The Kidney in Liver Disease. Jeff Kaufhold MD FACP Jan 2018
|
|
|
- Jasper Cobb
- 5 years ago
- Views:
Transcription
1 The Kidney in Liver Disease Jeff Kaufhold MD FACP Jan 2018
2 Objectives 1. Understand new evidence in the pathophysiology of Hepatorenal syndrome 2. Review current treatment guidelines and some over the horizon treatments.
3 Outline Associations between kidney disease and liver disease Causes of Acute renal failure and liver disease Pathophysiology of Hepatorenal Syndrome Current Treatment Octreotide/Midodrine Therapy Terlipressin Therapy Head Out Water Immersion Extracorporeal Liver Dialysis References
4 Associations Kidney Disease PCKD IgA Nephropathy Membranoproliferative GN (MPGN) Membranous GN Liver Disease Liver Cysts and Fibrosis Cirrhosis Cirrhosis Hepatitis B
5 Associations Kidney Disease Membranoproliferative GN (MPGN) Membranous GN Cryoglobulinemia Liver Disease Cirrhosis Hep C Hepatitis B Hep C Hep C
6 Patients with Diabetic nephropathy also have higher incidence of presence of Hep C Associations
7 Abnormal Liver Physiology Fibrosis VEGF Accumulation of Nitrogenous Wastes Increased Portal Pressure - ascites and hypersplenism Telangiectasias and Varices Hepatic Encephalopathy Increased substrate for Nitric Oxide Synthase (Nos)

8 Esophageal Varices
9 Nitric Oxide Functions: Regulate BP potent vasodilator Neurotransmitter Suppress Pathogens Studies describe Pathophysiology in: Pregnancy/Pre-ecclampsia Hypertension Hepatic Failure
10 Endothelin Function: Most potent vasoconstrictor Studies describe broad range of Pathophysiologic conditions.
11 Why is this Important? Inhibitors and Antagonists being developed which you will use soon You already use some: Nitroprusside Isordil/NTG Viagra
12 Nitric Oxide - NO Uncharged molecule - can go anywhere Unpaired electron - highly reactive Chemical generation: Arginine + O2-----> NO + Citrulline NOS
13 Enzyme Production Nitric Oxide Synthase (NOS) Two Types Constitutive vasodilator neurotransmitter Inducible Free radical scavenger Pathogen killer

14 NITRIC OXIDE
15 Nitric Oxide Targets: Vascular Smooth Muscle Neurons Pathogenic bacteria Effects: Vasodilator Feedback for ET-1 Neurotransmitter Free Radical/Killer
16 NO in Pregnancy: Progesterone Stimulates Nitric Oxide Synthase Leads to systemic Vasodilation Which causes lower BP, Which stimulates Aldosterone Which leads to volume expansion Which increases GFR/RBF Decreased response to Angiotensin
17 NonVascular Functions of NO Modulates immune response reduces toxicity of oxygen radicals reduces adhesion of neutrophils, etc inhibits mast cell degranulation Pregnancy is an Immune Tolerant Condition
18 ENDOTHELIN Three Types Produced by endothelial cells, most renal cell types. Two receptor types, A and B
19 ENDOTHELIN (ET) Stimulators of ET production: Vasoconstrictors (adrenalin, vasopressin) Thrombin Hypoxia Low shear stress Cytokines
20 ENDOTHELIN Inhibitors of production Vasodilators (nitric oxide) Heparin High shear stress
21 ENDOTHELIN Feedback inhibition by Nitric Oxide, PGI-2 (prostacyclin) Also inhibited by activation of ET-B receptor on the endothelial cell
22 ENDOTHELIN
23 ENDOTHELIN Target Vascular Smooth M. Renal Tubules Mesangial cells Effect Vasoconstriction Sodium excretion Proliferation, accumulation of Matrix, and contraction.
24 ENDOTHELIN Clinical Aspects ET plays a role in ATN Contrast nephrotoxicity Cyclosporine nephrotoxicity Endotoxic shock Hypertension Chronic renal failure
25 Clinical Aspects of N.O. Cirrhosis decreased BP, low SVR, angiogenesis NOS inhibitors work, sort of. Pregnancy reduced response to angiotensin natural inhibitor found in pre-ecclampsia
26 Theories for Fluid retention in Liver Failure Overfill - measured circulating volume is UP due to problems with portal hypertension, but doesn t explain why there is too much aldosterone Underfill Leads to too much aldosterone, but doesn t correlate with measured volume There must be a better reason!
27 Pathophysiology
28 Theories for Fluid retention in Liver Failure The vasodilation caused by excess Nitrous Oxide leads to poor perfusion of tissues, leading to stimulation of aldosterone and ADH. This is the concept of Effective Circulating Volume (ECV) or Effective Arterial Blood Volume (EABV).
29 Hemodynamic Insults of Cirrhosis Increased nitrogenous wastes like ammonia, amino acids, lead to increased production of Nitric Oxide, which leads to: Vasodilation, Lower BP Stimulates Aldosterone and ADH production Edema accumulation Hyponatremia
30 Causes of ARF in Liver Disease Volume depleted due to Nausea Septic - ATN Interstitial Nephritis from antibiotics or other drugs Drug induced from NSAID or ACE use Hepatorenal Syndrome
31 Hepatorenal Syndrome Syndrome where Compensated Cirrhosis becomes decompensated Marked by Very Low BP, Increased ammonia with encephalopathy Usually pt is pancytopenic as portal pressures rise causing hypersplenism Acute Renal Failure
32 ARF in HRS Creatinine climbs over 2 Pt usually poorly responsive to diuretics Develops edema, ascites Low urine sodium (low FENA) Hyponatremia due to increased stimulus for ADH Hyperkalemia due to ARF and spironolactone use Should rule out adrenal insufficiency
33 What makes Cirrhotic patient Sepsis usually Decompensate? Endotoxin leads to stimulation of Inducible Nitric Oxide Synthase, and worsens vasodilation, low BP, decreases EABV further. GI Bleed Increases nitrogenous wastes/substrate for Nos.
34 Proofs of Concept Hepatorenal syndrome Can improve BP, Perfusion pressure, renal blood flow, Urine output with: Head Out Water Immersion (HOWI) Uniform compression of peripheral vasculature Agents which antagonize Nos LNAME, LNMMA other substituted Arginine substances. Midodrine and Octreotide

35

36
37 Treatment of HRS Head Out Water Immersion (HOWI) Good for outpts to prevent problems I tell my patients to go swim at the YMCA 2-3 times a week. Agents which antagonize Nos Not used due to increased risk of Variceal hemorrhage! Midodrine and Octreotide Used for inpts with HRS, diuretic resistance.
38 Treatment of HRS Midodrine: 5-10 mg up to TID Octreotide: 50 Microgram SQ or IV BID or TID. Max dose 1500 mcg/day. Side effects: diarrhea, N/V, syncope, bradycardia.
