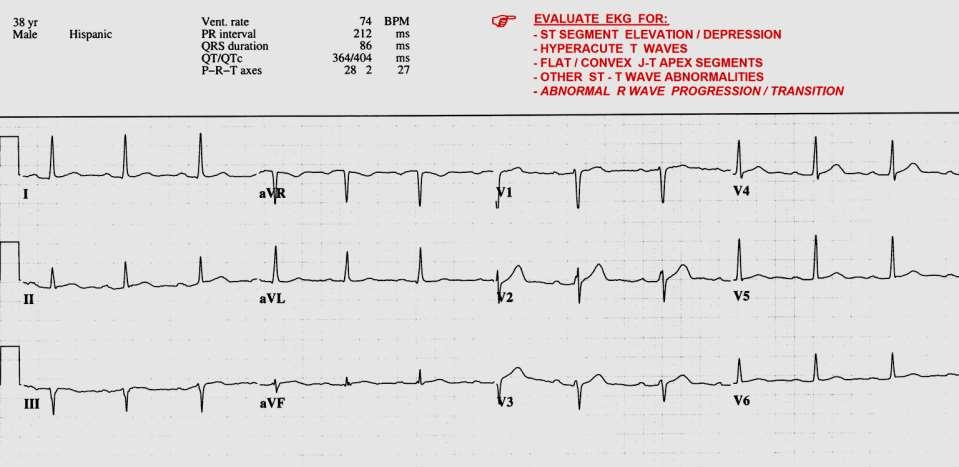
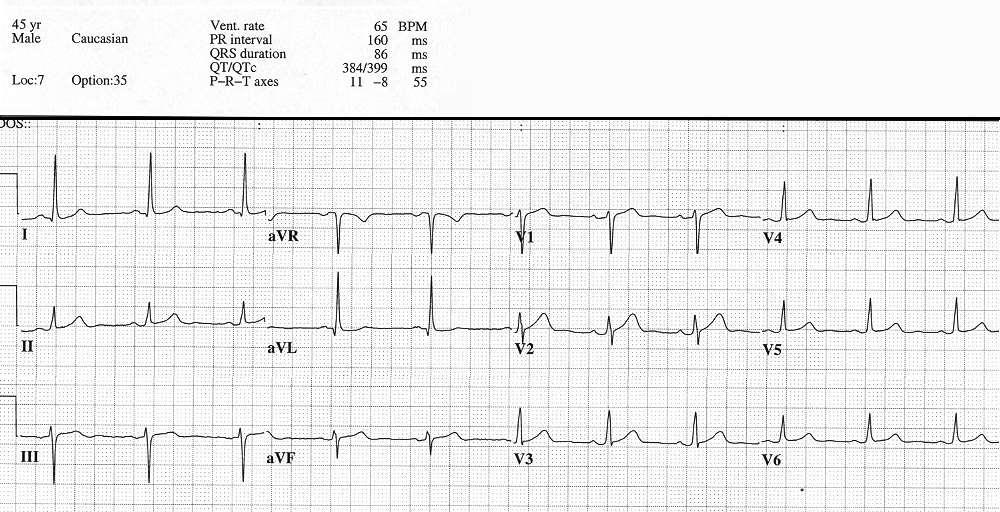
217 NON SPECIFIC ST-T WAVE ABNORMALITY: - III ST ELEVATION: -AVR ST DEPRESSION: -I -II -III -AVF -V2 -V3 -V4 -V5 -V6
218

219
220

221
222
223
224
225

226


227
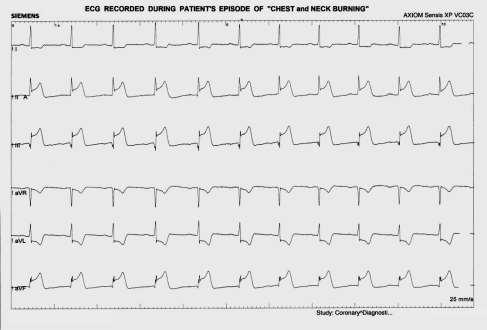
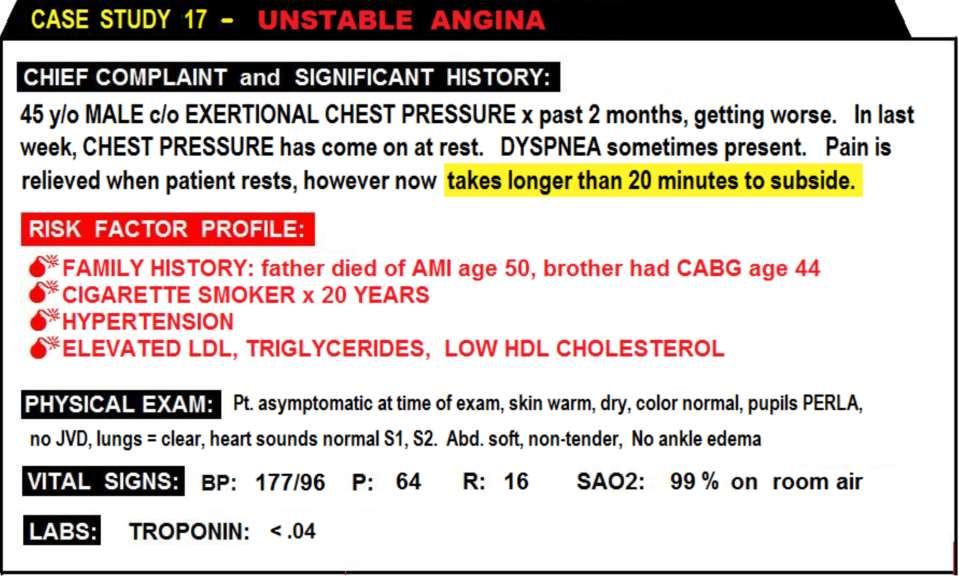
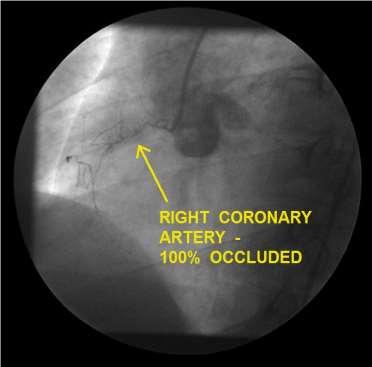
228 Prinzmetal or variant angina is caused by focal coronary artery vasospasm, and was first described by Myron Prinzmetal in 1959 as a syndrome of episodic chest pain that comes on at rest with ST segment elevation. [1] Prinzmetal angina is classified as unstable angina due to its unpredictability [2], and has been associated with myocardial infarction, ventricular dysrhythmias and cardiac arrest. The primary mechanism of vasospasm is hypercontraction of vascular smooth muscle cells. Variant angina is not an indicator of CAD; many patients are free of atherosclerotic plaque. Some factors known to provoke coronary artery vasospasm include: vasoconstrictor medications, stimulants such as cocaine, ephedrine and amphetamines, emotional duress, exposure to cold and alcohol withdraw. Typical Prinzmetal s variant angina occurs at rest, in the early hours of the morning. The pain is often described as severe chest tightness or pressure. Variant angina is usually treated with and responds well to calcium channel blockers and nitrates. [3] [1] Prinzmetal et al, Am J Med. 1959;27: [2] National Institutes of Health, Library of Medicine, [3] National Institutes of Health, Library of Medicine,
229
230

231

