What is Your Diagnosis?
|
|
|
- Buddy Goodwin
- 5 years ago
- Views:
Transcription
1 What is Your Diagnosis? A STORM R Dulgheru, Liege, Belgium


2 Faculty disclosure Raluca Dulgheru I have no financial relationships to disclose.
3 Case presentation 52 years old male Ongoing oppressive chest pain and severe dyspnoea (onset 6h before admission), but several episodes of chest pain in the past two weeks No known medical history Tabaco use (1 pac/day) Family history of premature heart disease (father with AMI at 45 years of age) Treatment: Omeprazole 20 mg/day
4 Clinical examination Distress, clammy skin Dyspnoea SaO2 = 92% on ambient air BP = 70/50 mmhg HR = 98 bpm Bilateral crackles up to the apices of both lungs No audible heart murmurs
5 ECG at admission
6 Arterial blood gas test at admission PH = 7.27 PCo2 = 56 mmhg Base excess = -2.6 mmol/l Standard bicarbonates 22.3 mmol/l Lactate 130 mg/l (normal range )
7 What is your diagnosis? 1. Acute pulmonary oedema 2. Acute pulmonary embolism 3. Cardiogenic shock 4. Respiratory acidosis of unknown aetiology
8 Cardiogenic shock Distress, clammy skin Dyspnoea SaO2 = 92% on ambient air BP = 70/50 mmhg HR = 98 bpm Bilateral crackles up to the apices of both lungs No audible heart murmurs Acute Heart Failure Signs Low BP and tissue hypo-perfusion signs Borderline tachycardia
9 What do you do next? 1. Send the patient to the cath lab for emergency coronary artery angiography 2. Angio CT of the thorax to rule out PE 3. Bed-side TTE 4. Bed-side chest X-ray

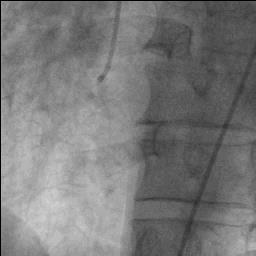
10 Coronary angiogram
11 Coronary angiogram
12 What is your diagnosis? 1. NSTEMI, severe three vessels disease complicated by cardiogenic shock 2. Cardiogenic shock, severe coronary artery disease but I need more to explain the clinical picture 3. Acute STEMI with IVS rupture

13 Cardiogenic shock, severe coronary artery disease but aetiology of shock is unknown yet
14 Ventriculography
15 What do you do next? 1. Call a friend to do an echo 2. Stent the right coronary artery 3. Call the lab to see the cardiac enzymes 4. Do a angio CT of the thorax
 LA")
 LA seems enlarged (chronic")
16 Ventriculography LV hyperdynamic (in discordance with the shock state) LA opacification in systole (Severe MR suspected) LA seems enlarged (chronic MR)
17 TTE
18 Blood samples at admission Hb 18 g/dl, Ht 52% Glucose 122 mg/dl Creatinine 1,14 mg/dl LDH 393 (<250) U/l CK 209 (<190) U/l CKMB 5.4 (<6.2) microg/l Troponin T hs 1291 ng/l (<14)
19 What is your diagnosis? 1. Cardiogenic shock, three vessels disease and IVS septal rupture 2. Cardiogenic shock and infero-posterior STEMI 3. Cardiogenic shock, NSTEMI, three vessels disease and severe chronic secondary MR 4. Cardiogenic shock, probably subacute MI, PM rupture, severe acute MR and three vessels disease
")
 microg/l Troponin T hs 1291 ng/l (<14) Floppy")
20 Q waves infero-posterior Inferior and infero-lateral wall akinesis Acute severe MR Cardiac enzyme tail LDH 393 (<250) U/l CK 209 (<190) U/l CKMB 5.4 (<6.2) microg/l Troponin T hs 1291 ng/l (<14) Floppy postero-medial PM suggestive of PM rupture


21 IABP and call a friend

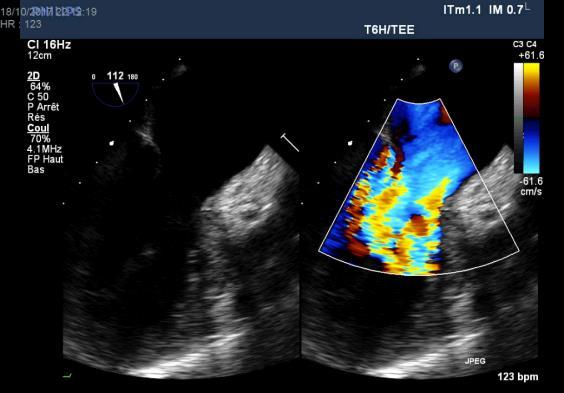

22 TOE in the OR
23 What does the echo show? 1. Complete transection of the postero-medial PM 2. Detachment of one of the antero-lateral PM heads 3. Complete transection of the antero-lateral PM 4. Detachment of one of the postero-medial PM heads
24 Detachment of one of the postero-medial PM heads
25 Clinical highlights 1. Angina recurrence in the context of subacute MI accompanied by sudden dyspnoea and followed by haemodynamic deterioration is suggestive of a mechanical complication of MI (PM rupture, IVS rupture, free-wall rupture) 2. Absence of cardiac murmur does not rule out acute MR 3. Cardiogenic shock in a patient with ACS needs prompt assessment of LV systolic function 4. Good/excellent LV systolic function suggests acute MR 5. Echocardiography is key exam to detect the MR aetiology



26 Echo highlights Complete transection of the papillary muscle is relatively rare, whereas rupture of the tip is more common Rupture of the tip of the PM Anterior mitral leaflet non involved, normal motion Complete transection Both leaflets with excessive motion
 occurs more often than rupture of the anterolateral papillary muscle (dual coronary")
27 Echo highlights Rupture of the posteromedial papillary muscle (supplied by a single coronary artery) occurs more often than rupture of the anterolateral papillary muscle (dual coronary supply)
28 Echo highlights Regional wall motion abnormalities may be subtle/unrecognized (hyperdynamic LV due to sudden decrease in afterload) Suboptimal transthoracic imaging windows (dyspnea, acute pulmonary oedema, patient lying flat) TOE may be required to confirm diagnosis (after endotracheal intubation in a non fasting patient)
29 Case particularities No occlusion of a coronary artery has been identified by coronarography which suggests spontaneous reperfusion, culprit artery was not identified by angio Wall motion abnormality was missed by conventional ventriculography but identified with TTE and TOE, indicating also the culprit vessel (RCA) Absence of severe tachycardia is not explained (chronotropic incompetence) Anterior leaflet was not involved because just one of the heads of the postero-medial papillary muscle was ruptured, probably the one giving chordae to the posterior leaflet Patient had three-vessels disease and late presentation after AMI which increases the risk of complications (such as PM rupture)
30 The silent storm Acknowledgements to Dr. Mathieu Lempereur and Prof. Mark Radermecker and his colleagues
A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD
 A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD NAVAL HOSPITAL OF ATHENS case presentation Female, 81yo Hx: diabetes mellitus, hypertension, chronic anaemia presented
A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD NAVAL HOSPITAL OF ATHENS case presentation Female, 81yo Hx: diabetes mellitus, hypertension, chronic anaemia presented
ECG Workshop. Nezar Amir
 ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
ANATOMICAL IMAGING USING 3D ECHOCARDIOGRAPHY IN PATIENTS WITH MECHANICAL COMPLICATIONS POST MYOCARDIAL INFARCTION
 Revista Română de Anatomie funcţională şi clinică, macro- şi microscopică şi de Antropologie Vol. XIV Nr. 2 2015 UPDATES ANATOMICAL IMAGING USING 3D ECHOCARDIOGRAPHY IN PATIENTS WITH MECHANICAL COMPLICATIONS
Revista Română de Anatomie funcţională şi clinică, macro- şi microscopică şi de Antropologie Vol. XIV Nr. 2 2015 UPDATES ANATOMICAL IMAGING USING 3D ECHOCARDIOGRAPHY IN PATIENTS WITH MECHANICAL COMPLICATIONS
Pulmonary Embolism Is it the Greatest Danger in Deep Vein Thrombosis?
