From Sodium Retention to Therapy for Refractory Ascites The Role for New Drugs. Florence Wong University of Toronto. Falk Symposium October 14, 2007
|
|
|
- Rudolf Tyler
- 5 years ago
- Views:
Transcription


1 From Sodium Retention to Therapy for Refractory Ascites The Role for New Drugs Florence Wong University of Toronto Falk Symposium October 14, 2007

2 Sodium Retention in Cirrhosis Occurs as a result of hemodynamic changes that leads to underfilling of the effective arterial circulation Compensatory activation of various neurohumoral mechanisms that act on various parts of the nephron to retain sodium and water
3 Stages of Sodium Retention in Cirrhosis Subtle sodium retention Obvious sodium retention Avid sodium retention Functional Renal failure Pre-Ascites Responsive ascites Refractory ascites Hepatorenal syndrome Hepatorenal interaction Portal hypertension Systemic arterial vasodilatation Renal vasoconstriction

4 Refractory Ascites Weight loss 1.5kg/week while on 400mg of spironolactone or 30mg of amiloride plus 160mg of furosemide daily two weeks Dietary sodium restriction 50mmol per day

5 Management of Refractory Ascites Sodium Restriction Mandatory at all stages of ascites in order to reduce the rate of accumulation of ascites
6 Management of Refractory Ascites OR Large volume paracentesis TIPS
7 But. Large volume paracentesis is inconvenient for some patients with refractory ascites TIPS insertion is not appropriate for many patients
8 Albumin Most abundant plasma protein Physiological function is to maintain colloid osmotic pressure Can improve effective arterial blood volume in cirrhosis Has other ligand binding, antioxidant, anti-inflammatory and transport functions Old drug with new indications for use
9 (Gentilini et al, J Hepatology 1999) Albumin for Management of Ascites 141 patients Bed rest & sodium-restricted diet 15 Responders 126 Non-responders Potassium Canrenoate 200mg Furosemide 25mg Potassium Canrenoate 200mg Furosemide 25mg Albumin 25g/wk for 1 year, then 25g/2 wks for 2nd & 3rd years 47 Responders 16 Non-responders (74.7%) ( 25.3%) 57 Responders* 6 Non-responders (90.5%) ( 9.5%)
10 Albumin for Management of Ascites Ascites re-accumulation Hospital re-admission for Ascites Diuretics P<0.03 Diuretics P<0.03 Albumin + diuretics Albumin + diuretics (Gentilini et al, J Hepatology 1999)
11 Albumin for Management of Ascites Survival P= Albumin + diuretics Diuretics (Romanelli et al, World J Gastroenterol 2007)
12 Albumin for Refractory Ascites 19 patients with refractory ascites Mean age: 54.5 years 50gm of albumin infused per week Assessment made before and after 8 weeks of infusion Serum Serum INR MELD [Na] creatinine Before After (Trotter et al, Dig Dis Sci 2005)
13 Albumin for Refractory Ascites P=0.005 P=0.002 gm/l Serum albumin Before After (Trotter et al, Dig Dis Sci 2005) lb Before After Weight
 is enormous Await definitive studies to establish albumin as treatment for refractory")
14 Albumin for Management of Ascites Makes physiological sense Improves survival in patients with diuretic responsive ascites Impact on survival in patients with refractory ascites is unknown Cost (albumin & medical manpower) is enormous Await definitive studies to establish albumin as treatment for refractory ascites
15 Vasoconstrictors for Management of Ascites Aim at reducing the extent of arterial vasodilatation Improves effective arterial circulation Dampens the activated vasoconstrictor systems Should improve renal hemodynamics Increase in renal sodium retention should follow
16 Vasoconstrictors for Management of Ascites Terlipressin Single intravenous dose of 2mg Improvement in systemic hemodynamics No measurement of renal hemodynmics No improvement in renal sodium excretion in ascitic patients (Kalambokis et al, J Gastroenterol Hepatol 2005)
17 Vasoconstrictors for Management of Ascites Terlipressin I mg/4hr intravenous administration in patients with refractory ascites and type 2 HRS for 7days Improvement in systemic hemodynamics Improvement in renal hemodynmics No improvement of renal sodium excretion (Alessandria et al, Euro J Gastroenterol Hepatol 2002)
18 Vasoconstrictors for Management of Ascites Midodrine Orally active alpha agonist Single oral dose of 15mg in ascitic patients Improvement in systemic and renal hemodynmics ml/min µmol/min Before GFR P<0.025 UNaV 3 hours after Increase in renal sodium excretion Reduction in vasoconstrictor levels Effects maintained for at least 3 hours (Angeli et al, Hepatology 1998) Before P< hours after
19 Vasoconstrictors for Management of Ascites Midodrine 7.5mg t.i.d. for 7 days Delayed improvement in systemic and renal hemodynmics Delayed improvement in renal sodium excretion Reduction in vasoconstrictor levels Significant correlation between change in systemic hemodynamics & increase in GFR and increase in UNaV (Kalambokis et al, J Hepatol 2007) ml/min mmol/day GFR P<0.01 Before Day 7 UNaV P<0.05 Before Day 7
20 Vaspressin Receptor Antagonists Urinary space Collecting Principal Duct Cell Basolateral space H 2 O H 2 O H 2 O AP2 PKA camp V 2 receptor S G protein AVP AVP AVP Adenyl cyclase ATP H 2 O H 2 O H2 O H 2 O H2 O S = V 2 receptor antagonist
21 Vaspressin Receptor Antagonists Aquaretic agents Initially developed for the treatment of hyponatremia from whatever cause promote aquaresis in conditions of water excess: - congestive heart failure - decompensated cirrhosis - syndrome of inappropriate ADH
22 Aquaretic Agents- Vaptans Aquaretic agents are collectively known as Vaptans - Mozavaptan (OPC-31260) - Lixivaptan (VPA-985) - Tolvaptan (OPC-41061) - RWJ Satavaptan - Conivaptan (V 1 & V 2 receptor antagonist)
23 Lixivaptan Corrects Hyponatremia Lixivaptan - VPA Serum [Na] 135 ** * * Serum [Na] in mmol/l ± SEM Baseline Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 7 Day -1 (Wong F et al, Hepatology 2004)
24 Satavaptan Corrects Hyponatremia Mean serum sodium (mmol/l) (±SE) HypoCAT Satavaptan Placebo Day Week
25 Vaptans for Ascites Management Vasopressin receptor antagonists act on a different site of the nephron compared to standard diuretics to induce a water diuresis They may help to improve the control of ascites and reduce recurrence after large volume paracentesis Mannitol Metolazone Spironolactone Amiloride furosemide H20 V 2 receptor antagonist
26 Satavaptan for Ascites Management (14 days) Kg Change in body weight at day 14 compared to baseline Worsening ascites * -2.08* -2.28* placebo 5mg 12.5mg 25mg Satavaptan *p<0.05 compared to placebo Patients (%) ** 10** placebo 5mg 12.5mg 25mg Satavaptan ** p<0.1 vs. placebo
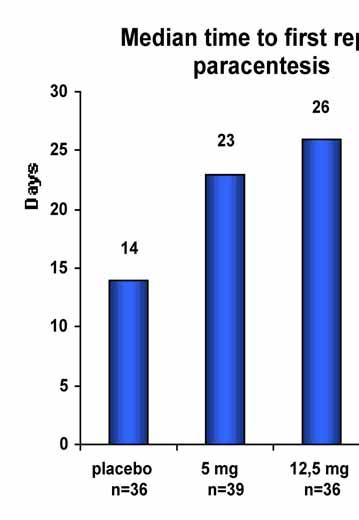
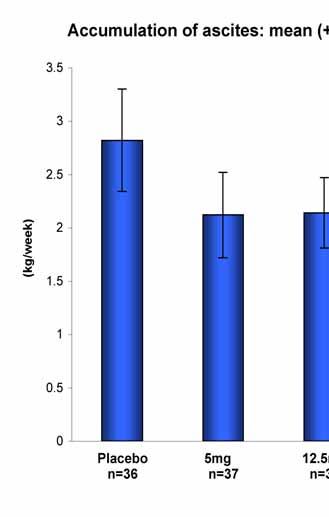
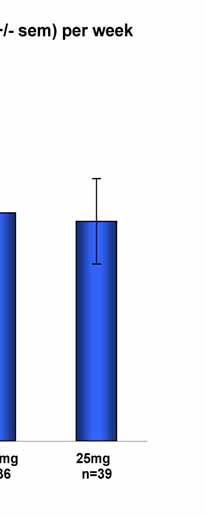
27 Satavaptan for Ascites Management (12 weeks)


28 Satavaptan for Ascites Management (12 weeks) Reduction in number of paracenteses versus placebo Relative risk of paracentesis was 0.69, 0.66, 0.63 for the 5 mg, 12.5 mg and 25 mg groups respectively Corresponding adjusted p-values are 0.026, 0.018, for the three treated groups n=36 n=39 n=36 n=40