232 QUESTIONS???

233 My top two reasons for giving everything in life the best I have to offer.
STAT 12 Lead ECG Workshop: Basics & ACS
 STAT 12 Lead ECG Workshop: Basics & ACS Part 2: Acute Coronary Syndrome WAYNE W RUPPERT, CVT, CCCC, NREMT-P Cardiovascular Coordinator Bayfront Health Seven Rivers Crystal River, Florida Interventional
STAT 12 Lead ECG Workshop: Basics & ACS Part 2: Acute Coronary Syndrome WAYNE W RUPPERT, CVT, CCCC, NREMT-P Cardiovascular Coordinator Bayfront Health Seven Rivers Crystal River, Florida Interventional
All About STEMIs. Presented By: Brittney Urvand, RN, BSN, CCCC. Essentia Health Fargo Cardiovascular Program Manager.
 All About STEMIs Presented By: Brittney Urvand, RN, BSN, CCCC Essentia Health Fargo Cardiovascular Program Manager Updated 10/2/2018 None Disclosures Objectives Identify signs and symptoms of a heart attack
All About STEMIs Presented By: Brittney Urvand, RN, BSN, CCCC Essentia Health Fargo Cardiovascular Program Manager Updated 10/2/2018 None Disclosures Objectives Identify signs and symptoms of a heart attack
ACUTE CORONARY SYNDROME
 12 LEAD ECG INTERPRETATION in ACUTE CORONARY SYNDROME WAYNE W RUPPERT, CVT, CCCC, NREMT P Cardiovascular C di l Clinical Cli i l Coordinator C di t Bayfront Health Dade City Dade City, FL Education Specialist
12 LEAD ECG INTERPRETATION in ACUTE CORONARY SYNDROME WAYNE W RUPPERT, CVT, CCCC, NREMT P Cardiovascular C di l Clinical Cli i l Coordinator C di t Bayfront Health Dade City Dade City, FL Education Specialist
Wayne Ruppert and Dr. James Irwin, St Joseph s Hospital, Tampa, FL 2006
 The EMS 12 Lead 101 Wayne W Ruppert, CVT, CCCC, NREMT-P Interventional Cardiovascular Technologist Cardiovascular Coordinator Bayfront Health Seven Rivers Welcome! Wayne Ruppert and Dr. James Irwin, St
The EMS 12 Lead 101 Wayne W Ruppert, CVT, CCCC, NREMT-P Interventional Cardiovascular Technologist Cardiovascular Coordinator Bayfront Health Seven Rivers Welcome! Wayne Ruppert and Dr. James Irwin, St
12 Lead Electrocardiogram (ECG) PFN: SOMACL17. Terminal Learning Objective. References
 PFN: SOMACL17. Terminal Learning Objective. References") 12 Lead Electrocardiogram (ECG) PFN: SOMACL17 Slide 1 Terminal Learning Objective Action: Communicate knowledge of 12 Lead Electrocardiogram (ECG) Condition: Given a lecture in a classroom environment
12 Lead Electrocardiogram (ECG) PFN: SOMACL17 Slide 1 Terminal Learning Objective Action: Communicate knowledge of 12 Lead Electrocardiogram (ECG) Condition: Given a lecture in a classroom environment
ECG in coronary artery disease. By Sura Boonrat Central Chest Institute
 ECG in coronary artery disease By Sura Boonrat Central Chest Institute EKG P wave = Atrium activation PR interval QRS = Ventricle activation T wave= repolarization J-point EKG QT interval Abnormal repolarization
ECG in coronary artery disease By Sura Boonrat Central Chest Institute EKG P wave = Atrium activation PR interval QRS = Ventricle activation T wave= repolarization J-point EKG QT interval Abnormal repolarization
Observation Medicine ECG Instructor Workshop session 2 Serial 12 Lead ECG Interpretation
 American College of Cardiology 20 th Congress 2017 Observation Medicine ECG Instructor Workshop session 2 Serial 12 Lead ECG Interpretation Part 1 By: Wayne W Ruppert, CVT, CCCC, NREMT-P This curriculum
American College of Cardiology 20 th Congress 2017 Observation Medicine ECG Instructor Workshop session 2 Serial 12 Lead ECG Interpretation Part 1 By: Wayne W Ruppert, CVT, CCCC, NREMT-P This curriculum
The Fundamentals of 12 Lead EKG. ECG Recording. J Point. Reviewing the Cardiac Conductive System. Dr. E. Joe Sasin, MD Rusty Powers, NRP
 The Fundamentals of 12 Lead EKG Dr. E. Joe Sasin, MD Rusty Powers, NRP SA Node Intranodal Pathways AV Junction AV Fibers Bundle of His Septum Bundle Branches Purkinje System Reviewing the Cardiac Conductive
The Fundamentals of 12 Lead EKG Dr. E. Joe Sasin, MD Rusty Powers, NRP SA Node Intranodal Pathways AV Junction AV Fibers Bundle of His Septum Bundle Branches Purkinje System Reviewing the Cardiac Conductive
12 Lead ECG Interpretation
 12 Lead ECG Interpretation Julie Zimmerman, MSN, RN, CNS, CCRN Significant increase in mortality for every 15 minutes of delay! N Engl J Med 2007;357:1631-1638 Who should get a 12-lead ECG? Also include
12 Lead ECG Interpretation Julie Zimmerman, MSN, RN, CNS, CCRN Significant increase in mortality for every 15 minutes of delay! N Engl J Med 2007;357:1631-1638 Who should get a 12-lead ECG? Also include
Ischemic heart disease
 Ischemic heart disease Introduction In > 90% of cases: the cause is: reduced coronary blood flow secondary to: obstructive atherosclerotic vascular disease so most of the time it is called: coronary artery
Ischemic heart disease Introduction In > 90% of cases: the cause is: reduced coronary blood flow secondary to: obstructive atherosclerotic vascular disease so most of the time it is called: coronary artery
Myocardial Infarction. Reading Assignment (p66-78 in Outline )
") Myocardial Infarction Reading Assignment (p66-78 in Outline ) Objectives 1. Why do ST segments go up or down in ischemia? 2. STEMI locations and culprit vessels 3. Why 15-lead ECGs? 4. What s up with avr?
