AnnMarie Papa, DNP,RN,CEN,NE-BC,FAEN, FAAN Clinical Director, Emergency, Medical & Observation Nursing Hospital of the University of Pennsylvania
|
|
|
- Alicia Beverley Blair
- 5 years ago
- Views:
Transcription


1 AnnMarie Papa, DNP,RN,CEN,NE-BC,FAEN, FAAN Clinical Director, Emergency, Medical & Observation Nursing Hospital of the University of Pennsylvania

2 Who Am I?
3 Except on few occasions, the patient appears to die from the body s response to infection rather than from [the infection itself.] Sir William Osler, 1904
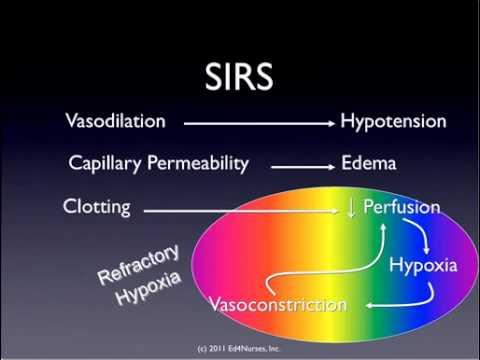
4 Endothelial, mitorchondrial and cell membrane pump dysfunction Intracellular edema Leakage of intracellular contents into the extracellular space Inflammatory cascade
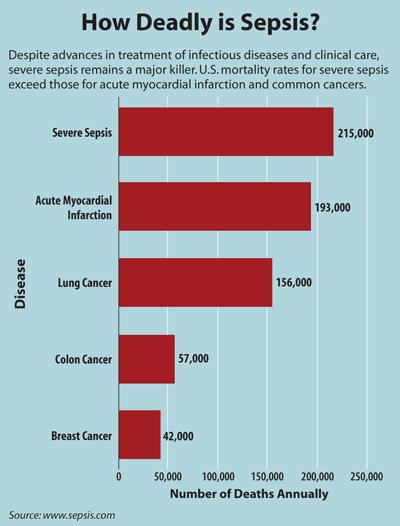
5 } A patient a minute presents to a US ED } 750,000 cases/yr of severe sepsis in USA } 215,000 deaths/yr directly related to sepsis } Tenth leading cause of death in USA } Rate of sepsis cases is increasing faster than the population } 37% of severe sepsis patients come through the ED Wang et al. Crit Care Med, 2007 Angus et al. Crit Care Med, 2001
6

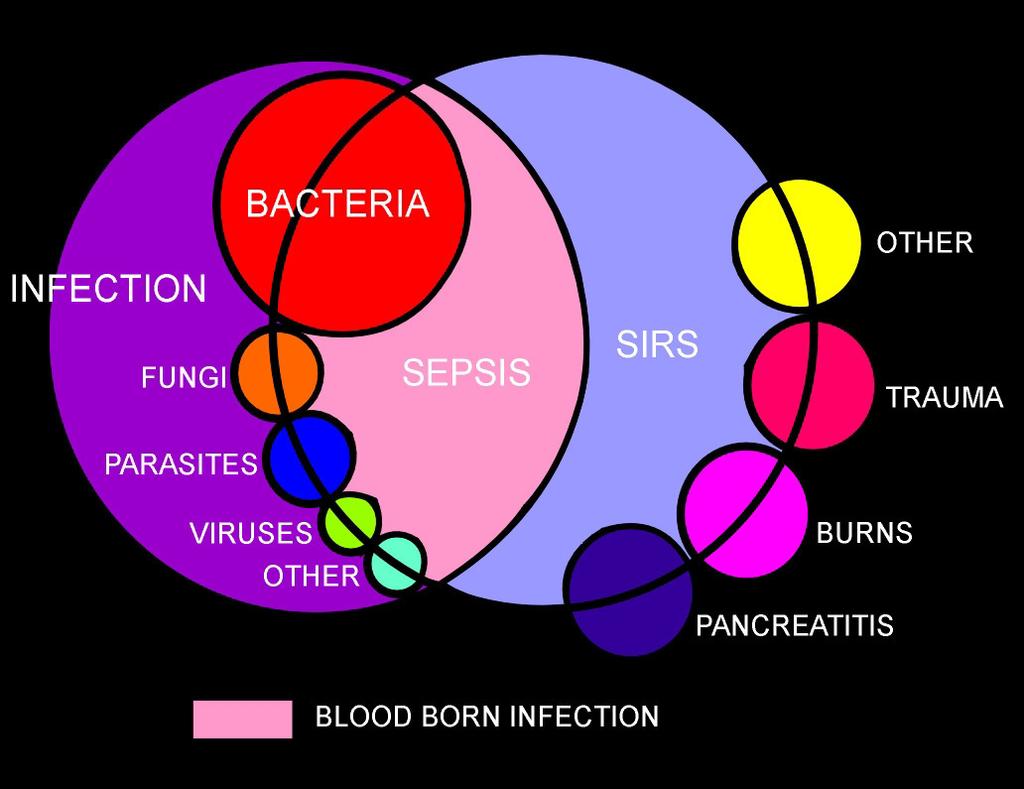
7 } The Continuum SIRS Sepsis Severe Sepsis Septic Shock

