Do the Data Support Endovascular Therapy for Descending Thoracic AD? Woong Chol Kang, M.D.
|
|
|
- Sandra Mathews
- 5 years ago
- Views:
Transcription

1 Do the Data Support Endovascular Therapy for Descending Thoracic AD? Woong Chol Kang, M.D. Gil Hospital, Gachon University Incheon, Korea
 (IIIa, b) type B dissections account for")
2 Classification of AD Acute vs. Chronic (2weeks) (IIIa, b) type B dissections account for about 40% of all dissections.
3 Management of type B AD IRAD. JAMA. 2000;283: , Lancet 2008; 372: 55 66
4 Complication to acute type B Dissection Malperfusion Refractionary hypertension Continued pain 30% Mortality : 20% at day 2, 25-50% at 1 M
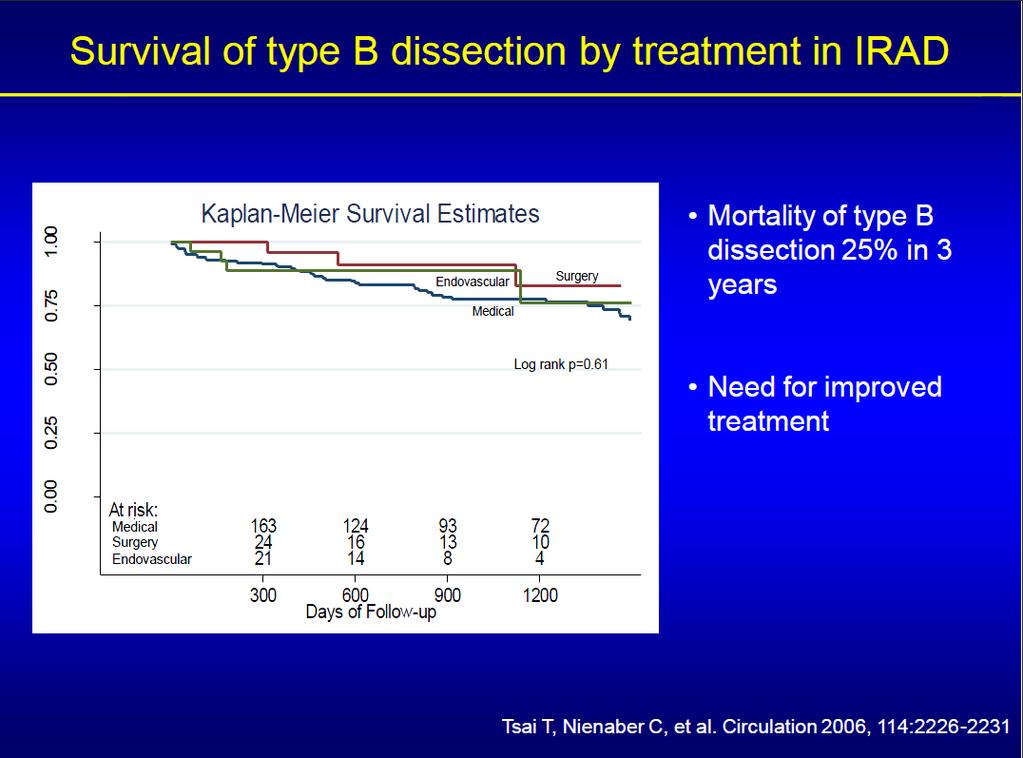
5 Survival of type B uncomplicated AD Dilatation/Aneurysm 20-50%/1-5yr Rupture or impending rupture Mortality : 25%/3yrs Intervention Open surgical repair Endovascular therapy Circulation. 2006;114:
6 Open Surgical Repair Rupture : Graft replacement Expansion : Graft replacement Ischemia : Fenestration High in-hospital mortality (29%) New neurologic deficit (23%) Stroke (9%) Sustained paraplegia (5%) from IRAD registry (Circulation 2006)
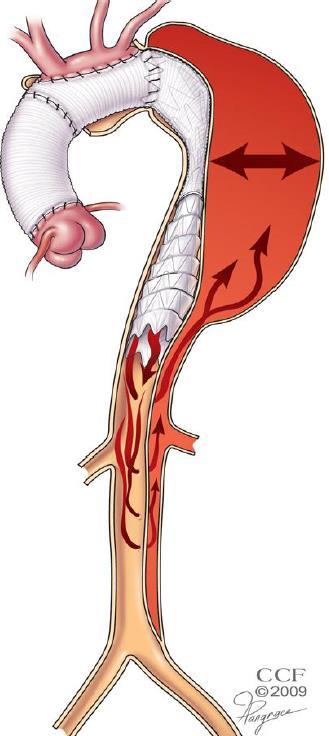
7 Concept of Endovascular therapy in AD Closure of the Proximal Entry tear Depressurization of the False Lumen Redirection of blood flow towards the TL Thrombosis of the FL Induction of aortic remodeling
8 Classification of AD for treatment strategy Acute vs. Chronic Complicated vs. Uncomplicated
9 Classification of AD for treatment modality Acute vs. Chronic Complicated vs. Uncomplicated Open vs. Endovascular repair
.")
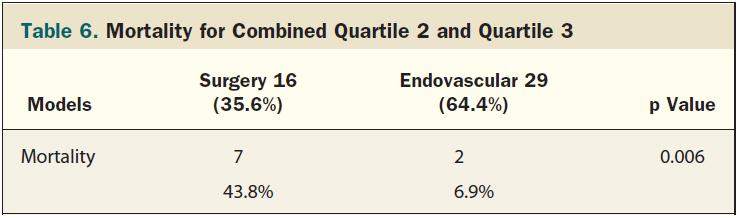
10 Complicated Acute Type B AD:Is Surgery Still the Best Option?- Demographics IRAD represents 21 large centers in 11 countries which between 1996 and 2003 collected 571 type B AD. Patients with symptoms of ischemia or refractory pain underwent an intervention (N=125, surgery or endovascular therapy). Patients submitted to surgery presented with a wider aortic diameter than patients treated by endovascular therapy (5.36±1.7 vs. 4.62±1.4 cm, p=0.003). IRAD registry : JACC Int. 2008;1:
11 Complicated Acute Type B Dissection : Is Surgery Still the Best Option? -IH complication & mortality IRAD registry : JACC Int. 2008;1:
12 Complicated Acute Type B AD:Is Surgery Still the Best Option?-IH Cx & mortality The less invasive nature of endovascular treatment seems to provide better in-hospital survival in patients with acute type B dissection. IRAD registry : JACC Int. 2008;1:
13 Early Open and Endovascular Thoracic Aortic Repair for Complicated Type B AD Seventy-three patients (mean age 66.3 yrs) with type B AD underwent early open descending aortic repair (n=24) or TEVAR (n=49). Patients undergoing TEVAR were older and had an increased incidence of coronary artery disease and renal impairment (all p < 0.05). Ann Thorac Surg 2013 (In Press)
14 Endovascular Stent-Graft Placement or Open Surgery for the Treatment of Acute Type B Aortic Dissection: A Meta-Analysis Thirty-day mortality Stroke Long-term mortality Reintervention Ann Vasc Surg 2012; 26:
15 Classification of AD for treatment modality Acute vs. Chronic Complicated vs. Uncomplicated OMT vs. Endovascular repair
 Alone (2007)")
16 ADSORB Trial Prospective, Randomized, Multicentric, European study in Acute Uncompicated Aortic Dissection Type B Evaluating Stent-Graft Placement OR Best Medical Treatment (BMT) Alone (2007)
17 Thoracic Endovascular Aortic Repair or Medical Management Alone?-Late events 193 consecutive patients in 2 hospitals (Nanjing and Cleveland Clinic) were enrolled. TEVAR group TEVAR and medications (n=152) vs. Medicine group-medically alone (n=41). All TEVAR procedures were performed in the acute phase. Late events Aortic rupture Retrograde Dissection Aortic enlargement Type-I and -II endoleaks Ulcerlike projection Late death 1Y 3Y 5Y TEVAR 97% 89% 67% Medicine 97% 63% 34% J Am Coll Cardiol Intv 2013;6:185 91
18 Thoracic Endovascular Aortic Repair or Medical Management Alone?-Death All-cause Death Aortic related Death Aortic related Death & Unknown Death Patients with type-b AAD treated with TEVAR experienced fewer late adverse events than those treated with medical management, but there was no significant difference among the groups in 5-year mortality rates. J Am Coll Cardiol Intv 2013;6:185 91
19 Classification of AD for treatment modality Acute vs. Chronic Complicated vs. Uncomplicated OMT vs. Endovascular repair
20 Randomized Comparison of Strategies for Uncomplicated Chronic Type B AD The INvestigation of STEnt Grafts in Aortic Dissection (INSTEAD) Trial Primary EP all-cause death at 2yrs Secondary EP aorta-related death AD progression aortic remodeling The study achieved 100% technical success in all TEVAR group. Circulation 2009;120:
21 Cumulative survival (95.6%) (88.9%) Aorta-related mortality (97.0%) (94.4%) Combined end point of progression and adverse events (77.2%) (72.5%) Three neurological adverse events occurred in the TEVAR group (1 paraplegia, 1 stroke, and 1 transient paraparesis), versus 1 case of paraparesis with medical treatment. Circulation 2009;120:
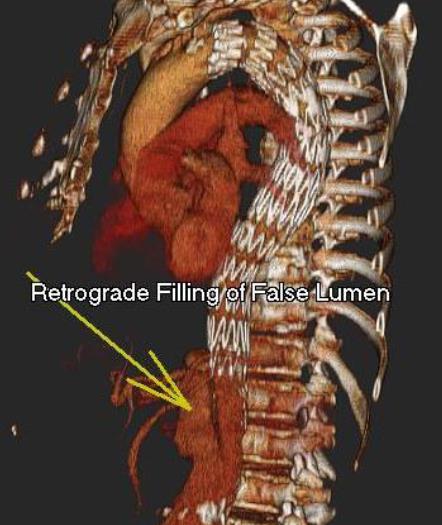
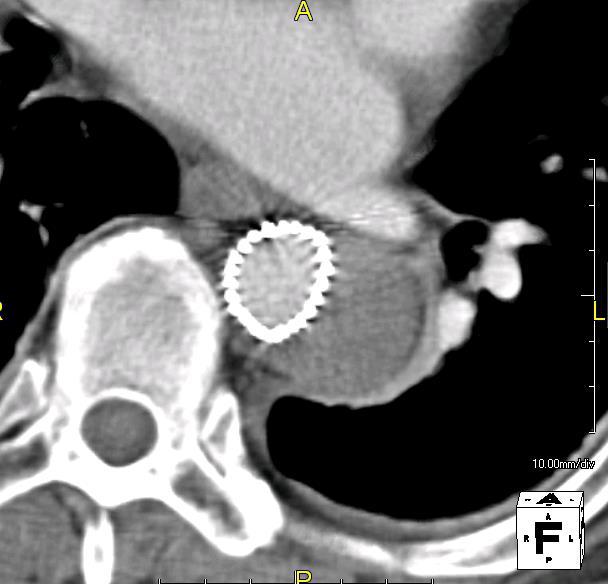
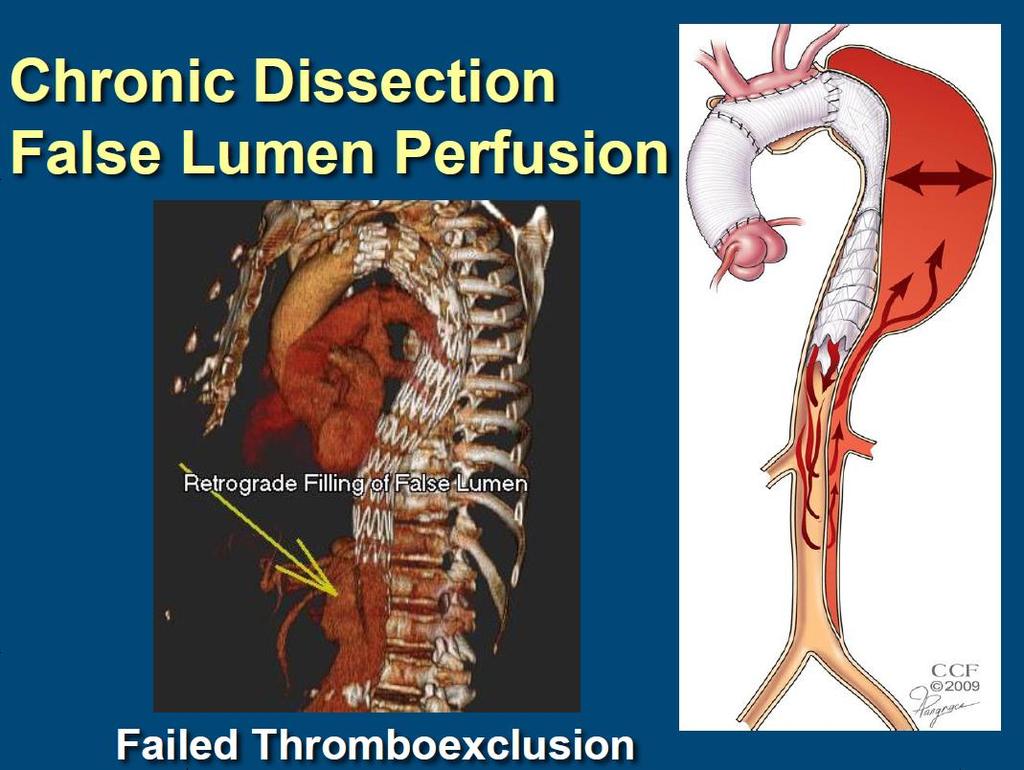
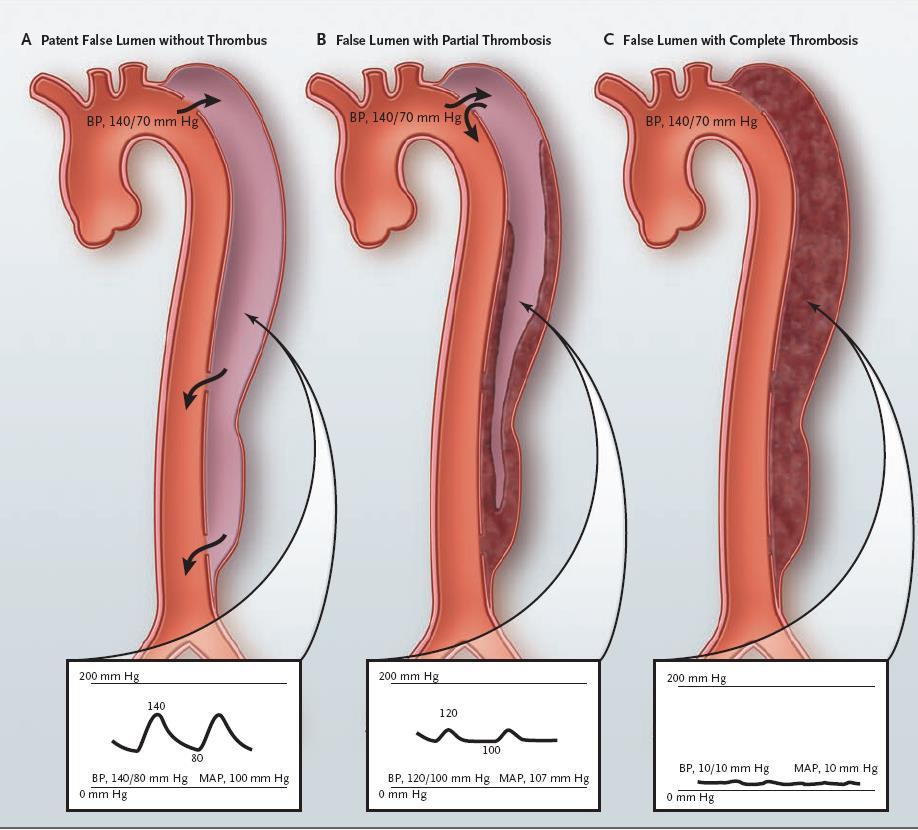
22 Persistent perfusion of the false lumen
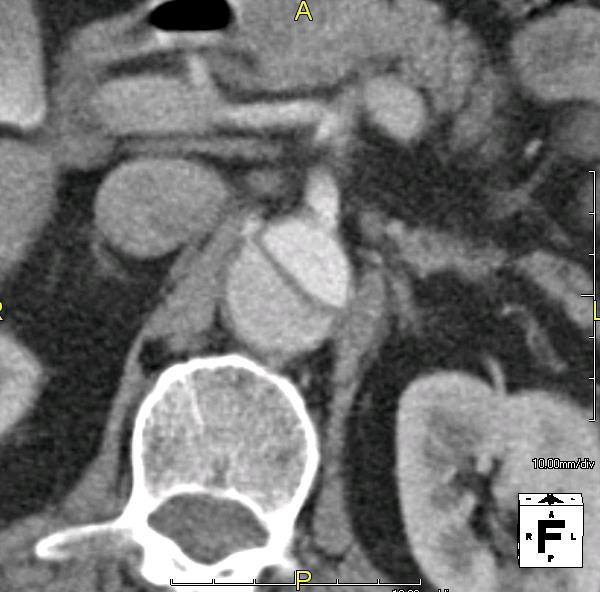
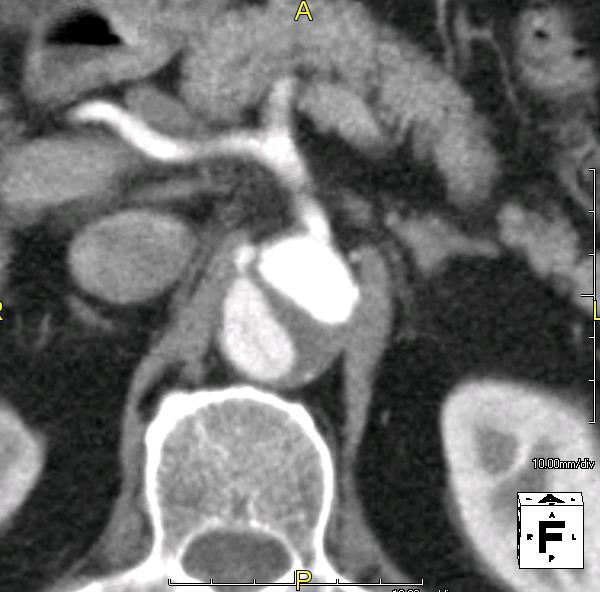
23 Aortic remodeling Aortic remodeling (with truelumen recovery and thoracic false-lumen thrombosis) occurred in 91.3% of patients with TEVAR vs. 19.4% of those who received medical treatment (P<0.001), which suggests ongoing aortic remodeling. Circulation 2009;120:
24 Conclusion : INSTEAD Trial No difference in mortality endpoint (Underpowered) Significant crossover to TEVAR Remodeling Benefit (91.3% with TEVAR vs. 19.4% with medical treatment alone (p<0.001)
25 The results of stent graft vs. medication for chronic type B AD Prospective multicenter comparative study. 303 consecutive patients with chronic type B AD who were prospectively enrolled and treated by either OMT or TEVAR. Baseline diameter of the thoracic aorta was 41.2 (19.1) mm and dissection extended beyond the celiac axis in 87.1% of cases. J Vasc Surg 2013;57:406-14
26 The results of stent graft vs. medication for chronic type B-Cumulative survival P= Y 4Y TEVAR 87.5% 82.7% Medicine 77.5% 69.1% J Vasc Surg 2013;57:406-14
27 The results of stent graft vs. medication for chronic type B-Aorta related mortality 2Y 4Y TEVAR 91.6% 88.1% Medicine 82.8% 73.9% P= J Vasc Surg 2013;57:406-14
28 The results of stent graft vs. medication for chronic type B-Aortic remodeling J Vasc Surg 2013;57:406-14
29 Classification of AD for treatment modality Acute vs. Chronic Complicated vs. Uncomplicated Open vs. Endovascular repair
30 NONSURGICAL RECONSTRUCTION OF THORACIC AD BY STENT GRAFT PLACEMENT NEJM 1999;340:
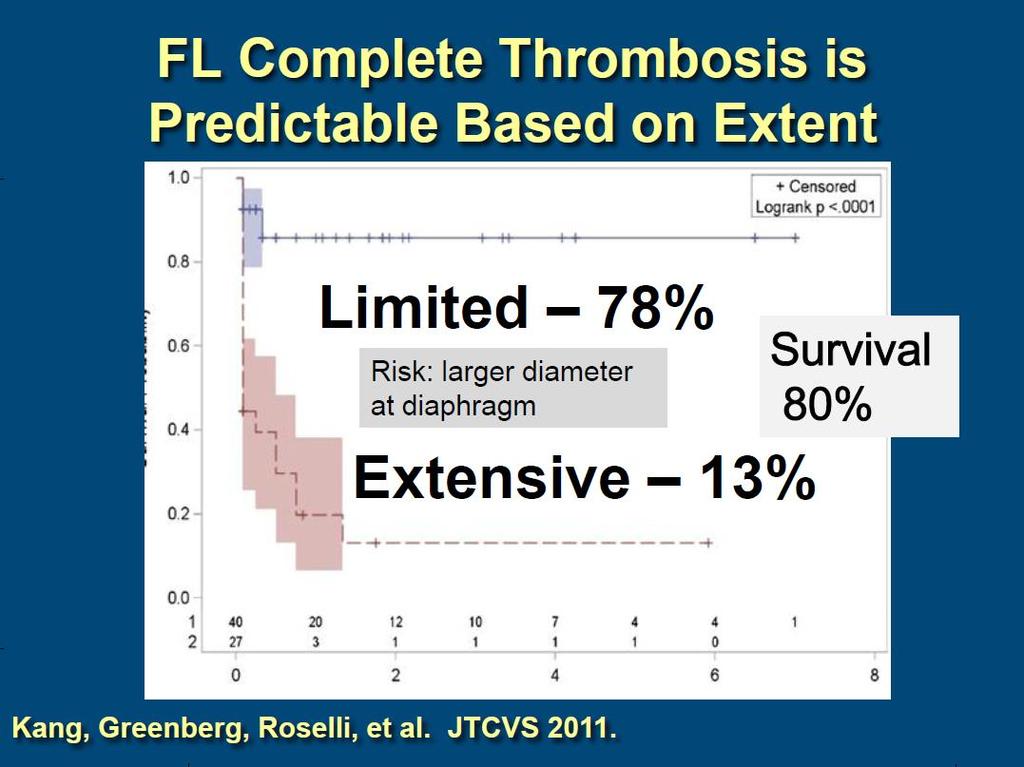
31 Endovascular repair of complicated chronic distal AD: Intermediate outcomes and complications All cases (N=76) of TEVAR for complicated (aortic growth, malperfusion, intractable pain) CDAD were retrospectively reviewed. Aortic morphology (aneurysm size, false lumen thrombosis) was assessed at multiple levels with 3-dimensional image analysis techniques. JTCVS 2011;142:
32 JTCVS 2011;142: Endovascular repair of complicated chronic distal AD: Intermediate outcomes and complications Mean clinical FU : 34 months (all) Mean imaging FU : 24 months (67pts) Early (<30 postoperative days) mortality was 5% (4 patients). No paraplegia, and 1 patient died of stroke. Overall survival Freedom free reintervention 86%, 82%, and 80% at 12, 24, 36 M 72%, 64%, and 59% at 12, 24, 36 M








