Hyponatraemia. Detlef Bockenhauer
|
|
|
- Cameron Hunter
- 6 years ago
- Views:
Transcription

1 Hyponatraemia Detlef Bockenhauer
2 Key message Plasma sodium can be low due to either excess water or deficiency of salt In clinical practice, dysnatraemias almost always reflect an abnormality of water
3 ?
4 Collecting duct cell: action of AVP Blood Lumen
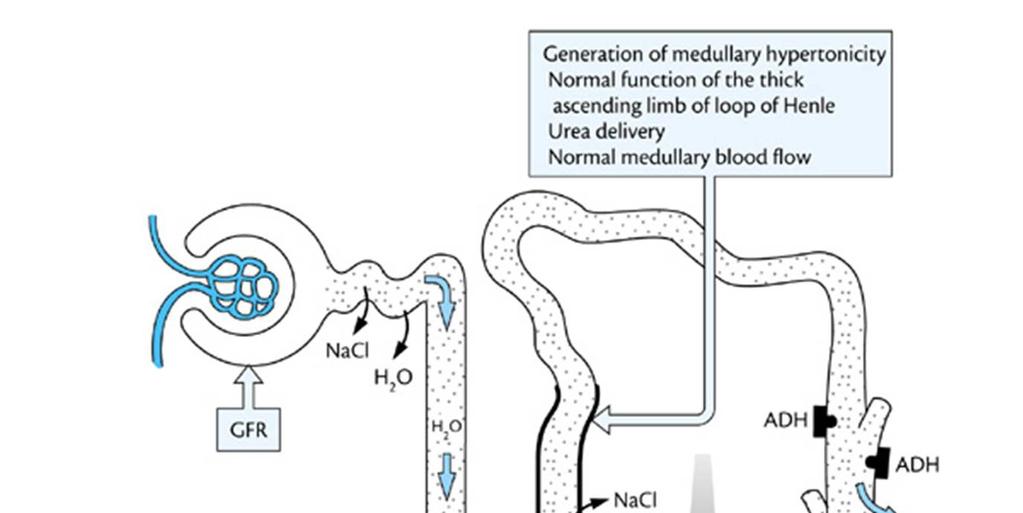
5 The role of the kidneys Appropriate water excretion Under control of ADH Dependent on osmotic load (consists of salt and protein intake) Usually mosm/kg => a 10-kg child with osmotic load of 200 mosm can adjust water excretion between 0.2 litres (Uosm 1000) and 4 litres (Uosm 50 mosm/kg)
6 Back to the hyponatraemic patient
7 Why is the sodium low? Too little salt Weight should be decreased Signs of dehydration/volume depletion Too much water Weight should be stable or increased Oedema forming states
8 Too much water Identify defect in water excretion Low GFR--neonates, renal insufficiency Enhanced proximal reabsorption--chf, Low albumin [Cirrhosis, Nephrosis, Enteropathy ] Defect in ascending limb function--diuretics, intrinsic lesions Inability to turn off ADH SIADH Insufficient osmotic load ( tea and toast )
9 Clinical euvolemic or edematous Increased body weight Too much water Serum Na U na high U osm < P osm U Na Low U osm > P osm U Na High U osm = P osm U Na High U osm > P osm Excessi water intake Heart failure Nephrosis Cirrhosis Enteropathy Low albumin Diuretics Intrinsic renal disease PKD SIADH
10 case 1 6-months old boy with astrocytoma Receives vincristine and carboplatin 10 days later presents for routine follow-up Examination: well perfused, wt: 4.7 kg (+0.2 kg), BP: 82 mmhg date Day 1 serum sodium 125 serum osmolality 255 urine sodium 32 urine osmolality 677
11 Diagnosis? Too much water? Too little salt? Too little salt? Too much water?
12 Clinical euvolemic or edematous Increased body weight Too much water Serum Na U na high U osm < P osm U Na Low U osm > P osm U Na High U osm = P osm U Na High U osm > P osm Excess water intake Heart failure Nephrosis Cirrhosis Enteropathy Low albumin Diuretics Intrinsic renal disease PKD SIADH
13 Further course date Day 4 Day 8 Day 11 Day14 weight BP in out serum sodium serum osmolality urine sodium urine osmolality sodium in (mmol/kg)
14 Key message Sodium is reabsorbed to preserve intravascular volume and in response to renal perfusion Kidney does not sense or detect serum sodium
15 Treatment Fluid restriction vaptans
16 Hyponatraemia-case 2 11-months old girl referred for assessment of hyponatraemia, first noted incidentally during investigations for viral illness and confirmed several times subsequently Examination: well perfused, BP: 90 mmhg biochemistries plasma urine unit Sodium mmol/l osmolality mosmol/kg Creatinine <1.0 mmol/l
17 Diagnosis? Too much water? Too little salt? Too little salt? Too much water?
18 Clinical euvolemic or edematous Increased body weight Too much water Serum Na U na high U osm < P osm U Na Low U osm > P osm U Na High U osm = P osm U Na High U osm > P osm Water overload Heart failure Nephrosis Cirrhosis Enteropathy Low albumin Diuretics Intrinsic renal disease PKD SIADH
19 Family History Mother and maternal grandmother were known to have had hyponatraemia. Maternal uncle has developmental delay and recurrent hyponatraemia (often with seizures) Mum and grandmother don t drink
20 Diagnosis? Nephrogenic Syndrome of inappropriate antidiuresis X-linked inherited Gain-of-function in AVPR2: R137C/L Females usually less affected

21 AJKD, 2012 Apr;59(4):566-8
22 Treatment Intuitive by patients!?increased osmotic load during infancy (urea)
23 Case 3 14-week old girl, presents with 5-week history of vomiting and unusual weight gain (1.1 kg over past 2 weeks) Examination: generalised pitting oedema, BP: 120 mmhg, weight 6 kg (75 th %ile) biochemistries plasma urine unit Sodium 99 <5 mmol/l osmolality mosmol/kg Creatinine mmol/l Albumin g/l
24 Diagnosis? Too much water? Too little salt? Too little salt? Too much water?
25 Clinical euvolemic or edematous Increased body weight Too much water Serum Na U na high U osm < P osm U Na Low U osm > P osm U Na High U osm = P osm U Na High U osm > P osm Water overload Heart failure Nephrosis Cirrhosis Enteropathy Low albumin Diuretics Intrinsic renal disease PKD SIADH
26 Treatment Underlying condition Diuretics NOT salt!!!
27 Case 4 5-months old baby presents with irritability. On examination, well perfused, systolic BP of 124 mmhg biochemistries plasma urine unit Sodium mmol/l osmolality mosmol/kg Creatinine mmol/l
28 Diagnosis? Too much water? Too little salt? Too little salt? Too much water?
29 Clinical euvolemic or edematous Increased body weight Too much water Serum Na U Na high U osm < P osm U Na Low U osm > P osm U Na High U osm = P osm U Na High U osm > P osm Water overload Heart failure Nephrosis Cirrhosis Enteropathy Low albumin Diuretics Intrinsic renal disease PKD SIADH
30 Collecting duct cell: action of AVP Blood Lumen vaptans
31 Further course date Day 1 Day 3 Day 5 Day 12 Tolvaptan [mg] vitapro serum sodium serum osmolality urine sodium urine osmolality
32 Excess water: Conclusions SIADH and cerebral salt wasting are biochemically indistinguishable Kidneys do not sense sodium concentration, just perfusion A Uosm=Posm in the face of hyponatraemia and water overload is inappropriate Treatment aimed at underlying defect and depends on chronicity Diluting capacity can be assessed with AVPR-blockers (vaptans)