29 Take Home Messages From Sodium Retention to Therapy for Refractory Ascites The Role for New Drugs Sodium restriction is still an important and necessary part of the management of refractory ascites Albumin may be useful as an adjunct treatment for refractory ascites Vasoconstrictor therapy shows promise in improving natriuresis, but long-term studies are lacking. V 2 receptor antagonists correct hyponatremia, and therefore may allow re-introduction of diuretics in patients with diuretic resistant ascites V 2 receptor antagonists, independent of serum [Na], have the potential to reduce recurrence of ascites for up to 12 weeks of treatment
The Management of Ascites & Hepatorenal Syndrome. Florence Wong University of Toronto. Falk Symposium March 14, 2008
 The Management of Ascites & Hepatorenal Syndrome Florence Wong University of Toronto Falk Symposium March 14, 2008 Management of Ascites Sodium Restriction Mandatory at all stages of ascites in order to
The Management of Ascites & Hepatorenal Syndrome Florence Wong University of Toronto Falk Symposium March 14, 2008 Management of Ascites Sodium Restriction Mandatory at all stages of ascites in order to
Management of Ascites and Hepatorenal Syndrome. Florence Wong University of Toronto. June 4, /16/ Gore & Associates: Consultancy
 Management of Ascites and Hepatorenal Syndrome Florence Wong University of Toronto June 4, 2016 6/16/2016 1 Disclosures Gore & Associates: Consultancy Sequana Medical: Research Funding Mallinckrodt Pharmaceutical:
Management of Ascites and Hepatorenal Syndrome Florence Wong University of Toronto June 4, 2016 6/16/2016 1 Disclosures Gore & Associates: Consultancy Sequana Medical: Research Funding Mallinckrodt Pharmaceutical:
Initial approach to ascites
 Ascites: Filling and Draining the Water Balloon Common Pathogenesis in Refractory Ascites, Hyponatremia, and Cirrhosis intrahepatic resistance sinusoidal portal hypertension Splanchnic vasodilation (effective
Ascites: Filling and Draining the Water Balloon Common Pathogenesis in Refractory Ascites, Hyponatremia, and Cirrhosis intrahepatic resistance sinusoidal portal hypertension Splanchnic vasodilation (effective
Management of Cirrhotic Complications Uncontrolled Ascites. Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University
 Management of Cirrhotic Complications Uncontrolled Ascites Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University Topic Definition, pathogenesis Current therapeutic options Experimental treatments
Management of Cirrhotic Complications Uncontrolled Ascites Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University Topic Definition, pathogenesis Current therapeutic options Experimental treatments
Hepatorenal syndrome a defined entity with a standard treatment?
 Hepatorenal syndrome a defined entity with a standard treatment? Falk Symposium 162 Dresden - October 14, 2007 Alexander L. Gerbes Klinikum of the University of Munich Grosshadern Department of Medicine
Hepatorenal syndrome a defined entity with a standard treatment? Falk Symposium 162 Dresden - October 14, 2007 Alexander L. Gerbes Klinikum of the University of Munich Grosshadern Department of Medicine
Hyponatremia as a Cardiovascular Biomarker
 Hyponatremia as a Cardiovascular Biomarker Uri Elkayam, MD Professor of Medicine University of Southern California Keck School of Medicine elkayam@usc.edu Disclosure Research grant from Otsuka for the
Hyponatremia as a Cardiovascular Biomarker Uri Elkayam, MD Professor of Medicine University of Southern California Keck School of Medicine elkayam@usc.edu Disclosure Research grant from Otsuka for the
Hepatorenal syndrome. Jan T. Kielstein Departent of Nephrology Medical School Hannover
 Hepatorenal syndrome Jan T. Kielstein Departent of Nephrology Medical School Hannover Hepatorenal Syndrome 1) History of HRS 2) Pathophysiology of HRS 3) Definition of HRS 4) Clinical presentation of HRS
Hepatorenal syndrome Jan T. Kielstein Departent of Nephrology Medical School Hannover Hepatorenal Syndrome 1) History of HRS 2) Pathophysiology of HRS 3) Definition of HRS 4) Clinical presentation of HRS
JOURNAL PRESENTATION. Dr Tina Fan Tseung Kwan O Hospital 17 th Jan 2013
 JOURNAL PRESENTATION Dr Tina Fan Tseung Kwan O Hospital 17 th Jan 2013 THE COMBINATION OF OCTREOTIDE AND MIDODRINE IS NOT SUPERIOR TO ALBUMIN IN PREVENTING RECURRENCE OF ASCITES AFTER LARGE-VOLUME PARACENTESIS
JOURNAL PRESENTATION Dr Tina Fan Tseung Kwan O Hospital 17 th Jan 2013 THE COMBINATION OF OCTREOTIDE AND MIDODRINE IS NOT SUPERIOR TO ALBUMIN IN PREVENTING RECURRENCE OF ASCITES AFTER LARGE-VOLUME PARACENTESIS
Hyponatremia in Heart Failure: why it is important and what should we do about it?
 Objectives Hyponatremia in Heart Failure: why it is important and what should we do about it? Pathophysiology of sodium and water retention in heart failure Hyponatremia in heart failure (mechanism and
Objectives Hyponatremia in Heart Failure: why it is important and what should we do about it? Pathophysiology of sodium and water retention in heart failure Hyponatremia in heart failure (mechanism and
Diuretic Agents Part-2. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Diuretic Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Potassium-sparing diuretics The Ion transport pathways across the luminal and basolateral
Diuretic Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Potassium-sparing diuretics The Ion transport pathways across the luminal and basolateral
DIURETICS-4 Dr. Shariq Syed
 DIURETICS-4 Dr. Shariq Syed AIKTC - Knowledge Resources & Relay Center 1 Pop Quiz!! Loop diuretics act on which transporter PKCC NKCC2 AIKTCC I Don t know AIKTC - Knowledge Resources & Relay Center 2 Pop
DIURETICS-4 Dr. Shariq Syed AIKTC - Knowledge Resources & Relay Center 1 Pop Quiz!! Loop diuretics act on which transporter PKCC NKCC2 AIKTCC I Don t know AIKTC - Knowledge Resources & Relay Center 2 Pop
Ascites Management. Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology
 Ascites Management Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Disclosure 1. The speaker Atif Zaman, MD MPH have no relevant
Ascites Management Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Disclosure 1. The speaker Atif Zaman, MD MPH have no relevant
Arginine vasopressin (AVP) is a
 is a") Akash Parashar, MD; Patrick Martinucci, DO; Mandip Panesar, MD The authors are with the University at Buffalo, Erie County Medical Center, Buffalo, New York. Dr. Panesar is a member of D&T s Editorial
Akash Parashar, MD; Patrick Martinucci, DO; Mandip Panesar, MD The authors are with the University at Buffalo, Erie County Medical Center, Buffalo, New York. Dr. Panesar is a member of D&T s Editorial
EDUCATION PRACTICE. Cirrhosis With Refractory Ascites: Serial Large Volume Paracentesis, TIPS, or Transplantation?
