Maternal Cardiac Disease Diagnosis and Management
|
|
|
- Kelley Martin
- 5 years ago
- Views:
Transcription



1 Maternal Cardiac Disease Diagnosis and Management Dr. Şevki ÇELEN ZTB Maternity and Teaching Hospital Department of Perinatology
2 Heart diseases in pregnancy Today, 0.2-4% of all pregnancies are accompanied by cardiovascular diseases The most important cause of maternal deaths in developed countries is CVD
3 Congenital heart diseases in developed countries and rheumatic heart diseases in developing countries are more common. Ischemic heart disease and myocardial infarction are rare.
4 Maternal mortality due to cardiac disease was 15.5% in 2007, 18.4% in 2008 and 15.8% in 2009.
5
6 Haemodynamic Changes in Pregnancy Blood volume Cardiac Output (30-50%) Heart rate (10-20/min) Systemic vascular resistance
7 Haemodynamic Changes in Pregnancy Blood pressure; Decreases in first trimester, Returns to normal in second trimester, After the 32 week, it starts to increase slightly. Pregnancy is a kind of STRESS TEST for cardiovascular system The decrease in diastolic blood pressure is greater..


8 Physiological Changes That Produce Thrombosis Risks in Pregnancy Venous stasis Decrease in venous flow Mechanical pressure of the uterus Decrease in movement THROMBOSIS Prothrombotic state Increase in thrombin formation Increase in procoagulant factor levels Factor VII, VIII, X, fibrinogen, von Willebrand factor Decrease in anticoagulant protein S level Acquired active protein C resistance Decrease in fibrinolysis There is a tendency to hypercoagulability in pregnancy.
9 Hemodynamic changes in Labour First Stage Uterine contractions increase heart rate due to increased venous return. Oxygen consumption increases threefold due to sympathetic tonus increase throughout the labour.
10 Hemodynamic changes in Labour Second Stage Intra abdominal pressure increase (Valsalva) increases venous return and increases heart rate (25-50%). Especially in second stage Blood Pressure increases.
11 Hemodynamic changes in Labour Third Stage The venous return increases even further after the uterus has left the pressure on the VCI after birth. The most important hemodynamic changes occur in the first 24 hours of the postpartum.

12 Postpartum hemodynamic changes VCI pressure is off Venous return auto-transfusion Contracted uterus to Systemic circulation Effective blood volume - Blood loss at birth LV filling pressure, Stroke volume and cardiac output Clinical worsening
13 60 40 Maternal Mortality 20 0
14 Classification of the functional capacity of the heart
15 The New York Heart Association (NYHA) CLASS I CLASS II CLASS III CLASS IV Patients with cardiac disease but without resulting limitations of physical activity. Patients with cardiac disease resulting in slight limitation of physical activity. Patients with cardiac disease resulting in marked limitation of physical activity. Patients with cardiac disease resulting in inability to carry on any physical activity without discomfort.
16 Which heart disease has a higher risk of mortality?
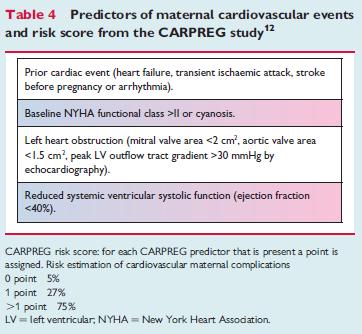
17 1. Low risk for maternal mortality(< %1) (a) Septal defects (b) Cardiac functional capacity I-II (c) Patent ductus arteriosus (d) Pulmonary / Tricuspid lesions 2. Moderate risk for maternal mortality(5-15%) (a) Cardiac functional capacity III-IV (b) Mitral-Aort stenosis (c) Marfan s syndrome(normal aorta) (d) Uncomplicated aortic coarctation (e) MI history
18 3. High risk for maternal mortality (25-50%). (a) Eissenmenger s syndrome (b) Pulmonary hypertension (c) Marfan s syndrome (abnormal aortic root) (d) Peripartum cardiomyopathy (e) Symptomatic obstructive lesions(as, PS) (f) Severe ventricular dysfunction(ef <30% ) (g) Severe cyanotic heart diseases (h) Prostatic valve diseases (ı) Significant uncorrected CHD
19
20
21
22 Valvular disease Regurgitant valve lesions are better tolerated than stenotic lesions. The risk of developing complications in patients with left valve problems is greater than in right valves.
23 Heart Diseases - Management Anticoagulant Medication in Heart Diseases

24 All mechanical heart valve pregnancies need anticoagulant therapy Warfarin is especially suitable for 2nd and 3rd trimester It is recommended that all valve patients receive Aspirin mg at 2 and 3 trimester
25 Warfarin Passes the placenta Abortion, preterm labor, embryopathy in the first trimester (6-12 hft) NS & Eye anomalies(2 3 trimester) Fetal bleeding (especially at birth)

26 What is the optimal management of pregnant women with valvular heart disease in pregnancy? Chan WS Haemostasis women-1234 pregnancies OA during pregnancy Heparin during pregnancy 1.tr Heparin, 2-3.tr OA Embryopathy % Thromboembolic complication % Maternal death % Chan WS Haemostasis 1999
27 1. Trimester Pregnant with mechanical heart valve disease Anticoagulant Therapy Basal Warfarin Dose 5 mg/d Basal Warfarin Dose >5 mg/d Continue Warfarin with INR LMWH (Anti Xa) UFH IV infusion (APTT ) AHA/ACC 2014
28 2 and 3. Trimester Warfarin (INR) and ASA mg 36.W - Before vaginal delivery is planned Warfarin stop and LMWH or IV UFH infusion AHA/ACC 2014
29 Labour After 36 w LMWH therapy IV UFH infusion Labor induction or planned C/S change treatment at least 36 h before IV UFH infusion Stop 4-6 h before birth ESC 2011-AHA/ACC 2014 Begin 4-6 h after birth
30 Heart Diseases - Management Emergency birth management in anticoagulated pregnants
31 Patient using Warfarin Cesarean section is necessary if birth is started during warfarin treatment. The fresh frozen plasma can be given before the cesarean section to keep the INR within the range of Oral K vit (0.5-1 mg) may be given, but the effect requires 4-6 hours to start
32 Patient using UFH / LMWH Protamine should be used (1 ml Protamine neutralizes 1000 IU heparin) It should not be forgotten that Protamine will partially reduce the effect of LMWH
33 Heart Diseases - Management Infective endocarditis prophylaxis in heart patients


34 Routine IE prophylaxis is not recommended for every vaginal or caesarean delivery
35 Antibiotic prophylaxis is only; History of infective endocarditis Artificial valve replacement Complex cyanotic heart disease Heart transplantation

36
37 Dilated cardiomyopathy and pregnancy Pregnancy is not recommended for EF<40% Termination is recommended if pregnancy has occurred. EF 40-50%, if the effort test is bad, the functional capacity can not tolerate pregnancy.
