The Relentless Journey of TAVR to Lower-Risk Patients: Are We There Yet? Martin B. Leon, MD
|
|
|
- Phebe Davidson
- 5 years ago
- Views:
Transcription

1 The Relentless Journey of TAVR to Lower-Risk Patients: Are We There Yet? Martin B. Leon, MD 10 mins Columbia University Medical Center Cardiovascular Research Foundation New York City
 listed below.")
2 Disclosure Statement of Financial Interest TVT 2016, Chicago, IL; June 15-18, 2016 Martin B. Leon, MD Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement or affiliation with the organization(s) listed below. Affiliation / Financial Relationship Grant / Research Support / SAB Consulting Fees / Honoraria Shareholder / Equity Company Abbott, Boston Scientific, Edwards Lifescience, Medtronic None Claret, GDS, Mitralign, Valve Medical
3 TAVR Journey Global Demographics and Economics The Low-Risk Journey Proposing New Guidelines The Durability Controversy Mission Central = Next Steps to Further Enhance TAVR Value

4 TAVR Journey Global Demographics and Economics Over the next decade 4X growth in TAVR procedures predicted, associated with faster growth in the US, Japan, and ROW marked regional growth heterogeneity due to differing reimbursement patterns stabilization of trained operator sites continued under-diagnosis and undertreatment of AS

5 TAVR is Available in More Than 65 Countries Around the World >250,000 total implants to date

6 Estimated Global TAVR Procedure Growth SOURCE: Credit Suisse TAVI Comment January 8, ASP assumption for 2024 and 2025 based on analyst model. Revenue split assumption in 2025 is 45% U.S., 35% EU, 10% Japan, 10% ROW In the next 10 years, TAVR growth will increase X4!


7 Estimated Global TAVR Economic Growth SOURCE: Credit Suisse TAVI Comment January 8, ASP assumption for 2024 and 2025 based on analyst model. Revenue split assumption in 2025 is 45% U.S., 35% EU, 10% Japan, 10% ROW; Morgan Stanley Comment July 6,2015 In the next 10 years, TAVR economics will increase X4!

8 TAVR Underutilization is Largely Driven by Variation in Health Policy and Reimbursement 2015 Country TAVR Penetration Total TAVR Units / Millions of Inhabitants SOURCE: Eurostat, U.S. Census Bureau, Industry estimates 8



9 Estimated US and EU TAVR Sites 9
10 Medicare AV Cases in 2015 TAVR now accounts for 32% of all AV replacements SAVR Tissue SAVR Mech TF TAVR TA TAVR SOURCE: FY2015 MedPAR, all cases on file regardless of IPPS status
11 TAVR Journey Global Demographics and Economics Economic concerns due to high procedure costs have influenced TAVR growth and utilization cw surgery. Improved efficiencies of clinical care pathways after TAVR have reduced the differences and narrowed the gap.
12 Procedural efficiencies are reducing TAVR costs in the US Total index hospitalization cost* (TF TAVR) $76,063 $71,118 $64,772 $62,587 $59,893 $45,485 PARTNER Cohort B MedPAR 2013 MedPAR 2014 MedPAR 2015 MedPAR 1 2 Length of stay (TF TAVR) Emory optimized approach 10.1 days 8.1 days 7.9 days 7.1 days 6.4 days 3.0 days *Index hospitalization cost adjusted to reflect commercial device price Reynolds et al.,cost Effectiveness of Transcatheter Aortic Valve Replacement Compared with Standard Care. Circulation. 2012;125: Babaliaros et al., Comparison of a Minimalist Approach Transfemoral TAVR with Standard Approach Transfemoral TAVR. J Am Coll Cardiol. 2014;63(12_S)
13 TAVR Journey The Low-Risk Journey The relentless evolution of TAVR clinical growth has been driven by: the multi-disciplinary heart team commitment to evidence-based medicine rapid technology enhancement simplification of the procedure striking reduction in complications
14 The Low-Risk Journey My Favorite Drink = Double-shot Mocha Latte
15 The Low-Risk Journey STS database (141,905 pts) 6.2% 13.9% High risk (STS > 8%) Intermediate risk (STS 4-8%) 79.9% Low risk (STS <4%)
16 The Low-Risk Journey STS database (141,905 pts) 6.2% 13.9% 79.9% High risk (STS > 8%) Intermediate risk (STS 4-8%) Low risk (STS <4%) Since 2007, in the U.S., >15,000 patients have been enrolled in FDA studies (including 6 RCTs) with multiple generations of two TAVR systems!
17 The Low-Risk Journey STS database (141,905 pts) 6.2% 13.9% High risk (STS > 8%) Intermediate risk (STS 4-8%) PARTNER 1A, 1B CoreValve Extreme/High-Risk 79.9% Low risk (STS <4%)


18 PARTNER Manuscripts in NEJM (October, 2010 May, 2012)


19 CoreValve High-Risk U.S. Pivotal Trial (1 and 2-Yr Follow-up)


20 All-Cause Mortality ACC 2015 Δ = 6.5 Δ = % 28.6% 22.2% 14.1% Log-rank P=0.04 Months Post-Procedure
21 The Low-Risk Journey STS database (141,905 pts) 6.2% 13.9% High risk (STS > 8%) Intermediate risk (STS 4-8%) PARTNER 2A, S3i SURTAVI, UK TAVI 79.9% Low risk (STS <4%)

22 The PARTNER 2A and S3i Trial The NEJM and Lancet On-line
 79.")
23 The Low-Risk Journey STS database (141,905 pts) 6.2% High risk (STS > 8%) 13.9% Intermediate risk (STS 4-8%) 79.9% Low risk (STS <4%) NOTION All Comers, PARTNER 3 LR, CoreValve LR

24 All-cause Mortality MI, or Stroke (%) NOTION: Death (all-cause), Stroke or MI at 1 Year (as-treated) 20% SAVR TAVR P value (log rank) = % 15.7% 10% 11.9% 11.3% 5% 6.3% No. at risk: TAVR SAVR 0% Months Post-procedure
25 TAVR Journey The Low-Risk Journey Risk stratification for TAVR, especially based upon surgical risk scores, is imprecise, heavily biased, and mainly served a regulatory purpose to control clinical expansion of TAVR and to encourage a disciplined commitment to evidence-based risk-cohort studies!
26 ACC/AHA 2014 Risk Assessment (with MHT*) Combining STS Risk Estimate, Frailty, Major Organ System Dysfunction, and Procedure-Specific Impediments Low Risk (ALL criteria) Intermediate Risk (any 1) High Risk (any 1 criteria) Prohibitive Risk (any 1 criteria) STS PROM* <4% AND Frailty None AND 4% to 8% OR 1 index (mild) OR >8% OR 2 or more indices (moderate-severe) OR Predicted risk with surgery of death or major morbidity (allcause) >50% at 1 y OR Major organ system compromise not to be improved postop None AND 1 organ system OR No more than 2 organ systems OR 3 or more organ systems OR Procedure-specific impediment None Possible procedurespecific impediment Possible procedurespecific impediment Severe procedurespecific impediment * Multi-disciplinary Heart Team

27 The Low-Risk Journey Imagery of TAVR Risk Strata AS Patient Population Requiring Treatment


28 The Low-Risk Journey Imagery of TAVR Risk Strata AS Patient Population Requiring Treatment

29 The Low-Risk Journey Imagery of TAVR Risk Strata AS Patient Population Requiring Treatment

30 TAVR Risk Model from TVT Registry Development sample = 13,718 consecutive U.S. patients from 265 centers in the STS/ACC TVT registry undergoing TAVR from Nov 1, 2011 to Feb 28, Validation cohort 6,868 consecutive patients from March 1 to Oct 8, 2014 Covariates selected based on expert opinion and statistical analysis; relationship between in-hospital mortality and baseline covariates estimated by logistic egression; final predictors selected via stepwise variable selection JAMA Cardiol; March 9, 2016

31 TAVR Risk Model from TVT Registry Model Coefficients Development sample: mean age 82.1 yrs, 51.1% women and in-hospital mortality = 5.3% C statistic for discrimination = 0.67 (95% CI ) JAMA Cardiol; March 9, 2016
32 TAVR Journey The Low-Risk Journey Realization of TAVR (society guidelines and reimbursement) for essentially ALL patients (including low-risk) with AS requiring treatment, will still require completion of the low-risk RCTs meaningful TAVR risk scores management of valve durability issues
 Surgery (Bioprosthetic Valve) PARTNER 3 Registries Alternative Access (n=100) (TA/TAo/Subclavian) CT Imaging Sub-Study (n=200)")
 (n=100) Follow-up: 30 days, 6 mos, 1 year and annually")
33 The PARTNER 3 Trial Study Design Symptomatic Severe Calcific Aortic Stenosis Low Risk ASSESSMENT by Heart Team (STS < 4%, TF only) TF - TAVR (SAPIEN 3) 1:1 Randomization (n=1228) Surgery (Bioprosthetic Valve) PARTNER 3 Registries Alternative Access (n=100) (TA/TAo/Subclavian) CT Imaging Sub-Study (n=200) Actigraphy/QoL Sub-Study (n=100) CT Imaging Sub-Study (n=200) Actigraphy/QoL Sub-Study (n=100) Bicuspid Valves (n=100) PRIMARY ENDPOINT: Composite of all-cause mortality, all strokes, or re-hospitalization at 1 year post-procedure ViV (AV and MV) (n=100) Follow-up: 30 days, 6 mos, 1 year and annually through 10 years