39 Hepatorenal Syndrome (HRS) First described in 1932 for post-op biliary tract Sx resulting in ATN Found to be a cascade of events Kidneys histologically normal Acute renal dysfunction occurs in 15% to 25% of hospitalized pts w/ cirrhosis HRS an extension of prerenal therefore potentially reversible Annual frequency of HRS 8% to 40% SBP or other infection 30% Severe alcoholic hepatitis 25%
40 Pathophysiology Splanchnic & Systemic Arterial Vasodilatation Hallmarks of progression of portal HTN in cirrhosis Mediated by numerous endogenous substances Early compensation includes increase in HR & CO Cardiac dysfunction HRS developed in cirrhotic pt w/ more severe arterial vasodilation and lower CO
41 Pathophysiology Renal Arterial Vasoconstriction Mediated by stimulation of SNS, activation of RAAS, nonosmotic release and activity of vasopressin(adh) Precise intrarenal mechanisms are speculative Balance between vasoconstrictive responses in kidney and splanchnic vasodilation is lost

42 Pathophysiology
43 Diagnosis International Ascites Club Consensus Workshop 2007
44 Diagnosis of HRS No prior evidence or history of renal impairment criteria include inc creat by 50% above baseline to level > 1.5 Subset of pt w/ cirrhosis and ESLD have profound decrease in muscle mass and urea synthesis Results in lower BUN and creat levels. Many medications may influence intravascular volume status and renal perfusion Diuretics, lactulose, ACE, ARBs, NSAIDs

45 Burr cells and target cells in liver disease
46 Classification Type 1 HRS: rapidly progressive form of renal dysfunction Serum creat doubles to > 2.5 w/in 2 weeks Rapid decline in hemodynamic parameters Bacterial infxn, GIB, Surgery, acute liver injury Type 2 HRS: more slowly progressing entity Severe ascites (diuretic resistant) Serum creat < 2.5 Type 3 HRS? Many pts w/ cirrhosis and portal hypertension also have underlying CKD
47 Prevention- Try to Avoid insults Intravascular volume depletion, Overdiuresis, diarrhea caused by lactulose, GIB (varices), large-volume paracentesis w/o colloid administration Nephrotoxins Infection Prophylactic administration of Abx to pts at high risk of SBP (Neomycin1 gm q6h)
48 Treatment IV Albumin: Bolus 1g/kg/d on presentation (max 100 g/d) Continue at g/d to keep Terlipressin: 1 mg IV Q4hr & up to 2 mg if baseline serum creat does not improve by 25% at day 3 (not available in US) Midodrine & Octreotide M: mg PO TID up to 15 mg TID O: 100 mcg SQ TID to 200 mcg TID or 25 mcg IV bolus + 25 mcg/hr Norepinephrine: mcg/kg/min and inc by 0.05 Q4hr Duration of vasopressor treatment is generally a max of 2 weeks until reversal of HRS or OTL
49 Treatment Transjugular Intrahepatic Portosystemic Shunt - TIPS Effective for treatment of diuretic-resistant ascites 4 pilot studies have evaluated the use of TIPS in nontransplant candidates with type 1 & 2 Limited by potential to accelerate liver dysfunction and worsen encephalopathy

50 TIPS
51 Treatment Liver Transplantation (OTL) ONLY therapy that has the potential to reverse Should be considered in any pt found to have HRS 35% of pts w/ HRS require long-term renal replacement 3 yr survival is approximately 60% Degree of renal dysfunction preoperatively may be independent predictors of survival Pts who responded to a vasopressin analog prior to OTL had outcomes similar to those of pts who had OTL w/o HRS
52 HRS Treatments under going study Pentoxifylline 400 mg TID with meals Trental Vaptans : Samsca mg daily, Tolvaptan = samsca Conivaptan - Vaprisol (IV version)
53 Liver Dialysis Hepatassist treatment Dialysis like treatment that clears plasma of nitrogenous wastes Actually more like a combo of plasmapheresis and hemodialysis

54 Whole blood frac5ons
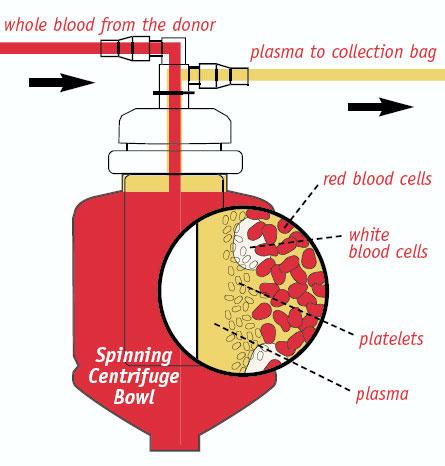
55 Plasmapheresis Centrifuge

56 Plasmapheresis Pa5ent

57 Hepatassist for liver failure Plasmapheresis Circuit for Regenera5on of Perfusate and Oxygena5on Hollow fiber kidney Porcine Hepatocytes
58 Prognosis Prior to advent of newer therapies median survival for pts w/ type 1 HRS was 1.7 weeks and 90% dead w/in 10 wks Today treatments have allowed some increase in short-term prognosis
59 References Sleisenger & Fordtran s Gastrointestinal and Liver Disease Pathphysiology/Diagnosis/Management. 9 th edition. Ch 92 P.A. McCormick. Management of hepatorenal syndrome. Pharm & Therap. 119 (2008) 1-6. T Restuccia. et al. Effects of treatment of hepatorenal syndrome before transplantation on post transplantation outcome. A case-control study. Journ of Hepat. 40 (2004) P Gines. Renal Failure in Cirrhosis. N Engl J Med. 2009;361:
The Kidney in Liver Disease. Jeff Kaufhold MD FACP Nephrology Assoc. of Dayton Oct 2018
 The Kidney in Liver Disease Jeff Kaufhold MD FACP Nephrology Assoc. of Dayton Oct 2018 Objectives 1. Understand new evidence in the pathophysiology of Hepatorenal syndrome 2. Review current treatment guidelines
The Kidney in Liver Disease Jeff Kaufhold MD FACP Nephrology Assoc. of Dayton Oct 2018 Objectives 1. Understand new evidence in the pathophysiology of Hepatorenal syndrome 2. Review current treatment guidelines
Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome
 Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome Disclosure I have no conflicts of interest to disclose Name: Margarita Taburyanskaya Title: PharmD, PGY1 Pharmacy Practice Resident
Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome Disclosure I have no conflicts of interest to disclose Name: Margarita Taburyanskaya Title: PharmD, PGY1 Pharmacy Practice Resident
Management of Cirrhotic Complications Uncontrolled Ascites. Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University
 Management of Cirrhotic Complications Uncontrolled Ascites Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University Topic Definition, pathogenesis Current therapeutic options Experimental treatments
Management of Cirrhotic Complications Uncontrolled Ascites Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University Topic Definition, pathogenesis Current therapeutic options Experimental treatments
Hepatorenal syndrome. Jan T. Kielstein Departent of Nephrology Medical School Hannover
 Hepatorenal syndrome Jan T. Kielstein Departent of Nephrology Medical School Hannover Hepatorenal Syndrome 1) History of HRS 2) Pathophysiology of HRS 3) Definition of HRS 4) Clinical presentation of HRS
Hepatorenal syndrome Jan T. Kielstein Departent of Nephrology Medical School Hannover Hepatorenal Syndrome 1) History of HRS 2) Pathophysiology of HRS 3) Definition of HRS 4) Clinical presentation of HRS
Initial approach to ascites
 Ascites: Filling and Draining the Water Balloon Common Pathogenesis in Refractory Ascites, Hyponatremia, and Cirrhosis intrahepatic resistance sinusoidal portal hypertension Splanchnic vasodilation (effective
