Approach to the patient with Shortness of Breath
|
|
|
- Ellen Angelina Gibson
- 6 years ago
- Views:
Transcription
1 Approach to the patient with Shortness of Breath Colin Edwards AUG 2015
2 Dyspnoea Basic concepts Definition: Dyspnoea is defined as abnormal or uncomfortable breathing in the context of what is normal for a person according to his or her level of fitness and exertional threshold for breathlessness Common and important symptom- which may be due to:- - Pulmonary disease - Cardiac disease OR - Combination of both OR - Non-cardiac and non-pulmonary deconditioning, anemia, psychosomatic Cardiac Dyspnoea May be due to 1 or more of the following:- Coronary disease, myocardial disease, valve disease, rhythm disorders, pericardial disease Important symptom denotes severity of disease.
3 Case 1 HISTORY: Ms V - 35 year old female patient solo mother - 5 year old daughter. A+E 3-month history of breathlessness, wheeze and cough. PM/SH: nil- normal pregnancy and delivery 5 years ago Meds: nil SOCIAL: Not working. Previous heavy alcohol intake, along with other substance use (marijuana), however has stopped 5 years ago. EXAM: Afebrile PR 100 bpm BP: 100/60mmHg, no pallor, normal BMI CVS- tachycardic, no obvious mumurs Chest: bilateral rhonchi with an expiratory wheeze Peripheries: no oedema
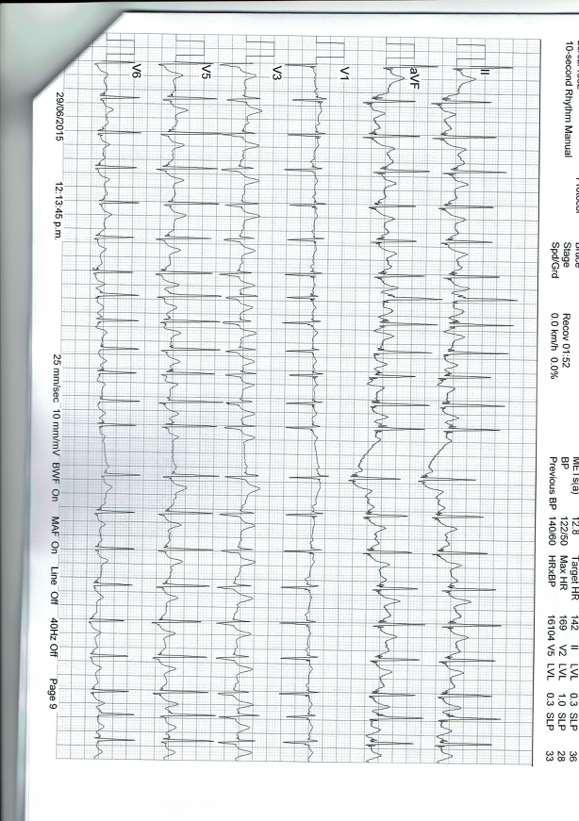
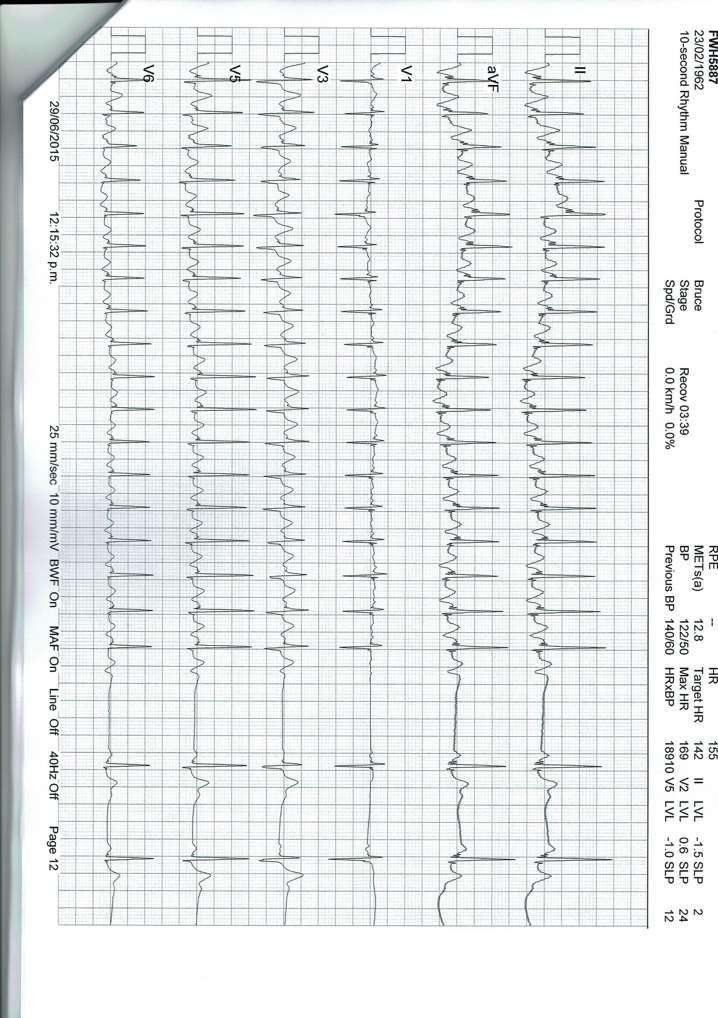
4 ASSESSMENT:? Adult onset asthma and LRTI. MANAGEMENT: Peak flow was mildly reduced. Given a nebulizer and observed for 30 min had improved. Rx Ventolin, Flixotide and Augmentin After the nebulizer complained of severe palpitations ECG was done
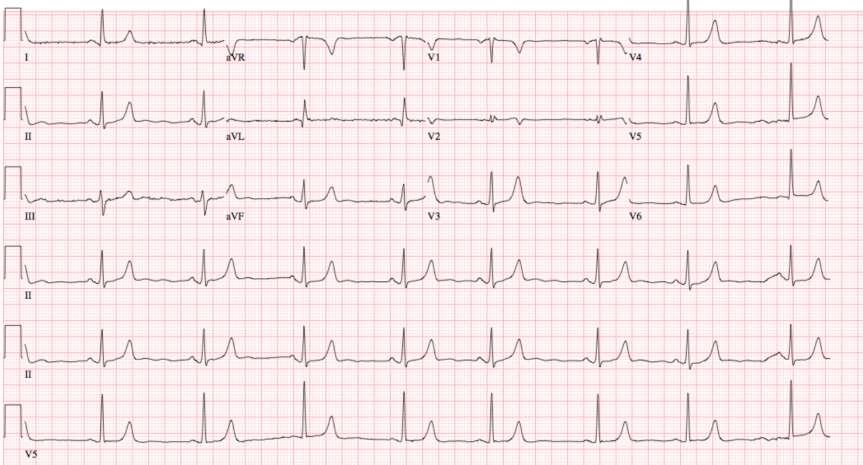
5 ECG done on the way out.
6 QUESTION ECG is compatible with acute asthma OR Need to re-assess the diagnosis. RE-ASSESS THE DIAGNOSIS

7 ECG done on the way out.
8 History Re-visited 3 months ago- bad episode of flu never recovered fully 3 lots of antibiotics Orthopnea - Often wakes at night coughing and sensation of suffocation Breathless on minimal exertion dressing or showering (NYHA FC III) Family history of cardiomyopathy

9 Examination Tachycardia, hypotension 100/60mmHg Raised JVP S3 gallop rhythm KENTUCKY Crackles, wheezes, Peripheral oedema - trace
10
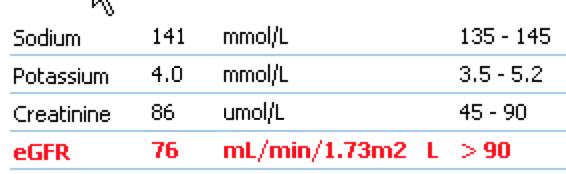
11 Bloods
12 Distinguishing Cardiac from Respiratory Dyspnoea History Examination ECG Bloods

13 History -Characterizing Dyspnoea DESCRIPTOR PATHOPHYSIOLOGY CONDITION Chest tightness effort of breathing, unsatisfying breaths, can t get a deep breath Bronchoconstriction Interstitial oedema Airway obstruction Chest wall compliance Asthma Myocardial ischaemia COPD, asthma Pulmonary fibrosis Air hunger, urge to breathe Drive to breathe CHF, severe COPD, asthma Suffocating, smothering, air hunger Heavy breathing, breathing more Alveolar oedema Inadequate oxygen delivery Pulmonary oedema Deconditioning
14 Clinical Diagnosis of Heart Failure SYMPTOMS Dyspnea on exertion Orthopnoea- most specific symptom of raised filling pressures Paroxysmal nocturnal dyspnoea Fatigue SIGNS Elevated JVP and positive hepatojugular reflux- most reliable sign of raised filling pressures* Third Heart Sound- prognostic for future CHF events* Displaced apex beat Pulmonary crackles-insensitive for heart failure Peripheral oedema Pulsus alternans
15 12 lead ECG and Dyspnoea Rate and Rhythm Ischaemia, infarction LV hypertrophy and atrial enlargement Right heart pathology



16 ECG: Cardiac dyspnoea versus Respiratory dyspnoea. DYSPNOEA LEFT HEART DISEASE -p-mitrale -LBBB -LVH -L Axis deviation RIGHT HEART DISEASE -p pulmonale -RBBB -R Axis deviation -RV strain pattern
17 Brain Natriuretic Peptide Natriuretic hormone released from the ventricles volume expansion and increased wall stress. BNP inhibits the RAAS. NT-proBNP has a longer plasma half-life and rises more in CHF than does BNP.