38 JAMA. 2000;283(9):
39 Peripartum CMP- Etiology Dedected in 2-4 thousand live births Etiology was not clearly demonstrated. Angiogenic disorders Prolactin Inflammatory cytokines Myokarditis Abnormal immune response
40 Peripartum CMP-Risk factors Pregnancies over 30 years Race Multiple pregnancies Preeclampsia-Eclampsia-Chronic HT history Maternal cocaine use Long-term oral tocolytic therapy with β- adrenergics
41 Peripartum CMP-Prognosis Complete or near complete improvement is seen within 6 months after delivery at 50-60%. Worsening, heart failure and transplantation need Mortality rate 10-32% Repetitive risk for subsequent gestation is 30%

42 Mortality 25% Complete cure 46%

43 Chest Pain- Management Generally, emergency service issue
44 Cardiac causes ACUTE CORONARY SYNDROME ACUTE PULMONARY EMBOLISM ACUTE AORT DISSECTION ACUTE MYO-PERİCARDİTİS! HIGH MORTALITY RISK, THESE DIAGNOSIS SHOULD BE EXCLUDED BEFORE LEAVİNG ER
45 Patients presenting with chest pain to the ER Monitorisation, Vital signs Medical History / Physical examination EKG Blood sample for routine tests These steps must be completed within 10 minutes of the patient entering the emergency department door.
46 Differential diagnosis 1. Step Which clinic is compatible with chest pain? 2. Step Which clinic is compatible with physical examination and ECG findings? 3. Step Biomarkers for preliminary confirmation 4. Step Imaging methods for preliminary confirmation and determination of treatment
47 Heart Diseases - Management Heart diseases Antenatal care
48 Frequency Cardiologic follow-up According to the modified WHO classification; I 1-2 times during pregnancy II Each trimester II-III Each trimester every month III At least once a month twice a month IV Contraindicated Termination If pregnancy continues, at least once a month - twice a month
49 Heart Diseases - Management Heart Diseases - Birth planning
50 Vaginal delivery should be preferred In those with normal cardiac function, spontaneous term delivery should be preferred. Oxytocin is suitable for induction of labor There is no absolute contraindication for misoprostol and dinoprostone
51 Cesarean section indications Birth with warfarin treatment Marfan syndrome (aortic root> 45 mm) Acute or chronic aortic dissection Patients with severe heart failure
52 Suitable for caesarean section; Severe aortic stenosis Severe PHT Eisenmenger syndrome Patients with mechanical heart valve
53 Epidural analgesia/anesthesia is recommended Delivery can be assisted by forceps or vacuum extraction. Routine antibiotic prophylaxis is not recommended
54 Labour If the cervix is appropriate; Oxytocin Artifical rupture of membranes If the cervix is not appropriate; Mechanical Foley catheter CRB (Cervical Ripening Baloon) Prostoglandine
55 Preterm labour-tocolysis İndomethacin Nifedipine Beta adrenerjik agonist Atosiban (oxytocin receptor antagonist)
56 Postpartum Hemodynamic and ECG monitoring should continue for hours postnatally.
57 Pregnancy outcomes
58 - Premature birth 17% - RDS and IVH 3% (for premature infants 16%) - Fetal and Neonatal mortality 1% Risk factors for poor pregnancy outcomes NYHA III-IV Cyanosis Left cardiac stenosis Smoking Multiple pregnancy Use of anticoagulant throughout pregnancy
59 Heredity Increased risk for recurrence risks in offspring of adults with CHD % J Am Coll Cardiol 2003; 42:923 J Am Coll Cardiol 1994; 23:1459 Lancet 1998; 351:311 Circulation 2001; 104:515 All pregnancies with CHD, fetal ECO should be recommended during gestational weeks
60 Which method of contraception is appropriate for heart disease?
61 WHO medical eligibility for contraceptive use: Cardiovascular disease (2010) Multiple risk for arterial CVD (age, DM, HT, smoking ) COC POP DMPA Cu-IUD LNG-IUD 3/ DVT/PE WHO 1-Appropriate WHO 2-Preferable WHO 3-Should be used with caution WHO 4- Contraindicated
62 COC POP DMPA Cu-IUD LNG-IUD Valvular HD Uncomplicated Complicated (PHT, Risk of atrial fibrillation, subacute bacterial endocarditis history) PPCMP Normal Moderate to severe cardiac dysfunction WHO 1-Appropriate WHO 2-Preferable WHO 3-Should be used with caution WHO 4- Contraindicated
63 Monitoring, treatment and care of a pregnancy candidate or pregnant woman with heart disease is a team work Midwife Family physician Obstetrician Cardiologists Anesthetist Pediatricians
64 THANK YOU
Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!!
 Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!! Abha'Khandelwal,'MD,'MS' 'Stanford'University'School'of'Medicine'
Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!! Abha'Khandelwal,'MD,'MS' 'Stanford'University'School'of'Medicine'
ESC Guidelines on the Management of Cardiovascular Diseases during Pregnancy
 ESC Guidelines on the Management of Cardiovascular Diseases during Pregnancy Task force on the management of CVD during pregnancy of the ESC Chair: Vera Regitz-Zagrosek, Charite, Berlin None DECLARATION
ESC Guidelines on the Management of Cardiovascular Diseases during Pregnancy Task force on the management of CVD during pregnancy of the ESC Chair: Vera Regitz-Zagrosek, Charite, Berlin None DECLARATION
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials
 Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Pregnancy and Congenital Heart Disease Case Review Heidi M. Connolly, M.D. Professor of Medicine Chair for Education
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Pregnancy and Congenital Heart Disease Case Review Heidi M. Connolly, M.D. Professor of Medicine Chair for Education
Pregnancy and Heart Disease. Shilpa Kshatriya, MD, FACC Heartland Cardiology, PA
 Pregnancy and Heart Disease Shilpa Kshatriya, MD, FACC Heartland Cardiology, PA Pregnancy and the Heart 2 % of pregnancies involve maternal CV disease CV disease does not preclude pregnancy but poses risk
Pregnancy and Heart Disease Shilpa Kshatriya, MD, FACC Heartland Cardiology, PA Pregnancy and the Heart 2 % of pregnancies involve maternal CV disease CV disease does not preclude pregnancy but poses risk
Pregnancy and Heart Disease. Alexandra A Frogoudaki Adult Congenital Heart Clinic ATTIKON University Hospital
 Pregnancy and Heart Disease Alexandra A Frogoudaki Adult Congenital Heart Clinic ATTIKON University Hospital Pregnancy is not a state Hemodynamic changes During pregnancy Estrogens 1. Renin 2.
Pregnancy and Heart Disease Alexandra A Frogoudaki Adult Congenital Heart Clinic ATTIKON University Hospital Pregnancy is not a state Hemodynamic changes During pregnancy Estrogens 1. Renin 2.
