Treadmill Exercise ECG Test. Pai-Feng Kao MD Taipei Medical University-Wan Fang Hospital Date:
|
|
|
- Opal Fitzgerald
- 6 years ago
- Views:
Transcription
1 Treadmill Exercise ECG Test Pai-Feng Kao MD Taipei Medical University-Wan Fang Hospital Date:


2 Foam Cells Atherosclerosis Timeline Fatty Streak Intermediate Lesion Atheroma Fibrous Plaque Complicated Lesion/ Rupture From First Decade Endothelial Dysfunction From Third Decade From Fourth Decade Adapted from Pepine CJ. Am J Cardiol. 1998;82(suppl 104).
3 Coronary Artery Disease a chronic disorder clinically defined phases: asymptomatic stable angina progressive angina acute coronary syndrome unstable angina, NQMI, acute MI
4 Thrombus Formation and ACS Plaque Disruption/Fissure/Erosion Thrombus Formation Old Terminology: UA NQMI STE-MI New Terminology: Non-ST-Segment Elevation Acute Coronary Syndrome (ACS) ST-Segment Elevation Acute Coronary Syndrome (ACS)

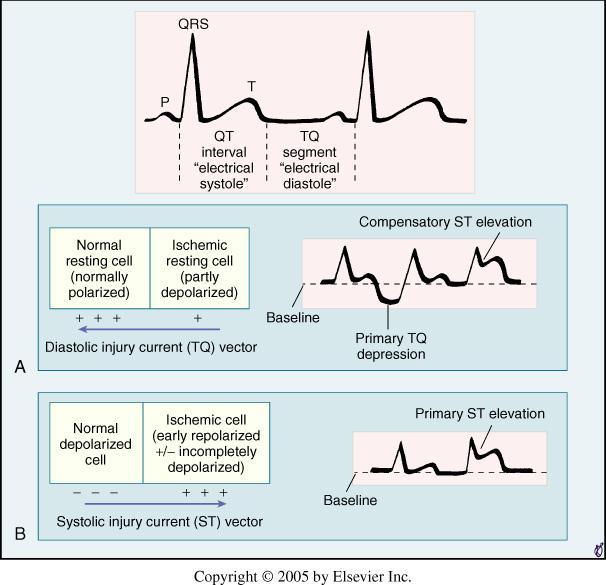
5 Schema of the ischemic cascade
6 Evaluation and Diagnosis In patients presenting with chest pain detailed symptom history focused physical examination directed risk-factor assessment Estimate the probability of significant CAD (i.e., low, intermediate, high)
7 Pretest Likelihood of CAD in Symptomatic Patients According to Age and Sex (Combined Diamond/Forrester and CASS Data) Nonanginal Age Chest Pain Atypical Angina Typical Angina Years Men Women Men Women Men Women *Each value represents the percent with significant CAD on catheterization
8 Probability Estimate the Duke and Stanford models The likelihood of disease for women <55 years old with atypical angina and no risk factors is < 10 %; but if diabetes, smoking and hyperlipidemia are present, the likelihood jumps to 40 %. Am J Med 1983;75: ; Am J Med 1990;89:7-14 Ann Intern Med 1993;118:81-90
9 12 Lead Resting ECG should be recorded in all patients with symptoms suggestive of angina pectoris normal in 50% of patients a normal ECG does not exclude severe CAD; however, it does imply normal LV function with favorable prognosis
10 Clinical Assessment Recommendations for Stress test Electrocardiography Echocardiography or Radionuclide Angiography
11 Treadmill exercise ECG test

12 Stress Thallium 201 scan

13 Stress echocardiography
14 Multislice CT

15 Coronary angiography
16 Stress Tests - cost issues exercise ECG is least costly stress echocardiography stress SPECT myocardial imaging coronary angiography 1X 2X 5X 20X
17 Comparison of Stress Tests meta-analysis on 44 articles (published between 1990 and 199 Sensitivity Specificity ECG 52% 71% Echocardiography 85% 77% Scintigraphy 87% 64% not adjusted for referral bias, exercise echocardiography had significantly better discriminatory power than exercise myocardial perfusion imaging JAMA 1998;280:913-20
18 Exercise Stress Tests stepwise strategy Exercise ECG simplicity, lower cost and familiarity the initial test in patients who are not taking digoxin, have a normal rest ECG, and are able to exercise Stress-imaging techniques for patients with widespread rest ST depression (>1 mm), complete left bundle-branch block, ventricular paced rhythm or preexcitation

19 Ischemic Heart Disease and Resting Electrocardiography

20
21
22
23

24 Chest Pain and Ischemic Heart Disease
25 Exercise
26 Exercise Physiology Acceleration of ventricular rate Vagal withdrawal Increase alveolar ventilation Sympathetic vasoconstriction- Increased venous return Increase cardiac output
27 Treadmill Exercise Test
28 Introduction The evaluation of chest pain can be very difficult. It is possible to have a normal resting ECG with considerable narrowing of the coronary arteries. Exercise testing was developed in the 1950s with the Bruce protocol published in It is now a well established technique.
29 Exercise ECG testing can be used in the following circumstances: Assessing a clinical diagnosis of angina Risk stratification after myocardial infarction Risk stratification in patients with hypertrophic cardiomyopathy Evaluation of revascularisation procedures or drug treatment Evaluation of exercise tolerance and cardiac function Assessment of cardiopulmonary function in patients with dilated cardiomyopathy or heart failure Assessment of treatment for arrhythmia Assessment of asymptomatic people in high risk occupations like airline pilots.

30 Cardiopulmonary exercise test in a healthy 53-year-old man using the Bruce protocol.
31 Metabolic equivalent MET: Resting V o for 70-Kg 40 y/o male 2 1 MET= 3.5ml/min/kg of body weight

32 Estimated oxygen cost of bicycle ergometer and selected treadmill protocols
33 The Bruce protocol is very widely used and has been extensively validated. There are 7 stages of 3 minutes each so that a complete test takes 21 minutes.
34 A modified Bruce protocol is used for exercise testing within one week of myocardial infarction and for those who are old and frail or expected to have poor exercise tolerance for other reasons. It starts at a lower work level and so takes longer to achieve the required heart rate. This would make the patient more susceptible to fatigue before achieving the required rate but it seems that judicious use of either the Bruce or modified Bruce protocols gives satisfactory results.
35 Absolute Contraindications to Exercise Testing Acute myocardial infarction (within 2 d) High-risk unstable angina* Uncontrolled cardiac arrhythmias causing symptoms or hemodynamic compromise Symptomatic severe aortic stenosis Uncontrolled symptomatic heart failure Acute pulmonary embolus or pulmonary infarction Acute myocarditis or pericarditis Acute aortic dissection AHA/ACC Guideline 2002
36 Relative Contraindications for Treadmill Testing Left main coronary stenosis Moderate stenotic valvular heart disease Electrolyte abnormalities Severe arterial hypertension Tachyarrhythmias or bradyarrhythmias Hypertrophic cardiomyopathy and other forms of outflow tract obstruction Mental or physical impairment leading to inability to exercise adequately High-degree atrioventricular block AHA/ACC Guideline 2002
37 Complications of Treadmill Testing Brady / Tachyarrythmias AMI / Sudden Death CHF / Shock MSK Trauma / Fatigue / Malaise
38 Safety and Risks of Exercise testing Nonselective patient population Mortality <0.01% Morbidity <0.05% Survey of tests for within 4 weeks of AMI Mortality <0.03% 0.09% had nonfatal reinfarction or resuscitated from cardiac arrest Major complication 2X in symptom-limited protocol than low-level protocol
39 Treadmill Testing: Procedures Physiology Exercise creates increase CO Four to six fold increase from rest at peak CO increase by increase HR and PB and decreased vagal tone HR affected by Age, sex, motivation, habitus, blood volume, health SBP increases with exercise DBP stays same or slightly decreases Hypotension ominous sign Outflow obstruction, ventricular dysfunction or ischemia
40 Treadmill Testing: Procedures Equipment Treadmill or cycle ergometer Cycle has major pitfall of rapid fatigue of quadriceps in older patients Most studies use treadmill Handrails, Rest Area Assistant, Supervisor Resuscitation Equipment
41 Treadmill Testing: Procedures Preparation Fast 3 hours prior / dress appropriately footwear Medications reviewed by physician prior History and physical prior regarding change in disease CHF; valvular disease; onset of unstable angina; bronchospasm Consent Baseline supine and upright ECG
42 Treadmill Testing: Procedures Protocols Most diagnostic and prognostic studies based on Bruce protocol Seven phases Change in grade and speed every 3 minutes Correlation with METS Large incremental stages Not correlated for height / weight / stride Ideal protocol lasts 6-12 minutes and adjusts for patients ability Others include Naughton, McHenry, USAF, Blake
43 The aim of the exercise is for the patient to achieve the target heart rate of 85% of maximum.
44 Ideally, for an adequate test the patient should achieve 85% of maximum heart rate. Maximum heart rate is calculated as 220- age in years for men and 210- age for women.
45 Blood pressure is measured before starting and at the end of each stage of exercise. Blood pressure may fall or be stable during the early stages. Systolic blood pressure should increase as the exercise level rises. Up to 225 mm Hg is normal, although athletes can have higher levels. Diastolic pressure usually falls slightly.
46 Simple Estimation of Ex Intensity Low Intensity: 3-5 METs Moderate Intensity: 4-7 METs High Intensity: 8-12 METs

