Management of acute Cardiac Arrhythmias
|
|
|
- Jayson Clinton Bond
- 6 years ago
- Views:
Transcription
1 Management of acute Cardiac Arrhythmias Dr. Zulkeflee Muhammad MBChB (New Zealand), MRCP (United Kingdom) Cardiologist Electrophysiology Unit Istitut Jantung Negara
2 Objectives Review the etiology and recognition of common arrhythmias. Review management of cardiac arrhythmias, with a focus on the relevant recent literature.
3 Depolarization mv Phase 1 Phase 2 (Plateau Phase) Cardiac Action Potential Phase 0 Phase 3-80 Resting membrane Potential -100 Na Na ca ++ Na+ + m Na + h K + ca ++ K + K + K + K + ca ca++ Na+ Phase 4 K + ATPase

4 Depolarization mv Phase 1 Phase 2 (Plateau Phase) Cardiac Action Potential Phase 0 Phase 3 Phase 4 (only in pacemaker cells R.M.P -80 Phase Na Na ca ++ Na+ + m Na + h K + ca ++ K + K + K + K + ca ca++ Na+ ATPase K +
5
6
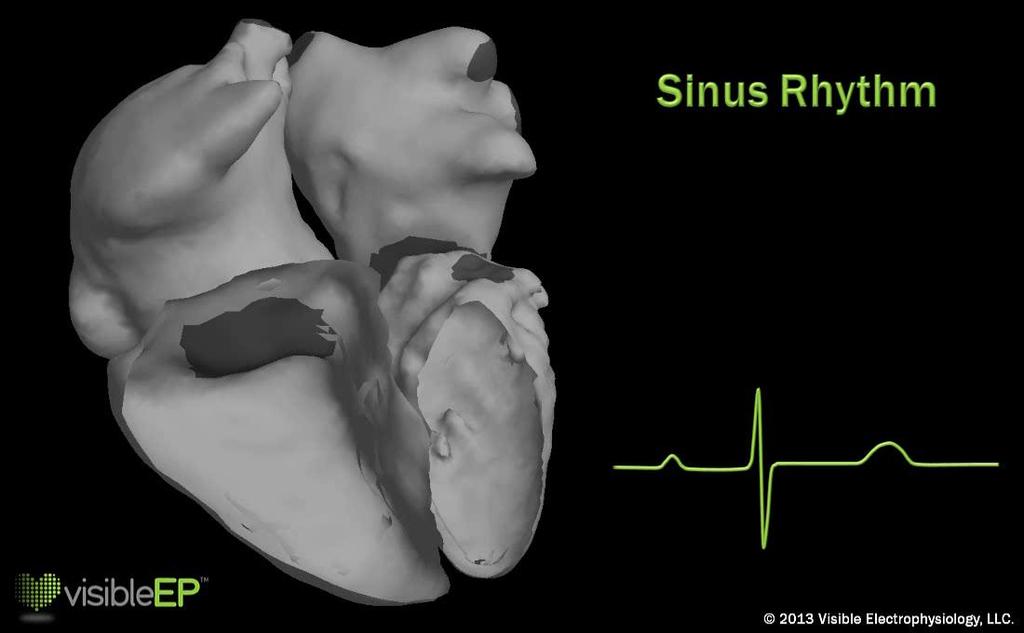
7 Normal Sinus Rhythm Implies normal sequence of conduction, originating in the sinus node and proceeding to the ventricles via the AV node and His-Purkinje system. EKG Characteristics: Regular narrow-complex rhythm Rate bpm Each QRS complex is proceeded by a P wave P wave is upright in lead II & downgoing in lead avr
8 Managing Acute Arrythmia Steps Take a deep breath Things will go a lot slower if you rush or panic Make use of those around you Pride can be dangerous Keep moving forward
9 Mechanism of Arrhthmogensis 1. Disorder of impulse formation. a) Automaticity. b) Triggered Activity. 1) Early after depolarization. 2) Delayed after depolarization. 2. Disorder of impulse conduction. a) Block Reentry. b) Reflection. 3. Combined disorder.
10 Case Study A 42 year old man presents to the hospital complaining of weakness and dizziness following an acute chest pain He is pale and diaphoretic appearing but awake Blood pressure 62/30 mm Hg Pulse 40/minute; slightly irregular Physical examination otherwise normal

11 ECG
12 Acute Management of this patient A: Thrombolysis B: Stabilized and treat bradycardia C: Emergent PCI D: Cardioversion E: Refer for permanent Pacemaker implant

13 Treatment of Acute Bradyarrythmia

14 PPM after AMI The need for TPW after AMI doesn t automatically indicate a need for PPM Transient conduction disturbances or LAHB are not indications for PPM after AMI. PPM is indicated in the presence of advanced AVB (2 nd / 3 rd degree) whether (persistent) or (transient with associated BBB)
15 Factors that help determine the need for brady pacemaker include: A: Symptoms such as syncope / presyncope B: bradyarrhythmia C: symptoms correlated to bradyarrhythmia D: symptoms not correlated to arrhythmia E: none of the above
16 Factors that help determine the need for brady pacemaker include: A: Symptoms such as syncope / presyncope B: bradyarrhythmia C: symptoms correlated to bradyarrhythmia D: symptoms not correlated to arrhythmia E: none of the above
17 ACC/ AHA Class I indications for pacing in 3 rd (and advanced 2 nd ) degree AVB Symptomatic bradycardia Asymptomatic CHB with asystole > 3 sec or awake HR < 40 bpm Before catheter ablation of AVN Arrhythmias / medical conditions requiring drugs that result in symptomatic bradycardia Neuromuscular disease with AVB
18 Case 2 ECG recorded from 55 years old male with history of heart disease in the ED.
19
20
21 Regular rhythm 120 beats/min Wide QRS AV dissociation dissociated P s Fusion complexes
22 Management of Acute Tachyarrythmia
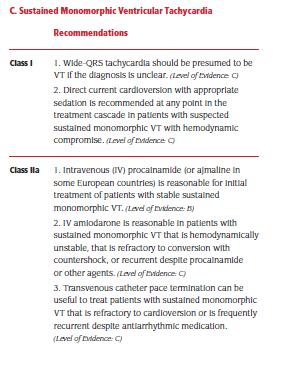
23 Monomorphic VT Procainamide is back in favour! For stable monomorphic VT, procainamide is listed as a class IIa intervention with a higher level of evidence than amiodarone (Class IIa, level of evidence B; amio Class IIa, level of evidence C). IV amiodarone is most reasonable for patients with sustained monomorphic VT that are hemodynamically unstable despite DC shocks or VT that is persistent / recurrent despite procainamide or other agents. Lignocaine is considered reasonable and effective when VT is thought to be related to myocardial ischemia or infarction. In cases of repetitive monomorphic VT in the setting of ACS, add beta blockers to your list of treatment options.
24 CASE STUDY Ms T. B. Y. 57 year lady Chinese Background Type 2 DM for 5 years Depression Taking Setraline since December 2010 Fainted 5 times over the past 3 years Preceded by exertion or hunger, sweating, dizziness and collapse Spontaneously recovered Family history Father SCD age 56 while at work Niece SCD at age of 10

25 CASE STUDY
26 CASE STUDY What are the differential diagnosis : 1. Ventricular Tachycardia 2. Ventricular Fibrillation 3. SVT with abberancy 4. Polymorphic Ventricular Tachycardia 5. None of the above
27 CASE STUDY How would you treat this patient? IV amiodarone DC shock 200j IV magnesium sulphate IV Adenosine IV Lidocaine
28 Management of Acute Tachyarrythmia