18 Elevated plasma BNP levels Not specific for CHF-lends weight to the diagnosis of HF LV filling pressures, reduced LVEF, LV hypertrophy, Acute MI and ischemia Pulmonary embolism, COPD and cor pulmonale Natriuretic peptides are sensitive to biological factors age, sex, weight, and renal function elevated in women and in people over 60 years of age who do not have HF. Lower in obese patients
19 NT-proBNP NT-proBNP levels below 35pmol/l - CHF unlikely negative predictive value of 98 percent. GOOD RULE OUT TEST AGE NT-proBNP(pmol/l) <50 yrs yrs 100 >75 yrs 210 Sens 90%, spec 84%
20 Case 2 68 year old patient CABG 12 years ago (3 grafts- LIMA to LAD, radial to OM, SVG to distal RCA) Normal LV function. Ex smoker (40 pack years) COPD FEV1 1.4L 55% of predicted Hypertension, Impaired glucose tolerance (HbA1C-46), treated hyperlipidemia Worsening dyspnoea on exertion 2 chest infections requiring antibiotic Rx 2 recent courses of Prednisone Hasn t got back to his baseline fitness No chest pain
21 Medication: Ventolin Flixotide Seretide Aspirin 100mg/d Liptor -40mg/d Inhibace 5mg/d EXAM: PR 80bpm BP 150/90mmHg JVP-1 CVS- distant heart sounds, no mumurs, no gallop Chest_ hyperinflated, no crackles or wheezes Abd: central obesity Peripheries- no oedema, mild PVD
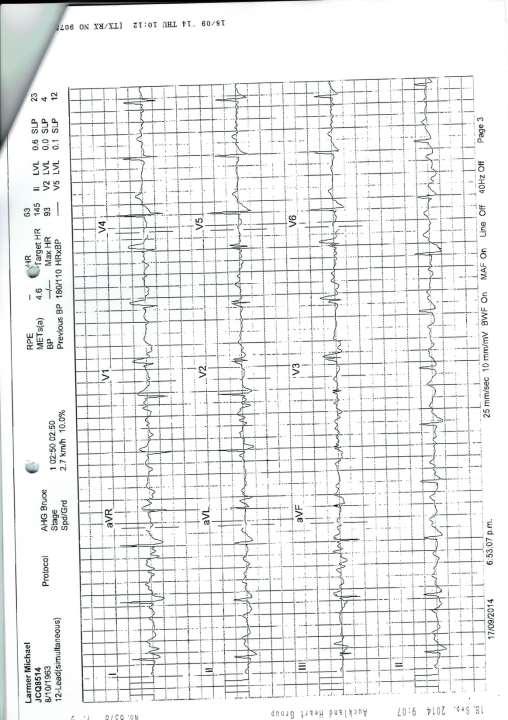
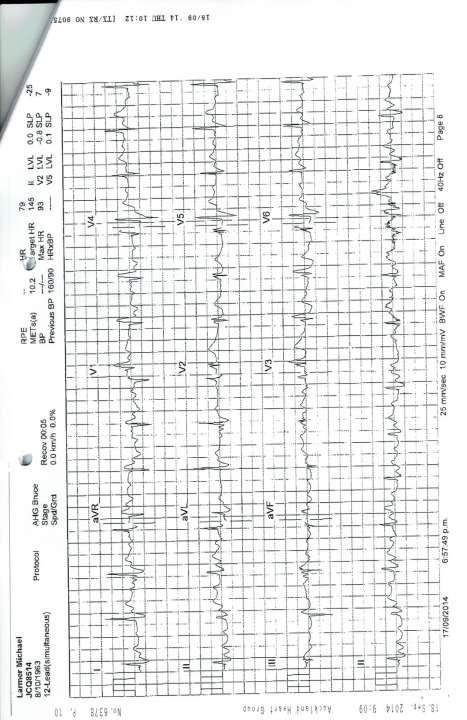
22 ECG

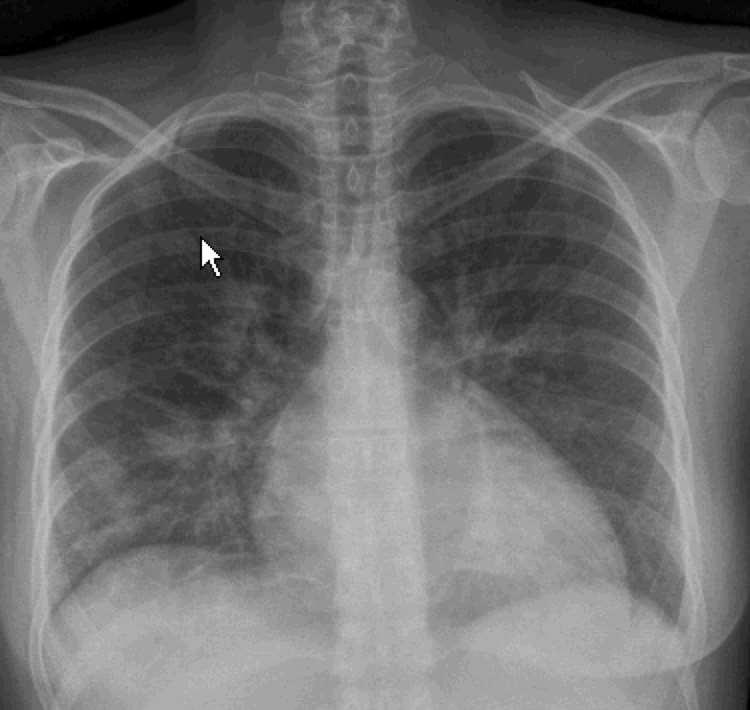
23 Investigations CXR- normal CTR,? Hyperinflation, no failure, no infection Bloods- unremarkable no anaemia, normal S creat, trop I neg, NT-proBNP 83pmol/l ETT equivocal, inadequate HR, quite SOB Coronary angiography: Severe native vessel disease Grafts were patent No targets for revsacularisation LV EF 50%, LVEDP 18mmHg
24 Dyspnoea and Coronary Disease DYSPNOEIC patients with known CAD or SUSPECTED CAD -generally high risk recommend specialist assessment Dyspnea and fatigue often herald important CAD in elderly patients. Breathlessness alone can be the presenting symptom even for acute coronary syndrome and was found to be present in 25% of patients in the EuroHeart data set. In a large series of patients referred for evaluation of dyspnea, 42% with this symptom alone had ischemia on exercise echocardiography



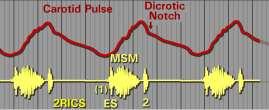
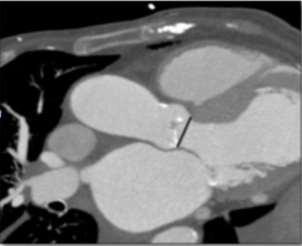
25 CASE 83 year old usually well. Complains of exertional breathlessness. Severe Calcific Aortic Stenosis
26 Case Mrs DR- 53 years of age. Intermittent episodes of breathlessness on exertion x 3months (with vacuuming) No chest discomfort or palpitations Some days are normal. PM/SH: Late onset asthma in her 20 s No hypertension CV risk factors- low CV risk Examination: Mildly raised body mass index. Her pulse rate was 74 bpm. Blood pressure was well controlled at 100/60mmHg. Heart sounds were normal with no murmurs.