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2011;9:931 935 EDUCATION PRACTICE Cirrhosis With Refractory Ascites: Serial Large Volume Paracentesis, TIPS, or Transplantation? VANDANA KHUNGAR* and SAMMY SAAB*,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2011;9:931 935 EDUCATION PRACTICE Cirrhosis With Refractory Ascites: Serial Large Volume Paracentesis, TIPS, or Transplantation? VANDANA KHUNGAR* and SAMMY SAAB*,
Management of ascites in cirrhosis
 doi:10.1111/j.1440-1746.2011.06925.x ADVANCES IN CLINICAL PRACTICE jgh_6925 11..20 Management of ascites in cirrhosis Florence Wong Department of Medicine, Toronto General Hospital, University of Toronto,
doi:10.1111/j.1440-1746.2011.06925.x ADVANCES IN CLINICAL PRACTICE jgh_6925 11..20 Management of ascites in cirrhosis Florence Wong Department of Medicine, Toronto General Hospital, University of Toronto,
Hepatorenal syndrome. Jan Jan T. T. Kielstein Departent of of Nephrology Medical School School Hannover
 Hepatorenal syndrome Jan Jan T. T. Kielstein Departent of of Nephrology Medical School School Hannover Hepatorenal Syndrome 1) History of HRS 2) Pathophysiology of HRS 3) Definition of HRS 4) Clinical
Hepatorenal syndrome Jan Jan T. T. Kielstein Departent of of Nephrology Medical School School Hannover Hepatorenal Syndrome 1) History of HRS 2) Pathophysiology of HRS 3) Definition of HRS 4) Clinical
Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome
 Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome Disclosure I have no conflicts of interest to disclose Name: Margarita Taburyanskaya Title: PharmD, PGY1 Pharmacy Practice Resident
Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome Disclosure I have no conflicts of interest to disclose Name: Margarita Taburyanskaya Title: PharmD, PGY1 Pharmacy Practice Resident
Ascites and hepatorenal syndrome in cirrhosis: pathophysiological basis of therapy and current management
 Journal of Hepatology 38 (2003) S69 S89 www.elsevier.com/locate/jhep Ascites and hepatorenal syndrome in cirrhosis: pathophysiological basis of therapy and current management Vicente Arroyo*, Jordi Colmenero
Journal of Hepatology 38 (2003) S69 S89 www.elsevier.com/locate/jhep Ascites and hepatorenal syndrome in cirrhosis: pathophysiological basis of therapy and current management Vicente Arroyo*, Jordi Colmenero
Prof. Mohammad Umar. MBBS, MCPS, FCPS, FACG (USA), FRCP (London), FRCP (Glasgow), FAGA
, FRCP (London), FRCP (Glasgow), FAGA") Prof. Mohammad Umar MBBS, MCPS, FCPS, FACG (USA), FRCP (London), FRCP (Glasgow), FAGA Chairman and Head Department of Medicine Rawalpindi Medical College, Rawalpindi. Consultant Gastroenterologist / Hepatologist
Prof. Mohammad Umar MBBS, MCPS, FCPS, FACG (USA), FRCP (London), FRCP (Glasgow), FAGA Chairman and Head Department of Medicine Rawalpindi Medical College, Rawalpindi. Consultant Gastroenterologist / Hepatologist
A Study To Evaluate The Efficacy Of Tolvaptan In Correction Of Hyponatremia And Its Effect On..
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 5 Ver. 11 (May. 2018), PP 29-34 www.iosrjournals.org A Study To Evaluate The Efficacy Of Tolvaptan
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 5 Ver. 11 (May. 2018), PP 29-34 www.iosrjournals.org A Study To Evaluate The Efficacy Of Tolvaptan
Ascites is the most frequent complication of cirrhosis,
 Beneficial Effect of Midodrine in Hypotensive Cirrhotic Patients with Refractory Ascites G & H C l i n i c a l C a s e S t u d i e s Achuthan Sourianarayanane, MD, MRCP 1 David S. Barnes, MD 1,2 Arthur
Beneficial Effect of Midodrine in Hypotensive Cirrhotic Patients with Refractory Ascites G & H C l i n i c a l C a s e S t u d i e s Achuthan Sourianarayanane, MD, MRCP 1 David S. Barnes, MD 1,2 Arthur
Case Report Tolvaptan in the Treatment of Acute Hyponatremia Associated with Acute Kidney Injury
 Case Reports in Nephrology Volume 2013, Article ID 801575, 4 pages http://dx.doi.org/10.1155/2013/801575 Case Report Tolvaptan in the Treatment of Acute Hyponatremia Associated with Acute Kidney Injury
Case Reports in Nephrology Volume 2013, Article ID 801575, 4 pages http://dx.doi.org/10.1155/2013/801575 Case Report Tolvaptan in the Treatment of Acute Hyponatremia Associated with Acute Kidney Injury
State of the Art Treatment - Hyponatremia, Heart Rate, et al
 State of the Art Treatment - Hyponatremia, Heart Rate, et al Uri Elkayam, MD Professor of Medicine University of Southern California Keck School of Medicine elkayam@usc.edu Disclosure Research grant from
State of the Art Treatment - Hyponatremia, Heart Rate, et al Uri Elkayam, MD Professor of Medicine University of Southern California Keck School of Medicine elkayam@usc.edu Disclosure Research grant from
Controversies in Management of Portal Hypertension and Cirrhosis Complications in the Transplant Candidate
 Controversies in Management of Portal Hypertension and Cirrhosis Complications in the Transplant Candidate Patrick Northup, MD, FAASLD, FACG Medical Director, Liver Transplantation University of Virginia
Controversies in Management of Portal Hypertension and Cirrhosis Complications in the Transplant Candidate Patrick Northup, MD, FAASLD, FACG Medical Director, Liver Transplantation University of Virginia
Beta-blockers in cirrhosis: Cons
 Beta-blockers in cirrhosis: Cons Eric Trépo MD, PhD Dept. of Gastroenterology. Hepatopancreatology and Digestive Oncology. C.U.B. Hôpital Erasme. Université Libre de Bruxelles. Bruxelles. Belgium Laboratory
Beta-blockers in cirrhosis: Cons Eric Trépo MD, PhD Dept. of Gastroenterology. Hepatopancreatology and Digestive Oncology. C.U.B. Hôpital Erasme. Université Libre de Bruxelles. Bruxelles. Belgium Laboratory
The Cardiorenal Syndrome in Heart Failure
 The Cardiorenal Syndrome in Heart Failure Van N Selby, MD Assistant Professor of Medicine Advanced Heart Failure Program, UCSF October 9, 2015 Disclosures None 1 Cardiorenal Syndrome (CRS) A pathophysiologic
The Cardiorenal Syndrome in Heart Failure Van N Selby, MD Assistant Professor of Medicine Advanced Heart Failure Program, UCSF October 9, 2015 Disclosures None 1 Cardiorenal Syndrome (CRS) A pathophysiologic
AASLD PRACTICE GUIDELINE Management of Adult Patients with Ascites Due to Cirrhosis: Update 2012
 AASLD PRACTICE GUIDELINE Management of Adult Patients with Ascites Due to Cirrhosis: Update 2012 Bruce A. Runyon, M.D. Preamble This guideline has been approved by the American Association for the Study
AASLD PRACTICE GUIDELINE Management of Adult Patients with Ascites Due to Cirrhosis: Update 2012 Bruce A. Runyon, M.D. Preamble This guideline has been approved by the American Association for the Study
Uri Elkayam, MD. Professor of Medicine University of Southern California Keck School of Medicine
 Mihai Gheorghiade, MD Memorial Lecture Use of Vasopressin Antagonists for the Management of Hyponatremia and Volume Overload Uri Elkayam, MD Professor of Medicine University of Southern California Keck
Mihai Gheorghiade, MD Memorial Lecture Use of Vasopressin Antagonists for the Management of Hyponatremia and Volume Overload Uri Elkayam, MD Professor of Medicine University of Southern California Keck
Hepatorenal Syndrome
 Necker Seminars in Nephrology Institut Pasteur Paris, April 22, 2013 Hepatorenal Syndrome Dr. Richard Moreau 1 INSERM U773, Centre de Recherche Biomédicale Bichat-Beaujon CRB3, 2 Université Paris Diderot
Necker Seminars in Nephrology Institut Pasteur Paris, April 22, 2013 Hepatorenal Syndrome Dr. Richard Moreau 1 INSERM U773, Centre de Recherche Biomédicale Bichat-Beaujon CRB3, 2 Université Paris Diderot
EDUCATION PRACTICE. Management of Refractory Ascites. Clinical Scenario. The Problem
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:1187 1191 EDUCATION PRACTICE Management of Refractory Ascites ANDRÉS CÁRDENAS and PERE GINÈS Liver Unit, Institute of Digestive Diseases, Hospital Clínic,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:1187 1191 EDUCATION PRACTICE Management of Refractory Ascites ANDRÉS CÁRDENAS and PERE GINÈS Liver Unit, Institute of Digestive Diseases, Hospital Clínic,
Therapeutics of Diuretics
 (Last Updated: 08/22/2018) Created by: Socco, Samantha Therapeutics of Diuretics Thambi, M. (2017). The Clinical Use of Diuretics. Lecture presented at PHAR 503 Lecture in UIC College of Pharmacy, Chicago.
