EMERGENCIES IN THE CHEST. Michal Kozub
|
|
|
- Julia Butler
- 5 years ago
- Views:
Transcription


1 EMERGENCIES IN THE CHEST Michal Kozub



2 CHEST IMAGING

3 CHEST IMAGING

4 1.Consolidation - any pathologic process that fills the alveoli with fluid, pus, blood, cells (including tumor cells) or other substances resulting in lobar, diffuse or multifocal ill-defined opacities. 2.Interstitial - involvement of the supporting tissue of the lung parenchyma resulting in fine or coarse reticular opacities or small nodules. 3.Nodule or mass - any space occupying lesion either solitary or multiple. 4.Atelectasis - collapse of a part of the lung due to a decrease in the amount of air in the alveoli resulting in volume loss and increased density.

5 CHEST RADIOGRAPH Portable chest radiography is the initial imaging method used at the emergency workup of the polytrauma patient and it is useful for detecting serious life-threatening conditions, such as a tension pneumothorax or haemothorax, mediastinal haematoma, flail chest or malpositioned tubes. Usually AP Often supine Frequently in poor inspiration 405/


6 CT The superiority of CT over chest radiography has been documented in the literature. CT detects significant disease in patients with normal initial radiographs and in 20% will reveal more extensive injuries compared with the abnormal initial radiographs, necessitating a change of management. Reformats without additional scanning. Usually on spontaneous breath Motion artifact Metal artifact/high-density foreign material artifact

7 MRI MRI allows the radiologist to directly evaluate the soft tissues of the spine and is, therefore, crucial in the evaluation of the patient with ligamentous injury and instability. a prolonged acquisition time unavailability at many institutions contraindications, including patients with pacemakers, ferromagnetic aneurysm clips, metallic fragments in the spinal cord, and claustrophobia. MRI in acute spinal trauma By Michael C. Hollingshead, MD, and Mauricio Castillo, MD, FACR
:282-287. doi:10.")
8 When computed tomographic angiography (CTA) is contraindicated, MRI and MRA are important alternative imaging modalities for diagnosis and management of patients with acute PE, AD and MI. MRI Hochhegger B, Ley-Zaporozhan J, Marchiori E, et al. Magnetic resonance imaging findings in acute pulmonary embolism. The British Journal of Radiology. 2011;84(999): doi: /bjr/
 Since CT has better accuracy for diagnosing torso injuries, the FAST exam is most useful in")
9 ULTRASOUND???? Focused Assessment Sonography for Trauma (FAST) Since CT has better accuracy for diagnosing torso injuries, the FAST exam is most useful in situations where CT is not practical due to time constraints or when CT scan can be reasonably avoided.

10 CLINICAL SCENARIOS WHERE FAST IS MOST USEFUL: Hemodynamically unstable patients, when the cause of hypotension is unclear. Patients who need an emergent bedside procedure. Patients at a community hospital who require transfer to a trauma center. Consider pericardiocentesis if a pericardial effusion is found, consider early blood transfusion for significant hemoperitoneum, and consider a chest tube if a hemothorax or pneumothorax is discovered, especially if aeromedical transport is planned. Intoxicated patients who can be observed and reexamined. Patients with penetrating trauma with multiple wounds or unclear trajectory, especially with wounds in upper abdomen or lower chest. Patients with a concerning mechanism of injury but no indication for CT. Consider a period of observation and serial FAST exams.
11 CHEST EMERGENCIES Trauma Non traumatic emergencies
12 TRAUMA Lung trauma Pulmonary contusions Pulmonary lacerations Traumatic lung herniation Torsion of the lung Pneumothorax Haemothorax Haemopneumothorax Tracheobronchial injuries Mediastinal Pneumomediastinum Mediastinal haematoma Aortic injury Oesophageal injuries Thoracic duct trauma Cardiac trauma
13 TRAUMA Skeletal trauma Rib fractures Flail chest Sternal fractures Scapula fractures Thoracic spine fractures Diaphragmatic trauma Diaphragmatic injuries Oikonomou A, Prassopoulos P. CT imaging of blunt chest trauma. Insights into Imaging. 2011;2(3): doi: /s
14 NON TRAUMA Pulmonary embolism Pneumothorax ( tension pneumothorax ) Airway foreign bodies Pneumoperitoneum Pericardial effusions Acute respiratory distress syndrome Thoracic aortic aneurysms Diaphragmatic hernias Congestive heart failure Aspiration pneumonia Hydropneumothorax
15 ATELECTASIS Atelectasis, (also called collapse), a loss of volume of lung parenchyma caused by a reduced inflation. Some mechanisms may be responsible for atelectasis: bronchial obstruction extrinsic compression such as pleural fluid or air, or the presence of any space-occupying intrathoracic lesion resulting in extrinsic compression of adjacent parenchyma; cicatrization atelectasis resulting from lung parenchymal fibrosis; adhesive atelectasis resulting from loss of surfactant.


16 ATELECTASIS The most frequent cause of atelactasis is bronchial obstruction. The major radiological signs of atelectasis are opacity of the lobe/lung and evidence of loss of volume. Opacity results from the presence of intra-alveolar fluid in the case of obstructive atelectasis or passive atelectasis or from scarring or lung fibrosis in the case of cicatrization atelectasis.


17 ATELECTASIS The signs of loss of volume include: displacement of fissures, pulmonary blood vessels and major bronchi, Shift of other structures to compensate for the loss of volume. In the case of obstructive atelectasis, the presence of a large tumour mass located in a parahilar situation may produce a bulge in the contour of the collapsed lobe (golden S sign)


18 ATELECTASIS OF RIGHT UPPER LOBE The right hilum becomes elevated; The major and minor fissures are displaced upwards and rotated towards the mediastinum. As a result, the collapsed lobe packs against the mediastinum and lung apex.
.")

19 ATELECTASIS OF LEFT UPPER LOBE The hilum is displaced upwards and the major fissure forwards (next slice). The lobe retains much of its original contact with the anterior chest wall. Displacement of the anterior mediastinum fat and displacement of the trachea towards the left are commonly present. The left hemidiaphragm is moderately elevated
20 ATELECTASIS OF MIDDLE LOBE The collapsed right middle lobe is easily recognized on the lateral chest radiograph. The major and minor fissures move towards one another and the collapsed lobe resembles a curved, elongated wedge. The right hilum is not displaced. The right hemidiaphragm and mediastinum are in a normal position.


21 ATELECTASIS OF LOWER LOBE The lower lobe collapse is seen with obstruction to lower lobe s bronchus. The major fissure is displaced downward and backward creating an opacity that obliterates the dome of the hemidiaphragm. Ipsilateral hilum, mainstem bronchus and upper lobar bronchus are displaced downward.

22 AIRWAY FOREIGN BODIES Airway foreign bodies are most often found in pediatric patients. The most common site of foreign bodies is the right mainstem bronchus due to its posterior location, shallow angle to the trachea and wide diameter. The density of the ingested item will determine whether it can be directly identified on radiographs.

.")
23 Indirect signs of ingestion include: focal overinflation (if there is partial obstruction), atelectasis (if there is more complete obstruction). AIRWAY FOREIGN BODIES
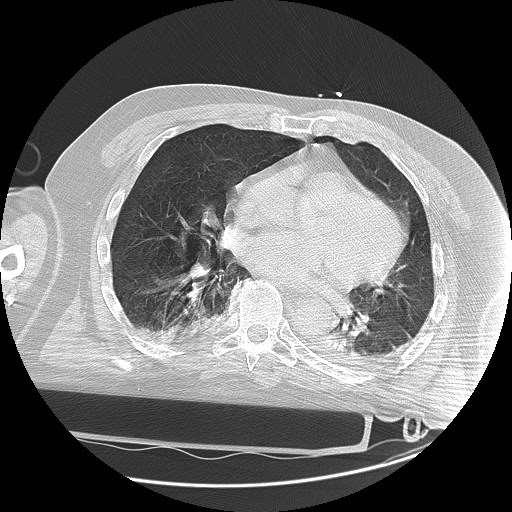
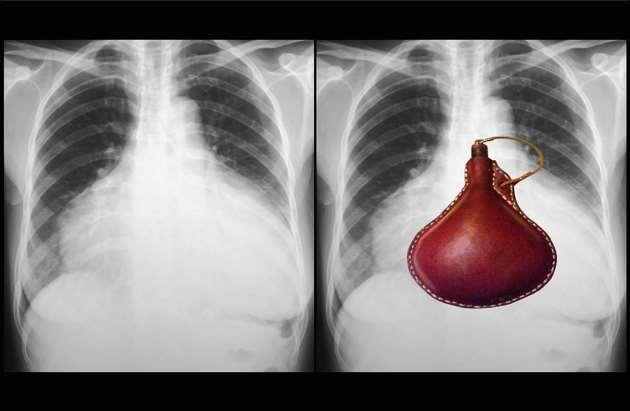
24 PERICARDIAL EFFUSIONS Pericardial effusions result from the accumulation of fluid within the pericardial space.

