Καρδιοπάθειες και κύηση. Υπάρχουν ενδείξεις διακοπής; Λαζαρίδου Φωτεινή, ΕΒ Καρδιολόγος Νοσοκομείο «Αγ Παύλος», Θεσσαλονίκη
|
|
|
- Gillian O’Connor’
- 5 years ago
- Views:
Transcription

1 Καρδιοπάθειες και κύηση. Υπάρχουν ενδείξεις διακοπής; Λαζαρίδου Φωτεινή, ΕΒ Καρδιολόγος Νοσοκομείο «Αγ Παύλος», Θεσσαλονίκη
2 ~ 3% of women years of age have cardiac disease ~ 1% of pregnancies are complicated by cardiac disease. Cardiac conditions account for 10 25% of maternal mortality in the USA In the past, rheumatic heart disease was the most common form of cardiac disease in pregnant women; it still predominates in developing countries and in immigrant populations in the USA. Advanced maternal age +underlying medical conditions (HT, DM, Chol) increase the incidence of acquired heart disease complicating pregnancy. Congenital heart disease in pregnancy is increasingly common as more affected women are surviving into reproductive age. US Department of Health and Human Services, Health Resources and Services Administration, Maternal and Child Health Bureau. Women s Health USA Rockville, MD: US Department of Health and Human Services; Burlew BS. Managing the pregnant patient with heart disease. Clin Cardiol 1990; 13: Koonin LM, Atrash HK, Lawson HW, Smith JC. Maternal mortality surveillance, United States, MMWR Morb Mortal Wkly Rep 1991;40:1-13.

3 Maternal mortality rates from cardiac causes of death in the UK The progressive rise in cardiac deaths is more related to acquired disease, such as myocardial infarction and cardiomyopathy
4 The leading cardiac causes of maternal death in UK are now acquired disease, rising from 3.8 per million in 1990 to 20.8 per million in Myocardial infarction (MI), aortic dissection and cardiomyopathy are the main diseases. Rheumatic heart disease has re emerged as a cause of maternal health in immigrants Current Opinion in Obstetrics and Gynecology 2009, 21:
5 Heart 2004;90:

6 Hemodynamic alterations
7 Heart 2004;90:

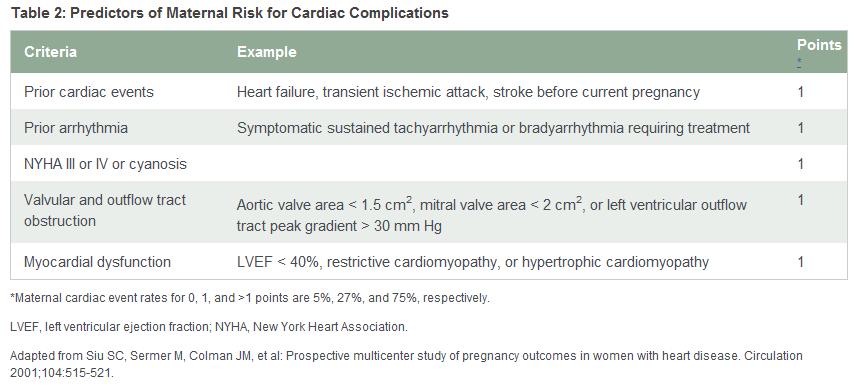
8 Predictors of cardiovascular complications during pregnancy in the CARPREG study The estimated risk of complications during pregnancy in patients with heart disease, but no risk factors, was 5%; with 1 risk factor, 27%; and with 2 risk factors, 75%.
9 Fetal complications/ prognosis Siu et al documented that the incidence of fetal complications (premature delivery and low birth weight) reached 20%, and severe complications (respiratory distress syndrome, intracranial bleeding and death) were confirmed in 5%. The factors that exacerbated fetal prognosis were NYHA class > II or cyanotic heart disease, anticoagulant therapy, smoking, multiple pregnancy and left ventricular obstruction In addition to the above factors, another study documented other risk factors; severe pulmonary regurgitation and right ventricular dysfunction Siu: Circulation 2001; 104: Khairy: Circulation 2006; 113:
10
11 Congenital heart lesions
12 Congenital heart disease is the most common congenital defect (approximately 1% of newborns are affected around the world). At least 85% of patients with congenital heart disease now survive to adulthood and half of them are women, most of reproductive age.

13 Non cyanotic heart disease: L R shunts Left to right shunts (ASD, VSD, PFO, and PDA) are sometimes diagnosed during pregnancy due to loud heart murmur from increased shunt volume caused by increased circulating blood volume. In pts with large shunt volume, decreases in peripheral vascular resistance balances out the increased blood volume. If no pulmonary hypertension then pregnancy, labor and delivery are completed without any complications. Risk of paradoxical embolism during labor and delivery VSD, 3 rd trimester VSD, 1 year after delivery In case of rapid bleeding, peripheral vasoconstriction may increase shunt blood flow, decrease cardiac output and cause congestive heart failure, shock and ventricular fibrillation. J Echocardiogr Vol.6, No.2, 2008 Cleveland clinic J of Medicine Vol 71, No 12, 2004
14 Aortic stenosis Most cases are congenital (bicuspid) or are associated with mitral stenosis AS is a risk factor for fetal complications. All pts with symptomatic AS should postpone pregnancy until after heart surgery. The risk is generally low if mean aortic gradient remains 50mmHg during pregnancy If pts remain severely symptomatic relieve aortic stenosis before delivery: Balloon aortic valvotomy in experienced centers Pregnant women with bicuspid AV associated with aortic dilatation are at risk for spontaneous aortic dissection, usually 3rd trimester, especially if there is an associated aortic coarctation For women planning pregnancy, prophylactic aortic root or ascending aorta surgery should be considered if the aortic diameter is >45mm, the rate of increase in diameter is 5 mm/year and/or there is worsening aortic regurgitation (AR).
15 AORTIC COARCTATION Maternal mortality in women with unrepaired aortic coarctation (CoA) has been estimated to be 3%. The main complications reported are associated with severe hypertension, including aortic dissection. MRI should be used before pregnancy, but can be safely performed during pregnancy if there is concern about recoarctation or aneurysm formation. Blood pressure should be controlled with b blockers. Changes in the aortic wall during pregnancy increase the risk inherent to CoA.
16 Pulmonary Stenosis (PS) Mild (<50mmHg), moderate (50 79mmHg) PS, or PS treated by valvuloplasty or surgery is well tolerated during pregnancy, with good maternal and fetal prognosis. However, in patients with severe PS, pregnancy can cause right sided heart failure or atrial arrhythmias.