29 CASE STUDY Revert to sinus rhythm QTc = 650ms

30 CASE STUDY QTc = 540ms
31 VULNERABL E WINDOW
32 Mechanism of triggered arrhythmias
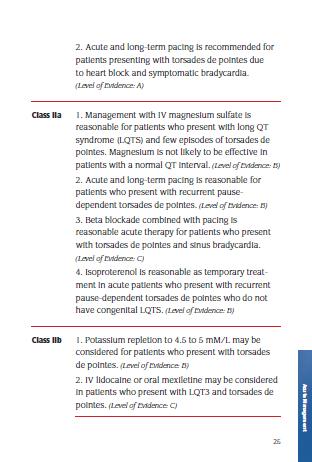
33 Torsades de Pointes type of PVT TdP is a PVT associated with a prolonged QT interval. Thus drugs that prolong the QT interval (including the sodium channel blocking antiarrhythmics - amiodarone, procainamide, probably lignocaine also) are best avoided. Magnesium is the first line drug (unlikely to be effective if the QT interval is normal - i.e. generic PVT). Other options include (overdrive) pacing and isoproterenol. Immediate withdrawal of any offending drugs or correction of electrolyte abnormalities (hypo-k, hypo-mg, hypo-ca) is very important.
34 Polymorphic VT (PVT) DC cardioversion is probably the best, and often the only, choice if the rhythm is persistent. For intermittent or recurrent PVT, consider IV Beta Blockers or IV amiodarone (ONLY if the patient has a normal QTs). Procainamide is also probably useful, and Lignocaine can be used especially if in the setting of suspected ACS. If ACS is suspected or can t be excluded urgent angiography should be considered. Magnesium is not likely to be effective in these patients (normal QT patients).
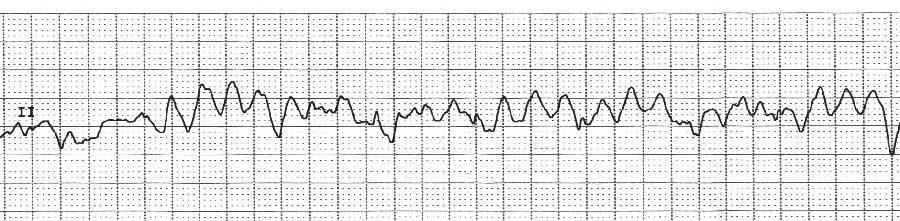
35 Case 3 Young patient presenting with sudden onset palpitations. ECG recorded in the ED.
36

37 AV nodal re-entrant tachycardia 60%+ of SVT, F > M Acute termination with adenosine Antiarrhythmic prophylaxis Beta-blockade Verapamil Flecainide Curable with radiofrequency ablation Success rates 95% P Risk of AV node damage 1-2% Therefore usually when medical therapy failed or unacceptable
38
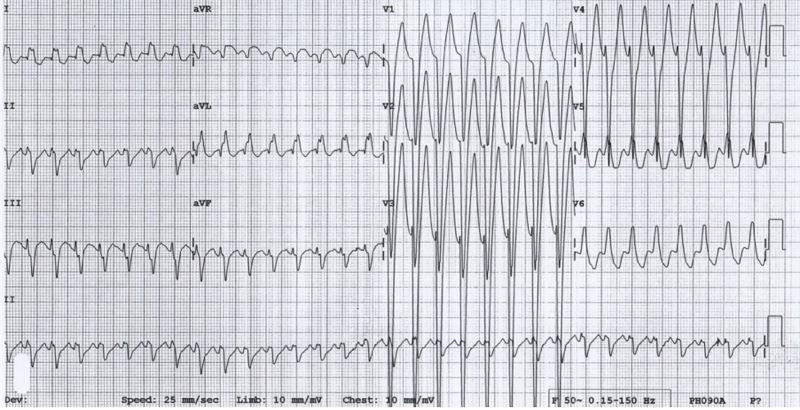
39 Case 4 A 28 y.o. medical officer comes to your clinic describing an incident of fluttering in her chest that began this morning after an overnight call. She has no relevant past medical history and takes no medications. Her pulse is 136 and regular. She drank a full 2-liter bottle of Mountain Dew this AM before rounds to wake up. ECG
40

41 Wolff-Parkinson-White Syndrome
42
43 Tachyarrythmia - Stable
44
45 Case 5 A 75 y.o. man with long-standing hypertension diagnosed 30 years ago, comes to your office complaining of fatigue and a sense of his heart pounding for the past day. He has never had this feeling before. His pulse is rapid and irregularly, irregular EKG

46 Case 5 Diagnosis: Atrial Fibrillation
47 CASE STUDY How would you treat this patient? IV amiodarone DC shock 200j IV magnesium sulphate IV Adenosine IV Lidocaine

48 Case 5 : After IV Amiodarone Diagnosis: Atrial Flutter (2:1)
49

50 AF Treatment Strategy
51 CHADS 2 score Data from Gage BF et al. JAMA 2001;285: Estimation of stroke risk in AF using CHADS 2 CHADS 2 criteria Score Congestive heart failure 1 Hypertension 1 Age >75 yrs 1 Diabetes mellitus 1 Stroke/transient ischaemic attack Annual stroke rate (%) 30


52
53 What is happening in the real world? AF population Low risk 25% Moderate/high risk 75% Optimal antithrombotic treatment ASA/no treatment VKA Limited VKA use due to contraindications Not eligible for VKA 35% Eligible for VKA 65% Limited VKA use due to logistical problems and underestimation benefit-risk ratio Not receiving VKA 50% Receiving VKA 50% What really happens! Aspirin / no treatment 75% VKA 25%
54 Classification of Anti-Arrhythmic Drugs Class IV: Ca ++ channel blockers - Phase 2 (Plateau Phase) - Class II: Beta blockers Class I: Na + channel blockers. Phase 1 Phase 3 Phase 0 - Pacemaker potential - R.M.P - Class III: K + channel blockers Phase 4
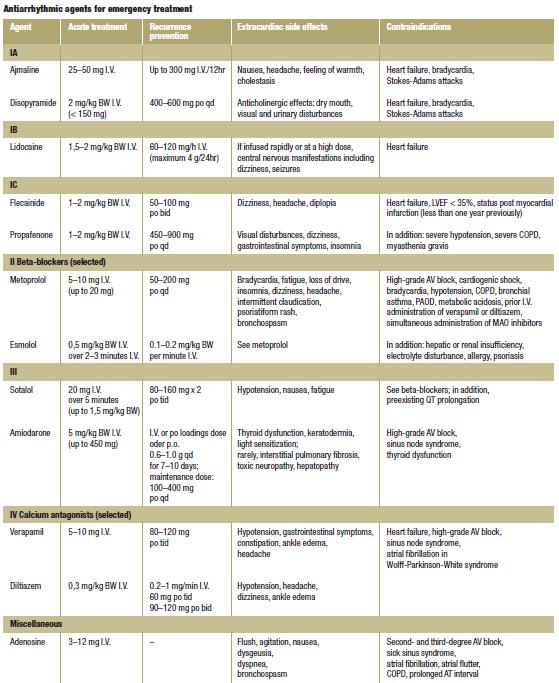
55 Classification of Antiarrhythmic Drugs based on Drug Action CLASS ACTION DRUGS I. Sodium Channel Blockers 1A. Moderate phase 0 depression and slowed conduction (2+); prolong repolarization 1B. Minimal phase 0 depression and slow conduction (0-1+); shorten repolarization 1C. Marked phase 0 depression and slow conduction (4+); little effect on repolarization Quinidine, Procainamide, Disopyramide Lidocaine Flecainide II. Beta-Adrenergic Blockers Propranolol, esmolol III. K + Channel Blockers (prolong repolarization) Amiodarone, Sotalol, Ibutilide IV. Calcium Channel Blockade Verapamil, Diltiazem
56
57 Amiodarone Been first-line drug for the treatment of stable ventricular tachycardia (VT) in recent years. Reason for preference: repeated demonstration that Lignocaine (prev drug of choice) is effective in terminating < 25% of cases of VT; another was that Procainamide is very slow to work. 1) Amiodarone Is Poorly Effective for the Acute Termination of Ventricular Tachycardia Marill KA, desouza IS, Nishijima DK, et al. Ann Emerg Med 2006;47: Set out to assess how effect Amiodarone is at terminating VF
58 33 VT patients 5 required electrical treatment within 20 minutes of initiation of Amiodarone (due to presyncope, hypotension, or other adverse effects which seemed related to the amiodarone). Only 8 (29%) of remaining 28 pts successfully converted. 18 of the 33 patients (55%) required electrical therapy (overdrive pacing, cardioversion or defibrillation) because of worsening symptoms or failure to respond. 5 (18%) of pts that did not respond to amiodarone did respond to another antidysrhythmic. Direct current cardioversion with sedation is still the most effective means of terminating VT and should be the preferred treatment in the emergency setting. Amiodarone is probably not as effective as previously thought; be wary of side effects & have electricity on hand!
59
60 Evidence Arrhythmic Complications of Electrical Cardioversion: Relationship to Shock Energy Gallagher MM, Yap YG, Padula M, et al. Int J Cardiol 2008;123: Guidelines for electrical cardioversion (ECV) of patients with atrial dysrhythmias have recommended starting with low energy (e.g. 50J-100J) and increasing in increments if the initial shocks fail. This recommendation is based on fears that high-energy shocks might induce myocardial damage or induce ventricular fibrillation. Authors proposed that higher energy levels may be safe and more effective.
61 For biphasic defibrillators, the Guidelines for ECV of AFib (1) suggest starting at 200 J, which is equivalent to monophasic shocks of 360 J. Since the authors caution against using monophasic shocks < 200J, they correspondingly caution against using biphasic shocks of < 100J. In the discussion, the authors make an interesting point, stating that It has been shown (2) that the initial use of a higher energy setting reduces the number of shocks required to effect [successful] cardioversion and in many cases [actually] reduces the total energy delivered. So it appears that higher energy levels are more effective and associated with slightly fewer complications. 1. Fuster V, Ryden LE, Cannom DS, et al. ACC/AHA/ESC 2006 Guidelines for the management of patients with atrial fibrillation. Eur Heart J 2006;27: Gallagher MM, Guo X, Ploneicki J, et al. Initial energy setting, outcome and efficiency in direct current cardioversion of atrial fibrillation and flutter. J Am Coll Cardiol 2001;38:
62 ACC/AHA/ESC Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death Executive Summary (MANY AUTHORS) CIRCULATION 2006;114:

