GI Emergencies and the On-Call Call
|
|
|
- Zoe Ferguson
- 5 years ago
- Views:
Transcription

1 GI Emergencies and the On-Call Call Julie Yang, MD, FASGE Director of Therapeutic Endoscopy Assistant Professor of Medicine Montefiore Medical Center Albert Einstein College of Medicine
2 Objectives Scenarios of non-emergent, but common calls Define the few true emergencies in GI How to obtain relevant clinical history for quick decision-making
3 QUIZ 1 Are you a black cloud? A) Not been on call yet yes! B) Was on call, best sleep ever C) Was on call, got some calls but didn t have to go in phew! D) Was on call, still have PTSD my mom was right, I should have went into derm
4 CASE 1 It s your first night on-call as a first year GI fellow (black cloud) 5:05pm: your pager starts beeping Is it a GI bleeder? A food impaction?
5 CASE 1 Nope, it s a patient with a prep question: Doc, my colonoscopy is tomorrow AM and I lost my prep instructions. What do I do?
6 Colonoscopy Preps Know which preps and dosing your home institution uses 4L PEG: Golytely, Nulytely, Trilyte 2L PEG: Halflytely, Moviprep Low volume: Suprep, Prepopik Off label: Miralax + Gatorade ASGE guidelines 2015

7 Colonoscopy Preps Split prep vs. AM of dosing? Diet instructions? Clears NPO at least 2 hours before colonoscopy
8 CASE 1 It s me again Doc! I just puked up some of this nasty stuff!
 Hard candy (sugar-free menthol candy drops) 1 Consider antiemetic 1 Sharara et al.")
9 Patient Vomiting Prep Stop for mins, then resume at slower pace Keep prep chilled Straw to bypass tongue Improve palatability Adding flavoring (non-red Crystal Light) Hard candy (sugar-free menthol candy drops) 1 Consider antiemetic 1 Sharara et al. GIE 2013
10 CASE 2 8pm: you get a page from the ICU resident

11 Is this the GI fellow? THANK GOD!! I have a patient with a GI bleed and my senior wants you to scope him NOW!!

12 Emergent vs Urgent Endoscopy Emergent: going in tonight! Scope as soon as the pt is stabilized Urgent: see you first thing in AM Usually within hours Hemodynamically stable
13 QUIZ 2 Which does not require emergent endoscopy? A) 35 yo M with chest pain and spitting up saliva after eating steak B) 63 yo F with ascites and vomiting blood C) 70 yo M on Eliquis with red blood clots per rectum with stable vitals D) 85 yo F with abdominal distention and coffee bean shaped loop of colon on KUB
 35 yo M with chest pressure and spitting up saliva after eating steak B) 63 yo F with ascites and vomiting blood C) 70 yo M on Eliquis with red blood")
14 QUIZ 2 Which does not require emergent endoscopy? A) 35 yo M with chest pressure and spitting up saliva after eating steak B) 63 yo F with ascites and vomiting blood C) 70 yo M on Eliquis with red blood clots per rectum with stable vitals D) 85 yo F with distention and coffee bean shaped loop of colon on KUB


15 Indications for Emergent Scope Major GI bleeding Food impaction Acute colonic obstruction Unstable cholangitis
16 Initial Assessment Vitals How does the patient look? Age, comorbidities Multiorgan failure? Medications anticoagulants, immunosupressants Risk factors- ETOH, NSAIDs Do I need more diagnostic tests?

17 On-Call Assessment Give specific directions What to do in what order Call me back with Call me back if Assess the patient yourself!

18 On-Call Assessment- ABCs Respiratory Status? Can patient tolerate endoscopy? Does the patient need to be intubated? Respiratory distress Massive hematemesis Any altered mental status Cardiac Disease? Troponins and EKG? Massive blood transfusion protocol?
19 Triage Where is the patient? Should they be in the ICU? Are they appropriately monitored? Safe for endoscopy and recovery? Do I need back up? Perforation, ischemia Uncontrollable bleed Surgery! IR!
20 CASE 2 This is an ETOHic patient who started vomiting red blood and is hypotensive. What should we do?



21 Major GI Bleeding Varices Dieulafoy s lesion Visible vessel Bleeding post intervention (EMR/ESD or sphincterotomy)
22 You ask the ICU to: Intubate Start 2 large bore IVs CASE 2 Transfuse blood products Start IV PPI, octreotide, antibiotics Follow up labs EGD is performed at the bedside and bleeding esophageal varices are banded (by your attending)!
23 QUIZ 3 Meanwhile, you receive 4 more calls. Which is an urgent indication for ERCP? A) cholangitis without sepsis B) bile leak after liver transplant C) malignant biliary obstruction D) gallstone pancreatitis with normalizing LFTs
24 QUIZ 3 Meanwhile, you receive 4 more calls. Which is an urgent indication for ERCP? A) cholangitis without sepsis B) bile leak after liver transplant C) malignant biliary obstruction D) gallstone pancreatitis with normalizing LFTs
25 Emergent ERCP When do I contact the ERCP team? Unstable ascending cholangitis Charcot s triad = RUQ pain, fever, jaundice Reynold s Pentad Hemodynamically unstable Mental status changes

![2 (95% CI 0.06-0.68), I 2 =0], systemic [RR 0.37 (95% CI 0.18-0.78), I 2 =0], and and local complications [RR 0.](/docs-images/94/122371252/images/26-5.jpg "45 (95% CI 0.20-0.")
26 Urgent ERCP (within 48hrs) Bile leak post surgery (without a drain) Incidence: 2-25% of liver transplant Risk factor for developing biliary stricture 1 Gallstone pancreatitis + Cholangitis Reduces mortality [RR 0.2 (95% CI ), I 2 =0], systemic [RR 0.37 (95% CI ), I 2 =0], and and local complications [RR 0.45 (95% CI )] 2 Gallstone pancreatitis + CBD stone Maheshwari et al , Tse et al , ASGE guideline 2018

27 Biliary Emergency Pneumobilia = Air in the biliary tree Intact GB? Prior ERCP/PTC/surgery? Spontaneous biliary-enteric fistula? Emphysematous cholecystitis/cholangitis!


28 Emphysematous Cholecystitis Gas forming organism Elderly diabetic Heralds development of gangrene and perforation Mortality up to 25% Under-diagnosed Differential ddx Portal venous gas = necrotic bowel Air more peripheral in liver Call surgery! Lorenz et al 1990
29 CASE 3 11:15pm: you re about to head home but you get another page I have a patient here in the ER who has a giant belly and has not passed stool or flatus in a week! What should I do?
30 Acute Colonic Obstruction Peritoneal signs or symptoms? Fever, rigors Elevated WBC Acute abdomen Low threshold for antibiotics! When was the last time stool and/or gas passed? > 6 days? What is the diameter of the cecum? Surrounding colonic wall edema or abscess? > 10cm Call surgery!
31 Causes of Acute Colonic Obstruction Volvulus = kidney bean sign Torsion obstruction ischemia Sigmoid colon You! Cecum IR/surgery: cecostomy Elderly, institutionalized
32 Pseudo-obstruction, Ogilvie Syndrome Absence of a mechanical obstruction Spontaneous perforation 3-15% Conservative management for first 24hrs Meds, electrolytes (K, Ca, Mg), mobilization, rectal tube Neostigmine (anticholinesterase) Bradycardia, asystole, hypotension Endoscopic decompression Followed by daily PEG Decreases relapse (0% vs. 33%, p= 0.04) 1 Loftus et al

