What Have We Learned: Selection for Endovascular Stroke Therapy
|
|
|
- Mariah Boyd
- 6 years ago
- Views:
Transcription





1 What Have We Learned: Selection for Endovascular Stroke Therapy Raul G Nogueira, MD Associate Professor in Neurology, Neurosurgery, and Radiology Emory University Director, Neuroendovascular Service Director, Neurocritical Care Service Grady Memorial Hospital Atlanta, GA
2 Disclosures: Stryker Neurovacular/ Concentric Medical Trevo-2 Trial PI, DAWN Trial PI Physician Advisory Committee Covidien/ ev3 Neurovacular SWIFT and SWIFT-PRIME Trial Steering Committee STAR Trial Core Lab, Physician Advisory Committee, Onyx Proctor Penumbra 3-D Separator Trial Executive Committee Coaxia Physician Advisory Committee Rapid Medical Physician Advisory Committee, Consultant
3 Acute Reperfusion Therapy Patient Selection
4 Patient Selection: Proximal Arterial Occlusion Significant Clinical Deficit Limited Infarct Core Age vs. Functional Status Time to Treatment? Safety data (PROACT-II, MERCI, Multi MERCI, Penumbra trials) for < 8 hours from onset Advanced Imaging (MRI or CTP) for > 8 hours, unknown time of onset, and wake-up strokes currently under investigation in the DAWN Trial Vertebrobasilar occlusion with severe deficits: just do it!
5 Imaging Selection and Core
6 Mismatch vs. Penumbra: Basic Concepts hypoperfused tissue infarct core vessel occlusion Mismatch tissue at risk

7 Mismatch vs. Penumbra: A Word of Caution DREAM REALITY Penumbra equals not only regions of DWI-PWI mismatch but also a portion of the DWI abnormality itself. PWI includes areas of benign oligemia. Kidwell CS, et al. Stroke. 2003;34(11): Copyright 2003 American Heart Association, Inc.
8 Imaging Selection Menu: Infarct Core Estimation: Non-Contrast CT ASPECTS Fast Less Reliable Higher Inter-Rater Variability Poor correlation with Infarct Volumes CTA-SI ASPECTS Easier but may overestimate core Yoo AJ et al. J Neuroimaging Oct;22(4): CTA Collaterals Menon B et al. AJNR Am J Neuroradiol 2011;32: CTA Collaterals CALGARY CT Perfusion Core rcbf<30% (RAPID) DWI Core Gold Standard second only to PET SPEED ACCURACY
9 Imaging Selection Menu: Penumbra Estimation Perfusion Imaging Tmax >4 sec = Benign Oligemia Tmax >6 sec= Penumbra Tmax >10 sec = Critical Penumbra/ Imminent Core Clinical Core Mismatch bnihss 8 and DWI volume 25cc Davalos et al. Neurology Jun 22;62(12): DAWN a cc core infarct and NIHSS 10 (and age 80 years old) b cc core infarct and NIHSS 10 (and age < 80 years old) c. 31 cc to < 50 cc core infarct and NIHSS 20 (and age < 80 years old
10 Why I Use CT? Advantages Available Fast Quantitative Low cost Accurate CTA But CT Perfusion is Good Enough! Disadvantages Contrast limits over 1st 24-hrs Radiation risk minimal Variable coverage DWI more sensitive for core Lacunes, small emboli Straka M. ISC 2012








11 RAPID Processing Stroke MRI/CTP 00:00:30 image arrival RAPID 00:05:00 Images on PACS 00:04:30 RAPID image analysis complete CT/MR tech pushes CTP/DWI & PWI to RAPID via DICOM Mini Computer PACS auto-send via DICOM auto-send via secure Auto Image Analysis: motion & time correction AIF & VOF selection deconvolution & map generation CTP or DWI and PWI lesion segmentation Lesion volume calculation

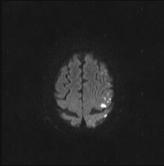
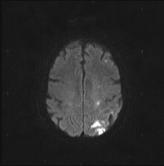
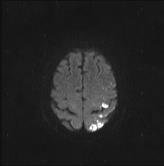
12 83 yo Man NIHSS 14 CTA Right M2 Cutoff Not IV TPA Candidate Patient/Family Declined IAT RAPID: Prediction of Core and Penumbra





13 RAPID: Lack of Reperfusion and Core Progression in to Predicted Penumbra Penumbra: Core Progression: Pre-Rx CTP Tmax Post-DWI >6 secs
14 How Much is Too Much (Infarct Core)? It depends on our goals: Functional Independence (90-day mrs 0-2): ASPECTS >7 (Hill et al., Stroke 2003) Volume <30-40 ml (less if age >80) (Zaidi S, Nogueira RG, Jovin TG et al. Stroke.2013) Little chance if Volume > 70 ml (Yoo AJ et al, Stroke 2009) mrs Shift every ml brain volume likely matters ASPECTS 5-7 likely reasonable Volumes ml likely reasonable Prevent hemicraniectomy or death Can we carefully consider Volumes >100 ml/ >1/3 MCA Territory? The risks is SICH/Edema >100 ML (Albers GW et al, Ann Neurol 2006)
 similar in IAT vs. Medical. IAT: mtici 2B=67%; ICH: Symptomatic=10%; Asymptomatic=36% IAT 90-day Outcomes: mrs 2=20%; mrs 3=33%; Death=43% Successful IAT reperfusion = smaller FIV (p=0.")
15 Endovascular Therapy in ASPECTS 5-7 LVOS with ASPECTS 5-7 treated with IAT (n=86) or medical therapy alone (± IV t-pa; n=15) at two centers from Age (67±14 vs. 67±19yrs) and bnihss (20±5 vs. 20±6) similar in IAT vs. Medical. IAT: mtici 2B=67%; ICH: Symptomatic=10%; Asymptomatic=36% IAT 90-day Outcomes: mrs 2=20%; mrs 3=33%; Death=43% Successful IAT reperfusion = smaller FIV (p=0.015) and higher rates of good (p=0.02) and acceptable (p=0.03) outcomes. Strong trend towards a higher hemicraniectomy requirement in medical vs. endovascular pts (20% vs. 6%, p=0.06) despite similar in-hospital mortality. Median FIV significant lower with IAT vs. medical therapy (80ml[IQR, ] vs. 190ml[ ], p=0.015). A P=0.07 B P=0.1 C P=0.02 D P=0.015 N=6 N=21 N=42 N= N=15 80 N=81

16 Basilar Occlusion, Core, and Outcomes Full Functional Independence Following Endovascular Treatment for Basilar Artery Occlusion Despite Extensive Bilateral Pontine Infarcts on DWI: Refuting at Sell-Fulfilling Prophecy. 3 out of 40 BAO pts who had extensive bilateral pontine DWI changes and achieved 90-day mrs 0-2 Patient #1: 18 year-old man with embolic BAO due to a PFO. 90- day mrs=0 Patients #2 (age 73) and #3 (age 56) had atherosclerotic occlusions that required adjunctive intracranial stenting and angioplasty, respectively. 90-day mrs 1 and 2, respectively
17 Thrombectomy and Age