 Difficult issues in Deep Vein Thrombosis: Pulmonary Embolism Is it the Greatest Danger in Deep Vein Thrombosis? Raluca Dulgheru; C Gherghinescu; B Dorobat; H Muresan; R Darabont; M Cinteza; D Vinereanu
Difficult issues in Deep Vein Thrombosis: Pulmonary Embolism Is it the Greatest Danger in Deep Vein Thrombosis? Raluca Dulgheru; C Gherghinescu; B Dorobat; H Muresan; R Darabont; M Cinteza; D Vinereanu
2/14/2018 CASE STUDIES: COMPLICATIONS OF MYOCARDIAL INFARCTION. Judy Hung, MD Cardiology Division Massachusetts General Hospital Boston, MA CASE 1
 CASE STUDIES: COMPLICATIONS OF MYOCARDIAL INFARCTION Judy Hung, MD Cardiology Division Massachusetts General Hospital Boston, MA CASE 1 1 PRESENTATION 57 yo male with a past medical history of hypertension
CASE STUDIES: COMPLICATIONS OF MYOCARDIAL INFARCTION Judy Hung, MD Cardiology Division Massachusetts General Hospital Boston, MA CASE 1 1 PRESENTATION 57 yo male with a past medical history of hypertension
A Diagnostic Dilemma saved by sound
 A Diagnostic Dilemma saved by sound Dr Syam Ravindranath MBBS DNB, Dr Ash Mukherjee FCEM FACEM We p r e s e n t a d i a g n o s t i c a l l y c h a l l e n g i n g s c e n a r i o in a 59 y e a r old f
A Diagnostic Dilemma saved by sound Dr Syam Ravindranath MBBS DNB, Dr Ash Mukherjee FCEM FACEM We p r e s e n t a d i a g n o s t i c a l l y c h a l l e n g i n g s c e n a r i o in a 59 y e a r old f
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases
 Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Difficult Data Definitions and Scenario s
 Difficult Data Definitions and Scenario s Presenter Disclosure Information Cornelia Anderson BSN, RN To following relationships exist related to this presentation: No Disclosures Objectives Discuss key
Difficult Data Definitions and Scenario s Presenter Disclosure Information Cornelia Anderson BSN, RN To following relationships exist related to this presentation: No Disclosures Objectives Discuss key
Practitioner Education Course
 2015 Practitioner Education Course ST Elevation Myocardial Infarction 2 Pathology Concept of vulnerable plaque Mild Atheroma Diagnosis IVUS OCT 3 Diagnosis This is based on : Clinical History ECG Changes.
2015 Practitioner Education Course ST Elevation Myocardial Infarction 2 Pathology Concept of vulnerable plaque Mild Atheroma Diagnosis IVUS OCT 3 Diagnosis This is based on : Clinical History ECG Changes.
Acute heart failure in a patient with lower urinary tract infection Case report of an infection-induced Reverse Takotsubo syndrome
 Acute heart failure in a patient with lower urinary tract infection Case report of an infection-induced Reverse Takotsubo syndrome N.Μoschos, A.Dimitra, E.Tsakiri, D.Stavrianakis, A.Nouli CARDIOLOGY DEPARTMENT
Acute heart failure in a patient with lower urinary tract infection Case report of an infection-induced Reverse Takotsubo syndrome N.Μoschos, A.Dimitra, E.Tsakiri, D.Stavrianakis, A.Nouli CARDIOLOGY DEPARTMENT
Complications of Myocardial Infarction
 Complications of Myocardial Infarction Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director,
Complications of Myocardial Infarction Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director,
Case-based session. Infective Endocarditis. Applying the new guidelines. A case of large vegetation with neurological complication.
 Case-based session. Infective Endocarditis. Applying the new guidelines. A case of large vegetation with neurological complication. María Nazarena Pizzi Hospital Universitari Vall d Hebron Barcelona. I
Case-based session. Infective Endocarditis. Applying the new guidelines. A case of large vegetation with neurological complication. María Nazarena Pizzi Hospital Universitari Vall d Hebron Barcelona. I
A Nightmare. R Dulgheru, CHU Liege
 A Nightmare R Dulgheru, CHU Liege Faculty disclosure Raluca Dulgheru I have no financial relationships to disclose. MB, 57 years old male 18/03/2016 to the ER for altered mental status, First weight name
A Nightmare R Dulgheru, CHU Liege Faculty disclosure Raluca Dulgheru I have no financial relationships to disclose. MB, 57 years old male 18/03/2016 to the ER for altered mental status, First weight name
STEMI and Cardiogenic Shock. The rules and solution. Dave Kettles St Dominics and Frere Hospitals East London ZA
 STEMI and Cardiogenic Shock. The rules and solution Dave Kettles St Dominics and Frere Hospitals East London ZA Definitions: Shock is a life threatening, but initially reversible state of cellular and
STEMI and Cardiogenic Shock. The rules and solution Dave Kettles St Dominics and Frere Hospitals East London ZA Definitions: Shock is a life threatening, but initially reversible state of cellular and
A walk through a STEMI
 A walk through a STEMI M.M. s Story Kim Robison Ashley Corcoran Situation M.M. is an 82 year old male brought in by private vehicle on 10/22/17 to the Emergency Department Pt. c/o left arm numbness, pain
A walk through a STEMI M.M. s Story Kim Robison Ashley Corcoran Situation M.M. is an 82 year old male brought in by private vehicle on 10/22/17 to the Emergency Department Pt. c/o left arm numbness, pain
A Qadeer Negahban. Cardiologist Barnsley Hospital United Kingdom
 A Qadeer Negahban Cardiologist Barnsley Hospital United Kingdom Tako Tsubo Cardiomyopathy Transient left ventricular (LV) apical ballooning syndrome Broken heart syndrome Stress induced myocardial stunning
A Qadeer Negahban Cardiologist Barnsley Hospital United Kingdom Tako Tsubo Cardiomyopathy Transient left ventricular (LV) apical ballooning syndrome Broken heart syndrome Stress induced myocardial stunning
Echocardiography as a diagnostic and management tool in medical emergencies
 Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
2. Case Report. 1. Introduction
 Case Reports in Cardiology Volume 2016, Article ID 3251032, 5 pages http://dx.doi.org/10.1155/2016/3251032 Case Report Ventricular Septal Perforation after Biventricular Takotsubo Cardiomyopathy Successfully
Case Reports in Cardiology Volume 2016, Article ID 3251032, 5 pages http://dx.doi.org/10.1155/2016/3251032 Case Report Ventricular Septal Perforation after Biventricular Takotsubo Cardiomyopathy Successfully
Progress. Four weeks later. What becomes of the broken hearted? What do you think her coronary angiogram shows? 18/06/2018.