63
64
65






66 QUESTION AND DISCUSSION
Chapter 9. Learning Objectives. Learning Objectives 9/11/2012. Cardiac Arrhythmias. Define electrical therapy
 Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014
 Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014 Financial disclosures Consultant Medtronic 3 reasons to evaluate and treat arrhythmias
Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014 Financial disclosures Consultant Medtronic 3 reasons to evaluate and treat arrhythmias
Antiarrhythmic Drugs
 Antiarrhythmic Drugs DR ATIF ALQUBBANY A S S I S T A N T P R O F E S S O R O F M E D I C I N E / C A R D I O L O G Y C O N S U L T A N T C A R D I O L O G Y & I N T E R V E N T I O N A L E P A C H D /
Antiarrhythmic Drugs DR ATIF ALQUBBANY A S S I S T A N T P R O F E S S O R O F M E D I C I N E / C A R D I O L O G Y C O N S U L T A N T C A R D I O L O G Y & I N T E R V E N T I O N A L E P A C H D /
Treatment of Arrhythmias in the Emergency Setting
 Treatment of Arrhythmias in the Emergency Setting Zian H. Tseng, M.D. Assistant Professor of Medicine Cardiac Electrophysiology Section Cardiology Division University of California, San Francisco There
Treatment of Arrhythmias in the Emergency Setting Zian H. Tseng, M.D. Assistant Professor of Medicine Cardiac Electrophysiology Section Cardiology Division University of California, San Francisco There
Pediatrics ECG Monitoring. Pediatric Intensive Care Unit Emergency Division
 Pediatrics ECG Monitoring Pediatric Intensive Care Unit Emergency Division 1 Conditions Leading to Pediatric Cardiology Consultation 12.7% of annual consultation Is arrhythmias problems Geggel. Pediatrics.
Pediatrics ECG Monitoring Pediatric Intensive Care Unit Emergency Division 1 Conditions Leading to Pediatric Cardiology Consultation 12.7% of annual consultation Is arrhythmias problems Geggel. Pediatrics.
The most common. hospitalized patients. hypotension due to. filling time Rate control in ICU patients may be difficult as many drugs cause hypotension
 Arrhythmias in the critically ill ICU patients: Approach for rapid recognition & management Objectives Be able to identify and manage: Atrial fibrillation with a rapid ventricular response Atrial flutter
Arrhythmias in the critically ill ICU patients: Approach for rapid recognition & management Objectives Be able to identify and manage: Atrial fibrillation with a rapid ventricular response Atrial flutter
APPROACH TO TACHYARRYTHMIAS
 APPROACH TO TACHYARRYTHMIAS PROF.DR.MD.ZAKIR HOSSAIN PROFESSOR AND HEAD DEPARTMENT OF MEDICINE SZMCH TACHYARRYTHMIA Cardiac arrythmia is a disturbance of electrical rhythm of heart. Cardac arrythmia with
APPROACH TO TACHYARRYTHMIAS PROF.DR.MD.ZAKIR HOSSAIN PROFESSOR AND HEAD DEPARTMENT OF MEDICINE SZMCH TACHYARRYTHMIA Cardiac arrythmia is a disturbance of electrical rhythm of heart. Cardac arrythmia with
Chapter 16: Arrhythmias and Conduction Disturbances
 Complete the following. Chapter 16: Arrhythmias and Conduction Disturbances 1. Cardiac arrhythmias result from abnormal impulse, abnormal impulse, or both mechanisms together. 2. is the ability of certain
Complete the following. Chapter 16: Arrhythmias and Conduction Disturbances 1. Cardiac arrhythmias result from abnormal impulse, abnormal impulse, or both mechanisms together. 2. is the ability of certain
Nathan Cade, MD Brandon Fainstad, MD Andrew Prouse, MD
 Nathan Cade, MD Brandon Fainstad, MD Andrew Prouse, MD OBJECTIVES 1. Identify the basic electrophysiology of the four causes of wide complex tachycardia. 2. Develop a simple framework for acute management
Nathan Cade, MD Brandon Fainstad, MD Andrew Prouse, MD OBJECTIVES 1. Identify the basic electrophysiology of the four causes of wide complex tachycardia. 2. Develop a simple framework for acute management
Atrial Fibrillation 10/2/2018. Depolarization & ECG. Atrial Fibrillation. Hemodynamic Consequences
 Depolarization & ECG Atrial Fibrillation How to make ORDER out of CHAOS Julia Shih, VMD, DACVIM (Cardiology) October 27, 2018 Depolarization & ECG Depolarization & ECG Atrial Fibrillation Hemodynamic Consequences
Depolarization & ECG Atrial Fibrillation How to make ORDER out of CHAOS Julia Shih, VMD, DACVIM (Cardiology) October 27, 2018 Depolarization & ECG Depolarization & ECG Atrial Fibrillation Hemodynamic Consequences
Chapter 26. Media Directory. Dysrhythmias. Diagnosis/Treatment of Dysrhythmias. Frequency in Population Difficult to Predict
 Chapter 26 Drugs for Dysrythmias Slide 33 Slide 35 Media Directory Propranolol Animation Amiodarone Animation Upper Saddle River, New Jersey 07458 All rights reserved. Dysrhythmias Abnormalities of electrical
Chapter 26 Drugs for Dysrythmias Slide 33 Slide 35 Media Directory Propranolol Animation Amiodarone Animation Upper Saddle River, New Jersey 07458 All rights reserved. Dysrhythmias Abnormalities of electrical
Anti arrhythmic drugs. Hilal Al Saffar College of medicine Baghdad University
 Anti arrhythmic drugs Hilal Al Saffar College of medicine Baghdad University Mechanism of Arrhythmia Abnormal heart pulse formation Abnormal heart pulse conduction Classification of Arrhythmia Abnormal
Anti arrhythmic drugs Hilal Al Saffar College of medicine Baghdad University Mechanism of Arrhythmia Abnormal heart pulse formation Abnormal heart pulse conduction Classification of Arrhythmia Abnormal
Cardiac arrhythmias. Janusz Witowski. Department of Pathophysiology Poznan University of Medical Sciences. J. Witowski
 Cardiac arrhythmias Janusz Witowski Department of Pathophysiology Poznan University of Medical Sciences A 68-year old man presents to the emergency department late one evening complaining of increasing
Cardiac arrhythmias Janusz Witowski Department of Pathophysiology Poznan University of Medical Sciences A 68-year old man presents to the emergency department late one evening complaining of increasing
AF and arrhythmia management. Dr Rhys Beynon Consultant Cardiologist and Electrophysiologist University Hospital of North Staffordshire
 AF and arrhythmia management Dr Rhys Beynon Consultant Cardiologist and Electrophysiologist University Hospital of North Staffordshire Atrial fibrillation Paroxysmal AF recurrent AF (>2 episodes) that
AF and arrhythmia management Dr Rhys Beynon Consultant Cardiologist and Electrophysiologist University Hospital of North Staffordshire Atrial fibrillation Paroxysmal AF recurrent AF (>2 episodes) that
Arrhythmic Complications of MI. Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine
 Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Arrhythmias. Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center
 Arrhythmias Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center 2012 Clinical Congress Presenter Disclosure Slide American College of Surgeons
Arrhythmias Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center 2012 Clinical Congress Presenter Disclosure Slide American College of Surgeons
Management of ATRIAL FIBRILLATION. in general practice. 22 BPJ Issue 39
 Management of ATRIAL FIBRILLATION in general practice 22 BPJ Issue 39 What is atrial fibrillation? Atrial fibrillation (AF) is the most common cardiac arrhythmia encountered in primary care. It is often
Management of ATRIAL FIBRILLATION in general practice 22 BPJ Issue 39 What is atrial fibrillation? Atrial fibrillation (AF) is the most common cardiac arrhythmia encountered in primary care. It is often
