Maternal Fetal Medicine 6/14/2013
|
|
|
- Gordon Reginald Melton
- 6 years ago
- Views:
Transcription
1 Todd Lovgren, MD Maternal Fetal Medicine 6/14/2013 Obstetric Hemorrhage: The First Thing You Should Think About at Every Delivery
2 Disclosures I have no financial disclosures. I picked the Shockers to go out in the Sweet Sixteen.
3 Objectives Identify common causes of postpartum hemorrhage Describe medical and surgical management of obstetric hemorrhage Review management of severe obstetric hemorrhage and resuscitative management.
4 Background
5 Incidence of Hemorrahge Hemorrhage- 4-6%* SVD >500ml Cesarean >1000ml Life threatening obstetric hemorrhage 1:1000** Second most common cause of maternal mortality in the US 0.9/100, *** *ACOG Practice Bulletin 76 **Drife J. BJOG (1997) 104:275 7 ***CDC; NVSR, V 58:19, May 2010, tables 33 and 34
6 Preventable State wide review in North Carolina 90% of Maternal Deaths Related to Hemorrhage considered PREVENTABLE Areas needed to improve? Berg CJ, Obstet Gynecol 2005
7 Causes of Maternal Death Inadequate resources and personnel Failure to prepare- IV access Delay in recognition of hemorrhage Delay in treatment Treatment failure
8 Physiologic Changes 50% increase in plasma volume Can be up to 100% in multiple gestations 30% increase in RBC mass Anemia of pregnancy. Mean Hgb 11g/dL Average blood volume ml
9 Physiologic Changes Marked increase in Factors VII, VIII, X, XII and XIII Acquired Protein C resistance Increased thrombin generation Increased fibrinogen Decrease in Factor XI Decreased Protein S activity
10 Physiologic Changes
11 Physiologic Changes Result of all these changes are prothrombotic state Decreased INR Decreased fibrinolytic i potential ti Due to increase PAI 1 and 2
12 Potential 10-15% of CO to gravid Uterus ml/min Up to 1L/min in multiple gestation Primary mechanism for hemostasis post delivery is mechanical Blood vessels travel through interwoven muscle fibers, involution results in cessation of fblood dflow.
13 Consequences of PPH Obstetric and non-obstetric rabbits Hemorrhagic shock and resuscitation Obstetric rabbits (within 2 hours postpartum) Shorter survival More severe systemic inflammatory response Increased TNF alpha, decreased IL-10 More severe lung injury Alveolar and interstitial fluid accumulation Increased markers for lung injury (myeloperoxidase, tumor necrosis factor, etc.) Sheng C, Crit Care Med 2012; (40)


14 Consequences of OB Hemorrhage ICU patients admitted with PPH and hypovolemic shock Incidence of myocardial ischemia i = 50% Troponin and tissue oxygen delivery Risk factors include: Hgb <6g/dL Systolic BP <88 mmhg Diastolic BP <50 mmhg HR >115 bpm Use of catecholamines Karpati PC. Anesthesiology 2004; (100):30 36
15 Always Read Your Dictation (NOTHING has been altered) The patient is a 29 y/o female status post NSVD low-transverse 6 week postpartum visit. Weight today is questionable as patient does not agree with the scale. Documentation of phone message left for patient after x-ray for arm pain Hooray! No fracture.
16 Etiology
17 Etiology Atony A Atony Atony Abruptio placentae Laceration (cervical/vaginal/perineal) Placenta accreta Retained placenta Uterine rupture Hematoma







18 Etiology


19 Etiology
20 Etiology Other AFE Laceration Hematoma Operative delivery, pudendal or uterine artery injury Uterine Rupture Uterine Inversion
21 Etiology of Maternal Death Hemorrhage is 30% of all maternal mortality Abruption 19% Uterine Rupture 19% Atony 15% Coagulopathy 14% Previa 7% Accreta 6% Chichaki et al, 1999




22




23
24




25








26
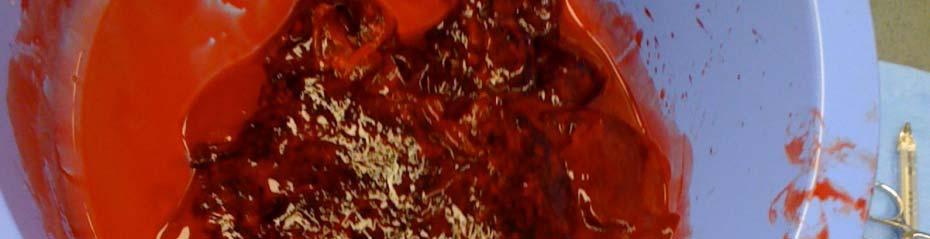
27 Estimated Blood Loss A 24 y/o patient only bled onto these 4 laparotomy sponges at the time of cesarean. What is her estimated blood loss?


28 Emphasis on Estimated Ability to estimate blood loss only exceeded by our ability to estimate fetal weight. Underestimate t by 30-50% Error persists regardless of volume.* =250ml Dildy Obstet Gynecol :601 6.
29 Code White/Code Red/Action Plan/Hemorrhage Protocol Activate hemorrhage protocol Notify appropriate p services Anesthesia NICU/Pediatrician if still pregnant Blood bank Laboratory (37 types of Stat labs) Main OR Supplies/Instruments Pharmacy Back-up/Surgical assistant House supervisor Interventional Radiology




30 18 Week impending atony
31 Management of Atony Bimanual massage Drain the bladder Uterotonics Oxytocin Hemabate (up to 4 doses 15 min apart) Not in asthma. Low on priority list but give lomotil once patient is stable. Methergine (up to 4 doses min apart) Not in hypertension. Rectal cytotec ( mcg) y ( g) 600 mcg Buccal This doesn t get absorbed for minutes. Good for maintaining uterine tone but not ideal if there is ongoing bleeding.
32 Management of Atony Rule out other causes Physical exam should be the first step! Thorough h examination of vagina, cervix and bimanual massage. Examination of placenta Ultrasound Manual exploration Tamponade Balloon


33 Tamponade Balloon Foley first! +/- Curettage- Move to the OR if planning curettage. Manual placement of balloon under ultrasound guidance Inflation of balloon- 500ml capacity Hold base in place with ring forceps/hand. Begin packing moistened Kerlex with other hand while partner/assistant inflates balloon. Continue to monitor balloon with Ultrasound Frequently migrates into vagina after a vaginal delivery. Remove in 24 hours. Best for lower uterine segment atony
34 Impending Surgical Intervention ti
35 Transverse


36 Surgical Management Curettage Uterine compression suture B-Lynch Cho technique U-Suture O leary- uterine artery ligation Place below level of bleeding. Internal iliac artery ligation Often impractical/difficult lt to perform in face of hemorrhage. h *Cho,Obstet Gynecol, :1,
37 Hysterectomy Subtotal vs Total Hysterectomy Subtotal % Total % Bladder Injury Reoperation GI complications Transfusion LoS Perioperative death Wright, Obstet Gynecol, ;6,
38 Miscellaneous Subtotal unless history of carcinoma/severe dysplasia or inordinately stable. Widely spaced skin staples No suture, no glue. If coagulopathic Subfascial pelvic drain +/- Subcutaneous drain, I place in morbidly obese pt.
39 Interventional Radiology Hemodynamically stable patient Placental bed +/- uterine artery +/- internal iliac artery. Most useful for continued/postoperative bleeding or hematomas. Risks Procedural complications, ovarian embolization, fistula formation, bowel injury.
40 Always Read Your Dictation DISCHARGE DIAGNOSIS: 1. Term intrauterine t i pregnancy. 2. Precipitous delivery. 3. Postpartum hemorrhage. 4. History of sexual thoughts.
41 Resuscitation Vital signs Lethal Triad Fluids and Blood products
42 VS Changes with PPH EBL (ml) % Blood Volume Lost Physiologic Changes Hear t Rate (bpm) Blood Pressure (mmhg) Urine Output (ml) Mental Status circulating catecholamines; fluid shifts compensate for blood loss <100 NC NC NC circulating catecholamines; peripheral vasoconstriction NC or pulse pressure Slight Anxiety Hypoperfusion, SBP ; Anxiety, 2000 moderate shock pulse (5-15 confusion pressure ml/hr) >2000 >40 Extreme hypoperfusion; severe >140 <80 mmhg; Possible shock complete anuria Lethargy; loss of consciousness Devine PC. Semin Perinatol 2009; 33: 76-81
43 Beware the Cliff While helpful.. Due to changes in volume, multiple compensatory mechanisms and rapid blood loss, patients tend to fall off the cliff rather than progress stepwise through stages of hypovolemic shock.



44 Lethal Triad Coagulopathy Acidosis Hypothermia
45 Goals of Resuscitation 1. Maintain perfusion 2. Maintain oxygenation 3. Maintain body temperature 4. Prevent or treat coagulopathy
46 Laboratory Evaluation of Postpartum Hemorrhage Patient Complete blood count Protime/Prothrombin Time and INR Fibrinogen Comprehensive metabolic panel Crossmatch blood or call for trauma blood
47 Resuscitation Management Two peripheral IV s Arterial line Central line depending on cause or if maternal condition warrants AFE, sepsis, shock, maternal cardiac or pulmonary disease Level 1 transfuser/infuser Warms fluid/blood administered. Bear hugger Sequential compression devices
48 Fluid Resuscitation Lactated ringers vs Normal Saline vs Albumin No difference in outcomes based on trauma literature Transfusion of large volumes can lead to dilutional coagulopathy. Cochrane Database 2007 Crystalloid - 3:1 resuscitation Hetastarch (Hextend/Hespan)- 1:1 resuscitation Transfusion of >1000ml (20ml/kg) independently associated with coagulopathy. Stump et al 1985 I prefer to avoid in OB hemorrhage b/c of contribution to coagulopathy and rapid availability of blood products.
49 Packed Red Blood Cells ml Should raise Hgb 1 g / Hct 3% Citrate preservative Trauma Blood Typically y will at least be type specific Type and hold or screen should be in BB Will get crossmatched after it has been sent!
50 Fresh frozen plasma (FFP) 200 ml mg Fibrinogen Deficient in Factor V and VIII First line for coagulopathy (INR>1.7) +/- hypofibrinogenemia Cryoprecipitate ml mg Fibrinogen Rich in vwf, Factor VIII and XIII Useful for isolated hypofibrinogenemia, volume overload or volume sensitive cardio/pulmonary disease. Not appropriate for vwf or Factor VIII (Hemophilia A) deficiency
51 Apheresis pack equivalent to older 6 pack platelets Single donor Lower risk of infection Increase platelets 25-50K Indication Bleeding with count <50 K or within 24 hours surgery Post op/delivery with no bleeding with count <25 K Spontaneous bleeding occurs at <10 K
52 PPH complicated by coagulopathy 1877 patients with PPH Almost universal (97%) transfusion >2500ml EBL Only coagulopathic patients required massive transfusion 43% risk of coagulopathy in patients with EBL >3000ml
53 Post Hemorrhage Management Laboratory values will frequently fluctuate Trends are important Vital signs are critical Maintain uterine tone Magnesium should be continued in severe preeclamptic patients. Consider ICU admission if there is significant hemorrhage (2500+ ml EBL) or there are comorbiditieschorioamnionitis, extensive surgery, preeclampsia, general anesthesia, coagulopathy.
54 Pearls Trust your clinical judgement. If she s behaving coagulopathic start transfusing. Labs should guide additional transfusion not the initiation of transfusion. Ampule of Calcium for every 4-6 units prbc Critical to coagulation cascade and platelet function Blood product preservative (citrate) binds free calcium in vivo. Type and cross patients with positive antibody screen on admission to L and D for delivery. Usually 2 units. If they have other risk factors- 4 units prbc
55 Pearls Detection of hemolysis Haptoglobin UA dip (lysed hemoglobin) Peripheral smear LDH is frequently used but acute liver injury can also elevate LDH (Preeclampsia, AFLP, HELLP, etc.) Red top Tape to the wall or put in the Anesthesiologist s pocket Should clot in 6 minutes and should not lyse for 30 minutes. Preeclamptics don t tolerate blood loss p Vasoconstricted and volume depleted so they are likely to decompensate at lower blood loss.
56 Pearls Restore euvolemia and tissue perfusion. Young healthy patients can maintain normal heart rates and BP s when it s not appropriate. Remember the Lethal Triad Tissue hypoxia secondary to loss of oxygen carrying capacity and vasoconstriction will worsen acidosis worsen coagulopathy further bleeding ensues We typically have young healthy patients who do not decompensate slowly but SUDDENLY.
57 Pearls Re-dose antibiotics Lab results tell you how she was doing 30 minutes ago. Fibrinogen is elevated in pregnancy Low normal represents DEPLETION/CONSUMPTION 150 is not normal More blood products do not fix the problem. If you reconstitute blood products in equal parts the result is anemic, thrombocytopenic and coagulopathic.
58 Always Read Your Dictation EBL: 1000ml Fluids: 28000ml crystalloid Preop Diagnosis: Arrest of dilation. Feels intolerant of labor Patient pushed me to do vacuum. It actually worked with 3 pulls! (I did not add the exclamation point)
59 Conclusion Think about how you are going to manage each patient before they have a complication. Challenge yourself as you work through it in Challenge yourself as you work through it in your head- always try to have a next step in mind
60 Advice for those leaving the nest Get to know your new institution How long do labs take? What about blood products? How easily can nursing staff obtain medications? What instruments do they have immediately available in or near the OR? Where do they get additional instruments if you need them? Does L&D have dedicated anesthesia? How quickly can you or the anesthesiologist get help?
61 Thank You
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE
 MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
Unrestricted. Dr ppooransari fellowship of perenatalogy
 Unrestricted Dr ppooransari fellowship of perenatalogy Assessment of severity of hemorrhage Significant drops in blood pressure are generally not manifested until substantial bleeding has occurred, and
Unrestricted Dr ppooransari fellowship of perenatalogy Assessment of severity of hemorrhage Significant drops in blood pressure are generally not manifested until substantial bleeding has occurred, and
M-AFRAKHTEH. MD OCT.2017 SHOHADA HOSPITAL TAJRISH
 Unrestricted M-AFRAKHTEH. MD OCT.2017 SHOHADA HOSPITAL TAJRISH Patients at imminent risk of exsanguination Manual aortic compression Resuscitative endovascular balloon occlusion of the aorta Uterine tourniquet
Unrestricted M-AFRAKHTEH. MD OCT.2017 SHOHADA HOSPITAL TAJRISH Patients at imminent risk of exsanguination Manual aortic compression Resuscitative endovascular balloon occlusion of the aorta Uterine tourniquet
the bleeding won t stop? Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital
 Royal Alexandra Hospital") What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
Transfusion Requirements and Management in Trauma RACHEL JACK
 Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Massive Transfusion. MPQC Spring Summit April 29, Roger Belizaire MD PhD
 Massive Transfusion MPQC Spring Summit April 29, 2015 Roger Belizaire MD PhD Take home points 1. Blood is always available. Requests for massive transfusion or emergency release typically only require
Massive Transfusion MPQC Spring Summit April 29, 2015 Roger Belizaire MD PhD Take home points 1. Blood is always available. Requests for massive transfusion or emergency release typically only require
Massive transfusion: Recent advances, guidelines & strategies. Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad
 Massive transfusion: Recent advances, guidelines & strategies Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad Massive Hemorrhage Introduction Hemorrhage is a major cause
Massive transfusion: Recent advances, guidelines & strategies Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad Massive Hemorrhage Introduction Hemorrhage is a major cause
Damage Control in Abdominal and Pelvic Injuries
 Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Use of Condom tamponade to manage Massive Obstetric Hemorrhage at a tertiary centre in Rajasthan.
 Use of Condom tamponade to manage Massive Obstetric Hemorrhage at a tertiary centre in Rajasthan. INTRODUCTION: Conventionally PPH has been defined as blood loss of more than 500ml following vaginal delivery
Use of Condom tamponade to manage Massive Obstetric Hemorrhage at a tertiary centre in Rajasthan. INTRODUCTION: Conventionally PPH has been defined as blood loss of more than 500ml following vaginal delivery
TRANSFUSIONS FIRST, DO NO HARM
 TRANSFUSIONS FIRST, DO NO HARM BECAUSE BLOOD CAN KILL 7 TRALI DEATHS SINCE 2002 WMC 5 women BECAUSE In OB you are transfusing 2 instead of 1 BECAUSE BLOOD IS A LIQUID TRANSPLANT RISKS versus BENEFITS versus
TRANSFUSIONS FIRST, DO NO HARM BECAUSE BLOOD CAN KILL 7 TRALI DEATHS SINCE 2002 WMC 5 women BECAUSE In OB you are transfusing 2 instead of 1 BECAUSE BLOOD IS A LIQUID TRANSPLANT RISKS versus BENEFITS versus
2/2/2011. Blood Components and Transfusions. Why Blood Transfusion?
 Blood Components and Transfusions Describe blood components Identify nursing responsibilities r/t blood transfusion Discuss factors r/t blood transfusion including blood typing, Rh factor, and cross matching
Blood Components and Transfusions Describe blood components Identify nursing responsibilities r/t blood transfusion Discuss factors r/t blood transfusion including blood typing, Rh factor, and cross matching
Effective Date: Approved by: Laboratory Director, Jerry Barker (electronic signature)
") 1 of 5 Policy #: 702 (PHL-702-05) Effective Date: 9/30/2004 Reviewed Date: 8/1/2016 Subject: TRANSFUSION GUIDELINES Approved by: Laboratory Director, Jerry Barker (electronic signature) Approved by: Laboratory
1 of 5 Policy #: 702 (PHL-702-05) Effective Date: 9/30/2004 Reviewed Date: 8/1/2016 Subject: TRANSFUSION GUIDELINES Approved by: Laboratory Director, Jerry Barker (electronic signature) Approved by: Laboratory
Damage Control Resuscitation. VGH Trauma Rounds 2018 Harvey Hawes
 Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
Policy REVISED: 6/30/2016 3:30 PM. Applies To: ObGyn Responsible Department: ObGyn Revised: June 30, 2016
 Title: Antihypertensive Treatment for Severe Hypertension During Pregnancy Applies To: ObGyn Responsible Department: ObGyn Revised: June 30, 2016 Policy POLICY STATEMENT: Pregnant or postpartum patients
Title: Antihypertensive Treatment for Severe Hypertension During Pregnancy Applies To: ObGyn Responsible Department: ObGyn Revised: June 30, 2016 Policy POLICY STATEMENT: Pregnant or postpartum patients
Maternal Collapse Guideline
 Maternal Collapse Guideline Guideline Number: 664 Supersedes: Classification Clinical Version No: Date of EqIA: Approved by: Date Approved: Date made active: Review Date: 1 Obstetric Written Documentation
Maternal Collapse Guideline Guideline Number: 664 Supersedes: Classification Clinical Version No: Date of EqIA: Approved by: Date Approved: Date made active: Review Date: 1 Obstetric Written Documentation
Transfusion 2004: Current Practice Standards. Kay Elliott, MT (ASCP) SBB SWMC Transfusion Service
 SBB SWMC Transfusion Service") Transfusion 2004: Current Practice Standards Kay Elliott, MT (ASCP) SBB SWMC Transfusion Service Massive Transfusion Protocol (MTP) When should it be activated? Massive bleeding i.e. loss of one blood
Transfusion 2004: Current Practice Standards Kay Elliott, MT (ASCP) SBB SWMC Transfusion Service Massive Transfusion Protocol (MTP) When should it be activated? Massive bleeding i.e. loss of one blood
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
LifeBridge Health Transfusion Service Sinai Hospital of Baltimore Northwest Hospital Center BQA Transfusion Criteria Version#2 POLICY NO.
 LifeBridge Health Transfusion Service Sinai Hospital of Baltimore Northwest Hospital Center BQA 1011.02 Transfusion Criteria Version#2 Department POLICY NO. PAGE NO. Blood Bank Quality Assurance Manual
LifeBridge Health Transfusion Service Sinai Hospital of Baltimore Northwest Hospital Center BQA 1011.02 Transfusion Criteria Version#2 Department POLICY NO. PAGE NO. Blood Bank Quality Assurance Manual
RENAL & HEMATOLOGY EMERGENCIES JEFF SIMONS B.S. F-PC
 RENAL & HEMATOLOGY EMERGENCIES JEFF SIMONS B.S. F-PC GOALS Overview of renal system anatomy / physiology Discuss common medical / trauma renal issues Identify associated assessment keys GOALS Introduction
RENAL & HEMATOLOGY EMERGENCIES JEFF SIMONS B.S. F-PC GOALS Overview of renal system anatomy / physiology Discuss common medical / trauma renal issues Identify associated assessment keys GOALS Introduction
GUIDANCE DOCUMENT FOR MASSIVE HEMORRHAGE MANAGEMENT IN ADULTS
 GUIDANCE DOCUMENT FOR MASSIVE HEMORRHAGE MANAGEMENT IN ADULTS 1.0 Definitions & Acronyms 1.1 Massive Hemorrhage Event (MHE): Transfusion of a volume of blood components equivalent to a patient s estimated
GUIDANCE DOCUMENT FOR MASSIVE HEMORRHAGE MANAGEMENT IN ADULTS 1.0 Definitions & Acronyms 1.1 Massive Hemorrhage Event (MHE): Transfusion of a volume of blood components equivalent to a patient s estimated
My Bloody Talk. Dr Ben Turner MBBS, FANZCA, FCICM The Royal Children s Hospital, Melbourne
 My Bloody Talk Dr Ben Turner MBBS, FANZCA, FCICM The Royal Children s Hospital, Melbourne Disclosures No conflicts of interest Interest in conflict Blood transfusion Massive transfusion definitions Transfusion
My Bloody Talk Dr Ben Turner MBBS, FANZCA, FCICM The Royal Children s Hospital, Melbourne Disclosures No conflicts of interest Interest in conflict Blood transfusion Massive transfusion definitions Transfusion
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC
, RN, RNC-NIC") Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
Interventional Options in Management of Placenta Abnormalities
 Interventional Options in Management of Placenta Abnormalities Caroline Clausen and Lars Lönn Department of Cardiovascular Radiology Faculty of Health Sciences Copenhagen University Rigshospitalet, Denmark.
Interventional Options in Management of Placenta Abnormalities Caroline Clausen and Lars Lönn Department of Cardiovascular Radiology Faculty of Health Sciences Copenhagen University Rigshospitalet, Denmark.
Mercy San Juan Medical Center. Preeclampsia and Other Hypertensive Disorders of Pregnancy
 SUBJECT: Preeclampsia and Other Hypertensive Disorders of Pregnancy DEPARTMENTS: FBC, Emergency Department PURPOSE: To outline the nursing management of inpatients who have preeclampsia or other hypertensive
SUBJECT: Preeclampsia and Other Hypertensive Disorders of Pregnancy DEPARTMENTS: FBC, Emergency Department PURPOSE: To outline the nursing management of inpatients who have preeclampsia or other hypertensive
Management of the Trauma Patient. Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015
 Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
23/10/2011. Case One: Mrs. B. Mrs. B., 36 year old, 30 weeks pregnant, 2 nd baby Blood type A negative Belted driver of minivan, struck a parked car
 GETTING IT BLOODY RIGHT: CHOOSING THE BEST PRODUCT Kathleen Eckert, ART, Transfusion Safety Officer, LHSC Brenda Morgan, RN BScN MSc, CNS, Critical Care, Victoria Hospital, LHSC http://www.transfusionontario.org/public-en/public.php
GETTING IT BLOODY RIGHT: CHOOSING THE BEST PRODUCT Kathleen Eckert, ART, Transfusion Safety Officer, LHSC Brenda Morgan, RN BScN MSc, CNS, Critical Care, Victoria Hospital, LHSC http://www.transfusionontario.org/public-en/public.php
Shock is defined as a state of cellular and tissue hypoxia due to : reduced oxygen delivery and/or increased oxygen consumption or inadequate oxygen
 Shock is defined as a state of cellular and tissue hypoxia due to : reduced oxygen delivery and/or increased oxygen consumption or inadequate oxygen utilization The effects of shock are initially reversible
Shock is defined as a state of cellular and tissue hypoxia due to : reduced oxygen delivery and/or increased oxygen consumption or inadequate oxygen utilization The effects of shock are initially reversible
Blood Transfusion Guidelines in Clinical Practice
 Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
JMSCR Vol 05 Issue 07 Page July 2017
 www.jmscr.igmpublication.org Impact Factor 5.84 Index Copernicus Value: 83.27 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v5i7.181 Evaluating Foleys Balloon Catheter Tamponade
www.jmscr.igmpublication.org Impact Factor 5.84 Index Copernicus Value: 83.27 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v5i7.181 Evaluating Foleys Balloon Catheter Tamponade
Transfusion Pitfalls. Objectives. Packed Red Blood Cells. TRICC trial (subgroups): Is transfusion always good? Components
: Is transfusion always good? Components") Objectives Transfusion Pitfalls Gregory W. Hendey, MD, FACEP Professor and Chief UCSF Fresno, Emergency Medicine To list risks and benefits of various blood products To discuss controversy over liberal
Objectives Transfusion Pitfalls Gregory W. Hendey, MD, FACEP Professor and Chief UCSF Fresno, Emergency Medicine To list risks and benefits of various blood products To discuss controversy over liberal
Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors. THOR Collaboration
 Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors THOR Collaboration Agenda What is Remote Damage Control Resuscitation? Putting RDCR into Practice Control Hemorrhage
Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors THOR Collaboration Agenda What is Remote Damage Control Resuscitation? Putting RDCR into Practice Control Hemorrhage
Bleeding, Coagulopathy, and Thrombosis in the Injured Patient
 Bleeding, Coagulopathy, and Thrombosis in the Injured Patient June 7, 2008 Kristan Staudenmayer, MD Trauma Fellow UCSF/SFGH Trauma deaths Sauaia A, et al. J Trauma. Feb 1995;38(2):185 Coagulopathy is Multi-factorial
Bleeding, Coagulopathy, and Thrombosis in the Injured Patient June 7, 2008 Kristan Staudenmayer, MD Trauma Fellow UCSF/SFGH Trauma deaths Sauaia A, et al. J Trauma. Feb 1995;38(2):185 Coagulopathy is Multi-factorial
Presented by: Indah Dwi Pratiwi
 Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Example CLINICAL GUIDELINES for Postpartum IUD insertion
 Example CLINICAL GUIDELINES for Postpartum IUD insertion Postpartum Intrauterine Device Insertion 1.0 Indications: 1.1 Insertion of an intrauterine device (IUD) for long-acting reversible contraception
Example CLINICAL GUIDELINES for Postpartum IUD insertion Postpartum Intrauterine Device Insertion 1.0 Indications: 1.1 Insertion of an intrauterine device (IUD) for long-acting reversible contraception
-Cardiogenic: shock state resulting from impairment or failure of myocardium
 Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Financial Disclosure. Objectives 9/24/2018
 Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Case Scenario 3: Shock and Sepsis
 Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Successful extracorporeal cardiopulmonary resuscitation in a postpartum patient with amniotic fluid embolism
 Case Report Successful extracorporeal cardiopulmonary resuscitation in a postpartum patient with amniotic fluid embolism Gil Myeong Seong 1, Su Wan Kim 2, Hye Sim Kang 3, Hyun Wook Kang 4 1 Department
Case Report Successful extracorporeal cardiopulmonary resuscitation in a postpartum patient with amniotic fluid embolism Gil Myeong Seong 1, Su Wan Kim 2, Hye Sim Kang 3, Hyun Wook Kang 4 1 Department
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Blood Components & Indications for Transfusion. Neda Kalhor
 Blood Components & Indications for Transfusion Neda Kalhor Blood products Cellular Components: Red blood cells - Leukocyte-reduced RBCs - Washed RBCs - Irradiated RBCs Platelets - Random-donor platelets
Blood Components & Indications for Transfusion Neda Kalhor Blood products Cellular Components: Red blood cells - Leukocyte-reduced RBCs - Washed RBCs - Irradiated RBCs Platelets - Random-donor platelets
Learning Objectives: At the end of this exercise, the student will be able to:
 Applications in Transfusion Medicine- A CBL Exercise- Student Guide 1 Title: Applications in Transfusion Medicine A CBL Exercise Purpose: At the conclusion of this exercise, students will be able to apply
Applications in Transfusion Medicine- A CBL Exercise- Student Guide 1 Title: Applications in Transfusion Medicine A CBL Exercise Purpose: At the conclusion of this exercise, students will be able to apply
RESUSCITATION IN TRAUMA. Important things I have learnt
 RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
EMSS17: Bleeding patients course material
 EMSS17: Bleeding patients course material Introduction During the bleeding patients workshop at the Emergency Medicine Summer School 2017 (EMSS17) you will learn how to assess and treat bleeding patients
EMSS17: Bleeding patients course material Introduction During the bleeding patients workshop at the Emergency Medicine Summer School 2017 (EMSS17) you will learn how to assess and treat bleeding patients
GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS
 CHILDREN S HOSPITALS AND CLINICS OF MINNESOTA Introduction: GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS These guidelines have been developed in conjunction with the hospital Transfusion Committee.
CHILDREN S HOSPITALS AND CLINICS OF MINNESOTA Introduction: GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS These guidelines have been developed in conjunction with the hospital Transfusion Committee.
Pediatric massive transfusion protocols
 University of New Mexico UNM Digital Repository Emergency Medicine Research and Scholarship Emergency Medicine 2014 Pediatric massive transfusion protocols Ramsey Tate Follow this and additional works
University of New Mexico UNM Digital Repository Emergency Medicine Research and Scholarship Emergency Medicine 2014 Pediatric massive transfusion protocols Ramsey Tate Follow this and additional works
What s in the Massive Transfusion Protocol (MTP) Package?
 Package?") What s in the Massive Transfusion Protocol (MTP) Package? The Massive Transfusion Protocol Package is a set of documents intended to improve the coordination of a Massive Transfusion Protocol. The kit
What s in the Massive Transfusion Protocol (MTP) Package? The Massive Transfusion Protocol Package is a set of documents intended to improve the coordination of a Massive Transfusion Protocol. The kit
Blood Product Utilization A Mythbusters! Style Review. Amanda Haynes, DO 4/28/18
 Blood Product Utilization A Mythbusters! Style Review Amanda Haynes, DO 4/28/18 Objectives Describe concepts in Patient Blood Management Review common misconceptions surrounding blood transfusion Summarize
Blood Product Utilization A Mythbusters! Style Review Amanda Haynes, DO 4/28/18 Objectives Describe concepts in Patient Blood Management Review common misconceptions surrounding blood transfusion Summarize
Sepsis Early Recognition and Management. Therese Hughes, PhD, MPA, RN
 Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium
 Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium MARIA E. MANDICH MD Fairbanks Memorial Hospital Emergency Department Attending Physician Interior Region EMS Council Medical Director
Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium MARIA E. MANDICH MD Fairbanks Memorial Hospital Emergency Department Attending Physician Interior Region EMS Council Medical Director
Major Haemorrhage Protocol. Commentary
 Hairmyres Hospital Monklands Hospital Wishaw General Hospital Major Haemorrhage Protocol Commentary N.B. There is a separate NHSL protocol for the Management of Obstetric Haemorrhage Authors Dr Tracey
Hairmyres Hospital Monklands Hospital Wishaw General Hospital Major Haemorrhage Protocol Commentary N.B. There is a separate NHSL protocol for the Management of Obstetric Haemorrhage Authors Dr Tracey
SHOCK Susanna Hilda Hutajulu, MD, PhD
 SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
CrackCast Episode 7 Blood and Blood Components
 CrackCast Episode 7 Blood and Blood Components Episode Overview: 1) Describe the 3 categories of blood antigens 2) Who is the universal donor and why? 3) Define massive transfusion 4) List 5 physiologic
CrackCast Episode 7 Blood and Blood Components Episode Overview: 1) Describe the 3 categories of blood antigens 2) Who is the universal donor and why? 3) Define massive transfusion 4) List 5 physiologic
Preeclampsia. &Eclampsia. Hypertensive Disorders of Pregnancy. What we need to know about. Hypertensive Disorders of Pregnancy.
 Preeclampsia &Eclampsia Hypertensive Disorders of Pregnancy Barbara Koop MS, RNC-OB What we need to know about Hypertensive Disorders of Pregnancy Define clinical criteria for: Gestational hypertension,
Preeclampsia &Eclampsia Hypertensive Disorders of Pregnancy Barbara Koop MS, RNC-OB What we need to know about Hypertensive Disorders of Pregnancy Define clinical criteria for: Gestational hypertension,
Supplemental Digital Content: Definitions Based on the International Classification of Diseases, Ninth Revision, Clinical Modification
 Supplemental Digital Content: Definitions Based on the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) Diagnose and Procedures Codes 1. ICD-9-CM definition of
Supplemental Digital Content: Definitions Based on the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) Diagnose and Procedures Codes 1. ICD-9-CM definition of
SEPSIS: IT ALL BEGINS WITH INFECTION. Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft.
 SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
OBSTETRIC ADMISSION ORDERS 1 of 4
 OBSTETRIC ADMISSION 1 of 4 Actual Estimated Weight kg Actual Estimated Height cm ALLERGIES: REFER TO ALLERGY PROFILE/ POWERCHART ADMIT TO: Labor and Delivery ( ) Check, circle and/or fill in all orders
OBSTETRIC ADMISSION 1 of 4 Actual Estimated Weight kg Actual Estimated Height cm ALLERGIES: REFER TO ALLERGY PROFILE/ POWERCHART ADMIT TO: Labor and Delivery ( ) Check, circle and/or fill in all orders
What is. InSpectra StO 2?
 What is InSpectra StO 2? www.htibiomeasurement.com What is InSpectra StO 2? Hemoglobin O 2 saturation is measured in three areas: 1) Arterial (SaO 2, SpO 2 ) Assesses how well oxygen is loading onto hemoglobin
What is InSpectra StO 2? www.htibiomeasurement.com What is InSpectra StO 2? Hemoglobin O 2 saturation is measured in three areas: 1) Arterial (SaO 2, SpO 2 ) Assesses how well oxygen is loading onto hemoglobin
Blood/Blood Component Utilization and Administration Annual Compliance Education
 Blood/Blood Component Utilization and Administration Annual Compliance Education This course contains annual compliance education necessary to meet compliance and regulatory requirements. Instructions:
Blood/Blood Component Utilization and Administration Annual Compliance Education This course contains annual compliance education necessary to meet compliance and regulatory requirements. Instructions:
Alister Jones Patient Blood Management Practitioner NHS Blood and Transplant. Lab Matters study day Oake Manor, Taunton, 8 th July 2015
 Alister Jones Patient Blood Management Practitioner NHS Blood and Transplant Lab Matters study day Oake Manor, Taunton, 8 th July 2015 NPSA Rapid Response Report 2010 Transfusion of blood and blood components
Alister Jones Patient Blood Management Practitioner NHS Blood and Transplant Lab Matters study day Oake Manor, Taunton, 8 th July 2015 NPSA Rapid Response Report 2010 Transfusion of blood and blood components
Sepsis Awareness and Education
 Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Intrauterine balloon tamponade for the control of postpartum haemorrhage
 22 ORIGINAL ARTICLE Intrauterine balloon tamponade for the control of postpartum haemorrhage Rajni Lohano, 1 Gulfishan Haq, 2 Sarah Kazi, 3 Saima Sheikh 4 Abstract Objective: To evaluate the effectiveness
22 ORIGINAL ARTICLE Intrauterine balloon tamponade for the control of postpartum haemorrhage Rajni Lohano, 1 Gulfishan Haq, 2 Sarah Kazi, 3 Saima Sheikh 4 Abstract Objective: To evaluate the effectiveness
A Challenging Case: Von Willebrand Disease and Pulmonary Hypertension in Pregnancy
 A Challenging Case: Von Willebrand Disease and Pulmonary Hypertension in Pregnancy Diana S. Wolfe, MD, MPH Assistant Professor Department of Obstetrics & Gynecology and Women s Health Associate Fellowship
A Challenging Case: Von Willebrand Disease and Pulmonary Hypertension in Pregnancy Diana S. Wolfe, MD, MPH Assistant Professor Department of Obstetrics & Gynecology and Women s Health Associate Fellowship
State of Florida Hypothermia Protocol. Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology
 State of Florida Hypothermia Protocol Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. Entry Criteria 1. Gestational Age greater than or equal to 35 weeks gestation
State of Florida Hypothermia Protocol Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. Entry Criteria 1. Gestational Age greater than or equal to 35 weeks gestation
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
LEARNING OBJECTIVES 2/20/2017
 HYPERTENSION IN PREGNANCY: PREVENTING SEVERE MATERNAL MORBIDITY & MORTALITY THROUGH THE IMPLEMENTATION OF EVIDENCED BASED PROTOCOLS Laura Senn, RN, PhD, CNS Sutter Medical Center, Sacramento LEARNING OBJECTIVES
HYPERTENSION IN PREGNANCY: PREVENTING SEVERE MATERNAL MORBIDITY & MORTALITY THROUGH THE IMPLEMENTATION OF EVIDENCED BASED PROTOCOLS Laura Senn, RN, PhD, CNS Sutter Medical Center, Sacramento LEARNING OBJECTIVES
Example Clinical Guideline for Immediate Postpartum LARC Insertion
 Example Clinical Guideline for Immediate Postpartum LARC Insertion RATIONALE Delay in contraceptive provision until the six week postpartum appointment can leave some women at risk for rapid repeat pregnancy.
Example Clinical Guideline for Immediate Postpartum LARC Insertion RATIONALE Delay in contraceptive provision until the six week postpartum appointment can leave some women at risk for rapid repeat pregnancy.
Transfusion in major bleeding: new insights. Gert Poortmans
 Transfusion in major bleeding: new insights Gert Poortmans Trauma Cardiac Surgery Major Surgery with ongoing blood loss Burn Surgery Lethal Triad Polytransfusion: definitions Coagulation Coagulopathy of
Transfusion in major bleeding: new insights Gert Poortmans Trauma Cardiac Surgery Major Surgery with ongoing blood loss Burn Surgery Lethal Triad Polytransfusion: definitions Coagulation Coagulopathy of
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT
 PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
Components of Blood. N26 Blood Administration 4/24/2012. Cabrillo College ADN/C. Madsen RN, MSN 1. Formed elements Cells. Plasma. What can we give?
 Components of Blood Formed elements Cells Erythrocytes (RBCs) Leukocytes (WBCs) Thrombocytes (platelets) Plasma 90% water 10% solutes Proteins, clotting factors 1 What can we give? Whole blood Packed RBC
Components of Blood Formed elements Cells Erythrocytes (RBCs) Leukocytes (WBCs) Thrombocytes (platelets) Plasma 90% water 10% solutes Proteins, clotting factors 1 What can we give? Whole blood Packed RBC
MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY
 MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY 19th ANNUAL CONTROVERSIES AND PROBLEMS IN SURGERY Thabo Mothabeng General Surgery: 1 Military Hospital HH Stone et al. Ann Surg. May 1983; 197(5):
MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY 19th ANNUAL CONTROVERSIES AND PROBLEMS IN SURGERY Thabo Mothabeng General Surgery: 1 Military Hospital HH Stone et al. Ann Surg. May 1983; 197(5):
Results of Ischemic Heart Disease
 Ischemic Heart Disease: Angina and Myocardial Infarction Ischemic heart disease; syndromes causing an imbalance between myocardial oxygen demand and supply (inadequate myocardial blood flow) related to
Ischemic Heart Disease: Angina and Myocardial Infarction Ischemic heart disease; syndromes causing an imbalance between myocardial oxygen demand and supply (inadequate myocardial blood flow) related to
Surgical management of hepatic complications HELLP ד"ר ערן שדות יחידת ניתוחי כבד לבלב ודרכי מרה מרכז רפואי רבין, קמפוס בלינסון
 Surgical management of hepatic complications HELLP ד"ר ערן שדות יחידת ניתוחי כבד לבלב ודרכי מרה מרכז רפואי רבין, קמפוס בלינסון Outline Introduction HELPP and surgical liver complications 5 slides Real-life
Surgical management of hepatic complications HELLP ד"ר ערן שדות יחידת ניתוחי כבד לבלב ודרכי מרה מרכז רפואי רבין, קמפוס בלינסון Outline Introduction HELPP and surgical liver complications 5 slides Real-life
12/1/2009. Chapter 19: Hemorrhage. Hemorrhage and Shock Occurs when there is a disruption or leak in the vascular system Internal hemorrhage
 Chapter 19: Hemorrhage Hemorrhage and Shock Occurs when there is a disruption or leak in the vascular system External hemorrhage Internal hemorrhage Associated with higher morbidity and mortality than
Chapter 19: Hemorrhage Hemorrhage and Shock Occurs when there is a disruption or leak in the vascular system External hemorrhage Internal hemorrhage Associated with higher morbidity and mortality than
Chest diseases Hospital Laboratory Hematology Practice guidelines
 Chest diseases Hospital Laboratory Hematology Practice guidelines Title RBCs transfusion in Adults SOP Code Policy Owner Hematology Unit Section Hematology Prepared By Dr. Taher Ahmed Abdelhameed Issuing
Chest diseases Hospital Laboratory Hematology Practice guidelines Title RBCs transfusion in Adults SOP Code Policy Owner Hematology Unit Section Hematology Prepared By Dr. Taher Ahmed Abdelhameed Issuing
Sign up to receive ATOTW weekly
 MANAGEMENT OF MAJOR HAEMORRHAGE PART ONE: INITIAL RESPONSE ANAESTHESIA TUTORIAL OF THE WEEK 136 1 ST JUNE 2009 Katrina Webster (Senior Registrar in Anaesthesia) Royal Hobart Hospital, Tasmania, Australia.
MANAGEMENT OF MAJOR HAEMORRHAGE PART ONE: INITIAL RESPONSE ANAESTHESIA TUTORIAL OF THE WEEK 136 1 ST JUNE 2009 Katrina Webster (Senior Registrar in Anaesthesia) Royal Hobart Hospital, Tasmania, Australia.
Use of Blood Lactate Measurements in the Critical Care Setting
 Use of Blood Lactate Measurements in the Critical Care Setting John G Toffaletti, PhD Director of Blood Gas and Clinical Pediatric Labs Professor of Pathology Duke University Medical Center Chief, VAMC
Use of Blood Lactate Measurements in the Critical Care Setting John G Toffaletti, PhD Director of Blood Gas and Clinical Pediatric Labs Professor of Pathology Duke University Medical Center Chief, VAMC
ADULT TRANSFUSION GUIDELINES ORDERED COMPONENT
 ADULT TRANSFUSIN GUIDELINES RDERED Packed red cells (RBCs) RBCs, WBCs, platelets & plasma (minimal) Increase red cell mass and oxygen carrying capacity; generally indicated when Hgb is 7 gm or Hct 21 unless
ADULT TRANSFUSIN GUIDELINES RDERED Packed red cells (RBCs) RBCs, WBCs, platelets & plasma (minimal) Increase red cell mass and oxygen carrying capacity; generally indicated when Hgb is 7 gm or Hct 21 unless
CEDR 2018 QCDR Measures for CMS 2018 MIPS Performance Year Reporting
 ACEP19 Emergency Department Utilization of CT for Minor Blunt Head Trauma for Aged 18 Years and Older Percentage of visits for aged 18 years and older who presented with a minor blunt head trauma who had
ACEP19 Emergency Department Utilization of CT for Minor Blunt Head Trauma for Aged 18 Years and Older Percentage of visits for aged 18 years and older who presented with a minor blunt head trauma who had
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
McHenry Western Lake County EMS System CE for Paramedics, EMT-B and PHRN s Sepsis Patients. November/December 2017
 McHenry Western Lake County EMS System CE for Paramedics, EMT-B and PHRN s Sepsis Patients November/December 2017 This month we are going to take a look at the patient with Sepsis. Webster s defines septic
McHenry Western Lake County EMS System CE for Paramedics, EMT-B and PHRN s Sepsis Patients November/December 2017 This month we are going to take a look at the patient with Sepsis. Webster s defines septic
The Use of Dynamic Parameters in Perioperative Fluid Management
 The Use of Dynamic Parameters in Perioperative Fluid Management Gerard R. Manecke Jr., M.D. Chief, Cardiac Anesthesia UCSD Medical Center San Diego, CA, USA Thanks to Tom Higgins, M.D. 1 Goals of today
The Use of Dynamic Parameters in Perioperative Fluid Management Gerard R. Manecke Jr., M.D. Chief, Cardiac Anesthesia UCSD Medical Center San Diego, CA, USA Thanks to Tom Higgins, M.D. 1 Goals of today
HYPOVOLEMIA AND HEMORRHAGE UPDATE ON VOLUME RESUSCITATION HEMORRHAGE AND HYPOVOLEMIA DISTRIBUTION OF BODY FLUIDS 11/7/2015
 UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
Hypertensive Disorders of Pregnancy Guideline
 Hypertensive Disorders of Pregnancy Guideline Approved by: Senior Director of Operations, Women s & Child Health, GNCH/MCH Facility Chief, Obstetrics/Gynecology, GNCH Facility Chief, Obstetrics/Gynecology,
Hypertensive Disorders of Pregnancy Guideline Approved by: Senior Director of Operations, Women s & Child Health, GNCH/MCH Facility Chief, Obstetrics/Gynecology, GNCH Facility Chief, Obstetrics/Gynecology,
Intraoperative haemorrhage and haemostasis. Dr. med. Christian Quadri Capoclinica Anestesia, ORL
 Intraoperative haemorrhage and haemostasis Dr. med. Christian Quadri Capoclinica Anestesia, ORL Haemostasis is like love. Everybody talks about it, nobody understands it. JH Levy 2000 Intraoperative Haemorrhage
Intraoperative haemorrhage and haemostasis Dr. med. Christian Quadri Capoclinica Anestesia, ORL Haemostasis is like love. Everybody talks about it, nobody understands it. JH Levy 2000 Intraoperative Haemorrhage
Hematology Review. CCRN exam. The Coagulation Cascade. The Coagulation Cascade. Components include: Intrinsic pathway Extrinsic pathway Common pathway
 CCRN exam Hematology Review CCRN Review October 2013 Department of Critical Care Nursing Hematology is 2% of the exam Focus on coagulation cascade, DIC, and HIT Anatomy of the hematologic system Bone marrow
CCRN exam Hematology Review CCRN Review October 2013 Department of Critical Care Nursing Hematology is 2% of the exam Focus on coagulation cascade, DIC, and HIT Anatomy of the hematologic system Bone marrow
Bassett Medical Center The Mary Imogene Bassett Hospital Clinical Laboratory Blood Bank Title: MTP 2016 Revision: 2.00 Created By: Admin, The Last
 Bassett Medical Center The Mary Imogene Bassett Hospital Clinical Laboratory Blood Bank Title: MTP 2016 Revision: 2.00 Created By: Admin, The Last Approved Time: 7/22/2016 12:44:54 PM Massive Transfusion
Bassett Medical Center The Mary Imogene Bassett Hospital Clinical Laboratory Blood Bank Title: MTP 2016 Revision: 2.00 Created By: Admin, The Last Approved Time: 7/22/2016 12:44:54 PM Massive Transfusion
ICU treatment of the trauma patient. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 ICU treatment of the trauma patient Intensive Care Training Program Radboud University Medical Centre Nijmegen Christian Kleber Surgical Intensive Care Unit - The trauma surgery Perspective Langenbecks
ICU treatment of the trauma patient Intensive Care Training Program Radboud University Medical Centre Nijmegen Christian Kleber Surgical Intensive Care Unit - The trauma surgery Perspective Langenbecks
Blood Component Therapy
 Blood Component Therapy Dr Anupam Chhabra Incharge-Transfusion Medicine Pushpanjali Crosslay Hopital NCR-Delhi Introduction Blood a blood components are considered drugs because of their use in treating
Blood Component Therapy Dr Anupam Chhabra Incharge-Transfusion Medicine Pushpanjali Crosslay Hopital NCR-Delhi Introduction Blood a blood components are considered drugs because of their use in treating
Case year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50
 Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
IV Fluids. I.V. Fluid Osmolarity Composition 0.9% NaCL (Normal Saline Solution, NSS) Uses/Clinical Considerations
 Uses/Clinical Considerations") IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
Maternal Cardiac Disease In Pregnancy. August 25, 2017 PREGNANCY ECHO CONFERENCE
 Maternal Cardiac Disease In Pregnancy August 25, 2017 PREGNANCY ECHO CONFERENCE Maternal Physiology Cardiac Output = HR x SV Non-pregnant: 4.5 L/min Pregnant: 6.0 L/min Increase most acute in first 10
Maternal Cardiac Disease In Pregnancy August 25, 2017 PREGNANCY ECHO CONFERENCE Maternal Physiology Cardiac Output = HR x SV Non-pregnant: 4.5 L/min Pregnant: 6.0 L/min Increase most acute in first 10
Nothing to Disclose. Severe Pulmonary Hypertension
 Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Clinical Usefulness of Bakri Balloon Tamponade in the Treatment of Massive Postpartum Uterine Hemorrhage
 Original Contribution This is Advance Publication Article Kurume Medical Journal, 62, 17-21, 2015 Clinical Usefulness of Bakri Balloon Tamponade in the Treatment of Massive Postpartum Uterine Hemorrhage
Original Contribution This is Advance Publication Article Kurume Medical Journal, 62, 17-21, 2015 Clinical Usefulness of Bakri Balloon Tamponade in the Treatment of Massive Postpartum Uterine Hemorrhage
MATERNAL COLLAPSE. University Hospital of Wales Steve Morris (Huw Davis)
") MATERNAL COLLAPSE University Hospital of Wales Steve Morris (Huw Davis) Thought for the day The real troubles in your life are apt to be things that never crossed your worried mind; the kind that blindside
MATERNAL COLLAPSE University Hospital of Wales Steve Morris (Huw Davis) Thought for the day The real troubles in your life are apt to be things that never crossed your worried mind; the kind that blindside
Obstetric Anal Sphincter Injury. An update on best practices. Objectives
 Obstetric Anal Sphincter Injury An update on best practices Erin Crosby MD Assistant Professor Department of OB/Gyn Division of FPMRS 1 Objectives Describe the anatomy of the anal sphincter complex Discuss
Obstetric Anal Sphincter Injury An update on best practices Erin Crosby MD Assistant Professor Department of OB/Gyn Division of FPMRS 1 Objectives Describe the anatomy of the anal sphincter complex Discuss
MASSIVE TRANSFUSION PROTOCOL
 MASSIVE TRANSFUSION PROTOCOL IF YOU ANTICIPATE EMERGENT NEED FOR LARGE AMOUNTS OF BLOOD IN A SHORT PERIOD OF TIME Call Blood Bank: 6622121 Tell them you have a patient who needs a Massive Transfusion and
MASSIVE TRANSFUSION PROTOCOL IF YOU ANTICIPATE EMERGENT NEED FOR LARGE AMOUNTS OF BLOOD IN A SHORT PERIOD OF TIME Call Blood Bank: 6622121 Tell them you have a patient who needs a Massive Transfusion and
How and why I give IV fluid Disclosures SCA Fluids and public health 4/1/15. Andrew Shaw MB FRCA FCCM FFICM
 How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
Severe post-partum haemorrhage (PPH) occurs
 occurs") Acta Anaesthesiol Scand 2012; : Printed in Singapore. All rights reserved 2012 The Authors Acta Anaesthesiologica Scandinavica 2012 The Acta Anaesthesiologica Scandinavica Foundation ACTA ANAESTHESIOLOGICA
Acta Anaesthesiol Scand 2012; : Printed in Singapore. All rights reserved 2012 The Authors Acta Anaesthesiologica Scandinavica 2012 The Acta Anaesthesiologica Scandinavica Foundation ACTA ANAESTHESIOLOGICA
Postpartum LARC. (Long Acting Reversible Contraception) NURSING EDUCATION
 NURSING EDUCATION") Postpartum LARC (Long Acting Reversible Contraception) NURSING EDUCATION What is LARC Long-acting reversible contraception (LARC) methods include the intrauterine device (IUD) and the birth control implant.
Postpartum LARC (Long Acting Reversible Contraception) NURSING EDUCATION What is LARC Long-acting reversible contraception (LARC) methods include the intrauterine device (IUD) and the birth control implant.