 What becomes of the broken hearted? Stephen Glen What do you think her coronary angiogram shows? 1. Mid LAD stenosis 2. Ostial LAD stenosis 3. LMS stenosis 4. RCA occlusion 5. Normal Four weeks later CT
What becomes of the broken hearted? Stephen Glen What do you think her coronary angiogram shows? 1. Mid LAD stenosis 2. Ostial LAD stenosis 3. LMS stenosis 4. RCA occlusion 5. Normal Four weeks later CT
DISCUSSION QUESTION - 1
 CASE PRESENTATION 87 year old male No past history of diabetes, HTN, dyslipidemia or smoking Very active Medications: omeprazole for heart burn Admitted because of increasing retrosternal chest pressure
CASE PRESENTATION 87 year old male No past history of diabetes, HTN, dyslipidemia or smoking Very active Medications: omeprazole for heart burn Admitted because of increasing retrosternal chest pressure
You Won t Believe What I Saw on. Disclosures. Goals. Dimensions 2013 October 18 th Michael Pfeiffer, MD. No Financial Disclosures
 You Won t Believe What I Saw on that ECHO! Dimensions 2013 October 18 th Michael Pfeiffer, MD Disclosures No Financial Disclosures Goals Review unusual and unique echocardiographic images. Briefly present
You Won t Believe What I Saw on that ECHO! Dimensions 2013 October 18 th Michael Pfeiffer, MD Disclosures No Financial Disclosures Goals Review unusual and unique echocardiographic images. Briefly present
Takotsubo Cardiomyopathy
 Advances in Heart Disease 2008 Takotsubo Cardiomyopathy Mary O. Gray, MD, FAHA, FACC Associate Professor of Medicine University of California, San Francisco Staff Cardiologist and Training Faculty Divisions
Advances in Heart Disease 2008 Takotsubo Cardiomyopathy Mary O. Gray, MD, FAHA, FACC Associate Professor of Medicine University of California, San Francisco Staff Cardiologist and Training Faculty Divisions
Chest pain management. Ruvin Gabriel and Niels van Pelt August 2011
 Chest pain management Ruvin Gabriel and Niels van Pelt August 2011 Introduction Initial assessment Case 1 Case 2 and 3 Comparison of various diagnostic techniques Summary 1-2 % of GP consultations are
Chest pain management Ruvin Gabriel and Niels van Pelt August 2011 Introduction Initial assessment Case 1 Case 2 and 3 Comparison of various diagnostic techniques Summary 1-2 % of GP consultations are
UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME. DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18
 Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18") UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18 INTRODUCTION The clinical entities that comprise acute coronary syndromes (ACS)-ST-segment
UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18 INTRODUCTION The clinical entities that comprise acute coronary syndromes (ACS)-ST-segment
Complications of Acute MI Cases. Disclosures
 Complications of Acute MI Cases Neil J. Weissman, M.D. Director, CV Core Laboratories President, MedStar Health Research Inst Professor of Medicine, Georgetown Univ Washington, DC Disclosures Director
Complications of Acute MI Cases Neil J. Weissman, M.D. Director, CV Core Laboratories President, MedStar Health Research Inst Professor of Medicine, Georgetown Univ Washington, DC Disclosures Director
What is a myocardial infarction and how do we treat it? Paul Das Consultant Cardiologist North Wales Cardiac Centre Glan Clwyd Hospital
 What is a myocardial infarction and how do we treat it? Paul Das Consultant Cardiologist North Wales Cardiac Centre Glan Clwyd Hospital What is a myocardial infarction? THEY AINT WHAT THEY USED TO BE Case
What is a myocardial infarction and how do we treat it? Paul Das Consultant Cardiologist North Wales Cardiac Centre Glan Clwyd Hospital What is a myocardial infarction? THEY AINT WHAT THEY USED TO BE Case
All About STEMIs. Presented By: Brittney Urvand, RN, BSN, CCCC. Essentia Health Fargo Cardiovascular Program Manager.
 All About STEMIs Presented By: Brittney Urvand, RN, BSN, CCCC Essentia Health Fargo Cardiovascular Program Manager Updated 10/2/2018 None Disclosures Objectives Identify signs and symptoms of a heart attack
All About STEMIs Presented By: Brittney Urvand, RN, BSN, CCCC Essentia Health Fargo Cardiovascular Program Manager Updated 10/2/2018 None Disclosures Objectives Identify signs and symptoms of a heart attack
J. Schwitter, MD, FESC Section of Cardiology
 J. Schwitter, MD, FESC Section of Cardiology CMR Center of the CHUV University Hospital Lausanne - CHUV Switzerland Centre de RM Cardiaque J. Schwitter, MD, FESC Section of Cardiology CMR Center of the
J. Schwitter, MD, FESC Section of Cardiology CMR Center of the CHUV University Hospital Lausanne - CHUV Switzerland Centre de RM Cardiaque J. Schwitter, MD, FESC Section of Cardiology CMR Center of the
Cardiovascular emergencies. 05/March/2014 László Rudas Szeged
 Cardiovascular emergencies 05/March/2014 László Rudas Szeged Acute chest pain Acute heart failure Sudden cardiac death Acute chest pain What is the etiology? Chest pain signals emergency: - ACS - Pulmonary
Cardiovascular emergencies 05/March/2014 László Rudas Szeged Acute chest pain Acute heart failure Sudden cardiac death Acute chest pain What is the etiology? Chest pain signals emergency: - ACS - Pulmonary
NOT ANOTHER TALK ABOUT A - FIB
 NOT ANOTHER TALK ABOUT A - FIB CASES KUDOS AND A CHALLENGE Case 1 67 y/o female s/p R mastectomy 3 months earlier Second course of adjuvant chemotherapy Muga scan E.F. 35% What do we do next? Case 1 Cardiology
NOT ANOTHER TALK ABOUT A - FIB CASES KUDOS AND A CHALLENGE Case 1 67 y/o female s/p R mastectomy 3 months earlier Second course of adjuvant chemotherapy Muga scan E.F. 35% What do we do next? Case 1 Cardiology
Clinical Decision Seminar Imaging
 Cardiology Update 2013, Davos, Switzerland February 2013 Clinical Decision Seminar Imaging Dr. med. Robert Manka Cardiovascular MRI and Interventional Cardiology University Hospital Zurich Institute for
Cardiology Update 2013, Davos, Switzerland February 2013 Clinical Decision Seminar Imaging Dr. med. Robert Manka Cardiovascular MRI and Interventional Cardiology University Hospital Zurich Institute for
10/22/16. Lay of the land. Definition of ACS. Why do we worry about ST elevations?