Case-Based Practical ECG Interpretation for the Generalist
 Case-Based Practical ECG Interpretation for the Generalist Paul D. Varosy, MD, FACC, FAHA, FHRS Director of Cardiac Electrophysiology VA Eastern Colorado Health Care System Associate Professor of Medicine
Case-Based Practical ECG Interpretation for the Generalist Paul D. Varosy, MD, FACC, FAHA, FHRS Director of Cardiac Electrophysiology VA Eastern Colorado Health Care System Associate Professor of Medicine
PHARMACOLOGY OF ARRHYTHMIAS
 PHARMACOLOGY OF ARRHYTHMIAS Course: Integrated Therapeutics 1 Lecturer: Dr. E. Konorev Date: November 27, 2012 Materials on: Exam #5 Required reading: Katzung, Chapter 14 1 CARDIAC ARRHYTHMIAS Abnormalities
PHARMACOLOGY OF ARRHYTHMIAS Course: Integrated Therapeutics 1 Lecturer: Dr. E. Konorev Date: November 27, 2012 Materials on: Exam #5 Required reading: Katzung, Chapter 14 1 CARDIAC ARRHYTHMIAS Abnormalities
Recurrent Implantable Defibrillator Discharges (ICD) Discharges ICD Storm
 Discharges ICD Storm") Recurrent Implantable Defibrillator Discharges (ICD) Discharges ICD Storm Guy Amit, MD, MPH Soroka University Medical Center Ben-Gurion University of the Negev Beer-Sheva, Israel Disclosures Consultant:
Recurrent Implantable Defibrillator Discharges (ICD) Discharges ICD Storm Guy Amit, MD, MPH Soroka University Medical Center Ben-Gurion University of the Negev Beer-Sheva, Israel Disclosures Consultant:
SHOCK THE PATIENT. Disclosures. Goals of the Talk. Tachyarrhythmias- Unstable 11/7/2017
 Disclosures Common Heart Rhythms in the Hospital Research Support: NIH, PCORI, Medtronic, Cardiogram Consulting: InCarda, Johnson & Johnson, Lifewatch Equity: InCarda Gregory M Marcus, MD, MAS Associate
Disclosures Common Heart Rhythms in the Hospital Research Support: NIH, PCORI, Medtronic, Cardiogram Consulting: InCarda, Johnson & Johnson, Lifewatch Equity: InCarda Gregory M Marcus, MD, MAS Associate
1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material
 1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material Arrhythmia recognition This tutorial builds on the ECG lecture and provides a framework for approaching any ECG to allow the
1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material Arrhythmia recognition This tutorial builds on the ECG lecture and provides a framework for approaching any ECG to allow the
Atrial Fibrillation Etiologies and Treatment. Shawn Liu Learner Centered Learning Goal
 Atrial Fibrillation Etiologies and Treatment Shawn Liu Learner Centered Learning Goal Pathophysiology Defined by the absence of coordinated atrial systole Results from multiple reentrant electrical waves
Atrial Fibrillation Etiologies and Treatment Shawn Liu Learner Centered Learning Goal Pathophysiology Defined by the absence of coordinated atrial systole Results from multiple reentrant electrical waves
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: WPW Revised: 11/2013
 Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: WPW Revised: 11/2013 Wolff-Parkinson-White syndrome (WPW) is a syndrome of pre-excitation of the
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: WPW Revised: 11/2013 Wolff-Parkinson-White syndrome (WPW) is a syndrome of pre-excitation of the
Case #1. 73 y/o man with h/o HTN and CHF admitted with dizziness and SOB Treated for CHF exacerbation with Lasix Now HR 136
 Tachycardias Case #1 73 y/o man with h/o HTN and CHF admitted with dizziness and SOB Treated for CHF exacerbation with Lasix Now HR 136 Initial Assessment Check Telemetry screen if pt on tele Telemetry
Tachycardias Case #1 73 y/o man with h/o HTN and CHF admitted with dizziness and SOB Treated for CHF exacerbation with Lasix Now HR 136 Initial Assessment Check Telemetry screen if pt on tele Telemetry
Antiarrhythmic Drugs 1/31/2018 1
 Antiarrhythmic Drugs 1/31/2018 1 Normal conduction pathway: 1- SA node generates action potential and delivers it to the atria and the AV node 2- The AV node delivers the impulse to purkinje fibers Other
Antiarrhythmic Drugs 1/31/2018 1 Normal conduction pathway: 1- SA node generates action potential and delivers it to the atria and the AV node 2- The AV node delivers the impulse to purkinje fibers Other
Dysrhythmias. Dysrythmias & Anti-Dysrhythmics. EKG Parameters. Dysrhythmias. Components of an ECG Wave. Dysrhythmias
 Dysrhythmias Dysrythmias & Anti-Dysrhythmics Rhythm bad in the heart: Whitewater rafting Electrical impulses coordinate heart Reduction in Cardiac Output PEA Asystole Components of an ECG Wave EKG Parameters
Dysrhythmias Dysrythmias & Anti-Dysrhythmics Rhythm bad in the heart: Whitewater rafting Electrical impulses coordinate heart Reduction in Cardiac Output PEA Asystole Components of an ECG Wave EKG Parameters
Arrhythmias. A/Prof Drew Richardson. The Canberra Hospital May MB BS (Hons) FACEM Grad CertHE MD
 FACEM Grad CertHE MD") Arrhythmias A/Prof Drew Richardson MB BS (Hons) FACEM Grad CertHE MD The Canberra Hospital May 2013 Objectives Recognise the features of the common nonlethal arrhythmias Describe the emergency treatment
Arrhythmias A/Prof Drew Richardson MB BS (Hons) FACEM Grad CertHE MD The Canberra Hospital May 2013 Objectives Recognise the features of the common nonlethal arrhythmias Describe the emergency treatment
Dos and Don t in Cardiac Arrhythmia. Case 1 -ECG. Case 1. Management. Emergency Admissions. Reduction of TE risk -CHADS 2 score. Hospital Admissions
 Emergency Admissions Dos and Don t in Cardiac Arrhythmia Tom Wong, MD, FESC Consultant Cardiologist, Honorary Senior Lecturer Royal Brompton & Harefield Hospitals National Heart and Lung Institute, Imperial
Emergency Admissions Dos and Don t in Cardiac Arrhythmia Tom Wong, MD, FESC Consultant Cardiologist, Honorary Senior Lecturer Royal Brompton & Harefield Hospitals National Heart and Lung Institute, Imperial
Ventricular tachycardia Ventricular fibrillation and ICD
 EKG Conference Ventricular tachycardia Ventricular fibrillation and ICD Samsung Medical Center CCU D.I. Hur Ji Won 2006.05.20 Ventricular tachyarrhythmia ventricular tachycardia ventricular fibrillation
EKG Conference Ventricular tachycardia Ventricular fibrillation and ICD Samsung Medical Center CCU D.I. Hur Ji Won 2006.05.20 Ventricular tachyarrhythmia ventricular tachycardia ventricular fibrillation
ECGs and Arrhythmias: Family Medicine Board Review 2009
 Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
Intraoperative and Postoperative Arrhythmias: Diagnosis and Treatment
 Intraoperative and Postoperative Arrhythmias: Diagnosis and Treatment Karen L. Booth, MD, Lucile Packard Children s Hospital Arrhythmias are common after congenital heart surgery [1]. Postoperative electrolyte
Intraoperative and Postoperative Arrhythmias: Diagnosis and Treatment Karen L. Booth, MD, Lucile Packard Children s Hospital Arrhythmias are common after congenital heart surgery [1]. Postoperative electrolyte
ECGs and Arrhythmias: Family Medicine Board Review 2012
 Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
Arrhythmias. Simple-dysfunction cause abnormalities in impulse formation and conduction in the myocardium.
 Arrhythmias Simple-dysfunction cause abnormalities in impulse formation and conduction in the myocardium. However, in clinic it present as a complex family of disorders that show variety of symptoms, for