(Last Updated: 08/22/2018) Created by: Socco, Samantha Therapeutics of Diuretics Thambi, M. (2017). The Clinical Use of Diuretics. Lecture presented at PHAR 503 Lecture in UIC College of Pharmacy, Chicago.
Arginine vasopressin has attracted attention as a potentially
 New Drugs and Technologies Arginine Vasopressin Antagonists for the Treatment of Heart Failure and Hyponatremia John J. Finley IV, MD; Marvin A. Konstam, MD; James E. Udelson, MD Arginine vasopressin has
New Drugs and Technologies Arginine Vasopressin Antagonists for the Treatment of Heart Failure and Hyponatremia John J. Finley IV, MD; Marvin A. Konstam, MD; James E. Udelson, MD Arginine vasopressin has
Therapy Insight: management of hepatorenal syndrome
 Therapy Insight: management of hepatorenal syndrome Andrés Cárdenas and Pere Ginès* SUMMARY Hepatorenal syndrome (HRS), a feared complication of advanced cirrhosis, is characterized by functional renal
Therapy Insight: management of hepatorenal syndrome Andrés Cárdenas and Pere Ginès* SUMMARY Hepatorenal syndrome (HRS), a feared complication of advanced cirrhosis, is characterized by functional renal
Ascites is a serious complication of cirrhosis, occurring
 Terlipressin Improves Renal Function in Patients with Cirrhosis and Ascites Without Hepatorenal Syndrome Aleksander Krag, 1,2 Søren Møller, 2 Jens H. Henriksen, 2 Niels-Henrik Holstein-Rathlou, 3 Fin Stolze
Terlipressin Improves Renal Function in Patients with Cirrhosis and Ascites Without Hepatorenal Syndrome Aleksander Krag, 1,2 Søren Møller, 2 Jens H. Henriksen, 2 Niels-Henrik Holstein-Rathlou, 3 Fin Stolze
The Kidney in Liver Disease. Jeff Kaufhold MD FACP Nephrology Assoc. of Dayton Oct 2018
 The Kidney in Liver Disease Jeff Kaufhold MD FACP Nephrology Assoc. of Dayton Oct 2018 Objectives 1. Understand new evidence in the pathophysiology of Hepatorenal syndrome 2. Review current treatment guidelines
The Kidney in Liver Disease Jeff Kaufhold MD FACP Nephrology Assoc. of Dayton Oct 2018 Objectives 1. Understand new evidence in the pathophysiology of Hepatorenal syndrome 2. Review current treatment guidelines
EASL clinical practice guidelines on the management of ascites, spontaneous bacterial peritonitis, and hepatorenal syndrome in cirrhosis
 EASL clinical practice guidelines on the management of ascites, spontaneous bacterial peritonitis, and hepatorenal syndrome in cirrhosis European Association for the Study of the Liver 1 Ascites is the
EASL clinical practice guidelines on the management of ascites, spontaneous bacterial peritonitis, and hepatorenal syndrome in cirrhosis European Association for the Study of the Liver 1 Ascites is the
Management of Acute Decompensation of Cirrhosis JOHN O GRADY KING S COLLEGE HOSPITAL
 Management of Acute Decompensation of Cirrhosis JOHN O GRADY KING S COLLEGE HOSPITAL Terminology Acute decompensation of cirrhosis - stable patient with sudden deterioration Acute-on-chronic liver failure
Management of Acute Decompensation of Cirrhosis JOHN O GRADY KING S COLLEGE HOSPITAL Terminology Acute decompensation of cirrhosis - stable patient with sudden deterioration Acute-on-chronic liver failure
Tiny Jaarsma Linköping University No conflict of interest
 Detrimental effects of sodium in heart failure - Tiny Jaarsma Linköping University No conflict of interest Sodium restriction in Heart Failure Why? Prevention of heart failure Blood pressure treatment
Detrimental effects of sodium in heart failure - Tiny Jaarsma Linköping University No conflict of interest Sodium restriction in Heart Failure Why? Prevention of heart failure Blood pressure treatment
Case Report Low-Dose Tolvaptan for the Treatment of Dilutional Hyponatremia in Cirrhosis: A Case Report and Literature Review
 Case Reports in Hepatology, Article ID 795261, 4 pages http://dx.doi.org/10.1155/2014/795261 Case Report Low-Dose Tolvaptan for the Treatment of Dilutional Hyponatremia in Cirrhosis: A Case Report and
Case Reports in Hepatology, Article ID 795261, 4 pages http://dx.doi.org/10.1155/2014/795261 Case Report Low-Dose Tolvaptan for the Treatment of Dilutional Hyponatremia in Cirrhosis: A Case Report and
Original Article. Noradrenaline is as Effective as Terlipressin in Hepatorenal Syndrome Type 1: A Prospective, Randomized Trial
 30 Journal of The Association of Physicians of India Vol. 64 September 2016 Original Article Noradrenaline is as Effective as Terlipressin in Hepatorenal Syndrome Type 1: A Prospective, Randomized Trial
30 Journal of The Association of Physicians of India Vol. 64 September 2016 Original Article Noradrenaline is as Effective as Terlipressin in Hepatorenal Syndrome Type 1: A Prospective, Randomized Trial
SAMSCA (tolvaptan) oral tablet
 oral tablet") SAMSCA (tolvaptan) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
SAMSCA (tolvaptan) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
Case Report Triple Diuretics and Aquaretic Strategy for Acute Decompensated Heart Failure due to Volume Overload
 Case Reports in Cardiology Volume 2013, Article ID 750794, 4 pages http://dx.doi.org/10.1155/2013/750794 Case Report Triple Diuretics and Aquaretic Strategy for Acute Decompensated Heart Failure due to
Case Reports in Cardiology Volume 2013, Article ID 750794, 4 pages http://dx.doi.org/10.1155/2013/750794 Case Report Triple Diuretics and Aquaretic Strategy for Acute Decompensated Heart Failure due to
Association between the Serum Sodium Levels and the Response to Tolvaptan in Liver Cirrhosis Patients with Ascites and Hyponatremia
 doi: 10.2169/internalmedicine.0629-17 Intern Med 57: 2451-2458, 2018 http://internmed.jp ORIGINAL ARTICLE Association between the Serum Sodium Levels and the Response to Tolvaptan in Liver Cirrhosis Patients
doi: 10.2169/internalmedicine.0629-17 Intern Med 57: 2451-2458, 2018 http://internmed.jp ORIGINAL ARTICLE Association between the Serum Sodium Levels and the Response to Tolvaptan in Liver Cirrhosis Patients
Hepatorenal syndrome
 Annals of Hepatology 2003; 2(1): January-March: 23-29 Concise Review Annals of Hepatology Hepatorenal syndrome Andrés Cárdenas, M.D., 1 Vicente Arroyo, M.D. 2 Abstract Hepatorenal syndrome is complication
Annals of Hepatology 2003; 2(1): January-March: 23-29 Concise Review Annals of Hepatology Hepatorenal syndrome Andrés Cárdenas, M.D., 1 Vicente Arroyo, M.D. 2 Abstract Hepatorenal syndrome is complication
REVIEW. Ariel W. Aday, M.D.,* Nicole E. Rich, M.D.,* Arjmand R. Mufti, M.D., and Shannan R. Tujios, M.D.