47 HR Responses During Exercise
48 Treadmill Testing: Procedures Borg Scale Correlation of scale to actual fatigue 6-20 grade scale for exertion 10 grade scale for exertion now adopted 0 nothing 9 very strong 10 very, very strong Continues to be a clinical assessment of fatigue by technician (skilled) and supervisor Mainly used as repetitive assessment tool in rehab Borg. Sports and Exercise
49 Treadmill Testing: Procedures Measurements ST depression / elevation (60-80 ms; J point changes) ST slope (downsloping worse than horizontal) Duration of changes into recovery Exercise induced arrhythmias Peak HR / BP Total Duration Exertional hypotension Angina Other exercise induced symptoms
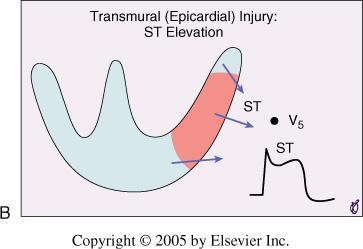
50 Absolute Indications for Terminating Exercise Testing Drop in systolic blood pressure of >10 mm Hg Moderate to severe angina Increasing nervous system symptoms (eg, ataxia, dizziness, or near-syncope) Signs of poor perfusion (cyanosis or pallor) Technical difficulties in monitoring ECG or systolic blood pressure Subject s desire to stop Sustained ventricular tachycardia ST elevation ( 1.0 mm) in leads without diagnostic Q-waves (other than V1 or avr)
51 Relative Indications for Terminating Exercise Testing Drop in systolic blood pressure of ( 10 mm Hg from baseline blood pressure despite an increase in workload, in the absence of other evidence of ischemia ST or QRS changes such as excessive ST depression (>2 mm of horizontal or downsloping ST-segment depression) or marked axis shift Arrhythmias other than sustained ventricular tachycardia, including multifocal PVCs, triplets of PVCs, supraventricular tachycardia, heart block, or bradyarrhythmias Fatigue, shortness of breath, wheezing, leg cramps, or claudication Development of bundle-branch block or IVCD that cannot be distinguished from ventricular tachycardia Increasing chest pain Hypertensive response*

52 Interpretation of Exercise ECG
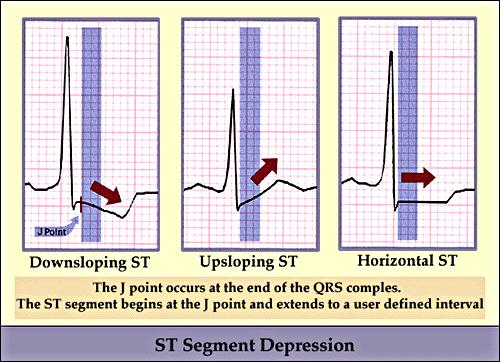
53 Measurement of STsegment displacement Isoelectric point: PQ junction-j point Abnormal response: ST-segment depressed 0.10mV 60 to 80 msec after the J point in 3 consecutive beats with a stable baseline

54 Magnified ischemic exercise induced electrocardiographic pattern. Three consecutive complexes with a relatively stable baseline are selected. The PQ junction (1) and J point (2) are determined; the ST 80 (3) is determined at 80 msec after the J point.
55
56
57
58 Criteria for a positive exercise test: Conventional criteria Horizontal or downsloping ST segment depression 1mm Upsloping ST segment depression 1.5mm with a duration 0.08 sec

59 J point depression of 2 to 3 mm in leads V 4 to V 6 with rapid upsloping ST segments depressed approximately 1mm 80msec after the J point.
 result is abnormal early in the test,")
60 Bruce protocol. lead V 4, the exercise electrocardiographic ( ECG ) result is abnormal early in the test, reaching 0.3mV (3mm) of horizontal ST segment depression at the end of exercise.

61 Bruce protocol. In this type of ischemic pattern, the J point at peak exertion is depressed 2.5mm, the ST segment slope is 1.5mV/sec, and the ST segment level at 80msec after the J point is depressed 1.6mm.
 result is not yet abnormal")
62 Bruce protocol. The exercise electrocardiographic ( ECG ) result is not yet abnormal at 8:50 minutes but becomes abnormal at 9:30 minutes
 patterns at rest and at")
63 Illustration of eight typical exercise electrocardiographic ( ECG ) patterns at rest and at peak exertion.
 result developed marked ST segment elevation associated")
64 A 48-year-old man with several atherosclerotic risk factors and a normal resting electrocardiographic ( ECG ) result developed marked ST segment elevation associated with angina.

65 Pseudonormalization of T waves in a 49-year-old man referred for exercise testing. The patient had previously been seen for typical angina. The resting electrocardiogram in this patient with coronary artery disease shows inferior and anterolateral T wave inversion, an adverse long-term prognosticator.
 block on the resting")
66 A 67-year-old man with ischemic cardiomyopathy referred for exercise testing had a left bundle branch block and first-degree atrioventricular (AV) block on the resting ECG.

67 A 75-year-old woman with chronic atrial fibrillation and a 6-month history of atypical chest pain underwent mitral valve repair 1 year before testing, at which time nonobstructive coronary disease was noted.

68 A 58-year-old hypertensive diabetic man with prior history of cigarette smoking was referred for evaluation of dyspnea and early fatigability during exercise. The abnormal 2.5 to 3 mm downsloping ST segment depression in lead II during the LBBB is nondiagnostic for coronary artery disease because of the conduction disturbance.
 are common in patients with RBBB and are secondary to the conduction")
69 Exercise -induced ST segment depression is noted in leads V 2 to V 3 (arrows) in this patient with a resting right bundle branch block (RBBB) pattern. Exercise - induced horizontal or downsloping ST segment responses in the early anterior precordial leads (V 1 through V 4 ) are common in patients with RBBB and are secondary to the conduction disturbance. The presence of this finding in leads V 1 through V 4 is not diagnostic of obstructive coronary disease.

70 61-year-old man with atypical angina and a hiatal hernia was referred for diagnostic exercise testing. The test was stopped because of dyspnea. The standing resting ECG shows an intermittent Wolff-Parkinson-White pattern (arrows).
71 Treadmill Testing: Results Prognostic Duke Score Time in minutes ST depression in mm Type of pain 0 - none 1 typical anginal pain limited by time / fatigue / other 2 limiting anginal pain
72 Treadmill Testing: Results Duke Score = Time(m) 4X Angina 5X depression(mm) Score: 5 & above low risk 4 to 9 intermediate risk -10 & below high risk
73 Survival According to Risk Groups Based on Duke Treadmill Score 4 -Year Annual Risk Group (Score) Total Survival Mortality Low ( +5) 62% 99% 0.25% Moderate (-10 to +4) 34% 95% 1.25% High (< -10) 4% 79% 5.00% N Engl J Med 1991;325:849-53
74 Use of Exercise Test Results in Patient Management predicted average recommended risk score annual mortality treatment low <1% per year medical therapy intermediate 1% to 3% cardiac catheterization exercise imaging study high-risk score >3% per year cardiac catheterization * <5% pt with low-risk treadmill score will be identified as high risk after imaging * those with known LV dysfunction should have cardiac catheterization
75 Treadmill Testing: Results Exercise Capacity Reasonable to Use exercise testing for Surgical patients recovering from Congenital repair Valvular replacement Cardiac transplant CHF DM CRF Chronic Lung Disease No exercise induced symptoms AHA Guidelines Carliner et al. Am J Card. 1985
76 Treadmill Testing: Results Exercise Capacity and Prognostication 1575 men; mean age 43 Failure to achieve 85 % of age predicted maximum heart rate associated with increase in death of 1.84 Extrapolation techniques used Lauer and Fletcher. Circulation
77 Treadmill Testing: Results Evaluation of Medical Therapy Look for improvement of exercise capacity to previous before angina or ST depression Evaluation of Valvular Disease Strict guideline for evaluation of AS Evaluation of Dysrrythmias PVC, Sick sinus Syndrome Pre-operative Anesthetists 2 nd largest user of stress test for evaluation of patient for non cardiac surgery AHA Guidelines
78 Notable Studies Exercise Hypotension Looking at SBP drop with exercise Looked at 0, 10, 20 drop of SBP Drop of 20 associated with increased PPV of at least 50% Left Main or Triple Vessel Disease Dubach et al. Circulation. 1989
79 Notable Studies Variables 3974 men Kaplan-Meier regression Four variables predict mortality within 5 year Rate of change of rate-pressure product Age > 65 Maximum MET <5 LVH on ECG Prakash et al. Am Heart J. 2001
80 Notable Studies METS Found that sensitivity increases if MET >7 Also found that METS achieved may be a stronger variable than rate-pressure product High heart rate at low MET (<5) level carries adverse prognosis Ramamurthy et al. Chest
81 Notable Studies Risk Factors Multiple Risk Factor Intervention Trial 12,866 participants Those with ST changes on Stress Treadmill benefit to greater degree with risk factor modification than controls. Am J Cardiol. MRFIT
82 Notable Studies Women Large number of false positives Mitral valve prolapse; Higher incidence atypical chest pain Hormonal, esp. estrogen mimickery of digoxin Ventilation Responses and Metabolic Alkalosis Curzen. Heart women Compared with coronary angiography 42 false positives & 31 false negatives (36 % of total) Increase false positives correlated with Increasing age to 52 Increasing coronary risks to 3
83 Notable Studies Early Stress Testing 276 low risk patients Stress test within 48 hours Similar prognostication numbers 0.5 % event rate Additional variables over 6 months 15% less ED visits 30% fewer admission Polanczyk. Am J Card
84 Noncoronary Causes of ST Segment Depression Severe aortic stenosis Severe hypertension Cardiomyopathy Anemia Hypokalemia Severe hypoxia Digitalis Sudden excessive exercise Glucose load Left ventricular hypertrophy Hyperventilation Mitral valve prolapse Intraventricular conduction disturbance Preexcitation syndrome Severe volume overload (aortic, mitral regurgitation Supraventricular tachyarrhythmias
85
86
87 This is a non-invasive screening test rather than a "gold standard". The following findings suggest high probability of coronary artery disease Horizontal ST segment depression of <2 mm Down-sloping ST segment depression Early positive findings within 6 minutes Persistence of ST depression for more than 6 minutes after stopping ST segment depression in 5 or more leads Hypotension with exercise
88 Exercise Parameters Associated with an Adverse Prognosis and Multi-vessel Coronary Artery Disease Duration of symptom-limiting exercise (< 5 METs) Failure to increase systolic blood pressure 120 mm Hg, or a sustained decrease 10 mm Hg, or below rest levels, during progressive exercise ST segment depression 2 mm, downsloping ST segment, starting at < 5 METs, involving 5 leads, persisting 5 minutes into recovery Exercise-induced ST segment elevation (avr excluded) Angina pectoris at low exercise loads Reproducible sustained (> 30 sec) or symptomatic ventricular tachycardia Acute systemic illness (pulmonary embolism, aortic dissection)
89 References Heart disease 7th edition ACC/AHA 2002 Guideline Update for Exercise Testing Exercise Treadmill Testing Dr. Peter Krampl 2001 Exercise ECG Testing: EMIS Last Updated: 22 Nov 2006 Review Date: 21 Nov 2008

90 Thanks For Your Attention
Exercise Test: Practice and Interpretation. Jidong Sung Division of Cardiology Samsung Medical Center Sungkyunkwan University School of Medicine
 Exercise Test: Practice and Interpretation Jidong Sung Division of Cardiology Samsung Medical Center Sungkyunkwan University School of Medicine 2 Aerobic capacity and survival Circulation 117:614, 2008
Exercise Test: Practice and Interpretation Jidong Sung Division of Cardiology Samsung Medical Center Sungkyunkwan University School of Medicine 2 Aerobic capacity and survival Circulation 117:614, 2008
My Patient Needs a Stress Test
 My Patient Needs a Stress Test Amy S. Burhanna,, MD, FACC Coastal Cardiology Cape May Court House, New Jersey Absolute and relative contraindications to exercise testing Absolute Acute myocardial infarction
My Patient Needs a Stress Test Amy S. Burhanna,, MD, FACC Coastal Cardiology Cape May Court House, New Jersey Absolute and relative contraindications to exercise testing Absolute Acute myocardial infarction
Contra-indications, Risks, and Safety Precautions for Stress Testing. ACSM guidelines, pg 20 7 ACSM RISK FACTORS. Risk Classifications pg 27
 Contra-indications, Risks, and Safety Precautions for Stress Testing Data to Support Stress Testing How safe is stress testing? Contra-indications Termination Criteria Ellstad Chapt 5 ACSM Chapts 3-6 Seattle
Contra-indications, Risks, and Safety Precautions for Stress Testing Data to Support Stress Testing How safe is stress testing? Contra-indications Termination Criteria Ellstad Chapt 5 ACSM Chapts 3-6 Seattle
Chapter 21: Clinical Exercise Testing Procedures
 Publisher link: thepoint http://thepoint.lww.com/book/show/2930 Chapter 21: Clinical Exercise Testing Procedures American College of Sports Medicine. (2010). ACSM's resource manual for guidelines for exercise
Publisher link: thepoint http://thepoint.lww.com/book/show/2930 Chapter 21: Clinical Exercise Testing Procedures American College of Sports Medicine. (2010). ACSM's resource manual for guidelines for exercise
Graded exercise testing (GXT): extension of medical history and physical examination
: extension of medical history and physical examination") Related Readings Fletcher, G. F., Balady, G. J., Amsterdam, E. A., Chaitman, B., Eckel, R., Fleg, J., et al. (2001). Exercise standards for testing and training: A statement for healthcare professionals
Related Readings Fletcher, G. F., Balady, G. J., Amsterdam, E. A., Chaitman, B., Eckel, R., Fleg, J., et al. (2001). Exercise standards for testing and training: A statement for healthcare professionals
Risk Stratification for CAD for the Primary Care Provider
 Risk Stratification for CAD for the Primary Care Provider Shimoli Shah MD Assistant Professor of Medicine Directory, Ambulatory Cardiology Clinic Knight Cardiovascular Institute Oregon Health & Sciences
Risk Stratification for CAD for the Primary Care Provider Shimoli Shah MD Assistant Professor of Medicine Directory, Ambulatory Cardiology Clinic Knight Cardiovascular Institute Oregon Health & Sciences
Stress ECG is still Viable in Suleiman M Kharabsheh, MD, FACC Consultant Invasive Cardiologist KFHI KFSHRC-Riyadh
 Stress ECG is still Viable in 2016 Suleiman M Kharabsheh, MD, FACC Consultant Invasive Cardiologist KFHI KFSHRC-Riyadh Stress ECG Do we still need stress ECG with all the advances we have in the CV field?
Stress ECG is still Viable in 2016 Suleiman M Kharabsheh, MD, FACC Consultant Invasive Cardiologist KFHI KFSHRC-Riyadh Stress ECG Do we still need stress ECG with all the advances we have in the CV field?
Using and Interpreting Exercise Stress Testing in Clinical Practice
 Using and Interpreting Exercise Stress Testing in Clinical Practice Exercise stress testing may be useful to elicit the presence of cardiovascular disease and in later evaluation of such disease. Anthony
Using and Interpreting Exercise Stress Testing in Clinical Practice Exercise stress testing may be useful to elicit the presence of cardiovascular disease and in later evaluation of such disease. Anthony
CHRONIC CAD DIAGNOSIS
 CHRONIC CAD DIAGNOSIS Chest Pain Evaluation 1. Approach to diagnosis of CAD 2. Classification of chest pain 3. Pre-test likelihood CAD 4. Algorithm for chest pain evaluation in women 5. Indications for
CHRONIC CAD DIAGNOSIS Chest Pain Evaluation 1. Approach to diagnosis of CAD 2. Classification of chest pain 3. Pre-test likelihood CAD 4. Algorithm for chest pain evaluation in women 5. Indications for
Chad Morsch B.S., ACSM CEP
 What Is Cardiac Stress Testing? Chad Morsch B.S., ACSM CEP A Cardiac Stress Test is a test used to measure the heart's ability to respond to external stress in a controlled clinical environment. Cardiac
What Is Cardiac Stress Testing? Chad Morsch B.S., ACSM CEP A Cardiac Stress Test is a test used to measure the heart's ability to respond to external stress in a controlled clinical environment. Cardiac
Choosing the Appropriate Stress Test: Brett C. Stoll, MD, FACC February 24, 2018
 Choosing the Appropriate Stress Test: Brett C. Stoll, MD, FACC February 24, 2018 Choosing the Appropriate Stress Test: Does it Really Matter? Brett C. Stoll, MD, FACC February 24, 2018 Conflicts of Interest
Choosing the Appropriate Stress Test: Brett C. Stoll, MD, FACC February 24, 2018 Choosing the Appropriate Stress Test: Does it Really Matter? Brett C. Stoll, MD, FACC February 24, 2018 Conflicts of Interest
The importance of follow-up after a cardiac event: CARDIAC REHABILITATION. Dr. Guy Letcher
 The importance of follow-up after a cardiac event: CARDIAC REHABILITATION Dr. Guy Letcher The National Medicare Experience Mortality After Angioplasty 225,915 patients Mortality After Bypass Surgery 357,885
The importance of follow-up after a cardiac event: CARDIAC REHABILITATION Dr. Guy Letcher The National Medicare Experience Mortality After Angioplasty 225,915 patients Mortality After Bypass Surgery 357,885
Disclosure. 3. ST depression indicative of ischemia is most commonly observed in leads: 1. V1-V2. 2. I and avl 3. V
 Interpreting Stress Induced Ischemia by ECG, Bundle Branch Block & Arrhythmias Disclosure Gregory S Thomas MD, MPH Medical Director, MemorialCare Heart & Vascular Institute, Long Beach Memorial Astellas
Interpreting Stress Induced Ischemia by ECG, Bundle Branch Block & Arrhythmias Disclosure Gregory S Thomas MD, MPH Medical Director, MemorialCare Heart & Vascular Institute, Long Beach Memorial Astellas
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases
 Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Study methodology for screening candidates to athletes risk
 1. Periodical Evaluations: each 2 years. Study methodology for screening candidates to athletes risk 2. Personal history: Personal history of murmur in childhood; dizziness, syncope, palpitations, intolerance
1. Periodical Evaluations: each 2 years. Study methodology for screening candidates to athletes risk 2. Personal history: Personal history of murmur in childhood; dizziness, syncope, palpitations, intolerance
The Fundamentals of 12 Lead EKG. ECG Recording. J Point. Reviewing the Cardiac Conductive System. Dr. E. Joe Sasin, MD Rusty Powers, NRP
 The Fundamentals of 12 Lead EKG Dr. E. Joe Sasin, MD Rusty Powers, NRP SA Node Intranodal Pathways AV Junction AV Fibers Bundle of His Septum Bundle Branches Purkinje System Reviewing the Cardiac Conductive
The Fundamentals of 12 Lead EKG Dr. E. Joe Sasin, MD Rusty Powers, NRP SA Node Intranodal Pathways AV Junction AV Fibers Bundle of His Septum Bundle Branches Purkinje System Reviewing the Cardiac Conductive
Case Question. Evaluation of Chest pain in the Office and Cardiac Stress Testing
 Evaluation of Chest pain in the Office and Cardiac Stress Testing Chad Link, DO FACC Sparrow Hospital Thoracic and Cardiovascular Institute Chairman- TCI Cardiology Section Disclosures Speakers Bureau
Evaluation of Chest pain in the Office and Cardiac Stress Testing Chad Link, DO FACC Sparrow Hospital Thoracic and Cardiovascular Institute Chairman- TCI Cardiology Section Disclosures Speakers Bureau
REtrive. REpeat. RElearn Design by. Test-Enhanced Learning based ECG practice E-book
 Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Myocardial Infarction. Reading Assignment (p66-78 in Outline )
") Myocardial Infarction Reading Assignment (p66-78 in Outline ) Objectives 1. Why do ST segments go up or down in ischemia? 2. STEMI locations and culprit vessels 3. Why 15-lead ECGs? 4. What s up with avr?
Myocardial Infarction Reading Assignment (p66-78 in Outline ) Objectives 1. Why do ST segments go up or down in ischemia? 2. STEMI locations and culprit vessels 3. Why 15-lead ECGs? 4. What s up with avr?
I have no financial disclosures
 Manpreet Singh MD I have no financial disclosures Exercise Treadmill Bicycle Functional capacity assessment Well validated prognostic value Ischemic assessment ECG changes ST segments Arrhythmias Hemodynamic
Manpreet Singh MD I have no financial disclosures Exercise Treadmill Bicycle Functional capacity assessment Well validated prognostic value Ischemic assessment ECG changes ST segments Arrhythmias Hemodynamic
Listing Form: Heart or Cardiovascular Impairments. Medical Provider:
 Listing Form: Heart or Cardiovascular Impairments Medical Provider: Printed Name Signature Patient Name: Patient DOB: Patient SS#: Date: Dear Provider: Please indicate whether your patient s condition
Listing Form: Heart or Cardiovascular Impairments Medical Provider: Printed Name Signature Patient Name: Patient DOB: Patient SS#: Date: Dear Provider: Please indicate whether your patient s condition
ECG Cases and Questions. Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology
 ECG Cases and Questions Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology 32 yo female Life Insurance Physical 56 yo male with chest pain Terminology Injury ST elevation Ischemia T wave inversion
ECG Cases and Questions Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology 32 yo female Life Insurance Physical 56 yo male with chest pain Terminology Injury ST elevation Ischemia T wave inversion
Cardiovascular Disorders. Heart Disorders. Diagnostic Tests for CV Function. Bio 375. Pathophysiology
 Cardiovascular Disorders Bio 375 Pathophysiology Heart Disorders Heart disease is ranked as a major cause of death in the U.S. Common heart diseases include: Congenital heart defects Hypertensive heart
Cardiovascular Disorders Bio 375 Pathophysiology Heart Disorders Heart disease is ranked as a major cause of death in the U.S. Common heart diseases include: Congenital heart defects Hypertensive heart
Electrical System Overview Electrocardiograms Action Potentials 12-Lead Positioning Values To Memorize Calculating Rates
 Electrocardiograms Electrical System Overview James Lamberg 2/ 74 Action Potentials 12-Lead Positioning 3/ 74 4/ 74 Values To Memorize Inherent Rates SA: 60 to 100 AV: 40 to 60 Ventricles: 20 to 40 Normal
Electrocardiograms Electrical System Overview James Lamberg 2/ 74 Action Potentials 12-Lead Positioning 3/ 74 4/ 74 Values To Memorize Inherent Rates SA: 60 to 100 AV: 40 to 60 Ventricles: 20 to 40 Normal
A Review of Cardiac Pathophysiology and EKG. Jamie Dyson PT, DPT Kathy Swanick PT, DPT, OCS
 A Review of Cardiac Pathophysiology and EKG Jamie Dyson PT, DPT Kathy Swanick PT, DPT, OCS Cardiac Pathophysiology Coronary Artery Disease Congestive Heart Failure Valvular Heart Disease Athletic Heart
A Review of Cardiac Pathophysiology and EKG Jamie Dyson PT, DPT Kathy Swanick PT, DPT, OCS Cardiac Pathophysiology Coronary Artery Disease Congestive Heart Failure Valvular Heart Disease Athletic Heart
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014
 Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
HEART CONDITIONS IN SPORT
 HEART CONDITIONS IN SPORT Dr. Anita Green CHD Risk Factors Smoking Hyperlipidaemia Hypertension Obesity Physical Inactivity Diabetes Risks are cumulative (multiplicative) Lifestyles predispose to RF One
HEART CONDITIONS IN SPORT Dr. Anita Green CHD Risk Factors Smoking Hyperlipidaemia Hypertension Obesity Physical Inactivity Diabetes Risks are cumulative (multiplicative) Lifestyles predispose to RF One
Common Codes for ICD-10
 Common Codes for ICD-10 Specialty: Cardiology *Always utilize more specific codes first. ABNORMALITIES OF HEART RHYTHM ICD-9-CM Codes: 427.81, 427.89, 785.0, 785.1, 785.3 R00.0 Tachycardia, unspecified
Common Codes for ICD-10 Specialty: Cardiology *Always utilize more specific codes first. ABNORMALITIES OF HEART RHYTHM ICD-9-CM Codes: 427.81, 427.89, 785.0, 785.1, 785.3 R00.0 Tachycardia, unspecified
When Should I Order a Stress Test or an Echocardiogram
 When Should I Order a Stress Test or an Echocardiogram Updates in Cardiology 2015 March 7, 2015 Donald L. Lappé, MD, FAHA, FACC Chairman, Cardiovascular Department Medical Director, Intermountain Cardiovascular
When Should I Order a Stress Test or an Echocardiogram Updates in Cardiology 2015 March 7, 2015 Donald L. Lappé, MD, FAHA, FACC Chairman, Cardiovascular Department Medical Director, Intermountain Cardiovascular
Chest Pain in Women ;What is Your Diagnostic Plan? No Need for Noninvasive Test
 Chest Pain in Women ;What is Your Diagnostic Plan? No Need for Noninvasive Test Jang-Ho Bae, MD., PhD., FACC. Konyang University Hospital Daejeon, Korea Chest pain in Women ACS Atypical Stable angina F/29
Chest Pain in Women ;What is Your Diagnostic Plan? No Need for Noninvasive Test Jang-Ho Bae, MD., PhD., FACC. Konyang University Hospital Daejeon, Korea Chest pain in Women ACS Atypical Stable angina F/29
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition
 Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series
 ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
P F = R. Disorder of the Breast. Approach to the Patient with Chest Pain. Typical Characteristics of Angina Pectoris. Myocardial Ischemia
 Disorder of the Breast Approach to the Patient with Chest Pain Anthony J. Minisi, MD Department of Internal Medicine, Division of Cardiology Virginia Commonwealth University School of Medicine William
Disorder of the Breast Approach to the Patient with Chest Pain Anthony J. Minisi, MD Department of Internal Medicine, Division of Cardiology Virginia Commonwealth University School of Medicine William
12 Lead ECG Interpretation
 12 Lead ECG Interpretation Julie Zimmerman, MSN, RN, CNS, CCRN Significant increase in mortality for every 15 minutes of delay! N Engl J Med 2007;357:1631-1638 Who should get a 12-lead ECG? Also include
12 Lead ECG Interpretation Julie Zimmerman, MSN, RN, CNS, CCRN Significant increase in mortality for every 15 minutes of delay! N Engl J Med 2007;357:1631-1638 Who should get a 12-lead ECG? Also include
Arrhythmic Complications of MI. Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine
 Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Paediatric ECG Interpretation
 Paediatric ECG Interpretation Dr Sanj Fernando (thanks to http://lifeinthefastlane.com/ecg-library/paediatric-ecginterpretation/) 3 yo boy complaining of abdominal pain and chest pain Child ECG vs Adult
Paediatric ECG Interpretation Dr Sanj Fernando (thanks to http://lifeinthefastlane.com/ecg-library/paediatric-ecginterpretation/) 3 yo boy complaining of abdominal pain and chest pain Child ECG vs Adult
ECG Workshop. Nezar Amir
 ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
Index of subjects. effect on ventricular tachycardia 30 treatment with 101, 116 boosterpump 80 Brockenbrough phenomenon 55, 125
 145 Index of subjects A accessory pathways 3 amiodarone 4, 5, 6, 23, 30, 97, 102 angina pectoris 4, 24, 1l0, 137, 139, 140 angulation, of cavity 73, 74 aorta aortic flow velocity 2 aortic insufficiency
145 Index of subjects A accessory pathways 3 amiodarone 4, 5, 6, 23, 30, 97, 102 angina pectoris 4, 24, 1l0, 137, 139, 140 angulation, of cavity 73, 74 aorta aortic flow velocity 2 aortic insufficiency
Severe Hypertension. Pre-referral considerations: 1. BP of arm and Leg 2. Ambulatory BP 3. Renal causes
 Severe Hypertension *Prior to making a referral, call office or Doc Halo, to speak with a Cardiologist or APP to discuss patient and possible treatment options. Please only contact the patient's cardiologist.
Severe Hypertension *Prior to making a referral, call office or Doc Halo, to speak with a Cardiologist or APP to discuss patient and possible treatment options. Please only contact the patient's cardiologist.
7. Echocardiography Appropriate Use Criteria (by Indication)
") Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
DEPARTMENT NAME PRE-PARTICIPATION SCREENING THE SPORTS PHYSICAL
 PRE-PARTICIPATION SCREENING THE SPORTS PHYSICAL Michele Krenek, MSN, RN, FNP-C TCHAPP Conference, Houston, TX April 4, 2019 PRE-PARTICIPATION SPORTS SCREENING According to the AHA the definition of the
PRE-PARTICIPATION SCREENING THE SPORTS PHYSICAL Michele Krenek, MSN, RN, FNP-C TCHAPP Conference, Houston, TX April 4, 2019 PRE-PARTICIPATION SPORTS SCREENING According to the AHA the definition of the
ECG Interpretation Cat Williams, DVM DACVIM (Cardiology)
") ECG Interpretation Cat Williams, DVM DACVIM (Cardiology) Providing the best quality care and service for the patient, the client, and the referring veterinarian. GOAL: Reduce Anxiety about ECGs Back to
ECG Interpretation Cat Williams, DVM DACVIM (Cardiology) Providing the best quality care and service for the patient, the client, and the referring veterinarian. GOAL: Reduce Anxiety about ECGs Back to
December 2018 Tracings
 Tracings Tracing 1 Tracing 4 Tracing 1 Answer Tracing 4 Answer Tracing 2 Tracing 5 Tracing 2 Answer Tracing 5 Answer Tracing 3 Tracing 6 Tracing 3 Answer Tracing 6 Answer Questions? Contact Dr. Nelson
Tracings Tracing 1 Tracing 4 Tracing 1 Answer Tracing 4 Answer Tracing 2 Tracing 5 Tracing 2 Answer Tracing 5 Answer Tracing 3 Tracing 6 Tracing 3 Answer Tracing 6 Answer Questions? Contact Dr. Nelson
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
Choosing the Right Cardiac Test. Outline
 Choosing the Right Cardiac Test Atif Qasim, M.D., M.S.C.E. University of California, San Francisco Disclosures: None 2013 Outline Focus on choosing the optimal tests for coronary disease evaluation Overview
Choosing the Right Cardiac Test Atif Qasim, M.D., M.S.C.E. University of California, San Francisco Disclosures: None 2013 Outline Focus on choosing the optimal tests for coronary disease evaluation Overview
Masqueraders of STEMI
 Masqueraders of STEMI Steven M. Costa, M.D. Assistant Professor Department of Medicine Division of Cardiology Scott & White Memorial Hospital and Clinic Texas A&M University Health Science Center Disclosures
Masqueraders of STEMI Steven M. Costa, M.D. Assistant Professor Department of Medicine Division of Cardiology Scott & White Memorial Hospital and Clinic Texas A&M University Health Science Center Disclosures
Please check your answers with correct statements in answer pages after the ECG cases.
 ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
TOPICS IN EMERGENCY MEDICINE SEMI-FINAL
 RISK ASSESSMENT IN PATIENTS WITH CHEST PAIN Nora Goldschlager, M.D. FACP, FACC, FAHA, FHRS Cardiology - San Francisco General Hospital UCSF Disclosures: None 1 CHEST PAIN NOT DUE TO MYOCARDIAL ISCHEMIA
RISK ASSESSMENT IN PATIENTS WITH CHEST PAIN Nora Goldschlager, M.D. FACP, FACC, FAHA, FHRS Cardiology - San Francisco General Hospital UCSF Disclosures: None 1 CHEST PAIN NOT DUE TO MYOCARDIAL ISCHEMIA
402 Index. B β-blockers, 4, 5 Bradyarrhythmias, 76 77
 Index A Acquired immunodeficiency syndrome (AIDS), 126, 163 Action potentials, 1, 5, 27 Acute coronary syndromes, 123t, 129 Adenosine, intravenous, 277 Alcohol abuse, as T wave inversion cause, 199 Aneurysm,
Index A Acquired immunodeficiency syndrome (AIDS), 126, 163 Action potentials, 1, 5, 27 Acute coronary syndromes, 123t, 129 Adenosine, intravenous, 277 Alcohol abuse, as T wave inversion cause, 199 Aneurysm,
Cardiology/Cardiothoracic
 Cardiology/Cardiothoracic ICD-9-CM to ICD-10-CM Code Mapper 800-334-5724 www.contexomedia.com 2013 ICD-9-CM 272.0 Pure hypercholesterolemia 272.2 Mixed hyperlipidemia 272.4 Other and hyperlipidemia 278.00
Cardiology/Cardiothoracic ICD-9-CM to ICD-10-CM Code Mapper 800-334-5724 www.contexomedia.com 2013 ICD-9-CM 272.0 Pure hypercholesterolemia 272.2 Mixed hyperlipidemia 272.4 Other and hyperlipidemia 278.00
Cardiovascular Disease
 Cardiovascular Disease Session Guidelines This is a 15 minute webinar session for CNC physicians and staff CNC holds webinars on the 3 rd Wednesday of each month to address topics related to risk adjustment
Cardiovascular Disease Session Guidelines This is a 15 minute webinar session for CNC physicians and staff CNC holds webinars on the 3 rd Wednesday of each month to address topics related to risk adjustment
Return to Basics. ECG Rate and Rhythm. Management of the Hospitalized Patient September 25, 2009
 Management of the Hospitalized Patient September 25, 2009 ECG Refresher and Update 2009 Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Management of the Hospitalized Patient September 25, 2009 ECG Refresher and Update 2009 Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Acute Coronary Syndromes Unstable Angina Non ST segment Elevation MI (NSTEMI) ST segment Elevation MI (STEMI)
 ST segment Elevation MI (STEMI)") Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Evaluate common abnormalities that mimic myocardial infarction. Identify
Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Evaluate common abnormalities that mimic myocardial infarction. Identify
Clinical Policy: Holter Monitors Reference Number: CP.MP.113
 Clinical Policy: Reference Number: CP.MP.113 Effective Date: 05/18 Last Review Date: 04/18 Coding Implications Revision Log Description Ambulatory electrocardiogram (ECG) monitoring provides a view of
Clinical Policy: Reference Number: CP.MP.113 Effective Date: 05/18 Last Review Date: 04/18 Coding Implications Revision Log Description Ambulatory electrocardiogram (ECG) monitoring provides a view of
Recommended Evaluation Data Excerpt from NVIC 04-08
 Recommended Evaluation Data Excerpt from NVIC 04-08 Purpose: This document is an excerpt from the Medical and Physical Evaluations Guidelines for Merchant Mariner Credentials, contained in enclosure 3
Recommended Evaluation Data Excerpt from NVIC 04-08 Purpose: This document is an excerpt from the Medical and Physical Evaluations Guidelines for Merchant Mariner Credentials, contained in enclosure 3
DIAGNOSTIC CRITERIA OF AMI/ACS
 DIAGNOSTIC CRITERIA OF AMI/ACS Diagnostic criteria are used to validate clinical diagnoses. Those used in epidemiological studies are here below reported. 1. MONICA - Monitoring trends and determinants
DIAGNOSTIC CRITERIA OF AMI/ACS Diagnostic criteria are used to validate clinical diagnoses. Those used in epidemiological studies are here below reported. 1. MONICA - Monitoring trends and determinants
ASE 2011 Appropriate Use Criteria for Echocardiography
 ASE 2011 Appropriate Use Criteria for Echocardiography Table 1. TTE for General Evaluation of Cardiac Structure and Function 1 2 Suspected Cardiac Etiology General With TTE Symptoms or conditions potentially
ASE 2011 Appropriate Use Criteria for Echocardiography Table 1. TTE for General Evaluation of Cardiac Structure and Function 1 2 Suspected Cardiac Etiology General With TTE Symptoms or conditions potentially
EXERCISE TESTING GUIDELINE
 EXERCISE TESTING GUIDELINE This guidance does not override the individual responsibility of health professionals to make appropriate decision according to the circumstances of the individual patient in
EXERCISE TESTING GUIDELINE This guidance does not override the individual responsibility of health professionals to make appropriate decision according to the circumstances of the individual patient in
C1: Medical Standards for Safety Critical Workers with Cardiovascular Disorders
 C1: Medical Standards for Safety Critical Workers with Cardiovascular Disorders GENERAL ISSUES REGARDING MEDICAL FITNESS-FOR-DUTY 1. These medical standards apply to Union Pacific Railroad (UPRR) employees
C1: Medical Standards for Safety Critical Workers with Cardiovascular Disorders GENERAL ISSUES REGARDING MEDICAL FITNESS-FOR-DUTY 1. These medical standards apply to Union Pacific Railroad (UPRR) employees
Return to Basics. Normal Intervals & Axes. ECG Rate and Rhythm
 Return to Basics Management of the Hospitalized Patient October 15, 2010 ECG Refresher and Update 2010 Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Return to Basics Management of the Hospitalized Patient October 15, 2010 ECG Refresher and Update 2010 Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Acute Coronary Syndrome. Sonny Achtchi, DO
 Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
CURRENT STATUS OF STRESS TESTING JOHN HAMATY D.O.
 CURRENT STATUS OF STRESS TESTING JOHN HAMATY D.O. INTRODUCTION Form of imprisonment in 1818 Edward Smith s observations TECHNIQUE Heart rate Blood pressure ECG parameters Physical appearance INDICATIONS
CURRENT STATUS OF STRESS TESTING JOHN HAMATY D.O. INTRODUCTION Form of imprisonment in 1818 Edward Smith s observations TECHNIQUE Heart rate Blood pressure ECG parameters Physical appearance INDICATIONS
Cardiac Pathology & Rehabilitation
 Cardiac Pathology & Rehabilitation Which of the following best describes the physical activity performed in my leisure time? A. I perform vigorous physical activity 3X/week for 20 minutes each time B.
Cardiac Pathology & Rehabilitation Which of the following best describes the physical activity performed in my leisure time? A. I perform vigorous physical activity 3X/week for 20 minutes each time B.
Practitioner Education Course
 2015 Practitioner Education Course ST Elevation Myocardial Infarction 2 Pathology Concept of vulnerable plaque Mild Atheroma Diagnosis IVUS OCT 3 Diagnosis This is based on : Clinical History ECG Changes.
2015 Practitioner Education Course ST Elevation Myocardial Infarction 2 Pathology Concept of vulnerable plaque Mild Atheroma Diagnosis IVUS OCT 3 Diagnosis This is based on : Clinical History ECG Changes.
Review of Cardiac Imaging Modalities in the Renal Patient. George Youssef
 Review of Cardiac Imaging Modalities in the Renal Patient George Youssef ECHO Left ventricular hypertrophy (LVH) assessment Diastolic dysfunction Stress ECHO Cardiac CT angiography Echocardiography - positives
Review of Cardiac Imaging Modalities in the Renal Patient George Youssef ECHO Left ventricular hypertrophy (LVH) assessment Diastolic dysfunction Stress ECHO Cardiac CT angiography Echocardiography - positives
UNDERSTANDING YOUR ECG: A REVIEW
 UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
General Introduction to ECG. Reading Assignment (p2-16 in PDF Outline )
") General Introduction to ECG Reading Assignment (p2-16 in PDF Outline ) Objectives 1. Practice the 5-step Method 2. Differential Diagnosis: R & L axis deviation 3. Differential Diagnosis: Poor R-wave progression
General Introduction to ECG Reading Assignment (p2-16 in PDF Outline ) Objectives 1. Practice the 5-step Method 2. Differential Diagnosis: R & L axis deviation 3. Differential Diagnosis: Poor R-wave progression
Pearls & Pitfalls in nuclear cardiology
 Pearls & Pitfalls in nuclear cardiology Maythinee Chantadisai, MD., NM physician Division of Nuclear Medicine, Department of radiology, KCMH Principle of myocardial perfusion imaging (MPI) Radiotracer
Pearls & Pitfalls in nuclear cardiology Maythinee Chantadisai, MD., NM physician Division of Nuclear Medicine, Department of radiology, KCMH Principle of myocardial perfusion imaging (MPI) Radiotracer
Congestive Heart Failure or Heart Failure
 Congestive Heart Failure or Heart Failure Dr Hitesh Patel Ascot Cardiology Group Heart Failure Workshop April, 2014 Question One What is the difference between congestive heart failure and heart failure?
Congestive Heart Failure or Heart Failure Dr Hitesh Patel Ascot Cardiology Group Heart Failure Workshop April, 2014 Question One What is the difference between congestive heart failure and heart failure?
Review Packet EKG Competency This packet is a review of the information you will need to know for the proctored EKG competency test.
 Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
12 Lead EKG Chapter 4 Worksheet
 Match the following using the word bank. 1. A form of arteriosclerosis in which the thickening and hardening of the vessels walls are caused by an accumulation of fatty deposits in the innermost lining
Match the following using the word bank. 1. A form of arteriosclerosis in which the thickening and hardening of the vessels walls are caused by an accumulation of fatty deposits in the innermost lining
12 Lead ECG Workshop. Virginia Hass, DNP, FNP-C, PA-C Kim Newlin, CNS, ANP-C, FPCNA. California Association of Nurse Practitioners March 18, 2016
 12 Lead ECG Workshop Virginia Hass, DNP, FNP-C, PA-C Kim Newlin, CNS, ANP-C, FPCNA California Association of Nurse Practitioners March 18, 2016 Learning Objectives Identify key changes on the ECG which
12 Lead ECG Workshop Virginia Hass, DNP, FNP-C, PA-C Kim Newlin, CNS, ANP-C, FPCNA California Association of Nurse Practitioners March 18, 2016 Learning Objectives Identify key changes on the ECG which
12-Lead ECG Interpretation. Kathy Kuznar, RN, ANP
 12-Lead ECG Interpretation Kathy Kuznar, RN, ANP The 12-Lead ECG Objectives Identify the normal morphology and features of the 12- lead ECG. Perform systematic analysis of the 12-lead ECG. Recognize abnormalities
12-Lead ECG Interpretation Kathy Kuznar, RN, ANP The 12-Lead ECG Objectives Identify the normal morphology and features of the 12- lead ECG. Perform systematic analysis of the 12-lead ECG. Recognize abnormalities
Echocardiography as a diagnostic and management tool in medical emergencies
 Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
10 ECGs No Practitioner Can Afford to Miss. Objectives
 10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
Ekg pra pr c a tice D.HAMMOUDI.MD
 Ekg practice D.HAMMOUDI.MD Anatomy Revisited RCA (Right Coronary Artery) Right ventricle Inferior wall of LV Posterior wall of LV (75%) SA Node (60%) AV Node (>80%) LCA (Left Coronary Artery) Septal wall
Ekg practice D.HAMMOUDI.MD Anatomy Revisited RCA (Right Coronary Artery) Right ventricle Inferior wall of LV Posterior wall of LV (75%) SA Node (60%) AV Node (>80%) LCA (Left Coronary Artery) Septal wall
The use of Cardiac CT and MRI in Clinical Practice
 The use of Cardiac CT and MRI in Clinical Practice Matthew W. Martinez, MD Assistant Professor of Medicine LVPG - Lehigh Valley Heart Specialists Lehigh Valley Health Network Oct. 3, 2009 DISCLOSURE Relevant
The use of Cardiac CT and MRI in Clinical Practice Matthew W. Martinez, MD Assistant Professor of Medicine LVPG - Lehigh Valley Heart Specialists Lehigh Valley Health Network Oct. 3, 2009 DISCLOSURE Relevant
Skin supplied by T1-4 (medial upper arm and neck) T5-9- epigastrium Visceral afferents from skin and heart are the same dorsal root ganglio
 T5-9- epigastrium Visceral afferents from skin and heart are the same dorsal root ganglio") Cardio 2 ECG... 3 Cardiac Remodelling... 11 Valvular Diseases... 13 Hypertension... 18 Aortic Coarctation... 24 Erythropoiesis... 27 Haemostasis... 30 Anaemia... 36 Atherosclerosis... 44 Angina... 48 Myocardial
Cardio 2 ECG... 3 Cardiac Remodelling... 11 Valvular Diseases... 13 Hypertension... 18 Aortic Coarctation... 24 Erythropoiesis... 27 Haemostasis... 30 Anaemia... 36 Atherosclerosis... 44 Angina... 48 Myocardial
Optimal testing for coronary artery disease in symptomatic and asymptomatic patients
 Optimal testing for coronary artery disease in symptomatic and asymptomatic patients Alexandre C Ferreira, MD Clinical Chief of Cardiology Jackson Health System Director, Interventional Cardiology Training
Optimal testing for coronary artery disease in symptomatic and asymptomatic patients Alexandre C Ferreira, MD Clinical Chief of Cardiology Jackson Health System Director, Interventional Cardiology Training
Basics of Cardiopulmonary Exercise Test Interpretation. Robert Kempainen, MD Hennepin County Medical Center
 Basics of Cardiopulmonary Exercise Test Interpretation Robert Kempainen, MD Hennepin County Medical Center None Conflicts of Interest Objectives Explain what normally limits exercise Summarize basic protocol
Basics of Cardiopulmonary Exercise Test Interpretation Robert Kempainen, MD Hennepin County Medical Center None Conflicts of Interest Objectives Explain what normally limits exercise Summarize basic protocol
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016
 Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
Local Coverage Determination (LCD) for Cardiac Catheterization (L29090)
 for Cardiac Catheterization (L29090)") Local Coverage Determination (LCD) for Cardiac Catheterization (L29090) Contractor Information Contractor Name First Coast Service Options, Inc. Contractor Number 09102 Contractor Type MAC - Part B LCD
Local Coverage Determination (LCD) for Cardiac Catheterization (L29090) Contractor Information Contractor Name First Coast Service Options, Inc. Contractor Number 09102 Contractor Type MAC - Part B LCD
Junctional Premature Contraction (JPC)
") Where s the PAC? Junctional Premature Contraction (JPC) A junctional premature contraction (JPC) is a beat that originates prematurely in the AV node. It can occur sporadically or in a grouped pattern.
Where s the PAC? Junctional Premature Contraction (JPC) A junctional premature contraction (JPC) is a beat that originates prematurely in the AV node. It can occur sporadically or in a grouped pattern.
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST F. Baborski 1, I. Scuric 1, D. Cerovec 1, M. Novoselec 1, V. Slivnjak 1, K. Fuckar 1, N. Lakusic 1, Z. Vajdic 2, R. Bernat 3, K. Kapov-Svilicic 3 (1) Special Hospital
DECLARATION OF CONFLICT OF INTEREST F. Baborski 1, I. Scuric 1, D. Cerovec 1, M. Novoselec 1, V. Slivnjak 1, K. Fuckar 1, N. Lakusic 1, Z. Vajdic 2, R. Bernat 3, K. Kapov-Svilicic 3 (1) Special Hospital
Ischemic Heart Disease
 Ischemic Heart Disease Dr Rodney Itaki Lecturer Division of Pathology University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology General Consideration Results from partial
Ischemic Heart Disease Dr Rodney Itaki Lecturer Division of Pathology University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology General Consideration Results from partial
SIMPLY ECGs. Dr William Dooley
 SIMPLY ECGs Dr William Dooley 1 No anatomy just interpretation 2 Setting up an ECG 3 Setting up an ECG 1 V1-4 th Right intercostal space at sternal border 2 V2-4 th Left intercostal space at sternal border
SIMPLY ECGs Dr William Dooley 1 No anatomy just interpretation 2 Setting up an ECG 3 Setting up an ECG 1 V1-4 th Right intercostal space at sternal border 2 V2-4 th Left intercostal space at sternal border
Results of Ischemic Heart Disease
 Ischemic Heart Disease: Angina and Myocardial Infarction Ischemic heart disease; syndromes causing an imbalance between myocardial oxygen demand and supply (inadequate myocardial blood flow) related to
Ischemic Heart Disease: Angina and Myocardial Infarction Ischemic heart disease; syndromes causing an imbalance between myocardial oxygen demand and supply (inadequate myocardial blood flow) related to
Return to Basics. ECG Rate and Rhythm. Management of the Hospitalized Patient October 4, 2007
 Management of the Hospitalized Patient October 4, 2007 ECG Refresher for the Hospitalists Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare
Management of the Hospitalized Patient October 4, 2007 ECG Refresher for the Hospitalists Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare
Heart Disorders. Cardiovascular Disorders (Part B-1) Module 5 -Chapter 8. Overview Heart Disorders Vascular Disorders
 Module 5 -Chapter 8. Overview Heart Disorders Vascular Disorders") Cardiovascular Disorders (Part B-1) Module 5 -Chapter 8 Overview Heart Disorders Vascular Disorders Susie Turner, MD 1/7/13 Heart Disorders Coronary Artery Disease Cardiac Arrhythmias Congestive Heart
Cardiovascular Disorders (Part B-1) Module 5 -Chapter 8 Overview Heart Disorders Vascular Disorders Susie Turner, MD 1/7/13 Heart Disorders Coronary Artery Disease Cardiac Arrhythmias Congestive Heart
Cardiac arrhythmias. Janusz Witowski. Department of Pathophysiology Poznan University of Medical Sciences. J. Witowski
 Cardiac arrhythmias Janusz Witowski Department of Pathophysiology Poznan University of Medical Sciences A 68-year old man presents to the emergency department late one evening complaining of increasing
Cardiac arrhythmias Janusz Witowski Department of Pathophysiology Poznan University of Medical Sciences A 68-year old man presents to the emergency department late one evening complaining of increasing
Chapter 2 Practical Approach
 Chapter 2 Practical Approach There are beginners in electrocardiogram (ECG) analysis who are fascinated by a special pattern (e.g., a bundle-branch block or a striking Q wave) and thereby overlook other
Chapter 2 Practical Approach There are beginners in electrocardiogram (ECG) analysis who are fascinated by a special pattern (e.g., a bundle-branch block or a striking Q wave) and thereby overlook other
Acute Coronary Syndrome
 ACUTE CORONOARY SYNDROME, ANGINA & ACUTE MYOCARDIAL INFARCTION Administrative Consultant Service 3/17 Acute Coronary Syndrome Acute Coronary Syndrome has evolved as a useful operational term to refer to
ACUTE CORONOARY SYNDROME, ANGINA & ACUTE MYOCARDIAL INFARCTION Administrative Consultant Service 3/17 Acute Coronary Syndrome Acute Coronary Syndrome has evolved as a useful operational term to refer to
Essam Mahfouz, MD. Professor of Cardiology, Mansoura University
 By Essam Mahfouz, MD. Professor of Cardiology, Mansoura University Agenda Definitions Classifications Epidemiology Risk stratification What is new? What is MI? Myocardial infarction is the death of part
By Essam Mahfouz, MD. Professor of Cardiology, Mansoura University Agenda Definitions Classifications Epidemiology Risk stratification What is new? What is MI? Myocardial infarction is the death of part
Abnormal, Autoquant Adenosine Myocardial Perfusion Heart Imaging. ID: GOLD Date: Age: 46 Sex: M John Doe Phone (310)
") Background: Reason: preoperative assessment of CAD, Shortness of Breath Symptom: atypical chest pain Risk factors: hypertension Under influence: a beta blocker Medications: digoxin Height: 66 in. Weight:
Background: Reason: preoperative assessment of CAD, Shortness of Breath Symptom: atypical chest pain Risk factors: hypertension Under influence: a beta blocker Medications: digoxin Height: 66 in. Weight:
Sudden cardiac death: Primary and secondary prevention
 Sudden cardiac death: Primary and secondary prevention By Kai Chi Chan Penultimate Year Medical Student St George s University of London at UNic Sheba Medical Centre Definition Sudden cardiac arrest (SCA)
Sudden cardiac death: Primary and secondary prevention By Kai Chi Chan Penultimate Year Medical Student St George s University of London at UNic Sheba Medical Centre Definition Sudden cardiac arrest (SCA)
CHEST PAIN CDU INCLUSION CRITERIA
 CHEST PAIN CDU INCLUSION CRITERIA No clinical criteria for ACS Stable vital signs Initial ECG and cardiac biomarkers not consistent with ACS Low to intermediate ACS risk (HEART score 0-6) [Ref 1, 2] Plan
CHEST PAIN CDU INCLUSION CRITERIA No clinical criteria for ACS Stable vital signs Initial ECG and cardiac biomarkers not consistent with ACS Low to intermediate ACS risk (HEART score 0-6) [Ref 1, 2] Plan
Chest Pain. Dr. Amitesh Aggarwal. Department of Medicine
 Chest Pain Dr. Amitesh Aggarwal Department of Medicine BACKGROUND Approx 5% of all ED visits 15 % - AMI 25-30 % - Unstable angina 50-55 % - Other conditions Atypical presentations common 2% of patients
Chest Pain Dr. Amitesh Aggarwal Department of Medicine BACKGROUND Approx 5% of all ED visits 15 % - AMI 25-30 % - Unstable angina 50-55 % - Other conditions Atypical presentations common 2% of patients
Acute Coronary Syndromes. Disclosures
 Acute Coronary Syndromes Disclosures I work for Virginia Garcia Memorial Health Center, Beaverton, OR. Jon Tardiff, BS, PA-C OHSU Clinical Assistant Professor And I am a medical editor for Jones & Bartlett
Acute Coronary Syndromes Disclosures I work for Virginia Garcia Memorial Health Center, Beaverton, OR. Jon Tardiff, BS, PA-C OHSU Clinical Assistant Professor And I am a medical editor for Jones & Bartlett
UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME. DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18
 Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18") UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18 INTRODUCTION The clinical entities that comprise acute coronary syndromes (ACS)-ST-segment
UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18 INTRODUCTION The clinical entities that comprise acute coronary syndromes (ACS)-ST-segment
Cardiology Updates: Syncope and Stress Testing. Kathleen Morris, DO Cardiology Fellow St. Vincent Hospital
 Cardiology Updates: Syncope and Stress Testing Kathleen Morris, DO Cardiology Fellow St. Vincent Hospital Disclosures NONE PART ONE: Let s start with SYNCOPE Objectives: Definition of Syncope Brief review
Cardiology Updates: Syncope and Stress Testing Kathleen Morris, DO Cardiology Fellow St. Vincent Hospital Disclosures NONE PART ONE: Let s start with SYNCOPE Objectives: Definition of Syncope Brief review