 Lay of the land Update on Acute Coronary Syndrome: Five Things Hospitalists Must Know Dhruv S. Kazi, MD, MSc, MS Assistant Professor Department of Medicine (Cardiology), Department of Epidemiology and
Lay of the land Update on Acute Coronary Syndrome: Five Things Hospitalists Must Know Dhruv S. Kazi, MD, MSc, MS Assistant Professor Department of Medicine (Cardiology), Department of Epidemiology and
Massive pulmonary embolism with ST-elevation in the inferior leads and other interesting ECG findings
 CASE REPORT Massive pulmonary embolism with ST-elevation in the inferior leads and other interesting ECG findings Said Alsidawi 1, Mouhamad Abdalla 2, Tarek Helmy 2 1. Department of Internal Medicine,
CASE REPORT Massive pulmonary embolism with ST-elevation in the inferior leads and other interesting ECG findings Said Alsidawi 1, Mouhamad Abdalla 2, Tarek Helmy 2 1. Department of Internal Medicine,
Cardiogenic Shock in Acute MI
 Cardiogenic Shock in Acute MI Mark Sheldon, MD UNMH Interventional Cardiology Objectives Overview Treatment Definition Shock profiles Causes Medical Mechanical Illustrative case Questions? Revascularization
Cardiogenic Shock in Acute MI Mark Sheldon, MD UNMH Interventional Cardiology Objectives Overview Treatment Definition Shock profiles Causes Medical Mechanical Illustrative case Questions? Revascularization
Correlation Between Regional Wall Motion Abnormalities via 2-Dimensional Echocardiography, and Coronary Angiographic Findings
 THE ECHOCARDIOGRAPHY, IRAQI POSTGRADUATE MEDICAL AND CORONARY JOURNAL ANGIOGRAPHIC FINDINGS VOL.11, SUPPLEMENT,2012 Correlation Between Regional Wall Motion Abnormalities via 2-Dimensional Echocardiography,
THE ECHOCARDIOGRAPHY, IRAQI POSTGRADUATE MEDICAL AND CORONARY JOURNAL ANGIOGRAPHIC FINDINGS VOL.11, SUPPLEMENT,2012 Correlation Between Regional Wall Motion Abnormalities via 2-Dimensional Echocardiography,
ST ELEVATION MYOCARDIAL INFARCTION (STEMI) Gordon Kritzer, MD, FACC Virginia Mason Medical Center, Seattle
 Gordon Kritzer, MD, FACC Virginia Mason Medical Center, Seattle") ST ELEVATION MYOCARDIAL INFARCTION (STEMI) Gordon Kritzer, MD, FACC Virginia Mason Medical Center, Seattle STEMI ACS and STEMI History and physical, differential diagnosis ECGs Initial Therapy and management
ST ELEVATION MYOCARDIAL INFARCTION (STEMI) Gordon Kritzer, MD, FACC Virginia Mason Medical Center, Seattle STEMI ACS and STEMI History and physical, differential diagnosis ECGs Initial Therapy and management
CCS/CAIC/CSCS Position Statement on Revascularization Multi-vessel CAD. Teo et al, Canadian Journal of Cardiology 2014;30:
 CCS/CAIC/CSCS Position Statement on Revascularization Multi-vessel CAD Teo et al, Canadian Journal of Cardiology 2014;30: 1482-1491 Parallel Paper: Canadian Cardiovascular Society Guidelines for the Diagnosis
CCS/CAIC/CSCS Position Statement on Revascularization Multi-vessel CAD Teo et al, Canadian Journal of Cardiology 2014;30: 1482-1491 Parallel Paper: Canadian Cardiovascular Society Guidelines for the Diagnosis
Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend )
") Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend ) Stephen G. Ellis, MD Section Head, Interventional Cardiology Professor of Medicine Cleveland
Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend ) Stephen G. Ellis, MD Section Head, Interventional Cardiology Professor of Medicine Cleveland
Coronary arteriography in complicated acute myocardial infarction; clinical and angiographic correlates
 Coronary arteriography in complicated acute myocardial ; clinical and angiographic correlates Luis M. de la Fuente, M.D. Buenos Aires, Argentina From January 1979 to June 30, 1979, we performed coronary
Coronary arteriography in complicated acute myocardial ; clinical and angiographic correlates Luis M. de la Fuente, M.D. Buenos Aires, Argentina From January 1979 to June 30, 1979, we performed coronary
Antonio Colombo. Centro Cuore Columbus and S. Raffaele Scientific Institute, Milan, Italy. Miracor Symposium. Speaker: 15. Parigi: May 16-19, 2017
 Parigi: May 16-19, 2017 Miracor Symposium Speaker: 15 Antonio Colombo Centro Cuore Columbus and S. Raffaele Scientific Institute, Milan, Italy Nothing to disclose PiCSO Impulse System Elective high risk
Parigi: May 16-19, 2017 Miracor Symposium Speaker: 15 Antonio Colombo Centro Cuore Columbus and S. Raffaele Scientific Institute, Milan, Italy Nothing to disclose PiCSO Impulse System Elective high risk
Acute Myocardial Infarction
 Acute Myocardial Infarction Hafeza Shaikh, DO, FACC, RPVI Lourdes Cardiology Services Asst.Program Director, Cardiology Fellowship Associate Professor, ROWAN-SOM Acute Myocardial Infarction Definition:
Acute Myocardial Infarction Hafeza Shaikh, DO, FACC, RPVI Lourdes Cardiology Services Asst.Program Director, Cardiology Fellowship Associate Professor, ROWAN-SOM Acute Myocardial Infarction Definition:
Acute Valve Regurgitation Catherine M. Otto, MD J. Ward Kennedy-Hamilton Endowed Chair in Cardiology University of Washington, Seattle
 Acute Valve Regurgitation Catherine M. Otto, MD J. Ward Kennedy-Hamilton Endowed Chair in Cardiology University of Washington, Seattle No conflicts of interest Acute Aortic Regurgitation Causes aortic
Acute Valve Regurgitation Catherine M. Otto, MD J. Ward Kennedy-Hamilton Endowed Chair in Cardiology University of Washington, Seattle No conflicts of interest Acute Aortic Regurgitation Causes aortic
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM. General Instructions: ID NUMBER: FORM NAME: H F A DATE: 10/13/2017 VERSION: CONTACT YEAR NUMBER:
 ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM General Instructions: The Heart Failure Hospital Record Abstraction Form is completed for all heart failure-eligible cohort hospitalizations. Refer to
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM General Instructions: The Heart Failure Hospital Record Abstraction Form is completed for all heart failure-eligible cohort hospitalizations. Refer to
ST - segment Elevation Myocardial Infarction complicating an atypical Kawasaki disease
 ST - segment Elevation Myocardial Infarction complicating an atypical Kawasaki disease Raluca PRISECARU, Marc VINCENT, Steven VERCAUTEREN Brussels Heart Center, Brussels, Belgium Disclosure None Clinical
ST - segment Elevation Myocardial Infarction complicating an atypical Kawasaki disease Raluca PRISECARU, Marc VINCENT, Steven VERCAUTEREN Brussels Heart Center, Brussels, Belgium Disclosure None Clinical
Common Codes for ICD-10
 Common Codes for ICD-10 Specialty: Cardiology *Always utilize more specific codes first. ABNORMALITIES OF HEART RHYTHM ICD-9-CM Codes: 427.81, 427.89, 785.0, 785.1, 785.3 R00.0 Tachycardia, unspecified
Common Codes for ICD-10 Specialty: Cardiology *Always utilize more specific codes first. ABNORMALITIES OF HEART RHYTHM ICD-9-CM Codes: 427.81, 427.89, 785.0, 785.1, 785.3 R00.0 Tachycardia, unspecified
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014
 Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Acute Coronary Syndrome. Sonny Achtchi, DO
 Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Value of troponin measurements in carotid artery revascularization
 Value of troponin measurements in carotid artery revascularization Gert J de Borst Department of Vascular Surgery Postoperative myocardial infarction after NCS: Magnitude of the problem POISE-1: 367 /8,351=
Value of troponin measurements in carotid artery revascularization Gert J de Borst Department of Vascular Surgery Postoperative myocardial infarction after NCS: Magnitude of the problem POISE-1: 367 /8,351=
Myocardial Infarction. Reading Assignment (p66-78 in Outline )
") Myocardial Infarction Reading Assignment (p66-78 in Outline ) Objectives 1. Why do ST segments go up or down in ischemia? 2. STEMI locations and culprit vessels 3. Why 15-lead ECGs? 4. What s up with avr?