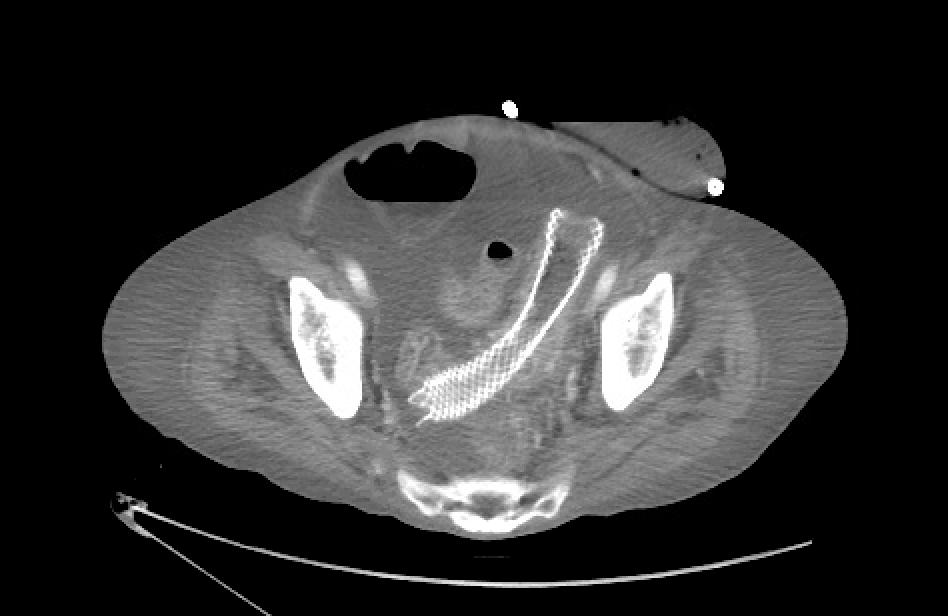
33 Malignant Colonic Obstruction Primary colon cancer Bridge to surgery Allows pre-op complete colon evaluation Allows time for appropriate staging Allows for 1-stage operation Palliation Colonic Stent Secondary from metastases Palliation Surgery: >10% mortality and >40% morbidity ASGE guideline 2018
 Uncovered")

34 Colon Stents Self-expanding metal stent (SEMS) Uncovered Fluoroscopy Enemas! >90% clinical success Watt et al 2007
35 QUIZ 4 In which colonic obstruction scenario would you NOT stent? A) Metastatic descending colon cancer B) Apple-core sigmoid lesion on CT C) Metastatic ovarian to the sigmoid D) Palpable rectal mass on DRE
36 QUIZ 4 In which colonic obstruction scenario would you NOT stent? A) Metastatic descending colon cancer B) Apple-core sigmoid lesion on CT C) Metastatic ovarian to the sigmoid D) Palpable rectal mass on DRE

37 Malignant Colonic Obstruction
38 CASE 3 You call in your GI team and successfully place a colonic stent. There is immediate gas and stool expulsion through the stent you ve never seen a more beautiful thing!
39 Take-Home Points Only few true emergencies in GI Best evaluation is done by YOU! Who, what, when, where Communication is key