 REVIEW CON ( The Window Is Closed ): In Patients With Cirrhosis With Ascites, the Clinical Risks of Nonselective beta-blocker Outweigh the Benefits and Should NOT Be Prescribed Ariel W. Aday, M.D.,* Nicole
REVIEW CON ( The Window Is Closed ): In Patients With Cirrhosis With Ascites, the Clinical Risks of Nonselective beta-blocker Outweigh the Benefits and Should NOT Be Prescribed Ariel W. Aday, M.D.,* Nicole
Over- and underfill: not all nephrotic states are equal. Detlef Bockenhauer
 Over- and underfill: not all nephrotic states are equal Detlef Bockenhauer Objectives Review pathophysiology of oedema: undervs overfill Treatment options The clinical setting: case 1 A6-y old girl with
Over- and underfill: not all nephrotic states are equal Detlef Bockenhauer Objectives Review pathophysiology of oedema: undervs overfill Treatment options The clinical setting: case 1 A6-y old girl with
Pathophysiology, diagnosis and treatment of ascites in cirrhosis
 Annals of hepatology 2002; 1(2): April-June: 72-79 Concise Review Annals of hepatology Pathophysiology, diagnosis and treatment of ascites in cirrhosis Vicente Arroyo 1, M.D. Abstract The mechanism by
Annals of hepatology 2002; 1(2): April-June: 72-79 Concise Review Annals of hepatology Pathophysiology, diagnosis and treatment of ascites in cirrhosis Vicente Arroyo 1, M.D. Abstract The mechanism by
CIRRHOTIC MANAGEMENT
 DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
Developed for Scotland by the National Plasma Product Expert Advisory Group. Clinical Guidelines for Human Albumin Use
 Approved by NPPEAG 28 May 2018 Reviewed 1 June 2018 To be reviewed 1 June 2020 Developed for Scotland by the National Plasma Product Expert Advisory Group Clinical Guidelines for Human Albumin Use 1 National
Approved by NPPEAG 28 May 2018 Reviewed 1 June 2018 To be reviewed 1 June 2020 Developed for Scotland by the National Plasma Product Expert Advisory Group Clinical Guidelines for Human Albumin Use 1 National
Management of Cirrhosis Related Complications
 Management of Cirrhosis Related Complications Ke-Qin Hu, MD, FAASLD Professor of Clinical Medicine Director of Hepatology University of California, Irvine Disclosure I have no disclosure related to this
Management of Cirrhosis Related Complications Ke-Qin Hu, MD, FAASLD Professor of Clinical Medicine Director of Hepatology University of California, Irvine Disclosure I have no disclosure related to this
Hyponatraemia. Detlef Bockenhauer
 Hyponatraemia Detlef Bockenhauer Key message Plasma sodium can be low due to either excess water or deficiency of salt In clinical practice, dysnatraemias almost always reflect an abnormality of water
Hyponatraemia Detlef Bockenhauer Key message Plasma sodium can be low due to either excess water or deficiency of salt In clinical practice, dysnatraemias almost always reflect an abnormality of water
Optimal management of ascites
 Optimal management of ascites P. Angeli, Dept. of Medicine, Unit of Internal Medicine and epatology (), University of Padova (Italy) pangeli@unipd.it 10th Paris epatology Conference National Conference
Optimal management of ascites P. Angeli, Dept. of Medicine, Unit of Internal Medicine and epatology (), University of Padova (Italy) pangeli@unipd.it 10th Paris epatology Conference National Conference
Pathophysiology of ascites and dilutional hyponatremia: Contemporary use of aquaretic agents
 Annals of Hepatology 2007; 6(4): October-December: 214-221 Annals of Hepatology Concise Review Pathophysiology of ascites and dilutional hyponatremia: Contemporary use of aquaretic agents Jorge García
Annals of Hepatology 2007; 6(4): October-December: 214-221 Annals of Hepatology Concise Review Pathophysiology of ascites and dilutional hyponatremia: Contemporary use of aquaretic agents Jorge García
Therapeutic Potential of Vasopressin-Receptor Antagonists in Heart Failure
 J Pharmacol Sci 124, 000 000 (2014) Journal of Pharmacological Sciences The Japanese Pharmacological Society Current Perspective Therapeutic Potential of Vasopressin-Receptor Antagonists in Heart Failure
J Pharmacol Sci 124, 000 000 (2014) Journal of Pharmacological Sciences The Japanese Pharmacological Society Current Perspective Therapeutic Potential of Vasopressin-Receptor Antagonists in Heart Failure
Hyponatremia: A Review
 Analytic Review Hyponatremia: A Review Mary Ansley Buffington, MD, JD 1 and Kenneth Abreo, MD 1 Journal of Intensive Care Medicine 2016, Vol. 31(4) 223-236 ª The Author(s) 2015 Reprints and permission:
Analytic Review Hyponatremia: A Review Mary Ansley Buffington, MD, JD 1 and Kenneth Abreo, MD 1 Journal of Intensive Care Medicine 2016, Vol. 31(4) 223-236 ª The Author(s) 2015 Reprints and permission:
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,100 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,100 116,000 120M Open access books available International authors and editors Downloads Our
Cardiorenal Syndrome Prof. Dr. Bülent ALTUN Hacettepe University Faculty of Medicine Department of Internal Medicine Division of Nephrology
 Cardiorenal Syndrome Prof. Dr. Bülent ALTUN Hacettepe University Faculty of Medicine Department of Internal Medicine Division of Nephrology Heart and Kidney The kidney yin dominates water, The heart yang
Cardiorenal Syndrome Prof. Dr. Bülent ALTUN Hacettepe University Faculty of Medicine Department of Internal Medicine Division of Nephrology Heart and Kidney The kidney yin dominates water, The heart yang
Hepatology on the AMU
 Hepatology on the AMU RCP day, 8 th February 2018 Jo Leithead Consultant in Hepatology and Liver Transplantation Addenbrookes Hospital Cambridge Is liver disease relevant to me? Williams R, Lancet 2014
Hepatology on the AMU RCP day, 8 th February 2018 Jo Leithead Consultant in Hepatology and Liver Transplantation Addenbrookes Hospital Cambridge Is liver disease relevant to me? Williams R, Lancet 2014
All but Vaptans. Pr Guy DECAUX Service de Médecine Interne Général Cliniques Universitaires Erasme, Bruxelles
 All but Vaptans Pr Guy DECAUX Service de Médecine Interne Général Cliniques Universitaires Erasme, Bruxelles [ Na ] = Na + e + K + e TBW 60 y BW 66 kg, TBW ± 33 L, SNa 140 meq/l TBW 1 L SNa: 3% (or 4.2
All but Vaptans Pr Guy DECAUX Service de Médecine Interne Général Cliniques Universitaires Erasme, Bruxelles [ Na ] = Na + e + K + e TBW 60 y BW 66 kg, TBW ± 33 L, SNa 140 meq/l TBW 1 L SNa: 3% (or 4.2
Filippo Schepis, MD Università degli Studi di Modena e Reggio Emilia
 Filippo Schepis, MD Università degli Studi di Modena e Reggio Emilia Il sottoscritto dichiara di non aver avuto/di aver avuto negli ultimi 12 mesi conflitto d interesse in relazione a questa presentazione
Filippo Schepis, MD Università degli Studi di Modena e Reggio Emilia Il sottoscritto dichiara di non aver avuto/di aver avuto negli ultimi 12 mesi conflitto d interesse in relazione a questa presentazione
Hyponatremia. Mis-named talk? Basic Pathophysiology
 Hyponatremia Great Lakes Hospital Medicine Symposium by Brian Wolfe, MD Assistant Professor of Internal Medicine University of Colorado Denver Mis-named talk? Why do we care about Hyponatremia? concentration
Hyponatremia Great Lakes Hospital Medicine Symposium by Brian Wolfe, MD Assistant Professor of Internal Medicine University of Colorado Denver Mis-named talk? Why do we care about Hyponatremia? concentration
Chapter 21. Diuretic Agents. Mosby items and derived items 2008, 2002 by Mosby, Inc., an affiliate of Elsevier Inc.