34 MEDTRONIC TAVR IN LOW RISK PATIENTS TRIAL DESIGN & LEAFLET SUB-STUDY Patient Population: Low Risk Cohort Determined by Heart Team to be low surgical risk Primary Endpoint: Safety: Death, all stroke, life-threatening bleeding, major vascular complications, or AKI at 30 days Efficacy: Death or major stroke at 2 years Sample Size: ~1200 Subjects Follow-up Evaluations: 30-days, 6-month, 18-month, and 1 Through 5 years Number of Sites: Up to 80 sites 34
35 TAVR Journey Proposing New Guidelines The current TAVR guidelines (ESC and AHA/ACC) are already anachronistic and don t reflect clinical practice!
36 2014 ACC/AHA Valve Guidelines CHOICE of Intervention for AS Indication for AVR Heart Valve Team (I) Low-intermediate surgical risk High surgical risk Bridge to SAVR or TAVR for severe symptoms Prohibitive surgical risk Predicted post-tavr survival > 1 yr BAV (IIb) YES NO Surgical AVR (I) TAVR (IIa) TAVR (I) Palliative Care
37 TAVR Journey Proposing New Guidelines Therefore, until the guidelines are updated, we should consider introducing clinical guidelines to help the practicing TAVR community, based upon ALL available clinical trial evidence global trends and accepted clinical practices important secondary endpoints which better indicate the impact/value of TAVR

38 2014 ACC/AHA Valve Guidelines CLASSIFICATION of Recommendations
39 TAVR Clinical Use in 2016 (evidence + common sense) CLASS I Benefit >>> Risk SHOULD be performed Class Ia (of course!) Cannot have surgery (= inoperable, extreme risk, prohibitive risk) esp. technical reasons (e.g. hostile chest, chest RT, etc.) beware futility (e.g. wheelchair-bound, ultra-frail, extreme co-morbidities) Very high-risk for surgery e.g. severe COPD, chronic liver disease, dementia, severe PH
40 TAVR Clinical Use in 2016 (evidence + common sense) CLASS I Benefit >>> Risk SHOULD be performed Class Ib (enough already!) 90 years old All other high-risk patients Aortic valve-in-valve (high-risk) Special considerations low EF (esp. <30%) CKD on dialysis small annulus (esp. in women) low flow-low gradient AS
41 TAVR Clinical Use in 2016 (evidence + common sense) CLASS IIa Benefit >> Risk IT IS REASONABLE to perform Class IIa (strong preference!) Intermediate-risk patients (esp. TF) 80 years old Aortic valve-in-valve (normal risk) Severe asymptomatic AS (PV > 5 m/s) Concomitant disease previous CABG CKD not requiring dialysis CAD non-complex RH failure
42 TAVR Clinical Use in 2016 (evidence + common sense) CLASS IIb Benefit Risk MAY BE CONSIDERED to perform Class IIb (on the fence = need more evidence; proceed with caution) Low-risk patients (except as above)? bicuspid aortic valve disease < 65 years old (the durability issue) High anatomic risk for TAVR extreme calcification (esp. LVOT) and high risk of rupture or CA occlusion marked horizontal aorta
43 TAVR Clinical Use in 2016 (evidence + common sense) CLASS III No Benefit OR Harm SHOULD NOT be performed Class III (stay away!) Concomitant CV lesions requiring surgery (e.g. aortopathies, complex CAD, other valve lesions) Poor candidates for TAVR due to technical or anatomic reasons annulus size too small/large LV thrombus or endocarditis
44 TAVR Journey The Durability Controversy Until there is long-term (>10 years) reliable clinical and echo data on normal-risk patients treated with modern era transcatheter bioprosthetic valves, there will always be concerns regarding durability!


45 PARTNER 5-year FU in Lancet (March, 2015)
46 Mean Gradient (mmhg) Mean Gradient & Valve Area (AT) P1B - All Patients 70 EOA Mean Gradient Error bars = ± 1 Std Dev Valve Area (cm²) 0 N = Baseline 1 Year 2 Years 3 Years 4 Years 5 Years
47 TAVR Durability Issues
48 EuroPCR: Degenerated TAVR Not Uncommon by 10 Years May 17, 2016 by Nicole Lou MedPage EuroPCR 2016: Study casts doubt on long-term TAVR durability May 19, 2016 by Brad Perriello MASSDEVICE Should We Worry about TAVR Durability? Marie Thibault May 19, 2016 by Marie Thibault MDDI Early Transcatheter Aortic-Valve Device Durability Comes Under Scrutiny May 31, 2016 by Patrice Wendling Medscape
49 TAVR Durability Issues Some of the problems associated with this type of analysis 2 center experience, ultra-sick patients, earliest versions of the Sapien THV Incorrect statistical methods - THV degeneration is a time-dependent process, not a clinical event Competing risks of frequent deaths in these patients with multiple co-morbidities creates censoring problems Echo data are incomplete - ascertainment and interpretation, and definitions used were spurious - creates significant biases No. at risk after 5 years drops precipitously - tail shape unreliable Clinical SVD - freedom from re-intervention - never discussed



50 TAVR Durability Issues The Gold Standards CE Perimount Hancock II
51 Actuarial Freedom from SVD (%) Freedom from Structural Valve Deterioration of Pericardial Aortic Bioprostheses Actuarial Freedom from Structural Valve Deterioration Pericardial Aortic Bioprostheses EW SRN STJ EW SRN STJ EW SRN STJ Pelletier 1 Cosgrove* 2 Carrier 3 Murakami 4 Aupart 5 Aupart 6 Aupart 7 Gao* 8 Le Tourneau 9 39 Mazzucotelli 24 Alvarez 25 Minami 26 Sjögren 27 Jamieson 28 Banbury 10 Dellgren 11 Nakajima 12 Neville 13 Pellerin 14 Poirier 15 Frater 16 Banbury* 17 Jamieson 18 McClure 19 Biglioli* 20 Bergoënd 21 Aupart 22 5 Houel 29 Benhameid 30 Minami 31 ISTHMUS Investigators Year Results* 23 Yankah 33 Years Age NA All All All All All All All All All All All All All All NA All All All All All All All All All All 18 All 18 All 18 All 15 All All All 18 All NA NA All NA NA 10 Years 11 to 19 Years 20 Years * Freedom from explant / prosthesis replacement / reoperation due to SVD Methodology: Comprehensive literature searches were conducted utilizing a combination of key words. See references section for key words, filters, and a search results summary. Note: Patients and results are a subset of each study. See references section for total cohort size, patient mean age, and at risk population size.

52 TAVR Durability Issues Early Failures of Surgical Valves
53 Number of Cases Bioprosthetic Surgical Valve Failure from VIVD Registry Time to Failure - All VIVID Cases (n = 1304) 7-11 years Time to Failure (years)
54 Number of Cases Bioprosthetic Surgical Valve Failure from VIVD Registry Time to Failure - Sorin Mitroflow (n = 261) 6-9 years Time to Failure (Years)

55 TAVR Durability Issues General concepts
56 TAVR Journey The Durability Controversy Given the sensitivity of these long-term FU data, it s the responsibility of all TAVR investigators to carefully examine their late FU patients according to agreed-upon principles and definitions, including FDA studies like PARTNER, which will now extend clinical and echo FU to 10 years!

57 CHU Rouen 239 pts from (> 5 years FU) Freedom from either reoperation, or if asymp, echo mean valve gradient >40 mmhg or severe AR (effective ROA > 0.3cm 2 ) Among survivors, none with MG >40 and only 1 pt with severe AR resulting in ViV procedure
58 Vancouver 266 pts from before 2011 (> 5 years FU) Freedom from Severe Failure Freedom from Reintervention

59 Valve Leaflet Abnormalities Diastole Systole Makkar, et al. 2015
60 TAVR Journey The Durability Controversy An ancillary concern has been valve leaflet thickening/thrombosis - incidence and clinical implications - multiple ongoing 4D CTA studies (>2,000 pts) RESOLVE (400 pts, target = 1,000 pts) and SAVORY (120 pts) GALILEO Substudy (300 pts) PORTICO Substudy (200 pts), PARTNER 3 LR and Evolut LR studies (400 pts each)
61 TAVR Journey Mission Central = Next Steps to Further Enhance TAVR Value Continued expansion of clinical indications (test the outer limits)!
 TAVR UNLOAD Trial International Multicenter")
 Moderate AS R TAVR + OHFT OHFT Alone Follow-up: 1 month")


62 TAVR - UNLOAD Trial Design Moderate AS + HF (600 patients, 1:1 randomized) TAVR UNLOAD Trial International Multicenter Randomized Heart Failure LVEF < 50% NYHA 2 Optimal HF therapy (OHFT) Moderate AS R TAVR + OHFT OHFT Alone Follow-up: 1 month 6 months 1 year Clinical endpoints Symptoms Echo QoL Primary Endpoint Hierarchical occurrence of: All-cause death Disabling stroke Hospitalizations for HF, aortic valve disease Change in KCCQ Reduced AFTERLOAD Improved LV systolic and diastolic function
63 TAVR Journey Mission Central = Next Steps to Further Enhance TAVR Value Continued expansion of clinical indications (test the outer limits)! Continued reduction of TAVR-related complications (strokes, PVL, and PM)