Ascites: Filling and Draining the Water Balloon Common Pathogenesis in Refractory Ascites, Hyponatremia, and Cirrhosis intrahepatic resistance sinusoidal portal hypertension Splanchnic vasodilation (effective
Hepatorenal Syndrome
 Necker Seminars in Nephrology Institut Pasteur Paris, April 22, 2013 Hepatorenal Syndrome Dr. Richard Moreau 1 INSERM U773, Centre de Recherche Biomédicale Bichat-Beaujon CRB3, 2 Université Paris Diderot
Necker Seminars in Nephrology Institut Pasteur Paris, April 22, 2013 Hepatorenal Syndrome Dr. Richard Moreau 1 INSERM U773, Centre de Recherche Biomédicale Bichat-Beaujon CRB3, 2 Université Paris Diderot
Sign up to receive ATOTW weekly -
 HEPATORENAL SYNDROME ANAESTHESIA TUTORIAL OF THE WEEK 240 10 TH SEPTEMBER 2011 Gerry Lynch Rotherham General Hospital Correspondence to gerry.lynch@rothgen.nhs.uk QUESTIONS Before continuing, try to answer
HEPATORENAL SYNDROME ANAESTHESIA TUTORIAL OF THE WEEK 240 10 TH SEPTEMBER 2011 Gerry Lynch Rotherham General Hospital Correspondence to gerry.lynch@rothgen.nhs.uk QUESTIONS Before continuing, try to answer
Dialyzing challenging patients: Patients with hepato-renal conditions
 Dialyzing challenging patients: Patients with hepato-renal conditions Nidyanandh Vadivel MD Medical Director for Living kidney Donor and Pancreas Transplant Programs Swedish Organ Transplant, Seattle Acute
Dialyzing challenging patients: Patients with hepato-renal conditions Nidyanandh Vadivel MD Medical Director for Living kidney Donor and Pancreas Transplant Programs Swedish Organ Transplant, Seattle Acute
JOURNAL PRESENTATION. Dr Tina Fan Tseung Kwan O Hospital 17 th Jan 2013
 JOURNAL PRESENTATION Dr Tina Fan Tseung Kwan O Hospital 17 th Jan 2013 THE COMBINATION OF OCTREOTIDE AND MIDODRINE IS NOT SUPERIOR TO ALBUMIN IN PREVENTING RECURRENCE OF ASCITES AFTER LARGE-VOLUME PARACENTESIS
JOURNAL PRESENTATION Dr Tina Fan Tseung Kwan O Hospital 17 th Jan 2013 THE COMBINATION OF OCTREOTIDE AND MIDODRINE IS NOT SUPERIOR TO ALBUMIN IN PREVENTING RECURRENCE OF ASCITES AFTER LARGE-VOLUME PARACENTESIS
Management of Ascites and Hepatorenal Syndrome. Florence Wong University of Toronto. June 4, /16/ Gore & Associates: Consultancy
 Management of Ascites and Hepatorenal Syndrome Florence Wong University of Toronto June 4, 2016 6/16/2016 1 Disclosures Gore & Associates: Consultancy Sequana Medical: Research Funding Mallinckrodt Pharmaceutical:
Management of Ascites and Hepatorenal Syndrome Florence Wong University of Toronto June 4, 2016 6/16/2016 1 Disclosures Gore & Associates: Consultancy Sequana Medical: Research Funding Mallinckrodt Pharmaceutical:
The Management of Ascites & Hepatorenal Syndrome. Florence Wong University of Toronto. Falk Symposium March 14, 2008
 The Management of Ascites & Hepatorenal Syndrome Florence Wong University of Toronto Falk Symposium March 14, 2008 Management of Ascites Sodium Restriction Mandatory at all stages of ascites in order to
The Management of Ascites & Hepatorenal Syndrome Florence Wong University of Toronto Falk Symposium March 14, 2008 Management of Ascites Sodium Restriction Mandatory at all stages of ascites in order to
Hepatorenal syndrome. Jan Jan T. T. Kielstein Departent of of Nephrology Medical School School Hannover
 Hepatorenal syndrome Jan Jan T. T. Kielstein Departent of of Nephrology Medical School School Hannover Hepatorenal Syndrome 1) History of HRS 2) Pathophysiology of HRS 3) Definition of HRS 4) Clinical
Hepatorenal syndrome Jan Jan T. T. Kielstein Departent of of Nephrology Medical School School Hannover Hepatorenal Syndrome 1) History of HRS 2) Pathophysiology of HRS 3) Definition of HRS 4) Clinical
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Accelerated intravascular coagulation and fibrinolysis (AICF) in liver disease, 390 391 Acid suppression in liver disease, 403 404 ACLF.
Index Note: Page numbers of article titles are in boldface type. A Accelerated intravascular coagulation and fibrinolysis (AICF) in liver disease, 390 391 Acid suppression in liver disease, 403 404 ACLF.
Ascites Management. Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology
 Ascites Management Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Disclosure 1. The speaker Atif Zaman, MD MPH have no relevant
Ascites Management Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Disclosure 1. The speaker Atif Zaman, MD MPH have no relevant
Complications of Cirrhosis
 Complications of Cirrhosis Causes of Cirrhosis Alcohol Chronic Viral Hepatitis (B/C) Haemochromatosis Autoimmune Hepatitis NAFLD/NASH Primary Biliary Cirrhosis Primary Sclerosing Cholangitis 1-AT deficiency
Complications of Cirrhosis Causes of Cirrhosis Alcohol Chronic Viral Hepatitis (B/C) Haemochromatosis Autoimmune Hepatitis NAFLD/NASH Primary Biliary Cirrhosis Primary Sclerosing Cholangitis 1-AT deficiency
From Sodium Retention to Therapy for Refractory Ascites The Role for New Drugs. Florence Wong University of Toronto. Falk Symposium October 14, 2007
 From Sodium Retention to Therapy for Refractory Ascites The Role for New Drugs Florence Wong University of Toronto Falk Symposium October 14, 2007 Sodium Retention in Cirrhosis Occurs as a result of hemodynamic
From Sodium Retention to Therapy for Refractory Ascites The Role for New Drugs Florence Wong University of Toronto Falk Symposium October 14, 2007 Sodium Retention in Cirrhosis Occurs as a result of hemodynamic
CIRCULATORY AND RENAL FAILURE IN CIRRHOSIS
 CIRCULATORY AND RENAL FAILURE IN CIRRHOSIS Pere Ginès, MD Liver Unit, Hospital Clínic Barcelona, Catalunya, Spain CIRCULATORY AND RENAL FAILURE IN CIRRHOSIS Hecker R and Sherlock S, The Lancet 1956 RENAL
CIRCULATORY AND RENAL FAILURE IN CIRRHOSIS Pere Ginès, MD Liver Unit, Hospital Clínic Barcelona, Catalunya, Spain CIRCULATORY AND RENAL FAILURE IN CIRRHOSIS Hecker R and Sherlock S, The Lancet 1956 RENAL
Management of Cirrhosis Related Complications
 Management of Cirrhosis Related Complications Ke-Qin Hu, MD, FAASLD Professor of Clinical Medicine Director of Hepatology University of California, Irvine Disclosure I have no disclosure related to this
Management of Cirrhosis Related Complications Ke-Qin Hu, MD, FAASLD Professor of Clinical Medicine Director of Hepatology University of California, Irvine Disclosure I have no disclosure related to this
PORTAL HYPERTENSION An Introduction to the Culprit of Many Liver Failure Complications
 PORTAL HYPERTENSION An Introduction to the Culprit of Many Liver Failure Complications Edy G. Trujillo, RN, MSN, ACNP-BC Liver Transplant RRUCLA Medical Center July 31, 2018 What Do We All Look Forward
PORTAL HYPERTENSION An Introduction to the Culprit of Many Liver Failure Complications Edy G. Trujillo, RN, MSN, ACNP-BC Liver Transplant RRUCLA Medical Center July 31, 2018 What Do We All Look Forward
THE KIDNEY IN HYPOTENSIVE STATES. Benita S. Padilla, M.D.