27
28 Case 50 year old, English journalist with his own a advertising business. Regular gymn attendant- 4 month hx of unexplained breathlessness and lethargy. No chest discomfort Known bicuspid aortic valve normal valve fx Known hypertensive on Rx - Hyzaar Non-smoker, no diabetes, no family hx of CAD.
29 Case cont. EXAM: BP 180/110mmHg PR 63bpm JVP- no raised raised BMI - 28 CVS- ejection click, no mumurs Chest normal Abdomen normal CNS-normal Peripheries- normal

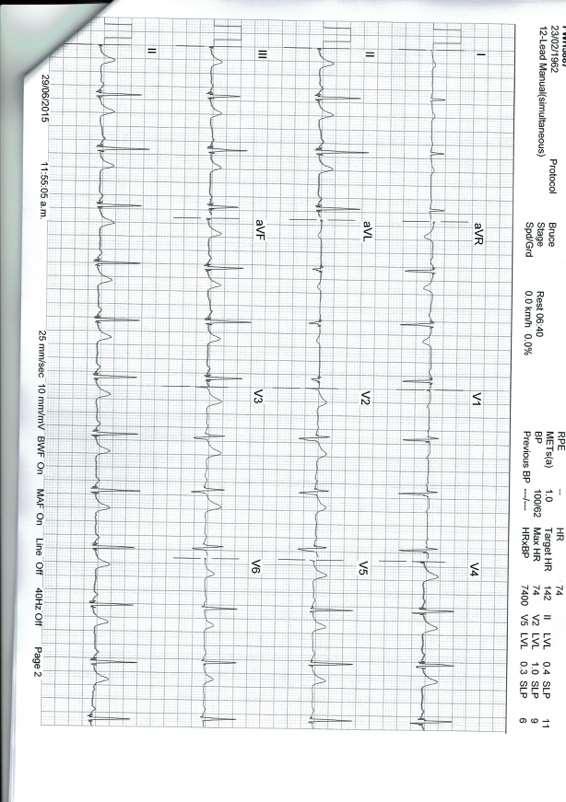
30 ECG and ETT
31 Relationship between age and maximal heart rate in >5000 asymptomatic women, with 95% confidence limits. Peter H. Brubaker, and Dalane W. Kitzman Circulation. 2011;123: Copyright American Heart Association, Inc. All rights reserved.
32

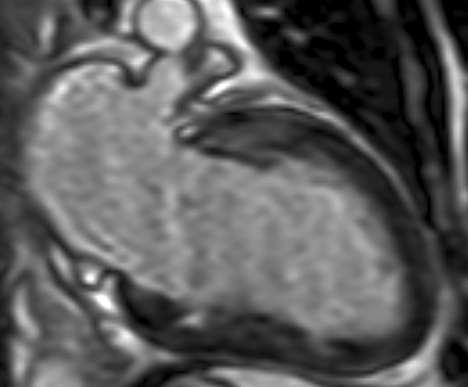
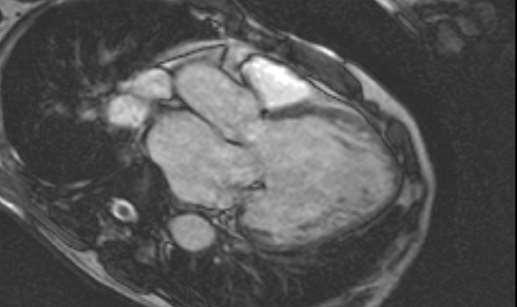
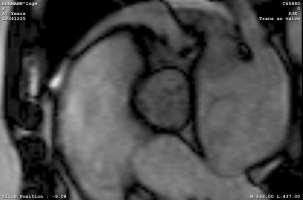
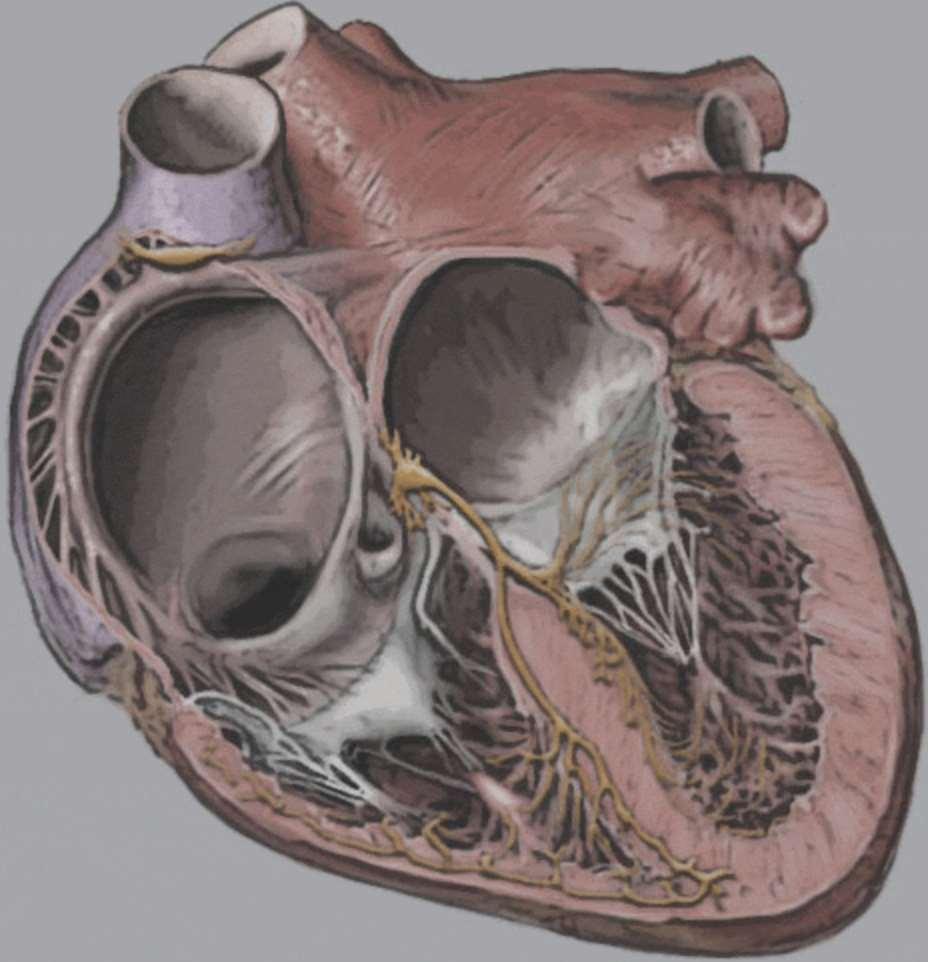
33 Contrast CMR


34 Coronary angio
, atrioventricular block, coronary artery")
35 Discussion During maximal aerobic exercise in healthy humans, cardiac output increases approximately 4-fold. CO = HR X SV 2.2-fold increase in heart rate (HR) 0.3-fold increase in stroke volume Chronotropic incompetence relatively common in patients with sick sinus syndrome (elderly), atrioventricular block, coronary artery disease, and HF.
36 Need a good history and examination Orthopnoea, smothering, suffocating JVP, S3 gallop ( KENTUCKY ) Conclusion 12 lead ECG: rhythm, ischaemia, ventricular hypertrophy L sided p mitrale, LVH LBBB, L axis cardiac cause for SOB R sided- p pulmonale, RBBB,, R axis pulmonary cause for SOB CXR: Cardiomegaly, upper lobe venous blood diversion, interstitial oedema NT-proBNP Low level <35pmol/l GOOD RULE OUT TEST for heart failure Suspected IHD - Unexplained breathlessness in patients with known or suspected IHD high risk and require specialist assessment Exertional arrhythmias- often present with intermittent episodes of breathlessness (PAF most commonly)
37 THANK YOU Colin Edwards
NT-proBNP: Evidence-based application in primary care
 NT-proBNP: Evidence-based application in primary care Associate Professor Rob Doughty The University of Auckland, Auckland City Hospital, Auckland Heart Group NT-proBNP: Evidence in Primary Care The problem
NT-proBNP: Evidence-based application in primary care Associate Professor Rob Doughty The University of Auckland, Auckland City Hospital, Auckland Heart Group NT-proBNP: Evidence in Primary Care The problem
Heart Failure. Cardiac Anatomy. Functions of the Heart. Cardiac Cycle/Hemodynamics. Determinants of Cardiac Output. Cardiac Output
 Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept
 Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept (MBBS)(SBMD) Introduction Epidemiology Pathophysiology diastolic/systolic Risk factors Signs and symptoms Classification of HF
Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept (MBBS)(SBMD) Introduction Epidemiology Pathophysiology diastolic/systolic Risk factors Signs and symptoms Classification of HF
HEART FAILURE. Study day November 2018 Sarah Briggs
 HEART FAILURE Study day November 2018 Sarah Briggs Overview and Introduction This course is an introduction and overview of heart failure. Normal heart function and basic pathophysiology of heart failure
HEART FAILURE Study day November 2018 Sarah Briggs Overview and Introduction This course is an introduction and overview of heart failure. Normal heart function and basic pathophysiology of heart failure
Dr Dinna Soon. Consultant Cardiologist, Department of Cardiology. GP symposium 2 April 2016
 Dr Dinna Soon Consultant Cardiologist, Department of Cardiology GP symposium 2 April 2016 Case presentation 76 years old male, chronic smoker, hypertension, previous MI 3/7 SOB and chest tightness BP
Dr Dinna Soon Consultant Cardiologist, Department of Cardiology GP symposium 2 April 2016 Case presentation 76 years old male, chronic smoker, hypertension, previous MI 3/7 SOB and chest tightness BP
Congestive Heart Failure or Heart Failure
 Congestive Heart Failure or Heart Failure Dr Hitesh Patel Ascot Cardiology Group Heart Failure Workshop April, 2014 Question One What is the difference between congestive heart failure and heart failure?