 Chapter 21 Diuretic Agents Renal Structure and Function Kidneys at level of umbilicus Each weighs 160 to 175 g and is 10 to 12 cm long Most blood flow per gram of weight in body 22% of cardiac output (CO)
Chapter 21 Diuretic Agents Renal Structure and Function Kidneys at level of umbilicus Each weighs 160 to 175 g and is 10 to 12 cm long Most blood flow per gram of weight in body 22% of cardiac output (CO)
Liver-Kidney Crosstalk in Liver and Kidney Diseases
 Liver-Kidney Crosstalk in Liver and Kidney Diseases Sundararaman Swaminathan MD Associate Professor Division of Nephrology University of Virginia Health System Charlottesville, VA Hepatonephrologist busily
Liver-Kidney Crosstalk in Liver and Kidney Diseases Sundararaman Swaminathan MD Associate Professor Division of Nephrology University of Virginia Health System Charlottesville, VA Hepatonephrologist busily
CIRCULATORY AND RENAL FAILURE IN CIRRHOSIS
 CIRCULATORY AND RENAL FAILURE IN CIRRHOSIS Pere Ginès, MD Liver Unit, Hospital Clínic Barcelona, Catalunya, Spain CIRCULATORY AND RENAL FAILURE IN CIRRHOSIS Hecker R and Sherlock S, The Lancet 1956 RENAL
CIRCULATORY AND RENAL FAILURE IN CIRRHOSIS Pere Ginès, MD Liver Unit, Hospital Clínic Barcelona, Catalunya, Spain CIRCULATORY AND RENAL FAILURE IN CIRRHOSIS Hecker R and Sherlock S, The Lancet 1956 RENAL
Developed for Scotland by the National Plasma Product Expert Advisory Group. Clinical Guidelines for Human Albumin Use
 Approved by NPPEAG 10 December 2010 Reviewed 1 June 2012 To be reviewed 1 June 2014 Developed for Scotland by the National Plasma Product Expert Advisory Group Clinical Guidelines for Human Albumin Use
Approved by NPPEAG 10 December 2010 Reviewed 1 June 2012 To be reviewed 1 June 2014 Developed for Scotland by the National Plasma Product Expert Advisory Group Clinical Guidelines for Human Albumin Use
The Kidney in Liver Disease. Jeff Kaufhold MD FACP Jan 2018
 The Kidney in Liver Disease Jeff Kaufhold MD FACP Jan 2018 Objectives 1. Understand new evidence in the pathophysiology of Hepatorenal syndrome 2. Review current treatment guidelines and some over the
The Kidney in Liver Disease Jeff Kaufhold MD FACP Jan 2018 Objectives 1. Understand new evidence in the pathophysiology of Hepatorenal syndrome 2. Review current treatment guidelines and some over the
Intravenous Furosemide and Human Albumin for Treatment of Cirrhotic Ascites: Useful or Harmful?
 Ibnosina J Med BS 83 ARTICLE Intravenous Furosemide and Human Albumin for Treatment of Cirrhotic Ascites: Useful or Harmful? Faisal O. Abubakor, Hind I. Fallatah, Hisham O. Akbar Department of Medicine,
Ibnosina J Med BS 83 ARTICLE Intravenous Furosemide and Human Albumin for Treatment of Cirrhotic Ascites: Useful or Harmful? Faisal O. Abubakor, Hind I. Fallatah, Hisham O. Akbar Department of Medicine,
The Art and Science of Diuretic therapy
 The Art and Science of Diuretic therapy Dr. Fayez EL Shaer Associate Professour of cardiology Consultant cardiologist MD, MSc, PhD, CBNC, NBE FESC, ACCP, FASNC,HFA KKUH, KFCC Heart failure: fluid overload
The Art and Science of Diuretic therapy Dr. Fayez EL Shaer Associate Professour of cardiology Consultant cardiologist MD, MSc, PhD, CBNC, NBE FESC, ACCP, FASNC,HFA KKUH, KFCC Heart failure: fluid overload
T herapeutic (that is, total) paracentesis is used in patients
 paracentesis is used in patients") 90 LIVER AND BILIARY DISEASE Comparison of the effect of terlipressin and albumin on arterial blood volume in patients with cirrhosis and tense ascites treated by : a randomised pilot study R Moreau, T
90 LIVER AND BILIARY DISEASE Comparison of the effect of terlipressin and albumin on arterial blood volume in patients with cirrhosis and tense ascites treated by : a randomised pilot study R Moreau, T
Vasopressin and Vasopressin Receptor Antagonists
 Review article Electrolyte & Blood Pressure 6:51-55, 2008 51 1) Vasopressin and Vasopressin Receptor Antagonists Yun Kyu Oh, M.D. Department of Internal Medicine, Seoul National University Boramae Hospital
Review article Electrolyte & Blood Pressure 6:51-55, 2008 51 1) Vasopressin and Vasopressin Receptor Antagonists Yun Kyu Oh, M.D. Department of Internal Medicine, Seoul National University Boramae Hospital
RENAL DISEASE IN END STAGE LIVER DISEASE
 RENAL DISEASE IN END STAGE LIVER DISEASE Mitchell L Shiffman, MD Director Health System Richmond and Newport News, VA Medical Group Good Help to Those in Need Mitchell L Shiffman, MD POTENTIAL CONFLICTS
RENAL DISEASE IN END STAGE LIVER DISEASE Mitchell L Shiffman, MD Director Health System Richmond and Newport News, VA Medical Group Good Help to Those in Need Mitchell L Shiffman, MD POTENTIAL CONFLICTS
Pharmacology I [PHL 313] Diuretics. Dr. Mohammad Nazam Ansari
![Pharmacology I [PHL 313] Diuretics. Dr. Mohammad Nazam Ansari](/thumbs/90/104323364.jpg "Pharmacology I [PHL 313] Diuretics. Dr. Mohammad Nazam Ansari") Pharmacology I [PHL 313] Diuretics Dr. Mohammad Nazam Ansari Renal Pharmacology Kidneys: Each adult kidney weighs 125-170g in males and 115-155g in females, represent 0.5% of total body weight, but receive
Pharmacology I [PHL 313] Diuretics Dr. Mohammad Nazam Ansari Renal Pharmacology Kidneys: Each adult kidney weighs 125-170g in males and 115-155g in females, represent 0.5% of total body weight, but receive
The Yellow Patient. Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust
 The Yellow Patient Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust there s a yellow patient in bed 40. It s one of yours. Liver Cirrhosis Why.When.What.etc.