 Primary")
64 SENTINEL Study Design (TAVR RCT) US Co-PIs: Samir Kapadia Susheel Kodali German Co-PI: Axel Linke Population: Subjects with severe AS with clinical indications for TAVR with the Edwards Sapien THV/XT/S3 or Medtronic CoreValve/Evolut-R N=296 subjects randomized 1:1:1 at sites in the U.S and Germany. SAFETY ARM TAVR with Sentinel TEST ARM TAVR with Sentinel RCT CONTROL ARM TAVR only Histopathology Safety Follow-up Safety Follow-up MRI Assessments Neurological and Neurocognitive Tests Primary (superiority) Efficacy Endpoint: Reduction in median total new lesion volume assessed by 3T DW-MR by baseline subtraction (3-7 days) Primary (non-inferiority) Safety Endpoint: Occurrence of all MACCE at 30 days
65 TAVR Journey Mission Central = Next Steps to Further Enhance TAVR Value Continued expansion of clinical indications (test the outer limits)! Continued reduction of TAVR-related complications (strokes, PVL, and PM) Elimination of trans-thoracic access in non-tf cases


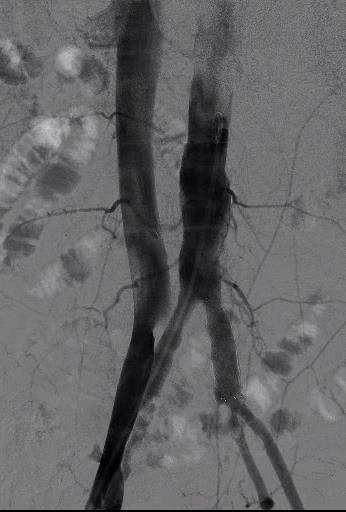



66 Trans-Caval Access for TAVR (202 pts in 28 centers - 5/14/16) guidewire to wire convertor microcatheter Electrosurgery pencil Back end of guidewire


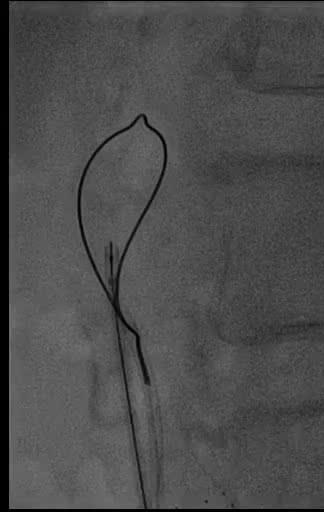
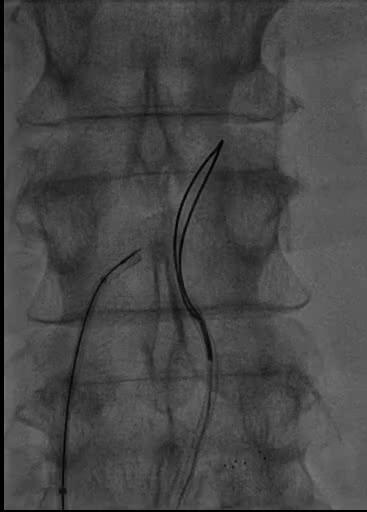
67 Direct Mediastinal Access for TAVR
68 TAVR Journey Mission Central = Next Steps to Further Enhance TAVR Value Continued expansion of clinical indications (test the outer limits)! Continued reduction of TAVR-related complications (strokes, PVL, and PM) Elimination of trans-thoracic access in non-tf cases Rational and properly studied adjunctive pharmacotherapy regimens

69 TAVR Adjunct Pharmacology Customized Patient-Based Therapy
70 Final Thoughts TAVR Journey Are We There Yet? The ultimate role of TAVR is yet to be determined. But we can foresee a future time when the use of TAVR (vs. surgery) will be a risk-benefit assessment based upon clinical and anatomic factors, and not an imprecise risk stratification model!