17 Cyanotic heart disease without pulmonary hypertension During pregnancy, systemic vascular resistance decreases to elevate right to left shunt, thus exacerbating cyanosis. While the incidence of complications is high in pregnant women with cyanotic heart diseases, cyanosis is treatable and mortality risk is low. In patients without pulmonary hypertension, e.g., pulmonary atresia managed via Blalock Taussig shunt (BT), mortality during pregnancy is around 5%. Maternal risk for such patients depends largely on ventricular function (other risks hemohrrage, paradoxical embolism, heart failure, increasing cyanosis) Fetal prognosis is poor, and in severe cyanosis, fetal development is hindered (the rate of live births is 12% at 85% oxygen saturation). In one study of 96 pregnancies in 44 patients with cyanotic heart diseases, maternal cardiac complications were seen in 32%, and the rate of live births was 43%. Hemoglobin 16g/dL and oxygen saturation 85% were found to be prognosticators Circulation 1994;89:
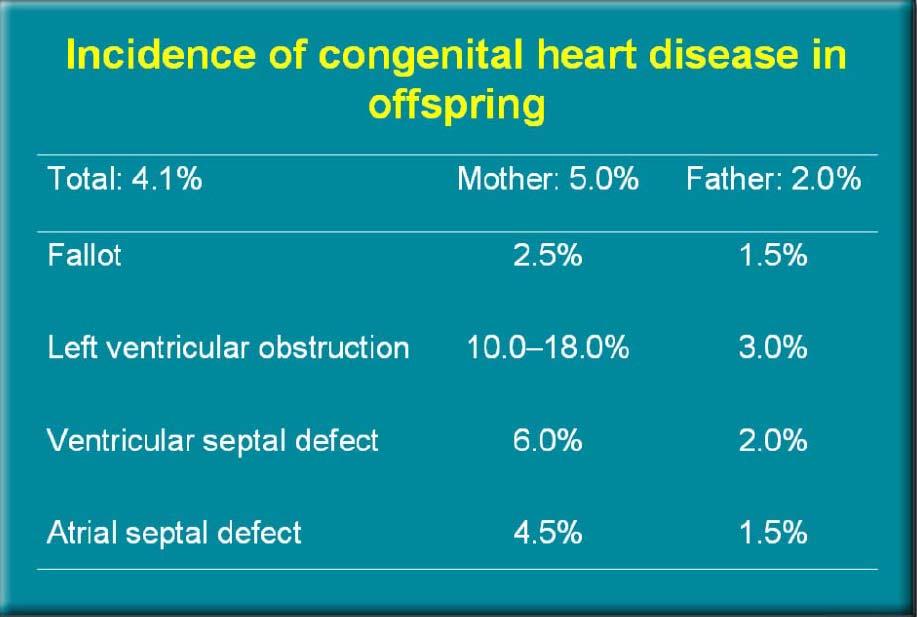
18 Cyanotic heart disease after surgical correction TOF In patients with good functional class (NYHA class I or II) and sinus rhythm, pregnancy and delivery are possible, but the incidence of miscarriage is high. The children of mothers with TOF have a 3% possibility of having some type of heart disease Repaired tetralogy of Fallot (TOF): In patients who underwent corrective surgery, pregnancy and delivery are possible. (delivery rate: 73%, cardiac events: 14%) [J Am Coll Cardiol 2004; 44: ]). Pregnancy risk factors included: residual VSD, moderate to severe pulmonary valve stenosis and insufficiency, aortic insufficiency, pulmonary hypertension, dilated aorta ( 40 mm), ventricular dysfunction, and past history of tachyarrhythmia.
19 Repaired cyanotic heart disease (TOF systemic RV) Pregnancy is well tolerated in women who have had radical repair of tetralogy of Fallot, as long as ventricular function is good and there is no significant right ventricular outflow tract obstruction (delivery rate: 73%, cardiac events: 14%) Pregnancy is likely to be well tolerated in asymptomatic patients with congenitally corrected transposition of the great arteries (ctga). However, systemic right ventricular function may deteriorate during pregnancy, presenting with heart failure With the exceptions of a narrowed pulmonary venous pathway or development of pulmonary vascular disease, pregnancy is usually well tolerated in NYHA class I II patients post Mustard. Post Fontan type operation: these patients are often advised against pregnancy. However, the maternal risk of pregnancy is not prohibitively high in NYHA class I II patients, provided ventricular function is good. Ventricular failure and arrhythmia are the main causes of maternal morbidity.
20 Marfan s syndrome During pregnancy, estrogen and other hormones make vessels more fragile, and as a result, in pregnant women with Marfan s syndrome, the risk for aortic dissection is higher than in non pregnant women. An aortic root diameter >40 mm in women with MFS identifies a high risk group, with risk of dissection during pregnancy ~ 10% (ESC2003). The 2010 ACC/AHA/American Association of Thoracic Surgeons (AATS) guidelines for the thoracic aorta note that it is reasonable to prophylactically replace the aortic root and ascending aorta if the aortic diameter exceeds 40 mm in women with MFS who are contemplating pregnancy. At <40 mm, normal delivery is possible. Treatment with beta blockers should be maintained during pregnancy J Echocardiogr Vol.6, No.2, 2008 Rev Esp Cardiol. 2006;59(9):971-84
21 Pulmonary hypertension Eisenmengers syndrome In patients with primary pulmonary hypertension, maternal mortality exceeds 50%, and pregnancy is contraindicated. In patients with Eisenmenger syndrome, maternal mortality ranges from 30 to 70%, and fetal mortality is as high as 50% Pulmonary hypertension is tolerated badly during pregnancy because of insufficient adaptation of the right heart to increases in cardiac output, in association with a poorly compliant pulmonary vasculature. The greatest risk occurs in the peripartum period and most deaths occur between 2 and 9 days postpartum Br J Obstet Gynaecol 1998; 105: J Am Coll Cardiol 1999; 34: Br J Anaesth 2004; 93:
22 Rheumatic Heart Disease Aquired Heart Disease Cardiomyopathies


23 Valvuloplasty or surgery in all symptomatic patients should be considered before pregnancy Beta-blockers should be prescribed to all symptomatic woman or whose PAP> than 50 mm Hg Patients who are symptomatic despite medical treatment should be considered for balloon mitral valvuloplasty during pregnancy Rev Esp Cardiol. 2006;59(9):971-84

24 Algorithm for the management of mitral stenosis in the pregnant patient. MS, mitral stenosis; PBMV, percutaneous balloon mitral valvuloplasty.
25 ACC/ AHA 2006 guidelines for the management of patients with valvular heart disease: Circulation 2006; 114: e
26 Prosthetic heart valves Mechanical heart valves are associated with an increased incidence of thromboembolic events during pregnancy. The procoagulant state of pregnancy increases the risk of valve thrombus formation among women with mechanical valves. Approximately 30 to 35% of heterograft prostheses and 10 to 20% of homograft prostheses fail within 10 to 15 years of implantation
27 Anticoagulant regimen Choice of anticoagulant regimen is a balance between maternal and foetal risks. The incidence of valve thrombosis is lower with oral anticoagulants (warfarin) than with UFH or LMWH, but foetal risk is higher. Warfarin embryopathy occurs in 4 10% of cases and may be dose dependent, the risk being less at doses below 5mg daily Both UFH and LMWH are safer for the foetus as they do not cross the placenta
28 ESC 2007 and ACC/AHA 2006 guidelines recommend continuing oral anticoagulants until pregnancy is confirmed. Thereafter, the treatment options include (1) continuation of warfarin until week 36 [ (INR) 3.0], dose adjusted UFH [(APPT) twice control] or LMWH (anti Xa levels U/ml 4 h after administration) until delivery, (2) dose adjusted LMWH/UFH 6 12 weeks and close to term with warfarin at other times and (3) dose adjusted LMWH throughout pregnancy. Low dose aspirin (75 to 162 mg/day) might be added to women deemed to be at high thromboembolic risk
29 Peripartum cardiomyopathy In peripartum cardiomyopathy, cardiac function recovers in about half of patients, but in this relatively rare disease (occurring in 1 in pregnancies), 20% of patients die or require a heart transplant. Maternal mortality is up to 20%. Adverse risk factors include age > 30 years, multiparity, twin pregnancy, and the 50% of women in whom left ventricular dilation and dysfunction persist. The risk for cardiac events during first or subsequent pregnancy is dependent on the severity of left ventricular dysfunction N Engl J Med 2001; 344:
30 Hypertrophic cardiomyopathy Among pregnant women with hypertrophic cardiomyopathy, maternal mortality is around 1%, and most patients can go through pregnancy. However, in about half of the patients who had symptoms before pregnancy, the NYHA functional class was exacerbated (NYHA class III/IV) during pregnancy. We often recognize elevated intraventricular pressure gradient and pulmonary hypertension in obstructive patients. Beta blockers should not be discontinued during pregnancy, avoiding severe vasodilatation, and vaginal childbirth should be indicated. J Am Coll Cardiol 2002; 40:
31 Dilated cardiomyopathy (DCM) In dilated cardiomyopathy, because prognosis is poor, especially for young patients, and most patients take medication such as an ACE inhibitor, very few patients become pregnant. Pregnancy is poorly tolerated in women with DCM. The risk of maternal death is approximately 7% if the patient is in NYHA functional class III or IV. Other adverse risks factors include EF < 20%, mitral regurgitation, right ventricular failure, atrial fibrillation, and systemic hypotension. Such patients should be counselled against pregnancy
32 Supraventricular arrhytmias The most common arrhythmia in women with structurally normal hearts is paroxysmal supraventricular tachycardia (PSVT), including AVNRT and AVRT. Management with vagal manouvres, adenosine, AV nodal blocking agents (ie,digoxin, beta blockers, or verapamil). If hemodynamic compromise is evident, DC cardioversion should be performed. AF and flutter during pregnancy are less common than PSVT and often occur in women with structural heart disease. In pregnant women with atrial fibrillation, a rhythm control strategy is preferred Pregnancy is a prothrombotic state, and thresholds for initiating anticoagulation are often lower than in the nonpregnant state. There is no standardized anticoagulation regime during pregnancy and the choice of anticoagulation should be tailored to the individual.