 THE KIDNEY IN HYPOTENSIVE STATES Benita S. Padilla, M.D. Objectives To discuss what happens when the kidney encounters low perfusion To discuss new developments and clinical application points in two scenarios
THE KIDNEY IN HYPOTENSIVE STATES Benita S. Padilla, M.D. Objectives To discuss what happens when the kidney encounters low perfusion To discuss new developments and clinical application points in two scenarios
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI)
") Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
Treating patients with end-stage liver disease: Are we ready? Dr. Mino R. Mitri, M.D., C.M., M.Ed., FRCPC
 Treating patients with end-stage liver disease: Are we ready? Dr. Mino R. Mitri, M.D., C.M., M.Ed., FRCPC mino.mitri@ubc.ca No Conflict of Interest 157 patients 157 patients 6 transplanted Criteria Liver
Treating patients with end-stage liver disease: Are we ready? Dr. Mino R. Mitri, M.D., C.M., M.Ed., FRCPC mino.mitri@ubc.ca No Conflict of Interest 157 patients 157 patients 6 transplanted Criteria Liver
Therapy Insight: management of hepatorenal syndrome
 Therapy Insight: management of hepatorenal syndrome Andrés Cárdenas and Pere Ginès* SUMMARY Hepatorenal syndrome (HRS), a feared complication of advanced cirrhosis, is characterized by functional renal
Therapy Insight: management of hepatorenal syndrome Andrés Cárdenas and Pere Ginès* SUMMARY Hepatorenal syndrome (HRS), a feared complication of advanced cirrhosis, is characterized by functional renal
Elevated Creatinine in a Patient With Cirrhosis
 REVIEW Elevated Creatinine in a Patient With Cirrhosis Heather L. Klavan, M.D., and Brett E. Fortune, M.D., M.S. Elevation in serum creatinine is a common laboratory finding for patients with cirrhosis
REVIEW Elevated Creatinine in a Patient With Cirrhosis Heather L. Klavan, M.D., and Brett E. Fortune, M.D., M.S. Elevation in serum creatinine is a common laboratory finding for patients with cirrhosis
Cardiorenal and Renocardiac Syndrome
 And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
Hepatorenal Syndrome: Clinical Considerations
 426 Medicine Update 74 Hepatorenal Syndrome: Clinical Considerations VIVEK A SARASWAT, RAVI RATHI BACKGROUND The hepatorenal syndrome (HRS) is a life-threatening form of functional renal failure associated
426 Medicine Update 74 Hepatorenal Syndrome: Clinical Considerations VIVEK A SARASWAT, RAVI RATHI BACKGROUND The hepatorenal syndrome (HRS) is a life-threatening form of functional renal failure associated
Definition: fibrosis and nodular regeneration resulting from hepatocellular injury
 Cirrhosis Understanding the liver: Patterns of LFT Abnormalities - Hepatocellular/Transaminitis: o Ratio of AST: ALT >2:1 ETOH (keep in mind AST is also produced by red cells, heart muscle) o If Aminotransferases
Cirrhosis Understanding the liver: Patterns of LFT Abnormalities - Hepatocellular/Transaminitis: o Ratio of AST: ALT >2:1 ETOH (keep in mind AST is also produced by red cells, heart muscle) o If Aminotransferases
Management of the Cirrhotic Patient in the ICU
 Management of the Cirrhotic Patient in the ICU Peter E. Morris, MD Professor & Chief, Pulmonary, Critical Care and Sleep Medicine University of Kentucky Conflict of Interest Funding US National Institutes
Management of the Cirrhotic Patient in the ICU Peter E. Morris, MD Professor & Chief, Pulmonary, Critical Care and Sleep Medicine University of Kentucky Conflict of Interest Funding US National Institutes
Hepatorenal Syndrome 2018
 Hepatorenal Syndrome 2018 Warren Kupin, MD FACP Professor of Medicine Miami Transplant Institute Katz Family Division of Nephrology and Hypertension University of Miami Miller School of Medicine creat
Hepatorenal Syndrome 2018 Warren Kupin, MD FACP Professor of Medicine Miami Transplant Institute Katz Family Division of Nephrology and Hypertension University of Miami Miller School of Medicine creat
Acute Kidney Injury IM Resident Lecture. Yongen Chang, MD, PhD Nephrology July 2018
 Acute Kidney Injury IM Resident Lecture Yongen Chang, MD, PhD Nephrology July 2018 Objectives Epidemiology Definition and Staging Etiology and Diagnostic Approach Specific syndromes of AKI Treatment Biomarkers
Acute Kidney Injury IM Resident Lecture Yongen Chang, MD, PhD Nephrology July 2018 Objectives Epidemiology Definition and Staging Etiology and Diagnostic Approach Specific syndromes of AKI Treatment Biomarkers
The Cardiorenal Syndrome in Heart Failure
 The Cardiorenal Syndrome in Heart Failure Van N Selby, MD Assistant Professor of Medicine Advanced Heart Failure Program, UCSF October 9, 2015 Disclosures None 1 Cardiorenal Syndrome (CRS) A pathophysiologic
The Cardiorenal Syndrome in Heart Failure Van N Selby, MD Assistant Professor of Medicine Advanced Heart Failure Program, UCSF October 9, 2015 Disclosures None 1 Cardiorenal Syndrome (CRS) A pathophysiologic
Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals. By: Dr. Kevin Dolehide
 Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals By: Dr. Kevin Dolehide Overview DX Cirrhosis and Prognosis Compensated Decompensated Complications Of Cirrhosis Management Of Complications
Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals By: Dr. Kevin Dolehide Overview DX Cirrhosis and Prognosis Compensated Decompensated Complications Of Cirrhosis Management Of Complications
Beta-blockers in cirrhosis: Cons
 Beta-blockers in cirrhosis: Cons Eric Trépo MD, PhD Dept. of Gastroenterology. Hepatopancreatology and Digestive Oncology. C.U.B. Hôpital Erasme. Université Libre de Bruxelles. Bruxelles. Belgium Laboratory
Beta-blockers in cirrhosis: Cons Eric Trépo MD, PhD Dept. of Gastroenterology. Hepatopancreatology and Digestive Oncology. C.U.B. Hôpital Erasme. Université Libre de Bruxelles. Bruxelles. Belgium Laboratory
Liver-Kidney Crosstalk in Liver and Kidney Diseases
 Liver-Kidney Crosstalk in Liver and Kidney Diseases Sundararaman Swaminathan MD Associate Professor Division of Nephrology University of Virginia Health System Charlottesville, VA Hepatonephrologist busily
Liver-Kidney Crosstalk in Liver and Kidney Diseases Sundararaman Swaminathan MD Associate Professor Division of Nephrology University of Virginia Health System Charlottesville, VA Hepatonephrologist busily
REVIEW. Ariel W. Aday, M.D.,* Nicole E. Rich, M.D.,* Arjmand R. Mufti, M.D., and Shannan R. Tujios, M.D.