33 SCA Prox. TA Mid TA Distal TA Celiac A SMA Abdominal Aorta Renal A

34 Arterial diameter changes TEVAR resulted in significantly decreased aortic diameter through the stent grafted segment but not untreated segments.
35 Complete thrombosis of FL Limited AD (78%) limited extensive P<.001 Extensive AD (13%) IIIa IIIb Debakey JTCVS 2011;142:


36 Limited AD


37 baseline Post 4M Post 4Y limited, complete resolution


38 Extensive AD baseline immediate post S-G



39 S-G decrease, below S-G no change Post 2yrs Post 4yrs

40 Unanswered question for Endovascular therapy in AD When : Acute vs. Chronic Retrograde dissection Acute << Chronic Aortic remodeling Acute >> Chronic


 vs.")
41 Unanswered question for Endovascular therapy in AD How extent? Entry tear (aortic remodeling ) vs. As possible as long (neurologic Cx )
42 Summary Acute complicated IRAD : OP<S-G (mortality) Acute uncomplicated OMT<S-G (no mortality), ADSORB (?) Chronic uncomplicated OMT<S-G (aortic remodeling), INSTEAD (-) Chronic complicated S-G : Acceptable, limitation in extensive AD
43 Thank you for your attention!
44 Aortic Dissection : endovascular Tx vs. other Tx Type A Type B Open repair With complication Without complication Open repair Endo Tx Medical Tx Endo Tx ADSORB : Medical Tx vs. S-G (?) Acute With complication Without complication Chronic Open repair Endo Tx Medical Tx Endo Tx IRAD : Surgery << S-G INSTEAD : Medical Tx = S-G S-G : Acceptable, need more data
45
46
47
48
49 Our data showed Management of complicated CDAD remains challenging for clinicians. TEVAR is a reasonable treatment modality for dissections limited to the thoracic aorta and for prevention of focal aortic growth in extensive dissections. Late complications and the need for secondary interventions emphasize the complexity of this patient population and the need for long-term follow-up.
50 Aortic Dissection : endovascular Tx vs. other Tx Type A Type B Open repair With complication Without complication Open repair Endo Tx Medical Tx Endo Tx ADSORB : Medical Tx vs. S-G (?) Acute With complication Without complication Chronic Open repair Endo Tx Medical Tx Endo Tx IRAD : Surgery << S-G INSTEAD : Medical Tx = S-G S-G : Acceptable, need more data
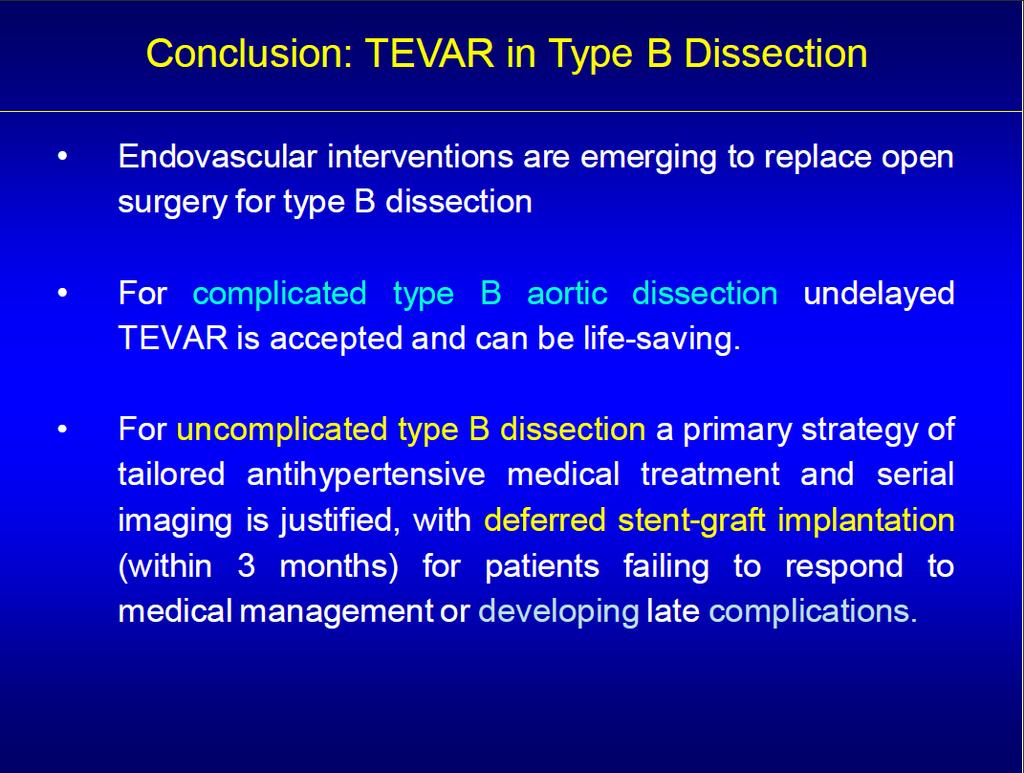
51 Conclusions The optimal treatment of AD remains a challenging clinical dilemma. Open aortic repair carries a high mortality rate, in addition to a high stroke and paraplegia rate. For uncomplicated type B AD a primary strategy of tailored antihypertensive medical treatment and serial imaging is justified, with deffered intervention. The concept of using aortic stent-graft to treat type B AD is relatively new and continues to evolve, as experience with this technique grows and technology improves. TEVAR is a reasonable alternative for patient with complicated type B AD and provides satisfactory mid-term clinical outcomes. TEVAR stabilizes the descending aorta in most patients and promo tes aortic remodeling. However, careful attention should be given to the dissected aorta situated below the level of the stent-graft to detect late aneurysm al degeneration.
52
53
54
55
56
57
58
59
60
61
62
63 Open repair of chronic distal AD in the endovascular era: Implications for disease management From 2000 to 2008, 169 patients underwent open repair of the descending thoracic artery only (n=88) or thoracoabdominal (n=81) chronic aortic dissection (elective in 98, urgent/emergency in 71). Chart review and 3-dimensional assessment of computed tomography were performed. Poor outcome included all cause mortality or vascular reintervention. J Thorac Cardiovasc 2012;144:866-73
64 Open repair of chronic distal AD in the endovascular era-event-free survival 1Y 2Y 5Y DA 80% 69% 51% TAA 69% 62% 47% J Thorac Cardiovasc 2012;144:866-73
65 Open repair of chronic distal AD in the endovascular era-freedom free reintervention 1Y 2Y 5Y 1Y 2Y 5Y DA 84% 74% 54% DA 95% 91% 81% TAA 74% 67% 55% TAA 89% 85% 79% J Thorac Cardiovasc 2012;144:866-73
66 J Thorac Cardiovasc 2012;144:866-73
67 Complication to type B Acute Dissection Type B dissections are commonly stratified as acute onset complicated, acute onset uncomplicated, and chronic. About 20% of cases are complicated at the time of diagnosis, requiring either endovascular or surgical repair. Rupture 10 % Organ Ischemia (malperfusion) 5-10 % Refractory Hypertension 5-10 % Dilatation/Aneurysm 25 %/4yr
68 IRAD : International Registry of Aortic Dissection The International Registry of Aortic Dissection (IRAD) represents 21 large centers in 11 countries which between 1996 and 2003 collected 532 type B AD. Patients with symptoms of ischemia or refractory pain underwent an intervention. In-hospital mortality was 29% for open traditional surgery, 11% for endovascular therapies, and 10% for medical therapy alone.
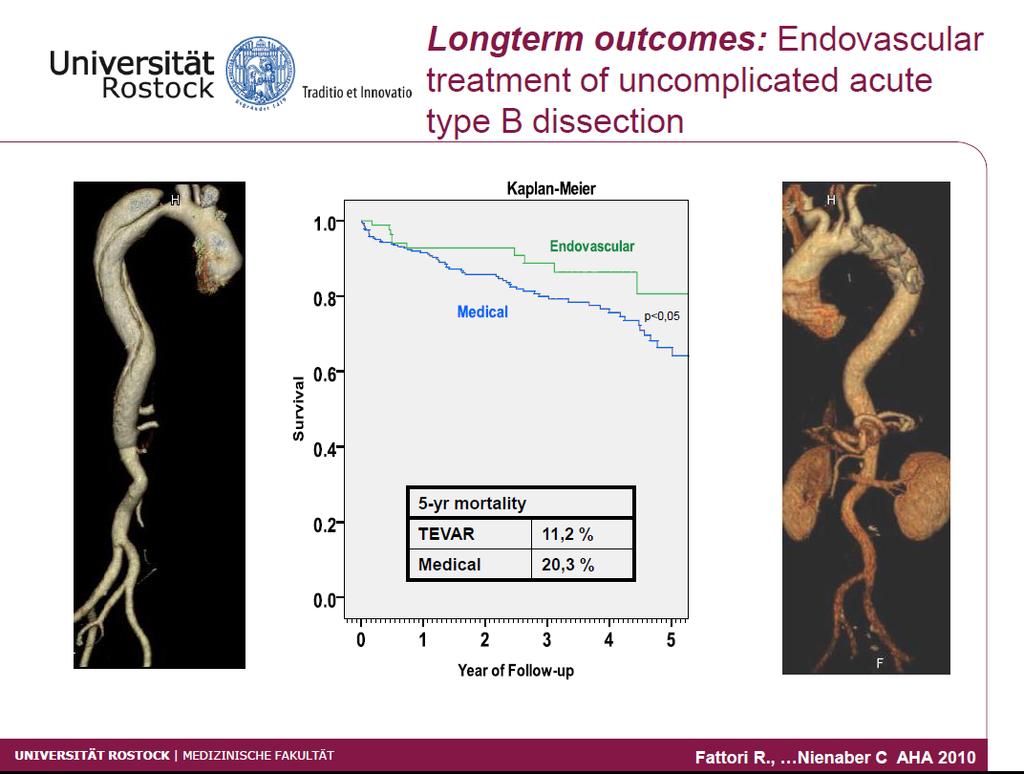
69 Kaplan-Meier Survival Estimates Those patients who survived discharge from the hospital, 96% were alive 1 year after surgery, 89% 1 year after endovascular therapy and 90% with medical therapy alone. At 3 years, 83% of the surgical group was alive, 76% of the endovascular group and 78% of the medical treatment only group.
70 IRAD. JAMA. 2000;283:
71 Classification Acute vs. Chronic (2weeks) Disease extension (anatomic consideration) Stanford or Debakey, Svensson (ESC) Complicated vs. Uncomplicated Expansion/ imminent rupture Persistent thoracic pain Drug-resistant hypertension Development of malperfusion syndrome Development of aneurysm of the false lumen
")
72 Ann Thorac Surg 2013 (In Press)
73 Conclusion : INSTEAD This is the first randomized study on elective stent-graft placement in survivors of uncomplicated type B aortic dissection. TEVAR failed to improve 2-year survival and adverse event rates despite favorable aortic remodeling. The INSTEAD trial with 3 year data did not show a statistically significant difference between medical management and endovascular therapy. This trial was underpowered to reach statistical significance. Also of note, the medical group did include 16% of patients who eventually had to go for repair of the aorta due to degenerative aneurysmal disease with aortic diameter > 6 cm. This trial with long-term follow-up may find a survival advantage for stent-grafting over medical management especially when late aneurismal degeneration is considered.
74 Background Patients with distal chronic aortic dissections (DCAD) remain at high-risk for secondary aortic-related events and subsequent reinterventions. However, the ideal strategy to manage complicated DCAD is not defined yet: open surgical strategies are fraught with high rates of morbidity and mortality, while the results of the endovascular aortic repair (EVAR) are poorly known in this indication.
75 Methods. Data regarding the demographics, the indication for repair, the complications, and the morphologic changes of the a orta during follow-up was collected using medical records and CT-scan analysis. Statistical analysis was performed to evaluate the evolution of the aortic wall (aneurysm size, false lumen thrombosis) a ccording to the aortic level.
76 Indication for DCAD repair (1) Maximum aortic diameter 55 mm; (2) Rapid aortic enlargement ( 10 mm per year); (3) Clinical or radiographic evidence of rupture or impending rupture; (4) Intractable chest pain, despite maximal medical therapy; (5) Symptomatic branch vessel stenosis/occlusion with subsequent visceral ischemia.
77 RESULTS
78 NEJM 2007;357:349-59
79 NEJM 2007;357:349-59