Myocardial Infarction Reading Assignment (p66-78 in Outline ) Objectives 1. Why do ST segments go up or down in ischemia? 2. STEMI locations and culprit vessels 3. Why 15-lead ECGs? 4. What s up with avr?
INTERPRETAZIONE ECG NEL PAZIENTE CON SOSPETTO STEMI
 INTERPRETAZIONE ECG NEL PAZIENTE CON SOSPETTO STEMI Giacomo Veronese Scuola di Specializzazione Medicina d Emergenza e Urgenza Università Milano-Bicocca Siete d accordo se vi propongo per una relazione..
INTERPRETAZIONE ECG NEL PAZIENTE CON SOSPETTO STEMI Giacomo Veronese Scuola di Specializzazione Medicina d Emergenza e Urgenza Università Milano-Bicocca Siete d accordo se vi propongo per una relazione..
12 Lead ECGs: Ischemia, Injury & Infarction. Kevin Handke NRP, FP-C, CCP, CMTE STEMI Coordinator Flight Paramedic
 12 Lead ECGs: Ischemia, Injury & Infarction Kevin Handke NRP, FP-C, CCP, CMTE STEMI Coordinator Flight Paramedic None Disclosures Objectives Upon completion of this program the learner will be able to
12 Lead ECGs: Ischemia, Injury & Infarction Kevin Handke NRP, FP-C, CCP, CMTE STEMI Coordinator Flight Paramedic None Disclosures Objectives Upon completion of this program the learner will be able to
Hot Topics in Cardiac Arrest. Should the patient go To the Cath Lab?
 Hot Topics in Cardiac Arrest Should the patient go To the Cath Lab? Tim Russert 1950-2008 Host of NBC s Meet the Press Sudden Cardiac Arrest : Autopsy showed plaque rupture in his LAD ( per LA Times,
Hot Topics in Cardiac Arrest Should the patient go To the Cath Lab? Tim Russert 1950-2008 Host of NBC s Meet the Press Sudden Cardiac Arrest : Autopsy showed plaque rupture in his LAD ( per LA Times,
ECG Workshop. Nezar Amir
 ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
Acute Coronary Syndromes Unstable Angina Non ST segment Elevation MI (NSTEMI) ST segment Elevation MI (STEMI)
 ST segment Elevation MI (STEMI)") Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Evaluate common abnormalities that mimic myocardial infarction. Identify
Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Evaluate common abnormalities that mimic myocardial infarction. Identify
12 LEAD EKG BASICS. By: Steven Jones, NREMT P CLEMC
 12 LEAD EKG BASICS By: Steven Jones, NREMT P CLEMC ECG Review Waves and Intervals P wave: the sequential activation (depolarization) of the right and left atria QRS complex: right and left ventricular
12 LEAD EKG BASICS By: Steven Jones, NREMT P CLEMC ECG Review Waves and Intervals P wave: the sequential activation (depolarization) of the right and left atria QRS complex: right and left ventricular
Cardiac Ischemia ECG Workshop
 Cardiac Ischemia ECG Workshop Classic, Confusing, and Confounding Patterns Amal Mattu, MD, NE Professor and Vice Chair Department of Emergency Medicine University of Maryland School of Medicine amalmattu@comcast.net
Cardiac Ischemia ECG Workshop Classic, Confusing, and Confounding Patterns Amal Mattu, MD, NE Professor and Vice Chair Department of Emergency Medicine University of Maryland School of Medicine amalmattu@comcast.net
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases
 Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Acute Coronary Syndromes. Disclosures
 Acute Coronary Syndromes Disclosures I work for Virginia Garcia Memorial Health Center, Beaverton, OR. Jon Tardiff, BS, PA-C OHSU Clinical Assistant Professor And I am a medical editor for Jones & Bartlett
Acute Coronary Syndromes Disclosures I work for Virginia Garcia Memorial Health Center, Beaverton, OR. Jon Tardiff, BS, PA-C OHSU Clinical Assistant Professor And I am a medical editor for Jones & Bartlett
12 Lead ECG Interpretation: Color Coding for MI s
 12 Lead ECG Interpretation: Color Coding for MI s Anna E. Story, RN, MS Director, Continuing Professional Education Critical Care Nurse Online Instructional Designer 2004 Anna Story 1 Objectives review
12 Lead ECG Interpretation: Color Coding for MI s Anna E. Story, RN, MS Director, Continuing Professional Education Critical Care Nurse Online Instructional Designer 2004 Anna Story 1 Objectives review
12 Lead EKG Chapter 4 Worksheet
 Match the following using the word bank. 1. A form of arteriosclerosis in which the thickening and hardening of the vessels walls are caused by an accumulation of fatty deposits in the innermost lining
Match the following using the word bank. 1. A form of arteriosclerosis in which the thickening and hardening of the vessels walls are caused by an accumulation of fatty deposits in the innermost lining
Preface: Wang s Viewpoints
 AHA/ACCF/HRS Recommendations for the Standardization and Interpretation of the Electrocardiogram: Part IV, Ischemia and Infarction Presented by: WANG, TZONG LUEN, MD, PhD, JM, FACC, FESC, FCAPSC Professor,
AHA/ACCF/HRS Recommendations for the Standardization and Interpretation of the Electrocardiogram: Part IV, Ischemia and Infarction Presented by: WANG, TZONG LUEN, MD, PhD, JM, FACC, FESC, FCAPSC Professor,
12 Lead EKG. The Basics
 12 Lead EKG The Basics Objectives Demonstrate proper 12 EKG lead placement Determine electrical axis Identify ST and T wave changes as they relate to myocardial ischemia Describe possible complications
12 Lead EKG The Basics Objectives Demonstrate proper 12 EKG lead placement Determine electrical axis Identify ST and T wave changes as they relate to myocardial ischemia Describe possible complications
Masqueraders of STEMI
 Masqueraders of STEMI Steven M. Costa, M.D. Assistant Professor Department of Medicine Division of Cardiology Scott & White Memorial Hospital and Clinic Texas A&M University Health Science Center Disclosures
Masqueraders of STEMI Steven M. Costa, M.D. Assistant Professor Department of Medicine Division of Cardiology Scott & White Memorial Hospital and Clinic Texas A&M University Health Science Center Disclosures
By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG
 By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG recording Identify the ECG changes that occur in the presence
By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG recording Identify the ECG changes that occur in the presence
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series
 ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
Other 12-Lead ECG Findings