 REVIEW CON ( The Window Is Closed ): In Patients With Cirrhosis With Ascites, the Clinical Risks of Nonselective beta-blocker Outweigh the Benefits and Should NOT Be Prescribed Ariel W. Aday, M.D.,* Nicole
REVIEW CON ( The Window Is Closed ): In Patients With Cirrhosis With Ascites, the Clinical Risks of Nonselective beta-blocker Outweigh the Benefits and Should NOT Be Prescribed Ariel W. Aday, M.D.,* Nicole
The Yellow Patient. Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust
 The Yellow Patient Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust there s a yellow patient in bed 40. It s one of yours. Liver Cirrhosis Why.When.What.etc.
The Yellow Patient Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust there s a yellow patient in bed 40. It s one of yours. Liver Cirrhosis Why.When.What.etc.
The Use of Albumin for the Prevention of Hepatorenal Syndrome in Patients with Spontaneous Bacterial Peritonitis and Cirrhosis
 The Use of Albumin for the Prevention of Hepatorenal Syndrome in Patients with Spontaneous Bacterial Peritonitis and Cirrhosis http://www.funnyjunk.com/funny_pictures/1743659/enlarged/ Daniel Giddings,
The Use of Albumin for the Prevention of Hepatorenal Syndrome in Patients with Spontaneous Bacterial Peritonitis and Cirrhosis http://www.funnyjunk.com/funny_pictures/1743659/enlarged/ Daniel Giddings,
Prof. Mohammad Umar. MBBS, MCPS, FCPS, FACG (USA), FRCP (London), FRCP (Glasgow), FAGA
, FRCP (London), FRCP (Glasgow), FAGA") Prof. Mohammad Umar MBBS, MCPS, FCPS, FACG (USA), FRCP (London), FRCP (Glasgow), FAGA Chairman and Head Department of Medicine Rawalpindi Medical College, Rawalpindi. Consultant Gastroenterologist / Hepatologist
Prof. Mohammad Umar MBBS, MCPS, FCPS, FACG (USA), FRCP (London), FRCP (Glasgow), FAGA Chairman and Head Department of Medicine Rawalpindi Medical College, Rawalpindi. Consultant Gastroenterologist / Hepatologist
Hepatorenal syndrome
 Annals of Hepatology 2003; 2(1): January-March: 23-29 Concise Review Annals of Hepatology Hepatorenal syndrome Andrés Cárdenas, M.D., 1 Vicente Arroyo, M.D. 2 Abstract Hepatorenal syndrome is complication
Annals of Hepatology 2003; 2(1): January-March: 23-29 Concise Review Annals of Hepatology Hepatorenal syndrome Andrés Cárdenas, M.D., 1 Vicente Arroyo, M.D. 2 Abstract Hepatorenal syndrome is complication
Control of blood tissue blood flow. Faisal I. Mohammed, MD,PhD
 Control of blood tissue blood flow Faisal I. Mohammed, MD,PhD 1 Objectives List factors that affect tissue blood flow. Describe the vasodilator and oxygen demand theories. Point out the mechanisms of autoregulation.
Control of blood tissue blood flow Faisal I. Mohammed, MD,PhD 1 Objectives List factors that affect tissue blood flow. Describe the vasodilator and oxygen demand theories. Point out the mechanisms of autoregulation.
Chronic Hepatic Disease
 Chronic Hepatic Disease 10 th Leading Cause of Death Liver Functions Energy Metabolism Protein Synthesis Solubilization, Transport, and Storage Protects and Clears drugs, damaged cells Causes of Liver
Chronic Hepatic Disease 10 th Leading Cause of Death Liver Functions Energy Metabolism Protein Synthesis Solubilization, Transport, and Storage Protects and Clears drugs, damaged cells Causes of Liver
Etiology of liver cirrhosis
 Liver cirrhosis 1 Liver cirrhosis Liver cirrhosis is the progressive replacement of normal hepatic cells by fibrous scar tissue, This scarring is accompanied by the loss of viable hepatocytes, which are
Liver cirrhosis 1 Liver cirrhosis Liver cirrhosis is the progressive replacement of normal hepatic cells by fibrous scar tissue, This scarring is accompanied by the loss of viable hepatocytes, which are
RENAL DISEASE IN END STAGE LIVER DISEASE
 RENAL DISEASE IN END STAGE LIVER DISEASE Mitchell L Shiffman, MD Director Health System Richmond and Newport News, VA Medical Group Good Help to Those in Need Mitchell L Shiffman, MD POTENTIAL CONFLICTS
RENAL DISEASE IN END STAGE LIVER DISEASE Mitchell L Shiffman, MD Director Health System Richmond and Newport News, VA Medical Group Good Help to Those in Need Mitchell L Shiffman, MD POTENTIAL CONFLICTS
Review article: hepatorenal syndrome definitions and diagnosis
 Aliment Pharmacol Ther 2004; 20 (Suppl. 3): 24 28. Review article: hepatorenal syndrome definitions and diagnosis R. MOREAU & D. LEBREC Laboratoire d Hémodynamique Splanchnique et de Biologie Vasculaire,
Aliment Pharmacol Ther 2004; 20 (Suppl. 3): 24 28. Review article: hepatorenal syndrome definitions and diagnosis R. MOREAU & D. LEBREC Laboratoire d Hémodynamique Splanchnique et de Biologie Vasculaire,
Cardiorenal Syndrome
 SOCIEDAD ARGENTINA DE CARDIOLOGIA Cardiorenal Syndrome Joint session ESC-SAC ESC Congress 2012, Munich César A. Belziti Hospital Italiano de Buenos Aires I have no conflicts of interest to declare Cardiorenal
SOCIEDAD ARGENTINA DE CARDIOLOGIA Cardiorenal Syndrome Joint session ESC-SAC ESC Congress 2012, Munich César A. Belziti Hospital Italiano de Buenos Aires I have no conflicts of interest to declare Cardiorenal
Management of Acute Decompensation of Cirrhosis JOHN O GRADY KING S COLLEGE HOSPITAL
 Management of Acute Decompensation of Cirrhosis JOHN O GRADY KING S COLLEGE HOSPITAL Terminology Acute decompensation of cirrhosis - stable patient with sudden deterioration Acute-on-chronic liver failure
Management of Acute Decompensation of Cirrhosis JOHN O GRADY KING S COLLEGE HOSPITAL Terminology Acute decompensation of cirrhosis - stable patient with sudden deterioration Acute-on-chronic liver failure
Acute kidney injury in children with chronic liver disease
 Pediatric Nephrology https://doi.org/10.1007/s00467-018-3893-7 EDUCATIONAL REVIEW Acute kidney injury in children with chronic liver disease Akash Deep 1 & Romit Saxena 1 & Bipin Jose 1 Received: 10 July
Pediatric Nephrology https://doi.org/10.1007/s00467-018-3893-7 EDUCATIONAL REVIEW Acute kidney injury in children with chronic liver disease Akash Deep 1 & Romit Saxena 1 & Bipin Jose 1 Received: 10 July
APPROPRIATE PATIENT SELECTION AS A KEY TO INCREASE THE BENEFIT/RISK RATIO FOR ELAD
 APPROPRIATE PATIENT SELECTION AS A KEY TO INCREASE THE BENEFIT/RISK RATIO FOR ELAD Ram Subramanian M.D. Hepatology and Critical Care Emory University School of Medicine Atlanta, USA OUTLINE Review the
APPROPRIATE PATIENT SELECTION AS A KEY TO INCREASE THE BENEFIT/RISK RATIO FOR ELAD Ram Subramanian M.D. Hepatology and Critical Care Emory University School of Medicine Atlanta, USA OUTLINE Review the
Stages of Chronic Kidney Disease (CKD)
") Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
Recent Treatment of Pulmonary Artery Hypertension. Cardiology Division Yonsei University College of Medicine
 Recent Treatment of Pulmonary Artery Hypertension Cardiology Division Yonsei University College of Medicine Definition Raised Pulmonary arterial pressure (PAP) WHO criteria : spap>40 mmhg NIH Criteria