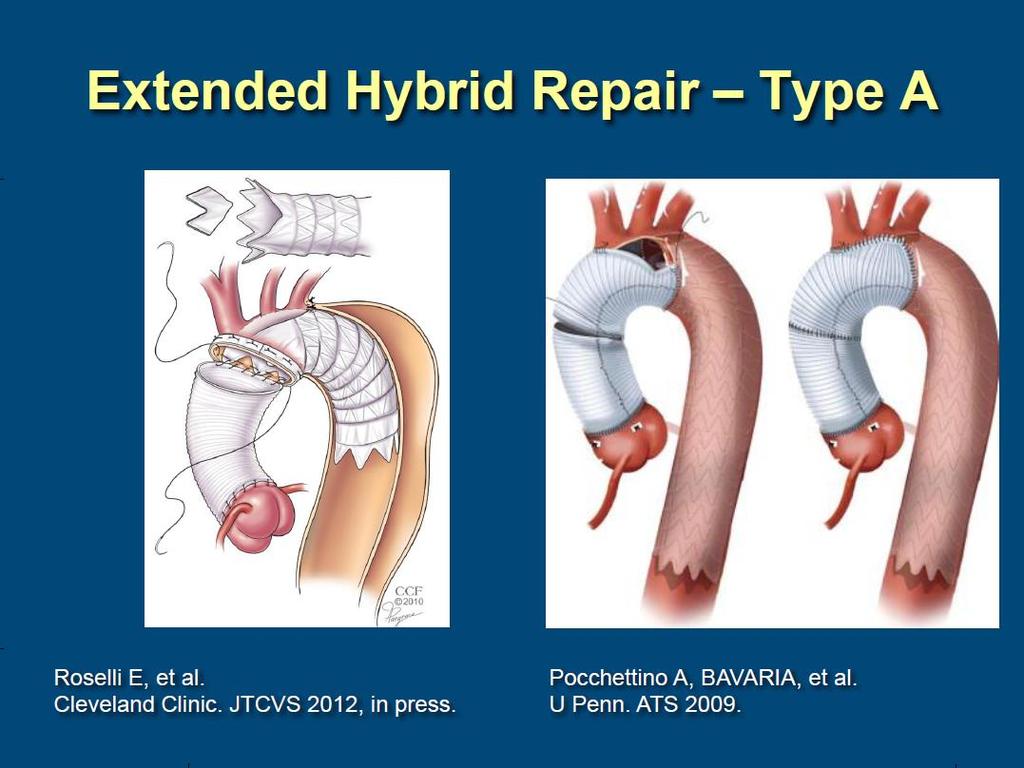
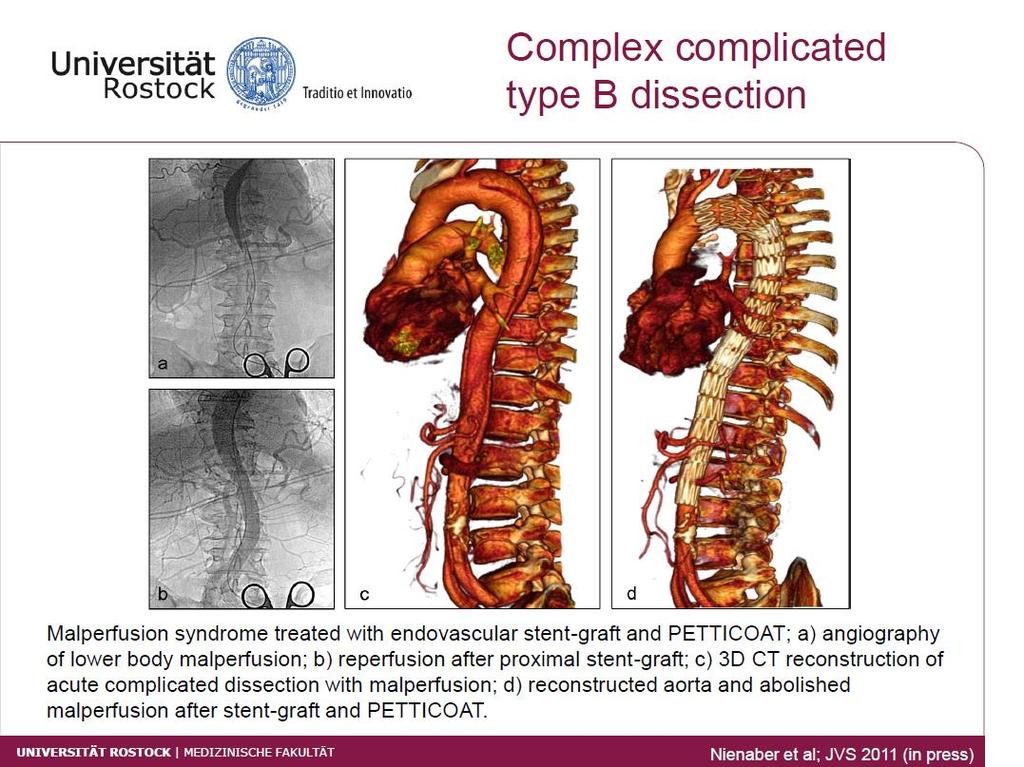
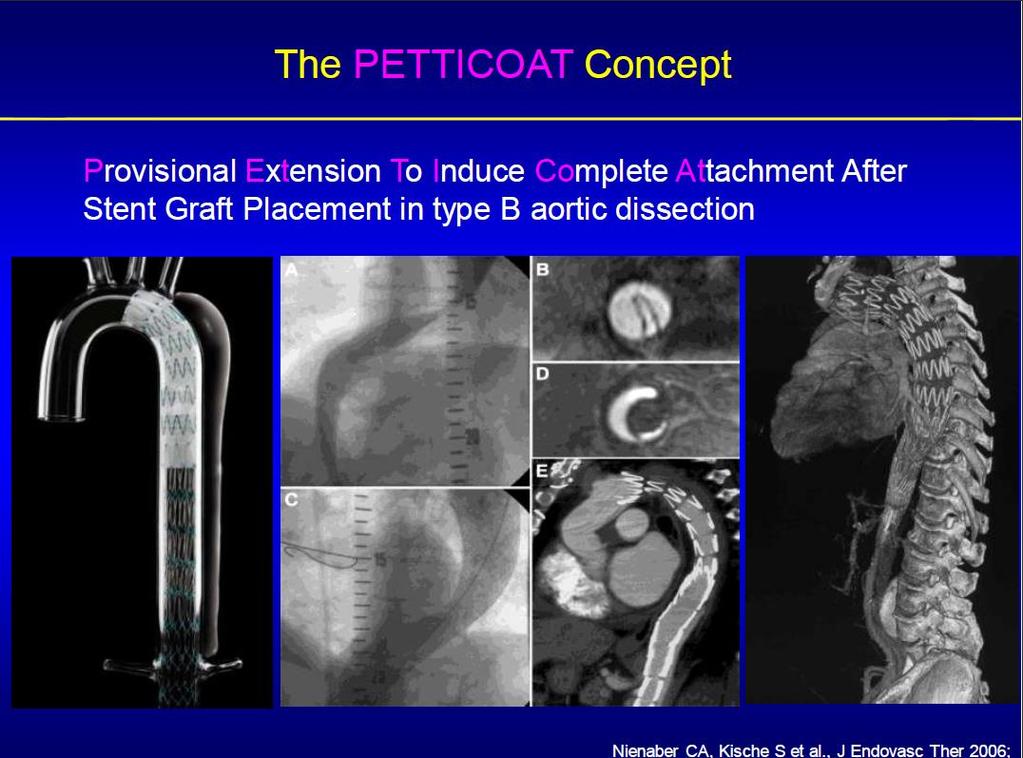
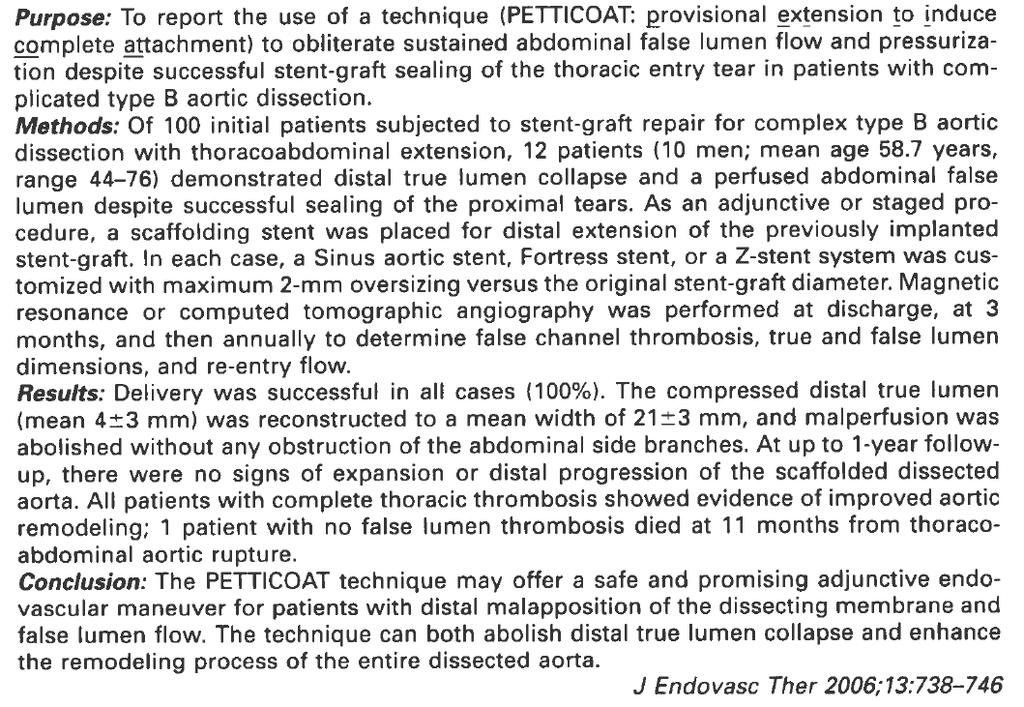
80 Provisional Extension To Induce COmplete ATtachment After Stent-Graft Placement in Type B Aortic Dissection : The PETTICOAT Concept J Endovasc Ther 2006;13:
81
82 Conclusions EVAR is a reasonable alternative for patient with complicated DCA D and provides satisfactory mid-term clinical outcomes. EVAR stabilizes the descending aorta in most patients and promot es aortic remodeling. However, careful attention should be given to the dissected aorta situated below the level of the SG to detect late aneurysmal degen eration.
83 Timing of Endovascular Repair The optimal timing for endovascular intervention in type B dissections remains controversial. Acute : fragile dissecting membrane, inflammation, greater potential for stent-graft induced complete remodelling of the entire aorta. Chronic : more fibrotic and seemingly stable membrane in the chronic phase, progressive thickening of the intimal flap due to fi brosis and frequently possess multiple natural fenestrations in the septum which may not be sufficient to obliterate flow in the false lumen
84
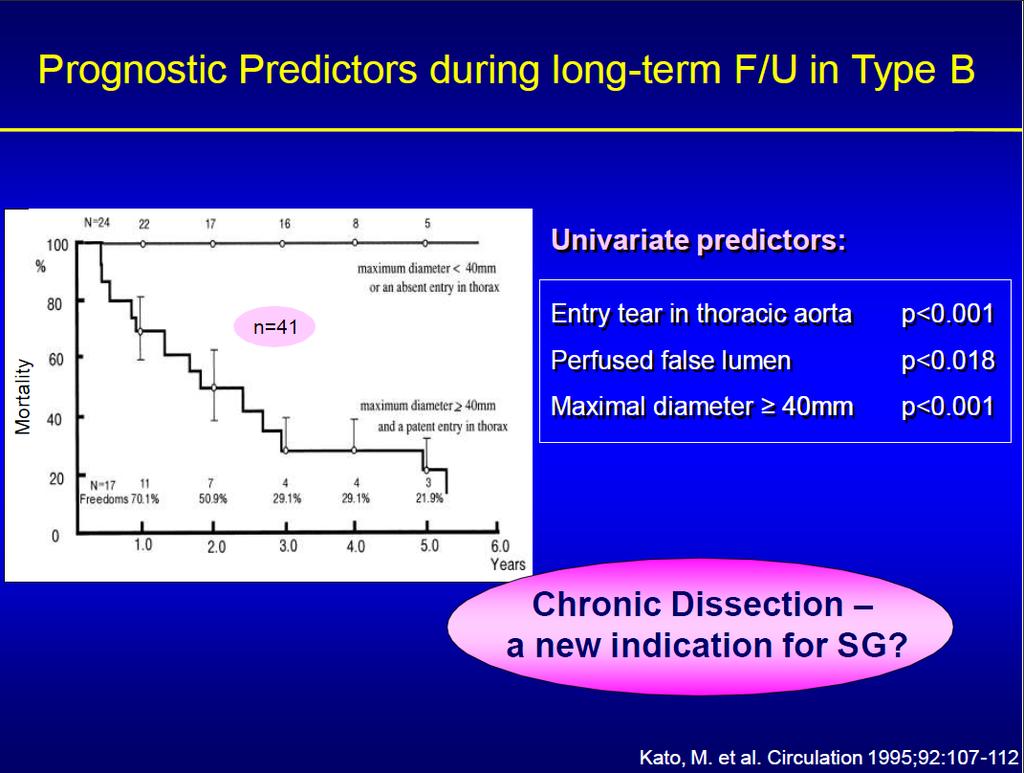
85 Kato et al. J Thorac Cardiovasc Surg 2002;124:
86 Timing of Endovascular Repair In fact, due to lack of prospective randomised data comparing immediate and delayed intervention in various clinical and anatomical constellations, no general recommendation has been issued with respect to timing of endovascular treatment so far; observational evidence, however, may favour an early intervention, when justified by complications.
87 Endovascular Repair for distal Aortic Dissection Woong Chol Kang, M.D. Gil Hospital, Gachon University, Incheon, Korea




88 Do the Data Support Endovascular Therapy for Descending Thoracic Aortic Dissections? Woong Chol Kang, M.D. Gil Hospital, Gachon University, Incheon, Korea
89
90




91 Aortic Dissection Uncommon but highly lethal Tear in the intimal layer. Blood passes into the aortic media through the tear : creating a false lumen. Propagation of the dissection causes complications :, tamponade, AI, malperfusion syndromes, aneurysm, rupture.
92 Classification Acute vs. Chronic (2weeks) Disease extension (anatomic consideration) Stanford or Debakey, Svensson (ESC) Complicated vs. Uncomplicated
93 ESC Classification
94 Complication to type B Dissection Malperfusion Refractionary hypertension Continued pain Dilatation/Aneurysm Rupture or impending rupture 20-50%/1-5yr About 30% of cases are complicated at the time of diagnosis, requiring either endovascular or surgical repair. (mortality : 20% at day 2, 25-50% at 1 M) Acute vs. Chronic and Complicated vs. Uncomplicated.
95 Unanswered question for Endovascular therapy in AD When Acute vs. Chronic
96
97 Open Surgical Repair Rupture : Graft replacement Expansion : Graft replacement Ischemia : Fenestration high in-hospital mortality (29%) new neurologic deficit (23%) stroke (9%) sustained paraplegia (5%) from IRAD registry (Circulation 2006)
98 Open Surgical Repair Rupture : Graft replacement Expansion : Graft replacement Ischemia : Fenestration high in-hospital mortality (29%) new neurologic deficit (23%) stroke (9%) sustained paraplegia (5%) from IRAD registry (Circulation 2006)
99 Current treatment of type B AD Optimal Medical Treatment Open Surgical Repair High in-hospital mortality (29%) New neurologic deficit (23%) Stroke (9%) Sustained paraplegia (5%) Circulation. 2006;114:
100 Aortic Dissection : Endovascular Tx vs. Other Tx Type A Type B Open repair With complication Without complication Open repair Endo Tx Medical Tx Endo Tx Acute With complication Without complication Chronic Open repair Endo Tx Medical Tx Endo Tx IRAD

101 Association Between Surgery and IH Mortality in Patients With Acute Complicated Type B AD: Effect of Multivariate Adjustment IRAD registry : JACC Int. 2008;1:
102
103


104 Concept of Endovascular Repair in AD Closure of the Proximal Entry tear Depressurization of the False Lumen Redirection of blood flow towards the TL Thrombosis of the FL Induction of aortic remodeling
105 IRAD : International Registry of Aortic Dissection The International Registry of Aortic Dissection (IRAD) represents 21 large centers in 11 countries which between 1996 and 2003 collected 571 type B AD. Patients with symptoms of ischemia or refractory pain underwent an intervention (surgery or endovascular therapy). IRAD registry : JACC Int. 2008;1:
106 Kaplan-Meier overall in-hospital survival estimates IRAD registry : JACC Int. 2008;1:
107 Conclusion : IRAD The less invasive nature of endovascular treatment seems to provide better in-hospital survival in patients with acute type B dissection. Larger randomized trials or comprehensive registries are needed to access impact on outcomes.
108
109
110 Early Open and Endovascular Thoracic Aortic Repair for Complicated Type B AD Seventy-three patients (mean age 66.3 yrs) with type B dissection (1995 to 2012) underwent early open descending aortic repair (n=24) or TEVAR (n=49). Intervention occurred in the acute (n=53) or subacute (n=20) period. Patients undergoing TEVAR were older and had an increased incidence of coronary artery disease and renal impairment (all p < 0.05). Ann Thorac Surg 2013 (In Press)
111 Early Outcomes for Open vs. TEVAR Ann Thorac Surg 2013 (In Press)
112 Early Open and Endovascular Thoracic Aortic Repair for Complicated Type B AD 57.5% Ann Thorac Surg 2013 (In Press)
113 Early Open and Endovascular Thoracic Aortic Repair for Complicated Type B AD 82.8% 80.0% Ann Thorac Surg 2013 (In Press)
114 Early Open and Endovascular Thoracic Aortic Repair for Complicated Type B AD Early aortic repair for complicated type B dissection is associated with high rates of morbidity, late mortality, and reintervention. Despite its use in a higher risk group, outcomes seen with TEVAR were similar to open repair, thus supporting the recent paradigm shift toward an endovascular approach. Ann Thorac Surg 2013 (In Press)

115 Ann Vasc Surg 2012; 26:
116 Aortic Dissection : Endovascular Tx vs. Other Tx Type A Type B Open repair With complication Without complication Open repair Endo Tx Medical Tx Endo Tx ADSORB Acute With complication Without complication Chronic Open repair Endo Tx Medical Tx Endo Tx IRAD Mortality 1M : 10.1% 1Y : 16% 5Y : 20%
117
118 Treatment of Acute Type-B AD Thoracic Endovascular Aortic Repair or Medical Management Alone? From January 2004 to May 2008, 193 consecutive patients in 2 hospitals (Nanjing and Cleveland Clinic) were treated and retrospectively placed into 1 of 2 groups TEVAR group TEVAR and antihypertensive medications (n=152) vs. Medicine group-medically alone (n=41). All TEVAR procedures were performed in the acute phase. J Am Coll Cardiol Intv 2013;6:185 91