 Other 12-Lead ECG Findings Left Atrial Enlargement Left atrial enlargement is illustrated by increased P wave duration in lead II, top ECG, and by the prominent negative P terminal force in lead V1, bottom
Other 12-Lead ECG Findings Left Atrial Enlargement Left atrial enlargement is illustrated by increased P wave duration in lead II, top ECG, and by the prominent negative P terminal force in lead V1, bottom
ECG pre-reading manual. Created for the North West Regional EMET training program
 ECG pre-reading manual Created for the North West Regional EMET training program Author:- Dr Juan Carlos Ascencio-Lane juan.ascencio-lane@ths.tas.gov.au 1 Disclaimer This handbook has been created for
ECG pre-reading manual Created for the North West Regional EMET training program Author:- Dr Juan Carlos Ascencio-Lane juan.ascencio-lane@ths.tas.gov.au 1 Disclaimer This handbook has been created for
A Review of Cardiac Pathophysiology and EKG. Jamie Dyson PT, DPT Kathy Swanick PT, DPT, OCS
 A Review of Cardiac Pathophysiology and EKG Jamie Dyson PT, DPT Kathy Swanick PT, DPT, OCS Cardiac Pathophysiology Coronary Artery Disease Congestive Heart Failure Valvular Heart Disease Athletic Heart
A Review of Cardiac Pathophysiology and EKG Jamie Dyson PT, DPT Kathy Swanick PT, DPT, OCS Cardiac Pathophysiology Coronary Artery Disease Congestive Heart Failure Valvular Heart Disease Athletic Heart
Acute Myocardial Infarction. Willis E. Godin D.O., FACC
 Acute Myocardial Infarction Willis E. Godin D.O., FACC Acute Myocardial Infarction Definition: Decreased delivery of oxygen and nutrients to the myocardium Myocardial tissue necrosis causing irreparable
Acute Myocardial Infarction Willis E. Godin D.O., FACC Acute Myocardial Infarction Definition: Decreased delivery of oxygen and nutrients to the myocardium Myocardial tissue necrosis causing irreparable
UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME. DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18
 Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18") UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18 INTRODUCTION The clinical entities that comprise acute coronary syndromes (ACS)-ST-segment
UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18 INTRODUCTION The clinical entities that comprise acute coronary syndromes (ACS)-ST-segment
Acute chest pain and ECG need for immediate coronary angiography?
 Acute chest pain and ECG need for immediate coronary angiography? Kjell Nikus, MD, PhD Heart Center, Tampere University Hospital, Finland and Samuel Sclarovsky, MD, PhD Tel Aviv University, Israel There
Acute chest pain and ECG need for immediate coronary angiography? Kjell Nikus, MD, PhD Heart Center, Tampere University Hospital, Finland and Samuel Sclarovsky, MD, PhD Tel Aviv University, Israel There
Acute Myocardial Infarction
 Acute Myocardial Infarction Hafeza Shaikh, DO, FACC, RPVI Lourdes Cardiology Services Asst.Program Director, Cardiology Fellowship Associate Professor, ROWAN-SOM Acute Myocardial Infarction Definition:
Acute Myocardial Infarction Hafeza Shaikh, DO, FACC, RPVI Lourdes Cardiology Services Asst.Program Director, Cardiology Fellowship Associate Professor, ROWAN-SOM Acute Myocardial Infarction Definition:
A walk through a STEMI
 A walk through a STEMI M.M. s Story Kim Robison Ashley Corcoran Situation M.M. is an 82 year old male brought in by private vehicle on 10/22/17 to the Emergency Department Pt. c/o left arm numbness, pain
A walk through a STEMI M.M. s Story Kim Robison Ashley Corcoran Situation M.M. is an 82 year old male brought in by private vehicle on 10/22/17 to the Emergency Department Pt. c/o left arm numbness, pain
12 Lead Interpretation
 12 Lead Interpretation Objectives Ischemia, injury and infarction ECG complex review J point ST segment STEMI recognition Ischemia to Infarct Infarction is an evolving process As the infarct evolves ECG
12 Lead Interpretation Objectives Ischemia, injury and infarction ECG complex review J point ST segment STEMI recognition Ischemia to Infarct Infarction is an evolving process As the infarct evolves ECG
Acute Coronary Syndrome. Emergency Department Updated Jan. 2017
 Acute Coronary Syndrome Emergency Department Updated Jan. 2017 Goals and Objectives To reduce mortality and morbidity for people who have cardiovascular disease, with a focus on those who experience an
Acute Coronary Syndrome Emergency Department Updated Jan. 2017 Goals and Objectives To reduce mortality and morbidity for people who have cardiovascular disease, with a focus on those who experience an
12 Lead Acquisition and Interpretation APRIL 23 11:00 AM
 12 Lead Acquisition and Interpretation APRIL 23 11:00 AM Presented by : Jennifer Robson, Prehospital Care Specialist Dr. Don Eby, Local Medical Director Objectives Upon completion of this webinar, you
12 Lead Acquisition and Interpretation APRIL 23 11:00 AM Presented by : Jennifer Robson, Prehospital Care Specialist Dr. Don Eby, Local Medical Director Objectives Upon completion of this webinar, you
Electrocardiography for Healthcare Professionals. Chapter 14 Basic 12-Lead ECG Interpretation
 Electrocardiography for Healthcare Professionals Chapter 14 Basic 12-Lead ECG Interpretation 2012 The Companies, Inc. All rights reserved. Learning Outcomes 14.1 Discuss the anatomic views seen on a 12-lead
Electrocardiography for Healthcare Professionals Chapter 14 Basic 12-Lead ECG Interpretation 2012 The Companies, Inc. All rights reserved. Learning Outcomes 14.1 Discuss the anatomic views seen on a 12-lead
Electrocardiography 501: ECG Findings You Might Miss
 Electrocardiography 501: ECG Findings You Might Miss Christopher B. Colwell, M.D. City of San Francisco EMS Zuckerberg San Francisco General Hospital and Trauma Center Disclosures None 12-Lead EKG Paramedics
Electrocardiography 501: ECG Findings You Might Miss Christopher B. Colwell, M.D. City of San Francisco EMS Zuckerberg San Francisco General Hospital and Trauma Center Disclosures None 12-Lead EKG Paramedics
Case Study 50 YEAR OLD MALE WITH UNSTABLE ANGINA
 Case Study 50 YEAR OLD MALE WITH UNSTABLE ANGINA Case History A 50-year-old man with type 1 diabetes mellitus and hypertension presents after experiencing 1 hour of midsternal chest pain that began after
Case Study 50 YEAR OLD MALE WITH UNSTABLE ANGINA Case History A 50-year-old man with type 1 diabetes mellitus and hypertension presents after experiencing 1 hour of midsternal chest pain that began after