71 Outpatient Same-Day TAVR Sacre-Coeur Hospital; Montreal, CN Philippe Genereux Philippe Demers Donald Palisaitis
TAVR in 2020: What is Next!!!!
 TAVR in 2020: What is Next!!!! Vinod H. Thourani, MD Professor of Surgery Chairman, Department of Cardiac Surgery Medstar Heart and Vascular Institute Washington Hospital Center Washington, DC Disclosures
TAVR in 2020: What is Next!!!! Vinod H. Thourani, MD Professor of Surgery Chairman, Department of Cardiac Surgery Medstar Heart and Vascular Institute Washington Hospital Center Washington, DC Disclosures
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central
 TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
Severe Aortic Valve Disease: TAVR in Four Ages and Four Etiologies Age 25 y/o Congenital, 50 y/o Bicuspid, 75 y/o Rheumatic, 100 y/o Degenerative
 Severe Aortic Valve Disease: TAVR in Four Ages and Four Etiologies Age 25 y/o Congenital, 50 y/o Bicuspid, 75 y/o Rheumatic, 100 y/o Degenerative Samin K. Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Severe Aortic Valve Disease: TAVR in Four Ages and Four Etiologies Age 25 y/o Congenital, 50 y/o Bicuspid, 75 y/o Rheumatic, 100 y/o Degenerative Samin K. Sharma, MD, FACC, FSCAI Director Clinical & Interventional
TAVR 2015: A Breakthrough Technology GOES VIRAL! Issues and Controversies. Martin B. Leon, MD
 TAVR 2015: A Breakthrough Technology GOES VIRAL! Issues and Controversies Martin B. Leon, MD Columbia University Medical Center Cardiovascular Research Foundation New York City Disclosure Statement of
TAVR 2015: A Breakthrough Technology GOES VIRAL! Issues and Controversies Martin B. Leon, MD Columbia University Medical Center Cardiovascular Research Foundation New York City Disclosure Statement of
Le TAVI pour tout le monde?
 Le TAVI pour tout le monde? Thierry Lefèvre Institut Cardiovasculaire Paris Sud, Massy Disclosure Statement of Financial Interest I currently have, or have had over the last two years, an affiliation or
Le TAVI pour tout le monde? Thierry Lefèvre Institut Cardiovasculaire Paris Sud, Massy Disclosure Statement of Financial Interest I currently have, or have had over the last two years, an affiliation or
TAVR: Intermediate Risk Patients
 TAVR: Intermediate Risk Patients Oscar A. Mendiz.MD.FACC.FSCAI Director Cardiology & Cardiovascular Institute (ICyCC) Chief Interventional Cardiology Department Board of Directors Hospital & Favaloro University
TAVR: Intermediate Risk Patients Oscar A. Mendiz.MD.FACC.FSCAI Director Cardiology & Cardiovascular Institute (ICyCC) Chief Interventional Cardiology Department Board of Directors Hospital & Favaloro University
Igor Palacios, MD Director of Interventional Cardiology Massachusetts General Hospital Professor of Medicine Harvard Medical School
 Aortic Stenosis: Current State of Percutaneous Therapies, Emerging Technologies and Future Directions Igor Palacios, MD Director of Interventional Cardiology Massachusetts General Hospital Professor of
Aortic Stenosis: Current State of Percutaneous Therapies, Emerging Technologies and Future Directions Igor Palacios, MD Director of Interventional Cardiology Massachusetts General Hospital Professor of
Aortic Stenosis: Open vs TAVR vs Nothing
 Aortic Stenosis: Open vs TAVR vs Nothing Wilson Y. Szeto, MD Associate Professor of Surgery Surgical Director, Transcatheter Cardio-Aortic Therapies Associate Director, Thoracic Aortic Surgery Division
Aortic Stenosis: Open vs TAVR vs Nothing Wilson Y. Szeto, MD Associate Professor of Surgery Surgical Director, Transcatheter Cardio-Aortic Therapies Associate Director, Thoracic Aortic Surgery Division
The Future of Medicine. Who to TAVR? Azeem Latib MD EMO-GVM Centro Cuore Columbus and San Raffaele Scientific Institute, Milan, Italy
 The Future of Medicine Who to TAVR? Azeem Latib MD EMO-GVM Centro Cuore Columbus and San Raffaele Scientific Institute, Milan, Italy FIRST PATIENT TO UNDERGO PTCA FIRST PATIENT TO UNDERGO TAVI Grüntzig
The Future of Medicine Who to TAVR? Azeem Latib MD EMO-GVM Centro Cuore Columbus and San Raffaele Scientific Institute, Milan, Italy FIRST PATIENT TO UNDERGO PTCA FIRST PATIENT TO UNDERGO TAVI Grüntzig
Vinod H. Thourani, MD, FACC, FACS
 Considering SAVR in the TAVR era: Surgical Implications of TAVR Vinod H. Thourani, MD, FACC, FACS Professor of Cardiothoracic Surgery and Medicine Chief of Cardiothoracic Surgery, Emory Hospital Midtown
Considering SAVR in the TAVR era: Surgical Implications of TAVR Vinod H. Thourani, MD, FACC, FACS Professor of Cardiothoracic Surgery and Medicine Chief of Cardiothoracic Surgery, Emory Hospital Midtown
Update on TAVR. Howard C. Herrmann, MD, FACC, MSCAI
 Update on TAVR Howard C. Herrmann, MD, FACC, MSCAI John Bryfogle Professor of Cardiovascular Medicine and Surgery Health System Director for Interventional Cardiology Director, Cardiac Cath Labs, Hospital
Update on TAVR Howard C. Herrmann, MD, FACC, MSCAI John Bryfogle Professor of Cardiovascular Medicine and Surgery Health System Director for Interventional Cardiology Director, Cardiac Cath Labs, Hospital
TAVI limitations for low risk patients
 TAVI limitations for low risk patients Dr. T. Modine / P. Lancellotti MD, PhD, MBA CHRU de Lille, France Potential conflicts of interest Speaker's name: Thomas Modine I have the following potential conflicts
TAVI limitations for low risk patients Dr. T. Modine / P. Lancellotti MD, PhD, MBA CHRU de Lille, France Potential conflicts of interest Speaker's name: Thomas Modine I have the following potential conflicts
The TAVI Journey: Update on Evidence And Future trials
 The TAVI Journey: Update on Evidence And Future trials Philippe Généreux, MD Interventional Cardiologist, Hôpital du Sacré-Coeur de Montréal, Canada Director, Angiographic Core Laboratory, Cardiovascular
The TAVI Journey: Update on Evidence And Future trials Philippe Généreux, MD Interventional Cardiologist, Hôpital du Sacré-Coeur de Montréal, Canada Director, Angiographic Core Laboratory, Cardiovascular
2/15/2018 DISCLOSURES OBJECTIVES. Consultant for BioSense Webster, a J&J Co. Aortic stenosis background. Short history of TAVR
 TRANSCATHETER AORTIC VALVE REPLACEMENT IN 2018: IS IT NOW THE STANDARD OF CARE? 22 ND ANNUAL COASTAL CARDIAC & VASCULAR CONFERENCE FEBRUARY 17, 2018 R. David Anderson, MD, MS, FACC, FSCAI Professor of
TRANSCATHETER AORTIC VALVE REPLACEMENT IN 2018: IS IT NOW THE STANDARD OF CARE? 22 ND ANNUAL COASTAL CARDIAC & VASCULAR CONFERENCE FEBRUARY 17, 2018 R. David Anderson, MD, MS, FACC, FSCAI Professor of
Incorporating the intermediate risk in Transcatheter Aortic Valve Implantation (TAVI)
") Incorporating the intermediate risk in Transcatheter Aortic Valve Implantation (TAVI) Larry S. Dean, MD, MSCAI Past President SCAI Professor of Medicine and Surgery University of Washington School of Medicine
Incorporating the intermediate risk in Transcatheter Aortic Valve Implantation (TAVI) Larry S. Dean, MD, MSCAI Past President SCAI Professor of Medicine and Surgery University of Washington School of Medicine
Is TAVI ready for prime time in: - Intermediate risk patients? - Low risk patients?
 Is TAVI ready for prime time in: - Intermediate risk patients? - Low risk patients? Didier TCHETCHE, MD. Clinique PASTEUR, Toulouse, France, Conflicts of interest: -Consultant for Edwards LifeSciences
Is TAVI ready for prime time in: - Intermediate risk patients? - Low risk patients? Didier TCHETCHE, MD. Clinique PASTEUR, Toulouse, France, Conflicts of interest: -Consultant for Edwards LifeSciences
TAVR today: High Risk, Intermediate Risk Population, and Valve in Valve Therapy
 TAVR today: High Risk, Intermediate Risk Population, and Valve in Valve Therapy Alan Zajarias, MD FACC Structural Interventional Fellowship Director Associate Professor Medicine Cardiovascular Division
TAVR today: High Risk, Intermediate Risk Population, and Valve in Valve Therapy Alan Zajarias, MD FACC Structural Interventional Fellowship Director Associate Professor Medicine Cardiovascular Division
Appropriate Use of TAVR - now and in the future. A Surgeon s Perspective. Neil Moat Royal Brompton Hospital, London, UK
 Appropriate Use of TAVR - now and in the future A Surgeon s Perspective Neil Moat Royal Brompton Hospital, London, UK Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner
Appropriate Use of TAVR - now and in the future A Surgeon s Perspective Neil Moat Royal Brompton Hospital, London, UK Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner
After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients?
 After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients? Vinod H. Thourani, MD Professor of Surgery and Medicine Emory University Disclosure Statement of Financial
After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients? Vinod H. Thourani, MD Professor of Surgery and Medicine Emory University Disclosure Statement of Financial
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV?
 Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Transcatheter Aortic Valve Implantation. SSVQ November 23, 2012 Centre Mont-Royal 15:40
 Transcatheter Aortic Valve Implantation SSVQ November 23, 2012 Centre Mont-Royal 15:40 Nicolo Piazza MD, PhD, FRCPC, FESC, FACC McGill University Health Center German Heart Center Munich 1 First-in-Human
Transcatheter Aortic Valve Implantation SSVQ November 23, 2012 Centre Mont-Royal 15:40 Nicolo Piazza MD, PhD, FRCPC, FESC, FACC McGill University Health Center German Heart Center Munich 1 First-in-Human