33 Ventricular arrhythmias Arrhythmias are the most common cardiac complication encountered during pregnancy in women with and without structural heart disease. Ventricular tachyarrhythmias are frequently associated with acquired or structural heart disease Monomorphic ventricular tachycardia without apparent structural heart disease is considered idiopathic. The most common type originates from the right ventricular outflow tract, and this form of ventricular tachycardia can often be successfully treated with beta blockers or verapamil. Women with the long QT syndrome are at risk for ventricular tachycardia, especially in the postpartum period. Ventricular tachyarrhythmias in the presence of structural heart disease are potentially lifethreatening and require immediate evaluation for hemodynamic instability to determine whether electrical cardioversion or defibrillation is indicated. Circulation. 2001;104(5):515.
34 Myocardial infarction Incidence of 6.2 in 100,000 pregnancies (data ). mortality 37 50% Most cases occur in the third trimester and six week postpartum period. In a review of 103 cases from , coronary artery morphology was evaluated in 96 by arteriography or autopsy. coronary atherosclerosis with or without intracoronary thrombus (40 %), thrombus in a normal coronary artery (8 %), coronary artery dissection (27%),(near term or postpartum, affecting LAD, mortality 30 40%) spasm in (2%), emboli (2%), and normal coronary arteries (13%). J Am Coll Cardiol. 2008;52(3):171.

35 ACS management Low dose aspirin (75 to 162 mg/day), beta blockers, and nitrates Pregnancy is a relative contraindication to fibrinolytic therapy (postpartum bleeding). Heparin does not cross the placenta and thus does not affect the fetus directly. Bleeding complications (eg, threatened miscarriage) Angiotensin converting enzyme inhibitors, angiotensin II receptor blockers, and statins are contraindicated in pregnancy.
36 Infective Endocarditis Diagnosis and treatment are the same as outside pregnancy If gentamycin is used, drug levels should be measured (risk for foetal deafness) Decision for surgery should be made early as the foetal risk is determined on the maternal condition Antibiotic prophylaxis should be given in Prosthetic valves History of previous endocarditis

37 Cardiovascular drugs used during pregnancy
38 Title

39
40
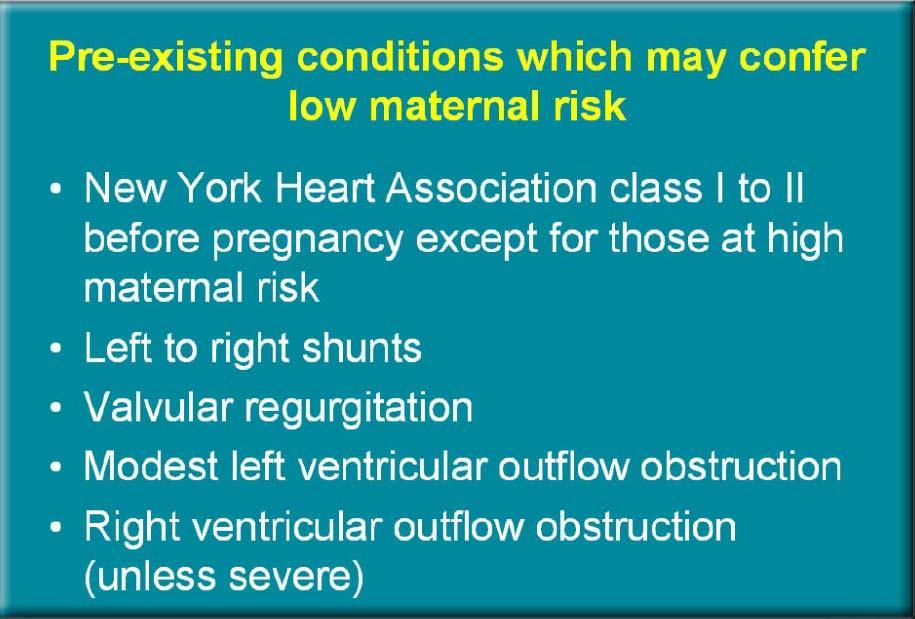
41 Risk assessment before pregnancy Risk assessment can be aquired from Cardiovascular history and examination ECG Echo Arterial O2 saturation measurement Risk can be stratified according to Nature of lesion Maternal functional class or cyanosis Use of risk index (functional class, LV systolic dysfunction, left heart obstruction, cardiac event arrhythmia, stroke,pulmonary edema ) Maternal age Neonatal risk Risk for transmission (CHD) Anticipated maternal and paternal survival (CHD)
42
43
Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!!
 Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!! Abha'Khandelwal,'MD,'MS' 'Stanford'University'School'of'Medicine'
Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!! Abha'Khandelwal,'MD,'MS' 'Stanford'University'School'of'Medicine'
Pregnancy and Heart Disease. Shilpa Kshatriya, MD, FACC Heartland Cardiology, PA
 Pregnancy and Heart Disease Shilpa Kshatriya, MD, FACC Heartland Cardiology, PA Pregnancy and the Heart 2 % of pregnancies involve maternal CV disease CV disease does not preclude pregnancy but poses risk
Pregnancy and Heart Disease Shilpa Kshatriya, MD, FACC Heartland Cardiology, PA Pregnancy and the Heart 2 % of pregnancies involve maternal CV disease CV disease does not preclude pregnancy but poses risk
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials
 Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Pregnancy and Congenital Heart Disease Case Review Heidi M. Connolly, M.D. Professor of Medicine Chair for Education
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Pregnancy and Congenital Heart Disease Case Review Heidi M. Connolly, M.D. Professor of Medicine Chair for Education
Maternal Cardiac Disease In Pregnancy. August 25, 2017 PREGNANCY ECHO CONFERENCE
 Maternal Cardiac Disease In Pregnancy August 25, 2017 PREGNANCY ECHO CONFERENCE Maternal Physiology Cardiac Output = HR x SV Non-pregnant: 4.5 L/min Pregnant: 6.0 L/min Increase most acute in first 10
Maternal Cardiac Disease In Pregnancy August 25, 2017 PREGNANCY ECHO CONFERENCE Maternal Physiology Cardiac Output = HR x SV Non-pregnant: 4.5 L/min Pregnant: 6.0 L/min Increase most acute in first 10
PREGNANCY AND CONGENITAL HEART DISEASE
 PREGNANCY AND CONGENITAL HEART DISEASE SIDDHARTH JADHAV M.D. Assistant Professor of Radiology E.B. Singleton Department of Pediatric Radiology Texas Children's Hospital COMMERCIAL DISCLOSURE - None Objectives
PREGNANCY AND CONGENITAL HEART DISEASE SIDDHARTH JADHAV M.D. Assistant Professor of Radiology E.B. Singleton Department of Pediatric Radiology Texas Children's Hospital COMMERCIAL DISCLOSURE - None Objectives
Valve Disease in the Pregnant Patient
 Valve Disease in the Pregnant Patient Julie B. Damp, MD December 6, 2012 VanderbiltHeart.com If single, do not allow marriage. If fertile, do not allow pregnancy. If pregnant, do not allow delivery. If
Valve Disease in the Pregnant Patient Julie B. Damp, MD December 6, 2012 VanderbiltHeart.com If single, do not allow marriage. If fertile, do not allow pregnancy. If pregnant, do not allow delivery. If
ESC Guidelines on the Management of Cardiovascular Diseases during Pregnancy
 ESC Guidelines on the Management of Cardiovascular Diseases during Pregnancy Task force on the management of CVD during pregnancy of the ESC Chair: Vera Regitz-Zagrosek, Charite, Berlin None DECLARATION
ESC Guidelines on the Management of Cardiovascular Diseases during Pregnancy Task force on the management of CVD during pregnancy of the ESC Chair: Vera Regitz-Zagrosek, Charite, Berlin None DECLARATION
Index. cardiology.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACHD. See Adult congenital heart disease (ACHD) Adult congenital heart disease (ACHD), 503 512 across life span prevalence of, 504 506
Index Note: Page numbers of article titles are in boldface type. A ACHD. See Adult congenital heart disease (ACHD) Adult congenital heart disease (ACHD), 503 512 across life span prevalence of, 504 506
Congenital Heart Disease Patient and Pregnancy
 Congenital Heart Disease Patient and Pregnancy Gurur Biliciler-Denktas, M.D. Assistant Professor Division of Pediatric Cardiology, Department of Pediatrics The University of Texas Health Science Center
Congenital Heart Disease Patient and Pregnancy Gurur Biliciler-Denktas, M.D. Assistant Professor Division of Pediatric Cardiology, Department of Pediatrics The University of Texas Health Science Center
EVALUATION OF PREGNANT PATIENTS WITH HEART DISEASE. Karen Stout, MD University of Washington Seattle Children s Seattle, WA
 EVALUATION OF PREGNANT PATIENTS WITH HEART DISEASE Karen Stout, MD University of Washington Seattle Children s Seattle, WA CASE PRESENTATION 24 year old woman with aortic regurgitation referred for evaluation
EVALUATION OF PREGNANT PATIENTS WITH HEART DISEASE Karen Stout, MD University of Washington Seattle Children s Seattle, WA CASE PRESENTATION 24 year old woman with aortic regurgitation referred for evaluation
Έγκυος και συγγενής καρδιοπάθεια: Τι πρέπει να γνωρίζει ο Καρδιολόγος Ενηλίκων
 Έγκυος και συγγενής καρδιοπάθεια: Τι πρέπει να γνωρίζει ο Καρδιολόγος Ενηλίκων Αντώνιος Π. Βλάχος Αναπληρωτής Καθηγητής Παιδοκαρδιολογίας Πανεπιστήμιο Ιωαννίνων No conflict of interest Pregnancy and CHD
Έγκυος και συγγενής καρδιοπάθεια: Τι πρέπει να γνωρίζει ο Καρδιολόγος Ενηλίκων Αντώνιος Π. Βλάχος Αναπληρωτής Καθηγητής Παιδοκαρδιολογίας Πανεπιστήμιο Ιωαννίνων No conflict of interest Pregnancy and CHD
Pregnancy and Heart Disease. Alexandra A Frogoudaki Adult Congenital Heart Clinic ATTIKON University Hospital
 Pregnancy and Heart Disease Alexandra A Frogoudaki Adult Congenital Heart Clinic ATTIKON University Hospital Pregnancy is not a state Hemodynamic changes During pregnancy Estrogens 1. Renin 2.