Chapter 76 Acute Coronary Syndromes Part A
 Chapter 76 Acute Coronary Syndromes Part A Episode Overview: 1. Define Stable Angina, UA, AMI 2. Describe the pathophysiology of AMI 3. What are the components of prehospital management of AMI 4. List
Chapter 76 Acute Coronary Syndromes Part A Episode Overview: 1. Define Stable Angina, UA, AMI 2. Describe the pathophysiology of AMI 3. What are the components of prehospital management of AMI 4. List
3/4/2018. March Martina Frost, PA C Desert Cardiology. Electricity moving towards/away from electrode create downward/upward directions of waves
 March 2018 Martina Frost, PA C Desert Cardiology Electricity moving towards/away from electrode create downward/upward directions of waves Frontal view Limb leads: I, II, III, avl, avf, (avr) Horizontal
March 2018 Martina Frost, PA C Desert Cardiology Electricity moving towards/away from electrode create downward/upward directions of waves Frontal view Limb leads: I, II, III, avl, avf, (avr) Horizontal
Heart disease remains the leading cause of morbidity and mortality in industrialized nations. It accounts for nearly 40% of all deaths in the United
 Heart disease remains the leading cause of morbidity and mortality in industrialized nations. It accounts for nearly 40% of all deaths in the United States, totaling about 750,000 individuals annually
Heart disease remains the leading cause of morbidity and mortality in industrialized nations. It accounts for nearly 40% of all deaths in the United States, totaling about 750,000 individuals annually
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016
 Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
Family Medicine for English language students of Medical University of Lodz ECG. Jakub Dorożyński
 Family Medicine for English language students of Medical University of Lodz ECG Jakub Dorożyński Parts of an ECG The standard ECG has 12 leads: six of them are considered limb leads because they are placed
Family Medicine for English language students of Medical University of Lodz ECG Jakub Dorożyński Parts of an ECG The standard ECG has 12 leads: six of them are considered limb leads because they are placed
Electrocardiography. Hilal Al Saffar College of Medicine,Baghdad University
 Electrocardiography Hilal Al Saffar College of Medicine,Baghdad University Which of the following is True 1. PR interval, represent the time taken for the impulse to travel from SA node to AV nose. 2.
Electrocardiography Hilal Al Saffar College of Medicine,Baghdad University Which of the following is True 1. PR interval, represent the time taken for the impulse to travel from SA node to AV nose. 2.
2/7/ LEAD ECG CASE STUDIES Lisa Riggs MSN, RN, ACNS-BC, CCRN-K CASE #1 WHAT ELSE WOULD YOU ASSESS? WHAT S YOUR DIAGNOSIS?
 12 LEAD ECG CASE STUDIES Lisa Riggs MSN, RN, ACNS-BC, CCRN-K CASE #1 31 y/o male is a direct admit from the physician s office with c/o chest pain and SOA WHAT ELSE WOULD YOU ASSESS? WHAT S YOUR DIAGNOSIS?
12 LEAD ECG CASE STUDIES Lisa Riggs MSN, RN, ACNS-BC, CCRN-K CASE #1 31 y/o male is a direct admit from the physician s office with c/o chest pain and SOA WHAT ELSE WOULD YOU ASSESS? WHAT S YOUR DIAGNOSIS?
Preface: Wang s Viewpoints
 AHA/ACCF/HRS Recommendations for the Standardization and Interpretation of the Electrocardiogram: Ischemia and Infarction 103.10.07 Presented by: WANG, TZONG LUEN, MD, PhD, JM, FACC, FESC, FCAPSC Professor,
AHA/ACCF/HRS Recommendations for the Standardization and Interpretation of the Electrocardiogram: Ischemia and Infarction 103.10.07 Presented by: WANG, TZONG LUEN, MD, PhD, JM, FACC, FESC, FCAPSC Professor,
Coronary Heart Disease. Raja Nursing Instructor RN, DCHN, Post RN. BSc.N
 Coronary Heart Disease Raja Nursing Instructor RN, DCHN, Post RN. BSc.N 31/03/2016 Objectives Define coronary heart disease (CHD). Identify the causes and risk factors of CHD Discuss the pathophysiological
Coronary Heart Disease Raja Nursing Instructor RN, DCHN, Post RN. BSc.N 31/03/2016 Objectives Define coronary heart disease (CHD). Identify the causes and risk factors of CHD Discuss the pathophysiological
Comments or Questions? me:
 Comments or Questions? Email me: amalmattu@comcast.net Interested in short video tutorials on electrocardiography? Check out www.ecgweekly.com Subscription fee < cost of a cup of coffee/week Covers every
Comments or Questions? Email me: amalmattu@comcast.net Interested in short video tutorials on electrocardiography? Check out www.ecgweekly.com Subscription fee < cost of a cup of coffee/week Covers every
ECG Cases and Questions. Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology
 ECG Cases and Questions Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology 32 yo female Life Insurance Physical 56 yo male with chest pain Terminology Injury ST elevation Ischemia T wave inversion
ECG Cases and Questions Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology 32 yo female Life Insurance Physical 56 yo male with chest pain Terminology Injury ST elevation Ischemia T wave inversion
Understanding the 12-lead ECG, part II
 Bundle-branch blocks Understanding the 12-lead ECG, part II Most common electrocardiogram (ECG) abnormality Appears as a wider than normal S complex Occurs when one of the two bundle branches can t conduct
Bundle-branch blocks Understanding the 12-lead ECG, part II Most common electrocardiogram (ECG) abnormality Appears as a wider than normal S complex Occurs when one of the two bundle branches can t conduct
Chest Pain. Dr Robert Huggett Consultant Cardiologist
 Chest Pain Dr Robert Huggett Consultant Cardiologist Outline Diagnosis of cardiac chest pain 2016 NICE update on stable chest pain Assessment of unstable chest pain/acs and MI definition Scope of the
Chest Pain Dr Robert Huggett Consultant Cardiologist Outline Diagnosis of cardiac chest pain 2016 NICE update on stable chest pain Assessment of unstable chest pain/acs and MI definition Scope of the
REtrive. REpeat. RElearn Design by. Test-Enhanced Learning based ECG practice E-book
 Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Foundations EKG I - Unit 1 Summary
