Acute Kidney Injury. Dr S Mathavakkannan Consultant Nephrologist
|
|
|
- Philippa Ball
- 6 years ago
- Views:
Transcription
1 Acute Kidney Injury Dr S Mathavakkannan Consultant Nephrologist
2

3 1. 2. Epidemiology 3. Physiology 4. Markers of Injury 5. Survival 6. Treatment 7. AKI Scope
4 1. ADQI 1. RIFLE Criteria Acute renal failure definition, outcome measures, animal models, fluid therapy and information technology needs: the Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group; 2004 Risk (Class R) Injury (Class I) Failure (Class F)
")
5 Stra%fica%on Based on RIFLE RIFLE criteria for acute kidney injury are associated with hospital mortality in critically ill patients: a cohort analysis Hoste et al ; Critical Care 2006 (10) R73
6 Outcomes of all Patients based on RIFLE Class
7 Survival: Based on RIFLE Categorisation
8 1. ADQI 1. RIFLE Criteria 2. AKIN 1. Modified RIFLE Criteria 1. Serum rises by 26µmol/L from the baseline value within 48 hours 2. Serum rises 1.5 fold from the baseline value 3. urine output is < 0.5ml/kg/hr for >6 hours

9

10
11 in AKI
12

13

14
15 Incidence of AKI 1. US: 1. 1% % 2. UK: pmp pmp 3. AKI- RRT: pmp 3. Care: % of develop AKI % of admissions require RRT 3. AKI accounts 10% Hospital Days 4. AKI in Hospital: % mortality 2. Uncomplicted AKI: Mortality of 10% 3. AKI in organ failure: 50% 4. AKI requiring RRT in organ failure : 80%
16
17 Study overview Proposed by the Renal Associa4on Prevalent and serious problem amongst hospitalised All hospital regardless of specialty, are at risk of AKI It is unknown to what degree strategies to reduce the risk of AKI are implemented
18 Primary aim To examine the process of care of who died in hospital with AKI, in order to remediable factors in the care received by these

19 Data returns
20 Key findings Only 50% of AKI care considered good Poor assessment of risk factors Unacceptable delay in of post- admission in AKI in 43% 22 died with a primary diagnosis of post- admission AKI which was predictable and avoidable Complica@ons missed (13%), avoidable (17%) or badly managed (22%)
21 NCEPOD Report 2009
22 Comprehensive Assessment in AKI 1. notes 2. AKI risk factors 1. age > 75 yrs 2. chronic kidney disease (CKD, egfr < 60 mls/min/ 1.73m 2 ) 3. Cardiac failure 4. Atherosclero@c peripheral vascular disease 5. Liver disease 6. Diabetes mellitus 7. Nephrotoxic medica@ons 3. poten@al causes for AKI including 3. reduced fluid intake 4. increased fluid losses 5. urinary tract symptoms 6. recent drug inges@on 7. sepsis 4. systemic clinical features 4. fever 5. rash 6. joint pains
23 Comprehensive Assessment in AKI general rash joint swelling assessment of volume status core temperature peripheral perfusion heart rate blood pressure jugular venous pressure signs of renovascular disease audible bruits impalpable peripheral pulses abdominal palpable bladder
24 biochemistry Urea and electrolytes haematology FBC urinalysis (± microscopy) microbiology urine culture (if is suspected) blood culture (if is suspected) renal immunology urinary biochemistry electrolytes osmolality ECG chest x- ray abdominal x- ray renal tract ultrasound (within 24hrs if suspected) kidney biopsy
25 Measurement of Crea%nine 1. Poor Biomarker 1. Jaffe (1886) 2. Inter- laboratory and interference 3. Interference 1. Protein, glucose, ascorbate, pyurvate, cephalosporins 2. Bilirubin 4. Assays 1. sarcosine oxidase 5. against IDMS

26 Proteinuria (3+ or >) Haematuria Lucocyturia Eosinophiluria Crystalluria EG TLS S, AcyC, IndinV, TriamT, Myoglobinuria Urine Microscopy
27 Urine Electrolyte 1. FE Na 2. FE Urea 3. Urinary Sodium 4. Free water clearence 5. Clearence 6. Blood 1. Pre- Renal Azotemia 2. ATN 3. Hepatorenal Syndrome
28 1. NGAL 2. KIM Cysta@n C 4. IL NAG 6. L- FABP Biomarkers of AKI

29 Urinary biomarkers for acute kidney injury (AKI) evaluated in at least 2 human studies (Belcher et al; AJKD; March 2011)

30 NGAL: in Pre- Renal vs AKI Scenario Singer et al; KI 16 March 2011
31 AKI- Strategies Major Surgery Sepsis: SIRS v CARS; EGDT; Volume and Pressor support; euglycemia; Low Tidal Vol CI- AKI Rhabdomyolysis
 Need for RRT n=9; 1215; OR 0.5 Survival n=11; 1640; OR 0.")
32 AKI: Strategies Contrast Induced AKI (CI- AKI) Parameter Number Number in Total n=12; 1854 of CI- AKI using bicarbonate n = 12; 1652; OR 0.46 ( ) Need for RRT n=9; 1215; OR 0.5 Survival n=11; 1640; OR 0.51 Bicarbonate use in CCF No difference in Survival; no excessive LVF episodes Compare with REMEDIAL (NS+NAC v NaHCO3+NAC v NAC+Vit C+NS Hoste et al AJKD 2009 Brer et al JASN
33 Contrast Induced AKI (CI- AKI)
34 Contrast Induced AKI (CI- AKI)
35 Flowchart of meta-analysis. Brar S S et al. CJASN 2009;4: by American Society of Nephrology
36 Forest plot of randomized trials meeting inclusion criteria. Brar S S et al. CJASN 2009;4: by American Society of Nephrology
37 AKI- Rhabdomyolysis Factors 1. Trauma 2. Burns 3. Compartment Syndrome 4. Drugs Coccaine 3. Ecstasy Management 1. Volume Assessment 2. Aggressive UO 100ml/hr 2. Urine ph>6.5
38 1. Fluid General Management 1. Crystalloid vs Colloid 2. Oliguric vs Non- Oliguric AKI 2. Pharmacological Therapy 1. Frusemide: 2. Dopamine 3. Fenoldopam 4. ANP


39 AKI- General Management: Fluid and Euglycemia Intensive Insulin Therapy and Pentastarch in Severe Sepsis N Engl J Med 2008;358:

40 AKI- General Management: Role of Frusemide Meta- analysis of frusemide to prevent or treat acute renal failure Ho and Sheridan BMJ ; 7565 pp445

41 Ho K M, Sheridan D J BMJ 2006;333:420 Effect of frusemide on in-hospital mortality and proportion of patients requiring renal replacement therapy or dialysis.

42 Number of dialysis sessions required after frusemide or control treatments. Ho K M, Sheridan D J BMJ 2006;333: by British Medical Journal Publishing Group

43 Proportion of patients remaining oliguric (urine output <500 ml/day) after frusemide or control treatments and those mentioning tinnitus or deafness. Ho K M, Sheridan D J BMJ 2006;333: by British Medical Journal Publishing Group
44 AKI- Pharmacological Fenoldopam Beneficial Impact of Fenoldopam in Cri%cally Ill Pa%ents With or at Risk for Acute Renal Failure: A Meta- Analysis of Randomized Clinical Trials Landoni et al; AJKD 2007 Parameter Results RCTs in Meta- analysis 16 Number of pa@ents 1290 Risk for AKI OR 0.43 Risk of Death 0.64 RRT Requirement OR 0.54 Hypotension Frequency in Fenoldopam group not higher ICU Stay Dopamine A 1 Receptor agonist 2. Short ac@ng 3. Decreases SVR 4. Increases both cor@cal and medullary blood flow
45 AKI- Pharmacological ANP CJASN 2009; Nigwekar et al; 19 Trials 1861 patients
46 AKI- General Management : Nutri@on 1. Calories: 25-35kcal/kg/day 2. Amino acids: 1.7g/kg/day 3. Die@cian Input within 24 hours 4. Supplement water soluble Vitamins if receiving RRT 5. Treat Hyperglycemia Cau@ously 6. Consider Selenium 7. Vit C supplementa@on not necessary 8. Vit K levels may be elevated 9. Enteral route vastly superior 10. Electrolyte disturbances to be treated as required
47 AKI- General Principles: Place of Care Most AKI outside Renal Unit Factors + or non- renal organ failure Requirement for RRT Renal Specialist Input Key Interfaces Cri@cal care outreach Acute renal outreach Specialist renal/icu Interface Avoiding deficiencies in ini@al assessment and management Physiological Early Warning Scores (MEWS/PARA scoring) Educa@on Wrisen guidelines Senior Specialist Renal Input
48 AKI- General Principles: Place of Care 1. flow from care to renal services: a year- long survey in a cri@cal care network (Wright et al QJM Aug 2008) /527 pa@ents survived 2. Incidence of RRT in ICU 234 pmp/year 3. Dura@on of RRT in ICU: 4 DAYS /219 required renal support outside ICU 5. 74/129 were provided RRT in ICU as for single organ failure ICU days u@lised to provide this support 2. Kanagasundaram NS, Jones KE. Transfer of pa@ents with acute kidney injury to specialist renal services- - physiological early- warning systems, applied prior to transfer from outside hospitals, can iden@fy those at risk of deteriora@on. QJM 2008;101: SOFA Score to assess need for escala@on
49 Management in AKI Principles ü Volume ü Acid- base, electrolytes ü ü Adequate dosing if fails
50 RRT CRRT vs IHD Hybrid Therapies
51 Which When How much
52
53