 HR > 90 BPM RR > 20/min or PaCO PaCO2 < 32 mm Hg")
8 } Systemic Inflammatory Response Syndrome Manifested by 2 or more of the following: Temperature > 38 C (100.4F) or < 36 C (96.8F) HR > 90 BPM RR > 20/min or PaCO PaCO2 < 32 mm Hg WBC 12,000 or >10 bands Systemic
9

10 The Continuum of Sepsis SIRS Sepsis Severe Sepsis Septic Shock Systemic Inflammatory Response Syndrome SIRS criteria Temp < 96.8 or > F HR > 90 RR > 20 or PCO 2 < 32 WBC < 4 or > 12 or bands > 10% Bone et al. Chest 1992



11 The Continuum of Sepsis SIRS Sepsis Severe Sepsis Septic Shock Systemic Inflammatory Response to Infection Suspected or confirmed infection 2 or more SIRS criteria Bone et al. Chest 1992
12 The Continuum of Sepsis SIRS Sepsis Severe Sepsis Septic Shock Sepsis plus Organ Dysfunction Elevated Creatinine Elevated INR Altered Mental Status Elevated Lactate Hypotension that responds to fluid Levy et al. Crit Care Med; 2003
13 The Continuum of Sepsis SIRS Sepsis Severe SepsisSeptic Shock Cryptic Shock Normotensive Severe Sepsis and Hypotension Hypotension that does NOT respond to fluid (30 cc/kg bolus) Lactate > 4 Bone et al. Chest, 1992 Rivers et al. NEJM, 2001
14
15 } In 2004 Surviving Sepsis Campaign Adapted the original Rivers Protocol and other research Created practice guidelines. Outlined resuscitation and management bundles. Stated goal was 25% reduction in mortality. } Severe Sepsis Resuscitation Bundle. } Goal was to perform outlined tasks within six hours.
16

17 Rivers et al. NEJM, 2001 Algorithmic
18 } Resuscitation Bundle included: Measurement of Lactic Acid. Blood cultures prior to antibiotic administration. Appropriate broad spectrum antibiotics in 3 hours (ED arrival). IF hypotension IV fluid bolus (20ml\kg initial) IF continued hypotension or lactic acid > 4 Achieve MAP > 65 Achieve central venous pressure 8 mmhg or greater Achieve central venous oxygen sat. of 70%
19 Achieve MAP > 65 Continued fluid boluses. Adequate fluid resuscitation is a key component. Initiation of vasopressor agents. Norepinephrine Dopamine Norepinephrine appears to be the more common choice. Sepsi
20 } Norepinephrine Extensive a-adrenergic response. Moderate b-adrenergic response. Works mostly through vasoconstrictive actions. Does not change heart rate, cardiac output microgram\kg\minute (titrated to effect).
21 Achieve CVP 8 mmhg or greater Goal is 12 mmhg in intubated patients. Generally measured via an above the diaphragm central venous line. Subclavian Internal Jugular (preferred for US guided) Achieved through repeated fluid boluses (normal saline, lactated ringers). S
22 } Central Venous Pressure Pressure in Right Atrium Reflective of Preload Normal between 5 and 10 mmhg Can be measured through a standard triple lumen catheter
23 Achieve central venous O 2 Sat of 70% Can be drawn from same central line and run in a blood gas analyzer. (intermittent) Continual monitoring available from a specialized catheter. (PreSep, Edwards) If Hgb less than 10 mg\dl, transfuse PRBCs until you meet this goal. If Hgb already above 10 mg\dl, use dobutamine to achieve this goal.
24 } Dobutamine Inotrope Strong beta adrenergic response Start at 5 mcg\kg\minute Maximum of 20 mcg\kg\minute May increase hypotension so norepinephrine may be required to counteract this effect Goal is to increase cardiac output t
25 } Summarizing EGDT Achieve adequate fluid resuscitation. Vasopressors to keep MAP > 65 mmhg. Measure CVP and Central Venous Oxygen Saturation Additional fluids to achieve adequate CVP. CV oxygenation as a marker of adequate tissue perfusion Maximize other parameters first (especially CVP). If anemic transfuse. If not anemic consider an inotrope (dobutamine).
26 } Summarizing EGDT Continuing research is being done to fine tune and support this approach. Clearly being more aggressive is beneficial. Septic shock patients tended to be under-resuscitated coming out of ED. Better coordination between ED and ICU is critical.
27 60.0% 56.9% 50.0% 46.5% 49.0% 44.3% 40.0% 30.0% 20.0% 30.5% 33.3% Standard EGDT 10.0% 0.0% In House 28-Day 60-Day 15.7% at 28-days and 12.6% at 60-days. Rivers et al NEJM, 2001
28 Mortality % absolute increase in mortality per hour Time 0 1 hour 2 hours 3 hours 4 hours 5 hours 6 hours Time to Antibiotic Kumar et al. Critical Care Medicine. 2006

29 } To study the relationship between time to antibiotics and mortality in patients treated with EGDT in the ED } 261 patients } Average time to antibiotics: Triage to antibiotics: 119 minutes Qualification for EGDT to antibiotics: 42 minutes Gaieski et al Crit Care Med, 2010