 Foundations EKG I - Unit 1 Summary The accurate diagnosis of ST elevation myocardial infarction (STEMI) is one of the most time critical duties in the practice of EM. Diagnosis is not always easy so guidelines
Foundations EKG I - Unit 1 Summary The accurate diagnosis of ST elevation myocardial infarction (STEMI) is one of the most time critical duties in the practice of EM. Diagnosis is not always easy so guidelines
Marcin Dada, MD December 03, 2013
 STEMI Imposters Marcin Dada, MD December 03, 2013 Marcin Dada, MD Associate Director, Chest Pain Center Hartford Hospital, Hartford, CT Member, AHA Mission Lifeline Steering Committee Outline of Topics
STEMI Imposters Marcin Dada, MD December 03, 2013 Marcin Dada, MD Associate Director, Chest Pain Center Hartford Hospital, Hartford, CT Member, AHA Mission Lifeline Steering Committee Outline of Topics
Acute Coronary Syndromes
 Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist. Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI
 Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
10 ECGs No Practitioner Can Afford to Miss. Objectives
 10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology
 Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
Difficult Data Definitions and Scenario s
 Difficult Data Definitions and Scenario s Presenter Disclosure Information Cornelia Anderson BSN, RN To following relationships exist related to this presentation: No Disclosures Objectives Discuss key
Difficult Data Definitions and Scenario s Presenter Disclosure Information Cornelia Anderson BSN, RN To following relationships exist related to this presentation: No Disclosures Objectives Discuss key
Basic electrocardiography reading. R3 lee wei-chieh
 Basic electrocardiography reading R3 lee wei-chieh The Normal Conduction System Lead Placement avf Limb Leads Precordial Leads Interpretation Rate Rhythm Interval Axis Chamber abnormality QRST change What
Basic electrocardiography reading R3 lee wei-chieh The Normal Conduction System Lead Placement avf Limb Leads Precordial Leads Interpretation Rate Rhythm Interval Axis Chamber abnormality QRST change What
15 th Sukaman Memorial Lecture ST Segment Elevation: New Electrocardiographic Insights in 2014
 DOI 10.7603/s40602-016-0006-3 ASEAN Heart Journal http://www.globalsciencejournals.com/journal/40602 Vol. 24, no.1, 98 105 (2016) ISSN: 2315-4551 15 th Sukaman Memorial Lecture ST Segment Elevation: New
DOI 10.7603/s40602-016-0006-3 ASEAN Heart Journal http://www.globalsciencejournals.com/journal/40602 Vol. 24, no.1, 98 105 (2016) ISSN: 2315-4551 15 th Sukaman Memorial Lecture ST Segment Elevation: New
MICS OF MYOCARDIAL ISCHEMIA AND INFARCTION REVISED FOR LAS VEGAS
 ECG MIMICS OF MYOCARDIAL ISCHEMIA AND INFARCTION 102.06.05 Tzong-Luen Wang MD, PhD, JM, FESC, FACC Professor. Medical School, Fu-Jen Catholic University Chief, Emergency Department, Shin-Kong Wu Ho-Su
ECG MIMICS OF MYOCARDIAL ISCHEMIA AND INFARCTION 102.06.05 Tzong-Luen Wang MD, PhD, JM, FESC, FACC Professor. Medical School, Fu-Jen Catholic University Chief, Emergency Department, Shin-Kong Wu Ho-Su
Common Codes for ICD-10
 Common Codes for ICD-10 Specialty: Cardiology *Always utilize more specific codes first. ABNORMALITIES OF HEART RHYTHM ICD-9-CM Codes: 427.81, 427.89, 785.0, 785.1, 785.3 R00.0 Tachycardia, unspecified
Common Codes for ICD-10 Specialty: Cardiology *Always utilize more specific codes first. ABNORMALITIES OF HEART RHYTHM ICD-9-CM Codes: 427.81, 427.89, 785.0, 785.1, 785.3 R00.0 Tachycardia, unspecified
Section V. Objectives
 Section V Landscape of an MI Objectives At the conclusion of this presentation the participant will be able to Outline a systematic approach to 12 lead ECG interpretation Demonstrate the process for determining
Section V Landscape of an MI Objectives At the conclusion of this presentation the participant will be able to Outline a systematic approach to 12 lead ECG interpretation Demonstrate the process for determining
Ischemic Heart Diseases. Dr. Nabila Hamdi MD, PhD
 Ischemic Heart Diseases Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast the different types of angina regarding their pathogenesis, clinical manifestations and evolution. Discuss myocardial infarct,
Ischemic Heart Diseases Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast the different types of angina regarding their pathogenesis, clinical manifestations and evolution. Discuss myocardial infarct,
Acute Coronary Syndrome
 ACUTE CORONOARY SYNDROME, ANGINA & ACUTE MYOCARDIAL INFARCTION Administrative Consultant Service 3/17 Acute Coronary Syndrome Acute Coronary Syndrome has evolved as a useful operational term to refer to
ACUTE CORONOARY SYNDROME, ANGINA & ACUTE MYOCARDIAL INFARCTION Administrative Consultant Service 3/17 Acute Coronary Syndrome Acute Coronary Syndrome has evolved as a useful operational term to refer to
MWLCEMS SYSTEM Continuing Education Packet Management of the Acute MI Patient
 MWLCEMS SYSTEM Continuing Education Packet Management of the Acute MI Patient In this CE we will discuss the patient presenting with an acute ST-Elevation Myocardial Infarction (STEMI) Definition: Myocardial
MWLCEMS SYSTEM Continuing Education Packet Management of the Acute MI Patient In this CE we will discuss the patient presenting with an acute ST-Elevation Myocardial Infarction (STEMI) Definition: Myocardial
Disclosure. 3. ST depression indicative of ischemia is most commonly observed in leads: 1. V1-V2. 2. I and avl 3. V
 Interpreting Stress Induced Ischemia by ECG, Bundle Branch Block & Arrhythmias Disclosure Gregory S Thomas MD, MPH Medical Director, MemorialCare Heart & Vascular Institute, Long Beach Memorial Astellas
Interpreting Stress Induced Ischemia by ECG, Bundle Branch Block & Arrhythmias Disclosure Gregory S Thomas MD, MPH Medical Director, MemorialCare Heart & Vascular Institute, Long Beach Memorial Astellas
TOPICS IN EMERGENCY MEDICINE SEMI-FINAL
 RISK ASSESSMENT IN PATIENTS WITH CHEST PAIN Nora Goldschlager, M.D. FACP, FACC, FAHA, FHRS Cardiology - San Francisco General Hospital UCSF Disclosures: None 1 CHEST PAIN NOT DUE TO MYOCARDIAL ISCHEMIA
RISK ASSESSMENT IN PATIENTS WITH CHEST PAIN Nora Goldschlager, M.D. FACP, FACC, FAHA, FHRS Cardiology - San Francisco General Hospital UCSF Disclosures: None 1 CHEST PAIN NOT DUE TO MYOCARDIAL ISCHEMIA
Goals: Widen Your Understanding of the Wide QRS!