25 PERICARDIAL EFFUSIONS The classic finding on a chest radiograph is an enlarged cardiac silhouette, the so-called water-bottle heart. However, if the fluid accumulates rapidly, then minimal cardiomegaly may be present. Other potential findings include pleural effusion and rarely pericardial calcifications.


26
27 ACUTE RESPIRATORY DISTRESS SYNDROME ARDS defined by the American/European Consensus Committee, as acute and persistent severe hypoxia, bilateral radiographic lung infiltrates, no evidence of congestive heart failure. Patients with lesser degrees of hypoxia are classified as having acute lung injury.
 The clinical approach to and radiographic understanding of ARDS has assumed that the type of underlying injury was not relevant to life support strategies and")
28 ACUTE RESPIRATORY DISTRESS SYNDROME ARDS is not a disease but a syndrome that may be due to direct parenchymal injury (trauma, pneumonia, aspiration) or due to capillary leak oedema from systemic inflammation (sepsis, hypotension) The clinical approach to and radiographic understanding of ARDS has assumed that the type of underlying injury was not relevant to life support strategies and imaging interpretation. Recent evidence suggests that lung mechanics and radiographic appearance may be different in those with ARDS due to pulmonary causes (ARDSp) and those with ARDS due to extrapulmonary causes.
29 THE CLASSICAL RADIOGRAPHIC DESCRIPTIONS OF ARDS During the first hours after a systemic insult, the chest radiograph is normal or it shows mild generalized atelectasis. Over the next 48 hours, there is a rapid increase in density throughout the lungs and often diffuse groundglass to alveolar consolidation symmetrically distributed. The appearance then stabilizes for several days. Toward the end of the first week, the consolidation becomes less dense, eventually forming a fibrotic pattern.

30 ACUTE RESPIRATORY DISTRESS SYNDROME The classical radiographic descriptions of ARDS are as follows: During the first hours after a systemic insult, the chest radiograph is normal or it shows mild generalized atelectasis. Over the next 48 hours, there is a rapid increase in density throughout the lungs and often diffuse ground-glass to alveolar consolidation symmetrically distributed. The appearance then stabilizes for several days. Toward the end of the first week, the consolidation becomes less dense, eventually forming a fibrotic pattern.



31 CT shows bilateral diffuse ground-glass opacification of ARDS due to sepsis. There is also pneumomediastinum due to barotrauma CT shows asymmetrical consolidation from ARDS due to bacterial pneumonia
32 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) The most common findings on chest radiographs are bilateral, predominately peripheral, asymmetric consolidations with air bronchograms. Septal lines and pleural effusions are uncommon findings. Early findings during the exudative phase are bilateral consolidations that obscure the pulmonary vascular markings. These opacities extend to more extensive diffuse consolidations that are typically asymmetric. Most radiographic abnormalities begin to resolve after days if the patient survives.
33 CONGESTIVE HEART FAILURE Congestive heart failure is a clinical syndrome in which the heart fails to adequately pump blood to tissues. A number of typical findings may be present on a chest radiograph: With cardiomegaly, the cardiothoracic ratio increases to greater than 50% on a posterior-anterior chest radiograph. Kerley B lines may be present on the lung periphery that are the result of interlobular septal thickening. Accumulated pleural fluid may blunt costophrenic angles or cause large pleural effusions.

34 With cardiomegaly, the cardiothoracic ratio increases to greater than 50% on a posterior-anterior chest radiograph.

35 Kerley B lines may be present on the lung periphery that are the result of interlobular septal thickening.


36 Accumulated pleural fluid may blunt the costophrenic angles or cause large pleural effusions.

37 Pulmonary edema may cause bilateral increased lung markings in a perihilar, or bat-winged, distribution. Increased pulmonary capillary pressure causes the upper lobe vessels to be equal or larger in caliber than the lower lobe vessels, referred to as cephalization.
38 PULMONARY OEDEMA Abnormal accumulation of fluid in the interstitial compartment of the lung with or without associated airspace filling. The oedema is due to changes in hydrostatic forces in the capillaries, to increased capillary permeability or to impaired lymphatic drainage. Transudative pulmonary oedema is due to increased hydrostatic pressure or, rarely, due to decreased oncotic pressure across a functioning capillary membrane. Hydrostatic pulmonary oedema can result from cardiogenic or noncardiogenic (renal failure, fluid overload) causes. Cardiogenic pulmonary oedema is a consequence of elevated left-sided pressure which may result from left ventricular dysfunction, mitral valve disease, left atrial disease or, rarely, pulmonary venous obstruction.

39 PULMONARY OEDEMA The radiographic changes of hydrostatic oedema are quite characteristic. "cephalization" with the upper lobe vessels becoming larger than the lower lobe vessels In left heart failure, the artery enlarges relative to the bronchus. Since they are in the same plane, magnification is not an issue.


40 PULMONARY OEDEMA The upper lobe pulmonary vessels are enlarged. Peribronchial cuffing is seen in the anterior segmental bronchus of the left upper lobe. There is a moderate right pleural effusion in the major and minor fissures. There is a moderate subpulmonary effusion on the left.

41 PULMONARY OEDEMA Posteroanterior radiograph of a 14-year-old child with an acute cardiomyopathy. The airspace shadowing, which is more severe on the right, is typical of pulmonary oedema.


42 PULMONARY OEDEMA The radiograph in cardiogenic pulmonary oedema may show cardiomegaly, alteration of cardiac contour due to congenital heart disease or abnormality of the pulmonary vasculature due to a right-to-left shunt. The earliest radiographic change visible in increased pulmonary venous pressure is redistribution of blood flow, with an increase in prominence of the normally smaller upper lobe vessels. Also, the supine film does not allow detection of any change in distribution.


43 PULMONARY OEDEMA cardiogenic pulmonary oedema
44 THORACIC AORTIC ANEURYSMS Thoracic aortic aneurysms are defined as a greater than 50% aneurysmal dilatation of normal ascending thoracic aorta, aortic arch, or descending thoracic aorta. The descending thoracic aorta is the most common site.
.")
45 THORACIC AORTIC ANEURYSMS On chest radiographs, the most common findings are a widening of the mediastinal silhouette (white arrow), enlargement of the aortic knob and tracheal displacement (red arrow). Other radiographic findings include a double-opacity appearance to the aorta representing true and false lumens, localized bulges along the aortic contour and a disparity in the caliber of the descending and ascending aorta.




46 THORACIC AORTIC ANEURYSMS
47
48 AORTIC DISSECTION Splitting of the media of the aortic wall by blood. It may occur by means of a tear in the aortic intima with blood passing from the lumen into the wall causing the intima to be torn from the wall for a variable distance. Dissection may also occur by spontaneous bleeding of the vasa vasorum causing intramural haematoma without rupture of the intima and consequently no connection between the lumen and the intramural dissection.
49 AORTIC DISSECTION Degeneration of the aortic media, cystic medial necrosis, is the pathological substrate for aortic dissection. This may be induced by chronic stress against the wall such as occurs with systemic hypertension, aortic coarctation, aortic stenosis and bicuspid aortic valve. Cystic medial necrosis is a feature of hereditary defects of connective tissue, especially Marfans syndrome and Ehlers Danlos syndrome. The risk of dissection is increased during pregnancy.
50 AORTIC DISSECTION There are two classifications of aortic dissection. The Stanford classification recognizes Type A (involvement of ascending aorta alone or involvement of ascending and descending aorta) and Type B (involvement of descending aorta alone). The De Bakey classification describes Type I (ascending and descending aorta), Type II (ascending aorta alone) and Type III (descending aorta only). Stanford A and De Bakey I and II are treated by emergency surgery.
51 AORTIC DISSECTION Diagram showing the two classification systems. Stanford Type A includes DeBakey Type I and II
52 AORTIC DISSECTION - IMAGING The chest X-ray is neither sensitive nor specific for establishing the diagnosis of aortic dissection. The chest radiograph frequently demonstrates an enlarged thoracic aorta as a consequence of underlying predisposing diseases such as hypertension or aortic valvular disease. The chest X-ray may display features indicative of Marfans syndrome such as sternal deformity, scoliosis and elongated thorax. Infrequently, the chest X-ray may demonstrate inward displacement of intimal calcification in the aortic arch on the frontal view or an apical pleural cap.
53 THE DEFINITIVE DIAGNOSIS OF AORTIC DISSECTION CAN BE ESTABLISHED BY: thoracic aortography, computed tomography angiograhy, magnetic resonance imaging angiograhy, echocardiography.
54 AORTIC DISSECTION - IMAGING The goals of imaging studies in the typical dissection are to identify: the intimal flap; extent of the dissection; involvement of aortic branches; patency of the false channel; periaortic hematoma or haemorrhagic pericardial effusion; aortic regurgitation.


55 AORTIC DISSECTION
 in the distal aortic arch and descending")
56 AORTIC DISSECTION Partition of a three-dimensional contrastenhanced MRA shows intimal flap (arrows) in the distal aortic arch and descending aorta.
57 AORTIC DISSECTION CT angiography, and MR angiography are highly sensitive and specific for the diagnosis of aortic dissection. They display the presence and extent of the intimal flap and the sizes and configurations of the true and false channels. Because of limitations in acquiring diagnostic images in some subjects and lower diagnostic accuracy, transthoracic echocardiography has been replaced by transoesophageal echocardiography. The portability of transoesophageal echocardiography is a highly attractive attribute since it can be taken to the patient in the emergency department or intensive care unit.
58 PULMONARY EMBOLISM (PE) Embolic occlusion of the pulmonary arterial system. The majority of cases result from thrombotic occlusion and therefore the condition is frequently termed pulmonary thrombo-embolism Clinical signs and symptoms are non-specific. Dyspnoea, chest pain, and haemoptysis have been described as a classic triad in pulmonary embolism. 2 scores: Wells score, Geneva score. Markers: D-dimer (normal D-dimer has almost 100% negative predictive value (virtually excludes PE): no further testing is required. Raised D-dimer is caused by many other diseases than PE = Raised D Dimer is non-specific: it indicates the need for further testing if pulmonary embolism is suspected)!
59 PULMONARY EMBOLISM (PE) Risk factors primary hypercoagulable states (protein C or S deficency, antithrombin III deficiency) recent surgery pregnancy prolonged bed rest / immobility malignancy oral contraceptive use
 https://radiopaedia.")
60 PLAIN RADIOGRAPH Fleishner sign: enlarged pulmonary artery (20%)


61 Hampton hump: peripheral wedge of airspace opacity and implies lung infarction (20%) PLAIN RADIOGRAPH
62 PLAIN RADIOGRAPH Westermark's sign: focal peripheral hyperlucency secondary to focal hypovolemia pleural effusion (35%) elevated diaphragm




63 CT PULMONARY ANGIOGRAPHY (CTPA) shows filling defects within pulmonary vasculature with acute pulmonary emboli
 shows filling")

64 CT PULMONARY ANGIOGRAPHY (CTPA) shows filling defects within pulmonary vasculature with acute pulmonary emboli

65 VQ scan will show ventilationperfusion mismatches. NUCLEAR MEDICINE
66 MRI???


67 MR findings for acute PE were similar to those seen by CT or angiography, because all provided morphological representations of the same pathological process. We classified the MR features of pulmonary thromboembolism as vascular signs or parenchymal sign: Pulmonary arterial signs Signs of pulmonary hypertension Collateral systemic supply Parenchymal signs A meta-analysis of studies that adopted gadoliniumenhanced MR for imaging acute PE used conventional pulmonary angiography as the reference standard. A broad range of sensitivities, from 77% to 100%, was reported, with uniformly high specificities of 95% to 98%. Hochhegger B, Ley-Zaporozhan J, Marchiori E, et al. Magnetic resonance imaging findings in acute pulmonary embolism. The British Journal of Radiology. 2011;84(999): doi: /bjr/

68 DIAPHRAGMATIC HERNIAS Diaphragmatic hernias are caused when a defect in the diaphragmatic wall allows for the herniation of abdominal contents into the thoracic cavity. The majority of tears are on the left side and are thought to represent either weakness of the left hemidiaphragm or protection by the liver.
.")

69 DIAPHRAGMATIC HERNIAS On chest radiographs, asymmetry of hemidiaphragm or changing diaphragmatic levels may be present (arrows). Gas-filled organs or a nasogastric tube within thoracic cavity will confirm the diagnosis. Solid abdominal organs will appear as mushroom-shaped homogeneous opacities. Potential misdiagnosis can occur in the case of diaphragmatic paralysis or after lung reduction surgery.
70 HEMITHORAX WHITE-OUT Complete white-out of a hemithorax on the chest x-ray has a limited number of causes. The differential diagnosis can be shortened further with one simple observation - the position of trachea. Is it central, pulled or pushed from the side of opacification?

71 TRACHEA PULLED TOWARD THE OPACIFIED SIDE Pneumonectomy total lung collapse: e.g. endobronchial intubation pulmonary agenesis pulmonary hypoplasia

72 TRACHEA PULLED TOWARD THE OPACIFIED SIDE Pneumonectomy total lung collapse: e.g. endobronchial intubation pulmonary agenesis pulmonary hypoplasia

73 TRACHEA REMAINS CENTRAL IN POSITION Consolidation pulmonary oedema/ards pleural mass: e.g. mesothelioma chest wall mass: e.g. Askin/Ewing sarcoma


74 PUSHED AWAY FROM THE OPACIFIED SIDE pleural effusion diaphragmatic hernia large pulmonary mass
75 Pneumoperitoneum
76 Pneumoperitoneum refers to air within the peritoneal cavity, most commonly from perforation of an abdominal viscus. Air will accumulate in the least dependent portion of abdominal cavity. During upright chest radiographs, air will separate liver, spleen and intestines from diaphragm producing dark crescents. To ensure adequate air migration, patients should be kept upright for at least 5 minutes before the image is taken.

77 THANKS FOR ATTENTION
78 THANKS FOR ATTENTION Hochhegger B, Ley-Zaporozhan J, Marchiori E, et al. Magnetic resonance imaging findings in acute pulmonary embolism. The British Journal of Radiology. 2011;84(999): doi: /bjr/ Oikonomou A, Prassopoulos P. CT imaging of blunt chest trauma. Insights into Imaging. 2011;2(3): doi: /s ECR 2008 / C-275Blunt chest trauma: Spectrum of findings with emphasis on MDCT
Interpreting thoracic x-ray of the supine immobile patient: Syllabus
 Interpreting thoracic x-ray of the supine immobile patient: Syllabus Johannes Godt Dep. of Radiology and Nuclear Medicine Oslo University Hospital Ullevål NORDTER 2017, Helsinki Content - Why bedside chest
Interpreting thoracic x-ray of the supine immobile patient: Syllabus Johannes Godt Dep. of Radiology and Nuclear Medicine Oslo University Hospital Ullevål NORDTER 2017, Helsinki Content - Why bedside chest
4/16/2017. Learning Objectives. Interpretation of the Chest Radiograph. Components. Production of the Radiograph. Density & Appearance
 Interpretation of the Arthur Jones, EdD, RRT Learning Objectives Identify technical defects in chest radiographs Identify common radiographic abnormalities This Presentation is Approved for 1 CRCE Credit
Interpretation of the Arthur Jones, EdD, RRT Learning Objectives Identify technical defects in chest radiographs Identify common radiographic abnormalities This Presentation is Approved for 1 CRCE Credit
B-I-2 CARDIAC AND VASCULAR RADIOLOGY
 (YEARS 1 3) CURRICULUM FOR RADIOLOGY 13 B-I-2 CARDIAC AND VASCULAR RADIOLOGY KNOWLEDGE To describe the normal anatomy of the heart and vessels including the lymphatic system as demonstrated by radiographs,
(YEARS 1 3) CURRICULUM FOR RADIOLOGY 13 B-I-2 CARDIAC AND VASCULAR RADIOLOGY KNOWLEDGE To describe the normal anatomy of the heart and vessels including the lymphatic system as demonstrated by radiographs,
Advances in MDCT of Thoracic Trauma
 Baltic Congress of Radiology, Riga 2010 Advances in MDCT of Thoracic Trauma Robert A. Novelline, MD Professor of Radiology, Harvard Medical School Director of Emergency Radiology, Massachusetts General
Baltic Congress of Radiology, Riga 2010 Advances in MDCT of Thoracic Trauma Robert A. Novelline, MD Professor of Radiology, Harvard Medical School Director of Emergency Radiology, Massachusetts General
10/17/2016. Nuts and Bolts of Thoracic Radiology. Objectives. Techniques
 Nuts and Bolts of Thoracic Radiology October 20, 2016 Carleen Risaliti Objectives Understand the basics of chest radiograph Develop a system for interpreting chest radiographs Correctly identify thoracic
Nuts and Bolts of Thoracic Radiology October 20, 2016 Carleen Risaliti Objectives Understand the basics of chest radiograph Develop a system for interpreting chest radiographs Correctly identify thoracic
Chest X-ray Interpretation
 Chest X-ray Interpretation Introduction Routinely obtained Pulmonary specialist consultation Inherent physical exam limitations Chest x-ray limitations Physical exam and chest x-ray provide compliment
Chest X-ray Interpretation Introduction Routinely obtained Pulmonary specialist consultation Inherent physical exam limitations Chest x-ray limitations Physical exam and chest x-ray provide compliment
Imaging of Thoracic Trauma: Tips and Traps. Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania
 Imaging of Thoracic Trauma: Tips and Traps Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania None Disclosures Objectives Describe blunt and penetrating traumatic
Imaging of Thoracic Trauma: Tips and Traps Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania None Disclosures Objectives Describe blunt and penetrating traumatic
Learning Radiology: Recognizing the Basics. Text with Student Consult Online Access Code
 Learning Radiology: Recognizing the Basics. Text with Student Consult Online Access Code Herring, W ISBN-13: 9780323074445 Table of Contents 1. Recognizing Anything The "colorful" world of radiology A
Learning Radiology: Recognizing the Basics. Text with Student Consult Online Access Code Herring, W ISBN-13: 9780323074445 Table of Contents 1. Recognizing Anything The "colorful" world of radiology A
Chest X rays and Case Studies. No disclosures. Outline 5/31/2018. Carlo Manalo, M.D. Department of Radiology Loma Linda University Children s Hospital
 Chest X rays and Case Studies Carlo Manalo, M.D. Department of Radiology Loma Linda University Children s Hospital No disclosures. Outline Importance of history Densities delineated on radiography An approach
Chest X rays and Case Studies Carlo Manalo, M.D. Department of Radiology Loma Linda University Children s Hospital No disclosures. Outline Importance of history Densities delineated on radiography An approach
Chest X-ray (CXR) Interpretation Brent Burbridge, MD, FRCPC
 Interpretation Brent Burbridge, MD, FRCPC") Chest X-ray (CXR) Interpretation Brent Burbridge, MD, FRCPC An approach to reviewing a chest x-ray will create a foundation that will facilitate the detection of abnormalities. You should create your own
Chest X-ray (CXR) Interpretation Brent Burbridge, MD, FRCPC An approach to reviewing a chest x-ray will create a foundation that will facilitate the detection of abnormalities. You should create your own
CT of Acute Thoracic Aortic Syndromes Stuart S. Sagel, M.D.
 CT of Acute Thoracic Aortic Syndromes Stuart S. Sagel, M.D. Thoracic Aortic Aneurysms Atherosclerotic Dissection Penetrating ulcer Mycotic Inflammatory (vasculitis) Traumatic Aortic Imaging Options Catheter
CT of Acute Thoracic Aortic Syndromes Stuart S. Sagel, M.D. Thoracic Aortic Aneurysms Atherosclerotic Dissection Penetrating ulcer Mycotic Inflammatory (vasculitis) Traumatic Aortic Imaging Options Catheter
Shedding Light on Neonatal X-rays. Objectives. Indications for X-Rays 5/14/2018
 Shedding Light on Neonatal X-rays Barbara C. Mordue, MSN, NNP-BC Neonatal Nurse Practitioner LLUH Children s Hospital, NICU Objectives Utilize a systematic approach to neonatal x-ray interpretation Identify
Shedding Light on Neonatal X-rays Barbara C. Mordue, MSN, NNP-BC Neonatal Nurse Practitioner LLUH Children s Hospital, NICU Objectives Utilize a systematic approach to neonatal x-ray interpretation Identify
Chest XRay interpretation INTERPRETATIONS Identifications: Name & Date Technical evaluation Basic Interpretations
 Chest XRay interpretation INTERPRETATIONS Identifications: Name & Date Technical evaluation Basic Interpretations TECHNICAL EVALUATION 1. Projection: AP/PA view To differentiate between AP & PA films,
Chest XRay interpretation INTERPRETATIONS Identifications: Name & Date Technical evaluation Basic Interpretations TECHNICAL EVALUATION 1. Projection: AP/PA view To differentiate between AP & PA films,
TB Radiology for Nurses Garold O. Minns, MD
 TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
Introduction to Chest Radiography
 Introduction to Chest Radiography RSTH 366: DIAGNOSTIC TECHNIQUES Alan Alipoon BS, RCP, RRT Instructor Department of Cardiopulmonary Sciences 1 Introduction Discovered in 1895 by Wilhelm Roentgen Terminology
Introduction to Chest Radiography RSTH 366: DIAGNOSTIC TECHNIQUES Alan Alipoon BS, RCP, RRT Instructor Department of Cardiopulmonary Sciences 1 Introduction Discovered in 1895 by Wilhelm Roentgen Terminology
UERMMMC Department of Radiology. Basic Chest Radiology
 UERMMMC Department of Radiology Basic Chest Radiology PHYSICS DENSITIES BONE SOFT TISSUES WATER FAT AIR TELEROENTGENOGRAM Criteria for an Ideal Chest Radiograph 1. Upright 2. Posteroanterior View 3. Full
UERMMMC Department of Radiology Basic Chest Radiology PHYSICS DENSITIES BONE SOFT TISSUES WATER FAT AIR TELEROENTGENOGRAM Criteria for an Ideal Chest Radiograph 1. Upright 2. Posteroanterior View 3. Full
Signs in Chest Radiology
 Signs in Chest Radiology Jonathan H. Chung, MD Disclosures No pertinent disclosures Jonathan H. Chung, MD Assistant Professor Institute t of fadvanced d Biomedical Imaging National Jewish Health Denver,
Signs in Chest Radiology Jonathan H. Chung, MD Disclosures No pertinent disclosures Jonathan H. Chung, MD Assistant Professor Institute t of fadvanced d Biomedical Imaging National Jewish Health Denver,
Approach to CXR. Terminology. 1.Identification. Greg Blecher SCH Respir Fellow. Correct patient Correct date and time Correct examination
 Approach to CXR Greg Blecher SCH Respir Fellow From Rob Posteraro http://home.earthlink.net/~rhpos/cxr_interpret.txt.html ; http://home.earthlink.net/~rhpos/cxr_main.txt.html) Approach to viewing Chest
Approach to CXR Greg Blecher SCH Respir Fellow From Rob Posteraro http://home.earthlink.net/~rhpos/cxr_interpret.txt.html ; http://home.earthlink.net/~rhpos/cxr_main.txt.html) Approach to viewing Chest
Undergraduate Teaching
 Prof. James F Meaney Undergraduate Teaching Chest X-Ray Understanding the normal anatomical by reference to cross sectional imaging Radiology? It s FUN! Cryptic puzzle Sudoku (Minecraft?) It s completely
Prof. James F Meaney Undergraduate Teaching Chest X-Ray Understanding the normal anatomical by reference to cross sectional imaging Radiology? It s FUN! Cryptic puzzle Sudoku (Minecraft?) It s completely
Radiology of the respiratory disease
 Radiology of the respiratory disease [ Color index: Important Notes Extra ] [ Editing file Feedback Share your notes Shared notes ] Resources: - 435 Slides - 434 Team - 435 Notes Done by: - Mai Alageel
Radiology of the respiratory disease [ Color index: Important Notes Extra ] [ Editing file Feedback Share your notes Shared notes ] Resources: - 435 Slides - 434 Team - 435 Notes Done by: - Mai Alageel
Interactive Lecture. Lecture 7 - Interactive. Radiology of cardiorespiratory disease. Editing File. Done By. Color Coding Important Notes Extra
 Lecture 7 - Interactive 436 Teams Interactive Lecture Radiology of cardiorespiratory disease Done By Team Leaders: Khalid Alshehri Hanin Bashaikh Team Members: Ghaida Alsaeed Maha Alissa Nawwaf AlHarbi
Lecture 7 - Interactive 436 Teams Interactive Lecture Radiology of cardiorespiratory disease Done By Team Leaders: Khalid Alshehri Hanin Bashaikh Team Members: Ghaida Alsaeed Maha Alissa Nawwaf AlHarbi
General Imaging. Imaging modalities. Incremental CT. Multislice CT Multislice CT [ MDCT ]
![General Imaging. Imaging modalities. Incremental CT. Multislice CT Multislice CT [ MDCT ]](/thumbs/76/74079340.jpg "General Imaging. Imaging modalities. Incremental CT. Multislice CT Multislice CT [ MDCT ]") General Imaging Imaging modalities Conventional X-rays Ultrasonography [ US ] Computed tomography [ CT ] Radionuclide imaging Magnetic resonance imaging [ MRI ] Angiography conventional, CT,MRI Interventional
General Imaging Imaging modalities Conventional X-rays Ultrasonography [ US ] Computed tomography [ CT ] Radionuclide imaging Magnetic resonance imaging [ MRI ] Angiography conventional, CT,MRI Interventional
Radiological conference. Left upper lobe collapse. Citation Hong Kong Practitioner, 1998, v. 20 n. 9, p
 Title Radiological conference. Left upper lobe collapse Author(s) Wong, LLS; Peh, WCG Citation Hong Kong Practitioner, 1998, v. 20 n. 9, p. 513-517 Issued Date 1998 URL http://hdl.handle.net/10722/44672
Title Radiological conference. Left upper lobe collapse Author(s) Wong, LLS; Peh, WCG Citation Hong Kong Practitioner, 1998, v. 20 n. 9, p. 513-517 Issued Date 1998 URL http://hdl.handle.net/10722/44672
An Introduction to Radiology for TB Nurses
 An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
Radiology of the respiratory/cardiac diseases (part 2)
") Cardiology Cycle - Lecture 6 436 Teams Radiology of the respiratory/cardiac diseases (part 2) Objectives Done By Team Leaders: Khalid Alshehri Hanin Bashaikh Team Members: Leena Alwakeel Aroob Alhuthail
Cardiology Cycle - Lecture 6 436 Teams Radiology of the respiratory/cardiac diseases (part 2) Objectives Done By Team Leaders: Khalid Alshehri Hanin Bashaikh Team Members: Leena Alwakeel Aroob Alhuthail
X-Rays. Prepared by Prof.Dr. Magda Hassab Allah Assist.lecturer Marwa Al Hady
 X-Rays Prepared by Prof.Dr. Magda Hassab Allah Assist.lecturer Marwa Al Hady CHEST X-RAYS Normal Chest X-ray Comments on chest X ray includes examination of 1- Bony cage (ribs,clavicles &vertebral column
X-Rays Prepared by Prof.Dr. Magda Hassab Allah Assist.lecturer Marwa Al Hady CHEST X-RAYS Normal Chest X-ray Comments on chest X ray includes examination of 1- Bony cage (ribs,clavicles &vertebral column
Children are not small adults Children are Not Small Adults Anatomic considerations Pliable bony & cartilagenous structures - Significant thoracic inj
 PEDIATRIC CHEST TRAUMA Children are not small adults Role of imaging Spectrum of injury Children are not small adults Children are Not Small Adults Anatomic considerations Pliable bony & cartilagenous
PEDIATRIC CHEST TRAUMA Children are not small adults Role of imaging Spectrum of injury Children are not small adults Children are Not Small Adults Anatomic considerations Pliable bony & cartilagenous
Acute Aortic Syndromes
 Acute Aortic Syndromes Carole J. Dennie, MD Acute Thoracic Aortic Syndromes Background Non-Traumatic Acute Thoracic Aortic Syndromes Carole Dennie MD FRCPC Associate Professor of Radiology and Cardiology
Acute Aortic Syndromes Carole J. Dennie, MD Acute Thoracic Aortic Syndromes Background Non-Traumatic Acute Thoracic Aortic Syndromes Carole Dennie MD FRCPC Associate Professor of Radiology and Cardiology
PATIENT DATA EVALUATION AND RECOMMENDATION: IMAGING STUDIES
 PATIENT DATA EVALUATION AND RECOMMENDATION: IMAGING STUDIES Robert Harwood, MSA, RRT-NPS Objectives At the end of this presentation the student should be able to: Describe the indications of a chest radiograph.
PATIENT DATA EVALUATION AND RECOMMENDATION: IMAGING STUDIES Robert Harwood, MSA, RRT-NPS Objectives At the end of this presentation the student should be able to: Describe the indications of a chest radiograph.
X-Rays. Kunal D Patel Research Fellow IMM
 X-Rays Kunal D Patel Research Fellow IMM The 12-Steps } 1: Name 2: Date 3: Old films 4: What type of view(s) 5: Penetration } Pre-read 6: Inspiration 7: Rotation Quality Control 8: Angulation 9: Soft tissues
X-Rays Kunal D Patel Research Fellow IMM The 12-Steps } 1: Name 2: Date 3: Old films 4: What type of view(s) 5: Penetration } Pre-read 6: Inspiration 7: Rotation Quality Control 8: Angulation 9: Soft tissues
Diseases of the Aorta
 Diseases of the Aorta ASE Review 2018 Susan E Wiegers, MD, FASE, FACC Professor of Medicine My great friend Dr. Roberto Lang Disclosure None related to this presentation 1 Objectives Aneurysm Dissection
Diseases of the Aorta ASE Review 2018 Susan E Wiegers, MD, FASE, FACC Professor of Medicine My great friend Dr. Roberto Lang Disclosure None related to this presentation 1 Objectives Aneurysm Dissection
ARDS - a must know. Page 1 of 14
 ARDS - a must know Poster No.: C-1683 Congress: ECR 2016 Type: Authors: Keywords: DOI: Educational Exhibit M. Cristian; Turda/RO Education and training, Edema, Acute, Localisation, Education, Digital radiography,
ARDS - a must know Poster No.: C-1683 Congress: ECR 2016 Type: Authors: Keywords: DOI: Educational Exhibit M. Cristian; Turda/RO Education and training, Edema, Acute, Localisation, Education, Digital radiography,
Elderly Man with Dyspnoea
 Asia Pacific Family Medicine, 2004; 3 (1-2): 46-50 RADIOLOGY SERIES Elderly Man with Dyspnoea Wei-Yang LIM Faculty of Medicine National University of Singapore, Singapore Wilfred CG PEH Singapore Health
Asia Pacific Family Medicine, 2004; 3 (1-2): 46-50 RADIOLOGY SERIES Elderly Man with Dyspnoea Wei-Yang LIM Faculty of Medicine National University of Singapore, Singapore Wilfred CG PEH Singapore Health
Imaging of Pleural Effusion: Comparing Ultrasound, X-Ray and CT findings
 Imaging of Pleural Effusion: Comparing Ultrasound, X-Ray and CT findings Poster No.: C-2067 Congress: ECR 2017 Type: Educational Exhibit Authors: J. M. Almeida, N. Antunes, C. Leal, L. Figueiredo ; Lisboa/PT,
Imaging of Pleural Effusion: Comparing Ultrasound, X-Ray and CT findings Poster No.: C-2067 Congress: ECR 2017 Type: Educational Exhibit Authors: J. M. Almeida, N. Antunes, C. Leal, L. Figueiredo ; Lisboa/PT,
Disclosure. Clinical Chest Radiography Interpretation Part I
 Clinical Chest Radiography Interpretation Part I Anthony M. Angelow, PhD(c), MSN, ACNPC, AGACNP-BC, CEN Associate Lecturer, Fitzgerald Health Education Associates Clinical practice Division of Trauma Surgery
Clinical Chest Radiography Interpretation Part I Anthony M. Angelow, PhD(c), MSN, ACNPC, AGACNP-BC, CEN Associate Lecturer, Fitzgerald Health Education Associates Clinical practice Division of Trauma Surgery
Cardiac Radiography. Jared D. Christensen, M.D.
 Cardiac Radiography Jared D. Christensen, M.D. Cardiac radiography Jared D. Christensen, M.D. Overview Basic Concepts Technique Normal anatomy Cases Technique 3 Standard Views Posterior-Anterior (PA) Anterior-Posterior
Cardiac Radiography Jared D. Christensen, M.D. Cardiac radiography Jared D. Christensen, M.D. Overview Basic Concepts Technique Normal anatomy Cases Technique 3 Standard Views Posterior-Anterior (PA) Anterior-Posterior
A pictorial review of thoracic imaging of intensive care patients
 A pictorial review of thoracic imaging of intensive care patients Poster No.: C-1003 Congress: ECR 2010 Type: Educational Exhibit Topic: Chest Authors: E. Y. P. Lee, H. C. Mathias; Cardiff/UK Keywords:
A pictorial review of thoracic imaging of intensive care patients Poster No.: C-1003 Congress: ECR 2010 Type: Educational Exhibit Topic: Chest Authors: E. Y. P. Lee, H. C. Mathias; Cardiff/UK Keywords:
An Image Repository for Chest CT
 An Image Repository for Chest CT Francesco Frajoli for the Chest CT in Antibody Deficiency Group An Image Repository for Chest CT he Chest CT in Antibody Deficiency Group is an international and interdisciplinary
An Image Repository for Chest CT Francesco Frajoli for the Chest CT in Antibody Deficiency Group An Image Repository for Chest CT he Chest CT in Antibody Deficiency Group is an international and interdisciplinary
Disclosure. Clinical Chest Radiography Interpretation Part II
 Clinical Chest Radiography Interpretation Part II Anthony M. Angelow, PhD(c), MSN, ACNPC, AGACNP-BC, CEN Associate Lecturer, Fitzgerald Health Education Associates Clinical practice Division of Trauma
Clinical Chest Radiography Interpretation Part II Anthony M. Angelow, PhD(c), MSN, ACNPC, AGACNP-BC, CEN Associate Lecturer, Fitzgerald Health Education Associates Clinical practice Division of Trauma
In ESH we usually see blunt chest trauma but penetrating injuries also treated here (usually as single injuries, like stab wound)
") Chest Trauma Dr Csaba Dioszeghy MD PhD FRCEM FFICM FERC East Surrey Hospital Emergency Department Scope Thoracic injuries are common and can be life threatening In ESH we usually see blunt chest trauma
Chest Trauma Dr Csaba Dioszeghy MD PhD FRCEM FFICM FERC East Surrey Hospital Emergency Department Scope Thoracic injuries are common and can be life threatening In ESH we usually see blunt chest trauma
Interpretation of the chest radiograph Elizabeth Puddy MB ChB FCARCSI Catherine Hill MB ChB MRCP FRCR
 Interpretation of the chest radiograph Elizabeth Puddy MB ChB FCARCSI Catherine Hill MB ChB MRCP FRCR The traditional technique used in the acquisition and development of a chest radiograph uses methods
Interpretation of the chest radiograph Elizabeth Puddy MB ChB FCARCSI Catherine Hill MB ChB MRCP FRCR The traditional technique used in the acquisition and development of a chest radiograph uses methods
Chest Radiology Interpretation: Findings of Tuberculosis
 Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
Eun-Young Kang, M.D., Jae Wook Lee, M.D., Ji Yung Choo, M.D., Hwan Seok Yong, M.D., Ki Yeol Lee, M.D., Yu-Whan Oh, M.D.
 Eun-Young Kang, M.D., Jae Wook Lee, M.D., Ji Yung Choo, M.D., Hwan Seok Yong, M.D., Ki Yeol Lee, M.D., Yu-Whan Oh, M.D. Department of Radiology, Korea University Guro Hospital, College of Medicine, Korea
Eun-Young Kang, M.D., Jae Wook Lee, M.D., Ji Yung Choo, M.D., Hwan Seok Yong, M.D., Ki Yeol Lee, M.D., Yu-Whan Oh, M.D. Department of Radiology, Korea University Guro Hospital, College of Medicine, Korea
Case 1. A 35-year-old male presented with fever, cough, and purulent sputum for one week. This was his CXR (Fig. 1.1). What is the diagnosis?
. What is the diagnosis?") 1 Interpreting Chest X-Rays CASE 1 Fig. 1.1 Case 1. A 35-year-old male presented with fever, cough, and purulent sputum for one week. This was his CXR (Fig. 1.1). What is the diagnosis? CASE 1 Interpreting
1 Interpreting Chest X-Rays CASE 1 Fig. 1.1 Case 1. A 35-year-old male presented with fever, cough, and purulent sputum for one week. This was his CXR (Fig. 1.1). What is the diagnosis? CASE 1 Interpreting
Alexander A Schult, M.D., FCCP. October 21, 2017 Revised 1/10/18
 Alexander A Schult, M.D., FCCP October 21, 2017 Revised 1/10/18 Identifying normal anatomy Identifying various pathologic states Identifying placement of hardware Identifying limitations of portable CXR
Alexander A Schult, M.D., FCCP October 21, 2017 Revised 1/10/18 Identifying normal anatomy Identifying various pathologic states Identifying placement of hardware Identifying limitations of portable CXR
Radiological Anatomy of Thorax. Dr. Jamila Elmedany & Prof. Saeed Abuel Makarem
 Radiological Anatomy of Thorax Dr. Jamila Elmedany & Prof. Saeed Abuel Makarem Indications for Chest x - A chest x-ray may be used to diagnose and plan treatment for various conditions, including: Diseases/Fractures
Radiological Anatomy of Thorax Dr. Jamila Elmedany & Prof. Saeed Abuel Makarem Indications for Chest x - A chest x-ray may be used to diagnose and plan treatment for various conditions, including: Diseases/Fractures
Interesting Cases. Pulmonary
 Interesting Cases Pulmonary 54M with prior history of COPD, hep B/C, and possible history of TB presented with acute on chronic dyspnea, and productive cough Hazy opacity overlying the left hemithorax
Interesting Cases Pulmonary 54M with prior history of COPD, hep B/C, and possible history of TB presented with acute on chronic dyspnea, and productive cough Hazy opacity overlying the left hemithorax
CHEST & ABDOMINAL X-RAYS MALIKA IBRAHIM CORE MEDICAL TRAINEE BLACKPOOL VICTORIA HOSPITAL DATA INTERPRETATION COURSE FEB 20, 2017
 CHEST & ABDOMINAL X-RAYS MALIKA IBRAHIM CORE MEDICAL TRAINEE BLACKPOOL VICTORIA HOSPITAL DATA INTERPRETATION COURSE FEB 20, 2017 1. Sample x-rays 2. Basic chest x-ray interpretation skills 3. Chest x-ray
CHEST & ABDOMINAL X-RAYS MALIKA IBRAHIM CORE MEDICAL TRAINEE BLACKPOOL VICTORIA HOSPITAL DATA INTERPRETATION COURSE FEB 20, 2017 1. Sample x-rays 2. Basic chest x-ray interpretation skills 3. Chest x-ray
Concepts in Small Animal Thoracic Radiology Thoracic Radiology
 Concepts in Small Animal Thoracic Radiology + Radiology of the Pleural Space VMB 960 2/21/2011 Optimizing Image Quality Inherent subject contrast Thorax has high inherent subject contrast c/f abdomen Primarily
Concepts in Small Animal Thoracic Radiology + Radiology of the Pleural Space VMB 960 2/21/2011 Optimizing Image Quality Inherent subject contrast Thorax has high inherent subject contrast c/f abdomen Primarily
Pulmonary Embolism. Thoracic radiologist Helena Lauri
 Pulmonary Embolism Thoracic radiologist Helena Lauri 8.5.2017 Statistics 1-2 out of 1000 adults annually are diagnosed with deep vein thrombosis (DVT) and/or pulmonary embolism (PE) About half of patients
Pulmonary Embolism Thoracic radiologist Helena Lauri 8.5.2017 Statistics 1-2 out of 1000 adults annually are diagnosed with deep vein thrombosis (DVT) and/or pulmonary embolism (PE) About half of patients
PULMONARY TUBERCULOSIS RADIOLOGY
 PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
Management of Pleural Effusion
 Management of Pleural Effusion Development of Pleural Effusion pulmonary capillary pressure (CHF) capillary permeability (Pneumonia) intrapleural pressure (atelectasis) plasma oncotic pressure (hypoalbuminemia)
Management of Pleural Effusion Development of Pleural Effusion pulmonary capillary pressure (CHF) capillary permeability (Pneumonia) intrapleural pressure (atelectasis) plasma oncotic pressure (hypoalbuminemia)
Diseases of the aorta
 Diseases of the aorta Aneurysm, dissection and aortitis are the main pathologies (Fig. 18.79 ). data:text/html;charset=utf-8,%3ch2%20id%3d%22cc5a0836d6aa490ca26dd7c15632b559%22%20style%3d%22margin%3a%201.3em%200px%200.5em%3b%20padding%3a%200px%3b%20border%3a%200px%3b%20font-fa
Diseases of the aorta Aneurysm, dissection and aortitis are the main pathologies (Fig. 18.79 ). data:text/html;charset=utf-8,%3ch2%20id%3d%22cc5a0836d6aa490ca26dd7c15632b559%22%20style%3d%22margin%3a%201.3em%200px%200.5em%3b%20padding%3a%200px%3b%20border%3a%200px%3b%20font-fa
Chest and cardiovascular
 Module 1 Chest and cardiovascular A. Doss and M. J. Bull 1. Regarding the imaging modalities of the chest: High resolution computed tomography (HRCT) uses a slice thickness of 4 6 mm to identify mass lesions
Module 1 Chest and cardiovascular A. Doss and M. J. Bull 1. Regarding the imaging modalities of the chest: High resolution computed tomography (HRCT) uses a slice thickness of 4 6 mm to identify mass lesions
Life-Threatening Chest Pain. Case Scenarios 王宗倫主任. Case 1. Case 1. Case 1. Case 1
 Life-Threatening Chest Pain Case Scenarios 王宗倫主任 101.07.17 Acute Coronary Syndrome Dissecting Aortic Aneurysm Pulmonary Embolism Tension Pneumothorax Cardiac Tamponade Esophageal Rupture 1 2 A 70-year-old
Life-Threatening Chest Pain Case Scenarios 王宗倫主任 101.07.17 Acute Coronary Syndrome Dissecting Aortic Aneurysm Pulmonary Embolism Tension Pneumothorax Cardiac Tamponade Esophageal Rupture 1 2 A 70-year-old
Chest Roentgenography for Cardiovascular Evaluation
 34 Chest Roentgenography for Cardiovascular Evaluation ERIC MANHEIMER Definition and Basic Science These topics are presented in Chapter 48, Chest Roentgenography for Pulmonary Evaluation. Technique and
34 Chest Roentgenography for Cardiovascular Evaluation ERIC MANHEIMER Definition and Basic Science These topics are presented in Chapter 48, Chest Roentgenography for Pulmonary Evaluation. Technique and
CT Chest. Verification of an opacity seen on the straight chest X ray
 CT Chest Indications: To assess equivocal plain x-ray findings Staging of lung neoplasm Merastatic workup of extra thoraces malignancies Diagnosis of diffuse lung diseases with HRCT Assessment of bronchietasis
CT Chest Indications: To assess equivocal plain x-ray findings Staging of lung neoplasm Merastatic workup of extra thoraces malignancies Diagnosis of diffuse lung diseases with HRCT Assessment of bronchietasis
Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine
 Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine Venous thromboembolism: pulmonary embolism (PE) deep vein thrombosis (DVT) 1% of all patients admitted to hospital 5% of in-hospital mortality
Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine Venous thromboembolism: pulmonary embolism (PE) deep vein thrombosis (DVT) 1% of all patients admitted to hospital 5% of in-hospital mortality
Chapter 2 Cardiac Interpretation of Pediatric Chest X-Ray
 Chapter 2 Cardiac Interpretation of Pediatric Chest X-Ray Ra-id Abdulla and Douglas M. Luxenberg Key Facts The cardiac silhouette occupies 50 55% of the chest width on an anterior posterior chest X-ray
Chapter 2 Cardiac Interpretation of Pediatric Chest X-Ray Ra-id Abdulla and Douglas M. Luxenberg Key Facts The cardiac silhouette occupies 50 55% of the chest width on an anterior posterior chest X-ray
AORTIC DISSECTIONS Current Management. TOMAS D. MARTIN, MD, LAT Professor, TCV Surgery Director UF Health Aortic Disease Center University of Florida
 AORTIC DISSECTIONS Current Management TOMAS D. MARTIN, MD, LAT Professor, TCV Surgery Director UF Health Aortic Disease Center University of Florida DISCLOSURES Terumo Medtronic Cook Edwards Cryolife AORTIC
AORTIC DISSECTIONS Current Management TOMAS D. MARTIN, MD, LAT Professor, TCV Surgery Director UF Health Aortic Disease Center University of Florida DISCLOSURES Terumo Medtronic Cook Edwards Cryolife AORTIC
A Practical Approach to Ultrasound Assessment of Respiratory Distress
 A Practical Approach to Ultrasound Assessment of Respiratory Distress Yanick Beaulieu, MD, FRCPC Director, Bedside Ultrasound Curriculum Division of Cardiology and Critical Care Hôpital du Sacré-Coeur
A Practical Approach to Ultrasound Assessment of Respiratory Distress Yanick Beaulieu, MD, FRCPC Director, Bedside Ultrasound Curriculum Division of Cardiology and Critical Care Hôpital du Sacré-Coeur
Enter modality here Enter modality here, enter none if none. Principal Modality (2): Case Report # [] Date accepted: April 2015
![Enter modality here Enter modality here, enter none if none. Principal Modality (2): Case Report # [] Date accepted: April 2015](/thumbs/83/87309292.jpg "Enter modality here Enter modality here, enter none if none. Principal Modality (2): Case Report # [] Date accepted: April 2015") Radiological Category: Enter category here Principal Modality (1): Principal Modality (2): Enter modality here Enter modality here, enter none if none Case Report # [] Submitted by: Varun Rachakonda, M.D.
Radiological Category: Enter category here Principal Modality (1): Principal Modality (2): Enter modality here Enter modality here, enter none if none Case Report # [] Submitted by: Varun Rachakonda, M.D.
Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations
: Pleuropulmonary Manifestations") 08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
An aneurysm is a localized abnormal dilation of a blood vessel or the heart Types: 1-"true" aneurysm it involves all three layers of the arterial
 An aneurysm is a localized abnormal dilation of a blood vessel or the heart Types: 1-"true" aneurysm it involves all three layers of the arterial wall (intima, media, and adventitia) or the attenuated
An aneurysm is a localized abnormal dilation of a blood vessel or the heart Types: 1-"true" aneurysm it involves all three layers of the arterial wall (intima, media, and adventitia) or the attenuated
Heart and Lungs. LUNG Coronal section demonstrates relationship of pulmonary parenchyma to heart and chest wall.
 Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
Case 47 Clinical Presentation
 93 Case 47 C Clinical Presentation 45-year-old man presents with chest pain and new onset of a murmur. Echocardiography shows severe aortic insufficiency. 94 RadCases Cardiac Imaging Imaging Findings C
93 Case 47 C Clinical Presentation 45-year-old man presents with chest pain and new onset of a murmur. Echocardiography shows severe aortic insufficiency. 94 RadCases Cardiac Imaging Imaging Findings C
IMAGING the AORTA. Mirvat Alasnag FACP, FSCAI, FSCCT, FASE June 1 st, 2011
 IMAGING the AORTA Mirvat Alasnag FACP, FSCAI, FSCCT, FASE June 1 st, 2011 September 11, 2003 Family is asking $67 million in damages from two doctors Is it an aneurysm? Is it a dissection? What type of
IMAGING the AORTA Mirvat Alasnag FACP, FSCAI, FSCCT, FASE June 1 st, 2011 September 11, 2003 Family is asking $67 million in damages from two doctors Is it an aneurysm? Is it a dissection? What type of
Case 9799 Stanford type A aortic dissection: US and CT findings
 Case 9799 Stanford type A aortic dissection: US and CT findings Accogli S, Aringhieri G, Scalise P, Angelini G, Pancrazi F, Bemi P, Bartolozzi C Department of Diagnostic and Interventional Radiology, University
Case 9799 Stanford type A aortic dissection: US and CT findings Accogli S, Aringhieri G, Scalise P, Angelini G, Pancrazi F, Bemi P, Bartolozzi C Department of Diagnostic and Interventional Radiology, University
Unilateral pulmonary oedema, a forgotten presentation.
 Unilateral pulmonary oedema, a forgotten presentation. Poster No.: C-2146 Congress: ECR 2018 Type: Educational Exhibit Authors: C. A. Arboleda Vallejo, M. I. carvajal, M. Perez ; Medellin, 1 2 1 1 2 Antioquia/CO,
Unilateral pulmonary oedema, a forgotten presentation. Poster No.: C-2146 Congress: ECR 2018 Type: Educational Exhibit Authors: C. A. Arboleda Vallejo, M. I. carvajal, M. Perez ; Medellin, 1 2 1 1 2 Antioquia/CO,
FUNDAMENTALS OF CXR INTERPRETATION THE BASICS
 FUNDAMENTALS OF CXR INTERPRETATION THE BASICS PART I QUALITY ASSESSMENT 1 PATIENT-DEPENDENT FACTORS 3 REVIEW OF IMPORTANT ANATOMY 7 LUNGS AND PLEURA 11 DIAPHRAGMS 13 BONES AND SOFT TISSUES 14 A BRIEF LOOK
FUNDAMENTALS OF CXR INTERPRETATION THE BASICS PART I QUALITY ASSESSMENT 1 PATIENT-DEPENDENT FACTORS 3 REVIEW OF IMPORTANT ANATOMY 7 LUNGS AND PLEURA 11 DIAPHRAGMS 13 BONES AND SOFT TISSUES 14 A BRIEF LOOK
Lecture 2: Clinical anatomy of thoracic cage and cavity II
 Lecture 2: Clinical anatomy of thoracic cage and cavity II Dr. Rehan Asad At the end of this session, the student should be able to: Identify and discuss clinical anatomy of mediastinum such as its deflection,
Lecture 2: Clinical anatomy of thoracic cage and cavity II Dr. Rehan Asad At the end of this session, the student should be able to: Identify and discuss clinical anatomy of mediastinum such as its deflection,
Manage TB Dr. A. Chitrakumar Madras Medical College and RGGGH Institute of Thoracic Medicine, Chennai
 Manage TB Dr. A. Chitrakumar Madras Medical College and RGGGH Institute of Thoracic Medicine, Chennai Lecture 16 Radiology in diagnosis of Tuberculosis Session 01 So, welcome to the session Radiology in
Manage TB Dr. A. Chitrakumar Madras Medical College and RGGGH Institute of Thoracic Medicine, Chennai Lecture 16 Radiology in diagnosis of Tuberculosis Session 01 So, welcome to the session Radiology in
ACUTE AORTIC SYNDROMES
 ACUTE AORTIC SYNDROMES AGNETA FLINCK MD, PhD Dept. of Thoracic Radiology Sahlgrenska University Hospital ACUTE AORTIC SYNDROMES Aortic dissection Intramural hematoma (IMH) 5-20% Penetrating atherosclerotic
ACUTE AORTIC SYNDROMES AGNETA FLINCK MD, PhD Dept. of Thoracic Radiology Sahlgrenska University Hospital ACUTE AORTIC SYNDROMES Aortic dissection Intramural hematoma (IMH) 5-20% Penetrating atherosclerotic
Two Cases of Incidentally Picked Up Adult Unilateral Pulmonary Artery Atresia with Variable Imaging Features
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 16, Issue 12 Ver. III (Dec. 2017), PP 45-49 www.iosrjournals.org Two Cases of Incidentally Picked Up
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 16, Issue 12 Ver. III (Dec. 2017), PP 45-49 www.iosrjournals.org Two Cases of Incidentally Picked Up
Restrictive Pulmonary Diseases
 Restrictive Pulmonary Diseases Causes: Acute alveolo-capillary sysfunction Interstitial disease Pleural disorders Chest wall disorders Neuromuscular disease Resistance Pathophysiology Reduced compliance
Restrictive Pulmonary Diseases Causes: Acute alveolo-capillary sysfunction Interstitial disease Pleural disorders Chest wall disorders Neuromuscular disease Resistance Pathophysiology Reduced compliance
Cardio-vascular syndrome. Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology
 Cardio-vascular syndrome Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Left pulmonary artery Right pulmonary artery OFCP Left
Cardio-vascular syndrome Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Left pulmonary artery Right pulmonary artery OFCP Left
Radiological Investigations of Abdominal Trauma
 76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
The Management of Chest Trauma. Tom Scaletta, MD FAAEM Immediate Past President, AAEM
 The Management of Chest Trauma Tom Scaletta, MD FAAEM Immediate Past President, AAEM Trichotomizing Rib Fractures Upper 1-3 vascular injuries Middle 4-9 Lower 10-12 12 liver/spleen injuries Management
The Management of Chest Trauma Tom Scaletta, MD FAAEM Immediate Past President, AAEM Trichotomizing Rib Fractures Upper 1-3 vascular injuries Middle 4-9 Lower 10-12 12 liver/spleen injuries Management
Case Acute ascending thoracic aortic rupture due to penetrating atherosclerotic ulcer
 Case 12305 Acute ascending thoracic aortic rupture due to penetrating atherosclerotic ulcer Lopes Dias J, Costa NV, Leal C, Alves P, Bilhim T Section: Chest Imaging Published: 2014, Dec. 19 Patient: 68
Case 12305 Acute ascending thoracic aortic rupture due to penetrating atherosclerotic ulcer Lopes Dias J, Costa NV, Leal C, Alves P, Bilhim T Section: Chest Imaging Published: 2014, Dec. 19 Patient: 68
Pitfalls of the Pediatric Chest and Abdomen SPR 2017
 Pitfalls of the Pediatric Chest and Abdomen SPR 2017 Richard I. Markowitz, MD, FACR Children s Hospital of Philadelphia Perelman School of Medicine University of Pennsylvania No Disclosures Cognitive Perceptual
Pitfalls of the Pediatric Chest and Abdomen SPR 2017 Richard I. Markowitz, MD, FACR Children s Hospital of Philadelphia Perelman School of Medicine University of Pennsylvania No Disclosures Cognitive Perceptual
Lecture 3. Inflammatory Processes
 Lecture 3 Inflammatory Processes Process: Increased vascular permeability Water and cellular infiltrations Results: Abscess, ulceration, cavitation Penetration, perforation and fistula formation Scarring,
Lecture 3 Inflammatory Processes Process: Increased vascular permeability Water and cellular infiltrations Results: Abscess, ulceration, cavitation Penetration, perforation and fistula formation Scarring,
AORTIC DISSECTION. DISSECTING ANEURYSMS OF THE AORTA or CLASSIFICATION
 DISSECTING ANEURYSMS OF THE AORTA or AORTIC DISSECTION CLASSIFICATION DeBakey classified aortic dissections into types I, II, and III :- Type I dissection the tear site originates in the ascending aorta,
DISSECTING ANEURYSMS OF THE AORTA or AORTIC DISSECTION CLASSIFICATION DeBakey classified aortic dissections into types I, II, and III :- Type I dissection the tear site originates in the ascending aorta,
Lung Cancer - Suspected
 Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
The Chest X-ray for Cardiologists
 Mayo Clinic & British Cardiovascular Society at the Royal College of Physicians, London : 21-23-October 2013 Cases-Controversies-Updates 2013 The Chest X-ray for Cardiologists Michael Rubens Royal Brompton
Mayo Clinic & British Cardiovascular Society at the Royal College of Physicians, London : 21-23-October 2013 Cases-Controversies-Updates 2013 The Chest X-ray for Cardiologists Michael Rubens Royal Brompton
Introduction to Chest CT Interpretation. Objectives 8/28/2017
 Introduction to Chest CT Interpretation Deborah Stein ACNP BC, CCRN NP Education Specialist Department of Anesthesia and Critical Care Medicine August 28, 2017 Objectives Basic Principles Thoracic Anatomy
Introduction to Chest CT Interpretation Deborah Stein ACNP BC, CCRN NP Education Specialist Department of Anesthesia and Critical Care Medicine August 28, 2017 Objectives Basic Principles Thoracic Anatomy
Computed tomography of the chest: I. Basic principles
 BJA Education, 15 (6): 299 304 (2015) doi: 10.1093/bjaceaccp/mku063 Advance Access Publication Date: 2 February 2015 Matrix reference 1A03, 2A12 Computed tomography of the chest: I. Basic principles P
BJA Education, 15 (6): 299 304 (2015) doi: 10.1093/bjaceaccp/mku063 Advance Access Publication Date: 2 February 2015 Matrix reference 1A03, 2A12 Computed tomography of the chest: I. Basic principles P
The opaque hemithorax
 The opaque hemithorax Poster No.: C-1480 Congress: ECR 2013 Type: Educational Exhibit Authors: M. Iordache, M. Hanachiuc, C. Moldoveanu, D. Negru; Iasi/RO Keywords: Infection, Atelectasis, elearning, Ultrasound,
The opaque hemithorax Poster No.: C-1480 Congress: ECR 2013 Type: Educational Exhibit Authors: M. Iordache, M. Hanachiuc, C. Moldoveanu, D. Negru; Iasi/RO Keywords: Infection, Atelectasis, elearning, Ultrasound,
Right lung. -fissures:
 -Right lung is shorter and wider because it is compressed by the right copula of the diaphragm by the live.. 2 fissure, 3 lobes.. hilum : 2 bronchi ( ep-arterial, hyp-arterial ), one artery mediastinal
-Right lung is shorter and wider because it is compressed by the right copula of the diaphragm by the live.. 2 fissure, 3 lobes.. hilum : 2 bronchi ( ep-arterial, hyp-arterial ), one artery mediastinal
Surgical indications: Non-malignant pulmonary diseases. Punnarerk Thongcharoen
 Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
CHEST INJURY PULMONARY CONTUSION
 CHEST INJURY PULMONARY CONTUSION Introduction Pulmonary contusion refers to blunt traumatic lung parenchymal injury which results in oedema and haemorrhaging into alveolar spaces. It may also result in
CHEST INJURY PULMONARY CONTUSION Introduction Pulmonary contusion refers to blunt traumatic lung parenchymal injury which results in oedema and haemorrhaging into alveolar spaces. It may also result in
Objectives. What is a Chest X Ray? CXR Workshop. Definition (diagnostic tool/internal PE) Types. Cost
 Types. Cost") Objectives CAPA 2011 Christy Wilson, PA C Georgia Lung Associates Identify the radiographic landmarks on a chest radiograph Recognize identifiers of poor quality on the chest radiograph Outline an approach
Objectives CAPA 2011 Christy Wilson, PA C Georgia Lung Associates Identify the radiographic landmarks on a chest radiograph Recognize identifiers of poor quality on the chest radiograph Outline an approach
Radiology. Undergraduate Radiology Sample Questions
 Radiology Undergraduate Radiology Sample Questions April 2012 The following examples are offered of questions that might be used to assess undergraduate radiology. There are 3 different styles: An OSCE
Radiology Undergraduate Radiology Sample Questions April 2012 The following examples are offered of questions that might be used to assess undergraduate radiology. There are 3 different styles: An OSCE
8/14/2017. Objective: correlate radiographic findings of common lung diseases to actual lung pathologic features
 What is that lung disease? Pulmonary Patterns & Correlated Pathology Dr. Russell Tucker, DACVR Objective: correlate radiographic findings of common lung diseases to actual lung pathologic features Improved
What is that lung disease? Pulmonary Patterns & Correlated Pathology Dr. Russell Tucker, DACVR Objective: correlate radiographic findings of common lung diseases to actual lung pathologic features Improved
PLR3 12/7/04 8:16 PM Page 65. Chapter 3. Cardiovascular system
 PLR3 12/7/04 8:16 PM Page 65 Chapter 3 Cardiovascular system 65 PLR3 12/7/04 8:16 PM Page 66 Chapter 3 Cardiovascular system Cardiovascular investigations Plain films Evaluate heart size and chamber enlargement.
PLR3 12/7/04 8:16 PM Page 65 Chapter 3 Cardiovascular system 65 PLR3 12/7/04 8:16 PM Page 66 Chapter 3 Cardiovascular system Cardiovascular investigations Plain films Evaluate heart size and chamber enlargement.
9/8/2009 < 1 1,2 3,4 5,6 7,8 9,10 11,12 13,14 15,16 17,18 > 18. Tetralogy of Fallot. Complex Congenital Heart Disease.
 Current Indications for Pediatric CTA S Bruce Greenberg Professor of Radiology Arkansas Children s Hospital University of Arkansas for Medical Sciences greenbergsbruce@uams.edu 45 40 35 30 25 20 15 10
Current Indications for Pediatric CTA S Bruce Greenberg Professor of Radiology Arkansas Children s Hospital University of Arkansas for Medical Sciences greenbergsbruce@uams.edu 45 40 35 30 25 20 15 10
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
LIVER INJURIES PROFF. S.FLORET
 LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
Acute Aortic Syndromes
 Acute Aortic Syndromes None Disclosures Smita Patel, M.B.B.S., M.R.C.P., F.R.C.R. Associate Professor, University of Michigan Ann Arbor, MI Objectives To review common CTA findings of acute aortic syndromes
Acute Aortic Syndromes None Disclosures Smita Patel, M.B.B.S., M.R.C.P., F.R.C.R. Associate Professor, University of Michigan Ann Arbor, MI Objectives To review common CTA findings of acute aortic syndromes
Aneurysms & a Brief Discussion on Embolism
 Aneurysms & a Brief Discussion on Embolism Aneurysms, overview = congenital or acquired dilations of blood vessels or the heart True aneurysms -involve all three layers of the artery (intima, media, and
Aneurysms & a Brief Discussion on Embolism Aneurysms, overview = congenital or acquired dilations of blood vessels or the heart True aneurysms -involve all three layers of the artery (intima, media, and