33 Questions?
Disorders o f of water water Detlef Bockenhauer
 Disorders of water Detlef Bockenhauer How do we measure water? How do we measure water? Not directly! Reflected best in Na concentration Water overload => Hyponatraemia Water deficiency => Hypernatraemia
Disorders of water Detlef Bockenhauer How do we measure water? How do we measure water? Not directly! Reflected best in Na concentration Water overload => Hyponatraemia Water deficiency => Hypernatraemia
Southern Derbyshire Shared Care Pathology Guidelines. Hyponatraemia in Adults
 Southern Derbyshire Shared Care Pathology Guidelines Hyponatraemia in Adults Purpose of Guideline The investigation and management of adult patients with newly diagnosed hyponatraemia. Hyponatraemia can
Southern Derbyshire Shared Care Pathology Guidelines Hyponatraemia in Adults Purpose of Guideline The investigation and management of adult patients with newly diagnosed hyponatraemia. Hyponatraemia can
Guidelines for management of. Hyponatremia
 Guidelines for management of Hyponatremia Children s Kidney Centre University Hospital of Wales Cardiff CF14 4XW DISCLAIMER: These guidelines were produced in good faith by the authors reviewing available
Guidelines for management of Hyponatremia Children s Kidney Centre University Hospital of Wales Cardiff CF14 4XW DISCLAIMER: These guidelines were produced in good faith by the authors reviewing available
Over- and underfill: not all nephrotic states are equal. Detlef Bockenhauer
 Over- and underfill: not all nephrotic states are equal Detlef Bockenhauer Objectives Review pathophysiology of oedema: undervs overfill Treatment options The clinical setting: case 1 A6-y old girl with
Over- and underfill: not all nephrotic states are equal Detlef Bockenhauer Objectives Review pathophysiology of oedema: undervs overfill Treatment options The clinical setting: case 1 A6-y old girl with
Abnormalities in serum sodium. David Metz Paediatric Nephrology
 Abnormalities in serum sodium David Metz Paediatric Nephrology Basics Total body sodium regulated by aldosterone and ANP Mediated by intravascular volume (not sodium) RAAS and intrarenal determines Na
Abnormalities in serum sodium David Metz Paediatric Nephrology Basics Total body sodium regulated by aldosterone and ANP Mediated by intravascular volume (not sodium) RAAS and intrarenal determines Na
Wales Critical Care & Trauma Network (North) Management of Hyponatraemia in Intensive Care Guidelines
 Management of Hyponatraemia in Intensive Care Guidelines") Wales Critical Care & Trauma Network (North) Management of Hyponatraemia in Intensive Care Guidelines Author: Richard Pugh June 2015 Guideline for management of hyponatraemia in intensive care Background
Wales Critical Care & Trauma Network (North) Management of Hyponatraemia in Intensive Care Guidelines Author: Richard Pugh June 2015 Guideline for management of hyponatraemia in intensive care Background
Hyponatraemia: confident diagnosis, effective treatment and avoiding disasters. Dr James Ahlquist Endocrinologist Southend Hospital
 Hyponatraemia: confident diagnosis, effective treatment and avoiding disasters Dr James Ahlquist Endocrinologist Southend Hospital Hyponatraemia: a common electrolyte disorder Electrolyte disorder Prevalence
Hyponatraemia: confident diagnosis, effective treatment and avoiding disasters Dr James Ahlquist Endocrinologist Southend Hospital Hyponatraemia: a common electrolyte disorder Electrolyte disorder Prevalence
HYPONATRAEMIA: NUH GUIDELINE FOR INITIAL ASSESSMENT AND MANAGEMENT.
 HYPONATRAEMIA: NUH GUIDELINE FOR INITIAL ASSESSMENT AND MANAGEMENT. HYPONATRAEMIA: SODIUM < 130 MMOL/L SIGNIFICANT. Symptoms/signs usually only occur when sodium < 125 mmol/l. Acute hyponatraemia is less
HYPONATRAEMIA: NUH GUIDELINE FOR INITIAL ASSESSMENT AND MANAGEMENT. HYPONATRAEMIA: SODIUM < 130 MMOL/L SIGNIFICANT. Symptoms/signs usually only occur when sodium < 125 mmol/l. Acute hyponatraemia is less
Hyponatraemia- Principles, Investigation and Management. Sirazum Choudhury Biochemistry
 Hyponatraemia- Principles, Investigation and Management Sirazum Choudhury Biochemistry Contents Background Investigation Classification Normal Osmolality General management and SIADH Cases Background Relatively
Hyponatraemia- Principles, Investigation and Management Sirazum Choudhury Biochemistry Contents Background Investigation Classification Normal Osmolality General management and SIADH Cases Background Relatively
INTRAVENOUS FLUIDS PRINCIPLES
 INTRAVENOUS FLUIDS PRINCIPLES Postnatal physiological weight loss is approximately 5-10% Postnatal diuresis is delayed in Respiratory Distress Syndrome (RDS) Preterm babies have limited capacity to excrete
INTRAVENOUS FLUIDS PRINCIPLES Postnatal physiological weight loss is approximately 5-10% Postnatal diuresis is delayed in Respiratory Distress Syndrome (RDS) Preterm babies have limited capacity to excrete
Disorders of water and sodium homeostasis. Prof A. Pomeranz 2017
 Disorders of water and sodium homeostasis Prof A. Pomeranz 2017 Pediatric (Nephrology) Tool Box Disorders of water and sodium homeostasis Pediatric Nephrology Tool Box Hyponatremiaand and Hypernatremia
Disorders of water and sodium homeostasis Prof A. Pomeranz 2017 Pediatric (Nephrology) Tool Box Disorders of water and sodium homeostasis Pediatric Nephrology Tool Box Hyponatremiaand and Hypernatremia
Faculty version with model answers
 Faculty version with model answers Urinary Dilution & Concentration Bruce M. Koeppen, M.D., Ph.D. University of Connecticut Health Center 1. Increased urine output (polyuria) can result in a number of
Faculty version with model answers Urinary Dilution & Concentration Bruce M. Koeppen, M.D., Ph.D. University of Connecticut Health Center 1. Increased urine output (polyuria) can result in a number of
INTRAVENOUS FLUID THERAPY
 INTRAVENOUS FLUID THERAPY PRINCIPLES Postnatal physiological weight loss is approximately 5 10% in first week of life Preterm neonates have more total body water and may lose 10 15% of their weight in
INTRAVENOUS FLUID THERAPY PRINCIPLES Postnatal physiological weight loss is approximately 5 10% in first week of life Preterm neonates have more total body water and may lose 10 15% of their weight in
Cardiorenal and Renocardiac Syndrome
 And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
SODIUM BALANCE Overview
 SODIUM BALANCE Overview UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY PBL MBBS III Seminar VJ Temple 1 How are solute and solvent related to solution?
SODIUM BALANCE Overview UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY PBL MBBS III Seminar VJ Temple 1 How are solute and solvent related to solution?