 Goals: Widen Your Understanding of the Wide QRS! 1. Describe an approach to diagnosis of LBBB 2. Describe the predictive value of New LBBB 3. Describe the ST segment changes that are diagnostic of AMI
Goals: Widen Your Understanding of the Wide QRS! 1. Describe an approach to diagnosis of LBBB 2. Describe the predictive value of New LBBB 3. Describe the ST segment changes that are diagnostic of AMI
A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD
 A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD NAVAL HOSPITAL OF ATHENS case presentation Female, 81yo Hx: diabetes mellitus, hypertension, chronic anaemia presented
A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD NAVAL HOSPITAL OF ATHENS case presentation Female, 81yo Hx: diabetes mellitus, hypertension, chronic anaemia presented
Different ECG patterns at presentation in ACS. D. Goldwasser F. Molina A. Bayes de Luna
 Different ECG patterns at presentation in ACS D. Goldwasser F. Molina A. Bayes de Luna Acute Coronary syndromes: The importance of the ECG There are two types of ACS: STE- ACS and Non STE-ACS The most
Different ECG patterns at presentation in ACS D. Goldwasser F. Molina A. Bayes de Luna Acute Coronary syndromes: The importance of the ECG There are two types of ACS: STE- ACS and Non STE-ACS The most
E CG Challenges. The ST segment on an electrocardiogram (ECG) correlates to the plateau. Wellens Syndrome
 correlates to the plateau. Wellens Syndrome") AACN Advanced Critical Care Volume 29, Number 3, pp 360-364 2018 AACN E CG Challenges Karen M. Marzlin, DNP, RN, CCNS, ACNPC-AG, CCRN-CMC, CHFN Department Editor Wellens Syndrome Karen M. Marzlin, DNP,
AACN Advanced Critical Care Volume 29, Number 3, pp 360-364 2018 AACN E CG Challenges Karen M. Marzlin, DNP, RN, CCNS, ACNPC-AG, CCRN-CMC, CHFN Department Editor Wellens Syndrome Karen M. Marzlin, DNP,
WE ARE STEMI HUNTERS. LearningObjectives. I have no relevant disclosures. Myth: Jennifer Carlquist PA-C, ER CAQ
 WE ARE STEMI HUNTERS Jennifer Carlquist PA-C, ER CAQ Salinas Valley Memorial, ER Central Coast Cardiology, Specializing in EP LearningObjectives How to use pattern recognition to detect ischemia Triage
WE ARE STEMI HUNTERS Jennifer Carlquist PA-C, ER CAQ Salinas Valley Memorial, ER Central Coast Cardiology, Specializing in EP LearningObjectives How to use pattern recognition to detect ischemia Triage
2017 Cardiology Survival Guide
 2017 Cardiology Survival Guide Chapter 4: Cardiac Catheterization/Percutaneous Coronary Intervention A cardiac catheterization involves a physician inserting a thin plastic tube (catheter) into an artery
2017 Cardiology Survival Guide Chapter 4: Cardiac Catheterization/Percutaneous Coronary Intervention A cardiac catheterization involves a physician inserting a thin plastic tube (catheter) into an artery
Objectives. Identify early signs and symptoms of Acute Coronary Syndrome Initiate proper protocol for ACS patient 10/2013 2
 10/2013 1 Objectives Identify early signs and symptoms of Acute Coronary Syndrome Initiate proper protocol for ACS patient 10/2013 2 Purpose of this Education Module: Chest Pain Center Accreditation involves
10/2013 1 Objectives Identify early signs and symptoms of Acute Coronary Syndrome Initiate proper protocol for ACS patient 10/2013 2 Purpose of this Education Module: Chest Pain Center Accreditation involves
CASE 10. What would the ST segment of this ECG look like? On which leads would you see this ST segment change? What does the T wave represent?
 CASE 10 A 57-year-old man presents to the emergency center with complaints of chest pain with radiation to the left arm and jaw. He reports feeling anxious, diaphoretic, and short of breath. His past history
CASE 10 A 57-year-old man presents to the emergency center with complaints of chest pain with radiation to the left arm and jaw. He reports feeling anxious, diaphoretic, and short of breath. His past history
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH
 ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
Takotsubo Cardiomyopathy: Pathophysiology and Assessment
 Takotsubo Cardiomyopathy: Pathophysiology and Assessment Roberto M Lang, MD Tako-Tsubo Cardiomyopathy Broken Heart Syndrome Apical Balooning 1. Sato H, Tateishi H, Uchida T, et al. Takotsubo type cardiomyopathy
Takotsubo Cardiomyopathy: Pathophysiology and Assessment Roberto M Lang, MD Tako-Tsubo Cardiomyopathy Broken Heart Syndrome Apical Balooning 1. Sato H, Tateishi H, Uchida T, et al. Takotsubo type cardiomyopathy
ST SEGMENT IN LEAD A VR IN ACUTE INFERIOR MYOCARDIAL INFARCTION
 ST SEGMENT IN LEAD A VR IN ACUTE INFERIOR MYOCARDIAL INFARCTION Pages with reference to book, From 365 To 366 Shehbaz A. Kureshi, Yoshiharu Yonekura, Yutaka Konishi, Kanji Torizuka ( Kyoto University School
ST SEGMENT IN LEAD A VR IN ACUTE INFERIOR MYOCARDIAL INFARCTION Pages with reference to book, From 365 To 366 Shehbaz A. Kureshi, Yoshiharu Yonekura, Yutaka Konishi, Kanji Torizuka ( Kyoto University School
SIMPLY ECGs. Dr William Dooley
 SIMPLY ECGs Dr William Dooley Content Basic ECG interpretation pattern Some common (examined) abnormalities Presenting ECGs in context Setting up an ECG Setting up an ECG 1 V1-4 th Right intercostal space
SIMPLY ECGs Dr William Dooley Content Basic ECG interpretation pattern Some common (examined) abnormalities Presenting ECGs in context Setting up an ECG Setting up an ECG 1 V1-4 th Right intercostal space
10/22/16. Lay of the land. Definition of ACS. Why do we worry about ST elevations?