Congestive Heart Failure or Heart Failure Dr Hitesh Patel Ascot Cardiology Group Heart Failure Workshop April, 2014 Question One What is the difference between congestive heart failure and heart failure?
Congestive Heart Failure Patient Profile. Patient Identity - Mr. Douglas - 72 year old man - No drugs, smokes, moderate social alcohol consumption
 Congestive Heart Failure Patient Profile Patient Identity - Mr. Douglas - 72 year old man - No drugs, smokes, moderate social alcohol consumption Chief Complaint - SOB - When asked: Increasing difficulty
Congestive Heart Failure Patient Profile Patient Identity - Mr. Douglas - 72 year old man - No drugs, smokes, moderate social alcohol consumption Chief Complaint - SOB - When asked: Increasing difficulty
Presentation, symptoms and signs of heart failure
 3 Presentation, symptoms and signs of heart failure What will I learn? In this section you will learn: Who is at risk of heart failure The symptoms of heart failure The signs of heart failure The importance
3 Presentation, symptoms and signs of heart failure What will I learn? In this section you will learn: Who is at risk of heart failure The symptoms of heart failure The signs of heart failure The importance
Copyright 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. Normal Cardiac Anatomy
 Mosby,, an affiliate of Elsevier Normal Cardiac Anatomy Impaired cardiac pumping Results in vasoconstriction & fluid retention Characterized by ventricular dysfunction, reduced exercise tolerance, diminished
Mosby,, an affiliate of Elsevier Normal Cardiac Anatomy Impaired cardiac pumping Results in vasoconstriction & fluid retention Characterized by ventricular dysfunction, reduced exercise tolerance, diminished
HEART FAILURE. Study day November 2017 Sarah Briggs and Janet Laing
 HEART FAILURE Study day November 2017 Sarah Briggs and Janet Laing Overview and Introduction This course is an introduction and overview of heart failure. Normal heart function and basic pathophysiology
HEART FAILURE Study day November 2017 Sarah Briggs and Janet Laing Overview and Introduction This course is an introduction and overview of heart failure. Normal heart function and basic pathophysiology
Value of echocardiography in chronic dyspnea
 Value of echocardiography in chronic dyspnea Jahrestagung Schweizerische Gesellschaft für /Schweizerische Gesellschaft für Pneumologie B. Kaufmann 16.06.2016 Chronic dyspnea Shortness of breath lasting
Value of echocardiography in chronic dyspnea Jahrestagung Schweizerische Gesellschaft für /Schweizerische Gesellschaft für Pneumologie B. Kaufmann 16.06.2016 Chronic dyspnea Shortness of breath lasting
ECG Workshop. Nezar Amir
 ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
8:30-10:30 WS #4: Cardiology :00-13:00 WS #11: Cardiology 101 (Repeated)
") Professor Ralph Stewart Cardiologist Auckland City Hospital Green Lane Cardiovascular Research Unit Auckland Heart Group Fiona Stewart Cardiologist Green Lane Hospital National Women's Hospital Professor
Professor Ralph Stewart Cardiologist Auckland City Hospital Green Lane Cardiovascular Research Unit Auckland Heart Group Fiona Stewart Cardiologist Green Lane Hospital National Women's Hospital Professor
Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό
 Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό Diastolic HF DD: Diastolic Dysfunction DHF: Diastolic HF HFpEF: HF with preserved EF DD Pathophysiologic condition: impaired relaxation, LV compliance, LV filling
Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό Diastolic HF DD: Diastolic Dysfunction DHF: Diastolic HF HFpEF: HF with preserved EF DD Pathophysiologic condition: impaired relaxation, LV compliance, LV filling
Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF
 CLASSIFICATION OF HEART FAILURE Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF DISCLOSURES: NONE CLASSIFICATION C OF HEART FAILURE NYHA I IV New paradigm Stage A: Pts at high risk of developing
CLASSIFICATION OF HEART FAILURE Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF DISCLOSURES: NONE CLASSIFICATION C OF HEART FAILURE NYHA I IV New paradigm Stage A: Pts at high risk of developing
Chest pain management. Ruvin Gabriel and Niels van Pelt August 2011
 Chest pain management Ruvin Gabriel and Niels van Pelt August 2011 Introduction Initial assessment Case 1 Case 2 and 3 Comparison of various diagnostic techniques Summary 1-2 % of GP consultations are
Chest pain management Ruvin Gabriel and Niels van Pelt August 2011 Introduction Initial assessment Case 1 Case 2 and 3 Comparison of various diagnostic techniques Summary 1-2 % of GP consultations are
Peripartum Cardiomyopathy. Lavanya Rai Manipal
 Peripartum Cardiomyopathy Lavanya Rai Manipal Definition - PPCM - Dilated cardiomyopathy of unknown cause resulting in cardiac failure that occurs in the peripartum period in women without any preexisting
Peripartum Cardiomyopathy Lavanya Rai Manipal Definition - PPCM - Dilated cardiomyopathy of unknown cause resulting in cardiac failure that occurs in the peripartum period in women without any preexisting
Heart Valve disease: MR. AS tough patient When to echo, When to refer, What s new
 Heart Valve disease: MR. AS tough patient When to echo, When to refer, What s new B. Sonnenberg UAH Cardiology CME Day 5 May 2015 Disclosures Speaker s or Advisory Boards: none Research grants: none (co-investigator
Heart Valve disease: MR. AS tough patient When to echo, When to refer, What s new B. Sonnenberg UAH Cardiology CME Day 5 May 2015 Disclosures Speaker s or Advisory Boards: none Research grants: none (co-investigator
The adult with recurrent breathlessness. A/Prof Gerald Chua Medicine NTFGH
 The adult with recurrent breathlessness A/Prof Gerald Chua Medicine NTFGH Dyspnoea Subjective experience of breathing discomfort Variable among individuals with apparently similar degrees of impairment
The adult with recurrent breathlessness A/Prof Gerald Chua Medicine NTFGH Dyspnoea Subjective experience of breathing discomfort Variable among individuals with apparently similar degrees of impairment
Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year
![Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year](/thumbs/76/74263761.jpg "Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year") PAST MEDICAL HISTORY Has the subject had a prior episode of heart failure? o Does the subject have a prior history of exposure to cardiotoxins, such as anthracyclines? URGENT HEART FAILURE VISIT Did heart
PAST MEDICAL HISTORY Has the subject had a prior episode of heart failure? o Does the subject have a prior history of exposure to cardiotoxins, such as anthracyclines? URGENT HEART FAILURE VISIT Did heart
THE PROPER APPROACH TO DIAGNOSING HEART FAILURE WITH PRESERVED EJECTION FRACTION
 THE PROPER APPROACH TO DIAGNOSING HEART FAILURE WITH PRESERVED EJECTION FRACTION James C. Fang, MD, FACC Professor and Chief Cardiovascular Division University of Utah School of Medicine Disclosures Data
THE PROPER APPROACH TO DIAGNOSING HEART FAILURE WITH PRESERVED EJECTION FRACTION James C. Fang, MD, FACC Professor and Chief Cardiovascular Division University of Utah School of Medicine Disclosures Data
March yr. old male, newspaper writer, with worsening dyspnea /orthopnea past few months
 Case 1 March 2016 59 yr. old male, newspaper writer, with worsening dyspnea /orthopnea past few months PMH diabetes, celiac disease Reports chest discomfort, positional coughing and pedal edema last 10
Case 1 March 2016 59 yr. old male, newspaper writer, with worsening dyspnea /orthopnea past few months PMH diabetes, celiac disease Reports chest discomfort, positional coughing and pedal edema last 10
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM. General Instructions: ID NUMBER: FORM NAME: H F A DATE: 10/13/2017 VERSION: CONTACT YEAR NUMBER:
 ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM General Instructions: The Heart Failure Hospital Record Abstraction Form is completed for all heart failure-eligible cohort hospitalizations. Refer to
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM General Instructions: The Heart Failure Hospital Record Abstraction Form is completed for all heart failure-eligible cohort hospitalizations. Refer to
COPD as a comorbidity of heart failure in elderly patients
 COPD as a comorbidity of heart failure in elderly patients Professor Mitja Lainscak, MD, PhD, FESC, FHFA Departments of Cardiology and Research&Education, General Hospital Celje Faculty of Medicine, University
COPD as a comorbidity of heart failure in elderly patients Professor Mitja Lainscak, MD, PhD, FESC, FHFA Departments of Cardiology and Research&Education, General Hospital Celje Faculty of Medicine, University
Managing the Low Output Low Gradient Aortic Stenosis Patient
 Managing the Low Output Low Gradient Aortic Stenosis Patient R A Nishimura MD Judd and Mary Leighton Professor of CV Mayo Clinic No disclosures Valvular Stenosis Severity of Aortic Stenosis Mean gradient
Managing the Low Output Low Gradient Aortic Stenosis Patient R A Nishimura MD Judd and Mary Leighton Professor of CV Mayo Clinic No disclosures Valvular Stenosis Severity of Aortic Stenosis Mean gradient
 Stress Echocardiography: Illustrative Cases Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director,
Stress Echocardiography: Illustrative Cases Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director,
Cardiac Symptom Template Guide 2015 V1
 Cardiac Symptom Template Guide 2015 V1 1 Template Control Page Cardiac Symptom Template Title Cardiac Symptom CEG TEST Author CEG Version 1 Descriptor Helps support the cardiac project funded by UCLP/NCCG
Cardiac Symptom Template Guide 2015 V1 1 Template Control Page Cardiac Symptom Template Title Cardiac Symptom CEG TEST Author CEG Version 1 Descriptor Helps support the cardiac project funded by UCLP/NCCG
Pulmonary-Vascular Disease. Howard J. Sachs, MD.