40 3am: zzz. Questions?
9/21/15. Joshua Pruitt, MD, FAAEM Medical Director, LifeGuard Air Ambulance Iowa PA Society Fall CME Conference September 29, 2015
 Unless they prove otherwise. ~Every ED attending ever Joshua Pruitt, MD, FAAEM Medical Director, LifeGuard Air Ambulance Iowa PA Society Fall CME Conference September 29, 2015 AAA with rupture Mesenteric
Unless they prove otherwise. ~Every ED attending ever Joshua Pruitt, MD, FAAEM Medical Director, LifeGuard Air Ambulance Iowa PA Society Fall CME Conference September 29, 2015 AAA with rupture Mesenteric
Endoscopic Treatment of Luminal Perforations and Leaks
 Endoscopic Treatment of Luminal Perforations and Leaks Ali A. Siddiqui, MD Professor of Medicine Director of Interventional Endoscopy Jefferson Medical College Philadelphia, PA When Do You Suspect a Luminal
Endoscopic Treatment of Luminal Perforations and Leaks Ali A. Siddiqui, MD Professor of Medicine Director of Interventional Endoscopy Jefferson Medical College Philadelphia, PA When Do You Suspect a Luminal
Abdominal Pain. Luke Donnelly, MD Emergency Medicine
 Abdominal Pain Luke Donnelly, MD Emergency Medicine Objectives Approach to abdominal pain Evaluation Critical diagnoses and treatments Abdominal Pain Most Common ER Complaint Broad Differential Can often
Abdominal Pain Luke Donnelly, MD Emergency Medicine Objectives Approach to abdominal pain Evaluation Critical diagnoses and treatments Abdominal Pain Most Common ER Complaint Broad Differential Can often
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN
 UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
GENERAL SURGERY FOR SMART PEOPLE JOE NOLD MD, FACS WICHITA SURGICAL SPECIALISTS
 GENERAL SURGERY FOR SMART PEOPLE JOE NOLD MD, FACS WICHITA SURGICAL SPECIALISTS CONFLICTS/DECLARATIONS I have no financial conflicts or declarations I AM always willing to see a consult for you TEXT TOPICS
GENERAL SURGERY FOR SMART PEOPLE JOE NOLD MD, FACS WICHITA SURGICAL SPECIALISTS CONFLICTS/DECLARATIONS I have no financial conflicts or declarations I AM always willing to see a consult for you TEXT TOPICS
Vesalius SCALpel : Biliary (see also: biliary/pancreatic folios) Physiology
 Physiology") Vesalius SCALpel : Biliary (see also: biliary/pancreatic folios) Physiology 95% of bile acids reabsorbed; colic and chenodeoxycolic primary bile acids cholecystokinin (CCK) major stimulus of gallbladder
Vesalius SCALpel : Biliary (see also: biliary/pancreatic folios) Physiology 95% of bile acids reabsorbed; colic and chenodeoxycolic primary bile acids cholecystokinin (CCK) major stimulus of gallbladder
12 Blueprints Q&A Step 2 Surgery
 12 Blueprints Q&A Step 2 Surgery 34. A 40-year-old female has been referred to you for a recent ER and hospital admission, from which she was given a diagnosis of acute diverticulitis. Treatment at that
12 Blueprints Q&A Step 2 Surgery 34. A 40-year-old female has been referred to you for a recent ER and hospital admission, from which she was given a diagnosis of acute diverticulitis. Treatment at that
Management of Gallbladder Disease
 Management of Gallbladder Disease Steven B. Johnson, MD, FACS, FCCM Professor and Chairman, Department of Surgery Program Director, Phoenix Integrated Surgical Residency University of Arizona College of
Management of Gallbladder Disease Steven B. Johnson, MD, FACS, FCCM Professor and Chairman, Department of Surgery Program Director, Phoenix Integrated Surgical Residency University of Arizona College of
The Bile Duct (and Pancreas) and the Physician
 and the Physician") The Bile Duct (and Pancreas) and the Physician Javaid Iqbal Consultant in Gastroenterology and Pancreato-biliary Medicine University Hospital South Manchester Not so common?! Two weeks 38 ERCP s 20 15
The Bile Duct (and Pancreas) and the Physician Javaid Iqbal Consultant in Gastroenterology and Pancreato-biliary Medicine University Hospital South Manchester Not so common?! Two weeks 38 ERCP s 20 15
LARGE BOWEL OBSTRUCTION MARCUS BURNSTEIN
 LARGE BOWEL OBSTRUCTION MARCUS BURNSTEIN MCQ A 78 yr. old man (HT, DM, 2 coronary stents) has 3 mos. of irregular bowel habits and 72 hrs. of LBO. Distended, non-tender. Normal blood work. Plain xray,
LARGE BOWEL OBSTRUCTION MARCUS BURNSTEIN MCQ A 78 yr. old man (HT, DM, 2 coronary stents) has 3 mos. of irregular bowel habits and 72 hrs. of LBO. Distended, non-tender. Normal blood work. Plain xray,
ERCP / PTC Surgical Laparoscopic vs open Timing and order of approach
 Choledocholithiasis Which Approach and When? Lygia Stewart, MD University of California, San Francisco 2010 Naffziger Post-Graduate Course Clinical Manifestations of Choledocholithiasis Asymptomatic (no
Choledocholithiasis Which Approach and When? Lygia Stewart, MD University of California, San Francisco 2010 Naffziger Post-Graduate Course Clinical Manifestations of Choledocholithiasis Asymptomatic (no
LOKUN! I got stomach ache!
 LOKUN! I got stomach ache! Mr L is a 67year old Chinese gentleman who is a non smoker, social drinker. He has a medical history significant for Hypertension, Hyperlipidemia, Type 2 Diabetes Mellitus, Chronic
LOKUN! I got stomach ache! Mr L is a 67year old Chinese gentleman who is a non smoker, social drinker. He has a medical history significant for Hypertension, Hyperlipidemia, Type 2 Diabetes Mellitus, Chronic
Long Term Follow-up. 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown. Is the patient alive? Yes No
 Long Term Follow-up 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown Is the patient alive? Yes No Was an exam performed by a bariatric physician or PA/NP? Yes No Was the patient
Long Term Follow-up 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown Is the patient alive? Yes No Was an exam performed by a bariatric physician or PA/NP? Yes No Was the patient
7/11/2017. We re gonna help a lot of people today. Biliary/Pancreatic Endoscopy. AGS July 1-2, Kenneth M. Sigman, MD
 Biliary/Pancreatic Endoscopy AGS July 1-2, 2017 Kenneth M. Sigman, MD We re gonna help a lot of people today 1 2 3 4 Cannulation It all starts with cannulation Double Wire Cannulation Difficult cannulations
Biliary/Pancreatic Endoscopy AGS July 1-2, 2017 Kenneth M. Sigman, MD We re gonna help a lot of people today 1 2 3 4 Cannulation It all starts with cannulation Double Wire Cannulation Difficult cannulations
When to Scope in Lower GI Bleeding: It Must Be Done Now. Lisa L. Strate, MD, MPH Assistant Professor of Medicine University of Washington, Seattle, WA
 When to Scope in Lower GI Bleeding: It Must Be Done Now Lisa L. Strate, MD, MPH Assistant Professor of Medicine University of Washington, Seattle, WA Outline Epidemiology Overview of available tests Urgent
When to Scope in Lower GI Bleeding: It Must Be Done Now Lisa L. Strate, MD, MPH Assistant Professor of Medicine University of Washington, Seattle, WA Outline Epidemiology Overview of available tests Urgent
Gustavo Mariño, MD VA Medical Center Washington, DC
 Gustavo Mariño, MD VA Medical Center Washington, DC True emergency? Likelihood that an intervention is required to improve outcomes Optimal timing Other factors: VIPs?, demanding patient?, convenience?,
Gustavo Mariño, MD VA Medical Center Washington, DC True emergency? Likelihood that an intervention is required to improve outcomes Optimal timing Other factors: VIPs?, demanding patient?, convenience?,
COPYRIGHTED MATERIAL. 1 Approach to the patient with gross gastrointestinal bleeding. Grace H. Elta, Mimi Takami