 Lay of the land Update on Acute Coronary Syndrome: Five Things Hospitalists Must Know Dhruv S. Kazi, MD, MSc, MS Assistant Professor Department of Medicine (Cardiology), Department of Epidemiology and
Lay of the land Update on Acute Coronary Syndrome: Five Things Hospitalists Must Know Dhruv S. Kazi, MD, MSc, MS Assistant Professor Department of Medicine (Cardiology), Department of Epidemiology and
Management of Coronary Artery Spasm
 Management of Coronary Artery Spasm J. C. Kaski and R. Arroyo-Espliguero Cardiovascular Biology Research Centre Division of Cardiac and Vascular Sciences St George s, University of London Prinzmetal s
Management of Coronary Artery Spasm J. C. Kaski and R. Arroyo-Espliguero Cardiovascular Biology Research Centre Division of Cardiac and Vascular Sciences St George s, University of London Prinzmetal s
CME Article Brugada pattern masking anterior myocardial infarction
 Electrocardiography Series Singapore Med J 2011; 52(9) : 647 CME Article Brugada pattern masking anterior myocardial infarction Seow S C, Omar A R, Hong E C T Cardiology Department, National University
Electrocardiography Series Singapore Med J 2011; 52(9) : 647 CME Article Brugada pattern masking anterior myocardial infarction Seow S C, Omar A R, Hong E C T Cardiology Department, National University
APPENDIX F: CASE REPORT FORM
 APPENDIX F: CASE REPORT FORM Instruction: Complete this form to notify all ACS admissions at your centre to National Cardiovascular Disease Registry. Where check boxes are provided, check ( ) one or more
APPENDIX F: CASE REPORT FORM Instruction: Complete this form to notify all ACS admissions at your centre to National Cardiovascular Disease Registry. Where check boxes are provided, check ( ) one or more
Essam Mahfouz, MD. Professor of Cardiology, Mansoura University
 By Essam Mahfouz, MD. Professor of Cardiology, Mansoura University Agenda Definitions Classifications Epidemiology Risk stratification What is new? What is MI? Myocardial infarction is the death of part
By Essam Mahfouz, MD. Professor of Cardiology, Mansoura University Agenda Definitions Classifications Epidemiology Risk stratification What is new? What is MI? Myocardial infarction is the death of part
CABG Surgery following STEMI
 CABG Surgery following STEMI Susana Harrington, MS,APRN-NP Cardio-Thoracic Surgery Nebraska Methodist Hospital February 15, 2018 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction:
CABG Surgery following STEMI Susana Harrington, MS,APRN-NP Cardio-Thoracic Surgery Nebraska Methodist Hospital February 15, 2018 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction:
Solutions for Every Day Problems Cardiologists and the ECG: Are We Really That Good at It? Part II Daniel José Piñeiro Profesor Titular de Medicina,
 Solutions for Every Day Problems Cardiologists and the ECG: Are We Really That Good at It? Part II Daniel José Piñeiro Profesor Titular de Medicina, Universidad de Buenos Aires, Argentina Member, Membership
Solutions for Every Day Problems Cardiologists and the ECG: Are We Really That Good at It? Part II Daniel José Piñeiro Profesor Titular de Medicina, Universidad de Buenos Aires, Argentina Member, Membership
12 Lead ECG. Presented by Rebecca Sevigny BSN, RN Professional Practice & Development Dept.
 12 Lead ECG Presented by Rebecca Sevigny BSN, RN Professional Practice & Development Dept. Two Main Coronary Arteries RCA LCA which branches into Left Anterior Descending Circumflex Artery Two Main Coronary
12 Lead ECG Presented by Rebecca Sevigny BSN, RN Professional Practice & Development Dept. Two Main Coronary Arteries RCA LCA which branches into Left Anterior Descending Circumflex Artery Two Main Coronary
A few new tools for better detection and understanding of STEMIs in the field.
 A few new tools for better detection and understanding of STEMIs in the field. Let s talk, prep and placement. Try to shoot for quality, consistency and no artifact! (looking sometimes for 1 or 2 mm changes)
A few new tools for better detection and understanding of STEMIs in the field. Let s talk, prep and placement. Try to shoot for quality, consistency and no artifact! (looking sometimes for 1 or 2 mm changes)
OVERVIEW ACUTE CORONARY SYNDROME SYMPTOMS 9/30/14 TYPICAL WHAT IS ACUTE CORONARY SYNDROME? SYMPTOMS, IDENTIFICATION, MANAGEMENT
 OVERVIEW ACUTE CORONARY SYNDROME SYMPTOMS, IDENTIFICATION, MANAGEMENT OCTOBER 7, 2014 PETE PERAUD, MD SYMPTOMS TYPICAL ATYPICAL IDENTIFICATION EKG CARDIAC BIOMARKERS STEMI VS NON-STEMI VS USA MANAGEMENT
OVERVIEW ACUTE CORONARY SYNDROME SYMPTOMS, IDENTIFICATION, MANAGEMENT OCTOBER 7, 2014 PETE PERAUD, MD SYMPTOMS TYPICAL ATYPICAL IDENTIFICATION EKG CARDIAC BIOMARKERS STEMI VS NON-STEMI VS USA MANAGEMENT
Supplementary Material to Mayer et al. A comparative cohort study on personalised
 Suppl. Table : Baseline characteristics of the patients. Characteristic Modified cohort Non-modified cohort P value (n=00) Age years 68. ±. 69.5 ±. 0. Female sex no. (%) 60 (0.0) 88 (.7) 0.0 Body Mass
Suppl. Table : Baseline characteristics of the patients. Characteristic Modified cohort Non-modified cohort P value (n=00) Age years 68. ±. 69.5 ±. 0. Female sex no. (%) 60 (0.0) 88 (.7) 0.0 Body Mass
Biphasic T-wave in patient with chest pain (Wellens syndrome)
") www.edoriumjournals.com CLINICAL IMAGES PEER REVIEWED OPEN ACCESS Biphasic T-wave in patient with chest pain (Wellens syndrome) Ahmed Zedan, Osama Mukarram, Umer Malik, Raja Naidu ABSTRACT Abstract is
www.edoriumjournals.com CLINICAL IMAGES PEER REVIEWED OPEN ACCESS Biphasic T-wave in patient with chest pain (Wellens syndrome) Ahmed Zedan, Osama Mukarram, Umer Malik, Raja Naidu ABSTRACT Abstract is
Ischemic Heart Disease
 Ischemic Heart Disease Dr Rodney Itaki Lecturer Division of Pathology University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology General Consideration Results from partial
Ischemic Heart Disease Dr Rodney Itaki Lecturer Division of Pathology University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology General Consideration Results from partial
Bundle Branch & Fascicular Blocks. Reading Assignment (p53-58 in Outline )
") Bundle Branch & Fascicular Blocks Reading Assignment (p53-58 in Outline ) Objectives 1. QRS analysis of Right and Left BBB 2. Uncomplicated vs complicated BBB 3. Diagnosis of RBBB with LAFB and LPFB 4.
Bundle Branch & Fascicular Blocks Reading Assignment (p53-58 in Outline ) Objectives 1. QRS analysis of Right and Left BBB 2. Uncomplicated vs complicated BBB 3. Diagnosis of RBBB with LAFB and LPFB 4.
12 Lead ECGs: Ischemia, Injury, Infarction
 12 Lead ECGs: Ischemia, Injury, Infarction This course has been awarded four (4) contact hours. This course expires on March 31, 2019. Copyright 2015 by RN.com. All Rights Reserved. Reproduction and distribution
12 Lead ECGs: Ischemia, Injury, Infarction This course has been awarded four (4) contact hours. This course expires on March 31, 2019. Copyright 2015 by RN.com. All Rights Reserved. Reproduction and distribution