Hyponatremia. Mis-named talk? Basic Pathophysiology
 Hyponatremia Great Lakes Hospital Medicine Symposium by Brian Wolfe, MD Assistant Professor of Internal Medicine University of Colorado Denver Mis-named talk? Why do we care about Hyponatremia? concentration
Hyponatremia Great Lakes Hospital Medicine Symposium by Brian Wolfe, MD Assistant Professor of Internal Medicine University of Colorado Denver Mis-named talk? Why do we care about Hyponatremia? concentration
Hyponatraemia. Dr Andy Lewington Consultant Nephrologist/Honorary Clinical Associate Professor Leeds Teaching Hospitals
 Hyponatraemia Dr Andy Lewington Consultant Nephrologist/Honorary Clinical Associate Professor Leeds Teaching Hospitals A.J.P.Lewington@leeds.ac.uk Disclosures of Interest Associate Clinical Director NIHR
Hyponatraemia Dr Andy Lewington Consultant Nephrologist/Honorary Clinical Associate Professor Leeds Teaching Hospitals A.J.P.Lewington@leeds.ac.uk Disclosures of Interest Associate Clinical Director NIHR
Case Report Tolvaptan in the Treatment of Acute Hyponatremia Associated with Acute Kidney Injury
 Case Reports in Nephrology Volume 2013, Article ID 801575, 4 pages http://dx.doi.org/10.1155/2013/801575 Case Report Tolvaptan in the Treatment of Acute Hyponatremia Associated with Acute Kidney Injury
Case Reports in Nephrology Volume 2013, Article ID 801575, 4 pages http://dx.doi.org/10.1155/2013/801575 Case Report Tolvaptan in the Treatment of Acute Hyponatremia Associated with Acute Kidney Injury
Hyponatremia and Hypokalemia
 Hyponatremia and Hypokalemia Critical Care in the ED March 21 st, 2019 Hannah Ferenchick, MD 1 No financial disclosures 2 1 Outline: 1. Hyponatremia Diagnosis Initial treatment 2. Hyperkalemia Diagnosis
Hyponatremia and Hypokalemia Critical Care in the ED March 21 st, 2019 Hannah Ferenchick, MD 1 No financial disclosures 2 1 Outline: 1. Hyponatremia Diagnosis Initial treatment 2. Hyperkalemia Diagnosis
Basic approach to: Hyponatremia Adley Wong, MHS PA-C
 2016 Topics in Acute and Ambulatory Care CAPA Conference 2018 for Advanced Practice Providers Basic approach to: Hyponatremia Adley Wong, MHS PA-C Goals Physiology of hyponatremia Why we care about hyponatremia
2016 Topics in Acute and Ambulatory Care CAPA Conference 2018 for Advanced Practice Providers Basic approach to: Hyponatremia Adley Wong, MHS PA-C Goals Physiology of hyponatremia Why we care about hyponatremia
NATURAL HISTORY AND SURVIVAL OF PATIENTS WITH ASCITES. PATIENTS WHO DO NOT DEVELOP COMPLICATIONS HAVE MARKEDLY BETTER SURVIVAL THAN THOSE WHO DEVELOP
 PROGNOSIS Mortality rates as high as 18-30% are reported for hyponatremic patients. High mortality rates reflect the severity of underlying conditions and are not influenced by treatment of hyponatremia
PROGNOSIS Mortality rates as high as 18-30% are reported for hyponatremic patients. High mortality rates reflect the severity of underlying conditions and are not influenced by treatment of hyponatremia
Hyponatræmia: analysis
 ESPEN Congress Nice 2010 Hyper- and hyponatraemia - serious and iatrogenic problems Hyponatræmia: analysis Mathias Plauth Hyponatremia Case Analysis Mathias Plauth Klinik für Innere Medizin Städtisches
ESPEN Congress Nice 2010 Hyper- and hyponatraemia - serious and iatrogenic problems Hyponatræmia: analysis Mathias Plauth Hyponatremia Case Analysis Mathias Plauth Klinik für Innere Medizin Städtisches
Distal and proximal RTA. Detlef Bockenhauer
 Distal and proximal RTA Detlef Bockenhauer acidosis: Is it real? H + + HCO 3 - > H2 O + CO 2 What do you need to assess an acid-base disorder Blood: blood gas, electrolytes including bicarbonate (measured)
Distal and proximal RTA Detlef Bockenhauer acidosis: Is it real? H + + HCO 3 - > H2 O + CO 2 What do you need to assess an acid-base disorder Blood: blood gas, electrolytes including bicarbonate (measured)
Objectives. Objectives
 Objectives Volume regulation entails the physiology of salt content regulation The edematous states reflect the pathophysiology of salt content regulation The mechanisms of normal volume regulation mediate
Objectives Volume regulation entails the physiology of salt content regulation The edematous states reflect the pathophysiology of salt content regulation The mechanisms of normal volume regulation mediate
Iposodiemia: diagnosi e trattamento
 Iposodiemia: diagnosi e trattamento Enrico Fiaccadori Unita di Fisiopatologia dell Insufficienza Renale Acuta e Cronica Dipartimento di Medicina Clinica e Sperimentale Universita degli Studi di Parma Hyponatremia
Iposodiemia: diagnosi e trattamento Enrico Fiaccadori Unita di Fisiopatologia dell Insufficienza Renale Acuta e Cronica Dipartimento di Medicina Clinica e Sperimentale Universita degli Studi di Parma Hyponatremia
DIURETICS-4 Dr. Shariq Syed
 DIURETICS-4 Dr. Shariq Syed AIKTC - Knowledge Resources & Relay Center 1 Pop Quiz!! Loop diuretics act on which transporter PKCC NKCC2 AIKTCC I Don t know AIKTC - Knowledge Resources & Relay Center 2 Pop
DIURETICS-4 Dr. Shariq Syed AIKTC - Knowledge Resources & Relay Center 1 Pop Quiz!! Loop diuretics act on which transporter PKCC NKCC2 AIKTCC I Don t know AIKTC - Knowledge Resources & Relay Center 2 Pop
Renal Quiz - June 22, 21001
 Renal Quiz - June 22, 21001 1. The molecular weight of calcium is 40 and chloride is 36. How many milligrams of CaCl 2 is required to give 2 meq of calcium? a) 40 b) 72 c) 112 d) 224 2. The extracellular
Renal Quiz - June 22, 21001 1. The molecular weight of calcium is 40 and chloride is 36. How many milligrams of CaCl 2 is required to give 2 meq of calcium? a) 40 b) 72 c) 112 d) 224 2. The extracellular
Two Little Water Cravers
 Two Little Water Cravers Baby Mo (5mths/M) Chief complaint Repeated vomiting since 2 months old with poor weight gain PMH Gestation 40+6wks, BW 3.375kg Hx of fracture Rt clavicle at birth HbH disease on
Two Little Water Cravers Baby Mo (5mths/M) Chief complaint Repeated vomiting since 2 months old with poor weight gain PMH Gestation 40+6wks, BW 3.375kg Hx of fracture Rt clavicle at birth HbH disease on
Dysnatremias: All About the Salt? Internal Medicine Resident Lecture 1/12/16 Steve Schinker, MD
 Dysnatremias: All About the Salt? Internal Medicine Resident Lecture 1/12/16 Steve Schinker, MD Water or salt? Dysnatremias In general, disorder of water balance, not sodium balance Volume status is tied
Dysnatremias: All About the Salt? Internal Medicine Resident Lecture 1/12/16 Steve Schinker, MD Water or salt? Dysnatremias In general, disorder of water balance, not sodium balance Volume status is tied
BIPN100 F15 Human Physiology (Kristan) Lecture 18: Endocrine control of renal function. p. 1
 Lecture 18: Endocrine control of renal function. p. 1") BIPN100 F15 Human Physiology (Kristan) Lecture 18: Endocrine control of renal function. p. 1 Terms you should understand by the end of this section: diuresis, antidiuresis, osmoreceptors, atrial stretch
