Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington
|
|
|
- Alexis Howard
- 5 years ago
- Views:
Transcription
1 Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington
 Consultant")
2 Disclosures: SWIFT PRIME site (Medtronic) Physician Proctor & Speaker Bureau (Medtronic) Consultant (Stryker)
3 Impact Stroke Every 45 seconds someone in the U.S. has a stroke Stroke is #4 cause of death Stroke is #1 cause of adult disability Approximately 87% ischemic Limited treatment options Intravenous lytic Limitation: must be administered within 4.5 hours of stroke onset Estimated <5% of stroke patients receive IV lytic Mechanical revascularization with Merci, Penumbra, Solitaire, and Trevo Systems Provide option for patients with large vessel occlusions

4 Signs of Large Vessel Occlusion (LVO) The no brainer stroke: Weak or paralyzed on one side of body Facial droop Absent or slurred speech. If you have these symptoms, there is a high likelihood of a large vessel occlusion. Transport to hospital capable of performing thrombectomy.
 Vertebral / Basilar Artery Patient prognosis with these types of stroke is poor Vessel Mortality Rate ICA 53% MCA 27% Basilar Artery")
5 35-40% of Ischemic Strokes are Considered LVO This subset of ischemic stroke comprises blockages in the: Internal Carotid Artery (ICA) Middle Cerebral Artery (MCA) Vertebral / Basilar Artery Patient prognosis with these types of stroke is poor Vessel Mortality Rate ICA 53% MCA 27% Basilar Artery 89-90%




6 Large Vessel Occlusions How responsive to IV TPA? Clot Location and Response to IV TPA 80$! Large vessel occlusions respond poorly to IV TPA! Clot burden is major determinate of response to IV TPA! ICA < extensive M1 < min M1 < M2 <M3 70$ 60$ 50$ 40$ 30$ 20$ 10$ 0$ ICA$ M1$ M2$ Complete$ Partial$ None$ Kimura et al. Eur Neurol 2009


7 Goal of Interventional Stroke Therapy Salvage the Penumbra

 the")


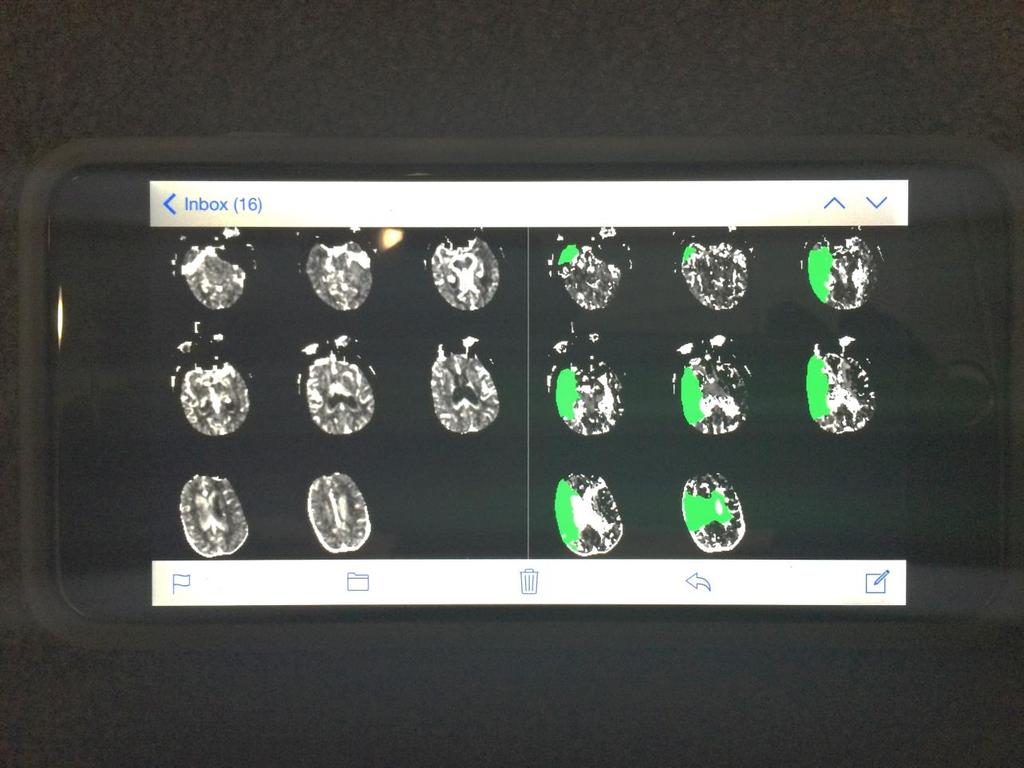
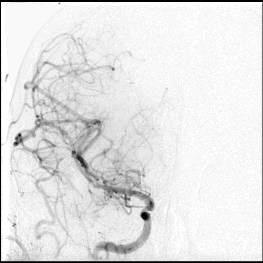
8 Fate of the Penumbra? 75 yo WM presents to BHL ED 2 hrs after onset of dysarthria and left facial droop. Because of mild deficits (NIHSS 3) the patient was not administered IV tpa. CT Perfusion was performed demonstrating sizeable ischemic pneumbra (with relatively small core infarct, MRA showed right MCA occlusion. TTD rcbv RAPID core CTP DWI


9 Fate of the Penumbra? Initial CTP showing penumbra in red Initial CTP showing core in purple Initial DWI 2 days later, the patient declined the following evening with increasing lethargy, slurred speech, and left sided weakness. 2 days later, further decline, requiring PEG placement.

10


11 Endovascular Thrombectomy of Cerebral Vessels Merci Retriever First surgical device cleared by the FDA for acute ischemic stroke patients in 2005 Restores blood flow to the brain by physically removing thrombus from the occluded precerebral or cerebral vessel Indications for Use: Patients who are ineligible for treatment with intravenous t-pa : outside 4.5 hour window other clinical factors, eg. recent surgery, long-term current use of anticoagulants for atrial fibrillation, allergy to t-pa Patients who have failed (or not responding to) prior intravenous t-pa therapy
12
13
14

15
16 Merci Registry The Largest, Prospective Multi-Center Study of Mechanical Embolectomy for Acute Ischemic Stroke Prospective, multi-center study (36 centers) 1,000 patients enrolled in 3 years Interim results presented at ISC 2010 analyzed 625 patients Inclusion criteria: procedure must have included a Merci Retriever and patient informed consent No exclusion criteria Interim results validated MERCI and Multi MERCI results in a much larger unconstrained cohort

17 TICI, mrs,???

18 Revasc Rates by Final TICI Score Merci Registry TICI 2b or higher = 53.7% Average Procedure Time = 115 minutes


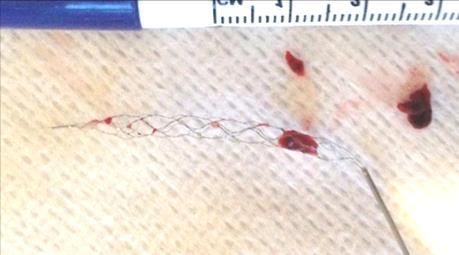
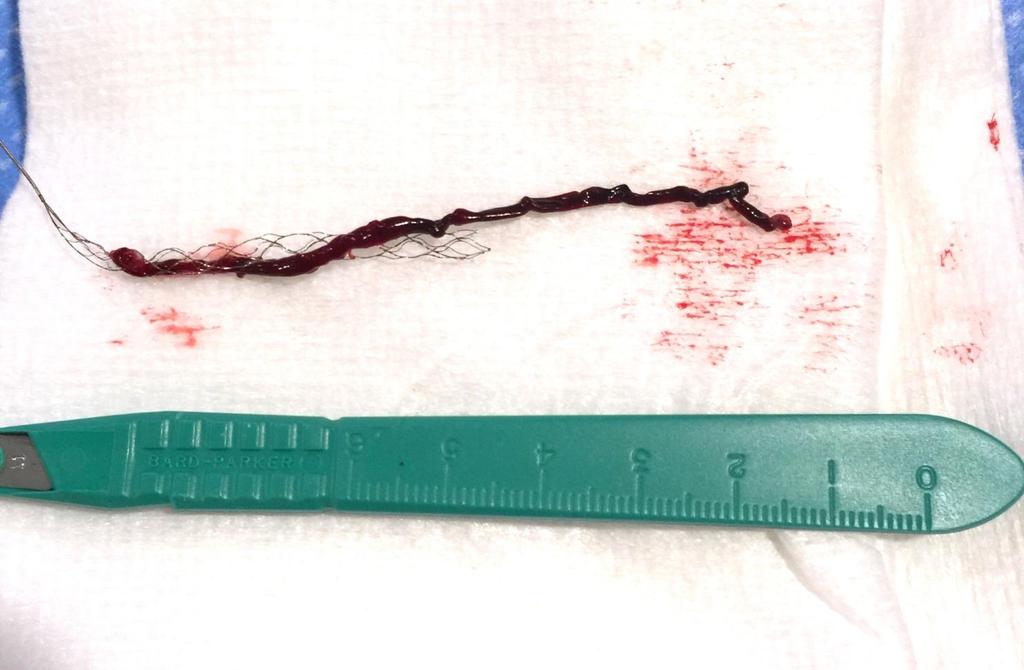
19 So What s Next? Retrieve with Confidence Trevo Stent-retrievers Solitaire and Trevo Allow for faster and higher recanalization rates, with fewer device deployments ( passes ), and improved clinical outcomes relative to Merci
20


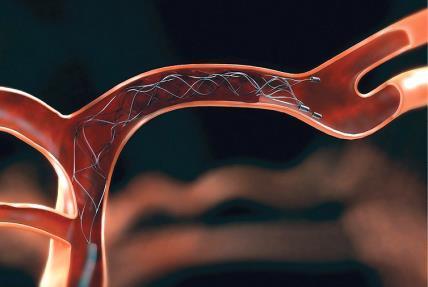

21 Merci Solitaire
22 Every Minute Counts: Time is Brain Estimated Pace of Neural Circuitry Loss in Typical Large Vessel, Supratentorial Acute Ischemic Stroke Neurons Synapses Myelinated Accelerated Lost Lost Fibers Lost Aging Per Stroke 1.2 billion 8.3 trillion 7140 km/4470 miles 36 yrs Per Hour 120 billion 830 billion 714/447 miles 3.6 yrs Per Minute 1.9 million 14 billion 12 km/7.5 miles 3.1 weeks Per Second 32, million 200 meters/218 yards 8.7 hours IMS I & II Trials showed a 10% decrease in probability of functional independence (mrs 0-2) with every 30 min delay from time of symptom onset to reperfusion.