Maternal Cardiac Disease In Pregnancy. August 25, 2017 PREGNANCY ECHO CONFERENCE
 Maternal Cardiac Disease In Pregnancy August 25, 2017 PREGNANCY ECHO CONFERENCE Maternal Physiology Cardiac Output = HR x SV Non-pregnant: 4.5 L/min Pregnant: 6.0 L/min Increase most acute in first 10
Maternal Cardiac Disease In Pregnancy August 25, 2017 PREGNANCY ECHO CONFERENCE Maternal Physiology Cardiac Output = HR x SV Non-pregnant: 4.5 L/min Pregnant: 6.0 L/min Increase most acute in first 10
Valve Disease in the Pregnant Patient
 Valve Disease in the Pregnant Patient Julie B. Damp, MD December 6, 2012 VanderbiltHeart.com If single, do not allow marriage. If fertile, do not allow pregnancy. If pregnant, do not allow delivery. If
Valve Disease in the Pregnant Patient Julie B. Damp, MD December 6, 2012 VanderbiltHeart.com If single, do not allow marriage. If fertile, do not allow pregnancy. If pregnant, do not allow delivery. If
PREGNANCY AND CONGENITAL HEART DISEASE
 PREGNANCY AND CONGENITAL HEART DISEASE SIDDHARTH JADHAV M.D. Assistant Professor of Radiology E.B. Singleton Department of Pediatric Radiology Texas Children's Hospital COMMERCIAL DISCLOSURE - None Objectives
PREGNANCY AND CONGENITAL HEART DISEASE SIDDHARTH JADHAV M.D. Assistant Professor of Radiology E.B. Singleton Department of Pediatric Radiology Texas Children's Hospital COMMERCIAL DISCLOSURE - None Objectives
SESSION D5. The Heart of the Matter: Cardiac Disease in Pregnancy Brad M. Dolinsky, MD, MFM
 37th Annual Advanced Practice in Primary and Acute Care Conference: October 9-11, 2014 2:45 SESSION D5 Session Description: The Heart of the Matter: Cardiac Disease in Pregnancy Brad M. Dolinsky, MD, MFM
37th Annual Advanced Practice in Primary and Acute Care Conference: October 9-11, 2014 2:45 SESSION D5 Session Description: The Heart of the Matter: Cardiac Disease in Pregnancy Brad M. Dolinsky, MD, MFM
Pregnancy and Cardiovascular Disease
 Pregnancy and Cardiovascular Disease Cindy M. Martin, M.D. Co-Director, Adult Congenital and Cardiovascular Genetics Center No Disclosures Objectives Discuss the hemodynamic changes during pregnancy Define
Pregnancy and Cardiovascular Disease Cindy M. Martin, M.D. Co-Director, Adult Congenital and Cardiovascular Genetics Center No Disclosures Objectives Discuss the hemodynamic changes during pregnancy Define
EVALUATION OF PREGNANT PATIENTS WITH HEART DISEASE. Karen Stout, MD University of Washington Seattle Children s Seattle, WA
 EVALUATION OF PREGNANT PATIENTS WITH HEART DISEASE Karen Stout, MD University of Washington Seattle Children s Seattle, WA CASE PRESENTATION 24 year old woman with aortic regurgitation referred for evaluation
EVALUATION OF PREGNANT PATIENTS WITH HEART DISEASE Karen Stout, MD University of Washington Seattle Children s Seattle, WA CASE PRESENTATION 24 year old woman with aortic regurgitation referred for evaluation
Using an anti-xa level nomogram to adjust intravenous unfractionated heparin infusion for arrhythmia in pregnancy
 Using an anti-xa level nomogram to adjust intravenous unfractionated heparin infusion for arrhythmia in pregnancy W. Sia, E. Toor, N. Wahab, J. Windram, R. Khurana Cardiac Problems in Pregnancy Congress
Using an anti-xa level nomogram to adjust intravenous unfractionated heparin infusion for arrhythmia in pregnancy W. Sia, E. Toor, N. Wahab, J. Windram, R. Khurana Cardiac Problems in Pregnancy Congress
Cardiac disease in pre pr gnancy
 IN THE NAME OF GOD Cardiac disease in pregn nancy MITRAL STENOSIS 33 y/o G3L2(2c/s) GA 34 + 5 CC: LP & dyspnea PMHx: MS sinse 4 yrs ago due to Rheumatism PSHx: 2c/s DHx: metoral 50 mg q6h/ ASA/ Enoxaparin
IN THE NAME OF GOD Cardiac disease in pregn nancy MITRAL STENOSIS 33 y/o G3L2(2c/s) GA 34 + 5 CC: LP & dyspnea PMHx: MS sinse 4 yrs ago due to Rheumatism PSHx: 2c/s DHx: metoral 50 mg q6h/ ASA/ Enoxaparin
Maternal And Fetal Outcome In Pregnancies Complicated With Maternal Cardiac Diseases: Experience At A Tertiary Care Hospital
 ISPUB.COM The Internet Journal of Gynecology and Obstetrics Volume 19 Number 1 Maternal And Fetal Outcome In Pregnancies Complicated With Maternal Cardiac Diseases: Experience At A Tertiary Care Hospital
ISPUB.COM The Internet Journal of Gynecology and Obstetrics Volume 19 Number 1 Maternal And Fetal Outcome In Pregnancies Complicated With Maternal Cardiac Diseases: Experience At A Tertiary Care Hospital
More History. Organization. Maternal Cardiac Disease: a historical perspective. The Parturient with Cardiac Disease 9/21/2012
 The Parturient with Cardiac Disease Pamela Flood M.D. Professor of Anesthesia and Perioperative Care Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco Maternal Cardiac
The Parturient with Cardiac Disease Pamela Flood M.D. Professor of Anesthesia and Perioperative Care Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco Maternal Cardiac
HEART DISEASE IN PREGNANCY
 HEART DISEASE IN PREGNANCY DR. JOSHI SUYAJNA D. www.suyajna.com VIMS-BELLARY Pre-conceptional counseling a. Objective Risk assessment with» 1. Clarke s table 2. NYHA b. Feasibility of pregnancy care c.
HEART DISEASE IN PREGNANCY DR. JOSHI SUYAJNA D. www.suyajna.com VIMS-BELLARY Pre-conceptional counseling a. Objective Risk assessment with» 1. Clarke s table 2. NYHA b. Feasibility of pregnancy care c.