BIPN100 F15 Human Physiology (Kristan) Lecture 18: Endocrine control of renal function. p. 1 Terms you should understand by the end of this section: diuresis, antidiuresis, osmoreceptors, atrial stretch
Hyponatremia Clinical Significance. Ágnes Haris MD PhD, St. Margit Hospital, Budapest
 Hyponatremia Clinical Significance Ágnes Haris MD PhD, St. Margit Hospital, Budapest 1 Case of hyponatremia 70 years old male Past medical history: DM, HTN Heavy smoker (20 packs/day) Recently: epigastrial
Hyponatremia Clinical Significance Ágnes Haris MD PhD, St. Margit Hospital, Budapest 1 Case of hyponatremia 70 years old male Past medical history: DM, HTN Heavy smoker (20 packs/day) Recently: epigastrial
Done By: Lulu Al-Obaid - Abdulrahman Al-Rashed Reviewed By: Mohammed Jameel Khulood Al-Raddadi
 Done By: Lulu Al-Obaid - Abdulrahman Al-Rashed Reviewed By: Mohammed Jameel Khulood Al-Raddadi At the end of this lecture student should be able to describe: The loop of Henle is referred to as countercurrent
Done By: Lulu Al-Obaid - Abdulrahman Al-Rashed Reviewed By: Mohammed Jameel Khulood Al-Raddadi At the end of this lecture student should be able to describe: The loop of Henle is referred to as countercurrent
BALANCE 13 DISORDERS OF WATER DISORDERS CHARACTERISED BY POLYDIPSIA AND POLYURIA. (vasopressin deficiency) 1 [primary] [secondary 6C] insipidus
![BALANCE 13 DISORDERS OF WATER DISORDERS CHARACTERISED BY POLYDIPSIA AND POLYURIA. (vasopressin deficiency) 1 [primary] [secondary 6C] insipidus](/thumbs/80/80940031.jpg "BALANCE 13 DISORDERS OF WATER DISORDERS CHARACTERISED BY POLYDIPSIA AND POLYURIA. (vasopressin deficiency) 1 [primary] [secondary 6C] insipidus") Wit JM, Ranke MB, Kelnar CJH (eds): ESPE classification of paediatric endocrine diagnosis. 13. Disorders of water balance. Horm Res 2007;68(suppl 2):96 97 ESPE Code Diagnosis OMIM ICD10 13 DISORDERS OF
Wit JM, Ranke MB, Kelnar CJH (eds): ESPE classification of paediatric endocrine diagnosis. 13. Disorders of water balance. Horm Res 2007;68(suppl 2):96 97 ESPE Code Diagnosis OMIM ICD10 13 DISORDERS OF
For more information about how to cite these materials visit
 Author(s): Michael Heung, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Michael Heung, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Renal-Related Questions
 Renal-Related Questions 1) List the major segments of the nephron and for each segment describe in a single sentence what happens to sodium there. (10 points). 2) a) Describe the handling by the nephron
Renal-Related Questions 1) List the major segments of the nephron and for each segment describe in a single sentence what happens to sodium there. (10 points). 2) a) Describe the handling by the nephron
Metabolism of water and electrolytes. 2. Special pathophysiology disturbances of intravascular volume and
 Metabolism of water and electrolytes 1. Physiology and general pathophysiology Compartments of body fluids Regulation of volume and tonicity (osmolality) Combinations of volume and osmolality disorders
Metabolism of water and electrolytes 1. Physiology and general pathophysiology Compartments of body fluids Regulation of volume and tonicity (osmolality) Combinations of volume and osmolality disorders
KD02 [Mar96] [Feb12] Which has the greatest renal clearance? A. PAH B. Glucose C. Urea D. Water E. Inulin
![KD02 [Mar96] [Feb12] Which has the greatest renal clearance? A. PAH B. Glucose C. Urea D. Water E. Inulin](/thumbs/87/96174332.jpg "KD02 [Mar96] [Feb12] Which has the greatest renal clearance? A. PAH B. Glucose C. Urea D. Water E. Inulin") Renal Physiology MCQ KD01 [Mar96] [Apr01] Renal blood flow is dependent on: A. Juxtaglomerular apparatus B. [Na+] at macula densa C. Afferent vasodilatation D. Arterial pressure (poorly worded/recalled
Renal Physiology MCQ KD01 [Mar96] [Apr01] Renal blood flow is dependent on: A. Juxtaglomerular apparatus B. [Na+] at macula densa C. Afferent vasodilatation D. Arterial pressure (poorly worded/recalled
HYPONATRAEMIA GUIDELINES
 HYPONATRAEMIA GUIDELINES Na + < 130 mmol/l For all patients: Acute = onset < 48 hours Chronic = onset > 48 hours or not known Follow acute hyponatraemia flow chart on page 2 Follow chronic hyponatraemia
HYPONATRAEMIA GUIDELINES Na + < 130 mmol/l For all patients: Acute = onset < 48 hours Chronic = onset > 48 hours or not known Follow acute hyponatraemia flow chart on page 2 Follow chronic hyponatraemia
DOWNLOAD OR READ : SYNDROME OF INAPPROPRIATE SECRETION OF ANTIDIURETIC HORMONE IN MALIGNANCY PDF EBOOK EPUB MOBI
 DOWNLOAD OR READ : SYNDROME OF INAPPROPRIATE SECRETION OF ANTIDIURETIC HORMONE IN MALIGNANCY PDF EBOOK EPUB MOBI Page 1 Page 2 syndrome of inappropriate secretion of antidiuretic hormone in malignancy
DOWNLOAD OR READ : SYNDROME OF INAPPROPRIATE SECRETION OF ANTIDIURETIC HORMONE IN MALIGNANCY PDF EBOOK EPUB MOBI Page 1 Page 2 syndrome of inappropriate secretion of antidiuretic hormone in malignancy
Comparison of tolvaptan treatment between patients with the SIADH and congestive heart failure: a single-center experience
 ORIGINAL ARTICLE Korean J Intern Med 2018;33:561-567 Comparison of tolvaptan treatment between patients with the SIADH and congestive heart failure: a single-center experience Gun Ha Park 1,2, Chang Min
ORIGINAL ARTICLE Korean J Intern Med 2018;33:561-567 Comparison of tolvaptan treatment between patients with the SIADH and congestive heart failure: a single-center experience Gun Ha Park 1,2, Chang Min
MS1 Physiology Review of Na+, K+, H + /HCO 3. /Acid-base, Ca+² and PO 4 physiology
 MS1 Physiology Review of,, / /Acidbase, Ca+² and PO 4 physiology I. David Weiner, M.D. Professor of Medicine and Physiology University of Florida College of Medicine Basic principles Proximal tubule Majority
MS1 Physiology Review of,, / /Acidbase, Ca+² and PO 4 physiology I. David Weiner, M.D. Professor of Medicine and Physiology University of Florida College of Medicine Basic principles Proximal tubule Majority
Kidney Physiology. Mechanisms of Urine Formation TUBULAR SECRETION Eunise A. Foster Shalonda Reed
 Kidney Physiology Mechanisms of Urine Formation TUBULAR SECRETION Eunise A. Foster Shalonda Reed The purpose of tubular secrection To dispose of certain substances that are bound to plasma proteins. To
Kidney Physiology Mechanisms of Urine Formation TUBULAR SECRETION Eunise A. Foster Shalonda Reed The purpose of tubular secrection To dispose of certain substances that are bound to plasma proteins. To
BCH 450 Biochemistry of Specialized Tissues
 BCH 450 Biochemistry of Specialized Tissues VII. Renal Structure, Function & Regulation Kidney Function 1. Regulate Extracellular fluid (ECF) (plasma and interstitial fluid) through formation of urine.
