EKG of the WEEK Questions
|
|
|
- Ruth Carroll
- 5 years ago
- Views:
Transcription
1 EKG of the WEEK Questions
2 ECG 1
3 EKG 2 A one month old with some symptoms and physical signs compatible with cardiac disease (tachypnea, FTT and loud P2). The child was born to a 42 years old mother and was also noticed to have increased nuchal translucency on a routine nuchal scan performed at 13 weeks gestation. 1. The first question was to identify the rhythm and the anomalies on the EKG. 2. Name the most likely cardiac malformation associating these clinical and EKG findings.

4 EKG of the week 1-5 Oct 2012 Survey EKG of the week 1-5 Oct 2012 EKG :41 PM 8 year old boy was brought to ER for chest pain. He has mild developmental delay and ADHD and is on Concerta. He feels the pain mostly at night when he goes to sleep. 1. What is the rhythm? 1. Sinus arrhythmia 2. Junctional extrasystole 3. Premature atrial contractions 4. Premature ventricular contractions 5. Second degree AV block Mobitz 1 (Wenckebach) Done Powered by SurveyMonkey Check out our sample surveys and create your own now! Page 1 of 2
5 EKG of the week 1-5 Oct 2012 Survey EKG :41 PM Page 2 of 2

6 EKG of the week 8-12 Oct 2012 Survey EKG of the week 8-12 Oct 2012 EKG :14 PM This baby was brought directly from the delivery room to the NICU due to increased HR noticed immediately after delivery. The baby is alert, crying, breathing spontaneously with good respiratory effort. The HR is 210/min. An UVC is put in place. 1. List at least 2 possible causes for this rhythm and describe how you would differentiate between them. Page 1 of 2
7

8 EKG of the week Oct 29th - Nov 2nd 2012 Survey EKG of the week Oct 29th - Nov 2nd 2012 EKG :11 AM 1. Before you begin the test, please identify yourself with one of the following groups 1. CHEO 2. DGP McMaster 3. Sickkids 4. MacPeds A one month old boy is brought by his parents to the ER for runny nose, tachypnea and decreased feeding. On exam the baby is alert, afebrile, respiratory rate is 80/min with mild-moderate respiratory distress, arterial saturation are 85%. The precordium is active, 2/6 systolic murmur is heard on auscultation, the liver in normal in size and the peripheral pulses are equally palpated throughout. CBC shows hemoglobin 140 g/l. An EKG and a CXR are done. Page 1 of 2

9 EKG of the week Oct 29th - Nov 2nd 2012 Survey EKG :11 AM 2. Enumerate the anomalies encountered on the EKG. What is the rhythm? 3. Considering the findings listed above, should the baby have central cyanosis? 1. Yes 2. No 4. What is the most likely cardiac lesion in this child? 1. Tetralogy of Fallot 2. Tricuspid atresia 3. Large VSD 4. AVSD+TGA 5. Ebstein anomaly Done Powered by SurveyMonkey Check out our sample surveys and create your own now! Page 2 of 2

10 EKG of the week Nov 5th - Nov 9th 2012 Survey EKG of the week Nov 5th - Nov 9th 2012 EKG :43 AM 1. Before you begin the test, please identify yourself with one of the following groups 1. CHEO 2. DGP McMaster 3. Sickkids 4. MacPeds 4 year old girl comes to the ER after an episode of seizures lasting for about 1 minute occurring during a febrile illness. This is her third episode of this kind, only this time she complained of chest pain before losing consciousness. On admission her temperature is 38.5 C, she is confused, irritable, mildly tachycardic, but otherwise her vitals are reassuring. The physical examination reveals a 2/6 mid-systolic vibratory murmur at the LLSB, the rest of the cardiovascular examination is normal. You order an EKG and a CXR to rule-out heart disease. 2. What does the EKG and the clinical assessment suggest? 1. Possible ASD. 2. Brugada. 3. Complete RBBB. Page 1 of 2
11 EKG of the week Nov 5th - Nov 9th 2012 Survey 4. Acute anterior myocardial infarction. 5. Pericarditis. 6. Long QT syndrome. 7. Febrile seizures + innocent heart murmur 8. Mitral valve regurgitation, possible endocarditis EKG :43 AM 3. What are the (2-3) supporting arguments for your choice? Done Powered by SurveyMonkey Check out our sample surveys and create your own now! Page 2 of 2

12 EKG of the week Nov 12th - Nov 16th 2012 Survey EKG of the week Nov 12th - Nov 16th 2012 EKG :34 PM 1. Please start by choosing your appropriate affiliation from the list below. 1. CHEO 2. DGP McMaster 3. Sickkids 4. MacPeds A 5 year old girl was brought to the pediatrician's office by her mother because of coughing during exercise for the past 3 weeks that was now interfering with her sporting activities. On examination the child looked normally developed and in no distress. There was no tachypnea, the chest was clear on auscultation with good air entry bilaterally and no adventitious sounds. The PMI was palpated in the 5th intercostal space lateral to the MCL, the precordium was active, a 2/6 pansystolic murmur radiating to the axila could be heard at the apex. The pediatrician performs an EKG and a CXR. CXR AP Page 1 of 3


13 EKG of the week Nov 12th - Nov 16th 2012 Survey EKG :34 PM CXR Lateral 2. What is the rhythm? Enumerate the anomalies encountered on this EKG. Page 2 of 3
14 EKG of the week Nov 12th - Nov 16th 2012 Survey 3. What is the most likely scenario in this child? 1. VSD, heart failure, sinus tachycardia 2. Chronic aortic valve regurgitation, secondary heart failure, sinus tachycardia EKG :34 PM 3. Dilated cardiomyopathy, heart failure, secondary mitral valve regurgitation, sinus tachycardia 4. Tachycardia-induced cardiomyopathy, heart failure, secondary mitral valve regurgitation 5. Exercise-induced asthma, innocent heart murmur, sinus tachycardia Done Powered by SurveyMonkey Check out our sample surveys and create your own now! Page 3 of 3

15 EKG Dec 10th - Dec 15th 2012 EKG Question 9 1. Please start by choosing your appropriate affiliation from the list below. 1. CHEO 2. DGP McMaster 3. Sickkids 4. MacPeds A 6 year old boy was brought to the ER by his mother for a recurrent episode of wheezing. On examination the child looked normally developed, t = 38C, the RR was about 35/min with moderate respiratory distress, HR = 110/min, SpO2= 90% in room air, warm and well perfused, BP= 105/68 mmhg. On auscultation there were diffuse wheezes and crackles bilaterally. The precordium was quiet, PMI in the 5th i.c. space on left mid clavicular line, S1 and S2 were normal but the cardiac auscultation was difficult due to the respiratory noises. The liver was firm and palpated at 2 cm below the right costal margin on the mid clavicular line. The child received Salbutamol nebulizations, 2 L/min O2 by nasal prongs and Tylenol for fever after which the SpO2 increased to 95% and RR decreased to 25/min. Later the child fell asleep and you repeated the cardiac exam. The cardiac rhythm was irregular, a variable split of the S2 and a 2/6 mid systolic vibratory murmur at the LLSB could be heard. You explained to the mother the findings and your decision to perform an EKG to help you in the differential diagnosis. 2. The mother was anxious because nobody has told her before that the child had anything wrong with his heart. What do you tell the mother after reviewing the EKG? (from the corresponding columns choose one or more EKG and one or more Clinical findings that you would include in you answer)
16 EKG Findings 1. PACs due to Salbutamol nebulizations 2. Second degree AV block Mobitz 1 during sleep 3. Sinus arrhythmia 4. Possible RV hypertrophy (positive T in V2 before 8 years of age) EKG Question 9 Clinical findings 1. CHF 2. Still's murmur 3. Tricuspid valve regurgitation 4. VSD 3. Justify your selection. 4. What would be your management plan? 1. Reassure 2. Refer to cardiologist 3. Order echo Done
 This 12 year old is brought to the pediatrician's office for repeated headaches.")
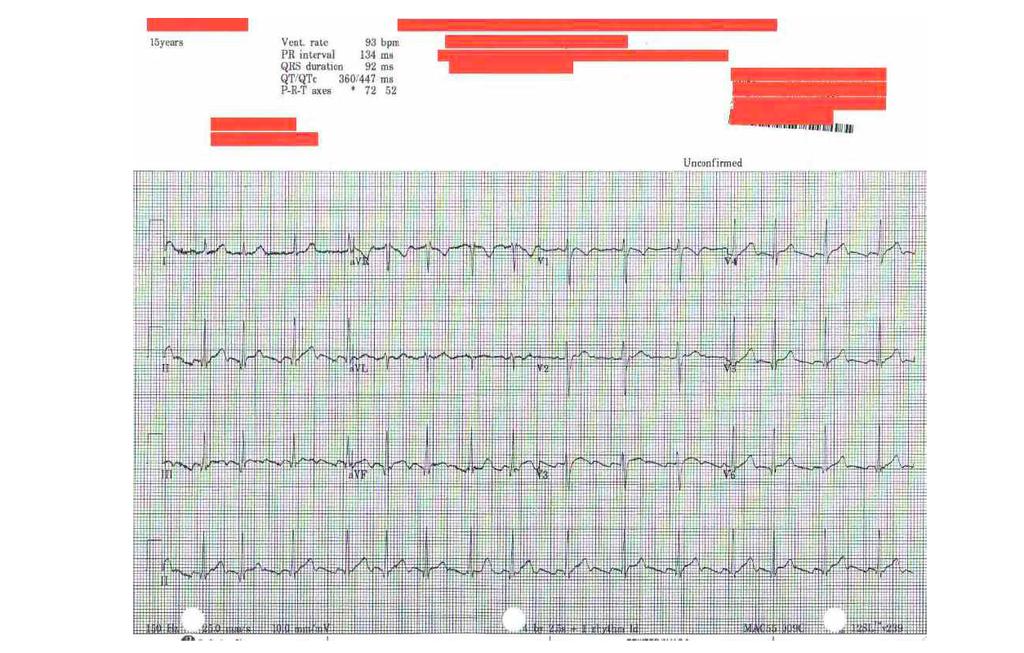
17 EKG Feb 4th 2013 EKG Question Please start by choosing your appropriate affiliation from the list below. 1. CHEO 2. DGP McMaster 3. Sickkids 4. MacPeds Other (please specify) This 12 year old is brought to the pediatrician's office for repeated headaches. On exam you notice that his BP was above the 95% for age and height on two consecutive measurements. The nurse performs a 12 lead EKG. 2. What is your decison based on the above findings? 1. The clinical and EKG findings suggest the child may have persistent hypertension 2. The EKG is normal, the child may have "white coat" hypertension 3. You would repeat the EKG as it is suboptimal Done
 Term baby noticed to have an irregular heart rhythm on routine physical examination before hospital discharge.")
18 EKG March 1st 2013 EKG Please start by choosing your appropriate affiliation from the list below. 1. CHEO 2. DGP McMaster 3. Sickkids 4. MacPeds Other (please specify) Term baby noticed to have an irregular heart rhythm on routine physical examination before hospital discharge. A 12 lead EKG is done as part of the initial investigation. 2. What is the rhythm? 1. Sinus arrhythmia 2. Second degree AV block Mobitz 1 (Wenkebach) 3. Atrial trigeminy 3. Atrial Fibrilation 4. Ventricular bigeminy
19 EKG 11 Done
 16 old previously healthy female comes to the emergency room 5 days after delivering a term baby with chest pain and shortness of breath.")
20 EKG March 18th 2013 EKG Please start by choosing your appropriate affiliation from the list below. 1. CHEO 2. DGP McMaster 3. Sickkids 4. MacPeds Other (please specify) 16 old previously healthy female comes to the emergency room 5 days after delivering a term baby with chest pain and shortness of breath. Past medical history is significant for Kawasaki disease in childhood. 2. What is the most concerning finding on this EKG?
21 3. In the clinical context described above, this EKG is compatible with which of the following: EKG Pulmonary embolism 2. Congestive heart failure 3. Myocardial ischemia 4. Cardiac tamponade 5. All of the above Done

22 April EKG Week 13 4 months old with ALTE 1. What is the diagnosis? 1. Left ventricular hypertrophy 2. Left bundle branch block 3. Premature atrial contractions 4. Accelerated idioventricular rhythm 5. Premature ventricular contractions Done
 2. What cardiac malformation does this EKG best correlate with? 1. ASD 2. Pulmonary valve stenosis 3. VSD 4. AVSD 5.")
23 May 22nd Please start by choosing your appropriate affiliation from the list below. 1. CHEO 2. DGP McMaster 3. Sickkids 4. MacPeds Other (please specify) 2. What cardiac malformation does this EKG best correlate with? 1. ASD 2. Pulmonary valve stenosis 3. VSD 4. AVSD 5. Coarctation of the aorta Done
24
25 June 3rd 2013 EKG Please start by choosing your appropriate affiliation from the list below. 1. CHEO 2. DGP McMaster 3. Sickkids 4. MacPeds Other (please specify) 2. What is the cause of this boys' irregular heart rhythm? 1. Blocked PACs 2. Wenckebach 3. Frequent PACs 4. Polymorphic PVCs 5. Sinus arrhythmia 3. Why does the QRS morphology vary?
26 EKG Done15

27 Aug Please start by choosing your appropriate affiliation from the list below. 1. CHEO 2. DGP McMaster 3. Sickkids 4. MacPeds 5. Gomoiu 6. IOMC 7. Other Other (please specify) 2. The EKG was performed to clarify a rhythm irregularity seen on the monitor in this newborn. What abnormality do you see on this rhythm strip? 1. Blocked PACs 2. Artefacts 3. Frequent PACs 4. Interpolated PVCs 5. Sinus arrhythmia
28 3. Justify your answer to the previous question Done
29 Sept Question EKG Please start by choosing your appropriate affiliation from the list below. 1. CHEO 2. DGP McMaster 3. Sickkids 4. MacPeds 5. Gomoiu 6. IOMC 7. Other Other (please specify) year old asian boy was brought to the ER by parents with chest pain. What does the EKG show? 1. Inferior myocardial infarction 2. LVH 3. Left bundle branch block 4. WPW 5. Left anterior hemiblock 3. What technical issue is there on this EKG?
30 Question EKG If this child would complain of frequently recurring chest pain accompanied by chest pounding and lightheadedness, particularly associated with exercise, what test would be most likely to discover something abnormal? 1. Echocardiogram 2. CT angio 3. Angiogram 4. Holter Other (please specify) Done
 2. 2 year old boy comes to the Emergency Department for minor chest trauma. The child was examined and an EKG was performed.")
31 Oct Survey Oct EKG :46 PM 1. Please start by choosing your affiliation from the list below. 1. CHEO 2. DGP McMaster 3. Sickkids 4. MacPeds 5. Gomoiu 6. IOMC 7. Other Other (please specify) 2. 2 year old boy comes to the Emergency Department for minor chest trauma. The child was examined and an EKG was performed. He was in no distress, there was no obvious bruising on his chest and no pain on gentle pressure. The precordium was quiet and the point of maximum impulse was in the 4th intercostal space on the left mid clavicular line. S1 was normal, S2 was variably split and there was a 2/6 mid-systolic vibratory murmur at the left lower border. The Page 1 of 2
32 Oct Survey EKG 18 diastole was quiet. The rest of the physical exam was normal. The family history was reassuring and the past medical history unremarkable :46 PM What does the EKG show? 3. What would you decide next? 1. Discharge the child 2. Order an echocardiogram 3. Repeat the EKG 4. Admit the child 5. Order cardiac enzymes 4. Questions or comments related to this quiz? Done Page 2 of 2
ECG Workshop. Nezar Amir
 ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
2) VSD & PDA - Dr. Aso
 VSD & PDA - Dr. Aso") 2) VSD & PDA - Dr. Aso Ventricular Septal Defect (VSD) Most common cardiac malformation 25-30 % Types of VSD: According to position perimembranous, inlet, muscular. According to size small, medium, large.
2) VSD & PDA - Dr. Aso Ventricular Septal Defect (VSD) Most common cardiac malformation 25-30 % Types of VSD: According to position perimembranous, inlet, muscular. According to size small, medium, large.
Paediatrics Revision Session Cardiology. Emma Walker 7 th May 2016
 Paediatrics Revision Session Cardiology Emma Walker 7 th May 2016 Cardiovascular Examination! General:! Make it fun!! Change how you act depending on their age! Introduction! Introduce yourself & check
Paediatrics Revision Session Cardiology Emma Walker 7 th May 2016 Cardiovascular Examination! General:! Make it fun!! Change how you act depending on their age! Introduction! Introduce yourself & check
Cardiac Examination. Pediatrics Clinical Examination
 Pediatrics Clinical Examination Symptoms of Cardiovascular Affection: Cardiac Examination 1. Perinatal history: Maternal DM, cyanosis, respiratory distress 2. Symptoms of lung congestion: Poor interrupted
Pediatrics Clinical Examination Symptoms of Cardiovascular Affection: Cardiac Examination 1. Perinatal history: Maternal DM, cyanosis, respiratory distress 2. Symptoms of lung congestion: Poor interrupted
Anatomy & Physiology
 1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
Congenital heart disease. By Dr Saima Ali Professor of pediatrics
 Congenital heart disease By Dr Saima Ali Professor of pediatrics What is the most striking clinical finding in this child? Learning objectives By the end of this lecture, final year student should be able
Congenital heart disease By Dr Saima Ali Professor of pediatrics What is the most striking clinical finding in this child? Learning objectives By the end of this lecture, final year student should be able
Appendix D Output Code and Interpretation of Analysis
 Appendix D Output Code and Interpretation of Analysis 8 Arrhythmia Code No. Description 8002 Marked rhythm irregularity 8110 Sinus rhythm 8102 Sinus arrhythmia 8108 Marked sinus arrhythmia 8120 Sinus tachycardia
Appendix D Output Code and Interpretation of Analysis 8 Arrhythmia Code No. Description 8002 Marked rhythm irregularity 8110 Sinus rhythm 8102 Sinus arrhythmia 8108 Marked sinus arrhythmia 8120 Sinus tachycardia
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM. General Instructions: ID NUMBER: FORM NAME: H F A DATE: 10/13/2017 VERSION: CONTACT YEAR NUMBER:
 ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM General Instructions: The Heart Failure Hospital Record Abstraction Form is completed for all heart failure-eligible cohort hospitalizations. Refer to
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM General Instructions: The Heart Failure Hospital Record Abstraction Form is completed for all heart failure-eligible cohort hospitalizations. Refer to
REtrive. REpeat. RElearn Design by. Test-Enhanced Learning based ECG practice E-book
 Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Recommended Evaluation Data Excerpt from NVIC 04-08
 Recommended Evaluation Data Excerpt from NVIC 04-08 Purpose: This document is an excerpt from the Medical and Physical Evaluations Guidelines for Merchant Mariner Credentials, contained in enclosure 3
Recommended Evaluation Data Excerpt from NVIC 04-08 Purpose: This document is an excerpt from the Medical and Physical Evaluations Guidelines for Merchant Mariner Credentials, contained in enclosure 3
High Yield Associations Cardio for Step 1. Amanda Krauss, Adee Elhamdani
 High Yield Associations Cardio for Step 1 Amanda Krauss, Adee Elhamdani EKGs Irregularly irregular with no p waves and inconsistent RR intervals High Yield new onset MC risk factors Regular PP intervals
High Yield Associations Cardio for Step 1 Amanda Krauss, Adee Elhamdani EKGs Irregularly irregular with no p waves and inconsistent RR intervals High Yield new onset MC risk factors Regular PP intervals
CongHeartDis.doc. Андрій Миколайович Лобода
 CongHeartDis.doc Андрій Миколайович Лобода 2015 Зміст 3 Зміст Зміст 4 A child with tetralogy of Fallot is most likely to exhibit: -Increased pulmonary blood flow -Increased pressure in the right ventricle
CongHeartDis.doc Андрій Миколайович Лобода 2015 Зміст 3 Зміст Зміст 4 A child with tetralogy of Fallot is most likely to exhibit: -Increased pulmonary blood flow -Increased pressure in the right ventricle
physiology 6 Mohammed Jaafer Turquoise team
 15 physiology 6 Mohammed Jaafer 22-3-2016 Turquoise team Cardiac Arrhythmias and Their Electrocardiographic Interpretation Today, we are going to talk about the abnormal excitation. As we said before,
15 physiology 6 Mohammed Jaafer 22-3-2016 Turquoise team Cardiac Arrhythmias and Their Electrocardiographic Interpretation Today, we are going to talk about the abnormal excitation. As we said before,
Introduction. Pediatric Cardiology. General Appearance. Tools of Assessment. Auscultation. Vital Signs
 Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
12-Lead ECG Interpretation. Kathy Kuznar, RN, ANP
 12-Lead ECG Interpretation Kathy Kuznar, RN, ANP The 12-Lead ECG Objectives Identify the normal morphology and features of the 12- lead ECG. Perform systematic analysis of the 12-lead ECG. Recognize abnormalities
12-Lead ECG Interpretation Kathy Kuznar, RN, ANP The 12-Lead ECG Objectives Identify the normal morphology and features of the 12- lead ECG. Perform systematic analysis of the 12-lead ECG. Recognize abnormalities
Notes by Sandra Dankwa 2009 HF- Heart Failure DS- Down Syndrome IE- Infective Endocarditis ET- Exercise Tolerance. Small VSD Symptoms -asymptomatic
 Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition
 Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Chad Morsch B.S., ACSM CEP
 What Is Cardiac Stress Testing? Chad Morsch B.S., ACSM CEP A Cardiac Stress Test is a test used to measure the heart's ability to respond to external stress in a controlled clinical environment. Cardiac
What Is Cardiac Stress Testing? Chad Morsch B.S., ACSM CEP A Cardiac Stress Test is a test used to measure the heart's ability to respond to external stress in a controlled clinical environment. Cardiac
A walk through a STEMI
 A walk through a STEMI M.M. s Story Kim Robison Ashley Corcoran Situation M.M. is an 82 year old male brought in by private vehicle on 10/22/17 to the Emergency Department Pt. c/o left arm numbness, pain
A walk through a STEMI M.M. s Story Kim Robison Ashley Corcoran Situation M.M. is an 82 year old male brought in by private vehicle on 10/22/17 to the Emergency Department Pt. c/o left arm numbness, pain
Basic Dysrhythmia Interpretation
 Basic Dysrhythmia Interpretation Objectives 2 To understand the Basic ECG To understand the meaning of Dysrhythmia To describe the normal heart conduction system. To describe the normal impulse pathways.
Basic Dysrhythmia Interpretation Objectives 2 To understand the Basic ECG To understand the meaning of Dysrhythmia To describe the normal heart conduction system. To describe the normal impulse pathways.
Rhythm ECG Characteristics Example. Normal Sinus Rhythm (NSR)
") Normal Sinus Rhythm (NSR) Rate: 60-100 per minute Rhythm: R- R = P waves: Upright, similar P-R: 0.12-0.20 second & consistent P:qRs: 1P:1qRs Sinus Tachycardia Exercise Hypovolemia Medications Fever Substances
Normal Sinus Rhythm (NSR) Rate: 60-100 per minute Rhythm: R- R = P waves: Upright, similar P-R: 0.12-0.20 second & consistent P:qRs: 1P:1qRs Sinus Tachycardia Exercise Hypovolemia Medications Fever Substances
HISTORY. Question: How do you interpret the patient s history? CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: 45-year-old man.
 HISTORY 45-year-old man. CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: His dyspnea began suddenly and has been associated with orthopnea, but no chest pain. For two months he has felt
HISTORY 45-year-old man. CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: His dyspnea began suddenly and has been associated with orthopnea, but no chest pain. For two months he has felt
Uptofate Study Summary
 CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
Heart sounds and murmurs. Dr. Szathmári Miklós Semmelweis University First Department of Medicine 15. Oct
 Heart sounds and murmurs Dr. Szathmári Miklós Semmelweis University First Department of Medicine 15. Oct. 2013. Conditions for auscultation of the heart Quiet room Patient comfortable Chest fully exposed
Heart sounds and murmurs Dr. Szathmári Miklós Semmelweis University First Department of Medicine 15. Oct. 2013. Conditions for auscultation of the heart Quiet room Patient comfortable Chest fully exposed
PAEDIATRIC EMQs. Andrew A Mallick Paediatrics.info.
 PAEDIATRIC EMQs Andrew A Mallick Paediatrics.info www.paediatrics.info Paediatric EMQs Paediatrics.info First published in the United Kingdom in 2012. While the advice and information in this book is believed
PAEDIATRIC EMQs Andrew A Mallick Paediatrics.info www.paediatrics.info Paediatric EMQs Paediatrics.info First published in the United Kingdom in 2012. While the advice and information in this book is believed
Please check your answers with correct statements in answer pages after the ECG cases.
 ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
Electrical System Overview Electrocardiograms Action Potentials 12-Lead Positioning Values To Memorize Calculating Rates
 Electrocardiograms Electrical System Overview James Lamberg 2/ 74 Action Potentials 12-Lead Positioning 3/ 74 4/ 74 Values To Memorize Inherent Rates SA: 60 to 100 AV: 40 to 60 Ventricles: 20 to 40 Normal
Electrocardiograms Electrical System Overview James Lamberg 2/ 74 Action Potentials 12-Lead Positioning 3/ 74 4/ 74 Values To Memorize Inherent Rates SA: 60 to 100 AV: 40 to 60 Ventricles: 20 to 40 Normal
Junctional Premature Contraction (JPC)
") Where s the PAC? Junctional Premature Contraction (JPC) A junctional premature contraction (JPC) is a beat that originates prematurely in the AV node. It can occur sporadically or in a grouped pattern.
Where s the PAC? Junctional Premature Contraction (JPC) A junctional premature contraction (JPC) is a beat that originates prematurely in the AV node. It can occur sporadically or in a grouped pattern.
APPROACH TO CARDIAC HISTORY TAKING. Index
 Christopher Cheung APPROACH TO CARDIAC HISTORY TAKING Index General Presentation...1 2 Table 1 Congenital Heart Conditions...2 Questions to Ask...2 Table 2 PQRSTAAA Mnemonic Approach to Chest Pain...3
Christopher Cheung APPROACH TO CARDIAC HISTORY TAKING Index General Presentation...1 2 Table 1 Congenital Heart Conditions...2 Questions to Ask...2 Table 2 PQRSTAAA Mnemonic Approach to Chest Pain...3
Congenital Heart Disease: Physiology and Common Defects
 Congenital Heart Disease: Physiology and Common Defects Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director,
Congenital Heart Disease: Physiology and Common Defects Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director,
Cardiology Competency Based Goals and Objectives
 Cardiology Competency Based Goals and Objectives COMPETENCY 1. Patient Care. Provide family centered patient care that is developmentally and age appropriate, compassionate, and effective for the treatment
Cardiology Competency Based Goals and Objectives COMPETENCY 1. Patient Care. Provide family centered patient care that is developmentally and age appropriate, compassionate, and effective for the treatment
EKG Competency for Agency
 EKG Competency for Agency Name: Date: Agency: 1. The upper chambers of the heart are known as the: a. Atria b. Ventricles c. Mitral Valve d. Aortic Valve 2. The lower chambers of the heart are known as
EKG Competency for Agency Name: Date: Agency: 1. The upper chambers of the heart are known as the: a. Atria b. Ventricles c. Mitral Valve d. Aortic Valve 2. The lower chambers of the heart are known as
12 Lead ECG Interpretation
 12 Lead ECG Interpretation Julie Zimmerman, MSN, RN, CNS, CCRN Significant increase in mortality for every 15 minutes of delay! N Engl J Med 2007;357:1631-1638 Who should get a 12-lead ECG? Also include
12 Lead ECG Interpretation Julie Zimmerman, MSN, RN, CNS, CCRN Significant increase in mortality for every 15 minutes of delay! N Engl J Med 2007;357:1631-1638 Who should get a 12-lead ECG? Also include
Approach to a baby with cyanosis
 Approach to a baby with cyanosis Objectives Cyanosis : types Differentials: cardiac vs. non cardiac Approach Case scenarios Cyanosis Greek word kuaneos meaning dark blue Bluish discolouration of skin,
Approach to a baby with cyanosis Objectives Cyanosis : types Differentials: cardiac vs. non cardiac Approach Case scenarios Cyanosis Greek word kuaneos meaning dark blue Bluish discolouration of skin,
Pathological Arrhythmias/ Tachyarrhythmias
 Pathological Arrhythmias/ Tachyarrhythmias caused by: 1.Ectopic focus: Extrasystole or premature beat. If discharge is occasional. Can be: Atrial Extrasystole Vevtricular Extrasystole 2.Cardiac Arrhythmia
Pathological Arrhythmias/ Tachyarrhythmias caused by: 1.Ectopic focus: Extrasystole or premature beat. If discharge is occasional. Can be: Atrial Extrasystole Vevtricular Extrasystole 2.Cardiac Arrhythmia
Dear Parent/Guardian,
 Dear Parent/Guardian, You have indicated on school records that your child has an ongoing health problem that may require medication and/or treatment during the school day with rescue medication. Attached
Dear Parent/Guardian, You have indicated on school records that your child has an ongoing health problem that may require medication and/or treatment during the school day with rescue medication. Attached
Pediatric Board Review Congenital Heart Disease. Steven H. Todman, M.D. Pediatric Cardiologist Louisiana State University
 Pediatric Board Review Congenital Heart Disease Steven H. Todman, M.D. Pediatric Cardiologist Louisiana State University Our Mission To discuss various types of congenital heart disease that are commonly
Pediatric Board Review Congenital Heart Disease Steven H. Todman, M.D. Pediatric Cardiologist Louisiana State University Our Mission To discuss various types of congenital heart disease that are commonly
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Cardiology/Cardiothoracic
 Cardiology/Cardiothoracic ICD-9-CM to ICD-10-CM Code Mapper 800-334-5724 www.contexomedia.com 2013 ICD-9-CM 272.0 Pure hypercholesterolemia 272.2 Mixed hyperlipidemia 272.4 Other and hyperlipidemia 278.00
Cardiology/Cardiothoracic ICD-9-CM to ICD-10-CM Code Mapper 800-334-5724 www.contexomedia.com 2013 ICD-9-CM 272.0 Pure hypercholesterolemia 272.2 Mixed hyperlipidemia 272.4 Other and hyperlipidemia 278.00
Syncope: Ockham s Razor
 Syncope: Ockham s Razor Time/Place Wednesday, 25 th January 2006 10am-12pm Room 210, Wallace Wurth Building Facilitators Michael Grimm & Tony Grabs Aims Illustrate multiple possible causes for a common
Syncope: Ockham s Razor Time/Place Wednesday, 25 th January 2006 10am-12pm Room 210, Wallace Wurth Building Facilitators Michael Grimm & Tony Grabs Aims Illustrate multiple possible causes for a common
CARDIAC EXAMINATION MINI-QUIZ
 CARDIAC EXAMINATION MINI-QUIZ 1. Sitting bolt upright, your dyspneic (short of breath) patient has visible jugular venous pulsations to the angle of his jaw, which is 12 cm above his sternal angle. What
CARDIAC EXAMINATION MINI-QUIZ 1. Sitting bolt upright, your dyspneic (short of breath) patient has visible jugular venous pulsations to the angle of his jaw, which is 12 cm above his sternal angle. What
Congenital Heart Disease
 Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
15 16 September Seminar W10O. ECG for General Practice
 15 16 September 2012 Seminar W10O ECG for General Practice Speaker: Ms Natasha Eaton ECG for General Practice Speaker: Natasha Eaton Cardiac CNC Executive Representative Electrocardiography The graphic
15 16 September 2012 Seminar W10O ECG for General Practice Speaker: Ms Natasha Eaton ECG for General Practice Speaker: Natasha Eaton Cardiac CNC Executive Representative Electrocardiography The graphic
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016
 Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Congenital Heart Disease Cases
 Congenital Heart Disease Cases Sabrina Phillips, MD FACC FASE Mayo Clinic Congenital Heart Disease Center 2013 MFMER slide-1 No Disclosures 2013 MFMER slide-2 1 CASE 1 2013 MFMER slide-3 63 year old Woman
Congenital Heart Disease Cases Sabrina Phillips, MD FACC FASE Mayo Clinic Congenital Heart Disease Center 2013 MFMER slide-1 No Disclosures 2013 MFMER slide-2 1 CASE 1 2013 MFMER slide-3 63 year old Woman
Appropriate Use Criteria for Initial Transthoracic Echocardiography in Outpatient Pediatric Cardiology (scores listed by Appropriate Use rating)
") Appropriate Use Criteria for Initial Transthoracic Echocardiography in Outpatient Pediatric Cardiology (scores listed by Appropriate Use rating) Table 1: Appropriate indications (median score 7-9) Indication
Appropriate Use Criteria for Initial Transthoracic Echocardiography in Outpatient Pediatric Cardiology (scores listed by Appropriate Use rating) Table 1: Appropriate indications (median score 7-9) Indication
CONGENITAL HEART DISEASE (CHD)
") CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
Valvular Heart Disease Mitral Stenosis
 Valvular Heart Disease Mitral Stenosis A 75 year old woman with loud first heart sound and mid-diastolic murmur Chronic dyspnea Class 2/4 Fatigue Recent orthopnea/pnd Nocturnal palpitation Pedal edema
Valvular Heart Disease Mitral Stenosis A 75 year old woman with loud first heart sound and mid-diastolic murmur Chronic dyspnea Class 2/4 Fatigue Recent orthopnea/pnd Nocturnal palpitation Pedal edema
HEART CONDITIONS IN SPORT
 HEART CONDITIONS IN SPORT Dr. Anita Green CHD Risk Factors Smoking Hyperlipidaemia Hypertension Obesity Physical Inactivity Diabetes Risks are cumulative (multiplicative) Lifestyles predispose to RF One
HEART CONDITIONS IN SPORT Dr. Anita Green CHD Risk Factors Smoking Hyperlipidaemia Hypertension Obesity Physical Inactivity Diabetes Risks are cumulative (multiplicative) Lifestyles predispose to RF One
WOLFF PARKINSON WHITE SYNDROME. Katarzyna Bigaj PGY-1
 WOLFF PARKINSON WHITE SYNDROME Katarzyna Bigaj PGY-1 Preexcitation is defined as a premature activation of the ventricular myocardium by an impulse that travels by an anomalous path and avoids physiologic
WOLFF PARKINSON WHITE SYNDROME Katarzyna Bigaj PGY-1 Preexcitation is defined as a premature activation of the ventricular myocardium by an impulse that travels by an anomalous path and avoids physiologic
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series
 ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
PATENT DUCTUS ARTERIOSUS (PDA)
") PATENT DUCTUS ARTERIOSUS (PDA) It is a channel that connect the pulmonary artery with the descending aorta (isthumus part). It results from the persistence of patency of the fetal ductus arteriosus after
PATENT DUCTUS ARTERIOSUS (PDA) It is a channel that connect the pulmonary artery with the descending aorta (isthumus part). It results from the persistence of patency of the fetal ductus arteriosus after
DORV: The Great Chameleon. Heart Conference October 15, 2016 Tina Kwan, MD
 DORV: The Great Chameleon Heart Conference October 15, 2016 Tina Kwan, MD Kenneth Maehara, Ph.D. May 7, 1942 - August 26, 2013 A.R. A classic case of broken heart 38 week AGA F born at an OSH to
DORV: The Great Chameleon Heart Conference October 15, 2016 Tina Kwan, MD Kenneth Maehara, Ph.D. May 7, 1942 - August 26, 2013 A.R. A classic case of broken heart 38 week AGA F born at an OSH to
What s That Sound? Pediatric Murmur Evaluation
 What s That Sound? Pediatric Murmur Evaluation Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director, Pediatric
What s That Sound? Pediatric Murmur Evaluation Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director, Pediatric
HR: 50 bpm (Sinus) PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70. Sinus bradycardia with one ventricular escape (*)
 PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70. Sinus bradycardia with one ventricular escape (*)") 1? HR: 50 bpm (Sinus) PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70 1 Sinus P waves? 2 sinus cycles The pause (2 sinus cycles) suggests that the sinus fired (?) but did not conduct to the atria (i.e., missing
1? HR: 50 bpm (Sinus) PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70 1 Sinus P waves? 2 sinus cycles The pause (2 sinus cycles) suggests that the sinus fired (?) but did not conduct to the atria (i.e., missing
Severe Hypertension. Pre-referral considerations: 1. BP of arm and Leg 2. Ambulatory BP 3. Renal causes
 Severe Hypertension *Prior to making a referral, call office or Doc Halo, to speak with a Cardiologist or APP to discuss patient and possible treatment options. Please only contact the patient's cardiologist.
Severe Hypertension *Prior to making a referral, call office or Doc Halo, to speak with a Cardiologist or APP to discuss patient and possible treatment options. Please only contact the patient's cardiologist.
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions
 Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS Pediatric Cardiology
 Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Ben Taylor, PhD, PA-C
 Ben Taylor, PhD, PA-C The patient is a 23-year-old white male with a history of polysubstance abuse who was found unresponsive, last seen the day before. Classic signs of systemic hypothermia with prominent
Ben Taylor, PhD, PA-C The patient is a 23-year-old white male with a history of polysubstance abuse who was found unresponsive, last seen the day before. Classic signs of systemic hypothermia with prominent
Common Codes for ICD-10
 Common Codes for ICD-10 Specialty: Cardiology *Always utilize more specific codes first. ABNORMALITIES OF HEART RHYTHM ICD-9-CM Codes: 427.81, 427.89, 785.0, 785.1, 785.3 R00.0 Tachycardia, unspecified
Common Codes for ICD-10 Specialty: Cardiology *Always utilize more specific codes first. ABNORMALITIES OF HEART RHYTHM ICD-9-CM Codes: 427.81, 427.89, 785.0, 785.1, 785.3 R00.0 Tachycardia, unspecified
Heart Valve disease: MR. AS tough patient When to echo, When to refer, What s new
 Heart Valve disease: MR. AS tough patient When to echo, When to refer, What s new B. Sonnenberg UAH Cardiology CME Day 5 May 2015 Disclosures Speaker s or Advisory Boards: none Research grants: none (co-investigator
Heart Valve disease: MR. AS tough patient When to echo, When to refer, What s new B. Sonnenberg UAH Cardiology CME Day 5 May 2015 Disclosures Speaker s or Advisory Boards: none Research grants: none (co-investigator
Atrial Septal Defect Closure. Stephen Brecker Director, Cardiac Catheterisation Labs
 Stephen Brecker Director, Cardiac Catheterisation Labs ADVANCED ANGIOPLASTY Incorporating The Left Main 5 Plus Course Conflicts of Interest The following companies have supported educational courses held
Stephen Brecker Director, Cardiac Catheterisation Labs ADVANCED ANGIOPLASTY Incorporating The Left Main 5 Plus Course Conflicts of Interest The following companies have supported educational courses held
The Blue Baby. Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin
 The Blue Baby Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin Session Structure Definitions and assessment of cyanosis Causes of blue baby Structured approach to assessing
The Blue Baby Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin Session Structure Definitions and assessment of cyanosis Causes of blue baby Structured approach to assessing
How to Recognize a Suspected Cardiac Defect in the Neonate
 Neonatal Nursing Education Brief: How to Recognize a Suspected Cardiac Defect in the Neonate https://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/
Neonatal Nursing Education Brief: How to Recognize a Suspected Cardiac Defect in the Neonate https://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영
 When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
Screening for Critical Congenital Heart Disease
 Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
Physical Exam Part II
 Physical Exam Part II University of Michigan Cardiovascular Center Kim A. Eagle, MD Albion Walter Hewlett Professor Director Physical Exam: Part II Heart Sounds Heart Murmurs HEART SOUNDS S1 MITRAL + TRICUSPID
Physical Exam Part II University of Michigan Cardiovascular Center Kim A. Eagle, MD Albion Walter Hewlett Professor Director Physical Exam: Part II Heart Sounds Heart Murmurs HEART SOUNDS S1 MITRAL + TRICUSPID
Reading Assignment (p1-91 in Outline ) Objectives What s in an ECG?
 Objectives What s in an ECG?") Reading Assignment (p1-91 in Outline ) Objectives What s in an ECG? The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis= 1. Compute the 5 basic
Reading Assignment (p1-91 in Outline ) Objectives What s in an ECG? The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis= 1. Compute the 5 basic
Study methodology for screening candidates to athletes risk
 1. Periodical Evaluations: each 2 years. Study methodology for screening candidates to athletes risk 2. Personal history: Personal history of murmur in childhood; dizziness, syncope, palpitations, intolerance
1. Periodical Evaluations: each 2 years. Study methodology for screening candidates to athletes risk 2. Personal history: Personal history of murmur in childhood; dizziness, syncope, palpitations, intolerance
Presentation, symptoms and signs of heart failure
 3 Presentation, symptoms and signs of heart failure What will I learn? In this section you will learn: Who is at risk of heart failure The symptoms of heart failure The signs of heart failure The importance
3 Presentation, symptoms and signs of heart failure What will I learn? In this section you will learn: Who is at risk of heart failure The symptoms of heart failure The signs of heart failure The importance
Clinical significance of cardiac murmurs: Get the sound and rhythm!
 Clinical significance of cardiac murmurs: Get the sound and rhythm! Prof. dr. Gunther van Loon, DVM, PhD, Ass Member ECVDI, Dip ECEIM Dept. of Large Animal Internal Medicine Ghent University, Belgium Murmurs
Clinical significance of cardiac murmurs: Get the sound and rhythm! Prof. dr. Gunther van Loon, DVM, PhD, Ass Member ECVDI, Dip ECEIM Dept. of Large Animal Internal Medicine Ghent University, Belgium Murmurs
Myocardial Infarction. Reading Assignment (p66-78 in Outline )
") Myocardial Infarction Reading Assignment (p66-78 in Outline ) Objectives 1. Why do ST segments go up or down in ischemia? 2. STEMI locations and culprit vessels 3. Why 15-lead ECGs? 4. What s up with avr?
Myocardial Infarction Reading Assignment (p66-78 in Outline ) Objectives 1. Why do ST segments go up or down in ischemia? 2. STEMI locations and culprit vessels 3. Why 15-lead ECGs? 4. What s up with avr?
Arrhythmic Complications of MI. Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine
 Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
CORONARY ARTERIES HEART
 CARDIAC/ECG MODULE THE HEART CORONARY ARTERIES FIBRILLATING HEART CORONARY ARTERIES HEART PRACTICE RHYTHMS PRACTICE RHYTHMS ELECTRICAL CONDUCTION SA Node (60 100) Primary pacemaker AV Node (40 60) ***Creates
CARDIAC/ECG MODULE THE HEART CORONARY ARTERIES FIBRILLATING HEART CORONARY ARTERIES HEART PRACTICE RHYTHMS PRACTICE RHYTHMS ELECTRICAL CONDUCTION SA Node (60 100) Primary pacemaker AV Node (40 60) ***Creates
ECG S: A CASE-BASED APPROACH December 6,
 ECG S: A CASE-BASED APPROACH December 6, 2018 1 Faculty Disclosure Faculty: Lorne Gula MD, FRCPC Professor, Western University Cardiologist, Hearth Rhythm Specialist Director, Electrophysiology Laboratory,
ECG S: A CASE-BASED APPROACH December 6, 2018 1 Faculty Disclosure Faculty: Lorne Gula MD, FRCPC Professor, Western University Cardiologist, Hearth Rhythm Specialist Director, Electrophysiology Laboratory,
Pre-Participation Athletic Cardiac Screening
 Pre-Participation Athletic Cardiac Screening Kimberly A Krabill, MD Pediatric and Fetal Cardiologist Northwest Congenital Heart Care, Division of MedNax Cardiology Update for Primary Care Symposium July
Pre-Participation Athletic Cardiac Screening Kimberly A Krabill, MD Pediatric and Fetal Cardiologist Northwest Congenital Heart Care, Division of MedNax Cardiology Update for Primary Care Symposium July
The Heart of the Matter
 The Heart of the Matter Is the Heart the Matter? --Chest pain in the Pediatric Patient-- 19th Interregional Symposium November 2, 2018 Session A, 9:35-10:50 am John-Charles Loo, MD Pediatric Cardiology,
The Heart of the Matter Is the Heart the Matter? --Chest pain in the Pediatric Patient-- 19th Interregional Symposium November 2, 2018 Session A, 9:35-10:50 am John-Charles Loo, MD Pediatric Cardiology,
PEDIATRIC HEART MURMURS. Manish Bansal, MD Clinical Assistant Professor Division of Pediatric Cardiology University of Iowa
 PEDIATRIC HEART MURMURS Manish Bansal, MD Clinical Assistant Professor Division of Pediatric Cardiology University of Iowa Murmur murmur. (n.d.). Dictionary.com Unabridged. Retrieved March 9, 2018 from
PEDIATRIC HEART MURMURS Manish Bansal, MD Clinical Assistant Professor Division of Pediatric Cardiology University of Iowa Murmur murmur. (n.d.). Dictionary.com Unabridged. Retrieved March 9, 2018 from
Masqueraders of STEMI
 Masqueraders of STEMI Steven M. Costa, M.D. Assistant Professor Department of Medicine Division of Cardiology Scott & White Memorial Hospital and Clinic Texas A&M University Health Science Center Disclosures
Masqueraders of STEMI Steven M. Costa, M.D. Assistant Professor Department of Medicine Division of Cardiology Scott & White Memorial Hospital and Clinic Texas A&M University Health Science Center Disclosures
the Young Athlete David B. Gremmels, MD Pediatric Cardiologist Children s Hospitals and Clinics of MN
 Cardiovascular Risk Assessment in the Young Athlete David B. Gremmels, MD Pediatric Cardiologist Children s Heart Clinic Children s Hospitals and Clinics of MN No disclosure or financial relationships
Cardiovascular Risk Assessment in the Young Athlete David B. Gremmels, MD Pediatric Cardiologist Children s Heart Clinic Children s Hospitals and Clinics of MN No disclosure or financial relationships
10 ECGs No Practitioner Can Afford to Miss. Objectives
 10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
HISTORY. Question: What category of heart disease is suggested by this history? CHIEF COMPLAINT: Heart murmur present since early infancy.
 HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
CMS Limitations Guide - Radiology Services
 CMS Limitations Guide - Radiology Services Starting October 1, 2015, CMS will update their existing medical necessity limitations on tests and procedures to correspond to ICD-10 codes. This limitations
CMS Limitations Guide - Radiology Services Starting October 1, 2015, CMS will update their existing medical necessity limitations on tests and procedures to correspond to ICD-10 codes. This limitations
Slide 1. Slide 2. Slide 3. Sudden Cardiac Death In Athletes. Epidemiology. Epidemiology. Shaun McMurtry, MD Primary Care Sports Medicine
 Slide 1 Sudden Cardiac Death In Athletes Shaun McMurtry, MD Primary Care Sports Medicine Slide 2 Epidemiology College and Professional Athletes 500,000 participants each year Competitive Athletics Estimated
Slide 1 Sudden Cardiac Death In Athletes Shaun McMurtry, MD Primary Care Sports Medicine Slide 2 Epidemiology College and Professional Athletes 500,000 participants each year Competitive Athletics Estimated
Cases in Adult Congenital Heart Disease
 Cases in Adult Congenital Heart Disease Sabrina Phillips, MD FACC FASE Associate Professor of Medicine The University of Oklahoma Health Sciences Center No Disclosures I Have Palpitations 18 Year old Man
Cases in Adult Congenital Heart Disease Sabrina Phillips, MD FACC FASE Associate Professor of Medicine The University of Oklahoma Health Sciences Center No Disclosures I Have Palpitations 18 Year old Man
: Provide cardiovascular preventive counseling to parents and patients with specific cardiac diseases about:
 Children s Hospital & Research Center Oakland Cardiology Primary Goals for this Rotation 5.13 GOAL: Prevention, Counseling and Screening (Cardiovascular). Understand the role of the pediatrician in preventing
Children s Hospital & Research Center Oakland Cardiology Primary Goals for this Rotation 5.13 GOAL: Prevention, Counseling and Screening (Cardiovascular). Understand the role of the pediatrician in preventing
Congestive Heart Failure or Heart Failure
 Congestive Heart Failure or Heart Failure Dr Hitesh Patel Ascot Cardiology Group Heart Failure Workshop April, 2014 Question One What is the difference between congestive heart failure and heart failure?
Congestive Heart Failure or Heart Failure Dr Hitesh Patel Ascot Cardiology Group Heart Failure Workshop April, 2014 Question One What is the difference between congestive heart failure and heart failure?
Transcatheter closure of right coronary artery fistula to the right ventricle
 Case Report Transcatheter closure of right coronary artery fistula to the right ventricle Abstract Coronary artery fistula (CAF) is an uncommon anomaly usually congenital but can be acquired. Although,
Case Report Transcatheter closure of right coronary artery fistula to the right ventricle Abstract Coronary artery fistula (CAF) is an uncommon anomaly usually congenital but can be acquired. Although,
Skin supplied by T1-4 (medial upper arm and neck) T5-9- epigastrium Visceral afferents from skin and heart are the same dorsal root ganglio
 T5-9- epigastrium Visceral afferents from skin and heart are the same dorsal root ganglio") Cardio 2 ECG... 3 Cardiac Remodelling... 11 Valvular Diseases... 13 Hypertension... 18 Aortic Coarctation... 24 Erythropoiesis... 27 Haemostasis... 30 Anaemia... 36 Atherosclerosis... 44 Angina... 48 Myocardial
Cardio 2 ECG... 3 Cardiac Remodelling... 11 Valvular Diseases... 13 Hypertension... 18 Aortic Coarctation... 24 Erythropoiesis... 27 Haemostasis... 30 Anaemia... 36 Atherosclerosis... 44 Angina... 48 Myocardial
Central Sleep Apnea Problem Based Learning Module
 Central Sleep Apnea Problem Based Learning Module Vidya Krishnan, and Sutapa Mukherjee for the Sleep Education for Pulmonary Fellows and Practitioners, SRN ATS Committee 2015 Case Section I A 75 year old
Central Sleep Apnea Problem Based Learning Module Vidya Krishnan, and Sutapa Mukherjee for the Sleep Education for Pulmonary Fellows and Practitioners, SRN ATS Committee 2015 Case Section I A 75 year old
Case # 1. Page: 8. DUKE: Adams
 Case # 1 Page: 8 1. The cardiac output in this patient is reduced because of: O a) tamponade physiology O b) restrictive physiology O c) coronary artery disease O d) left bundle branch block Page: 8 1.
Case # 1 Page: 8 1. The cardiac output in this patient is reduced because of: O a) tamponade physiology O b) restrictive physiology O c) coronary artery disease O d) left bundle branch block Page: 8 1.
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT
 ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
Hemodynamic Monitoring
 Perform Procedure And Interpret Results Hemodynamic Monitoring Tracheal Tube Cuff Pressure Dean R. Hess PhD RRT FAARC Hemodynamic Monitoring Cardiac Rate and Rhythm Arterial Blood Pressure Central Venous
Perform Procedure And Interpret Results Hemodynamic Monitoring Tracheal Tube Cuff Pressure Dean R. Hess PhD RRT FAARC Hemodynamic Monitoring Cardiac Rate and Rhythm Arterial Blood Pressure Central Venous
Pulmonary-Vascular Disease. Howard J. Sachs, MD.
 Pulmonary-Vascular Disease Howard J. Sachs, MD www.12daysinmarch.com Dyspnea Cardiac Pulmonary CAD Pump Failure Chest Wall Airways Valve Disease Pericardial Disease Alveoli Interstitium Rhythm Disturbance
Pulmonary-Vascular Disease Howard J. Sachs, MD www.12daysinmarch.com Dyspnea Cardiac Pulmonary CAD Pump Failure Chest Wall Airways Valve Disease Pericardial Disease Alveoli Interstitium Rhythm Disturbance
Heart and Soul Evaluation of the Fetal Heart
 Heart and Soul Evaluation of the Fetal Heart Ivana M. Vettraino, M.D., M.B.A. Clinical Associate Professor, Michigan State University College of Human Medicine Objectives Review the embryology of the formation
Heart and Soul Evaluation of the Fetal Heart Ivana M. Vettraino, M.D., M.B.A. Clinical Associate Professor, Michigan State University College of Human Medicine Objectives Review the embryology of the formation
DAY1_CARDIOVASCULAR PRACTICE QUESTIONS
 DAY1_CARDIOVASCULAR PRACTICE QUESTIONS 1 P age 1. A 59-year-old male is admitted complaining of chest pain and dyspnea. ST elevation and T-wave inversion were seen on the ECG in V2, V3, and V4. IV thrombolytic
DAY1_CARDIOVASCULAR PRACTICE QUESTIONS 1 P age 1. A 59-year-old male is admitted complaining of chest pain and dyspnea. ST elevation and T-wave inversion were seen on the ECG in V2, V3, and V4. IV thrombolytic
12 LEAD EKG & CXR INTERPRETATION.
 12 LEAD EKG & CXR INTERPRETATION www.cherylherrmann.com cherrmann@frontier.com Audio Product Recording discount for participants $60 Nonparticipants = $190 o Get CEs and manual https://catalog.vyne.com
12 LEAD EKG & CXR INTERPRETATION www.cherylherrmann.com cherrmann@frontier.com Audio Product Recording discount for participants $60 Nonparticipants = $190 o Get CEs and manual https://catalog.vyne.com
HISTORY. Question: What type of heart disease is suggested by this history? CHIEF COMPLAINT: Decreasing exercise tolerance.
 HISTORY 15-year-old male. CHIEF COMPLAINT: Decreasing exercise tolerance. PRESENT ILLNESS: A heart murmur was noted in childhood, but subsequent medical care was sporadic. Easy fatigability and slight
HISTORY 15-year-old male. CHIEF COMPLAINT: Decreasing exercise tolerance. PRESENT ILLNESS: A heart murmur was noted in childhood, but subsequent medical care was sporadic. Easy fatigability and slight