A new option for the Diagnosis and Management of Valvular Heart Disease. Oregon Comprehensive Valve Center
 A new option for the Diagnosis and Management of Valvular Heart Disease Oregon Comprehensive Valve Center I have no disclosures Oregon Comprehensive Valve Center Weekly multidisciplinary case conferences
A new option for the Diagnosis and Management of Valvular Heart Disease Oregon Comprehensive Valve Center I have no disclosures Oregon Comprehensive Valve Center Weekly multidisciplinary case conferences
Neal Kleiman, MD Houston Methodist DeBakey Heart and Vascular Institute
 Neal Kleiman, MD Houston Methodist DeBakey Heart and Vascular Institute Despite a 33 fold growth in the first five years, there is still tremendous variability among penetration in different countries
Neal Kleiman, MD Houston Methodist DeBakey Heart and Vascular Institute Despite a 33 fold growth in the first five years, there is still tremendous variability among penetration in different countries
SAPIEN 3: Evaluation of a Balloon- Expandable Transcatheter Aortic Valve in High-Risk and Inoperable Patients With Aortic Stenosis One-Year Outcomes
 SAPIEN 3: Evaluation of a Balloon- Expandable Transcatheter Aortic Valve in High-Risk and Inoperable Patients With Aortic Stenosis One-Year Outcomes Howard C. Herrmann, MD on behalf of The PARTNER II Trial
SAPIEN 3: Evaluation of a Balloon- Expandable Transcatheter Aortic Valve in High-Risk and Inoperable Patients With Aortic Stenosis One-Year Outcomes Howard C. Herrmann, MD on behalf of The PARTNER II Trial
Debate: SAVR for Low-Risk Patients in 2017 is Obsolete AVR vs TAVI
 Debate: SAVR for Low-Risk Patients in 2017 is Obsolete AVR vs TAVI Joseph E. Bavaria, MD Roberts-Measey Professor of Surgery Vice Chair, Division of Cardiovascular Surgery University of Pennsylvania Immediate
Debate: SAVR for Low-Risk Patients in 2017 is Obsolete AVR vs TAVI Joseph E. Bavaria, MD Roberts-Measey Professor of Surgery Vice Chair, Division of Cardiovascular Surgery University of Pennsylvania Immediate
TAVI: The Real Deal? Marc Pelletier, MD Head, Department of Cardiac Surgery New Brunswick Heart Centre
 TAVI: The Real Deal? Marc Pelletier, MD Head, Department of Cardiac Surgery New Brunswick Heart Centre Disclosure St. Jude Medical: Consultant and Proctor Edwards Lifesciences: Proctor Medtronic: Research
TAVI: The Real Deal? Marc Pelletier, MD Head, Department of Cardiac Surgery New Brunswick Heart Centre Disclosure St. Jude Medical: Consultant and Proctor Edwards Lifesciences: Proctor Medtronic: Research
Transcatheter Aortic Valve Replacement with a Self-Expanding Prosthesis or Surgical Aortic Valve Replacement in Intermediate-Risk Patients:
 Transcatheter Aortic Valve Replacement with a Self-Expanding Prosthesis or Surgical Aortic Valve Replacement in Intermediate-Risk Patients: 1-Year Results from the SURTAVI Clinical Trial Nicolas M. Van
Transcatheter Aortic Valve Replacement with a Self-Expanding Prosthesis or Surgical Aortic Valve Replacement in Intermediate-Risk Patients: 1-Year Results from the SURTAVI Clinical Trial Nicolas M. Van
TAVR for Complex Aortic Valvular Conditions
 TAVR for Complex Aortic Valvular Conditions Wilson Y. Szeto, MD Professor of Surgery Chief, Cardiovascular Surgery at Penn Presbyterian Surgical Director, Transcatheter Cardio-Aortic Therapies Associate
TAVR for Complex Aortic Valvular Conditions Wilson Y. Szeto, MD Professor of Surgery Chief, Cardiovascular Surgery at Penn Presbyterian Surgical Director, Transcatheter Cardio-Aortic Therapies Associate
TAVR IN INTERMEDIATE-RISK PATIENTS
 TAVR IN INTERMEDIATE-RISK PATIENTS K. Lampropoulos MD, PhD, FESC, MEAPCI Interventional Cardiologist Evangelismos General Hospital The Burden of Valve Disease Prevalence Survival NATURAL HISTORY OF AS
TAVR IN INTERMEDIATE-RISK PATIENTS K. Lampropoulos MD, PhD, FESC, MEAPCI Interventional Cardiologist Evangelismos General Hospital The Burden of Valve Disease Prevalence Survival NATURAL HISTORY OF AS
TAVR: Review of the Robust Data from Randomized Trials
 TAVR: Review of the Robust Data from Randomized Trials Nicholas J. Ruggiero II, MD,FACP, FACC, FSCAI, FSVM, FCPP Director, Structural Heart Disease and Non-Coronary Interventions Director, Jefferson Heart
TAVR: Review of the Robust Data from Randomized Trials Nicholas J. Ruggiero II, MD,FACP, FACC, FSCAI, FSVM, FCPP Director, Structural Heart Disease and Non-Coronary Interventions Director, Jefferson Heart
TAVR in Intermediate Risk Populations /Optimizing Systems for TAVR
 TAVR in Intermediate Risk Populations /Optimizing Systems for TAVR Saibal Kar, MD, FACC, FAHA, FSCAI Professor of Medicine Director of Interventional Cardiac Research Smidt Heart Institute, Cedars-Sinai
TAVR in Intermediate Risk Populations /Optimizing Systems for TAVR Saibal Kar, MD, FACC, FAHA, FSCAI Professor of Medicine Director of Interventional Cardiac Research Smidt Heart Institute, Cedars-Sinai
Transcatheter Aortic Valve Replacement
 Transcatheter Aortic Valve Replacement Jesse Jorgensen, MD Medical Director, Cardiac Catheterization Laboratory Greenville Health System Greenville, South Carolina, USA January 30, 2016 Aortic Stenosis
Transcatheter Aortic Valve Replacement Jesse Jorgensen, MD Medical Director, Cardiac Catheterization Laboratory Greenville Health System Greenville, South Carolina, USA January 30, 2016 Aortic Stenosis
Five-Year Outcomes of Transcatheter Aortic Valve Replacement (TAVR) in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial
 in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial") Five-Year Outcomes of Transcatheter Aortic Valve Replacement (TAVR) in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial Samir R. Kapadia, MD On behalf of The PARTNER Trial Investigators
Five-Year Outcomes of Transcatheter Aortic Valve Replacement (TAVR) in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial Samir R. Kapadia, MD On behalf of The PARTNER Trial Investigators
Evolving and Expanding Indications for TAVR
 Evolving and Expanding Indications for TAVR Wilson Y. Szeto, MD Associate Professor of Surgery Surgical Director, Transcatheter Cardio-Aortic Therapies Associate Director, Thoracic Aortic Surgery Division
Evolving and Expanding Indications for TAVR Wilson Y. Szeto, MD Associate Professor of Surgery Surgical Director, Transcatheter Cardio-Aortic Therapies Associate Director, Thoracic Aortic Surgery Division
1-YEAR OUTCOMES FROM JOHN WEBB, MD
 1-YEAR OUTCOMES FROM JOHN WEBB, MD ON BEHALF OF THE SAPIEN 3 INVESTIGATORS UNIVERSITY OF BRITISH COLUMBIA VANCOUVER, CANADA Potential conflicts of interest Speaker's name: John Webb I have the following
1-YEAR OUTCOMES FROM JOHN WEBB, MD ON BEHALF OF THE SAPIEN 3 INVESTIGATORS UNIVERSITY OF BRITISH COLUMBIA VANCOUVER, CANADA Potential conflicts of interest Speaker's name: John Webb I have the following
Extension to medium and low risk patients? Friedrich Eckstein University Hospital Basel
 TAVI CON Extension to medium and low risk patients? Friedrich Eckstein University Hospital Basel Extension to medium and low risk patients? In octogenerians already reality in most of the swiss clinics!?
TAVI CON Extension to medium and low risk patients? Friedrich Eckstein University Hospital Basel Extension to medium and low risk patients? In octogenerians already reality in most of the swiss clinics!?
TAVR 2018: TAVR has high clinical efficacy according to baseline patient risk! ii. Con
 TAVR 2018: TAVR has high clinical efficacy according to baseline patient risk! ii. Con Dimitrios C. Angouras, MD, FETCS Associate Professor of Cardiac Surgery National and Kapodistrian University of Athens,
TAVR 2018: TAVR has high clinical efficacy according to baseline patient risk! ii. Con Dimitrios C. Angouras, MD, FETCS Associate Professor of Cardiac Surgery National and Kapodistrian University of Athens,
Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data
 Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data Echo Florida 2013 Jonathan J. Passeri, M.D. Co-Director, Heart Valve Program Director,
Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data Echo Florida 2013 Jonathan J. Passeri, M.D. Co-Director, Heart Valve Program Director,
Indication, Timing, Assessment and Update on TAVI
 Indication, Timing, Assessment and Update on TAVI Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Starr- Edwards Mechanical
Indication, Timing, Assessment and Update on TAVI Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Starr- Edwards Mechanical
LOW RISK TAVR. WHAT THE FUTURE HOLDS
 LOW RISK TAVR. WHAT THE FUTURE HOLDS Michael J. Reardon, M.D. Professor of Cardiothoracic Surgery Allison Family Distinguish Chair of Cardiovascular Research Houston Methodist DeBakey Heart & Vascular
LOW RISK TAVR. WHAT THE FUTURE HOLDS Michael J. Reardon, M.D. Professor of Cardiothoracic Surgery Allison Family Distinguish Chair of Cardiovascular Research Houston Methodist DeBakey Heart & Vascular
Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis
 Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis George L. Zorn, III On Behalf of the CoreValve US Clinical Investigators
Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis George L. Zorn, III On Behalf of the CoreValve US Clinical Investigators
Is TAVR Now Indicated in Even Low Risk Aortic Valve Disease Patients
 Is TAVR Now Indicated in Even Low Risk Aortic Valve Disease Patients Saibal Kar, MD, FACC, FAHA, FSCAI Director of Interventional Cardiac Research Cedars Sinai Heart Institute, Los Angeles, CA Potential