 Pulmonary-Vascular Disease Howard J. Sachs, MD www.12daysinmarch.com Dyspnea Cardiac Pulmonary CAD Pump Failure Chest Wall Airways Valve Disease Pericardial Disease Alveoli Interstitium Rhythm Disturbance
Pulmonary-Vascular Disease Howard J. Sachs, MD www.12daysinmarch.com Dyspnea Cardiac Pulmonary CAD Pump Failure Chest Wall Airways Valve Disease Pericardial Disease Alveoli Interstitium Rhythm Disturbance
The NEW Heart Failure Guidelines
 The NEW Heart Failure Guidelines Daily Practice HF scenario of the Case Presentations HF as a complex and heterogeneous syndrome Several proposed pathophysiological mechanisms involving the heart and the
The NEW Heart Failure Guidelines Daily Practice HF scenario of the Case Presentations HF as a complex and heterogeneous syndrome Several proposed pathophysiological mechanisms involving the heart and the
CHRONIC CAD DIAGNOSIS
 CHRONIC CAD DIAGNOSIS Chest Pain Evaluation 1. Approach to diagnosis of CAD 2. Classification of chest pain 3. Pre-test likelihood CAD 4. Algorithm for chest pain evaluation in women 5. Indications for
CHRONIC CAD DIAGNOSIS Chest Pain Evaluation 1. Approach to diagnosis of CAD 2. Classification of chest pain 3. Pre-test likelihood CAD 4. Algorithm for chest pain evaluation in women 5. Indications for
Pulmonary Pearls. Medical Pearls. Case 1: Case 1 (cont.): Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):
: Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):") Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
Heart Failure in Women: Dr Goh Ping Ping Cardiologist Asian Heart & Vascular Centre
 Heart Failure in Women: More than EF? Dr Goh Ping Ping Cardiologist Asian Heart & Vascular Centre Overview Review pathophysiology as it relates to diagnosis and management Rational approach to workup:
Heart Failure in Women: More than EF? Dr Goh Ping Ping Cardiologist Asian Heart & Vascular Centre Overview Review pathophysiology as it relates to diagnosis and management Rational approach to workup:
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
TSDA Boot Camp September 13-16, Introduction to Aortic Valve Surgery. George L. Hicks, Jr., MD
 TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
Cor pulmonale. Dr hamid reza javadi
 1 Cor pulmonale Dr hamid reza javadi 2 Definition Cor pulmonale ;pulmonary heart disease; is defined as dilation and hypertrophy of the right ventricle (RV) in response to diseases of the pulmonary vasculature
1 Cor pulmonale Dr hamid reza javadi 2 Definition Cor pulmonale ;pulmonary heart disease; is defined as dilation and hypertrophy of the right ventricle (RV) in response to diseases of the pulmonary vasculature
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM
 ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM ID NUMBER: FORM NAME: H F A DATE: 10/01/2015 VERSION: D CONTACT YEAR NUMBER: FORM SEQUENCE NUMBER: General Instructions: The Heart Failure Hospital Record
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM ID NUMBER: FORM NAME: H F A DATE: 10/01/2015 VERSION: D CONTACT YEAR NUMBER: FORM SEQUENCE NUMBER: General Instructions: The Heart Failure Hospital Record
Heart failure 1: pathogenesis, presentation and diagnosis
 Heart failure Keywords Cardiac dysfunction/ Ejection fraction/nyha classification This article has been double-blind peer reviewed In this article... Pathophysiology and aetiology of heart failure Different
Heart failure Keywords Cardiac dysfunction/ Ejection fraction/nyha classification This article has been double-blind peer reviewed In this article... Pathophysiology and aetiology of heart failure Different
12 Lead ECG Workshop. Virginia Hass, DNP, FNP-C, PA-C Kim Newlin, CNS, ANP-C, FPCNA. California Association of Nurse Practitioners March 18, 2016
 12 Lead ECG Workshop Virginia Hass, DNP, FNP-C, PA-C Kim Newlin, CNS, ANP-C, FPCNA California Association of Nurse Practitioners March 18, 2016 Learning Objectives Identify key changes on the ECG which
12 Lead ECG Workshop Virginia Hass, DNP, FNP-C, PA-C Kim Newlin, CNS, ANP-C, FPCNA California Association of Nurse Practitioners March 18, 2016 Learning Objectives Identify key changes on the ECG which
The new Guidelines: Focus on Chronic Heart Failure
 The new Guidelines: Focus on Chronic Heart Failure Petros Nihoyannopoulos MD, FRCP, FESC Professor of Cardiology Imperial College London and National & Kapodistrian University of Athens 2 3 4 The principal
The new Guidelines: Focus on Chronic Heart Failure Petros Nihoyannopoulos MD, FRCP, FESC Professor of Cardiology Imperial College London and National & Kapodistrian University of Athens 2 3 4 The principal
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Pericardial Disease: Case Examples. Echo Fiesta 2017
 Pericardial Disease: Case Examples Echo Fiesta 2017 2014 2014 MFMER MFMER 3346252-1 slide-1 Objectives Have a systematic approach to evaluation of constriction 2014 MFMER 3346252-2 CASE 1 2013 MFMER 3248567-3
Pericardial Disease: Case Examples Echo Fiesta 2017 2014 2014 MFMER MFMER 3346252-1 slide-1 Objectives Have a systematic approach to evaluation of constriction 2014 MFMER 3346252-2 CASE 1 2013 MFMER 3248567-3
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies
 Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
SAUDI FELLOWSHIP TRAINING PROGRAM. Adult Cardiology. Final Written Examination 2019
 SAUDI FELLOWSHIP TRAINING PROGRAM Adult Cardiology Final Written Examination 2019 Objectives 1. Determine the trainee has sufficient competency related to the required specialty. 2. Determine the eligibility
SAUDI FELLOWSHIP TRAINING PROGRAM Adult Cardiology Final Written Examination 2019 Objectives 1. Determine the trainee has sufficient competency related to the required specialty. 2. Determine the eligibility
Colin Edwards. Cardiologist Auckland Heart Group Waitemata Health
 Colin Edwards Cardiologist Auckland Heart Group Waitemata Health August 2011 BP MEASUREMENTS measured seated mean of 2 or BP recordings at least 2 visits 2 x risk of developing true hypertension Size of