BCH 450 Biochemistry of Specialized Tissues VII. Renal Structure, Function & Regulation Kidney Function 1. Regulate Extracellular fluid (ECF) (plasma and interstitial fluid) through formation of urine.
RENAL SYSTEM 2 TRANSPORT PROPERTIES OF NEPHRON SEGMENTS Emma Jakoi, Ph.D.
 RENAL SYSTEM 2 TRANSPORT PROPERTIES OF NEPHRON SEGMENTS Emma Jakoi, Ph.D. Learning Objectives 1. Identify the region of the renal tubule in which reabsorption and secretion occur. 2. Describe the cellular
RENAL SYSTEM 2 TRANSPORT PROPERTIES OF NEPHRON SEGMENTS Emma Jakoi, Ph.D. Learning Objectives 1. Identify the region of the renal tubule in which reabsorption and secretion occur. 2. Describe the cellular
Renal Physiology II Tubular functions
 Renal Physiology II Tubular functions LO. 42, 43 Dr. Kékesi Gabriella Basic points of renal physiology 1. Glomerular filtration (GF) a) Ultrafiltration 2. Tubular functions active and passive a) Reabsorption
Renal Physiology II Tubular functions LO. 42, 43 Dr. Kékesi Gabriella Basic points of renal physiology 1. Glomerular filtration (GF) a) Ultrafiltration 2. Tubular functions active and passive a) Reabsorption
Diuretic Agents Part-2. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Diuretic Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Potassium-sparing diuretics The Ion transport pathways across the luminal and basolateral
Diuretic Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Potassium-sparing diuretics The Ion transport pathways across the luminal and basolateral
Overview. Fluid & Electrolyte Disorders. Water distribution. Introduction 5/10/2014
 Overview Fluid & Electrolyte Disorders Dr Nicola Barlow Clinical Biochemistry Department, City Hospital Introduction Fluid and electrolyte homeostasis Electrolyte disturbances Analytical parameters Methods
Overview Fluid & Electrolyte Disorders Dr Nicola Barlow Clinical Biochemistry Department, City Hospital Introduction Fluid and electrolyte homeostasis Electrolyte disturbances Analytical parameters Methods
Hyponatremia FOSPED 2018
 Hyponatremia FOSPED 2018 Prof. Dr. Mirjam Christ-Crain Department of Endocrinology, Diabetology and Metabolism University Hospital Basel Schweizerische Gesellschaft für Endokrinologie und Diabetologie
Hyponatremia FOSPED 2018 Prof. Dr. Mirjam Christ-Crain Department of Endocrinology, Diabetology and Metabolism University Hospital Basel Schweizerische Gesellschaft für Endokrinologie und Diabetologie
Public Assessment Report. Scientific discussion. Natriumklorid Abcur (sodium chloride) SE/H/1443/01/MR
 SE/H/1443/01/MR") Public Assessment Report Scientific discussion Natriumklorid Abcur (sodium chloride) SE/H/1443/01/MR This module reflects the scientific discussion for the approval of Natriumklorid Abcur. The procedure
Public Assessment Report Scientific discussion Natriumklorid Abcur (sodium chloride) SE/H/1443/01/MR This module reflects the scientific discussion for the approval of Natriumklorid Abcur. The procedure
Questions? Homework due in lab 6. PreLab #6 HW 15 & 16 (follow directions, 6 points!)
") Questions? Homework due in lab 6 PreLab #6 HW 15 & 16 (follow directions, 6 points!) Part 3 Variations in Urine Formation Composition varies Fluid volume Solute concentration Variations in Urine Formation
Questions? Homework due in lab 6 PreLab #6 HW 15 & 16 (follow directions, 6 points!) Part 3 Variations in Urine Formation Composition varies Fluid volume Solute concentration Variations in Urine Formation
Hyponatremia in Heart Failure: why it is important and what should we do about it?
 Objectives Hyponatremia in Heart Failure: why it is important and what should we do about it? Pathophysiology of sodium and water retention in heart failure Hyponatremia in heart failure (mechanism and
Objectives Hyponatremia in Heart Failure: why it is important and what should we do about it? Pathophysiology of sodium and water retention in heart failure Hyponatremia in heart failure (mechanism and
Renal Regulation of Sodium and Volume. Dr. Dave Johnson Associate Professor Dept. Physiology UNECOM
 Renal Regulation of Sodium and Volume Dr. Dave Johnson Associate Professor Dept. Physiology UNECOM Maintaining Volume Plasma water and sodium (Na + ) are regulated independently - you are already familiar
Renal Regulation of Sodium and Volume Dr. Dave Johnson Associate Professor Dept. Physiology UNECOM Maintaining Volume Plasma water and sodium (Na + ) are regulated independently - you are already familiar
Biochemistry case studies. Dr Narelle Hadlow Clinical Associate Professor School of Medicine, UWA
 Biochemistry case studies Dr Narelle Hadlow Clinical Associate Professor School of Medicine, UWA 72 y.o. woman History of HT, diuretics History of hypertension, complains thirsty, feels under the weather
Biochemistry case studies Dr Narelle Hadlow Clinical Associate Professor School of Medicine, UWA 72 y.o. woman History of HT, diuretics History of hypertension, complains thirsty, feels under the weather
The principal functions of the kidneys
 Renal physiology The principal functions of the kidneys Formation and excretion of urine Excretion of waste products, drugs, and toxins Regulation of body water and mineral content of the body Maintenance
Renal physiology The principal functions of the kidneys Formation and excretion of urine Excretion of waste products, drugs, and toxins Regulation of body water and mineral content of the body Maintenance
In nocturnal enuresis
 The role of the kidney In nocturnal enuresis Kostas Kamperis MD PhD Dept of Pediatrics, Section of Nephrology Aarhus University Hospital, Aarhus, Denmark Enuresis prototypes Nocturnal polyuria Bladder
The role of the kidney In nocturnal enuresis Kostas Kamperis MD PhD Dept of Pediatrics, Section of Nephrology Aarhus University Hospital, Aarhus, Denmark Enuresis prototypes Nocturnal polyuria Bladder
PARTS OF THE URINARY SYSTEM
 EXCRETORY SYSTEM Excretory System How does the excretory system maintain homeostasis? It regulates heat, water, salt, acid-base concentrations and metabolite concentrations 1 ORGANS OF EXCRETION Skin and
EXCRETORY SYSTEM Excretory System How does the excretory system maintain homeostasis? It regulates heat, water, salt, acid-base concentrations and metabolite concentrations 1 ORGANS OF EXCRETION Skin and
Potassium secretion. E k = -61 log ([k] inside / [k] outside).