23 Comparison b/w Merci Retriever and Solitaire (mrs 0-2) The Solitaire FR device Retrospective data demonstrates higher angiographic and neurological outcomes when compared to these Merci registries. **TICI 2a-3 classification was used
. Initial NIHSS was 24 upon arrival to CBH.")
24 79 yo WM awoke and walked to bathroom at 9am, wife heard loud noise and went to find husband lying in the floor of bathroom, aphasic and right sided hemiplegic. Transferred to CBH and received full-dose t-pa at 12pm (approx. 3hrs after symptom onset). Initial NIHSS was 24 upon arrival to CBH. CT Perfusion scan shows large area of ischemia in left MCA territory consistent with large vessel occlusion, sent for possible thrombectomy.
25
26
27


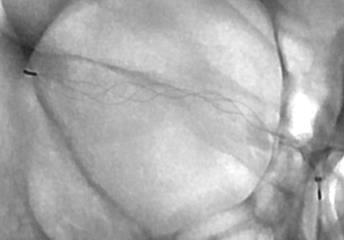
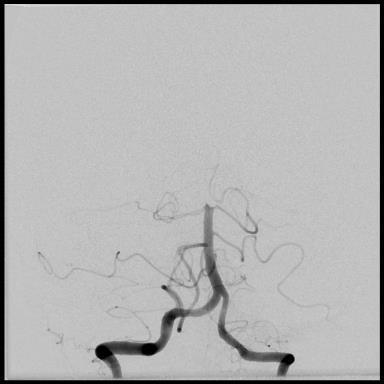
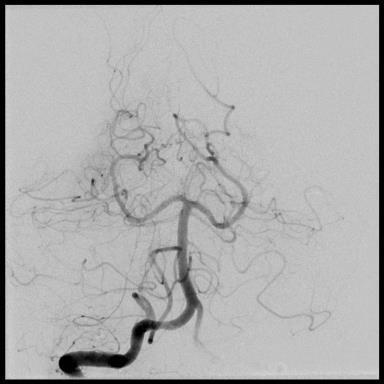
28 Partial flow restoration with Solitaire at 130pm (4.5 hrs after sx onset)

29
30

.")
31 The next day, the patient had regained anti-gravity strength in the right upper and lower extremities and significant improvement in speech (mild-moderate residual expressive aphasia). 24 hr NIHSS had improved to 6 (initial was 24).
32 Why Use Imaging to Triage Care? TTD rcbv TTD rcbv Both patients present around 4 hours after symptom onset, both candidates for IV tpa
33 Why Use Imaging to Triage Care? TTD rcbv TTD rcbv Both patients present around 4 hours after symptom onset, both candidates for IV tpa

34 Why Use Imaging to Triage Care? TTD rcbv TTD rcbv Both patients present around 4 hours after symptom onset, both candidates for IV tpa


35 Why Use Imaging to Triage Care? TTD rcbv TTD rcbv Both patients present around 4 hours after symptom onset, both candidates for IV tpa
36 Recent Stroke Trials MR CLEAN ESCAPE EXTEND-IA SWIFT PRIME REVASCAT
 or best medical therapy (including IV tpa) plus mechanical thrombectomy with stent retriever (Solitaire).")
37 MR CLEAN Multicenter (16 Centers in Netherlands), prospective, randomized trial, open label treatment and: Blinded assessment of functional outcome at 90 days Blinded assessment of neuro-imaging at baseline and follow-up 500 patients randomized to best medical therapy (including IV tpa) or best medical therapy (including IV tpa) plus mechanical thrombectomy with stent retriever (Solitaire). 233 mechanical thrombectomy, 267 to best medical therapy Masked, web-based, 1:1 random treatment allocation Intraarterial treatment (IA thrombolysis, mechanical treatment or both) plus usual care (could include IV tpa) Usual care alone (control group) Inclusion Criteria Acute ischemic stroke, Age 18, NIHSS 2 Intracranial anterior circulation occlusion (confirmed by CTA) Initiation of IA treatment within 6 hours from onset
38 MR CLEAN Stent Retrievers were 97% of IAT Treatment in the Intervention Arm 1 (0%) 5 (3%) Devices Used Stent Retrievers Thrombolysis 190 (97%) Other Mechanical Devices N= 196 patients

39 MR CLEAN Effect Of Intervention On Primary Outcome mrs % mrs %
 Treat as fast as possible (no waiting to assess tpa failure ) Use the most effective device (stent")
40 EXTEND-IA EXTEND IA EXtending the Time for thrombolysis in Emergency Neurological Deficits Intra Arterial Rational: To select patients with the best chance of benefit from reperfusion ( Dual Target ) Proven major vessel occlusion AND Salvageable tissue with ischemic core <70mL (CT perfusion) Treat as fast as possible (no waiting to assess tpa failure ) Use the most effective device (stent retriever) Methods: Randomized, open-label with blinded endpoint (PROBE) design Intervention: Stent Retriever (Solitaire FR) + IV tpa Control: IV tpa
41 EXTEND-IA Inclusion Criteria Acute ischemic stroke Age > 18 years Pre-stroke mrs 0-1 Intra-arterial clot retrieval treatment can commence (groin puncture) within 6 hours of stroke onset. Imaging inclusion criteria. Dual target: CTA reveals large artery occlusion in anterior anatomy (ICA, M1 or M2) Mismatch - Using CT or MRI with a Tmax >6 second delay perfusion volume and either CT-rCBF or DWI infarct core volume. Mismatch ratio of greater than 1.2 and Absolute mismatch volume of greater than 10ml and Infarct core lesion volume of less than 70mL
42 EXTEND-IA Only used the Solitaire Device for intervention Devices Used Solitaire Device 35/35 (100%) N= 35 patients
43 EXTEND-IA Revascularization in the IV tpa + Endovascular Arm (N=29) 100.0% 90.0% 80.0% 70.0% 60.0% 50.0% 40.0% 30.0% 20.0% 10.0% 0.0% 86.0% 48.0% TICI 2b/3 TICI 3
44 EXTEND-IA mrs 0-2 at 90-days 90.0% 75.0% 60.0% 45.0% 30.0% 15.0% 0.0% 71.0% Intervention N=35 NNT = 3.2 for independence 40.0% Control N=35
45 EXTEND-IA Conclusions Early mechanical stent thrombectomy after tpa using Solitaire FR led to faster and more complete reperfusion Patients treated with Solitaire spent significantly less time in the hospital or in rehabilitation before returning home (15 vs. 73 days, p=0.006) In this population selected for vessel occlusion and salvageable tissue this translated to: Improved early neurological recovery Improved functional outcome at 3 months No safety concerns tpa + mechanical stent thrombectomy should be the new standard of care

46 SWIFT PRIME SWIFT PRIME Solitaire FR With the Intention For Thrombectomy as PRIMary Endovascular treatment for acute ischemic stroke Purpose: To determine if patients experiencing an Acute Ischemic Stroke due to large vessel occlusion, treated with combined IV t-pa and Solitaire FR within 6 hours of symptom onset have less stroke-related disability than those patients treated with IV t-pa alone. Methods: Randomized, open-label with blinded outcome evaluation, parallel group trial Intervention: IV tpa with Solitaire FR Device Control: IV tpa alone


47 SWIFT PRIME
48 SWIFT PRIME mrs 0-2 at 90-days 75.0% 60.0% 45.0% 30.0% 15.0% 0.0% 60.2% Intervention N= % Control N=97 NNT = 4 P=0.0008
 Used in Intervention Arm IA Lytic (138), Merci Retriever (95), EKOS (22), Penumbra (54), Solitaire FR (5) Merci Retriever, EKOS, IA Lytic, Penumbra TICI 2b/3 Revascularizati on Rate in")
49 Trial Summaries Trial IMS III Imaging Required to Confirm Occlusion Prior to Randomization? No Device(s) Used in Intervention Arm IA Lytic (138), Merci Retriever (95), EKOS (22), Penumbra (54), Solitaire FR (5) Merci Retriever, EKOS, IA Lytic, Penumbra TICI 2b/3 Revascularizati on Rate in the Intervention Arm 38% ICA 44% M1 44% M2 23% multi M2 24% pen (n=34) 27% nonp (n=30) Intervention Arm 40.8% (N=415) 21% pen (n=34) 17% nonp (n=30) mrs 0-2 Control Arm 38.7% (N=214) 26% pen (n=34) 10% nonp (n=20) Odds Ratio (95% CI) 0.02 (-0.06 to 0.09) SWIFT PRIME & EXTEND-IA Superior recanalization rates and 90 day mrs scores may be attributable to: MR 1. Utilization of Viability Imaging (ASPECTS and/or Perfusion Imaging) No RESCUE % Stent Retrievers 3. Encouraged BCG usage NS MR CLEAN Yes 97% Stent Retrievers, 2% other Mechanical 58.7% (N=196) 33% (N=233) 19% (N=267) 2.16 ( ) ESCAPE Yes 86% Stent Retriever 72.4% (n=156) 53.0% (n=164) 29.3% (n=147) 1.8 ( ) SWIFT PRIME Yes 100% Stent Retriever 88.0% (n=83) 60.2% (n=98) 35.5% (n=93) 2.75 (1.53,4.95) EXTEND-IA Yes 100% Stent Retriever 86.2% (n=29) 71% (n=35) 40% (n=35) 4.2 (1.3-13)
50 The American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists Endorsed by the: American Association of Neurological Surgeons (AANS) Congress of Neurological Surgeons (CNS) AANS/CNS Cerebrovascular Section American Society of Neuroradiology (ASNR) Society of Vascular and Interventional Neurology
51 RECOMMENDATIONS Patients eligible for IV-tPA should receive IV-tPA even if endovascular therapy is being considered (Class I) Patients should undergo stent retriever endovascular therapy (Class I): Pre-stroke mrs 0-1 AIS receiving IV-tPA within 4.5 hours Occlusion of ICA or M1 segment MCA Age > 18, NIHSS > 6, ASPECTS > 6 Treatment onset within 6 hours of symptom onset Observing patients after IV-tPA to assess for clinical response before pursuing endovascular therapy is NOT required and is NOT recommended
52