Pregnancy and Heart Disease Alexandra A Frogoudaki Adult Congenital Heart Clinic ATTIKON University Hospital Pregnancy is not a state Hemodynamic changes During pregnancy Estrogens 1. Renin 2.
Cardiac Disease in Pregnancy
 Cardiac Disease in Pregnancy DATE: SEPTEMBER 11, 2016 PRESENTED BY: ABIGAIL KHAN, MD Outline Scope of the problem Physiology of pregnancy Cardiac risk in pregnancy Pregnancy management Contraception 1
Cardiac Disease in Pregnancy DATE: SEPTEMBER 11, 2016 PRESENTED BY: ABIGAIL KHAN, MD Outline Scope of the problem Physiology of pregnancy Cardiac risk in pregnancy Pregnancy management Contraception 1
More History. Organization. Maternal Cardiac Disease: a historical perspective. The Parturient with Cardiac Disease 9/21/2012
 The Parturient with Cardiac Disease Pamela Flood M.D. Professor of Anesthesia and Perioperative Care Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco Maternal Cardiac
The Parturient with Cardiac Disease Pamela Flood M.D. Professor of Anesthesia and Perioperative Care Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco Maternal Cardiac
Outline. Maternal Congenital Heart Disease in Pregnancy. Maternal congenital heart disease. Cardiovascular disease in pregnancy 10/18/2017
 I have no disclosures or conflicts of interest to report. Maternal Congenital Heart Disease in Pregnancy Jennifer A. Jolley, MD Associate Clinical Professor University of California, Irvine Department
I have no disclosures or conflicts of interest to report. Maternal Congenital Heart Disease in Pregnancy Jennifer A. Jolley, MD Associate Clinical Professor University of California, Irvine Department
Pregnancy and Heart Disease Sharon L. Roble, MD Echo Hawaii 2016
 1 Pregnancy and Heart Disease Sharon L. Roble, MD Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Cardiovascular Effects of Pregnancy Anatomic Ventricular muscle mass increases
1 Pregnancy and Heart Disease Sharon L. Roble, MD Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Cardiovascular Effects of Pregnancy Anatomic Ventricular muscle mass increases
RF & RHD Workshop 22 nd March MANAGEMENT of RHEUMATIC HEART DISEASE in PREGNANCY. Dr Dorothy Radford
 RF & RHD Workshop 22 nd March 2016 MANAGEMENT of RHEUMATIC HEART DISEASE in PREGNANCY Dr Dorothy Radford PREGNANCY PHYSIOLOGY Increased cardiac output 30%-50% Increased blood volume 30%-50% Increased heart
RF & RHD Workshop 22 nd March 2016 MANAGEMENT of RHEUMATIC HEART DISEASE in PREGNANCY Dr Dorothy Radford PREGNANCY PHYSIOLOGY Increased cardiac output 30%-50% Increased blood volume 30%-50% Increased heart
SESSION D5. The Heart of the Matter: Cardiac Disease in Pregnancy Brad M. Dolinsky, MD, MFM
 37th Annual Advanced Practice in Primary and Acute Care Conference: October 9-11, 2014 2:45 SESSION D5 Session Description: The Heart of the Matter: Cardiac Disease in Pregnancy Brad M. Dolinsky, MD, MFM
37th Annual Advanced Practice in Primary and Acute Care Conference: October 9-11, 2014 2:45 SESSION D5 Session Description: The Heart of the Matter: Cardiac Disease in Pregnancy Brad M. Dolinsky, MD, MFM
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
Management of Heart Failure and Cardiomyopathies in Pregnancy
 Management of Heart Failure and Cardiomyopathies in Pregnancy Professor Sanjay Sharma Disclosures: None Epidemiology of Cardiac Disease In Pregnancy Cardiovascular disease in pregnancy is increasing in
Management of Heart Failure and Cardiomyopathies in Pregnancy Professor Sanjay Sharma Disclosures: None Epidemiology of Cardiac Disease In Pregnancy Cardiovascular disease in pregnancy is increasing in
Survival Rates of Children with Congenital Heart Disease continue to improve.
 DOROTHY RADFORD Survival Rates of Children with Congenital Heart Disease continue to improve. 1940-20% 1960-40% 1980-70% 2010->90% Percentage of children with CHD reaching age of 18 years 1938 First Patent
DOROTHY RADFORD Survival Rates of Children with Congenital Heart Disease continue to improve. 1940-20% 1960-40% 1980-70% 2010->90% Percentage of children with CHD reaching age of 18 years 1938 First Patent
Pregnancy, Heart Disease and Imaging. Hemodynamics. Decreased systemic vascular resistance. Physiology anemia
 Pregnancy, Heart Disease and Imaging Sangeeta Shah, MD, FASE, FACC Associate Professor, Ochsner Clinical School of Medicine Advanced CV Imaging and Adult Congenital Heart Disease New Orleans, LA Hemodynamics
Pregnancy, Heart Disease and Imaging Sangeeta Shah, MD, FASE, FACC Associate Professor, Ochsner Clinical School of Medicine Advanced CV Imaging and Adult Congenital Heart Disease New Orleans, LA Hemodynamics
Uptofate Study Summary
 CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
Maternal And Fetal Outcome In Pregnancies Complicated With Maternal Cardiac Diseases: Experience At A Tertiary Care Hospital
 ISPUB.COM The Internet Journal of Gynecology and Obstetrics Volume 19 Number 1 Maternal And Fetal Outcome In Pregnancies Complicated With Maternal Cardiac Diseases: Experience At A Tertiary Care Hospital
ISPUB.COM The Internet Journal of Gynecology and Obstetrics Volume 19 Number 1 Maternal And Fetal Outcome In Pregnancies Complicated With Maternal Cardiac Diseases: Experience At A Tertiary Care Hospital
Cardiac disease in pre pr gnancy
 IN THE NAME OF GOD Cardiac disease in pregn nancy MITRAL STENOSIS 33 y/o G3L2(2c/s) GA 34 + 5 CC: LP & dyspnea PMHx: MS sinse 4 yrs ago due to Rheumatism PSHx: 2c/s DHx: metoral 50 mg q6h/ ASA/ Enoxaparin
IN THE NAME OF GOD Cardiac disease in pregn nancy MITRAL STENOSIS 33 y/o G3L2(2c/s) GA 34 + 5 CC: LP & dyspnea PMHx: MS sinse 4 yrs ago due to Rheumatism PSHx: 2c/s DHx: metoral 50 mg q6h/ ASA/ Enoxaparin
Maternal Cardiac Disease Diagnosis and Management
 Maternal Cardiac Disease Diagnosis and Management Dr. Şevki ÇELEN ZTB Maternity and Teaching Hospital Department of Perinatology Heart diseases in pregnancy Today, 0.2-4% of all pregnancies are accompanied
Maternal Cardiac Disease Diagnosis and Management Dr. Şevki ÇELEN ZTB Maternity and Teaching Hospital Department of Perinatology Heart diseases in pregnancy Today, 0.2-4% of all pregnancies are accompanied
Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada
 PVR Following Repair of TOF Now? When? Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada Late Complications after TOF repair Repair will be necessary
PVR Following Repair of TOF Now? When? Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada Late Complications after TOF repair Repair will be necessary
When to implant an ICD in systemic right ventricle?