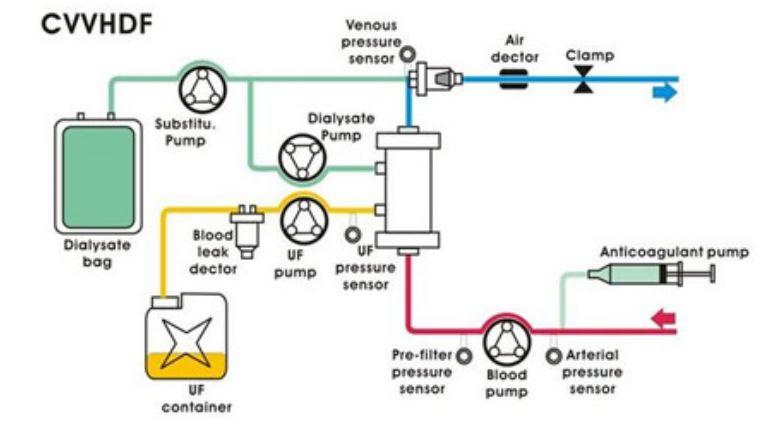
54 Dialysis therapies CVVHDF AN69 membrane ml/min blood flow Heparin or no IHD F50/60/80 Dialysers ml/min UF ml/h 3-4 hours
55 Story of beser haemodynamic stability in CRRT vs IHD Authors/Setting n Outcome ITU/1993/Davenport et al 32 combined AKI/hepatic failure Intermittent vs CAVH/ CAVHD 35 vs 25 treatments Increased ICP, decreased CO, decreased DO2 Van der Scheuren 1996 N=11 IHD increases systemic O2 consumption Heering 1997 N=33 Cytokine removal with CVVH, improvement in CV haemodynamics Misset 1996 N=27 CAVH vs HD; MAP changes similar in both groups John and Griesbach 2001 N=30 (20 cvvh 10 hd) CVVH vs HD in sepsis; drop in HR, slight increase BP, splanchnic perfusion parameters unchanged Kumar 2000 N=42 (25 EDD, 17 CVVH) 367 vs 117 treatment days, 7.5 vs 19.5 hours, Kielstein JT N= 39, (CVVH 19, EDD 20) Earlier correction of acidosis, less heparin
56 Evidence NephSAP September 2007
57 Uehlinger et al NDT 2005 Hypothesis: CVVHD beser in- hospital mortality length of hospital stay N 125 Definition of AKI CVVHDF 70 IHD 55 Matching Catecholamine use (75% overall) Ventilation (75%) Creatinine >350, UO <20ml/h Demographics Cause of AKI Severity of illness Identical in both arms Identical in both arms ICU Mortality 34% vs 38% In hospital mortality 47% vs 51% Duration of RRT Renal recovery Identical Recovery of renal func@on 97% (1 in each group HD dependant)
58 Blood pressure and of during ICU stay CVVHDF vs IHD
59 Hemodiafe (Vinsonneau et al, The Lancet 29 th July 2006) Eligibility: AKI >350; urea >36; UO <200ml/16h; need for RRT

60 Survival: 32.6% vs 31.5% IHD survival improved through trial period? CVVHDF dose inadequate
61 Flow chart of the SHARF 4 study. Lins R L et al. Nephrol. Dial. Transplant. 2009;24: The Author [2008]. Published by Oxford University Press on behalf of ERA-EDTA. All rights reserved. For Permissions, please journals.permissions@oxfordjournals.org

62
63 Preference of one modality over another Parameter CRRT IHD q IHD modality of choice for managing AKI in ICU (Mehta et al) Geography Europe/Australia/SE Asia US/Canada? Anticoagulation q Local preferences; >97% - of treatments for AKI in Australia + are CRRT Therapeutic q Haemodynamic agents stability governs - choice of therapy + Nutrition - + Volume q Con@nuous management removal of inflammatory? more error cytokines prone beser (?) easier Dialysate q Blood membrane contact Less is pro- inflammatory standardised across regions Haemodynamic stability + (perceived) - simpler Training Personnel intensive Relatively easier Ease of dialysis dose delivery? - + Convective clearence + BUT is it useful? _ Inflammatory cascade Dubious value None, may be less proinflammatory as bloodmembrane contact less Cost - +
64 AKI- RRT : Equipment 1. Dialyser: Synthe@c or Modified Cellulosaic 2. Bicarbonate buffer 3. Microbiological Integrity of Dialysate 4. An@coagula@on 1. Heparin vs Citrate 2. Prostacycline 3. Saline Flushes 4. Choice if HIT 1. Danaproid/Fondaparineux 2. Hirudin/Lepirudin 3. Argotroban 4. Nafamostat
65 Kt/V ~ 1.2 URR > 65% AKI- Dose of RRT Evidence: 1. Veteran Affairs/Na@onal Ins@tute of Health Acute Renal Failure Trial Network 2. Randomised Evalua@on of Normal Versus Augmented Level Renal Replacement Therapy (RENAL)
66 How much? Ronco et al Lancet July 2000 Efficacy of three different doses of CVVH
67 Intensity of Renal Support in Cri%cally Ill Pa%ents with Acute Kidney Injury
68 Intensity of Renal Support in Cri%cally Ill Pa%ents with Acute Kidney Injury Intense vs IHD/SLED CVVH at 35ml/kg/hour
69 Mortality at 60 days
70 RENAL Study Design
71 RENAL: Outcome Summary
72 AKI- When to Start RRT
73 Era Number Criteria 1960s/1970s/1980s 3 BUN mg/dl 1990s At least 2 of importance n=100; higher survival in early initiation n= 64, Cardiac ITU, 22 vs 43:: early/late PICARD n=243 Survival 80 & 65 (early) 75 & 59 (late) RR 1.85 (co-variate adj) RR 2.07 (propensity sco) BUT Urea cannot be a surrogate for dura@on of AKI AND spontaneous recovery or death without RRT <60 BUN group vs >60 8 hr oliguria / >84mg/dl <76mg/dl vs >76mg/dl
74 Early start a good idea How early is early AKI- When to Start RRT Perhaps Stage 3 of AKIN Balance Early start with Morbidity associated with RRT? Delays recovery from AKI Many pa@ents pull back from brink with suppor@ve therapy Urea of 28mmol/L a cut off? 21.5mmol/l? UO <100ml/ 8hr

75 PICARD Study ( Cho et al JASN 2006) Observa@onal study CRRT vs IHD Feb (1999- Aug 2001) (n=398, 206 CRRT, 198 IHD) AKI defini@on: q q q Increase in serum crea@nine by >44μmol/L from baseline, if baseline <132μmol/L Increase in serum crea@nine by >88μmol/L if baseline 132<B<440 Baseline CKD egfr<30ml/min Who got what? CRRT Respiratory organ failure Fluid overload IHD Older No PA monitoring Higher BUN and creatinine Non-white population Higher SBP
76 AKI- Timing of RRT Timing of renal replacement therapy and clinical outcomes in cri%cally ill pa%ents with severe acute kidney injury Beginning and Ending Therapy for the Kidney (BEST Kidney) Bagshaw et al; JoCC March 2009 Parameter Results Type 23 countries, 52 ICUs, 1238 Criteria Early vs Late Factors: Urea <24.2 vs >24.2 OR 0.92/1.25 (63.4 VS 61.4%) <309 vs >309 OR 0.46/0.51 (53.4 vs 71.3) ICU Stay: <2, 3-5, > vs 62.3 vs 59
77 AKI-
78

