Renal Denervation: Back to the Future?
|
|
|
- Alicia May
- 5 years ago
- Views:
Transcription

1 Renal Denervation: Back to the Future? RCP BHS Hypertension State of the Art 27 th June 2016 Adrian J.B. Brady MD, FRCP(Glasg), FRCPE, FBHS, FESC, FAHA Associate Professor, University of Glasgow Consultant Cardiologist Glasgow, UK President, British Hypertension Society Council, British Cardiovascular Society European Society of Cardiology Global Spokesperson for Hypertension Disclosures: Research grants from: AstraZeneca, Bayer, Boehringer Ingelheim, Merck,, Roche, Servier Honoraria/Consultancy: AstraZeneca, Bayer, Boehringer Ingelheim, Merck, Pfizer, Servier
2 Question: Which risk factor accounts for the most CV disease according to the World Health Organisation? 1. Smoking 2. Dyslipidaemia 3. Family History of CVD 4. Obesity 5. Diabetes 6. Hypertension 7. Low birth Weight 8. Urban pollution
3 Which risk factor accounts for the most CV disease according to the World Health Organisation?
4
5 Percentage of Hypertensive Patients with controlled Blood Pressure (<140/90 mmhg) in Europe Czech Republic England Frankreich Deutschland Griechenland Ungarn Italien Polen Spanien Schweden Türkei Prof. Schmieder, FAU Erlangen FAU, Prof. Schmieder ESH Newsletter 2007;8:No 3
6 2013 Definitions: ESC/ESH AHA BHS 1. BP above goal on a rational >3 med regimen with complementary mechanisms of action at optimal doses preferably including a diuretic. BHS: A+C+D 2. Controlled Resistant Hypertension. BP controlled to goal on 4 BP meds (optimal doses, preferably including a diuretic). Calhoun DA, et al. Hypertension. 2008;51: Mancia G, et al. Eur Heart J 2013 doi: /eurheartj/eht151
7 556 patients with TRH, based on office BP 338 (61%) had confirmation of TRH on 24-hr ABPM. Mean follow-up 4.8 years Salles GF, et al. Arch Int Med. 2008;168: (Brazil)
8 1. ABPM / HBPM 2. Identify contributing lifestyle factors 3. Discontinue / minimize drugs that BP 4. Investigate for secondary causes of hypertension 5. Maximize and optimize pharmacotherapy 6. Consider interventional procedures



9 ABPM and HBPM superior to office BP
10 Cuff too small = mm Hg Talking during measurement: 20 mm Hg Clues to measurement artifacts: Less target organ damage than expected 4 Hypotensive symptoms with treated 1 JAMA 1988;259: Am J Hypertens 2001;14: Hypertension 1983;5: Ann Int Med 1990;112:
11 Case report: Mrs PC 76 HT 15y Atenolol 100 mg, Enalapril 20 mg, Amlodipine 10 mg, Doxazosin 8 mg, Bendroflumethiazide 2.5 mg, Amiloride 5 mg. Referred for specialist opinion 177/79 mm Hg Heart sounds normal; heart rate 88, regular
12 Case report: Mrs PC 76 HT 15y Admitted as day case given her own medication Collapse in hospital shop BP 70/40 mm Hg
13
14 Singer D et al. Hypertension 1995;25:
15 Only alteration salt restriction and switch to LoSalt (K+ based) HBPM ~ 137/78 mm Hg
16 Case Presentation: 55 y/o man 12 year HT & arthritis. HBPM ~156/94 mm Hg. HCTZ 25 + Losartan 100 mg daily. Celebrex 200 mg 1 2 /d Office BP 162/98 mm Hg & BMI 29 Rx: Switch COX 2 to paracetamol, follow the DASH Eating Plan and take more exercise. Egan BM, unpublished
17 1 month follow up visit: Paracetamol 500 mg bd, HCTZ+ Losartan Too busy to change eating and exercise patterns. BP 118/72 mm Hg, BMI unchanged Re-challenge with celocoxib X 2 raises BP 40 50/20 25 mmhg within 1 2 days with return to normal BP values within 2 3 days. Egan BM, unpublished
18 Renal artery stenosis Sleep apnoea Drug-induced or drug-related hypertension (e.g. NSAIDs) Chronic renal disease Primary aldosteronism Renovascular disease Chronic steroid therapy and Cushing s syndrome Pheochromocytoma Coarctation of the aorta Thyroid or parathyroid disease Brady AJB, et al. Mayo Clinic Textbook of Cardiology 2013
19 Case Report 68 year old female First diagnosed with hypertension 1979 (age 36) /86 mm Hg ramipril/atenolol/valsartan/ amlodipine/furosemide/spironolactone Renin/aldosterone profile in normal range MRI adrenals normal /99 aliskerin added: now on 7 antihypertensive drugs
20 20/09/10- admitted for renal denervation as part of SYMPLICITY-2-HTN trial Admission BP 220/120 (same therapy) Pre-procedure 190/100

21
22 Post procedure BP 163/77 No antihypertensives given that night Next morning 135/74 pre therapy Discharged on atenolol 25mg Stopped 1 week later 1 year later BP 134/77 mm Hg, no antihypertensive Rx Creatinine 76, ACR 10.5
23 Glasgow Renal Artery Sympathectomy Study (GRASS) summary Mark P, Brady AJB, et al. J Human Hypertension 2013 suppl Promising treatment for resistant hypertension In our hands approx 20-25% non responder The rest- variable degrees of response representing real world experience Considerable need for pre, peri, post procedural care- i.e. not a day case procedure Longer term studies in real world and in better defined patient groups required

24 Laragh JH, Baer L, Brunner HR, BOhler FR, Sealey JE, Vaughan ED Jj: The renin-angiotensin-aldosterone system in pathogenesis and management of hypertensive vascular disease. In Hypertension Manual, edited by Laragh JH. New York, Yorke Medical Books, 1976, p 313

25 Angiotensin II Stress Chemoreceptors Baroreceptors vagal efferents Ach renin NE Cardiac afferents NE EPI Renal afferents sympathetic efferents NE 25
26
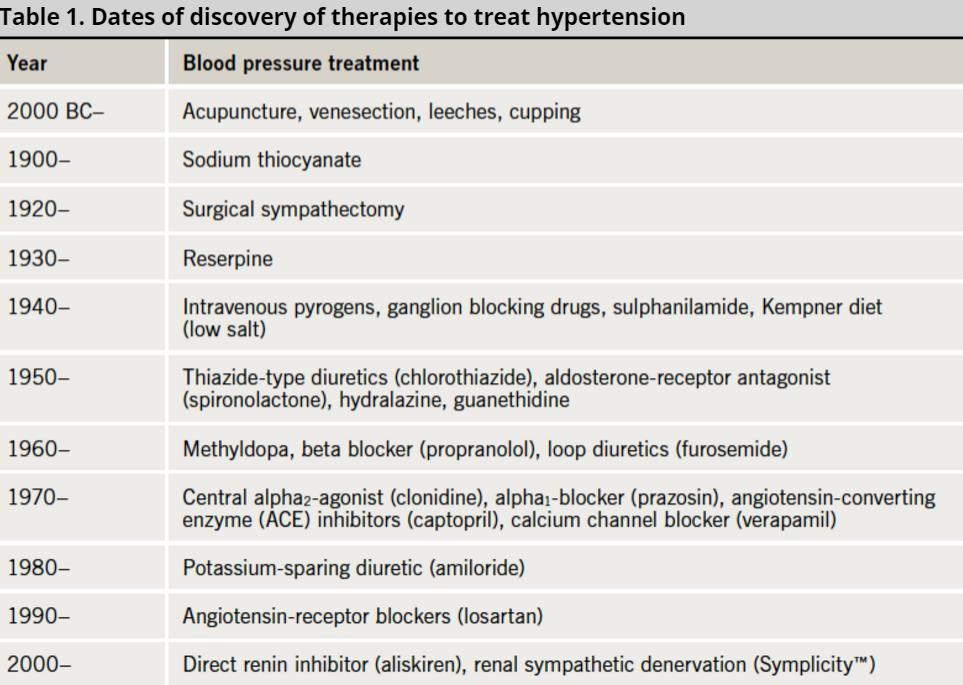
27 Ann Intern Med. 1938;11(12): Ann Intern Med. 1949;30(2):