 1 Approach to the patient with gross gastrointestinal bleeding Grace H. Elta, Mimi Takami Gastrointestinal (GI) bleeding is a common clinical problem that requires more than 300 000 hospitalizations annually
1 Approach to the patient with gross gastrointestinal bleeding Grace H. Elta, Mimi Takami Gastrointestinal (GI) bleeding is a common clinical problem that requires more than 300 000 hospitalizations annually
Early management of complicated gallstones and acute pancreatitis
 Early management of complicated gallstones and acute pancreatitis A/Prof Richard Cade George Kalogeropoulos ( Fellow) HPB/Upper GI Unit Eastern Health, Melbourne biliary colic/acute cholecystitis common
Early management of complicated gallstones and acute pancreatitis A/Prof Richard Cade George Kalogeropoulos ( Fellow) HPB/Upper GI Unit Eastern Health, Melbourne biliary colic/acute cholecystitis common
Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam
 Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam By Sarmad Aji, MD., FACS. A comprehensive review of the most commonly asked questions on the American Board of Surgery
Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam By Sarmad Aji, MD., FACS. A comprehensive review of the most commonly asked questions on the American Board of Surgery
Acute Abdomen. Nirav Patel MD, FACS Banner University Medical Center - Phoenix
 Acute Abdomen Nirav Patel MD, FACS Banner University Medical Center - Phoenix ? Diffuse periumbilical with localization to RLQ + Nausea, anorexia, fevers - Diarrhea, emesis Exacerbated by movement, bumps
Acute Abdomen Nirav Patel MD, FACS Banner University Medical Center - Phoenix ? Diffuse periumbilical with localization to RLQ + Nausea, anorexia, fevers - Diarrhea, emesis Exacerbated by movement, bumps
Colorectal non-inflammatory emergencies
 Colorectal non-inflammatory emergencies Prof. Hesham Amer Professor of general surgery, Kasr Alainy hospital, Cairo university Dr. Doaa Mansour Dr. Ahmed Nabil Dr. Ahmed Abdel-Salam Lecturers of general
Colorectal non-inflammatory emergencies Prof. Hesham Amer Professor of general surgery, Kasr Alainy hospital, Cairo university Dr. Doaa Mansour Dr. Ahmed Nabil Dr. Ahmed Abdel-Salam Lecturers of general
Correspondence should be addressed to Justin Cochrane;
 Case Reports in Gastrointestinal Medicine Volume 2015, Article ID 794282, 4 pages http://dx.doi.org/10.1155/2015/794282 Case Report Acute on Chronic Pancreatitis Causing a Highway to the Colon with Subsequent
Case Reports in Gastrointestinal Medicine Volume 2015, Article ID 794282, 4 pages http://dx.doi.org/10.1155/2015/794282 Case Report Acute on Chronic Pancreatitis Causing a Highway to the Colon with Subsequent
Management of Gastroenterology Emergencies Tim Gardner, MD Director, Pancreatic Disorders Section of Gastroenterology and Hepatology
 Management of Gastroenterology Emergencies Tim Gardner, MD Director, Pancreatic Disorders Section of Gastroenterology and Hepatology DHMC CREST Symposium November 7, 2008 There are no financial disclosures
Management of Gastroenterology Emergencies Tim Gardner, MD Director, Pancreatic Disorders Section of Gastroenterology and Hepatology DHMC CREST Symposium November 7, 2008 There are no financial disclosures
Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology
 Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology Faculty representative: David L. Burns, MD, CNSP Resident representative: Tom Castiglione, MD Revision date: March 6, 2006
Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology Faculty representative: David L. Burns, MD, CNSP Resident representative: Tom Castiglione, MD Revision date: March 6, 2006
From Inflammation to Ischemia May apply to all luminal structures Obstruction Small or large bowel Appendix Gall bladder Ureter Hydrostatic Pressure:
 The Acute Abdomen Surgical Issues for the Family Practitioner Rochelle A. Dicker, MD Assistant Professor of Surgery and Anesthesia UC San Francisco Visceral Pain Vague Deep Associated with nausea/vomiting
The Acute Abdomen Surgical Issues for the Family Practitioner Rochelle A. Dicker, MD Assistant Professor of Surgery and Anesthesia UC San Francisco Visceral Pain Vague Deep Associated with nausea/vomiting
Hepatobiliary Ultrasound Rimon Bengiamin, MD, RDMS Assistant Clinical Professor Director of Emergency Ultrasound UCSF Fresno. Objectives. Why?
 Hepatobiliary Ultrasound Rimon Bengiamin, MD, RDMS Assistant Clinical Professor Director of Emergency Ultrasound UCSF Fresno Objectives Discuss the goals of point-of-care biliary ultrasound Review the
Hepatobiliary Ultrasound Rimon Bengiamin, MD, RDMS Assistant Clinical Professor Director of Emergency Ultrasound UCSF Fresno Objectives Discuss the goals of point-of-care biliary ultrasound Review the
Chapter Goal. Learning Objectives 9/12/2012. Chapter 29. Nontraumatic Abdominal Injuries
 Chapter 29 Nontraumatic Abdominal Injuries Chapter Goal Use assessment findings to formulate field impression & implement treatment plan for patients with nontraumatic abdominal pain Learning Objectives
Chapter 29 Nontraumatic Abdominal Injuries Chapter Goal Use assessment findings to formulate field impression & implement treatment plan for patients with nontraumatic abdominal pain Learning Objectives
Chapter 14: Training in Radiology. DDSEP Chapter 1: Question 12
 DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
GASTROINESTINAL BLEEDING. Dr.Ammar I. Abdul-Latif
 GASTROINESTINAL BLEEDING Dr.Ammar I. Abdul-Latif CLASSIFICATION OF G.I.BLEEDING GIB Appearance Acuity Site Apparent Acute Upper Obscure Chronic Lower UPPER&LOWER G.I.BLEEDING CAUSES OF UPPER G.I. BLEEDING
GASTROINESTINAL BLEEDING Dr.Ammar I. Abdul-Latif CLASSIFICATION OF G.I.BLEEDING GIB Appearance Acuity Site Apparent Acute Upper Obscure Chronic Lower UPPER&LOWER G.I.BLEEDING CAUSES OF UPPER G.I. BLEEDING
Christopher Lau Kings County Hospital SUNY Downstate Medical Center February 24, 2011
 Christopher Lau Kings County Hospital SUNY Downstate Medical Center February 24, 2011 37 year old male presented with 1 day history of abdominal pain Pain was diffuse but worst in the epigastric area No
Christopher Lau Kings County Hospital SUNY Downstate Medical Center February 24, 2011 37 year old male presented with 1 day history of abdominal pain Pain was diffuse but worst in the epigastric area No
Slide 1. Slide 2. Slide 3 Pancreatic Cancer- Case #1. Endoscopic management of GI malignancy. Endoscopic approaches in GI malignancy- Agenda
 Slide 1 A teaching hospital of Harvard Medical School Endoscopic management of GI malignancy Tyler Berzin MD, MS Center for Advanced Endoscopy Division of Gastroenterology Beth Israel Deaconess Medical
Slide 1 A teaching hospital of Harvard Medical School Endoscopic management of GI malignancy Tyler Berzin MD, MS Center for Advanced Endoscopy Division of Gastroenterology Beth Israel Deaconess Medical
Biliary Tree Ultrasound - In a nutshell. Pamela Parker Lead Sonographer
 Biliary Tree Ultrasound - In a nutshell Pamela Parker Lead Sonographer Aims Review what we know about the biliary system Common pathologies Pitfalls Reporting tips The Nutshell Background Biliary examinations
Biliary Tree Ultrasound - In a nutshell Pamela Parker Lead Sonographer Aims Review what we know about the biliary system Common pathologies Pitfalls Reporting tips The Nutshell Background Biliary examinations