Colin Edwards Cardiologist Auckland Heart Group Waitemata Health August 2011 BP MEASUREMENTS measured seated mean of 2 or BP recordings at least 2 visits 2 x risk of developing true hypertension Size of
2016 ESC Heart Failure Guidelines: what is new? Piotr Ponikowski Wroclaw, Poland
 2016 ESC Heart Failure Guidelines: what is new? Piotr Ponikowski Wroclaw, Poland Disclosures Consultancy fees and speaker s honoraria from: Amgen, Servier, Novartis, Johnson & Johnson, Merck, Berlin Chemie,
2016 ESC Heart Failure Guidelines: what is new? Piotr Ponikowski Wroclaw, Poland Disclosures Consultancy fees and speaker s honoraria from: Amgen, Servier, Novartis, Johnson & Johnson, Merck, Berlin Chemie,
My Patient Needs a Stress Test
 My Patient Needs a Stress Test Amy S. Burhanna,, MD, FACC Coastal Cardiology Cape May Court House, New Jersey Absolute and relative contraindications to exercise testing Absolute Acute myocardial infarction
My Patient Needs a Stress Test Amy S. Burhanna,, MD, FACC Coastal Cardiology Cape May Court House, New Jersey Absolute and relative contraindications to exercise testing Absolute Acute myocardial infarction
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
CARDIOVASCULAR DISEASE ASSESSMENT IN PREGNANT AND POSTPARTUM WOMEN
 ! ASSESSMENT IN PREGNANT AND POSTPARTUM WOMEN Afshan'Hameed,'MD' 'University'of'California,'Irvine'Medical'Center' Elyse'Foster,'MD' 'University'of'California,'San'Francisco' Elliott'Main,'MD' 'California'Maternal'Quality'Care'Collaborative'
! ASSESSMENT IN PREGNANT AND POSTPARTUM WOMEN Afshan'Hameed,'MD' 'University'of'California,'Irvine'Medical'Center' Elyse'Foster,'MD' 'University'of'California,'San'Francisco' Elliott'Main,'MD' 'California'Maternal'Quality'Care'Collaborative'
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
C1: Medical Standards for Safety Critical Workers with Cardiovascular Disorders
 C1: Medical Standards for Safety Critical Workers with Cardiovascular Disorders GENERAL ISSUES REGARDING MEDICAL FITNESS-FOR-DUTY 1. These medical standards apply to Union Pacific Railroad (UPRR) employees
C1: Medical Standards for Safety Critical Workers with Cardiovascular Disorders GENERAL ISSUES REGARDING MEDICAL FITNESS-FOR-DUTY 1. These medical standards apply to Union Pacific Railroad (UPRR) employees
SUPPLEMENTAL MATERIAL
 SUPPLEMENTAL MATERIAL Table S1: Number and percentage of patients by age category Distribution of age Age
SUPPLEMENTAL MATERIAL Table S1: Number and percentage of patients by age category Distribution of age Age
Dr Emma Copsey Consultant Cardiologist Glenfield Hospital 28 th September 2017
 Dr Emma Copsey Consultant Cardiologist Glenfield Hospital 28 th September 2017 Educational Objectives Objectives To review the GIM & Cardiology syllabus for HF To review the new nomenclature/classification
Dr Emma Copsey Consultant Cardiologist Glenfield Hospital 28 th September 2017 Educational Objectives Objectives To review the GIM & Cardiology syllabus for HF To review the new nomenclature/classification
Heart Failure. Dr. William Vosik. January, 2012
 Heart Failure Dr. William Vosik January, 2012 Questions for clinicians to ask Is this heart failure? What is the underlying cause? What are the associated disease processes? Which evidence-based treatment
Heart Failure Dr. William Vosik January, 2012 Questions for clinicians to ask Is this heart failure? What is the underlying cause? What are the associated disease processes? Which evidence-based treatment
Heart disease remains the leading cause of morbidity and mortality in industrialized nations. It accounts for nearly 40% of all deaths in the United
 Heart disease remains the leading cause of morbidity and mortality in industrialized nations. It accounts for nearly 40% of all deaths in the United States, totaling about 750,000 individuals annually
Heart disease remains the leading cause of morbidity and mortality in industrialized nations. It accounts for nearly 40% of all deaths in the United States, totaling about 750,000 individuals annually
UPDATE HEART FAILURE MANAGEMENT
 Save Thais from Heart Diseases 2019 UPDATE HEART FAILURE MANAGEMENT Orawan Anupraiwan, MD. Central Chest Institute of Thailand Definition of HF Heart failure is a clinical syndrome characterized by typical
Save Thais from Heart Diseases 2019 UPDATE HEART FAILURE MANAGEMENT Orawan Anupraiwan, MD. Central Chest Institute of Thailand Definition of HF Heart failure is a clinical syndrome characterized by typical
The right heart: the Cinderella of heart failure
 The right heart: the Cinderella of heart failure Piotr Ponikowski, MD, PhD, FESC Medical University, Centre for Heart Disease Clinical Military Hospital Wroclaw, Poland none Disclosure Look into the Heart
The right heart: the Cinderella of heart failure Piotr Ponikowski, MD, PhD, FESC Medical University, Centre for Heart Disease Clinical Military Hospital Wroclaw, Poland none Disclosure Look into the Heart
The Causes of Heart Failure
 The Causes of Heart Failure Andy Birchall HFSN Right heart failure LVSD - HFREF Valve regurgitation or stenosis Dropsy CCF congestive cardiac failure Cor pulmonale Pulmonary hypertension HFPEF LVF Definitions
The Causes of Heart Failure Andy Birchall HFSN Right heart failure LVSD - HFREF Valve regurgitation or stenosis Dropsy CCF congestive cardiac failure Cor pulmonale Pulmonary hypertension HFPEF LVF Definitions
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Echocardiography as a diagnostic and management tool in medical emergencies
 Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Cardiology. Presented by: Dr Paul Bethell GP Lead for Planned Care
 Cardiology Presented by: Dr Paul Bethell GP Lead for Planned Care 16 th April 2015 Integrated Cardiology Service for Ipswich and East Suffolk CCG IHT 6 consultants - all with specialist areas PCI CoW rapid
Cardiology Presented by: Dr Paul Bethell GP Lead for Planned Care 16 th April 2015 Integrated Cardiology Service for Ipswich and East Suffolk CCG IHT 6 consultants - all with specialist areas PCI CoW rapid
10. Definition of cardiovascular disease 10.1 Nosologic definitions Acute myocardial infarction: myocardial cell death due to prolonged ischaemia 62.
 10. Definition of cardiovascular disease 10.1 Nosologic definitions Acute myocardial infarction: myocardial cell death due to prolonged ischaemia 62. Acute coronary syndrome: it is a big category which
10. Definition of cardiovascular disease 10.1 Nosologic definitions Acute myocardial infarction: myocardial cell death due to prolonged ischaemia 62. Acute coronary syndrome: it is a big category which
Assessment and Diagnosis of Heart Failure
 Assessment and Diagnosis of Heart Failure Heart failure (HF) is a complex clinical syndrome resulting from any structural or functional impairment of ventricular filling or ejection of blood and is characterized
Assessment and Diagnosis of Heart Failure Heart failure (HF) is a complex clinical syndrome resulting from any structural or functional impairment of ventricular filling or ejection of blood and is characterized
Case Presentations TAVR: The Good Bad and The Ugly
 Case Presentations TAVR: The Good Bad and The Ugly Vincent J. Pompili, MD, FACC, FSCAI Professor of Internal Medicine Director of Interventional Cardiovascular Medicine and Cardiac Catheterization Laboratories
Case Presentations TAVR: The Good Bad and The Ugly Vincent J. Pompili, MD, FACC, FSCAI Professor of Internal Medicine Director of Interventional Cardiovascular Medicine and Cardiac Catheterization Laboratories
12 Lead ECG Interpretation
 12 Lead ECG Interpretation Julie Zimmerman, MSN, RN, CNS, CCRN Significant increase in mortality for every 15 minutes of delay! N Engl J Med 2007;357:1631-1638 Who should get a 12-lead ECG? Also include
12 Lead ECG Interpretation Julie Zimmerman, MSN, RN, CNS, CCRN Significant increase in mortality for every 15 minutes of delay! N Engl J Med 2007;357:1631-1638 Who should get a 12-lead ECG? Also include
Building Higher Order Thinking Skills in Tomorrow s Health Care Professionals A Quality Enhancement Plan for the GSBS
 Building Higher Order Thinking Skills in Tomorrow s Health Care Professionals A Quality Enhancement Plan for the GSBS Focus of the QEP at UNTHSC: To improve students Higher Order Thinking (HOT) skills
Building Higher Order Thinking Skills in Tomorrow s Health Care Professionals A Quality Enhancement Plan for the GSBS Focus of the QEP at UNTHSC: To improve students Higher Order Thinking (HOT) skills
Heart Failure from a GP perspective
 Heart Failure from a GP perspective Jane Gilmour, Alison Wright Clinical Nurse Specialists for Heart Failure The Heart failure Team Dr Ganesan Kumar- Consultant Cardiologist Dr D Maras- Staff Grade Cardiology
Heart Failure from a GP perspective Jane Gilmour, Alison Wright Clinical Nurse Specialists for Heart Failure The Heart failure Team Dr Ganesan Kumar- Consultant Cardiologist Dr D Maras- Staff Grade Cardiology
CASE DISCUSSION. Dr JAYASREE VEERABOINA 2nd yr PG MS OBG
 CASE DISCUSSION Dr JAYASREE VEERABOINA 2nd yr PG MS OBG Normal Cardiovascular changes in Pregnancy CARDIAC OUTPUT 5 th wk -- starts 12 wks -- 30-35% 30-32 wks -- 40% During labour -- 50% After delivery
CASE DISCUSSION Dr JAYASREE VEERABOINA 2nd yr PG MS OBG Normal Cardiovascular changes in Pregnancy CARDIAC OUTPUT 5 th wk -- starts 12 wks -- 30-35% 30-32 wks -- 40% During labour -- 50% After delivery
Case based learning: CMR in Heart Failure
 Case based learning: CMR in Heart Failure Milind Y Desai, MD FACC FAHA FESC Associate Professor of Medicine Heart and Vascular Institute, Cleveland Clinic Cleveland, OH Disclosures: none Use of Gadolinium
Case based learning: CMR in Heart Failure Milind Y Desai, MD FACC FAHA FESC Associate Professor of Medicine Heart and Vascular Institute, Cleveland Clinic Cleveland, OH Disclosures: none Use of Gadolinium
The use of Cardiac CT and MRI in Clinical Practice
 The use of Cardiac CT and MRI in Clinical Practice Matthew W. Martinez, MD Assistant Professor of Medicine LVPG - Lehigh Valley Heart Specialists Lehigh Valley Health Network Oct. 3, 2009 DISCLOSURE Relevant
The use of Cardiac CT and MRI in Clinical Practice Matthew W. Martinez, MD Assistant Professor of Medicine LVPG - Lehigh Valley Heart Specialists Lehigh Valley Health Network Oct. 3, 2009 DISCLOSURE Relevant
Valvular Heart Disease Mitral Stenosis
 Valvular Heart Disease Mitral Stenosis A 75 year old woman with loud first heart sound and mid-diastolic murmur Chronic dyspnea Class 2/4 Fatigue Recent orthopnea/pnd Nocturnal palpitation Pedal edema
Valvular Heart Disease Mitral Stenosis A 75 year old woman with loud first heart sound and mid-diastolic murmur Chronic dyspnea Class 2/4 Fatigue Recent orthopnea/pnd Nocturnal palpitation Pedal edema
Chest Pain. Dr. Amitesh Aggarwal. Department of Medicine
 Chest Pain Dr. Amitesh Aggarwal Department of Medicine BACKGROUND Approx 5% of all ED visits 15 % - AMI 25-30 % - Unstable angina 50-55 % - Other conditions Atypical presentations common 2% of patients
Chest Pain Dr. Amitesh Aggarwal Department of Medicine BACKGROUND Approx 5% of all ED visits 15 % - AMI 25-30 % - Unstable angina 50-55 % - Other conditions Atypical presentations common 2% of patients
Susan P. D Anna MSN, APRN BC February 14, 2019
 Is there Equal Opportunity in Heart Failure?? Susan P. D Anna MSN, APRN BC February 14, 2019 Disclosures: I have no financial disclosures. I am not an expert on this topic, but see a lot of women with
Is there Equal Opportunity in Heart Failure?? Susan P. D Anna MSN, APRN BC February 14, 2019 Disclosures: I have no financial disclosures. I am not an expert on this topic, but see a lot of women with
Valvular Heart Disease: Assessment and Timing of Intervention. Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust
 Valvular Heart Disease: Assessment and Timing of Intervention Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust Disclosures: Speaker fee: Bayer Acknowledgements: Matt Shun-Shin
Valvular Heart Disease: Assessment and Timing of Intervention Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust Disclosures: Speaker fee: Bayer Acknowledgements: Matt Shun-Shin
Heart Disorders. Cardiovascular Disorders (Part B-1) Module 5 -Chapter 8. Overview Heart Disorders Vascular Disorders
 Module 5 -Chapter 8. Overview Heart Disorders Vascular Disorders") Cardiovascular Disorders (Part B-1) Module 5 -Chapter 8 Overview Heart Disorders Vascular Disorders Susie Turner, MD 1/7/13 Heart Disorders Coronary Artery Disease Cardiac Arrhythmias Congestive Heart
Cardiovascular Disorders (Part B-1) Module 5 -Chapter 8 Overview Heart Disorders Vascular Disorders Susie Turner, MD 1/7/13 Heart Disorders Coronary Artery Disease Cardiac Arrhythmias Congestive Heart
REtrive. REpeat. RElearn Design by. Test-Enhanced Learning based ECG practice E-book
 Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Review of Cardiac Imaging Modalities in the Renal Patient. George Youssef
 Review of Cardiac Imaging Modalities in the Renal Patient George Youssef ECHO Left ventricular hypertrophy (LVH) assessment Diastolic dysfunction Stress ECHO Cardiac CT angiography Echocardiography - positives
Review of Cardiac Imaging Modalities in the Renal Patient George Youssef ECHO Left ventricular hypertrophy (LVH) assessment Diastolic dysfunction Stress ECHO Cardiac CT angiography Echocardiography - positives
Evaluation of a diagnostic pathway in heart failure in primary care, using electrocardiography and brain natriuretic peptide guided echocardiography
 Evaluation of a diagnostic pathway in heart failure in primary care, using electrocardiography and brain natriuretic peptide guided echocardiography Rebecka Karlsson Pardeep Jhund 1 Material and methods
Evaluation of a diagnostic pathway in heart failure in primary care, using electrocardiography and brain natriuretic peptide guided echocardiography Rebecka Karlsson Pardeep Jhund 1 Material and methods
Diagnosis is it really Heart Failure?
 ESC Congress Munich - 25-29 August 2012 Heart Failure with Preserved Ejection Fraction From Bench to Bedside Diagnosis is it really Heart Failure? Prof. Burkert Pieske Department of Cardiology Med.University
ESC Congress Munich - 25-29 August 2012 Heart Failure with Preserved Ejection Fraction From Bench to Bedside Diagnosis is it really Heart Failure? Prof. Burkert Pieske Department of Cardiology Med.University
EKG of the WEEK Questions
 EKG of the WEEK Questions ECG 1 EKG 2 A one month old with some symptoms and physical signs compatible with cardiac disease (tachypnea, FTT and loud P2). The child was born to a 42 years old mother and
EKG of the WEEK Questions ECG 1 EKG 2 A one month old with some symptoms and physical signs compatible with cardiac disease (tachypnea, FTT and loud P2). The child was born to a 42 years old mother and
Prevention of Atrial Fibrillation and Heart Failure in the Hypertensive Patient
 Prevention of Atrial Fibrillation and Heart Failure in the Hypertensive Patient The Issue of Primary Prevention of A.Fib. (and Heart Failure) and not the Prevention of Recurrent A.Fib. after Electroconversion
Prevention of Atrial Fibrillation and Heart Failure in the Hypertensive Patient The Issue of Primary Prevention of A.Fib. (and Heart Failure) and not the Prevention of Recurrent A.Fib. after Electroconversion
Detailed Order Request Checklists for Cardiology
 Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
A Diagnostic Dilemma saved by sound
 A Diagnostic Dilemma saved by sound Dr Syam Ravindranath MBBS DNB, Dr Ash Mukherjee FCEM FACEM We p r e s e n t a d i a g n o s t i c a l l y c h a l l e n g i n g s c e n a r i o in a 59 y e a r old f
A Diagnostic Dilemma saved by sound Dr Syam Ravindranath MBBS DNB, Dr Ash Mukherjee FCEM FACEM We p r e s e n t a d i a g n o s t i c a l l y c h a l l e n g i n g s c e n a r i o in a 59 y e a r old f
Heart Failure with Johnny Crash: LEFT VENTRICULAR EJECTION FRACTION (LVEF) SYMPTOMATOLOGY: Assess VENTRICULAR DYSFUNCTION HEART FAILURE:
 SYMPTOMATOLOGY: Assess VENTRICULAR DYSFUNCTION HEART FAILURE:") Heart Failure with Johnny Crash: Joan E. King, PhD, ACNP-BC, ANP-BC Melissa Smith, DNP, ANP-BC Vanderbilt University School of Nursing HEART FAILURE: Heart Failure (HF): a complex clinical syndrome resulting
Heart Failure with Johnny Crash: Joan E. King, PhD, ACNP-BC, ANP-BC Melissa Smith, DNP, ANP-BC Vanderbilt University School of Nursing HEART FAILURE: Heart Failure (HF): a complex clinical syndrome resulting
HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM
 REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
Coronary Heart Disease. Iqbal Malik
 Coronary Heart Disease Iqbal Malik Pathophysiology IHD Case chest pain Question -interactive What is the result of the exercise test? 1. negative 2. positive 3. equivocal 4. other Q2 answer STEMI! What
Coronary Heart Disease Iqbal Malik Pathophysiology IHD Case chest pain Question -interactive What is the result of the exercise test? 1. negative 2. positive 3. equivocal 4. other Q2 answer STEMI! What
Ben Taylor, PhD, PA-C
 Ben Taylor, PhD, PA-C The patient is a 23-year-old white male with a history of polysubstance abuse who was found unresponsive, last seen the day before. Classic signs of systemic hypothermia with prominent
Ben Taylor, PhD, PA-C The patient is a 23-year-old white male with a history of polysubstance abuse who was found unresponsive, last seen the day before. Classic signs of systemic hypothermia with prominent
What Is Valvular Heart Disease? Heart valve disease occurs when your heart's valves do not work the way they should.
 What Is Valvular Heart Disease? Heart valve disease occurs when your heart's valves do not work the way they should. How Do Heart Valves Work? MAINTAIN ONE-WAY BLOOD FLOW THROUGH YOUR HEART The four heart
What Is Valvular Heart Disease? Heart valve disease occurs when your heart's valves do not work the way they should. How Do Heart Valves Work? MAINTAIN ONE-WAY BLOOD FLOW THROUGH YOUR HEART The four heart
Chapter 14 Cardiovascular Emergencies Cardiovascular Emergencies Cardiovascular disease has been leading killer of Americans since.
 1 2 3 4 5 Chapter 14 Cardiovascular Emergencies Cardiovascular Emergencies Cardiovascular disease has been leading killer of Americans since. Accounts for 1 of every 2.8 deaths Cardiovascular disease (CVD)
1 2 3 4 5 Chapter 14 Cardiovascular Emergencies Cardiovascular Emergencies Cardiovascular disease has been leading killer of Americans since. Accounts for 1 of every 2.8 deaths Cardiovascular disease (CVD)
Advanced Heart Failure Management. Dr Andrew Hannah Consultant Cardiologist Aberdeen Royal Infirmary
 Advanced Heart Failure Management Dr Andrew Hannah Consultant Cardiologist Aberdeen Royal Infirmary Grading of heart failure Mr WY age 73 3/12 dyspnoea, fatigue and some ankle oedema PMH: hypertension
Advanced Heart Failure Management Dr Andrew Hannah Consultant Cardiologist Aberdeen Royal Infirmary Grading of heart failure Mr WY age 73 3/12 dyspnoea, fatigue and some ankle oedema PMH: hypertension
Hemodynamic Changes in Obstetric Anesthesia. Sonia Vaida PANA, Hershey, April 2009
 Hemodynamic Changes in Obstetric Anesthesia Sonia Vaida PANA, Hershey, April 2009 Pregnancy is a normal healthy condition and is simultaneously the most common altered physiologic state to which human
Hemodynamic Changes in Obstetric Anesthesia Sonia Vaida PANA, Hershey, April 2009 Pregnancy is a normal healthy condition and is simultaneously the most common altered physiologic state to which human
See below for descriptions of the waveform
 The internal jugular vein (IJV) connects to the right atrium without any intervening valves. The pulsation of the right atrium therefore causes the column of blood in the IJV to rise and fall this is called
The internal jugular vein (IJV) connects to the right atrium without any intervening valves. The pulsation of the right atrium therefore causes the column of blood in the IJV to rise and fall this is called
AF in the ER: Common Scenarios CASE 1. Fast facts. Diagnosis. Management
 AF in the ER: Common Scenarios Atrial fibrillation is a common problem with a wide spectrum of presentations. Below are five common emergency room scenarios and the management strategies for each. Evan
AF in the ER: Common Scenarios Atrial fibrillation is a common problem with a wide spectrum of presentations. Below are five common emergency room scenarios and the management strategies for each. Evan
THE HEART OF THE MATTER MAYANNA LUND CMH
 THE HEART OF THE MATTER MAYANNA LUND CMH CARDIOLOGY ASSESSMENT AND WHEN TO REFER CHEST PAIN - ACUTE History Examination: vital signs are vital ECG Troponin Concerns: MI, unstable angina, PE, aortic dissection
THE HEART OF THE MATTER MAYANNA LUND CMH CARDIOLOGY ASSESSMENT AND WHEN TO REFER CHEST PAIN - ACUTE History Examination: vital signs are vital ECG Troponin Concerns: MI, unstable angina, PE, aortic dissection
Diagnosis & Management of Heart Failure. Abena A. Osei-Wusu, M.D. Medical Fiesta
 Diagnosis & Management of Heart Failure Abena A. Osei-Wusu, M.D. Medical Fiesta Learning Objectives: 1) Become familiar with pathogenesis of congestive heart failure. 2) Discuss clinical manifestations
Diagnosis & Management of Heart Failure Abena A. Osei-Wusu, M.D. Medical Fiesta Learning Objectives: 1) Become familiar with pathogenesis of congestive heart failure. 2) Discuss clinical manifestations
Cardiovascular Disorders. Heart Disorders. Diagnostic Tests for CV Function. Bio 375. Pathophysiology
 Cardiovascular Disorders Bio 375 Pathophysiology Heart Disorders Heart disease is ranked as a major cause of death in the U.S. Common heart diseases include: Congenital heart defects Hypertensive heart
Cardiovascular Disorders Bio 375 Pathophysiology Heart Disorders Heart disease is ranked as a major cause of death in the U.S. Common heart diseases include: Congenital heart defects Hypertensive heart
Colin Edwards. Cardiologist Auckland Heart Group Waitemata Health
 Colin Edwards Cardiologist Auckland Heart Group Waitemata Health AUG 2012 Introduction Case Summary BP MEASUREMENTS measured seated mean of 2 BP recordings per visit at least 2 visits Diet Exercise Weight
Colin Edwards Cardiologist Auckland Heart Group Waitemata Health AUG 2012 Introduction Case Summary BP MEASUREMENTS measured seated mean of 2 BP recordings per visit at least 2 visits Diet Exercise Weight
Case Summary. Workshop Overview. Mr. M
 9:00 10:30 Workshop Overview Mr. M Who is this document primarily intended to reach? What is the format? How soon should I see a newly referred heart failure patient? How often should my heart failure
9:00 10:30 Workshop Overview Mr. M Who is this document primarily intended to reach? What is the format? How soon should I see a newly referred heart failure patient? How often should my heart failure
Images have been removed from the PowerPoint slides in this handout due to copyright restrictions.
 Heart Failure Heart Failure Introduction and History AHA 2015 Statistics About 6 million Americans 870,000 new cases each year 1 in 9 deaths related to HF Almost 1 million hospitalizations each year (cost
Heart Failure Heart Failure Introduction and History AHA 2015 Statistics About 6 million Americans 870,000 new cases each year 1 in 9 deaths related to HF Almost 1 million hospitalizations each year (cost
Use of Nuclear Cardiology in Myocardial Viability Assessment and Introduction to PET and PET/CT for Advanced Users
 Use of Nuclear Cardiology in Myocardial Viability Assessment and Introduction to PET and PET/CT for Advanced Users February 1 5, 2011 University of Santo Tomas Hospital Angelo King A-V Auditorium Manila,
Use of Nuclear Cardiology in Myocardial Viability Assessment and Introduction to PET and PET/CT for Advanced Users February 1 5, 2011 University of Santo Tomas Hospital Angelo King A-V Auditorium Manila,