Arrhythmias Simple-dysfunction cause abnormalities in impulse formation and conduction in the myocardium. However, in clinic it present as a complex family of disorders that show variety of symptoms, for
Arrhythmias. 1. beat too slowly (sinus bradycardia). Like in heart block
. Like in heart block") Arrhythmias It is a simple-dysfunction caused by abnormalities in impulse formation and conduction in the myocardium. The heart is designed in such a way that allows it to generate from the SA node electrical
Arrhythmias It is a simple-dysfunction caused by abnormalities in impulse formation and conduction in the myocardium. The heart is designed in such a way that allows it to generate from the SA node electrical
ECG S: A CASE-BASED APPROACH December 6,
 ECG S: A CASE-BASED APPROACH December 6, 2018 1 Faculty Disclosure Faculty: Lorne Gula MD, FRCPC Professor, Western University Cardiologist, Hearth Rhythm Specialist Director, Electrophysiology Laboratory,
ECG S: A CASE-BASED APPROACH December 6, 2018 1 Faculty Disclosure Faculty: Lorne Gula MD, FRCPC Professor, Western University Cardiologist, Hearth Rhythm Specialist Director, Electrophysiology Laboratory,
Acute Arrhythmias in the Hospitalized Patient
 Acute Arrhythmias in the Hospitalized Patient Gregory M Marcus, MD, MAS Associate Professor of Medicine Division of Cardiology University of California, San Francisc Disclosures Medtronic: Research Support
Acute Arrhythmias in the Hospitalized Patient Gregory M Marcus, MD, MAS Associate Professor of Medicine Division of Cardiology University of California, San Francisc Disclosures Medtronic: Research Support
Use of Antiarrhythmic Drugs for AF Who, What and How? Dr. Marc Cheng Queen Elizabeth Hospital
 Use of Antiarrhythmic Drugs for AF Who, What and How? Dr. Marc Cheng Queen Elizabeth Hospital Content i. Rhythm versus Rate control ii. Anti-arrhythmic for Rhythm Control iii. Anti-arrhythmic for Rate
Use of Antiarrhythmic Drugs for AF Who, What and How? Dr. Marc Cheng Queen Elizabeth Hospital Content i. Rhythm versus Rate control ii. Anti-arrhythmic for Rhythm Control iii. Anti-arrhythmic for Rate
CRC 431 ECG Basics. Bill Pruitt, MBA, RRT, CPFT, AE-C
 CRC 431 ECG Basics Bill Pruitt, MBA, RRT, CPFT, AE-C Resources White s 5 th ed. Ch 6 Electrocardiography Einthoven s Triangle Chest leads and limb leads Egan s 10 th ed. Ch 17 Interpreting the Electrocardiogram
CRC 431 ECG Basics Bill Pruitt, MBA, RRT, CPFT, AE-C Resources White s 5 th ed. Ch 6 Electrocardiography Einthoven s Triangle Chest leads and limb leads Egan s 10 th ed. Ch 17 Interpreting the Electrocardiogram
Dysrhythmias 11/7/2017. Disclosures. 3 reasons to evaluate and treat dysrhythmias. None. Eliminate symptoms and improve hemodynamics
 Dysrhythmias CYDNEY STEWART MD, FACC NOVEMBER 3, 2017 Disclosures None 3 reasons to evaluate and treat dysrhythmias Eliminate symptoms and improve hemodynamics Prevent imminent death/hemodynamic compromise
Dysrhythmias CYDNEY STEWART MD, FACC NOVEMBER 3, 2017 Disclosures None 3 reasons to evaluate and treat dysrhythmias Eliminate symptoms and improve hemodynamics Prevent imminent death/hemodynamic compromise
UNDERSTANDING YOUR ECG: A REVIEW
 UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
Chapter 14. Agents used in Cardiac Arrhythmias
 Chapter 14 Agents used in Cardiac Arrhythmias Cardiac arrhythmia Approximately 50% of post-myocardial infarction fatalities result from ventricular tachycarida (VT) or ventricular fibrillation (VF). These
Chapter 14 Agents used in Cardiac Arrhythmias Cardiac arrhythmia Approximately 50% of post-myocardial infarction fatalities result from ventricular tachycarida (VT) or ventricular fibrillation (VF). These
Drugs Controlling Myocyte Excitability and Conduction at the AV node Singh and Vaughan-Williams Classification
 Drugs Controlling Myocyte Excitability and Conduction at the AV node Singh and Vaughan-Williams Classification Class I Na Channel Blockers Flecainide Propafenone Class III K channel Blockers Dofetilide,
Drugs Controlling Myocyte Excitability and Conduction at the AV node Singh and Vaughan-Williams Classification Class I Na Channel Blockers Flecainide Propafenone Class III K channel Blockers Dofetilide,
Pediatrics. Arrhythmias in Children: Bradycardia and Tachycardia Diagnosis and Treatment. Overview
 Pediatrics Arrhythmias in Children: Bradycardia and Tachycardia Diagnosis and Treatment See online here The most common form of cardiac arrhythmia in children is sinus tachycardia which can be caused by
Pediatrics Arrhythmias in Children: Bradycardia and Tachycardia Diagnosis and Treatment See online here The most common form of cardiac arrhythmia in children is sinus tachycardia which can be caused by
ANTI - ARRHYTHMIC DRUGS
 ANTI - ARRHYTHMIC DRUGS CARDIAC ACTION POTENTIAL K Out Balance Ca in/k out Na in K Out GENERATION OF ARRHYTHMIAS Four mechanisms of arrhythmia generation; Increased normal automaticity Abnormal automaticity
ANTI - ARRHYTHMIC DRUGS CARDIAC ACTION POTENTIAL K Out Balance Ca in/k out Na in K Out GENERATION OF ARRHYTHMIAS Four mechanisms of arrhythmia generation; Increased normal automaticity Abnormal automaticity
The patient with (without) an ICD and heart failure: Management of electrical storm
 an ICD and heart failure: Management of electrical storm") ISHNE Heart Failure Virtual Symposium April 2008 The patient with (without) an ICD and heart failure: Management of electrical storm Westfälische Wilhelms-Universität Münster Günter Breithardt, MD, FESC,
ISHNE Heart Failure Virtual Symposium April 2008 The patient with (without) an ICD and heart failure: Management of electrical storm Westfälische Wilhelms-Universität Münster Günter Breithardt, MD, FESC,
Paramedic Rounds. Tachyarrhythmia's. Sean Sutton Dallas Wood
 Paramedic Rounds Tachyarrhythmia's Sean Sutton Dallas Wood Objectives At the end of this session, the paramedic will be able to: State the key components of the cardiac conduction pathway, along with the
Paramedic Rounds Tachyarrhythmia's Sean Sutton Dallas Wood Objectives At the end of this session, the paramedic will be able to: State the key components of the cardiac conduction pathway, along with the
ARRHYTHMIAS IN THE ICU
 ARRHYTHMIAS IN THE ICU Nora Goldschlager, MD MACP, FACC, FAHA, FHRS SFGH Division of Cardiology UCSF IDENTIFIED VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar) Electrolyte imbalance Proarrhythmia
ARRHYTHMIAS IN THE ICU Nora Goldschlager, MD MACP, FACC, FAHA, FHRS SFGH Division of Cardiology UCSF IDENTIFIED VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar) Electrolyte imbalance Proarrhythmia
Core Content In Urgent Care Medicine
 Palpitations/Arrhythmias Ebrahim Barkoudah, MD Clinical Instructor in Internal Medicine Harvard Medical School Assistant in Internal Medicine & Pediatrics Massachusetts General Hospital MGH Chelsea Chelsea,
Palpitations/Arrhythmias Ebrahim Barkoudah, MD Clinical Instructor in Internal Medicine Harvard Medical School Assistant in Internal Medicine & Pediatrics Massachusetts General Hospital MGH Chelsea Chelsea,
Antiarrhythmic Drugs. Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018
 Antiarrhythmic Drugs Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018 2 Ion Permeability Changes Potential Changes Genes and Proteins 3 Cardiac Na+ channels 5 6