79
80
Rationale for renal replacement therapy in ICU: indications, approaches and outcomes. Richard Beale
 Rationale for renal replacement therapy in ICU: indications, approaches and outcomes Richard Beale RIFLE classification (ADQI group) 2004 Outcome AKIN classification Definition: Abrupt (within 48 hrs)
Rationale for renal replacement therapy in ICU: indications, approaches and outcomes Richard Beale RIFLE classification (ADQI group) 2004 Outcome AKIN classification Definition: Abrupt (within 48 hrs)
Decision making in acute dialysis
 Decision making in acute dialysis Geoffrey Bihl MB.BCh M.MED FCP(SA) Nephrologist and Director Winelands Kidney and Dialysis Centre Somerset West South Africa Important questions in AKI What is the cause?
Decision making in acute dialysis Geoffrey Bihl MB.BCh M.MED FCP(SA) Nephrologist and Director Winelands Kidney and Dialysis Centre Somerset West South Africa Important questions in AKI What is the cause?
Comparing RRT Modalities: Does It Matter What You Use If The Job Is Done?
 Comparing RRT Modalities: Does It Matter What You Use If The Job Is Done? Sean M Bagshaw, MD, MSc Division of Critical Care Medicine University of Alberta Disclosure Consulting: Alere, Baxter, Gambro,
Comparing RRT Modalities: Does It Matter What You Use If The Job Is Done? Sean M Bagshaw, MD, MSc Division of Critical Care Medicine University of Alberta Disclosure Consulting: Alere, Baxter, Gambro,
Who? Dialysis for Acute Renal Failure: Who, What, How, and When? Kathleen D. Liu, MD, PhD, MAS June 2011
 Dialysis for Acute Renal Failure: Who, What, How, and When? Kathleen D. Liu, MD, PhD, MAS June 2011 Dorre Nicholau MD PhD Clinical Professor Department of Anesthesia and Perioperative Care University of
Dialysis for Acute Renal Failure: Who, What, How, and When? Kathleen D. Liu, MD, PhD, MAS June 2011 Dorre Nicholau MD PhD Clinical Professor Department of Anesthesia and Perioperative Care University of
Renal replacement therapy in Pediatric Acute Kidney Injury
 Renal replacement therapy in Pediatric Acute Kidney Injury ASCIM 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Important topic: AKI
Renal replacement therapy in Pediatric Acute Kidney Injury ASCIM 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Important topic: AKI
Timing, Dosing and Selecting of modality of RRT for AKI - the ERBP position statement
 Timing, Dosing and Selecting of modality of RRT for AKI - the ERBP position statement Prof. Dr. Achim Jörres Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Timing, Dosing and Selecting of modality of RRT for AKI - the ERBP position statement Prof. Dr. Achim Jörres Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
LESSONS FROM EVIDENCE BASED MEDICINEIN THE CARE OF ARF AND ESRD. Prof. Dr. Adrian Covic University of Medicine Gr. T. Popa, Iaşi
 LESSONS FROM EVIDENCE BASED MEDICINEIN THE CARE OF ARF AND ESRD 2008 Prof. Dr. Adrian Covic University of Medicine Gr. T. Popa, Iaşi Effect of acute renal failure requiring renal replacement therapy on
LESSONS FROM EVIDENCE BASED MEDICINEIN THE CARE OF ARF AND ESRD 2008 Prof. Dr. Adrian Covic University of Medicine Gr. T. Popa, Iaşi Effect of acute renal failure requiring renal replacement therapy on
Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? Modalities of Dialysis
 How Wise is Early Dialysis in Critically Ill Patients? Modalities of Dialysis") Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? A common condition in ICU patients Associated with high mortality and morbidity Renal Replacement Therapy (RRT) is the cornerstone
Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? A common condition in ICU patients Associated with high mortality and morbidity Renal Replacement Therapy (RRT) is the cornerstone
What s new in kidneys a renal update for Anaesthetists
 What s new in kidneys a renal update for Anaesthetists Thursday 11 th December 2014 Roslyn Simms Clinical Lecturer in Nephrology Renal update What s new/update AKI When to start RRT in AKI? Perioperative
What s new in kidneys a renal update for Anaesthetists Thursday 11 th December 2014 Roslyn Simms Clinical Lecturer in Nephrology Renal update What s new/update AKI When to start RRT in AKI? Perioperative
ENDPOINTS FOR AKI STUDIES
 ENDPOINTS FOR AKI STUDIES Raymond Vanholder, University Hospital, Ghent, Belgium SUMMARY! AKI as an endpoint! Endpoints for studies in AKI 2 AKI AS AN ENDPOINT BEFORE RIFLE THE LIST OF DEFINITIONS WAS
ENDPOINTS FOR AKI STUDIES Raymond Vanholder, University Hospital, Ghent, Belgium SUMMARY! AKI as an endpoint! Endpoints for studies in AKI 2 AKI AS AN ENDPOINT BEFORE RIFLE THE LIST OF DEFINITIONS WAS
Section 3: Prevention and Treatment of AKI
 http://www.kidney-international.org & 2012 KDIGO Summary of ommendation Statements Kidney International Supplements (2012) 2, 8 12; doi:10.1038/kisup.2012.7 Section 2: AKI Definition 2.1.1: AKI is defined
http://www.kidney-international.org & 2012 KDIGO Summary of ommendation Statements Kidney International Supplements (2012) 2, 8 12; doi:10.1038/kisup.2012.7 Section 2: AKI Definition 2.1.1: AKI is defined
Acute Kidney Injury for the General Surgeon
 Acute Kidney Injury for the General Surgeon UCSF Postgraduate Course in General Surgery Maui, HI March 20, 2011 Epidemiology & Definition Pathophysiology Clinical Studies Management Summary Hobart W. Harris,
Acute Kidney Injury for the General Surgeon UCSF Postgraduate Course in General Surgery Maui, HI March 20, 2011 Epidemiology & Definition Pathophysiology Clinical Studies Management Summary Hobart W. Harris,
Adding Insult to Injury. Marlies Ostermann Consultant in Nephrology & Critical Care Guy s & St Thomas Hospital, London
 Acute Kidney Injury Adding Insult to Injury Marlies Ostermann Consultant in Nephrology & Critical Care Guy s & St Thomas Hospital, London Content 1. Brief review of AKI and its impact 2. Comments on the
Acute Kidney Injury Adding Insult to Injury Marlies Ostermann Consultant in Nephrology & Critical Care Guy s & St Thomas Hospital, London Content 1. Brief review of AKI and its impact 2. Comments on the
CRRT Fundamentals Pre- and Post- Test. AKI & CRRT Conference 2018
 CRRT Fundamentals Pre- and Post- Test AKI & CRRT Conference 2018 Question 1 Which ONE of the following statements regarding solute clearance in CRRT is MOST correct? A. Convective and diffusive solute
CRRT Fundamentals Pre- and Post- Test AKI & CRRT Conference 2018 Question 1 Which ONE of the following statements regarding solute clearance in CRRT is MOST correct? A. Convective and diffusive solute
ECMO & Renal Failure Epidemeology Renal failure & effect on out come
 ECMO Induced Renal Issues Transient renal dysfunction Improvement in renal function ECMO & Renal Failure Epidemeology Renal failure & effect on out come With or Without RRT Renal replacement Therapy Utilizes
ECMO Induced Renal Issues Transient renal dysfunction Improvement in renal function ECMO & Renal Failure Epidemeology Renal failure & effect on out come With or Without RRT Renal replacement Therapy Utilizes
CRRT: The Technical Questions Modality & Dose. Ashita J. Tolwani, MD, MSc University of Alabama at Birmingham 2018
 CRRT: The Technical Questions Modality & Dose Ashita J. Tolwani, MD, MSc University of Alabama at Birmingham 2018 Case A 24YOM with HTN and OSA presents with acute pancreatitis. Despite aggressive fluid
CRRT: The Technical Questions Modality & Dose Ashita J. Tolwani, MD, MSc University of Alabama at Birmingham 2018 Case A 24YOM with HTN and OSA presents with acute pancreatitis. Despite aggressive fluid
Fluid Management in Critically Ill AKI Patients
 Fluid Management in Critically Ill AKI Patients Sang Kyung Jo, MD, PhD Department of Internal Medicine Korea University Medical College KO/MG31/15-0017 Outline Fluid balance in critically ill patients:
Fluid Management in Critically Ill AKI Patients Sang Kyung Jo, MD, PhD Department of Internal Medicine Korea University Medical College KO/MG31/15-0017 Outline Fluid balance in critically ill patients:
Managing Patients with Sepsis
 Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
higher dose with progress in technical equipment. Continuous Dialysis: Dose and Antikoagulation. prescribed and delivered
 1 2 Continuous Dialysis: Dose and Antikoagulation higher dose with progress in technical equipment Comparison of pump-driven and spontaneous continuous haemofiltration in postoperative acute renal failure.
1 2 Continuous Dialysis: Dose and Antikoagulation higher dose with progress in technical equipment Comparison of pump-driven and spontaneous continuous haemofiltration in postoperative acute renal failure.
Acute Kidney Injury; get the basics right first!
 Acute Kidney Injury; get the basics right first! Dr Christopher Wong, Consultant Nephrologist and General Physician, University Hospital Aintree (UHA), Liverpool, UK Acute kidney injury (AKI) Why a new
Acute Kidney Injury; get the basics right first! Dr Christopher Wong, Consultant Nephrologist and General Physician, University Hospital Aintree (UHA), Liverpool, UK Acute kidney injury (AKI) Why a new
ASN Board Review: Acute Renal Replacement Therapies
 ASN Board Review: Acute Renal Replacement Therapies Ashita Tolwani, M.D., M.Sc. University of Alabama at Birmingham 2014 Key issues for boards: RRT for AKI When should therapy be initiated? What are the
ASN Board Review: Acute Renal Replacement Therapies Ashita Tolwani, M.D., M.Sc. University of Alabama at Birmingham 2014 Key issues for boards: RRT for AKI When should therapy be initiated? What are the
Citrate Anticoagulation
 Strategies for Optimizing the CRRT Circuit Citrate Anticoagulation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum Berlin, Germany
Strategies for Optimizing the CRRT Circuit Citrate Anticoagulation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum Berlin, Germany
ACUTE KIDNEY INJURY. Stuart Linas U. Colorado SOM
 ACUTE KIDNEY INJURY Stuart Linas U. Colorado SOM Marked increases in incidence of dialysis-requiring AKI in last decade JASN 24 37 2013 Question 1 Of patients who recover from an episode of AKI, what percentage
ACUTE KIDNEY INJURY Stuart Linas U. Colorado SOM Marked increases in incidence of dialysis-requiring AKI in last decade JASN 24 37 2013 Question 1 Of patients who recover from an episode of AKI, what percentage
PD In Acute Kidney Injury. February 7 th -9 th, 2013
 PD In Acute Kidney Injury February 7 th -9 th, 2013 Objectives PD as a viable initial therapy PD in AKI PD versus dhd PD versus CVVHD Why not PD first PD for AKI Early days (1970 s) PD was the option of
PD In Acute Kidney Injury February 7 th -9 th, 2013 Objectives PD as a viable initial therapy PD in AKI PD versus dhd PD versus CVVHD Why not PD first PD for AKI Early days (1970 s) PD was the option of
CRRT Fundamentals Pre- and Post- Test Answers. AKI & CRRT 2017 Practice Based Learning in CRRT
 CRRT Fundamentals Pre- and Post- Test Answers AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling
CRRT Fundamentals Pre- and Post- Test Answers AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling
CRRT Fundamentals Pre-Test. AKI & CRRT 2017 Practice Based Learning in CRRT
 CRRT Fundamentals Pre-Test AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling at home. He
CRRT Fundamentals Pre-Test AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling at home. He
Acute Kidney Injury. Amandeep Khurana, MD Southwest Kidney Institute
 Acute Kidney Injury Amandeep Khurana, MD Southwest Kidney Institute 66 yr white male w/ DM, HTN, CAD admitted to an OSH w/ E Coli UTI on 7/24/16, developed E Coli bacteremia and Shock (on vaso + levo)
Acute Kidney Injury Amandeep Khurana, MD Southwest Kidney Institute 66 yr white male w/ DM, HTN, CAD admitted to an OSH w/ E Coli UTI on 7/24/16, developed E Coli bacteremia and Shock (on vaso + levo)
Can We Achieve Precision Solute Control with CRRT?
 Can We Achieve Precision Solute Control with CRRT? Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference February, 2019 Disclosures I have no actual or potential
Can We Achieve Precision Solute Control with CRRT? Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference February, 2019 Disclosures I have no actual or potential
Acute Kidney Injury- What Is It and How Do I Treat It?
 Acute Kidney Injury- What Is It and How Do I Treat It? Jayant Kumar, MD Renal Medicine Assoc., Albuquerque, NM Incidence of ARF in ICU Causes of ARF Non -ICU ICU 1 KDIGO criteria for AKI Increase in serum
Acute Kidney Injury- What Is It and How Do I Treat It? Jayant Kumar, MD Renal Medicine Assoc., Albuquerque, NM Incidence of ARF in ICU Causes of ARF Non -ICU ICU 1 KDIGO criteria for AKI Increase in serum
CRRT for the Experience User 1. Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference March, 2018
 CRRT for the Experience User 1 Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference March, 2018 Disclosures I have no actual or potential conflict of interest
CRRT for the Experience User 1 Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference March, 2018 Disclosures I have no actual or potential conflict of interest
Nephrology. 3 rd Year Revision Session 06/05/17 Cathal Hannan
 Nephrology 3 rd Year Revision Session 06/05/17 Cathal Hannan Aims Acute Kidney Injury-recognition and management Sample OSCE Station Clinically relevant renal physiology Aetiology of Chronic Kidney Disease
Nephrology 3 rd Year Revision Session 06/05/17 Cathal Hannan Aims Acute Kidney Injury-recognition and management Sample OSCE Station Clinically relevant renal physiology Aetiology of Chronic Kidney Disease
Update in. Acute Kidney Injury. Mark Devonald Consultant Nephrologist. Nottingham AKI Research Group
 Update in Acute Kidney Injury Mark Devonald Consultant Nephrologist If you stay awake you might hear about Why AKI is important Some cases to illustrate some specific points A couple of updates on AKI
Update in Acute Kidney Injury Mark Devonald Consultant Nephrologist If you stay awake you might hear about Why AKI is important Some cases to illustrate some specific points A couple of updates on AKI
Renal Replacement Therapy in Acute Renal Failure
 CHAPTER 82 Renal Replacement Therapy in Acute Renal Failure R. Deshpande Introduction Acute renal failure (ARF) is defined as an abrupt decrease in renal function sufficient to result in retention of nitrogenous
CHAPTER 82 Renal Replacement Therapy in Acute Renal Failure R. Deshpande Introduction Acute renal failure (ARF) is defined as an abrupt decrease in renal function sufficient to result in retention of nitrogenous
Update in Nephrology. Case: Question 1. Case presentation. Acute Kidney Injury. For her hypertension management, you decide to:
 Update in Nephrology Chronic Kidney Disease Renoprotection and Proteinuria, ACE and/or ARB Anemia management Update in Nephrology Renal artery stenosis Nephrogenic systemic fibrosis Division of Nephrology
Update in Nephrology Chronic Kidney Disease Renoprotection and Proteinuria, ACE and/or ARB Anemia management Update in Nephrology Renal artery stenosis Nephrogenic systemic fibrosis Division of Nephrology