 When to implant an ICD in systemic right ventricle? Département de rythmologie et de stimulation cardiaque Nicolas Combes n.combes@clinique-pasteur.com Pôle de cardiologie pédiatrique et congénitale Risk
When to implant an ICD in systemic right ventricle? Département de rythmologie et de stimulation cardiaque Nicolas Combes n.combes@clinique-pasteur.com Pôle de cardiologie pédiatrique et congénitale Risk
The dos and don ts των νέων Κατευθυντηρίων Οδηγιών της Ευρωπαϊκής Καρδιολογικής Εταιρείας Για την καρδιαγγειακή νόσο στην εγκυμοσύνη
 The dos and don ts των νέων Κατευθυντηρίων Οδηγιών της Ευρωπαϊκής Καρδιολογικής Εταιρείας Για την καρδιαγγειακή νόσο στην εγκυμοσύνη Θωμάς Κ. Μακρής, MD FA, FES Συντονιστής Διευθυντής Καρδιολογικού Τμήματος
The dos and don ts των νέων Κατευθυντηρίων Οδηγιών της Ευρωπαϊκής Καρδιολογικής Εταιρείας Για την καρδιαγγειακή νόσο στην εγκυμοσύνη Θωμάς Κ. Μακρής, MD FA, FES Συντονιστής Διευθυντής Καρδιολογικού Τμήματος
Pregnancy and Heart Disease
 Pregnancy and Heart Disease Heidi M. Connolly, MD No disclosures 2011 MFMER 3138928-1 Regitz-Zagrosek V, Lundqvist C, Borghi C, et al. Pregnancy and the Heart 2% of pregnancies involve maternal CV disease
Pregnancy and Heart Disease Heidi M. Connolly, MD No disclosures 2011 MFMER 3138928-1 Regitz-Zagrosek V, Lundqvist C, Borghi C, et al. Pregnancy and the Heart 2% of pregnancies involve maternal CV disease
ACHD & Heart Disease and Pregnancy: Guidelines and Cases Michael A. Gatzoulis
 ACHD & Heart Disease and Pregnancy: Guidelines and Cases Michael A. Gatzoulis Adult Congenital Heart Centre & National Centre for Pulmonary Hypertension Royal Brompton Hospital/National Heart & Lung Institute,
ACHD & Heart Disease and Pregnancy: Guidelines and Cases Michael A. Gatzoulis Adult Congenital Heart Centre & National Centre for Pulmonary Hypertension Royal Brompton Hospital/National Heart & Lung Institute,
Adult Congenital Heart Disease: A Growing Problem. Dr. Gary Webb Cincinnati Children s Hospital Heart Institute
 Adult Congenital Heart Disease: A Growing Problem Dr. Gary Webb Cincinnati Children s Hospital Heart Institute ACHD Resources in Ohio ACHAHEART.ORG Situations When We Might Help When you don t know a
Adult Congenital Heart Disease: A Growing Problem Dr. Gary Webb Cincinnati Children s Hospital Heart Institute ACHD Resources in Ohio ACHAHEART.ORG Situations When We Might Help When you don t know a
Anatomy & Physiology
 1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
ΔΙΑΧΕΙΡΙΣΗ ΑΣΘΕΝΩΝ ΜΕ ΜΕΣΟΚΟΛΠΙΚΗ ΕΠΙΚΟΙΝΩΝΙΑ ΖΑΧΑΡΑΚΗ ΑΓΓΕΛΙΚΗ ΚΑΡΔΙΟΛΟΓΟΣ ΗΡΑΚΛΕΙΟ - ΚΡΗΤΗ
 ΔΙΑΧΕΙΡΙΣΗ ΑΣΘΕΝΩΝ ΜΕ ΜΕΣΟΚΟΛΠΙΚΗ ΕΠΙΚΟΙΝΩΝΙΑ ΖΑΧΑΡΑΚΗ ΑΓΓΕΛΙΚΗ ΚΑΡΔΙΟΛΟΓΟΣ ΗΡΑΚΛΕΙΟ - ΚΡΗΤΗ European Accreditation in TTE, TEE and CHD Echocardiography NOTHING TO DECLARE ATRIAL SEPTAL DEFECT TYPES SECUNDUM
ΔΙΑΧΕΙΡΙΣΗ ΑΣΘΕΝΩΝ ΜΕ ΜΕΣΟΚΟΛΠΙΚΗ ΕΠΙΚΟΙΝΩΝΙΑ ΖΑΧΑΡΑΚΗ ΑΓΓΕΛΙΚΗ ΚΑΡΔΙΟΛΟΓΟΣ ΗΡΑΚΛΕΙΟ - ΚΡΗΤΗ European Accreditation in TTE, TEE and CHD Echocardiography NOTHING TO DECLARE ATRIAL SEPTAL DEFECT TYPES SECUNDUM
A pregnant patient with a prosthetic valve Giacomo Boccuzzi, MD, FESC
 A pregnant patient with a prosthetic valve Giacomo Boccuzzi, MD, FESC Department of Invasive Cardiology, Ospedale San Giovanni Bosco, Turin, Italy *C.V. was born the 24th May 1980 Rheumatic fever during
A pregnant patient with a prosthetic valve Giacomo Boccuzzi, MD, FESC Department of Invasive Cardiology, Ospedale San Giovanni Bosco, Turin, Italy *C.V. was born the 24th May 1980 Rheumatic fever during
How pregnancy impacts adult cyanotic congenital heart disease
 How pregnancy impacts adult cyanotic congenital heart disease Magalie Ladouceur Adult Congenital Heart Disease Unit, Hôpital Européen Georges Pompidou, Centre de reference des Malformations Cardiaques
How pregnancy impacts adult cyanotic congenital heart disease Magalie Ladouceur Adult Congenital Heart Disease Unit, Hôpital Européen Georges Pompidou, Centre de reference des Malformations Cardiaques
PATENT DUCTUS ARTERIOSUS (PDA)
") PATENT DUCTUS ARTERIOSUS (PDA) It is a channel that connect the pulmonary artery with the descending aorta (isthumus part). It results from the persistence of patency of the fetal ductus arteriosus after
PATENT DUCTUS ARTERIOSUS (PDA) It is a channel that connect the pulmonary artery with the descending aorta (isthumus part). It results from the persistence of patency of the fetal ductus arteriosus after
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials
 Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Pregnancy and Congenital Heart Disease Heidi M. Connolly, M.D. Professor of Medicine Chair for Education Division
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Pregnancy and Congenital Heart Disease Heidi M. Connolly, M.D. Professor of Medicine Chair for Education Division
Images in Cardiovascular Medicine
 Images in Cardiovascular Medicine Management of Severe Mitral Stenosis During Pregnancy Rebecca S. Norrad, MBBS; Omid Salehian, MSc, MD, FRCPC, FACC, FAHA A 37-year-old woman originally from Iraq was referred
Images in Cardiovascular Medicine Management of Severe Mitral Stenosis During Pregnancy Rebecca S. Norrad, MBBS; Omid Salehian, MSc, MD, FRCPC, FACC, FAHA A 37-year-old woman originally from Iraq was referred
Heart Failure treatment during pregnancy
 Heart Failure treatment during pregnancy Angeles Alonso García Hospital Universitario Puerta de Hierro. Majadahonda. Madrid. Spain European Society of Cardiology. Stockholm. 29 August 2010 Starting Point
Heart Failure treatment during pregnancy Angeles Alonso García Hospital Universitario Puerta de Hierro. Majadahonda. Madrid. Spain European Society of Cardiology. Stockholm. 29 August 2010 Starting Point
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Focused. se with 2008 F. lar Heart Diseas. date. ents With Valvul. Upd. gement of Patie. lines for Manag. HA 2006 Guidel ACC/AH. Fig.