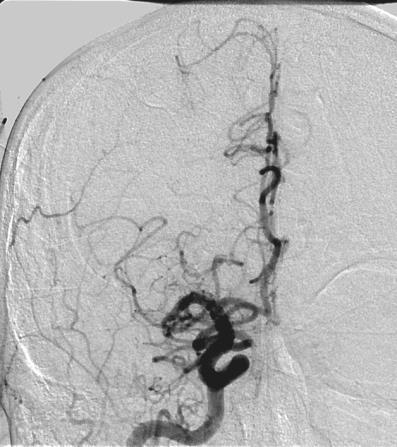
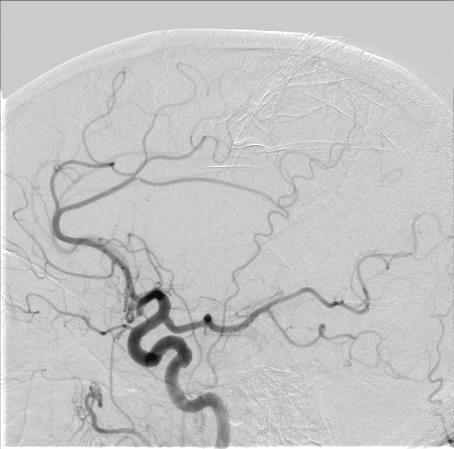
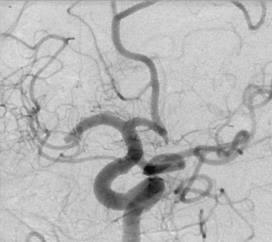
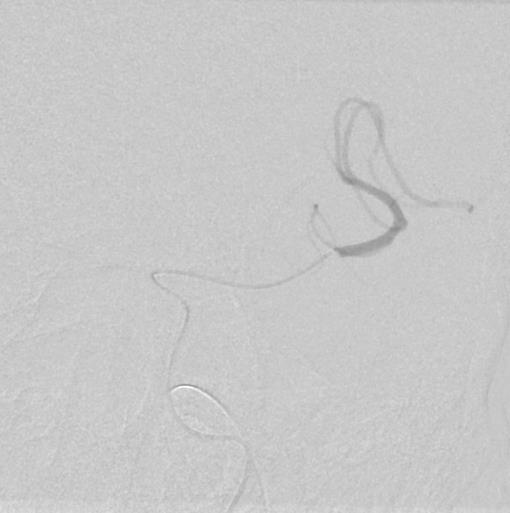
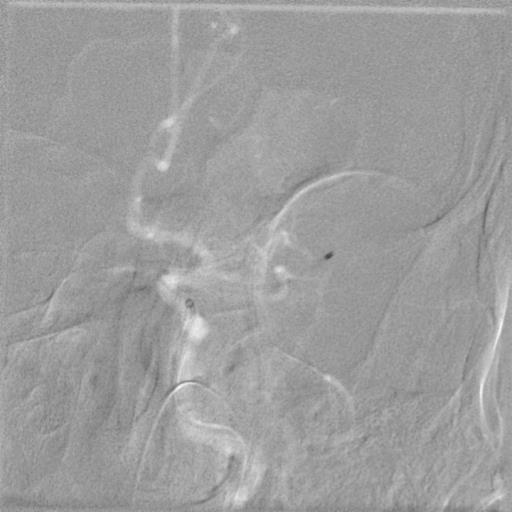
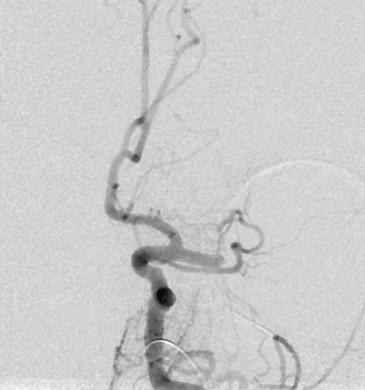
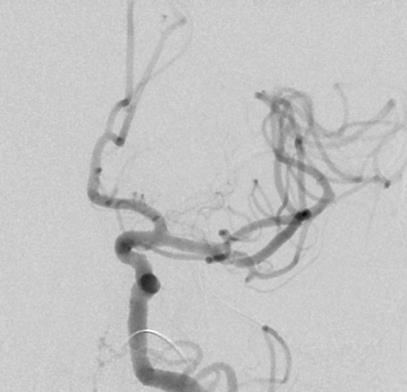
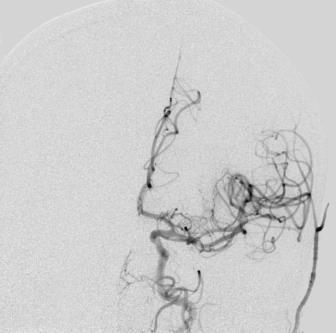
53 63 yo WM presented 2 hrs after acute onset of dense left hemiplegia, slurred speech, and left facial droop (NIHSS 17). PMH notable for prior CABG 14 days prior thus deemed not a candidate for IV tpa therapy. So what should be done nothing???


54 Right Carotid Left Carotid

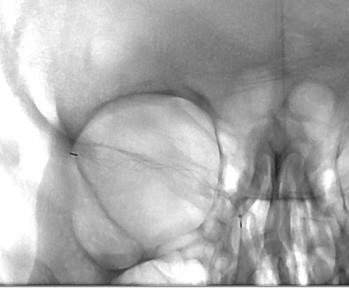
55 4x20mm

56 4x20mm
 the next day.")
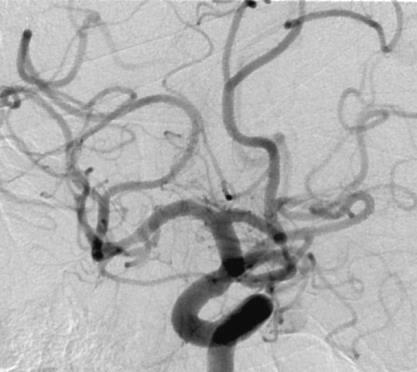
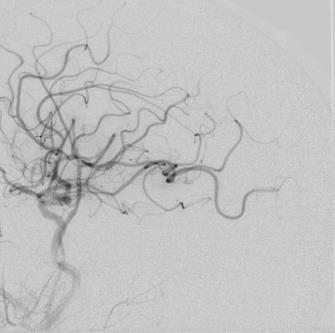
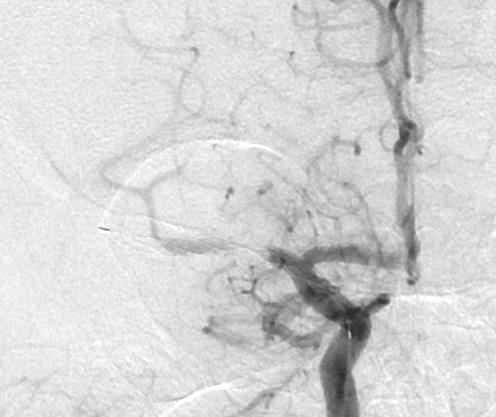
57 Rapid improvement on the Cath Lab table, NIHSS had improved from 17 2 before leaving the cath lab. NIHSS was normal (17 0) the next day.
58 Wake Up /Unknown Time of Onset Strokes 54 year-old female with history of atrial fibrillation, treated with ASA therapy, awoke with symptoms of aphasia and right hemiplegia (NIHSS 22). Traditionally do not qualify for any aggressive therapy, patients are not a candidate for IV t-pa therapy. At BHL, we utilize CT Perfusion imaging to offer treatment for these patients Time-to-Peak CT Perfusion map showing large area of ischemia, shown to be penumbra, involving the left MCA vascular territory.


59 4x20mm Solitaire
. The patient returned to normal within 4hrs post-procedure (NIHSS 0).")
60 Time-to-Peak CT Perfusion map showing large area of ischemia, shown to be penumbra, involving the left MCA vascular territory. MRI the next day shows only punctate area of infarction within the left temporal cortex (arrow). The patient returned to normal within 4hrs post-procedure (NIHSS 0). The patient was started on oral anticoagulation therapy for her atrial fibrillation and was discharged home.
 Not candidate for IV tpa as he was a wake up")
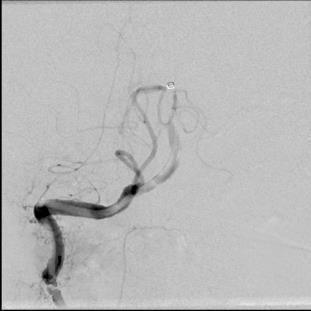
61 Acute Carotid Occlusions with Distal Emboli 57 year-old who awoke with slurred speech and left hemiplegia (NIHSS 17) Not candidate for IV tpa as he was a wake up stroke

62 Acute Carotid Occlusions with Distal Emboli
63 Presenting NIHSS17 0 D/C home the next day

64 Presenting NIHSS17 0 D/C home the next day
65 RECOMMENDATIONS Endovascular therapy with stent retrievers may be REASONABLE in: Anterior circulation occlusions who have contraindications to IV-tPA, stent retriever endovascular therapy completed within 6 hours of symptom onset is REASONABLE (Class IIa) AIS in who have M2/3 MCA occlusion, ACA, VA/Basilar/PCA (Class IIb) Patients < 18 years of age with AIS and LVO that can be initiated within 6 hours of symptom onset (Class IIb) AIS with pre-stroke mrs>1 or NIHSS<6 (Class IIb) Angioplasty/stenting of cervical ICA stenosis or occlusion at the time of thrombectomy may be considered, usefulness is unknown (Class IIb) The effectiveness of endovascular therapy is uncertain in AIS beyond 6 hours (Class IIb)
66 IMAGING If endovascular therapy is contemplated, a non-invasive intracranial vascular study is strongly recommended during the INITIAL imaging evaluation of the acute stroke patient, but should not delay IV-tPA administration (Class I) The benefit of additional imaging beyond CT/CTA or MR/MRA, such as perfusion imaging, for selecting patients for endovascular therapy are unknown (Class IIb)

67 Presenting NIHSS 20 Found down

68

69 Discharged to rehab NIHSS 20 2 mrs 0 at 30 days


70 SYSTEMS OF STROKE CARE Patients should be rapidly transported to the closest available PSC or CSC (Class I, Level A). In some instances, this may involve air medical transport and hospital bypass Regional systems of care should be developed, consisting of: Healthcare facilities that provide initial emergency care, including of IV-tPA, including PSC, CSC, and other facilities Centers capable of performing endovascular stroke treatment with comprehensive periprocedural care, including CSC and other healthcare facilities Endovascular therapy requires the patient to be at an experienced stroke center with rapid access to cerebral angiography and qualified neurointerventionalists (Class I, Level E)
71 CONCLUSIONS Stroke therapy is an evolving field, but we now have techniques and devices, combined with randomized controlled trials that provide: Reliable & reproducible recanalization rates Times to recanalization that are exceptional Patient safety profiles that are comparable (if not better) to IV t-pa Triage of patients to determine salvageable brain Data to support mechanical thrombectomy with stent retrievers as standard of care for large vessel occlusions with severe stroke symptoms and favorable imaging patterns (CT perfusion, ASPECTS). American Heart/American Stroke Society guidelines recommending thrombectomy from experienced centers as the standard of care
Endovascular Neurointervention in Cerebral Ischemia
 Endovascular Neurointervention in Cerebral Ischemia Beyond Thrombolytics Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington 72 y/o female with a recent diagnosis
Endovascular Neurointervention in Cerebral Ischemia Beyond Thrombolytics Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington 72 y/o female with a recent diagnosis
UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015
 UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015 NEW STUDIES FOR 2015 MR CLEAN ESCAPE EXTEND-IA REVASCAT SWIFT PRIME RECOGNIZED LIMITATIONS IV Alteplase proven benefit
UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015 NEW STUDIES FOR 2015 MR CLEAN ESCAPE EXTEND-IA REVASCAT SWIFT PRIME RECOGNIZED LIMITATIONS IV Alteplase proven benefit
Update on Early Acute Ischemic Stroke Interventions
 Update on Early Acute Ischemic Stroke Interventions Diana Goodman MD Lead Neurohospitalist Maine Medical Center Assistant Professor of Neurology, Tufts University School of Medicine I have no disclosures
Update on Early Acute Ischemic Stroke Interventions Diana Goodman MD Lead Neurohospitalist Maine Medical Center Assistant Professor of Neurology, Tufts University School of Medicine I have no disclosures
The DAWN of a New Era for Wake-up Stroke
 The DAWN of a New Era for Wake-up Stroke Alan H. Yee, D.O. Stroke and Critical Care Neurology Department of Neurology University of California Davis Medical Center Objectives Review Epidemiology and Natural
The DAWN of a New Era for Wake-up Stroke Alan H. Yee, D.O. Stroke and Critical Care Neurology Department of Neurology University of California Davis Medical Center Objectives Review Epidemiology and Natural
Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients
 Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School
Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School
Endovascular Treatment Updates in Stroke Care
 Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Mechanical Thrombectomy: Where Are We Now? T. Adam Oliver, MD Tallahassee Neurological Clinic Tallahassee, Florida TMH Neurosymposium June 11, 2016
 Mechanical Thrombectomy: Where Are We Now? T. Adam Oliver, MD Tallahassee Neurological Clinic Tallahassee, Florida TMH Neurosymposium June 11, 2016 none DISCLOSURES Where did we come from? Spiotta, et
Mechanical Thrombectomy: Where Are We Now? T. Adam Oliver, MD Tallahassee Neurological Clinic Tallahassee, Florida TMH Neurosymposium June 11, 2016 none DISCLOSURES Where did we come from? Spiotta, et
Mechanical thrombectomy in Plymouth. Will Adams. Will Adams
 Mechanical thrombectomy in Plymouth Will Adams Will Adams History Intra-arterial intervention 1995 (NINDS) iv tpa improved clinical outcome in patients treated within 3 hours of ictus but limited recanalisation
Mechanical thrombectomy in Plymouth Will Adams Will Adams History Intra-arterial intervention 1995 (NINDS) iv tpa improved clinical outcome in patients treated within 3 hours of ictus but limited recanalisation
Mechanical thrombectomy beyond the 6 hours. Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital
 Mechanical thrombectomy beyond the 6 hours Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital Disclosures None Worldwide statistics 1 IN 6 people will have a stroke at some
Mechanical thrombectomy beyond the 6 hours Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital Disclosures None Worldwide statistics 1 IN 6 people will have a stroke at some
Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke
 Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke Alexander A. Khalessi MD MS Director of Endovascular Neurosurgery Surgical Director of NeuroCritical Care University
Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke Alexander A. Khalessi MD MS Director of Endovascular Neurosurgery Surgical Director of NeuroCritical Care University
Evidence for Mechanical ThrombectomyFor Acute Ischemic Stroke. Kenneth V Snyder MD PhD SUNY Buffalo, NY
 Evidence for Mechanical ThrombectomyFor Acute Ischemic Stroke Kenneth V Snyder MD PhD SUNY Buffalo, NY Disclosure Speaker name:... I have the following potential conflicts of interest to report: Honorarium
Evidence for Mechanical ThrombectomyFor Acute Ischemic Stroke Kenneth V Snyder MD PhD SUNY Buffalo, NY Disclosure Speaker name:... I have the following potential conflicts of interest to report: Honorarium
Interventional Treatment of Stroke
 Interventional Treatment of Stroke Andrew F. Ducruet, MD Barrow Neurological Institute 2018 BNI Stroke Rehab Symposium October 13, 2018 Disclosures Consultant: Medtronic, Penumbra, Cerenovus Lecture Overview
Interventional Treatment of Stroke Andrew F. Ducruet, MD Barrow Neurological Institute 2018 BNI Stroke Rehab Symposium October 13, 2018 Disclosures Consultant: Medtronic, Penumbra, Cerenovus Lecture Overview
Stroke Treatment Beyond Traditional Time Windows. Rishi Gupta, MD, MBA
 Stroke Treatment Beyond Traditional Time Windows Rishi Gupta, MD, MBA Director, Stroke and Neurocritical Care Endovascular Neurosurgery Wellstar Health System THE PAST THE PRESENT 2015 American Heart Association/American
Stroke Treatment Beyond Traditional Time Windows Rishi Gupta, MD, MBA Director, Stroke and Neurocritical Care Endovascular Neurosurgery Wellstar Health System THE PAST THE PRESENT 2015 American Heart Association/American
Stroke Update Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center
 Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices
 Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices Joey English MD, PhD Medical Director, Neurointerventional Services California Pacific Medical Center Hospitals, San Francisco,
Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices Joey English MD, PhD Medical Director, Neurointerventional Services California Pacific Medical Center Hospitals, San Francisco,
Acute Stroke Treatment: Current Trends 2010
 Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
IMAGING IN ACUTE ISCHEMIC STROKE
 IMAGING IN ACUTE ISCHEMIC STROKE Timo Krings MD, PhD, FRCP (C) Professor of Radiology & Surgery Braley Chair of Neuroradiology, Chief and Program Director of Diagnostic and Interventional Neuroradiology;
IMAGING IN ACUTE ISCHEMIC STROKE Timo Krings MD, PhD, FRCP (C) Professor of Radiology & Surgery Braley Chair of Neuroradiology, Chief and Program Director of Diagnostic and Interventional Neuroradiology;
Broadening the Stroke Window in Light of the DAWN Trial
 Broadening the Stroke Window in Light of the DAWN Trial South Jersey Neurovascular and Stroke Symposium April 26, 2018 Rohan Chitale, MD Assistant Professor of Neurological Surgery Vanderbilt University
Broadening the Stroke Window in Light of the DAWN Trial South Jersey Neurovascular and Stroke Symposium April 26, 2018 Rohan Chitale, MD Assistant Professor of Neurological Surgery Vanderbilt University
BGS Spring Conference 2015
 Neuroradiology in hyperacute stroke: what is the UK position? Dr Shelley Renowden Bristol NICE HIS July, 2013 The current evidence on mechanical clot retrieval for treating acute ischaemic stroke shows
Neuroradiology in hyperacute stroke: what is the UK position? Dr Shelley Renowden Bristol NICE HIS July, 2013 The current evidence on mechanical clot retrieval for treating acute ischaemic stroke shows
Updates on Endovascular Therapy
 Updates on Endovascular Therapy 5 th Annual Intermountain Stroke Conference October 16, 2017 M. Shazam Hussain, MD, FRCP(C), FAHA Director, Cerebrovascular Center Associate Professor, CCLCM Staff, Vascular
Updates on Endovascular Therapy 5 th Annual Intermountain Stroke Conference October 16, 2017 M. Shazam Hussain, MD, FRCP(C), FAHA Director, Cerebrovascular Center Associate Professor, CCLCM Staff, Vascular
5/31/2018. Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment. Disclosures. Impact of clot burden
 Good Outcome (%) Rankin 0-2 at 90 days 5/31/2018 Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment Disclosures Cerenovus: I am on Executive Committee for ARISE2 Trial
Good Outcome (%) Rankin 0-2 at 90 days 5/31/2018 Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment Disclosures Cerenovus: I am on Executive Committee for ARISE2 Trial
Acute Stroke Identification and Treatment
 Acute Stroke Identification and Treatment James S. McKinney, MD, FAHA Medical Director, NHRMC Stroke Center SE NC is located in the buckle of the Stroke Belt, seeing the highest stroke incidence and mortality
Acute Stroke Identification and Treatment James S. McKinney, MD, FAHA Medical Director, NHRMC Stroke Center SE NC is located in the buckle of the Stroke Belt, seeing the highest stroke incidence and mortality
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Acute Ischemic Stroke Imaging. Ronald L. Wolf, MD, PhD Associate Professor of Radiology
 Acute Ischemic Stroke Imaging Ronald L. Wolf, MD, PhD Associate Professor of Radiology Title of First Slide of Substance An Illustrative Case 2 Disclosures No financial disclosures Off-label uses of some
Acute Ischemic Stroke Imaging Ronald L. Wolf, MD, PhD Associate Professor of Radiology Title of First Slide of Substance An Illustrative Case 2 Disclosures No financial disclosures Off-label uses of some
ACUTE ISCHEMIC STROKE. Current Treatment Approaches for Acute Ischemic Stroke
 ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
IMAGING IN ACUTE ISCHEMIC STROKE
 IMAGING IN ACUTE ISCHEMIC STROKE Timo Krings MD, PhD, FRCP (C) Professor of Radiology & Surgery Braley Chair of Neuroradiology, Chief and Program Director of Diagnostic and Interventional Neuroradiology;