Can We Achieve Precision Solute Control with CRRT?
 Can We Achieve Precision Solute Control with CRRT? Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference February, 2019 Disclosures I have no actual or potential
Can We Achieve Precision Solute Control with CRRT? Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference February, 2019 Disclosures I have no actual or potential
Dialysis Dose Prescription and Delivery. William Clark, M.D. Claudio Ronco, M.D. Rolando Claure-Del Granado, M.D. CRRT Conference February 15, 2012
 Dialysis Dose Prescription and Delivery William Clark, M.D. Claudio Ronco, M.D. Rolando Claure-Del Granado, M.D. CRRT Conference February 15, 2012 Dose in RRT: Key concepts Dose definition Quantifying
Dialysis Dose Prescription and Delivery William Clark, M.D. Claudio Ronco, M.D. Rolando Claure-Del Granado, M.D. CRRT Conference February 15, 2012 Dose in RRT: Key concepts Dose definition Quantifying
Olistic Approach to Treatment Adequacy in AKI
 Toronto - Canada, 2014 Olistic Approach to Treatment Adequacy in AKI Claudio Ronco, MD Department of Nephrology, St. Bortolo Hospital, International Renal Research Institute Vicenza - Italy 1) RRT
Toronto - Canada, 2014 Olistic Approach to Treatment Adequacy in AKI Claudio Ronco, MD Department of Nephrology, St. Bortolo Hospital, International Renal Research Institute Vicenza - Italy 1) RRT
Acute Kidney Injury. Arvind Bagga All India Institute of Medical Sciences New Delhi, India
 Acute Kidney Injury Arvind Bagga All India Institute of Medical Sciences New Delhi, India What is AKI? Sudden loss of renal function, over hrdays, with derangement(s) in fluid balance, acid base & electrolytes
Acute Kidney Injury Arvind Bagga All India Institute of Medical Sciences New Delhi, India What is AKI? Sudden loss of renal function, over hrdays, with derangement(s) in fluid balance, acid base & electrolytes
Acute Kidney Injury in The Acute Oncology Patient
 Acute Kidney Injury in The Acute Oncology Patient Dr Andrew Lewington BSc MEd MD FRCP Consultant Renal Physician/Honorary Senior Lecturer Leeds Teaching Hospitals Definition Definitions and terminology
Acute Kidney Injury in The Acute Oncology Patient Dr Andrew Lewington BSc MEd MD FRCP Consultant Renal Physician/Honorary Senior Lecturer Leeds Teaching Hospitals Definition Definitions and terminology
Recent advances in CRRT
 Recent advances in CRRT JAE IL SHIN, M.D., Ph.D. Department of Pediatrics, Severance Children s Hospital, Yonsei University College of Medicine, Seoul, Korea Pediatric AKI epidemiology and demographics
Recent advances in CRRT JAE IL SHIN, M.D., Ph.D. Department of Pediatrics, Severance Children s Hospital, Yonsei University College of Medicine, Seoul, Korea Pediatric AKI epidemiology and demographics
egfr 34 ml/min egfr 130 ml/min Am J Kidney Dis 2002;39(suppl 1):S17-S31
:S17-S31") Update on Renal Therapeutics Caroline Ashley Lead Pharmacist Renal Services UCL Centre for Nephrology, Royal Free Hospital, London Kongress für Arzneimittelinformation January 2011 What are we going to
Update on Renal Therapeutics Caroline Ashley Lead Pharmacist Renal Services UCL Centre for Nephrology, Royal Free Hospital, London Kongress für Arzneimittelinformation January 2011 What are we going to
Paul R. Bowlin, M.D. University of Colorado Denver. May 12 th, 2008
 Paul R. Bowlin, M.D. University of Colorado Denver May 12 th, 2008 Presentation Overview Background / Definitions History Indications for initiation of therapy Outcomes Studies Conclusions Questions Background
Paul R. Bowlin, M.D. University of Colorado Denver May 12 th, 2008 Presentation Overview Background / Definitions History Indications for initiation of therapy Outcomes Studies Conclusions Questions Background
Renal failure in sepsis and septic shock
 Renal failure in sepsis and septic shock Dr. Venugopal Reddy. MD, EDIC, FCARCSI Associate Professor of Anesthesiology and Critical Care medicine Department of Anaesthesia and CCM Penn State College of
Renal failure in sepsis and septic shock Dr. Venugopal Reddy. MD, EDIC, FCARCSI Associate Professor of Anesthesiology and Critical Care medicine Department of Anaesthesia and CCM Penn State College of
Continuous renal replacement therapy. David Connor
 Continuous renal replacement therapy David Connor Overview Classification of AKI Indications Principles Types of CRRT Controversies RIFL criteria Stage GFR Criteria Urine Output Criteria Risk Baseline
Continuous renal replacement therapy David Connor Overview Classification of AKI Indications Principles Types of CRRT Controversies RIFL criteria Stage GFR Criteria Urine Output Criteria Risk Baseline
Prevention of Acute Renal Failure Role of vasoactive drugs and diuretic agents
 of Acute Renal Failure Role of vasoactive drugs and diuretic agents Armand R.J. Girbes Prof.dr. A.R.J. Girbes Chairman department of Intensive Care VU University Medical Center Netherlands (Failure of)
of Acute Renal Failure Role of vasoactive drugs and diuretic agents Armand R.J. Girbes Prof.dr. A.R.J. Girbes Chairman department of Intensive Care VU University Medical Center Netherlands (Failure of)
Blood purification in sepsis
 Blood purification in sepsis Joannes-Boyau O Dept of anesthesiology and intensive care, University Hospital of Bordeaux, France 1 Types of Blood Purification hemofilters regular pore size (MW < 40,000D)
Blood purification in sepsis Joannes-Boyau O Dept of anesthesiology and intensive care, University Hospital of Bordeaux, France 1 Types of Blood Purification hemofilters regular pore size (MW < 40,000D)
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
When and how to start RRT in critically ill patients? Intensive Care Training Program Radboud University Medical Centre Nijmegen
 When and how to start RRT in critically ill patients? Intensive Care Training Program Radboud University Medical Centre Nijmegen Case history (1) 64 Hypertension 2004 AVR 2009 Paravalvular leak - dilated
When and how to start RRT in critically ill patients? Intensive Care Training Program Radboud University Medical Centre Nijmegen Case history (1) 64 Hypertension 2004 AVR 2009 Paravalvular leak - dilated
MODALITIES of Renal Replacement Therapy in AKI
 MODALITIES of Renal Replacement Therapy in AKI Jorge Cerdá, MD, MS, FACP, FASN Clinical Professor of Medicine Albany Medical College Albany, NY, USA cerdaj@mail.amc.edu In AKI, RRT is a multidimensional
MODALITIES of Renal Replacement Therapy in AKI Jorge Cerdá, MD, MS, FACP, FASN Clinical Professor of Medicine Albany Medical College Albany, NY, USA cerdaj@mail.amc.edu In AKI, RRT is a multidimensional
AKI: definitions, detection & pitfalls. Jon Murray
 AKI: definitions, detection & pitfalls Jon Murray Previous conventional definition Acute renal failure (ARF) An abrupt and sustained decline in renal excretory function due to a reduction in glomerular
AKI: definitions, detection & pitfalls Jon Murray Previous conventional definition Acute renal failure (ARF) An abrupt and sustained decline in renal excretory function due to a reduction in glomerular
Nutrition in Acute Kidney Injury Enrico Fiaccadori
 Nutrition in Acute Kidney Injury Enrico Fiaccadori Nephrology Dept. Parma University Medical School Parma, Italy Diagnosis, epidemiology and prognostic impact of proteinenergy wasting (PEW) in AKI Pathogenetic
Nutrition in Acute Kidney Injury Enrico Fiaccadori Nephrology Dept. Parma University Medical School Parma, Italy Diagnosis, epidemiology and prognostic impact of proteinenergy wasting (PEW) in AKI Pathogenetic
CRRT. ICU Fellowship Training Radboudumc
 CRRT ICU Fellowship Training Radboudumc Timing RRT Consider the following: Underlying cause and reversibility. Rapid improvement unlikely with high dose vasopressors and continuous exposure to other risk
CRRT ICU Fellowship Training Radboudumc Timing RRT Consider the following: Underlying cause and reversibility. Rapid improvement unlikely with high dose vasopressors and continuous exposure to other risk
Dialyzing challenging patients: Patients with hepato-renal conditions
 Dialyzing challenging patients: Patients with hepato-renal conditions Nidyanandh Vadivel MD Medical Director for Living kidney Donor and Pancreas Transplant Programs Swedish Organ Transplant, Seattle Acute
Dialyzing challenging patients: Patients with hepato-renal conditions Nidyanandh Vadivel MD Medical Director for Living kidney Donor and Pancreas Transplant Programs Swedish Organ Transplant, Seattle Acute
CRRT. Sustained low efficiency daily dialysis, SLEDD. Sustained low efficiency daily diafiltration, SLEDD-f. inflammatory cytokine IL-1 IL-6 TNF-
 RRT, renal replacement therapy IHDCRRT CRRT 24 CRRT Sustained low efficiency daily dialysis, SLEDD 6 ~ 12 300 Sustained low efficiency daily diafiltration, SLEDD-f inflammatory cytokine IL-1 IL-6 TNF-
RRT, renal replacement therapy IHDCRRT CRRT 24 CRRT Sustained low efficiency daily dialysis, SLEDD 6 ~ 12 300 Sustained low efficiency daily diafiltration, SLEDD-f inflammatory cytokine IL-1 IL-6 TNF-
The role of the Nephrologist in Acute Kidney Injury. Rebecca Brown Consultant Nephrologist Royal Liverpool University Hospital
 The role of the Nephrologist in Acute Kidney Injury Rebecca Brown Consultant Nephrologist Royal Liverpool University Hospital Overview Impact of AKI Need for change Who needs a Nephrologist Are we making
The role of the Nephrologist in Acute Kidney Injury Rebecca Brown Consultant Nephrologist Royal Liverpool University Hospital Overview Impact of AKI Need for change Who needs a Nephrologist Are we making
Ricky Bell Renal/ICM Registrar
 Ricky Bell Renal/ICM Registrar Objectives When to call renal How to manage the patient with AKI How the manage the patient with CKD (HD/PD) Special AKI situations What do the guidelines say? My referral
Ricky Bell Renal/ICM Registrar Objectives When to call renal How to manage the patient with AKI How the manage the patient with CKD (HD/PD) Special AKI situations What do the guidelines say? My referral
[1] Levy [3] (odds ratio) 5.5. mannitol. (renal dose) dopamine 1 µg/kg/min atrial natriuretic peptide (ANP)
![[1] Levy [3] (odds ratio) 5.5. mannitol. (renal dose) dopamine 1 µg/kg/min atrial natriuretic peptide (ANP)](/thumbs/92/109602349.jpg "[1] Levy [3] (odds ratio) 5.5. mannitol. (renal dose) dopamine 1 µg/kg/min atrial natriuretic peptide (ANP)") [1] Levy [3] 183 174 (odds ratio) 5.5 Woodrow [1] 1956 1989 mannitol (renal dose) dopamine 1 µg/kg/min atrial natriuretic peptide (ANP) McCarthy [2] 1970 1990 insulin-like growth factor-1 (IGF-1) ANP 92
[1] Levy [3] 183 174 (odds ratio) 5.5 Woodrow [1] 1956 1989 mannitol (renal dose) dopamine 1 µg/kg/min atrial natriuretic peptide (ANP) McCarthy [2] 1970 1990 insulin-like growth factor-1 (IGF-1) ANP 92
Implementing therapy-delivery, dose adjustments and fluid balance. Eileen Lischer MA, BSN, RN, CNN University of California San Diego March 6, 2018
 Implementing therapy-delivery, dose adjustments and fluid balance. Eileen Lischer MA, BSN, RN, CNN University of California San Diego March 6, 2018 Objectives By the end of this session the learner will
Implementing therapy-delivery, dose adjustments and fluid balance. Eileen Lischer MA, BSN, RN, CNN University of California San Diego March 6, 2018 Objectives By the end of this session the learner will
Renal Replacement Therapy in ICU. Dr. Sunil Sharma Senior Resident Dept of Pulmonary Medicine
 Renal Replacement Therapy in ICU Dr. Sunil Sharma Senior Resident Dept of Pulmonary Medicine Introduction Need for RRT in patients with ARF is a common & increasing problem in ICUs Leading cause of ARF
Renal Replacement Therapy in ICU Dr. Sunil Sharma Senior Resident Dept of Pulmonary Medicine Introduction Need for RRT in patients with ARF is a common & increasing problem in ICUs Leading cause of ARF
Acute Liver Failure: Supporting Other Organs
 Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Une promenade dans l'épidémiologie de l'insuffisance rénale aiguë en quatre étapes
 Une promenade dans l'épidémiologie de l'insuffisance rénale aiguë en quatre étapes Fernando Liaño Hospital Universitario Ramón y Cajal Madrid, España Genéve, 14-12-2012 Une promenade dans l'épidémiologie
Une promenade dans l'épidémiologie de l'insuffisance rénale aiguë en quatre étapes Fernando Liaño Hospital Universitario Ramón y Cajal Madrid, España Genéve, 14-12-2012 Une promenade dans l'épidémiologie
WEEK. MPharm Programme. Acute Kidney Injury. Alan M. Green MPHM13: Acute Kidney Injury. Slide 1 of 47
 MPharm Programme Acute Kidney Injury Alan M. Green 2017 Slide 1 of 47 Overview Renal Function What is it? Why does it matter? What causes it? Who is at risk? What can we (Pharmacists) do? How do you recognise
MPharm Programme Acute Kidney Injury Alan M. Green 2017 Slide 1 of 47 Overview Renal Function What is it? Why does it matter? What causes it? Who is at risk? What can we (Pharmacists) do? How do you recognise
ESPEN Congress Vienna Nutritional implications of renal replacement therapy in ICU Nutritional consequences of RRT. E. Fiaccadori (Italy)
") ESPEN Congress Vienna 2009 Nutritional implications of renal replacement therapy in ICU Nutritional consequences of RRT E. Fiaccadori (Italy) Nutritional consequences of RRT Enrico Fiaccadori Internal
ESPEN Congress Vienna 2009 Nutritional implications of renal replacement therapy in ICU Nutritional consequences of RRT E. Fiaccadori (Italy) Nutritional consequences of RRT Enrico Fiaccadori Internal
Acute Kidney Injury in Trauma. David Lee Skinner MBChB FCS(SA) Trauma Unit Inkosi Albert Luthuli Central Hospital KwaZulu Natal South Africa
 Trauma Unit Inkosi Albert Luthuli Central Hospital KwaZulu Natal South Africa") Acute Kidney Injury in Trauma David Lee Skinner MBChB FCS(SA) Trauma Unit Inkosi Albert Luthuli Central Hospital KwaZulu Natal South Africa Acute Kidney Injury Acute Renal Failure RIFLE & AKIN RIFLE criteria
Acute Kidney Injury in Trauma David Lee Skinner MBChB FCS(SA) Trauma Unit Inkosi Albert Luthuli Central Hospital KwaZulu Natal South Africa Acute Kidney Injury Acute Renal Failure RIFLE & AKIN RIFLE criteria
Acute Kidney Injury Care in the Chronic Unit
 Acute Kidney Injury Care in the Chronic Unit BONNIE B GREENSPAN WITH ASSIST FROM: DENISE MURCEK, JINA BOGLE, MARY SCHIRA, OCTOBER 5, 2017 Objectives At the completion of the session, engaged participants
Acute Kidney Injury Care in the Chronic Unit BONNIE B GREENSPAN WITH ASSIST FROM: DENISE MURCEK, JINA BOGLE, MARY SCHIRA, OCTOBER 5, 2017 Objectives At the completion of the session, engaged participants
Renal replacement therapy in acute kidney injury
 6 February 2009 CONTENTS Renal replacement therapy in acute kidney injury S Jithoo Commentator: CL Quantock Moderator: LW Drummond INTRODUCTION... 3 WHAT IS RENAL REPLACEMENT THERAPY?... 3 MODES OF RENAL
6 February 2009 CONTENTS Renal replacement therapy in acute kidney injury S Jithoo Commentator: CL Quantock Moderator: LW Drummond INTRODUCTION... 3 WHAT IS RENAL REPLACEMENT THERAPY?... 3 MODES OF RENAL
RCP : Regional Update in Medicine Acute Kidney Injury : A Renal Problem?
 RCP : Regional Update in Medicine Acute Kidney Injury : A Renal Problem? Lui G Forni : Consultant Intensivist & Nephrologist Faculty of Health Sciences : University of Surrey Disclosures Research Funding
RCP : Regional Update in Medicine Acute Kidney Injury : A Renal Problem? Lui G Forni : Consultant Intensivist & Nephrologist Faculty of Health Sciences : University of Surrey Disclosures Research Funding
Pediatric Continuous Renal Replacement Therapy
 Pediatric Continuous Renal Replacement Therapy Farahnak Assadi Fatemeh Ghane Sharbaf Pediatric Continuous Renal Replacement Therapy Principles and Practice Farahnak Assadi, M.D. Professor Emeritus Department
Pediatric Continuous Renal Replacement Therapy Farahnak Assadi Fatemeh Ghane Sharbaf Pediatric Continuous Renal Replacement Therapy Principles and Practice Farahnak Assadi, M.D. Professor Emeritus Department
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
Competency assessment in CRRT core curriculum. G07
 Competency assessment in CRRT core curriculum. G07 San Diego 2011 Hilton Bayfront Ian Baldwin R.N. PhD. Austin Hospital RMIT University Australia Heamofiltration Continuous Renal Replacement Therapy (CRRT)
Competency assessment in CRRT core curriculum. G07 San Diego 2011 Hilton Bayfront Ian Baldwin R.N. PhD. Austin Hospital RMIT University Australia Heamofiltration Continuous Renal Replacement Therapy (CRRT)
Preven'ng AKI. Lessons from Contrast-associated AKI It s all about urine output
 Preven'ng AKI Lessons from Contrast-associated AKI It s all about urine output CASE A 76 y/o male comes to the ED complaining of substernal crushing chest pain. The pain started a few hours ago while he
Preven'ng AKI Lessons from Contrast-associated AKI It s all about urine output CASE A 76 y/o male comes to the ED complaining of substernal crushing chest pain. The pain started a few hours ago while he
UNDERSTANDING THE CRRT MACHINE
 UNDERSTANDING THE CRRT MACHINE Helen Dickie Renal Sister Critical Care Unit Guy s and St.Thomas NHS Foundation Trust 18.10.14 RRT options - IHD vs CRRT (1) Intermittent HaemoDialysis e.g. 4hrs daily or
UNDERSTANDING THE CRRT MACHINE Helen Dickie Renal Sister Critical Care Unit Guy s and St.Thomas NHS Foundation Trust 18.10.14 RRT options - IHD vs CRRT (1) Intermittent HaemoDialysis e.g. 4hrs daily or
Acute kidney injury (AKI), previously
, previously") Concise Definitive Review Jonathan E. Sevransky, MD, MHS, Section Editor Acute kidney injury in the intensive care unit: An update and primer for the intensivist Paula Dennen, MD; Ivor S. Douglas, MD;
Concise Definitive Review Jonathan E. Sevransky, MD, MHS, Section Editor Acute kidney injury in the intensive care unit: An update and primer for the intensivist Paula Dennen, MD; Ivor S. Douglas, MD;
NO ADDED MORTALITY BENEFIT FROM CURRENT APPROACHES TO RENAL REPLACEMENT THERAPY IN ICU PATIENTS
 NO ADDED MORTALITY BENEFIT FROM CURRENT APPROACHES TO RENAL REPLACEMENT THERAPY IN ICU PATIENTS *Helmut Schiffl Department of Internal Medicine IV, University Hospital Munich, Munich, Germany *Correspondence
NO ADDED MORTALITY BENEFIT FROM CURRENT APPROACHES TO RENAL REPLACEMENT THERAPY IN ICU PATIENTS *Helmut Schiffl Department of Internal Medicine IV, University Hospital Munich, Munich, Germany *Correspondence
HHS. Hyperglycaemic Hyperosmolar State Care Pathway 1 Presenta8on to 6 hours. Page 1 of 2 AFFIX PATIENT LABEL ! INFORM DIABETES TEAM OF ADMISSION!
 Hyperglycaemic Hyperosmolar State Care Pathway 1 Presenta8on to 6 hours Page 1 of 2 Time of Arrival Loca8on Date / / Diagnosis the characteris8c features of a person with HHS are a) Hypovolaemia b) Marked
Hyperglycaemic Hyperosmolar State Care Pathway 1 Presenta8on to 6 hours Page 1 of 2 Time of Arrival Loca8on Date / / Diagnosis the characteris8c features of a person with HHS are a) Hypovolaemia b) Marked
PICANet Custom Audit Definitions Renal Dataset
 PICANet Custom Audit s Renal Dataset Version 1.0 (July 2016) PICANet Renal Custom Audit Data s Manual Version 1.0 July 2016 Renal Dataset Contents PICANet Custom Audit s... 1 Renal Dataset... 1 Version
PICANet Custom Audit s Renal Dataset Version 1.0 (July 2016) PICANet Renal Custom Audit Data s Manual Version 1.0 July 2016 Renal Dataset Contents PICANet Custom Audit s... 1 Renal Dataset... 1 Version
Acute Kidney Injury in the ED
 + Acute Kidney Injury in the ED + Dr Eric Clark, MD FRCPC University of Ottawa Canada Canadian Association of Emergency Physicians + Outline 1. Diagnostic challenges 2. ED treatment 3. Contrast induced
+ Acute Kidney Injury in the ED + Dr Eric Clark, MD FRCPC University of Ottawa Canada Canadian Association of Emergency Physicians + Outline 1. Diagnostic challenges 2. ED treatment 3. Contrast induced
Caring for the AKI Survivor: What is Required?
 Caring for the AKI Survivor: What is Required? Ron Wald, MDCM MPH FRCPC Division of Nephrology St. Michael s Hospital and University of Toronto February 28, 2019 A patient in your ICU 65M with DM, HTN,
Caring for the AKI Survivor: What is Required? Ron Wald, MDCM MPH FRCPC Division of Nephrology St. Michael s Hospital and University of Toronto February 28, 2019 A patient in your ICU 65M with DM, HTN,
Large RCT s s in RRT : What can be learnt for nursing?
 Large RCT s s in RRT : What can be learnt for nursing? Ian Baldwin Dept. of Intensive Care, Austin Hospital Adjunct Professor, RMIT University CRRT 2011 Hilton Bayfront, February 22-25 SanDiego Key Hypothesis
Large RCT s s in RRT : What can be learnt for nursing? Ian Baldwin Dept. of Intensive Care, Austin Hospital Adjunct Professor, RMIT University CRRT 2011 Hilton Bayfront, February 22-25 SanDiego Key Hypothesis
Las dos caras de la cretinina sérica The two sides of serum creatinine
 Las dos caras de la cretinina sérica The two sides of serum creatinine ASOCIACION COSTARRICENSE DE MEDICINA INTERNA San José, Costa Rica June 2017 Kianoush B. Kashani, MD, MSc, FASN, FCCP 2013 MFMER 3322132-1
Las dos caras de la cretinina sérica The two sides of serum creatinine ASOCIACION COSTARRICENSE DE MEDICINA INTERNA San José, Costa Rica June 2017 Kianoush B. Kashani, MD, MSc, FASN, FCCP 2013 MFMER 3322132-1
The changing face of
 The changing face of sepsis. @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser (maternal sepsis) to WHO Breast cancer Cognitive impairment Mild 3.8 7.1
The changing face of sepsis. @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser (maternal sepsis) to WHO Breast cancer Cognitive impairment Mild 3.8 7.1
decline in kidney function within 90 days Drug treatment: NAC NCT IV UK Recruiting (6/2012) NAC Coronary angiography in healthy
 NAC Coronary angiography in healthy") Identifier Phase Location Status (estimated 2x2 factorial design NCT01467466 III USA Not yet recruiting (4/2015) NAC vs. placebo and Intervention Setting Kidney outcome measures Estimated Coronary and
Identifier Phase Location Status (estimated 2x2 factorial design NCT01467466 III USA Not yet recruiting (4/2015) NAC vs. placebo and Intervention Setting Kidney outcome measures Estimated Coronary and
Drug dosing in patients with acute kidney injury
 Drug dosing in patients with acute kidney injury They don t know what they are doing Jan Jan T. T. Kielstein Department of of Nephrology and and Hypertension Medical School School Hannover Drug dosing
Drug dosing in patients with acute kidney injury They don t know what they are doing Jan Jan T. T. Kielstein Department of of Nephrology and and Hypertension Medical School School Hannover Drug dosing
Acute Kidney Injury State of the art
 Acute Kidney Injury State of the art JM. Hougardy, MD, PhD Nephrology, Dialysis & Renal transplanta@on ULB Hôpital Erasme Joint Mee@ng SBN---BVN/BeSEDiM, 24th October 2013, UCL, Brussels The normal kidney
Acute Kidney Injury State of the art JM. Hougardy, MD, PhD Nephrology, Dialysis & Renal transplanta@on ULB Hôpital Erasme Joint Mee@ng SBN---BVN/BeSEDiM, 24th October 2013, UCL, Brussels The normal kidney
SAFETY IN THE CATH LAB How to Minimise Contrast Toxicity
 SAFETY IN THE CATH LAB How to Minimise Contrast Toxicity Dr. Vijay Kunadian MBBS, MD, MRCP Senior Lecturer and Consultant Interventional Cardiologist Institute of Cellular Medicine, Faculty of Medical
SAFETY IN THE CATH LAB How to Minimise Contrast Toxicity Dr. Vijay Kunadian MBBS, MD, MRCP Senior Lecturer and Consultant Interventional Cardiologist Institute of Cellular Medicine, Faculty of Medical
Acute Kidney Injury. I. David Weiner, M.D. Division of Nephrology, Hypertension and Transplantation University of Florida and NF/SGVHS
 Acute Kidney Injury I. David Weiner, M.D. Division of Nephrology, Hypertension and Transplantation University of Florida and NF/SGVHS 374-6102 David.Weiner@medicine.ufl.edu www.renallectures.com Concentration
Acute Kidney Injury I. David Weiner, M.D. Division of Nephrology, Hypertension and Transplantation University of Florida and NF/SGVHS 374-6102 David.Weiner@medicine.ufl.edu www.renallectures.com Concentration
Evidence-based practice in nephrology : Meta-analysis
 Evidence-based practice in nephrology : Meta-analysis Paweena Susantitaphong, MD,Ph.D 1-3 1 Associate Professor, Division of Nephrology, Department of Medicine, King Chulalongkorn Memorial Hospital, Chulalongkorn
Evidence-based practice in nephrology : Meta-analysis Paweena Susantitaphong, MD,Ph.D 1-3 1 Associate Professor, Division of Nephrology, Department of Medicine, King Chulalongkorn Memorial Hospital, Chulalongkorn
Ruolo della clinica e del laboratorio nella diagnosi di IRA
 Ruolo della clinica e del laboratorio nella diagnosi di IRA Antonio Granata Ospedale San Giovanni di Dio - Agrigento Scuola Nazionale Specialistica di Ecografia Nefrologica SIUMB Centro di Riferimento
Ruolo della clinica e del laboratorio nella diagnosi di IRA Antonio Granata Ospedale San Giovanni di Dio - Agrigento Scuola Nazionale Specialistica di Ecografia Nefrologica SIUMB Centro di Riferimento
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Initiation Strategies for Renal Replacement Therapy in ICU
 Initiation Strategies for Renal Replacement Therapy in ICU The Artificial Kidney Initiation in Kidney Injury trial AKIKI Stéphane Gaudry Réanimation médico-chirurgicale Hôpital Louis Mourier, Colombes
Initiation Strategies for Renal Replacement Therapy in ICU The Artificial Kidney Initiation in Kidney Injury trial AKIKI Stéphane Gaudry Réanimation médico-chirurgicale Hôpital Louis Mourier, Colombes
CKD and risk management : NICE guideline
 CKD and risk management : NICE guideline 2008-2014 Shahed Ahmed Consultant Nephrologist shahed.ahmed@rlbuht.nhs.uk Key points : Changing parameters of CKD and NICE guidance CKD and age related change of
CKD and risk management : NICE guideline 2008-2014 Shahed Ahmed Consultant Nephrologist shahed.ahmed@rlbuht.nhs.uk Key points : Changing parameters of CKD and NICE guidance CKD and age related change of
Objectives. Peritoneal Dialysis vs. Hemodialysis 02/27/2018. Peritoneal Dialysis Prescription and Adequacy Monitoring
 Peritoneal Dialysis Prescription and Adequacy Monitoring Christine B. Sethna, MD, EdM Division Director, Pediatric Nephrology Cohen Children s Medical Center Associate Professor Hofstra Northwell School
Peritoneal Dialysis Prescription and Adequacy Monitoring Christine B. Sethna, MD, EdM Division Director, Pediatric Nephrology Cohen Children s Medical Center Associate Professor Hofstra Northwell School
SUPPLEMENTARY INFORMATION
 Supplementary information S1 Studies of the effect of AKI duration on outcomes Study Study group (n) Criteria for AKI Definition of RR Outcomes Uchino et al. All patients admitted to (2010) 1 a university-affiliated
Supplementary information S1 Studies of the effect of AKI duration on outcomes Study Study group (n) Criteria for AKI Definition of RR Outcomes Uchino et al. All patients admitted to (2010) 1 a university-affiliated
Prof Patrick Honoré,MD, PhD,FCCM Intensivist-Nephrologist
 Pro-Con Debate on High Volume Hemofiltration :Burial or Ressurection? The Pro Position 1.-Why Moving From Dose To Membranes? 4.-AN69 Oxiris LPS Adsorptive Membranes in Sepsis 2.- High Cut-Off Membranes
Pro-Con Debate on High Volume Hemofiltration :Burial or Ressurection? The Pro Position 1.-Why Moving From Dose To Membranes? 4.-AN69 Oxiris LPS Adsorptive Membranes in Sepsis 2.- High Cut-Off Membranes
Managing Acid Base and Electrolyte Disturbances with RRT
 Managing Acid Base and Electrolyte Disturbances with RRT John R Prowle MA MSc MD MRCP FFICM Consultant in Intensive Care & Renal Medicine RRT for Regulation of Acid-base and Electrolyte Acid base load
Managing Acid Base and Electrolyte Disturbances with RRT John R Prowle MA MSc MD MRCP FFICM Consultant in Intensive Care & Renal Medicine RRT for Regulation of Acid-base and Electrolyte Acid base load
PICANet Custom Audit Definitions Renal Dataset
 PICANet Custom Audit s Renal Dataset Version 2.0 (March 2017) PICANet Renal Custom Audit Data s Manual Version 2.0 29/03/2017 Renal Dataset Contents PICANet Custom Audit s... 1 Renal Dataset... 1 Version
PICANet Custom Audit s Renal Dataset Version 2.0 (March 2017) PICANet Renal Custom Audit Data s Manual Version 2.0 29/03/2017 Renal Dataset Contents PICANet Custom Audit s... 1 Renal Dataset... 1 Version
CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018
 CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018 Case 1 Potassium Clearance A 70 kg male is placed on CVVH with a total ultrafiltration rate (effluent rate) of 20 ml/kg/hr. The Blood Flow
CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018 Case 1 Potassium Clearance A 70 kg male is placed on CVVH with a total ultrafiltration rate (effluent rate) of 20 ml/kg/hr. The Blood Flow
CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018
 CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018 Case 1 Potassium Clearance A 70 kg male is placed on CVVH with a total ultrafiltration rate (effluent rate) of 20 ml/kg/hr. The Blood Flow
CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018 Case 1 Potassium Clearance A 70 kg male is placed on CVVH with a total ultrafiltration rate (effluent rate) of 20 ml/kg/hr. The Blood Flow
ACUTE KIDNEY INJURY FOCUS ON OBSTETRICS DONNA HIGGINS, CLINICAL NURSE EDUCATOR, NORTHERN LINCOLNSHIRE HOSPITALS NHS FOUNDATION TRUST
 ACUTE KIDNEY INJURY FOCUS ON OBSTETRICS DONNA HIGGINS, CLINICAL NURSE EDUCATOR, NORTHERN LINCOLNSHIRE HOSPITALS NHS FOUNDATION TRUST AIMS & OBJECTIVES Review the functions of the kidney Identify renal
ACUTE KIDNEY INJURY FOCUS ON OBSTETRICS DONNA HIGGINS, CLINICAL NURSE EDUCATOR, NORTHERN LINCOLNSHIRE HOSPITALS NHS FOUNDATION TRUST AIMS & OBJECTIVES Review the functions of the kidney Identify renal
Bedside assessment of fluid status
 Bedside assessment of fluid status 2nd AKI Academy October 18 th 2014 David Treacher Guy s & St Thomas NHS Trust Assessing the circulation - the 3 key questions v Is my patient adequately filled? v What
Bedside assessment of fluid status 2nd AKI Academy October 18 th 2014 David Treacher Guy s & St Thomas NHS Trust Assessing the circulation - the 3 key questions v Is my patient adequately filled? v What