 ACC/AH HA 2006 Guidel nic severe AI (Fig. 4). ned by age, ay also be helpful nd echo. For AI, ollow up may be or MRI rather than mension; SD, end lines for Manag gement of Patie Upd ents With Valvul date
ACC/AH HA 2006 Guidel nic severe AI (Fig. 4). ned by age, ay also be helpful nd echo. For AI, ollow up may be or MRI rather than mension; SD, end lines for Manag gement of Patie Upd ents With Valvul date
Pregnancy and Cardiovascular Disease
 Pregnancy and Cardiovascular Disease Cindy M. Martin, M.D. Co-Director, Adult Congenital and Cardiovascular Genetics Center No Disclosures Objectives Discuss the hemodynamic changes during pregnancy Define
Pregnancy and Cardiovascular Disease Cindy M. Martin, M.D. Co-Director, Adult Congenital and Cardiovascular Genetics Center No Disclosures Objectives Discuss the hemodynamic changes during pregnancy Define
Cardiac Emergencies in Infants. Michael Luceri, DO
 Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
Echocardiography in Adult Congenital Heart Disease
 Echocardiography in Adult Congenital Heart Disease Michael Vogel Kinderherz-Praxis München CHD missed in childhood Subsequent lesions after repaired CHD Follow-up of cyanotic heart disease CHD missed in
Echocardiography in Adult Congenital Heart Disease Michael Vogel Kinderherz-Praxis München CHD missed in childhood Subsequent lesions after repaired CHD Follow-up of cyanotic heart disease CHD missed in
Effect of maternal heart disease on pregnancy outcomes
 Expert Review of Obstetrics & Gynecology ISSN: 1747-4108 (Print) 1747-4116 (Online) Journal homepage: http://www.tandfonline.com/loi/ierb20 Effect of maternal heart disease on pregnancy outcomes Emily
Expert Review of Obstetrics & Gynecology ISSN: 1747-4108 (Print) 1747-4116 (Online) Journal homepage: http://www.tandfonline.com/loi/ierb20 Effect of maternal heart disease on pregnancy outcomes Emily
42yr Old Male with Severe AR Mild LV dysfunction s/p TOF -AV Replacement(tissue valve) or AoV plasty- Kyung-Hwan Kim
 or AoV plasty- Kyung-Hwan Kim") 42yr Old Male with Severe AR Mild LV dysfunction s/p TOF -AV Replacement(tissue valve) or AoV plasty- Kyung-Hwan Kim Current Guideline for AR s/p TOF Surgery is reasonable in adults with prior repair of
42yr Old Male with Severe AR Mild LV dysfunction s/p TOF -AV Replacement(tissue valve) or AoV plasty- Kyung-Hwan Kim Current Guideline for AR s/p TOF Surgery is reasonable in adults with prior repair of
CONGENITAL HEART DEFECTS IN ADULTS
 CONGENITAL HEART DEFECTS IN ADULTS THE ROLE OF CATHETER INTERVENTIONS Mario Carminati CONGENITAL HEART DEFECTS IN ADULTS CHD in natural history CHD with post-surgical sequelae PULMONARY VALVE STENOSIS
CONGENITAL HEART DEFECTS IN ADULTS THE ROLE OF CATHETER INTERVENTIONS Mario Carminati CONGENITAL HEART DEFECTS IN ADULTS CHD in natural history CHD with post-surgical sequelae PULMONARY VALVE STENOSIS
S. Bruce Greenberg, MD FNASCI and President, NASCI Professor of Radiology and Pediatrics University of Arkansas for Medical Sciences
 S. Bruce Greenberg, MD FNASCI and President, NASCI Professor of Radiology and Pediatrics University of Arkansas for Medical Sciences No financial disclosures Aorta Congenital aortic stenosis/insufficiency
S. Bruce Greenberg, MD FNASCI and President, NASCI Professor of Radiology and Pediatrics University of Arkansas for Medical Sciences No financial disclosures Aorta Congenital aortic stenosis/insufficiency
Sudden cardiac death: Primary and secondary prevention
 Sudden cardiac death: Primary and secondary prevention By Kai Chi Chan Penultimate Year Medical Student St George s University of London at UNic Sheba Medical Centre Definition Sudden cardiac arrest (SCA)
Sudden cardiac death: Primary and secondary prevention By Kai Chi Chan Penultimate Year Medical Student St George s University of London at UNic Sheba Medical Centre Definition Sudden cardiac arrest (SCA)
Valvular Heart Disease Mitral Stenosis
 Valvular Heart Disease Mitral Stenosis A 75 year old woman with loud first heart sound and mid-diastolic murmur Chronic dyspnea Class 2/4 Fatigue Recent orthopnea/pnd Nocturnal palpitation Pedal edema
Valvular Heart Disease Mitral Stenosis A 75 year old woman with loud first heart sound and mid-diastolic murmur Chronic dyspnea Class 2/4 Fatigue Recent orthopnea/pnd Nocturnal palpitation Pedal edema
Miscellaneous Cardiology Topics pregnancy - congenital - myocarditis - pericardial disease. Pregnancy and Cardiovascular Disease MCQ
 Miscellaneous Cardiology Topics pregnancy - congenital - myocarditis - pericardial disease Maan Jokhadar, MD, FACC Emory Center for Advanced Heart Failure Therapy Emory Adult Congenital Heart Center Pregnancy
Miscellaneous Cardiology Topics pregnancy - congenital - myocarditis - pericardial disease Maan Jokhadar, MD, FACC Emory Center for Advanced Heart Failure Therapy Emory Adult Congenital Heart Center Pregnancy
Congenital Heart Disease
 Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014
 Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Dysrhythmias 11/7/2017. Disclosures. 3 reasons to evaluate and treat dysrhythmias. None. Eliminate symptoms and improve hemodynamics
 Dysrhythmias CYDNEY STEWART MD, FACC NOVEMBER 3, 2017 Disclosures None 3 reasons to evaluate and treat dysrhythmias Eliminate symptoms and improve hemodynamics Prevent imminent death/hemodynamic compromise
Dysrhythmias CYDNEY STEWART MD, FACC NOVEMBER 3, 2017 Disclosures None 3 reasons to evaluate and treat dysrhythmias Eliminate symptoms and improve hemodynamics Prevent imminent death/hemodynamic compromise
Adults with Congenital Heart Disease. Michael E. McConnell MD, Wendy Book MD Teresa Lyle RN NNP
 Adults with Congenital Heart Disease Michael E. McConnell MD, Wendy Book MD Teresa Lyle RN NNP Outline History of CHD Statistics Specific lesions (TOF, TGA, Single ventricle) Erythrocytosis Pregnancy History
Adults with Congenital Heart Disease Michael E. McConnell MD, Wendy Book MD Teresa Lyle RN NNP Outline History of CHD Statistics Specific lesions (TOF, TGA, Single ventricle) Erythrocytosis Pregnancy History
Cardiovascular Recommendation Tables
 Cardiovascular Recommendation Tables Current as of: February, 2009 The first publication of the Cardiovascular Recommendation Tables occurred in the October 2002, Cardiovascular Advisory Panel Guidelines
Cardiovascular Recommendation Tables Current as of: February, 2009 The first publication of the Cardiovascular Recommendation Tables occurred in the October 2002, Cardiovascular Advisory Panel Guidelines
Heart disease complicating pregnancy management strategies
 www.slcog.lk/sljog LEADING ARTICLE Heart disease complicating pregnancy management strategies Priyadharshan P¹ Introduction Heart disease is the third most common cause of maternal death and the leading
www.slcog.lk/sljog LEADING ARTICLE Heart disease complicating pregnancy management strategies Priyadharshan P¹ Introduction Heart disease is the third most common cause of maternal death and the leading
Antithrombotic therapy for patients with congenital heart disease. George Giannakoulas, MD, PhD AHEPA University Hospital Thessaloniki
 Antithrombotic therapy for patients with congenital heart disease George Giannakoulas, MD, PhD AHEPA University Hospital Thessaloniki Disclosures Educational fees from Astra Zeneca, GSK Research fees from
Antithrombotic therapy for patients with congenital heart disease George Giannakoulas, MD, PhD AHEPA University Hospital Thessaloniki Disclosures Educational fees from Astra Zeneca, GSK Research fees from
Catherine Nelson-Piercy. Guy s & St Thomas Hospitals & Queen Charlotte s Hospital London, UK
 Cardiac Disease and Pregnancy Catherine Nelson-Piercy Guy s & St Thomas Hospitals & Queen Charlotte s Hospital London, UK Physiological changes in pregnancy Cardiac Output (CO) increases by 40% Further
Cardiac Disease and Pregnancy Catherine Nelson-Piercy Guy s & St Thomas Hospitals & Queen Charlotte s Hospital London, UK Physiological changes in pregnancy Cardiac Output (CO) increases by 40% Further
Peripartum Cardiomyopathy. Lavanya Rai Manipal
 Peripartum Cardiomyopathy Lavanya Rai Manipal Definition - PPCM - Dilated cardiomyopathy of unknown cause resulting in cardiac failure that occurs in the peripartum period in women without any preexisting
Peripartum Cardiomyopathy Lavanya Rai Manipal Definition - PPCM - Dilated cardiomyopathy of unknown cause resulting in cardiac failure that occurs in the peripartum period in women without any preexisting
Review Article Heart Disease and Pregnancy
 Hellenic J Cardiol 47: 275-291, 2006 Review Article Heart Disease and Pregnancy AIKATERINI CHAMAIDI, MICHAEL A. GATZOULIS Adult Congenital Heart Centre and Centre for Pulmonary Hypertension, Royal Brompton
Hellenic J Cardiol 47: 275-291, 2006 Review Article Heart Disease and Pregnancy AIKATERINI CHAMAIDI, MICHAEL A. GATZOULIS Adult Congenital Heart Centre and Centre for Pulmonary Hypertension, Royal Brompton
I have nothing to disclose.