Καρδιοπάθειες και κύηση. Υπάρχουν ενδείξεις διακοπής; Λαζαρίδου Φωτεινή, ΕΒ Καρδιολόγος Νοσοκομείο «Αγ Παύλος», Θεσσαλονίκη
 Καρδιοπάθειες και κύηση. Υπάρχουν ενδείξεις διακοπής; Λαζαρίδου Φωτεινή, ΕΒ Καρδιολόγος Νοσοκομείο «Αγ Παύλος», Θεσσαλονίκη ~ 3% of women 18 44 years of age have cardiac disease ~ 1% of pregnancies are
Καρδιοπάθειες και κύηση. Υπάρχουν ενδείξεις διακοπής; Λαζαρίδου Φωτεινή, ΕΒ Καρδιολόγος Νοσοκομείο «Αγ Παύλος», Θεσσαλονίκη ~ 3% of women 18 44 years of age have cardiac disease ~ 1% of pregnancies are
Έγκυος και συγγενής καρδιοπάθεια: Τι πρέπει να γνωρίζει ο Καρδιολόγος Ενηλίκων
 Έγκυος και συγγενής καρδιοπάθεια: Τι πρέπει να γνωρίζει ο Καρδιολόγος Ενηλίκων Αντώνιος Π. Βλάχος Αναπληρωτής Καθηγητής Παιδοκαρδιολογίας Πανεπιστήμιο Ιωαννίνων No conflict of interest Pregnancy and CHD
Έγκυος και συγγενής καρδιοπάθεια: Τι πρέπει να γνωρίζει ο Καρδιολόγος Ενηλίκων Αντώνιος Π. Βλάχος Αναπληρωτής Καθηγητής Παιδοκαρδιολογίας Πανεπιστήμιο Ιωαννίνων No conflict of interest Pregnancy and CHD
Congenital Heart Disease Patient and Pregnancy
 Congenital Heart Disease Patient and Pregnancy Gurur Biliciler-Denktas, M.D. Assistant Professor Division of Pediatric Cardiology, Department of Pediatrics The University of Texas Health Science Center
Congenital Heart Disease Patient and Pregnancy Gurur Biliciler-Denktas, M.D. Assistant Professor Division of Pediatric Cardiology, Department of Pediatrics The University of Texas Health Science Center
Rate of CHD at birth: 4~12/1,000
 Risk assessment and management for the pregnant ACHD woman Suk-Joo Choi Department of Obstetrics and Gynecology Samsung Medical Center Sungkyunkwan k University i School of Medicine i Cardiac diseases
Risk assessment and management for the pregnant ACHD woman Suk-Joo Choi Department of Obstetrics and Gynecology Samsung Medical Center Sungkyunkwan k University i School of Medicine i Cardiac diseases
A pregnant patient with a prosthetic valve Giacomo Boccuzzi, MD, FESC
 A pregnant patient with a prosthetic valve Giacomo Boccuzzi, MD, FESC Department of Invasive Cardiology, Ospedale San Giovanni Bosco, Turin, Italy *C.V. was born the 24th May 1980 Rheumatic fever during
A pregnant patient with a prosthetic valve Giacomo Boccuzzi, MD, FESC Department of Invasive Cardiology, Ospedale San Giovanni Bosco, Turin, Italy *C.V. was born the 24th May 1980 Rheumatic fever during
Pregnancy and Heart Disease
 Pregnancy and Heart Disease Heidi M. Connolly, MD No disclosures 2011 MFMER 3138928-1 Regitz-Zagrosek V, Lundqvist C, Borghi C, et al. Pregnancy and the Heart 2% of pregnancies involve maternal CV disease
Pregnancy and Heart Disease Heidi M. Connolly, MD No disclosures 2011 MFMER 3138928-1 Regitz-Zagrosek V, Lundqvist C, Borghi C, et al. Pregnancy and the Heart 2% of pregnancies involve maternal CV disease
Cardiac Disease in Pregnancy
 Cardiac Disease in Pregnancy DATE: SEPTEMBER 11, 2016 PRESENTED BY: ABIGAIL KHAN, MD Outline Scope of the problem Physiology of pregnancy Cardiac risk in pregnancy Pregnancy management Contraception 1
Cardiac Disease in Pregnancy DATE: SEPTEMBER 11, 2016 PRESENTED BY: ABIGAIL KHAN, MD Outline Scope of the problem Physiology of pregnancy Cardiac risk in pregnancy Pregnancy management Contraception 1
Anatomy & Physiology
 1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
Focused. se with 2008 F. lar Heart Diseas. date. ents With Valvul. Upd. gement of Patie. lines for Manag. HA 2006 Guidel ACC/AH. Fig.
 ACC/AH HA 2006 Guidel nic severe AI (Fig. 4). ned by age, ay also be helpful nd echo. For AI, ollow up may be or MRI rather than mension; SD, end lines for Manag gement of Patie Upd ents With Valvul date
ACC/AH HA 2006 Guidel nic severe AI (Fig. 4). ned by age, ay also be helpful nd echo. For AI, ollow up may be or MRI rather than mension; SD, end lines for Manag gement of Patie Upd ents With Valvul date
Cardiac disease in pregnancy guideline (GL802)
") Cardiac disease in pregnancy guideline (GL802) Approval Approval Group Job Title, Chair of Committee Date Maternity & Children s Services Clinical Governance Committee Chair, Maternity Clinical Governance
Cardiac disease in pregnancy guideline (GL802) Approval Approval Group Job Title, Chair of Committee Date Maternity & Children s Services Clinical Governance Committee Chair, Maternity Clinical Governance
Survival Rates of Children with Congenital Heart Disease continue to improve.
 DOROTHY RADFORD Survival Rates of Children with Congenital Heart Disease continue to improve. 1940-20% 1960-40% 1980-70% 2010->90% Percentage of children with CHD reaching age of 18 years 1938 First Patent
DOROTHY RADFORD Survival Rates of Children with Congenital Heart Disease continue to improve. 1940-20% 1960-40% 1980-70% 2010->90% Percentage of children with CHD reaching age of 18 years 1938 First Patent
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
Cardiovascular disease complicates 1% to 3% of all
 Pregnancy Complicated by Valvular Heart Disease: An Update Michael Nanna, MD; Kathleen Stergiopoulos, MD, PhD, FASE, FACC, FAHA Cardiovascular disease complicates 1% to 3% of all pregnancies and is responsible
Pregnancy Complicated by Valvular Heart Disease: An Update Michael Nanna, MD; Kathleen Stergiopoulos, MD, PhD, FASE, FACC, FAHA Cardiovascular disease complicates 1% to 3% of all pregnancies and is responsible
RF & RHD Workshop 22 nd March MANAGEMENT of RHEUMATIC HEART DISEASE in PREGNANCY. Dr Dorothy Radford
 RF & RHD Workshop 22 nd March 2016 MANAGEMENT of RHEUMATIC HEART DISEASE in PREGNANCY Dr Dorothy Radford PREGNANCY PHYSIOLOGY Increased cardiac output 30%-50% Increased blood volume 30%-50% Increased heart
RF & RHD Workshop 22 nd March 2016 MANAGEMENT of RHEUMATIC HEART DISEASE in PREGNANCY Dr Dorothy Radford PREGNANCY PHYSIOLOGY Increased cardiac output 30%-50% Increased blood volume 30%-50% Increased heart
Uptofate Study Summary
 CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
Peripartum management of Rheumatic Heart Disease
 Peripartum management of Rheumatic Heart Disease Dr James Sartain Director of Anaesthesia & Perioperative Medicine Cairns & Hinterland Hospital & Health Service Talk outline Why (still) talk about RHD
Peripartum management of Rheumatic Heart Disease Dr James Sartain Director of Anaesthesia & Perioperative Medicine Cairns & Hinterland Hospital & Health Service Talk outline Why (still) talk about RHD
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Peripartum Cardiomyopathy. Lavanya Rai Manipal
 Peripartum Cardiomyopathy Lavanya Rai Manipal Definition - PPCM - Dilated cardiomyopathy of unknown cause resulting in cardiac failure that occurs in the peripartum period in women without any preexisting
Peripartum Cardiomyopathy Lavanya Rai Manipal Definition - PPCM - Dilated cardiomyopathy of unknown cause resulting in cardiac failure that occurs in the peripartum period in women without any preexisting
Management of Heart Failure and Cardiomyopathies in Pregnancy
 Management of Heart Failure and Cardiomyopathies in Pregnancy Professor Sanjay Sharma Disclosures: None Epidemiology of Cardiac Disease In Pregnancy Cardiovascular disease in pregnancy is increasing in
Management of Heart Failure and Cardiomyopathies in Pregnancy Professor Sanjay Sharma Disclosures: None Epidemiology of Cardiac Disease In Pregnancy Cardiovascular disease in pregnancy is increasing in
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials
 Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Pregnancy and Congenital Heart Disease Heidi M. Connolly, M.D. Professor of Medicine Chair for Education Division
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Pregnancy and Congenital Heart Disease Heidi M. Connolly, M.D. Professor of Medicine Chair for Education Division