Douglas G. Adler MD. ACG Regional Postgraduate Course - Nashville, TN Copyright 2013 American College of Gastroenterology
 Enteral Stents 2013: State of the Art Douglas G. Adler MD Associate Professor of Medicine Director of Therapeutic Endoscopy University of Utah School of Medicine Huntsman Cancer Center Esophageal Stents
Enteral Stents 2013: State of the Art Douglas G. Adler MD Associate Professor of Medicine Director of Therapeutic Endoscopy University of Utah School of Medicine Huntsman Cancer Center Esophageal Stents
3/22/2011. Inflammatory Bowel Disease. Inflammatory Bowel Disease Objectives: Appendicitis. Lemone and Burke Chapter 26
 Inflammatory Bowel Disease Lemone and Burke Chapter 26 Inflammatory Bowel Disease Objectives: Discuss etiology, patho and clinical manifestations of Appendicitis Peritonitis Ulcerative Colitis Crohn s
Inflammatory Bowel Disease Lemone and Burke Chapter 26 Inflammatory Bowel Disease Objectives: Discuss etiology, patho and clinical manifestations of Appendicitis Peritonitis Ulcerative Colitis Crohn s
Emergency Surgery Course Graz, March UPPER GI BLEEDING. Carlos Mesquita Coimbra
 UPPER GI BLEEDING Carlos Mesquita Coimbra Aim Causes Management Problem Above angle of Treitz Common emergency 1-2/1000 pts 10% rebleeed 1% angioembolization 20% over 60
UPPER GI BLEEDING Carlos Mesquita Coimbra Aim Causes Management Problem Above angle of Treitz Common emergency 1-2/1000 pts 10% rebleeed 1% angioembolization 20% over 60
General Surgery Service
 General Surgery Service Patient Care Goals and Objectives Stomach/Duodenum and Bariatric assessed for a) Obesity surgery b) Treatment of i) Adenocarcinoma of the stomach ii) GIST iii) Carcinoid 2) Optimize
General Surgery Service Patient Care Goals and Objectives Stomach/Duodenum and Bariatric assessed for a) Obesity surgery b) Treatment of i) Adenocarcinoma of the stomach ii) GIST iii) Carcinoid 2) Optimize
Case 1- B.N. 66 yr old F with PMHx of breast cancer s/ p mastectomy, HTN, DM presented with dysphagia to solids and liquids.
 Case 1- B.N 66 yr old F with PMHx of breast cancer s/ p mastectomy, HTN, DM presented with dysphagia to solids and liquids. Reports retching to clear esophagus. Case 1- B.N EGD: Stricture in the distal
Case 1- B.N 66 yr old F with PMHx of breast cancer s/ p mastectomy, HTN, DM presented with dysphagia to solids and liquids. Reports retching to clear esophagus. Case 1- B.N EGD: Stricture in the distal
What can you expect after your ERCP?
 ERCP Explained and respond to bed rest, pain relief and fasting to rest the gut with the patient needing to stay in hospital for only a few days. Some patients develop severe pancreatitis and may require
ERCP Explained and respond to bed rest, pain relief and fasting to rest the gut with the patient needing to stay in hospital for only a few days. Some patients develop severe pancreatitis and may require
Capsule Endoscopy and Deep Enteroscopy
 Capsule Endoscopy and Deep Enteroscopy Are they complementary? ACG Governors / ASGE 2012 Best Practices Course January 29, 2012 The Hyatt Regency Huntington Beach, California John A. Martin, MD Disclosure
Capsule Endoscopy and Deep Enteroscopy Are they complementary? ACG Governors / ASGE 2012 Best Practices Course January 29, 2012 The Hyatt Regency Huntington Beach, California John A. Martin, MD Disclosure
Extreme Endo Toolbox. Slide 1. Slide 2. Slide 3. Outline. Endo Toolbox - Requisites
 Slide 1 Extreme Endo Toolbox Pramod Malik, MD, FACG, FASGE, AGAF, CPI Gastroenterology Associates of Tidewater Slide 2 Outline New Tools - Confocal endomicroscopy (Cellvizio) - HD/ NBI/ FICE - Ovesco clip
Slide 1 Extreme Endo Toolbox Pramod Malik, MD, FACG, FASGE, AGAF, CPI Gastroenterology Associates of Tidewater Slide 2 Outline New Tools - Confocal endomicroscopy (Cellvizio) - HD/ NBI/ FICE - Ovesco clip
Abdo Pain rules & regulations. Mark Hartnell 2010
 Abdo Pain rules & regulations Mark Hartnell 2010 Aims Simple rules which might help in patients with abdominal pain Talk about some myths and realities Discuss some practical how to s in day to day treatment
Abdo Pain rules & regulations Mark Hartnell 2010 Aims Simple rules which might help in patients with abdominal pain Talk about some myths and realities Discuss some practical how to s in day to day treatment
Approach to the Biliary Stricture
 Approach to the Biliary Stricture ACG Eastern Postgraduate Course Washington DC June 8, 2014 Steven A. Edmundowicz MD FASGE Chief of Endoscopy Division of Gastroenterology Professor of Medicine Disclosures
Approach to the Biliary Stricture ACG Eastern Postgraduate Course Washington DC June 8, 2014 Steven A. Edmundowicz MD FASGE Chief of Endoscopy Division of Gastroenterology Professor of Medicine Disclosures
DISCLAIMER. No Conflict of Interest
 DISCLAIMER No Conflict of Interest EXCLAIMER No Interest in Conflict GALLSTONES FAQs and FACTS John Dunn, FRACS Laparoscopy Auckland YOU GOTTA KNOW THIS STUFF HOW DO THEY FORM? Gallbladder Lithogenic
DISCLAIMER No Conflict of Interest EXCLAIMER No Interest in Conflict GALLSTONES FAQs and FACTS John Dunn, FRACS Laparoscopy Auckland YOU GOTTA KNOW THIS STUFF HOW DO THEY FORM? Gallbladder Lithogenic
Kathy P. Bull-Henry, MD, FACG Dr. Bull-Henry has indicated no relevant financial relationships. Don t Waste Time With No Chance to See
 Don t Waste Time with No Chance to See Kathy P. Bull-Henry, MD, FACG Dr. Bull-Henry has indicated no relevant financial relationships. Don t Waste Time With No Chance to See Kathy Bull-Henry, MD, FACG
Don t Waste Time with No Chance to See Kathy P. Bull-Henry, MD, FACG Dr. Bull-Henry has indicated no relevant financial relationships. Don t Waste Time With No Chance to See Kathy Bull-Henry, MD, FACG
Colon ischemia. ACG Clinical Guideline; Am J Gastroenterol 2015
 Colon ischemia ACG Clinical Guideline; Am J Gastroenterol 2015 Manifestations Acute, reversible Irreversible : gangrene, fulminant colitis/stricture formation, chronic ischemic colitis Recurrent sepsis
Colon ischemia ACG Clinical Guideline; Am J Gastroenterol 2015 Manifestations Acute, reversible Irreversible : gangrene, fulminant colitis/stricture formation, chronic ischemic colitis Recurrent sepsis
STRICTURES OF THE BILE DUCTS Session No.: 5. Andrea Tringali Digestive Endoscopy Unit Catholic University Rome - Italy
 STRICTURES OF THE BILE DUCTS Session No.: 5 Andrea Tringali Digestive Endoscopy Unit Catholic University Rome - Italy Drainage of biliary strictures. The history before 1980 Surgical bypass Percutaneous
STRICTURES OF THE BILE DUCTS Session No.: 5 Andrea Tringali Digestive Endoscopy Unit Catholic University Rome - Italy Drainage of biliary strictures. The history before 1980 Surgical bypass Percutaneous
Colon Cancer Surgery
 Colon Cancer Surgery Introduction Colon cancer is a life-threatening condition that affects thousands of people. Doctors usually recommend surgery for the removal of colon cancer. If your doctor recommends
Colon Cancer Surgery Introduction Colon cancer is a life-threatening condition that affects thousands of people. Doctors usually recommend surgery for the removal of colon cancer. If your doctor recommends
DOMINATE THE CLERKSHIP REVIEW PACKET. What are the electrolyte compositions of NS, LR, Plasmalyte A? Na Cl K HCO3 Ca Mg ph NS LR Plasmalyte A
 DOMINATE THE CLERKSHIP REVIEW PACKET POST OP CARE Fluids What percent of total body water does each compartment (extracellular, intracellular, interstitial, intravascular) make up? What are the electrolyte