Myocardial Infarction Reading Assignment (p66-78 in Outline ) Objectives 1. Why do ST segments go up or down in ischemia? 2. STEMI locations and culprit vessels 3. Why 15-lead ECGs? 4. What s up with avr?
10/16/2014. CCRN Review - Cardiovascular. CCRN Review - Cardiovascular. CCRN Review - Cardiovascular
 Hypertrophic (IHSS) Diagnosis Chest x ray cardiomegaly Electrocardiography LV hypertrophy, ST segment T was changes, Q waves in inferior & precordial leads Atrial & ventricular dysrhythmias Hypertrophic
Hypertrophic (IHSS) Diagnosis Chest x ray cardiomegaly Electrocardiography LV hypertrophy, ST segment T was changes, Q waves in inferior & precordial leads Atrial & ventricular dysrhythmias Hypertrophic
HISTORY. Question: How do you interpret the patient s history? CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: 45-year-old man.
 HISTORY 45-year-old man. CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: His dyspnea began suddenly and has been associated with orthopnea, but no chest pain. For two months he has felt
HISTORY 45-year-old man. CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: His dyspnea began suddenly and has been associated with orthopnea, but no chest pain. For two months he has felt
Acute coronary syndromes
 Acute coronary syndromes 1 Acute coronary syndromes Acute coronary syndromes results primarily from diminished myocardial blood flow secondary to an occlusive or partially occlusive coronary artery thrombus.
Acute coronary syndromes 1 Acute coronary syndromes Acute coronary syndromes results primarily from diminished myocardial blood flow secondary to an occlusive or partially occlusive coronary artery thrombus.
Richard Grocott Mason
 Richard Grocott Mason What to do with a 50 year old man with chest pain? Does the pain sound cardiac? Is this a possible acute coronary syndrome? Does patient have a previous cardiac history? Natural history
Richard Grocott Mason What to do with a 50 year old man with chest pain? Does the pain sound cardiac? Is this a possible acute coronary syndrome? Does patient have a previous cardiac history? Natural history
Characteristics of Transient ST-Elevation versus ST-Elevation and Non-ST-Elevation Myocardial Infarction
 Characteristics of Transient ST-Elevation versus ST-Elevation and Non-ST-Elevation Myocardial Infarction Blondheim DS, Shochat M, Asif A, Kazatsker M, Frimerman A, Vassilenko L, Abu Fane R, Neiman E, Barel
Characteristics of Transient ST-Elevation versus ST-Elevation and Non-ST-Elevation Myocardial Infarction Blondheim DS, Shochat M, Asif A, Kazatsker M, Frimerman A, Vassilenko L, Abu Fane R, Neiman E, Barel
Definition. Low-cardiac-output state resulting in life threatening end-organ hypoperfusion. Criteria: MAP 30 mm Hg lower than baseline)
") Definition Low-cardiac-output state resulting in life threatening end-organ hypoperfusion Criteria: 1. Persistent hypotension (SBP
Definition Low-cardiac-output state resulting in life threatening end-organ hypoperfusion Criteria: 1. Persistent hypotension (SBP
Complicated PTCA of Left Main Total Occlusion in NSTEMI
 Complicated PTCA of Left Main Total Occlusion in NSTEMI Dr AM Thirugnanam MD, FSCAI, PhD Sr. Interventional Cardiologist Ipcard Cardiac Care Center, Hyderabad, India Disclosure Statement of Financial Interest
Complicated PTCA of Left Main Total Occlusion in NSTEMI Dr AM Thirugnanam MD, FSCAI, PhD Sr. Interventional Cardiologist Ipcard Cardiac Care Center, Hyderabad, India Disclosure Statement of Financial Interest
DAY1_CARDIOVASCULAR PRACTICE QUESTIONS
 DAY1_CARDIOVASCULAR PRACTICE QUESTIONS 1 P age 1. A 59-year-old male is admitted complaining of chest pain and dyspnea. ST elevation and T-wave inversion were seen on the ECG in V2, V3, and V4. IV thrombolytic
DAY1_CARDIOVASCULAR PRACTICE QUESTIONS 1 P age 1. A 59-year-old male is admitted complaining of chest pain and dyspnea. ST elevation and T-wave inversion were seen on the ECG in V2, V3, and V4. IV thrombolytic
Post Operative Troponin Leak: David Smyth Christchurch New Zealand
 Post Operative Troponin Leak: Does It Really Matter? David Smyth Christchurch New Zealand Life Was Simple Once Transmural Infarction Subendocardial Infarction But the Blood Tests Were n t Perfect Creatine
Post Operative Troponin Leak: Does It Really Matter? David Smyth Christchurch New Zealand Life Was Simple Once Transmural Infarction Subendocardial Infarction But the Blood Tests Were n t Perfect Creatine
Cindy Stephens, MSN, ANP Kelly Walker, MS, ACNP Peter Cohn, MD, FACC
 Cindy Stephens, MSN, ANP Kelly Walker, MS, ACNP Peter Cohn, MD, FACC Define Acute Coronary syndromes Explain the Cause Assessment, diagnosis and therapy Reperfusion for STEMI Complications to look for
Cindy Stephens, MSN, ANP Kelly Walker, MS, ACNP Peter Cohn, MD, FACC Define Acute Coronary syndromes Explain the Cause Assessment, diagnosis and therapy Reperfusion for STEMI Complications to look for
DECLARATION OF CONFLICT OF INTEREST. None
 DECLARATION OF CONFLICT OF INTEREST None How low should we go to avoid harm in hypertensives with comorbidities? CORONARY ARTERY DISEASE Prof. Dr. Maria DOROBANTU, FESC,FACC CARDIOLOGY EMERGENCY HOSPITAL
DECLARATION OF CONFLICT OF INTEREST None How low should we go to avoid harm in hypertensives with comorbidities? CORONARY ARTERY DISEASE Prof. Dr. Maria DOROBANTU, FESC,FACC CARDIOLOGY EMERGENCY HOSPITAL
Diastolic Heart Function: Applying the New Guidelines Case Studies
 Diastolic Heart Function: Applying the New Guidelines Case Studies Mitral Regurgitation The New ASE William Guidelines: A. Zoghbi Role MD, of FASE, 2D/3D MACCand CMR Professor and Chairman, Department
Diastolic Heart Function: Applying the New Guidelines Case Studies Mitral Regurgitation The New ASE William Guidelines: A. Zoghbi Role MD, of FASE, 2D/3D MACCand CMR Professor and Chairman, Department
How will new high sensitive troponins affect the criteria?