![Potassium secretion. E k = -61 log ([k] inside / [k] outside).](/thumbs/80/80478709.jpg "Potassium secretion. E k = -61 log ([k] inside / [k] outside).") 1 Potassium secretion In this sheet, we will continue talking about ultrafiltration in kidney but with different substance which is K+. Here are some informations that you should know about potassium;
1 Potassium secretion In this sheet, we will continue talking about ultrafiltration in kidney but with different substance which is K+. Here are some informations that you should know about potassium;
A boy with water-like urine
 ANNUAL SCIENTIFIC MEETING 2018 HONG KONG PAEDIATRIC NEPHROLOGY SOCIETY A boy with water-like urine Dr Alvin Hui (Paediatrics, QEH) Dr MT Leung (Chemical Pathology, QEH) Case history M/37 days Full term
ANNUAL SCIENTIFIC MEETING 2018 HONG KONG PAEDIATRIC NEPHROLOGY SOCIETY A boy with water-like urine Dr Alvin Hui (Paediatrics, QEH) Dr MT Leung (Chemical Pathology, QEH) Case history M/37 days Full term
Dr. Carlos Fernando Estrada Garzona. Departamento de Farmacología Universidad de Costa Rica
 Dr. Carlos Fernando Estrada Garzona Departamento de Farmacología Universidad de Costa Rica OBJETIVOS FISIOLOGIA LIQUIDOS CORPORALES SOLUCIONES PARENTERALES PRINCIPIOS DE FLUIDOTERAPIA CRISTALOIDE VS COLOIDE
Dr. Carlos Fernando Estrada Garzona Departamento de Farmacología Universidad de Costa Rica OBJETIVOS FISIOLOGIA LIQUIDOS CORPORALES SOLUCIONES PARENTERALES PRINCIPIOS DE FLUIDOTERAPIA CRISTALOIDE VS COLOIDE
April 08, biology 2201 ch 11.3 excretion.notebook. Biology The Excretory System. Apr 13 9:14 PM EXCRETORY SYSTEM.
 Biology 2201 11.3 The Excretory System EXCRETORY SYSTEM 1 Excretory System How does the excretory system maintain homeostasis? It regulates heat, water, salt, acid base concentrations and metabolite concentrations
Biology 2201 11.3 The Excretory System EXCRETORY SYSTEM 1 Excretory System How does the excretory system maintain homeostasis? It regulates heat, water, salt, acid base concentrations and metabolite concentrations
Excretory System 1. a)label the parts indicated above and give one function for structures Y and Z
label the parts indicated above and give one function for structures Y and Z") Excretory System 1 1. Excretory System a)label the parts indicated above and give one function for structures Y and Z W- X- Y- Z- b) Which of the following is not a function of the organ shown? A. to produce
Excretory System 1 1. Excretory System a)label the parts indicated above and give one function for structures Y and Z W- X- Y- Z- b) Which of the following is not a function of the organ shown? A. to produce
Serum [ Serum Na] = 128 meq/l Question~ why Question~ wh edema?
![Serum [ Serum Na] = 128 meq/l Question~ why Question~ wh edema?](/thumbs/95/124873940.jpg "Serum [ Serum Na] = 128 meq/l Question~ why Question~ wh edema?") Objectives Case Summary Volume regulation entails the physiology of salt content regulation The edematous states reflect the pathophysiology of salt content regulation The mechanisms of normal volume regulation
Objectives Case Summary Volume regulation entails the physiology of salt content regulation The edematous states reflect the pathophysiology of salt content regulation The mechanisms of normal volume regulation
Module : Clinical correlates of disorders of metabolism Block 3, Week 2
 Module : Clinical correlates of disorders of metabolism Block 3, Week 2 Department of Paediatrics and Child Health University of Pretoria Tutor : Prof DF Wittenberg : dwittenb@medic.up.ac.za Aim of this
Module : Clinical correlates of disorders of metabolism Block 3, Week 2 Department of Paediatrics and Child Health University of Pretoria Tutor : Prof DF Wittenberg : dwittenb@medic.up.ac.za Aim of this
Treating the syndrome of inappropriate ADH secretion with isotonic saline
 Q J Med 1998; 91:749 753 Treating the syndrome of inappropriate ADH secretion with isotonic saline W. MUSCH and G. DECAUX1 From the Department of Internal Medicine, Bracops Hospital, Brussels, and 1Department
Q J Med 1998; 91:749 753 Treating the syndrome of inappropriate ADH secretion with isotonic saline W. MUSCH and G. DECAUX1 From the Department of Internal Medicine, Bracops Hospital, Brussels, and 1Department
Renal Functions: Renal Functions: Renal Function: Produce Urine
 Renal Functions: Excrete metabolic waste products Reabsorb vital nutrients Regulate osmolarity: Maintain ion balance Regulate extracellular fluid volume (and thus blood pressure) Renal Functions: Regulate
Renal Functions: Excrete metabolic waste products Reabsorb vital nutrients Regulate osmolarity: Maintain ion balance Regulate extracellular fluid volume (and thus blood pressure) Renal Functions: Regulate
Diuretics (Saluretics)
") Diuretics (Saluretics) Diuretics increase urine excretion mainly by reabsorption of salts and water from kidney tubules These agents are ion transport inhibitors that decrease the reabsorption of Na+ at
Diuretics (Saluretics) Diuretics increase urine excretion mainly by reabsorption of salts and water from kidney tubules These agents are ion transport inhibitors that decrease the reabsorption of Na+ at
JUAN MIGUEL GIL R. ORTIZ, MD, FPCP, FPSN University of Santo Tomas Hospital
 JUAN MIGUEL GIL R. ORTIZ, MD, FPCP, FPSN University of Santo Tomas Hospital HYPONATREMIA Hb 88 Creatinine 7 Na 130 K 5.8 Nonhypotonic Hyponatremia 1. Pseudohyponatremia 2. Presence of non-na effective
JUAN MIGUEL GIL R. ORTIZ, MD, FPCP, FPSN University of Santo Tomas Hospital HYPONATREMIA Hb 88 Creatinine 7 Na 130 K 5.8 Nonhypotonic Hyponatremia 1. Pseudohyponatremia 2. Presence of non-na effective
Excretory System. Biology 2201
 Excretory System Biology 2201 Excretory System How does the excretory system maintain homeostasis? It regulates: Body heat Water-salt concentrations Acid-base concentrations Metabolite concentrations ORGANS
Excretory System Biology 2201 Excretory System How does the excretory system maintain homeostasis? It regulates: Body heat Water-salt concentrations Acid-base concentrations Metabolite concentrations ORGANS
Excretory System. Excretory System
 Excretory System Biology 2201 Excretory System How does the excretory system maintain homeostasis? It regulates: Body heat Water-salt concentrations Acid-base concentrations Metabolite concentrations 1
Excretory System Biology 2201 Excretory System How does the excretory system maintain homeostasis? It regulates: Body heat Water-salt concentrations Acid-base concentrations Metabolite concentrations 1
Dr. Dafalla Ahmed Babiker Jazan University
 Dr. Dafalla Ahmed Babiker Jazan University objectives Overview Definition of dehydration Causes of dehydration Types of dehydration Diagnosis, signs and symptoms Management of dehydration Complications
Dr. Dafalla Ahmed Babiker Jazan University objectives Overview Definition of dehydration Causes of dehydration Types of dehydration Diagnosis, signs and symptoms Management of dehydration Complications
Acute Kidney Injury (AKI) Undergraduate nurse education
 Undergraduate nurse education") Acute Kidney Injury (AKI) Undergraduate nurse education Year One Developed Summer 2017 Overview Basic A & P of: Urinary system Kidneys Followed by: Introduction to Acute Kidney Injury Urinary System The
Acute Kidney Injury (AKI) Undergraduate nurse education Year One Developed Summer 2017 Overview Basic A & P of: Urinary system Kidneys Followed by: Introduction to Acute Kidney Injury Urinary System The
Hyponatremia as a Cardiovascular Biomarker
 Hyponatremia as a Cardiovascular Biomarker Uri Elkayam, MD Professor of Medicine University of Southern California Keck School of Medicine elkayam@usc.edu Disclosure Research grant from Otsuka for the
Hyponatremia as a Cardiovascular Biomarker Uri Elkayam, MD Professor of Medicine University of Southern California Keck School of Medicine elkayam@usc.edu Disclosure Research grant from Otsuka for the
Extracellular fluid (ECF) compartment volume control
