The Petticoat Technique Managing Type B Dissection with both Early and Long Term Considerations
|
|
|
- Kristina Atkinson
- 5 years ago
- Views:
Transcription
1 The Petticoat Technique Managing Type B Dissection with both Early and Long Term Considerations Joseph V. Lombardi, MD Professor & Chief, Division of Vascular & Endovascular Surgery Department of Surgery, Cooper University Hospital Cooper Medical School of Rowan University 1
2 Disclosure Statement of Financial Interest Grant/Research Support Consulting Fees/Honoraria CookMedical Covidien Gore CookMedical
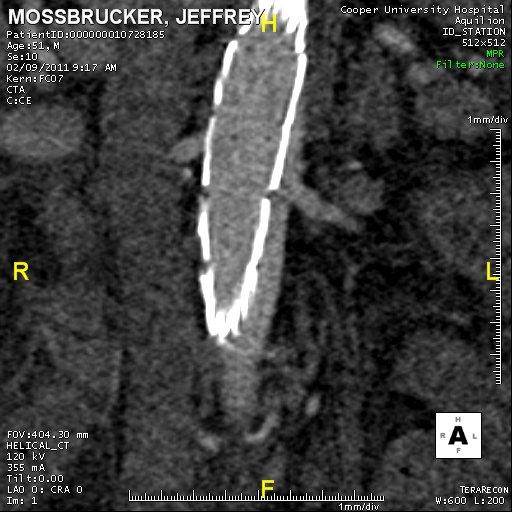
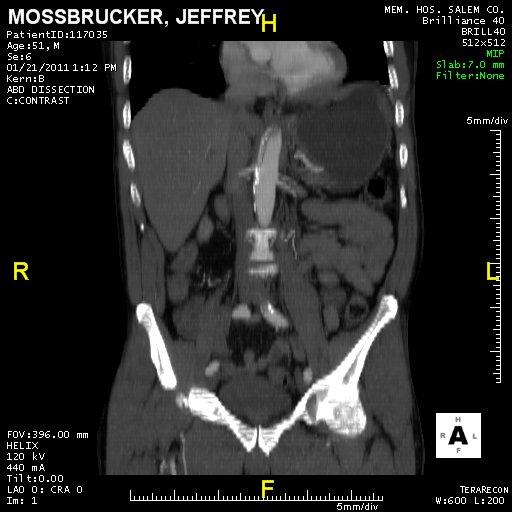
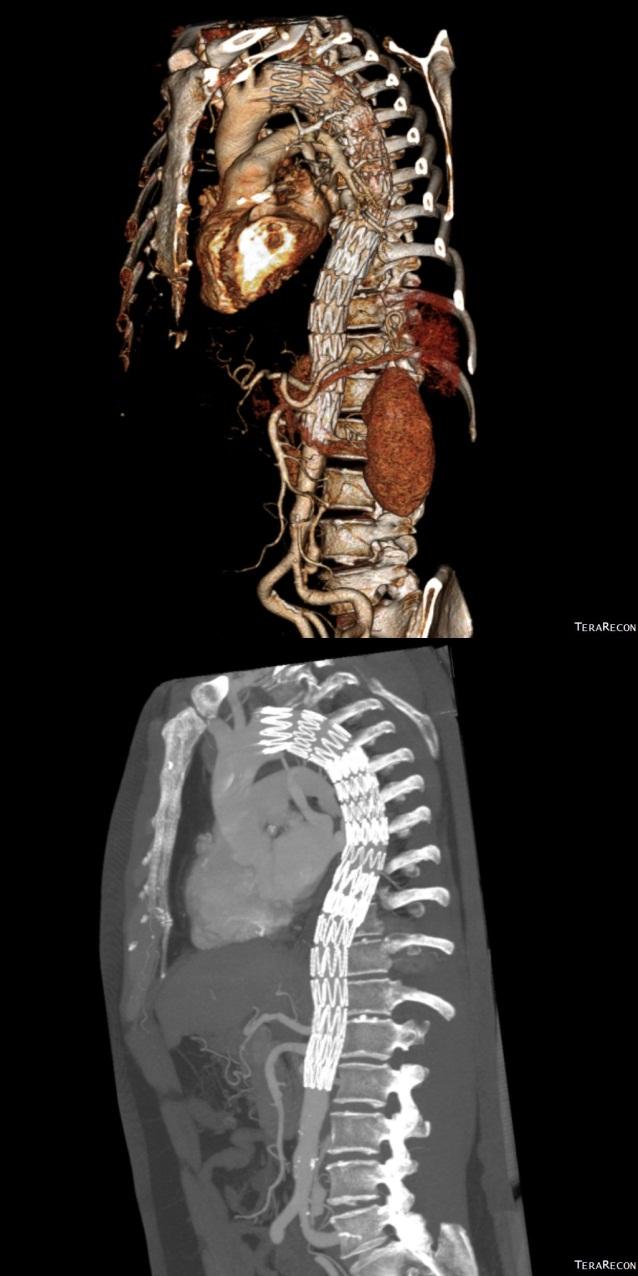
3 Case Presentation Acute Complicated TBAD 53 y/o with Tearing back pain X 4hours Severe HTN Renal failure Lower extremity ischemia
4
5
6

7 Courtesy of Terry Devine, Melbourne Australia Investigational device, limited by federal (U.S.A.) law to investigational use

8 Courtesy of Terry Devine, Melbourne Australia Investigational device, limited by federal (U.S.A.) law to investigational use

 law to")
9 Investigational device, limited by federal (U.S.A.) law to investigational use

10

11 Investigational device, limited by federal (U.S.A.) law to investigational use
12
13
14
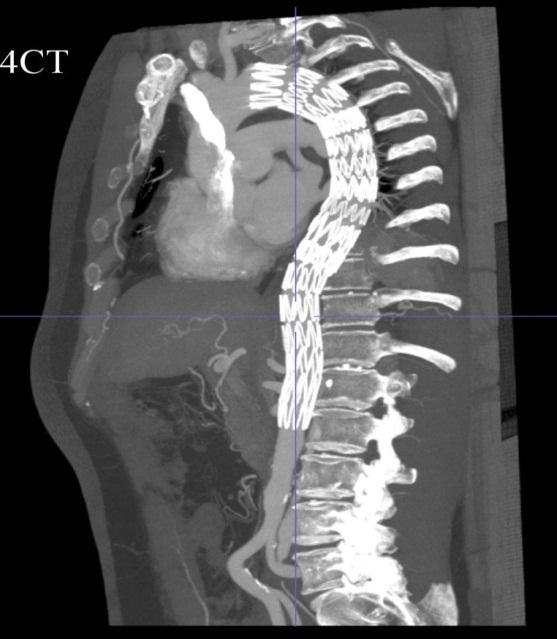
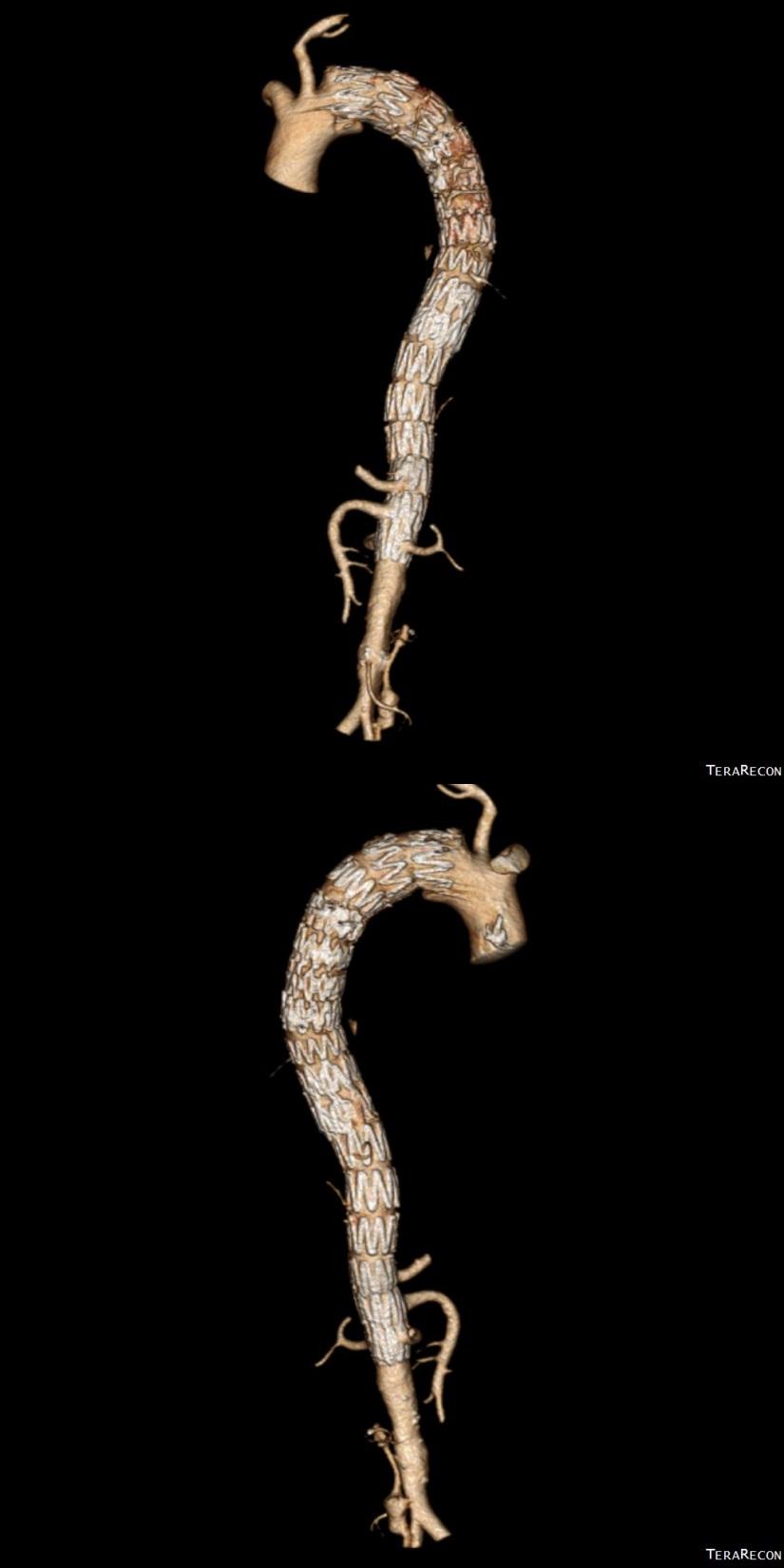
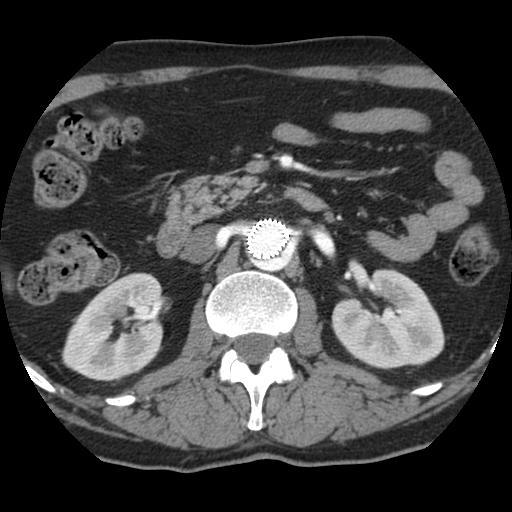
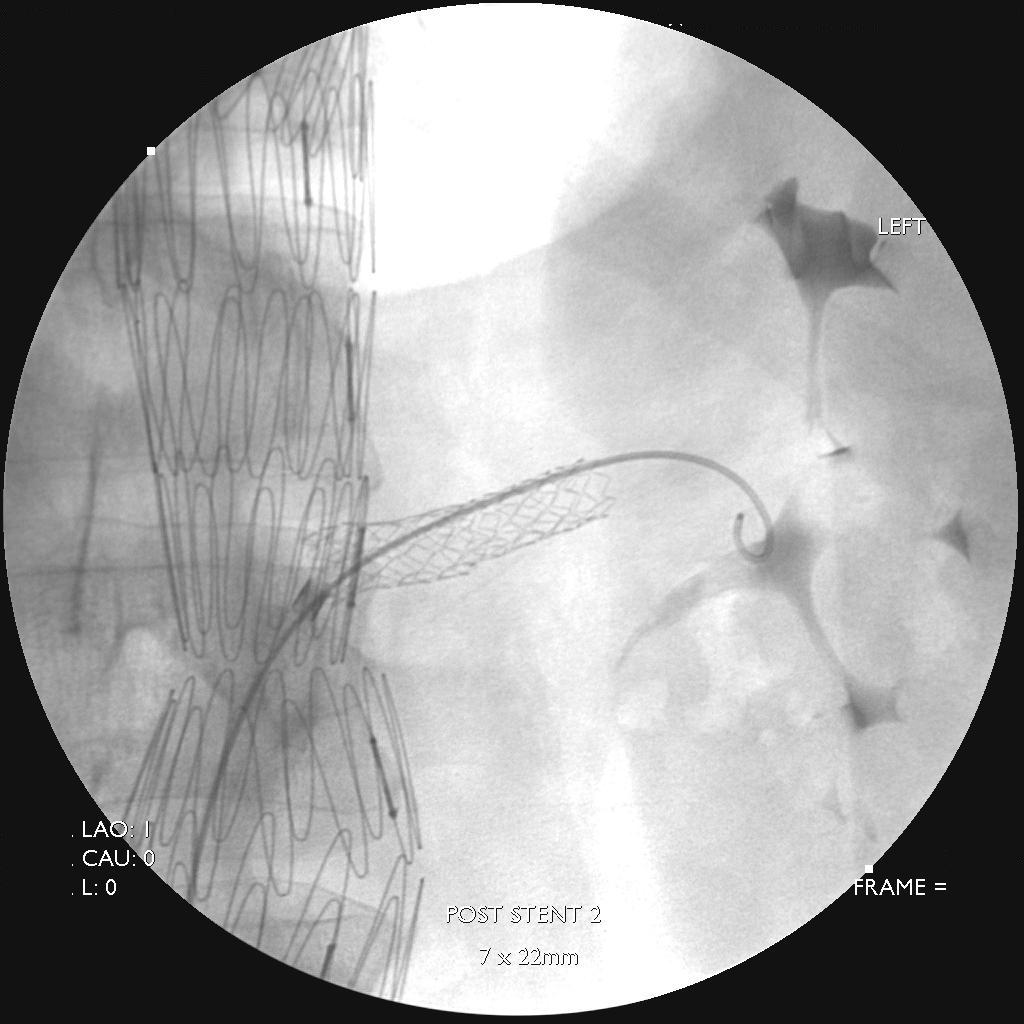
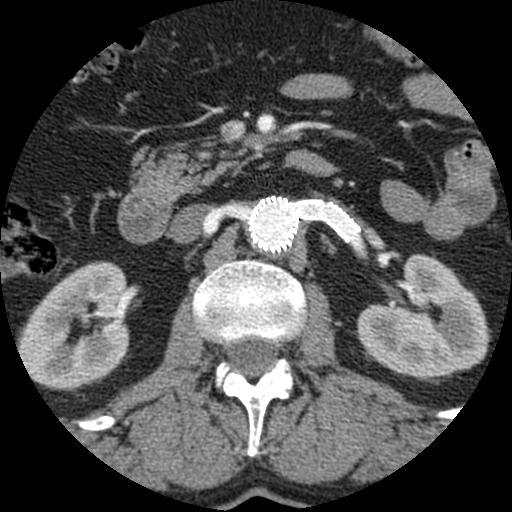
15 Bare Metal Stent Properties: Re-approximates delaminated intima Alleviate persistent Dynamic obstruction Reduces False lumen volume Expands True lumen volume Favorably positions pt for future intervention
16 Composite Device Design Complicated Dissection STABLE I Completed enrollment 86 pts 3 year data available Real world data STABLE II Enrollment Completed Device modification TX2: no proximal barbs Nitinol bare metal stent Enrollment eligibilty Malperfusion Rupture Acute (< 14 days)


17 Composite System Zenith TX2 Endovascular Graft Caution - Investigational device. Limited by Federal (or United States) law to investigational use. Zenith Dissection Endovascular Stent 17

18 STABLE I 2 Year follow-up 30 day mortality: 4.7% All cause mortality: 15% Positive aortic remodeling Acute phase treatment: Higher rate of: Stroke Retrograde dissection Aortic growth
19 STABLE I Study - Patients 86 patients (73% male; mean age 59 years) Type B aortic dissections warranting surgical intervention or not responding well to medical management All treated within 90 days of symptom onset Phase treated % (n/n) Mean time to treatment, days Acute (0-14 days) 64% (55/86) 4.2 ± 3.7 (0-14) Non-acute (15-90 days) 36% (31/86) 40.5 ± 22.5 (15-86) 19
20 STABLE I Study - Dissections Complicated Type B aortic dissections Inclusion criteria Acute, % (n/n) N = 55 Non-acute, % (n/n) N = 31 P value Branch vessel obstruction/compromise 69% (38/55) 58% (18/31).35 Peri-aortic effusion/hematoma 20% (11/55) 10% (3/31).36 Resistant hypertension 55% (30/55) 55% (17/31) >.99 Persistent pain/symptoms 82% (45/55) 65% (20/31).12 Transaortic growth 5 mm within 3 months (or transaortic diameter 40 mm) 35% (19/55) 74% (23/31) <.001 Dissection was extensive in most patients Extending below the diaphragm in 99% In or below common iliac arteries in 77% 20
 A majority of patients received only 1 TX2 component (79%) Successful device deployment in all patients, with 100% patency 21")
21 STABLE I Study - Devices TX2 TXD Dissection stent was placed in 93% of patients (6 patients did not receive a dissection stent at physician s discretion) A majority of patients received only 1 TX2 component (79%) Successful device deployment in all patients, with 100% patency 21
22 Mortality Within 30 Days 30-day mortality Acute dissection: 5.5% (3/55) Non-acute dissection: 3.2% (1/31) Overall group: 4.7% (4/86) Patient Days to death Cause of death Acute 5 Stroke Related Acute 11 Stroke Related Acute 11 Aortic rupture Related CEC adjudication of relationship to dissection repair Non-acute 29 Unknown Unable to determine 22
23 Acute Dissection: 30-Day Results Comparison to Literature 30-Day Event STABLE I Acute (N = 55) White 2011 Pooled SVS dataset Acute, complicated (N = 85) Fattori 2013 Pooled results on TEVAR Acute (N = 2,359) Mortality 5.5% (3/55) 10.6% (9/85) Stroke 10.9% (6/55) 9.4% (8/85) 10.2% 30-day or in-hospital mortality 4.9% 30-day or in-hospital stroke Paraplegia 1.8% (1/55) 9.4% (8/85) Paralysis/paraparesis 4.2% 30-day or in-hospital spinal cord ischemia Bowel ischemia 1.8% (1/55) 3.5% (3/85) Not reported Renal failure 10.9% (6/55) 9.4% (8/85) Not reported White et al. J Vasc Surg. 2011;53: Fattori et al. J Am Coll Cardiol. 2013;61:
24 Non-Acute Dissection: 30-Day Results Comparison to Literature 30-Day Event STABLE I Non-acute (15-90 days, N = 31) White 2011 Pooled SVS dataset Sub-acute/chronic (15-90 days, N = 14) Fattori 2013 Pooled results on TEVAR Chronic (>60 days, N = 1,098) Mortality 3.2% (1/31) 7.1% (1/14) Stroke 0% (0/31) 0% (0/14) 6.6% 30-day or in-hospital mortality 1.9% 30-day or in-hospital stroke Paraplegia 0% (0/31) Bowel ischemia 0% (0/14) Paralysis/paraparesis 1.5% 30-day or in-hospital spinal cord ischemia 0% (0/31) 0% (0/14) Not reported Renal failure 3.2% (1/31) 0% (0/14) Not reported White et al. J Vasc Surg. 2011;53: Fattori et al. J Am Coll Cardiol. 2013;61:
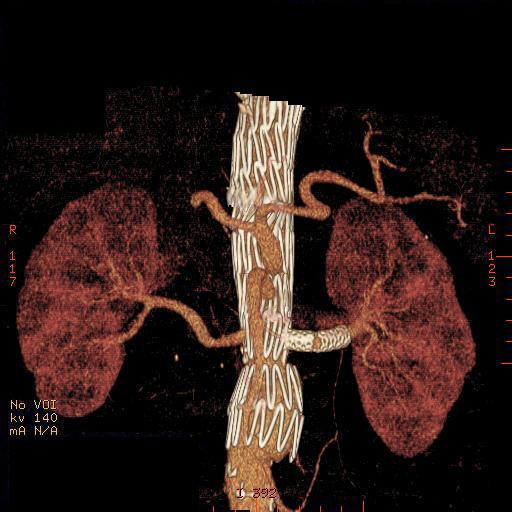
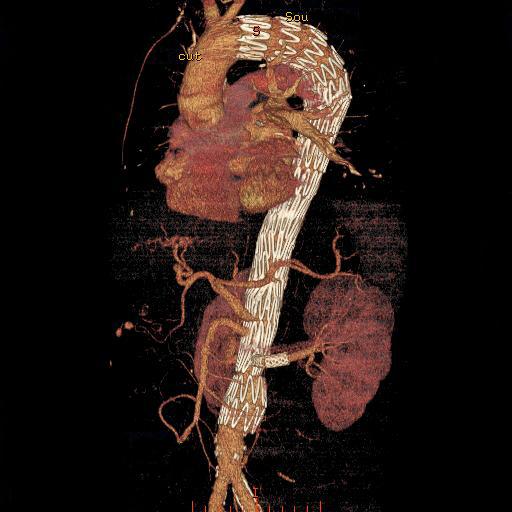
25 Aortic Remodeling Pre-procedure 24-month 48-month 48-month 25
26 False Lumen Thrombosis Descending thoracic aorta (down to the celiac artery) Complete thrombosis Pre-op 1-year 3-year Acute dissection: 0% 38% 53% Non-acute dissection: 0% 25% 40% No patent false lumen at 6 months and beyond Abdominal aorta Complete thrombosis Pre-op 1-year 3-year Acute dissection: 1.8% 12% 9.7% Non-acute dissection: 0% 4.2% 20% Patent false lumen: 58% (pre-procedure) to 4.3% (3 years) 26
27 Remodeling - Descending Thoracic Aorta Acute dissections (N = 55) Non-acute dissections (N = 31) Significant true lumen expansion and false lumen compression 27
28 Remodeling Abdominal Aorta Estimated changes in the true and false lumen diameters Acute dissections (N = 55) Non-acute dissections (N = 31) 28
29 Growth of Aorta Definition: Increase >5mm in the transaortic diameter compared to post-procedure (or 1-month if post-procedure measurement was not available) Largest diameter Time Acute Non-acute Descending thoracic aorta, % (n/n*) 1-year 29% (12/41) 4.0% (1/25) 2-year 37% (14/38) 14% (3/21) 3-year 29% (9/31) 13% (2/15) Largest diameter Time Acute Non-acute Abdominal aorta, % (n/n*) 1-year 29% (12/42) 8.0% (2/25) 2-year 51% (19/37) 9.5% (2/21) 3-year 47% (15/32) n/a *Number of patients with available CT images (with adequate quality) analyzed by the core laboratory 29
30 Aortic Growth after TEVAR Study Resch 2006 Sobocinski 2013 Fattori 2013 IRAD registry Dissections N = 74 (mixed acute and chronic) TEVAR (stent-graft alone) N = 52 (all acute) TEVAR (stent-graft alone) N = 276 (all acute) TEVAR Thoracic Aorta (> 5mm increase) Abdominal Aorta (> 5mm increase) 14% Not reported 25% at 1 year 33% at 12 months 28% at 1 year 33% at 2 years 63% at 5 years Lombardi 2013 STABLE Trial N = 86 acute and chronic TEVAR / Petticoat 29% at 1 year 37% at 2 years 29% at 3 years 29% at 1 year 51% at 2 years 47% at 3 years Brunkwall Adsorb trial 2014 N = 30 (acute uncomplicated) 1 year Not reported Resch et al. J Cardiovasc Surg (Torino). 2006;47: Sobocinski et al. Eur J Vasc Endovasc Surg. 2013;45:
31 Secondary Interventions Within 3 years in overall patient group: 29 secondary interventions in 23 patients: Persistent entry-flow or sealing of re-entry tear, n = 13 Malperfusion or ischemia, n = 5 Type A or retrograde dissection, n = 5 Aneurysm growth or degeneration, n = 5 Device migration, separation, or kink, n = 4 Aortic rupture, n = 2 31

32 Persistent False Lumen flow Patients treated ACUTE Setting % Future Growth Re-entry tears: Iliac Renal Celiac Management? Re-entry tear exclusion False lumen embolization


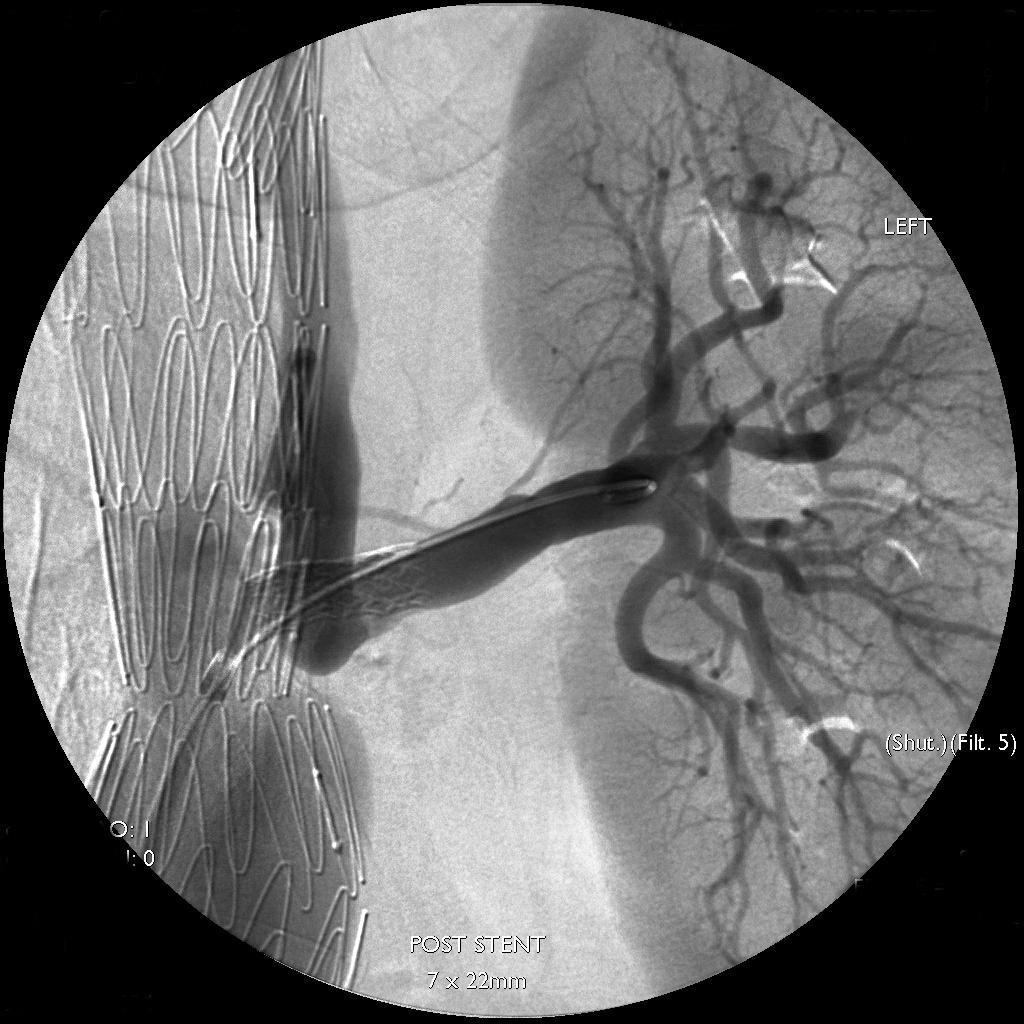
33 Adjunctive Stent Placement & Direct False Lumen Embolization

34
35
36

37
38

39
40

41
42
43
44
45 Conclusions Low 30-day mortality and paraplegia rates for petticoat technique using the Zenith dissection system. Aortic remodeling was observed within and beyond the stent-grafted segment, in both acute and non-acute dissections There exists a risk of aortic dilation, especially in dissections treated in the acute phase Management of ctabd is a long-term commitment 45
UC SF An Algorithm to Choose Which Uncomplicated (Asymptomatic) Acute Type B Dissection Patients Should Undergo TEVAR. Disclosures.
 Acute Type B Dissection Patients Should Undergo TEVAR. Disclosures.") An Algorithm to Choose Which Uncomplicated (Asymptomatic) Acute Type B Dissection Patients Should Undergo TEVAR Disclosures Royalties and research grant support from Cook Medical, Inc. Jade S. Hiramoto,
An Algorithm to Choose Which Uncomplicated (Asymptomatic) Acute Type B Dissection Patients Should Undergo TEVAR Disclosures Royalties and research grant support from Cook Medical, Inc. Jade S. Hiramoto,
UC SF. Disclosures. Thoracic Endovascular Aortic Repair 4/24/2009. Management of Acute Dissections: Is There Still a Role for Open Surgery?
 UC SF Management of Acute Dissections: Is There Still a Role for Open Surgery? Darren B. Schneider, M.D. Assistant Professor of Surgery and Radiology Division of Vascular Surgery University of California
UC SF Management of Acute Dissections: Is There Still a Role for Open Surgery? Darren B. Schneider, M.D. Assistant Professor of Surgery and Radiology Division of Vascular Surgery University of California
Clinical Trials of Acute and Chronic Dissections. Gregory Landry MD
 Clinical Trials of Acute and Chronic Dissections Gregory Landry MD No disclosures Acute vs chronic dissection: Definitions 1950s: Acute < 2 weeks, Chronic > 2 weeks 2013: European Interdisciplinary Consensus
Clinical Trials of Acute and Chronic Dissections Gregory Landry MD No disclosures Acute vs chronic dissection: Definitions 1950s: Acute < 2 weeks, Chronic > 2 weeks 2013: European Interdisciplinary Consensus
Is there a way to predict the risk in uncomplicated Type B aortic dissections? FRANS MOLL University Medical Centre Utrecht - Netherlands
 Is there a way to predict the risk in uncomplicated Type B aortic dissections? FRANS MOLL University Medical Centre Utrecht - Netherlands Disclosures: - Consultant Philips Health Care - Best Doctors Overview
Is there a way to predict the risk in uncomplicated Type B aortic dissections? FRANS MOLL University Medical Centre Utrecht - Netherlands Disclosures: - Consultant Philips Health Care - Best Doctors Overview
UC SF Early Intervention in Type B Dissection: Results From the INSTEAD XL Trial. Acute Type B Dissection. Outline. Disclosures.
 Early Intervention in Type B Dissection: Results From the INSTEAD XL Trial None Disclosures Jade S. Hiramoto, MD, MAS April 4, 2014 Outline Background Current treatment Results from INSTEAD trial Results
Early Intervention in Type B Dissection: Results From the INSTEAD XL Trial None Disclosures Jade S. Hiramoto, MD, MAS April 4, 2014 Outline Background Current treatment Results from INSTEAD trial Results
Total endovascular techniques utilization in aortic dissection radical treatment
 Total endovascular techniques utilization in aortic dissection radical treatment Chang Shu, MD, PhD Vascular Surgery Center National Center for Cardiovascular Diseases. Fuwai Hospital, CAMS & PUMC Beijing,
Total endovascular techniques utilization in aortic dissection radical treatment Chang Shu, MD, PhD Vascular Surgery Center National Center for Cardiovascular Diseases. Fuwai Hospital, CAMS & PUMC Beijing,
Performance of the conformable GORE TAG device in Type B aortic dissection from the GORE GREAT real world registry
 University of Milan Thoracic Aortic Research Center Performance of the conformable GORE TAG device in Type B aortic dissection from the GORE GREAT real world registry Santi Trimarchi, MD, PhD Associate
University of Milan Thoracic Aortic Research Center Performance of the conformable GORE TAG device in Type B aortic dissection from the GORE GREAT real world registry Santi Trimarchi, MD, PhD Associate
Type B Dissection Sub-Categories
 Disclosure Nothing to disclose Type B Dissection On Whom to Operate on and When to do it Charles Eichler Professor, Department of Surgery Division of Vascular and Endovascular Surgery University of California
Disclosure Nothing to disclose Type B Dissection On Whom to Operate on and When to do it Charles Eichler Professor, Department of Surgery Division of Vascular and Endovascular Surgery University of California
Malperfusion Syndromes Type B Aortic Dissection with Malperfusion
 Malperfusion Syndromes Type B Aortic Dissection with Malperfusion Jade S. Hiramoto, MD, MAS April 27, 2012 Associated with early mortality Occurs when there is end organ ischemia secondary to aortic branch
Malperfusion Syndromes Type B Aortic Dissection with Malperfusion Jade S. Hiramoto, MD, MAS April 27, 2012 Associated with early mortality Occurs when there is end organ ischemia secondary to aortic branch
Do the Data Support Endovascular Therapy for Descending Thoracic AD? Woong Chol Kang, M.D.
 Do the Data Support Endovascular Therapy for Descending Thoracic AD? Woong Chol Kang, M.D. Gil Hospital, Gachon University Incheon, Korea Classification of AD Acute vs. Chronic (2weeks) (IIIa, b) type
Do the Data Support Endovascular Therapy for Descending Thoracic AD? Woong Chol Kang, M.D. Gil Hospital, Gachon University Incheon, Korea Classification of AD Acute vs. Chronic (2weeks) (IIIa, b) type
Animesh Rathore, MD 4/22/17. The Great Debate 45yo Man With Uncomplicated Acute TBAD: The Case For Medical Management
 Animesh Rathore, MD 4/22/17 The Great Debate 45yo Man With Uncomplicated Acute TBAD: The Case For Medical Management Disclosures Just a young vascular surgeon who would like to keep his job My opponent
Animesh Rathore, MD 4/22/17 The Great Debate 45yo Man With Uncomplicated Acute TBAD: The Case For Medical Management Disclosures Just a young vascular surgeon who would like to keep his job My opponent
Optimal Treatment of Chronic Dissection
 Optimal Treatment of Chronic Dissection Chun-Che Shih 施俊哲 MD, Ph.D. Chief, Professor Institute of Clinical Medicine National Yang Ming University Division of Cardiovascular Surgery Taipei Veterans General
Optimal Treatment of Chronic Dissection Chun-Che Shih 施俊哲 MD, Ph.D. Chief, Professor Institute of Clinical Medicine National Yang Ming University Division of Cardiovascular Surgery Taipei Veterans General
Combined Endovascular and Surgical Repair of Thoracoabdominal Aortic Pathology: Hybrid TEVAR
 Combined Endovascular and Surgical Repair of Thoracoabdominal Aortic Pathology: Hybrid TEVAR William J. Quinones-Baldrich MD Professor of Surgery Director UCLA Aortic Center UCLA Medical Center Los Angeles,
Combined Endovascular and Surgical Repair of Thoracoabdominal Aortic Pathology: Hybrid TEVAR William J. Quinones-Baldrich MD Professor of Surgery Director UCLA Aortic Center UCLA Medical Center Los Angeles,
Acute dissections of the descending thoracic aorta (Debakey
 Endovascular Treatment of Acute Descending Thoracic Aortic Dissections Nimesh D. Desai, MD, PhD, and Joseph E. Bavaria, MD Acute dissections of the descending thoracic aorta (Debakey type III or Stanford
Endovascular Treatment of Acute Descending Thoracic Aortic Dissections Nimesh D. Desai, MD, PhD, and Joseph E. Bavaria, MD Acute dissections of the descending thoracic aorta (Debakey type III or Stanford
Acute Type B dissection. Closure of the infra diaphragmatic tear: how and when?
 Acute Type B dissection. Closure of the infra diaphragmatic tear: how and when? Prof. Olgierd Rowiński II Department of Clinical Radiology Medical University of Warsaw Disclosure Speaker name: Olgierd
Acute Type B dissection. Closure of the infra diaphragmatic tear: how and when? Prof. Olgierd Rowiński II Department of Clinical Radiology Medical University of Warsaw Disclosure Speaker name: Olgierd
I-Hui Wu, M.D. Ph.D. Clinical Assistant Professor Cardiovascular Surgical Department National Taiwan University Hospital
 Comparisons of Aortic Remodeling and Outcomes after Endovascular Repair of Acute and Chronic Complicated Type B Aortic Dissections I-Hui Wu, M.D. Ph.D. Clinical Assistant Professor Cardiovascular Surgical
Comparisons of Aortic Remodeling and Outcomes after Endovascular Repair of Acute and Chronic Complicated Type B Aortic Dissections I-Hui Wu, M.D. Ph.D. Clinical Assistant Professor Cardiovascular Surgical
Dissection de type B: l étude Instead et corollaire stratégique
 Dissection de type B: l étude Instead et corollaire stratégique Christoph A. Nienaber, MD, FACC University Rostock Heartcenter Med. Clinic I Cardiology christoph.nienaber@med.uni-rostock.de Type B aortic
Dissection de type B: l étude Instead et corollaire stratégique Christoph A. Nienaber, MD, FACC University Rostock Heartcenter Med. Clinic I Cardiology christoph.nienaber@med.uni-rostock.de Type B aortic
CT angiography in type I acute aortic dissection complicated with malperfusion - a visual review of obstruciton patterns
 CT angiography in type I acute aortic dissection complicated with malperfusion - a visual review of obstruciton patterns Eneva M. St. Ekaterna University Hospital Report objectives 1. Review malperfusion
CT angiography in type I acute aortic dissection complicated with malperfusion - a visual review of obstruciton patterns Eneva M. St. Ekaterna University Hospital Report objectives 1. Review malperfusion
Pioneering EVAR techniques in aortic dissection
 Pioneering EVAR techniques in aortic dissection Jianing Yue, Weiguo Fu Department of Vascular Surgery Zhongshan Hospital Fudan University Shanghai, China LINC Asia-Pacific 2016 March 8-10, 2016 Hong Kong
Pioneering EVAR techniques in aortic dissection Jianing Yue, Weiguo Fu Department of Vascular Surgery Zhongshan Hospital Fudan University Shanghai, China LINC Asia-Pacific 2016 March 8-10, 2016 Hong Kong
Acute dissections: who should we treat, and how?
 Acute dissections: who should we treat, and how? J Sobocinski, R Azzaoui, B Maurel, R Spear, T Martin-Gonzalez, A Hertault, S Haulon Centre de l Aorte, Chirurgie vasculaire, Hôpital Cardiologique, CHRU
Acute dissections: who should we treat, and how? J Sobocinski, R Azzaoui, B Maurel, R Spear, T Martin-Gonzalez, A Hertault, S Haulon Centre de l Aorte, Chirurgie vasculaire, Hôpital Cardiologique, CHRU
Treatment of acute type B aortic dissection: Current status
 MEET Cannes, 18. - 21.06.2009 Treatment of acute type B aortic dissection: Current status Christoph A. Nienaber, MD, FACC University of Rostock Department of Internal Medicine, Cardiology christoph.nienaber@med.uni-rostock.de
MEET Cannes, 18. - 21.06.2009 Treatment of acute type B aortic dissection: Current status Christoph A. Nienaber, MD, FACC University of Rostock Department of Internal Medicine, Cardiology christoph.nienaber@med.uni-rostock.de
Is a Paradigm Shift towards Early Endovascular Treatment of Type B Dissection justified?
 Is a Paradigm Shift towards Early Endovascular Treatment of Type B Dissection justified? Dittmar Böckler Department of Vascular and Endovascular Surgery University of Heidelberg, Germany Disclosure Speaker
Is a Paradigm Shift towards Early Endovascular Treatment of Type B Dissection justified? Dittmar Böckler Department of Vascular and Endovascular Surgery University of Heidelberg, Germany Disclosure Speaker
No Disclosure. Aortic Dissection in Japan. This. The Challenge of Acute and Chronic Type B Aortic Dissections with Endovascular Aortic Repair
 No Disclosure The Challenge of Acute and Chronic Type B Aortic Dissections with Endovascular Aortic Repair Toru Kuratani Department of Cardiovascular Surgery Osaka University Graduate School of Medicine,
No Disclosure The Challenge of Acute and Chronic Type B Aortic Dissections with Endovascular Aortic Repair Toru Kuratani Department of Cardiovascular Surgery Osaka University Graduate School of Medicine,
Are stent-grafts for acute type B dissection durable? Est-ce que les stents graft pour la dissection aigue de type B sont efficaces à moyen terme?
 Are stent-grafts for acute type B dissection durable? Est-ce que les stents graft pour la dissection aigue de type B sont efficaces à moyen terme? Martin Björck, Johnny Steuer, Anders Wanhainen Uppsala
Are stent-grafts for acute type B dissection durable? Est-ce que les stents graft pour la dissection aigue de type B sont efficaces à moyen terme? Martin Björck, Johnny Steuer, Anders Wanhainen Uppsala
ADSORB trial results: Is it enough to switch the paradigm?
 ADSORB trial results: Is it enough to switch the paradigm? Jan Brunkwall, MD, PhD Professor and Chairman Complications to acute type B dissection Mortality Rupture Organ Ischemia Dilatation/Aneurysm Refractory
ADSORB trial results: Is it enough to switch the paradigm? Jan Brunkwall, MD, PhD Professor and Chairman Complications to acute type B dissection Mortality Rupture Organ Ischemia Dilatation/Aneurysm Refractory
What is the best treatment for False Lumen growth after type B Dissection
 What is the best treatment for False Lumen growth after type B Dissection Nikolaos Tsilimparis, Fiona Rohlffs, Yuk Law, Sebastian Debus, Tilo Kölbel N. Tsilimparis, MD, PhD, FEBVS Deputy Head of German
What is the best treatment for False Lumen growth after type B Dissection Nikolaos Tsilimparis, Fiona Rohlffs, Yuk Law, Sebastian Debus, Tilo Kölbel N. Tsilimparis, MD, PhD, FEBVS Deputy Head of German
Endovascular Management of Thoracic Aortic Pathology Stéphan Haulon, J Sobocinski, B Maurel, T Martin-Gonzalez, R Spear, A Hertault, R Azzaoui
 Endovascular Management of Thoracic Aortic Pathology Stéphan Haulon, J Sobocinski, B Maurel, T Martin-Gonzalez, R Spear, A Hertault, R Azzaoui Aortic Center, Lille University Hospital, France Disclosures
Endovascular Management of Thoracic Aortic Pathology Stéphan Haulon, J Sobocinski, B Maurel, T Martin-Gonzalez, R Spear, A Hertault, R Azzaoui Aortic Center, Lille University Hospital, France Disclosures
Understanding the Predictors of Aneurysmal Degeneration in Type B Dissection
 Understanding the Predictors of Aneurysmal Degeneration in Type B Dissection A case example illustrating when early endovascular intervention may provide the best outcome. BY DITTMAR BÖCKLER, MD, PhD;
Understanding the Predictors of Aneurysmal Degeneration in Type B Dissection A case example illustrating when early endovascular intervention may provide the best outcome. BY DITTMAR BÖCKLER, MD, PhD;
Optimal repair of acute aortic dissection
 Optimal repair of acute aortic dissection Dept. of Vascular Surgery, The 2nd Xiang-Yale Hospital, Central-South University, China Hunan Major Vessels Diseases Clinical Center Chang Shu Email:changshu01@yahoo.com
Optimal repair of acute aortic dissection Dept. of Vascular Surgery, The 2nd Xiang-Yale Hospital, Central-South University, China Hunan Major Vessels Diseases Clinical Center Chang Shu Email:changshu01@yahoo.com
TEVAR for Chronic dissections: indications for TEVAR, long term results
 TEVAR for Chronic dissections: indications for TEVAR, long term results J Sobocinski, R Azzaoui, B Maurel, R Spear, T Martin-Gonzalez, A Hertault, S Haulon Centre de l Aorte, Chirurgie vasculaire, Hôpital
TEVAR for Chronic dissections: indications for TEVAR, long term results J Sobocinski, R Azzaoui, B Maurel, R Spear, T Martin-Gonzalez, A Hertault, S Haulon Centre de l Aorte, Chirurgie vasculaire, Hôpital
Global Evidence for the Treatment of Type B Aortic Dissection
 Global Evidence for the Treatment of Type B Aortic Dissection Ross Milner, MD Professor of Surgery Director, Center for Aortic Diseases September 17, 2016 Disclosures Consultant Cook, Endospan, Medtronic,
Global Evidence for the Treatment of Type B Aortic Dissection Ross Milner, MD Professor of Surgery Director, Center for Aortic Diseases September 17, 2016 Disclosures Consultant Cook, Endospan, Medtronic,
Endovascular therapy for Ischemic versus Nonischemic complicated acute type B aortic dissection (catbad).
.") Endovascular therapy for Ischemic versus Nonischemic complicated acute type B aortic dissection (catbad). AS. Eleshra, MD 1, T. Kölbel, MD, PhD 1, F. Rohlffs, MD 1, N. Tsilimparis, MD, PhD 1,2 Ahmed Eleshra
Endovascular therapy for Ischemic versus Nonischemic complicated acute type B aortic dissection (catbad). AS. Eleshra, MD 1, T. Kölbel, MD, PhD 1, F. Rohlffs, MD 1, N. Tsilimparis, MD, PhD 1,2 Ahmed Eleshra
Indications for stent grafts in type B aortic dissection
 expert opinion I Akin C A Nienaber Indications for stent grafts in type B aortic dissection ibrahim akin christoph a nienaber Department of Medicine, Divisions of Cardiology, Pulmology and Intensive Care
expert opinion I Akin C A Nienaber Indications for stent grafts in type B aortic dissection ibrahim akin christoph a nienaber Department of Medicine, Divisions of Cardiology, Pulmology and Intensive Care
F. Terzi, S. Gianstefani, R. Fattori. cardiology and interventional cardiology unit, ospedali riuniti Marche nord, pesaro.
 14_14 03/02/17 14.16 Pagina 101 Type B aortic dissection: it should Be TreaTed F. Terzi, S. Gianstefani, R. Fattori cardiology and interventional cardiology unit, ospedali riuniti Marche nord, pesaro.
14_14 03/02/17 14.16 Pagina 101 Type B aortic dissection: it should Be TreaTed F. Terzi, S. Gianstefani, R. Fattori cardiology and interventional cardiology unit, ospedali riuniti Marche nord, pesaro.
Aggressive Resection/Reconstruction of the Aortic Arch in Type A Dissection
 Aggressive Resection/Reconstruction of the Aortic Arch in Type A Dissection M. Grabenwoger Dept. of Cardiovascular Surgery Hospital Hietzing Vienna, Austria Disclosure Statement Consultant of Jotec, Hechingen,
Aggressive Resection/Reconstruction of the Aortic Arch in Type A Dissection M. Grabenwoger Dept. of Cardiovascular Surgery Hospital Hietzing Vienna, Austria Disclosure Statement Consultant of Jotec, Hechingen,
Residual Dissection and False Lumen Aneurysm After TEVAR
 WHAT WOULD YOU DO? Residual Dissection and False Lumen Aneurysm After MODERATOR: MARK FARBER, MD PANEL: YAZAN DUWAYRI, MD; MATTHEW J. EAGLETON, MD; WILLIAM D. JORDAN Jr, MD; TILO KÖLBEL, MD, PhD; AND ERIC
WHAT WOULD YOU DO? Residual Dissection and False Lumen Aneurysm After MODERATOR: MARK FARBER, MD PANEL: YAZAN DUWAYRI, MD; MATTHEW J. EAGLETON, MD; WILLIAM D. JORDAN Jr, MD; TILO KÖLBEL, MD, PhD; AND ERIC
Nellix Endovascular System: Clinical Outcomes and Device Overview
 Nellix Endovascular System: Clinical Outcomes and Device Overview Jeffrey P. Carpenter, MD Professor and Chief, Department of Surgery CAUTION: Investigational device. This product is under clinical investigation
Nellix Endovascular System: Clinical Outcomes and Device Overview Jeffrey P. Carpenter, MD Professor and Chief, Department of Surgery CAUTION: Investigational device. This product is under clinical investigation
Evaluation of Dynamic Intimal Flap Movement in Acute Stanford Type B Aortic Dissections (ATBD) and the Effects of Thoracic Endovascular Stent Grafting
 and the Effects of Thoracic Endovascular Stent Grafting") Evaluation of Dynamic Intimal Flap Movement in Acute Stanford Type B Aortic Dissections (ATBD) and the Effects of Thoracic Endovascular Stent Grafting Frank R. Arko, III, MD, Jeko Madjarov, MD, Aaron Hurd,
Evaluation of Dynamic Intimal Flap Movement in Acute Stanford Type B Aortic Dissections (ATBD) and the Effects of Thoracic Endovascular Stent Grafting Frank R. Arko, III, MD, Jeko Madjarov, MD, Aaron Hurd,
Management of Acute Aortic Syndromes. M. Grabenwoger, MD Dept. of Cardiovascular Surgery Hospital Hietzing, Vienna, Austria
 Management of Acute Aortic Syndromes M. Grabenwoger, MD Dept. of Cardiovascular Surgery Hospital Hietzing, Vienna, Austria I have nothing to disclose. Acute Aortic Syndromes Acute Aortic Dissection Type
Management of Acute Aortic Syndromes M. Grabenwoger, MD Dept. of Cardiovascular Surgery Hospital Hietzing, Vienna, Austria I have nothing to disclose. Acute Aortic Syndromes Acute Aortic Dissection Type
Indications for use. Contraindications within the United States
 Indications for use Indications within the United States The GORE TAG Thoracic Endoprosthesis is intended for endovascular repair of all lesions of the descending thoracic aorta, including: Isolated lesions
Indications for use Indications within the United States The GORE TAG Thoracic Endoprosthesis is intended for endovascular repair of all lesions of the descending thoracic aorta, including: Isolated lesions
Total Endovascular Repair Type A Dissection. Eric Herget Interventional Radiology
 Total Endovascular Repair Type A Dissection Eric Herget Interventional Radiology 65 year old male Acute Type A Dissection Severe Aortic Regurgitation No co-morbidities Management? Part II Evolving Global
Total Endovascular Repair Type A Dissection Eric Herget Interventional Radiology 65 year old male Acute Type A Dissection Severe Aortic Regurgitation No co-morbidities Management? Part II Evolving Global
Endovascular Treatment of Malperfusion Syndrome
 Endovascular Treatment of Malperfusion Syndrome in Type B Aortic Dissection Department of Cardiology, Pusan National luniveristy i Hospital, Han Cheol Lee Endovascular Treatment Indication of Type B Aortic
Endovascular Treatment of Malperfusion Syndrome in Type B Aortic Dissection Department of Cardiology, Pusan National luniveristy i Hospital, Han Cheol Lee Endovascular Treatment Indication of Type B Aortic
Introducing the GORE TAG Conformable Thoracic Stent Graft with ACTIVE CONTROL System
 Introducing the GORE TAG Conformable Thoracic Stent Graft with ACTIVE CONTROL System K. Oikonomou Department of Vascular Surgery Regensburg University Disclosures W.L. Gore & Associates Sponsored Presentation
Introducing the GORE TAG Conformable Thoracic Stent Graft with ACTIVE CONTROL System K. Oikonomou Department of Vascular Surgery Regensburg University Disclosures W.L. Gore & Associates Sponsored Presentation
Abdominal and thoracic aneurysm repair
 Abdominal and thoracic aneurysm repair William A. Gray MD Director, Endovascular Intervention Cardiovascular Research Foundation Columbia University Medical Center Abdominal Aortic Aneurysm Endografts
Abdominal and thoracic aneurysm repair William A. Gray MD Director, Endovascular Intervention Cardiovascular Research Foundation Columbia University Medical Center Abdominal Aortic Aneurysm Endografts
Development of Stent Graft. Kato et al. Development of an expandable intra-aortic prothesis for experimental aortic dissection.
 Development of Stent Graft Kato et al. Development of an expandable intra-aortic prothesis for experimental aortic dissection. ASAIO J 1993 The New England Journal of Medicine Downloaded from nejm.org
Development of Stent Graft Kato et al. Development of an expandable intra-aortic prothesis for experimental aortic dissection. ASAIO J 1993 The New England Journal of Medicine Downloaded from nejm.org
RETROGRADE BRANCH. Gustavo S. Oderich MD Professor of Surgery Director of Endovascular Therapy Division of Vascular and Endovascular Surgery
 RETROGRADE BRANCH Gustavo S. Oderich MD Professor of Surgery Director of Endovascular Therapy Division of Vascular and Endovascular Surgery FACULTY DISCLOSURE Consulting* Cook Medical Inc., WL Gore Research
RETROGRADE BRANCH Gustavo S. Oderich MD Professor of Surgery Director of Endovascular Therapy Division of Vascular and Endovascular Surgery FACULTY DISCLOSURE Consulting* Cook Medical Inc., WL Gore Research
Percutaneous Approaches to Aortic Disease in 2018
 Percutaneous Approaches to Aortic Disease in 2018 Wendy Tsang, MD, SM Assistant Professor, University of Toronto Toronto General Hospital, University Health Network Case 78 year old F Lower CP and upper
Percutaneous Approaches to Aortic Disease in 2018 Wendy Tsang, MD, SM Assistant Professor, University of Toronto Toronto General Hospital, University Health Network Case 78 year old F Lower CP and upper
Ovation. Sean Lyden, MD Department Chair, Vascular Surgery Cleveland Clinic
 Ovation Sean Lyden, MD Department Chair, Vascular Surgery Cleveland Clinic Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement
Ovation Sean Lyden, MD Department Chair, Vascular Surgery Cleveland Clinic Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement
The role of false lumen intervention to promote remodelling via induced thrombosis the FLIRT concept
 The role of false lumen intervention to promote remodelling via induced thrombosis the FLIRT concept Professor Christoph A. Nienaber The Royal Brompton and Harefield NHS Trust Cardiology and Aortic Centre
The role of false lumen intervention to promote remodelling via induced thrombosis the FLIRT concept Professor Christoph A. Nienaber The Royal Brompton and Harefield NHS Trust Cardiology and Aortic Centre
Santi Trimarchi, MD, PhD Vascular Surgeon Thoracic Aortic Research Center, Director IRCCS Policlinico San Donato University of Milan
 The Gore GREAT Registry: Update about a real life data collection Santi Trimarchi, MD, PhD Vascular Surgeon Thoracic Aortic Research Center, Director IRCCS Policlinico San Donato University of Milan Disclosures
The Gore GREAT Registry: Update about a real life data collection Santi Trimarchi, MD, PhD Vascular Surgeon Thoracic Aortic Research Center, Director IRCCS Policlinico San Donato University of Milan Disclosures
La sindrome aortica acuta oggi
 University of Milan Thoracic Aortic Research Center La sindrome aortica acuta oggi Santi Trimarchi, MD, PhD Professore Associato di Chirurgia Vascolare, Università degli Studi di Milano Direttore, Divisione
University of Milan Thoracic Aortic Research Center La sindrome aortica acuta oggi Santi Trimarchi, MD, PhD Professore Associato di Chirurgia Vascolare, Università degli Studi di Milano Direttore, Divisione
Development of a Branched LSA Endograft & Ascending Aorta Endograft
 Development of a Branched LSA Endograft & Ascending Aorta Endograft Frank R. Arko III, MD Sanger Heart & Vascular Institute Carolinas Medical Center Charlotte, North Carolina, USA Disclosures Proximal
Development of a Branched LSA Endograft & Ascending Aorta Endograft Frank R. Arko III, MD Sanger Heart & Vascular Institute Carolinas Medical Center Charlotte, North Carolina, USA Disclosures Proximal
Antegrade Thoracic Stent Grafting during Repair of Acute Debakey I Dissection: Promotes Distal Aortic Remodeling and Reduces Late Open Re-operation
 Antegrade Thoracic Stent Grafting during Repair of Acute Debakey I Dissection: Promotes Distal Aortic Remodeling and Reduces Late Open Re-operation Vallabhajosyula, P: Szeto, W; Desai, N; Pulsipher, A;
Antegrade Thoracic Stent Grafting during Repair of Acute Debakey I Dissection: Promotes Distal Aortic Remodeling and Reduces Late Open Re-operation Vallabhajosyula, P: Szeto, W; Desai, N; Pulsipher, A;
TEVAR. (Thoracic Endovascular Aortic Repair) for Aneurysm and Dissection. Bruce Tjaden MD Vascular Surgery Fellow
 for Aneurysm and Dissection. Bruce Tjaden MD Vascular Surgery Fellow") Department of Cardiothoracic & Vascular Surgery McGovern Medical School / The University of Texas Health Science Center at Houston TEVAR (Thoracic Endovascular Aortic Repair) for Aneurysm and Dissection
Department of Cardiothoracic & Vascular Surgery McGovern Medical School / The University of Texas Health Science Center at Houston TEVAR (Thoracic Endovascular Aortic Repair) for Aneurysm and Dissection
History of the Powerlink System Design and Clinical Results. Edward B. Diethrich Arizona Heart Hospital Phoenix, AZ
 History of the Powerlink System Design and Clinical Results Edward B. Diethrich Arizona Heart Hospital Phoenix, AZ Powerlink System: Unibody-Bifurcated Design Long Main Body Low-Porosity Proprietary eptfe
History of the Powerlink System Design and Clinical Results Edward B. Diethrich Arizona Heart Hospital Phoenix, AZ Powerlink System: Unibody-Bifurcated Design Long Main Body Low-Porosity Proprietary eptfe
Hybrid Repair of a Complex Thoracoabdominal Aortic Aneurysm
 Hybrid Repair of a Complex Thoracoabdominal Aortic Aneurysm Virendra I. Patel MD MPH Assistant Professor of Surgery Massachusetts General Hospital Division of Vascular and Endovascular Surgery Disclosure
Hybrid Repair of a Complex Thoracoabdominal Aortic Aneurysm Virendra I. Patel MD MPH Assistant Professor of Surgery Massachusetts General Hospital Division of Vascular and Endovascular Surgery Disclosure
An Overview of Post-EVAR Endoleaks: Imaging Findings and Management. Ravi Shergill BSc Sean A. Kennedy MD Mark O. Baerlocher MD FRCPC
 An Overview of Post-EVAR Endoleaks: Imaging Findings and Management Ravi Shergill BSc Sean A. Kennedy MD Mark O. Baerlocher MD FRCPC Disclosure Slide Mark O. Baerlocher: Current: Consultant for Boston
An Overview of Post-EVAR Endoleaks: Imaging Findings and Management Ravi Shergill BSc Sean A. Kennedy MD Mark O. Baerlocher MD FRCPC Disclosure Slide Mark O. Baerlocher: Current: Consultant for Boston
Experience of endovascular procedures on abdominal and thoracic aorta in CA region
 Experience of endovascular procedures on abdominal and thoracic aorta in CA region May 14-15, 2015, Dubai Dr. Viktor Zemlyanskiy National Research Center of Emergency Care Astana, Kazakhstan Region Characteristics
Experience of endovascular procedures on abdominal and thoracic aorta in CA region May 14-15, 2015, Dubai Dr. Viktor Zemlyanskiy National Research Center of Emergency Care Astana, Kazakhstan Region Characteristics
Asymptomatic Radiology / Clinical data Report / Cohort bias Referral bias. UCSF Vascular Symposium April 7-9, Acute Aortic Dissection
 Aortic Dissection: Natural History What is the Natural History of Aortic Dissection? UCSF Vascular Symposium April 7-9, 2011 Asymptomatic Radiology / Clinical data Report / Cohort bias Referral bias Stephen
Aortic Dissection: Natural History What is the Natural History of Aortic Dissection? UCSF Vascular Symposium April 7-9, 2011 Asymptomatic Radiology / Clinical data Report / Cohort bias Referral bias Stephen
Vascular Intervention
 10 : 389-393, 2001 B Vascular Intervention 1 1 2 1 1 1 1 3 2 1 1997 7 2000 4 B 29 19 10 50 84 66.1 stent graft S/G primary entry stenting S/G 12 4 2 1 1 40 mm 8 1 MOF 1 endoleak + 11 91.6% 10 stenting
10 : 389-393, 2001 B Vascular Intervention 1 1 2 1 1 1 1 3 2 1 1997 7 2000 4 B 29 19 10 50 84 66.1 stent graft S/G primary entry stenting S/G 12 4 2 1 1 40 mm 8 1 MOF 1 endoleak + 11 91.6% 10 stenting
Challenges. 1. Sizing. 2. Proximal landing zone 3. Distal landing zone 4. Access vessels 5. Spinal cord ischemia 6. Endoleak
 Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic, Gore Employment in industry Stockholder of a healthcare company Owner of a healthcare company Other(s)
Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic, Gore Employment in industry Stockholder of a healthcare company Owner of a healthcare company Other(s)
The natural history of uncomplicated type B dissection, PAU and IMH: the IRAD knowledge. Santi Trimarchi, MD, PhD
 IRCCS Policlinico San Donato University of Milan Thoracic Aortic Research Center The natural history of uncomplicated type B dissection, PAU and IMH: the IRAD knowledge Santi Trimarchi, MD, PhD No COI
IRCCS Policlinico San Donato University of Milan Thoracic Aortic Research Center The natural history of uncomplicated type B dissection, PAU and IMH: the IRAD knowledge Santi Trimarchi, MD, PhD No COI
Prospective multicenter clinical trial (STABLE) on the endovascular treatment of complicated type B aortic dissection using a composite device design
 on the endovascular treatment of complicated type B aortic dissection using a composite device design") CLINICAL RESEARCH STUDIES From the Society for Vascular Surgery Prospective multicenter clinical trial (STABLE) on the endovascular treatment of complicated type B aortic dissection using a composite device
CLINICAL RESEARCH STUDIES From the Society for Vascular Surgery Prospective multicenter clinical trial (STABLE) on the endovascular treatment of complicated type B aortic dissection using a composite device
Current treatment of Aortic Aneurysms and Dissections. Adam Keefer, MD, FACS Sean Hislop, MD, FACS
 Current treatment of Aortic Aneurysms and Dissections Adam Keefer, MD, FACS Sean Hislop, MD, FACS Patient 1 69 year old well-educated man with reoccurring pain in his upper abdomen and a pulsatile mass.
Current treatment of Aortic Aneurysms and Dissections Adam Keefer, MD, FACS Sean Hislop, MD, FACS Patient 1 69 year old well-educated man with reoccurring pain in his upper abdomen and a pulsatile mass.
Open fenestration for complicated acute aortic B dissection
 Art of Operative Techniques Open fenestration for complicated acute aortic B dissection Santi Trimarchi 1, Sara Segreti 1, Viviana Grassi 1, Chiara Lomazzi 1, Marta Cova 1, Gabriele Piffaretti 2, Vincenzo
Art of Operative Techniques Open fenestration for complicated acute aortic B dissection Santi Trimarchi 1, Sara Segreti 1, Viviana Grassi 1, Chiara Lomazzi 1, Marta Cova 1, Gabriele Piffaretti 2, Vincenzo
Follow-up of Aortic Dissection: How, How Often, Which Consequences Euro Echo 2011
 Follow-up of Aortic Dissection: How, How Often, Which Consequences Euro Echo 2011 Susan E. Wiegers, MD, FASE Director of Clinical Echocardiography Hospital of the University of Pennsylvania Disclosure
Follow-up of Aortic Dissection: How, How Often, Which Consequences Euro Echo 2011 Susan E. Wiegers, MD, FASE Director of Clinical Echocardiography Hospital of the University of Pennsylvania Disclosure
Objective assessment of current stent grafts: which graft for which lesion. Ludovic Canaud, MD, PhD Pierre Alric, MD, PhD Montpellier, France
 Objective assessment of current stent grafts: which graft for which lesion Ludovic Canaud, MD, PhD Pierre Alric, MD, PhD Montpellier, France Conflict of interest: none 1 Introduction Different diseases
Objective assessment of current stent grafts: which graft for which lesion Ludovic Canaud, MD, PhD Pierre Alric, MD, PhD Montpellier, France Conflict of interest: none 1 Introduction Different diseases
Modified candy-plug technique for chronic type B aortic dissection with aneurysmal dilatation: a case report
 Kotani et al. Journal of Cardiothoracic Surgery (2017) 12:77 DOI 10.1186/s13019-017-0647-8 CASE REPORT Modified candy-plug technique for chronic type B aortic dissection with aneurysmal dilatation: a case
Kotani et al. Journal of Cardiothoracic Surgery (2017) 12:77 DOI 10.1186/s13019-017-0647-8 CASE REPORT Modified candy-plug technique for chronic type B aortic dissection with aneurysmal dilatation: a case
Low profile TEVAR: is it an added value? Michel Bosiers, G. Torsello Münster
 Low profile TEVAR: is it an added value? Michel Bosiers, G. Torsello Münster Disclosure Speaker name:...michel Bosiers... I have the following potential conflicts of interest to report: Consulting Employment
Low profile TEVAR: is it an added value? Michel Bosiers, G. Torsello Münster Disclosure Speaker name:...michel Bosiers... I have the following potential conflicts of interest to report: Consulting Employment
THORACOABDOMINAL AORTIC ANEURYSMS HYBRID REPAIR
 Update on Open and Endovascular Therapeutic Option for Aortic Repair CENTRE CARDIO-TORACIQUE DE MONACO Friday November 7 th, 2014 THORACOABDOMINAL AORTIC ANEURYSMS HYBRID REPAIR Roberto Chiesa Vascular
Update on Open and Endovascular Therapeutic Option for Aortic Repair CENTRE CARDIO-TORACIQUE DE MONACO Friday November 7 th, 2014 THORACOABDOMINAL AORTIC ANEURYSMS HYBRID REPAIR Roberto Chiesa Vascular
Access More Patients. Customize Each Seal.
 Access More. Customize Each Seal. The Least Invasive Path Towards Proven Patency ULTRA LOW PROFILE TO EASE ADVANCEMENT The flexible, ultra-low 12F ID Ovation ix delivery system enables you to navigate
Access More. Customize Each Seal. The Least Invasive Path Towards Proven Patency ULTRA LOW PROFILE TO EASE ADVANCEMENT The flexible, ultra-low 12F ID Ovation ix delivery system enables you to navigate
WHICH PLACE FOR EMERGENT INTERVENTION IN COMPLICATED ACUTE TYPE B DISSECTION (ctbaod)
") WHICH PLACE FOR EMERGENT INTERVENTION IN COMPLICATED ACUTE TYPE B DISSECTION (ctbaod) Epidemiology of type B Aortic Dissection TYPE B dissection: 0,5-2,1/100.000/year (40% of all dissection) Hospital mortality
WHICH PLACE FOR EMERGENT INTERVENTION IN COMPLICATED ACUTE TYPE B DISSECTION (ctbaod) Epidemiology of type B Aortic Dissection TYPE B dissection: 0,5-2,1/100.000/year (40% of all dissection) Hospital mortality
Title. Different arch branched devices are available, is morphology the. main criteria of choice? Ciro Ferrer, MD
 Different arch branched devices are available, is morphology the Title main criteria of choice? Ciro Ferrer, MD Vascular Surgery Unit Sapienza University of Rome Disclosure Speaker name: Ciro Ferrer Proctoring/speaking
Different arch branched devices are available, is morphology the Title main criteria of choice? Ciro Ferrer, MD Vascular Surgery Unit Sapienza University of Rome Disclosure Speaker name: Ciro Ferrer Proctoring/speaking
IMH/Penetrating Aortic Ulcers/ Saccular Aneurysms: How to manage and when to intervene
 IMH/Penetrating Aortic Ulcers/ Saccular Aneurysms: How to manage and when to intervene UCSF Vascular Surgery Symposium 2018 Sukgu M Han, MD, MS Assistant Professor of Clinical Surgery Co-director, Comprehensive
IMH/Penetrating Aortic Ulcers/ Saccular Aneurysms: How to manage and when to intervene UCSF Vascular Surgery Symposium 2018 Sukgu M Han, MD, MS Assistant Professor of Clinical Surgery Co-director, Comprehensive
Technique and Outcome of Laser Fenestration For Arch Vessels
 Technique and Outcome of Laser Fenestration For Arch Vessels Jean M. Panneton MD, FRCSC, FACS Professor of Surgery Chief & Program Director Division of Vascular Surgery Eastern Virginia Medical School
Technique and Outcome of Laser Fenestration For Arch Vessels Jean M. Panneton MD, FRCSC, FACS Professor of Surgery Chief & Program Director Division of Vascular Surgery Eastern Virginia Medical School
Endovascular Stent Grafts for Disorders of the Thoracic Aorta
 Endovascular Stent Grafts for Disorders of the Thoracic Aorta Policy Number: 7.01.86 Last Review: 9/2017 Origination: 5/2006 Next Review: 9/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC)
Endovascular Stent Grafts for Disorders of the Thoracic Aorta Policy Number: 7.01.86 Last Review: 9/2017 Origination: 5/2006 Next Review: 9/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC)
Thoracic Aortic Research Center. University of Milan
 University of Milan Thoracic Aortic Research Center Update on IRAD Santi Trimarchi, MD, PhD Associate Professor of Vascular Surgery, University of Milan Head, Unit of Vascular Surgery II Director, Thoracic
University of Milan Thoracic Aortic Research Center Update on IRAD Santi Trimarchi, MD, PhD Associate Professor of Vascular Surgery, University of Milan Head, Unit of Vascular Surgery II Director, Thoracic
Endovascular Stent Grafts for Disorders of the Thoracic Aorta
 Endovascular Stent Grafts for Disorders of the Thoracic Aorta Policy Number: 7.01.86 Last Review: 9/2018 Origination: 5/2006 Next Review: 9/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC)
Endovascular Stent Grafts for Disorders of the Thoracic Aorta Policy Number: 7.01.86 Last Review: 9/2018 Origination: 5/2006 Next Review: 9/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC)
Risks for Retrograde Type-A Dissection After TEVAR
 Risks for Retrograde Type-A Dissection After TEVAR Frank R. Arko, III, MD Chief, Vascular and Endovascular Surgery Professor, Cardiovascular Surgery Co-Director, Aortic Institute Sanger Heart and Vascular
Risks for Retrograde Type-A Dissection After TEVAR Frank R. Arko, III, MD Chief, Vascular and Endovascular Surgery Professor, Cardiovascular Surgery Co-Director, Aortic Institute Sanger Heart and Vascular
Intravascular Ultrasound in the Treatment of Complex Aortic Pathologies. Naixin Kang, M.D. Vascular Surgery Fellow April 26 th, 2018
 Intravascular Ultrasound in the Treatment of Complex Aortic Pathologies Naixin Kang, M.D. Vascular Surgery Fellow April 26 th, 2018 DISCLOSURES Nothing To Disclose 2 ENDOVASCULAR AORTIC INTERVENTION Improved
Intravascular Ultrasound in the Treatment of Complex Aortic Pathologies Naixin Kang, M.D. Vascular Surgery Fellow April 26 th, 2018 DISCLOSURES Nothing To Disclose 2 ENDOVASCULAR AORTIC INTERVENTION Improved
Acute non-complicated TBD Do need TEVAR treatment
 Acute non-complicated TBD Do need TEVAR treatment Prof. Dr. med. Christoph A. Nienaber Universität Rostock Universitäres Herzzentrum christoph.nienaber@med.uni-rostock.de Survival in type B dissection
Acute non-complicated TBD Do need TEVAR treatment Prof. Dr. med. Christoph A. Nienaber Universität Rostock Universitäres Herzzentrum christoph.nienaber@med.uni-rostock.de Survival in type B dissection
Endoleaks after F-BEVAR How to Assess & Treat? Gustavo S. Oderich, MD Mayo Clinic Rochester, MN
 Endoleaks after F-BEVAR How to Assess & Treat? Gustavo S. Oderich, MD Mayo Clinic Rochester, MN FACULTY DISCLOSURE Gustavo S. Oderich MD Consulting, DSMB, CEC* Cook Medical Inc., WL Gore, Lombardi Honoraria
Endoleaks after F-BEVAR How to Assess & Treat? Gustavo S. Oderich, MD Mayo Clinic Rochester, MN FACULTY DISCLOSURE Gustavo S. Oderich MD Consulting, DSMB, CEC* Cook Medical Inc., WL Gore, Lombardi Honoraria
Three year experience with multilayer stent in the treatment of thoracoabdominal aneurysms no evidence for aneurysm stabilization
 Three year experience with multilayer stent in the treatment of thoracoabdominal aneurysms no evidence for aneurysm stabilization Thomas Larzon, MD, PhD Head of Vascular Surgery Dept of Cardiothoracic
Three year experience with multilayer stent in the treatment of thoracoabdominal aneurysms no evidence for aneurysm stabilization Thomas Larzon, MD, PhD Head of Vascular Surgery Dept of Cardiothoracic
Evolution of Thoracic Aortic Surgery A Rapidly Advancing Paradigm. October 15 th, 2014 Family Practice Evening Course University of Calgary
 Evolution of Thoracic Aortic Surgery A Rapidly Advancing Paradigm October 15 th, 2014 Family Practice Evening Course University of Calgary Jehangir Appoo Division of Cardiac Surgery Libin Cardiovascular
Evolution of Thoracic Aortic Surgery A Rapidly Advancing Paradigm October 15 th, 2014 Family Practice Evening Course University of Calgary Jehangir Appoo Division of Cardiac Surgery Libin Cardiovascular
What Determines Aortic False Lumen Growth Post Dissection?
 Aortic Dissections What Determines Aortic False Lumen Growth Post Dissection? UCSF Vascular Symposium April 26, 2012 Most common aortic emergency Incidence of aortic dissections are 2/100,000 person-years
Aortic Dissections What Determines Aortic False Lumen Growth Post Dissection? UCSF Vascular Symposium April 26, 2012 Most common aortic emergency Incidence of aortic dissections are 2/100,000 person-years
Animesh Rathore, MD 4/21/17. Penetrating atherosclerotic ulcers of aorta
 Animesh Rathore, MD 4/21/17 Penetrating atherosclerotic ulcers of aorta Disclosures No financial disclosures Thank You Dr. Panneton for giving this lecture for me. I am stuck at Norfolk with an emergency
Animesh Rathore, MD 4/21/17 Penetrating atherosclerotic ulcers of aorta Disclosures No financial disclosures Thank You Dr. Panneton for giving this lecture for me. I am stuck at Norfolk with an emergency
Talent Abdominal Stent Graft
 Talent Abdominal with THE Xcelerant Hydro Delivery System Expanding the Indications for EVAR Treat More Patients Short Necks The Talent Abdominal is the only FDA-approved device for proximal aortic neck
Talent Abdominal with THE Xcelerant Hydro Delivery System Expanding the Indications for EVAR Treat More Patients Short Necks The Talent Abdominal is the only FDA-approved device for proximal aortic neck
Therapeutic Pathway In Acute Aortic Dissection. Speaker: Cesare Quarto Consultant Cardiac Surgeon Royal Brompton Hospital, London UK
 Therapeutic Pathway In Acute Aortic Dissection Speaker: Cesare Quarto Consultant Cardiac Surgeon Royal Brompton Hospital, London UK Disclosure of Interest Speaker name: Cesare Quarto I do not have any
Therapeutic Pathway In Acute Aortic Dissection Speaker: Cesare Quarto Consultant Cardiac Surgeon Royal Brompton Hospital, London UK Disclosure of Interest Speaker name: Cesare Quarto I do not have any
Early outcomes of acute retrograde dissection in the aortic arch and the ascending aorta data from IRAD
 Early outcomes of acute retrograde dissection in the aortic arch and the ascending aorta data from IRAD Foeke JH Nauta, MD, PhD Resident Cardiothoracic Surgery, Academic Medical Center, Amsterdam Disclosure
Early outcomes of acute retrograde dissection in the aortic arch and the ascending aorta data from IRAD Foeke JH Nauta, MD, PhD Resident Cardiothoracic Surgery, Academic Medical Center, Amsterdam Disclosure
EVAR and TEVAR: Extending Their Use for Rupture and Traumatic Injury. Conflict of Interest. Hypotensive shock 5/5/2014. none
 EVAR and TEVAR: Extending Their Use for Rupture and Traumatic Injury Bruce H. Gray, DO MSVM FSCAI Professor of Surgery/Vascular Medicine USC SOM-Greenville Greenville, South Carolina none Conflict of Interest
EVAR and TEVAR: Extending Their Use for Rupture and Traumatic Injury Bruce H. Gray, DO MSVM FSCAI Professor of Surgery/Vascular Medicine USC SOM-Greenville Greenville, South Carolina none Conflict of Interest
Description. Section: Surgery Effective Date: October 15, 2016 Subsection: Surgery Original Policy Date: December 7, 2011 Subject:
 Last Review Status/Date: September 2016 Page: 1 of 30 Description Thoracic endovascular aneurysm repair (TEVAR) involves the percutaneous placement of a stent graft in the descending thoracic or thoracoabdominal
Last Review Status/Date: September 2016 Page: 1 of 30 Description Thoracic endovascular aneurysm repair (TEVAR) involves the percutaneous placement of a stent graft in the descending thoracic or thoracoabdominal
State of Art Hybrid Approach
 State of Art Hybrid Approach for Complex Aorta Diseases Won Ho Kim, MD Division of Cardiology, Eulji University Hospital Eulji University School of Medicine, Daejeon, Korea Introduction.Hybrid procedure
State of Art Hybrid Approach for Complex Aorta Diseases Won Ho Kim, MD Division of Cardiology, Eulji University Hospital Eulji University School of Medicine, Daejeon, Korea Introduction.Hybrid procedure
Aortic Neck Issues Associated Clinical Sequelae/Implications for Graft Choice
 Aortic Neck Issues Associated Clinical Sequelae/Implications for Graft Choice Eric Verhoeven, MD, PhD, A. Katsargyris, MD Department of Vascular and Endovascular Surgery, Paracelsus Medical University,
Aortic Neck Issues Associated Clinical Sequelae/Implications for Graft Choice Eric Verhoeven, MD, PhD, A. Katsargyris, MD Department of Vascular and Endovascular Surgery, Paracelsus Medical University,
Subject: Endovascular Stent Grafts for Disorders of the Thoracic Aorta
 02-33000-29 Original Effective Date: 04/15/03 Reviewed: 07/26/18 Revised: 08/15/18 Subject: Endovascular Stent Grafts for Disorders of the Thoracic Aorta THIS MEDICAL COVERAGE GUIDELINE IS NOT AN AUTHORIZATION,
02-33000-29 Original Effective Date: 04/15/03 Reviewed: 07/26/18 Revised: 08/15/18 Subject: Endovascular Stent Grafts for Disorders of the Thoracic Aorta THIS MEDICAL COVERAGE GUIDELINE IS NOT AN AUTHORIZATION,
Neurological Complications of TEVAR. Frank J Criado, MD. Union Memorial-MedStar Health Baltimore, MD USA
 ISES Online Neurological Complications of Frank J Criado, MD TEVAR Union Memorial-MedStar Health Baltimore, MD USA frank.criado@medstar.net Paraplegia Incidence is 0-4% after surgical Rx of TAAs confined
ISES Online Neurological Complications of Frank J Criado, MD TEVAR Union Memorial-MedStar Health Baltimore, MD USA frank.criado@medstar.net Paraplegia Incidence is 0-4% after surgical Rx of TAAs confined
Jean M Panneton, MD Professor of Surgery Program Director Vascular Surgery Chief EVMS. Arch Pathology: The Endovascular Era is here
 Jean M Panneton, MD Professor of Surgery Program Director Vascular Surgery Chief EVMS Arch Pathology: The Endovascular Era is here Disclosures Consultant: Cook Medical, Bolton Medical, Medtronic Inc, Volcano,
Jean M Panneton, MD Professor of Surgery Program Director Vascular Surgery Chief EVMS Arch Pathology: The Endovascular Era is here Disclosures Consultant: Cook Medical, Bolton Medical, Medtronic Inc, Volcano,
The Role of Stent-Grafts in Marfan Syndrome
 The Role of Stent-Grafts in Marfan Syndrome James H. Black, III, MD, FACS The David Goldfarb, MD, Associate Professor of Surgery Chief, Division of Vascular Surgery and Endovascular Therapy The Johns Hopkins
The Role of Stent-Grafts in Marfan Syndrome James H. Black, III, MD, FACS The David Goldfarb, MD, Associate Professor of Surgery Chief, Division of Vascular Surgery and Endovascular Therapy The Johns Hopkins
Considerations for a Durable Repair
 Considerations for a Durable Repair Eric Verhoeven, MD, PhD, A. Katsargyris, MD Department of Vascular and Endovascular Surgery, Paracelsus Medical University, Nuremberg, Germany Disclosures William Cook
Considerations for a Durable Repair Eric Verhoeven, MD, PhD, A. Katsargyris, MD Department of Vascular and Endovascular Surgery, Paracelsus Medical University, Nuremberg, Germany Disclosures William Cook
Thoracic Endovascular Aortic Repair (TEVAR) Indications and Basic Procedure
 Indications and Basic Procedure") Thoracic Endovascular Aortic Repair (TEVAR) Indications and Basic Procedure Tilo Kölbel, MD, PhD University Heart Center Hamburg University Hospital Eppendorf Disclosure Speaker name: Tilo Kölbel, MD I
Thoracic Endovascular Aortic Repair (TEVAR) Indications and Basic Procedure Tilo Kölbel, MD, PhD University Heart Center Hamburg University Hospital Eppendorf Disclosure Speaker name: Tilo Kölbel, MD I
Accepted Manuscript. Is A More Extensive Operation Justified for Acute Type A Dissection Repair? Dr. Leonard N. Girardi
 Accepted Manuscript Is A More Extensive Operation Justified for Acute Type A Dissection Repair? Dr. Leonard N. Girardi PII: S0022-5223(18)32552-2 DOI: 10.1016/j.jtcvs.2018.09.048 Reference: YMTC 13502
Accepted Manuscript Is A More Extensive Operation Justified for Acute Type A Dissection Repair? Dr. Leonard N. Girardi PII: S0022-5223(18)32552-2 DOI: 10.1016/j.jtcvs.2018.09.048 Reference: YMTC 13502