Is TAVR Now Indicated in Even Low Risk Aortic Valve Disease Patients Saibal Kar, MD, FACC, FAHA, FSCAI Director of Interventional Cardiac Research Cedars Sinai Heart Institute, Los Angeles, CA Potential
Disclosures 4/16/2018. What s New in Valvularand Structural Heart Disease. None relevant to the presentation
 What s New in Valvularand Structural Heart Disease Ryan C. Shelstad, MD Surgical Enthusiast, Valvular and Structural Heart Disease Bryan Heart Cardiothoracic Surgery Disclosures None relevant to the presentation
What s New in Valvularand Structural Heart Disease Ryan C. Shelstad, MD Surgical Enthusiast, Valvular and Structural Heart Disease Bryan Heart Cardiothoracic Surgery Disclosures None relevant to the presentation
CIPG Transcatheter Aortic Valve Replacement- When Is Less, More?
 CIPG 2013 Transcatheter Aortic Valve Replacement- When Is Less, More? James D. Rossen, M.D. Professor of Medicine and Neurosurgery Director, Cardiac Catheterization Laboratory and Interventional Cardiology
CIPG 2013 Transcatheter Aortic Valve Replacement- When Is Less, More? James D. Rossen, M.D. Professor of Medicine and Neurosurgery Director, Cardiac Catheterization Laboratory and Interventional Cardiology
The Role of TAVI in high-risk and normal-risk Patients
 The Role of TAVI in high-risk and normal-risk Patients Joachim Schofer Hamburg University Cardiovascular Center and Department for percutaneous treatment of structural heart disease Albertinen Heart Center
The Role of TAVI in high-risk and normal-risk Patients Joachim Schofer Hamburg University Cardiovascular Center and Department for percutaneous treatment of structural heart disease Albertinen Heart Center
Transcatheter Heart Valve Therapy
 Edwards Lifesciences 2017 Investor Conference Transcatheter Heart Valve Therapy Larry L. Wood Corporate Vice President, Transcatheter Heart Valves Leader in ~$3B Global Transcatheter Heart Valves Primary
Edwards Lifesciences 2017 Investor Conference Transcatheter Heart Valve Therapy Larry L. Wood Corporate Vice President, Transcatheter Heart Valves Leader in ~$3B Global Transcatheter Heart Valves Primary
Update on Percutaneous Therapies for Structural Heart Disease. William Thomas MD Director of Structural Heart Program Tucson Medical Center
 Update on Percutaneous Therapies for Structural Heart Disease William Thomas MD Director of Structural Heart Program Tucson Medical Center NCVH 2014- Tucson Disclosure of Financial Interest Research: Stock
Update on Percutaneous Therapies for Structural Heart Disease William Thomas MD Director of Structural Heart Program Tucson Medical Center NCVH 2014- Tucson Disclosure of Financial Interest Research: Stock
Aortic Stenosis: Background
 Transcatheter Aortic Valve Replacement in Low Surgical Risk Patients Barry George, MD The Ohio State University Structural Heart Disease Course May 19 th, 2017 Aortic Stenosis: Background Severe Symptomatic
Transcatheter Aortic Valve Replacement in Low Surgical Risk Patients Barry George, MD The Ohio State University Structural Heart Disease Course May 19 th, 2017 Aortic Stenosis: Background Severe Symptomatic
The Sentinel Dual Filter Device Design Features & EU Clinical Trial Results
 The Sentinel Dual Filter Device Design Features & EU Clinical Trial Results Nicolas M. Van Mieghem, MD, PhD, FESC Director of Interventional Cardiology Thoraxcenter, Erasmus MC Rotterdam Disclosure Statement
The Sentinel Dual Filter Device Design Features & EU Clinical Trial Results Nicolas M. Van Mieghem, MD, PhD, FESC Director of Interventional Cardiology Thoraxcenter, Erasmus MC Rotterdam Disclosure Statement
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair?
 TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
Neuroprotection During TAVR
 Neuroprotection During TAVR Samir Kapadia, MD Professor of Medicine Section head, Interventional Cardiology Director, Cardiac Catheterization Laboratories Cleveland Clinic Cleveland Clinic Disclosure Co
Neuroprotection During TAVR Samir Kapadia, MD Professor of Medicine Section head, Interventional Cardiology Director, Cardiac Catheterization Laboratories Cleveland Clinic Cleveland Clinic Disclosure Co
Valvular Intervention
 Valvular Intervention Outline Introduction Aortic Stenosis Mitral Regurgitation Conclusion Calcific Aortic Stenosis Deformed Eccentric Calcified Nodular Rigid HOSTILE TARGET difficult to displace prone
Valvular Intervention Outline Introduction Aortic Stenosis Mitral Regurgitation Conclusion Calcific Aortic Stenosis Deformed Eccentric Calcified Nodular Rigid HOSTILE TARGET difficult to displace prone
Transcatheter Aortic Valve Replacement. Larry L. Wood Corporate Vice President
 Transcatheter Aortic Valve Replacement Larry L. Wood Corporate Vice President Leader in ~$3.5B Global Transcatheter Aortic Valve Replacement Market Primary global growth drivers: indication expansion,
Transcatheter Aortic Valve Replacement Larry L. Wood Corporate Vice President Leader in ~$3.5B Global Transcatheter Aortic Valve Replacement Market Primary global growth drivers: indication expansion,
Current Evidence in TAVI patients using ACURATE and LOTUS valves
 Current Evidence in TAVI patients using ACURATE and LOTUS valves Giuseppe Tarantini, MD, PhD, FESC, Professor and Director of Interventional Cardiology University of Padua GISE President Potential conflicts
Current Evidence in TAVI patients using ACURATE and LOTUS valves Giuseppe Tarantini, MD, PhD, FESC, Professor and Director of Interventional Cardiology University of Padua GISE President Potential conflicts
TAVI After PARTNER-2 : The Hamilton Approach
 TAVI After PARTNER-2 : The Hamilton Approach James L. Velianou MD FRCPC Interventional Cardiology Hamilton General Hospital St Catharines General Hospital Associate Professor of Medicine McMaster University
TAVI After PARTNER-2 : The Hamilton Approach James L. Velianou MD FRCPC Interventional Cardiology Hamilton General Hospital St Catharines General Hospital Associate Professor of Medicine McMaster University
L evoluzione nel management della valvulopatia aortica
 L evoluzione nel management della valvulopatia aortica Giuseppe Tarantini, MD, PhD, FESC Director of Interventional Cardiology University of Padua GISE president TAVI: BIG BANG 2002 TAVI - EVOLUTIONs Commitment
L evoluzione nel management della valvulopatia aortica Giuseppe Tarantini, MD, PhD, FESC Director of Interventional Cardiology University of Padua GISE president TAVI: BIG BANG 2002 TAVI - EVOLUTIONs Commitment
Should We Reconsider using Anticoagulation for Biological Tissue Valves
 Should We Reconsider using Anticoagulation for Biological Tissue Valves No Disclosures Disclosures Watching grass grow Complete with audio 1 hour 8 minutes 9884 views Subclinical Leaflet Thrombosis in
Should We Reconsider using Anticoagulation for Biological Tissue Valves No Disclosures Disclosures Watching grass grow Complete with audio 1 hour 8 minutes 9884 views Subclinical Leaflet Thrombosis in
Is Stroke Frequency Declining?
 Is Stroke Frequency Declining? Etiologic Factors Clinical, Anatomic, Technique-related, and Device-specific Samir Kapadia, MD Professor of Medicine Section head, Interventional Cardiology Director, Cardiac
Is Stroke Frequency Declining? Etiologic Factors Clinical, Anatomic, Technique-related, and Device-specific Samir Kapadia, MD Professor of Medicine Section head, Interventional Cardiology Director, Cardiac
TAVR in 2017 What we know? What to expect?
 Journal of Geriatric Cardiology (2018) 15: 55 60 2018 JGC All rights reserved; www.jgc301.com Perspective Open Access TAVR in 2017 What we know? What to expect? Panagiota Kourkoveli 1,*, Konstantinos Spargias
Journal of Geriatric Cardiology (2018) 15: 55 60 2018 JGC All rights reserved; www.jgc301.com Perspective Open Access TAVR in 2017 What we know? What to expect? Panagiota Kourkoveli 1,*, Konstantinos Spargias
Clinical and Echocardiographic Outcomes at 30 Days with the SAPIEN 3 TAVR System in Inoperable, High-Risk and Intermediate-Risk AS Patients
 Clinical and Echocardiographic Outcomes at 30 Days with the SAPIEN 3 TAVR System in Inoperable, High-Risk and Intermediate-Risk AS Patients Susheel Kodali, MD on behalf of The PARTNER Trial Investigators
Clinical and Echocardiographic Outcomes at 30 Days with the SAPIEN 3 TAVR System in Inoperable, High-Risk and Intermediate-Risk AS Patients Susheel Kodali, MD on behalf of The PARTNER Trial Investigators
Aortic Stenosis Background and Breakthroughs in Treatment: TAVR Update
 Aortic Stenosis Background and Breakthroughs in Treatment: TAVR Update Howard J Broder MD Interventional Cardiology DaVita Medical Group/ Healthcare Partners Cardiology Disclosures for Howard J Broder
Aortic Stenosis Background and Breakthroughs in Treatment: TAVR Update Howard J Broder MD Interventional Cardiology DaVita Medical Group/ Healthcare Partners Cardiology Disclosures for Howard J Broder
Edwards Sapien. Medtronic CoreValve. Inoperable FDA approved High risk: in trials. FDA approved
 Transcatheter Aortic Valve Replacement Symptomatic Aortic Stenosis Asymptomatic Juan Crestanello, MD Interim Director, Division of Cardiac Surgery Associate Professor Division of Cardiac Surgery The Ohio
Transcatheter Aortic Valve Replacement Symptomatic Aortic Stenosis Asymptomatic Juan Crestanello, MD Interim Director, Division of Cardiac Surgery Associate Professor Division of Cardiac Surgery The Ohio