 compartment volume control") Water Balance Made Easier Joon K. Choi, DO. Extracellular fluid (ECF) compartment volume control Humans regulate ECF volume mainly by regulating body sodium content. Several major systems work together
Water Balance Made Easier Joon K. Choi, DO. Extracellular fluid (ECF) compartment volume control Humans regulate ECF volume mainly by regulating body sodium content. Several major systems work together
1. a)label the parts indicated above and give one function for structures Y and Z
label the parts indicated above and give one function for structures Y and Z") Excretory System 1 1. Excretory System a)label the parts indicated above and give one function for structures Y and Z W- renal cortex - X- renal medulla Y- renal pelvis collecting center of urine and then
Excretory System 1 1. Excretory System a)label the parts indicated above and give one function for structures Y and Z W- renal cortex - X- renal medulla Y- renal pelvis collecting center of urine and then
From Sodium Retention to Therapy for Refractory Ascites The Role for New Drugs. Florence Wong University of Toronto. Falk Symposium October 14, 2007
 From Sodium Retention to Therapy for Refractory Ascites The Role for New Drugs Florence Wong University of Toronto Falk Symposium October 14, 2007 Sodium Retention in Cirrhosis Occurs as a result of hemodynamic
From Sodium Retention to Therapy for Refractory Ascites The Role for New Drugs Florence Wong University of Toronto Falk Symposium October 14, 2007 Sodium Retention in Cirrhosis Occurs as a result of hemodynamic
Hyponatremia and Hypomagnesemia
 Hyponatremia and Hypomagnesemia Dre Kathy Ferguson,nephrologist Hyponatremia Salt and water imbalance Management Acute vs chronic Approach! How to make the correct diagnosis?! How to treat safely? Etiology!
Hyponatremia and Hypomagnesemia Dre Kathy Ferguson,nephrologist Hyponatremia Salt and water imbalance Management Acute vs chronic Approach! How to make the correct diagnosis?! How to treat safely? Etiology!
Workshop on Hyponatremia
 Workshop on Hyponatremia Debbie Rosenbaum MDCM FRCPc University of British Columbia Rocky Mountain / ACP Internal Medicine Meeting November 13 2009 Objectives Approach to diagnosis of hyponatremia Acute
Workshop on Hyponatremia Debbie Rosenbaum MDCM FRCPc University of British Columbia Rocky Mountain / ACP Internal Medicine Meeting November 13 2009 Objectives Approach to diagnosis of hyponatremia Acute
Excretion Chapter 29. The Mammalian Excretory System consists of. The Kidney. The Nephron: the basic unit of the kidney.
 Excretion Chapter 29 The Mammalian Excretory System consists of The Kidney 1. Vertebrate kidneys perform A. Ion balance B. Osmotic balance C. Blood pressure D. ph balance E. Excretion F. Hormone production
Excretion Chapter 29 The Mammalian Excretory System consists of The Kidney 1. Vertebrate kidneys perform A. Ion balance B. Osmotic balance C. Blood pressure D. ph balance E. Excretion F. Hormone production
014 Chapter 14 Created: 9:25:14 PM CST
 014 Chapter 14 Created: 9:25:14 PM CST Student: 1. Functions of the kidneys include A. the regulation of body salt and water balance. B. hydrogen ion homeostasis. C. the regulation of blood glucose concentration.
014 Chapter 14 Created: 9:25:14 PM CST Student: 1. Functions of the kidneys include A. the regulation of body salt and water balance. B. hydrogen ion homeostasis. C. the regulation of blood glucose concentration.
Chapter 15 Diuretic Agents
 Chapter 15 Diuretic Agents Diuretics Diuretics are agents that increase the rate of urine formation and salt excretion. Diuresis = increased water formation, but the term is also used to indicate increased
Chapter 15 Diuretic Agents Diuretics Diuretics are agents that increase the rate of urine formation and salt excretion. Diuresis = increased water formation, but the term is also used to indicate increased
Chapter 21. Diuretic Agents. Mosby items and derived items 2008, 2002 by Mosby, Inc., an affiliate of Elsevier Inc.
 Chapter 21 Diuretic Agents Renal Structure and Function Kidneys at level of umbilicus Each weighs 160 to 175 g and is 10 to 12 cm long Most blood flow per gram of weight in body 22% of cardiac output (CO)
Chapter 21 Diuretic Agents Renal Structure and Function Kidneys at level of umbilicus Each weighs 160 to 175 g and is 10 to 12 cm long Most blood flow per gram of weight in body 22% of cardiac output (CO)
بسم هللا الرحمن الرحيم ** Note: the curve discussed in this page [TF]/[P] curve is found in the slides, so please refer to them.**
![بسم هللا الرحمن الرحيم ** Note: the curve discussed in this page [TF]/[P] curve is found in the slides, so please refer to them.**](/thumbs/87/96174275.jpg "بسم هللا الرحمن الرحيم ** Note: the curve discussed in this page [TF]/[P] curve is found in the slides, so please refer to them.**") بسم هللا الرحمن الرحيم ** Note: the curve discussed in this page [TF]/[P] curve is found in the slides, so please refer to them.** INULIN characteristics : 1 filtered 100 %. 2-Not secreted. 3-Not reabsorbed
بسم هللا الرحمن الرحيم ** Note: the curve discussed in this page [TF]/[P] curve is found in the slides, so please refer to them.** INULIN characteristics : 1 filtered 100 %. 2-Not secreted. 3-Not reabsorbed
IX: Electrolytes. Sodium disorders. Specific Learning Objectives: Dan Henry, MD Clerkship Director University of Connecticut School of Medicine
 IX: Electrolytes. Sodium disorders Dan Henry, MD Clerkship Director University of Connecticut School of Medicine Specific Learning Objectives: Knowledge Subinterns should be able to describe: a) The differentinal
IX: Electrolytes. Sodium disorders Dan Henry, MD Clerkship Director University of Connecticut School of Medicine Specific Learning Objectives: Knowledge Subinterns should be able to describe: a) The differentinal
Neuroendocrine challenges following hemispherectomy
 Neuroendocrine challenges following hemispherectomy Philip S. Zeitler MD. PhD Professor and Head Section of Endocrinology Children s Hospital Colorado University of Colorado Anschutz Medical Campus I am
Neuroendocrine challenges following hemispherectomy Philip S. Zeitler MD. PhD Professor and Head Section of Endocrinology Children s Hospital Colorado University of Colorado Anschutz Medical Campus I am
Answers and Explanations
 Answers and Explanations 1. The answer is D [V B 4 b]. Distal K + secretion is decreased by factors that decrease the driving force for passive diffusion of K + across the luminal membrane. Because spironolactone
Answers and Explanations 1. The answer is D [V B 4 b]. Distal K + secretion is decreased by factors that decrease the driving force for passive diffusion of K + across the luminal membrane. Because spironolactone
Composition of Body Fluids
 Water and electrolytes disturbances Fluid and Electrolyte Disturbances Hao, Chuan-Ming MD Huashan Hospital Sodium balance Hypovolemia Water balance Hyponatremia Hypernatremia Potassium balance Hypokelemia
Water and electrolytes disturbances Fluid and Electrolyte Disturbances Hao, Chuan-Ming MD Huashan Hospital Sodium balance Hypovolemia Water balance Hyponatremia Hypernatremia Potassium balance Hypokelemia
Treatment of infantile SIADH with a vasopressin-receptor antagonist: 2 cases
 Treatment of infantile SIADH with a vasopressin-receptor antagonist: 2 cases Running title: tolvaptan in infantile SIADH Authors: Daniela Marx-Berger 1, David V Milford 2, Meenakshi Bandhakavi 3, William
Treatment of infantile SIADH with a vasopressin-receptor antagonist: 2 cases Running title: tolvaptan in infantile SIADH Authors: Daniela Marx-Berger 1, David V Milford 2, Meenakshi Bandhakavi 3, William
1.&Glomerular/Pressure&Filtration&
 Urine&Formation& Overall&Process&! Urine gets rid of wastes (NH 3, urea, uric acid, creatinine) and other substances (vitamins, penicillin, histamines) found in excess in the blood!! blood is filtered
Urine&Formation& Overall&Process&! Urine gets rid of wastes (NH 3, urea, uric acid, creatinine) and other substances (vitamins, penicillin, histamines) found in excess in the blood!! blood is filtered
Na + Transport 1 and 2 Linda Costanzo, Ph.D.