DOMINATE THE CLERKSHIP REVIEW PACKET POST OP CARE Fluids What percent of total body water does each compartment (extracellular, intracellular, interstitial, intravascular) make up? What are the electrolyte
GASTRO-INTESTINAL TRACT INFECTIONS - ANTIMICROBIAL MANAGEMENT
 GASTRO-INTESTINAL TRACT INFECTIONS - ANTIMICROBIAL MANAGEMENT Name & Title Of Author: Dr Linda Jewes, Consultant Microbiologist Date Amended: December 2016 Approved by Committee/Group: Drugs & Therapeutics
GASTRO-INTESTINAL TRACT INFECTIONS - ANTIMICROBIAL MANAGEMENT Name & Title Of Author: Dr Linda Jewes, Consultant Microbiologist Date Amended: December 2016 Approved by Committee/Group: Drugs & Therapeutics
Endoscopic Management of Perforations
 Endoscopic Management of Perforations Gregory G. Ginsberg, MD Professor of Medicine University of Pennsylvania Perelman School of Medicine Gastroenterology Division Executive Director of Endoscopic Services
Endoscopic Management of Perforations Gregory G. Ginsberg, MD Professor of Medicine University of Pennsylvania Perelman School of Medicine Gastroenterology Division Executive Director of Endoscopic Services
MANAGEMENT OF PYOGENIC LIVER ABSCESS BOYOUNG SONG, M.D. SUNY DOWNSTATE SURGERY 11/7/13
 MANAGEMENT OF PYOGENIC LIVER ABSCESS BOYOUNG SONG, M.D. SUNY DOWNSTATE SURGERY 11/7/13 CASE THE PATIENT IS A 79 YEAR OLD MALE WITH 3 DAY HISTORY OF LOWER ABDOMINAL PAIN, NAUSEA WITHOUT VOMITING, CHILLS
MANAGEMENT OF PYOGENIC LIVER ABSCESS BOYOUNG SONG, M.D. SUNY DOWNSTATE SURGERY 11/7/13 CASE THE PATIENT IS A 79 YEAR OLD MALE WITH 3 DAY HISTORY OF LOWER ABDOMINAL PAIN, NAUSEA WITHOUT VOMITING, CHILLS
The EM Educator Series
 The EM Educator Series The EM Educator Series: Why is my patient with gallbladder pathology so sick? Author: Alex Koyfman, MD (@EMHighAK) // Edited by: Brit Long, MD (@long_brit) and Manpreet Singh, MD
The EM Educator Series The EM Educator Series: Why is my patient with gallbladder pathology so sick? Author: Alex Koyfman, MD (@EMHighAK) // Edited by: Brit Long, MD (@long_brit) and Manpreet Singh, MD
Management of Gallbladder Disease. Cory Buschmann, MD PGY-5 11/28/2017
 Management of Gallbladder Disease Cory Buschmann, MD PGY-5 11/28/2017 Financial disclosures None Content Scope of gallbladder diseases Evaluation H&P Labs Imaging Cholecystectomy vs cholecystostomy Ancillary
Management of Gallbladder Disease Cory Buschmann, MD PGY-5 11/28/2017 Financial disclosures None Content Scope of gallbladder diseases Evaluation H&P Labs Imaging Cholecystectomy vs cholecystostomy Ancillary
Percutaneous Cecostomy Tube Placement
 Information About Your Child s Procedure Percutaneous Cecostomy Tube Placement Read this form so you understand the procedure and its risks. Please ask questions about anything you do not understand. What
Information About Your Child s Procedure Percutaneous Cecostomy Tube Placement Read this form so you understand the procedure and its risks. Please ask questions about anything you do not understand. What
Study of post cholecystectomy biliary leakage and its management
 Original Research Article Study of post cholecystectomy biliary leakage and its management P. Krishna Kishore 1*, B. Manju Sruthi 2, G. Obulesu 3 1 Assistant Professor, Departmentment of General Surgery,
Original Research Article Study of post cholecystectomy biliary leakage and its management P. Krishna Kishore 1*, B. Manju Sruthi 2, G. Obulesu 3 1 Assistant Professor, Departmentment of General Surgery,
Imaging of liver and pancreas
 Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
DR JAIKISHOR JOTHIRAJ MD POST GRADUATE DEPT OF RADIODIAGNOSIS
 DR JAIKISHOR JOTHIRAJ MD POST GRADUATE DEPT OF RADIODIAGNOSIS YASHODAMMAL 70 YRS OD LADY had C/o diffuse lower abdominal pain 20 days h/o blood in stools 4 days h/o vomiting 2 days h/o burning micturation
DR JAIKISHOR JOTHIRAJ MD POST GRADUATE DEPT OF RADIODIAGNOSIS YASHODAMMAL 70 YRS OD LADY had C/o diffuse lower abdominal pain 20 days h/o blood in stools 4 days h/o vomiting 2 days h/o burning micturation
Outline. GI-Bleeding. Initial intervention
 Internal Medicine Board Review 2016: GI-Bleeding Stephan Goebel, M.D. Assistant Professor Division of Digestive Diseases Management UGI-Bleeding (80%) Ulcers Varices others LGI-Bleeding (20%) Outline Initial
Internal Medicine Board Review 2016: GI-Bleeding Stephan Goebel, M.D. Assistant Professor Division of Digestive Diseases Management UGI-Bleeding (80%) Ulcers Varices others LGI-Bleeding (20%) Outline Initial
Gastroenterology. Certification Examination Blueprint. Purpose of the exam
 Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Plain abdomen The standard films are supine & erect AP views (alternative to erect, lateral decubitus film is used in ill patients).
.") Plain abdomen The standard films are supine & erect AP views (alternative to erect, lateral decubitus film is used in ill patients). The stomach can be readily identified by its location, gastric rugae
Plain abdomen The standard films are supine & erect AP views (alternative to erect, lateral decubitus film is used in ill patients). The stomach can be readily identified by its location, gastric rugae
CrackCast Episode 28 Jaundice
 CrackCast Episode 28 Jaundice Episode overview: 1) Describe heme metabolism 2) List common pre-hepatic/hepatic/post-hepatic causes of jaundice Wisecracks: 1) What are clinical signs of liver disease? 2)
CrackCast Episode 28 Jaundice Episode overview: 1) Describe heme metabolism 2) List common pre-hepatic/hepatic/post-hepatic causes of jaundice Wisecracks: 1) What are clinical signs of liver disease? 2)
General'Surgery'Service'
 General'Surgery'Service' Patient Care Goals and Objectives 1)! Stomach/Duodenum and Bariatric 2)! Interpret the results of clinical evaluations (history, physical examination) performed on patients being
General'Surgery'Service' Patient Care Goals and Objectives 1)! Stomach/Duodenum and Bariatric 2)! Interpret the results of clinical evaluations (history, physical examination) performed on patients being
Hepatobiliary Disease
 Hepatobiliary Disease 大林慈濟綜合醫院 魏昌國 一般外科 Cholelithiasis 膽道結石 Incidence (USA) 10% in adult 85% cholesterol stones 15% pigment stone Risk factors Cholesterol stones Age Female(2x, 25% versus 12% at age 60),
Hepatobiliary Disease 大林慈濟綜合醫院 魏昌國 一般外科 Cholelithiasis 膽道結石 Incidence (USA) 10% in adult 85% cholesterol stones 15% pigment stone Risk factors Cholesterol stones Age Female(2x, 25% versus 12% at age 60),
Chapter 23 Endoscopic Diagnostic Procedures and Tests B Y L Y N N E L S L O O R N C G R N
 Chapter 23 Endoscopic Diagnostic Procedures and Tests B Y L Y N N E L S L O O R N C G R N Objectives 1. Describe the different types of endoscopes and their components. 2. Discuss the indications for EGD,
Chapter 23 Endoscopic Diagnostic Procedures and Tests B Y L Y N N E L S L O O R N C G R N Objectives 1. Describe the different types of endoscopes and their components. 2. Discuss the indications for EGD,
Case Presentation: Mr. S
 Case Presentation: Mr. S History Seen as inpatient in May, but has significant prior history and is a poor historian 53 y.o. Male no PMH, has been out of contact with medicine for years aside from hernia
Case Presentation: Mr. S History Seen as inpatient in May, but has significant prior history and is a poor historian 53 y.o. Male no PMH, has been out of contact with medicine for years aside from hernia