Subclinical Thrombosis of Bioprosthetic Aortic Valves: Is It Clinically Relevant? Tarun Chakravarty, MD
 Subclinical Thrombosis of Bioprosthetic Aortic Valves: Is It Clinically Relevant? Tarun Chakravarty, MD Interventional Cardiology Cedars-Sinai Heart Institute Disclosures Consultant and proctor for Edwards
Subclinical Thrombosis of Bioprosthetic Aortic Valves: Is It Clinically Relevant? Tarun Chakravarty, MD Interventional Cardiology Cedars-Sinai Heart Institute Disclosures Consultant and proctor for Edwards
Transcatheter Aortic Valve Replacement TAVR
 Transcatheter Aortic Valve Replacement TAVR Paul Gordon, MD Associate Prof of Medicine, Brown University Director, Cardiac Catheterization Laboratory The Miriam Hospital Disclosures: none 100 Symptomatic
Transcatheter Aortic Valve Replacement TAVR Paul Gordon, MD Associate Prof of Medicine, Brown University Director, Cardiac Catheterization Laboratory The Miriam Hospital Disclosures: none 100 Symptomatic
RANDOMISED TRIALS TAVI WITH SAVR STEPHAN WINDECKER AORTIC VALVE DISEASE COMPARING
 AORTIC VALVE DISEASE RANDOMISED TRIALS COMPARING TAVI WITH SAVR STEPHAN WINDECKER DEPARTMENT OF CARDIOLOGY SWISS CARDIOVASCULAR CENTER AND CLINICAL TRIALS UNIT BERN BERN UNIVERSITY HOSPITAL, SWITZERLAND
AORTIC VALVE DISEASE RANDOMISED TRIALS COMPARING TAVI WITH SAVR STEPHAN WINDECKER DEPARTMENT OF CARDIOLOGY SWISS CARDIOVASCULAR CENTER AND CLINICAL TRIALS UNIT BERN BERN UNIVERSITY HOSPITAL, SWITZERLAND
State of the Art and Future perspective
 State of the Art and Future perspective Giuseppe Tarantini, MD, PhD, FESC Associate professor University of Padua Director Interventional Cardiology Dpt of Cardiac Thoracic and Vascular Sciences, Padua
State of the Art and Future perspective Giuseppe Tarantini, MD, PhD, FESC Associate professor University of Padua Director Interventional Cardiology Dpt of Cardiac Thoracic and Vascular Sciences, Padua
Assessment and Preparation of Patients with TAVI. Rob Tanzola Associate Professor, Queen s University
 Assessment and Preparation of Patients with TAVI Rob Tanzola Associate Professor, Queen s University My patient has aortic stenosis and needs non-cardiac surgery Should (s)he get a TAVI? Rob Tanzola Associate
Assessment and Preparation of Patients with TAVI Rob Tanzola Associate Professor, Queen s University My patient has aortic stenosis and needs non-cardiac surgery Should (s)he get a TAVI? Rob Tanzola Associate
TAVI and TAVR: Radical and Revolutionary: The Newest Insights for the CV Community and a Panel Discussion
 TAVI and TAVR: Radical and Revolutionary: The Newest Insights for the CV Community and a Panel Discussion Moderator: Joseph E. Bavaria, MD Roberts-Measey Professor of Surgery Vice Chair, Division of Cardiovascular
TAVI and TAVR: Radical and Revolutionary: The Newest Insights for the CV Community and a Panel Discussion Moderator: Joseph E. Bavaria, MD Roberts-Measey Professor of Surgery Vice Chair, Division of Cardiovascular
When Should We Consider TAVI. (Surgeon s Viewpoint)? Pyowon Park Samsung Medical Center Seoul, Korea
? Pyowon Park Samsung Medical Center Seoul, Korea") When Should We Consider TAVI Procedure in Korea (Surgeon s Viewpoint)? Pyowon Park Samsung Medical Center Seoul, Korea Aortic Stenosis in Korea Rapidly increasing valve disease in Korea Still low incidence
When Should We Consider TAVI Procedure in Korea (Surgeon s Viewpoint)? Pyowon Park Samsung Medical Center Seoul, Korea Aortic Stenosis in Korea Rapidly increasing valve disease in Korea Still low incidence
TAVI: Nouveaux Horizons
 TAVI: Nouveaux Horizons EUAPI580i 432HQ14NP02353 Institut de Cardiologie de la Pitié-Salpêtrière jean-philippe.collet@psl.aphp.fr www.action-coeur.org Objectifs Les recommandations Le TAVI en chiffre La
TAVI: Nouveaux Horizons EUAPI580i 432HQ14NP02353 Institut de Cardiologie de la Pitié-Salpêtrière jean-philippe.collet@psl.aphp.fr www.action-coeur.org Objectifs Les recommandations Le TAVI en chiffre La
Alec Vahanian,FESC, FRCP (Edin.) Bichat Hospital University Paris VII, Paris, France
 Bichat Hospital University Paris VII, Paris, France") Future Percutaneous Therapies for Mitral Valve Disease (Mitraclip,percutaneous annuloplasty and transcatheter valve implantation) Will they reach the TAVI s success? Alec Vahanian,FESC, FRCP (Edin.) Bichat
Future Percutaneous Therapies for Mitral Valve Disease (Mitraclip,percutaneous annuloplasty and transcatheter valve implantation) Will they reach the TAVI s success? Alec Vahanian,FESC, FRCP (Edin.) Bichat
Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat
 Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat Innovative Procedures, Devices & State of the Art Care for Arrhythmias, Heart Failure & Structural Heart Disease October 8-10,
Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat Innovative Procedures, Devices & State of the Art Care for Arrhythmias, Heart Failure & Structural Heart Disease October 8-10,
Mechanical vs. Bioprosthetic Aortic Valve Replacement: Time to Reconsider? Christian Shults, MD Cardiac Surgeon, Medstar Heart and Vascular Institute
 Mechanical vs. Bioprosthetic Aortic Valve Replacement: Time to Reconsider? Christian Shults, MD Cardiac Surgeon, Medstar Heart and Vascular Institute Assistant Professor, Georgetown School of Medicine
Mechanical vs. Bioprosthetic Aortic Valve Replacement: Time to Reconsider? Christian Shults, MD Cardiac Surgeon, Medstar Heart and Vascular Institute Assistant Professor, Georgetown School of Medicine
Transcatheter Aortic Valve Implantation (TAVI) Overview for Wales. Dr Richard Anderson University Hospital of Wales, Cardiff, UK
 Overview for Wales. Dr Richard Anderson University Hospital of Wales, Cardiff, UK") Transcatheter Aortic Valve Implantation (TAVI) Overview for Wales Dr Richard Anderson University Hospital of Wales, Cardiff, UK Aortic stenosis is a disease of old age Age demographics in Wales % Wales
Transcatheter Aortic Valve Implantation (TAVI) Overview for Wales Dr Richard Anderson University Hospital of Wales, Cardiff, UK Aortic stenosis is a disease of old age Age demographics in Wales % Wales
Measuring the risk in valve patients Lessons learnt from the TAVI story? Bernard Iung Bichat Hospital, Paris, France
 Measuring the risk in valve patients Lessons learnt from the TAVI story? Bernard Iung Bichat Hospital, Paris, France Faculty disclosure Bernard Iung I disclose the following financial relationships: Consultant
Measuring the risk in valve patients Lessons learnt from the TAVI story? Bernard Iung Bichat Hospital, Paris, France Faculty disclosure Bernard Iung I disclose the following financial relationships: Consultant
10 mins. Martin B. Leon, MD. Columbia University Medical Center Cardiovascular Research Foundation New York City
 10 mins Martin B. Leon, MD Columbia University Medical Center Cardiovascular Research Foundation New York City Tuesday, November 1, 2016 Disclosure Statement of Financial Interest TCT 2016 Washington,
10 mins Martin B. Leon, MD Columbia University Medical Center Cardiovascular Research Foundation New York City Tuesday, November 1, 2016 Disclosure Statement of Financial Interest TCT 2016 Washington,
The Case for and Against Cerebral Embolic Protection During TAVR. Susheel Kodali, MD
 The Case for and Against Cerebral Embolic Protection During TAVR Susheel Kodali, MD Director, Structural Heart & Valve Center Columbia University Medical Center New York Presbyterian Hospital Disclosure
The Case for and Against Cerebral Embolic Protection During TAVR Susheel Kodali, MD Director, Structural Heart & Valve Center Columbia University Medical Center New York Presbyterian Hospital Disclosure
Percutaneous Treatment of Valvular Heart Diseases: Lessons and Perspectives. Bernard Iung Bichat Hospital, Paris
 Percutaneous Treatment of Valvular Heart Diseases: Lessons and Perspectives Bernard Iung Bichat Hospital, Paris Euro Heart Survey on Valvular Diseases 3547 Patients with Native Valve Disease n= 1250 1000
Percutaneous Treatment of Valvular Heart Diseases: Lessons and Perspectives Bernard Iung Bichat Hospital, Paris Euro Heart Survey on Valvular Diseases 3547 Patients with Native Valve Disease n= 1250 1000
Transcatheter Valve Replacement: Current State in 2017
 Transcatheter Valve Replacement: Current State in 2017 Marc A. Sintek MD Assistant Professor of Medicine Interventional Cardiology Cardiovascular Division Washington University in St. Louis Missouri ACP
Transcatheter Valve Replacement: Current State in 2017 Marc A. Sintek MD Assistant Professor of Medicine Interventional Cardiology Cardiovascular Division Washington University in St. Louis Missouri ACP
Strokes After TAVR Reasons for Declining Frequency
 Strokes After TAVR Reasons for Declining Frequency Samir Kapadia, MD Professor of Medicine Director, Cardiac Catheterization Laboratory Cleveland Clinic Disclosure NONE Second Generation Valves Newer
Strokes After TAVR Reasons for Declining Frequency Samir Kapadia, MD Professor of Medicine Director, Cardiac Catheterization Laboratory Cleveland Clinic Disclosure NONE Second Generation Valves Newer
Lotus Valve System for Transcatheter Aortic Valve Implantation/Replacement (TAVI/R) Evidence
 Evidence") X Congreso Coilegio Colombiano Santiago de Cali, 29-31 Octubre des 2014 Lotus Valve System for Transcatheter Aortic Valve Implantation/Replacement (TAVI/R) Evidence Eberhard Grube MD, FACC, FSCAI University
X Congreso Coilegio Colombiano Santiago de Cali, 29-31 Octubre des 2014 Lotus Valve System for Transcatheter Aortic Valve Implantation/Replacement (TAVI/R) Evidence Eberhard Grube MD, FACC, FSCAI University
Stainless Steel. Cobalt-chromium
 Sapien is better than Corevalve! Raj R. Makkar, MD Associate Director, Cedars-Sinai Heart Institute Associate Professor, UCLA School of Medicine, Los Angeles Eberhard Grube: Pioneer in the field of TAVR
Sapien is better than Corevalve! Raj R. Makkar, MD Associate Director, Cedars-Sinai Heart Institute Associate Professor, UCLA School of Medicine, Los Angeles Eberhard Grube: Pioneer in the field of TAVR
Valvular Heart Disease Transcatheter Valve Therapies. October 2016 Brian Whisenant MD
 Valvular Heart Disease Transcatheter Valve Therapies October 2016 Brian Whisenant MD Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement
Valvular Heart Disease Transcatheter Valve Therapies October 2016 Brian Whisenant MD Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement
Potential conflicts of interest
 Potential conflicts of interest Speaker's name: Petros Dardas MEDTRONIC proctor for TAVI Intermediate risk 83 FEMALE COAD SEVERE AS NYHA III Mean gradient 35 mmhg, AVA 0.45cm2, SVI 21ml/m2 Paradoxical
Potential conflicts of interest Speaker's name: Petros Dardas MEDTRONIC proctor for TAVI Intermediate risk 83 FEMALE COAD SEVERE AS NYHA III Mean gradient 35 mmhg, AVA 0.45cm2, SVI 21ml/m2 Paradoxical
An Update on the Edwards TAVR Results. Zvonimir Krajcer, MD Director, Peripheral Intervention Texas Heart Institute at St.
 An Update on the Edwards TAVR Results Zvonimir Krajcer, MD Director, Peripheral Intervention Texas Heart Institute at St. Luke s Hospital Disclosures On the speaker s bureau for Endologix, TriVascular,
An Update on the Edwards TAVR Results Zvonimir Krajcer, MD Director, Peripheral Intervention Texas Heart Institute at St. Luke s Hospital Disclosures On the speaker s bureau for Endologix, TriVascular,
Current Controversies. Subclinical and clinical valve thrombosis
 Chapter 19: Current controversies, ongoing trials, new valves, and future directions Sukhdeep S. Basra, MD, MPH, Michael J. Mack, MD The Heart Hospital Baylor Plano, Texas Transcatheter Aortic Valve Replacement
Chapter 19: Current controversies, ongoing trials, new valves, and future directions Sukhdeep S. Basra, MD, MPH, Michael J. Mack, MD The Heart Hospital Baylor Plano, Texas Transcatheter Aortic Valve Replacement
Sentinel Dual Filter Device: Technology Overview and Status of the CLEAN-TAVI Randomized Trial. Martin B. Leon, MD
 8 mins Sentinel Dual Filter Device: Technology Overview and Status of the CLEAN-TAVI Randomized Trial Martin B. Leon, MD Columbia University Medical Center Cardiovascular Research Foundation New York City
8 mins Sentinel Dual Filter Device: Technology Overview and Status of the CLEAN-TAVI Randomized Trial Martin B. Leon, MD Columbia University Medical Center Cardiovascular Research Foundation New York City
Transcatheter Therapies For Aortic Valve Disease. March 2017 Brian Whisenant MD
 Transcatheter Therapies For Aortic Valve Disease March 2017 Brian Whisenant MD Introduction I got into this field to protect my turf. I must say, I have come full circle... - Kent W. Jones I got into this
Transcatheter Therapies For Aortic Valve Disease March 2017 Brian Whisenant MD Introduction I got into this field to protect my turf. I must say, I have come full circle... - Kent W. Jones I got into this
CoreValve in a Degenerative Surgical Valve
 CoreValve in a Degenerative Surgical Valve Ran Kornowski, MD, FESC, FACC Chairman Department of Cardiology Rabin Medical Center, Petach Tikva, Israel Disclosure Statement of Financial Interest I, Ran Kornowski,
CoreValve in a Degenerative Surgical Valve Ran Kornowski, MD, FESC, FACC Chairman Department of Cardiology Rabin Medical Center, Petach Tikva, Israel Disclosure Statement of Financial Interest I, Ran Kornowski,
Transcatheter procedures of the future; expanding the treatment options for patients with severe aortic stenosis
 Transcatheter procedures of the future; expanding the treatment options for patients with severe aortic stenosis John Webb MD Director interventional cardiology, St Paul s Hospital McLeod Professor of
Transcatheter procedures of the future; expanding the treatment options for patients with severe aortic stenosis John Webb MD Director interventional cardiology, St Paul s Hospital McLeod Professor of
Appropriate Patient Selection or Healthcare Rationing? Lessons from Surgical Aortic Valve Replacement in The PARTNER I Trial Wilson Y.
 Appropriate Patient Selection or Healthcare Rationing? Lessons from Surgical Aortic Valve Replacement in The PARTNER I Trial Wilson Y. Szeto, MD on behalf of The PARTNER Trial Investigators and The PARTNER
Appropriate Patient Selection or Healthcare Rationing? Lessons from Surgical Aortic Valve Replacement in The PARTNER I Trial Wilson Y. Szeto, MD on behalf of The PARTNER Trial Investigators and The PARTNER
Matthew R. Reynolds, M.D., M.Sc. On Behalf of the PARTNER Investigators
 Lifetime Cost Effectiveness of Transcatheter Aortic Valve Replacement Compared with Standard Care Among Inoperable Patients with Severe Aortic Stenosis: Results from the PARTNER Trial (Cohort B) Matthew
Lifetime Cost Effectiveness of Transcatheter Aortic Valve Replacement Compared with Standard Care Among Inoperable Patients with Severe Aortic Stenosis: Results from the PARTNER Trial (Cohort B) Matthew
Valvular Heart Disease and Adult Congenital Intervention. A Pichard, MD. Director Cath Labs, Washington Hospital Center. Georgetown University.
 Valvular Heart Disease and Adult Congenital Intervention. A Pichard, MD Director Cath Labs, Washington Hospital Center. ProfessorofMedicine (Cardiology), Georgetown University. Conflict of Interest Proctor
Valvular Heart Disease and Adult Congenital Intervention. A Pichard, MD Director Cath Labs, Washington Hospital Center. ProfessorofMedicine (Cardiology), Georgetown University. Conflict of Interest Proctor
Embolic Protection Devices for Transcatheter Aortic Valve Replacement
 Embolic Protection Devices for Transcatheter Aortic Valve Replacement James M. McCabe, MD Medical Director, Cardiac Cath Lab University of Washington Seattle, WA Disclosures Proctoring and honoraria for
Embolic Protection Devices for Transcatheter Aortic Valve Replacement James M. McCabe, MD Medical Director, Cardiac Cath Lab University of Washington Seattle, WA Disclosures Proctoring and honoraria for
Disclosures. LGH TAVR: Presentation Outline 2/2/2016. Updates in Transcatheter Aortic Valve Replacement (TAVR) and the LGH Experience
 and the LGH Experience") Updates in Transcatheter Aortic Valve Replacement (TAVR) and the LGH Experience The LGH TAVR Program James E. Harvey, MD, MSc Medical Director, Structural Heart Intervention The Heart Group of Lancaster
Updates in Transcatheter Aortic Valve Replacement (TAVR) and the LGH Experience The LGH TAVR Program James E. Harvey, MD, MSc Medical Director, Structural Heart Intervention The Heart Group of Lancaster
Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated?
 Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated? RM Suri, V Sharma, JA Dearani, HM Burkhart, RC Daly, LD Joyce, HV Schaff Division of Cardiovascular Surgery, Mayo Clinic, Rochester,
Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated? RM Suri, V Sharma, JA Dearani, HM Burkhart, RC Daly, LD Joyce, HV Schaff Division of Cardiovascular Surgery, Mayo Clinic, Rochester,
TAVI: 10 Years After the First Case Low-Risk and High-Risk Patients What are the Limits? Dr Bernard Prendergast DM FRCP FESC John Radcliffe Hospital
 TAVI: 10 Years After the First Case Low-Risk and High-Risk Patients What are the Limits? Dr Bernard Prendergast DM FRCP FESC John Radcliffe Hospital Oxford I have financial relationships to disclose Honoraria
TAVI: 10 Years After the First Case Low-Risk and High-Risk Patients What are the Limits? Dr Bernard Prendergast DM FRCP FESC John Radcliffe Hospital Oxford I have financial relationships to disclose Honoraria
Case Presentations TAVR: The Good Bad and The Ugly
 Case Presentations TAVR: The Good Bad and The Ugly Vincent J. Pompili, MD, FACC, FSCAI Professor of Internal Medicine Director of Interventional Cardiovascular Medicine and Cardiac Catheterization Laboratories
Case Presentations TAVR: The Good Bad and The Ugly Vincent J. Pompili, MD, FACC, FSCAI Professor of Internal Medicine Director of Interventional Cardiovascular Medicine and Cardiac Catheterization Laboratories
Tissue vs Mechanical What s the Data??
 Biological (Tissue) Valve in a 60 year old patient: Debate Tissue vs Mechanical What s the Data?? Joseph E. Bavaria, MD Immediate-Past President - Society of Thoracic Surgeons (STS) Brooke Roberts-William
Biological (Tissue) Valve in a 60 year old patient: Debate Tissue vs Mechanical What s the Data?? Joseph E. Bavaria, MD Immediate-Past President - Society of Thoracic Surgeons (STS) Brooke Roberts-William
Establishing a New Path Forward for Patients With Severe Symptomatic Aortic Stenosis THE PARTNER TRIAL CLINICAL RESULTS
 Establishing a New Path Forward for Patients With Severe Symptomatic Aortic Stenosis THE PARTNER TRIAL CLINICAL RESULTS E D W A R D S T R A N S C A T H E T E R H E A R T V A L V E P R O G R A M T h e Pa
Establishing a New Path Forward for Patients With Severe Symptomatic Aortic Stenosis THE PARTNER TRIAL CLINICAL RESULTS E D W A R D S T R A N S C A T H E T E R H E A R T V A L V E P R O G R A M T h e Pa