28 Long Term Effect of Renal Denervation in Human Hypertension Am J Surg 1948; 75: 48-68
29 Effects of Renal Sympathetic Nerve Activity on Renal Function Renin secretion rate 1 - adrenoceptor Juxtaglomerular granular cell: renin Tubular one nerve fiber sodium contacting multiple reabsorption effectors 1B - adrenoceptor RSNA Renal blood flow 1A - adrenoceptor DiBona GF, Kopp Am UC. J Physiol 279:R , Rev 77:75-197,
30 Renal DNX : prevents reflex induced renin secretion Renin secretion, ng/min CONTROL TILT Renin secretion, ng/min CONTROL FUROSEMIDE INN DNX Am J Physiol 232:H500-H507, 1977
31 Renal NE Concentration After Renal DNX Residual renal NE concentration 29% of control at days after DNX Am J Physiol 238: R353-R358, 1980
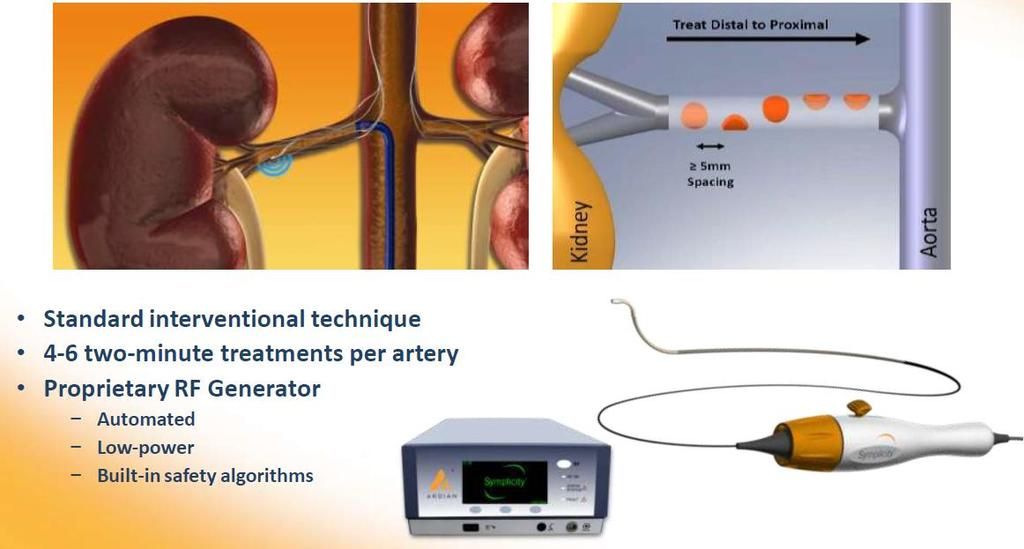
32 Renal Tissue NE (pg/mg) For distribution only in markets where the Symplicity TM renal denervation system is approved. Symplicity is a trademark of Medtronic, Inc. and is registered in one or more countries of the world. Not for distribution in the USA or Japan Medtronic, Inc. All rights reserved. MKG025 3/12 Renal Denervation Preclinical Efficacy and Safety Extensive research in >300 swine Effectiveness: P< Safety: Statistically significant reduction in renal tissue NE Verification testing included angiography, gross pathology, histopathology, & clinical pathology at 7, 30, 60, and 180 days Intact endothelium by 7 days Vascular healing observed at 30 and 60 days; by 180 days, arteries were well healed (no inflammatory cells) treatment sites were considered sterile and stable Untreated Control (N=24) 21 Catheter Denervation (N=33) P= Surgical Denervation (N=4) No stenosis or luminal reduction seen in any treated artery through 180 days Data on file. Medtronic, Inc.




33 Porcine Histology at 7 and 90 days 7-days: Circumferential nerve damage with minimal effect on artery; Less injury with NW 2013 formulation 90-days: Nerves covered in fibrous connective tissue; arteries look healthy 7 DAYS 90 DAYS TCT2013 Slide 33



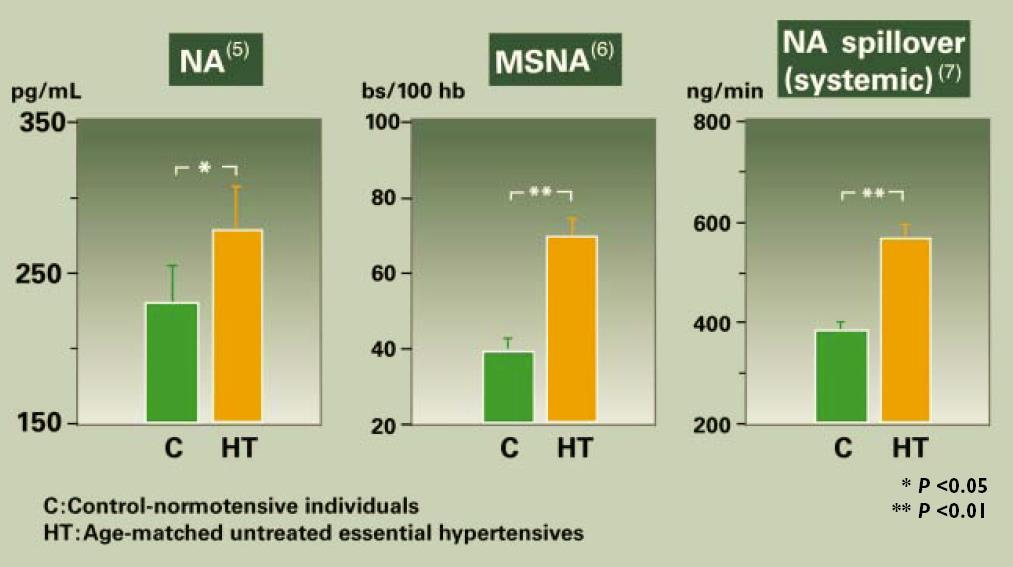
34 Overactive SNS is Driver for Resistant HTN Significantly more nerves in hypertensive patients nerves G. Sangiorgi et al., TCT TCT
35 Renal Denervation by RF Ablation Related Changes in Underlying Physiology Baseline 1 mo Office BP (mmhg) 161/ /90 Renal NE spillover (ng/min) - left kidney % - right kidney % Total body NE spillover (ng/min) % Plasma Renin (µg/l/hr) % Renal Plasma flow (ml/min) % LV Mass (cmri) dropped 7% (from 78.8 to 73.1 g/m2) from baseline to 12 months Schlaich et al. NEJM. 2009; 36(9):
36 Ablation of Renal Afferent Nerves: effect on muscle sympathetic nerve activity in a patient with Resistant hypertension Baseline 30 days FU 12 M FU ECG 200 BP MSNA 10 sec 56 bursts/min 41 bursts/min 19 bursts/min Schlaich et al. NEJM 2009;36:



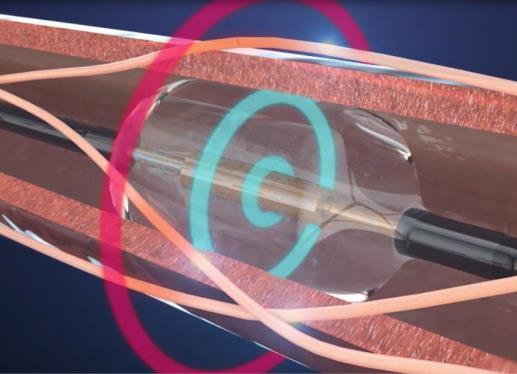
37 Targeting Renal Nerves Nerves arise from T10-L2 The nerves arborize around the artery and primarily lie within the adventitia Vessel Lumen Media Adventitia Renal Nerves



38 Catheter-based RDN Therapy: Ardian and more COV: One Shot STJ: EnligHTN RECOR BSX: Vessix KONA and more Dr.C.Venkata S.Ram TCT2013 Slide 38
39 Catheter-based Renal Denervation: Staged Clinical Evaluation First-in-Man Series of Pilot studies Symplicity HTN-1 Extended follow-up Symplicity HTN-2 Initial Randomized Clinical Trial Symplicity HTN-3 US PMA Randomized Clinical Trial (completed) Registries, Symplicity GLOBAL, ACC, LBCT, new tehniques