 How will new high sensitive troponins affect the criteria? Hugo A Katus MD Abteilung Innere Medizin III Kardiologie, Angiologie, Pulmologie Universitätsklinikum Heidelberg Even more sensitive: The new
How will new high sensitive troponins affect the criteria? Hugo A Katus MD Abteilung Innere Medizin III Kardiologie, Angiologie, Pulmologie Universitätsklinikum Heidelberg Even more sensitive: The new
Atherosclerotic Heart Disease: Coronary Vessels, EKG Localization of STEMI and Complications/Derivatives for USMLE Step One
 Atherosclerotic Heart Disease: Coronary Vessels, EKG Localization of STEMI and Complications/Derivatives for USMLE Step One Howard J. Sachs, MD Associate Professor of Medicine University of Massachusetts
Atherosclerotic Heart Disease: Coronary Vessels, EKG Localization of STEMI and Complications/Derivatives for USMLE Step One Howard J. Sachs, MD Associate Professor of Medicine University of Massachusetts
Severe Coronary Vasospasm Complicated with Ventricular Tachycardia
 Severe Coronary Vasospasm Complicated with Ventricular Tachycardia Göksel Acar, Serdar Fidan, Servet İzci and Anıl Avcı Kartal Koşuyolu High Specialty Education and Research Hospital, Cardiology Department,
Severe Coronary Vasospasm Complicated with Ventricular Tachycardia Göksel Acar, Serdar Fidan, Servet İzci and Anıl Avcı Kartal Koşuyolu High Specialty Education and Research Hospital, Cardiology Department,
Supplementary material 1. Definitions of study endpoints (extracted from the Endpoint Validation Committee Charter) 1.
 1.") Rationale, design, and baseline characteristics of the SIGNIFY trial: a randomized, double-blind, placebo-controlled trial of ivabradine in patients with stable coronary artery disease without clinical
Rationale, design, and baseline characteristics of the SIGNIFY trial: a randomized, double-blind, placebo-controlled trial of ivabradine in patients with stable coronary artery disease without clinical
Acute heart failure: ECMO Cardiology & Vascular Medicine 2012
 Acute heart failure: ECMO Cardiology & Vascular Medicine 2012 Lucia Jewbali cardiologist-intensivist 14 beds/8 ICU beds Acute coronary syndromes Heart failure/ Cardiogenic shock Post cardiotomy Heart
Acute heart failure: ECMO Cardiology & Vascular Medicine 2012 Lucia Jewbali cardiologist-intensivist 14 beds/8 ICU beds Acute coronary syndromes Heart failure/ Cardiogenic shock Post cardiotomy Heart
QUESTION EXAMPLES ECG
 ACEM Fellowship VAQ Examination QUESTION EXAMPLES ECG ECG 1: A 16 year old boy with a congenital heart problem presents to your ED with syncopal episodes. An ECG is taken. Describe and interpret his ECG
ACEM Fellowship VAQ Examination QUESTION EXAMPLES ECG ECG 1: A 16 year old boy with a congenital heart problem presents to your ED with syncopal episodes. An ECG is taken. Describe and interpret his ECG
Takotsubo syndrome. Ευτυχία Σμπαρούνη, FACC, FESC
 Takotsubo syndrome Ευτυχία Σμπαρούνη, FACC, FESC Definition Takotsubo Apical ballooning Broken heart syndrome Stress cardiomyopathy Cathecholaminergic cardiomyopathy Epidemiology 1990 first report by Japanese
Takotsubo syndrome Ευτυχία Σμπαρούνη, FACC, FESC Definition Takotsubo Apical ballooning Broken heart syndrome Stress cardiomyopathy Cathecholaminergic cardiomyopathy Epidemiology 1990 first report by Japanese
12 Lead ECGs: Ischemia, Injury & Infarction. Kevin Handke NRP, FP-C, CCP, CMTE STEMI Coordinator Flight Paramedic
 12 Lead ECGs: Ischemia, Injury & Infarction Kevin Handke NRP, FP-C, CCP, CMTE STEMI Coordinator Flight Paramedic None Disclosures Objectives Upon completion of this program the learner will be able to
12 Lead ECGs: Ischemia, Injury & Infarction Kevin Handke NRP, FP-C, CCP, CMTE STEMI Coordinator Flight Paramedic None Disclosures Objectives Upon completion of this program the learner will be able to
WHI Form Report of Cardiovascular Outcome Ver (For items 1-11, each question specifies mark one or mark all that apply.
 WHI Form - Report of Cardiovascular Outcome Ver. 6. COMMENTS To be completed by Physician Adjudicator Date Completed: - - (M/D/Y) Adjudicator Code: OMB# 095-044 Exp: 4/06 -Affix label here- Clinical Center/ID:
WHI Form - Report of Cardiovascular Outcome Ver. 6. COMMENTS To be completed by Physician Adjudicator Date Completed: - - (M/D/Y) Adjudicator Code: OMB# 095-044 Exp: 4/06 -Affix label here- Clinical Center/ID:
Imaging. Prof Geneviève DERUMEAUX Hôpital Henri Mondor Créteil, FRANCE
 Imaging Prof Geneviève DERUMEAUX Hôpital Henri Mondor Créteil, FRANCE Conflicts of Interest Speaker/advisor/research grant for Actelion, Sanofi, Servier, Toshiba # esccongress www.escardio.org/esc2014
Imaging Prof Geneviève DERUMEAUX Hôpital Henri Mondor Créteil, FRANCE Conflicts of Interest Speaker/advisor/research grant for Actelion, Sanofi, Servier, Toshiba # esccongress www.escardio.org/esc2014
Echo in CAD: Wall Motion Assessment
 Echo in CAD: Wall Motion Assessment Joe M. Moody, Jr, MD UTHSCSA and STVHCS October 2007 Relevant References ACC/AHA/ASE 2003 Guideline Update for the Clinical Application of Echocardiography Bayes de
Echo in CAD: Wall Motion Assessment Joe M. Moody, Jr, MD UTHSCSA and STVHCS October 2007 Relevant References ACC/AHA/ASE 2003 Guideline Update for the Clinical Application of Echocardiography Bayes de
DO NOT SUBMIT OR FAX THIS PAGE TO COR F M L DD MM YY
 DO NOT SUBMIT OR FAX THIS PAGE TO COR Patient # Patient Initials of Birth Medical Record Number F M L DD MM YY Patient Name Address Telephone (home) Telephone (work) Expected 6-month Follow-up Family Physician
DO NOT SUBMIT OR FAX THIS PAGE TO COR Patient # Patient Initials of Birth Medical Record Number F M L DD MM YY Patient Name Address Telephone (home) Telephone (work) Expected 6-month Follow-up Family Physician
Fifty shades of Troponin. Dr Liam Penny The Queens Hotel, Cheltenham 4 th October 2012
 Fifty shades of Troponin Dr Liam Penny The Queens Hotel, Cheltenham 4 th October 2012 Plaque-fissure and intracoronary thrombus Courtesy Prof. MJ Davies Acute Coronary Syndromes Plaque-fissure and intracoronary
Fifty shades of Troponin Dr Liam Penny The Queens Hotel, Cheltenham 4 th October 2012 Plaque-fissure and intracoronary thrombus Courtesy Prof. MJ Davies Acute Coronary Syndromes Plaque-fissure and intracoronary
Results of Ischemic Heart Disease
 Ischemic Heart Disease: Angina and Myocardial Infarction Ischemic heart disease; syndromes causing an imbalance between myocardial oxygen demand and supply (inadequate myocardial blood flow) related to
Ischemic Heart Disease: Angina and Myocardial Infarction Ischemic heart disease; syndromes causing an imbalance between myocardial oxygen demand and supply (inadequate myocardial blood flow) related to
Introduction to Risk Stratification
 Introduction to Risk Stratification Tim Fendler, MD, MSc Heart Failure/Transplant Fellow St. Luke s Mid America Heart Institute 1 Disclosures: No financial relationships to disclose. A 74 year-old male
Introduction to Risk Stratification Tim Fendler, MD, MSc Heart Failure/Transplant Fellow St. Luke s Mid America Heart Institute 1 Disclosures: No financial relationships to disclose. A 74 year-old male
An Approach to Chest Pain
 Oesophageal Spasm Acute Coronary Syndrome Pneumothorax An Approach to Chest Pain Musculoskeletal Pulmonary Embolism Aortic Dissection Ema Pitts Cardiology Registrar Basic Trainee Pain S Site O Onset C
Oesophageal Spasm Acute Coronary Syndrome Pneumothorax An Approach to Chest Pain Musculoskeletal Pulmonary Embolism Aortic Dissection Ema Pitts Cardiology Registrar Basic Trainee Pain S Site O Onset C
Left ventricle pseudoaneurysm as late postoperative complication of a large apical aneurysm
 CASE REPORT Left ventricle pseudoaneurysm as late postoperative complication of a large apical aneurysm Mariana M. Floria 1, 4, Carmen Elena Pleșoianu 2, 4, Michel Buche 3, Baudouin Marchandise 4, Erwin
CASE REPORT Left ventricle pseudoaneurysm as late postoperative complication of a large apical aneurysm Mariana M. Floria 1, 4, Carmen Elena Pleșoianu 2, 4, Michel Buche 3, Baudouin Marchandise 4, Erwin
Clinical Summary. Live Cases I - IX
 Clinical Summary Live Cases I - IX Patient: Male, 66 years Diagnosis: Single vessel CAD with normal LVEF Target lesion: proximal RCA Coronary risk factor: Hypertension, smoke (90py) Clinical course: ECG
Clinical Summary Live Cases I - IX Patient: Male, 66 years Diagnosis: Single vessel CAD with normal LVEF Target lesion: proximal RCA Coronary risk factor: Hypertension, smoke (90py) Clinical course: ECG
Emergency Echo, Emergency Setting, ABCD Approach
 ECHO Alex Conference 2010 Emergency Echo, Emergency Setting, ABCD Approach Aleksandar N. Nešković Clinical Hospital Center Zemun Belgrade University School of Medicine Emergency Echocardiography Why ECHO
ECHO Alex Conference 2010 Emergency Echo, Emergency Setting, ABCD Approach Aleksandar N. Nešković Clinical Hospital Center Zemun Belgrade University School of Medicine Emergency Echocardiography Why ECHO
The use of Cardiac CT and MRI in Clinical Practice
 The use of Cardiac CT and MRI in Clinical Practice Matthew W. Martinez, MD Assistant Professor of Medicine LVPG - Lehigh Valley Heart Specialists Lehigh Valley Health Network Oct. 3, 2009 DISCLOSURE Relevant
The use of Cardiac CT and MRI in Clinical Practice Matthew W. Martinez, MD Assistant Professor of Medicine LVPG - Lehigh Valley Heart Specialists Lehigh Valley Health Network Oct. 3, 2009 DISCLOSURE Relevant
Supplementary Table 1. Details of the components of the primary composite endpoint
 Supplementary Table 1. Details of the components of the primary composite endpoint 1. Death The cause of death will be defined by the underlying cause, not the immediate mode of death. Death will be classified
Supplementary Table 1. Details of the components of the primary composite endpoint 1. Death The cause of death will be defined by the underlying cause, not the immediate mode of death. Death will be classified
Topic. Updates on Definition of Myocardial Infarction
 Topic Updates on Definition of Myocardial Infarction In the past, general consensus for MI? Definition of MI by WHO - Combination of 2 of 3 characteristics - 1. Typical Symptoms 2. Enzyme Rise 3. Typical
Topic Updates on Definition of Myocardial Infarction In the past, general consensus for MI? Definition of MI by WHO - Combination of 2 of 3 characteristics - 1. Typical Symptoms 2. Enzyme Rise 3. Typical
12 Lead ECG Interpretation
 12 Lead ECG Interpretation Julie Zimmerman, MSN, RN, CNS, CCRN Significant increase in mortality for every 15 minutes of delay! N Engl J Med 2007;357:1631-1638 Who should get a 12-lead ECG? Also include
12 Lead ECG Interpretation Julie Zimmerman, MSN, RN, CNS, CCRN Significant increase in mortality for every 15 minutes of delay! N Engl J Med 2007;357:1631-1638 Who should get a 12-lead ECG? Also include
The Value of Stress MRI in Evaluation of Myocardial Ischemia
 The Value of Stress MRI in Evaluation of Myocardial Ischemia Dr. Saeed Al Sayari, MBBS, EBCR, MBA Department of Radiology and Nuclear Medicine Mafraq Hospital, Abu Dhabi United Arab Emirates Introduction
The Value of Stress MRI in Evaluation of Myocardial Ischemia Dr. Saeed Al Sayari, MBBS, EBCR, MBA Department of Radiology and Nuclear Medicine Mafraq Hospital, Abu Dhabi United Arab Emirates Introduction
Coronary Arteriovenous Malformation presenting as Acute Myocardial Infarction. Choon Ta NG, Aaron WONG, Foong-Koon CHEAH, Chi Keong CHING
 Coronary Arteriovenous Malformation presenting as Acute Myocardial Infarction Choon Ta NG, Aaron WONG, Foong-Koon CHEAH, Chi Keong CHING The patient 49 year old Male presented with Chest tightness x 1
Coronary Arteriovenous Malformation presenting as Acute Myocardial Infarction Choon Ta NG, Aaron WONG, Foong-Koon CHEAH, Chi Keong CHING The patient 49 year old Male presented with Chest tightness x 1
CLINCIAL APPLICATION OF GUIDELINES IN HEART FAILURE
 CLINCIAL APPLICATION OF GUIDELINES IN HEART FAILURE SSC Journée d Automne 25 novembre 2010 Dr. Charles Seydoux, spéc. FMH en médecine interne et en cardiologie, Lausanne Dr. Claudia Bösch, Oberärztin Herzinsuffizienz
CLINCIAL APPLICATION OF GUIDELINES IN HEART FAILURE SSC Journée d Automne 25 novembre 2010 Dr. Charles Seydoux, spéc. FMH en médecine interne et en cardiologie, Lausanne Dr. Claudia Bösch, Oberärztin Herzinsuffizienz
Acute Coronary Syndromes
 Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California
 High Risk PCI Making Possible the Impossible Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California Disclosures Abiomed Research Support Consulting Agreement
High Risk PCI Making Possible the Impossible Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California Disclosures Abiomed Research Support Consulting Agreement
Acute Coronary Syndromes Unstable Angina Non ST segment Elevation MI (NSTEMI) ST segment Elevation MI (STEMI)
 ST segment Elevation MI (STEMI)") Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Evaluate common abnormalities that mimic myocardial infarction. Identify
Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Evaluate common abnormalities that mimic myocardial infarction. Identify
STAT 12 Lead ECG Workshop: Basics & ACS
 STAT 12 Lead ECG Workshop: Basics & ACS Part 2: Acute Coronary Syndrome WAYNE W RUPPERT, CVT, CCCC, NREMT-P Cardiovascular Coordinator Bayfront Health Seven Rivers Crystal River, Florida Interventional
STAT 12 Lead ECG Workshop: Basics & ACS Part 2: Acute Coronary Syndrome WAYNE W RUPPERT, CVT, CCCC, NREMT-P Cardiovascular Coordinator Bayfront Health Seven Rivers Crystal River, Florida Interventional
Radiology of the respiratory/cardiac diseases (part 2)
") Cardiology Cycle - Lecture 6 436 Teams Radiology of the respiratory/cardiac diseases (part 2) Objectives Done By Team Leaders: Khalid Alshehri Hanin Bashaikh Team Members: Leena Alwakeel Aroob Alhuthail
Cardiology Cycle - Lecture 6 436 Teams Radiology of the respiratory/cardiac diseases (part 2) Objectives Done By Team Leaders: Khalid Alshehri Hanin Bashaikh Team Members: Leena Alwakeel Aroob Alhuthail
M/39 CC D. => peak CKMB (12 hr later) ng/ml T.chol/TG/HDL/LDL 180/150/48/102 mg/dl #
 ng/ml T.chol/TG/HDL/LDL 180/150/48/102 mg/dl #") Acute Coronary Syndrome - Case Review - Young-Guk Ko, MD Yonsei Cardiovascular Center Yonsei University College of Medicine Case 1 M/39 #4306212 CC D : Severe squeezing chest pain : 4 hours, aggravated
Acute Coronary Syndrome - Case Review - Young-Guk Ko, MD Yonsei Cardiovascular Center Yonsei University College of Medicine Case 1 M/39 #4306212 CC D : Severe squeezing chest pain : 4 hours, aggravated
12 th Annual West Virginia ACC Meeting April 8, 2017
 12 th Annual West Virginia ACC Meeting April 8, 2017 Rameez Sayyed, M.D., FACC, FSCAI Associate professor of Medicine Program Director for interventional cardiology Marshall University Joan C. Edwards
12 th Annual West Virginia ACC Meeting April 8, 2017 Rameez Sayyed, M.D., FACC, FSCAI Associate professor of Medicine Program Director for interventional cardiology Marshall University Joan C. Edwards
CABG Surgery following STEMI
 CABG Surgery following STEMI Susana Harrington, MS,APRN-NP Cardio-Thoracic Surgery Nebraska Methodist Hospital February 15, 2018 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction:
CABG Surgery following STEMI Susana Harrington, MS,APRN-NP Cardio-Thoracic Surgery Nebraska Methodist Hospital February 15, 2018 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction:
Emergency surgery in acute coronary syndrome
 Emergency surgery in acute coronary syndrome Teerawoot Jantarawan Division of Cardiothoracic Surgery, Department of Surgery, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
Emergency surgery in acute coronary syndrome Teerawoot Jantarawan Division of Cardiothoracic Surgery, Department of Surgery, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
Patient. Clinical data Indications: Operation date. Comorbidities: Patient code Birth date: / /
 Patient Patient code Birth date: / / Sex: Male Height (cm): Female Weight (kg): Risk Factors: Family history of coronary disease: Hypertension Dyslipidemia Peripheral disease Diabetes Comorbidities: No
Patient Patient code Birth date: / / Sex: Male Height (cm): Female Weight (kg): Risk Factors: Family history of coronary disease: Hypertension Dyslipidemia Peripheral disease Diabetes Comorbidities: No
New Jersey Cardiac Catheterization Data Registry, Version 2.0 (Please report data only for patients 16 years or older.)
") A. ADMINISTRATIVE New Jersey Cardiac Catheterization Data Registry, Version 2.0 (Please report data only for patients 16 years or older.) 1. Facility Code: 2. Facility Name: 3. Procedure Type (Choose only
A. ADMINISTRATIVE New Jersey Cardiac Catheterization Data Registry, Version 2.0 (Please report data only for patients 16 years or older.) 1. Facility Code: 2. Facility Name: 3. Procedure Type (Choose only
CARDIAC CHEST PAIN. 1. ST Elevation MI
 CARDIAC CHEST PAIN ACUTE ST ELEVATION MYOCARDIAL INFARCTION* and ACUTE CORONARY SYNDROME (ACS) are caused by instability/rupture of atheromatous plaques in the coronary circulation. Identifying ST Elevation
CARDIAC CHEST PAIN ACUTE ST ELEVATION MYOCARDIAL INFARCTION* and ACUTE CORONARY SYNDROME (ACS) are caused by instability/rupture of atheromatous plaques in the coronary circulation. Identifying ST Elevation