30 } EGDT } 261 patients } Age 59 } 41% female Inpatient Mortality (%) } 31.3% Mortality } Median TTA 119 minutes Goal Delayed 5 0 < 1 hour < 2 hour < 3 hour Antibiotic Timing Gaieski DF et al Crit Care Med 2010
31 Broad-Spectrum Antimicrobials: + Cefepime 1 gm IV (1) + Vancomycin 1 gm ( 70 kg) or 1.5 gm (> 70 kg) IV ± Amikacin 15 mg/kg or 7.5 mg/kg (CrCl < 20) IV (4) No PCN Allergy Yes Broad-Spectrum Antimicrobials: + Levofloxacin 750 mg IV + Vancomycin 1 gm ( 70 kg) or 1.5 gm (> 70 kg) IV ± Amikacin 15 mg/kg or 7.5 mg/kg (CrCl < 20) IV (4) Community Acquired Pneumonia: + Azithromycin 500mg IV (2) Anaerobic Source: + Metronidazole 500 mg IV (3) On TPN: + Fluconazole 400 mg IV Prolonged Neutropenia ± Steroids: + Caspofungin 70 mg IV ± Hydrocortisone mg IV Gaieski et al, CCM, 2011
32 } Stabilize patient } Eradicate source of infection } Restore perfusion } Modulate body s inflammatory and anti-inflammatory responses } Cessation of ongoing lactate production
33 Mortality in Admitted Patients Mortality, % No SIRS SIRS 2 SIRS 3 SIRS 4 Sepsis Severe Sepsis Septic Shock RANGEL-FRAUSTO JAMA 1995
34

35 In Triage, early iden.fica.on of the sepsis pa.ent is vital: Who is at risk? What are the signs to look for?
36 A Bacterial infection is a major risk factor for sepsis Those with a poor immune system are at higher risk (Immunosuppressive therapy, Diabetes, Cancer, Alcohol Abuse, HIV/AIDS Two thirds of patients with Sepsis are older than 65 Sepsis is more common in men African Americans are more prone than any other race

37 } Those with suspected sources of infection Pneumonia UTI s Wounds

38 } Patients with CVP s, PICC s } Foleys } Ventilators } Always consider bounce backs
39 Utilize the SIRS Criteria (Sudden Inflammatory Response Syndrome): Temp > F or < 96.8F HR > 90 BPM RR >20 breaths per minute WBC > 12,000 or < 4,000 (not usually known in triage)
 Insert CVC in IJV or SCV Evaluate ScV02 Calculate Apache II score and notify SAR for MICU bed Yes Yes ScvO 2 70% Yes No MAP 65 baseline ScvO 2 70% Bolus")
40 Severe Sepsis Pathway Hospital of the University of Pennsylvania Emergency Department Yes CVP 8 No 1. At least 2 SIRS criteria HR>90 RR>20 T>100.4 or <96.8 WBC >12 or <4) 2. Suspected infection 3. Lactate >4 or SBP<90 (after 30cc/kg IVF bolus) Insert CVC in IJV or SCV Evaluate ScV02 Calculate Apache II score and notify SAR for MICU bed Yes Yes ScvO 2 70% Yes No MAP 65 baseline ScvO 2 70% Bolus 500 ml NS q15-20 Assess for pulmonary edema if>3l given No 1. Start/Titrate norepi or dopamine 2. Dexamethasone for refractory hypotension 3. Place arterial line if time permits Recheck Hgb by super gas Transfuse PRBC s until HgB 10 No Start/Titrate Dobutamine Yes ScvO 2 70% No CVP, MAP, ScvO2 goals achieved Re-evaluate to achieve goals

41 } Any person that is a concern for Sepsis ESI 2 } If hypotensive, increased urgency } Triage protocols if room not immediately available; Labs, X rays
42 Assess patient Important for baseline assessment possible changes in condition later Cardiac Monitor Oxygen Vital signs q 1 hour minimum EKG CXR Treat fever IV access 2 peripheral IV sites 18g or 20g for fluid resuscitation
43 Labs CBC, BMP, LFT s, CMP, PT/PTT, Type and Screen, VBG and Serum Lactate Blood Cultures Urine Urinalysis, Urine C&S Cultures if applicable Wounds, sputum, stool for c diff IV fluid bolus 1 to 2 liters/hour Anticipate Vasopressors Hypotension not responding to initial fluid resuscitation to maintain MAP > 65 mm Hg
44 10 Symptoms of Physiologic Instability Temperature change Increased pulse New or changing pain Changes in respiratory rate Decreased systolic and mean arterial pressure Change in LOC (lethargy or anxiety) Capillary refill greater than 3 seconds Urine output < 30 ml/hr. Changes in ScVO2 (measured via blood gas analysis) SaO2 < 90% (oxygen saturation-arterial)

45 Mentation Malaise, lethargy, restlessness Decreased LOC, stupor, coma Cutaneous Warm, flushed, dry Cold, clammy, pale, mottled skin Heart rate Tachycardia, bounding pulses Tachycardia, weak thready pulses Respiratory rate > 20/min Shallow and tachypneic Urine Decreased Decreased to anuric Acid-base values Respiratory alkalosis Metabolic and respiratory acidosis Body temperature Fever and chills Hypothermic and mottled
46 Per Pharmacy protocol -for patients with Sepsis or Septic Shock Administer antibiotics with gram negative/anaerobic FIRST; Cefepime Aztreonam Levofloxacin Amikacin Metronidazole Administer antibiotics with gram positive coverage SECOND; Vancomycin Administer antibiotics with Fungal coverage THIRD; Fluconazole Caspofungin Rationale: better timing means improved outcomes
47
48 Add to Sepsis criteria any one of the following signs that would indicate hypoperfusion and organ dysfunction: Areas of mottled skin Urine output < 0.5 ml/kg for at least 1 hour Lactate > 2mmol/L Abrupt change in Mental Status Abnormal EEG findings Platelets < 100,000 Disseminated intravascular coagulation (DIC) Adult Respiratory Distress Syndrome (ARDS) Cardiac dysfunction
49 } Systemic mean Blood Pressure < 60 mmhg despite adequate fluid resuscitation (<80 in known hypertensive pt) } Maintaining Systemic mean BP > 60 mmhg requires } Medications Dopamine > 5mcg.kg/min Norepinephrine < 0.25 mcg.kg/min Epinephrine < 0.25 mcg/kg/min
50 Pressure in the thoracic vena cava Estimates right atrial pressure Estimates right ventricular pressure Estimates right ventricular volume Estimates preload


51 } Oxygen Saturation of Central Venous hemoglobin } Amount of oxygen left over after the body removes what it needs } Represents the balance between oxygen delivery and consumption
 then the oxygen supply is insufficient or the oxygen demand has increased.")
52 OXYGEN: BALANCE Oxygen balance is necessary to sustain life. SvO2 is the "watchdog" of this balance. When monitored, it serves as an early trouble indicator and can help clinicians adjust therapies. In a healthy individual, normal SvO2 is between 60% and 80% If SvO2 is low (below 60%) then the oxygen supply is insufficient or the oxygen demand has increased. If SvO2 is high (above 80%) then the oxygen demand has declined or the oxygen supply has increased.
53 } Aggressive fluid resuscitation-5l/6hours } Give in 500 cc bolus and assess for signs of Pulmonary Edema } Intubation and mechanical ventilation } Vasopressors } CVP monitoring } Transfusions for increased tissue perfusion } Inotropic therapies } Sequential serum lactates
54 } Patient dies as much from the body s response to infection as from the infection itself } Huge epidemiologic burden of sepsis } Recognition is major hurdle } Lactate is a marker for critical illness and can be used as a screening tool

55 Thank You!
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014
 December 17, 2014") Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT
 PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
Septic Shock. Rontgene M. Solante, MD, FPCP,FPSMID
 Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
Core Measures SEPSIS UPDATES
 Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Objectives. Management of Septic Shock. Definitions Progression of sepsis. Epidemiology of severe sepsis. Major goals of therapy
 Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Sepsis Story At Intermountain Healthcare Intensive Medicine Clinical Program
 Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Mortality Rate was unsightly!!! 4/24/2013. Sepsis Quality Improvement Project
 Libby, MT Sepsis Quality Improvement Project Barb Dumont RN, Director of Quality and Risk Management Mike Julius RN, ED Manager Cathy Wolfe RN, Chief Nursing Officer. Mortality Rate was unsightly!!! percent
Libby, MT Sepsis Quality Improvement Project Barb Dumont RN, Director of Quality and Risk Management Mike Julius RN, ED Manager Cathy Wolfe RN, Chief Nursing Officer. Mortality Rate was unsightly!!! percent
Dilemmas in Septic Shock
 Dilemmas in Septic Shock William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center A 62 year-old female presents to the ED with fever,
Dilemmas in Septic Shock William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center A 62 year-old female presents to the ED with fever,
Objectives. Epidemiology of Sepsis. Review Guidelines for Resuscitation. Tx: EGDT, timing/choice of abx, activated
 Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis is an important issue. Clinician s decision-making capability. Guideline recommendations
 Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Early Goal-Directed Therapy
 Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Sepsis. From EMS to ER to ICU. What we need to be doing
 Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Presented by: Indah Dwi Pratiwi
 Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Sepsis Awareness and Education
 Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Surviving Sepsis Campaign Guidelines 2012 & Update for David E. Tannehill, DO Critical Care Medicine Mercy Hospital St.
 Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Sepsis Care and the New Core Measures. Daniel S. Hagg, MD January 15, 2016
 Sepsis Care and the New Core Measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Sepsis Care and the New Core Measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Updates in Sepsis 2017
 Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
Sepsis Management: Past, Present, and Future
 Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Early Recognition and Management. Therese Hughes, PhD, MPA, RN
 Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Frank Sebat, MD - June 29, 2006
 Types of Shock Hypovolemic Shock Low blood volume decreasing cardiac output. AN INTEGRATED SYSTEM OF CARE FOR PATIENTS AT RISK SHOCK TEAM and RAPID RESPONSE TEAM Septic or Distributive Shock Decrease in
Types of Shock Hypovolemic Shock Low blood volume decreasing cardiac output. AN INTEGRATED SYSTEM OF CARE FOR PATIENTS AT RISK SHOCK TEAM and RAPID RESPONSE TEAM Septic or Distributive Shock Decrease in
Sepsis care and the new core measures
 Sepsis care and the new core measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Sepsis care and the new core measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
BREAK 11:10-11:
 1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
Nothing to disclose 9/25/2017
 Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the
 Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the differences between sepsis, severe sepsis and septic
Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the differences between sepsis, severe sepsis and septic
9/25/2017. Nothing to disclose
 Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Case Scenario 3: Shock and Sepsis
 Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
What is sepsis? RECOGNITION. Sepsis I Know It When I See It 9/21/2017
 Sepsis I Know It When I See It September 15, 2017 Matthew Exline, MD MPH Medical Director, Medical ICU What is sepsis? I shall not today attempt further to define the kinds of material [b]ut I know it
Sepsis I Know It When I See It September 15, 2017 Matthew Exline, MD MPH Medical Director, Medical ICU What is sepsis? I shall not today attempt further to define the kinds of material [b]ut I know it
Effectively Managing Sepsis Denials
 Effectively Managing Sepsis Denials Krysten Brooks, RN, BSN, MBA Senior Inpatient Consultant 3M Health Information Systems This is the Full Title of a Session Atlanta, GA 1 Learning Objectives At the completion
Effectively Managing Sepsis Denials Krysten Brooks, RN, BSN, MBA Senior Inpatient Consultant 3M Health Information Systems This is the Full Title of a Session Atlanta, GA 1 Learning Objectives At the completion
The changing face of
 The changing face of sepsis. @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser (maternal sepsis) to WHO Breast cancer Cognitive impairment Mild 3.8 7.1
The changing face of sepsis. @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser (maternal sepsis) to WHO Breast cancer Cognitive impairment Mild 3.8 7.1
SURVIVING SEPSIS: Early Management Saves Lives
 SURVIVING SEPSIS: Early Management Saves Lives Pat Posa RN, BSN, MSA System Performance Improvement Leader St. Joseph Mercy Health System Ann Arbor, MI Patricia.posa@stjoeshealth.org Objectives a. Understand
SURVIVING SEPSIS: Early Management Saves Lives Pat Posa RN, BSN, MSA System Performance Improvement Leader St. Joseph Mercy Health System Ann Arbor, MI Patricia.posa@stjoeshealth.org Objectives a. Understand
No conflicts of interest to disclose
 No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP
 SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
towards early goal directed therapy
 Paediatric Septic Shock- towards early goal directed therapy Elliot Long Paediatric Acute Care 2011 Conference Outline Emergency Department Rivers Protocol (EGDT) ACCM Sepsis Protocol Evidence Barriers
Paediatric Septic Shock- towards early goal directed therapy Elliot Long Paediatric Acute Care 2011 Conference Outline Emergency Department Rivers Protocol (EGDT) ACCM Sepsis Protocol Evidence Barriers
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
4/5/2018. Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY. I have no financial disclosures
 Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Sepsis overview. Dr. Tsang Hin Hung MBBS FHKCP FRCP
 Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
SHOCK Susanna Hilda Hutajulu, MD, PhD
 SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
Initial Resuscitation of Sepsis & Septic Shock
 Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Guidebook for ED and Inpatient Sepsis Order Set Initiatives 2018
 Background The leadership of the Surviving Sepsis Campaign (SSC) believes, since its inception, that both the SSC Guidelines and the SSC performance improvement indicators (1) will evolve as new evidence
Background The leadership of the Surviving Sepsis Campaign (SSC) believes, since its inception, that both the SSC Guidelines and the SSC performance improvement indicators (1) will evolve as new evidence
Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018
 Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018") Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018 Objectives 1. To identify the symptom of severe sepsis and septic shock syndrome.
Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018 Objectives 1. To identify the symptom of severe sepsis and septic shock syndrome.
Sepsis Update: Focus on Early Recognition and Intervention. Disclosures
 Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Sepsis as Seen by the CMO. Randy C. Roth, MD Chief Medical Officer
 Sepsis as Seen by the CMO Randy C. Roth, MD Chief Medical Officer 1 Challenges of Sepsis Sepsis, like many disease processes, is much more than a clinical challenge. For Hospitalists, we are treating the
Sepsis as Seen by the CMO Randy C. Roth, MD Chief Medical Officer 1 Challenges of Sepsis Sepsis, like many disease processes, is much more than a clinical challenge. For Hospitalists, we are treating the
Case year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50
 Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
The syndrome formerly known as. Severe Sepsis. James Rooks MD. Coordinator of critical care education OU College of Medicine, Tulsa
 The syndrome formerly known as Severe Sepsis James Rooks MD Coordinator of critical care education OU College of Medicine, Tulsa Disclosures I have no actual or practical conflicts of interest in relation
The syndrome formerly known as Severe Sepsis James Rooks MD Coordinator of critical care education OU College of Medicine, Tulsa Disclosures I have no actual or practical conflicts of interest in relation
Critical Care Treatment Guidelines
 Critical Care Treatment Guidelines West Virginia Office of Emergency Medical Services CCT Guidelines CCT Guidelines TABLE OF CONTENTS Preface Acknowledgments Using the Guidelines INITIAL TREATMENT / UNIVERSAL
Critical Care Treatment Guidelines West Virginia Office of Emergency Medical Services CCT Guidelines CCT Guidelines TABLE OF CONTENTS Preface Acknowledgments Using the Guidelines INITIAL TREATMENT / UNIVERSAL
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
SEPSIS RAPID RESPONSE
 SEPSIS RAPID RESPONSE Sepsis kills up to 50% of those infected. How many deaths will you prevent this year? 1 SEPSIS Back ground: According to the Institute for Health Improvement and the Surviving Sepsis
SEPSIS RAPID RESPONSE Sepsis kills up to 50% of those infected. How many deaths will you prevent this year? 1 SEPSIS Back ground: According to the Institute for Health Improvement and the Surviving Sepsis
Update in Sepsis. Conflicts of Interest: None. Bill Janssen, M.D.
 Update in Sepsis Bill Janssen, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Conflicts of Interest: None A 62 year-old female presents to the ED with fever,
Update in Sepsis Bill Janssen, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Conflicts of Interest: None A 62 year-old female presents to the ED with fever,
SEPSIS: Seeing Through the. W. Graham Carlos MD, MSCR, ATSF, FACP
 SEPSIS: Seeing Through the W. Graham Carlos MD, MSCR, ATSF, FACP Objectives Forget everything you have known about sepsis Learn new things Objectives Define sepsis Explain why Early Goal Directed Therapy
SEPSIS: Seeing Through the W. Graham Carlos MD, MSCR, ATSF, FACP Objectives Forget everything you have known about sepsis Learn new things Objectives Define sepsis Explain why Early Goal Directed Therapy
Sepsis or Severe Sepsis? Is there a right thing, and how do we do it?
 Sepsis or Severe Sepsis? Is there a right thing, and how do we do it? Steven Q Simpson, MD, FCCP, FACP Professor of Medicine Division of Pulmonary and Critical Care University of Kansas Disclosures No
Sepsis or Severe Sepsis? Is there a right thing, and how do we do it? Steven Q Simpson, MD, FCCP, FACP Professor of Medicine Division of Pulmonary and Critical Care University of Kansas Disclosures No
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand
 2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
Sepsis Management Update 2014
 Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Diagnosis and Management of Sepsis and Septic Shock. Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire
 Diagnosis and Management of Sepsis and Septic Shock Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire Financial: none Disclosures Objectives: Identify physiologic principles of septic
Diagnosis and Management of Sepsis and Septic Shock Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire Financial: none Disclosures Objectives: Identify physiologic principles of septic
10/25/2017. No financial disclosures. I am NOT a scorpiontologist or jelly fishologist. Jeremy Gonda MD
 10/25/2017 Jeremy Gonda MD Emergency Medicine & Critical Care Renown, REP, Care Flight No financial disclosures I am NOT a scorpiontologist or jelly fishologist 1 10/25/2017 Initial insult (may be minor)
10/25/2017 Jeremy Gonda MD Emergency Medicine & Critical Care Renown, REP, Care Flight No financial disclosures I am NOT a scorpiontologist or jelly fishologist 1 10/25/2017 Initial insult (may be minor)
IV fluid administration in sepsis. Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London
 IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
BC Sepsis Network Emergency Department Sepsis Guidelines
 The provincial Sepsis Clinical Expert Group developed the BC, taking into account the most up-to-date literature (references below) and expert opinion. For more information about the guidelines, and to
The provincial Sepsis Clinical Expert Group developed the BC, taking into account the most up-to-date literature (references below) and expert opinion. For more information about the guidelines, and to
Fluid Resuscitation and Monitoring in Sepsis. Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS
 Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Pediatric Sepsis Treatment:
 Disclosures Pediatric Sepsis Treatment: (treat) Early & (reevaluate) Often None June 11, 2018 Leslie Dervan, MD MS Pacific Northwest Sepsis Conference 1 Agenda Sepsis: pathophysiology at-a-glance Pediatric
Disclosures Pediatric Sepsis Treatment: (treat) Early & (reevaluate) Often None June 11, 2018 Leslie Dervan, MD MS Pacific Northwest Sepsis Conference 1 Agenda Sepsis: pathophysiology at-a-glance Pediatric
Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment
 Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment What is sepsis? Life-threatening organ dysfunction caused by a dysregulated host response to infection A 1991 consensus
Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment What is sepsis? Life-threatening organ dysfunction caused by a dysregulated host response to infection A 1991 consensus
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Diagnosis: Allergies:
 Patient Name: Diagnosis: Allergies: ICU Sepsis Version 5 1/11/17 This order set must be used with an admission order set if patient not already admitted. Nursing Orders Verify that cultures have been obtained
Patient Name: Diagnosis: Allergies: ICU Sepsis Version 5 1/11/17 This order set must be used with an admission order set if patient not already admitted. Nursing Orders Verify that cultures have been obtained
Sepsis & Beyond Guidelines & Goal-Directed Therapy
 Sepsis & Beyond Guidelines & Goal-Directed Therapy Canadian Association of Critical Care Nurses 2014 Quebec City Presented by: Nicole Kupchik RN, MN, CCNS, CCRN, PCCN Objectives Review the 2012 Surviving
Sepsis & Beyond Guidelines & Goal-Directed Therapy Canadian Association of Critical Care Nurses 2014 Quebec City Presented by: Nicole Kupchik RN, MN, CCNS, CCRN, PCCN Objectives Review the 2012 Surviving
IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING
 IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING Christopher Hunter, MD, PhD, FACEP Director, Health Services Department Associate Medical Director, Orange County EMS System Medical Director, Orlando Health
IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING Christopher Hunter, MD, PhD, FACEP Director, Health Services Department Associate Medical Director, Orange County EMS System Medical Director, Orlando Health
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK. Alexandria Rydz
 EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
4/4/2014. Of patients diagnosed with sepsis 50% will develop severe sepsis 25% will develop shock. SIRS Sepsis Severe Septic Sepsis Shock.
 A summary of pathophysiology, therapeutics, and how the pharmacy TECHNICIAN can help improve OUTCOMES Anthony Nelson 2014 Pharm.D. Candidate Tricia Aggers, Pharm.D. Affiliate Faculty, ISU College of Pharmacy
A summary of pathophysiology, therapeutics, and how the pharmacy TECHNICIAN can help improve OUTCOMES Anthony Nelson 2014 Pharm.D. Candidate Tricia Aggers, Pharm.D. Affiliate Faculty, ISU College of Pharmacy
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
Management of Severe Sepsis:
 Management of Severe Sepsis: Update from the Surviving Sepsis Campaign Barbara Birriel, MSN, ACNP-BC, FCCM The Pennsylvania State University NONE Disclosures Review evidence-based international sepsis
Management of Severe Sepsis: Update from the Surviving Sepsis Campaign Barbara Birriel, MSN, ACNP-BC, FCCM The Pennsylvania State University NONE Disclosures Review evidence-based international sepsis
9/15/2017. Joyce Turner RN Director of Clinical Program Development
 Joyce Turner RN Director of Clinical Program Development A toxic response to an infection that spirals out of control attacking the body s own organs and tissues. The infection can be bacterial, viral
Joyce Turner RN Director of Clinical Program Development A toxic response to an infection that spirals out of control attacking the body s own organs and tissues. The infection can be bacterial, viral
EARLY GOAL DIRECTED THERAPY : seminaires iris. Etat des lieux en Daniel De Backer
 EARLY GOAL DIRECTED THERAPY : Etat des lieux en 2017 Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past-President European
EARLY GOAL DIRECTED THERAPY : Etat des lieux en 2017 Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past-President European
-Cardiogenic: shock state resulting from impairment or failure of myocardium
 Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Looking for sepsis. Sepsis: Update. Prevalence of High Profile Dzs. Screening and risk stratification. Mortality of High Profile Diseases
 Sepsis: Update Prevalence of High Profile Dzs Edward A. Panacek, MD, MPH Professor and Chair, Emergency Medicine USA Medical Center, Mobile, AL NDAFP Conference Big Sky. 2016 Syllabus Angus Crit Care Med
Sepsis: Update Prevalence of High Profile Dzs Edward A. Panacek, MD, MPH Professor and Chair, Emergency Medicine USA Medical Center, Mobile, AL NDAFP Conference Big Sky. 2016 Syllabus Angus Crit Care Med
Critical Care Medicine Update for Non-Intensivists 2015
 27 March 2015 Boca Raton Critical Care Medicine Update for Non-Intensivists 2015 MARGARET M. JOHNSON, MD CHAIR, DIVISION OF PULMONARY MEDICINE MAYO CLINIC FLORIDA Critical Care Medicine Update for The
27 March 2015 Boca Raton Critical Care Medicine Update for Non-Intensivists 2015 MARGARET M. JOHNSON, MD CHAIR, DIVISION OF PULMONARY MEDICINE MAYO CLINIC FLORIDA Critical Care Medicine Update for The
Sepsis Update Allina Critical Care Conference February 28, 2018
 Sepsis Update Allina Critical Care Conference February 28, 2018 Sandy Fritzlar, MD Medical Director of the Allina Sepsis Program Emergency Care Consultants OBJECTIVES A brief HISTORY of Sepsis Understand
Sepsis Update Allina Critical Care Conference February 28, 2018 Sandy Fritzlar, MD Medical Director of the Allina Sepsis Program Emergency Care Consultants OBJECTIVES A brief HISTORY of Sepsis Understand
Surviving Sepsis Campaign
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview By professor Ahmad Alaysh BMC-MICU 1 Surviving Sepsis A global program to Reduce mortality rates in severe
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview By professor Ahmad Alaysh BMC-MICU 1 Surviving Sepsis A global program to Reduce mortality rates in severe
Key Points. Angus DC: Crit Care Med 29:1303, 2001
 Sepsis Key Points Sepsis is the combination of a known or suspected infection and an accompanying systemic inflammatory response (SIRS) Severe sepsis is sepsis with acute dysfunction of one or more organ
Sepsis Key Points Sepsis is the combination of a known or suspected infection and an accompanying systemic inflammatory response (SIRS) Severe sepsis is sepsis with acute dysfunction of one or more organ
MAKING SENSE OF IT ALL AUGUST 17
 MAKING SENSE OF IT ALL AUGUST 17 @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser to WHO SCALE AND BURDEN @sepsisuk Dr Ron Daniels B.E.M. CEO, UK Sepsis
MAKING SENSE OF IT ALL AUGUST 17 @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser to WHO SCALE AND BURDEN @sepsisuk Dr Ron Daniels B.E.M. CEO, UK Sepsis
McHenry Western Lake County EMS System CE for Paramedics, EMT-B and PHRN s Sepsis Patients. November/December 2017
 McHenry Western Lake County EMS System CE for Paramedics, EMT-B and PHRN s Sepsis Patients November/December 2017 This month we are going to take a look at the patient with Sepsis. Webster s defines septic
McHenry Western Lake County EMS System CE for Paramedics, EMT-B and PHRN s Sepsis Patients November/December 2017 This month we are going to take a look at the patient with Sepsis. Webster s defines septic
Inflammatory Statements
 Inflammatory Statements Using ETCO 2 Analysis in Sepsis Syndromes George A. Ralls M.D. Orange County EMS System Sepsis Sepsis Over 750,000 cases annually Expected growth of 1.5% per year Over 215,000 deaths
Inflammatory Statements Using ETCO 2 Analysis in Sepsis Syndromes George A. Ralls M.D. Orange County EMS System Sepsis Sepsis Over 750,000 cases annually Expected growth of 1.5% per year Over 215,000 deaths
Current State of Pediatric Sepsis. Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018
 Current State of Pediatric Sepsis Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018 Objectives Review the history of pediatric sepsis Review the current definition of pediatric sepsis Review triage
Current State of Pediatric Sepsis Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018 Objectives Review the history of pediatric sepsis Review the current definition of pediatric sepsis Review triage
Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand
 Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand Vital signs Symptoms LAB BT > 38.3 or < 36 ๐ C HR > 90 bpm RR > 20 /min
Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand Vital signs Symptoms LAB BT > 38.3 or < 36 ๐ C HR > 90 bpm RR > 20 /min
Joel Edminster MD FACEP EMS Live At Night 11/11/2014. Spokane County EMS
 Joel Edminster MD FACEP EMS Live At Night 11/11/2014 Spokane County EMS Objectives Define Sepsis Epidemiology and Relevance Pre-Hospital Impact Making the Diagnosis Appropriate Treatment The term Σήψις
Joel Edminster MD FACEP EMS Live At Night 11/11/2014 Spokane County EMS Objectives Define Sepsis Epidemiology and Relevance Pre-Hospital Impact Making the Diagnosis Appropriate Treatment The term Σήψις
Sepsis 3 & Early Identification. Disclosures. Objectives 9/19/2016. David Carlbom, MD Medical Director, HMC Sepsis Program
 Sepsis 3 & Early Identification David Carlbom, MD Medical Director, HMC Sepsis Program Disclosures I have no relevant financial relationships with a commercial interest and will not discuss off-label use
Sepsis 3 & Early Identification David Carlbom, MD Medical Director, HMC Sepsis Program Disclosures I have no relevant financial relationships with a commercial interest and will not discuss off-label use
Pharmacy, Presentations and Grand Rounds
 Thomas Jefferson University Jefferson Digital Commons Pharmacy, Presentations and Grand Rounds Pharmacy 10-16-2013 An Institution Wide Interdisciplinary Protocol for Improving the Recognition and Treatment
Thomas Jefferson University Jefferson Digital Commons Pharmacy, Presentations and Grand Rounds Pharmacy 10-16-2013 An Institution Wide Interdisciplinary Protocol for Improving the Recognition and Treatment
Ralph Palumbo, MD, FCCP
 Ralph Palumbo, MD, FCCP Septic shock is the leading cause of mortality in patients admitted to the ICU In the United States alone there are over 750,000 cases of severe sepsis and septic shock annually
Ralph Palumbo, MD, FCCP Septic shock is the leading cause of mortality in patients admitted to the ICU In the United States alone there are over 750,000 cases of severe sepsis and septic shock annually
Managing Patients with Sepsis
 Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Sepsis and Hemodynamic Support in September 15, 2017 Carleen Risaliti
 Sepsis and Hemodynamic Support in 2017 September 15, 2017 Carleen Risaliti Objectives Review fluid resuscitation guidelines in septic shock Discuss volume assessment v. fluid responsiveness Evaluate pros
Sepsis and Hemodynamic Support in 2017 September 15, 2017 Carleen Risaliti Objectives Review fluid resuscitation guidelines in septic shock Discuss volume assessment v. fluid responsiveness Evaluate pros
Sepsis and Shock States
 Sepsis and Shock States Presented By: Cynthia Webner BSN, RN, CCRN, CMC www.cardionursing.com CNEA 2009 1 INFECTION Inflammatory response to microorganisms, or Invasion of normally sterile tissues SYSTEMIC
Sepsis and Shock States Presented By: Cynthia Webner BSN, RN, CCRN, CMC www.cardionursing.com CNEA 2009 1 INFECTION Inflammatory response to microorganisms, or Invasion of normally sterile tissues SYSTEMIC
What is. InSpectra StO 2?
 What is InSpectra StO 2? www.htibiomeasurement.com What is InSpectra StO 2? Hemoglobin O 2 saturation is measured in three areas: 1) Arterial (SaO 2, SpO 2 ) Assesses how well oxygen is loading onto hemoglobin
What is InSpectra StO 2? www.htibiomeasurement.com What is InSpectra StO 2? Hemoglobin O 2 saturation is measured in three areas: 1) Arterial (SaO 2, SpO 2 ) Assesses how well oxygen is loading onto hemoglobin
SEPSIS SYNDROME
 INTRODUCTION Sepsis has been defined as a life threatening condition that arises when the body s response to an infection injures its own tissues and organs. Sepsis may lead to shock, multiple organ failure
INTRODUCTION Sepsis has been defined as a life threatening condition that arises when the body s response to an infection injures its own tissues and organs. Sepsis may lead to shock, multiple organ failure
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Shock and hemodynamic monitorization. Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital
 Shock and hemodynamic monitorization Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital Shock Leading cause of morbidity and mortality Worldwide: dehydration and hypovolemic
Shock and hemodynamic monitorization Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital Shock Leading cause of morbidity and mortality Worldwide: dehydration and hypovolemic