Moderator: Mitchell L. Schubert, MD, FACG Presenters: Sanjay Bangarulingam, MD and Pritesh Mutha, MD, MPH
 Virginia Commonwealth University Fellow Presentations Moderator: Mitchell L. Schubert, MD, FACG Presenters: Sanjay Bangarulingam, MD and Pit Pritesh hm Mutha, MD, MPH Benign Esophageal Stricture Sanjay
Virginia Commonwealth University Fellow Presentations Moderator: Mitchell L. Schubert, MD, FACG Presenters: Sanjay Bangarulingam, MD and Pit Pritesh hm Mutha, MD, MPH Benign Esophageal Stricture Sanjay
Historical perspective
 Raj Santharam, MD GI Associates, LLC Clinical Assistant Professor of Medicine Medical College of Wisconsin Historical perspective FFS first widespread use in the early 1970 s Expansion of therapeutic techniques
Raj Santharam, MD GI Associates, LLC Clinical Assistant Professor of Medicine Medical College of Wisconsin Historical perspective FFS first widespread use in the early 1970 s Expansion of therapeutic techniques
Perforated peptic ulcer
 Perforated peptic ulcer - Despite the widespread use of gastric anti-secretory agents and eradication therapy, the incidence of perforated peptic ulcer has changed little, age limits increase NSAIDs elderly
Perforated peptic ulcer - Despite the widespread use of gastric anti-secretory agents and eradication therapy, the incidence of perforated peptic ulcer has changed little, age limits increase NSAIDs elderly
ERCP complications and challenges in their diagnosis and management.
 ERCP complications and challenges in their diagnosis and management. Sandie R Thomson Chair of the Division of Gastroenterology, University of Cape Town ERCP Do I have a good Indication? . Algorithm for
ERCP complications and challenges in their diagnosis and management. Sandie R Thomson Chair of the Division of Gastroenterology, University of Cape Town ERCP Do I have a good Indication? . Algorithm for
Form 1: Demographics
 Form 1: Demographics Case Number: *LMRN: *DOB: / / *Gender: Male Female *Race: White Native Hawaiian/Other Pacific Islander Black or African American Asian American Indian or Alaska Native Unknown *Hispanic
Form 1: Demographics Case Number: *LMRN: *DOB: / / *Gender: Male Female *Race: White Native Hawaiian/Other Pacific Islander Black or African American Asian American Indian or Alaska Native Unknown *Hispanic
Jaundice. Agnieszka Dobrowolska- Zachwieja, MD, PhD
 Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL
 SIGNIFICANCE OF EXTRALUMINAL ABDOMINAL GAS: LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL SCBT/MR 2012 October 26,
SIGNIFICANCE OF EXTRALUMINAL ABDOMINAL GAS: LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL SCBT/MR 2012 October 26,
INVESTIGATIONS OF GASTROINTESTINAL DISEAS
 INVESTIGATIONS OF GASTROINTESTINAL DISEAS Lecture 1 and 2 دز اسماعيل داود فرع الطب كلية طب الموصل Radiological tests of structure (imaging) Plain X-ray: May shows soft tissue outlines like liver, spleen,
INVESTIGATIONS OF GASTROINTESTINAL DISEAS Lecture 1 and 2 دز اسماعيل داود فرع الطب كلية طب الموصل Radiological tests of structure (imaging) Plain X-ray: May shows soft tissue outlines like liver, spleen,
Imaging of Biliary Tract Emergencies in Jorge A. Soto, MD Professor of Radiology Boston University Medical Center.
 Imaging of Biliary Tract Emergencies in 2011 Jorge A. Soto, MD Professor of Radiology Boston University Medical Center Introduction Biliary emergencies are: Common Come in many flavors Deceiving: frequent
Imaging of Biliary Tract Emergencies in 2011 Jorge A. Soto, MD Professor of Radiology Boston University Medical Center Introduction Biliary emergencies are: Common Come in many flavors Deceiving: frequent
Together, putting patients first
 The Role of a Gastroenterologist in the Diagnosis and Management of Pancreatic Cancer Sarah Jowett, Consultant Gastroenterologist Bradford Teaching Hospitals Trust Leeds Regional Study Day, 12 September
The Role of a Gastroenterologist in the Diagnosis and Management of Pancreatic Cancer Sarah Jowett, Consultant Gastroenterologist Bradford Teaching Hospitals Trust Leeds Regional Study Day, 12 September
DIGESTIVE SYSTEM SURGICAL PROCEDURES December 22, 2015 (effective March 1, 2016) INTESTINES (EXCEPT RECTUM) Asst Surg Anae
 INTESTINES (EXCEPT RECTUM) Asst Surg Anae") December 22, 2015 (effective March 1, 201) INTESTINES (EXCEPT RECTUM) Z513 Hydrostatic - Pneumatic dilatation of colon stricture(s) through colonoscope... 10.50 Z50 Fulguration of first polyp through colonoscope...
December 22, 2015 (effective March 1, 201) INTESTINES (EXCEPT RECTUM) Z513 Hydrostatic - Pneumatic dilatation of colon stricture(s) through colonoscope... 10.50 Z50 Fulguration of first polyp through colonoscope...
Quality Measures In Colonoscopy: Why Should I Care?
 Quality Measures In Colonoscopy: Why Should I Care? David Greenwald, MD, FASGE Professor of Clinical Medicine Albert Einstein College of Medicine Montefiore Medical Center Bronx, New York ACG/ASGE Best
Quality Measures In Colonoscopy: Why Should I Care? David Greenwald, MD, FASGE Professor of Clinical Medicine Albert Einstein College of Medicine Montefiore Medical Center Bronx, New York ACG/ASGE Best
Making ERCP Easy: Tips From A Master
 Making ERCP Easy: Tips From A Master Raj J. Shah, M.D., FASGE Associate Professor of Medicine University of Colorado School of Medicine Co-Director, Endoscopy Director, Pancreaticobiliary Endoscopy Services
Making ERCP Easy: Tips From A Master Raj J. Shah, M.D., FASGE Associate Professor of Medicine University of Colorado School of Medicine Co-Director, Endoscopy Director, Pancreaticobiliary Endoscopy Services
USMLE and COMLEX II. CE / CK Review. General Surgery. 1. Northwestern Medical Review
 USMLE and COMLEX II CE / CK Review General Surgery 1. Northwestern Medical Review Northwestern Medical Review www.northwesternmedicalreview.com Lansing, Michigan 2014-2015 Acute Abdomen 1. Your patient
USMLE and COMLEX II CE / CK Review General Surgery 1. Northwestern Medical Review Northwestern Medical Review www.northwesternmedicalreview.com Lansing, Michigan 2014-2015 Acute Abdomen 1. Your patient
Surgical Management of IBD. Val Jefford Grand Rounds October 14, 2003
 Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
General Data. 王 X 村 78 y/o 男性
 General Data 王 X 村 78 y/o 男性 Chief Complaint Vomiting twice this early morning Fever up to 38.9ºC was noted Present Illness (1) Old CVA with left side weakness for more than 10 years and with bed ridden
General Data 王 X 村 78 y/o 男性 Chief Complaint Vomiting twice this early morning Fever up to 38.9ºC was noted Present Illness (1) Old CVA with left side weakness for more than 10 years and with bed ridden
Simon Everett. Consultant Gastroenterologist, SJUH, Leeds. if this is what greets you in the morning, you probably need to go see a doctor
 Simon Everett Consultant Gastroenterologist, SJUH, Leeds if this is what greets you in the morning, you probably need to go see a doctor Presentation Audit data and mortality NICE guidance Risk assessment
Simon Everett Consultant Gastroenterologist, SJUH, Leeds if this is what greets you in the morning, you probably need to go see a doctor Presentation Audit data and mortality NICE guidance Risk assessment
Frequently Asked Questions
 Frequently Asked Questions I. Questions about your Medications II. Questions about your Prep III. Questions about your Escort IV. Pre-Procedure Questions V. Post-Procedure Questions I. Questions About