Antiarrhythmic Drugs Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018 2 Ion Permeability Changes Potential Changes Genes and Proteins 3 Cardiac Na+ channels 5 6
Step by step approach to EKG rhythm interpretation:
 Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
The pill-in-the-pocket strategy for paroxysmal atrial fibrillation
 The pill-in-the-pocket strategy for paroxysmal atrial fibrillation KONSTANTINOS P. LETSAS, MD, FEHRA LABORATORY OF CARDIAC ELECTROPHYSIOLOGY EVANGELISMOS GENERAL HOSPITAL OF ATHENS ARRHYTHMIAS UPDATE,
The pill-in-the-pocket strategy for paroxysmal atrial fibrillation KONSTANTINOS P. LETSAS, MD, FEHRA LABORATORY OF CARDIAC ELECTROPHYSIOLOGY EVANGELISMOS GENERAL HOSPITAL OF ATHENS ARRHYTHMIAS UPDATE,
3. AV Block 1. First-degree AV block 1. Delay in AV node 2. Long PR interval 3. QRS complex follows each P wave 4. Benign, no tx
 1. Rhythms & arrhythmias SA nodal rhythms Sinus rhythm Sinus tachycardia Sinus bradycardia Sinus arrhythmia Sick sinus syndrome SA block Sinus arrest AV blocks First-degree Second-degree Mobitz Type I
1. Rhythms & arrhythmias SA nodal rhythms Sinus rhythm Sinus tachycardia Sinus bradycardia Sinus arrhythmia Sick sinus syndrome SA block Sinus arrest AV blocks First-degree Second-degree Mobitz Type I
Emergency treatment to SVT Evidence-based Approach. Tran Thao Giang
 Emergency treatment to SVT Evidence-based Approach Tran Thao Giang Description ECG manifestations: HR is extremely rapid and regular (240bpm ± 40) P wave is: usually invisible When visible: anormal P axis,
Emergency treatment to SVT Evidence-based Approach Tran Thao Giang Description ECG manifestations: HR is extremely rapid and regular (240bpm ± 40) P wave is: usually invisible When visible: anormal P axis,
Tachycardias II. Štěpán Havránek
 Tachycardias II Štěpán Havránek Summary 1) Supraventricular (supraventricular rhythms) Atrial fibrillation and flutter Atrial ectopic tachycardia / extrabeats AV nodal reentrant a AV reentrant tachycardia
Tachycardias II Štěpán Havránek Summary 1) Supraventricular (supraventricular rhythms) Atrial fibrillation and flutter Atrial ectopic tachycardia / extrabeats AV nodal reentrant a AV reentrant tachycardia
Electrical Storm in Coronary Artery Disease. Saeed Oraii MD, Cardiologist Interventional Electrophysiologist Tehran Arrhythmia Clinic July 2016
 Electrical Storm in Coronary Artery Disease Saeed Oraii MD, Cardiologist Interventional Electrophysiologist Tehran Arrhythmia Clinic July 2016 48 yrs. Old diabetic with ACS 48 yrs. Old diabetic with ACS
Electrical Storm in Coronary Artery Disease Saeed Oraii MD, Cardiologist Interventional Electrophysiologist Tehran Arrhythmia Clinic July 2016 48 yrs. Old diabetic with ACS 48 yrs. Old diabetic with ACS
ΚΟΛΠΙΚΗ ΜΑΡΜΑΡΥΓΗ ΦΑΡΜΑΚΕΥΤΙΚΗ ΗΛΕΚΤΡΙΚΗ ΑΝΑΤΑΞΗ. ΣΠΥΡΟΜΗΤΡΟΣ ΓΕΩΡΓΙΟΣ Καρδιολόγος, Ε/Α, Γ.Ν.Κατερίνης. F.E.S.C
 ΚΟΛΠΙΚΗ ΜΑΡΜΑΡΥΓΗ ΦΑΡΜΑΚΕΥΤΙΚΗ ΗΛΕΚΤΡΙΚΗ ΑΝΑΤΑΞΗ ΣΠΥΡΟΜΗΤΡΟΣ ΓΕΩΡΓΙΟΣ Καρδιολόγος, Ε/Α, Γ.Ν.Κατερίνης. F.E.S.C Definitions of AF: A Simplified Scheme Term Definition Paroxysmal AF AF that terminates
ΚΟΛΠΙΚΗ ΜΑΡΜΑΡΥΓΗ ΦΑΡΜΑΚΕΥΤΙΚΗ ΗΛΕΚΤΡΙΚΗ ΑΝΑΤΑΞΗ ΣΠΥΡΟΜΗΤΡΟΣ ΓΕΩΡΓΙΟΣ Καρδιολόγος, Ε/Α, Γ.Ν.Κατερίνης. F.E.S.C Definitions of AF: A Simplified Scheme Term Definition Paroxysmal AF AF that terminates
Current Guideline for AF Treatment. Young Keun On, MD, PhD, FHRS Samsung Medical Center Sungkyunkwan University School of Medicine
 Current Guideline for AF Treatment Young Keun On, MD, PhD, FHRS Samsung Medical Center Sungkyunkwan University School of Medicine Case 1 59 year-old lady Sudden palpitation and breathlessness for 12 hours
Current Guideline for AF Treatment Young Keun On, MD, PhD, FHRS Samsung Medical Center Sungkyunkwan University School of Medicine Case 1 59 year-old lady Sudden palpitation and breathlessness for 12 hours
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology
 Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
Arrhythmia Management Joshua M. Cooper, MD, FHRS, FACC
 Arrhythmia Management Joshua M. Cooper, MD, FHRS, FACC Professor of Medicine Director of Cardiac Electrophysiology Temple University Health System Plumbing Electrical System Bradyarrhythmias Sinus Node
Arrhythmia Management Joshua M. Cooper, MD, FHRS, FACC Professor of Medicine Director of Cardiac Electrophysiology Temple University Health System Plumbing Electrical System Bradyarrhythmias Sinus Node
CVD: Cardiac Arrhythmias. 1. Final Cardiac Arrhythmias_BMP. 1.1 Cardiovascular Disease. Notes:
 CVD: Cardiac Arrhythmias 1. Final Cardiac Arrhythmias_BMP 1.1 Cardiovascular Disease 1.2 Directions for taking this course 1.3 Content Experts 1.4 Disclosures 1.5 Accreditation Information 1.6 Learning
CVD: Cardiac Arrhythmias 1. Final Cardiac Arrhythmias_BMP 1.1 Cardiovascular Disease 1.2 Directions for taking this course 1.3 Content Experts 1.4 Disclosures 1.5 Accreditation Information 1.6 Learning
ARRHYTHMIAS IN THE ICU: DIAGNOSIS AND PRINCIPLES OF MANAGEMENT
 ARRHYTHMIAS IN THE ICU: DIAGNOSIS AND PRINCIPLES OF MANAGEMENT Nora Goldschlager, M.D. MACP, FACC, FAHA, FHRS SFGH Division of Cardiogy UCSF CLINICAL VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar)
ARRHYTHMIAS IN THE ICU: DIAGNOSIS AND PRINCIPLES OF MANAGEMENT Nora Goldschlager, M.D. MACP, FACC, FAHA, FHRS SFGH Division of Cardiogy UCSF CLINICAL VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar)
Arrhythmia 341. Ahmad Hersi Professor of Cardiology KSU
 Arrhythmia 341 Ahmad Hersi Professor of Cardiology KSU Objectives Epidemiology and Mechanisms of AF Evaluation of AF patients Classification of AF Treatment and Risk stratification of AF Identify other
Arrhythmia 341 Ahmad Hersi Professor of Cardiology KSU Objectives Epidemiology and Mechanisms of AF Evaluation of AF patients Classification of AF Treatment and Risk stratification of AF Identify other
Rate and Rhythm Control of Atrial Fibrillation
 Rate and Rhythm Control of Atrial Fibrillation April 21, 2017 춘계심혈관통합학술대회 Jaemin Shim, MD, PhD Arrhythmia Center Korea University Anam Hospital Treatment of AF Goal Reducing symptoms Preventing complication
Rate and Rhythm Control of Atrial Fibrillation April 21, 2017 춘계심혈관통합학술대회 Jaemin Shim, MD, PhD Arrhythmia Center Korea University Anam Hospital Treatment of AF Goal Reducing symptoms Preventing complication
DYSRHYTHMIAS. D. Assess whether or not it is the arrhythmia that is making the patient unstable or symptomatic
 DYSRHYTHMIAS GENERAL CONSIDERATIONS A. The 2015 American Heart Association Guidelines were referred to for this protocol development. Evidence-based science was implemented in those areas where the AHA
DYSRHYTHMIAS GENERAL CONSIDERATIONS A. The 2015 American Heart Association Guidelines were referred to for this protocol development. Evidence-based science was implemented in those areas where the AHA
Management of Arrhythmias The General Practitioners role
 Management of Arrhythmias The General Practitioners role Rohan Gunawardena MD, FRCP, FCCP, FACC Consultant Cardiac Electrophysiologist National Hospital of Sri Lanka Arrhythmias not common Palpitations
Management of Arrhythmias The General Practitioners role Rohan Gunawardena MD, FRCP, FCCP, FACC Consultant Cardiac Electrophysiologist National Hospital of Sri Lanka Arrhythmias not common Palpitations
I have nothing to disclose.