 Na + Transport 1 and 2 Linda Costanzo, Ph.D. OBJECTIVES: After studying this lecture, the student should understand: 1. The terminology applied to single nephron function, including the meaning of TF/P
Na + Transport 1 and 2 Linda Costanzo, Ph.D. OBJECTIVES: After studying this lecture, the student should understand: 1. The terminology applied to single nephron function, including the meaning of TF/P
Introduction to the kidney: regulation of sodium & glucose. Dr Nick Ashton Senior Lecturer in Renal Physiology Faculty of Biology, Medicine & Health
 Introduction to the kidney: regulation of sodium & glucose Dr Nick Ashton Senior Lecturer in Renal Physiology Faculty of Biology, Medicine & Health Objectives Overview of kidney structure & function Glomerular
Introduction to the kidney: regulation of sodium & glucose Dr Nick Ashton Senior Lecturer in Renal Physiology Faculty of Biology, Medicine & Health Objectives Overview of kidney structure & function Glomerular
Renal Function and Associated Laboratory Tests
 Renal Function and Associated Laboratory Tests Contents Glomerular Filtration Rate (GFR)... 2 Cockroft-Gault Calculation of Creatinine Clearance... 3 Blood Urea Nitrogen (BUN) to Serum Creatinine (SCr)
Renal Function and Associated Laboratory Tests Contents Glomerular Filtration Rate (GFR)... 2 Cockroft-Gault Calculation of Creatinine Clearance... 3 Blood Urea Nitrogen (BUN) to Serum Creatinine (SCr)
SATURDAY PRESENTATIONS
 Carolinas Chapter - American Association of Clinical Endocrinologists SATURDAY PRESENTATIONS 2018 Annual Meeting September 7-9, 2018 Kiawah Island Golf Resort Kiawah Island, SC This continuing medical
Carolinas Chapter - American Association of Clinical Endocrinologists SATURDAY PRESENTATIONS 2018 Annual Meeting September 7-9, 2018 Kiawah Island Golf Resort Kiawah Island, SC This continuing medical
Carolinas Chapter - American Association of Clinical Endocrinologists SATURDAY HANDOUTS Annual Meeting
 Carolinas Chapter - American Association of Clinical Endocrinologists SATURDAY HANDOUTS 2018 Annual Meeting September 7-9, 2018 Kiawah Island Golf Resort Kiawah Island, SC This continuing medical education
Carolinas Chapter - American Association of Clinical Endocrinologists SATURDAY HANDOUTS 2018 Annual Meeting September 7-9, 2018 Kiawah Island Golf Resort Kiawah Island, SC This continuing medical education
Urine Formation. Urinary Physiology Urinary Section pages Urine Formation. Glomerular Filtration 4/24/2016
 Urine Formation Urinary Physiology Urinary Section pages 9-17 Filtrate Blood plasma minus most proteins Urine
Urine Formation Urinary Physiology Urinary Section pages 9-17 Filtrate Blood plasma minus most proteins Urine
Outline Urinary System. Urinary System and Excretion. Urine. Urinary System. I. Function II. Organs of the urinary system
 Outline Urinary System Urinary System and Excretion Bio105 Chapter 16 Renal will be on the Final only. I. Function II. Organs of the urinary system A. Kidneys 1. Function 2. Structure III. Disorders of
Outline Urinary System Urinary System and Excretion Bio105 Chapter 16 Renal will be on the Final only. I. Function II. Organs of the urinary system A. Kidneys 1. Function 2. Structure III. Disorders of
Regulation of Extracellular Fluid Osmolarity and Sodium Concentration
 C H A P T E R 2 8 Regulation of Extracellular Fluid Osmolarity and Sodium Concentration For the cells of the body to function properly, they must be bathed in extracellular fluid with a relatively constant
C H A P T E R 2 8 Regulation of Extracellular Fluid Osmolarity and Sodium Concentration For the cells of the body to function properly, they must be bathed in extracellular fluid with a relatively constant
mid ihsan (Physiology ) GFR is increased when A -Renal blood flow is increased B -Sym. Ganglion activity is reduced C-A and B **
 GFR is increased when A -Renal blood flow is increased B -Sym. Ganglion activity is reduced C-A and B **") (Physiology ) mid ihsan GFR is increased when A -Renal blood flow is increased B -Sym. Ganglion activity is reduced C-A and B ** Colloid pressure in the efferent arteriole is: A- More than that leaving
(Physiology ) mid ihsan GFR is increased when A -Renal blood flow is increased B -Sym. Ganglion activity is reduced C-A and B ** Colloid pressure in the efferent arteriole is: A- More than that leaving
NORMAL POTASSIUM DISTRIBUTION AND BALANCE
 NORMAL POTASSIUM DISTRIBUTION AND BALANCE 98% of body potassium is contained within cells, principally muscle cells, and is readily exchangeable. Only 2% is in ECF. Daily intake exceeds the amount in ECF.
NORMAL POTASSIUM DISTRIBUTION AND BALANCE 98% of body potassium is contained within cells, principally muscle cells, and is readily exchangeable. Only 2% is in ECF. Daily intake exceeds the amount in ECF.
Chapter 10: Urinary System & Excretion
 Chapter 10: Urinary System & Excretion Organs of Urinary System Kidneys (2) form urine Ureters (2) Carry urine from kidneys to bladder Bladder Stores urine Urethra Carries urine from bladder to outside
Chapter 10: Urinary System & Excretion Organs of Urinary System Kidneys (2) form urine Ureters (2) Carry urine from kidneys to bladder Bladder Stores urine Urethra Carries urine from bladder to outside
WATER, SODIUM AND POTASSIUM
 WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality