Updates on Endovascular Therapy
|
|
|
- Adam Marcus Pearson
- 5 years ago
- Views:
Transcription
, FAHA Director, Cerebrovascular Center Associate Professor, CCLCM Staff, Vascular Neurology and Endovascular Surgical Neuroradiology")
1 Updates on Endovascular Therapy 5 th Annual Intermountain Stroke Conference October 16, 2017 M. Shazam Hussain, MD, FRCP(C), FAHA Director, Cerebrovascular Center Associate Professor, CCLCM Staff, Vascular Neurology and Endovascular Surgical Neuroradiology Cerebrovascular Center, Neurological Institute Cleveland Clinic hussais4@ccf.org
2 Disclosures Local PI Swift Prime, STRATIS study Pulsar Clinical events committee Off label uses of devices and therapies
3 Objectives Appraise the evidence supporting the use of mechanical thrombectomy in acute ischemic stroke in the early (<6 hours) time window. Appraise the evidence supporting the use of mechanical thrombectomy in acute ischemic stroke in the late (6-24 hour) time window. Contrast Time based selection and Tissue based selection of candidates for Mechanical Thrombectomy. Discuss Stroke Systems of Care Development.

4 4 Stroke is the No. 5 cause of death in the U.S. It is the No. 1 cause of disability in the U.S.
5 Time is Brain! Neurons Lost Synapses Lost Accelerated Aging Per Stroke 1.2 billion 8.3 trillion 36 yrs Per Hour 120 million 830 billion 3.6 yrs Per Minute 1.9 million 14 billion 3.1 weeks Per Second 32, million 8.7 hrs (Total number of neurons in the average human brain is 130 billion) Stroke 2006;37:

6 No Reperfusion Reperfusion


7 Acute Stroke Treatments Are Effective

8



9


10
11 2015: Level 1A Evidence Established FIVE major prospective, randomized controlled trials have been published comparing mechanical thrombectomy to best medical management: MR CLEAN ESCAPE EXTEND-IA SWIFT PRIME REVASCAT

12 A Multicenter Randomized CLinical trial of Endovascular treatment for Acute ischemic stroke in the Netherlands (MR CLEAN) Sites: 16 centers in Netherlands Patients: randomized to IA thrombectomy 267 randomized to medical management Age 18+ Included mild-severe stroke severity Time: Treatment initiated within 6 hrs Primary Outcome: mrs at 90 days Treatment in IA arm: No requirement, but retrievable stent in majority Berkhemer et al; NEJM, 2015
 Good Outcome (mrs 0-2): 33% in")

13 A Multicenter Randomized CLinical trial of Endovascular treatment for Acute ischemic stroke in the Netherlands (MR CLEAN) Good Outcome (mrs 0-2): 33% in IA thrombectomy group 19% in medical group Conclusion: Significantly better outcomes with thrombectomy compared to medical management Berkhemer et al; NEJM, 2015

14 Endovascular Treatment for Small Core and Proximal Occlusion Ischemic StrokE (ESCAPE) Sites: 22 centers mostly in N America Patients: 315 (halted early due to efficacy) 165 randomized to IA thrombectomy 150 randomized to medical Age 18+ Included mild-severe strokes Time: Treatment within 12 hours of onset Primary Outcome: mrs at 90 days Treatment in IA arm: Retrievable stent Goyal et al; NEJM, 2015
 Good Outcome (mrs 0-2): 53% in IA")

15 Endovascular Treatment for Small Core and Proximal Occlusion Ischemic StrokE (ESCAPE) Good Outcome (mrs 0-2): 53% in IA thrombectomy group 29% in medical group Conclusion: Significantly better outcomes with thrombectomy compared to medical management Goyal et al; NEJM, 2015

16 Extending the Time for Thrombolysis in Emergency Neurological Deficits Intra- Arterial (EXTEND-IA) Sites: 10 centers mostly in Australia and New Zealand Patients: 70 (halted early due to efficacy) 35 randomized to IA thrombectomy 35 randomized to medical Age 18+ Included mild-severe strokes Time: Within 6 hours of onset Primary Outcomes: 1. Reperfusion at 24 hours (% reduction in perfusionlesion volume) 2. Decrease in NIHSS of 8 or more points at 3 days, or NIHSS of 0 or 1 at 3 days Treatment in IA arm: retrievable stent Campbell et al; NEJM, 2015
 Good Outcome (mrs 0-2): 71% in IA")

17 Extending the Time for Thrombolysis in Emergency Neurological Deficits Intra- Arterial (EXTEND-IA) Good Outcome (mrs 0-2): 71% in IA thrombectomy group 40% in medical group Conclusion: Significantly better outcomes with thrombectomy compared to medical management Campbell et al; NEJM, 2015

18 Solitaire With the Intention For Thrombectomy as PRIMary Endovascular treatment (SWIFT PRIME) Sites: 39 centers mostly in US and Europe Patients: 196 (halted early due to efficacy) 98 randomized to IA thrombectomy 98 randomized to medical Age Included moderate-severe strokes Time: Within 6 hours of onset and within 1.5 hours of imaging Primary Outcome: mrs at 90 days Treatment in IA arm: retrievable stent Saver et al; NEJM, 2015
 Good Outcome (mrs 0-2): 60% in IA thrombectomy")

19 Solitaire With the Intention For Thrombectomy as PRIMary Endovascular treatment (SWIFT PRIME) Good Outcome (mrs 0-2): 60% in IA thrombectomy group 35% in medical group Conclusion: Significantly better outcomes with thrombectomy compared to medical management Saver et al; NEJM, 2015

20 Endovascular Revascularization With Solitaire Device Versus Best Medical Therapy in Anterior Circulation Stroke Within 8 Hours (REVASCAT) Sites: 4 centers in Spain Patients: randomized to IA thrombectomy 103 randomized to medical Age Included mild-severe strokes Time: Within 8 hours of onset Primary Outcome: mrs at 90 days Treatment in IA arm: retrievable stent Jovin et al; NEJM, 2015


21 Endovascular Revascularization With Solitaire Device Versus Best Medical Therapy in Anterior Circulation Stroke Within 8 Hours (REVASCAT) Good Outcome (mrs 0-2): 44% in IA thrombectomy group 28% in medical group Jovin et al; NEJM, 2015
22 Good Outcome (%) Rankin 0-2 at 90 days Stroke Trials: Outcome MR CLEAN REVASCAT ESCAPE SWIFT PRIME EXTEND- IA THERAPY P<0.5 P<0.05 P<0.001 P<0.001 P<0.01 NS MT 33% 44% 53% 60% 71% 38% Control 19% 28% 29% 36% 40% 30%

23




24 New Device Technology is a Game Changer Stentriever Large Bore Aspiration Catheters
25 Stroke Trials: Time to Reperfusion Patients with substantial (TICI 2b/3 reperfusion had better 90 day outcomes Patients with more rapid reperfusion had better 90 day outcomes Prabhakaran et al; JAMA, 2015

26 HERMES: Pooled Data of Trials Lancet 2016; 387:


27 AHA/ ASA Guidelines new revised unchanged Class I: Endovascular Therapy Pts should receive IAT if they: Have baseline mrs 1, received tpa, ICA or M1 occlusion, 18yo, NIHSS 6, ASPECTS 6, start treatment within 6hrs (LOE A, new) If considering IAT, vessel imaging recommended but should not delay IV tpa (LOE A, new)
28 AHA/ ASA Guidelines new revised unchanged Class II: Endovascular Therapy Treatment >6hrs, benefit unclear (IIb, LOE C, new) Treatment reasonable but benefit unclear in M2, M3, vertebral, basilar, PCA occlusions (IIb, LOE C, new) Treatment reasonable but benefit unclear in those <6hrs, mrs>1, ASPECTS<6, NIHSS<6 with ICA, M1 occlusion (IIb, LOE B-R, new) Goal TICI 2b/3 (IIb, LOE B-R, new) Treatment reasonable but benefit unclear in <18yo with LVO and tx within 6hrs (IIb, LOE C, new)
29 How Should This Change Practice Stroke team / endovascular team should be notified as soon as patient gets to the hospital or transfer is requested All patients should get IV tpa if eligible All patients should be considered for endovascular therapy Non-Contrast CT head to make initial decisions Vessel imaging only if it does not delay IV tpa Communicate with endovascular team as soon as possible
30 Extending the Window for Intra-arterial Stroke Therapy
31 Case: 45 y.o. with aphasia and right sided weakness History of Present Illness: Visiting mother, last seen well night before In am, mother found him later lying on bathroom floor unable to get up EMS called, noted to have global aphasia and dense right sided weakness
32 Case: Past Medical History: None Past Surgical History: None Social History: Ambulates independently Medications: None Family History: None Review of Systems: None
33 Case: Physical Exam: Vitals: Temp 36.8⁰C, HR 90, BP 150/84, RR 20, SpO 2 95% RA General: no acute distress Lungs: Clear to auscultation bilaterally, good air exchange Heart: regular rhythm, no murmurs Abdomen: soft, obese, non-tender, nondistended, normal bowel sounds Skin: Normal color, texture and turgor. No overt trauma
34 Case: NIHSS 1: Level of Consciousness (LOC) 6. Motor Leg 1a: LOC Responsiveness 0 6a: Motor L Leg 0 1b: LOC Questions 2 6b: Motor R Leg 4 1c: LOC Commands 2 7. Limb Ataxia 0 2. Horizontal Eye Movement (Best Gaze) 2 8. Sensory 2 3. Visual Field Test 2 9. Speech (Best Language) 3 4. Facial Palsy Dysarthria 0 5. Motor Arm 11: Extinction & Inattention 0 5a: Motor L Arm 0 5b: Motor R Arm 4 Total NIHSS: 23

35
36
37 Would you offer intra-arterial stroke therapy?
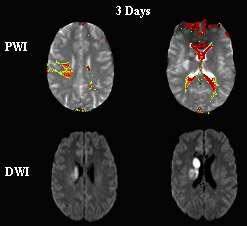
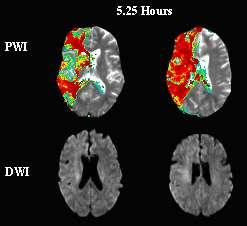
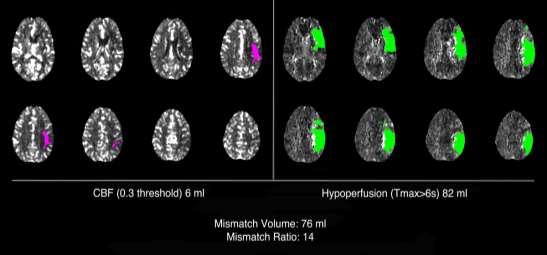
 to better identify core infarct/penumbral")
38 Need a proper target: Salvageable Brain We still do not have consensus on what the best selection approach is Time based: Time is most critical factor, thus, should minimize imaging before procedure Tissue based: Try to utilized advanced imaging (MRI DWI, MRI or CT Perfusion) to better identify core infarct/penumbral tissue/collaterals

39


40



41

42

43

44 Late-Presenting Strokes: The DEFUSE 3 and DAWN trials
45 Extending the Time Window DAWN and DEFUSE 3 2 Trials assessing extending the time window past 6 hours have recently been stopped due to overwhelming efficacy. DAWN: 6-24 hours post onset. Imaging selection (RAPID) Significant benefit in primary outcome (mrs 0-2 at 90 days) NNT 2.0!!! DEFUSE 3: Interim analysis suggested high likelihood of benefit. Results to be presented soon.
46 DAWN DWI or CTP Assessment with Clinical Mismatch In the Triage of Wake-Up and Late Presenting Strokes Undergoing Neurointervention with Trevo To demonstrate superior functional outcomes at 90 days with Trevo plus medical management compared to medical management alone in appropriately selected patients treated 6-24 hours after last seen well Courtesy of Drs. Jovin and Nogueira
47 DAWN Courtesy of Drs. Jovin and Nogueira

48 DAWN
49 Secondary Endpoints Significant benefit Less infarct growth Early response by NIHSS Recanalization rate at 24 hours No significant difference No mortality benefit Full analysis, results and publication pending

50 Principle Investigators Dr. Gregory W. Albers, Stanford University Dr. Michael P. Marks, Stanford University Funding NIH StrokeNet
51 DEFUSE 3 NIH-funded, prospective, randomized, multi-center, phase III, adaptive, blinded endpoint, controlled trial Paradigm shift From clock-based selection to imaging-based selection Target population Patients with anterior circulation ischemic strokes Presenting within 6-16 hours of last known well Imaging evidence of limited ischemic core and large penumbra
52 Clinical Criteria DEFUSE 3 Imaging Criteria Presentation consistent with an anterior circulation ischemic stroke Age years Baseline NIHSS 6 Pre-stroke mrs 0-2 Endovascular treatment feasible within 6-16 hours from LKW Key Inclusion Criteria Key Exclusion Criteria ASPECT Score 6 on non-contrast CT heaad MR or CT angiography shows an ICA or MCA-M1 occlusion Target mismatch on CTP or PWI (RAPID): Ischemic core < 70mL Mismatch ratio 1.8 and mismatch volume 15 ml Or DWI lesion <25 ml if obtained within 60 ml of CTA/MRA* Treatment with tpa > 4.5 h or thrombectomy < 6 h from LKW Stroke in multiple locations or suspected bacterial endocarditis Concurrent other serious illness or life expectancy < 6 months Evidence of intracranial tumor, acute intracranial hemorrhage, or AVM Significant mass effect with midline shift Evidence of ICA flow-limiting dissection or aortic dissection SBP > 185 / DBP > 110 mmhg not treatable with medications Contraindications for contrast, incl. refractory iodine allergy Participation in another investigational drug/device study/registry Occlusions in multiple vascular territories Intracranial stent implanted in the same vascular territory that would preclude safe deployment / removal of the neurothrombectomy device Only ~50% of patients in DEFUSE 3 are DAWN-eligible


53 DEFUSE 3 Eligibility
54 DEFUSE 3 DEFUSE 3 Planned Timetable Year 1 Year 2 Year 3 (or N=200 ) Install RAPID at all sites Begin enrollment (early 2016) Enrollment continues (projected total of 4 years) 1 st interim analysis Potential stop or modification of enrollment criteria based on adaptive design 1 st subject enrolled in May nd and final patient enrolled in May 2017 Pending 90-day follow-up Year 4 (or N=340 ) Year 5 2 nd interim analysis Potential stop or modification of enrollment criteria based on adaptive design Completion of enrollment, data analysis, and publication of results Enrollment halted after DAWN results announced Albers, GW et al. ISC 2016.
55 DEFUSE 3: Positive Result On Monday, July 24, 2017: The DSMB recommended study enrollment be permanently stopped for all subjects because of the high likelihood of benefit in the endovascular group. Results will be presented at the ISC in late January.
56 IMPLICATIONS OF EXTENDING PATIENT ELIGIBILITY FOR ENDOVASCULAR THERAPY
57 Extended Time Window Current treatment window <6 hours Large-vessel occlusion 11% of acute strokes Trials positive for patients up to hours Careful selection is key Possible further expansion of eligibility given on-going studies
58 Resources System structure likely needs to change Foreseeable challenges EMS training and availability Increase in ED volume Transfer resources to Comprehensive Stroke Centers Imaging volume Operational time, personnel, cost Hyperacute/acute stroke alerts Interventional Team availability Nurses, technicians, physicians
59

60
61 EMS Current Stroke System of Care EMS EMS PSC Spoke PSC Spoke EMS CSC Hub EMS EMS PSC Spoke EMS PSC Spoke EMS

62 Assessing Time Delays in a System Sun, Gupta et al. Circulation 2013 Sun, Gupta et al. Circulation 2013



63


64
65 How should we reorganize our stroke systems of care? a) Where should EMS bring stroke patients? b) Severity adjusted triage of patients by EMS c) Mobile Stroke Units to facilitate early recognition, appropriate triage, and quicker rtpa and IAT treatment
66 EMS Future Stroke System of Care EMS EMS PSC Spoke PSC Spoke EMS CSC Hub EMS EMS PSC Spoke EMS PSC Spoke EMS

67 Problem with all patients coming to CSCs Centralization can quickly overwhelm resources at CSCs Often are large tertiary/quaternary centers which are near capacity already Time range for bypass? 15min? 30 min? Likely would have to develop multiple CSCs based on population and geography Political issues

68
69 EMS determining severity in the field? LA Motor Score Cincinnati Pre Hospital Severity Scale RACE Score And many others

70 Cincinnati stroke scale Slide c/o Dr. R. Gupta

71 Los Angeles Motor Scale Nazliel B et al. Stroke. 2008;39: Slide c/o Dr. R. Gupta

72 85% accuracy with LAMS of 4 or 5 in detecting LVO Nazliel B et al. Stroke. 2008;39: Slide c/o Dr. R. Gupta

73 Mobile Stroke Treatment Unit: Diagnosis and Emergency Care Don t wait for the patient to go to ER Bring the CT and stroke expertise to the patient Initiate treatment at the scene Dramatically cut time-to-treatment decisions 73



74 First MSTU to solely utilize Telemedicine and Teleradiology for care.
 Reduced transfers to non-stroke unit centers Reduced ICHs transferred to non-neurosurgical")
75 Right Place, the first time Thus far, no patients have required a second transfer In keep with STEMO data (Wendt, Stroke 2015) Reduced transfers to non-stroke unit centers Reduced ICHs transferred to non-neurosurgical centers
76 Conclusions We now have Level 1A evidence for use of mechanical thrombectomy for Acute Ischemic stroke, both <6 hours and 6-24 hours post symptom onset. Patient with large vessel occlusion type stroke need to come to an interventional capable center as soon as possible Due to this, a redesign of stroke systems of care is required Careful planning based on population, geography etc is required.

77 Questions?
Broadening the Stroke Window in Light of the DAWN Trial
 Broadening the Stroke Window in Light of the DAWN Trial South Jersey Neurovascular and Stroke Symposium April 26, 2018 Rohan Chitale, MD Assistant Professor of Neurological Surgery Vanderbilt University
Broadening the Stroke Window in Light of the DAWN Trial South Jersey Neurovascular and Stroke Symposium April 26, 2018 Rohan Chitale, MD Assistant Professor of Neurological Surgery Vanderbilt University
Update on Early Acute Ischemic Stroke Interventions
 Update on Early Acute Ischemic Stroke Interventions Diana Goodman MD Lead Neurohospitalist Maine Medical Center Assistant Professor of Neurology, Tufts University School of Medicine I have no disclosures
Update on Early Acute Ischemic Stroke Interventions Diana Goodman MD Lead Neurohospitalist Maine Medical Center Assistant Professor of Neurology, Tufts University School of Medicine I have no disclosures
Stroke Treatment Beyond Traditional Time Windows. Rishi Gupta, MD, MBA
 Stroke Treatment Beyond Traditional Time Windows Rishi Gupta, MD, MBA Director, Stroke and Neurocritical Care Endovascular Neurosurgery Wellstar Health System THE PAST THE PRESENT 2015 American Heart Association/American
Stroke Treatment Beyond Traditional Time Windows Rishi Gupta, MD, MBA Director, Stroke and Neurocritical Care Endovascular Neurosurgery Wellstar Health System THE PAST THE PRESENT 2015 American Heart Association/American
The DAWN of a New Era for Wake-up Stroke
 The DAWN of a New Era for Wake-up Stroke Alan H. Yee, D.O. Stroke and Critical Care Neurology Department of Neurology University of California Davis Medical Center Objectives Review Epidemiology and Natural
The DAWN of a New Era for Wake-up Stroke Alan H. Yee, D.O. Stroke and Critical Care Neurology Department of Neurology University of California Davis Medical Center Objectives Review Epidemiology and Natural
Stroke Update Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center
 Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients
 Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School
Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School
Endovascular Treatment Updates in Stroke Care
 Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Endovascular Stroke Therapy
 Endovascular Stroke Therapy Update with Emphasis on Practical Clinical and Imaging Considerations Sachin Kishore Pandey, MD, FRCPC Disclosures I have no relevant financial disclosures or conflict of interest
Endovascular Stroke Therapy Update with Emphasis on Practical Clinical and Imaging Considerations Sachin Kishore Pandey, MD, FRCPC Disclosures I have no relevant financial disclosures or conflict of interest
Mechanical Thrombectomy: Where Are We Now? T. Adam Oliver, MD Tallahassee Neurological Clinic Tallahassee, Florida TMH Neurosymposium June 11, 2016
 Mechanical Thrombectomy: Where Are We Now? T. Adam Oliver, MD Tallahassee Neurological Clinic Tallahassee, Florida TMH Neurosymposium June 11, 2016 none DISCLOSURES Where did we come from? Spiotta, et
Mechanical Thrombectomy: Where Are We Now? T. Adam Oliver, MD Tallahassee Neurological Clinic Tallahassee, Florida TMH Neurosymposium June 11, 2016 none DISCLOSURES Where did we come from? Spiotta, et
Interventional Treatment of Stroke
 Interventional Treatment of Stroke Andrew F. Ducruet, MD Barrow Neurological Institute 2018 BNI Stroke Rehab Symposium October 13, 2018 Disclosures Consultant: Medtronic, Penumbra, Cerenovus Lecture Overview
Interventional Treatment of Stroke Andrew F. Ducruet, MD Barrow Neurological Institute 2018 BNI Stroke Rehab Symposium October 13, 2018 Disclosures Consultant: Medtronic, Penumbra, Cerenovus Lecture Overview
Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington
 Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington Disclosures: SWIFT PRIME site (Medtronic) Physician Proctor
Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington Disclosures: SWIFT PRIME site (Medtronic) Physician Proctor
Acute Stroke Treatment: Current Trends 2010
 Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
RBWH ICU Journal Club February 2018 Adam Simpson
 RBWH ICU Journal Club February 2018 Adam Simpson 3 THROMBOLYSIS Reperfusion therapy has become the mainstay of therapy for ischaemic stroke. Thrombolysis is now well accepted within 4.5 hours. - Improved
RBWH ICU Journal Club February 2018 Adam Simpson 3 THROMBOLYSIS Reperfusion therapy has become the mainstay of therapy for ischaemic stroke. Thrombolysis is now well accepted within 4.5 hours. - Improved
Disclosures. Current Management of Acute Ischemic Stroke. Overview. Focal brain ischemia. Nerissa U. Ko, MD, MAS Professor of Neurology May 8, 2015
 Disclosures Current Management of Acute Ischemic Nerissa U. Ko, MD, MAS Professor of Neurology May 8, 2015 Nothing to disclose Research Funding: American Heart Association NIH/NINDS Selected slides courtesy
Disclosures Current Management of Acute Ischemic Nerissa U. Ko, MD, MAS Professor of Neurology May 8, 2015 Nothing to disclose Research Funding: American Heart Association NIH/NINDS Selected slides courtesy
Mechanical thrombectomy beyond the 6 hours. Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital
 Mechanical thrombectomy beyond the 6 hours Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital Disclosures None Worldwide statistics 1 IN 6 people will have a stroke at some
Mechanical thrombectomy beyond the 6 hours Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital Disclosures None Worldwide statistics 1 IN 6 people will have a stroke at some
Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke
 Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke Alexander A. Khalessi MD MS Director of Endovascular Neurosurgery Surgical Director of NeuroCritical Care University
Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke Alexander A. Khalessi MD MS Director of Endovascular Neurosurgery Surgical Director of NeuroCritical Care University
CVA Updates Karen Greenberg, DO, FACOEP. Director Neurologic Emergency Department Crozer Chester Medical Center
 CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
Mechanical thrombectomy in Plymouth. Will Adams. Will Adams
 Mechanical thrombectomy in Plymouth Will Adams Will Adams History Intra-arterial intervention 1995 (NINDS) iv tpa improved clinical outcome in patients treated within 3 hours of ictus but limited recanalisation
Mechanical thrombectomy in Plymouth Will Adams Will Adams History Intra-arterial intervention 1995 (NINDS) iv tpa improved clinical outcome in patients treated within 3 hours of ictus but limited recanalisation
Better identification of patients who may benefit from therapy
 Jon Jui MD, MPH Large Vessel Occlusion Low rates of re-canalization after tpa Only 25 % of large vessel strokes re-canalization after tpa Newer invasive techniques Solitaire vs Merci Better identification
Jon Jui MD, MPH Large Vessel Occlusion Low rates of re-canalization after tpa Only 25 % of large vessel strokes re-canalization after tpa Newer invasive techniques Solitaire vs Merci Better identification
Stroke: The First Critical Hour. Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP
 Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
CT Perfusion is Essential for Stroke Triage. Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center
 CT Perfusion is Essential for Stroke Triage Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center CT Perfusion is Essential for Stroke Triage Disclosures:
CT Perfusion is Essential for Stroke Triage Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center CT Perfusion is Essential for Stroke Triage Disclosures:
5/31/2018. Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment. Disclosures. Impact of clot burden
 Good Outcome (%) Rankin 0-2 at 90 days 5/31/2018 Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment Disclosures Cerenovus: I am on Executive Committee for ARISE2 Trial
Good Outcome (%) Rankin 0-2 at 90 days 5/31/2018 Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment Disclosures Cerenovus: I am on Executive Committee for ARISE2 Trial
UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015
 UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015 NEW STUDIES FOR 2015 MR CLEAN ESCAPE EXTEND-IA REVASCAT SWIFT PRIME RECOGNIZED LIMITATIONS IV Alteplase proven benefit
UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015 NEW STUDIES FOR 2015 MR CLEAN ESCAPE EXTEND-IA REVASCAT SWIFT PRIME RECOGNIZED LIMITATIONS IV Alteplase proven benefit
Evidence for Mechanical ThrombectomyFor Acute Ischemic Stroke. Kenneth V Snyder MD PhD SUNY Buffalo, NY
 Evidence for Mechanical ThrombectomyFor Acute Ischemic Stroke Kenneth V Snyder MD PhD SUNY Buffalo, NY Disclosure Speaker name:... I have the following potential conflicts of interest to report: Honorarium
Evidence for Mechanical ThrombectomyFor Acute Ischemic Stroke Kenneth V Snyder MD PhD SUNY Buffalo, NY Disclosure Speaker name:... I have the following potential conflicts of interest to report: Honorarium
Endovascular Treatment of Ischemic Stroke
 Endovascular Treatment of Ischemic Stroke William Thorell, MD Associate Professor Neurosurgery UNMC Co-Director Stroke and Neurovascular Center Nebraska Medicine Overview Definitions of terms Review basic
Endovascular Treatment of Ischemic Stroke William Thorell, MD Associate Professor Neurosurgery UNMC Co-Director Stroke and Neurovascular Center Nebraska Medicine Overview Definitions of terms Review basic
BGS Spring Conference 2015
 Neuroradiology in hyperacute stroke: what is the UK position? Dr Shelley Renowden Bristol NICE HIS July, 2013 The current evidence on mechanical clot retrieval for treating acute ischaemic stroke shows
Neuroradiology in hyperacute stroke: what is the UK position? Dr Shelley Renowden Bristol NICE HIS July, 2013 The current evidence on mechanical clot retrieval for treating acute ischaemic stroke shows
Imaging Stroke: Is There a Stroke Equivalent of the ECG? Albert J. Yoo, MD Director of Acute Stroke Intervention Massachusetts General Hospital
 Imaging Stroke: Is There a Stroke Equivalent of the ECG? Albert J. Yoo, MD Director of Acute Stroke Intervention Massachusetts General Hospital Disclosures Penumbra, Inc. research grant (significant) for
Imaging Stroke: Is There a Stroke Equivalent of the ECG? Albert J. Yoo, MD Director of Acute Stroke Intervention Massachusetts General Hospital Disclosures Penumbra, Inc. research grant (significant) for
Endovascular Clot Retrieval. Teddy Wu Neurologist (and Stroke enthusiast) Christchurch Hospital
 Christchurch Hospital") Endovascular Clot Retrieval Teddy Wu Neurologist (and Stroke enthusiast) Christchurch Hospital Something you can do tomorrow Melbourne half marathon 2016 In 2009 Simple approach to stroke - blocked artery,
Endovascular Clot Retrieval Teddy Wu Neurologist (and Stroke enthusiast) Christchurch Hospital Something you can do tomorrow Melbourne half marathon 2016 In 2009 Simple approach to stroke - blocked artery,
EVOLUTION IN SYSTEMS OF STROKE CARE RIDWAN LIN, MD, PHD STROKE & INTERVENTIONAL NEUROLOGY BROWARD HEALTH
 EVOLUTION IN SYSTEMS OF STROKE CARE RIDWAN LIN, MD, PHD STROKE & INTERVENTIONAL NEUROLOGY BROWARD HEALTH STROKE SYSTEMS OF CARE: 7. Secondary prevention 1. Primary prevention Patient 3. Emergency transport
EVOLUTION IN SYSTEMS OF STROKE CARE RIDWAN LIN, MD, PHD STROKE & INTERVENTIONAL NEUROLOGY BROWARD HEALTH STROKE SYSTEMS OF CARE: 7. Secondary prevention 1. Primary prevention Patient 3. Emergency transport
Endovascular Neurointervention in Cerebral Ischemia
 Endovascular Neurointervention in Cerebral Ischemia Beyond Thrombolytics Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington 72 y/o female with a recent diagnosis
Endovascular Neurointervention in Cerebral Ischemia Beyond Thrombolytics Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington 72 y/o female with a recent diagnosis
Endovascular Treatment for Acute Ischemic Stroke
 ular Treatment for Acute Ischemic Stroke Vishal B. Jani MD Assistant Professor Interventional Neurology, Division of Department of Neurology. Creighton University/ CHI health Omaha NE Disclosure None 1
ular Treatment for Acute Ischemic Stroke Vishal B. Jani MD Assistant Professor Interventional Neurology, Division of Department of Neurology. Creighton University/ CHI health Omaha NE Disclosure None 1
Interventional Stroke Treatment
 Interventional Stroke Treatment Vishal B. Jani MD Medical Director Vascular Neurology Consultant Interventional Neurology CHI Health Assistant Professor, Creighton University School of Medicine Omaha,
Interventional Stroke Treatment Vishal B. Jani MD Medical Director Vascular Neurology Consultant Interventional Neurology CHI Health Assistant Professor, Creighton University School of Medicine Omaha,
12/4/2017. Disclosures. Study organization. Stryker Medtronic Penumbra Viz Route 92. Data safety monitoring board Tudor G.
 12/4/2017 Update on Stroke Trials:Extending the Window DWI or CTP Assessment with Clinical Mismatch in the Triage of Wake-Up and Late Presenting Strokes Undergoing Neurointervention with Trevo NP001713
12/4/2017 Update on Stroke Trials:Extending the Window DWI or CTP Assessment with Clinical Mismatch in the Triage of Wake-Up and Late Presenting Strokes Undergoing Neurointervention with Trevo NP001713
Latest Advances in the Neurointerventional Treatment of Ischemic Stroke P A C I F I C N E U R O. O R G
 Latest Advances in the Neurointerventional Treatment of Ischemic Stroke Neurointerventional Management of Ischemic Stroke 1. Thrombectomy for acute ischemic stroke 2. Carotid artery stenting 3. Management
Latest Advances in the Neurointerventional Treatment of Ischemic Stroke Neurointerventional Management of Ischemic Stroke 1. Thrombectomy for acute ischemic stroke 2. Carotid artery stenting 3. Management
Acute Stroke Identification and Treatment
 Acute Stroke Identification and Treatment James S. McKinney, MD, FAHA Medical Director, NHRMC Stroke Center SE NC is located in the buckle of the Stroke Belt, seeing the highest stroke incidence and mortality
Acute Stroke Identification and Treatment James S. McKinney, MD, FAHA Medical Director, NHRMC Stroke Center SE NC is located in the buckle of the Stroke Belt, seeing the highest stroke incidence and mortality
Advances in Neuro-Endovascular Care for Acute Stroke
 Advances in Neuro-Endovascular Care for Acute Stroke Ciarán J. Powers, MD, PhD, FAANS Associate Professor Program Director Department of Neurological Surgery Surgical Director Comprehensive Stroke Center
Advances in Neuro-Endovascular Care for Acute Stroke Ciarán J. Powers, MD, PhD, FAANS Associate Professor Program Director Department of Neurological Surgery Surgical Director Comprehensive Stroke Center
Case 1 5/26/2017 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE
 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
Getting the Right Stroke Patient to the Right Hospital: Pre-hospital Assessment Tools
 Getting the Right Stroke Patient to the Right Hospital: Pre-hospital Assessment Tools Francis X Guyette, MD, MPH Associate Professor of Emergency Medicine University of Pittsburgh School of Medicine Medical
Getting the Right Stroke Patient to the Right Hospital: Pre-hospital Assessment Tools Francis X Guyette, MD, MPH Associate Professor of Emergency Medicine University of Pittsburgh School of Medicine Medical
Statewide Acute Stroke Triage The Washington Story
 Statewide Acute Stroke Triage The Washington Story David Tirschwell, MD, MSc Medical Director of Comprehensive Stroke Care Professor, Department of Neurology UW Medicine Comprehensive Stroke Center at
Statewide Acute Stroke Triage The Washington Story David Tirschwell, MD, MSc Medical Director of Comprehensive Stroke Care Professor, Department of Neurology UW Medicine Comprehensive Stroke Center at
ACUTE ISCHEMIC STROKE
 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE HHS Stroke Annual Review March 7 and March 8, 2018 Objectives To review the stroke endovascular mechanical thrombectomy evidence
ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE HHS Stroke Annual Review March 7 and March 8, 2018 Objectives To review the stroke endovascular mechanical thrombectomy evidence
Disclosure. Advances in Interventional Neurology. Disclosure. Natural History of Disease 3/15/2018. Vishal B. Jani MD
 Advances in Interventional Neurology Disclosure Vishal B. Jani MD Medical Director Vascular Neurology Consultant Interventional Neurology CHI Health Assistant Professor, Creighton University School of
Advances in Interventional Neurology Disclosure Vishal B. Jani MD Medical Director Vascular Neurology Consultant Interventional Neurology CHI Health Assistant Professor, Creighton University School of
Acute Stroke Management Conference 2019: Stroke Clinical Vignettes
 Acute Stroke Management Conference 2019: Stroke Clinical Vignettes Cynthia Kenmuir MD PhD Director of Stroke Program, UPMC Altoona Director of Neurointerventional Program, UPMC Altoona 2015 Guideline for
Acute Stroke Management Conference 2019: Stroke Clinical Vignettes Cynthia Kenmuir MD PhD Director of Stroke Program, UPMC Altoona Director of Neurointerventional Program, UPMC Altoona 2015 Guideline for
Acute Ischemic Stroke Imaging. Ronald L. Wolf, MD, PhD Associate Professor of Radiology
 Acute Ischemic Stroke Imaging Ronald L. Wolf, MD, PhD Associate Professor of Radiology Title of First Slide of Substance An Illustrative Case 2 Disclosures No financial disclosures Off-label uses of some
Acute Ischemic Stroke Imaging Ronald L. Wolf, MD, PhD Associate Professor of Radiology Title of First Slide of Substance An Illustrative Case 2 Disclosures No financial disclosures Off-label uses of some
Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY
 Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part A. Objectives Epidemiology of AIS and of ELVO Concept: Acute Ischemic
Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part A. Objectives Epidemiology of AIS and of ELVO Concept: Acute Ischemic
How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval
 How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval Peter Howard MD FRCPC Disclosures No conflicts to disclose How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular
How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval Peter Howard MD FRCPC Disclosures No conflicts to disclose How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular
Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices
 Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices Joey English MD, PhD Medical Director, Neurointerventional Services California Pacific Medical Center Hospitals, San Francisco,
Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices Joey English MD, PhD Medical Director, Neurointerventional Services California Pacific Medical Center Hospitals, San Francisco,
Strokecenter Key lessons of MR CLEAN study
 Strokecenter Key lessons of MR CLEAN study Diederik Dippel Disclosures Funded by the Dutch Heart Foundation Nominal, unrestricted grants from AngioCare BV Medtronic/Covidien/EV3 MEDAC Gmbh/LAMEPRO Penumbra
Strokecenter Key lessons of MR CLEAN study Diederik Dippel Disclosures Funded by the Dutch Heart Foundation Nominal, unrestricted grants from AngioCare BV Medtronic/Covidien/EV3 MEDAC Gmbh/LAMEPRO Penumbra
1/19/2018. Endovascular Therapy for Stroke
 Endovascular Therapy for Stroke 1 PROACT II (1999, IA urokinase)first to demonstrate benefit of EST Newer trials (including MERCI in 2005) demonstrated vessel recanalization but no clinical benefit 2 Based
Endovascular Therapy for Stroke 1 PROACT II (1999, IA urokinase)first to demonstrate benefit of EST Newer trials (including MERCI in 2005) demonstrated vessel recanalization but no clinical benefit 2 Based
Interventional Neuroradiology. & Stroke INR PROCEDURES INR PROCEDURES. Dr Steve Chryssidis. 25-Sep-17. Interventional Neuroradiology
 Interventional Neuroradiology Interventional Neuroradiology & Stroke Dr Steve Chryssidis Interventional Neuroradiology (INR) is a subspecialty within Radiology INR -- broadly defined as treatment by endovascular
Interventional Neuroradiology Interventional Neuroradiology & Stroke Dr Steve Chryssidis Interventional Neuroradiology (INR) is a subspecialty within Radiology INR -- broadly defined as treatment by endovascular
Intra-arterial Stroke Therapy: 2018 Update
 Intra-arterial Stroke Therapy: 2018 Update Expanding the Treatment Window Parita Bhuva, M.D. Medical Director Enrolling investigator Stryker Neurovascular (DAWN trial) Disclosures Most common large vessel
Intra-arterial Stroke Therapy: 2018 Update Expanding the Treatment Window Parita Bhuva, M.D. Medical Director Enrolling investigator Stryker Neurovascular (DAWN trial) Disclosures Most common large vessel
Slide 1. Slide 2. Slide 3 EMS STROKE CARE AND CSTAT OREGON STROKE NETWORK CONFERENCE 2018 SHAWN WOOD, CLINICAL MANAGER DISCLOSURES MY PATH TO EMS
 Slide 1 EMS STROKE CARE AND CSTAT OREGON STROKE NETWORK CONFERENCE 2018 SHAWN WOOD, CLINICAL MANAGER METRO WEST AMBULANCE Slide 2 DISCLOSURES No Financial Conflicts. I work as the Clinical Manager for
Slide 1 EMS STROKE CARE AND CSTAT OREGON STROKE NETWORK CONFERENCE 2018 SHAWN WOOD, CLINICAL MANAGER METRO WEST AMBULANCE Slide 2 DISCLOSURES No Financial Conflicts. I work as the Clinical Manager for
Top 5 Big Things in Acute Stroke Care! Raymond W. Grams II, DO Vascular Neurology Stroke Medical Director DRMC, Intermountain Healthcare
 Top 5 Big Things in Acute Stroke Care! Raymond W. Grams II, DO Vascular Neurology Stroke Medical Director DRMC, Intermountain Healthcare Late Time Window Endovascular Trials 48.6% WITH intervention vs
Top 5 Big Things in Acute Stroke Care! Raymond W. Grams II, DO Vascular Neurology Stroke Medical Director DRMC, Intermountain Healthcare Late Time Window Endovascular Trials 48.6% WITH intervention vs
Size Matters: Differentiating Large Vessel Occlusion (LVO) and Small Vessel Occlusion (SVO) in Stroke
 and Small Vessel Occlusion (SVO) in Stroke") Size Matters: Differentiating Large Vessel Occlusion (LVO) and Small Vessel Occlusion (SVO) in Stroke Charles E. Romero, M.D. UPMC Hamot Great Lakes Neurosurgery & Neurointervention Case 1 83 yo RH F with
Size Matters: Differentiating Large Vessel Occlusion (LVO) and Small Vessel Occlusion (SVO) in Stroke Charles E. Romero, M.D. UPMC Hamot Great Lakes Neurosurgery & Neurointervention Case 1 83 yo RH F with
Stroke, Stroke, Stroke Where Do We Stop on the River? Comprehensive vs. Primary Stroke Centers
 Stroke, Stroke, Stroke Where Do We Stop on the River? Comprehensive vs. Primary Stroke Centers Peter D. Panagos, MD, FAHA, FACEP Departments of Neurology and Emergency Medicine Washington University School
Stroke, Stroke, Stroke Where Do We Stop on the River? Comprehensive vs. Primary Stroke Centers Peter D. Panagos, MD, FAHA, FACEP Departments of Neurology and Emergency Medicine Washington University School
WHY TIMELINESS MATTERS. W&M Wren Association Lecture Series
 WHY TIMELINESS MATTERS April 10, 2018 W&M Wren Association Lecture Series Pankajavalli Ramakrishnan, M.D., Ph.D. Stroke Neurologist and Neurointerventionalist Riverside Regional Medical Center Comprehensive
WHY TIMELINESS MATTERS April 10, 2018 W&M Wren Association Lecture Series Pankajavalli Ramakrishnan, M.D., Ph.D. Stroke Neurologist and Neurointerventionalist Riverside Regional Medical Center Comprehensive
Code Stroke in real life. Disclosures. Parkland Memorial Hospital. I have no disclosures. Has 1 million patient visits annually. Level 1 Trauma Center
 Code Stroke in real life Alejandro Magadán, M.D. University of Texas Southwestern Medical Center Medical Director for Stroke Parkland Memorial Hospital Disclosures I have no disclosures Parkland Memorial
Code Stroke in real life Alejandro Magadán, M.D. University of Texas Southwestern Medical Center Medical Director for Stroke Parkland Memorial Hospital Disclosures I have no disclosures Parkland Memorial
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Mechanical Endovascular Reperfusion Therapy
 Get With the Guidelines Stroke Mechanical Endovascular Reperfusion Therapy February 1, 2017 Speaker Lee H. Schwamm, MD Executive Vice Chairman and Director of Stroke/TeleStroke Services, Department of
Get With the Guidelines Stroke Mechanical Endovascular Reperfusion Therapy February 1, 2017 Speaker Lee H. Schwamm, MD Executive Vice Chairman and Director of Stroke/TeleStroke Services, Department of
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Lessons Learned from IMS III: Implications for the Future
 Lessons Learned from IMS III: Implications for the Future Pooja Khatri, MD, MSc Professor, Dept of Neurology Director of Acute Stroke, UC Stroke Team University of Cincinnati Disclosures Univ of Cincinnati
Lessons Learned from IMS III: Implications for the Future Pooja Khatri, MD, MSc Professor, Dept of Neurology Director of Acute Stroke, UC Stroke Team University of Cincinnati Disclosures Univ of Cincinnati
Stroke Belt Consortium
 Field Triage And Diversion of Acute Stroke Charles Sand, MD Stroke Belt Consortium 10/26/12 WCF EMS Acute Stroke Advisory Committee Formed 2001 5 Original members Now > 100 members interdisciplinary expertise
Field Triage And Diversion of Acute Stroke Charles Sand, MD Stroke Belt Consortium 10/26/12 WCF EMS Acute Stroke Advisory Committee Formed 2001 5 Original members Now > 100 members interdisciplinary expertise
Ongoing Acute Stroke Studies 10/5/2015
 Ongoing Acute Stroke Studies 10/5/2015 Wade S. Smith, MD, PhD Director UCSF Neurovascular Service Daryl R. Gress Professor of Neurocritical Care and Stroke Disclosures NIH U10 NS 086494 (PI) NorCal RCC
Ongoing Acute Stroke Studies 10/5/2015 Wade S. Smith, MD, PhD Director UCSF Neurovascular Service Daryl R. Gress Professor of Neurocritical Care and Stroke Disclosures NIH U10 NS 086494 (PI) NorCal RCC
Update on Neurointerventional Therapies: Stroke and Aneurysms
 Update on Neurointerventional Therapies: Stroke and Aneurysms Gary Duckwiler, MD Professor and Director Division of Interventional Neuroradiology David Geffen School of Medicine at UCLA Long Beach Memorial
Update on Neurointerventional Therapies: Stroke and Aneurysms Gary Duckwiler, MD Professor and Director Division of Interventional Neuroradiology David Geffen School of Medicine at UCLA Long Beach Memorial
Best medical therapy (includes iv t-pa in eligible patients)
") UDATE ON REVASCAT: (Randomized Trial Of Revascularization With Solitaire FR Device Versus Best Medical Therapy In The Treatment Of Acute Stroke Due To Anterior Circulation Large Vessel Occlusion Presenting
UDATE ON REVASCAT: (Randomized Trial Of Revascularization With Solitaire FR Device Versus Best Medical Therapy In The Treatment Of Acute Stroke Due To Anterior Circulation Large Vessel Occlusion Presenting
ACUTE ISCHEMIC STROKE. Current Treatment Approaches for Acute Ischemic Stroke
 ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
Significant Relationships
 Opening Large Vessels During Acute Ischemic Stroke Significant Relationships Wade S Smith, MD, PhD Director UCSF Neurovascular Service Professor of Neurology Daryl R Gress Endowed Chair of Neurocritical
Opening Large Vessels During Acute Ischemic Stroke Significant Relationships Wade S Smith, MD, PhD Director UCSF Neurovascular Service Professor of Neurology Daryl R Gress Endowed Chair of Neurocritical
framework for flow Objectives Acute Stroke Treatment Collaterals in Acute Ischemic Stroke framework & basis for flow
 Acute Stroke Treatment Collaterals in Acute Ischemic Stroke Objectives role of collaterals in acute ischemic stroke collateral therapeutic strategies David S Liebeskind, MD Professor of Neurology & Director
Acute Stroke Treatment Collaterals in Acute Ischemic Stroke Objectives role of collaterals in acute ischemic stroke collateral therapeutic strategies David S Liebeskind, MD Professor of Neurology & Director
Code Stroke!! Amit Kansara, MD, FAHA. Joint EMS Conference Providence Brain and Spine Institute Providence Heart and Vascular Institute
 Code Stroke!! Amit Kansara, MD, FAHA Joint EMS Conference Providence Brain and Spine Institute Providence Heart and Vascular Institute February 22, 2019 Patient History: Dispatch 20:45: You are dispatched
Code Stroke!! Amit Kansara, MD, FAHA Joint EMS Conference Providence Brain and Spine Institute Providence Heart and Vascular Institute February 22, 2019 Patient History: Dispatch 20:45: You are dispatched
Endovascular Therapy: Beyond the Guidelines
 Endovascular Therapy: Beyond the Guidelines Ashutosh P. Jadhav, MD PhD Assistant Professor, Neurology and Neurological Surgery Center for Neuro-endovascular Therapy UPMC Stroke Institute Pittsburgh, PA
Endovascular Therapy: Beyond the Guidelines Ashutosh P. Jadhav, MD PhD Assistant Professor, Neurology and Neurological Surgery Center for Neuro-endovascular Therapy UPMC Stroke Institute Pittsburgh, PA
Pr Roman Sztajzel Service de Neurologie HUG
 Pr Roman Sztajzel Service de Neurologie HUG Conflict of interest: none IV THROMBOLYSIS AND ENDOVASCULAR THROMBECTOMY approved treatments of acute stroke main criteria time (delay) IV thrombolysis radiological
Pr Roman Sztajzel Service de Neurologie HUG Conflict of interest: none IV THROMBOLYSIS AND ENDOVASCULAR THROMBECTOMY approved treatments of acute stroke main criteria time (delay) IV thrombolysis radiological
Is there even a time window?
 Is there even a time window? A brief summary of key 2018 trials: DAWN and DEFUSE-3 For Neurosciences Update Conference, February 22, 2018 Maxim D. Hammer, M.D. Executive Summary Based on DAWN and DEFUSE-3,
Is there even a time window? A brief summary of key 2018 trials: DAWN and DEFUSE-3 For Neurosciences Update Conference, February 22, 2018 Maxim D. Hammer, M.D. Executive Summary Based on DAWN and DEFUSE-3,
Historical. Medical Policy
 Medical Policy Subject: Mechanical Embolectomy for Treatment of Acute Stroke Policy #: SURG.00098 Current Effective Date: 01/01/2016 Status: Revised Last Review Date: 08/06/2015 Description/Scope This
Medical Policy Subject: Mechanical Embolectomy for Treatment of Acute Stroke Policy #: SURG.00098 Current Effective Date: 01/01/2016 Status: Revised Last Review Date: 08/06/2015 Description/Scope This
Practical Considerations in the Early Treatment of Acute Stroke
 Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
DISCLOSURES. Learning Objectives. David Lee Gordon, MD, FAHA Update in Stroke 2007 FINANCIAL DISCLOSURE UNLABELED/UNAPPROVED USES DISCLOSURE
 Acute Stroke Care and the Role of EMS Ryan Hakimi, DO, MS April 30, 2015 Assistant Professor Director, Critical Care Neurology Department of Neurology University of Oklahoma Health Sciences Center DISCLOSURES
Acute Stroke Care and the Role of EMS Ryan Hakimi, DO, MS April 30, 2015 Assistant Professor Director, Critical Care Neurology Department of Neurology University of Oklahoma Health Sciences Center DISCLOSURES
Maximising Delivery of Thrombectomy
 Maximising Delivery of Thrombectomy Professor Gary Ford Chief Executive Officer, Oxford Academic Health Science Network Consultant Stroke Physician, Oxford University Hospitals Visiting Professor of Clinical
Maximising Delivery of Thrombectomy Professor Gary Ford Chief Executive Officer, Oxford Academic Health Science Network Consultant Stroke Physician, Oxford University Hospitals Visiting Professor of Clinical
DISCLOSURES HUY TRAN MD UNM DEPARTMENT OF NEUROLOGY AND NEUROSURGERY NO DISCLOSURES
 DISCLOSURES ANDREW HARRELL MD FAEMS UNM DEPARTMENT OF EMERGENCY MEDICINEUNM EMS MEDICAL DIRECTION CONSORTIUM MEDICAL DIRECTOR, ALBUQUERQUE FIRE DEPARTMENT MEDICAL DIRECTOR, GRAND CANYON NATIONAL PARK TEMS
DISCLOSURES ANDREW HARRELL MD FAEMS UNM DEPARTMENT OF EMERGENCY MEDICINEUNM EMS MEDICAL DIRECTION CONSORTIUM MEDICAL DIRECTOR, ALBUQUERQUE FIRE DEPARTMENT MEDICAL DIRECTOR, GRAND CANYON NATIONAL PARK TEMS
ELVO update. Michael Wilder, MD Director, Neurointerventional Program PeaceHealth Sacred Heart Springfield, Oregon
 ELVO update Michael Wilder, MD Director, Neurointerventional Program PeaceHealth Sacred Heart Springfield, Oregon Riverbend 24/7 thrombectomy ELVO alert Access PH PACU Anesthesia Goyal et al. Lancet. 2016
ELVO update Michael Wilder, MD Director, Neurointerventional Program PeaceHealth Sacred Heart Springfield, Oregon Riverbend 24/7 thrombectomy ELVO alert Access PH PACU Anesthesia Goyal et al. Lancet. 2016
Stroke Systems of Care Claire Corbett, MMS, NRP Manager of Neurodiagnostics and Stroke Center New Hanover Regional Medical Center. What do we know?
 Stroke Systems of Care Claire Corbett, MMS, NRP Manager of Neurodiagnostics and Stroke Center New Hanover Regional Medical Center What do we know? Stroke: Time is Brain Shorter onset to treatment times
Stroke Systems of Care Claire Corbett, MMS, NRP Manager of Neurodiagnostics and Stroke Center New Hanover Regional Medical Center What do we know? Stroke: Time is Brain Shorter onset to treatment times
11/1/2018. Disclosure. Imaging in Acute Ischemic Stroke 2018 Neuro Symposium. Is NCCT good enough? Keystone Heart Consultant, Stock Options
 Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Parameter Optimized Treatment for Acute Ischemic Stroke
 Heart & Stroke Barnett Memorial Lectureship and Visiting Professorship Parameter Optimized Treatment for Acute Ischemic Stroke December 2, 2016, Thunder Bay, Ontario Adnan I. Qureshi MD Professor of Neurology,
Heart & Stroke Barnett Memorial Lectureship and Visiting Professorship Parameter Optimized Treatment for Acute Ischemic Stroke December 2, 2016, Thunder Bay, Ontario Adnan I. Qureshi MD Professor of Neurology,
What Have We Learned: Selection for Endovascular Stroke Therapy
 What Have We Learned: Selection for Endovascular Stroke Therapy Raul G Nogueira, MD Associate Professor in Neurology, Neurosurgery, and Radiology Emory University Director, Neuroendovascular Service Director,
What Have We Learned: Selection for Endovascular Stroke Therapy Raul G Nogueira, MD Associate Professor in Neurology, Neurosurgery, and Radiology Emory University Director, Neuroendovascular Service Director,
ACUTE STROKE IMAGING
 ACUTE STROKE IMAGING Mahesh V. Jayaraman M.D. Director, Inter ventional Neuroradiology Associate Professor Depar tments of Diagnostic Imaging and Neurosurger y Alper t Medical School at Brown University
ACUTE STROKE IMAGING Mahesh V. Jayaraman M.D. Director, Inter ventional Neuroradiology Associate Professor Depar tments of Diagnostic Imaging and Neurosurger y Alper t Medical School at Brown University
ESCAPE Endovascular treatment for Small Core and Anterior circulation Proximal occlusion with Emphasis on minimizing CT to recanalization times
 ESCAPE Endovascular treatment for Small Core and Anterior circulation Proximal occlusion with Emphasis on minimizing CT to recanalization times Michael D Hill, Mayank Goyal on behalf of the ESCAPE Trial
ESCAPE Endovascular treatment for Small Core and Anterior circulation Proximal occlusion with Emphasis on minimizing CT to recanalization times Michael D Hill, Mayank Goyal on behalf of the ESCAPE Trial
Acute Stroke Management What is State of the Art?
 Acute Stroke Management What is State of the Art? Karl-Titus Hoffmann Department of Neuroradiologie University of Leipzig / University Hospital Leipzig Disclosure Speaker name: Karl-Titus Hoffmann I have
Acute Stroke Management What is State of the Art? Karl-Titus Hoffmann Department of Neuroradiologie University of Leipzig / University Hospital Leipzig Disclosure Speaker name: Karl-Titus Hoffmann I have
Endovascular Treatment for Acute Ischemic Stroke: Considerations from Recent Randomized Trials
 Published online: March 13, 2015 1664 9737/15/0034 0115$39.50/0 Review Endovascular Treatment for Acute Ischemic Stroke: Considerations from Recent Randomized Trials Manabu Shirakawa a Shinichi Yoshimura
Published online: March 13, 2015 1664 9737/15/0034 0115$39.50/0 Review Endovascular Treatment for Acute Ischemic Stroke: Considerations from Recent Randomized Trials Manabu Shirakawa a Shinichi Yoshimura
Figures for Draft Response to IMS III, MR RESCUE, and SYNTHSESIS Trials
 Figures for Draft Response to IMS III, MR RESCUE, and SYNTHSESIS Trials Figure 1: Lay Press Judgment May Belie a Deeper Examination of the Data. Truman ultimately defeated Dewey for the Presidency Subject
Figures for Draft Response to IMS III, MR RESCUE, and SYNTHSESIS Trials Figure 1: Lay Press Judgment May Belie a Deeper Examination of the Data. Truman ultimately defeated Dewey for the Presidency Subject
A DIRECT ASPIRATION FIRST PASS TECHNIQUE (ADAPT) IN PATIENTS WITH ACUTE ISCHEMIC STROKE
 IN PATIENTS WITH ACUTE ISCHEMIC STROKE") A DIRECT ASPIRATION FIRST PASS TECHNIQUE (ADAPT) IN PATIENTS WITH ACUTE ISCHEMIC STROKE Hocine REDJEM Raphaël BLANC Bertrand LAPERGUE Gabriele CICCIO Stanislas SMAJDA Mikael MAZIGHI Georges RODESCH Michel
A DIRECT ASPIRATION FIRST PASS TECHNIQUE (ADAPT) IN PATIENTS WITH ACUTE ISCHEMIC STROKE Hocine REDJEM Raphaël BLANC Bertrand LAPERGUE Gabriele CICCIO Stanislas SMAJDA Mikael MAZIGHI Georges RODESCH Michel
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS. Justin Nolte, MD Assistant Profession Marshall University School of Medicine
 ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
Update on Thrombolysis and Thrombectomy. Seniorprofessur Neurologie UniversitätsKlinikum und Universität Heidelberg
 Update on Thrombolysis and Thrombectomy Relevant Disclosures I received financial compensation from Boehringer - Ingelheim for my time and efforts as Chairman of the SC of ECASS 1-3 and from Paion for
Update on Thrombolysis and Thrombectomy Relevant Disclosures I received financial compensation from Boehringer - Ingelheim for my time and efforts as Chairman of the SC of ECASS 1-3 and from Paion for
Stroke Update. Claire J. Creutzfeldt, MD January 12, 2018
 Stroke Update Claire J. Creutzfeldt, MD January 12, 2018 Disclosures None relevant to this presentation I receive funding from the NINDS What s new in stroke? A new model for cardioembolic stroke: atrial
Stroke Update Claire J. Creutzfeldt, MD January 12, 2018 Disclosures None relevant to this presentation I receive funding from the NINDS What s new in stroke? A new model for cardioembolic stroke: atrial
Further Pragmatic Trials of Thrombectomy are Needed
 Further Pragmatic Trials of Thrombectomy are Needed Prof Keith W Muir Institute of Neuroscience & Psychology University of Glasgow Institute of Neurological Sciences Queen Elizabeth University Hospital
Further Pragmatic Trials of Thrombectomy are Needed Prof Keith W Muir Institute of Neuroscience & Psychology University of Glasgow Institute of Neurological Sciences Queen Elizabeth University Hospital
IMAGING IN ACUTE ISCHEMIC STROKE
 IMAGING IN ACUTE ISCHEMIC STROKE Timo Krings MD, PhD, FRCP (C) Professor of Radiology & Surgery Braley Chair of Neuroradiology, Chief and Program Director of Diagnostic and Interventional Neuroradiology;
IMAGING IN ACUTE ISCHEMIC STROKE Timo Krings MD, PhD, FRCP (C) Professor of Radiology & Surgery Braley Chair of Neuroradiology, Chief and Program Director of Diagnostic and Interventional Neuroradiology;
Alex Abou-Chebl, MD Associate Professor of Neurology and Neurosurgery Director of Neurointerventional Services Director of Vascular and
 Alex Abou-Chebl, MD Associate Professor of Neurology and Neurosurgery Director of Neurointerventional Services Director of Vascular and Interventional Neurology Fellowships University of Louisville School
Alex Abou-Chebl, MD Associate Professor of Neurology and Neurosurgery Director of Neurointerventional Services Director of Vascular and Interventional Neurology Fellowships University of Louisville School
Epidemiology. Epidemiology 6/1/2015. Cerebral Ischemia
 Presenter Disclosure Information Paul Nyquist MD/MPH FCCM FAHA Updates on the Acute Care of Ischemic Stroke and Intracranial Hemorrhage Updates on the Acute Care of Ischemic Stroke Paul Nyquist MD/MPH,
Presenter Disclosure Information Paul Nyquist MD/MPH FCCM FAHA Updates on the Acute Care of Ischemic Stroke and Intracranial Hemorrhage Updates on the Acute Care of Ischemic Stroke Paul Nyquist MD/MPH,
BY MARILYN M. RYMER, MD
 Lytics, Devices, and Advanced Imaging The evolving art and science of acute stroke intervention. BY MARILYN M. RYMER, MD In 1996, when the US Food and Drug Administration (FDA) approved the use of intravenous
Lytics, Devices, and Advanced Imaging The evolving art and science of acute stroke intervention. BY MARILYN M. RYMER, MD In 1996, when the US Food and Drug Administration (FDA) approved the use of intravenous
Endovascular Procedures (Angioplasty and/or Stenting) for Intracranial Arterial Disease (Atherosclerosis and Aneurysms)
 for Intracranial Arterial Disease (Atherosclerosis and Aneurysms)") Endovascular Procedures (Angioplasty and/or Stenting) for Intracranial Arterial Disease (Atherosclerosis and Aneurysms) Policy Number: 2.01.54 Last Review: 11/2018 Origination: 4/2006 Next Review: 11/2019
Endovascular Procedures (Angioplasty and/or Stenting) for Intracranial Arterial Disease (Atherosclerosis and Aneurysms) Policy Number: 2.01.54 Last Review: 11/2018 Origination: 4/2006 Next Review: 11/2019
Neuro-vascular Intervention in Stroke. Will Adams Consultant Neuroradiologist Plymouth Hospitals NHS Trust
 Neuro-vascular Intervention in Stroke Will Adams Consultant Neuroradiologist Plymouth Hospitals NHS Trust Stroke before the mid 1990s Swelling Stroke extension Haemorrhagic transformation Intravenous thrombolysis
Neuro-vascular Intervention in Stroke Will Adams Consultant Neuroradiologist Plymouth Hospitals NHS Trust Stroke before the mid 1990s Swelling Stroke extension Haemorrhagic transformation Intravenous thrombolysis
Unclogging The Pipes. Zahraa Rabeeah MD Chief Resident February 9,2018
 Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine
 Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Intravenous thrombolysis State of Art. Carlos A. Molina Stroke Unit. Hospital Vall d Hebron Barcelona
 Intravenous thrombolysis State of Art Carlos A. Molina Stroke Unit. Hospital Vall d Hebron Barcelona Independent predictors of good outcome after iv tpa Factor SE OR(95%CI) p Constant 0.467(0.69) Recanalization
Intravenous thrombolysis State of Art Carlos A. Molina Stroke Unit. Hospital Vall d Hebron Barcelona Independent predictors of good outcome after iv tpa Factor SE OR(95%CI) p Constant 0.467(0.69) Recanalization