What to do when a heart failure patient becomes pregnant
 BSH Heart Failure Day for Revalidation and Training 2017 What to do when a heart failure patient becomes pregnant Dr Diane Barker Consultant Cardiologist Royal Stoke Hospital Conflicts of interest - sponsorship,
BSH Heart Failure Day for Revalidation and Training 2017 What to do when a heart failure patient becomes pregnant Dr Diane Barker Consultant Cardiologist Royal Stoke Hospital Conflicts of interest - sponsorship,
Outline. Maternal Congenital Heart Disease in Pregnancy. Maternal congenital heart disease. Cardiovascular disease in pregnancy 10/18/2017
 I have no disclosures or conflicts of interest to report. Maternal Congenital Heart Disease in Pregnancy Jennifer A. Jolley, MD Associate Clinical Professor University of California, Irvine Department
I have no disclosures or conflicts of interest to report. Maternal Congenital Heart Disease in Pregnancy Jennifer A. Jolley, MD Associate Clinical Professor University of California, Irvine Department
How to manage the pregnant woman with heart disease
 How to manage the pregnant woman with heart disease Dr Fiona Walker, The Heart Hospital,UCLH, London Dr Sara Thorne, University Hospital Birmingham Dr Cathy Head, The Heart Hospital, UCLH, London Dr Kate
How to manage the pregnant woman with heart disease Dr Fiona Walker, The Heart Hospital,UCLH, London Dr Sara Thorne, University Hospital Birmingham Dr Cathy Head, The Heart Hospital, UCLH, London Dr Kate
The Effect of Valvular Heart Diseases on Maternal and Fetal Outcome of Pregnancy Nada Salih Ameen*,Nawfal Fawzi Anwer**
 THE VALVULAR IRAQI POSTGRADUATE HEART DISEASES MEDICAL AND JOURNAL PREGNANCY The Effect of Valvular Heart Diseases on Maternal and Fetal Outcome of Pregnancy Nada Salih Ameen*,Nawfal Fawzi Anwer** ABSTRACT:
THE VALVULAR IRAQI POSTGRADUATE HEART DISEASES MEDICAL AND JOURNAL PREGNANCY The Effect of Valvular Heart Diseases on Maternal and Fetal Outcome of Pregnancy Nada Salih Ameen*,Nawfal Fawzi Anwer** ABSTRACT:
Review Article Heart Disease and Pregnancy
 Hellenic J Cardiol 47: 275-291, 2006 Review Article Heart Disease and Pregnancy AIKATERINI CHAMAIDI, MICHAEL A. GATZOULIS Adult Congenital Heart Centre and Centre for Pulmonary Hypertension, Royal Brompton
Hellenic J Cardiol 47: 275-291, 2006 Review Article Heart Disease and Pregnancy AIKATERINI CHAMAIDI, MICHAEL A. GATZOULIS Adult Congenital Heart Centre and Centre for Pulmonary Hypertension, Royal Brompton
Susan P. D Anna MSN, APRN BC February 14, 2019
 Is there Equal Opportunity in Heart Failure?? Susan P. D Anna MSN, APRN BC February 14, 2019 Disclosures: I have no financial disclosures. I am not an expert on this topic, but see a lot of women with
Is there Equal Opportunity in Heart Failure?? Susan P. D Anna MSN, APRN BC February 14, 2019 Disclosures: I have no financial disclosures. I am not an expert on this topic, but see a lot of women with
PHYSIOLOGICAL CHANGES IN PREGNANCY AND OBSTETRIC EMERGENCIES
 PHYSIOLOGICAL CHANGES IN PREGNANCY AND OBSTETRIC EMERGENCIES Shankari Arulkumaran BSc MSc MD MRCOG Consultant Obstetrician and Gynaecologist St Mary s Hospital Imperial College NHS Trust OVERVIEW Obstetric
PHYSIOLOGICAL CHANGES IN PREGNANCY AND OBSTETRIC EMERGENCIES Shankari Arulkumaran BSc MSc MD MRCOG Consultant Obstetrician and Gynaecologist St Mary s Hospital Imperial College NHS Trust OVERVIEW Obstetric
Heart Failure treatment during pregnancy
 Heart Failure treatment during pregnancy Angeles Alonso García Hospital Universitario Puerta de Hierro. Majadahonda. Madrid. Spain European Society of Cardiology. Stockholm. 29 August 2010 Starting Point
Heart Failure treatment during pregnancy Angeles Alonso García Hospital Universitario Puerta de Hierro. Majadahonda. Madrid. Spain European Society of Cardiology. Stockholm. 29 August 2010 Starting Point
Pregnancy, Heart Disease and Imaging. Hemodynamics. Decreased systemic vascular resistance. Physiology anemia
 Pregnancy, Heart Disease and Imaging Sangeeta Shah, MD, FASE, FACC Associate Professor, Ochsner Clinical School of Medicine Advanced CV Imaging and Adult Congenital Heart Disease New Orleans, LA Hemodynamics
Pregnancy, Heart Disease and Imaging Sangeeta Shah, MD, FASE, FACC Associate Professor, Ochsner Clinical School of Medicine Advanced CV Imaging and Adult Congenital Heart Disease New Orleans, LA Hemodynamics
Catherine Nelson-Piercy. Guy s & St Thomas Hospitals & Queen Charlotte s Hospital London, UK
 Cardiac Disease and Pregnancy Catherine Nelson-Piercy Guy s & St Thomas Hospitals & Queen Charlotte s Hospital London, UK Physiological changes in pregnancy Cardiac Output (CO) increases by 40% Further
Cardiac Disease and Pregnancy Catherine Nelson-Piercy Guy s & St Thomas Hospitals & Queen Charlotte s Hospital London, UK Physiological changes in pregnancy Cardiac Output (CO) increases by 40% Further
Anticoagulation Therapy and Valve Surgery. Dr Pau Kiew Kong Consultant Cardiothoracic Surgeon
 Anticoagulation Therapy and Valve Surgery Dr Pau Kiew Kong Consultant Cardiothoracic Surgeon Outline of lecture 1. Type of Valve Surgery 2. Anticoagulation requirements 3. Mechanical (Metallic) prosthetic
Anticoagulation Therapy and Valve Surgery Dr Pau Kiew Kong Consultant Cardiothoracic Surgeon Outline of lecture 1. Type of Valve Surgery 2. Anticoagulation requirements 3. Mechanical (Metallic) prosthetic
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acid base balance pregnancy-related changes to, 640 Acquired heart disease, 731 Acute fatty liver of pregnancy (AFLP), 618 Acute kidney
Index Note: Page numbers of article titles are in boldface type. A Acid base balance pregnancy-related changes to, 640 Acquired heart disease, 731 Acute fatty liver of pregnancy (AFLP), 618 Acute kidney
The dos and don ts των νέων Κατευθυντηρίων Οδηγιών της Ευρωπαϊκής Καρδιολογικής Εταιρείας Για την καρδιαγγειακή νόσο στην εγκυμοσύνη
 The dos and don ts των νέων Κατευθυντηρίων Οδηγιών της Ευρωπαϊκής Καρδιολογικής Εταιρείας Για την καρδιαγγειακή νόσο στην εγκυμοσύνη Θωμάς Κ. Μακρής, MD FA, FES Συντονιστής Διευθυντής Καρδιολογικού Τμήματος
The dos and don ts των νέων Κατευθυντηρίων Οδηγιών της Ευρωπαϊκής Καρδιολογικής Εταιρείας Για την καρδιαγγειακή νόσο στην εγκυμοσύνη Θωμάς Κ. Μακρής, MD FA, FES Συντονιστής Διευθυντής Καρδιολογικού Τμήματος
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014
 Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Images in Cardiovascular Medicine
 Images in Cardiovascular Medicine Management of Severe Mitral Stenosis During Pregnancy Rebecca S. Norrad, MBBS; Omid Salehian, MSc, MD, FRCPC, FACC, FAHA A 37-year-old woman originally from Iraq was referred
Images in Cardiovascular Medicine Management of Severe Mitral Stenosis During Pregnancy Rebecca S. Norrad, MBBS; Omid Salehian, MSc, MD, FRCPC, FACC, FAHA A 37-year-old woman originally from Iraq was referred
Effect of maternal heart disease on pregnancy outcomes
 Expert Review of Obstetrics & Gynecology ISSN: 1747-4108 (Print) 1747-4116 (Online) Journal homepage: http://www.tandfonline.com/loi/ierb20 Effect of maternal heart disease on pregnancy outcomes Emily
Expert Review of Obstetrics & Gynecology ISSN: 1747-4108 (Print) 1747-4116 (Online) Journal homepage: http://www.tandfonline.com/loi/ierb20 Effect of maternal heart disease on pregnancy outcomes Emily
Index. cardiology.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACHD. See Adult congenital heart disease (ACHD) Adult congenital heart disease (ACHD), 503 512 across life span prevalence of, 504 506
Index Note: Page numbers of article titles are in boldface type. A ACHD. See Adult congenital heart disease (ACHD) Adult congenital heart disease (ACHD), 503 512 across life span prevalence of, 504 506
CASE DISCUSSION. Dr JAYASREE VEERABOINA 2nd yr PG MS OBG