The Yellow Patient Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust there s a yellow patient in bed 40. It s one of yours. Liver Cirrhosis Why.When.What.etc.
Review Article Management of Renal Failure and Ascites in Patients with Cirrhosis
 SAGE-Hindawi Access to Research International Journal of Hepatology Volume 2011, Article ID 790232, 7 pages doi:10.4061/2011/790232 Review Article Management of Renal Failure and Ascites in Patients with
SAGE-Hindawi Access to Research International Journal of Hepatology Volume 2011, Article ID 790232, 7 pages doi:10.4061/2011/790232 Review Article Management of Renal Failure and Ascites in Patients with
Diuretics (Saluretics)
") Diuretics (Saluretics) Diuretics increase urine excretion mainly by reabsorption of salts and water from kidney tubules These agents are ion transport inhibitors that decrease the reabsorption of Na+ at
Diuretics (Saluretics) Diuretics increase urine excretion mainly by reabsorption of salts and water from kidney tubules These agents are ion transport inhibitors that decrease the reabsorption of Na+ at
ISPUB.COM. Management of Ascites. V Mahesh SOURCE OF SUPPORT DIAGNOSIS OF ASCITES INTRODUCTION CAUSES [,] DIAGNOSTIC TESTS
![ISPUB.COM. Management of Ascites. V Mahesh SOURCE OF SUPPORT DIAGNOSIS OF ASCITES INTRODUCTION CAUSES [,] DIAGNOSTIC TESTS](/thumbs/84/91182326.jpg "ISPUB.COM. Management of Ascites. V Mahesh SOURCE OF SUPPORT DIAGNOSIS OF ASCITES INTRODUCTION CAUSES [,] DIAGNOSTIC TESTS") ISPUB.COM The Internet Journal of Gastroenterology Volume 5 Number 2 Management of Ascites V Mahesh Citation V Mahesh. Management of Ascites. The Internet Journal of Gastroenterology. 2006 Volume 5 Number
ISPUB.COM The Internet Journal of Gastroenterology Volume 5 Number 2 Management of Ascites V Mahesh Citation V Mahesh. Management of Ascites. The Internet Journal of Gastroenterology. 2006 Volume 5 Number
Conflict of interest disclosures. Complications of end stage liver disease. None. The many complications of Cirrhosis. Portal Hypertension.
 Complications of end stage liver disease Conflict of interest disclosures None Amir Qamar, MD Instructor of Medicine Brigham and Women s s Hospital Harvard Medical School Boston, MA 02115 The many complications
Complications of end stage liver disease Conflict of interest disclosures None Amir Qamar, MD Instructor of Medicine Brigham and Women s s Hospital Harvard Medical School Boston, MA 02115 The many complications
Treatment and management of ascites and hepatorenal syndrome: an update
 564673TAG0010.1177/1756283X14564673Therapeutic Advances in GastroenterologyK. Lenz et al. review-article2014 Therapeutic Advances in Gastroenterology Review Treatment and management of ascites and hepatorenal
564673TAG0010.1177/1756283X14564673Therapeutic Advances in GastroenterologyK. Lenz et al. review-article2014 Therapeutic Advances in Gastroenterology Review Treatment and management of ascites and hepatorenal
بسم هللا الرحمن الرحيم ** Note: the curve discussed in this page [TF]/[P] curve is found in the slides, so please refer to them.**
![بسم هللا الرحمن الرحيم ** Note: the curve discussed in this page [TF]/[P] curve is found in the slides, so please refer to them.**](/thumbs/87/96174275.jpg "بسم هللا الرحمن الرحيم ** Note: the curve discussed in this page [TF]/[P] curve is found in the slides, so please refer to them.**") بسم هللا الرحمن الرحيم ** Note: the curve discussed in this page [TF]/[P] curve is found in the slides, so please refer to them.** INULIN characteristics : 1 filtered 100 %. 2-Not secreted. 3-Not reabsorbed
بسم هللا الرحمن الرحيم ** Note: the curve discussed in this page [TF]/[P] curve is found in the slides, so please refer to them.** INULIN characteristics : 1 filtered 100 %. 2-Not secreted. 3-Not reabsorbed
V2 Receptor Antagonist; Tolvaptan
 Review ISSN 1738-5997 (Print) ISSN 2092-9935 (Online) Electrolyte Blood Press 9:50-54, 2011 http://dx.doi.org/10.5049/ebp.2011.9.2.50 V2 Receptor Antagonist; Tolvaptan Joo-Hark Yi, M.D. Hyun-Jong Shin,
Review ISSN 1738-5997 (Print) ISSN 2092-9935 (Online) Electrolyte Blood Press 9:50-54, 2011 http://dx.doi.org/10.5049/ebp.2011.9.2.50 V2 Receptor Antagonist; Tolvaptan Joo-Hark Yi, M.D. Hyun-Jong Shin,
BIPN100 F15 Human Physiology (Kristan) Problem Set #8 Solutions p. 1
 Problem Set #8 Solutions p. 1") BIPN100 F15 Human Physiology (Kristan) Problem Set #8 Solutions p. 1 1. a. Proximal tubule. b. Proximal tubule. c. Glomerular endothelial fenestrae, filtration slits between podocytes of Bowman's capsule.
BIPN100 F15 Human Physiology (Kristan) Problem Set #8 Solutions p. 1 1. a. Proximal tubule. b. Proximal tubule. c. Glomerular endothelial fenestrae, filtration slits between podocytes of Bowman's capsule.
Medical Management of Acutely Decompensated Heart Failure. William T. Abraham, MD Director, Division of Cardiovascular Medicine
 Medical Management of Acutely Decompensated Heart Failure William T. Abraham, MD Director, Division of Cardiovascular Medicine Orlando, Florida October 7-9, 2011 Goals of Acute Heart Failure Therapy Alleviate
Medical Management of Acutely Decompensated Heart Failure William T. Abraham, MD Director, Division of Cardiovascular Medicine Orlando, Florida October 7-9, 2011 Goals of Acute Heart Failure Therapy Alleviate
TOLVAPTAN: A NEW APPROACH TO THE MANAGEMENT OF EU- VOLEMIC AND HYPERVOLEMIC HYPONATREMIA
 Volume 22, Issue 10 July 2007 TOLVAPTAN: A NEW APPROACH TO THE MANAGEMENT OF EU- VOLEMIC AND HYPERVOLEMIC HYPONATREMIA Olamide Oshikoya, Pharm. D Candidate Hyponatremia is the most common electrolyte disorder
Volume 22, Issue 10 July 2007 TOLVAPTAN: A NEW APPROACH TO THE MANAGEMENT OF EU- VOLEMIC AND HYPERVOLEMIC HYPONATREMIA Olamide Oshikoya, Pharm. D Candidate Hyponatremia is the most common electrolyte disorder
Hormonal Control of Osmoregulatory Functions *
 OpenStax-CNX module: m44828 1 Hormonal Control of Osmoregulatory Functions * OpenStax This work is produced by OpenStax-CNX and licensed under the Creative Commons Attribution License 3.0 By the end of
OpenStax-CNX module: m44828 1 Hormonal Control of Osmoregulatory Functions * OpenStax This work is produced by OpenStax-CNX and licensed under the Creative Commons Attribution License 3.0 By the end of
Renal effects of treatment with diuretics, octreotide or both, in non-azotemic cirrhotic patients with ascites
 Nephrol Dial Transplant (2005) 20: 1623 1629 doi:10.1093/ndt/gfh871 Advance Access publication 10 May 2005 Original Article Renal effects of treatment with diuretics, octreotide or both, in non-azotemic
Nephrol Dial Transplant (2005) 20: 1623 1629 doi:10.1093/ndt/gfh871 Advance Access publication 10 May 2005 Original Article Renal effects of treatment with diuretics, octreotide or both, in non-azotemic
Diuretics having the quality of exciting excessive excretion of urine. OED. Inhibitors of Sodium Reabsorption Saluretics not Aquaretics
 Diuretics having the quality of exciting excessive excretion of urine. OED Inhibitors of Sodium Reabsorption Saluretics not Aquaretics 1 Sodium Absorption Na Entry into the Cell down an electrochemical
Diuretics having the quality of exciting excessive excretion of urine. OED Inhibitors of Sodium Reabsorption Saluretics not Aquaretics 1 Sodium Absorption Na Entry into the Cell down an electrochemical
Management of refractory ascites in cirrhosis: Are we out of date?
 Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.4254/wjh.v8.i28.1182 World J Hepatol 2016 October 8; 8(28): 1182-1193 ISSN 1948-5182 (online)
Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.4254/wjh.v8.i28.1182 World J Hepatol 2016 October 8; 8(28): 1182-1193 ISSN 1948-5182 (online)
Potassium regulation. -Kidney is a major regulator for potassium Homeostasis.
 Potassium regulation. -Kidney is a major regulator for potassium Homeostasis. Normal potassium intake, distribution, and output from the body. Effects of severe hyperkalemia Partial depolarization of cell
Potassium regulation. -Kidney is a major regulator for potassium Homeostasis. Normal potassium intake, distribution, and output from the body. Effects of severe hyperkalemia Partial depolarization of cell
Wales Critical Care & Trauma Network (North) Management of Hyponatraemia in Intensive Care Guidelines
 Management of Hyponatraemia in Intensive Care Guidelines") Wales Critical Care & Trauma Network (North) Management of Hyponatraemia in Intensive Care Guidelines Author: Richard Pugh June 2015 Guideline for management of hyponatraemia in intensive care Background
Wales Critical Care & Trauma Network (North) Management of Hyponatraemia in Intensive Care Guidelines Author: Richard Pugh June 2015 Guideline for management of hyponatraemia in intensive care Background
The renal resistive index is a non-invasive indicator of hepatorenal syndrome in cirrhotics
 Journal of Advanced Clinical & Research Insights (2016), 3, 23 27 ORIGINAL ARTICLE The renal resistive index is a non-invasive indicator of hepatorenal syndrome in cirrhotics Mohsin Aslam, S. Ananth Ram,
Journal of Advanced Clinical & Research Insights (2016), 3, 23 27 ORIGINAL ARTICLE The renal resistive index is a non-invasive indicator of hepatorenal syndrome in cirrhotics Mohsin Aslam, S. Ananth Ram,
Hyponatremia 11/4/2010. Learning Objectives
 JAMES S. KALUS, PHARM.D, BCPS (AQ-CARDIOLOGY) Senior Manager, Patient Care Services, Department of Pharmacy Services Henry Ford Hospital, Detroit, MI NO RELATIONSHIPS TO DISCLOSE ANGELA STEWART, PHARM.D,
JAMES S. KALUS, PHARM.D, BCPS (AQ-CARDIOLOGY) Senior Manager, Patient Care Services, Department of Pharmacy Services Henry Ford Hospital, Detroit, MI NO RELATIONSHIPS TO DISCLOSE ANGELA STEWART, PHARM.D,
Hepatorenal Syndrome
 Review Abdussalam Shredi MD, Sakolwan Suchartlikitwong MD, Hawa Edriss MD Abstract Hepatorenal syndrome is a form of acute kidney injury that occurs in chronic liver disease and acute fulminant liver failure.
Review Abdussalam Shredi MD, Sakolwan Suchartlikitwong MD, Hawa Edriss MD Abstract Hepatorenal syndrome is a form of acute kidney injury that occurs in chronic liver disease and acute fulminant liver failure.
JUAN MIGUEL GIL R. ORTIZ, MD, FPCP, FPSN University of Santo Tomas Hospital
 JUAN MIGUEL GIL R. ORTIZ, MD, FPCP, FPSN University of Santo Tomas Hospital HYPONATREMIA Hb 88 Creatinine 7 Na 130 K 5.8 Nonhypotonic Hyponatremia 1. Pseudohyponatremia 2. Presence of non-na effective
JUAN MIGUEL GIL R. ORTIZ, MD, FPCP, FPSN University of Santo Tomas Hospital HYPONATREMIA Hb 88 Creatinine 7 Na 130 K 5.8 Nonhypotonic Hyponatremia 1. Pseudohyponatremia 2. Presence of non-na effective
Renal Pharmacology. Diuretics: Carbonic Anhydrase Inhibitors Thiazides Loop Diuretics Potassium-sparing Diuretics BIMM118
 Diuretics: Carbonic Anhydrase Inhibitors Thiazides Loop Diuretics Potassium-sparing Diuretics Renal Pharmacology Kidneys: Represent 0.5% of total body weight, but receive ~25% of the total arterial blood
Diuretics: Carbonic Anhydrase Inhibitors Thiazides Loop Diuretics Potassium-sparing Diuretics Renal Pharmacology Kidneys: Represent 0.5% of total body weight, but receive ~25% of the total arterial blood
BETA-BLOCKERS IN CIRRHOSIS.PRO.
 BETA-BLOCKERS IN CIRRHOSIS.PRO. Angela Puente Sánchez. MD PhD Hepatology Unit. Gastroenterology department Marques de Valdecilla University Hospital. Santander INTRODUCTION. Natural history of cirrhosis
BETA-BLOCKERS IN CIRRHOSIS.PRO. Angela Puente Sánchez. MD PhD Hepatology Unit. Gastroenterology department Marques de Valdecilla University Hospital. Santander INTRODUCTION. Natural history of cirrhosis
Portal hypertension is the main complication of cirrhosis
 GASTROENTEROLOGY 2001;120:726 748 Current Management of the Complications of Cirrhosis and Portal Hypertension: Variceal Hemorrhage, Ascites, and Spontaneous Bacterial Peritonitis GUADALUPE GARCIA TSAO
GASTROENTEROLOGY 2001;120:726 748 Current Management of the Complications of Cirrhosis and Portal Hypertension: Variceal Hemorrhage, Ascites, and Spontaneous Bacterial Peritonitis GUADALUPE GARCIA TSAO
PORTAL HYPERTENSION An Introduction to the Culprit of Many Liver Failure Complications
 PORTAL HYPERTENSION An Introduction to the Culprit of Many Liver Failure Complications Edy G. Trujillo, RN, MSN, ACNP-BC Liver Transplant RRUCLA Medical Center July 31, 2018 What Do We All Look Forward
PORTAL HYPERTENSION An Introduction to the Culprit of Many Liver Failure Complications Edy G. Trujillo, RN, MSN, ACNP-BC Liver Transplant RRUCLA Medical Center July 31, 2018 What Do We All Look Forward
Lithium-induced Tubular Dysfunction. Jun Ki Park 11/30/10
 Lithium-induced Tubular Dysfunction Jun Ki Park 11/30/10 Use of Lithium Mid 19 th century: treatment of gout Late 19 th century: used for psychiatric disorders Early 20 th century: sodium substitute to
Lithium-induced Tubular Dysfunction Jun Ki Park 11/30/10 Use of Lithium Mid 19 th century: treatment of gout Late 19 th century: used for psychiatric disorders Early 20 th century: sodium substitute to
LESSON ASSIGNMENT. Diuretic and Antidiuretic Agents. After you finish this lesson you should be able to:
 LESSON ASSIGNMENT SUBCOURSE MD0806 LESSON 8 Therapeutics III. Diuretic and Antidiuretic Agents. LESSON ASSIGNMENT Paragraphs 8-1--8-7. LESSON OBJECTIVES After you finish this lesson you should be able
LESSON ASSIGNMENT SUBCOURSE MD0806 LESSON 8 Therapeutics III. Diuretic and Antidiuretic Agents. LESSON ASSIGNMENT Paragraphs 8-1--8-7. LESSON OBJECTIVES After you finish this lesson you should be able