 Registries,")
40 Catheter-based Renal Denervation: Staged Clinical Evaluation First-in-Man Series of Pilot studies Symplicity HTN-1 Extended follow-up Symplicity HTN-2 Initial Randomized Clinical Trial Symplicity HTN-3 US PMA Randomized Clinical Trial (completed) Registries, Symplicity GLOBAL, ACC, LBCT
:")
41 Krum et al, Lancet (2013): [doi: /s (13) ]
42 Catheter-based Renal Denervation: Staged Clinical Evaluation First-in-Man Series of Pilot studies Symplicity HTN-1 Extended follow-up Symplicity HTN-2 Initial Randomized Clinical Trial Symplicity HTN-3 US PMA Randomized Clinical Trial (ACC LBCT, NEJM) Global Symplicity Registry (ACC LBCT)


43 Time course of office BP change 1M 3M 6M RDN from Baseline (mmhg) Systolic Diastolic -24 p< for between-group comparisons p=0.002 for between-group comparisons p=0.005 for between-group comparisons Two-way repeated measures ANOVA, p= Control from Baseline (mmhg) Systolic Diastolic Symplicity HTN-2 Investigators. The Lancet
44 Catheter-based Renal Denervation: Staged Clinical Evaluation First-in-Man Series of Pilot studies Symplicity HTN-1 Extended follow-up Symplicity HTN-2 Initial Randomized Clinical Trial Symplicity HTN-3 US PMA Randomized Clinical Trial (ACC LBCT) Global Simplicity Registry (ACC LBCT)

45

46 Symplicity HTN 3-Primary efficacy endpoint Bhatt DL, NEJM 2014

47 Lessons Learned from SYMPLICITY HTN-3 HTN-3 Factors Identified Procedural Medications Study Population
48 SPYRAL HTN Global Clinical Trial Program SYMPLICITY HTN-3 Factor Identified Medications Obtain off-med data Standardize meds No max dose titration Measure adherence SPYRAL HTN
49 Were there frequent drug changes between baseline and 6 months of follow up? Proportion of Patients With Drug Changes Between Baseline and 6 mo (%) Denervation Sham Protocol mandated: Maximum doses and No medication changes ~40% of patients underwent medication changes* 69% of first medication changes were medically necessary *Changes included class or dose unpublished
50 LC - HR - MS / MS Example Moxonidine at m/z Hydrochlorothiazide at m/z Minoxidil at m/z Ramipril at m/z Amlodipine at m/z Carvedilol at m/z Time (min) Reconstruction on a chromatogram of the protonated or deprotonated drugs after liquid chromatography high resolution tandem mass spectrometry (LC HR MS/MS) analysis. Arrows indicate retention times, at which drug should appear. Dashed lines represent background noise. In this patient example 3 out of 6 (50%) agents were taken as prescribed. Ewen et al., Clin Res Cardiol (2015)
51 Drugs taken (%) Drugs taken (%) Adherence After RDN A Responder office SBP B Non-responder office SBP 100 p= p= Baseline 6 months n=63 n=63 Baseline 6 months Baseline 6 months n=37 n=37 Baseline 6 months Ewen et al., Clin Res Cardiol (2015)
52 SPYRAL HTN Global Clinical Trial Program SYMPLICITY HTN-3 Factor Identified Medications Obtain off-med data Standardize meds No max dose titration Measure adherence SPYRAL HTN Study population Less severe HTN Fewer prescribed meds Focus on ABPM Patients from across globe Avoid changing patient behavior

53 Change in Blood Pressure in African-Americans vs Non-African-Americans Kandzari et al., 2014 submitted (Symplicity HTN-3), Hotline EurpPCR

54 Ewen et al., Hypertension 65: , 2015
55 SPYRAL HTN Global Clinical Trial Program SYMPLICITY HTN-3 Factor Identified Medications Obtain off-med data Standardize meds No max dose titration Measure adherence SPYRAL HTN Study population Less severe HTN Fewer prescribed meds Focus on ABPM Patients from across globe Avoid changing patient behavior Procedural Symplicity Spyral catheter Main and branch vessel treatment Experienced proceduralists

56 Office BP Response by Number of Ablation Attempts Kandzari et al., Eur Heart J, 2014 (Symplicity HTN-3)

57 BP Response by Circumferentiality of Ablation Kandzari et al., Eur Heart J, 2014 (Symplicity HTN-3)


58 Renal denervation in CE-marked devices

59 Our View of Renal Nerve Distribution Has Changed Renal nerves may have a positional bias on radial distance from arterial lumen: distal nerves are closer Distal Proximal Prior concept Uniform radial distribution Distal Proximal Current concept Non-uniform radial distribution Sakakura K, et al., JACC :634-43

60 NE Concentration (pg/mg) Combined Branch and Main Artery Treatment 500 I V Y N * $ 200 * Control Main Control Branch Control Branch + Main Treatment Mahfoud et al., JACC 2015 in press
61 SPYRAL HTN Global Clinical Trial Program First Phase Includes Two Parallel Trials 20 Sites Globally SPYRAL HTN OFF MED 100 patients Sham RCT (1:1) Main body and branch ablation No specific baseline medication requirement Compare ABPM change at 3 months QOL to be measured SPYRAL HTN ON MED 100 patients Sham RCT (1:1) Main body and branch ablation No max tolerated dose Compare ABPM change at 3 months QOL to be measured Second Phase SPYRAL HTN Pivotal Based on OFF/ON trial results Cost effectiveness data/qol to be measured








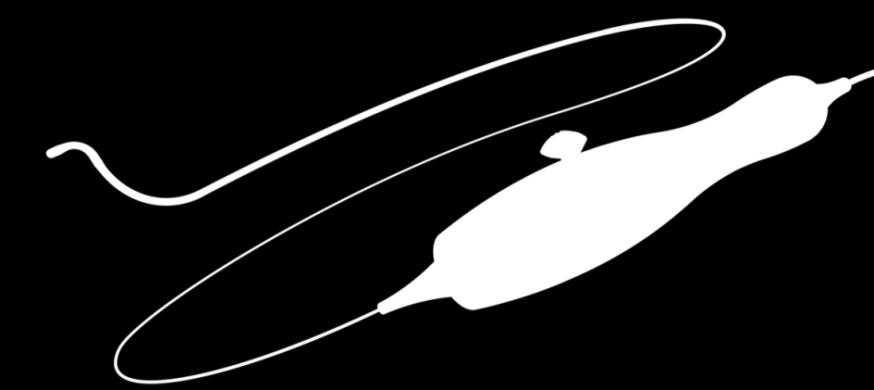
62 Kona Medical Surround Sound Hypertension Therapy Non-Invasive Renal Denervation 1 Imaging and therapy ultrasound positioned beneath patient 2 Ultrasound imaging used to identify renal artery External ultrasound energy guided by ultrasound image and motion tracking 3 4 Focused ultrasound energy administered in treatment pattern to ablate nerves located outside of artery 5 Energy field surrounds artery, ablates renal nerves Note: Kona Surround Sound Hypertension Therapy is investigational and not approved for sale

63 The future... What is planned?
64
65 Is diet and exercise just a big waste of time? Yes No Don t know
66
67

68
 and Rangers and Celtic Football Clubs.")
69 Delivering Health: An Alliance between the Royal College of Physicians and Surgeons of Glasgow (RCPSG) and Rangers and Celtic Football Clubs. Royal College of Physicians and Surgeons of Glasgow


70
71 Football Health Glasgow Staffing: At Ibrox/Parkhead grounds Coaching staff, medical staff, nurse, dietician, integration with present/former players NHS staff already identified and enthusiastic RCPSG support data, audit, statistics, long term support

72

73

74


75
76

77
78 Football Health Glasgow Pilot project - introduce a health programme running over 10 weeks via sessions for 20 participants at each club. Measurements of weight, blood pressure, cholesterol at start and end of 10 week programme Review planned 1 year after end of programme
79 P<0.001 Weight Programme start 3 months 15 months Brady A, et al. Eur Heart J Dec 2010
80 mmol/l 7.00 Total cholesterol p<0.01 p=ns Programme start 3 months 15 months Brady A, et al. Eur Heart J Dec 2010

81 mm Hg Results of Celtic Rangers Football Health Study Systolic BP 160 p=ns Start 3 months 15 months Brady A, et al. Eur Heart J Dec 2010
82 mm Hg Results of Celtic Rangers Football Health Study Diastolic BP 100 p=ns Start 3 months 15 months Brady A, et al. Eur Heart J Dec 2010

83 European Heart Journal 2010; 31:

84 2.5M grant 2000 men, cluster cohort design.

85 Results
86
87 Mean weight loss (%) Weight loss (%) Intervention Comparison weeks 12 months (Error bars represent 95% confidence intervals) Adjusted between-group difference 12 weeks 4 71% (CI 5.44, 3.98) p<.0001 Adjusted between-group difference 12 months 4.36% (CI 5.08,3.64) p<.0001 Hunt, Wyke, Gray, Anderson, Brady et al. Lancet 2014
88 Hunt, Wyke, Gray, Anderson, Brady et al. Lancet 2014 Weight loss over time
89 Mean BP reduction (mmhg) Lower blood pressure Intervention Comparison weeks 12 months 12 weeks 12 months Systolic Diastolic (Error bars represent 95% confidence intervals) Systolic (mmhg) Diastolic (mmhg) Adjusted between-group difference 12 weeks 4.51 (CI 6.36, 2.67) p<.0001 Adjusted between-group difference 12 months 2.27 (CI 4.01, 0.54) p<.0171 Adjusted between-group difference 12 weeks 2.51 (CI 3.71, 1.32) p<.0001 Adjusted between-group difference 12 months 1 36 (CI 2.48, 0.24) p=.0102
90 Mean change in self esteem (Rosenberg) Increased self esteem Intervention Comparison weeks 12 months (Error bars represent 95% confidence intervals) Adjusted between-group difference 12 weeks 0.19 (CI 0.14,-0.24) p<.0001 Adjusted between-group difference 12 months 0.12 (CI 0.07, 0.17) p<.0001 Hunt, Wyke, Gray, Anderson, Brady et al. Lancet 2014

91 The next challenge BHF 0.25M Children Diet and exercise Focused approach St Mungo s Academy, Glasgow UK

92
93
94
95 Preliminary discussions: Global Football Health Tottenham Hotspur Everton Fulham Barcelona, Spain DC United, Washington, USA Baltimore Blast, Baltimore, USA Kingfisher East Bengal FC, Kolkata, India Ajax, the Netherlands Two rugby clubs in New Zealand

96 Conclusions Diet and exercise are fundamental Delivery and sustainability is crucial
RISE, FALL AND RESURRECTION OF RENAL DENERVATION. Michael A. Weber, MD State University of New York Downstate College of Medicine
 RISE, FALL AND RESURRECTION OF RENAL DENERVATION Michael A. Weber, MD State University of New York Downstate College of Medicine Michael Weber, Disclosures Research/Trial Commitments and Consulting: Boston
RISE, FALL AND RESURRECTION OF RENAL DENERVATION Michael A. Weber, MD State University of New York Downstate College of Medicine Michael Weber, Disclosures Research/Trial Commitments and Consulting: Boston
Catheter-Based Renal Denervation (RDN)
") Hypertension lecture 3: Catheter-Based Renal Denervation (RDN) Adapted from slides prepared by Dr IOEBRAHIM, UNITAS HOSPITAL and others Hypertension Epidemiology 30% Untreated 35% Treated & Controlled
Hypertension lecture 3: Catheter-Based Renal Denervation (RDN) Adapted from slides prepared by Dr IOEBRAHIM, UNITAS HOSPITAL and others Hypertension Epidemiology 30% Untreated 35% Treated & Controlled
Catheter-Based Renal Denervation Reduces Total Body and Renal Noradrenaline Spillover and Blood Pressure in Resistant Hypertension
 Catheter-Based Renal Denervation Reduces Total Body and Renal Noradrenaline Spillover and Blood Pressure in Resistant Hypertension Murray Esler, Markus Schlaich, Paul Sobotka, Rob Whitbourn, Jerzy Sadowski,
Catheter-Based Renal Denervation Reduces Total Body and Renal Noradrenaline Spillover and Blood Pressure in Resistant Hypertension Murray Esler, Markus Schlaich, Paul Sobotka, Rob Whitbourn, Jerzy Sadowski,
Disclosures for Dr. Bhatt
 Renal Denervation Deepak L. Bhatt, MD, MPH, FACC, FAHA, FSCAI, FESC Executive Director of Interventional Cardiovascular Programs, BWH Heart & Vascular Center Professor of Medicine, Harvard Medical School
Renal Denervation Deepak L. Bhatt, MD, MPH, FACC, FAHA, FSCAI, FESC Executive Director of Interventional Cardiovascular Programs, BWH Heart & Vascular Center Professor of Medicine, Harvard Medical School
The Future of Renal Denervation
 The Future of Renal Denervation Ron Waksman, MD, FACC, FSCAI Professor of Medicine, (Cardiology) Georgetown University Director, Cardiovascular Research Advanced Education MedStar Heart Institute, Washington
The Future of Renal Denervation Ron Waksman, MD, FACC, FSCAI Professor of Medicine, (Cardiology) Georgetown University Director, Cardiovascular Research Advanced Education MedStar Heart Institute, Washington
Update on renal denervation: Latest data
 LINC 2018 Update on renal denervation: Latest data Felix Mahfoud Saarland University Hospital, Germany Potential Conflicts of Interest I have the following potential conflicts of interest to report: Research
LINC 2018 Update on renal denervation: Latest data Felix Mahfoud Saarland University Hospital, Germany Potential Conflicts of Interest I have the following potential conflicts of interest to report: Research
Catheter-Based Renal Sympathetic Denervation in the Management of Resistant Hypertension
 Catheter-Based Renal Sympathetic Denervation in the Management of Resistant Hypertension Henry Krum, Markus Schlaich, Paul Sobotka, Rob Whitbourn, Jerzy Sadowski, Krzysztof Bartus, Boguslaw Kapelak, Horst
Catheter-Based Renal Sympathetic Denervation in the Management of Resistant Hypertension Henry Krum, Markus Schlaich, Paul Sobotka, Rob Whitbourn, Jerzy Sadowski, Krzysztof Bartus, Boguslaw Kapelak, Horst
noradrenaline spillover and systemic blood pressure in patients with resistant hypertension
 Effects of renal sympathetic denervation on noradrenaline spillover and systemic blood pressure in patients with resistant hypertension Markus Schlaich Neurovascular Hypertension & Kidney Disease Laboratory
Effects of renal sympathetic denervation on noradrenaline spillover and systemic blood pressure in patients with resistant hypertension Markus Schlaich Neurovascular Hypertension & Kidney Disease Laboratory
What We've Learned from Simplicity HTN-1,2, and Registries
 ANGIOPLASTY SUMMIT-TCTAP 2012 Seoul, Korea, April 24-27, 2012 What We've Learned from Simplicity HTN-1,2, and Registries Horst Sievert, Ann-Kathrin Ziegler, Benjamin Kaltenbach, Ilona Hofmann, Undine Pittl
ANGIOPLASTY SUMMIT-TCTAP 2012 Seoul, Korea, April 24-27, 2012 What We've Learned from Simplicity HTN-1,2, and Registries Horst Sievert, Ann-Kathrin Ziegler, Benjamin Kaltenbach, Ilona Hofmann, Undine Pittl
Renal Denervation. Henry Krum MBBS PhD FRACP. Centre of Cardiovascular Research & Monash University/Alfred Hospital;
 Renal Denervation Henry Krum MBBS PhD FRACP Centre of Cardiovascular Research & Education in Therapeutics, Monash University/Alfred Hospital; Alfred Heart Centre, The Alfred Hospital, Melbourne Australia
Renal Denervation Henry Krum MBBS PhD FRACP Centre of Cardiovascular Research & Education in Therapeutics, Monash University/Alfred Hospital; Alfred Heart Centre, The Alfred Hospital, Melbourne Australia
Renal sympathetic denervation as a potential treatment for hypertension
 Renal sympathetic denervation as a potential treatment for hypertension (Why we must keep going) Dr Andrew SP Sharp Consultant Cardiologist and Honorary Senior Lecturer Royal Devon and Exeter Hospital
Renal sympathetic denervation as a potential treatment for hypertension (Why we must keep going) Dr Andrew SP Sharp Consultant Cardiologist and Honorary Senior Lecturer Royal Devon and Exeter Hospital
Renal Sympathetic Denervation Beyond Hypertension: Therapy for Arrhythmias and for Autonomic Nervous System Dysfunction?
 Renal Sympathetic Denervation Beyond Hypertension: Therapy for Arrhythmias and for Autonomic Nervous System Dysfunction? Vivek Y. Reddy, MD Helmsley Trust Professor of Medicine Director, Cardiac Arrhythmia
Renal Sympathetic Denervation Beyond Hypertension: Therapy for Arrhythmias and for Autonomic Nervous System Dysfunction? Vivek Y. Reddy, MD Helmsley Trust Professor of Medicine Director, Cardiac Arrhythmia
Treating Hypertension With a Catheter..Wait What? David P. Lee, M.D. 22 June 2013 Stanford University
 Treating Hypertension With a Catheter..Wait What? David P. Lee, M.D. 22 June 2013 Stanford University COI Medtronic: Research Grant, Consultant Boston Scientific: Research Grant, MAB Worldwide Prevalence
Treating Hypertension With a Catheter..Wait What? David P. Lee, M.D. 22 June 2013 Stanford University COI Medtronic: Research Grant, Consultant Boston Scientific: Research Grant, MAB Worldwide Prevalence
Renal denervation for treatment of resistant hypertension
 Renal denervation for treatment of resistant hypertension Dr U. Nqebelele Division of Nephrology Department of Internal Medicine Charlotte Maxeke Johannesburg Academic Hospital Thomas Willis: 1621-1675
Renal denervation for treatment of resistant hypertension Dr U. Nqebelele Division of Nephrology Department of Internal Medicine Charlotte Maxeke Johannesburg Academic Hospital Thomas Willis: 1621-1675
Renal Denervation. by Walead Latif, DO, MBA, CPE Assistant Clinical Professor Rutgers Medical School
 Renal Denervation by Walead Latif, DO, MBA, CPE Assistant Clinical Professor Rutgers Medical School Disclosure Information ACOI Annual Meeting I have the following financial relationships to disclose:
Renal Denervation by Walead Latif, DO, MBA, CPE Assistant Clinical Professor Rutgers Medical School Disclosure Information ACOI Annual Meeting I have the following financial relationships to disclose:
Devices and Long-Term Outcomes of Renal Denervation for Hypertension
 18th ANGIOPLASTY SUMMIT-TCTAP 2013 Seoul, Korea, April 23-26, 2013 Devices and Long-Term Outcomes of Renal Denervation for Hypertension Horst Sievert, Ilona Hofmann, Laura Vaskelyte, Stefan Bertog, Simon
18th ANGIOPLASTY SUMMIT-TCTAP 2013 Seoul, Korea, April 23-26, 2013 Devices and Long-Term Outcomes of Renal Denervation for Hypertension Horst Sievert, Ilona Hofmann, Laura Vaskelyte, Stefan Bertog, Simon
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Renal Artery Denervation New Concepts in Hypertension Treatment
 Renal Artery Denervation New Concepts in Hypertension Treatment Istanbul Course of Interventional Cardiology J. Weil Medizinische Klinik II Kardiologie, Angiologie und internistische Intensivmedizin Universitätsklinikum,
Renal Artery Denervation New Concepts in Hypertension Treatment Istanbul Course of Interventional Cardiology J. Weil Medizinische Klinik II Kardiologie, Angiologie und internistische Intensivmedizin Universitätsklinikum,
Real World Experience with Renal Denervation Therapy
 JCR 2013 Real World Experience with Renal Denervation Therapy Seung-Hyuk Choi Division of Cardiology Samsung Medical Center Seoul, Korea Hypertension A Major Public Health Burden Astonishing prevalence
JCR 2013 Real World Experience with Renal Denervation Therapy Seung-Hyuk Choi Division of Cardiology Samsung Medical Center Seoul, Korea Hypertension A Major Public Health Burden Astonishing prevalence
Hypertension Guidelines Michael A. Weber, MD Division of Cardiovascular Medicine State University of New York Downstate Medical Center
 Hypertension Guidelines 2016 Michael A. Weber, MD Division of Cardiovascular Medicine State University of New York Downstate Medical Center Speaker Disclosures I disclose that I am a Consultant for: Ablative
Hypertension Guidelines 2016 Michael A. Weber, MD Division of Cardiovascular Medicine State University of New York Downstate Medical Center Speaker Disclosures I disclose that I am a Consultant for: Ablative
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
RESISTENT HYPERTENSION. Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University
 RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
Σύγτρονη θεραπεία της ανθεκτικής σπέρτασης
 Σύγτρονη θεραπεία της ανθεκτικής σπέρτασης Κώζηας Τζιούθης Α Παν/κή Καρ/κή Κλινική Ιπποκράηειο Γ.Ν.Α. Resistant or Refractory to treatment Hypertension Office BP>140/90 or 130/80 mm Hg in patients with
Σύγτρονη θεραπεία της ανθεκτικής σπέρτασης Κώζηας Τζιούθης Α Παν/κή Καρ/κή Κλινική Ιπποκράηειο Γ.Ν.Α. Resistant or Refractory to treatment Hypertension Office BP>140/90 or 130/80 mm Hg in patients with
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Management of Resistant Hypertension in Diabetes
 Management of Resistant Hypertension in Diabetes Soon Hee Lee, M.D., Ph.D. Divisoin of Endocrinology & Metabolism, Department of Internal Medicine, Busan Paik Hospital, College of Medicine, Inje University,
Management of Resistant Hypertension in Diabetes Soon Hee Lee, M.D., Ph.D. Divisoin of Endocrinology & Metabolism, Department of Internal Medicine, Busan Paik Hospital, College of Medicine, Inje University,
Difficult-to-Control & Resistant Hypertension. Anthony Viera, MD, MPH, FAHA Professor and Chair
 Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Byeong-Keuk Kim, MD, PhD. Division of Cardiology, Severance Cardiovascular Hospital Yonsei University College of Medicine, Seoul, Korea
 Byeong-Keuk Kim, MD, PhD Division of Cardiology, Severance Cardiovascular Hospital Yonsei University College of Medicine, Seoul, Korea BP change (mmhg) from Baseline to 6 Months (mmhg) Catheter-based renal
Byeong-Keuk Kim, MD, PhD Division of Cardiology, Severance Cardiovascular Hospital Yonsei University College of Medicine, Seoul, Korea BP change (mmhg) from Baseline to 6 Months (mmhg) Catheter-based renal
Hypertension 2015: Recent Evidence that Will Change Your Practice
 Hypertension 2015: Recent Evidence that Will Change Your Practice Gerald W. Smetana, M.D. Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine Harvard Medical School
Hypertension 2015: Recent Evidence that Will Change Your Practice Gerald W. Smetana, M.D. Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine Harvard Medical School
Renal Denervation: The Case for Cardiology
 Renal Denervation: The Case for Cardiology John C. Gurley, MD University of Kentucky Presenter Disclosure Information John C Gurley, MD Renal Denervation: The Case for Cardiology FINANCIAL DISCLOSURE:
Renal Denervation: The Case for Cardiology John C. Gurley, MD University of Kentucky Presenter Disclosure Information John C Gurley, MD Renal Denervation: The Case for Cardiology FINANCIAL DISCLOSURE:
Treating Hypertension With a Catheter..Wait What? COI 5/3/2013. Worldwide Prevalence of Hypertension Is Increasing
 Treating Hypertension With a Catheter..Wait What? David P. Lee, M.D. 4 May 2013 Stanford University COI Medtronic: Research Grant, Consultant Boston Scientific: Research Grant, MAB Worldwide Prevalence
Treating Hypertension With a Catheter..Wait What? David P. Lee, M.D. 4 May 2013 Stanford University COI Medtronic: Research Grant, Consultant Boston Scientific: Research Grant, MAB Worldwide Prevalence
Renal Denervation For Hypertension: Status Update
 Samuel N. Steerman, Presenter MD, FACS, name RPVI EVMS Assistant Professor of Surgery Sentara Vascular Specialists Renal Denervation For Hypertension: Status Update Disclosures Disclosures Speaker s Panel
Samuel N. Steerman, Presenter MD, FACS, name RPVI EVMS Assistant Professor of Surgery Sentara Vascular Specialists Renal Denervation For Hypertension: Status Update Disclosures Disclosures Speaker s Panel
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ. Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH
 ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
Renal denervation: Current evidence and remaining uncertainties
 Renal denervation: Current evidence and remaining uncertainties Michel Azizi Georges Pompidou European Hospital Hypertension Unit ESH excellence Center Paris Descartes University Clinical Investigation
Renal denervation: Current evidence and remaining uncertainties Michel Azizi Georges Pompidou European Hospital Hypertension Unit ESH excellence Center Paris Descartes University Clinical Investigation
Preliminary Results of RETREAT
 LINC 2015 Leipzig, Germany, Jan 27-30, 2015 Preliminary Results of RETREAT (Renal Denervation with Ultrasound After Failed Radiofrequency Denervation) Horst Sievert, Jan Philipp Kulow, Stefan Bertog, Predrag
LINC 2015 Leipzig, Germany, Jan 27-30, 2015 Preliminary Results of RETREAT (Renal Denervation with Ultrasound After Failed Radiofrequency Denervation) Horst Sievert, Jan Philipp Kulow, Stefan Bertog, Predrag
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension: What s new since JNC 7. Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF
 Hypertension: What s new since JNC 7 Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF Disclosures Spectral Diagnostics Site investigator Eli Lilly Site investigator ACP IM ITE writing committee NBME Step
Hypertension: What s new since JNC 7 Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF Disclosures Spectral Diagnostics Site investigator Eli Lilly Site investigator ACP IM ITE writing committee NBME Step
Prof. Andrzej Wiecek Department of Nephrology, Endocrinology and Metabolic Diseases Medical University of Silesia Katowice, Poland.
 What could be the role of renal denervation in chronic kidney disease? Andrzej Wiecek, Katowice, Poland Chairs: Peter J. Blankestijn, Utrecht, The Netherlands Jonathan Moss, Glasgow, UK Prof. Andrzej Wiecek
What could be the role of renal denervation in chronic kidney disease? Andrzej Wiecek, Katowice, Poland Chairs: Peter J. Blankestijn, Utrecht, The Netherlands Jonathan Moss, Glasgow, UK Prof. Andrzej Wiecek
The Global SYMPLICITY Registry: Safety and Effectiveness of Renal Artery Denervation In Real World Patients With Uncontrolled Hypertension
 The Global SYMPLICITY Registry: Safety and Effectiveness of Renal Artery Denervation In Real World Patients With Uncontrolled Hypertension Michael Böhm, MD on behalf of the GSR Investigators March 30,
The Global SYMPLICITY Registry: Safety and Effectiveness of Renal Artery Denervation In Real World Patients With Uncontrolled Hypertension Michael Böhm, MD on behalf of the GSR Investigators March 30,
Transcatheter Perivascular Alcohol- Mediated Renal Denervation
 Transcatheter Perivascular Alcohol- Mediated Renal Denervation Wojtek Wojakowski, MD, PhD Medical University of Silesia American Heart of Poland Katowice, Poland I, Wojciech Wojakowski DO NOT have a financial
Transcatheter Perivascular Alcohol- Mediated Renal Denervation Wojtek Wojakowski, MD, PhD Medical University of Silesia American Heart of Poland Katowice, Poland I, Wojciech Wojakowski DO NOT have a financial
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Brent M. Egan, MD Professor of Medicine USCSOM Greenville
 Contemporary Management of Uncontrolled and Treatment Resistant Hypertension Brent M. Egan, MD Professor of Medicine USCSOM Greenville Disclosures (past 3 years): Honoraria: BCBSSC, Medtronic Grant Support:
Contemporary Management of Uncontrolled and Treatment Resistant Hypertension Brent M. Egan, MD Professor of Medicine USCSOM Greenville Disclosures (past 3 years): Honoraria: BCBSSC, Medtronic Grant Support:
With an unrestricted educational grant from. The Interventional Treatment of Resistant Hypertension
 With an unrestricted educational grant from The Interventional Treatment of Resistant Hypertension Felix Mahfoud Interventional Cardiology University Hospital Homburg/Saar Germany Dr. Mahfoud graduated
With an unrestricted educational grant from The Interventional Treatment of Resistant Hypertension Felix Mahfoud Interventional Cardiology University Hospital Homburg/Saar Germany Dr. Mahfoud graduated
Managing Hypertension in 2016
 Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
OLOMOUC I Study M. Táborský, M. Lazárová, J. Václavík, D. Richter ESC 2012, Munich,
 The effect of renal denervation in patients with advanced heart failure: OLOMOUC I Study M. Táborský, M. Lazárová, J. Václavík, D. Richter ESC 2012, Munich, 27.08.2012 Disclosures MT: honoraria Bayer,
The effect of renal denervation in patients with advanced heart failure: OLOMOUC I Study M. Táborský, M. Lazárová, J. Václavík, D. Richter ESC 2012, Munich, 27.08.2012 Disclosures MT: honoraria Bayer,
Relevance of sympathetic overactivity in hypertension and heart failure Therapeutic Implications
 Relevance of sympathetic overactivity in hypertension and heart failure Therapeutic Implications Uta C. Hoppe, MD, FESC Dep. of Internal Medicine II Paracelsus University Salzburg Austria Disclosures Within
Relevance of sympathetic overactivity in hypertension and heart failure Therapeutic Implications Uta C. Hoppe, MD, FESC Dep. of Internal Medicine II Paracelsus University Salzburg Austria Disclosures Within
Ambulatory Blood Pressure Measurement. Objectives of the Presentation. Methods of Measuring BP: Pros and Cons
 Ambulatory Blood Pressure Measurement William B. White, MD Professor of Medicine and Chief, Hypertension and Clinical Pharmacology Calhoun Cardiology Center University of Connecticut School of Medicine
Ambulatory Blood Pressure Measurement William B. White, MD Professor of Medicine and Chief, Hypertension and Clinical Pharmacology Calhoun Cardiology Center University of Connecticut School of Medicine
Renal Sympathetic Denervation for HTN
 Renal Sympathetic Denervation for HTN Se-Young Yim Department of CardioVascular Center Samsung Medical Center Worldwide Prevalence of Hypertension Is Increasing In 2000, 972 million (26%), of the adult
Renal Sympathetic Denervation for HTN Se-Young Yim Department of CardioVascular Center Samsung Medical Center Worldwide Prevalence of Hypertension Is Increasing In 2000, 972 million (26%), of the adult
Special Lecture 11/08/2013. Hypertension Dr. HN Mayrovitz
 Special Lecture 11/08/2013 Hypertension Dr. HN Mayrovitz Arterial Blood Pressure (ABP) Major Factors Summarized Sympathetic Hormones Arteriole MAP ~ Q x TPR + f (V / C) SV x HR Renal SBP Hypertension =
Special Lecture 11/08/2013 Hypertension Dr. HN Mayrovitz Arterial Blood Pressure (ABP) Major Factors Summarized Sympathetic Hormones Arteriole MAP ~ Q x TPR + f (V / C) SV x HR Renal SBP Hypertension =
Catheter Based Denervation for Heart Failure
 Catheter Based Denervation for Heart Failure David E. Kandzari, MD, FACC, FSCAI Chief Scientific Officer Director, Interventional Cardiology Piedmont Heart Institute Atlanta, Georgia david.kandzari@piedmont.org
Catheter Based Denervation for Heart Failure David E. Kandzari, MD, FACC, FSCAI Chief Scientific Officer Director, Interventional Cardiology Piedmont Heart Institute Atlanta, Georgia david.kandzari@piedmont.org
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure. No relevant financial relationships. Blood Pressure and Risk
 MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Treating Hypertension from
 Treating Hypertension from Initiation to Resistance: A Case Study Approach Michelle Krause, MD Division of Nephrology University of Arkansas for Medical Sciences Central Arkansas Veteran s Healthcare System
Treating Hypertension from Initiation to Resistance: A Case Study Approach Michelle Krause, MD Division of Nephrology University of Arkansas for Medical Sciences Central Arkansas Veteran s Healthcare System
EnligHTN I, First-in-Human Multicenter Study of a Multi-Electrode Renal Denervation Catheter in Patients with Drug-Resistant Hypertension
 EnligHTN I, First-in-Human Multicenter Study of a Multi-Electrode Renal Denervation Catheter in Patients with Drug-Resistant Hypertension Vasilios Papademetriou, MD 1 Prof. Stephen Worthley, MD 2 Costas
EnligHTN I, First-in-Human Multicenter Study of a Multi-Electrode Renal Denervation Catheter in Patients with Drug-Resistant Hypertension Vasilios Papademetriou, MD 1 Prof. Stephen Worthley, MD 2 Costas
Modern Management of Hypertension: Where Do We Draw the Line?
 Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Modern Management of Hypertension
 Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Hypertension in the Era of ACC/AHA: Practice Changing Evidence and Recommendations
 Hypertension in the Era of ACC/AHA: Practice Changing Evidence and Recommendations Gerald W. Smetana, M.D., MACP Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine
Hypertension in the Era of ACC/AHA: Practice Changing Evidence and Recommendations Gerald W. Smetana, M.D., MACP Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine
Disclosures. Hypertension: Nationwide Dilemma. Learning Objectives. What s Currently Recommended? Specific Concerns 3/9/2012
 How Should We ACCOMPLISH Good Blood Pressure Control In Our VETS? Disclosures No conflicts of interest to disclose Updates in the Management of HypertensionIn the Elderly Antoine T. Jenkins, Pharm.D.,
How Should We ACCOMPLISH Good Blood Pressure Control In Our VETS? Disclosures No conflicts of interest to disclose Updates in the Management of HypertensionIn the Elderly Antoine T. Jenkins, Pharm.D.,
Hypertension Management: A Moving Target
 9:45 :30am Hypertension Management: A Moving Target SPEAKER Karol Watson, MD, PhD, FACC Presenter Disclosure Information The following relationships exist related to this presentation: Karol E. Watson,
9:45 :30am Hypertension Management: A Moving Target SPEAKER Karol Watson, MD, PhD, FACC Presenter Disclosure Information The following relationships exist related to this presentation: Karol E. Watson,
Treating Hypertension in 2018: What Makes the Most Sense Today?
 Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
Renal Denervation for Resistant Hypertension
 Renal Denervation for Resistant Hypertension James W. Choi MD FACC FSCAI Cardiology Consultants of Texas Director Interventional Cardiology Fellowship Baylor University Medical Center Baylor Heart & Vascular
Renal Denervation for Resistant Hypertension James W. Choi MD FACC FSCAI Cardiology Consultants of Texas Director Interventional Cardiology Fellowship Baylor University Medical Center Baylor Heart & Vascular
Percutaneous Renal Denervation: A New Promise in the Treatment of RHT?
 BAD KROZINGEN Prof. T. Zeller, MD Bad Krozingen, Germany Percutaneous Renal Denervation: A New Promise in the Treatment of RHT? Potential conflicts of interest Speaker s name: Thomas Zeller X I have the
BAD KROZINGEN Prof. T. Zeller, MD Bad Krozingen, Germany Percutaneous Renal Denervation: A New Promise in the Treatment of RHT? Potential conflicts of interest Speaker s name: Thomas Zeller X I have the
Hypertension Pharmacotherapy: A Practical Approach
 Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets
 New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
CATHETER-BASED RENAL DENERVATION INCREASES INSULIN SENSITIVITY AND IMPROVES GLUCOSE METABOLISM IN PATIENTS WITH RESISTANT HYPERTENSION
 CATHETER-BASED RENAL DENERVATION INCREASES INSULIN SENSITIVITY AND IMPROVES GLUCOSE METABOLISM IN PATIENTS WITH RESISTANT HYPERTENSION F. Mahfoud, Ch. Ukena, B. Cremers, I. Kindermann, M. Kindermann, P.
CATHETER-BASED RENAL DENERVATION INCREASES INSULIN SENSITIVITY AND IMPROVES GLUCOSE METABOLISM IN PATIENTS WITH RESISTANT HYPERTENSION F. Mahfoud, Ch. Ukena, B. Cremers, I. Kindermann, M. Kindermann, P.
Stephen G. Worthley 1, Gerard T. Wilkins 2, Mark W. Webster 3,Joseph K. Montarello 1, Paul T. Antonis 4, Robert J. Whitbourn 5, Roderic J.
 Six Month Results of First-in-Human Sympathetic Renal Artery Denervation Using a Next Generation Multi-Electrode Renal Artery Denervation System in Patients with Drug-Resistant Hypertension Stephen G.
Six Month Results of First-in-Human Sympathetic Renal Artery Denervation Using a Next Generation Multi-Electrode Renal Artery Denervation System in Patients with Drug-Resistant Hypertension Stephen G.
Φαρµακευτική θεραπεία υπερτασικών ασθενών. Δ. Τσιαχρής, Καρδιολόγος, Α Πανεπιστηµαική Καρδιολογική Κλινική
 Φαρµακευτική θεραπεία υπερτασικών ασθενών Δ. Τσιαχρής, Καρδιολόγος, Α Πανεπιστηµαική Καρδιολογική Κλινική A 42-Year-Old Female with True Severe Resistant Hypertension Female, 42 years old, smoker BMI:
Φαρµακευτική θεραπεία υπερτασικών ασθενών Δ. Τσιαχρής, Καρδιολόγος, Α Πανεπιστηµαική Καρδιολογική Κλινική A 42-Year-Old Female with True Severe Resistant Hypertension Female, 42 years old, smoker BMI:
Hypertension Update. Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy
 Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, Financial Disclosures
 Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension
 Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
Best Therapy for Resistant Hypertension: The PATHWAY-2 2 Study
 Best Therapy for Resistant Hypertension: The PATHWAY-2 2 Study Antonio Coca MD, PhD, FRCP, FESC Council on Hypertension. European Society of Cardiology Hypertension and Vascular Risk Unit. Department of
Best Therapy for Resistant Hypertension: The PATHWAY-2 2 Study Antonio Coca MD, PhD, FRCP, FESC Council on Hypertension. European Society of Cardiology Hypertension and Vascular Risk Unit. Department of
Categories of HTN. Overview of Hypertension. Types of Hypertension
 Categories of HTN Overview of Hypertension Normal SBP 100 Quick review of the Basics: What is
Categories of HTN Overview of Hypertension Normal SBP 100 Quick review of the Basics: What is
The Evolution To Treatment Of Hypertension With Advanced Formulation
 The Evolution To Treatment Of Hypertension With Advanced Formulation Dr. Donald Ang MBChB (UK) FRCP (Edin) MD (UK) CCST Cardiology (UK) FESC (Europe) Consultant Cardiologist Island Hospital Penang High
The Evolution To Treatment Of Hypertension With Advanced Formulation Dr. Donald Ang MBChB (UK) FRCP (Edin) MD (UK) CCST Cardiology (UK) FESC (Europe) Consultant Cardiologist Island Hospital Penang High
Objectives. JNC 7 Is Nice But What s Up With JNC 8? Why Do We Care? Hypertension Background: Prevalence
 JNC 7 Is Nice But What s Up With JNC 8? 37 th Annual CAPA Conference October 4 th 2013 Ignacio de Artola, Jr. M.D. Assistant Professor of Clinical Family Medicine Medical Director, Primary Care Physician
JNC 7 Is Nice But What s Up With JNC 8? 37 th Annual CAPA Conference October 4 th 2013 Ignacio de Artola, Jr. M.D. Assistant Professor of Clinical Family Medicine Medical Director, Primary Care Physician
Christopher Valentine, MD
 Resistant Hypertension Christopher Valentine, MD Program Director, Nephrology Fellowship Program Department of Internal Medicine Division of Nephrology The Ohio State University Wexner Medical Center Disclosures
Resistant Hypertension Christopher Valentine, MD Program Director, Nephrology Fellowship Program Department of Internal Medicine Division of Nephrology The Ohio State University Wexner Medical Center Disclosures
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Renal Sympathetic Denervation Using an Irrigated Radiofrequency Ablation Catheter for the Management of Drug-Resistant Hypertension
 JACC: CARDIOVASCULAR INTERVENTIONS VOL. 5, NO. 7, 2012 2012 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 1936-8798/$36.00 PUBLISHED BY ELSEVIER INC. http://dx.doi.org/10.1016/j.jcin.2012.01.027
JACC: CARDIOVASCULAR INTERVENTIONS VOL. 5, NO. 7, 2012 2012 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 1936-8798/$36.00 PUBLISHED BY ELSEVIER INC. http://dx.doi.org/10.1016/j.jcin.2012.01.027
SPYRAL HTN ON MED. Disclosure
 Renal Denervation in the Presence of Antihypertensive Medications: Six-month Results from the Randomized, Blinded, Sham-controlled SPYRAL HTN-ON MED Trial Dr. David E. Kandzari Piedmont Heart Institute,
Renal Denervation in the Presence of Antihypertensive Medications: Six-month Results from the Randomized, Blinded, Sham-controlled SPYRAL HTN-ON MED Trial Dr. David E. Kandzari Piedmont Heart Institute,
Les techniques interventionnelles dans le traitement de l hypertension artérielle: faut-il y croire encore?
 Les techniques interventionnelles dans le traitement de l hypertension artérielle: faut-il y croire encore? Prof M Burnier Service de Néphrologie et Hypertension, CHUV, Lausanne Evian 2015 Approches non-médicamenteuses
Les techniques interventionnelles dans le traitement de l hypertension artérielle: faut-il y croire encore? Prof M Burnier Service de Néphrologie et Hypertension, CHUV, Lausanne Evian 2015 Approches non-médicamenteuses
Combination Therapy for Hypertension
 Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Transcatheter Renal Denervation and Hong Kong Experience
 Transcatheter Renal Denervation and Hong Kong Experience Dr. Steven Li Siu-lung FACC, FESC, FRCP, FACP Director, Heart Centre, Union Hospital President, Hong Kong Society of Congenital and Structural Heart
Transcatheter Renal Denervation and Hong Kong Experience Dr. Steven Li Siu-lung FACC, FESC, FRCP, FACP Director, Heart Centre, Union Hospital President, Hong Kong Society of Congenital and Structural Heart
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
STATE OF THE ART BP ASSESSMENT
 STATE OF THE ART BP ASSESSMENT PROFESSOR MOLECULAR PHARMACOLOGY CONWAY INSTITUE UNIVERSITY COLLEGE DUBLIN CO-CHAIRMAN BLOOD PRESCSURE MANAGEMENT IN LOW RESOURCE SETTINGS CENTRE FOR INTERNATIONAL HUMANITARIAN
STATE OF THE ART BP ASSESSMENT PROFESSOR MOLECULAR PHARMACOLOGY CONWAY INSTITUE UNIVERSITY COLLEGE DUBLIN CO-CHAIRMAN BLOOD PRESCSURE MANAGEMENT IN LOW RESOURCE SETTINGS CENTRE FOR INTERNATIONAL HUMANITARIAN
2017 CCS HF Guidelines Medical Therapy for HFrEF When What Order and How Much?
 2017 CCS HF Guidelines Medical Therapy for HFrEF When What Order and How Much? Dr. Shelley Zieroth University of Manitoba @ShelleyZieroth @CanHFSociety Disclosures Consulting/Advisory Board: Amgen, Astra
2017 CCS HF Guidelines Medical Therapy for HFrEF When What Order and How Much? Dr. Shelley Zieroth University of Manitoba @ShelleyZieroth @CanHFSociety Disclosures Consulting/Advisory Board: Amgen, Astra
Dr Diana R Holdright. MD, FRCP, FESC, FACC, MBBS, DA, BSc. Consultant Cardiologist HYPERTENSION.
 Dr Diana R Holdright MD, FRCP, FESC, FACC, MBBS, DA, BSc. Consultant Cardiologist HYPERTENSION www.drholdright.co.uk Blood pressure is the pressure exerted on the walls of the arteries when the heart pumps;
Dr Diana R Holdright MD, FRCP, FESC, FACC, MBBS, DA, BSc. Consultant Cardiologist HYPERTENSION www.drholdright.co.uk Blood pressure is the pressure exerted on the walls of the arteries when the heart pumps;
MPharmProgramme. Hypertension (HTN)
") MPharmProgramme Hypertension (HTN) Slide 1 of 30 Overview Definition Prevalence Type Causes Diagnosis Management Patients perspective Slide 2 of 30 Definition It is not a disease! So what is it? What two
MPharmProgramme Hypertension (HTN) Slide 1 of 30 Overview Definition Prevalence Type Causes Diagnosis Management Patients perspective Slide 2 of 30 Definition It is not a disease! So what is it? What two
Slide notes: References:
 1 2 3 Cut-off values for the definition of hypertension are systolic blood pressure (SBP) 135 and/or diastolic blood pressure (DBP) 85 mmhg for home blood pressure monitoring (HBPM) and daytime ambulatory
1 2 3 Cut-off values for the definition of hypertension are systolic blood pressure (SBP) 135 and/or diastolic blood pressure (DBP) 85 mmhg for home blood pressure monitoring (HBPM) and daytime ambulatory
Autumn Meeting Birmingham. Renal Denervation
 Autumn Meeting Birmingham Renal Denervation Andreas Baumbach, MD, FRCP, FESC Consultant Cardiologist, hon. Reader in Cardiology Bristol Heart Institute University Hospitals Bristol Renal Denervation BACKGROUND
Autumn Meeting Birmingham Renal Denervation Andreas Baumbach, MD, FRCP, FESC Consultant Cardiologist, hon. Reader in Cardiology Bristol Heart Institute University Hospitals Bristol Renal Denervation BACKGROUND
Hypertension Update 2009
 Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
COMPLEX HYPERTENSION. Anita Ralstin, FNP-BC Next Step Health Consultant, LLC
 COMPLEX HYPERTENSION Anita Ralstin, FNP-BC Next Step Health Consultant, LLC Incidence Of Hypertension About 70 million American adults have high blood pressure. About 33% of the population Only 52% have
COMPLEX HYPERTENSION Anita Ralstin, FNP-BC Next Step Health Consultant, LLC Incidence Of Hypertension About 70 million American adults have high blood pressure. About 33% of the population Only 52% have
5.2 Key priorities for implementation
 5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
NICE BHS Hypertension guidelines 2011 update
 NICE BHS Hypertension guidelines 2011 update Review for clinicians Sept 2011 Mark Thomas West Midlands Hypertension Centre Heart of England NHS Trust www.wmhc.co.uk mark.thomas@heartofengland.nhs.uk Full
NICE BHS Hypertension guidelines 2011 update Review for clinicians Sept 2011 Mark Thomas West Midlands Hypertension Centre Heart of England NHS Trust www.wmhc.co.uk mark.thomas@heartofengland.nhs.uk Full
2/11/2019 CLINICAL IMPLEMENTATION OF THE UPDATED BP GUIDELINES DUALITY OF INTEREST
 CLINICAL IMPLEMENTATION OF THE UPDATED BP GUIDELINES George L. Bakris, M.D.,F.A.S.N., F.A.H.A. Professor of Medicine Director, Am Heart Assoc. Comprehensive Hypertension Center University of Chicago Medicine
CLINICAL IMPLEMENTATION OF THE UPDATED BP GUIDELINES George L. Bakris, M.D.,F.A.S.N., F.A.H.A. Professor of Medicine Director, Am Heart Assoc. Comprehensive Hypertension Center University of Chicago Medicine
The American College of Cardiology (ACC) and American
 and American") Could it be PARADISE Found or is SYMPLICITY the Answer to the Treatment of Hypertension: The Resurrection of Renal Denervation to Treat Hypertension New Studies and Newer Options Richard R Heuser, MD and
Could it be PARADISE Found or is SYMPLICITY the Answer to the Treatment of Hypertension: The Resurrection of Renal Denervation to Treat Hypertension New Studies and Newer Options Richard R Heuser, MD and
Hypertension. Most important public health problem in developed countries
 Hypertension Strategy for Continued Success in Treatment for the 21st Century November 15, 2005 Arnold B. Meshkov, M.D. Associate Professor of Medicine Temple University School of Medicine Philadelphia,
Hypertension Strategy for Continued Success in Treatment for the 21st Century November 15, 2005 Arnold B. Meshkov, M.D. Associate Professor of Medicine Temple University School of Medicine Philadelphia,