Recent Treatment of Pulmonary Artery Hypertension Cardiology Division Yonsei University College of Medicine Definition Raised Pulmonary arterial pressure (PAP) WHO criteria : spap>40 mmhg NIH Criteria
Hepatic Encephalopathy
 Hepatic Encephalopathy John Barber UMassMedical Student, Class of 2019 www.12daysinmarch.com Outline Overview Normal Physiology Pathology Symptoms Diagnosis Treatment Overview Ammonia (NH 3 ) is a byproduct
Hepatic Encephalopathy John Barber UMassMedical Student, Class of 2019 www.12daysinmarch.com Outline Overview Normal Physiology Pathology Symptoms Diagnosis Treatment Overview Ammonia (NH 3 ) is a byproduct
AKI in Hospitalized Patients ACOI 2017
 AKI in Hospitalized Patients ACOI 2017 Objectives 1. Define AKI KDIGO Classification 2. Incidence and consequences of AKI 3. Causes of AKI and workup 4. Prevention of AKI 5. Treatment of AKI AKI Case 67
AKI in Hospitalized Patients ACOI 2017 Objectives 1. Define AKI KDIGO Classification 2. Incidence and consequences of AKI 3. Causes of AKI and workup 4. Prevention of AKI 5. Treatment of AKI AKI Case 67
HYPERTENSION IN CKD. LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL
 HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
Denver Shunts vs TIPS for Ascites
 Denver Shunts vs TIPS for Ascites Hooman Yarmohammadi MD Assistant Professor of Radiology Interventional Radiology & Image Guided Therapies Memorial Sloan-Kettering Cancer Center, New York, USA Hooman
Denver Shunts vs TIPS for Ascites Hooman Yarmohammadi MD Assistant Professor of Radiology Interventional Radiology & Image Guided Therapies Memorial Sloan-Kettering Cancer Center, New York, USA Hooman
Decompensated chronic liver disease
 Decompensated chronic liver disease Definition of decompensated chronic liver disease Patients with chronic liver disease can present with acute decompensation due to various causes. The decompensation
Decompensated chronic liver disease Definition of decompensated chronic liver disease Patients with chronic liver disease can present with acute decompensation due to various causes. The decompensation
Vasoactive Medications. Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis
 Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
Filippo Schepis, MD Università degli Studi di Modena e Reggio Emilia
 Filippo Schepis, MD Università degli Studi di Modena e Reggio Emilia Il sottoscritto dichiara di non aver avuto/di aver avuto negli ultimi 12 mesi conflitto d interesse in relazione a questa presentazione
Filippo Schepis, MD Università degli Studi di Modena e Reggio Emilia Il sottoscritto dichiara di non aver avuto/di aver avuto negli ultimi 12 mesi conflitto d interesse in relazione a questa presentazione
Acute Kidney Injury. I. David Weiner, M.D. Division of Nephrology, Hypertension and Transplantation University of Florida and NF/SGVHS
 Acute Kidney Injury I. David Weiner, M.D. Division of Nephrology, Hypertension and Transplantation University of Florida and NF/SGVHS 374-6102 David.Weiner@medicine.ufl.edu www.renallectures.com Concentration
Acute Kidney Injury I. David Weiner, M.D. Division of Nephrology, Hypertension and Transplantation University of Florida and NF/SGVHS 374-6102 David.Weiner@medicine.ufl.edu www.renallectures.com Concentration
Ascites. Matthew Johnson M.D.
 Ascites Matthew Johnson M.D. The most common complication of portal hypertension 50% of patients who have compensated cirrhosis develop ascites by 10 years Survival after ascites develops: 1-year: 85%
Ascites Matthew Johnson M.D. The most common complication of portal hypertension 50% of patients who have compensated cirrhosis develop ascites by 10 years Survival after ascites develops: 1-year: 85%
CIRRHOSIS Definition
 Cirrhosis Update Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of Gastroenterology & Hepatology Weill Cornell Medical College CIRRHOSIS Definition Irreversible fibrous
Cirrhosis Update Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of Gastroenterology & Hepatology Weill Cornell Medical College CIRRHOSIS Definition Irreversible fibrous
LXIV: DRUGS: 4. RAS BLOCKADE
 LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
The Continuum of Care for Advanced Liver Disease: Partnering with the Liver Specialist. K V Speeg, MD, PhD UT Health San Antonio
 The Continuum of Care for Advanced Liver Disease: Partnering with the Liver Specialist K V Speeg, MD, PhD UT Health San Antonio Objectives Review staging of liver disease Review consequences of end-stage
The Continuum of Care for Advanced Liver Disease: Partnering with the Liver Specialist K V Speeg, MD, PhD UT Health San Antonio Objectives Review staging of liver disease Review consequences of end-stage
Control of blood tissue blood flow. Faisal I. Mohammed, MD,PhD
 Control of blood tissue blood flow Faisal I. Mohammed, MD,PhD 1 Objectives List factors that affect tissue blood flow. Describe the vasodilator and oxygen demand theories. Point out the mechanisms of autoregulation.
Control of blood tissue blood flow Faisal I. Mohammed, MD,PhD 1 Objectives List factors that affect tissue blood flow. Describe the vasodilator and oxygen demand theories. Point out the mechanisms of autoregulation.
Over- and underfill: not all nephrotic states are equal. Detlef Bockenhauer
 Over- and underfill: not all nephrotic states are equal Detlef Bockenhauer Objectives Review pathophysiology of oedema: undervs overfill Treatment options The clinical setting: case 1 A6-y old girl with
Over- and underfill: not all nephrotic states are equal Detlef Bockenhauer Objectives Review pathophysiology of oedema: undervs overfill Treatment options The clinical setting: case 1 A6-y old girl with
Pathophysiology, diagnosis and treatment of ascites in cirrhosis
 Annals of hepatology 2002; 1(2): April-June: 72-79 Concise Review Annals of hepatology Pathophysiology, diagnosis and treatment of ascites in cirrhosis Vicente Arroyo 1, M.D. Abstract The mechanism by
Annals of hepatology 2002; 1(2): April-June: 72-79 Concise Review Annals of hepatology Pathophysiology, diagnosis and treatment of ascites in cirrhosis Vicente Arroyo 1, M.D. Abstract The mechanism by
CIRRHOTIC MANAGEMENT
 DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
Liver failure &portal hypertension
 Liver failure &portal hypertension Objectives: by the end of this lecture each student should be able to : Diagnose liver failure (acute or chronic) List the causes of acute liver failure Diagnose and
Liver failure &portal hypertension Objectives: by the end of this lecture each student should be able to : Diagnose liver failure (acute or chronic) List the causes of acute liver failure Diagnose and
Conflict of interest disclosures. Complications of end stage liver disease. None. The many complications of Cirrhosis. Portal Hypertension.