18 Thrombectomy in the Elderly: 91y/o female; NIHSS: 23 ; S/p Full IV dose rt-pa Post Merci L6 x k u of UK TICI 3 Recanalization 90-day mrs:0 Raul Nogueira, MD MGH, Boston
19 OCTOGENERIANS POOLED ANALYSIS MERCI/MULTIMERCI/REGISTRY N=233 90d Outcomes All Pts (n= 233) Nogueira RG, ISC 2010 Revasc (n= 171) Non-Revasc (n= 62) mrs % (40/231) 22.9% (39/170) 1.6% (1/61) p< mrs % (128/232) 47.4% (81/ 171) 77.0% (47/ 61) p< However, age is an imperfect surrogate of functional status Age = Population Functional Status = Your Patient!
20 IAT in the Elderly Revisited: Single Center 102 Consecutive IAT for pts 80 yrs - Sept.2010-Sept.2014 Age: 84.8 yrs (80-100) bnihss: 19.2 (4-33) ASPECTS 7: 58% Control pts 80 yrs: IST-3 trial: 6-month death/dependency = 75% if bnihss 6-14 and >95% if bnihss 15. IV tpa pts 80 yrs: SITS-ISTR/VISTA (n=2235; bnihss, 14): >2/3 dead/dependent at 3-months. IST-3: 72.7% dead/dependent at 6-months.
21 IAT in the Elderly Revisited: Hypothetical Outcomes in Young vs. Elderly: Absolute Benefit vs. Treatment Effect Size Treatment Control <80 years 80 years
22 IAT in the Elderly Revisited: Post-IAT outcomes in pts >80 years is undoubtfully worse vs. younger pts. However, given the extremely poor natural history of non-reperfused LVOS in the elderly it is likely that IAT has a larger treatment effect size in patients >80 years than in any other age group. Most of the currently published data is based on uncontrolled case series and have inadequately used absolute outcomes rather than treatment effect size as the metric to measure IAT success in the elderly. MR CLEAN trial: pts >80 yrs had twice the treatment effect of the younger patients (acor %CI[ ] vs. acor CI[ ]). If compared to historical controls from the SITS-ISTR/VISTA and IST-3 trials our IAT data is similarly suggestive of a high treatment effect in the elderly patient despite overall worse outcomes when compared to younger patients.
23 Refining the Therapeutic Window for Acute Reperfusion Therapy





:")
:")



24 Collaterals vs. Time: 69 y/o F NIHSS: 23 Head CTA/Head CT 67 y/o F NIHSS: 20 Head CTA/Brain MRI Time to Reperfusion (TICI 3): <3h Time to Reperfusion (TICI 2b): >12h 90-Day mrs: 4 90-Day mrs: 2 (NIHSS: 4) Post-Rx CT Post-Rx MRI
25 Different Brains Have Different Time Profiles! The pace of stroke progression appears to be highly variable and is likely dependent of multiple factors other than the duration and intensity of ischemia including: Collateral flow (via Circle of Willis and/or leptomeningeal collaterals) Ischemic preconditioning Cerebral perfusion pressure Cerebral blood volume Serum glucose S t r o k e V o l u m e Body temperature Oxygen delivery capacity Time


26 How Variable is the Infarct Growth Rate? In patients experiencing a typical large vessel acute ischemic stroke, 120 million neurons are lost each hour. Jeff Saver, 2006 Saver Time Is Brain Quantified. Stroke. 2006;37(1):10.
 and 63 (46.")
27 Temporal Distribution of Stroke Volumes and Clinical-Diffusion Mismatch in Proximal Arterial Occlusions 132 consecutive pts with bnihss 8 + PAO + DWI 8 hours from stroke onset: Age, 66±16.8 years; 57% females; Baseline NIHSS 17.5±5.3; Occlusion site: MCA-M1: 64% Intracranial-ICA: 29% Tandem, 5% TSO to DWI, 269.5± min DWI volume: 46.7±54.8 cc (range, ) and 63 (46.7%) patients had Clinical-DWI Mismatch No significant changes in age, gender, bnihss, or occlusion site amongst the different time quartiles. Median infarct volume (cc) increased (quartile #1=8.5; #2=30.1; #3=38.5; #4=29.4) and the chances of having a CDM decreased (p<0.0001) across the different time quartiles. Poor correlation between DWI volume and TSO to MRI (R-square=0.031, Figure) Significant proportion of the patients still had a CDM at later time epochs: #1=91.1%[20/22]; #2=47.8%[11/23]; #3=34.4% [21/61]; #4=42.3%[11/26]). Nogueira RG et al. ISC 2012
28 Baseline DWI Volume (ml) 230 Initial DWI Growth Rate in DEFUSE 2 Patients with M1 Occlusions Time between Symptom Onset and Baseline MRI (hrs)

29 Baseline DWI Volume (ml) 230 Initial DWI Growth Rate in DEFUSE 2 Patients with M1 Occlusions Time between Symptom Onset and Baseline MRI (hrs)

30 Baseline DWI Volume (ml) 230 Initial DWI Growth Rate in DEFUSE 2 Patients with M1 Occlusions Time between Symptom Onset and Baseline MRI (hrs)









31 Oct/31/2014: Acute Left MCA-M1 Occlusion: Age 74 NIHSS 26 Stroke Onset: 3PM - IV tpa: 4:48PM - CTP:4:53PM No IAT Baseline CTP -1st Slab Baseline NCCT CTA-SI CTA-MIPS Early Time but Poor Collaterals Follow-up DWI Baseline CTP -2 nd Slab = Poor Outcome FAST PROGRESSOR!

32 Oct/31/2014: Acute Left MCA-M1 Occlusion: Age 74 NIHSS 26 Stroke Onset: 3PM - IV tpa: 4:48PM - CTP:4:53PM No IAT Tmax MAPS = Collateral Strength = Time to Reperfuse




33 Oct/31/2014: Acute Left MCA-M1 Occlusion: Age 75 NIHSS 24 Last Seen Well: 8PM No IV tpa - CTP: 11:40AM IAT: 11:55AM Baseline CTP -1st Slab Baseline NCCT CTA-SI CTA-MIPS Late Time but Good Collaterals Follow-up DWI Baseline CTP -2 nd Slab = Good Outcome SLOW PROGRESSOR!
34 Oct/31/2014: Acute Left MCA-M1 Occlusion: Age 75 NIHSS 24 Last Seen Well: 8PM No IV tpa - CTP: 11:40AM IAT: 11:55AM Tmax MAPS = Collateral Strength = Time to Reperfuse


35 Oct/31/2014: Acute Left MCA-M1 Occlusion: Age 75 NIHSS 24 Last Seen Well: 8PM No IV tpa - CTP: 11:40AM IAT: 11:55AM IAT: 9F BCG + PTAS + 1 Pass Stentriever with Navien 072
36 DEFUSE 2 - Target Mismatch 90-days mrs 0 to 2 3 to 4 5 to 6 Reperfusion 6h R+ (N=22) 59% 27% 14% < 6 hours No reperfusion 6h R- (N=14) N=14 29% 29% 43% Reperfusion >6h R+ (N=24) 54% 29% 17% > 6 hours No reperfusion >6h R- (N=18) N=18 33% 28% 39%
37 DEFUSE 2 Lesion Growth Target Mismatch With Reperfusion <6 hrs >6 hrs (N=20) (N=22) Median Growth; ml (IQR) 41 (2-73) 26 (7-67) * 5 day FLAIR volume baseline DWI volume
38 DEFUSE 2 Lesion Growth Late Treated Patients Target Mismatch >6 hrs Median Growth; ml (IQR) Reperfusion (N=22) No Reperfusion (N=14) 26 (7-67) 108 (45-185) p=0.005 * 5 day FLAIR volume baseline DWI volume

39 Time, Stroke Severity, Penunbral Tissue and Collaterals OUTCOMES = COLLATERALS TIME
40 It's a beautiful day Skeptics fall, you feel like It's a beautiful day Don't let that clot get away Thanks to the MR CLEAN, ESCAPE, SWIFT PRIME, THERAPY, REVASCAT, EXTEND- IA, THRACE Investigators and above all the Patients! It is the DAWN of a New Era!

41 Regeneracion, Pasajes Neuronales, 2006 Thank you for your attention!
42 The Future of Imaging for Endovascular Stroke Therapy
:567-74 Time to Treatment = Basal Ganglia ICH 11% RR for every 10-min delay Raychev R et al. ISC 2012")
43 Outcomes After Reperfusion Outcomes = Collaterals Time Time to Reperfusion = Good Clinical Outcome 12% RR for every 30-min delay Khatri P et al. Lancet Neurol. 2014;13(6): Time to Treatment = Basal Ganglia ICH 11% RR for every 10-min delay Raychev R et al. ISC 2012





44 Opportunities to Shorten Times To Reperfusion: IMS-III Time Intervals We have to bypass the Emergency Room and CT Suite!! Goyal M et al. Circulation. 2014;130:





45 Why We Will Be Able Bypass the Emergency Room and CT Suite?



46 Why We Will Be Able Bypass the Emergency Room and CT Suite? Conventional CTP-CBV Flat detectorparenchymal blood volume (FD-PBV)

47 Reperfusion Therapy: Refining Time is Brain? Lost per minute Neurons: 1.9 x 10 6 Synapses: 14 x 10 9 Myelin fibers: 7.5 miles Saver JL, Stroke 2006; 37: NEJM Feb 2006: del Zoppo Time is Brain but.. variations according to: 1. Level of Occlusion 2. Individual Anatomy and Physiology (Collaterals)
48 Level of Occlusion vs. Time




49 Level of Occlusion vs. Time: We have known that different levels of occlusion deserve different pathophysiological and therapeutic considerations for a long time We have just decided to neglect this concept in stroke patients NSTEMI STEMI Distal Occlusion or Lacunar Stroke Proximal Occlusion Stroke
 IA treated pts (bnihss 17-20) IV thrombolysis patients Lacunes Distal Occlusions Proximal Occlusions Large role")
50 Level of Occlusion vs. Time: Time to Treatment Time to Reperfusion IV thrombolysis pts (bnihss 10-14) IA treated pts (bnihss 17-20) IV thrombolysis patients Lacunes Distal Occlusions Proximal Occlusions Large role for collateral flow Limited role for collateral flow No role for collateral flow Hacke W et al. Lancet. 2004;363(9411): IA thrombolysis patients Proximal Occlusions

51 Level of Occlusion vs. Time: Proximal Arterial Occlusion Non-Proximal Arterial Occlusion Copen WA et al., Radiology 2008 The rate of infarct growth appears to be dependent on the level of arterial occlusion Collateral flow stabilizes the penumbral tissue!
52 Pathophysiological Considerations in Large Vessel Occlusion

53 Physiology Time is Brain is Brain Cerebral Blood Flow Thresholds CBF ml / 100 gm / min Normal Penumbra = Ischemia - Infarction Penumbra = NIHSS - CT/MR image Penumbra = Clinical-Core Mismatch Hypoperfusion Oligemia Ischemia Penumbra Infarction Modified from W.T.Yuh and others
54 Physiology is Brain CBF CBV OEF S t r o k e V o l u m e Fast Growth: Autoregulation Failure Slow Growth: Collateral Failure Time Nogueira RG, AAN 2010
55 Individual Anatomy and Physiology vs. Time Time Window vs. Tissue Window
Opening the Window for Stroke Intervention How Far Can We Go?
 Opening the Window for Stroke Intervention How Far Can We Go? Raul G Nogueira, MD Associate Professor in Neurology, Neurosurgery, and Radiology Emory University Director, Neuroendovascular Service Grady
Opening the Window for Stroke Intervention How Far Can We Go? Raul G Nogueira, MD Associate Professor in Neurology, Neurosurgery, and Radiology Emory University Director, Neuroendovascular Service Grady
Broadening the Stroke Window in Light of the DAWN Trial
 Broadening the Stroke Window in Light of the DAWN Trial South Jersey Neurovascular and Stroke Symposium April 26, 2018 Rohan Chitale, MD Assistant Professor of Neurological Surgery Vanderbilt University
Broadening the Stroke Window in Light of the DAWN Trial South Jersey Neurovascular and Stroke Symposium April 26, 2018 Rohan Chitale, MD Assistant Professor of Neurological Surgery Vanderbilt University
The DAWN of a New Era for Wake-up Stroke
 The DAWN of a New Era for Wake-up Stroke Alan H. Yee, D.O. Stroke and Critical Care Neurology Department of Neurology University of California Davis Medical Center Objectives Review Epidemiology and Natural
The DAWN of a New Era for Wake-up Stroke Alan H. Yee, D.O. Stroke and Critical Care Neurology Department of Neurology University of California Davis Medical Center Objectives Review Epidemiology and Natural
Update on Early Acute Ischemic Stroke Interventions
 Update on Early Acute Ischemic Stroke Interventions Diana Goodman MD Lead Neurohospitalist Maine Medical Center Assistant Professor of Neurology, Tufts University School of Medicine I have no disclosures
Update on Early Acute Ischemic Stroke Interventions Diana Goodman MD Lead Neurohospitalist Maine Medical Center Assistant Professor of Neurology, Tufts University School of Medicine I have no disclosures
Imaging Stroke: Is There a Stroke Equivalent of the ECG? Albert J. Yoo, MD Director of Acute Stroke Intervention Massachusetts General Hospital
 Imaging Stroke: Is There a Stroke Equivalent of the ECG? Albert J. Yoo, MD Director of Acute Stroke Intervention Massachusetts General Hospital Disclosures Penumbra, Inc. research grant (significant) for
Imaging Stroke: Is There a Stroke Equivalent of the ECG? Albert J. Yoo, MD Director of Acute Stroke Intervention Massachusetts General Hospital Disclosures Penumbra, Inc. research grant (significant) for
Mechanical thrombectomy beyond the 6 hours. Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital
 Mechanical thrombectomy beyond the 6 hours Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital Disclosures None Worldwide statistics 1 IN 6 people will have a stroke at some
Mechanical thrombectomy beyond the 6 hours Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital Disclosures None Worldwide statistics 1 IN 6 people will have a stroke at some
Acute Ischemic Stroke Imaging Innovations
 Acute Ischemic Stroke Imaging Innovations Guilherme Dabus, MD, FAHA Director, Fellowship NeuroInterventional Surgery Miami Cardiac & Vascular Institute Baptist Neuroscience Center Baptist Neuroscience
Acute Ischemic Stroke Imaging Innovations Guilherme Dabus, MD, FAHA Director, Fellowship NeuroInterventional Surgery Miami Cardiac & Vascular Institute Baptist Neuroscience Center Baptist Neuroscience
Stroke Treatment Beyond Traditional Time Windows. Rishi Gupta, MD, MBA
 Stroke Treatment Beyond Traditional Time Windows Rishi Gupta, MD, MBA Director, Stroke and Neurocritical Care Endovascular Neurosurgery Wellstar Health System THE PAST THE PRESENT 2015 American Heart Association/American
Stroke Treatment Beyond Traditional Time Windows Rishi Gupta, MD, MBA Director, Stroke and Neurocritical Care Endovascular Neurosurgery Wellstar Health System THE PAST THE PRESENT 2015 American Heart Association/American
IMAGING IN ACUTE ISCHEMIC STROKE
 IMAGING IN ACUTE ISCHEMIC STROKE Timo Krings MD, PhD, FRCP (C) Professor of Radiology & Surgery Braley Chair of Neuroradiology, Chief and Program Director of Diagnostic and Interventional Neuroradiology;
IMAGING IN ACUTE ISCHEMIC STROKE Timo Krings MD, PhD, FRCP (C) Professor of Radiology & Surgery Braley Chair of Neuroradiology, Chief and Program Director of Diagnostic and Interventional Neuroradiology;
Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke
 Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke Alexander A. Khalessi MD MS Director of Endovascular Neurosurgery Surgical Director of NeuroCritical Care University
Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke Alexander A. Khalessi MD MS Director of Endovascular Neurosurgery Surgical Director of NeuroCritical Care University
IMAGING IN ACUTE ISCHEMIC STROKE
 IMAGING IN ACUTE ISCHEMIC STROKE Timo Krings MD, PhD, FRCP (C) Professor of Radiology & Surgery Braley Chair of Neuroradiology, Chief and Program Director of Diagnostic and Interventional Neuroradiology;
IMAGING IN ACUTE ISCHEMIC STROKE Timo Krings MD, PhD, FRCP (C) Professor of Radiology & Surgery Braley Chair of Neuroradiology, Chief and Program Director of Diagnostic and Interventional Neuroradiology;
RBWH ICU Journal Club February 2018 Adam Simpson
 RBWH ICU Journal Club February 2018 Adam Simpson 3 THROMBOLYSIS Reperfusion therapy has become the mainstay of therapy for ischaemic stroke. Thrombolysis is now well accepted within 4.5 hours. - Improved
RBWH ICU Journal Club February 2018 Adam Simpson 3 THROMBOLYSIS Reperfusion therapy has become the mainstay of therapy for ischaemic stroke. Thrombolysis is now well accepted within 4.5 hours. - Improved
11/1/2018. Disclosure. Imaging in Acute Ischemic Stroke 2018 Neuro Symposium. Is NCCT good enough? Keystone Heart Consultant, Stock Options
 Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Endovascular Therapy: Beyond the Guidelines
 Endovascular Therapy: Beyond the Guidelines Ashutosh P. Jadhav, MD PhD Assistant Professor, Neurology and Neurological Surgery Center for Neuro-endovascular Therapy UPMC Stroke Institute Pittsburgh, PA
Endovascular Therapy: Beyond the Guidelines Ashutosh P. Jadhav, MD PhD Assistant Professor, Neurology and Neurological Surgery Center for Neuro-endovascular Therapy UPMC Stroke Institute Pittsburgh, PA
Acute Ischemic Stroke Imaging. Ronald L. Wolf, MD, PhD Associate Professor of Radiology
 Acute Ischemic Stroke Imaging Ronald L. Wolf, MD, PhD Associate Professor of Radiology Title of First Slide of Substance An Illustrative Case 2 Disclosures No financial disclosures Off-label uses of some
Acute Ischemic Stroke Imaging Ronald L. Wolf, MD, PhD Associate Professor of Radiology Title of First Slide of Substance An Illustrative Case 2 Disclosures No financial disclosures Off-label uses of some
Interventional Treatment of Stroke
 Interventional Treatment of Stroke Andrew F. Ducruet, MD Barrow Neurological Institute 2018 BNI Stroke Rehab Symposium October 13, 2018 Disclosures Consultant: Medtronic, Penumbra, Cerenovus Lecture Overview
Interventional Treatment of Stroke Andrew F. Ducruet, MD Barrow Neurological Institute 2018 BNI Stroke Rehab Symposium October 13, 2018 Disclosures Consultant: Medtronic, Penumbra, Cerenovus Lecture Overview
Endovascular Treatment for Acute Ischemic Stroke
 ular Treatment for Acute Ischemic Stroke Vishal B. Jani MD Assistant Professor Interventional Neurology, Division of Department of Neurology. Creighton University/ CHI health Omaha NE Disclosure None 1
ular Treatment for Acute Ischemic Stroke Vishal B. Jani MD Assistant Professor Interventional Neurology, Division of Department of Neurology. Creighton University/ CHI health Omaha NE Disclosure None 1
Acute Stroke Treatment: Current Trends 2010
 Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Mechanical Thrombectomy: Where Are We Now? T. Adam Oliver, MD Tallahassee Neurological Clinic Tallahassee, Florida TMH Neurosymposium June 11, 2016
 Mechanical Thrombectomy: Where Are We Now? T. Adam Oliver, MD Tallahassee Neurological Clinic Tallahassee, Florida TMH Neurosymposium June 11, 2016 none DISCLOSURES Where did we come from? Spiotta, et
Mechanical Thrombectomy: Where Are We Now? T. Adam Oliver, MD Tallahassee Neurological Clinic Tallahassee, Florida TMH Neurosymposium June 11, 2016 none DISCLOSURES Where did we come from? Spiotta, et
CT Perfusion is Essential for Stroke Triage. Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center
 CT Perfusion is Essential for Stroke Triage Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center CT Perfusion is Essential for Stroke Triage Disclosures:
CT Perfusion is Essential for Stroke Triage Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center CT Perfusion is Essential for Stroke Triage Disclosures:
Strokecenter Key lessons of MR CLEAN study
 Strokecenter Key lessons of MR CLEAN study Diederik Dippel Disclosures Funded by the Dutch Heart Foundation Nominal, unrestricted grants from AngioCare BV Medtronic/Covidien/EV3 MEDAC Gmbh/LAMEPRO Penumbra
Strokecenter Key lessons of MR CLEAN study Diederik Dippel Disclosures Funded by the Dutch Heart Foundation Nominal, unrestricted grants from AngioCare BV Medtronic/Covidien/EV3 MEDAC Gmbh/LAMEPRO Penumbra
Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington
 Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington Disclosures: SWIFT PRIME site (Medtronic) Physician Proctor
Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington Disclosures: SWIFT PRIME site (Medtronic) Physician Proctor
Disclosure. Advances in Interventional Neurology. Disclosure. Natural History of Disease 3/15/2018. Vishal B. Jani MD
 Advances in Interventional Neurology Disclosure Vishal B. Jani MD Medical Director Vascular Neurology Consultant Interventional Neurology CHI Health Assistant Professor, Creighton University School of
Advances in Interventional Neurology Disclosure Vishal B. Jani MD Medical Director Vascular Neurology Consultant Interventional Neurology CHI Health Assistant Professor, Creighton University School of
Endovascular Treatment of Ischemic Stroke
 Endovascular Treatment of Ischemic Stroke William Thorell, MD Associate Professor Neurosurgery UNMC Co-Director Stroke and Neurovascular Center Nebraska Medicine Overview Definitions of terms Review basic
Endovascular Treatment of Ischemic Stroke William Thorell, MD Associate Professor Neurosurgery UNMC Co-Director Stroke and Neurovascular Center Nebraska Medicine Overview Definitions of terms Review basic
BGS Spring Conference 2015
 Neuroradiology in hyperacute stroke: what is the UK position? Dr Shelley Renowden Bristol NICE HIS July, 2013 The current evidence on mechanical clot retrieval for treating acute ischaemic stroke shows
Neuroradiology in hyperacute stroke: what is the UK position? Dr Shelley Renowden Bristol NICE HIS July, 2013 The current evidence on mechanical clot retrieval for treating acute ischaemic stroke shows
Interventional Stroke Treatment
 Interventional Stroke Treatment Vishal B. Jani MD Medical Director Vascular Neurology Consultant Interventional Neurology CHI Health Assistant Professor, Creighton University School of Medicine Omaha,
Interventional Stroke Treatment Vishal B. Jani MD Medical Director Vascular Neurology Consultant Interventional Neurology CHI Health Assistant Professor, Creighton University School of Medicine Omaha,
1/19/2018. Endovascular Therapy for Stroke
 Endovascular Therapy for Stroke 1 PROACT II (1999, IA urokinase)first to demonstrate benefit of EST Newer trials (including MERCI in 2005) demonstrated vessel recanalization but no clinical benefit 2 Based
Endovascular Therapy for Stroke 1 PROACT II (1999, IA urokinase)first to demonstrate benefit of EST Newer trials (including MERCI in 2005) demonstrated vessel recanalization but no clinical benefit 2 Based
ACUTE STROKE IMAGING
 ACUTE STROKE IMAGING Mahesh V. Jayaraman M.D. Director, Inter ventional Neuroradiology Associate Professor Depar tments of Diagnostic Imaging and Neurosurger y Alper t Medical School at Brown University
ACUTE STROKE IMAGING Mahesh V. Jayaraman M.D. Director, Inter ventional Neuroradiology Associate Professor Depar tments of Diagnostic Imaging and Neurosurger y Alper t Medical School at Brown University
How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval
 How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval Peter Howard MD FRCPC Disclosures No conflicts to disclose How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular
How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval Peter Howard MD FRCPC Disclosures No conflicts to disclose How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular
Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients
 Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School
Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School
Endovascular Treatment Updates in Stroke Care
 Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
5/31/2018. Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment. Disclosures. Impact of clot burden
 Good Outcome (%) Rankin 0-2 at 90 days 5/31/2018 Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment Disclosures Cerenovus: I am on Executive Committee for ARISE2 Trial
Good Outcome (%) Rankin 0-2 at 90 days 5/31/2018 Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment Disclosures Cerenovus: I am on Executive Committee for ARISE2 Trial
Significant Relationships
 Opening Large Vessels During Acute Ischemic Stroke Significant Relationships Wade S Smith, MD, PhD Director UCSF Neurovascular Service Professor of Neurology Daryl R Gress Endowed Chair of Neurocritical
Opening Large Vessels During Acute Ischemic Stroke Significant Relationships Wade S Smith, MD, PhD Director UCSF Neurovascular Service Professor of Neurology Daryl R Gress Endowed Chair of Neurocritical
Endovascular Stroke Therapy
 Endovascular Stroke Therapy Update with Emphasis on Practical Clinical and Imaging Considerations Sachin Kishore Pandey, MD, FRCPC Disclosures I have no relevant financial disclosures or conflict of interest
Endovascular Stroke Therapy Update with Emphasis on Practical Clinical and Imaging Considerations Sachin Kishore Pandey, MD, FRCPC Disclosures I have no relevant financial disclosures or conflict of interest
Acute Stroke Identification and Treatment
 Acute Stroke Identification and Treatment James S. McKinney, MD, FAHA Medical Director, NHRMC Stroke Center SE NC is located in the buckle of the Stroke Belt, seeing the highest stroke incidence and mortality
Acute Stroke Identification and Treatment James S. McKinney, MD, FAHA Medical Director, NHRMC Stroke Center SE NC is located in the buckle of the Stroke Belt, seeing the highest stroke incidence and mortality
Stroke Update Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center
 Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015
 UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015 NEW STUDIES FOR 2015 MR CLEAN ESCAPE EXTEND-IA REVASCAT SWIFT PRIME RECOGNIZED LIMITATIONS IV Alteplase proven benefit
UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015 NEW STUDIES FOR 2015 MR CLEAN ESCAPE EXTEND-IA REVASCAT SWIFT PRIME RECOGNIZED LIMITATIONS IV Alteplase proven benefit
Ongoing Acute Stroke Studies 10/5/2015
 Ongoing Acute Stroke Studies 10/5/2015 Wade S. Smith, MD, PhD Director UCSF Neurovascular Service Daryl R. Gress Professor of Neurocritical Care and Stroke Disclosures NIH U10 NS 086494 (PI) NorCal RCC
Ongoing Acute Stroke Studies 10/5/2015 Wade S. Smith, MD, PhD Director UCSF Neurovascular Service Daryl R. Gress Professor of Neurocritical Care and Stroke Disclosures NIH U10 NS 086494 (PI) NorCal RCC
Endovascular Clot Retrieval. Teddy Wu Neurologist (and Stroke enthusiast) Christchurch Hospital
 Christchurch Hospital") Endovascular Clot Retrieval Teddy Wu Neurologist (and Stroke enthusiast) Christchurch Hospital Something you can do tomorrow Melbourne half marathon 2016 In 2009 Simple approach to stroke - blocked artery,
Endovascular Clot Retrieval Teddy Wu Neurologist (and Stroke enthusiast) Christchurch Hospital Something you can do tomorrow Melbourne half marathon 2016 In 2009 Simple approach to stroke - blocked artery,
12/4/2017. Disclosures. Study organization. Stryker Medtronic Penumbra Viz Route 92. Data safety monitoring board Tudor G.
 12/4/2017 Update on Stroke Trials:Extending the Window DWI or CTP Assessment with Clinical Mismatch in the Triage of Wake-Up and Late Presenting Strokes Undergoing Neurointervention with Trevo NP001713
12/4/2017 Update on Stroke Trials:Extending the Window DWI or CTP Assessment with Clinical Mismatch in the Triage of Wake-Up and Late Presenting Strokes Undergoing Neurointervention with Trevo NP001713
ESCAPE Endovascular treatment for Small Core and Anterior circulation Proximal occlusion with Emphasis on minimizing CT to recanalization times
 ESCAPE Endovascular treatment for Small Core and Anterior circulation Proximal occlusion with Emphasis on minimizing CT to recanalization times Michael D Hill, Mayank Goyal on behalf of the ESCAPE Trial
ESCAPE Endovascular treatment for Small Core and Anterior circulation Proximal occlusion with Emphasis on minimizing CT to recanalization times Michael D Hill, Mayank Goyal on behalf of the ESCAPE Trial
Perils of Mechanical Thrombectomy in Acute Asymptomatic Large Vessel Occlusion
 Perils of Mechanical Thrombectomy in Acute Asymptomatic Large Vessel Occlusion Aman B. Patel, MD Robert & Jean Ojemann Associate Professor Director, Cerebrovascular Surgery Director, Neuroendovascular
Perils of Mechanical Thrombectomy in Acute Asymptomatic Large Vessel Occlusion Aman B. Patel, MD Robert & Jean Ojemann Associate Professor Director, Cerebrovascular Surgery Director, Neuroendovascular
framework for flow Objectives Acute Stroke Treatment Collaterals in Acute Ischemic Stroke framework & basis for flow
 Acute Stroke Treatment Collaterals in Acute Ischemic Stroke Objectives role of collaterals in acute ischemic stroke collateral therapeutic strategies David S Liebeskind, MD Professor of Neurology & Director
Acute Stroke Treatment Collaterals in Acute Ischemic Stroke Objectives role of collaterals in acute ischemic stroke collateral therapeutic strategies David S Liebeskind, MD Professor of Neurology & Director
Mechanical thrombectomy in Plymouth. Will Adams. Will Adams
 Mechanical thrombectomy in Plymouth Will Adams Will Adams History Intra-arterial intervention 1995 (NINDS) iv tpa improved clinical outcome in patients treated within 3 hours of ictus but limited recanalisation
Mechanical thrombectomy in Plymouth Will Adams Will Adams History Intra-arterial intervention 1995 (NINDS) iv tpa improved clinical outcome in patients treated within 3 hours of ictus but limited recanalisation
Advances in Neuro-Endovascular Care for Acute Stroke
 Advances in Neuro-Endovascular Care for Acute Stroke Ciarán J. Powers, MD, PhD, FAANS Associate Professor Program Director Department of Neurological Surgery Surgical Director Comprehensive Stroke Center
Advances in Neuro-Endovascular Care for Acute Stroke Ciarán J. Powers, MD, PhD, FAANS Associate Professor Program Director Department of Neurological Surgery Surgical Director Comprehensive Stroke Center
Updates on Endovascular Therapy
 Updates on Endovascular Therapy 5 th Annual Intermountain Stroke Conference October 16, 2017 M. Shazam Hussain, MD, FRCP(C), FAHA Director, Cerebrovascular Center Associate Professor, CCLCM Staff, Vascular
Updates on Endovascular Therapy 5 th Annual Intermountain Stroke Conference October 16, 2017 M. Shazam Hussain, MD, FRCP(C), FAHA Director, Cerebrovascular Center Associate Professor, CCLCM Staff, Vascular
EVOLUTION IN SYSTEMS OF STROKE CARE RIDWAN LIN, MD, PHD STROKE & INTERVENTIONAL NEUROLOGY BROWARD HEALTH
 EVOLUTION IN SYSTEMS OF STROKE CARE RIDWAN LIN, MD, PHD STROKE & INTERVENTIONAL NEUROLOGY BROWARD HEALTH STROKE SYSTEMS OF CARE: 7. Secondary prevention 1. Primary prevention Patient 3. Emergency transport
EVOLUTION IN SYSTEMS OF STROKE CARE RIDWAN LIN, MD, PHD STROKE & INTERVENTIONAL NEUROLOGY BROWARD HEALTH STROKE SYSTEMS OF CARE: 7. Secondary prevention 1. Primary prevention Patient 3. Emergency transport
Advanced Neuroimaging for Acute Stroke
 Advanced Neuroimaging for Acute Stroke E. Bradshaw Bunney, MD, FACEP Professor Department Of Emergency Medicine University of Illinois at Chicago Swedish American Belvidere Hospital Disclosures FERNE Board
Advanced Neuroimaging for Acute Stroke E. Bradshaw Bunney, MD, FACEP Professor Department Of Emergency Medicine University of Illinois at Chicago Swedish American Belvidere Hospital Disclosures FERNE Board
Disclosures. Current Management of Acute Ischemic Stroke. Overview. Focal brain ischemia. Nerissa U. Ko, MD, MAS Professor of Neurology May 8, 2015
 Disclosures Current Management of Acute Ischemic Nerissa U. Ko, MD, MAS Professor of Neurology May 8, 2015 Nothing to disclose Research Funding: American Heart Association NIH/NINDS Selected slides courtesy
Disclosures Current Management of Acute Ischemic Nerissa U. Ko, MD, MAS Professor of Neurology May 8, 2015 Nothing to disclose Research Funding: American Heart Association NIH/NINDS Selected slides courtesy
Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices
 Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices Joey English MD, PhD Medical Director, Neurointerventional Services California Pacific Medical Center Hospitals, San Francisco,
Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices Joey English MD, PhD Medical Director, Neurointerventional Services California Pacific Medical Center Hospitals, San Francisco,
What is the best imaging protocol for LVO screening when outside of 0-6h window?
 Klinik und Poliklinik für Neuroradiologische Diagnostik und Intervention Zentrum für Radiologie und Endoskopie WLNC, Los Angeles/CA, USA, May 15-17, 2017 What is the best imaging protocol for LVO screening
Klinik und Poliklinik für Neuroradiologische Diagnostik und Intervention Zentrum für Radiologie und Endoskopie WLNC, Los Angeles/CA, USA, May 15-17, 2017 What is the best imaging protocol for LVO screening
Parameter Optimized Treatment for Acute Ischemic Stroke
 Heart & Stroke Barnett Memorial Lectureship and Visiting Professorship Parameter Optimized Treatment for Acute Ischemic Stroke December 2, 2016, Thunder Bay, Ontario Adnan I. Qureshi MD Professor of Neurology,
Heart & Stroke Barnett Memorial Lectureship and Visiting Professorship Parameter Optimized Treatment for Acute Ischemic Stroke December 2, 2016, Thunder Bay, Ontario Adnan I. Qureshi MD Professor of Neurology,
Acute Stroke Management What is State of the Art?
 Acute Stroke Management What is State of the Art? Karl-Titus Hoffmann Department of Neuroradiologie University of Leipzig / University Hospital Leipzig Disclosure Speaker name: Karl-Titus Hoffmann I have
Acute Stroke Management What is State of the Art? Karl-Titus Hoffmann Department of Neuroradiologie University of Leipzig / University Hospital Leipzig Disclosure Speaker name: Karl-Titus Hoffmann I have
occlusions. Cerebral perfusion is driven fundamentally by regional cerebral
 Appendix Figures Figure A1. Hemodynamic changes that may occur in major anterior circulation occlusions. Cerebral perfusion is driven fundamentally by regional cerebral perfusion pressure (CPP). In response
Appendix Figures Figure A1. Hemodynamic changes that may occur in major anterior circulation occlusions. Cerebral perfusion is driven fundamentally by regional cerebral perfusion pressure (CPP). In response
Latest Advances in the Neurointerventional Treatment of Ischemic Stroke P A C I F I C N E U R O. O R G
 Latest Advances in the Neurointerventional Treatment of Ischemic Stroke Neurointerventional Management of Ischemic Stroke 1. Thrombectomy for acute ischemic stroke 2. Carotid artery stenting 3. Management
Latest Advances in the Neurointerventional Treatment of Ischemic Stroke Neurointerventional Management of Ischemic Stroke 1. Thrombectomy for acute ischemic stroke 2. Carotid artery stenting 3. Management
Stroke Cart Improves Efficiency in Acute Ischemic Stroke Intervention
 Stroke Cart Improves Efficiency in Acute Ischemic Stroke Intervention MR Amans, F Settecase, R Darflinger, M Alexander, A Nicholson, DL Cooke, SW Hetts, CF Dowd, RT Higashida, VV Halbach Interventional
Stroke Cart Improves Efficiency in Acute Ischemic Stroke Intervention MR Amans, F Settecase, R Darflinger, M Alexander, A Nicholson, DL Cooke, SW Hetts, CF Dowd, RT Higashida, VV Halbach Interventional
Figures for Draft Response to IMS III, MR RESCUE, and SYNTHSESIS Trials
 Figures for Draft Response to IMS III, MR RESCUE, and SYNTHSESIS Trials Figure 1: Lay Press Judgment May Belie a Deeper Examination of the Data. Truman ultimately defeated Dewey for the Presidency Subject
Figures for Draft Response to IMS III, MR RESCUE, and SYNTHSESIS Trials Figure 1: Lay Press Judgment May Belie a Deeper Examination of the Data. Truman ultimately defeated Dewey for the Presidency Subject
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Patient selection for i.v. thrombolysis and thrombectomy
 3 rd Congress of the European Academy of Neurology Amsterdam, The Netherlands, June 24 27, 2017 Teaching Course 8 Acute treatment and early secondary prevention of stroke Level 2 Patient selection for
3 rd Congress of the European Academy of Neurology Amsterdam, The Netherlands, June 24 27, 2017 Teaching Course 8 Acute treatment and early secondary prevention of stroke Level 2 Patient selection for
CVA Updates Karen Greenberg, DO, FACOEP. Director Neurologic Emergency Department Crozer Chester Medical Center
 CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
CT/MRI 第 42 回日本脳卒中学会講演シンポジウム 総説 はじめに. MRI magnetic resonance imaging DWI diffusion-weighted. DWI/CBF malignant profile
 第 42 回日本脳卒中学会講演シンポジウム 総説 CT/MRI 1 要旨 rt-pa MRI magnetic resonance imaging DWI diffusion-weighted image Tmax time-to-maximum DWI/PWI perfusion image mismatch CT computed tomography CBF cerebral blood flow
第 42 回日本脳卒中学会講演シンポジウム 総説 CT/MRI 1 要旨 rt-pa MRI magnetic resonance imaging DWI diffusion-weighted image Tmax time-to-maximum DWI/PWI perfusion image mismatch CT computed tomography CBF cerebral blood flow
Evidence for Mechanical ThrombectomyFor Acute Ischemic Stroke. Kenneth V Snyder MD PhD SUNY Buffalo, NY
 Evidence for Mechanical ThrombectomyFor Acute Ischemic Stroke Kenneth V Snyder MD PhD SUNY Buffalo, NY Disclosure Speaker name:... I have the following potential conflicts of interest to report: Honorarium
Evidence for Mechanical ThrombectomyFor Acute Ischemic Stroke Kenneth V Snyder MD PhD SUNY Buffalo, NY Disclosure Speaker name:... I have the following potential conflicts of interest to report: Honorarium
Intra-arterial Stroke Therapy: 2018 Update
 Intra-arterial Stroke Therapy: 2018 Update Expanding the Treatment Window Parita Bhuva, M.D. Medical Director Enrolling investigator Stryker Neurovascular (DAWN trial) Disclosures Most common large vessel
Intra-arterial Stroke Therapy: 2018 Update Expanding the Treatment Window Parita Bhuva, M.D. Medical Director Enrolling investigator Stryker Neurovascular (DAWN trial) Disclosures Most common large vessel
Stroke: The First Critical Hour. Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP
 Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Practical Considerations in the Early Treatment of Acute Stroke
 Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
ACUTE ISCHEMIC STROKE
 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE HHS Stroke Annual Review March 7 and March 8, 2018 Objectives To review the stroke endovascular mechanical thrombectomy evidence
ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE HHS Stroke Annual Review March 7 and March 8, 2018 Objectives To review the stroke endovascular mechanical thrombectomy evidence
Endovascular Procedures (Angioplasty and/or Stenting) for Intracranial Arterial Disease (Atherosclerosis and Aneurysms)
 for Intracranial Arterial Disease (Atherosclerosis and Aneurysms)") Endovascular Procedures (Angioplasty and/or Stenting) for Intracranial Arterial Disease (Atherosclerosis and Aneurysms) Policy Number: 2.01.54 Last Review: 11/2018 Origination: 4/2006 Next Review: 11/2019
Endovascular Procedures (Angioplasty and/or Stenting) for Intracranial Arterial Disease (Atherosclerosis and Aneurysms) Policy Number: 2.01.54 Last Review: 11/2018 Origination: 4/2006 Next Review: 11/2019
Further Pragmatic Trials of Thrombectomy are Needed
 Further Pragmatic Trials of Thrombectomy are Needed Prof Keith W Muir Institute of Neuroscience & Psychology University of Glasgow Institute of Neurological Sciences Queen Elizabeth University Hospital
Further Pragmatic Trials of Thrombectomy are Needed Prof Keith W Muir Institute of Neuroscience & Psychology University of Glasgow Institute of Neurological Sciences Queen Elizabeth University Hospital
Alex Abou-Chebl, MD Associate Professor of Neurology and Neurosurgery Director of Neurointerventional Services Director of Vascular and
 Alex Abou-Chebl, MD Associate Professor of Neurology and Neurosurgery Director of Neurointerventional Services Director of Vascular and Interventional Neurology Fellowships University of Louisville School
Alex Abou-Chebl, MD Associate Professor of Neurology and Neurosurgery Director of Neurointerventional Services Director of Vascular and Interventional Neurology Fellowships University of Louisville School
Mechanical Endovascular Reperfusion Therapy
 Get With the Guidelines Stroke Mechanical Endovascular Reperfusion Therapy February 1, 2017 Speaker Lee H. Schwamm, MD Executive Vice Chairman and Director of Stroke/TeleStroke Services, Department of
Get With the Guidelines Stroke Mechanical Endovascular Reperfusion Therapy February 1, 2017 Speaker Lee H. Schwamm, MD Executive Vice Chairman and Director of Stroke/TeleStroke Services, Department of
Lessons Learned from IMS III: Implications for the Future
 Lessons Learned from IMS III: Implications for the Future Pooja Khatri, MD, MSc Professor, Dept of Neurology Director of Acute Stroke, UC Stroke Team University of Cincinnati Disclosures Univ of Cincinnati
Lessons Learned from IMS III: Implications for the Future Pooja Khatri, MD, MSc Professor, Dept of Neurology Director of Acute Stroke, UC Stroke Team University of Cincinnati Disclosures Univ of Cincinnati
Interventional Neuroradiology. & Stroke INR PROCEDURES INR PROCEDURES. Dr Steve Chryssidis. 25-Sep-17. Interventional Neuroradiology
 Interventional Neuroradiology Interventional Neuroradiology & Stroke Dr Steve Chryssidis Interventional Neuroradiology (INR) is a subspecialty within Radiology INR -- broadly defined as treatment by endovascular
Interventional Neuroradiology Interventional Neuroradiology & Stroke Dr Steve Chryssidis Interventional Neuroradiology (INR) is a subspecialty within Radiology INR -- broadly defined as treatment by endovascular
Background. Recommendations for Imaging of Acute Ischemic Stroke: A Scientific Statement From the American Heart Association
 for Imaging of Acute Ischemic Stroke: A Scientific Statement From the American Heart Association An Scientific Statement from the Stroke Council, American Heart Association and American Stroke Association
for Imaging of Acute Ischemic Stroke: A Scientific Statement From the American Heart Association An Scientific Statement from the Stroke Council, American Heart Association and American Stroke Association
IV tpa and mechanical thrombectomy case selection
 IV tpa and mechanical thrombectomy case selection 22 April 2017, 9.50-10.30 Deidre De Silva SGH campus, NNI, Singapore OUTLINE Reperfusion concept Case Selection factors IV tpa & Mechanical Thrombectomy
IV tpa and mechanical thrombectomy case selection 22 April 2017, 9.50-10.30 Deidre De Silva SGH campus, NNI, Singapore OUTLINE Reperfusion concept Case Selection factors IV tpa & Mechanical Thrombectomy
The role of CT perfusion in patients selection for acute treatment
 The role of CT perfusion in patients selection for acute treatment Enrico Fainardi Unità Operativa di Neuroradiologia, Dipartimento di Neuroscienze e Riabilitazione, Azienda Ospedaliero-Universitaria,
The role of CT perfusion in patients selection for acute treatment Enrico Fainardi Unità Operativa di Neuroradiologia, Dipartimento di Neuroscienze e Riabilitazione, Azienda Ospedaliero-Universitaria,
Endovascular Therapy for Acute Ischemic Stroke: Reducing Door-to-puncture Time
 DOI: 10.5797/jnet.oa.2016-0140 Endovascular Therapy for Acute Ischemic Stroke: Reducing Door-to-puncture Time Yoichi Morofuji, 1,2 Nobutaka Horie, 1,2 Yohei Tateishi, 2,3 Minoru Morikawa, 4 Eisaku Sadakata,
DOI: 10.5797/jnet.oa.2016-0140 Endovascular Therapy for Acute Ischemic Stroke: Reducing Door-to-puncture Time Yoichi Morofuji, 1,2 Nobutaka Horie, 1,2 Yohei Tateishi, 2,3 Minoru Morikawa, 4 Eisaku Sadakata,
On Call Guide to CT Perfusion. Updated: March 2011
 On Call Guide to CT Perfusion Updated: March 2011 CT Stroke Protocol 1. Non contrast CT brain 2. CT perfusion: contrast 40cc bolus dynamic imaging at 8 slice levels ~ 60 sec creates perfusion color maps
On Call Guide to CT Perfusion Updated: March 2011 CT Stroke Protocol 1. Non contrast CT brain 2. CT perfusion: contrast 40cc bolus dynamic imaging at 8 slice levels ~ 60 sec creates perfusion color maps
Epidemiology. Epidemiology 6/1/2015. Cerebral Ischemia
 Presenter Disclosure Information Paul Nyquist MD/MPH FCCM FAHA Updates on the Acute Care of Ischemic Stroke and Intracranial Hemorrhage Updates on the Acute Care of Ischemic Stroke Paul Nyquist MD/MPH,
Presenter Disclosure Information Paul Nyquist MD/MPH FCCM FAHA Updates on the Acute Care of Ischemic Stroke and Intracranial Hemorrhage Updates on the Acute Care of Ischemic Stroke Paul Nyquist MD/MPH,
Update on Neurointerventional Therapies: Stroke and Aneurysms
 Update on Neurointerventional Therapies: Stroke and Aneurysms Gary Duckwiler, MD Professor and Director Division of Interventional Neuroradiology David Geffen School of Medicine at UCLA Long Beach Memorial
Update on Neurointerventional Therapies: Stroke and Aneurysms Gary Duckwiler, MD Professor and Director Division of Interventional Neuroradiology David Geffen School of Medicine at UCLA Long Beach Memorial
Title: Stability of Large Diffusion/Perfusion Mismatch in Anterior Circulation Strokes for 4 or More Hours
 Author's response to reviews Title: Stability of Large Diffusion/Perfusion Mismatch in Anterior Circulation Strokes for 4 or More Hours Authors: Ramon G. Gonzalez (rggonzalez@partners.org) Reza Hakimelahi
Author's response to reviews Title: Stability of Large Diffusion/Perfusion Mismatch in Anterior Circulation Strokes for 4 or More Hours Authors: Ramon G. Gonzalez (rggonzalez@partners.org) Reza Hakimelahi
BY MARILYN M. RYMER, MD
 Lytics, Devices, and Advanced Imaging The evolving art and science of acute stroke intervention. BY MARILYN M. RYMER, MD In 1996, when the US Food and Drug Administration (FDA) approved the use of intravenous
Lytics, Devices, and Advanced Imaging The evolving art and science of acute stroke intervention. BY MARILYN M. RYMER, MD In 1996, when the US Food and Drug Administration (FDA) approved the use of intravenous
Endovascular Neurointervention in Cerebral Ischemia
 Endovascular Neurointervention in Cerebral Ischemia Beyond Thrombolytics Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington 72 y/o female with a recent diagnosis
Endovascular Neurointervention in Cerebral Ischemia Beyond Thrombolytics Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington 72 y/o female with a recent diagnosis
Effect of Collateral Blood Flow on Patients Undergoing Endovascular Therapy for Acute Ischemic Stroke
 Effect of Collateral Blood Flow on Patients Undergoing Endovascular Therapy for Acute Ischemic Stroke Michael P. Marks, MD; Maarten G. Lansberg, MD; Michael Mlynash, MD; Jean-Marc Olivot, MD; Matus Straka,
Effect of Collateral Blood Flow on Patients Undergoing Endovascular Therapy for Acute Ischemic Stroke Michael P. Marks, MD; Maarten G. Lansberg, MD; Michael Mlynash, MD; Jean-Marc Olivot, MD; Matus Straka,
Update on Thrombolysis and Thrombectomy. Seniorprofessur Neurologie UniversitätsKlinikum und Universität Heidelberg
 Update on Thrombolysis and Thrombectomy Relevant Disclosures I received financial compensation from Boehringer - Ingelheim for my time and efforts as Chairman of the SC of ECASS 1-3 and from Paion for
Update on Thrombolysis and Thrombectomy Relevant Disclosures I received financial compensation from Boehringer - Ingelheim for my time and efforts as Chairman of the SC of ECASS 1-3 and from Paion for
Stroke Update. Claire J. Creutzfeldt, MD January 12, 2018
 Stroke Update Claire J. Creutzfeldt, MD January 12, 2018 Disclosures None relevant to this presentation I receive funding from the NINDS What s new in stroke? A new model for cardioembolic stroke: atrial
Stroke Update Claire J. Creutzfeldt, MD January 12, 2018 Disclosures None relevant to this presentation I receive funding from the NINDS What s new in stroke? A new model for cardioembolic stroke: atrial
Best medical therapy (includes iv t-pa in eligible patients)
") UDATE ON REVASCAT: (Randomized Trial Of Revascularization With Solitaire FR Device Versus Best Medical Therapy In The Treatment Of Acute Stroke Due To Anterior Circulation Large Vessel Occlusion Presenting
UDATE ON REVASCAT: (Randomized Trial Of Revascularization With Solitaire FR Device Versus Best Medical Therapy In The Treatment Of Acute Stroke Due To Anterior Circulation Large Vessel Occlusion Presenting
Neuro-vascular Intervention in Stroke. Will Adams Consultant Neuroradiologist Plymouth Hospitals NHS Trust
 Neuro-vascular Intervention in Stroke Will Adams Consultant Neuroradiologist Plymouth Hospitals NHS Trust Stroke before the mid 1990s Swelling Stroke extension Haemorrhagic transformation Intravenous thrombolysis
Neuro-vascular Intervention in Stroke Will Adams Consultant Neuroradiologist Plymouth Hospitals NHS Trust Stroke before the mid 1990s Swelling Stroke extension Haemorrhagic transformation Intravenous thrombolysis
AMSER Case of the Month: March 2019
 AMSER Case of the Month: March 2019 62 year-old male with left-sided weakness Ashley Graziano OMS IV, Lake Erie College of Osteopathic Medicine Erik Yannone MD, Charles Q. Li MD, Warren Chang MD, Matthew
AMSER Case of the Month: March 2019 62 year-old male with left-sided weakness Ashley Graziano OMS IV, Lake Erie College of Osteopathic Medicine Erik Yannone MD, Charles Q. Li MD, Warren Chang MD, Matthew
Is there even a time window?
 Is there even a time window? A brief summary of key 2018 trials: DAWN and DEFUSE-3 For Neurosciences Update Conference, February 22, 2018 Maxim D. Hammer, M.D. Executive Summary Based on DAWN and DEFUSE-3,
Is there even a time window? A brief summary of key 2018 trials: DAWN and DEFUSE-3 For Neurosciences Update Conference, February 22, 2018 Maxim D. Hammer, M.D. Executive Summary Based on DAWN and DEFUSE-3,
Endovascular stroke research after MRCLEAN. W. van Zwam
 1 Endovascular stroke research after MRCLEAN W. van Zwam 2 Layout 1. What do we know by now 2. Next research questions Anesthesia Aspiration 3. Ongoing and future research Dutch initiatives 3 4 N=70 Intervention
1 Endovascular stroke research after MRCLEAN W. van Zwam 2 Layout 1. What do we know by now 2. Next research questions Anesthesia Aspiration 3. Ongoing and future research Dutch initiatives 3 4 N=70 Intervention
Case 1 5/26/2017 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE
 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
Endovascular Treatment for Acute Ischemic Stroke: Considerations from Recent Randomized Trials
 Published online: March 13, 2015 1664 9737/15/0034 0115$39.50/0 Review Endovascular Treatment for Acute Ischemic Stroke: Considerations from Recent Randomized Trials Manabu Shirakawa a Shinichi Yoshimura
Published online: March 13, 2015 1664 9737/15/0034 0115$39.50/0 Review Endovascular Treatment for Acute Ischemic Stroke: Considerations from Recent Randomized Trials Manabu Shirakawa a Shinichi Yoshimura
Disclosures. CREST Trial: Summary. Lecture Outline 4/16/2015. Cervical Atherosclerotic Disease
 Disclosures Your Patient Has Carotid Bulb Stenosis and a Tandem Intracranial Stenosis: How Do SAMMPRIS and Other Evidence Inform Your Treatment? UCSF Vascular Symposium 2015 Steven W. Hetts, MD Associate
Disclosures Your Patient Has Carotid Bulb Stenosis and a Tandem Intracranial Stenosis: How Do SAMMPRIS and Other Evidence Inform Your Treatment? UCSF Vascular Symposium 2015 Steven W. Hetts, MD Associate
How to Manage LVO Stroke with Access Blocked by Cervical Carotid Occlusion
 How to Manage LVO Stroke with Access Blocked by Cervical Carotid Occlusion November 1 st, 2017 Johanna T. Fifi, MD Director, Endovascular Ischemic Stroke Associate Professor of Neurology, Neurosurgery,
How to Manage LVO Stroke with Access Blocked by Cervical Carotid Occlusion November 1 st, 2017 Johanna T. Fifi, MD Director, Endovascular Ischemic Stroke Associate Professor of Neurology, Neurosurgery,
Distal Mechanical Thrombectomy in Acute Ischemic Stroke Method and Benefit. Hans Henkes, Wiebke Kurre Stuttgart, Germany
 Distal Mechanical Thrombectomy in Acute Ischemic Stroke Method and Benefit Hans Henkes, Wiebke Kurre Stuttgart, Germany 1 Thrombectomy... with stent-retrievers is an evidence based therapy for intracranial
Distal Mechanical Thrombectomy in Acute Ischemic Stroke Method and Benefit Hans Henkes, Wiebke Kurre Stuttgart, Germany 1 Thrombectomy... with stent-retrievers is an evidence based therapy for intracranial
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS. Justin Nolte, MD Assistant Profession Marshall University School of Medicine
 ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
Acute Stroke Treatment Update for 2008
 Acute Stroke Treatment Update for 2008 * Michael R. Dobbs, MD Assistant Professor of Neurology, Preventive Medicine, and Graduate Center for Toxicology University of Kentucky College of Medicine The Stroke
Acute Stroke Treatment Update for 2008 * Michael R. Dobbs, MD Assistant Professor of Neurology, Preventive Medicine, and Graduate Center for Toxicology University of Kentucky College of Medicine The Stroke
Historical. Medical Policy
 Medical Policy Subject: Mechanical Embolectomy for Treatment of Acute Stroke Policy #: SURG.00098 Current Effective Date: 01/01/2016 Status: Revised Last Review Date: 08/06/2015 Description/Scope This
Medical Policy Subject: Mechanical Embolectomy for Treatment of Acute Stroke Policy #: SURG.00098 Current Effective Date: 01/01/2016 Status: Revised Last Review Date: 08/06/2015 Description/Scope This
Pr Roman Sztajzel Service de Neurologie HUG
 Pr Roman Sztajzel Service de Neurologie HUG Conflict of interest: none IV THROMBOLYSIS AND ENDOVASCULAR THROMBECTOMY approved treatments of acute stroke main criteria time (delay) IV thrombolysis radiological
Pr Roman Sztajzel Service de Neurologie HUG Conflict of interest: none IV THROMBOLYSIS AND ENDOVASCULAR THROMBECTOMY approved treatments of acute stroke main criteria time (delay) IV thrombolysis radiological
Endovascular Procedures for Intracranial Arterial Disease (Atherosclerosis and Aneurysms)
") Last Review Status/Date: December 2016 Page: 1 of 49 Arterial Disease (Atherosclerosis and Description Intracranial arterial disease includes thromboembolic events, vascular stenoses, and aneurysms. Endovascular
Last Review Status/Date: December 2016 Page: 1 of 49 Arterial Disease (Atherosclerosis and Description Intracranial arterial disease includes thromboembolic events, vascular stenoses, and aneurysms. Endovascular