 I have nothing to disclose. Antiarrhythmic Therapy in Pregnancy Prof. Ali Oto,MD,FESC,FACC,FHRS Department of Cardiology Hacettepe University,Faculty of Medicine Ankara Arrhythmias in pregnancy An increased
I have nothing to disclose. Antiarrhythmic Therapy in Pregnancy Prof. Ali Oto,MD,FESC,FACC,FHRS Department of Cardiology Hacettepe University,Faculty of Medicine Ankara Arrhythmias in pregnancy An increased
ECG Interactive Session
 SA HEART 2018 PRE-CONGRESS WORKSHOP 4 OCTOBER 2018 ECG Interactive Session Ashley Chin Cardiologist/Electrophysiologist University of Cape Town Groote Schuur Hospital ECG 1 Which ONE of the following is
SA HEART 2018 PRE-CONGRESS WORKSHOP 4 OCTOBER 2018 ECG Interactive Session Ashley Chin Cardiologist/Electrophysiologist University of Cape Town Groote Schuur Hospital ECG 1 Which ONE of the following is
Ventricular arrhythmias
 Ventricular arrhythmias Assoc.Prof. Lucie Riedlbauchová, MD, PhD Department of Cardiology University HospitalMotol and2nd FacultyofMedicine, Charles University in Prague Definition and classification Ventricular
Ventricular arrhythmias Assoc.Prof. Lucie Riedlbauchová, MD, PhD Department of Cardiology University HospitalMotol and2nd FacultyofMedicine, Charles University in Prague Definition and classification Ventricular
PEDIATRIC SVT MANAGEMENT
 PEDIATRIC SVT MANAGEMENT 1 INTRODUCTION Supraventricular tachycardia (SVT) can be defined as an abnormally rapid heart rhythm originating above the ventricles, often (but not always) with a narrow QRS
PEDIATRIC SVT MANAGEMENT 1 INTRODUCTION Supraventricular tachycardia (SVT) can be defined as an abnormally rapid heart rhythm originating above the ventricles, often (but not always) with a narrow QRS
Atrial fibrillation in the ICU
 Atrial fibrillation in the ICU Atrial fibrillation Preexisting or incident (new onset) among nearly one in three critically ill patients Formation of arrhythogenic substrate usually fibrosis (CHF, hypertension,
Atrial fibrillation in the ICU Atrial fibrillation Preexisting or incident (new onset) among nearly one in three critically ill patients Formation of arrhythogenic substrate usually fibrosis (CHF, hypertension,
! YOU NEED TO MONITOR QT INTERVALS IN THESE PATIENTS.
 Antiarrhythmic Pharmacopoeia Powerful drugs, split into 4 major classes, according to the predominant receptor they effect. Some fit into several classes at once, like sotolol. Some don t fit at all, owing
Antiarrhythmic Pharmacopoeia Powerful drugs, split into 4 major classes, according to the predominant receptor they effect. Some fit into several classes at once, like sotolol. Some don t fit at all, owing
ACTIVITY DISCLAIMER DISCLOSURE. Craig Barstow, MD, FAAFP. Learning Objectives. Associated Session(s) Arrhythmias and Dysrhythmias: PBL
 Arrhythmias and Dysrhythmias: PBL") ACTIVITY DISCLAIMER Arrhythmias and Dysrhythmias: PBL Craig Barstow, MD, FAAFP The material presented here is being made available by the American Academy of Family Physicians for educational purposes
ACTIVITY DISCLAIMER Arrhythmias and Dysrhythmias: PBL Craig Barstow, MD, FAAFP The material presented here is being made available by the American Academy of Family Physicians for educational purposes
Supraventricular Tachycardia: From Fetus to Adult. Mohamed Hamdan, MD
 Supraventricular Tachycardia: From Fetus to Adult Mohamed Hamdan, MD Learning Objectives Define type of SVT by age Describe clinical approach Describe prenatal and postnatal management of SVT 2 SVT Across
Supraventricular Tachycardia: From Fetus to Adult Mohamed Hamdan, MD Learning Objectives Define type of SVT by age Describe clinical approach Describe prenatal and postnatal management of SVT 2 SVT Across
CSI Skills Lab #5: Arrhythmia Interpretation and Treatment
 CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
Mission Statement for our Arrhythmia Care
 Mission Statement for our Arrhythmia Care We are dedicated to provide a compassionate and an outstanding care for patients with cardiac arrhythmias. We will be utilizing the cutting edge and the most advanced
Mission Statement for our Arrhythmia Care We are dedicated to provide a compassionate and an outstanding care for patients with cardiac arrhythmias. We will be utilizing the cutting edge and the most advanced
Antiarrhythmic Drugs. Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2017
 Antiarrhythmic Drugs Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2017 Types of Cardiac Arrhythmias Abnormalities of Impulse Formation: Rate disturbances. Triggered
Antiarrhythmic Drugs Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2017 Types of Cardiac Arrhythmias Abnormalities of Impulse Formation: Rate disturbances. Triggered
Patient Resources: Arrhythmias and Congenital Heart Disease
 Patient Resources: Arrhythmias and Congenital Heart Disease Overview Arrhythmias (abnormal heart rhythms) can develop in patients with congenital heart disease (CHD) due to thickening/weakening of their
Patient Resources: Arrhythmias and Congenital Heart Disease Overview Arrhythmias (abnormal heart rhythms) can develop in patients with congenital heart disease (CHD) due to thickening/weakening of their
Cardiac Implanted Electronic Devices Pacemakers, Defibrillators, Cardiac Resynchronization Devices, Loop Recorders, etc.
 Cardiac Implanted Electronic Devices Pacemakers, Defibrillators, Cardiac Resynchronization Devices, Loop Recorders, etc. The Miracle of Living February 21, 2018 Matthew Ostrom MD,FACC,FHRS Division of
Cardiac Implanted Electronic Devices Pacemakers, Defibrillators, Cardiac Resynchronization Devices, Loop Recorders, etc. The Miracle of Living February 21, 2018 Matthew Ostrom MD,FACC,FHRS Division of
Management strategies for atrial fibrillation Thursday, 20 October :27
 ALTHOUGH anyone who has had to run up a flight of steps or has had a frightening experience is quite familiar with a racing heartbeat, for the more than 2 million Americans who suffer from atrial fibrillation
ALTHOUGH anyone who has had to run up a flight of steps or has had a frightening experience is quite familiar with a racing heartbeat, for the more than 2 million Americans who suffer from atrial fibrillation
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif
 Heart Arrhythmias 2 - Dr. Abdullah Sharif") 2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
Understanding Atrial Fibrillation Management. Roy Lin, MD
 Understanding Atrial Fibrillation Management Roy Lin, MD Disclosure None Definition of atrial fibrillation Atrial fibrillation is a supraventricular tachyarrhythmia characterized by uncoordinated atrial
Understanding Atrial Fibrillation Management Roy Lin, MD Disclosure None Definition of atrial fibrillation Atrial fibrillation is a supraventricular tachyarrhythmia characterized by uncoordinated atrial
EHRA Accreditation Exam - Sample MCQs Cardiac Pacing and ICDs
 EHRA Accreditation Exam - Sample MCQs Cardiac Pacing and ICDs Dear EHRA Member, Dear Colleague, As you know, the EHRA Accreditation Process is becoming increasingly recognised as an important step for
EHRA Accreditation Exam - Sample MCQs Cardiac Pacing and ICDs Dear EHRA Member, Dear Colleague, As you know, the EHRA Accreditation Process is becoming increasingly recognised as an important step for
Review Packet EKG Competency This packet is a review of the information you will need to know for the proctored EKG competency test.
 Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
Update on Palpitations and AF February 28 th 2018
 Update on Palpitations and AF February 28 th 2018 Dr Mrinal Andrew Saha MA(Cantab) MBBS FRCP PhD Consultant Interventional Cardiologist GHNHSFT Dr Mrinal Saha Appointed 2010 Special interests: Angioplasty,
Update on Palpitations and AF February 28 th 2018 Dr Mrinal Andrew Saha MA(Cantab) MBBS FRCP PhD Consultant Interventional Cardiologist GHNHSFT Dr Mrinal Saha Appointed 2010 Special interests: Angioplasty,
The ABCs of EKGs/ECGs for HCPs. Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions
 The ABCs of EKGs/ECGs for HCPs Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions Learning Objectives Review the basic anatomy of the heart Describe the cardiac conducting
The ABCs of EKGs/ECGs for HCPs Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions Learning Objectives Review the basic anatomy of the heart Describe the cardiac conducting
FLB s What Are Those Funny-Looking Beats?
 FLB s What Are Those Funny-Looking Beats? Reading Assignment (pages 27-45 in Outline ) The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis=
FLB s What Are Those Funny-Looking Beats? Reading Assignment (pages 27-45 in Outline ) The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis=
Mr. Eknath Kole M.S. Pharm (NIPER Mohali)
") M.S. Pharm (NIPER Mohali) Drug Class Actions Therapeutic Uses Pharmacokinetics Adverse Effects Other Quinidine IA -Binds to open and inactivated Na+ -Decreases the slope of Phase 4 spontaneous depolarization
M.S. Pharm (NIPER Mohali) Drug Class Actions Therapeutic Uses Pharmacokinetics Adverse Effects Other Quinidine IA -Binds to open and inactivated Na+ -Decreases the slope of Phase 4 spontaneous depolarization
ECG Workshop. Carolyn Shepherd And Anya Horne UWE Principles of Cardiac Care
 ECG Workshop Carolyn Shepherd And Anya Horne UWE Principles of Cardiac Care ECG workshop case study1 44 Year old male. Reports SOB, Lethargy, tiredness. PMH: Hypertension, nil else. What tests? What treatment?
ECG Workshop Carolyn Shepherd And Anya Horne UWE Principles of Cardiac Care ECG workshop case study1 44 Year old male. Reports SOB, Lethargy, tiredness. PMH: Hypertension, nil else. What tests? What treatment?
How do arrhythmias occur?
 How do arrhythmias occur? An arrhythmia is an abnormal heart rhythm (= dysrhythmia). Can be fast (tachy) or slow (brady). Brady arrhythmias are usually due to conduc;on block, while tachyarrhythmias are
How do arrhythmias occur? An arrhythmia is an abnormal heart rhythm (= dysrhythmia). Can be fast (tachy) or slow (brady). Brady arrhythmias are usually due to conduc;on block, while tachyarrhythmias are
ANTI-ARRHYTHMICS AND WARFARIN. Dr Nithish Jayakumar
 ANTI-ARRHYTHMICS AND WARFARIN Dr Nithish Jayakumar Contents 1. Anti-arrhythmics Pacemaker and myocardial potentials Drug classes mechanisms; s/e; contra-indications Management of common arrhythmias 2.
ANTI-ARRHYTHMICS AND WARFARIN Dr Nithish Jayakumar Contents 1. Anti-arrhythmics Pacemaker and myocardial potentials Drug classes mechanisms; s/e; contra-indications Management of common arrhythmias 2.
Etienne Aliot. University of Nancy - France
 Etienne Aliot University of Nancy - France Disclosures Consulting fees : - Bayer, Boehringer Ingelheim,GSK, MedaPharma, Pfizer/BMS,Sanofi Aventis. - Biotronik,Medtronic,St Jude Medical. Electrical vs Pharmacological
Etienne Aliot University of Nancy - France Disclosures Consulting fees : - Bayer, Boehringer Ingelheim,GSK, MedaPharma, Pfizer/BMS,Sanofi Aventis. - Biotronik,Medtronic,St Jude Medical. Electrical vs Pharmacological
Clinical Problem. Management. Discussion
 Optimum management of atrial fibrillation in the Intensive Care Unit Clinical Problem A 61 year old man, PD, presented to the Intensive Care Unit (ICU) after angiography and intra arterial thrombolysis
Optimum management of atrial fibrillation in the Intensive Care Unit Clinical Problem A 61 year old man, PD, presented to the Intensive Care Unit (ICU) after angiography and intra arterial thrombolysis
Arrhythmias (II) Ventricular Arrhythmias. Disclosures
 Ventricular Arrhythmias. Disclosures") Arrhythmias (II) Ventricular Arrhythmias Amy Leigh Miller, MD, PhD Cardiovascular Electrophysiology, Brigham & Women s Hospital Disclosures None Rhythms and Mortality Implantable loop recorder post-mi
Arrhythmias (II) Ventricular Arrhythmias Amy Leigh Miller, MD, PhD Cardiovascular Electrophysiology, Brigham & Women s Hospital Disclosures None Rhythms and Mortality Implantable loop recorder post-mi
AF in the ER: Common Scenarios CASE 1. Fast facts. Diagnosis. Management
 AF in the ER: Common Scenarios Atrial fibrillation is a common problem with a wide spectrum of presentations. Below are five common emergency room scenarios and the management strategies for each. Evan
AF in the ER: Common Scenarios Atrial fibrillation is a common problem with a wide spectrum of presentations. Below are five common emergency room scenarios and the management strategies for each. Evan
Episode 112 Tachydysrhythmias
 Wide & regular tachydysrhythmias Ventricular Tachycardia (VT) vs SVT with aberrancy: Assume VT Episode 112 Tachydysrhythmias With Amal Mattu & Paul Dorion Prepared by Shaun Mehta, July 2018 General Approach
Wide & regular tachydysrhythmias Ventricular Tachycardia (VT) vs SVT with aberrancy: Assume VT Episode 112 Tachydysrhythmias With Amal Mattu & Paul Dorion Prepared by Shaun Mehta, July 2018 General Approach
TACHYARRHYTHMIAs. Pawel Balsam, MD, PhD
 TACHYARRHYTHMIAs Pawel Balsam, MD, PhD SupraVentricular Tachycardia Atrial Extra Systole Sinus Tachycardia Focal A. Tachycardia AVRT AVNRT Atrial Flutter Atrial Fibrillation Ventricular Tachycardia Ventricular
TACHYARRHYTHMIAs Pawel Balsam, MD, PhD SupraVentricular Tachycardia Atrial Extra Systole Sinus Tachycardia Focal A. Tachycardia AVRT AVNRT Atrial Flutter Atrial Fibrillation Ventricular Tachycardia Ventricular
ARRHYTHMIA SINUS RHYTHM
 ARRHYTHMIA Dr. Ahmed A. Elberry, MBBCH, MSc, MD Assistant Professor of Clinical Pharmacy Faculty of pharmacy, KAU 1 SINUS RHYTHM SA node is cardiac pacemaker Normal sinus rhythm 60-100 beats/min Depolarisation
ARRHYTHMIA Dr. Ahmed A. Elberry, MBBCH, MSc, MD Assistant Professor of Clinical Pharmacy Faculty of pharmacy, KAU 1 SINUS RHYTHM SA node is cardiac pacemaker Normal sinus rhythm 60-100 beats/min Depolarisation
Atrial Fibrillation and Common Supraventricular Tachycardias. Sunil Kapur MD
 Atrial Fibrillation and Common Supraventricular Tachycardias Sunil Kapur MD Cardiac Electrophysiology Brigham and Women s Hospital Instructor, Harvard Medical School No disclosures Cardiac Conduction:
Atrial Fibrillation and Common Supraventricular Tachycardias Sunil Kapur MD Cardiac Electrophysiology Brigham and Women s Hospital Instructor, Harvard Medical School No disclosures Cardiac Conduction:
Antidysrhythmics HST-151 1
 HST-151 1 Antidysrhythmics I. Ventricular muscle cell action potential a. Phase 0: Upstroke b. Phase 1: Early-fast repolarization c. Phase 2: Plateau d. Phase 3: Repolarization e. Phase 4: Diastole HST-151
HST-151 1 Antidysrhythmics I. Ventricular muscle cell action potential a. Phase 0: Upstroke b. Phase 1: Early-fast repolarization c. Phase 2: Plateau d. Phase 3: Repolarization e. Phase 4: Diastole HST-151