IMAGING IN ACUTE ISCHEMIC STROKE Timo Krings MD, PhD, FRCP (C) Professor of Radiology & Surgery Braley Chair of Neuroradiology, Chief and Program Director of Diagnostic and Interventional Neuroradiology;
Mechanical Endovascular Reperfusion Therapy
 Get With the Guidelines Stroke Mechanical Endovascular Reperfusion Therapy February 1, 2017 Speaker Lee H. Schwamm, MD Executive Vice Chairman and Director of Stroke/TeleStroke Services, Department of
Get With the Guidelines Stroke Mechanical Endovascular Reperfusion Therapy February 1, 2017 Speaker Lee H. Schwamm, MD Executive Vice Chairman and Director of Stroke/TeleStroke Services, Department of
Endovascular Stroke Therapy
 Endovascular Stroke Therapy Update with Emphasis on Practical Clinical and Imaging Considerations Sachin Kishore Pandey, MD, FRCPC Disclosures I have no relevant financial disclosures or conflict of interest
Endovascular Stroke Therapy Update with Emphasis on Practical Clinical and Imaging Considerations Sachin Kishore Pandey, MD, FRCPC Disclosures I have no relevant financial disclosures or conflict of interest
Strokecenter Key lessons of MR CLEAN study
 Strokecenter Key lessons of MR CLEAN study Diederik Dippel Disclosures Funded by the Dutch Heart Foundation Nominal, unrestricted grants from AngioCare BV Medtronic/Covidien/EV3 MEDAC Gmbh/LAMEPRO Penumbra
Strokecenter Key lessons of MR CLEAN study Diederik Dippel Disclosures Funded by the Dutch Heart Foundation Nominal, unrestricted grants from AngioCare BV Medtronic/Covidien/EV3 MEDAC Gmbh/LAMEPRO Penumbra
How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval
 How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval Peter Howard MD FRCPC Disclosures No conflicts to disclose How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular
How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval Peter Howard MD FRCPC Disclosures No conflicts to disclose How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular
Case 1 5/26/2017 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE
 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY
 Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part A. Objectives Epidemiology of AIS and of ELVO Concept: Acute Ischemic
Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part A. Objectives Epidemiology of AIS and of ELVO Concept: Acute Ischemic
Endovascular Treatment for Acute Ischemic Stroke
 ular Treatment for Acute Ischemic Stroke Vishal B. Jani MD Assistant Professor Interventional Neurology, Division of Department of Neurology. Creighton University/ CHI health Omaha NE Disclosure None 1
ular Treatment for Acute Ischemic Stroke Vishal B. Jani MD Assistant Professor Interventional Neurology, Division of Department of Neurology. Creighton University/ CHI health Omaha NE Disclosure None 1
Disclosure. Advances in Interventional Neurology. Disclosure. Natural History of Disease 3/15/2018. Vishal B. Jani MD
 Advances in Interventional Neurology Disclosure Vishal B. Jani MD Medical Director Vascular Neurology Consultant Interventional Neurology CHI Health Assistant Professor, Creighton University School of
Advances in Interventional Neurology Disclosure Vishal B. Jani MD Medical Director Vascular Neurology Consultant Interventional Neurology CHI Health Assistant Professor, Creighton University School of
RBWH ICU Journal Club February 2018 Adam Simpson
 RBWH ICU Journal Club February 2018 Adam Simpson 3 THROMBOLYSIS Reperfusion therapy has become the mainstay of therapy for ischaemic stroke. Thrombolysis is now well accepted within 4.5 hours. - Improved
RBWH ICU Journal Club February 2018 Adam Simpson 3 THROMBOLYSIS Reperfusion therapy has become the mainstay of therapy for ischaemic stroke. Thrombolysis is now well accepted within 4.5 hours. - Improved
CVA Updates Karen Greenberg, DO, FACOEP. Director Neurologic Emergency Department Crozer Chester Medical Center
 CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
Interventional Stroke Treatment
 Interventional Stroke Treatment Vishal B. Jani MD Medical Director Vascular Neurology Consultant Interventional Neurology CHI Health Assistant Professor, Creighton University School of Medicine Omaha,
Interventional Stroke Treatment Vishal B. Jani MD Medical Director Vascular Neurology Consultant Interventional Neurology CHI Health Assistant Professor, Creighton University School of Medicine Omaha,
Endovascular Therapy: Beyond the Guidelines
 Endovascular Therapy: Beyond the Guidelines Ashutosh P. Jadhav, MD PhD Assistant Professor, Neurology and Neurological Surgery Center for Neuro-endovascular Therapy UPMC Stroke Institute Pittsburgh, PA
Endovascular Therapy: Beyond the Guidelines Ashutosh P. Jadhav, MD PhD Assistant Professor, Neurology and Neurological Surgery Center for Neuro-endovascular Therapy UPMC Stroke Institute Pittsburgh, PA
Neuro-vascular Intervention in Stroke. Will Adams Consultant Neuroradiologist Plymouth Hospitals NHS Trust
 Neuro-vascular Intervention in Stroke Will Adams Consultant Neuroradiologist Plymouth Hospitals NHS Trust Stroke before the mid 1990s Swelling Stroke extension Haemorrhagic transformation Intravenous thrombolysis
Neuro-vascular Intervention in Stroke Will Adams Consultant Neuroradiologist Plymouth Hospitals NHS Trust Stroke before the mid 1990s Swelling Stroke extension Haemorrhagic transformation Intravenous thrombolysis
Stroke: The First Critical Hour. Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP
 Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Figures for Draft Response to IMS III, MR RESCUE, and SYNTHSESIS Trials
 Figures for Draft Response to IMS III, MR RESCUE, and SYNTHSESIS Trials Figure 1: Lay Press Judgment May Belie a Deeper Examination of the Data. Truman ultimately defeated Dewey for the Presidency Subject
Figures for Draft Response to IMS III, MR RESCUE, and SYNTHSESIS Trials Figure 1: Lay Press Judgment May Belie a Deeper Examination of the Data. Truman ultimately defeated Dewey for the Presidency Subject
Latest Advances in the Neurointerventional Treatment of Ischemic Stroke P A C I F I C N E U R O. O R G
 Latest Advances in the Neurointerventional Treatment of Ischemic Stroke Neurointerventional Management of Ischemic Stroke 1. Thrombectomy for acute ischemic stroke 2. Carotid artery stenting 3. Management
Latest Advances in the Neurointerventional Treatment of Ischemic Stroke Neurointerventional Management of Ischemic Stroke 1. Thrombectomy for acute ischemic stroke 2. Carotid artery stenting 3. Management
Endovascular Clot Retrieval. Teddy Wu Neurologist (and Stroke enthusiast) Christchurch Hospital
 Christchurch Hospital") Endovascular Clot Retrieval Teddy Wu Neurologist (and Stroke enthusiast) Christchurch Hospital Something you can do tomorrow Melbourne half marathon 2016 In 2009 Simple approach to stroke - blocked artery,
Endovascular Clot Retrieval Teddy Wu Neurologist (and Stroke enthusiast) Christchurch Hospital Something you can do tomorrow Melbourne half marathon 2016 In 2009 Simple approach to stroke - blocked artery,
Basilar artery stenosis with bilateral cerebellar strokes on coumadin
 Qaisar A. Shah, MD Patient Profile 68 years old female with a history of; Basilar artery stenosis with bilateral cerebellar strokes on coumadin Diabetes mellitus Hyperlipidemia Hypertension She developed
Qaisar A. Shah, MD Patient Profile 68 years old female with a history of; Basilar artery stenosis with bilateral cerebellar strokes on coumadin Diabetes mellitus Hyperlipidemia Hypertension She developed
Endovascular Treatment of Ischemic Stroke
 Endovascular Treatment of Ischemic Stroke William Thorell, MD Associate Professor Neurosurgery UNMC Co-Director Stroke and Neurovascular Center Nebraska Medicine Overview Definitions of terms Review basic
Endovascular Treatment of Ischemic Stroke William Thorell, MD Associate Professor Neurosurgery UNMC Co-Director Stroke and Neurovascular Center Nebraska Medicine Overview Definitions of terms Review basic
WHY TIMELINESS MATTERS. W&M Wren Association Lecture Series
 WHY TIMELINESS MATTERS April 10, 2018 W&M Wren Association Lecture Series Pankajavalli Ramakrishnan, M.D., Ph.D. Stroke Neurologist and Neurointerventionalist Riverside Regional Medical Center Comprehensive
WHY TIMELINESS MATTERS April 10, 2018 W&M Wren Association Lecture Series Pankajavalli Ramakrishnan, M.D., Ph.D. Stroke Neurologist and Neurointerventionalist Riverside Regional Medical Center Comprehensive
framework for flow Objectives Acute Stroke Treatment Collaterals in Acute Ischemic Stroke framework & basis for flow
 Acute Stroke Treatment Collaterals in Acute Ischemic Stroke Objectives role of collaterals in acute ischemic stroke collateral therapeutic strategies David S Liebeskind, MD Professor of Neurology & Director
Acute Stroke Treatment Collaterals in Acute Ischemic Stroke Objectives role of collaterals in acute ischemic stroke collateral therapeutic strategies David S Liebeskind, MD Professor of Neurology & Director
Imaging Stroke: Is There a Stroke Equivalent of the ECG? Albert J. Yoo, MD Director of Acute Stroke Intervention Massachusetts General Hospital
 Imaging Stroke: Is There a Stroke Equivalent of the ECG? Albert J. Yoo, MD Director of Acute Stroke Intervention Massachusetts General Hospital Disclosures Penumbra, Inc. research grant (significant) for
Imaging Stroke: Is There a Stroke Equivalent of the ECG? Albert J. Yoo, MD Director of Acute Stroke Intervention Massachusetts General Hospital Disclosures Penumbra, Inc. research grant (significant) for
Interventional Neuroradiology. & Stroke INR PROCEDURES INR PROCEDURES. Dr Steve Chryssidis. 25-Sep-17. Interventional Neuroradiology
 Interventional Neuroradiology Interventional Neuroradiology & Stroke Dr Steve Chryssidis Interventional Neuroradiology (INR) is a subspecialty within Radiology INR -- broadly defined as treatment by endovascular
Interventional Neuroradiology Interventional Neuroradiology & Stroke Dr Steve Chryssidis Interventional Neuroradiology (INR) is a subspecialty within Radiology INR -- broadly defined as treatment by endovascular
Significant Relationships
 Opening Large Vessels During Acute Ischemic Stroke Significant Relationships Wade S Smith, MD, PhD Director UCSF Neurovascular Service Professor of Neurology Daryl R Gress Endowed Chair of Neurocritical
Opening Large Vessels During Acute Ischemic Stroke Significant Relationships Wade S Smith, MD, PhD Director UCSF Neurovascular Service Professor of Neurology Daryl R Gress Endowed Chair of Neurocritical
Parameter Optimized Treatment for Acute Ischemic Stroke
 Heart & Stroke Barnett Memorial Lectureship and Visiting Professorship Parameter Optimized Treatment for Acute Ischemic Stroke December 2, 2016, Thunder Bay, Ontario Adnan I. Qureshi MD Professor of Neurology,
Heart & Stroke Barnett Memorial Lectureship and Visiting Professorship Parameter Optimized Treatment for Acute Ischemic Stroke December 2, 2016, Thunder Bay, Ontario Adnan I. Qureshi MD Professor of Neurology,
EVOLUTION IN SYSTEMS OF STROKE CARE RIDWAN LIN, MD, PHD STROKE & INTERVENTIONAL NEUROLOGY BROWARD HEALTH
 EVOLUTION IN SYSTEMS OF STROKE CARE RIDWAN LIN, MD, PHD STROKE & INTERVENTIONAL NEUROLOGY BROWARD HEALTH STROKE SYSTEMS OF CARE: 7. Secondary prevention 1. Primary prevention Patient 3. Emergency transport
EVOLUTION IN SYSTEMS OF STROKE CARE RIDWAN LIN, MD, PHD STROKE & INTERVENTIONAL NEUROLOGY BROWARD HEALTH STROKE SYSTEMS OF CARE: 7. Secondary prevention 1. Primary prevention Patient 3. Emergency transport
Disclosures. Current Management of Acute Ischemic Stroke. Overview. Focal brain ischemia. Nerissa U. Ko, MD, MAS Professor of Neurology May 8, 2015
 Disclosures Current Management of Acute Ischemic Nerissa U. Ko, MD, MAS Professor of Neurology May 8, 2015 Nothing to disclose Research Funding: American Heart Association NIH/NINDS Selected slides courtesy
Disclosures Current Management of Acute Ischemic Nerissa U. Ko, MD, MAS Professor of Neurology May 8, 2015 Nothing to disclose Research Funding: American Heart Association NIH/NINDS Selected slides courtesy
12/4/2017. Disclosures. Study organization. Stryker Medtronic Penumbra Viz Route 92. Data safety monitoring board Tudor G.
 12/4/2017 Update on Stroke Trials:Extending the Window DWI or CTP Assessment with Clinical Mismatch in the Triage of Wake-Up and Late Presenting Strokes Undergoing Neurointervention with Trevo NP001713
12/4/2017 Update on Stroke Trials:Extending the Window DWI or CTP Assessment with Clinical Mismatch in the Triage of Wake-Up and Late Presenting Strokes Undergoing Neurointervention with Trevo NP001713
Advances in Neuro-Endovascular Care for Acute Stroke
 Advances in Neuro-Endovascular Care for Acute Stroke Ciarán J. Powers, MD, PhD, FAANS Associate Professor Program Director Department of Neurological Surgery Surgical Director Comprehensive Stroke Center
Advances in Neuro-Endovascular Care for Acute Stroke Ciarán J. Powers, MD, PhD, FAANS Associate Professor Program Director Department of Neurological Surgery Surgical Director Comprehensive Stroke Center
Intra-arterial Stroke Therapy: 2018 Update
 Intra-arterial Stroke Therapy: 2018 Update Expanding the Treatment Window Parita Bhuva, M.D. Medical Director Enrolling investigator Stryker Neurovascular (DAWN trial) Disclosures Most common large vessel
Intra-arterial Stroke Therapy: 2018 Update Expanding the Treatment Window Parita Bhuva, M.D. Medical Director Enrolling investigator Stryker Neurovascular (DAWN trial) Disclosures Most common large vessel
Code Stroke!! Amit Kansara, MD, FAHA. Joint EMS Conference Providence Brain and Spine Institute Providence Heart and Vascular Institute
 Code Stroke!! Amit Kansara, MD, FAHA Joint EMS Conference Providence Brain and Spine Institute Providence Heart and Vascular Institute February 22, 2019 Patient History: Dispatch 20:45: You are dispatched
Code Stroke!! Amit Kansara, MD, FAHA Joint EMS Conference Providence Brain and Spine Institute Providence Heart and Vascular Institute February 22, 2019 Patient History: Dispatch 20:45: You are dispatched
ACUTE STROKE INTERVENTION: THE ROLE OF THROMBECTOMY AND IA LYSIS
 Associate Professor of Neurology Director of Neurointerventional Services University of Louisville School of Medicine ACUTE STROKE INTERVENTION: THE ROLE OF THROMBECTOMY AND IA LYSIS Conflict of Interest
Associate Professor of Neurology Director of Neurointerventional Services University of Louisville School of Medicine ACUTE STROKE INTERVENTION: THE ROLE OF THROMBECTOMY AND IA LYSIS Conflict of Interest
AHA/ASA Guideline. Downloaded from by on November 7, 2018
 AHA/ASA Guideline 2015 American Heart Association/American Stroke Association Focused Update of the 2013 Guidelines for the Early Management of Patients With Acute Ischemic Stroke Regarding Endovascular
AHA/ASA Guideline 2015 American Heart Association/American Stroke Association Focused Update of the 2013 Guidelines for the Early Management of Patients With Acute Ischemic Stroke Regarding Endovascular
Size Matters: Differentiating Large Vessel Occlusion (LVO) and Small Vessel Occlusion (SVO) in Stroke
 and Small Vessel Occlusion (SVO) in Stroke") Size Matters: Differentiating Large Vessel Occlusion (LVO) and Small Vessel Occlusion (SVO) in Stroke Charles E. Romero, M.D. UPMC Hamot Great Lakes Neurosurgery & Neurointervention Case 1 83 yo RH F with
Size Matters: Differentiating Large Vessel Occlusion (LVO) and Small Vessel Occlusion (SVO) in Stroke Charles E. Romero, M.D. UPMC Hamot Great Lakes Neurosurgery & Neurointervention Case 1 83 yo RH F with
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS. Justin Nolte, MD Assistant Profession Marshall University School of Medicine
 ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine
 Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
11/1/2018. Disclosure. Imaging in Acute Ischemic Stroke 2018 Neuro Symposium. Is NCCT good enough? Keystone Heart Consultant, Stock Options
 Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Historical. Medical Policy
 Medical Policy Subject: Mechanical Embolectomy for Treatment of Acute Stroke Policy #: SURG.00098 Current Effective Date: 01/01/2016 Status: Revised Last Review Date: 08/06/2015 Description/Scope This
Medical Policy Subject: Mechanical Embolectomy for Treatment of Acute Stroke Policy #: SURG.00098 Current Effective Date: 01/01/2016 Status: Revised Last Review Date: 08/06/2015 Description/Scope This
Extra- and intracranial tandem occlusions in the anterior circulation - clinical outcome of endovascular treatment in acute major stroke.
 Extra- and intracranial tandem occlusions in the anterior circulation - clinical outcome of endovascular treatment in acute major stroke. Poster No.: C-1669 Congress: ECR 2014 Type: Scientific Exhibit
Extra- and intracranial tandem occlusions in the anterior circulation - clinical outcome of endovascular treatment in acute major stroke. Poster No.: C-1669 Congress: ECR 2014 Type: Scientific Exhibit
Supplementary Online Content
 Supplementary Online Content Badhiwala JH, Nassiri F, Alhazzani W, et al. Endovascular Thrombectomy for Acute Ischemic Stroke: A Meta-analysis. JAMA. doi:10.1001/jama.2015.13767. etable 1. The modified
Supplementary Online Content Badhiwala JH, Nassiri F, Alhazzani W, et al. Endovascular Thrombectomy for Acute Ischemic Stroke: A Meta-analysis. JAMA. doi:10.1001/jama.2015.13767. etable 1. The modified
1/19/2018. Endovascular Therapy for Stroke
 Endovascular Therapy for Stroke 1 PROACT II (1999, IA urokinase)first to demonstrate benefit of EST Newer trials (including MERCI in 2005) demonstrated vessel recanalization but no clinical benefit 2 Based
Endovascular Therapy for Stroke 1 PROACT II (1999, IA urokinase)first to demonstrate benefit of EST Newer trials (including MERCI in 2005) demonstrated vessel recanalization but no clinical benefit 2 Based
Practical Considerations in the Early Treatment of Acute Stroke
 Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
CT Perfusion is Essential for Stroke Triage. Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center
 CT Perfusion is Essential for Stroke Triage Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center CT Perfusion is Essential for Stroke Triage Disclosures:
CT Perfusion is Essential for Stroke Triage Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center CT Perfusion is Essential for Stroke Triage Disclosures:
ACUTE STROKE IMAGING
 ACUTE STROKE IMAGING Mahesh V. Jayaraman M.D. Director, Inter ventional Neuroradiology Associate Professor Depar tments of Diagnostic Imaging and Neurosurger y Alper t Medical School at Brown University
ACUTE STROKE IMAGING Mahesh V. Jayaraman M.D. Director, Inter ventional Neuroradiology Associate Professor Depar tments of Diagnostic Imaging and Neurosurger y Alper t Medical School at Brown University
Ischemic Stroke Therapies: Resource Guide
 Ischemic Stroke Therapies: Resource Guide Ischemic Stroke Therapies Table of Contents Introduction...1 Stroke Protocol Roadmap...2 Public Awareness...3-4 Emergency Medical Services... 5-6 Emergency Department
Ischemic Stroke Therapies: Resource Guide Ischemic Stroke Therapies Table of Contents Introduction...1 Stroke Protocol Roadmap...2 Public Awareness...3-4 Emergency Medical Services... 5-6 Emergency Department
Perils of Mechanical Thrombectomy in Acute Asymptomatic Large Vessel Occlusion
 Perils of Mechanical Thrombectomy in Acute Asymptomatic Large Vessel Occlusion Aman B. Patel, MD Robert & Jean Ojemann Associate Professor Director, Cerebrovascular Surgery Director, Neuroendovascular
Perils of Mechanical Thrombectomy in Acute Asymptomatic Large Vessel Occlusion Aman B. Patel, MD Robert & Jean Ojemann Associate Professor Director, Cerebrovascular Surgery Director, Neuroendovascular
Alex Abou-Chebl, MD Associate Professor of Neurology and Neurosurgery Director of Neurointerventional Services Director of Vascular and
 Alex Abou-Chebl, MD Associate Professor of Neurology and Neurosurgery Director of Neurointerventional Services Director of Vascular and Interventional Neurology Fellowships University of Louisville School
Alex Abou-Chebl, MD Associate Professor of Neurology and Neurosurgery Director of Neurointerventional Services Director of Vascular and Interventional Neurology Fellowships University of Louisville School
Endovascular Treatment for Acute Ischemic Stroke: Considerations from Recent Randomized Trials
 Published online: March 13, 2015 1664 9737/15/0034 0115$39.50/0 Review Endovascular Treatment for Acute Ischemic Stroke: Considerations from Recent Randomized Trials Manabu Shirakawa a Shinichi Yoshimura
Published online: March 13, 2015 1664 9737/15/0034 0115$39.50/0 Review Endovascular Treatment for Acute Ischemic Stroke: Considerations from Recent Randomized Trials Manabu Shirakawa a Shinichi Yoshimura
Statewide Acute Stroke Triage The Washington Story
 Statewide Acute Stroke Triage The Washington Story David Tirschwell, MD, MSc Medical Director of Comprehensive Stroke Care Professor, Department of Neurology UW Medicine Comprehensive Stroke Center at
Statewide Acute Stroke Triage The Washington Story David Tirschwell, MD, MSc Medical Director of Comprehensive Stroke Care Professor, Department of Neurology UW Medicine Comprehensive Stroke Center at
Interventional Revolution in Treatment of Stroke
 TCT RUSSIA 2018 XX Moscow s International Course on Endovascular Therapies Moscow, Russia, May 18-20, 2018 Interventional Revolution in Treatment of Stroke Horst Sievert, Ilona Hofmann, Laura Vaskelyte,
TCT RUSSIA 2018 XX Moscow s International Course on Endovascular Therapies Moscow, Russia, May 18-20, 2018 Interventional Revolution in Treatment of Stroke Horst Sievert, Ilona Hofmann, Laura Vaskelyte,
Stroke Cart Improves Efficiency in Acute Ischemic Stroke Intervention
 Stroke Cart Improves Efficiency in Acute Ischemic Stroke Intervention MR Amans, F Settecase, R Darflinger, M Alexander, A Nicholson, DL Cooke, SW Hetts, CF Dowd, RT Higashida, VV Halbach Interventional
Stroke Cart Improves Efficiency in Acute Ischemic Stroke Intervention MR Amans, F Settecase, R Darflinger, M Alexander, A Nicholson, DL Cooke, SW Hetts, CF Dowd, RT Higashida, VV Halbach Interventional
ACUTE ISCHEMIC STROKE
 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE HHS Stroke Annual Review March 7 and March 8, 2018 Objectives To review the stroke endovascular mechanical thrombectomy evidence
ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE HHS Stroke Annual Review March 7 and March 8, 2018 Objectives To review the stroke endovascular mechanical thrombectomy evidence
Acute brain vessel thrombectomie: when? Why? How?
 Acute brain vessel thrombectomie: when? Why? How? Didier Payen, MD, Ph D Université Paris 7 Département Anesthesiologie-Réanimation Univ Paris 7; Unité INSERM 1160 Hôpital Lariboisière AP-HParis current
Acute brain vessel thrombectomie: when? Why? How? Didier Payen, MD, Ph D Université Paris 7 Département Anesthesiologie-Réanimation Univ Paris 7; Unité INSERM 1160 Hôpital Lariboisière AP-HParis current
Benjamin Fox, MD Medical Director: Neurointerventional Radiology (NIR) DRMC Medical Director: Neurosurgery & Neurovascular, Intermountain Healthcare
 DRMC Medical Director: Neurosurgery & Neurovascular, Intermountain Healthcare") Update on neurointerventional (NIR) services at Dixie Regional Medical Center and in the Southwest Region Benjamin Fox, MD Medical Director: Neurointerventional Radiology (NIR) DRMC Medical Director: Neurosurgery
Update on neurointerventional (NIR) services at Dixie Regional Medical Center and in the Southwest Region Benjamin Fox, MD Medical Director: Neurointerventional Radiology (NIR) DRMC Medical Director: Neurosurgery
Endovascular Procedures (Angioplasty and/or Stenting) for Intracranial Arterial Disease (Atherosclerosis and Aneurysms)
 for Intracranial Arterial Disease (Atherosclerosis and Aneurysms)") Endovascular Procedures (Angioplasty and/or Stenting) for Intracranial Arterial Disease (Atherosclerosis and Aneurysms) Policy Number: 2.01.54 Last Review: 11/2018 Origination: 4/2006 Next Review: 11/2019
Endovascular Procedures (Angioplasty and/or Stenting) for Intracranial Arterial Disease (Atherosclerosis and Aneurysms) Policy Number: 2.01.54 Last Review: 11/2018 Origination: 4/2006 Next Review: 11/2019
Background. Recommendations for Imaging of Acute Ischemic Stroke: A Scientific Statement From the American Heart Association
 for Imaging of Acute Ischemic Stroke: A Scientific Statement From the American Heart Association An Scientific Statement from the Stroke Council, American Heart Association and American Stroke Association
for Imaging of Acute Ischemic Stroke: A Scientific Statement From the American Heart Association An Scientific Statement from the Stroke Council, American Heart Association and American Stroke Association
Lessons Learned from IMS III: Implications for the Future
 Lessons Learned from IMS III: Implications for the Future Pooja Khatri, MD, MSc Professor, Dept of Neurology Director of Acute Stroke, UC Stroke Team University of Cincinnati Disclosures Univ of Cincinnati
Lessons Learned from IMS III: Implications for the Future Pooja Khatri, MD, MSc Professor, Dept of Neurology Director of Acute Stroke, UC Stroke Team University of Cincinnati Disclosures Univ of Cincinnati
Distal Mechanical Thrombectomy in Acute Ischemic Stroke Method and Benefit. Hans Henkes, Wiebke Kurre Stuttgart, Germany
 Distal Mechanical Thrombectomy in Acute Ischemic Stroke Method and Benefit Hans Henkes, Wiebke Kurre Stuttgart, Germany 1 Thrombectomy... with stent-retrievers is an evidence based therapy for intracranial
Distal Mechanical Thrombectomy in Acute Ischemic Stroke Method and Benefit Hans Henkes, Wiebke Kurre Stuttgart, Germany 1 Thrombectomy... with stent-retrievers is an evidence based therapy for intracranial
Acute Stroke Treatment KPNC Stroke EXPRESS
 Acute Stroke Treatment 2018 KPNC Stroke EXPRESS EXpediting the PRocess of Evaluating & Stopping Stroke 1 Jeffrey G. Klingman, MD The Permanente Medical Group Stroke Treatment in the old days Prior to 1996:
Acute Stroke Treatment 2018 KPNC Stroke EXPRESS EXpediting the PRocess of Evaluating & Stopping Stroke 1 Jeffrey G. Klingman, MD The Permanente Medical Group Stroke Treatment in the old days Prior to 1996:
Best medical therapy (includes iv t-pa in eligible patients)
") UDATE ON REVASCAT: (Randomized Trial Of Revascularization With Solitaire FR Device Versus Best Medical Therapy In The Treatment Of Acute Stroke Due To Anterior Circulation Large Vessel Occlusion Presenting
UDATE ON REVASCAT: (Randomized Trial Of Revascularization With Solitaire FR Device Versus Best Medical Therapy In The Treatment Of Acute Stroke Due To Anterior Circulation Large Vessel Occlusion Presenting
ESCAPE Endovascular treatment for Small Core and Anterior circulation Proximal occlusion with Emphasis on minimizing CT to recanalization times
 ESCAPE Endovascular treatment for Small Core and Anterior circulation Proximal occlusion with Emphasis on minimizing CT to recanalization times Michael D Hill, Mayank Goyal on behalf of the ESCAPE Trial
ESCAPE Endovascular treatment for Small Core and Anterior circulation Proximal occlusion with Emphasis on minimizing CT to recanalization times Michael D Hill, Mayank Goyal on behalf of the ESCAPE Trial
ENDOVASCULAR THERAPIES FOR ACUTE STROKE
 ENDOVASCULAR THERAPIES FOR ACUTE STROKE Cerebral Arteriogram Cerebral Anatomy Cerebral Anatomy Brain Imaging Acute Ischemic Stroke (AIS) Therapy Main goal is to restore blood flow and improve perfusion
ENDOVASCULAR THERAPIES FOR ACUTE STROKE Cerebral Arteriogram Cerebral Anatomy Cerebral Anatomy Brain Imaging Acute Ischemic Stroke (AIS) Therapy Main goal is to restore blood flow and improve perfusion
BY MARILYN M. RYMER, MD
 Lytics, Devices, and Advanced Imaging The evolving art and science of acute stroke intervention. BY MARILYN M. RYMER, MD In 1996, when the US Food and Drug Administration (FDA) approved the use of intravenous
Lytics, Devices, and Advanced Imaging The evolving art and science of acute stroke intervention. BY MARILYN M. RYMER, MD In 1996, when the US Food and Drug Administration (FDA) approved the use of intravenous
Better identification of patients who may benefit from therapy
 Jon Jui MD, MPH Large Vessel Occlusion Low rates of re-canalization after tpa Only 25 % of large vessel strokes re-canalization after tpa Newer invasive techniques Solitaire vs Merci Better identification
Jon Jui MD, MPH Large Vessel Occlusion Low rates of re-canalization after tpa Only 25 % of large vessel strokes re-canalization after tpa Newer invasive techniques Solitaire vs Merci Better identification
AMSER Case of the Month: March 2019
 AMSER Case of the Month: March 2019 62 year-old male with left-sided weakness Ashley Graziano OMS IV, Lake Erie College of Osteopathic Medicine Erik Yannone MD, Charles Q. Li MD, Warren Chang MD, Matthew
AMSER Case of the Month: March 2019 62 year-old male with left-sided weakness Ashley Graziano OMS IV, Lake Erie College of Osteopathic Medicine Erik Yannone MD, Charles Q. Li MD, Warren Chang MD, Matthew
About 700,000 Americans each year suffer a new or recurrent stroke. On average, a stroke occurs every 45 seconds
 UCLA Stroke Center Stroke Facts About 700,000 Americans each year suffer a new or recurrent stroke On average, a stroke occurs every 45 seconds Stroke kills more than 150,000 people a year (1 of every
UCLA Stroke Center Stroke Facts About 700,000 Americans each year suffer a new or recurrent stroke On average, a stroke occurs every 45 seconds Stroke kills more than 150,000 people a year (1 of every
Pr Roman Sztajzel Service de Neurologie HUG
 Pr Roman Sztajzel Service de Neurologie HUG Conflict of interest: none IV THROMBOLYSIS AND ENDOVASCULAR THROMBECTOMY approved treatments of acute stroke main criteria time (delay) IV thrombolysis radiological
Pr Roman Sztajzel Service de Neurologie HUG Conflict of interest: none IV THROMBOLYSIS AND ENDOVASCULAR THROMBECTOMY approved treatments of acute stroke main criteria time (delay) IV thrombolysis radiological
Acute Management of Stroke due to Intracranial Steno-occlusion. Joon-Tae Kim, MD, PhD Department of Neurology Chonnam National University Hospital
 Acute Management of Stroke due to Intracranial Steno-occlusion Joon-Tae Kim, MD, PhD Department of Neurology Chonnam National University Hospital None Disclosure Contents Current status of acute management
Acute Management of Stroke due to Intracranial Steno-occlusion Joon-Tae Kim, MD, PhD Department of Neurology Chonnam National University Hospital None Disclosure Contents Current status of acute management
Acute Ischemic Stroke Imaging Innovations
 Acute Ischemic Stroke Imaging Innovations Guilherme Dabus, MD, FAHA Director, Fellowship NeuroInterventional Surgery Miami Cardiac & Vascular Institute Baptist Neuroscience Center Baptist Neuroscience
Acute Ischemic Stroke Imaging Innovations Guilherme Dabus, MD, FAHA Director, Fellowship NeuroInterventional Surgery Miami Cardiac & Vascular Institute Baptist Neuroscience Center Baptist Neuroscience
DISCLOSURES OBJECTIVES 11/18/2014. Stroke Network Update. None. Discuss
 Stroke Network Update MOUHAMMAD A. JUMAA MD ASSISTANT PROFESSOR VASCULAR & INTERVENTIONAL NEUROLOGY UNIVERSITY OF TOLEDO DISCLOSURES None OBJECTIVES Discuss Regional stroke systems of care in NW OHIO Evolution
Stroke Network Update MOUHAMMAD A. JUMAA MD ASSISTANT PROFESSOR VASCULAR & INTERVENTIONAL NEUROLOGY UNIVERSITY OF TOLEDO DISCLOSURES None OBJECTIVES Discuss Regional stroke systems of care in NW OHIO Evolution
Patient selection for i.v. thrombolysis and thrombectomy
 3 rd Congress of the European Academy of Neurology Amsterdam, The Netherlands, June 24 27, 2017 Teaching Course 8 Acute treatment and early secondary prevention of stroke Level 2 Patient selection for
3 rd Congress of the European Academy of Neurology Amsterdam, The Netherlands, June 24 27, 2017 Teaching Course 8 Acute treatment and early secondary prevention of stroke Level 2 Patient selection for
Stroke, Stroke, Stroke Where Do We Stop on the River? Comprehensive vs. Primary Stroke Centers
 Stroke, Stroke, Stroke Where Do We Stop on the River? Comprehensive vs. Primary Stroke Centers Peter D. Panagos, MD, FAHA, FACEP Departments of Neurology and Emergency Medicine Washington University School
Stroke, Stroke, Stroke Where Do We Stop on the River? Comprehensive vs. Primary Stroke Centers Peter D. Panagos, MD, FAHA, FACEP Departments of Neurology and Emergency Medicine Washington University School
Further Pragmatic Trials of Thrombectomy are Needed
 Further Pragmatic Trials of Thrombectomy are Needed Prof Keith W Muir Institute of Neuroscience & Psychology University of Glasgow Institute of Neurological Sciences Queen Elizabeth University Hospital
Further Pragmatic Trials of Thrombectomy are Needed Prof Keith W Muir Institute of Neuroscience & Psychology University of Glasgow Institute of Neurological Sciences Queen Elizabeth University Hospital
Case Report Successful Mechanical Thrombectomy of a Middle Cerebral Artery Occlusion 14 Hours after Stroke Onset
 Hindawi Case Reports in Neurological Medicine Volume 2017, Article ID 9289218, 4 pages https://doi.org/10.1155/2017/9289218 Case Report Successful Mechanical Thrombectomy of a Middle Cerebral Artery Occlusion
Hindawi Case Reports in Neurological Medicine Volume 2017, Article ID 9289218, 4 pages https://doi.org/10.1155/2017/9289218 Case Report Successful Mechanical Thrombectomy of a Middle Cerebral Artery Occlusion