Frequently Asked Questions I. Questions about your Medications II. Questions about your Prep III. Questions about your Escort IV. Pre-Procedure Questions V. Post-Procedure Questions I. Questions About
What Are Gallstones? GALLSTONES. Gallstones are pieces of hard, solid matter that form over time in. the gallbladder of some people.
 What Are Gallstones? Gallstones are pieces of hard, solid matter that form over time in the gallbladder of some people. The gallbladder sits under the liver and stores bile (a key digestive juice ). Gallstones
What Are Gallstones? Gallstones are pieces of hard, solid matter that form over time in the gallbladder of some people. The gallbladder sits under the liver and stores bile (a key digestive juice ). Gallstones
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute variceal bleeding management of, 251 262 balloon tamponade of esophagus in, 257 258 endoscopic therapies in, 255 257. See also Endoscopy,
Index Note: Page numbers of article titles are in boldface type. A Acute variceal bleeding management of, 251 262 balloon tamponade of esophagus in, 257 258 endoscopic therapies in, 255 257. See also Endoscopy,
PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE. PRESENTED BY: Susan DePasquale, CGRN, MSN
 PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE PRESENTED BY: Susan DePasquale, CGRN, MSN Pancreatic Fluid Collection (PFC) A result of pancreatic duct (PD) and side branch disruption,
PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE PRESENTED BY: Susan DePasquale, CGRN, MSN Pancreatic Fluid Collection (PFC) A result of pancreatic duct (PD) and side branch disruption,
Having a Stent Placed at ERCP
 Having a Stent Placed at ERCP Information for patients, relatives and carers This information leaflet should be read in conjunction with the ERCP information booklet (ref PIL 78) Endoscopy Unit For more
Having a Stent Placed at ERCP Information for patients, relatives and carers This information leaflet should be read in conjunction with the ERCP information booklet (ref PIL 78) Endoscopy Unit For more
Tools of the Gastroenterologist: Introduction to GI Endoscopy
 Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Radiology of hepatobiliary diseases
 GI cycle - Lecture 14 436 Teams Radiology of hepatobiliary diseases Objectives 1. To Interpret plan x-ray radiograph of abdomen with common pathologies. 2. To know the common pathologies presentation.
GI cycle - Lecture 14 436 Teams Radiology of hepatobiliary diseases Objectives 1. To Interpret plan x-ray radiograph of abdomen with common pathologies. 2. To know the common pathologies presentation.
Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter
 Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter KC 59 year old male Referred to Surgery clinic for incidentally discovered 5cm x 3cm pancreatic
Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter KC 59 year old male Referred to Surgery clinic for incidentally discovered 5cm x 3cm pancreatic
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #10 Acute GI Bleeds
 McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #10 Acute GI Bleeds Gastrointestinal bleeding is a very common problem in emergency medicine. Between
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #10 Acute GI Bleeds Gastrointestinal bleeding is a very common problem in emergency medicine. Between
Radiology of the abdomen Lecture -1-
 Radiology of the abdomen Lecture -1- Objectives To know radiology modalities used in abdomen imaging mainly GI tract. To know advantages and disadvantages of each modality. To know indications and contraindications
Radiology of the abdomen Lecture -1- Objectives To know radiology modalities used in abdomen imaging mainly GI tract. To know advantages and disadvantages of each modality. To know indications and contraindications
Nursing Care & Management of the Pre-Liver Transplant Population. Christine Kiamzon, RN, MSN, PCCN 8 North Educator
 Nursing Care & Management of the Pre-Liver Transplant Population Christine Kiamzon, RN, MSN, PCCN 8 North Educator Objectives 1. Identify key nursing interventions in caring for pre-transplant ESLD patients.
Nursing Care & Management of the Pre-Liver Transplant Population Christine Kiamzon, RN, MSN, PCCN 8 North Educator Objectives 1. Identify key nursing interventions in caring for pre-transplant ESLD patients.
Nursing Care & Management of the Pre-Liver Transplant Population
 Nursing Care & Management of the Pre-Liver Transplant Population Christine Kiamzon, RN, MSN, PCCN 8 North Educator Objectives 1. Identify key nursing interventions in caring for pre-transplant ESLD patients.
Nursing Care & Management of the Pre-Liver Transplant Population Christine Kiamzon, RN, MSN, PCCN 8 North Educator Objectives 1. Identify key nursing interventions in caring for pre-transplant ESLD patients.
LAPAROSCOPIC APPENDICECTOMY
 LAPAROSCOPIC APPENDICECTOMY WHAT IS THE APPENDIX? The appendix is a small, fingerlike pouch of the intestinal tract located where the small and large join. It has no known use. It is postulated that the
LAPAROSCOPIC APPENDICECTOMY WHAT IS THE APPENDIX? The appendix is a small, fingerlike pouch of the intestinal tract located where the small and large join. It has no known use. It is postulated that the
stents she/he is providing appropriate or inappropriate care?
 Pancreatic Stents Are They Now State of the Art Care? To Help Limit Post ERCP Pancreatitis Glen A. Lehman, M.D. Professor of Medicine and Radiology Division of Gastroenterology/Hepatology Indiana University
Pancreatic Stents Are They Now State of the Art Care? To Help Limit Post ERCP Pancreatitis Glen A. Lehman, M.D. Professor of Medicine and Radiology Division of Gastroenterology/Hepatology Indiana University
What is a Colonoscopy?
 What is a Colonoscopy? A colonoscopy is a test to look inside your colon. A colonoscopy is done by a gastroenterologist, a doctor trained in looking at the gastrointestinal (GI) tract. The main tool used
What is a Colonoscopy? A colonoscopy is a test to look inside your colon. A colonoscopy is done by a gastroenterologist, a doctor trained in looking at the gastrointestinal (GI) tract. The main tool used
Clinical Questions. Clinical Questions. Clinical Questions. Health-Process-Evidencebased Clinical Practice Guidelines Acute Abdomen
 Health-Process-Evidencebased Clinical Practice Guidelines Acute Abdomen 1. What is an operational concept of acute abdomen? any abdominal condition of acute onset from various causes involving the intraabdominal
Health-Process-Evidencebased Clinical Practice Guidelines Acute Abdomen 1. What is an operational concept of acute abdomen? any abdominal condition of acute onset from various causes involving the intraabdominal
LIVER CIRRHOSIS. The liver extracts nutrients from the blood and processes them for later use.
 LIVER CIRRHOSIS William Sanchez, M.D. & Jayant A. Talwalkar, M.D., M.P.H. Advanced Liver Disease Study Group Miles and Shirley Fiterman Center for Digestive Diseases Mayo College of Medicine Rochester,
LIVER CIRRHOSIS William Sanchez, M.D. & Jayant A. Talwalkar, M.D., M.P.H. Advanced Liver Disease Study Group Miles and Shirley Fiterman Center for Digestive Diseases Mayo College of Medicine Rochester,
The ABC s of Chest Trauma
 The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries