MANAGEMENT OF PYOGENIC LIVER ABSCESS BOYOUNG SONG, M.D. SUNY DOWNSTATE SURGERY 11/7/13
|
|
|
- Charity Fowler
- 5 years ago
- Views:
Transcription


1 MANAGEMENT OF PYOGENIC LIVER ABSCESS BOYOUNG SONG, M.D. SUNY DOWNSTATE SURGERY 11/7/13
2 CASE THE PATIENT IS A 79 YEAR OLD MALE WITH 3 DAY HISTORY OF LOWER ABDOMINAL PAIN, NAUSEA WITHOUT VOMITING, CHILLS AND WATERY BOWEL MOVEMENTS. FATIGUE AND SIGNIFICANT WEIGHT LOSS OF ~40LBS OVER 4 MONTHS.
3 CASE PMHX: ALZHEIMER S DEMENTIA, HTN, DM, CKD PSHX: NONE HOME MEDICATIONS: ENALAPRIL, NIFEDIPINE, JANUVIA, SIMVASTATIN, MEMANTINE SOCHX: LIVES AT PANAMA AND US, OCCASIONAL ETOH, NO DRUGS NKDA
4 CASE PHYSICAL EXAM F 91/ % ON RA AWAKE AND AROUSABLE, NAD S1S2 RRR CTA B/L SOFT ABDOMEN, NONDISTENDED, TENDER TO PALPATION IN UPPER QUADRANTS NEGATIVE FOR GUARDING OR REBOUND GUIAIC NEGATIVE
5 CASE LABORATORY WORK CBC 5.17 > 10.5/33.4 < 235 BANDEMIA 9% BMP 133 / 4.2 / 91 / 18 / 99 / 3.9 < 221 LFT 7 / 3.3 / 298 / 212 / 149 / 1 LACTATE 1.6

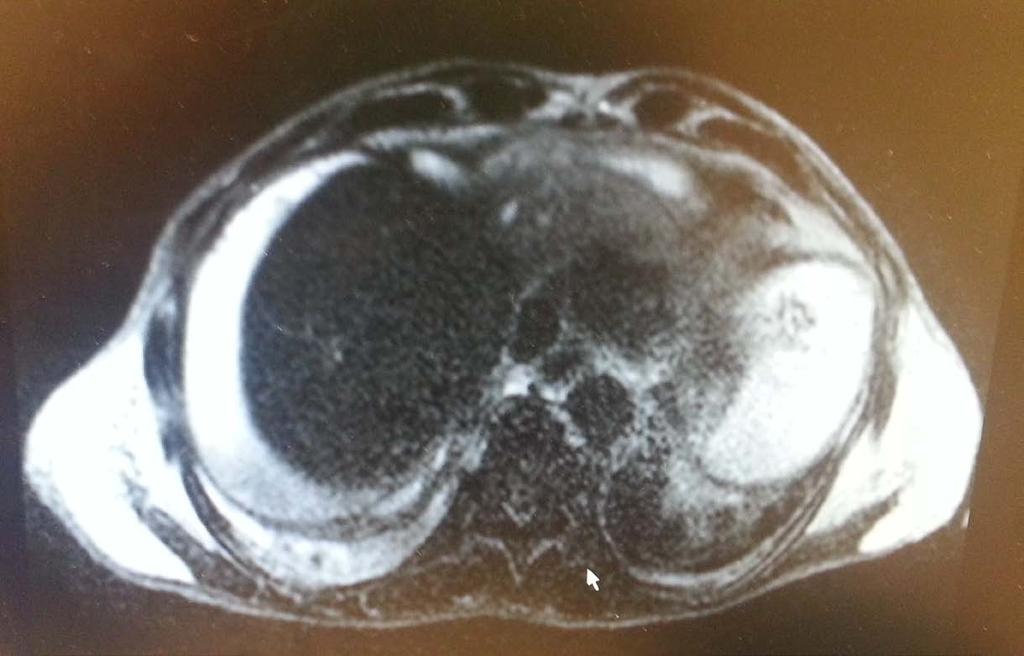
6 CASE CT LARGE HETEROGENEOUS MASS OCCUPYING MOST OF LEFT LOBE, MAY REPRESENT ABSCESS.

7 CASE CT LARGE HETEROGENEOUS MASS OCCUPYING MOST OF LEFT LOBE, MAY REPRESENT ABSCESS.
8 CASE ABDOMINAL SONOGRAM COMPLEX COLLECTION IN LEFT LOBE MEASURING 10CM X 11CM X 12CM A 5.5MM GALLSTONE AND SLUDGE IN GALLBLADDER NO GB WALL THICKNESS NO CBD DILATATION
9 CASE HOSPITAL DAY #0: ADMISSION TO SICU IV HYDRATION IV ANTIBIOTICS (FLAGYL AND CEFTRIAXONE) STARTED HOSPITAL DAY #1: IR DRAINAGE OF ABSCESS MICROBIOLOGY: BLOOD CULTURE AND ABSCESS CULTURE GROUP F STREPTOCOCCUS

10 CASE
11 CASE HOSPITAL DAY #2 4: WBC TRENDING UP WITH SIGNIFICANT BANDEMIA (25-66%) T. BILI TRENDING UP 3.4 DRAINAGE OUTPUT BILIOUS HOSPITAL DAY #5: MRCP
12 CASE

13 CASE FREE FLUID IN ABDOMINAL CAVITY INTENSE PERITONEAL ENHANCEMEN T SUGGESTIVE OF BILE PERITONITIS
14 CASE HOSPITAL DAY #6: IR DRAINAGE OF RIGHT GUTTER COLLECTION ~500ML OF PURULENCE DRAINED HOSPITAL DAY #7: ON TUBE FEEDS, WBC LATERAL BUT BANDEMIA IMPROVED HOSPITAL DAY #8: MORE DISTENDED AND TACHYCARDIC, OR FOR WASHOUT
15 CASE OPERATIVE FINDINGS MULTIPLE ABSCESSES IN THE PERIHEPATIC, PERICOLIC, PELVIC, AND INTERLOOP AREAS ~800ML OF PURULENT FLUID SUCTIONED THREE 10FR JACKSON PRATT DRAINS LEFT NO EVIDENCE OF DIVERTICULITIS AND APPENDICITIS OPERATION LAPAROSCOPIC WASHOUT AND PLACEMENT OF DRAINS
16 CASE POST OP COURSE EXTUBATED ON POST OP DAY #1 HEMODYNAMICALLY STABLE AND STORY CONTINUES

17 ?
18 PYOGENIC LIVER ABSCESS EPIDEMIOLOGY ANATOMY ETIOLOGY PRESENTATION DIAGNOSIS TREATMENT
19 EPIDEMIOLOGY INCIDENCE 2.3 PER 100,000 HISTORICALLY SEEN IN YOUNGER PATIENTS WITH APPENDICITIS CURRENTLY SEEN MORE IN ELDERLY, DEBILITATED POPULATION WITH UNDERLYING MALIGNANCY IN GI/BILIARY TRACT MORTALITY RATE CAN BE UP TO 10-20% IN PATIENTS WITH MULTIPLE COMORBIDITIES
20 ANATOMY
21 ANATOMY
22 ANATOMY

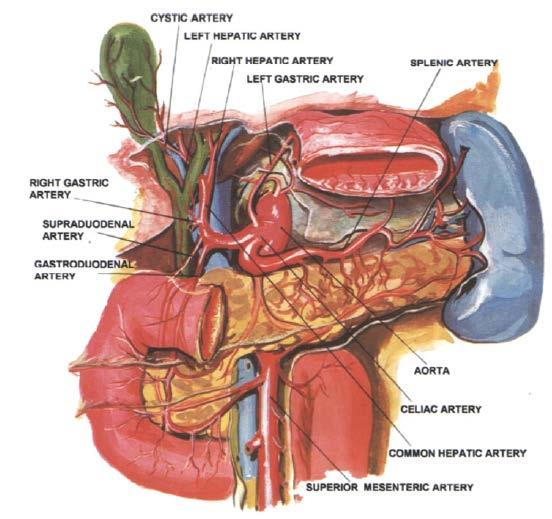
23 ANATOMY BLOOD SUPPLY TO LIVER 75% BLOOD FLOW FROM PORTAL VEIN 25% BLOOD FLOW FROM HEPATIC ARTERY
24 ETIOLOGY HEPATOBILIARY CHOLECYSTITI S ASCENDING CHOLANGITIS MALIGNANCY STRICTURES
25 ETIOLOGY HEPATOBILIARY CHOLECYSTITI S ASCENDING CHOLANGITIS MALIGNANCY STRICTURES GI VIA PORTAL APPENDICITIS DIVERTICULITIS INTESTINAL PERFORATION ANORECTAL SUPPURATION MALIGNANCY INFLAMMATORY BOWEL DISEASE
26 ETIOLOGY HEPATOBILIARY CHOLECYSTITI S ASCENDING CHOLANGITIS MALIGNANCY STRICTURES GI VIA PORTAL APPENDICITIS DIVERTICULITIS INTESTINAL PERFORATION ANORECTAL SUPPURATION MALIGNANCY INFLAMMATORY BOWEL DISEASE ARTERIAL VIA HA ENDOCARDITIS VASCULAR SEPSIS ENT, DENTAL INFECTION IVDA
27 ETIOLOGY TRAUMATIC BLUNT/PENETRATI NG ABDOMINAL TRAUMA LIVER INSTRUMENTATIO N (TACE, RFA, ETHANOL INJECTION)
28 ETIOLOGY TRAUMATIC BLUNT/PENETRATI NG ABDOMINAL TRAUMA LIVER INSTRUMENTATIO N (TACE, RFA, ETHANOL INJECTION) ADJACENT ABDOMINAL PATHOLOGY GASTRODUODENA L PERFORATION ACUTE CHOLECYSTITIS COLONIC PERFORATION
29 ETIOLOGY TRAUMATIC BLUNT/PENETRATI NG ABDOMINAL TRAUMA LIVER INSTRUMENTATIO N (TACE, RFA, ETHANOL INJECTION) ADJACENT ABDOMINAL PATHOLOGY GASTRODUODENA L PERFORATION ACUTE CHOLECYSTITIS COLONIC PERFORATION CRYPTOGENIC 40-67% OF THE CASES
30 ETIOLOGY MICROBIOLOGY OFTEN REFLECT THE SOURCE OF INFECTION GI/BILIARY TRACT POLYMICROBIAL (GRAM NEGATIVES AND ANAEROBES) HEMATOGENOUS SPREAD MONOMICROBIAL (STAPH OR STREPT) MOST COMMON E.COLI, STREPTOCOCCUS, KLEBSIELLA, ENTEROCOCCUS OTHERS PSEUDOMONAS, CLOSTRIDIUM, BACTEROIDES, STAPH
31 PRESENTATION FEVER 70-90% RIGHT UPPER QUADRANT PAIN CHILLS ANOREXIA WEIGHT LOSS MALAISE JAUNDICE
32 PRESENTATION FEVER RIGHT UPPER QUADRANT PAIN CHILLS ANOREXIA WEIGHT LOSS MALAISE JAUNDICE NO DIFFERENCE IN PRESENTING SYMPTOMS BETWEEN PATIENTS WITH SINGLE AND MULTIPLE LIVER ABSCESS
33 DIAGNOSIS LABORATORY FINDINGS LEUKOCYTOSIS 70% ELEVATED LFTS 50% SONOGRAM CT MRI/MRCP
34 TREATMENT GOALS OF THERAPY 1. COMPLETE DRAINAGE OF PUS AND INFECTED DEBRIS 2. INITIATION OF APPROPRIATE ANTIBIOTICS 3. IDENTIFICATION AND RESOLUTION OF UNDERLYING CAUSE
35 TREATMENT FACTORS LINKED TO MORTALITY EFFUSION HIGH ASA SCORE UNDERLYING MALIGNANCY PRESENCE OF PLEURAL SEPTIC SHOCK INCREASED CREATININE LOW ALBUMIN
36 TREATMENT ANTIBIOTICS EMPIRIC, BROAD SPECTRUM INTRAVENOUS ANTIBIOTICS AFTER BLOOD CULTURE ADEQUATE GRAM NEGATIVE AND ANAEROBIC COVERAGE ADJUST ABX ONCE CULTURES ARE RESULTED SHOULD BE GIVEN FOR 4-6 WEEKS

37 TREATMENT PERCUTANEOUS DRAINAGE IS STANDARD OF CARE BENEFITS AVOID GENERAL ANESTHESIA LESS INVASIVE
38 TREATMENT PERCUTANEOUS DRAINAGE IS STANDARD OF CARE BENEFITS AVOID GENERAL ANESTHESIA LESS INVASIVE LIMITATIONS SMALLERABSCESS MULTIPLE OR MULTI LOCULATED ABSCESS FAILURE RATE 15-30% MAY NOT BE ADEQUATE FOR THICK PUS OVERDISTENSION OF ABSCESS CAVITY
39 TREATMENT WHEN DO WE OPERATE? FAILURE OF PERCUTANEOUS DRAINAGE INTRAPERITONEAL RUPTURE OF ABSCESS CAUSING PERITONITIS UNDERLYING PATHOLOGY NEEDS SURGICAL INTERVENTION
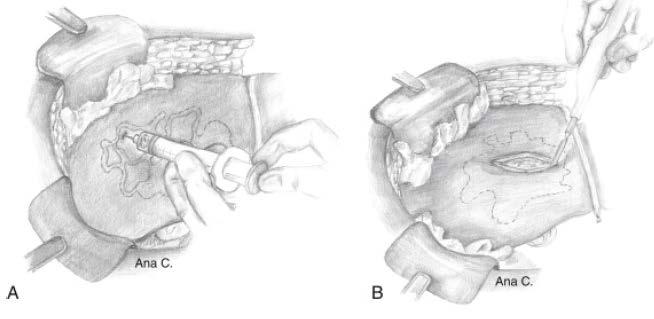
40 TREATMENT
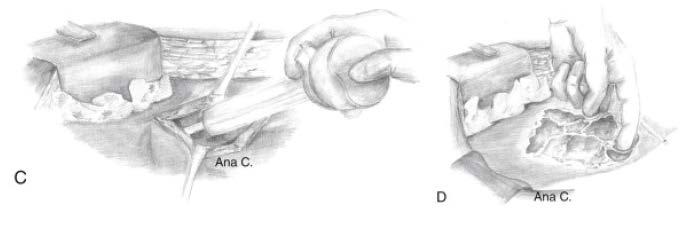
41 TREATMENT

42 TREATMENT HEPATIC RESECTION ONGOING UNCONTROLLED SEPSIS MULTILOCULATED ABSCESS PARENCHYMAL DESTRUCTION INFECTED OR NECROTIC TUMOR LONG STANDING BILIARY OBSTRUCTION

43 TREATMENT
44 TAKE HOME MESSAGES 1. PYOGENIC LIVER ABSCESS CAN BE FATAL IF DIAGNOSIS AND TREATMENT IS DELAYED 2. COMBINATION OF PERCUTANEOUS DRAINAGE AND IV ANTIBIOTICS IS THE FIRST LINE OF TREATMENT 3. SURGICAL DRAINAGE IS RESERVED FOR FAILED PERCUTANEOUS DRAINAGE 4. HEPATIC RESECTION MAY BE NECESSARY FOR SOME PATIENTS WHO CONTINUE TO HAVE ONGOING SEPSIS

45 THANK YOU
46 REFERENCES JARNAGIN & BLUMGART: BLUMGART S SURGERY OF THE LIVER, PANCREAS AND BILIARY TRACT 5 TH ED. CHAPTER 66 PYOGENIC LIVER ABSCESS GREENFIELDS SURGERY SCIENTIFIC PRINCIPLES AND PRACTICE. CHAPTER 57 HEPATIC INFECTION BARISH, E. HEPATIC ABSCESS. CURRENT SURGICAL THERAPY, 10 TH EDITION MEDDINGS, L., ET AL. A POPULATION BASED STUDY OF PYOGENIC LIVER ABSCESSES IN THE US. AM J GASTROENTEROL 2010; 105: ; DOI: /AJG ; PUBLISHED ONLINE 3 NOVEMBER 2009 PANG TCY, FUNG T, SAMRA J, HUGH TJ, SMITH RC. PYOGENIC LIVER ABSCESS: AN AUDIT OF 10 YEARS EXPERIENCE. WORLD J GASTROENT 2011; 17(12): STRONG, R., ET AL. HEPATECTOMY FOR PYOGENIC LIVE R ABSCESS. HPB 2003;5(2):86-90 ALKOFER, B., ET AL. ARE PYOGENIC LIVER ABSCESSES STILL A SURGICAL CONCERN? A WESTERN EXPERIENCE. HPB SURGERY 2012, VOLUME 2012
Disclosures. Extra-hepatic Biliary Disease and the Pancreas. Objectives. Pancreatitis 10/3/2018. No relevant financial disclosures to report
 Extra-hepatic Biliary Disease and the Pancreas Disclosures No relevant financial disclosures to report Jeffrey Coughenour MD FACS Clinical Associate Professor of Surgery and Emergency Medicine Division
Extra-hepatic Biliary Disease and the Pancreas Disclosures No relevant financial disclosures to report Jeffrey Coughenour MD FACS Clinical Associate Professor of Surgery and Emergency Medicine Division
3/22/2011. Inflammatory Bowel Disease. Inflammatory Bowel Disease Objectives: Appendicitis. Lemone and Burke Chapter 26
 Inflammatory Bowel Disease Lemone and Burke Chapter 26 Inflammatory Bowel Disease Objectives: Discuss etiology, patho and clinical manifestations of Appendicitis Peritonitis Ulcerative Colitis Crohn s
Inflammatory Bowel Disease Lemone and Burke Chapter 26 Inflammatory Bowel Disease Objectives: Discuss etiology, patho and clinical manifestations of Appendicitis Peritonitis Ulcerative Colitis Crohn s
GASTRO-INTESTINAL TRACT INFECTIONS - ANTIMICROBIAL MANAGEMENT
 GASTRO-INTESTINAL TRACT INFECTIONS - ANTIMICROBIAL MANAGEMENT Name & Title Of Author: Dr Linda Jewes, Consultant Microbiologist Date Amended: December 2016 Approved by Committee/Group: Drugs & Therapeutics
GASTRO-INTESTINAL TRACT INFECTIONS - ANTIMICROBIAL MANAGEMENT Name & Title Of Author: Dr Linda Jewes, Consultant Microbiologist Date Amended: December 2016 Approved by Committee/Group: Drugs & Therapeutics
Types of peritonitis and management. J olita Augus te, PGY-5 SUNY Downs tate Grand Rounds 11/3/2016
 Types of peritonitis and management J olita Augus te, PGY-5 SUNY Downs tate Grand Rounds 11/3/2016 Case Presentation xx year old patient presents to ED with complaints of one day of abdominal pain s ince
Types of peritonitis and management J olita Augus te, PGY-5 SUNY Downs tate Grand Rounds 11/3/2016 Case Presentation xx year old patient presents to ED with complaints of one day of abdominal pain s ince
Perforation of a Duodenal Diverticulum. Elective Student S. C.
 Perforation of a Duodenal Diverticulum 2008 4 Elective Student S. C. Case History An elderly male presented to the Emergency Department with abdominal pain. Chief Complaint: Worsening, diffuse abdominal
Perforation of a Duodenal Diverticulum 2008 4 Elective Student S. C. Case History An elderly male presented to the Emergency Department with abdominal pain. Chief Complaint: Worsening, diffuse abdominal
LIVER SURGERY 2. Case 1. Med 5 Refresher Course (Surgery) 2013/14. Dr Sunny Cheung
 2013/14. Dr Sunny Cheung") LIVER SURGERY 2 Med 5 Refresher Course (Surgery) 2013/14 24 Jun 2013 Dr Sunny Cheung Case 1 50/M Sudden onset of epigastric pain Abdominal distension Confused HR 120 BP 80/50 Haemocue = 8 What should you
LIVER SURGERY 2 Med 5 Refresher Course (Surgery) 2013/14 24 Jun 2013 Dr Sunny Cheung Case 1 50/M Sudden onset of epigastric pain Abdominal distension Confused HR 120 BP 80/50 Haemocue = 8 What should you
Abdominal Pain. Luke Donnelly, MD Emergency Medicine
 Abdominal Pain Luke Donnelly, MD Emergency Medicine Objectives Approach to abdominal pain Evaluation Critical diagnoses and treatments Abdominal Pain Most Common ER Complaint Broad Differential Can often
Abdominal Pain Luke Donnelly, MD Emergency Medicine Objectives Approach to abdominal pain Evaluation Critical diagnoses and treatments Abdominal Pain Most Common ER Complaint Broad Differential Can often
Surgical Management of IBD. Val Jefford Grand Rounds October 14, 2003
 Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
The EM Educator Series
 The EM Educator Series The EM Educator Series: Why is my patient with gallbladder pathology so sick? Author: Alex Koyfman, MD (@EMHighAK) // Edited by: Brit Long, MD (@long_brit) and Manpreet Singh, MD
The EM Educator Series The EM Educator Series: Why is my patient with gallbladder pathology so sick? Author: Alex Koyfman, MD (@EMHighAK) // Edited by: Brit Long, MD (@long_brit) and Manpreet Singh, MD
Appendix 5. EFSUMB Newsletter. Gastroenterological Ultrasound
 EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
Post-Operative Chylous Ascites. David Kashan, PGY-4 Richmond University Medical Center 7/30/15
 Post-Operative Chylous Ascites David Kashan, PGY-4 Richmond University Medical Center 7/30/15 HPI Patient is a 76 year old female p/w one day of worsening abdominal pain, +N/V, fevers and chills HPI PMHx:
Post-Operative Chylous Ascites David Kashan, PGY-4 Richmond University Medical Center 7/30/15 HPI Patient is a 76 year old female p/w one day of worsening abdominal pain, +N/V, fevers and chills HPI PMHx:
Management of Cholangiocarcinoma. Roseanna Lee, MD PGY-5 Kings County Hospital
 Management of Cholangiocarcinoma Roseanna Lee, MD PGY-5 Kings County Hospital Case Presentation 37 year old male from Yemen presented with 2 week history of epigastric pain, anorexia, jaundice and puritis.
Management of Cholangiocarcinoma Roseanna Lee, MD PGY-5 Kings County Hospital Case Presentation 37 year old male from Yemen presented with 2 week history of epigastric pain, anorexia, jaundice and puritis.
12 Blueprints Q&A Step 2 Surgery
 12 Blueprints Q&A Step 2 Surgery 34. A 40-year-old female has been referred to you for a recent ER and hospital admission, from which she was given a diagnosis of acute diverticulitis. Treatment at that
12 Blueprints Q&A Step 2 Surgery 34. A 40-year-old female has been referred to you for a recent ER and hospital admission, from which she was given a diagnosis of acute diverticulitis. Treatment at that
laparoscopic cholecystectomy
 Combined percutaneous and endoscopic approach in management of dropped gallstones following laparoscopic cholecystectomy John S.F. Shum 1*, K.H. Fung 1, George P.C. Yang 2, Chung Ngai Tang 2, Michael K.W.
Combined percutaneous and endoscopic approach in management of dropped gallstones following laparoscopic cholecystectomy John S.F. Shum 1*, K.H. Fung 1, George P.C. Yang 2, Chung Ngai Tang 2, Michael K.W.
GALLBLADDER CANCER. Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011
 GALLBLADDER CANCER Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011 Agenda Case Presentation Epidemiology Pathogenesis & Pathology Staging Presentation & Diagnosis Stage-wise Management Outcomes/Prognosis
GALLBLADDER CANCER Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011 Agenda Case Presentation Epidemiology Pathogenesis & Pathology Staging Presentation & Diagnosis Stage-wise Management Outcomes/Prognosis
ACG Clinical Guideline: Management of Acute Pancreatitis
 ACG Clinical Guideline: Management of Acute Pancreatitis Scott Tenner, MD, MPH, FACG 1, John Baillie, MB, ChB, FRCP, FACG 2, John DeWitt, MD, FACG 3 and Santhi Swaroop Vege, MD, FACG 4 1 State University
ACG Clinical Guideline: Management of Acute Pancreatitis Scott Tenner, MD, MPH, FACG 1, John Baillie, MB, ChB, FRCP, FACG 2, John DeWitt, MD, FACG 3 and Santhi Swaroop Vege, MD, FACG 4 1 State University
Imaging of liver and pancreas
 Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Study of post cholecystectomy biliary leakage and its management
 Original Research Article Study of post cholecystectomy biliary leakage and its management P. Krishna Kishore 1*, B. Manju Sruthi 2, G. Obulesu 3 1 Assistant Professor, Departmentment of General Surgery,
Original Research Article Study of post cholecystectomy biliary leakage and its management P. Krishna Kishore 1*, B. Manju Sruthi 2, G. Obulesu 3 1 Assistant Professor, Departmentment of General Surgery,
Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter
 Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter KC 59 year old male Referred to Surgery clinic for incidentally discovered 5cm x 3cm pancreatic
Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter KC 59 year old male Referred to Surgery clinic for incidentally discovered 5cm x 3cm pancreatic
LOKUN! I got stomach ache!
 LOKUN! I got stomach ache! Mr L is a 67year old Chinese gentleman who is a non smoker, social drinker. He has a medical history significant for Hypertension, Hyperlipidemia, Type 2 Diabetes Mellitus, Chronic
LOKUN! I got stomach ache! Mr L is a 67year old Chinese gentleman who is a non smoker, social drinker. He has a medical history significant for Hypertension, Hyperlipidemia, Type 2 Diabetes Mellitus, Chronic
Liver Abscess A scourge of the Tropics
 DOI: 10.7860/IJARS/2016/17457:2095 Surgery Section Original Article Liver Abscess A scourge of the Tropics SHARAD SETH, SEEMA SETH ABSTRACT Introduction: Liver abscess defined as a collection of pus within
DOI: 10.7860/IJARS/2016/17457:2095 Surgery Section Original Article Liver Abscess A scourge of the Tropics SHARAD SETH, SEEMA SETH ABSTRACT Introduction: Liver abscess defined as a collection of pus within
PSOAS ABSCESS. Dr Noman Ullah Wazir
 PSOAS ABSCESS Dr Noman Ullah Wazir Psoas Major muscle The psoas major is a long fusiform muscle located on the side of the lumbar region of the vertebral column and brim of the lesser pelvis. Psoas Major
PSOAS ABSCESS Dr Noman Ullah Wazir Psoas Major muscle The psoas major is a long fusiform muscle located on the side of the lumbar region of the vertebral column and brim of the lesser pelvis. Psoas Major
The Bile Duct (and Pancreas) and the Physician
 and the Physician") The Bile Duct (and Pancreas) and the Physician Javaid Iqbal Consultant in Gastroenterology and Pancreato-biliary Medicine University Hospital South Manchester Not so common?! Two weeks 38 ERCP s 20 15
The Bile Duct (and Pancreas) and the Physician Javaid Iqbal Consultant in Gastroenterology and Pancreato-biliary Medicine University Hospital South Manchester Not so common?! Two weeks 38 ERCP s 20 15
EAST MULTICENTER STUDY PROPOSAL
 EAST MULTICENTER STUDY PROPOSAL (Proposal forms must be completed in its entirety, incomplete forms will not be considered) GENERAL INFORMATION Study Title: Prospective Multi-Institutional Evaluation of
EAST MULTICENTER STUDY PROPOSAL (Proposal forms must be completed in its entirety, incomplete forms will not be considered) GENERAL INFORMATION Study Title: Prospective Multi-Institutional Evaluation of
Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010
 Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010 Case Presentation 30 y.o. woman with 2 weeks of RUQ abdominal
Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010 Case Presentation 30 y.o. woman with 2 weeks of RUQ abdominal
Cholelithiasis & cholecystitis
 1 Cholelithiasis & cholecystitis Dr. Muhammad Shamim FCPS (Pak), FACS (USA), FICS (USA) Assistant Professor, Dept. of Surgery College of Medicine, Prince Sattam bin Abdulaziz University Email: surgeon.shamim@gmail.com
1 Cholelithiasis & cholecystitis Dr. Muhammad Shamim FCPS (Pak), FACS (USA), FICS (USA) Assistant Professor, Dept. of Surgery College of Medicine, Prince Sattam bin Abdulaziz University Email: surgeon.shamim@gmail.com
Management of Gallbladder Disease
 Management of Gallbladder Disease Steven B. Johnson, MD, FACS, FCCM Professor and Chairman, Department of Surgery Program Director, Phoenix Integrated Surgical Residency University of Arizona College of
Management of Gallbladder Disease Steven B. Johnson, MD, FACS, FCCM Professor and Chairman, Department of Surgery Program Director, Phoenix Integrated Surgical Residency University of Arizona College of
A CASE REPORT OF SPONTANEOUS BILOMA - AN ENIGMATIC SURGICAL PROBLEM
 A CASE REPORT OF SPONTANEOUS BILOMA - AN ENIGMATIC SURGICAL PROBLEM *Sumanta Kumar Ghosh and Biswajit Mukherjee ESIC Medical College, Joka, Kolkata, India *Author for Correspondence ABSTRACT Occurrence
A CASE REPORT OF SPONTANEOUS BILOMA - AN ENIGMATIC SURGICAL PROBLEM *Sumanta Kumar Ghosh and Biswajit Mukherjee ESIC Medical College, Joka, Kolkata, India *Author for Correspondence ABSTRACT Occurrence
Early Klebsiella pneumoniae Liver Abscesses associated with Pylephlebitis Mimic
 Early Klebsiella pneumoniae Liver Abscesses associated with Pylephlebitis Mimic Hepatocellular Carcinoma Chih-Hao Shen, MD 3, Jung-Chung Lin, MD, PhD 2, Hsuan-Hwai Lin, MD 1, You-Chen Chao, MD 1, and Tsai-Yuan
Early Klebsiella pneumoniae Liver Abscesses associated with Pylephlebitis Mimic Hepatocellular Carcinoma Chih-Hao Shen, MD 3, Jung-Chung Lin, MD, PhD 2, Hsuan-Hwai Lin, MD 1, You-Chen Chao, MD 1, and Tsai-Yuan
Hepatobiliary Ultrasound Rimon Bengiamin, MD, RDMS Assistant Clinical Professor Director of Emergency Ultrasound UCSF Fresno. Objectives. Why?
 Hepatobiliary Ultrasound Rimon Bengiamin, MD, RDMS Assistant Clinical Professor Director of Emergency Ultrasound UCSF Fresno Objectives Discuss the goals of point-of-care biliary ultrasound Review the
Hepatobiliary Ultrasound Rimon Bengiamin, MD, RDMS Assistant Clinical Professor Director of Emergency Ultrasound UCSF Fresno Objectives Discuss the goals of point-of-care biliary ultrasound Review the
Severe β-lactam allergy. Alternative (use for mild-moderate β-lactam allergy) therapy
 therapy") Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
9/21/15. Joshua Pruitt, MD, FAAEM Medical Director, LifeGuard Air Ambulance Iowa PA Society Fall CME Conference September 29, 2015
 Unless they prove otherwise. ~Every ED attending ever Joshua Pruitt, MD, FAAEM Medical Director, LifeGuard Air Ambulance Iowa PA Society Fall CME Conference September 29, 2015 AAA with rupture Mesenteric
Unless they prove otherwise. ~Every ED attending ever Joshua Pruitt, MD, FAAEM Medical Director, LifeGuard Air Ambulance Iowa PA Society Fall CME Conference September 29, 2015 AAA with rupture Mesenteric
Liver Cancer (Hepatocellular Carcinoma or HCC) Overview
 Overview") Liver Cancer (Hepatocellular Carcinoma or HCC) Overview Recent advances in liver cancer care seek to address the rising incidence of liver cancer, which has steadily increased over the past three decades.
Liver Cancer (Hepatocellular Carcinoma or HCC) Overview Recent advances in liver cancer care seek to address the rising incidence of liver cancer, which has steadily increased over the past three decades.
Acute Abdomen. Nirav Patel MD, FACS Banner University Medical Center - Phoenix
 Acute Abdomen Nirav Patel MD, FACS Banner University Medical Center - Phoenix ? Diffuse periumbilical with localization to RLQ + Nausea, anorexia, fevers - Diarrhea, emesis Exacerbated by movement, bumps
Acute Abdomen Nirav Patel MD, FACS Banner University Medical Center - Phoenix ? Diffuse periumbilical with localization to RLQ + Nausea, anorexia, fevers - Diarrhea, emesis Exacerbated by movement, bumps
Complicated surgical infections
 Complicated surgical infections JASLYN DOSHI ID ADVANCED TRAINEE, WESTMEAD HOPC 46 F admitted 13 th March 2017 Epigastric pain Vomiting Diarrhoea Background Gastric banding 2009 Vomiting since last year
Complicated surgical infections JASLYN DOSHI ID ADVANCED TRAINEE, WESTMEAD HOPC 46 F admitted 13 th March 2017 Epigastric pain Vomiting Diarrhoea Background Gastric banding 2009 Vomiting since last year
Iatrogenic Duodenal Injuries. Downstate Medical Center July 25 th, 2013 David Vivas, MD
 Iatrogenic Duodenal Injuries Downstate Medical Center July 25 th, 2013 David Vivas, MD History Case 71 y/o female who was seen by her PMD c/o 2 h/o RUQ pain radiated to the back. Patient denied fevers,
Iatrogenic Duodenal Injuries Downstate Medical Center July 25 th, 2013 David Vivas, MD History Case 71 y/o female who was seen by her PMD c/o 2 h/o RUQ pain radiated to the back. Patient denied fevers,
RECURRENT PYOGENIC CHOLANGITIS
 RECURRENT PYOGENIC CHOLANGITIS Resident(s): Evan Raff, MD MHA Attending(s): Narasimham Dasika, MD Program/Dept(s): University of Michigan Health System, Department of Radiology CHIEF COMPLAINT & HPI Chief
RECURRENT PYOGENIC CHOLANGITIS Resident(s): Evan Raff, MD MHA Attending(s): Narasimham Dasika, MD Program/Dept(s): University of Michigan Health System, Department of Radiology CHIEF COMPLAINT & HPI Chief
Christopher Lau Kings County Hospital SUNY Downstate Medical Center February 24, 2011
 Christopher Lau Kings County Hospital SUNY Downstate Medical Center February 24, 2011 37 year old male presented with 1 day history of abdominal pain Pain was diffuse but worst in the epigastric area No
Christopher Lau Kings County Hospital SUNY Downstate Medical Center February 24, 2011 37 year old male presented with 1 day history of abdominal pain Pain was diffuse but worst in the epigastric area No
Surgical conditions of liver Somkit Mingphruedhi, M.D.
 Surgical conditions of liver Somkit Mingphruedhi, M.D. Division of HPB Surgery, Department of Surgery Ramathibodi Hospital Anatomy IVC Portal Vein Hepatic Artery Splenic Vein Gallbladder CBD SMV Anatomy
Surgical conditions of liver Somkit Mingphruedhi, M.D. Division of HPB Surgery, Department of Surgery Ramathibodi Hospital Anatomy IVC Portal Vein Hepatic Artery Splenic Vein Gallbladder CBD SMV Anatomy
Cholangiocarcinoma (Bile Duct Cancer)
") Cholangiocarcinoma (Bile Duct Cancer) The Bile Duct System (Biliary Tract) A network of bile ducts (tubes) connects the liver and the gallbladder to the small intestine. This network begins in the liver
Cholangiocarcinoma (Bile Duct Cancer) The Bile Duct System (Biliary Tract) A network of bile ducts (tubes) connects the liver and the gallbladder to the small intestine. This network begins in the liver
Correspondence should be addressed to Justin Cochrane;
 Case Reports in Gastrointestinal Medicine Volume 2015, Article ID 794282, 4 pages http://dx.doi.org/10.1155/2015/794282 Case Report Acute on Chronic Pancreatitis Causing a Highway to the Colon with Subsequent
Case Reports in Gastrointestinal Medicine Volume 2015, Article ID 794282, 4 pages http://dx.doi.org/10.1155/2015/794282 Case Report Acute on Chronic Pancreatitis Causing a Highway to the Colon with Subsequent
GENERAL SURGERY FOR SMART PEOPLE JOE NOLD MD, FACS WICHITA SURGICAL SPECIALISTS
 GENERAL SURGERY FOR SMART PEOPLE JOE NOLD MD, FACS WICHITA SURGICAL SPECIALISTS CONFLICTS/DECLARATIONS I have no financial conflicts or declarations I AM always willing to see a consult for you TEXT TOPICS
GENERAL SURGERY FOR SMART PEOPLE JOE NOLD MD, FACS WICHITA SURGICAL SPECIALISTS CONFLICTS/DECLARATIONS I have no financial conflicts or declarations I AM always willing to see a consult for you TEXT TOPICS
Early management of complicated gallstones and acute pancreatitis
 Early management of complicated gallstones and acute pancreatitis A/Prof Richard Cade George Kalogeropoulos ( Fellow) HPB/Upper GI Unit Eastern Health, Melbourne biliary colic/acute cholecystitis common
Early management of complicated gallstones and acute pancreatitis A/Prof Richard Cade George Kalogeropoulos ( Fellow) HPB/Upper GI Unit Eastern Health, Melbourne biliary colic/acute cholecystitis common
Table 0: Description of Grading System for Anatomic Severity of Disease in Emergency. Local disease confined to the organ with minimal abnormality
 Table 0: of Grading System for Anatomic Severity of Disease in Emergency Local disease confined to the organ with minimal Local disease confined to the organ with severe Local extension Table 1: Universal
Table 0: of Grading System for Anatomic Severity of Disease in Emergency Local disease confined to the organ with minimal Local disease confined to the organ with severe Local extension Table 1: Universal
Mediastinitis. Jonathan Parks, MD Kings County Medical Center December 3, 2015
 Mediastinitis Jonathan Parks, MD Kings County Medical Center December 3, 2015 Case Presentation 69 year-old male from nursing home PMHx: COPD, asthma, HTN, Afib on pradaxa, PTSD, BPH c/o pulled pork stuck
Mediastinitis Jonathan Parks, MD Kings County Medical Center December 3, 2015 Case Presentation 69 year-old male from nursing home PMHx: COPD, asthma, HTN, Afib on pradaxa, PTSD, BPH c/o pulled pork stuck
Hilar cholangiocarcinoma. Frank Wessels, Maarten van Leeuwen, UMCU utrecht
 Hilar cholangiocarcinoma Frank Wessels, Maarten van Leeuwen, UMCU utrecht Content Anatomy Biliary strictures (Hilar) Cholangiocarcinoom Staging Biliary tract 1 st order Ductus hepatica dextra Ductus hepaticus
Hilar cholangiocarcinoma Frank Wessels, Maarten van Leeuwen, UMCU utrecht Content Anatomy Biliary strictures (Hilar) Cholangiocarcinoom Staging Biliary tract 1 st order Ductus hepatica dextra Ductus hepaticus
Newcastle HPB MDM updated radiology imaging protocol recommendations. Author Dr John Scott. Consultant Radiologist Freeman Hospital
 Newcastle HPB MDM updated radiology imaging protocol recommendations Author Dr John Scott. Consultant Radiologist Freeman Hospital This document is intended as a guide to aid radiologists and clinicians
Newcastle HPB MDM updated radiology imaging protocol recommendations Author Dr John Scott. Consultant Radiologist Freeman Hospital This document is intended as a guide to aid radiologists and clinicians
Management of Gallbladder Disease. Cory Buschmann, MD PGY-5 11/28/2017
 Management of Gallbladder Disease Cory Buschmann, MD PGY-5 11/28/2017 Financial disclosures None Content Scope of gallbladder diseases Evaluation H&P Labs Imaging Cholecystectomy vs cholecystostomy Ancillary
Management of Gallbladder Disease Cory Buschmann, MD PGY-5 11/28/2017 Financial disclosures None Content Scope of gallbladder diseases Evaluation H&P Labs Imaging Cholecystectomy vs cholecystostomy Ancillary
FLANK DRAINAGE FOR PERITONITIS SECONDARY TO HOLLOW VISCUS PERFORATION Dinesh H. N 1, Shrivathsa Merta K 2, Jagadish Kumar C. D 3
 FLANK DRAINAGE FOR PERITONITIS SECONDARY TO HOLLOW VISCUS PERFORATION Dinesh H. N 1, Shrivathsa Merta K 2, Jagadish Kumar C. D 3 HOW TO CITE THIS ARTICLE: Dinesh H. N, Shrivathsa Merta K, Jagadish Kumar
FLANK DRAINAGE FOR PERITONITIS SECONDARY TO HOLLOW VISCUS PERFORATION Dinesh H. N 1, Shrivathsa Merta K 2, Jagadish Kumar C. D 3 HOW TO CITE THIS ARTICLE: Dinesh H. N, Shrivathsa Merta K, Jagadish Kumar
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN
 UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
OCCULT COLON CANCER IN A PATIENT WITH DIABETES AND RECURRENT KLEBSIELLA
 OCCULT COLON CANCER IN A PATIENT WITH DIABETES AND RECURRENT KLEBSIELLA PNEUMONIAE LIVER ABSCESS Wen-Hung Hsu, 1 Fang-Jung Yu, 1 Chien-Han Chuang, 2 Chin-Fan Chen, 3 Chien-Ting Lee, 4 and Chien-Yu Lu 1,5
OCCULT COLON CANCER IN A PATIENT WITH DIABETES AND RECURRENT KLEBSIELLA PNEUMONIAE LIVER ABSCESS Wen-Hung Hsu, 1 Fang-Jung Yu, 1 Chien-Han Chuang, 2 Chin-Fan Chen, 3 Chien-Ting Lee, 4 and Chien-Yu Lu 1,5
Imaging Criteria (CT findings) Inflammatory changes localized to appendix +/- appendiceal dilation +/- contrast non-filling
 Inflammatory changes localized to appendix +/- appendiceal dilation +/- contrast non-filling") Table 1. Data Dictionaries for Grading System for EGS Conditions A. Acute Appendicitis I Description Acutely inflamed appendix, intact Gangrenous appendix, intact Perforated appendix with local contamination
Table 1. Data Dictionaries for Grading System for EGS Conditions A. Acute Appendicitis I Description Acutely inflamed appendix, intact Gangrenous appendix, intact Perforated appendix with local contamination
Key words: liver abscess, polymicrobial infection of liver abscess, percutaneous transhepatic abscess drainage, multiple systemic organ failure
 Key words: liver abscess, polymicrobial infection of liver abscess, percutaneous transhepatic abscess drainage, multiple systemic organ failure 13(13) Table 1 Features of echogram and computerized tomogram
Key words: liver abscess, polymicrobial infection of liver abscess, percutaneous transhepatic abscess drainage, multiple systemic organ failure 13(13) Table 1 Features of echogram and computerized tomogram
Hospital-acquired Pneumonia
 Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
USMLE and COMLEX II. CE / CK Review. General Surgery. 1. Northwestern Medical Review
 USMLE and COMLEX II CE / CK Review General Surgery 1. Northwestern Medical Review Northwestern Medical Review www.northwesternmedicalreview.com Lansing, Michigan 2014-2015 Acute Abdomen 1. Your patient
USMLE and COMLEX II CE / CK Review General Surgery 1. Northwestern Medical Review Northwestern Medical Review www.northwesternmedicalreview.com Lansing, Michigan 2014-2015 Acute Abdomen 1. Your patient
ISF criteria (International sepsis forum consensus conference of infection in the ICU) Secondary peritonitis
 Secondary peritonitis") Appendix with supplementary material. This appendix was part of the submitted manuscript and has been peer reviewed. It is posted as supplied by the authors. Supplementary Tables Table S1. Definitions
Appendix with supplementary material. This appendix was part of the submitted manuscript and has been peer reviewed. It is posted as supplied by the authors. Supplementary Tables Table S1. Definitions
MAKING CONNECTIONS. Los Angeles Medical Center
 MAKING CONNECTIONS Los Angeles Medical Center Resident: Chris Molloy, MD Fellow: Christian Coroian, MD, MBA Attending: Tina Hardley, MD Program/Dept(s): Los Angeles Medical Center CHIEF COMPLAINT & HPI
MAKING CONNECTIONS Los Angeles Medical Center Resident: Chris Molloy, MD Fellow: Christian Coroian, MD, MBA Attending: Tina Hardley, MD Program/Dept(s): Los Angeles Medical Center CHIEF COMPLAINT & HPI
Comparative study of different modalities of treatment of liver abscess
 Comparative study of different modalities of treatment of liver abscess Original Research Article ISSN: 2394-0026 (P) A comparative study of different modalities of treatment of liver abscesss Alpesh B.
Comparative study of different modalities of treatment of liver abscess Original Research Article ISSN: 2394-0026 (P) A comparative study of different modalities of treatment of liver abscesss Alpesh B.
Common surgical disease of the liver and portal hypertension
 Common surgical disease of the liver and portal hypertension Liver functhion: Responsible for storing glucose as glycogen, or converting it to lactate Utilization of: Amino acids for hepatic and plasma
Common surgical disease of the liver and portal hypertension Liver functhion: Responsible for storing glucose as glycogen, or converting it to lactate Utilization of: Amino acids for hepatic and plasma
Abdominal ultrasound:
 Abdominal ultrasound: Non-traumatic acute abdomen Wittanee Na-ChiangMai, MD Department of Radiology ChiangMai University 26/04/2017 Contents Technique of examination Normal anatomy Emergency conditions
Abdominal ultrasound: Non-traumatic acute abdomen Wittanee Na-ChiangMai, MD Department of Radiology ChiangMai University 26/04/2017 Contents Technique of examination Normal anatomy Emergency conditions
Morbidity Conference. Presented by 肝膽腸胃科張瀚文
 Morbidity Conference Presented by 肝膽腸胃科張瀚文 Chief Complaint General weakness for three days Present Illness This 63-year-old female with diabetes and on oral hypoglycemic agents presented with 3-day history
Morbidity Conference Presented by 肝膽腸胃科張瀚文 Chief Complaint General weakness for three days Present Illness This 63-year-old female with diabetes and on oral hypoglycemic agents presented with 3-day history
Case Study: #3: Gallbladder Carcinoma?
 Case Study: #3: Gallbladder Carcinoma? By: Megan Wyatt K. SON Wyatt 225 2B1 RDMS, RVT Patient: Male 85 YOA Caucasian Indication: Elevated Alkaline Phosphatase History Annual physical showed elevated alkaline
Case Study: #3: Gallbladder Carcinoma? By: Megan Wyatt K. SON Wyatt 225 2B1 RDMS, RVT Patient: Male 85 YOA Caucasian Indication: Elevated Alkaline Phosphatase History Annual physical showed elevated alkaline
Abdominal Imaging. Gallbladder perforation: color Doppler findings
 Abdom Imaging 27:47 50 (2002) DOI: 10.1007/s00261-001-0048-1 Abdominal Imaging Springer-Verlag New York Inc. 2002 Gallbladder perforation: color Doppler findings K. Konno, 1 H. Ishida, 1 M. Sato, 1 H.
Abdom Imaging 27:47 50 (2002) DOI: 10.1007/s00261-001-0048-1 Abdominal Imaging Springer-Verlag New York Inc. 2002 Gallbladder perforation: color Doppler findings K. Konno, 1 H. Ishida, 1 M. Sato, 1 H.
Siddharth Gosavi, Vydehi Institute of Medical Sciences & Research Centre, India Under the guidance of Gillian Lieberman, MD
 Under the guidance of Gillian Lieberman, MD March 2016 RADIOLOGICAL HALLMARKS OF NECROTIZING PANCREATITIS Siddharth Gosavi, Vydehi Institute of Medical Sciences & Research Centre, India Under the guidance
Under the guidance of Gillian Lieberman, MD March 2016 RADIOLOGICAL HALLMARKS OF NECROTIZING PANCREATITIS Siddharth Gosavi, Vydehi Institute of Medical Sciences & Research Centre, India Under the guidance
Cholecystitis is defined as nonspecific inflammation of the gallbladder with or without cholelithiasis. Types: calculous and acalculous.
 Cholecystitis is defined as nonspecific inflammation of the gallbladder with or without cholelithiasis. Types: calculous and acalculous. Anatomy of the gallbladder The gallbladder, a pear-shaped reservoir
Cholecystitis is defined as nonspecific inflammation of the gallbladder with or without cholelithiasis. Types: calculous and acalculous. Anatomy of the gallbladder The gallbladder, a pear-shaped reservoir
Imaging of common diseases of hepatobiliary and GI system
 Imaging of common diseases of hepatobiliary and GI system Natthaporn Tanpowpong, M.D. Diagnostic radiology Faculty of Medicine, Chulalongkorn University Normal plain radiograph A = Common bile duct
Imaging of common diseases of hepatobiliary and GI system Natthaporn Tanpowpong, M.D. Diagnostic radiology Faculty of Medicine, Chulalongkorn University Normal plain radiograph A = Common bile duct
Small Bowel and Colon Surgery
 Small Bowel and Colon Surgery Why Do I Need a Small Bowel Resection? A variety of conditions can damage your small bowel. In severe cases, your doctor may recommend removing part of your small bowel. Conditions
Small Bowel and Colon Surgery Why Do I Need a Small Bowel Resection? A variety of conditions can damage your small bowel. In severe cases, your doctor may recommend removing part of your small bowel. Conditions
GI Emergencies and the On-Call Call
 GI Emergencies and the On-Call Call Julie Yang, MD, FASGE Director of Therapeutic Endoscopy Assistant Professor of Medicine Montefiore Medical Center Albert Einstein College of Medicine Objectives Scenarios
GI Emergencies and the On-Call Call Julie Yang, MD, FASGE Director of Therapeutic Endoscopy Assistant Professor of Medicine Montefiore Medical Center Albert Einstein College of Medicine Objectives Scenarios
You are called to see another patient. Melissa Wong, MD Richmond University Medical Center 30 April 2015
 You are called to see another patient Melissa Wong, MD Richmond University Medical Center 30 April 2015 Case Presentation 51F, progressive abdominal pain x 1d +flatus, +BM Last colonoscopy 2013 (hyperplastic
You are called to see another patient Melissa Wong, MD Richmond University Medical Center 30 April 2015 Case Presentation 51F, progressive abdominal pain x 1d +flatus, +BM Last colonoscopy 2013 (hyperplastic
Cholangitis/ Cholangiohepatitis Syndrome (Inflammation of the Bile Duct System and Liver) Basics
 Basics") Glendale Animal Hospital 623-934-7243 www.familyvet.com Cholangitis/ Cholangiohepatitis Syndrome (Inflammation of the Bile Duct System and Liver) Basics OVERVIEW The liver is the largest gland in the body;
Glendale Animal Hospital 623-934-7243 www.familyvet.com Cholangitis/ Cholangiohepatitis Syndrome (Inflammation of the Bile Duct System and Liver) Basics OVERVIEW The liver is the largest gland in the body;
LAPAROSCOPIC APPENDICECTOMY
 LAPAROSCOPIC APPENDICECTOMY WHAT IS THE APPENDIX? The appendix is a small, fingerlike pouch of the intestinal tract located where the small and large join. It has no known use. It is postulated that the
LAPAROSCOPIC APPENDICECTOMY WHAT IS THE APPENDIX? The appendix is a small, fingerlike pouch of the intestinal tract located where the small and large join. It has no known use. It is postulated that the
Case Discussion Splenic Abscess
 Case Discussion Splenic Abscess Personal Data Gender: male Birth Date: 1928/Mar/06th Allergy: Mefenamic Smoking: 0.5 PPD for 55 years Alcohol: negative (?) 4 Months Ago Abdominal pain: epigastric area
Case Discussion Splenic Abscess Personal Data Gender: male Birth Date: 1928/Mar/06th Allergy: Mefenamic Smoking: 0.5 PPD for 55 years Alcohol: negative (?) 4 Months Ago Abdominal pain: epigastric area
GENI Program: GI and Abdominal Chief Complaints. Kim Macfarlane Clinical Nurse Specialist, Critical Care February 2008
 GENI Program: GI and Abdominal Chief Complaints Kim Macfarlane Clinical Nurse Specialist, Critical Care February 2008 Dehydration Common acute and chronic problem Recognition is critically important to
GENI Program: GI and Abdominal Chief Complaints Kim Macfarlane Clinical Nurse Specialist, Critical Care February 2008 Dehydration Common acute and chronic problem Recognition is critically important to
Esophageal Perforation
 Esophageal Perforation Dr. Carmine Simone Thoracic Surgeon, Division of General Surgery Head, Division of Critical Care May 15, 2006 Overview Case presentation Radiology Pre-operative management Operative
Esophageal Perforation Dr. Carmine Simone Thoracic Surgeon, Division of General Surgery Head, Division of Critical Care May 15, 2006 Overview Case presentation Radiology Pre-operative management Operative
Morbidity & Mortality Conference Downstate Medical Center. Daniel Kaufman, MD
 Morbidity & Mortality Conference Downstate Medical Center University Case Presentation Hospital of Brooklyn Daniel Kaufman, MD Necrotizing Fasciitis and Soft- Tissue Infections Necrotizing Fasciitis Deep
Morbidity & Mortality Conference Downstate Medical Center University Case Presentation Hospital of Brooklyn Daniel Kaufman, MD Necrotizing Fasciitis and Soft- Tissue Infections Necrotizing Fasciitis Deep
DIVERTICULOSIS MEDICAL AND SURGICAL MANAGEMENT. Simon Radley Consultant Surgeon March 2013
 DIVERTICULOSIS MEDICAL AND SURGICAL MANAGEMENT Simon Radley Consultant Surgeon March 2013 Definitions Diverticulosis: presence of diverticulae Diverticular disease: diverticulae associated with symptoms
DIVERTICULOSIS MEDICAL AND SURGICAL MANAGEMENT Simon Radley Consultant Surgeon March 2013 Definitions Diverticulosis: presence of diverticulae Diverticular disease: diverticulae associated with symptoms
Severe and Tertiary Peritonitis
 Severe and Tertiary Peritonitis Addison K. May, MD FACS Professor of Surgery and Anesthesiology Division of Trauma and Surgical Critical Care Vanderbilt University Medical Center PS204: The Bad Infections:
Severe and Tertiary Peritonitis Addison K. May, MD FACS Professor of Surgery and Anesthesiology Division of Trauma and Surgical Critical Care Vanderbilt University Medical Center PS204: The Bad Infections:
General'Surgery'Service'
 General'Surgery'Service' Patient Care Goals and Objectives 1)! Stomach/Duodenum and Bariatric 2)! Interpret the results of clinical evaluations (history, physical examination) performed on patients being
General'Surgery'Service' Patient Care Goals and Objectives 1)! Stomach/Duodenum and Bariatric 2)! Interpret the results of clinical evaluations (history, physical examination) performed on patients being
Percutaneous Cholecystostomy Tube in Acute Cholecystitis: Our Experience in a Tertiary Center in Saudi Arabia
 9 KUWAIT MEDICAL JOURNAL June 0 Original Article Percutaneous Cholecystostomy Tube in Acute Cholecystitis: Our Experience in a Tertiary Center in Saudi Arabia Faisal A Al-Saif, Hamad S AlSubaie, Rafif
9 KUWAIT MEDICAL JOURNAL June 0 Original Article Percutaneous Cholecystostomy Tube in Acute Cholecystitis: Our Experience in a Tertiary Center in Saudi Arabia Faisal A Al-Saif, Hamad S AlSubaie, Rafif
INTRA-ABDOMINAL INFECTIONS
 INTRA-ABDOMINAL INFECTIONS Learning Objectives: 1. Describe patient risk factors, signs and symptoms that may indicate an intra-abdominal infection 2. Identify tests and significant laboratory values used
INTRA-ABDOMINAL INFECTIONS Learning Objectives: 1. Describe patient risk factors, signs and symptoms that may indicate an intra-abdominal infection 2. Identify tests and significant laboratory values used
Acute Cholangitis. Kelsey Knotts PharmD Candidate Class of 2016
 Acute Cholangitis Kelsey Knotts PharmD Candidate Class of 2016 Learning Objectives 1. Describe the mechanism of the development of acute cholangitis 2. Identify common causative organisms in acute cholangitis
Acute Cholangitis Kelsey Knotts PharmD Candidate Class of 2016 Learning Objectives 1. Describe the mechanism of the development of acute cholangitis 2. Identify common causative organisms in acute cholangitis
Jaundice. Agnieszka Dobrowolska- Zachwieja, MD, PhD
 Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
Adv Pathophysiology Unit 9: GI Page 1 of 10
 Adv Pathophysiology Unit 9: GI Page 1 of 10 Learning objectives for this file: 1. Recognize positive physical and lab findings that point to the diagnosis 2. Appreciate the appearance of the affected organ
Adv Pathophysiology Unit 9: GI Page 1 of 10 Learning objectives for this file: 1. Recognize positive physical and lab findings that point to the diagnosis 2. Appreciate the appearance of the affected organ
Information for Consent Cholecystectomy (Laparoscopic/Open) 膽囊切除術 ( 腹腔鏡 / 開放性 )
 膽囊切除術 ( 腹腔鏡 / 開放性 )") Version 1.0 Page 1 of 3 Information for Consent Cholecystectomy (Laparoscopic/Open) 膽囊切除術 ( 腹腔鏡 / 開放性 ) Introduction Gallbladder is a sac connected to the biliary tree. It serves the function of concentration
Version 1.0 Page 1 of 3 Information for Consent Cholecystectomy (Laparoscopic/Open) 膽囊切除術 ( 腹腔鏡 / 開放性 ) Introduction Gallbladder is a sac connected to the biliary tree. It serves the function of concentration
Together, putting patients first
 The Role of a Gastroenterologist in the Diagnosis and Management of Pancreatic Cancer Sarah Jowett, Consultant Gastroenterologist Bradford Teaching Hospitals Trust Leeds Regional Study Day, 12 September
The Role of a Gastroenterologist in the Diagnosis and Management of Pancreatic Cancer Sarah Jowett, Consultant Gastroenterologist Bradford Teaching Hospitals Trust Leeds Regional Study Day, 12 September
Liver Transplantation
 1 Liver Transplantation Department of Surgery Yonsei University Wonju College of Medicine Kim Myoung Soo M.D. ysms91@wonju.yonsei.ac.kr http://gs.yonsei.ac.kr History Development of Liver transplantation
1 Liver Transplantation Department of Surgery Yonsei University Wonju College of Medicine Kim Myoung Soo M.D. ysms91@wonju.yonsei.ac.kr http://gs.yonsei.ac.kr History Development of Liver transplantation
Acute Diverticulitis. Andrew B. Peitzman, MD Mark M. Ravitch Professor of Surgery University of Pittsburgh
 Acute Diverticulitis Andrew B. Peitzman, MD Mark M. Ravitch Professor of Surgery University of Pittsburgh Focus today: when to operate n Recurrent, uncomplicated diverticulitis; after how many episodes?
Acute Diverticulitis Andrew B. Peitzman, MD Mark M. Ravitch Professor of Surgery University of Pittsburgh Focus today: when to operate n Recurrent, uncomplicated diverticulitis; after how many episodes?
Case Presentation. Kasher Meron Michal MD Meir Hospital, Kfar sava, Israel
 Case Presentation Kasher Meron Michal MD Meir Hospital, Kfar sava, Israel On Presentation 62y old male, born in South Africa Osler Weber Rendu, Hereditary Hemorrhagic Telangiectasia (HHT) Recurrent Epistaxis.
Case Presentation Kasher Meron Michal MD Meir Hospital, Kfar sava, Israel On Presentation 62y old male, born in South Africa Osler Weber Rendu, Hereditary Hemorrhagic Telangiectasia (HHT) Recurrent Epistaxis.
Lutheran Medical Center. Daniel H. Hunt, M.D. June 10 th, 2005
 Lutheran Medical Center Daniel H. Hunt, M.D. June 10 th, 2005 History xx y.o. pt with primary CBD stones s/p ERCP xx months earlier for attempted stone extraction resulting in post ERCP pancreatitis. Patient
Lutheran Medical Center Daniel H. Hunt, M.D. June 10 th, 2005 History xx y.o. pt with primary CBD stones s/p ERCP xx months earlier for attempted stone extraction resulting in post ERCP pancreatitis. Patient
Always keep it in the differential
 Acute Appendicitis Lissa C. Sakata and Lindsey Perea 2 Always keep it in the differential Learning Objectives 1. The learner should be able to describe the etiology of acute appendicitis. 2. The learner
Acute Appendicitis Lissa C. Sakata and Lindsey Perea 2 Always keep it in the differential Learning Objectives 1. The learner should be able to describe the etiology of acute appendicitis. 2. The learner
Gastroenterology. Certification Examination Blueprint. Purpose of the exam
 Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Chapter Goal. Learning Objectives 9/12/2012. Chapter 29. Nontraumatic Abdominal Injuries
 Chapter 29 Nontraumatic Abdominal Injuries Chapter Goal Use assessment findings to formulate field impression & implement treatment plan for patients with nontraumatic abdominal pain Learning Objectives
Chapter 29 Nontraumatic Abdominal Injuries Chapter Goal Use assessment findings to formulate field impression & implement treatment plan for patients with nontraumatic abdominal pain Learning Objectives
Locally Advanced Colon Cancer. Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery
 Locally Advanced Colon Cancer Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery Case 34 yo man presented with severe RLQ abdominal pain X 24 hrs. No nausea/vomiting/fever. + flatus.
Locally Advanced Colon Cancer Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery Case 34 yo man presented with severe RLQ abdominal pain X 24 hrs. No nausea/vomiting/fever. + flatus.
What can you expect after your ERCP?
 ERCP Explained and respond to bed rest, pain relief and fasting to rest the gut with the patient needing to stay in hospital for only a few days. Some patients develop severe pancreatitis and may require
ERCP Explained and respond to bed rest, pain relief and fasting to rest the gut with the patient needing to stay in hospital for only a few days. Some patients develop severe pancreatitis and may require
Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013
 Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013 Case Report 42F with h/o chronic pancreatitis due to alcohol use with chronic upper
Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013 Case Report 42F with h/o chronic pancreatitis due to alcohol use with chronic upper
FAST TRACK MANAGEMENT OF PANCREATIC CANCER
 FAST TRACK MANAGEMENT OF PANCREATIC CANCER Jawad Ahmad Consultant Hepatobiliary Surgeon University Hospital Coventry and Warwickshire NHS Trust Part 1. Fast Track Surgery for Pancreatic Cancer Part 2.
FAST TRACK MANAGEMENT OF PANCREATIC CANCER Jawad Ahmad Consultant Hepatobiliary Surgeon University Hospital Coventry and Warwickshire NHS Trust Part 1. Fast Track Surgery for Pancreatic Cancer Part 2.
SASKATCHEWAN REGISTERED NURSES ASSOCIATION. RNs WITH ADDITIONAL AUTHORIZED PRACTICE CLINICAL DECISION TOOL AUGUST 2017
 DEFINITION Cholelithiasis Presence of gall stones in the biliary tract. Biliary Colic Right upper quadrant pain due to obstruction of a bile duct by a gallstone. Cholecystitis Inflammation of the gallbladder
DEFINITION Cholelithiasis Presence of gall stones in the biliary tract. Biliary Colic Right upper quadrant pain due to obstruction of a bile duct by a gallstone. Cholecystitis Inflammation of the gallbladder
Emergency Surgery Board Department of General Surgery Rambam Health Care Campus
 Emergency Surgery Board Department of General Surgery Rambam Health Care Campus Surgical Complications of Peptic Ulcer Disease Case Presentation and Review of the Literature Case Presentation 40y male
Emergency Surgery Board Department of General Surgery Rambam Health Care Campus Surgical Complications of Peptic Ulcer Disease Case Presentation and Review of the Literature Case Presentation 40y male
US in non-traumatic acute abdomen. Lalita, M.D. Radiologist Department of radiology Faculty of Medicine ChiangMai university
 US in non-traumatic acute abdomen Lalita, M.D. Radiologist Department of radiology Faculty of Medicine ChiangMai university Sagittal Orientation Transverse (Axial) Orientation Coronal Orientation Intercostal
US in non-traumatic acute abdomen Lalita, M.D. Radiologist Department of radiology Faculty of Medicine ChiangMai university Sagittal Orientation Transverse (Axial) Orientation Coronal Orientation Intercostal
Long Term Follow-up. 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown. Is the patient alive? Yes No
 Long Term Follow-up 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown Is the patient alive? Yes No Was an exam performed by a bariatric physician or PA/NP? Yes No Was the patient
Long Term Follow-up 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown Is the patient alive? Yes No Was an exam performed by a bariatric physician or PA/NP? Yes No Was the patient