 I have nothing to disclose. Antiarrhythmic Therapy in Pregnancy Prof. Ali Oto,MD,FESC,FACC,FHRS Department of Cardiology Hacettepe University,Faculty of Medicine Ankara Arrhythmias in pregnancy An increased
I have nothing to disclose. Antiarrhythmic Therapy in Pregnancy Prof. Ali Oto,MD,FESC,FACC,FHRS Department of Cardiology Hacettepe University,Faculty of Medicine Ankara Arrhythmias in pregnancy An increased
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT
 ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
Outline. Congenital Heart Disease. Special Considerations for Special Populations: Congenital Heart Disease
 Special Considerations for Special Populations: Congenital Heart Disease Valerie Bosco, FNP, EdD Alison Knauth Meadows, MD, PhD University of California San Francisco Adult Congenital Heart Program Outline
Special Considerations for Special Populations: Congenital Heart Disease Valerie Bosco, FNP, EdD Alison Knauth Meadows, MD, PhD University of California San Francisco Adult Congenital Heart Program Outline
Adult Cardiac Surgery
 Adult Cardiac Surgery Mahmoud ABU-ABEELEH Associate Professor Department of Surgery Division of Cardiothoracic Surgery School of Medicine University Of Jordan Adult Cardiac Surgery: Ischemic Heart Disease
Adult Cardiac Surgery Mahmoud ABU-ABEELEH Associate Professor Department of Surgery Division of Cardiothoracic Surgery School of Medicine University Of Jordan Adult Cardiac Surgery: Ischemic Heart Disease
Adult Congenital Heart Disease
 Adult Congenital Heart Disease Anne Marie Valente, MD Boston Adult Congenital Heart Disease and Pulmonary Hypertension Program Division of Cardiology Brigham and Women s Hospital, Boston Children s Hospital
Adult Congenital Heart Disease Anne Marie Valente, MD Boston Adult Congenital Heart Disease and Pulmonary Hypertension Program Division of Cardiology Brigham and Women s Hospital, Boston Children s Hospital
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions
 Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS Pediatric Cardiology
 Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acid base balance pregnancy-related changes to, 640 Acquired heart disease, 731 Acute fatty liver of pregnancy (AFLP), 618 Acute kidney
Index Note: Page numbers of article titles are in boldface type. A Acid base balance pregnancy-related changes to, 640 Acquired heart disease, 731 Acute fatty liver of pregnancy (AFLP), 618 Acute kidney
Introduction. Pediatric Cardiology. General Appearance. Tools of Assessment. Auscultation. Vital Signs
 Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
Mitral Valve Disease, When to Intervene
 Mitral Valve Disease, When to Intervene Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Current ACC/AHA guideline Stages
Mitral Valve Disease, When to Intervene Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Current ACC/AHA guideline Stages
Non-cardiac Surgery in Valvular Heart Disease
 Jafar Golshahi, MD; Shahnaz Aram, MD Abstract Background- Valvular heart disease is one of the common complications of acute rheumatic fever, which manifests its clinical complications one or two decades
Jafar Golshahi, MD; Shahnaz Aram, MD Abstract Background- Valvular heart disease is one of the common complications of acute rheumatic fever, which manifests its clinical complications one or two decades
Cardiac Catheterization Cases Primary Cardiac Diagnoses Facility 12 month period from to PRIMARY DIAGNOSES (one per patient)
") PRIMARY DIAGNOSES (one per patient) Septal Defects ASD (Atrial Septal Defect) PFO (Patent Foramen Ovale) ASD, Secundum ASD, Sinus venosus ASD, Coronary sinus ASD, Common atrium (single atrium) VSD (Ventricular
PRIMARY DIAGNOSES (one per patient) Septal Defects ASD (Atrial Septal Defect) PFO (Patent Foramen Ovale) ASD, Secundum ASD, Sinus venosus ASD, Coronary sinus ASD, Common atrium (single atrium) VSD (Ventricular
Cardiac MRI in ACHD What We. ACHD Patients
 Cardiac MRI in ACHD What We Have Learned to Apply to ACHD Patients Faris Al Mousily, MBChB, FAAC, FACC Consultant, Pediatric Cardiology, KFSH&RC/Jeddah Adjunct Faculty, Division of Pediatric Cardiology
Cardiac MRI in ACHD What We Have Learned to Apply to ACHD Patients Faris Al Mousily, MBChB, FAAC, FACC Consultant, Pediatric Cardiology, KFSH&RC/Jeddah Adjunct Faculty, Division of Pediatric Cardiology
Tetralogy of Fallot Latest data in risk stratification and replacement of pulmonic valve
 Tetralogy of Fallot Latest data in risk stratification and replacement of pulmonic valve Alexandra A Frogoudaki Adult Congenital Heart Clinic Second Cardiology Department ATTIKON University Hospital No
Tetralogy of Fallot Latest data in risk stratification and replacement of pulmonic valve Alexandra A Frogoudaki Adult Congenital Heart Clinic Second Cardiology Department ATTIKON University Hospital No
How to manage the pregnant woman with heart disease
 How to manage the pregnant woman with heart disease Dr Fiona Walker, The Heart Hospital,UCLH, London Dr Sara Thorne, University Hospital Birmingham Dr Cathy Head, The Heart Hospital, UCLH, London Dr Kate
How to manage the pregnant woman with heart disease Dr Fiona Walker, The Heart Hospital,UCLH, London Dr Sara Thorne, University Hospital Birmingham Dr Cathy Head, The Heart Hospital, UCLH, London Dr Kate
CONGENITAL HEART DISEASE (CHD)
") CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
UC SF DISCLOSURES MANAGEMENT OF MATERNAL CONGENITAL HEART DISEASE OBJECTIVES. No financial disclosures CARDIOVASCULAR CHANGES ANTEPARTUM 6/10/2011
 DISCLOSURES MANAGEMENT OF MATERNAL CONGENITAL HEART DISEASE No financial disclosures UC SF Lena H. Kim, MD AIM CONFERENCE June 10, 2011 spicecomments.com OBJECTIVES Physiologic cardiovascular changes of
DISCLOSURES MANAGEMENT OF MATERNAL CONGENITAL HEART DISEASE No financial disclosures UC SF Lena H. Kim, MD AIM CONFERENCE June 10, 2011 spicecomments.com OBJECTIVES Physiologic cardiovascular changes of
September 26, 2012 Philip Stockwell, MD Lifespan CVI Assistant Professor of Medicine (Clinical)
") September 26, 2012 Philip Stockwell, MD Lifespan CVI Assistant Professor of Medicine (Clinical) Advances in cardiac surgery have created a new population of adult patients with repaired congenital heart
September 26, 2012 Philip Stockwell, MD Lifespan CVI Assistant Professor of Medicine (Clinical) Advances in cardiac surgery have created a new population of adult patients with repaired congenital heart
Adults with Congenital Heart Disease
 Adults with Congenital Heart Disease Edward K. Rhee, MD, FACC Director, Pediatric-Adult Congenital Arrhythmia Service SJHMC Disclosures & Disclaimer I have no lucrative financial relationships with industry
Adults with Congenital Heart Disease Edward K. Rhee, MD, FACC Director, Pediatric-Adult Congenital Arrhythmia Service SJHMC Disclosures & Disclaimer I have no lucrative financial relationships with industry