 Complications of end stage liver disease Conflict of interest disclosures None Amir Qamar, MD Instructor of Medicine Brigham and Women s s Hospital Harvard Medical School Boston, MA 02115 The many complications
Complications of end stage liver disease Conflict of interest disclosures None Amir Qamar, MD Instructor of Medicine Brigham and Women s s Hospital Harvard Medical School Boston, MA 02115 The many complications
RISK STRATIFICATION IN CIRRHOSIS: FOCUS ON UMBILICAL HERNIA Sam Hawkins MD PGY5
 RISK STRATIFICATION IN CIRRHOSIS: FOCUS ON UMBILICAL HERNIA Sam Hawkins MD PGY5 PATIENT PRESENTATION 73M w/ Hep B Cirrhosis, HTN, DM II Liver disease followed at OSH x2 years (when moved from China), on
RISK STRATIFICATION IN CIRRHOSIS: FOCUS ON UMBILICAL HERNIA Sam Hawkins MD PGY5 PATIENT PRESENTATION 73M w/ Hep B Cirrhosis, HTN, DM II Liver disease followed at OSH x2 years (when moved from China), on
renoprotection therapy goals 208, 209
 Subject Index Aldosterone, plasminogen activator inhibitor-1 induction 163, 164, 168 Aminopeptidases angiotensin II processing 64 66, 214 diabetic expression 214, 215 Angiotensin I intrarenal compartmentalization
Subject Index Aldosterone, plasminogen activator inhibitor-1 induction 163, 164, 168 Aminopeptidases angiotensin II processing 64 66, 214 diabetic expression 214, 215 Angiotensin I intrarenal compartmentalization
End-Stage Liver Disease (ESLD): A Guide for HIV Physicians
: A Guide for HIV Physicians") Slide 1 of 32 End-Stage Liver Disease (ESLD): A Guide for HIV Physicians Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California
Slide 1 of 32 End-Stage Liver Disease (ESLD): A Guide for HIV Physicians Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California
Acute Liver Failure: Supporting Other Organs
 Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Acute Kidney Injury for the General Surgeon
 Acute Kidney Injury for the General Surgeon UCSF Postgraduate Course in General Surgery Maui, HI March 20, 2011 Epidemiology & Definition Pathophysiology Clinical Studies Management Summary Hobart W. Harris,
Acute Kidney Injury for the General Surgeon UCSF Postgraduate Course in General Surgery Maui, HI March 20, 2011 Epidemiology & Definition Pathophysiology Clinical Studies Management Summary Hobart W. Harris,
VARICEAL BLEEDING. Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta.
 VARICEAL BLEEDING Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta Disclosures: None OUTLINE Pathophysiology of portal hypertension Splanchnic
VARICEAL BLEEDING Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta Disclosures: None OUTLINE Pathophysiology of portal hypertension Splanchnic
Ascites and hepatorenal syndrome in cirrhosis: pathophysiological basis of therapy and current management
 Journal of Hepatology 38 (2003) S69 S89 www.elsevier.com/locate/jhep Ascites and hepatorenal syndrome in cirrhosis: pathophysiological basis of therapy and current management Vicente Arroyo*, Jordi Colmenero
Journal of Hepatology 38 (2003) S69 S89 www.elsevier.com/locate/jhep Ascites and hepatorenal syndrome in cirrhosis: pathophysiological basis of therapy and current management Vicente Arroyo*, Jordi Colmenero
Acute Kidney Injury (AKI)
") (Last Updated: 08/22/2018) Created by: Socco, Samantha Acute Kidney Injury (AKI) Thambi, M. (2017). Acute Kidney Injury. Lecture presented at PHAR 503 Lecture in UIC College of Pharmacy, Chicago. AKI This
(Last Updated: 08/22/2018) Created by: Socco, Samantha Acute Kidney Injury (AKI) Thambi, M. (2017). Acute Kidney Injury. Lecture presented at PHAR 503 Lecture in UIC College of Pharmacy, Chicago. AKI This
MANAGEMENT OF LIVER CIRRHOSIS: PRACTICE ESSENTIALS AND PATIENT SELF-MANAGEMENT
 MANAGEMENT OF LIVER CIRRHOSIS: PRACTICE ESSENTIALS AND PATIENT SELF-MANAGEMENT Sherona Bau, ACNP The Pfleger Liver Institute 200 UCLA Medical Plaza, Suite 214 Los Angeles, CA 90095 September 30, 2017 I
MANAGEMENT OF LIVER CIRRHOSIS: PRACTICE ESSENTIALS AND PATIENT SELF-MANAGEMENT Sherona Bau, ACNP The Pfleger Liver Institute 200 UCLA Medical Plaza, Suite 214 Los Angeles, CA 90095 September 30, 2017 I
Hepatorenal syndrome a defined entity with a standard treatment?
 Hepatorenal syndrome a defined entity with a standard treatment? Falk Symposium 162 Dresden - October 14, 2007 Alexander L. Gerbes Klinikum of the University of Munich Grosshadern Department of Medicine
Hepatorenal syndrome a defined entity with a standard treatment? Falk Symposium 162 Dresden - October 14, 2007 Alexander L. Gerbes Klinikum of the University of Munich Grosshadern Department of Medicine
Complications of Cirrhosis
 What is Cirrhosis? Complications of Cirrhosis Paul J. Gaglio, MD Center for Liver Disease and Transplantation Columbia University College of Physicians and Surgeons NAFLD 1 PHYSICAL EXAM FINDINGS Decreased
What is Cirrhosis? Complications of Cirrhosis Paul J. Gaglio, MD Center for Liver Disease and Transplantation Columbia University College of Physicians and Surgeons NAFLD 1 PHYSICAL EXAM FINDINGS Decreased
Doppler ultrasound, see Ultrasonography. Magnetic resonance imaging (MRI), kidney oxygenation assessment 75
, kidney oxygenation assessment 75") Subject Index Acidemia, cardiorenal syndrome type 3 146 Acute Dialysis Quality Initiative (ADQI) acute kidney injury biomarkers, see Acute kidney injury; specific biomarkers cardiorenal syndrome, see specific
Subject Index Acidemia, cardiorenal syndrome type 3 146 Acute Dialysis Quality Initiative (ADQI) acute kidney injury biomarkers, see Acute kidney injury; specific biomarkers cardiorenal syndrome, see specific
ESLD a Guide for HIV Physicians. Marion Peters University of California San Francisco June 2015
 ESLD a Guide for HIV Physicians Marion Peters University of California San Francisco June 2015 Disclosures Honararia from Johnson and Johnson Roche Merck Gilead Spouse employee of Hoffman La Roche Natural
ESLD a Guide for HIV Physicians Marion Peters University of California San Francisco June 2015 Disclosures Honararia from Johnson and Johnson Roche Merck Gilead Spouse employee of Hoffman La Roche Natural
Hepatology on the AMU
 Hepatology on the AMU RCP day, 8 th February 2018 Jo Leithead Consultant in Hepatology and Liver Transplantation Addenbrookes Hospital Cambridge Is liver disease relevant to me? Williams R, Lancet 2014
Hepatology on the AMU RCP day, 8 th February 2018 Jo Leithead Consultant in Hepatology and Liver Transplantation Addenbrookes Hospital Cambridge Is liver disease relevant to me? Williams R, Lancet 2014
CHAPTER 7. End Stage Liver Disease in the ICU: Walking a Tightrope. Lynn A. Kelso, MSN, APRN, FCCM, FAANP University of Kentucky College of Nursing
 CHAPTER 7 End Stage Liver Disease in the ICU: Walking a Tightrope Lynn A. Kelso, MSN, APRN, FCCM, FAANP University of Kentucky College of Nursing Besey Oren, Assistant Professor Istanbul University Health
CHAPTER 7 End Stage Liver Disease in the ICU: Walking a Tightrope Lynn A. Kelso, MSN, APRN, FCCM, FAANP University of Kentucky College of Nursing Besey Oren, Assistant Professor Istanbul University Health
Ibuprofen. Ibuprofen and Paracetamol: prescribing overview. Ibuprofen indications CYCLO-OXYGENASE (COX I) CYCLO-OXEGENASE (COX II) INFLAMMATORY PAIN
 CYCLO-OXEGENASE (COX II) INFLAMMATORY PAIN") Ibuprofen Ibuprofen and Paracetamol: prescribing overview Sarah Holloway Macmillan CNS in palliative care NSAID Non-selective COX inhibitor Oral bioavailability: 90% Onset of action: 20-30 mins (can take
Ibuprofen Ibuprofen and Paracetamol: prescribing overview Sarah Holloway Macmillan CNS in palliative care NSAID Non-selective COX inhibitor Oral bioavailability: 90% Onset of action: 20-30 mins (can take
COMPLICATIONS OF CIRRHOSIS: ASCITES & HEPATIC ENCEPHALOPATHY
 COMPLICATIONS OF CIRRHOSIS: ASCITES & HEPATIC ENCEPHALOPATHY DR. ESTER YAGUDAYEVA CLINICAL PHARMACIST HOSPICE PHARMACY SOLUTIONS OBJECTIVES Understand the prognosis of End Stage Liver Disease (ESLD) Identify
COMPLICATIONS OF CIRRHOSIS: ASCITES & HEPATIC ENCEPHALOPATHY DR. ESTER YAGUDAYEVA CLINICAL PHARMACIST HOSPICE PHARMACY SOLUTIONS OBJECTIVES Understand the prognosis of End Stage Liver Disease (ESLD) Identify
Heart Failure. Subjective SOB (shortness of breath) Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)
 Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)") Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
EDUCATION PRACTICE. Management of Refractory Ascites. Clinical Scenario. The Problem
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:1187 1191 EDUCATION PRACTICE Management of Refractory Ascites ANDRÉS CÁRDENAS and PERE GINÈS Liver Unit, Institute of Digestive Diseases, Hospital Clínic,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:1187 1191 EDUCATION PRACTICE Management of Refractory Ascites ANDRÉS CÁRDENAS and PERE GINÈS Liver Unit, Institute of Digestive Diseases, Hospital Clínic,
Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association
 CIRRHOSIS AND PORTAL HYPERTENSION Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association WHAT IS CIRRHOSIS? What is Cirrhosis? DEFINITION OF CIRRHOSIS
CIRRHOSIS AND PORTAL HYPERTENSION Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association WHAT IS CIRRHOSIS? What is Cirrhosis? DEFINITION OF CIRRHOSIS
DIURETICS-4 Dr. Shariq Syed
 DIURETICS-4 Dr. Shariq Syed AIKTC - Knowledge Resources & Relay Center 1 Pop Quiz!! Loop diuretics act on which transporter PKCC NKCC2 AIKTCC I Don t know AIKTC - Knowledge Resources & Relay Center 2 Pop
DIURETICS-4 Dr. Shariq Syed AIKTC - Knowledge Resources & Relay Center 1 Pop Quiz!! Loop diuretics act on which transporter PKCC NKCC2 AIKTCC I Don t know AIKTC - Knowledge Resources & Relay Center 2 Pop
The Triple Threat. Cardiac Care in the NT Annual Workshop 2017 is proudly supported by:
 The Triple Threat DR KELUM PRIYADARSHANA FRACP CONSULTANT NEPHROLOGIST ROYAL DARWIN HOSPITAL Cardiac Care in the NT Annual Workshop 2017 is proudly supported by: Pathogenesis Diabetes CKD CVD Diabetic
The Triple Threat DR KELUM PRIYADARSHANA FRACP CONSULTANT NEPHROLOGIST ROYAL DARWIN HOSPITAL Cardiac Care in the NT Annual Workshop 2017 is proudly supported by: Pathogenesis Diabetes CKD CVD Diabetic
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome.
 Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Nothing to Disclose. Severe Pulmonary Hypertension
 Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Cardiovascular System B L O O D V E S S E L S 2
 Cardiovascular System B L O O D V E S S E L S 2 Blood Pressure Main factors influencing blood pressure: Cardiac output (CO) Peripheral resistance (PR) Blood volume Peripheral resistance is a major factor
Cardiovascular System B L O O D V E S S E L S 2 Blood Pressure Main factors influencing blood pressure: Cardiac output (CO) Peripheral resistance (PR) Blood volume Peripheral resistance is a major factor
following the last documented transfusion; thereafter, evaluate the residual impairment(s).
.") Adult Listings 5.01 Category of Impairments, Digestive System 5.02 Gastrointestinal hemorrhaging from any cause, requiring blood transfusion (with or without hospitalization) of at least 2 units of blood
Adult Listings 5.01 Category of Impairments, Digestive System 5.02 Gastrointestinal hemorrhaging from any cause, requiring blood transfusion (with or without hospitalization) of at least 2 units of blood
Managing Cirrhosis. Cirrhosis of the liver is a progressive, fibrosing. Ascites. By Cameron Ghent, MD, FRCPC. Complications of Cirrhosis
 Focus on CME at the University of Western Ontario Managing Cirrhosis By Cameron Ghent, MD, FRCPC Cirrhosis of the liver is a progressive, fibrosing process resulting in nodule formation and microvascular
Focus on CME at the University of Western Ontario Managing Cirrhosis By Cameron Ghent, MD, FRCPC Cirrhosis of the liver is a progressive, fibrosing process resulting in nodule formation and microvascular
Pharmacology in Liver Disease. Sandeep Whitehead Advanced Clinical Pharmacist Hepatology and Liver Transplant
 Pharmacology in Liver Disease Sandeep Whitehead Advanced Clinical Pharmacist Hepatology and Liver Transplant Objectives Outline the drug management for patients with: Ascites Spontaneous Bacterial Peritonitis
Pharmacology in Liver Disease Sandeep Whitehead Advanced Clinical Pharmacist Hepatology and Liver Transplant Objectives Outline the drug management for patients with: Ascites Spontaneous Bacterial Peritonitis
Portal hypertension is the main complication of cirrhosis
 GASTROENTEROLOGY 2001;120:726 748 Current Management of the Complications of Cirrhosis and Portal Hypertension: Variceal Hemorrhage, Ascites, and Spontaneous Bacterial Peritonitis GUADALUPE GARCIA TSAO
GASTROENTEROLOGY 2001;120:726 748 Current Management of the Complications of Cirrhosis and Portal Hypertension: Variceal Hemorrhage, Ascites, and Spontaneous Bacterial Peritonitis GUADALUPE GARCIA TSAO
RRT in Advanced Heart Failure and Liver Failure When to start and when to stop?
 Critical Care Medicine Apollo Hospitals RRT in Advanced Heart Failure and Liver Failure When to start and when to stop? Ramesh Venkataraman, AB (Int. Med), AB (CCM) Senior Consultant, Critical Care Medicine
Critical Care Medicine Apollo Hospitals RRT in Advanced Heart Failure and Liver Failure When to start and when to stop? Ramesh Venkataraman, AB (Int. Med), AB (CCM) Senior Consultant, Critical Care Medicine
Cell-Derived Inflammatory Mediators
 Cell-Derived Inflammatory Mediators Introduction about chemical mediators in inflammation Mediators may be Cellular mediators cell-produced or cell-secreted derived from circulating inactive precursors,
Cell-Derived Inflammatory Mediators Introduction about chemical mediators in inflammation Mediators may be Cellular mediators cell-produced or cell-secreted derived from circulating inactive precursors,