 CASE DISCUSSION Dr JAYASREE VEERABOINA 2nd yr PG MS OBG Normal Cardiovascular changes in Pregnancy CARDIAC OUTPUT 5 th wk -- starts 12 wks -- 30-35% 30-32 wks -- 40% During labour -- 50% After delivery
CASE DISCUSSION Dr JAYASREE VEERABOINA 2nd yr PG MS OBG Normal Cardiovascular changes in Pregnancy CARDIAC OUTPUT 5 th wk -- starts 12 wks -- 30-35% 30-32 wks -- 40% During labour -- 50% After delivery
By Dr.Asmaa Al sanjary
 By Dr.Asmaa Al sanjary Preterm delivery is defined by a birth occurring before 37 completed weeks of gestation. Prematurity is multifactorial and its incidence has increased during the last decade in most
By Dr.Asmaa Al sanjary Preterm delivery is defined by a birth occurring before 37 completed weeks of gestation. Prematurity is multifactorial and its incidence has increased during the last decade in most
Cardiology Competency Based Goals and Objectives
 Cardiology Competency Based Goals and Objectives COMPETENCY 1. Patient Care. Provide family centered patient care that is developmentally and age appropriate, compassionate, and effective for the treatment
Cardiology Competency Based Goals and Objectives COMPETENCY 1. Patient Care. Provide family centered patient care that is developmentally and age appropriate, compassionate, and effective for the treatment
Peripartum kardiomyopati
 Fall 3 Peripartum kardiomyopati Roman A roch 2017 01 26 2 3 Dg. PPCM Symptoms ECG, pro-bnp echocardiography 4 Peripartum cardiomyopathy: a systematic literature review Acta Obstetricia et Gynecologica
Fall 3 Peripartum kardiomyopati Roman A roch 2017 01 26 2 3 Dg. PPCM Symptoms ECG, pro-bnp echocardiography 4 Peripartum cardiomyopathy: a systematic literature review Acta Obstetricia et Gynecologica
Congenital heart disease. By Dr Saima Ali Professor of pediatrics
 Congenital heart disease By Dr Saima Ali Professor of pediatrics What is the most striking clinical finding in this child? Learning objectives By the end of this lecture, final year student should be able
Congenital heart disease By Dr Saima Ali Professor of pediatrics What is the most striking clinical finding in this child? Learning objectives By the end of this lecture, final year student should be able
Mitral Valve Disease, When to Intervene
 Mitral Valve Disease, When to Intervene Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Current ACC/AHA guideline Stages
Mitral Valve Disease, When to Intervene Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Current ACC/AHA guideline Stages
Ventricular tachyarrhythmia during pregnancy in women with heart disease: data from the ROPAC
 Ventricular tachyarrhythmia during pregnancy in women with heart disease: data from the ROPAC Ebru Ertekin MD, Iris M. Van Hagen MD, Amar M. Salam MD, Titia P.E. Ruys MD PhD, Jolien W. Roos-Hesselink MD
Ventricular tachyarrhythmia during pregnancy in women with heart disease: data from the ROPAC Ebru Ertekin MD, Iris M. Van Hagen MD, Amar M. Salam MD, Titia P.E. Ruys MD PhD, Jolien W. Roos-Hesselink MD
Results of Ischemic Heart Disease
 Ischemic Heart Disease: Angina and Myocardial Infarction Ischemic heart disease; syndromes causing an imbalance between myocardial oxygen demand and supply (inadequate myocardial blood flow) related to
Ischemic Heart Disease: Angina and Myocardial Infarction Ischemic heart disease; syndromes causing an imbalance between myocardial oxygen demand and supply (inadequate myocardial blood flow) related to
Heart disease complicating pregnancy management strategies
 www.slcog.lk/sljog LEADING ARTICLE Heart disease complicating pregnancy management strategies Priyadharshan P¹ Introduction Heart disease is the third most common cause of maternal death and the leading
www.slcog.lk/sljog LEADING ARTICLE Heart disease complicating pregnancy management strategies Priyadharshan P¹ Introduction Heart disease is the third most common cause of maternal death and the leading
CONGENITAL HEART DISEASE (CHD)
") CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
Acute Coronary Syndrome. Sonny Achtchi, DO
 Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
UC SF DISCLOSURES MANAGEMENT OF MATERNAL CONGENITAL HEART DISEASE OBJECTIVES. No financial disclosures CARDIOVASCULAR CHANGES ANTEPARTUM 6/10/2011
 DISCLOSURES MANAGEMENT OF MATERNAL CONGENITAL HEART DISEASE No financial disclosures UC SF Lena H. Kim, MD AIM CONFERENCE June 10, 2011 spicecomments.com OBJECTIVES Physiologic cardiovascular changes of
DISCLOSURES MANAGEMENT OF MATERNAL CONGENITAL HEART DISEASE No financial disclosures UC SF Lena H. Kim, MD AIM CONFERENCE June 10, 2011 spicecomments.com OBJECTIVES Physiologic cardiovascular changes of
Imaging Cardiovascular Disease in Pregnancy
 Imaging Cardiovascular Disease in Pregnancy Karen Ordovas MD, MAS Associate Professor of Radiology and Medicine Director of Cardiac Imaging University of California San Francisco Cardiac MRI during pregnancy
Imaging Cardiovascular Disease in Pregnancy Karen Ordovas MD, MAS Associate Professor of Radiology and Medicine Director of Cardiac Imaging University of California San Francisco Cardiac MRI during pregnancy
Expert consensus document on management of cardiovascular diseases during pregnancy
 European Heart Journal (2003) 24, 761 781 Guidelines Expert consensus document on management of cardiovascular diseases during pregnancy The Task Force on the Management of Cardiovascular Diseases During
European Heart Journal (2003) 24, 761 781 Guidelines Expert consensus document on management of cardiovascular diseases during pregnancy The Task Force on the Management of Cardiovascular Diseases During
CARDIAC DISEASE IN PREGNANCY: TUTORIAL 2 TUTORIAL OF THE WEEK TH NOVEMBER 2008
 CARDIAC DISEASE IN PREGNANCY: TUTORIAL 2 TUTORIAL OF THE WEEK 118 10 TH NOVEMBER 2008 Dr. Abbi Walker, Christchurch Hospital, New Zealand Dr. Matt Rucklidge, Royal Devon & Exeter Hospital, UK mattrucklidge@yahoo.co.uk
CARDIAC DISEASE IN PREGNANCY: TUTORIAL 2 TUTORIAL OF THE WEEK 118 10 TH NOVEMBER 2008 Dr. Abbi Walker, Christchurch Hospital, New Zealand Dr. Matt Rucklidge, Royal Devon & Exeter Hospital, UK mattrucklidge@yahoo.co.uk
Supplemental Digital Content: Definitions Based on the International Classification of Diseases, Ninth Revision, Clinical Modification
 Supplemental Digital Content: Definitions Based on the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) Diagnose and Procedures Codes 1. ICD-9-CM definition of
Supplemental Digital Content: Definitions Based on the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) Diagnose and Procedures Codes 1. ICD-9-CM definition of
Effects of pregnancy-related hemodynamic and hormonal changes
 Information extracted from WWW.HEARTDISEASEANDPREGNANCY.COM CORONARY ARTERY DISEASE Background Coronary artery disease (CAD) is the leading cause of death worldwide in women. It has already been noted
Information extracted from WWW.HEARTDISEASEANDPREGNANCY.COM CORONARY ARTERY DISEASE Background Coronary artery disease (CAD) is the leading cause of death worldwide in women. It has already been noted
CMS Limitations Guide - Radiology Services
 CMS Limitations Guide - Radiology Services Starting October 1, 2015, CMS will update their existing medical necessity limitations on tests and procedures to correspond to ICD-10 codes. This limitations
CMS Limitations Guide - Radiology Services Starting October 1, 2015, CMS will update their existing medical necessity limitations on tests and procedures to correspond to ICD-10 codes. This limitations
2) VSD & PDA - Dr. Aso
 VSD & PDA - Dr. Aso") 2) VSD & PDA - Dr. Aso Ventricular Septal Defect (VSD) Most common cardiac malformation 25-30 % Types of VSD: According to position perimembranous, inlet, muscular. According to size small, medium, large.
2) VSD & PDA - Dr. Aso Ventricular Septal Defect (VSD) Most common cardiac malformation 25-30 % Types of VSD: According to position perimembranous, inlet, muscular. According to size small, medium, large.
Holy Crap! Why is a Cardiologist Speaking at a GI Meeting? Jonathan A. Rapp, MD, FACC, FSCAI Cardiologist, Mercy Heart Institute Cincinnati, OH
 Holy Crap! Why is a Cardiologist Speaking at a GI Meeting? Jonathan A. Rapp, MD, FACC, FSCAI Cardiologist, Mercy Heart Institute Cincinnati, OH Goals and Objectives Discuss cardiac considerations for patients
Holy Crap! Why is a Cardiologist Speaking at a GI Meeting? Jonathan A. Rapp, MD, FACC, FSCAI Cardiologist, Mercy Heart Institute Cincinnati, OH Goals and Objectives Discuss cardiac considerations for patients
Valvular defects. Lectures from Pathological Physiology. Study materials from Pathological Physiology, 2017/2018 Oliver Rácz, Eva Sedláková
 Valvular defects Lectures from Pathological Physiology Study materials from Pathological Physiology, 2017/2018 Oliver Rácz, Eva Sedláková 1 2 3 1 Valvular dysfunction - introduction Stenosis block of flow;
Valvular defects Lectures from Pathological Physiology Study materials from Pathological Physiology, 2017/2018 Oliver Rácz, Eva Sedláková 1 2 3 1 Valvular dysfunction - introduction Stenosis block of flow;
Pregnancy and cyanotic congenital heart disease. A. Pijuan Domènech (U. de C. Congènites de l Adult) Hospital Vall d Hebron Barcelona, Spain
 Hospital Vall d Hebron Barcelona, Spain") Pregnancy and cyanotic congenital heart disease A. Pijuan Domènech (U. de C. Congènites de l Adult) Hospital Vall d Hebron Barcelona, Spain I have nothing to disclose. Pregnancy and cyanotic congenital
Pregnancy and cyanotic congenital heart disease A. Pijuan Domènech (U. de C. Congènites de l Adult) Hospital Vall d Hebron Barcelona, Spain I have nothing to disclose. Pregnancy and cyanotic congenital
The right ventricle in chronic heart failure
 The right ventricle in chronic heart failure ESC 2012 Christian Opitz, Berlin There are no conflicts of interest relevant to this presentation Percent of Population Prevalence of Heart Failure by Age and
The right ventricle in chronic heart failure ESC 2012 Christian Opitz, Berlin There are no conflicts of interest relevant to this presentation Percent of Population Prevalence of Heart Failure by Age and
A Challenging Case: Von Willebrand Disease and Pulmonary Hypertension in Pregnancy
 A Challenging Case: Von Willebrand Disease and Pulmonary Hypertension in Pregnancy Diana S. Wolfe, MD, MPH Assistant Professor Department of Obstetrics & Gynecology and Women s Health Associate Fellowship
A Challenging Case: Von Willebrand Disease and Pulmonary Hypertension in Pregnancy Diana S. Wolfe, MD, MPH Assistant Professor Department of Obstetrics & Gynecology and Women s Health Associate Fellowship
Screening for Critical Congenital Heart Disease
 Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
Aerobic Exercise Screening Stratification Tool
 Aerobic Screening Stratification Tool Disclaimer: The Aerobics Screening Stratification Tool is a working document currently used within the Stroke Rehabilitation Service of St. Joseph s Care Group- Thunder
Aerobic Screening Stratification Tool Disclaimer: The Aerobics Screening Stratification Tool is a working document currently used within the Stroke Rehabilitation Service of St. Joseph s Care Group- Thunder
Drugs used in obstetrics
 Drugs used in obstetrics Drugs used in obstetrics Drugs may be used to modify uterine contractions. These include oxytocic drugs used to stimulate uterine contractions both in induction of labour and to
Drugs used in obstetrics Drugs used in obstetrics Drugs may be used to modify uterine contractions. These include oxytocic drugs used to stimulate uterine contractions both in induction of labour and to
Birth Control in Patients with Congenital Heart Disease
 Birth Control in Patients with Congenital Heart Disease Arwa Saidi MB. BCh. MEd. FACC University of Florida Departments of Pediatrics and Internal Medicine Gainesville, FL There are an increasing number
Birth Control in Patients with Congenital Heart Disease Arwa Saidi MB. BCh. MEd. FACC University of Florida Departments of Pediatrics and Internal Medicine Gainesville, FL There are an increasing number
Pregnancy and Heart Disease Sharon L. Roble, MD Echo Hawaii 2016
 1 Pregnancy and Heart Disease Sharon L. Roble, MD Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Cardiovascular Effects of Pregnancy Anatomic Ventricular muscle mass increases
1 Pregnancy and Heart Disease Sharon L. Roble, MD Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Cardiovascular Effects of Pregnancy Anatomic Ventricular muscle mass increases
Clinical study of cardiac diseases during pregnancy
 International Journal of Reproduction, Contraception, Obstetrics and Gynecology Kamat AV et al. Int J Reprod Contracept Obstet Gynecol. 2016 Mar;5(3):855-859 www.ijrcog.org pissn 2320-1770 eissn 2320-1789
International Journal of Reproduction, Contraception, Obstetrics and Gynecology Kamat AV et al. Int J Reprod Contracept Obstet Gynecol. 2016 Mar;5(3):855-859 www.ijrcog.org pissn 2320-1770 eissn 2320-1789
PRIMARY PULMONARY ARTERIAL HYPERTENSION AND PREGNANCY HOW PREPARED ARE WE?
 PRIMARY PULMONARY ARTERIAL HYPERTENSION AND PREGNANCY HOW PREPARED ARE WE? DR TARAKESWARI S DR SUBHASHINI Y Pulmonary hypertension (PH) is an increase of blood pressure in the pulmonary artery, pulmonary
PRIMARY PULMONARY ARTERIAL HYPERTENSION AND PREGNANCY HOW PREPARED ARE WE? DR TARAKESWARI S DR SUBHASHINI Y Pulmonary hypertension (PH) is an increase of blood pressure in the pulmonary artery, pulmonary
Preterm Labour and Tocolysis
 Title: CLINICAL GUIDELINES ID TAG Preterm Labour and Tocolysis Authors: Designation: Speciality / Division: Directorate: Dr L Bell, Dr K Price, Dr G McKeown, Mr D Sim Trainee, Trainee, CAH Consultant,
Title: CLINICAL GUIDELINES ID TAG Preterm Labour and Tocolysis Authors: Designation: Speciality / Division: Directorate: Dr L Bell, Dr K Price, Dr G McKeown, Mr D Sim Trainee, Trainee, CAH Consultant,
Heart Valves: Before and after surgery
 Heart Valves: Before and after surgery Tim Sutton, Consultant Cardiologist Middlemore Hospital, Auckland Auckland Heart Group Indications for intervention in Valvular disease To prevent sudden death and
Heart Valves: Before and after surgery Tim Sutton, Consultant Cardiologist Middlemore Hospital, Auckland Auckland Heart Group Indications for intervention in Valvular disease To prevent sudden death and
ACHD & Heart Disease and Pregnancy: Guidelines and Cases Michael A. Gatzoulis
 ACHD & Heart Disease and Pregnancy: Guidelines and Cases Michael A. Gatzoulis Adult Congenital Heart Centre & National Centre for Pulmonary Hypertension Royal Brompton Hospital/National Heart & Lung Institute,
ACHD & Heart Disease and Pregnancy: Guidelines and Cases Michael A. Gatzoulis Adult Congenital Heart Centre & National Centre for Pulmonary Hypertension Royal Brompton Hospital/National Heart & Lung Institute,
Notes by Sandra Dankwa 2009 HF- Heart Failure DS- Down Syndrome IE- Infective Endocarditis ET- Exercise Tolerance. Small VSD Symptoms -asymptomatic
 Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Identification and Management of Cardiac Conditions During Labor and Delivery
 Identification and Management of Cardiac Conditions During Labor and Delivery 1 Contact Hour First Published: May 27, 2011 Course Review: July 21, 2014 Course Review: July 21, 2017 Course Expires: July
Identification and Management of Cardiac Conditions During Labor and Delivery 1 Contact Hour First Published: May 27, 2011 Course Review: July 21, 2014 Course Review: July 21, 2017 Course Expires: July
UKMEC SUMMARY TABLE HORMONAL AND INTRAUTERINE CONTRACEPTION
 SUMMARY TABLE SUMMARY TABLE HORMONAL AND INTRAUTERINE CONTRACEPTION Cu-IUD = Copper-bearing intrauterine device; LNG-IUS = Levonorgestrel-releasing intrauterine system; IMP = Progestogen-only implant;
SUMMARY TABLE SUMMARY TABLE HORMONAL AND INTRAUTERINE CONTRACEPTION Cu-IUD = Copper-bearing intrauterine device; LNG-IUS = Levonorgestrel-releasing intrauterine system; IMP = Progestogen-only implant;
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition
 Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Pathology. Congenital heart disease. congenital heart diseases. congenital heart diseases - etiology. lecture 7
 Pathology lecture 7 prof hab. n. med. Andrzej Marszałek Congenital heart disease congenital heart diseases Def.: anatomical anomalies present at delivery ambnormal embryogenesis 3. and 8. week of gestation
Pathology lecture 7 prof hab. n. med. Andrzej Marszałek Congenital heart disease congenital heart diseases Def.: anatomical anomalies present at delivery ambnormal embryogenesis 3. and 8. week of gestation
Detailed Order Request Checklists for Cardiology
 Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
Invasive and Medical Treatments for Atrial Fibrillation. Thomas J Dresing, MD Section of Electrophysiology and Pacing Cleveland Clinic
 Invasive and Medical Treatments for Thomas J Dresing, MD Section of Electrophysiology and Pacing Cleveland Clinic Disclosures Fellow s advisory panel for St Jude Medical Speaking honoraria from: Boston
Invasive and Medical Treatments for Thomas J Dresing, MD Section of Electrophysiology and Pacing Cleveland Clinic Disclosures Fellow s advisory panel for St Jude Medical Speaking honoraria from: Boston
MEDICAL SCIENCES Vol.I -Adult Congenital Heart Disease: A Challenging Population - Khalid Aly Sorour
 ADULT CONGENITAL HEART DISEASE: A CHALLENGING POPULATION Khalid Aly Sorour Cairo University, Kasr elaini Hospital, Egypt Keywords: Congenital heart disease, adult survival, specialized care centers. Contents
ADULT CONGENITAL HEART DISEASE: A CHALLENGING POPULATION Khalid Aly Sorour Cairo University, Kasr elaini Hospital, Egypt Keywords: Congenital heart disease, adult survival, specialized care centers. Contents
Clinical Indications for Echocardiography
 Clinical Indications for Echocardiography Echocardiography is widely utilised and potential applications are increasing with advances in technology. The aim of this document is two-fold: 1) To define clinical
Clinical Indications for Echocardiography Echocardiography is widely utilised and potential applications are increasing with advances in technology. The aim of this document is two-fold: 1) To define clinical
Asthma in Pregnancy, Labour and Postnatal Guidelines
 Asthma in Pregnancy, Labour and Postnatal Guidelines N.B. Staff should be discouraged from printing this document. This is to avoid the risk of out of date printed versions of the document. The Intranet
Asthma in Pregnancy, Labour and Postnatal Guidelines N.B. Staff should be discouraged from printing this document. This is to avoid the risk of out of date printed versions of the document. The Intranet
Understanding the Pediatric Ventricular Assist Device
 Understanding the Pediatric Ventricular Assist Device W. James Parks, MSc., MD Pediatric Cardiologist Assistant Professor of Pediatrics and Radiology Children s Healthcare of Atlanta Sibley Heart Center
Understanding the Pediatric Ventricular Assist Device W. James Parks, MSc., MD Pediatric Cardiologist Assistant Professor of Pediatrics and Radiology Children s Healthcare of Atlanta Sibley Heart Center
Atlas of Practical Cardiac Applications of MRI
 Atlas of Practical Cardiac Applications of MRI Atlas of Practical Cardiac Applications of MRI Guillcm Pons-LIado, MD. Director, Cardiac Imaging Unit, Cardiology Department, Hospital de la Santa Creu i
Atlas of Practical Cardiac Applications of MRI Atlas of Practical Cardiac Applications of MRI Guillcm Pons-LIado, MD. Director, Cardiac Imaging Unit, Cardiology Department, Hospital de la Santa Creu i
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or