5.8 Congenital Heart Disease
 5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
Congenital heart disease. By Dr Saima Ali Professor of pediatrics
 Congenital heart disease By Dr Saima Ali Professor of pediatrics What is the most striking clinical finding in this child? Learning objectives By the end of this lecture, final year student should be able
Congenital heart disease By Dr Saima Ali Professor of pediatrics What is the most striking clinical finding in this child? Learning objectives By the end of this lecture, final year student should be able
Detailed Order Request Checklists for Cardiology
 Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
Cardiovascular disease complicates 1% to 3% of all
 Pregnancy Complicated by Valvular Heart Disease: An Update Michael Nanna, MD; Kathleen Stergiopoulos, MD, PhD, FASE, FACC, FAHA Cardiovascular disease complicates 1% to 3% of all pregnancies and is responsible
Pregnancy Complicated by Valvular Heart Disease: An Update Michael Nanna, MD; Kathleen Stergiopoulos, MD, PhD, FASE, FACC, FAHA Cardiovascular disease complicates 1% to 3% of all pregnancies and is responsible
Dr.ssa Loredana Iannetta. Centro Cardiologico Monzino
 Dr.ssa Loredana Iannetta Centro Cardiologico Monzino Bicuspid aortic valve BAV is the most common congenital cardiac anomaly. Estimated incidence is 2% in general population. 4:1 male predominance. Frequency
Dr.ssa Loredana Iannetta Centro Cardiologico Monzino Bicuspid aortic valve BAV is the most common congenital cardiac anomaly. Estimated incidence is 2% in general population. 4:1 male predominance. Frequency
Pregnancy and cyanotic congenital heart disease. A. Pijuan Domènech (U. de C. Congènites de l Adult) Hospital Vall d Hebron Barcelona, Spain
 Hospital Vall d Hebron Barcelona, Spain") Pregnancy and cyanotic congenital heart disease A. Pijuan Domènech (U. de C. Congènites de l Adult) Hospital Vall d Hebron Barcelona, Spain I have nothing to disclose. Pregnancy and cyanotic congenital
Pregnancy and cyanotic congenital heart disease A. Pijuan Domènech (U. de C. Congènites de l Adult) Hospital Vall d Hebron Barcelona, Spain I have nothing to disclose. Pregnancy and cyanotic congenital
Valvular Heart Disease
 Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Congenital heart disease: When to act and what to do?
 Leading Article Congenital heart disease: When to act and what to do? Duminda Samarasinghe 1 Sri Lanka Journal of Child Health, 2010; 39: 39-43 (Key words: Congenital heart disease) Congenital heart disease
Leading Article Congenital heart disease: When to act and what to do? Duminda Samarasinghe 1 Sri Lanka Journal of Child Health, 2010; 39: 39-43 (Key words: Congenital heart disease) Congenital heart disease
When Should I Order a Stress Test or an Echocardiogram
 When Should I Order a Stress Test or an Echocardiogram Updates in Cardiology 2015 March 7, 2015 Donald L. Lappé, MD, FAHA, FACC Chairman, Cardiovascular Department Medical Director, Intermountain Cardiovascular
When Should I Order a Stress Test or an Echocardiogram Updates in Cardiology 2015 March 7, 2015 Donald L. Lappé, MD, FAHA, FACC Chairman, Cardiovascular Department Medical Director, Intermountain Cardiovascular
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
7. Echocardiography Appropriate Use Criteria (by Indication)
") Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Echocardiographic assessment in Adult Patients with Congenital Heart Diseases
 Echocardiographic assessment in Adult Patients with Congenital Heart Diseases Athanasios Koutsakis Cardiologist, Cl. Research Fellow George Giannakoulas Ass. Professor in Cardiology 1st Cardiology Department,
Echocardiographic assessment in Adult Patients with Congenital Heart Diseases Athanasios Koutsakis Cardiologist, Cl. Research Fellow George Giannakoulas Ass. Professor in Cardiology 1st Cardiology Department,
HEART DISEASE IN PREGNANCY
 HEART DISEASE IN PREGNANCY DR. JOSHI SUYAJNA D. www.suyajna.com VIMS-BELLARY Pre-conceptional counseling a. Objective Risk assessment with» 1. Clarke s table 2. NYHA b. Feasibility of pregnancy care c.
HEART DISEASE IN PREGNANCY DR. JOSHI SUYAJNA D. www.suyajna.com VIMS-BELLARY Pre-conceptional counseling a. Objective Risk assessment with» 1. Clarke s table 2. NYHA b. Feasibility of pregnancy care c.
Heart Valves: Before and after surgery
 Heart Valves: Before and after surgery Tim Sutton, Consultant Cardiologist Middlemore Hospital, Auckland Auckland Heart Group Indications for intervention in Valvular disease To prevent sudden death and
Heart Valves: Before and after surgery Tim Sutton, Consultant Cardiologist Middlemore Hospital, Auckland Auckland Heart Group Indications for intervention in Valvular disease To prevent sudden death and
Rate of CHD at birth: 4~12/1,000
 Risk assessment and management for the pregnant ACHD woman Suk-Joo Choi Department of Obstetrics and Gynecology Samsung Medical Center Sungkyunkwan k University i School of Medicine i Cardiac diseases
Risk assessment and management for the pregnant ACHD woman Suk-Joo Choi Department of Obstetrics and Gynecology Samsung Medical Center Sungkyunkwan k University i School of Medicine i Cardiac diseases
Expert consensus document on management of cardiovascular diseases during pregnancy
 European Heart Journal (2003) 24, 761 781 Guidelines Expert consensus document on management of cardiovascular diseases during pregnancy The Task Force on the Management of Cardiovascular Diseases During
European Heart Journal (2003) 24, 761 781 Guidelines Expert consensus document on management of cardiovascular diseases during pregnancy The Task Force on the Management of Cardiovascular Diseases During
Surgical Management of TOF in Adults. Dr Flora Tsang Associate Consultant Department of Cardiothoracic Surgery Queen Mary Hospital
 Surgical Management of TOF in Adults Dr Flora Tsang Associate Consultant Department of Cardiothoracic Surgery Queen Mary Hospital Tetralogy of Fallot (TOF) in Adults Most common cyanotic congenital heart
Surgical Management of TOF in Adults Dr Flora Tsang Associate Consultant Department of Cardiothoracic Surgery Queen Mary Hospital Tetralogy of Fallot (TOF) in Adults Most common cyanotic congenital heart
Appropriate Use Criteria for Initial Transthoracic Echocardiography in Outpatient Pediatric Cardiology (scores listed by Appropriate Use rating)
") Appropriate Use Criteria for Initial Transthoracic Echocardiography in Outpatient Pediatric Cardiology (scores listed by Appropriate Use rating) Table 1: Appropriate indications (median score 7-9) Indication
Appropriate Use Criteria for Initial Transthoracic Echocardiography in Outpatient Pediatric Cardiology (scores listed by Appropriate Use rating) Table 1: Appropriate indications (median score 7-9) Indication