119 Thoracic Endovascular Aortic Repair or Medical Management Alone?-Demographics J Am Coll Cardiol Intv 2013;6:185 91
120
121 Aortic Dissection : Endovascular Tx vs. Other Tx Type A Type B Open repair With complication Without complication Open repair Endo Tx Medical Tx Endo Tx ADSORB Acute With complication Without complication Chronic Open repair Endo Tx Medical Tx Endo Tx INSTEAD IRAD
122
123 The results of stent graft vs. medication for chronic type B AD This prospective multicenter comparative study. The study consisted of 303 consecutive patients with chronic type B AD from January 2007 to December 2010 who were prospectively enrolled and treated by either OMT or TEVAR. Of the patients, 219 were male and 84 were female (average age, 53.6 ± 20.3 years; range, years). Baseline diameter of the thoracic aorta was 41.2 (19.1) mm and dissection extended beyond the celiac axis in 87.1% of cases. J Vasc Surg 2013;57:406-14
124 The results of stent graft vs. medication for chronic type B AD-Midterm outcomes J Vasc Surg 2013;57:406-14
125 The results of stent graft vs. medication therapy for chronic type B-Progressive aorta disease J Vasc Surg 2013;57:406-14
126 Aortic Dissection : endovascular Tx vs. other Tx Type A Type B Open repair With complication Without complication Open repair Endo Tx Medical Tx Endo Tx ADSORB Acute With complication Without complication Chronic Open repair Endo Tx Medical Tx Endo Tx INSTEAD IRAD
127 J Thorac Cardiovasc Surg 2011;142:
128 Methods All cases of TEVAR for complicated (aortic growth, malperfusion, intractable pain) CDAD at our institution between 2000 and 2007 were retrospectively reviewed. Aortic morphology (aneurysm size, false lumen thrombosis) was assessed at multiple levels with 3- dimensional image analysis techniques.
129 Clinical data Thirty patients (39%) were considered to have a limited dissection, and the remainder (61%) had extensive dissections. limited extensive IIIa IIIb Debakey
130 Procedural data Technical success:73pts(96%). A total of 144 stent grafts were implanted.
.")
131 Patient who died on postoperative day 17 of a ruptured retrograde proximal dissection (identified at autopsy).
 Trial Circulation")
132 Randomized Comparison of Strategies for Uncomplicated Chronic Type B AD The INvestigation of STEnt Grafts in Aortic Dissection (INSTEAD) Trial Circulation 2009;120:
133
134 Conclusion : INSTEAD This is the first randomized study on elective stent-graft placement in survivors of uncomplicated type B aortic dissection. In the setting of clinically stable, so-called uncomplicated type B aortic dissection, elective stent-graft placement on top of optimized medical management fails to improve survival and adverse events within an observation period of 2 years, despite favorable aortic remodeling. This trial was underpowered to reach statistical significance. This trial with long-term follow-up may find a survival advantage for stent-grafting over medical management especially when late aneurismal degeneration is considered.
135
136 Patient who died on postoperative day 17 of a ruptured retrograde proximal dissection (identified at autopsy).
137 Timing of Endovascular Repair Acute Fragile dissecting membrane Inflammation Greater potential for stent-graft induced complete remodeling of the entire aorta. Chronic More fibrotic and seemingly stable membrane Progressive thickening of the intimal flap due to fibr osis and frequently possess multiple natural fenest rations in the septum which may not be sufficient to obliterate flow in the false lumen
138 Eur J Vasc Endovasc Surg 2009;37:
139 J Thorac Cardiovasc Surg 2002;124:
140 Complication to type B Dissection Malperfusion Refractionary hypertension Continued pain Dilatation/Aneurysm Rupture or impending rupture 30% 20-50%/1-5yr Intervention Open surgical repair Endovascular therapy
141 Complication to type B Dissection Malperfusion Refractionary hypertension Continued pain Dilatation/Aneurysm Rupture or impending rupture 30% 20-50%/1-5yr
142 Kaplan-Meier overall in-hospital survival estimates The less invasive nature of endovascular treatment seems to provide better in-hospital survival in patients with acute type B dissection. IRAD registry : JACC Int. 2008;1:
143 Complicated Acute Type B AD:Is Surgery Still the Best Option?-IH Cx & mortality IRAD registry : JACC Int. 2008;1:
144 Endovascular Stent-Graft Placement or Open Surgery for the Treatment of Acute Type B Aortic Dissection: A Meta-Analysis Thirty-day mortality Stroke Long-term mortality Reintervention TEVAR can be weakly recommended as an alternative for the selective treatment of ATBAD but cannot always be used in case of surgery. Ann Vasc Surg 2012; 26:

145 Endovascular treatment of uncomplicated acute type B AD-long term outcomes Fattori R, Nienaber C AHA 2010
146 The results of stent graft vs. medication for chronic type B-Aortic remodeling This was the first prospective multicenter comparative study on the treatment of type B aortic dissection in China. TEVAR had a significantly lower aorta-related mortality compared with OMT but failed to improve overall survival rate or lower the aorta-related adverse event rate. J Vasc Surg 2013;57:406-14
Treatment of acute type B aortic dissection: Current status
 MEET Cannes, 18. - 21.06.2009 Treatment of acute type B aortic dissection: Current status Christoph A. Nienaber, MD, FACC University of Rostock Department of Internal Medicine, Cardiology christoph.nienaber@med.uni-rostock.de
MEET Cannes, 18. - 21.06.2009 Treatment of acute type B aortic dissection: Current status Christoph A. Nienaber, MD, FACC University of Rostock Department of Internal Medicine, Cardiology christoph.nienaber@med.uni-rostock.de
UC SF An Algorithm to Choose Which Uncomplicated (Asymptomatic) Acute Type B Dissection Patients Should Undergo TEVAR. Disclosures.
 Acute Type B Dissection Patients Should Undergo TEVAR. Disclosures.") An Algorithm to Choose Which Uncomplicated (Asymptomatic) Acute Type B Dissection Patients Should Undergo TEVAR Disclosures Royalties and research grant support from Cook Medical, Inc. Jade S. Hiramoto,
An Algorithm to Choose Which Uncomplicated (Asymptomatic) Acute Type B Dissection Patients Should Undergo TEVAR Disclosures Royalties and research grant support from Cook Medical, Inc. Jade S. Hiramoto,
Animesh Rathore, MD 4/22/17. The Great Debate 45yo Man With Uncomplicated Acute TBAD: The Case For Medical Management
 Animesh Rathore, MD 4/22/17 The Great Debate 45yo Man With Uncomplicated Acute TBAD: The Case For Medical Management Disclosures Just a young vascular surgeon who would like to keep his job My opponent
Animesh Rathore, MD 4/22/17 The Great Debate 45yo Man With Uncomplicated Acute TBAD: The Case For Medical Management Disclosures Just a young vascular surgeon who would like to keep his job My opponent
Dissection de type B: l étude Instead et corollaire stratégique
 Dissection de type B: l étude Instead et corollaire stratégique Christoph A. Nienaber, MD, FACC University Rostock Heartcenter Med. Clinic I Cardiology christoph.nienaber@med.uni-rostock.de Type B aortic
Dissection de type B: l étude Instead et corollaire stratégique Christoph A. Nienaber, MD, FACC University Rostock Heartcenter Med. Clinic I Cardiology christoph.nienaber@med.uni-rostock.de Type B aortic
The Petticoat Technique Managing Type B Dissection with both Early and Long Term Considerations
 The Petticoat Technique Managing Type B Dissection with both Early and Long Term Considerations Joseph V. Lombardi, MD Professor & Chief, Division of Vascular & Endovascular Surgery Department of Surgery,
The Petticoat Technique Managing Type B Dissection with both Early and Long Term Considerations Joseph V. Lombardi, MD Professor & Chief, Division of Vascular & Endovascular Surgery Department of Surgery,
Clinical Trials of Acute and Chronic Dissections. Gregory Landry MD
 Clinical Trials of Acute and Chronic Dissections Gregory Landry MD No disclosures Acute vs chronic dissection: Definitions 1950s: Acute < 2 weeks, Chronic > 2 weeks 2013: European Interdisciplinary Consensus
Clinical Trials of Acute and Chronic Dissections Gregory Landry MD No disclosures Acute vs chronic dissection: Definitions 1950s: Acute < 2 weeks, Chronic > 2 weeks 2013: European Interdisciplinary Consensus
Global Evidence for the Treatment of Type B Aortic Dissection
 Global Evidence for the Treatment of Type B Aortic Dissection Ross Milner, MD Professor of Surgery Director, Center for Aortic Diseases September 17, 2016 Disclosures Consultant Cook, Endospan, Medtronic,
Global Evidence for the Treatment of Type B Aortic Dissection Ross Milner, MD Professor of Surgery Director, Center for Aortic Diseases September 17, 2016 Disclosures Consultant Cook, Endospan, Medtronic,
UC SF Early Intervention in Type B Dissection: Results From the INSTEAD XL Trial. Acute Type B Dissection. Outline. Disclosures.
 Early Intervention in Type B Dissection: Results From the INSTEAD XL Trial None Disclosures Jade S. Hiramoto, MD, MAS April 4, 2014 Outline Background Current treatment Results from INSTEAD trial Results
Early Intervention in Type B Dissection: Results From the INSTEAD XL Trial None Disclosures Jade S. Hiramoto, MD, MAS April 4, 2014 Outline Background Current treatment Results from INSTEAD trial Results
Is there a way to predict the risk in uncomplicated Type B aortic dissections? FRANS MOLL University Medical Centre Utrecht - Netherlands
 Is there a way to predict the risk in uncomplicated Type B aortic dissections? FRANS MOLL University Medical Centre Utrecht - Netherlands Disclosures: - Consultant Philips Health Care - Best Doctors Overview
Is there a way to predict the risk in uncomplicated Type B aortic dissections? FRANS MOLL University Medical Centre Utrecht - Netherlands Disclosures: - Consultant Philips Health Care - Best Doctors Overview
UC SF. Disclosures. Thoracic Endovascular Aortic Repair 4/24/2009. Management of Acute Dissections: Is There Still a Role for Open Surgery?
 UC SF Management of Acute Dissections: Is There Still a Role for Open Surgery? Darren B. Schneider, M.D. Assistant Professor of Surgery and Radiology Division of Vascular Surgery University of California
UC SF Management of Acute Dissections: Is There Still a Role for Open Surgery? Darren B. Schneider, M.D. Assistant Professor of Surgery and Radiology Division of Vascular Surgery University of California
Indications for stent grafts in type B aortic dissection
 expert opinion I Akin C A Nienaber Indications for stent grafts in type B aortic dissection ibrahim akin christoph a nienaber Department of Medicine, Divisions of Cardiology, Pulmology and Intensive Care
expert opinion I Akin C A Nienaber Indications for stent grafts in type B aortic dissection ibrahim akin christoph a nienaber Department of Medicine, Divisions of Cardiology, Pulmology and Intensive Care
No Disclosure. Aortic Dissection in Japan. This. The Challenge of Acute and Chronic Type B Aortic Dissections with Endovascular Aortic Repair
 No Disclosure The Challenge of Acute and Chronic Type B Aortic Dissections with Endovascular Aortic Repair Toru Kuratani Department of Cardiovascular Surgery Osaka University Graduate School of Medicine,
No Disclosure The Challenge of Acute and Chronic Type B Aortic Dissections with Endovascular Aortic Repair Toru Kuratani Department of Cardiovascular Surgery Osaka University Graduate School of Medicine,
Performance of the conformable GORE TAG device in Type B aortic dissection from the GORE GREAT real world registry
 University of Milan Thoracic Aortic Research Center Performance of the conformable GORE TAG device in Type B aortic dissection from the GORE GREAT real world registry Santi Trimarchi, MD, PhD Associate
University of Milan Thoracic Aortic Research Center Performance of the conformable GORE TAG device in Type B aortic dissection from the GORE GREAT real world registry Santi Trimarchi, MD, PhD Associate
Are stent-grafts for acute type B dissection durable? Est-ce que les stents graft pour la dissection aigue de type B sont efficaces à moyen terme?
 Are stent-grafts for acute type B dissection durable? Est-ce que les stents graft pour la dissection aigue de type B sont efficaces à moyen terme? Martin Björck, Johnny Steuer, Anders Wanhainen Uppsala
Are stent-grafts for acute type B dissection durable? Est-ce que les stents graft pour la dissection aigue de type B sont efficaces à moyen terme? Martin Björck, Johnny Steuer, Anders Wanhainen Uppsala
I-Hui Wu, M.D. Ph.D. Clinical Assistant Professor Cardiovascular Surgical Department National Taiwan University Hospital
 Comparisons of Aortic Remodeling and Outcomes after Endovascular Repair of Acute and Chronic Complicated Type B Aortic Dissections I-Hui Wu, M.D. Ph.D. Clinical Assistant Professor Cardiovascular Surgical
Comparisons of Aortic Remodeling and Outcomes after Endovascular Repair of Acute and Chronic Complicated Type B Aortic Dissections I-Hui Wu, M.D. Ph.D. Clinical Assistant Professor Cardiovascular Surgical
Acute non-complicated TBD Do need TEVAR treatment
 Acute non-complicated TBD Do need TEVAR treatment Prof. Dr. med. Christoph A. Nienaber Universität Rostock Universitäres Herzzentrum christoph.nienaber@med.uni-rostock.de Survival in type B dissection
Acute non-complicated TBD Do need TEVAR treatment Prof. Dr. med. Christoph A. Nienaber Universität Rostock Universitäres Herzzentrum christoph.nienaber@med.uni-rostock.de Survival in type B dissection
TEVAR for Chronic dissections: indications for TEVAR, long term results
 TEVAR for Chronic dissections: indications for TEVAR, long term results J Sobocinski, R Azzaoui, B Maurel, R Spear, T Martin-Gonzalez, A Hertault, S Haulon Centre de l Aorte, Chirurgie vasculaire, Hôpital
TEVAR for Chronic dissections: indications for TEVAR, long term results J Sobocinski, R Azzaoui, B Maurel, R Spear, T Martin-Gonzalez, A Hertault, S Haulon Centre de l Aorte, Chirurgie vasculaire, Hôpital
Early outcomes of acute retrograde dissection in the aortic arch and the ascending aorta data from IRAD
 Early outcomes of acute retrograde dissection in the aortic arch and the ascending aorta data from IRAD Foeke JH Nauta, MD, PhD Resident Cardiothoracic Surgery, Academic Medical Center, Amsterdam Disclosure
Early outcomes of acute retrograde dissection in the aortic arch and the ascending aorta data from IRAD Foeke JH Nauta, MD, PhD Resident Cardiothoracic Surgery, Academic Medical Center, Amsterdam Disclosure
Total endovascular techniques utilization in aortic dissection radical treatment
 Total endovascular techniques utilization in aortic dissection radical treatment Chang Shu, MD, PhD Vascular Surgery Center National Center for Cardiovascular Diseases. Fuwai Hospital, CAMS & PUMC Beijing,
Total endovascular techniques utilization in aortic dissection radical treatment Chang Shu, MD, PhD Vascular Surgery Center National Center for Cardiovascular Diseases. Fuwai Hospital, CAMS & PUMC Beijing,
Management of Acute Aortic Syndromes. M. Grabenwoger, MD Dept. of Cardiovascular Surgery Hospital Hietzing, Vienna, Austria
 Management of Acute Aortic Syndromes M. Grabenwoger, MD Dept. of Cardiovascular Surgery Hospital Hietzing, Vienna, Austria I have nothing to disclose. Acute Aortic Syndromes Acute Aortic Dissection Type
Management of Acute Aortic Syndromes M. Grabenwoger, MD Dept. of Cardiovascular Surgery Hospital Hietzing, Vienna, Austria I have nothing to disclose. Acute Aortic Syndromes Acute Aortic Dissection Type
Is a Paradigm Shift towards Early Endovascular Treatment of Type B Dissection justified?
 Is a Paradigm Shift towards Early Endovascular Treatment of Type B Dissection justified? Dittmar Böckler Department of Vascular and Endovascular Surgery University of Heidelberg, Germany Disclosure Speaker
Is a Paradigm Shift towards Early Endovascular Treatment of Type B Dissection justified? Dittmar Böckler Department of Vascular and Endovascular Surgery University of Heidelberg, Germany Disclosure Speaker
F. Terzi, S. Gianstefani, R. Fattori. cardiology and interventional cardiology unit, ospedali riuniti Marche nord, pesaro.
 14_14 03/02/17 14.16 Pagina 101 Type B aortic dissection: it should Be TreaTed F. Terzi, S. Gianstefani, R. Fattori cardiology and interventional cardiology unit, ospedali riuniti Marche nord, pesaro.
14_14 03/02/17 14.16 Pagina 101 Type B aortic dissection: it should Be TreaTed F. Terzi, S. Gianstefani, R. Fattori cardiology and interventional cardiology unit, ospedali riuniti Marche nord, pesaro.
ADSORB trial results: Is it enough to switch the paradigm?
 ADSORB trial results: Is it enough to switch the paradigm? Jan Brunkwall, MD, PhD Professor and Chairman Complications to acute type B dissection Mortality Rupture Organ Ischemia Dilatation/Aneurysm Refractory
ADSORB trial results: Is it enough to switch the paradigm? Jan Brunkwall, MD, PhD Professor and Chairman Complications to acute type B dissection Mortality Rupture Organ Ischemia Dilatation/Aneurysm Refractory
Antegrade Thoracic Stent Grafting during Repair of Acute Debakey I Dissection: Promotes Distal Aortic Remodeling and Reduces Late Open Re-operation
 Antegrade Thoracic Stent Grafting during Repair of Acute Debakey I Dissection: Promotes Distal Aortic Remodeling and Reduces Late Open Re-operation Vallabhajosyula, P: Szeto, W; Desai, N; Pulsipher, A;
Antegrade Thoracic Stent Grafting during Repair of Acute Debakey I Dissection: Promotes Distal Aortic Remodeling and Reduces Late Open Re-operation Vallabhajosyula, P: Szeto, W; Desai, N; Pulsipher, A;
Endovascular Treatment of Malperfusion Syndrome
 Endovascular Treatment of Malperfusion Syndrome in Type B Aortic Dissection Department of Cardiology, Pusan National luniveristy i Hospital, Han Cheol Lee Endovascular Treatment Indication of Type B Aortic
Endovascular Treatment of Malperfusion Syndrome in Type B Aortic Dissection Department of Cardiology, Pusan National luniveristy i Hospital, Han Cheol Lee Endovascular Treatment Indication of Type B Aortic
The conundrum about complicated and uncomplicated type B dissection New concepts?
 The conundrum about complicated and uncomplicated type B dissection New concepts? Professor Christoph A. Nienaber The Royal Brompton and Harefield NHS Trust Cardiology and Aortic Centre C.Nienaber@rbht.nhs.uk
The conundrum about complicated and uncomplicated type B dissection New concepts? Professor Christoph A. Nienaber The Royal Brompton and Harefield NHS Trust Cardiology and Aortic Centre C.Nienaber@rbht.nhs.uk
Acute Aortic Dissection: Decision and Outcome
 Acute Aortic Dissection: Decision and Outcome Marc R. Moon, M.D. John M. Shoenberg Chair in CV Disease Chief, Cardiac Surgery Director, Center for Diseases of the Thoracic Aorta Washington University School
Acute Aortic Dissection: Decision and Outcome Marc R. Moon, M.D. John M. Shoenberg Chair in CV Disease Chief, Cardiac Surgery Director, Center for Diseases of the Thoracic Aorta Washington University School
WHICH PLACE FOR EMERGENT INTERVENTION IN COMPLICATED ACUTE TYPE B DISSECTION (ctbaod)
") WHICH PLACE FOR EMERGENT INTERVENTION IN COMPLICATED ACUTE TYPE B DISSECTION (ctbaod) Epidemiology of type B Aortic Dissection TYPE B dissection: 0,5-2,1/100.000/year (40% of all dissection) Hospital mortality
WHICH PLACE FOR EMERGENT INTERVENTION IN COMPLICATED ACUTE TYPE B DISSECTION (ctbaod) Epidemiology of type B Aortic Dissection TYPE B dissection: 0,5-2,1/100.000/year (40% of all dissection) Hospital mortality
Acute dissections of the descending thoracic aorta (Debakey
 Endovascular Treatment of Acute Descending Thoracic Aortic Dissections Nimesh D. Desai, MD, PhD, and Joseph E. Bavaria, MD Acute dissections of the descending thoracic aorta (Debakey type III or Stanford
Endovascular Treatment of Acute Descending Thoracic Aortic Dissections Nimesh D. Desai, MD, PhD, and Joseph E. Bavaria, MD Acute dissections of the descending thoracic aorta (Debakey type III or Stanford
Contemporary Management of Acute Type B Aortic Dissection
 Contemporary Management of Acute Type B Aortic Dissection Bradley G. Leshnower MD Assistant Professor of Surgery Division of Cardiothoracic Surgery Emory University School of Medicine Georgia Vascular
Contemporary Management of Acute Type B Aortic Dissection Bradley G. Leshnower MD Assistant Professor of Surgery Division of Cardiothoracic Surgery Emory University School of Medicine Georgia Vascular
Type B Dissection Sub-Categories
 Disclosure Nothing to disclose Type B Dissection On Whom to Operate on and When to do it Charles Eichler Professor, Department of Surgery Division of Vascular and Endovascular Surgery University of California
Disclosure Nothing to disclose Type B Dissection On Whom to Operate on and When to do it Charles Eichler Professor, Department of Surgery Division of Vascular and Endovascular Surgery University of California
Endovascular surgery in Marfan syndrome: CON
 Perspective Endovascular surgery in Marfan syndrome: CON Nicholas T. Kouchoukos Division of Cardiovascular and Thoracic Surgery, Missouri Baptist Medical Center, BJC Healthcare, St. Louis, Missouri, USA
Perspective Endovascular surgery in Marfan syndrome: CON Nicholas T. Kouchoukos Division of Cardiovascular and Thoracic Surgery, Missouri Baptist Medical Center, BJC Healthcare, St. Louis, Missouri, USA
The role of false lumen intervention to promote remodelling via induced thrombosis the FLIRT concept
 The role of false lumen intervention to promote remodelling via induced thrombosis the FLIRT concept Professor Christoph A. Nienaber The Royal Brompton and Harefield NHS Trust Cardiology and Aortic Centre
The role of false lumen intervention to promote remodelling via induced thrombosis the FLIRT concept Professor Christoph A. Nienaber The Royal Brompton and Harefield NHS Trust Cardiology and Aortic Centre
Asymptomatic Radiology / Clinical data Report / Cohort bias Referral bias. UCSF Vascular Symposium April 7-9, Acute Aortic Dissection
 Aortic Dissection: Natural History What is the Natural History of Aortic Dissection? UCSF Vascular Symposium April 7-9, 2011 Asymptomatic Radiology / Clinical data Report / Cohort bias Referral bias Stephen
Aortic Dissection: Natural History What is the Natural History of Aortic Dissection? UCSF Vascular Symposium April 7-9, 2011 Asymptomatic Radiology / Clinical data Report / Cohort bias Referral bias Stephen
Combined Endovascular and Surgical Repair of Thoracoabdominal Aortic Pathology: Hybrid TEVAR
 Combined Endovascular and Surgical Repair of Thoracoabdominal Aortic Pathology: Hybrid TEVAR William J. Quinones-Baldrich MD Professor of Surgery Director UCLA Aortic Center UCLA Medical Center Los Angeles,
Combined Endovascular and Surgical Repair of Thoracoabdominal Aortic Pathology: Hybrid TEVAR William J. Quinones-Baldrich MD Professor of Surgery Director UCLA Aortic Center UCLA Medical Center Los Angeles,
Aggressive Resection/Reconstruction of the Aortic Arch in Type A Dissection
 Aggressive Resection/Reconstruction of the Aortic Arch in Type A Dissection M. Grabenwoger Dept. of Cardiovascular Surgery Hospital Hietzing Vienna, Austria Disclosure Statement Consultant of Jotec, Hechingen,
Aggressive Resection/Reconstruction of the Aortic Arch in Type A Dissection M. Grabenwoger Dept. of Cardiovascular Surgery Hospital Hietzing Vienna, Austria Disclosure Statement Consultant of Jotec, Hechingen,
Vascular Intervention
 10 : 389-393, 2001 B Vascular Intervention 1 1 2 1 1 1 1 3 2 1 1997 7 2000 4 B 29 19 10 50 84 66.1 stent graft S/G primary entry stenting S/G 12 4 2 1 1 40 mm 8 1 MOF 1 endoleak + 11 91.6% 10 stenting
10 : 389-393, 2001 B Vascular Intervention 1 1 2 1 1 1 1 3 2 1 1997 7 2000 4 B 29 19 10 50 84 66.1 stent graft S/G primary entry stenting S/G 12 4 2 1 1 40 mm 8 1 MOF 1 endoleak + 11 91.6% 10 stenting
Acute Type B dissection. Closure of the infra diaphragmatic tear: how and when?
 Acute Type B dissection. Closure of the infra diaphragmatic tear: how and when? Prof. Olgierd Rowiński II Department of Clinical Radiology Medical University of Warsaw Disclosure Speaker name: Olgierd
Acute Type B dissection. Closure of the infra diaphragmatic tear: how and when? Prof. Olgierd Rowiński II Department of Clinical Radiology Medical University of Warsaw Disclosure Speaker name: Olgierd
Endovascular therapy for Ischemic versus Nonischemic complicated acute type B aortic dissection (catbad).
.") Endovascular therapy for Ischemic versus Nonischemic complicated acute type B aortic dissection (catbad). AS. Eleshra, MD 1, T. Kölbel, MD, PhD 1, F. Rohlffs, MD 1, N. Tsilimparis, MD, PhD 1,2 Ahmed Eleshra
Endovascular therapy for Ischemic versus Nonischemic complicated acute type B aortic dissection (catbad). AS. Eleshra, MD 1, T. Kölbel, MD, PhD 1, F. Rohlffs, MD 1, N. Tsilimparis, MD, PhD 1,2 Ahmed Eleshra
Abdominal and thoracic aneurysm repair
 Abdominal and thoracic aneurysm repair William A. Gray MD Director, Endovascular Intervention Cardiovascular Research Foundation Columbia University Medical Center Abdominal Aortic Aneurysm Endografts
Abdominal and thoracic aneurysm repair William A. Gray MD Director, Endovascular Intervention Cardiovascular Research Foundation Columbia University Medical Center Abdominal Aortic Aneurysm Endografts
CT angiography in type I acute aortic dissection complicated with malperfusion - a visual review of obstruciton patterns
 CT angiography in type I acute aortic dissection complicated with malperfusion - a visual review of obstruciton patterns Eneva M. St. Ekaterna University Hospital Report objectives 1. Review malperfusion
CT angiography in type I acute aortic dissection complicated with malperfusion - a visual review of obstruciton patterns Eneva M. St. Ekaterna University Hospital Report objectives 1. Review malperfusion
Understanding the Predictors of Aneurysmal Degeneration in Type B Dissection
 Understanding the Predictors of Aneurysmal Degeneration in Type B Dissection A case example illustrating when early endovascular intervention may provide the best outcome. BY DITTMAR BÖCKLER, MD, PhD;
Understanding the Predictors of Aneurysmal Degeneration in Type B Dissection A case example illustrating when early endovascular intervention may provide the best outcome. BY DITTMAR BÖCKLER, MD, PhD;
Acute dissections: who should we treat, and how?
 Acute dissections: who should we treat, and how? J Sobocinski, R Azzaoui, B Maurel, R Spear, T Martin-Gonzalez, A Hertault, S Haulon Centre de l Aorte, Chirurgie vasculaire, Hôpital Cardiologique, CHRU
Acute dissections: who should we treat, and how? J Sobocinski, R Azzaoui, B Maurel, R Spear, T Martin-Gonzalez, A Hertault, S Haulon Centre de l Aorte, Chirurgie vasculaire, Hôpital Cardiologique, CHRU
Redo treatment and open conversion after TEVAR
 Redo treatment and open conversion after TEVAR Roberto Chiesa Vascular Surgery, Vita-Salute University Scientific Institute San Raffaele Milan, Italy Number of procedures Off-Label indications for TEVAR
Redo treatment and open conversion after TEVAR Roberto Chiesa Vascular Surgery, Vita-Salute University Scientific Institute San Raffaele Milan, Italy Number of procedures Off-Label indications for TEVAR
Optimal Treatment of Chronic Dissection
 Optimal Treatment of Chronic Dissection Chun-Che Shih 施俊哲 MD, Ph.D. Chief, Professor Institute of Clinical Medicine National Yang Ming University Division of Cardiovascular Surgery Taipei Veterans General
Optimal Treatment of Chronic Dissection Chun-Che Shih 施俊哲 MD, Ph.D. Chief, Professor Institute of Clinical Medicine National Yang Ming University Division of Cardiovascular Surgery Taipei Veterans General
Description. Section: Surgery Effective Date: October 15, 2016 Subsection: Surgery Original Policy Date: December 7, 2011 Subject:
 Last Review Status/Date: September 2016 Page: 1 of 30 Description Thoracic endovascular aneurysm repair (TEVAR) involves the percutaneous placement of a stent graft in the descending thoracic or thoracoabdominal
Last Review Status/Date: September 2016 Page: 1 of 30 Description Thoracic endovascular aneurysm repair (TEVAR) involves the percutaneous placement of a stent graft in the descending thoracic or thoracoabdominal
Evolution of Thoracic Aortic Surgery A Rapidly Advancing Paradigm. October 15 th, 2014 Family Practice Evening Course University of Calgary
 Evolution of Thoracic Aortic Surgery A Rapidly Advancing Paradigm October 15 th, 2014 Family Practice Evening Course University of Calgary Jehangir Appoo Division of Cardiac Surgery Libin Cardiovascular
Evolution of Thoracic Aortic Surgery A Rapidly Advancing Paradigm October 15 th, 2014 Family Practice Evening Course University of Calgary Jehangir Appoo Division of Cardiac Surgery Libin Cardiovascular
Follow-up of Aortic Dissection: How, How Often, Which Consequences Euro Echo 2011
 Follow-up of Aortic Dissection: How, How Often, Which Consequences Euro Echo 2011 Susan E. Wiegers, MD, FASE Director of Clinical Echocardiography Hospital of the University of Pennsylvania Disclosure
Follow-up of Aortic Dissection: How, How Often, Which Consequences Euro Echo 2011 Susan E. Wiegers, MD, FASE Director of Clinical Echocardiography Hospital of the University of Pennsylvania Disclosure
Experience of endovascular procedures on abdominal and thoracic aorta in CA region
 Experience of endovascular procedures on abdominal and thoracic aorta in CA region May 14-15, 2015, Dubai Dr. Viktor Zemlyanskiy National Research Center of Emergency Care Astana, Kazakhstan Region Characteristics
Experience of endovascular procedures on abdominal and thoracic aorta in CA region May 14-15, 2015, Dubai Dr. Viktor Zemlyanskiy National Research Center of Emergency Care Astana, Kazakhstan Region Characteristics
Research Article Propensity Score-Matched Analysis of Open Surgical and Endovascular Repair for Type B Aortic Dissection
 Hindawi Publishing Corporation International Journal of Vascular Medicine Volume 2011, Article ID 364046, 7 pages doi:10.1155/2011/364046 Research Article Propensity Score-Matched Analysis of Open Surgical
Hindawi Publishing Corporation International Journal of Vascular Medicine Volume 2011, Article ID 364046, 7 pages doi:10.1155/2011/364046 Research Article Propensity Score-Matched Analysis of Open Surgical
What is the best treatment for False Lumen growth after type B Dissection
 What is the best treatment for False Lumen growth after type B Dissection Nikolaos Tsilimparis, Fiona Rohlffs, Yuk Law, Sebastian Debus, Tilo Kölbel N. Tsilimparis, MD, PhD, FEBVS Deputy Head of German
What is the best treatment for False Lumen growth after type B Dissection Nikolaos Tsilimparis, Fiona Rohlffs, Yuk Law, Sebastian Debus, Tilo Kölbel N. Tsilimparis, MD, PhD, FEBVS Deputy Head of German
State of Art Hybrid Approach
 State of Art Hybrid Approach for Complex Aorta Diseases Won Ho Kim, MD Division of Cardiology, Eulji University Hospital Eulji University School of Medicine, Daejeon, Korea Introduction.Hybrid procedure
State of Art Hybrid Approach for Complex Aorta Diseases Won Ho Kim, MD Division of Cardiology, Eulji University Hospital Eulji University School of Medicine, Daejeon, Korea Introduction.Hybrid procedure
Endovascular Stent Grafts for Disorders of the Thoracic Aorta
 Endovascular Stent Grafts for Disorders of the Thoracic Aorta Policy Number: 7.01.86 Last Review: 9/2017 Origination: 5/2006 Next Review: 9/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC)
Endovascular Stent Grafts for Disorders of the Thoracic Aorta Policy Number: 7.01.86 Last Review: 9/2017 Origination: 5/2006 Next Review: 9/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC)
Therapeutic Pathway In Acute Aortic Dissection. Speaker: Cesare Quarto Consultant Cardiac Surgeon Royal Brompton Hospital, London UK
 Therapeutic Pathway In Acute Aortic Dissection Speaker: Cesare Quarto Consultant Cardiac Surgeon Royal Brompton Hospital, London UK Disclosure of Interest Speaker name: Cesare Quarto I do not have any
Therapeutic Pathway In Acute Aortic Dissection Speaker: Cesare Quarto Consultant Cardiac Surgeon Royal Brompton Hospital, London UK Disclosure of Interest Speaker name: Cesare Quarto I do not have any
Malperfusion Syndromes Type B Aortic Dissection with Malperfusion
 Malperfusion Syndromes Type B Aortic Dissection with Malperfusion Jade S. Hiramoto, MD, MAS April 27, 2012 Associated with early mortality Occurs when there is end organ ischemia secondary to aortic branch
Malperfusion Syndromes Type B Aortic Dissection with Malperfusion Jade S. Hiramoto, MD, MAS April 27, 2012 Associated with early mortality Occurs when there is end organ ischemia secondary to aortic branch
Percutaneous Approaches to Aortic Disease in 2018
 Percutaneous Approaches to Aortic Disease in 2018 Wendy Tsang, MD, SM Assistant Professor, University of Toronto Toronto General Hospital, University Health Network Case 78 year old F Lower CP and upper
Percutaneous Approaches to Aortic Disease in 2018 Wendy Tsang, MD, SM Assistant Professor, University of Toronto Toronto General Hospital, University Health Network Case 78 year old F Lower CP and upper
Three year experience with multilayer stent in the treatment of thoracoabdominal aneurysms no evidence for aneurysm stabilization
 Three year experience with multilayer stent in the treatment of thoracoabdominal aneurysms no evidence for aneurysm stabilization Thomas Larzon, MD, PhD Head of Vascular Surgery Dept of Cardiothoracic
Three year experience with multilayer stent in the treatment of thoracoabdominal aneurysms no evidence for aneurysm stabilization Thomas Larzon, MD, PhD Head of Vascular Surgery Dept of Cardiothoracic
Evaluation of Dynamic Intimal Flap Movement in Acute Stanford Type B Aortic Dissections (ATBD) and the Effects of Thoracic Endovascular Stent Grafting
 and the Effects of Thoracic Endovascular Stent Grafting") Evaluation of Dynamic Intimal Flap Movement in Acute Stanford Type B Aortic Dissections (ATBD) and the Effects of Thoracic Endovascular Stent Grafting Frank R. Arko, III, MD, Jeko Madjarov, MD, Aaron Hurd,
Evaluation of Dynamic Intimal Flap Movement in Acute Stanford Type B Aortic Dissections (ATBD) and the Effects of Thoracic Endovascular Stent Grafting Frank R. Arko, III, MD, Jeko Madjarov, MD, Aaron Hurd,
Frozen Elephant Trunk in Acute Aortic Dissection
 Frozen Elephant Trunk in Acute Aortic Dissection Derek R. Brinster, M.D. Professor of Cardiovascular and Thoracic Surgery Hofstra North Shore-LIJ School of Medicine Director of Aortic Surgery for the North
Frozen Elephant Trunk in Acute Aortic Dissection Derek R. Brinster, M.D. Professor of Cardiovascular and Thoracic Surgery Hofstra North Shore-LIJ School of Medicine Director of Aortic Surgery for the North
Endovascular Stent Grafts for Disorders of the Thoracic Aorta
 Endovascular Stent Grafts for Disorders of the Thoracic Aorta Policy Number: 7.01.86 Last Review: 9/2018 Origination: 5/2006 Next Review: 9/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC)
Endovascular Stent Grafts for Disorders of the Thoracic Aorta Policy Number: 7.01.86 Last Review: 9/2018 Origination: 5/2006 Next Review: 9/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC)
Optimal repair of acute aortic dissection
 Optimal repair of acute aortic dissection Dept. of Vascular Surgery, The 2nd Xiang-Yale Hospital, Central-South University, China Hunan Major Vessels Diseases Clinical Center Chang Shu Email:changshu01@yahoo.com
Optimal repair of acute aortic dissection Dept. of Vascular Surgery, The 2nd Xiang-Yale Hospital, Central-South University, China Hunan Major Vessels Diseases Clinical Center Chang Shu Email:changshu01@yahoo.com
Accepted Manuscript. Is A More Extensive Operation Justified for Acute Type A Dissection Repair? Dr. Leonard N. Girardi
 Accepted Manuscript Is A More Extensive Operation Justified for Acute Type A Dissection Repair? Dr. Leonard N. Girardi PII: S0022-5223(18)32552-2 DOI: 10.1016/j.jtcvs.2018.09.048 Reference: YMTC 13502
Accepted Manuscript Is A More Extensive Operation Justified for Acute Type A Dissection Repair? Dr. Leonard N. Girardi PII: S0022-5223(18)32552-2 DOI: 10.1016/j.jtcvs.2018.09.048 Reference: YMTC 13502
AORTIC DISSECTIONS Current Management. TOMAS D. MARTIN, MD, LAT Professor, TCV Surgery Director UF Health Aortic Disease Center University of Florida
 AORTIC DISSECTIONS Current Management TOMAS D. MARTIN, MD, LAT Professor, TCV Surgery Director UF Health Aortic Disease Center University of Florida DISCLOSURES Terumo Medtronic Cook Edwards Cryolife AORTIC
AORTIC DISSECTIONS Current Management TOMAS D. MARTIN, MD, LAT Professor, TCV Surgery Director UF Health Aortic Disease Center University of Florida DISCLOSURES Terumo Medtronic Cook Edwards Cryolife AORTIC
The morbidity and mortality rates associated with the. Outcome of Surgical Treatment in Patients With Acute Type B Aortic Dissection
 Outcome of Surgical Treatment in Patients With Acute Type B Aortic Dissection Tomoki Shimokawa, MD, Kazutaka Horiuchi, MD, Naomi Ozawa, MD, Kenu Fumimoto, MD, Susumu Manabe, MD, Tetsuya Tobaru, MD, and
Outcome of Surgical Treatment in Patients With Acute Type B Aortic Dissection Tomoki Shimokawa, MD, Kazutaka Horiuchi, MD, Naomi Ozawa, MD, Kenu Fumimoto, MD, Susumu Manabe, MD, Tetsuya Tobaru, MD, and
Emerging Roles for Distal Aortic Interventions in Type A Dissection Surgery
 Emerging Roles for Distal Aortic Interventions in Type A Dissection Surgery Type A Dissection Workshop 2014 CCC Vancouver Oct 26 th, 2014 Jehangir Appoo Libin Cardiovascular Institute University of Calgary
Emerging Roles for Distal Aortic Interventions in Type A Dissection Surgery Type A Dissection Workshop 2014 CCC Vancouver Oct 26 th, 2014 Jehangir Appoo Libin Cardiovascular Institute University of Calgary
Open fenestration for complicated acute aortic B dissection
 Art of Operative Techniques Open fenestration for complicated acute aortic B dissection Santi Trimarchi 1, Sara Segreti 1, Viviana Grassi 1, Chiara Lomazzi 1, Marta Cova 1, Gabriele Piffaretti 2, Vincenzo
Art of Operative Techniques Open fenestration for complicated acute aortic B dissection Santi Trimarchi 1, Sara Segreti 1, Viviana Grassi 1, Chiara Lomazzi 1, Marta Cova 1, Gabriele Piffaretti 2, Vincenzo
Intravascular Ultrasound in the Treatment of Complex Aortic Pathologies. Naixin Kang, M.D. Vascular Surgery Fellow April 26 th, 2018
 Intravascular Ultrasound in the Treatment of Complex Aortic Pathologies Naixin Kang, M.D. Vascular Surgery Fellow April 26 th, 2018 DISCLOSURES Nothing To Disclose 2 ENDOVASCULAR AORTIC INTERVENTION Improved
Intravascular Ultrasound in the Treatment of Complex Aortic Pathologies Naixin Kang, M.D. Vascular Surgery Fellow April 26 th, 2018 DISCLOSURES Nothing To Disclose 2 ENDOVASCULAR AORTIC INTERVENTION Improved
Endovascular Management of Thoracic Aortic Pathology Stéphan Haulon, J Sobocinski, B Maurel, T Martin-Gonzalez, R Spear, A Hertault, R Azzaoui
 Endovascular Management of Thoracic Aortic Pathology Stéphan Haulon, J Sobocinski, B Maurel, T Martin-Gonzalez, R Spear, A Hertault, R Azzaoui Aortic Center, Lille University Hospital, France Disclosures
Endovascular Management of Thoracic Aortic Pathology Stéphan Haulon, J Sobocinski, B Maurel, T Martin-Gonzalez, R Spear, A Hertault, R Azzaoui Aortic Center, Lille University Hospital, France Disclosures
Development of Stent Graft. Kato et al. Development of an expandable intra-aortic prothesis for experimental aortic dissection.
 Development of Stent Graft Kato et al. Development of an expandable intra-aortic prothesis for experimental aortic dissection. ASAIO J 1993 The New England Journal of Medicine Downloaded from nejm.org
Development of Stent Graft Kato et al. Development of an expandable intra-aortic prothesis for experimental aortic dissection. ASAIO J 1993 The New England Journal of Medicine Downloaded from nejm.org
Transluminal Stent-graft Placement endovascular surgery
 13 545 551 2004 Transluminal Stent-graft Placement endovascular surgery 1 1 2 2 1 1 1 3 2 1 1996 11Transluminal Stent-graft Placement TSGP 6 82 TSGP T42 O TSGP Th10 T 26 O 5 T 3 O 23T 6 O 2 T 47 A15B17B15O
13 545 551 2004 Transluminal Stent-graft Placement endovascular surgery 1 1 2 2 1 1 1 3 2 1 1996 11Transluminal Stent-graft Placement TSGP 6 82 TSGP T42 O TSGP Th10 T 26 O 5 T 3 O 23T 6 O 2 T 47 A15B17B15O
Aortic dissection is one of the most catastrophic events that affects
 Surgery for Acquired Cardiovascular Disease Midterm results of stent-graft repair of acute and chronic aortic dissection with descending tear: The complicationspecific approach Noriyuki Kato, MD a Takatsugu
Surgery for Acquired Cardiovascular Disease Midterm results of stent-graft repair of acute and chronic aortic dissection with descending tear: The complicationspecific approach Noriyuki Kato, MD a Takatsugu
La sindrome aortica acuta oggi
 University of Milan Thoracic Aortic Research Center La sindrome aortica acuta oggi Santi Trimarchi, MD, PhD Professore Associato di Chirurgia Vascolare, Università degli Studi di Milano Direttore, Divisione
University of Milan Thoracic Aortic Research Center La sindrome aortica acuta oggi Santi Trimarchi, MD, PhD Professore Associato di Chirurgia Vascolare, Università degli Studi di Milano Direttore, Divisione
Aortic Arch Treatment Open versus Endo Evidence versus Zeitgeist. M. Grabenwoger Dept. of Cardiovascular Surgery Hospital Hietzing Vienna, Austria
 Aortic Arch Treatment Open versus Endo Evidence versus Zeitgeist M. Grabenwoger Dept. of Cardiovascular Surgery Hospital Hietzing Vienna, Austria Evidence Surgical aortic arch replacement with a Dacron
Aortic Arch Treatment Open versus Endo Evidence versus Zeitgeist M. Grabenwoger Dept. of Cardiovascular Surgery Hospital Hietzing Vienna, Austria Evidence Surgical aortic arch replacement with a Dacron
ENCORE, a Study to Investigate the Durability of Polymer EVAR with Ovation A Contemporary Review of 1296 Patients
 ENCORE, a Study to Investigate the Durability of Polymer EVAR with Ovation A Contemporary Review of 1296 Patients The Ovation System is approved to treat infrarenal abdominal aortic aneurysms and is not
ENCORE, a Study to Investigate the Durability of Polymer EVAR with Ovation A Contemporary Review of 1296 Patients The Ovation System is approved to treat infrarenal abdominal aortic aneurysms and is not
Aortic Neck Issues Associated Clinical Sequelae/Implications for Graft Choice
 Aortic Neck Issues Associated Clinical Sequelae/Implications for Graft Choice Eric Verhoeven, MD, PhD, A. Katsargyris, MD Department of Vascular and Endovascular Surgery, Paracelsus Medical University,
Aortic Neck Issues Associated Clinical Sequelae/Implications for Graft Choice Eric Verhoeven, MD, PhD, A. Katsargyris, MD Department of Vascular and Endovascular Surgery, Paracelsus Medical University,
Current treatment of Aortic Aneurysms and Dissections. Adam Keefer, MD, FACS Sean Hislop, MD, FACS
 Current treatment of Aortic Aneurysms and Dissections Adam Keefer, MD, FACS Sean Hislop, MD, FACS Patient 1 69 year old well-educated man with reoccurring pain in his upper abdomen and a pulsatile mass.
Current treatment of Aortic Aneurysms and Dissections Adam Keefer, MD, FACS Sean Hislop, MD, FACS Patient 1 69 year old well-educated man with reoccurring pain in his upper abdomen and a pulsatile mass.
Pioneering EVAR techniques in aortic dissection
 Pioneering EVAR techniques in aortic dissection Jianing Yue, Weiguo Fu Department of Vascular Surgery Zhongshan Hospital Fudan University Shanghai, China LINC Asia-Pacific 2016 March 8-10, 2016 Hong Kong
Pioneering EVAR techniques in aortic dissection Jianing Yue, Weiguo Fu Department of Vascular Surgery Zhongshan Hospital Fudan University Shanghai, China LINC Asia-Pacific 2016 March 8-10, 2016 Hong Kong
An Overview of Post-EVAR Endoleaks: Imaging Findings and Management. Ravi Shergill BSc Sean A. Kennedy MD Mark O. Baerlocher MD FRCPC
 An Overview of Post-EVAR Endoleaks: Imaging Findings and Management Ravi Shergill BSc Sean A. Kennedy MD Mark O. Baerlocher MD FRCPC Disclosure Slide Mark O. Baerlocher: Current: Consultant for Boston
An Overview of Post-EVAR Endoleaks: Imaging Findings and Management Ravi Shergill BSc Sean A. Kennedy MD Mark O. Baerlocher MD FRCPC Disclosure Slide Mark O. Baerlocher: Current: Consultant for Boston
Optimised management of type A aortic dissection with visceral malperfusion concept to reconsider
 Optimised management of type A aortic dissection with visceral malperfusion concept to reconsider Matthias Thielmann, MD, PhD, FAHA Thoracic and Cardiovascular Surgery, West-German Heart and Vascular Center
Optimised management of type A aortic dissection with visceral malperfusion concept to reconsider Matthias Thielmann, MD, PhD, FAHA Thoracic and Cardiovascular Surgery, West-German Heart and Vascular Center
FEVAR FIFTEEN YEARS OF EFFICIENCY E.DUCASSE MD PHD FEBVS CHU DE BORDEAUX
 FEVAR FIFTEEN YEARS OF EFFICIENCY E.DUCASSE MD PHD FEBVS CHU DE BORDEAUX 2018 A BIT OF HISTORY First use of F-EVAR : 1990s Park et al. J Vasc Interv Radiol. 1996;7:819-823. Faruqi et al. J Endovasc Surg.
FEVAR FIFTEEN YEARS OF EFFICIENCY E.DUCASSE MD PHD FEBVS CHU DE BORDEAUX 2018 A BIT OF HISTORY First use of F-EVAR : 1990s Park et al. J Vasc Interv Radiol. 1996;7:819-823. Faruqi et al. J Endovasc Surg.
Morphological analysis of the thoracic aorta in case of TBAD without treatment.
 Master project: Hemodynamic pattern of type B aortic dissection progression and remodelling of the false lumen after endovascular treatment: imaging informed numerical simulations Aortic dissection is
Master project: Hemodynamic pattern of type B aortic dissection progression and remodelling of the false lumen after endovascular treatment: imaging informed numerical simulations Aortic dissection is
Aggressive Resection/Reconstruction of the Aortic Arch in Type A Dissection: Con
 Aggressive Resection/Reconstruction of the Aortic Arch in Type A Dissection: Con Thomas G. Gleason, M.D. Ronald V. Pellegrini Professor and Chief Division of Cardiac Surgery University of Pittsburgh Presenter
Aggressive Resection/Reconstruction of the Aortic Arch in Type A Dissection: Con Thomas G. Gleason, M.D. Ronald V. Pellegrini Professor and Chief Division of Cardiac Surgery University of Pittsburgh Presenter
TEVAR. (Thoracic Endovascular Aortic Repair) for Aneurysm and Dissection. Bruce Tjaden MD Vascular Surgery Fellow
 for Aneurysm and Dissection. Bruce Tjaden MD Vascular Surgery Fellow") Department of Cardiothoracic & Vascular Surgery McGovern Medical School / The University of Texas Health Science Center at Houston TEVAR (Thoracic Endovascular Aortic Repair) for Aneurysm and Dissection
Department of Cardiothoracic & Vascular Surgery McGovern Medical School / The University of Texas Health Science Center at Houston TEVAR (Thoracic Endovascular Aortic Repair) for Aneurysm and Dissection
Animesh Rathore, MD 4/21/17. Penetrating atherosclerotic ulcers of aorta
 Animesh Rathore, MD 4/21/17 Penetrating atherosclerotic ulcers of aorta Disclosures No financial disclosures Thank You Dr. Panneton for giving this lecture for me. I am stuck at Norfolk with an emergency
Animesh Rathore, MD 4/21/17 Penetrating atherosclerotic ulcers of aorta Disclosures No financial disclosures Thank You Dr. Panneton for giving this lecture for me. I am stuck at Norfolk with an emergency
The natural history of uncomplicated type B dissection, PAU and IMH: the IRAD knowledge. Santi Trimarchi, MD, PhD
 IRCCS Policlinico San Donato University of Milan Thoracic Aortic Research Center The natural history of uncomplicated type B dissection, PAU and IMH: the IRAD knowledge Santi Trimarchi, MD, PhD No COI
IRCCS Policlinico San Donato University of Milan Thoracic Aortic Research Center The natural history of uncomplicated type B dissection, PAU and IMH: the IRAD knowledge Santi Trimarchi, MD, PhD No COI
6. Endovascular aneurysm repair
 Introduction The standard treatment for aortic aneurysm, open repair, involves a large abdominal incision and cross-clamping of the aorta. In recent years, a minimally invasive technique, endovascular
Introduction The standard treatment for aortic aneurysm, open repair, involves a large abdominal incision and cross-clamping of the aorta. In recent years, a minimally invasive technique, endovascular
Carotid Artery Stenting
 Carotid Artery Stenting Woong Chol Kang M.D. Gil Medical Center, Gachon University of Medicine and Science, Incheon, Korea Carotid Stenosis and Stroke ~25% of stroke is due to carotid disease, the reminder
Carotid Artery Stenting Woong Chol Kang M.D. Gil Medical Center, Gachon University of Medicine and Science, Incheon, Korea Carotid Stenosis and Stroke ~25% of stroke is due to carotid disease, the reminder
Challenges. 1. Sizing. 2. Proximal landing zone 3. Distal landing zone 4. Access vessels 5. Spinal cord ischemia 6. Endoleak
 Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic, Gore Employment in industry Stockholder of a healthcare company Owner of a healthcare company Other(s)
Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic, Gore Employment in industry Stockholder of a healthcare company Owner of a healthcare company Other(s)
Remodeling of the Remnant Aorta after Acute Type A Aortic Dissection Surgery
 Remodeling of the Remnant Aorta after Acute Type A Aortic Dissection Surgery Are Young Patients More Likely to Develop Adverse Aortic Remodeling of the Remnant Aorta Over Time? Suk Jung Choo¹, Jihoon Kim¹,
Remodeling of the Remnant Aorta after Acute Type A Aortic Dissection Surgery Are Young Patients More Likely to Develop Adverse Aortic Remodeling of the Remnant Aorta Over Time? Suk Jung Choo¹, Jihoon Kim¹,
Endovascular Stent Grafts for Disorders of the Thoracic Aorta
 7.01.86 Endovascular Stent Grafts for Disorders of the Thoracic Aorta Section 7.0 Surgery Subsection Effective Date September 30, 2014 Original Policy Date September 27, 2013 Next Review Date September
7.01.86 Endovascular Stent Grafts for Disorders of the Thoracic Aorta Section 7.0 Surgery Subsection Effective Date September 30, 2014 Original Policy Date September 27, 2013 Next Review Date September
Current Trends in. Torin P. Fitton, MD Division of Cardiothoracic Surgery Lahey Clinic NO DISCLOSURES. Aortic Syndromes
 Current Trends in Aortic Syndromes Torin P. Fitton, MD Division of Cardiothoracic Surgery Lahey Clinic NO DISCLOSURES Aortic Syndromes Aortic Aneurysm Aortic Dissection Intramural Hematoma (IMH) Penetrating
Current Trends in Aortic Syndromes Torin P. Fitton, MD Division of Cardiothoracic Surgery Lahey Clinic NO DISCLOSURES Aortic Syndromes Aortic Aneurysm Aortic Dissection Intramural Hematoma (IMH) Penetrating
Chungbuk Regional Cardiovascular Center, Division of Cardiology, Departments of Internal Medicine, Chungbuk National University Hospital Sangmin Kim
 Endovascular Procedures for Isolated Common Iliac and Internal Iliac Aneurysm Chungbuk Regional Cardiovascular Center, Division of Cardiology, Departments of Internal Medicine, Chungbuk National University
Endovascular Procedures for Isolated Common Iliac and Internal Iliac Aneurysm Chungbuk Regional Cardiovascular Center, Division of Cardiology, Departments of Internal Medicine, Chungbuk National University
Total Endovascular Repair Type A Dissection. Eric Herget Interventional Radiology
 Total Endovascular Repair Type A Dissection Eric Herget Interventional Radiology 65 year old male Acute Type A Dissection Severe Aortic Regurgitation No co-morbidities Management? Part II Evolving Global
Total Endovascular Repair Type A Dissection Eric Herget Interventional Radiology 65 year old male Acute Type A Dissection Severe Aortic Regurgitation No co-morbidities Management? Part II Evolving Global
Hybrid Repair of a Complex Thoracoabdominal Aortic Aneurysm
 Hybrid Repair of a Complex Thoracoabdominal Aortic Aneurysm Virendra I. Patel MD MPH Assistant Professor of Surgery Massachusetts General Hospital Division of Vascular and Endovascular Surgery Disclosure
Hybrid Repair of a Complex Thoracoabdominal Aortic Aneurysm Virendra I. Patel MD MPH Assistant Professor of Surgery Massachusetts General Hospital Division of Vascular and Endovascular Surgery Disclosure
Surgical Considerations of TEVAR
 Surgical Considerations of TEVAR University of Alberta, June 14 th, 2013 Jehangir Appoo Libin Cardiovascular Institute University of Calgary, Today: Lesions/Pathology amenable to TEVAR On label Off label
Surgical Considerations of TEVAR University of Alberta, June 14 th, 2013 Jehangir Appoo Libin Cardiovascular Institute University of Calgary, Today: Lesions/Pathology amenable to TEVAR On label Off label
DISCLOSURES ISOLATED DTA LESION? TYPE B DISSECTIONS TREATMENT OPTIONS
 Endovascular Repair of Aortic Arch Pathologies; What is available/possible in the U.S. in 2018? Kaiser Permanente Endovascular Symposium 6/2/18 Sukgu M Han, MD, MS Assistant Professor of Clinical Surgery
Endovascular Repair of Aortic Arch Pathologies; What is available/possible in the U.S. in 2018? Kaiser Permanente Endovascular Symposium 6/2/18 Sukgu M Han, MD, MS Assistant Professor of Clinical Surgery
High Risk Uncomplicated Type B Dissection
 High Risk Uncomplicated Type B Dissection Ali Azizzadeh, MD, FACS Director, Vascular Surgery Vice Chair, Department of Surgery Associate Director, Heart Institute Cedars-Sinai Medical Center Los Angeles,
High Risk Uncomplicated Type B Dissection Ali Azizzadeh, MD, FACS Director, Vascular Surgery Vice Chair, Department of Surgery Associate Director, Heart Institute Cedars-Sinai Medical Center Los Angeles,
Jean M Panneton, MD Professor of Surgery Program Director Vascular Surgery Chief EVMS. Arch Pathology: The Endovascular Era is here
 Jean M Panneton, MD Professor of Surgery Program Director Vascular Surgery Chief EVMS Arch Pathology: The Endovascular Era is here Disclosures Consultant: Cook Medical, Bolton Medical, Medtronic Inc, Volcano,
Jean M Panneton, MD Professor of Surgery Program Director Vascular Surgery Chief EVMS Arch Pathology: The Endovascular Era is here Disclosures Consultant: Cook Medical, Bolton Medical, Medtronic Inc, Volcano,
Importance of false lumen thrombosis in type B aortic dissection prognosis
 Importance of false lumen thrombosis in type B aortic dissection prognosis Santi Trimarchi, MD, PhD, a Jip L. Tolenaar, MD, a Frederik H. W. Jonker, MD, PhD, b Brian Murray, MD, c Thomas T. Tsai, MD, d
Importance of false lumen thrombosis in type B aortic dissection prognosis Santi Trimarchi, MD, PhD, a Jip L. Tolenaar, MD, a Frederik H. W. Jonker, MD, PhD, b Brian Murray, MD, c Thomas T. Tsai, MD, d