Replacement of the Ascending Aorta, Aortic Root and Valve with a Novel Stentless
|
|
|
- Felix Sims
- 6 years ago
- Views:
Transcription
1 Title: Replacement of the Ascending Aorta, Aortic Root and Valve with a Novel Stentless Valved-Conduit Running Head: Replacement of Ascending Aorta and Valve Authors: Kelvin K.W. Lau MRCS DPhil Krystyna Bochenek-Klimczyk MD Manuel Galiñanes MD, PhD, FRCS Andrzej W. Sosnowski FRCS Institution and Affiliations: Cardiac Surgery Unit, Cardiovascular Sciences Department, Glenfield Hospital, University of Leicester, Groby Road, Leicester, LE3 9QP UK (all authors) Keywords: Aorta; Aortic valve, replacement; aortic root; aortic operation; Valve disease Word Count: 2379 Corresponding author: Manuel Galiñanes, Cardiac Surgery Unit, Cardiovascular Sciences Department, Glenfield Hospital, University of Leicester, Groby Road, Leicester, LE3 9QP, United Kingdom 1
2 Tel: Fax
3 Abstract: Purpose Biological valved-conduit grafts avoid the need for anticoagulation, and can exploit the excellent hemodynamic performance of stentless valves. Incorporation of sinuses of Valsalva into the neoaortic root can improve the function of the stentless valves. Description Here we present a novel prefabricated stentless valved-conduit incorporating sinuses of Valsalva and describe the technique of inplantation. The BioValsalva valvedconduit incorporates a stentless porcine aortic valve (Vascutek Elan ) suspended within a triple-layered vascular conduit (Triplex, Vascutek, Renfrewshire, Scotland) constructed with sinuses of Valsalva. Evaluation The BioValsalva valve-conduit was used in twelve patients with aortic regurgitation due to annuloaortic ectasia unsuitable for aortic valve repair and concomitant ascending aorta aneurysm with no mortality and excellent functioned result. Conclusion The prefabricated, composite stentless-valved-conduit, which material is hemostatic and reduces bleeding, is easy to implant with short ischemic time, and lends itself well to a variety of insertion techniques. 3
4 Introduction: The replacement of the aortic root, ascending aorta and aortic valve with a valvedconduit is a well-established procedure for the treatment of ascending aorta aneurysms and aortic dissection. However, this operation is still associated with high perioperative mortality and morbidity. The nature of the prosthetic material used may play a role in these complications. Knitted vascular conduits did not have favourable handling properties and hemostasis was suboptimal, contributing to mediastinal bleeding, a life-threatening complication. To overcome this problem, woven prostheses with zero-porosity were developed. The use of a xenograft root, which if necessary could be extended distally with a vascular graft, has also been proposed (1). However, the xenograft aortic wall is prone to calcification. If reoperation were required, then replacement of the entire xenograft root would be necessary, compounding the risk of surgery (2). The use of a mechanical valve in a composite graft requires long-term anticoagulation and is a disadvantage especially in elderly patients, in patients unsuitable for anticoagulation, and in patients with extended aortic pathologies, such as aortic dissection and thoracoabdominal aortic aneurysms. Composite valved-conduits using mechanical and bioprosthetic prostheses have traditionally been designed as straight tubes without incorporating the sinuses of Valsalva. The physiological importance of the sinuses is beginning to be recognised. Vortices which form at this site improve blood flow to the coronary arteries and promote earlier and more gradual valve leaflet closure, thus reducing stress of the leaflet coaptation (3). Furthermore, in the absence of the sinuses, there is a theoretical risk of collision of the valve leaflets with the vascular graft resulting in abrasive wear. Therefore, the ideal composite valved-conduit used for replacement of the aortic 4
5 valve, aortic root and ascending aorta should possess the following characteristics: (i) sinuses mimicking the anatomy of the aortic root, (ii) a synthetic conduit material which should be both hemostatic and easy to handle, whilst resistant to calcification and deterioration with time, and (iii) a valve which does not require anticoagulation, has good hemodynamics and is durable. Here we report on a new bioprosthetic valved-conduit BioValsalva (Vascutek Terumo, UK) which consists of a stentless bioprosthesis, the Elan valve that has been shown to afford excellent hemodynamics with performance (4), within a polyester and polytetrafluoroethylene (PTFE) triplelayered conduit which is hemostatic, has favourable handling properties and incorporates sinuses of Valsalva (Figure 1). Technology The BioValsalva prosthesis consists of a stentless porcine valve (Vascutek Elan ) pre-implanted within a longitudinally-corrugated Triplex vascular graft incorporating sinuses of Valsalva. The selected porcine valves were predilated and preserved with low-pressure fixation in 0.5% buffered glutaraldehyde. They did not receive anti-mineralisation treatment. Only two sizes of the prosthesis were used (26 and 28mm for the conduit and 25 and 27mm respectively for the valve). The diameters of the sinus of Valsalva for these conduits are 32mm and 35mm respectively. As discussed below, different implantation techniques can be used to accommodate one of these two prostheses sizes into a wide range of aortic anatomy. 5
6 Surgical technique The operation was performed through a median sternotomy. Transesophageal echocardiogram (TOE) was performed in all patients prior to and following separation from CPB. Standard CPB was established between the right atrium and aortic arch with moderate hypothermia (28ºC), or deep hypothermia (17ºC) if circulatory arrest was required. A modified Bentall technique with complete resection of the ascending aorta and aortic valve, and reimplantation of the coronary buttons was used in all patients. The sewing ring of the BioValsalva composite conduit was anastomosed to the aortic annulus using a variety of techniques depending on the aortic anatomy. When the tissue was healthy, continuous and semi-continuous sutures were used, with or without pledget reinforcement. When the tissue quality was poor and the annulus calcified, interrupted mattress sutures were used. Interrupted mattress sutures were also used when a small aortic annulus was encountered, allowing the implantation of a larger root into the supraannular position; whilst everted mattress sutures reinforced with continuous sutures were used when there was a large annulus, to allow a smaller root to be implanted in the intraannular position. The vascular graft was fenestrated with a punch (5.6 mm) and the coronary buttons were anastomosed to the BioValsalva graft using 5/0 Surgipro (Syneture, USA). Following completion of the coronary anastomoses, the tube graft was cut to length and an end-to-end anastomosis to the distal ascending aorta was fashioned using a continuous 3/0 Prolene (Ethicon, USA) suture reinforced with Teflon felt and tissue glue (Glubran, GEM, Viareggio, Italy). 6
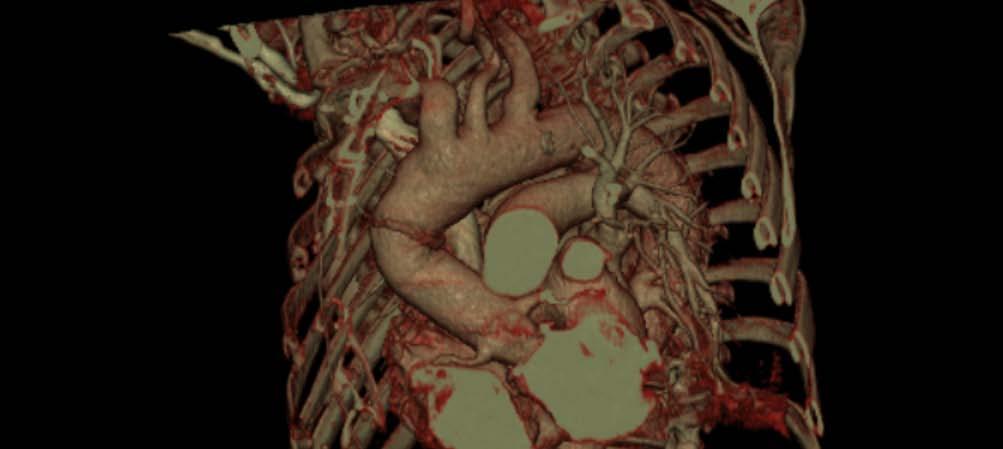
7 Patients with aneurysms extending distally underwent further ascending aorta and arch replacement with a 28mm Dacron conduit. The distal anastomosis was performed under circulatory arrest with a tube-graft inversion technique as described previously (5). Clinical Experience Between December 2006 and June 2007, 12 BioValsalva prostheses were implanted electively in 12 patients (9 males, 3 females) with annuloaortic ectasia and aortic regurgitation resulting from degenerative valve disease unsuitable for repair. The procedure was thoroughly explained and informed consent was obtained for all patients in accordance with the General Medical Council (UK) guidelines. The regional ethics committee has confirmed that ethical approval is not required under the NHS research governance guidelines. The mean CPB time was 145±28 minutes, and the mean aortic cross-clamp time was 95±21 minutes mean ± standard error of the mean). Deep hypothermic circulatory arrest (20-22 minutes) was used in three cases for distal ascending aorta and arch replacement with a 28mm Dacron conduit. There were no in-hospital deaths or reoperations for bleeding or tamponade. All patients underwent post-operative CT of aorta and echocardiography prior to discharge. Figure 2 is a representative axial CT section and Figure 3 shows the valved-conduit in a CT reconstruction. These confirm the presence of three distinct sinuses of Valsalva. The mean peak-gradient of the aortic valve prostheses was 18±6mmHg. The mean effective orifice area (EOA) ± standard error of the mean was and cm 2 for the 25 and 27mm prostheses, respectively. In all cases the 7
8 valve prostheses were functioning well with no evidence of regurgitation. Hematoma was noticed around the ascending aorta in 4 patients. In addition, one patient underwent MRI of the aorta. This latter investigation could not demonstrate obvious dynamic movements of the sinuses of Valsalva during the cardiac cycle, however this important issue should be addressed in future studies in a larger group of patients. Comments: We have shown here that the BioValsalva prosthesis, a novel valved-conduit, can be safely used with short aortic cross-clamp times and good hemostatic properties. We have also shown that the prosthesis is versatile, allowing the use of a variety of surgical techniques to accommodate specific anatomical findings. The availability of such a valve-conduit may have important implications for improving the surgical outcome of the correction of the aortic valve, aortic root and ascending aorta pathology. The Bentall procedure is the gold standard for repair of ascending aortic aneurysms and aortic regurgitation. Universal use of mechanical valves is limited by their need for anticoagulation and suboptimal hemodynamics. With improved durability of bioprosthetic valves coupled with their excellent hemodynamic profile, several groups have modified the Bentall procedure to incorporate stentless aortic valves (1, 6, 7). These were constructed intraoperatively following sizing of the annulus. Intraoperative construction requires an extended cross-clamp time. In addition, imperfectly placed sutures can result in distortion of the valve which might only be identified by TOE upon discontinuation of CPB (8). The new prefabricated BioValsalva valved-conduit eliminates the ischemic time required for the 8
9 construction of the valved-conduit construction during surgery and the risk of valve malfunction. Our results show a mean ischemic time of 95 minutes, which compares favourably to other series of Bentall operations (8). Composite grafts constructed from the first-generation Toronto SPV valve within a Dacron tube have been shown to have good hemodynamic performance accompanied by good medium-term clinical outcomes (3, 7). The BioValsalva prosthesis utilises an Elan stentless aortic valve that has also been shown to possess excellent hemodynamic performance and clinical results (4, 9). Bleeding is a significant morbidity associated with the Bentall procedure, and can result in the need for reoperation in over 10% in some series. Earlier ascending aorta replacements were complicated by bleeding from needle holes and anastamotic lines. The BioValsalva prosthesis contains a Triplex vascular graft, with an inner woven polyester layer and an outer PTFE layer. The superior hemostatic properties of this conduit can be seen where the valved-conduit was anastomosed to a distal conduit in repairs involving the aortic arch: notably, there was bleeding from the Dacron graft suture holes and not in the valved-conduit. In our series, there were no reoperations and little mediastinal drainage. An added benefit with this vascular graft material is the ease of fenestration with an aortic punch, avoiding the imprecise perforation with electrocautery. Nevertheless, care must be taken to ensure that the valve leaflets are not damaged by the punch because surface tension can draw the leaflets onto the conduit wall. Unlike mechanical valves, optimal functioning of biological valves is affected by the anatomy of the aortic root. The sinuses of Valsalva in particular, may play a role in 9
10 enhancing durability of the valves. The presence of the sinuses theoretically reduces the impact of the valve leaflets on the conduit during valve opening, and on each other during valve closure, and may improve blood flow in the coronary arteries (3). Another major advantage of the BioValsalva valved-conduit is the relative ease for explantation if a reoperation is needed as the valve is not incorporated into the suture line of the prosthesis to the aortic annulus. Early bioprosthetic valved-conduits were sutured in such a way that both the valve and the vascular graft were incorporated into the anastomosis (6) and in this case full explantation of the valved-conduit is necessary when valve replacement is required. Compared to homograft and xenograft roots, the polyester vascular prosthesis is relatively resistant to calcification and dilation, and would not require replacement. Therefore reoperation could be achieved through entering the graft and excising the stentless valve. A new stentless or stented valve could then be reimplanted into a suitable position. In conclusion, the BioValsalva bioprosthetic valved-conduit belongs to a new generation of prefabricated bioprosthetic valved-conduits with excellent hemodynamic profiles and hemostatic properties incorporating sinuses of Valsalva. Our series showed that this versatile valved-conduit could be implanted easily and safely using a wide range of techniques, for the replacement of the aortic valve, aortic root and ascending aorta, with good short term clinical outcomes. 10
11 Acknowledgements: No financial support or technical assistance was received for the study. However, Vascutek, Ltd contributed to the cost of publication of the color figures. Disclosure and Freedom of Investigation: BioValsalva valved-conduits were supplied at full cost to our department. The authors had full control in the patient selection, operative technique, study design, data analysis and preparation of the article. As mentioned in the acknowledgments, financial support was obtained for the publication of color figures from Vascutek, Ltd. 11
12 References: 1 Byrne JG, Mihaljevic T, Lipson WE, Smith B, Fox JA, Aranki SF. Composite stentless valve with graft extension for combined replacement of the aortic valve, root and ascending aorta. Eur J Cardiothorac Surg 2001;20: Dossche KM, Schepens MA, Morshuis WJ, de la Riviere AB, Knaepen PJ, Vermeulen FE. A 23-year experience with composite valve graft replacement of the aortic root. Ann Thorac Surg 1999;67: de Paulis R, Tomai F, Bertoldo F et al. Coronary flow characteristics after a Bentall procedure with or without sinuses of Valsalva. Eur J Cardiothorac Surg 2004;26: Flynn M, Iaccovoni A, Pathi V, Butler J, Macarthur KJ, Berg GA. The aortic Elan stentless aortic valve: excellent hemodynamics and ease of implantation. Semin Thorac Cardiovasc Surg 2001;13: Alexiou C, Sosnowski AW. Tube-graft inversion for the construction of an "open" distal anastomosis during ascending aortic replacement: a new technique. Ann Thorac Surg 2007;83: Urbanski PP. New vascular graft for assembling the stentless valve composite graft. Ann Thorac Surg 2007;84:
13 7 de Paulis R, Nardi P, De Matteis GM, Polisca P, Chiariello L. Bentall procedure with a stentless valve and a new aortic root prosthesis. Ann Thorac Surg 2001;71: Urbanski PP, Diegeler A, Siebel A, Zacher M, Hacker RW. Valved stentless composite graft: clinical outcomes and hemodynamic characteristics. Ann Thorac Surg 2003;75: Akar AR, Szafranek A, Alexiou C, et al. Use of stentless xenografts in the aortic position: determinants of early and late outcome. Ann Thorac Surg 2002;74: Galla JD, Lansman SL, Spielvogel D et al. Bioprosthetic valved conduit aortic root reconstruction: the Mount Sinai experience. Ann Thorac Surg 2002;74:S
14 Legends Figure 1: BioValsalva valved-conduit Figure 2: CT aorta after implantation of the BioValsalva valved-conduit demonstrating the origin of the coronary arteries (arrows) and the three sinuses of Valsalva (*) following implantation. Figure 3: CT reconstruction of the aorta following implantation of the BioValsalva valved-conduit. 14

15

16
17
The increasing number of elderly patients with complex
 Valved Stentless Composite Graft: Clinical Outcomes and Hemodynamic Characteristics Paul P. Urbanski, MD, Anno Diegeler, MD, Alexander Siebel, MD, Michael Zacher, MD, and Robert W. Hacker, MD Herz- und
Valved Stentless Composite Graft: Clinical Outcomes and Hemodynamic Characteristics Paul P. Urbanski, MD, Anno Diegeler, MD, Alexander Siebel, MD, Michael Zacher, MD, and Robert W. Hacker, MD Herz- und
Composite stentless valve with graft extension for combined replacement of the aortic valve, root and ascending aorta
 European Journal of Cardio-thoracic Surgery 20 (2001) 252±256 www.elsevier.com/locate/ejcts Composite stentless valve with graft extension for combined replacement of the aortic valve, root and ascending
European Journal of Cardio-thoracic Surgery 20 (2001) 252±256 www.elsevier.com/locate/ejcts Composite stentless valve with graft extension for combined replacement of the aortic valve, root and ascending
Valve-sparing versus composite root replacement procedures in patients with Marfan syndrome
 Masters of Cardiothoracic Surgery Valve-sparing versus composite root replacement procedures in patients with Marfan syndrome Joseph S. Coselli 1,2,3, Scott A. Weldon 1,4, Ourania Preventza 1,2,3, Kim
Masters of Cardiothoracic Surgery Valve-sparing versus composite root replacement procedures in patients with Marfan syndrome Joseph S. Coselli 1,2,3, Scott A. Weldon 1,4, Ourania Preventza 1,2,3, Kim
Disease of the aortic valve is frequently associated with
 Stentless Aortic Bioprosthesis for Disease of the Aortic Valve, Root and Ascending Aorta John R. Doty, MD, and Donald B. Doty, MD Disease of the aortic valve is frequently associated with morphologic abnormalities
Stentless Aortic Bioprosthesis for Disease of the Aortic Valve, Root and Ascending Aorta John R. Doty, MD, and Donald B. Doty, MD Disease of the aortic valve is frequently associated with morphologic abnormalities
How to Perform a Valve Sparing Root Replacement Joseph S. Coselli, M.D.
 How to Perform a Valve Sparing Root Replacement Joseph S. Coselli, M.D. AATS International Cardiovascular Symposium 2017 Session 6: Technical Aspects of Open Surgery on the Aortic Valve Sao Paulo, Brazil
How to Perform a Valve Sparing Root Replacement Joseph S. Coselli, M.D. AATS International Cardiovascular Symposium 2017 Session 6: Technical Aspects of Open Surgery on the Aortic Valve Sao Paulo, Brazil
Gelweave TM. Thoracic and Thoracoabdominal Graft Geometries. Ante-Flo TM 4 Branch Plexus. Siena Valsalva TM Trifurcate Arch Graft. Coselli.
 Gelweave TM Thoracic and Thoracoabdominal Graft Geometries Ante-Flo TM 4 Branch Plexus Siena Valsalva TM Trifurcate Arch Graft Coselli Lupiae Product availability subject to local regulatory approval.
Gelweave TM Thoracic and Thoracoabdominal Graft Geometries Ante-Flo TM 4 Branch Plexus Siena Valsalva TM Trifurcate Arch Graft Coselli Lupiae Product availability subject to local regulatory approval.
Management of Difficult Aortic Root, Old and New solutions
 Management of Difficult Aortic Root, Old and New solutions Hani K. Najm MD, Msc, FRCSC,, FACC, FESC Chairman, Pediatric and Congenital Heart Surgery Cleveland Clinic Conflict of Interest None Difficult
Management of Difficult Aortic Root, Old and New solutions Hani K. Najm MD, Msc, FRCSC,, FACC, FESC Chairman, Pediatric and Congenital Heart Surgery Cleveland Clinic Conflict of Interest None Difficult
Publicado : Interactive CardioVascular Thoracic Surgery 2011;12:650.
 Pulmonary embolism due to biological glue after repair of type A aortic dissection Jose Rubio Alvarez,MD, PhD, 1 Juan Sierra Quiroga, MD, PhD, 1 Anxo Martinez de Alegria MD 2, Jose-Manuel Martinez Comendador,
Pulmonary embolism due to biological glue after repair of type A aortic dissection Jose Rubio Alvarez,MD, PhD, 1 Juan Sierra Quiroga, MD, PhD, 1 Anxo Martinez de Alegria MD 2, Jose-Manuel Martinez Comendador,
Techniques to preserve the native aortic valve during aortic
 Valve-Sparing Aortic Root Replacement with the Valsalva Graft Duke Cameron, MD, and Luca Vricella, MD Techniques to preserve the native aortic valve during aortic root replacement have evolved considerably
Valve-Sparing Aortic Root Replacement with the Valsalva Graft Duke Cameron, MD, and Luca Vricella, MD Techniques to preserve the native aortic valve during aortic root replacement have evolved considerably
AORTIC ROOT RECONSTRUCTION WITH PRESERVATION OF NATIVE AORTIC VALVE AND SINUSES IN AORTIC ROOT DILATATION WITH AORTIC REGURGITATION
 AORTIC ROOT RECONSTRUCTION WITH PRESERVATION OF NATIVE AORTIC VALVE AND SINUSES IN AORTIC ROOT DILATATION WITH AORTIC REGURGITATION Jacques A. M. van Son, MD, PhD Roberto Battellini, MD Marco Mierzwa,
AORTIC ROOT RECONSTRUCTION WITH PRESERVATION OF NATIVE AORTIC VALVE AND SINUSES IN AORTIC ROOT DILATATION WITH AORTIC REGURGITATION Jacques A. M. van Son, MD, PhD Roberto Battellini, MD Marco Mierzwa,
The stentless bioprosthesis has many salient features that
 Aortic Valve Replacement with the Medtronic Freestyle Xenograft Using the Subcoronary Implantation Technique D. Michael Deeb, MD The stentless bioprosthesis has many salient features that make it an attractive
Aortic Valve Replacement with the Medtronic Freestyle Xenograft Using the Subcoronary Implantation Technique D. Michael Deeb, MD The stentless bioprosthesis has many salient features that make it an attractive
Early and Midterm Outcomes of the VSSR procedure with De Paulis valsalva graft: A Chinese single-center Experience in 38 patients
 Xu et al. Journal of Cardiothoracic Surgery (2015) 10:167 DOI 10.1186/s13019-015-0347-1 RESEARCH ARTICLE Open Access Early and Midterm Outcomes of the VSSR procedure with De Paulis valsalva graft: A Chinese
Xu et al. Journal of Cardiothoracic Surgery (2015) 10:167 DOI 10.1186/s13019-015-0347-1 RESEARCH ARTICLE Open Access Early and Midterm Outcomes of the VSSR procedure with De Paulis valsalva graft: A Chinese
14 Valvular Stenosis
 14 Valvular Stenosis 14-1. Valvular Stenosis unicuspid valve FIGUE 14-1. This photograph shows severe valvular stenosis as it occurs in a newborn. There is a unicuspid, horseshoe-shaped leaflet with a
14 Valvular Stenosis 14-1. Valvular Stenosis unicuspid valve FIGUE 14-1. This photograph shows severe valvular stenosis as it occurs in a newborn. There is a unicuspid, horseshoe-shaped leaflet with a
Hemodynamics Benefit of Supra-Annular Design in Failed Bio-Prosthetic Valves
 Hemodynamics Benefit of Supra-Annular Design in Failed Bio-Prosthetic Valves Speaker's name: I have the following potential conflicts of interest to report: Proctorship for Medtronic Agenda Failure modes
Hemodynamics Benefit of Supra-Annular Design in Failed Bio-Prosthetic Valves Speaker's name: I have the following potential conflicts of interest to report: Proctorship for Medtronic Agenda Failure modes
A Loeys-Dietz Patient with a Trans-Atlantic Odyssey. Repeated Aortic Root Surgery ending with a Huge Left Main Coronary Aneurysm 4
 1 2 3 A Loeys-Dietz Patient with a Trans-Atlantic Odyssey Repeated Aortic Root Surgery ending with a Huge Left Main Coronary Aneurysm 4 5 6 7 8 9 Thierry Carrel 1, Florian Schoenhoff 1 and Duke Cameron
1 2 3 A Loeys-Dietz Patient with a Trans-Atlantic Odyssey Repeated Aortic Root Surgery ending with a Huge Left Main Coronary Aneurysm 4 5 6 7 8 9 Thierry Carrel 1, Florian Schoenhoff 1 and Duke Cameron
Indications and Late Results of Aortic Valve Repair
 Indications and Late Results of Aortic Valve Repair Prof. Gebrine El Khoury Department of Cardiovascular and Thoracic Surgery Cliniques St. Luc Brussels, Belgium Aortic Valve Repair Question # 1 Can the
Indications and Late Results of Aortic Valve Repair Prof. Gebrine El Khoury Department of Cardiovascular and Thoracic Surgery Cliniques St. Luc Brussels, Belgium Aortic Valve Repair Question # 1 Can the
Aortic valve repair: When and how to employ this novel approach?
 Aortic valve repair: When and how to employ this novel approach? Konstadinos A Plestis, MD System Chief of Cardiac Thoracic and Vascular Surgery Main Line Health Care System Professor Sidney Kimmel Medical
Aortic valve repair: When and how to employ this novel approach? Konstadinos A Plestis, MD System Chief of Cardiac Thoracic and Vascular Surgery Main Line Health Care System Professor Sidney Kimmel Medical
To reduce the morbidity and mortality associated with
 Cardiac Surgery Aortic Arch Replacement/ Selective Antegrade Perfusion David Spielvogel, MD*, Steven L. Lansman, MD, PhD, and Randall B. Griepp, MD To reduce the morbidity and mortality associated with
Cardiac Surgery Aortic Arch Replacement/ Selective Antegrade Perfusion David Spielvogel, MD*, Steven L. Lansman, MD, PhD, and Randall B. Griepp, MD To reduce the morbidity and mortality associated with
Operative Strategy. Operative Technique
 Domingo Liotta, M.D.; Christian Cabrol, M.D; Miguel del Rio, M.D; Armando Diluch, M.D; Adriano Malusardi, M.D. Figure 11 Acute dissected aortic root and ascending aorta with valvular regurgitation. -Replacement
Domingo Liotta, M.D.; Christian Cabrol, M.D; Miguel del Rio, M.D; Armando Diluch, M.D; Adriano Malusardi, M.D. Figure 11 Acute dissected aortic root and ascending aorta with valvular regurgitation. -Replacement
Acute type A aortic dissection (Type I, proximal, ascending)
") Acute Type A Aortic Dissection R. Morton Bolman, III, MD Acute type A aortic dissection (Type I, proximal, ascending) is a true surgical emergency. It is estimated that patients suffering this calamity
Acute Type A Aortic Dissection R. Morton Bolman, III, MD Acute type A aortic dissection (Type I, proximal, ascending) is a true surgical emergency. It is estimated that patients suffering this calamity
Ascending Thoracic Aorta: Postsurgical CT Evaluation
 Ascending Thoracic Aorta: Postsurgical CT Evaluation Santiago Martinez Jimenez, MD GOALS Ascending Thoracic Aorta: Postsurgical CT Evaluation Santiago Martínez MD smartinez-jimenez@saint-lukes.org Saint
Ascending Thoracic Aorta: Postsurgical CT Evaluation Santiago Martinez Jimenez, MD GOALS Ascending Thoracic Aorta: Postsurgical CT Evaluation Santiago Martínez MD smartinez-jimenez@saint-lukes.org Saint
TAVR for Valve-In-Valve. Brian O Neill Assistant Professor of Medicine Department of Medicine, Section of Cardiology
 TAVR for Valve-In-Valve Brian O Neill Assistant Professor of Medicine Department of Medicine, Section of Cardiology Temple Hearth and Vascular Institute Disclosures: Consultant: Cardiac Assist TAVR for
TAVR for Valve-In-Valve Brian O Neill Assistant Professor of Medicine Department of Medicine, Section of Cardiology Temple Hearth and Vascular Institute Disclosures: Consultant: Cardiac Assist TAVR for
Aortic valve repair: Techniques and Pitfalls. Allan Stewart, MD Columbia University Medical Center New York, NY
 Aortic valve repair: Techniques and Pitfalls Allan Stewart, MD Columbia University Medical Center New York, NY Take Away Points 1. Valve anatomy is essential to assess repair 2. Unique Decisions with Aneurysm/AI
Aortic valve repair: Techniques and Pitfalls Allan Stewart, MD Columbia University Medical Center New York, NY Take Away Points 1. Valve anatomy is essential to assess repair 2. Unique Decisions with Aneurysm/AI
CT Appearance of Thoracic Aortic Graft Complications
 CT of ortic Graft Complications Cardiopulmonary Imaging Clinical Observations Baskaran Sundaram 1 Leslie Eisenbud Quint 1 Smita Patel 1 Himanshu J. Patel 2 G. Michael Deeb 2 Sundaram B, Quint LE, Patel
CT of ortic Graft Complications Cardiopulmonary Imaging Clinical Observations Baskaran Sundaram 1 Leslie Eisenbud Quint 1 Smita Patel 1 Himanshu J. Patel 2 G. Michael Deeb 2 Sundaram B, Quint LE, Patel
Surgery for Acquired Cardiovascular Disease ACD
 Surgery for Acquired Cardiovascular Disease Clinical outcomes after separate and composite replacement of the aortic valve and ascending aorta Thanos Sioris, MD Tirone E. David, MD Joan Ivanov, PhD Susan
Surgery for Acquired Cardiovascular Disease Clinical outcomes after separate and composite replacement of the aortic valve and ascending aorta Thanos Sioris, MD Tirone E. David, MD Joan Ivanov, PhD Susan
Case. 15-year-old boy with bicuspid AV Severe AR with moderate AS. Ross vs. AVR (or AVP)
") Case 15-year-old boy with bicuspid AV Severe AR with moderate AS Ross vs. AVR (or AVP) AMC case 14-year-old boy with bicuspid AV Severe AS with mild AR Body size Bwt: 55 kg, Ht: 154 cm, BSA: 1.53 m 2 Echocardiography
Case 15-year-old boy with bicuspid AV Severe AR with moderate AS Ross vs. AVR (or AVP) AMC case 14-year-old boy with bicuspid AV Severe AS with mild AR Body size Bwt: 55 kg, Ht: 154 cm, BSA: 1.53 m 2 Echocardiography
Bicuspid aortic root spared during ascending aorta surgery: an update of long-term results
 Short Communication Bicuspid aortic root spared during ascending aorta surgery: an update of long-term results Marco Russo, Guglielmo Saitto, Paolo Nardi, Fabio Bertoldo, Carlo Bassano, Antonio Scafuri,
Short Communication Bicuspid aortic root spared during ascending aorta surgery: an update of long-term results Marco Russo, Guglielmo Saitto, Paolo Nardi, Fabio Bertoldo, Carlo Bassano, Antonio Scafuri,
Transcatheter Pulmonary Valve Replacement Update on progress and outcomes
 Transcatheter Pulmonary Valve Replacement Update on progress and outcomes Barry Love, MD Director, Congenital Cardiac Catheterization Laboratory Mount Sinai Medical Center New York, New York Transcatheter
Transcatheter Pulmonary Valve Replacement Update on progress and outcomes Barry Love, MD Director, Congenital Cardiac Catheterization Laboratory Mount Sinai Medical Center New York, New York Transcatheter
Management of Acute Aortic Syndromes. M. Grabenwoger, MD Dept. of Cardiovascular Surgery Hospital Hietzing, Vienna, Austria
 Management of Acute Aortic Syndromes M. Grabenwoger, MD Dept. of Cardiovascular Surgery Hospital Hietzing, Vienna, Austria I have nothing to disclose. Acute Aortic Syndromes Acute Aortic Dissection Type
Management of Acute Aortic Syndromes M. Grabenwoger, MD Dept. of Cardiovascular Surgery Hospital Hietzing, Vienna, Austria I have nothing to disclose. Acute Aortic Syndromes Acute Aortic Dissection Type
The application of autologous pulmonary artery in surgical correction of complicated aortic arch anomaly
 Original Article The application of autologous pulmonary artery in surgical correction of complicated aortic arch anomaly Shusheng Wen, Jianzheng Cen, Jimei Chen, Gang Xu, Biaochuan He, Yun Teng, Jian
Original Article The application of autologous pulmonary artery in surgical correction of complicated aortic arch anomaly Shusheng Wen, Jianzheng Cen, Jimei Chen, Gang Xu, Biaochuan He, Yun Teng, Jian
CoreValve in a Degenerative Surgical Valve
 CoreValve in a Degenerative Surgical Valve Ran Kornowski, MD, FESC, FACC Chairman Department of Cardiology Rabin Medical Center, Petach Tikva, Israel Disclosure Statement of Financial Interest I, Ran Kornowski,
CoreValve in a Degenerative Surgical Valve Ran Kornowski, MD, FESC, FACC Chairman Department of Cardiology Rabin Medical Center, Petach Tikva, Israel Disclosure Statement of Financial Interest I, Ran Kornowski,
Valve-sparing aortic root replacement (VSRR) at the Johns
 at the Johns") Valve-Sparing Aortic Root Replacement With the Valsalva Graft Duke Cameron, MD, and Luca Vricella, MD Division of Cardiac Surgery, The Johns Hopkins Hospital, Baltimore, Maryland. Address reprint requests
Valve-Sparing Aortic Root Replacement With the Valsalva Graft Duke Cameron, MD, and Luca Vricella, MD Division of Cardiac Surgery, The Johns Hopkins Hospital, Baltimore, Maryland. Address reprint requests
Management of Fusiform Ascending Aortic Aneurysms
 Management of Fusiform Ascending Aortic Aneurysms Stuart Houser, M.D., Jose Mijangos, M.D., Amarenda Sengupta, M.D., Lawrence Zaroff, M.D., Robert Weiner, M.D., and James A. DeWeese, M.D. ABSTRACT Thirteen
Management of Fusiform Ascending Aortic Aneurysms Stuart Houser, M.D., Jose Mijangos, M.D., Amarenda Sengupta, M.D., Lawrence Zaroff, M.D., Robert Weiner, M.D., and James A. DeWeese, M.D. ABSTRACT Thirteen
Aortic Root Replacement With the Carboseal Composite Graft: 7-Year Experience With the First 100 Implants
 Aortic Root Replacement With the Carboseal Composite Graft: 7-Year Experience With the First 100 Implants Giovanni Battista Luciani, MD, Gianluca Casali, MD, Luca Barozzi, MD, and Alessandro Mazzucco,
Aortic Root Replacement With the Carboseal Composite Graft: 7-Year Experience With the First 100 Implants Giovanni Battista Luciani, MD, Gianluca Casali, MD, Luca Barozzi, MD, and Alessandro Mazzucco,
Use of pericardial baffle in the management of intractable bleeding in patients undergoing aortic surgery
 Use of pericardial baffle in the management of intractable bleeding in patients undergoing aortic surgery Introduction Intractable bleeding can occur in complex aortic surgeries such as redo aortic surgeries,
Use of pericardial baffle in the management of intractable bleeding in patients undergoing aortic surgery Introduction Intractable bleeding can occur in complex aortic surgeries such as redo aortic surgeries,
MITROFLOW VALSALVA CONDUIT TM
 TM Features the only bovine pericardium aortic root surgery system THE REPLICATES THE NATIVE SINUS, NATURALLY 2 TM LIVANOVA S INNOVATIVE IS DESIGNED TO: Provide a reproducible and easy solution for better
TM Features the only bovine pericardium aortic root surgery system THE REPLICATES THE NATIVE SINUS, NATURALLY 2 TM LIVANOVA S INNOVATIVE IS DESIGNED TO: Provide a reproducible and easy solution for better
Marfan s S drome: Combined Composite Valve GrAeplacement of the Aortic Root and Transaortic Mihal Valve Replacement
 Marfan s S drome: Combined Composite Valve GrAeplacement of the Aortic Root and Transaortic Mihal Valve Replacement E. Stanley Crawford, M.D., and Joseph S. Coselli, M.D. ABSTRACT Echocardiographic studies
Marfan s S drome: Combined Composite Valve GrAeplacement of the Aortic Root and Transaortic Mihal Valve Replacement E. Stanley Crawford, M.D., and Joseph S. Coselli, M.D. ABSTRACT Echocardiographic studies
Aneurysms of the proximal ascending aorta represent a
 Ascending Aortic Replacement With Aortic Valve Reimplantation Wolfgang Harringer, MD; Klaus Pethig, MD; Christian Hagl, MD; Gerd P. Meyer, MD; Axel Haverich, MD Background Reimplantation of the native,
Ascending Aortic Replacement With Aortic Valve Reimplantation Wolfgang Harringer, MD; Klaus Pethig, MD; Christian Hagl, MD; Gerd P. Meyer, MD; Axel Haverich, MD Background Reimplantation of the native,
Total arch replacement with separated graft technique and selective antegrade cerebral perfusion
 Masters of Cardiothoracic Surgery Total arch replacement with separated graft technique and selective antegrade cerebral perfusion Teruhisa Kazui 1,2 1 Hamamatsu University School of Medicine, Hamamatsu,
Masters of Cardiothoracic Surgery Total arch replacement with separated graft technique and selective antegrade cerebral perfusion Teruhisa Kazui 1,2 1 Hamamatsu University School of Medicine, Hamamatsu,
Valve-Sparing Aortic Root Replacement: Early Experience With the De Paulis Valsalva Graft in 51 Patients
 Valve-Sparing Aortic Root Replacement: Early Experience With the De Paulis Valsalva Graft in 51 Patients Nishant D. Patel, BA, Jason A. Williams, MD, Christopher J. Barreiro, MD, Brian T. Bethea, MD, Torin
Valve-Sparing Aortic Root Replacement: Early Experience With the De Paulis Valsalva Graft in 51 Patients Nishant D. Patel, BA, Jason A. Williams, MD, Christopher J. Barreiro, MD, Brian T. Bethea, MD, Torin
Surgical Procedures and Complications
 Radiological Society of North America, RSNA 2013 Refresher Course Program: Vascular Track Surgical Procedures and Complications Learning objectives Outline RC 112 : Key Concepts: Surgical Procedures and
Radiological Society of North America, RSNA 2013 Refresher Course Program: Vascular Track Surgical Procedures and Complications Learning objectives Outline RC 112 : Key Concepts: Surgical Procedures and
Controversy exists regarding the extent of proximal
 Does the Extent of Proximal or Distal Resection Influence Outcome for Type A Dissections? Marc R. Moon, MD, Thoralf M. Sundt III, MD, Michael K. Pasque, MD, Hendrick B. Barner, MD, Charles B. Huddleston,
Does the Extent of Proximal or Distal Resection Influence Outcome for Type A Dissections? Marc R. Moon, MD, Thoralf M. Sundt III, MD, Michael K. Pasque, MD, Hendrick B. Barner, MD, Charles B. Huddleston,
Results of Aortic Valve Preservation and Repair
 Results of Aortic Valve Preservation and Repair Department of Cardiothoracic and Vascular Surgery Cliniques Universitaires St. Luc Brussels, Belgium Gebrine Elkhoury Institutional experience in AV preservation
Results of Aortic Valve Preservation and Repair Department of Cardiothoracic and Vascular Surgery Cliniques Universitaires St. Luc Brussels, Belgium Gebrine Elkhoury Institutional experience in AV preservation
An anterior aortoventriculoplasty, known as the Konno-
 The Konno-Rastan Procedure for Anterior Aortic Annular Enlargement Mark E. Roeser, MD An anterior aortoventriculoplasty, known as the Konno-Rastan procedure, is a useful tool for the cardiac surgeon. Originally,
The Konno-Rastan Procedure for Anterior Aortic Annular Enlargement Mark E. Roeser, MD An anterior aortoventriculoplasty, known as the Konno-Rastan procedure, is a useful tool for the cardiac surgeon. Originally,
Redacement of the AsGending Aorta and Aortic Valve with a Composite Graft: Results in 25 Patients
 Redacement of the AsGending Aorta and Aortic Valve with a Composite Graft: Results in 25 Patients Nicholas T. Kouchoukos, M.D., Robert B. Karp, M.D., and William A. Lell, M.D. ABSTRACT Our experience with
Redacement of the AsGending Aorta and Aortic Valve with a Composite Graft: Results in 25 Patients Nicholas T. Kouchoukos, M.D., Robert B. Karp, M.D., and William A. Lell, M.D. ABSTRACT Our experience with
Reconstruction of the intervalvular fibrous body during aortic and
 Aortic and mitral valve replacement with reconstruction of the intervalvular fibrous body: An analysis of clinical outcomes Nilto C. De Oliveira, MD Tirone E. David, MD Susan Armstrong, MSc Joan Ivanov,
Aortic and mitral valve replacement with reconstruction of the intervalvular fibrous body: An analysis of clinical outcomes Nilto C. De Oliveira, MD Tirone E. David, MD Susan Armstrong, MSc Joan Ivanov,
42yr Old Male with Severe AR Mild LV dysfunction s/p TOF -AV Replacement(tissue valve) or AoV plasty- Kyung-Hwan Kim
 or AoV plasty- Kyung-Hwan Kim") 42yr Old Male with Severe AR Mild LV dysfunction s/p TOF -AV Replacement(tissue valve) or AoV plasty- Kyung-Hwan Kim Current Guideline for AR s/p TOF Surgery is reasonable in adults with prior repair of
42yr Old Male with Severe AR Mild LV dysfunction s/p TOF -AV Replacement(tissue valve) or AoV plasty- Kyung-Hwan Kim Current Guideline for AR s/p TOF Surgery is reasonable in adults with prior repair of
CROWN PRT. Inservice implantation guide
 Inservice implantation guide DEVICE DESCRIPTION The Crown PRT aortic pericardial heart valve consists of a single piece of bovine pericardium that is preserved with glutaraldehyde and sewn onto a polyester
Inservice implantation guide DEVICE DESCRIPTION The Crown PRT aortic pericardial heart valve consists of a single piece of bovine pericardium that is preserved with glutaraldehyde and sewn onto a polyester
Anatomy determines the close vicinity of the sinuses of
 Aortic Valve Reimplantation According to the David Type I Technique Matthias Karck, MD, and Axel Haverich, MD Department of Thoracic and Cardiovascular Surgery, Hannover Medical School, Hannover, Germany.
Aortic Valve Reimplantation According to the David Type I Technique Matthias Karck, MD, and Axel Haverich, MD Department of Thoracic and Cardiovascular Surgery, Hannover Medical School, Hannover, Germany.
Repair or Replacement
 Surgical intervention post MitraClip Device: Repair or Replacement Saudi Heart Association, February 21-24 Rüdiger Lange, MD, PhD Nicolo Piazza, MD, FRCPC, FESC German Heart Center, Munich, Germany Division
Surgical intervention post MitraClip Device: Repair or Replacement Saudi Heart Association, February 21-24 Rüdiger Lange, MD, PhD Nicolo Piazza, MD, FRCPC, FESC German Heart Center, Munich, Germany Division
Joseph E. Bavaria, M.D. Roberts Measy Professor and Vice Chief CardioVascular Surgery Director: Thoracic Aortic Surgery Program University of
 Joseph E. Bavaria, M.D. Roberts Measy Professor and Vice Chief CardioVascular Surgery Director: Thoracic Aortic Surgery Program University of Pennsylvania, USA North American Valve Repair, Philadelphia
Joseph E. Bavaria, M.D. Roberts Measy Professor and Vice Chief CardioVascular Surgery Director: Thoracic Aortic Surgery Program University of Pennsylvania, USA North American Valve Repair, Philadelphia
Advances in the Treatment of Acute Type A Dissection: An Integrated Approach
 Advances in the Treatment of Acute Type A Dissection: An Integrated Approach Joseph E. Bavaria, MD, Derek R. Brinster, MD, Robert C. Gorman, MD, Y. Joseph Woo, MD, Thomas Gleason, MD, and Alberto Pochettino,
Advances in the Treatment of Acute Type A Dissection: An Integrated Approach Joseph E. Bavaria, MD, Derek R. Brinster, MD, Robert C. Gorman, MD, Y. Joseph Woo, MD, Thomas Gleason, MD, and Alberto Pochettino,
Outcomes of Mitral Valve Repair for Mitral Regurgitation Due to Degenerative Disease
 Outcomes of Mitral Valve Repair for Mitral Regurgitation Due to Degenerative Disease TIRONE E. DAVID, MD ; SEMIN THORAC CARDIOVASC SURG 19:116-120c 2007 ELSEVIER INC. PRESENTED BY INTERN 許士盟 Mitral valve
Outcomes of Mitral Valve Repair for Mitral Regurgitation Due to Degenerative Disease TIRONE E. DAVID, MD ; SEMIN THORAC CARDIOVASC SURG 19:116-120c 2007 ELSEVIER INC. PRESENTED BY INTERN 許士盟 Mitral valve
Long-term results (22 years) of the Ross Operation a single institutional experience
 of the Ross Operation a single institutional experience") Long-term results (22 years) of the Ross Operation a single institutional experience Authors: Costa FDA, Schnorr GM, Veloso M,Calixto A, Colatusso D, Balbi EM, Torres R, Ferreira ADA, Colatusso C Department
Long-term results (22 years) of the Ross Operation a single institutional experience Authors: Costa FDA, Schnorr GM, Veloso M,Calixto A, Colatusso D, Balbi EM, Torres R, Ferreira ADA, Colatusso C Department
Annular Stabilization Techniques in the Context of Aortic Valve Repair
 Annular Stabilization Techniques in the Context of Aortic Valve Repair Prashanth Vallabhajosyula, MD MS University of Pennsylvania, Philadelphia, Pennsylvania 2 nd North American Aortic Valve Repair Symposium
Annular Stabilization Techniques in the Context of Aortic Valve Repair Prashanth Vallabhajosyula, MD MS University of Pennsylvania, Philadelphia, Pennsylvania 2 nd North American Aortic Valve Repair Symposium
Aortic root false aneurysm from gelatin-resorcinolformaldehyde GRF glue following surgical treatment for type A dissection
 Jichi Medical University Journal Aortic root false aneurysm from gelatin-resorcinolformaldehyde GRF glue following surgical treatment for type A dissection Yasuhito Sakano, Tsutomu Saito, Yoshio Misawa
Jichi Medical University Journal Aortic root false aneurysm from gelatin-resorcinolformaldehyde GRF glue following surgical treatment for type A dissection Yasuhito Sakano, Tsutomu Saito, Yoshio Misawa
The need for right ventricular outflow tract reconstruction
 Polytetrafluoroethylene Bicuspid Pulmonary Valve Implantation James A. Quintessenza, MD The need for right ventricular outflow tract reconstruction and pulmonary valve replacement is increasing for many
Polytetrafluoroethylene Bicuspid Pulmonary Valve Implantation James A. Quintessenza, MD The need for right ventricular outflow tract reconstruction and pulmonary valve replacement is increasing for many
Re-do aortic valve replacement after previous homograft aortic root replacement
 Re-do aortic valve replacement after previous homograft aortic root replacement Jullien Gaer, Toufan Bahrami, Fabio de Robertis, Ahmed Abdulsalam, John Pepper, NHS Foundation Trust, UK Professor Sir Magdi
Re-do aortic valve replacement after previous homograft aortic root replacement Jullien Gaer, Toufan Bahrami, Fabio de Robertis, Ahmed Abdulsalam, John Pepper, NHS Foundation Trust, UK Professor Sir Magdi
The Edge-to-Edge Technique f For Barlow's Disease
 The Edge-to-Edge Technique f For Barlow's Disease Ottavio Alfieri, Michele De Bonis, Elisabetta Lapenna, Francesco Maisano, Lucia Torracca, Giovanni La Canna. Department of Cardiac Surgery, San Raffaele
The Edge-to-Edge Technique f For Barlow's Disease Ottavio Alfieri, Michele De Bonis, Elisabetta Lapenna, Francesco Maisano, Lucia Torracca, Giovanni La Canna. Department of Cardiac Surgery, San Raffaele
Verbrede mediastinum: Treatment
 Verbrede mediastinum: Treatment Klinische les - Cardiale Heelkunde Gabriele Bislenghi ASO Heelkunde UZ Leuven Moderator: prof. B. Meuris Overview Aortic dissection Boerhaave Aortic Dissection Aortic dissection
Verbrede mediastinum: Treatment Klinische les - Cardiale Heelkunde Gabriele Bislenghi ASO Heelkunde UZ Leuven Moderator: prof. B. Meuris Overview Aortic dissection Boerhaave Aortic Dissection Aortic dissection
Stentless full root bioprosthesis in surgery for complex aortic valve-ascending aortic disease: a single center experience of over 300 patients
 European Journal of Cardio-thoracic Surgery 33 (2008) 554 559 www.elsevier.com/locate/ejcts Stentless full root bioprosthesis in surgery for complex aortic valve-ascending aortic disease: a single center
European Journal of Cardio-thoracic Surgery 33 (2008) 554 559 www.elsevier.com/locate/ejcts Stentless full root bioprosthesis in surgery for complex aortic valve-ascending aortic disease: a single center
Joseph E. Bavaria, M.D. Roberts Measy Professor and Vice Chief CardioVascular Surgery Director: Thoracic Aortic Surgery Program University of
 Joseph E. Bavaria, M.D. Roberts Measy Professor and Vice Chief CardioVascular Surgery Director: Thoracic Aortic Surgery Program University of Pennsylvania, USA AVRS Philadelphia Sept 2016 Pictures courtesy
Joseph E. Bavaria, M.D. Roberts Measy Professor and Vice Chief CardioVascular Surgery Director: Thoracic Aortic Surgery Program University of Pennsylvania, USA AVRS Philadelphia Sept 2016 Pictures courtesy
The Role Of Decellularized Valve Prostheses In The Young Patient
 The Role Of Decellularized Valve Prostheses In The Young Patient Francisco Diniz Affonso da Costa Human Tissue Bank PUCPR - Brazil Disclosures Ownership and patent license of the SDS decellularization
The Role Of Decellularized Valve Prostheses In The Young Patient Francisco Diniz Affonso da Costa Human Tissue Bank PUCPR - Brazil Disclosures Ownership and patent license of the SDS decellularization
The vast majority of patients, especially children, who
 Technique of Mechanical Pulmonary Valve Replacement John M. Stulak, MD, and Joseph A. Dearani, MD The vast majority of patients, especially children, who require pulmonary valve replacement (PVR), obtain
Technique of Mechanical Pulmonary Valve Replacement John M. Stulak, MD, and Joseph A. Dearani, MD The vast majority of patients, especially children, who require pulmonary valve replacement (PVR), obtain
SURGICAL INTERVENTION IN AORTOPATHIES ZOHAIR ALHALEES, MD RIYADH, SAUDI ARABIA
 SURGICAL INTERVENTION IN AORTOPATHIES ZOHAIR ALHALEES, MD RIYADH, SAUDI ARABIA In patients born with CHD, dilatation of the aorta is a frequent feature at presentation and during follow up after surgical
SURGICAL INTERVENTION IN AORTOPATHIES ZOHAIR ALHALEES, MD RIYADH, SAUDI ARABIA In patients born with CHD, dilatation of the aorta is a frequent feature at presentation and during follow up after surgical
Valve-Sparing Aortic Root Replacement in Loeys-Dietz Syndrome
 Valve-Sparing Aortic Root Replacement in Loeys-Dietz Syndrome Nishant D. Patel, MD, George J. Arnaoutakis, MD, Timothy J. George, MD, Jeremiah G. Allen, MD, Diane E. Alejo, BA, Harry C. Dietz, MD, Duke
Valve-Sparing Aortic Root Replacement in Loeys-Dietz Syndrome Nishant D. Patel, MD, George J. Arnaoutakis, MD, Timothy J. George, MD, Jeremiah G. Allen, MD, Diane E. Alejo, BA, Harry C. Dietz, MD, Duke
The Journal of Thoracic and Cardiovascular Surgery
 Accepted Manuscript Love the Root Not the Flowers Everyone Sees Tomasz A. Timek, MD PhD, Clinical Associate Professor PII: S0022-5223(18)31205-4 DOI: 10.1016/j.jtcvs.2018.04.068 Reference: YMTC 12941 To
Accepted Manuscript Love the Root Not the Flowers Everyone Sees Tomasz A. Timek, MD PhD, Clinical Associate Professor PII: S0022-5223(18)31205-4 DOI: 10.1016/j.jtcvs.2018.04.068 Reference: YMTC 12941 To
Clinical Commissioning Policy Proposition: Personalised External Aortic Root Support (PEARS) for surgical management of enlarged aortic root (adults)
 for surgical management of enlarged aortic root (adults)") Clinical Commissioning Policy Proposition: Personalised External Aortic Root Support (PEARS) for surgical management of enlarged aortic root (adults) Information Reader Box (IRB) to be inserted on inside
Clinical Commissioning Policy Proposition: Personalised External Aortic Root Support (PEARS) for surgical management of enlarged aortic root (adults) Information Reader Box (IRB) to be inserted on inside
SOLO SMART. The smart way to return to life. Native-like performance now with stented-like implantability
 SOLO SMART TM The smart way to return to life Native-like performance now with stented-like implantability MANY PATIENTS NEED SUPERIOR HEMODYNAMIC PERFORMANCE TO RETURN TO THEIR NORMAL LIFESTYLE. 2 SOLO
SOLO SMART TM The smart way to return to life Native-like performance now with stented-like implantability MANY PATIENTS NEED SUPERIOR HEMODYNAMIC PERFORMANCE TO RETURN TO THEIR NORMAL LIFESTYLE. 2 SOLO
ACD. Tirone E. David, MD, Christopher M. Feindel, MD, Susan Armstrong, MSc, and Manjula Maganti, MSc
 Replacement of the ascending aorta with reduction of the diameter of the sinotubular junction to treat aortic insufficiency in patients with ascending aortic aneurysm Tirone E. David, MD, Christopher M.
Replacement of the ascending aorta with reduction of the diameter of the sinotubular junction to treat aortic insufficiency in patients with ascending aortic aneurysm Tirone E. David, MD, Christopher M.
PPM: How to fit a big valve in a small heart
 PPM: How to fit a big valve in a small heart Hani K. Najm MD, Msc, FRCSC, FRCS (Glasgow), FACC, FESC King Abdulaziz Cardiac Centre National Guard Health Affairs Riyadh, Saudi Arabia GHA meeting Muscat
PPM: How to fit a big valve in a small heart Hani K. Najm MD, Msc, FRCSC, FRCS (Glasgow), FACC, FESC King Abdulaziz Cardiac Centre National Guard Health Affairs Riyadh, Saudi Arabia GHA meeting Muscat
Early and One-year Outcomes of Aortic Root Surgery in Marfan Syndrome Patients
 Early and One-year Outcomes of Aortic Root Surgery in Marfan Syndrome Patients A Prospective, Multi-Center, Comparative Study Joseph S. Coselli, Irina V. Volguina, Scott A. LeMaire, Thoralf M. Sundt, Elizabeth
Early and One-year Outcomes of Aortic Root Surgery in Marfan Syndrome Patients A Prospective, Multi-Center, Comparative Study Joseph S. Coselli, Irina V. Volguina, Scott A. LeMaire, Thoralf M. Sundt, Elizabeth
Aortic Arch/ Thoracoabdominal Aortic Replacement
 Aortic Arch/ Thoracoabdominal Aortic Replacement Joseph S. Coselli, M.D. Vice Chair, Department of Surgery Professor, Chief, and Cullen Foundation Endowed Chair Division of Cardiothoracic Surgery Baylor
Aortic Arch/ Thoracoabdominal Aortic Replacement Joseph S. Coselli, M.D. Vice Chair, Department of Surgery Professor, Chief, and Cullen Foundation Endowed Chair Division of Cardiothoracic Surgery Baylor
Aortic Regurgitation in Connective Tissue Disorders Special precautions? Carlos A. Mestres MD PhD FETCS
 Aortic Regurgitation in Connective Tissue Disorders Special precautions? Carlos A. Mestres MD PhD FETCS Senior Consultant Department of Cardiovascular Surgery University Hospital Zürich (Switzerland) Extraordinary
Aortic Regurgitation in Connective Tissue Disorders Special precautions? Carlos A. Mestres MD PhD FETCS Senior Consultant Department of Cardiovascular Surgery University Hospital Zürich (Switzerland) Extraordinary
separated graft technique 29 II HCA SCP continuous cold blood cardioplegia P<0.05 I cerebrovascular accident CVA II CVA
 12 115 122 2003 2003 2 43 29 2 12 4 Bentall 4 2 1996en bloc technique14 I 1997 separated graft technique29 II HCA SCP continuous cold blood cardioplegia CCBC HCA I 86.6 37.1 II 74.2 43.4 SCP I 55.6 15.6
12 115 122 2003 2003 2 43 29 2 12 4 Bentall 4 2 1996en bloc technique14 I 1997 separated graft technique29 II HCA SCP continuous cold blood cardioplegia CCBC HCA I 86.6 37.1 II 74.2 43.4 SCP I 55.6 15.6
Experience with 500 Stentless Aortic Valve Replacements
 Experience with 500 Stentless Aortic Valve Replacements Dimitrios C. Iliopoulos, MD Cardiac Surgeon Ass. Professor of Surgery University of Athens, School of Medicine I declare no conflict of interest
Experience with 500 Stentless Aortic Valve Replacements Dimitrios C. Iliopoulos, MD Cardiac Surgeon Ass. Professor of Surgery University of Athens, School of Medicine I declare no conflict of interest
Composite valve graft replacement has become
 A 23-Year Experience With Composite Valve Graft Replacement of the Aortic Root Karl M. Dossche, MD, Marc A. A. M. Schepens, MD, PhD, Wim J. Morshuis, MD, PhD, Aart Brutel de la Rivière, MD, PhD, Paul J.
A 23-Year Experience With Composite Valve Graft Replacement of the Aortic Root Karl M. Dossche, MD, Marc A. A. M. Schepens, MD, PhD, Wim J. Morshuis, MD, PhD, Aart Brutel de la Rivière, MD, PhD, Paul J.
Clinical outcomes of aortic root replacement after previous aortic root replacement
 Clinical outcomes of aortic root replacement after previous aortic root replacement Luis Garrido-Olivares, MD, MSc, Manjula Maganti, MSc, Susan Armstrong, MSc, and Tirone E. David, MD Objective: The study
Clinical outcomes of aortic root replacement after previous aortic root replacement Luis Garrido-Olivares, MD, MSc, Manjula Maganti, MSc, Susan Armstrong, MSc, and Tirone E. David, MD Objective: The study
New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor. Cardiothoracic Radiology
 New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor Cardiothoracic Radiology Disclosure I have no disclosure pertinent to this presentation.
New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor Cardiothoracic Radiology Disclosure I have no disclosure pertinent to this presentation.
We present the case of an asymptomatic, 75-year-old
 Images in Cardiovascular Medicine Asymptomatic Rupture of the Left Ventricle Lech Paluszkiewicz, MD; Stefan Ożegowski, MD; Mohammad Amin Parsa, MD; Jan Gummert, PhD, MD We present the case of an asymptomatic,
Images in Cardiovascular Medicine Asymptomatic Rupture of the Left Ventricle Lech Paluszkiewicz, MD; Stefan Ożegowski, MD; Mohammad Amin Parsa, MD; Jan Gummert, PhD, MD We present the case of an asymptomatic,
Role of Sutureless Valves in the Surgeon s Armamentarium Prof. Dr Malakh Shrestha Vice Chair, Director of Aortic Surgery Cardiothoracic,
 Role of Sutureless Valves in the Surgeon s Armamentarium Prof. Dr Malakh Shrestha Vice Chair, Director of Aortic Surgery Cardiothoracic, transplantation and Vascular Surgery Hannover Medical School, Germany
Role of Sutureless Valves in the Surgeon s Armamentarium Prof. Dr Malakh Shrestha Vice Chair, Director of Aortic Surgery Cardiothoracic, transplantation and Vascular Surgery Hannover Medical School, Germany
Midterm Outcome of Valve-Sparing Aortic Root Replacement in Inherited Connective Tissue Disorders. Patients
 Midterm Outcome of Valve-Sparing Aortic Root Replacement in Inherited Connective Tissue Disorders Hiroshi Tanaka, MD, PhD, Hitoshi Ogino, MD, PhD, Hitoshi Matsuda, MD, PhD, Kenji Minatoya, MD, PhD, Hiroaki
Midterm Outcome of Valve-Sparing Aortic Root Replacement in Inherited Connective Tissue Disorders Hiroshi Tanaka, MD, PhD, Hitoshi Ogino, MD, PhD, Hitoshi Matsuda, MD, PhD, Kenji Minatoya, MD, PhD, Hiroaki
Aortic valve leaflet sparing and salvage surgery: evolution of techniques for aortic root reconstruction q
 European Journal of Cardio-thoracic Surgery 24 (2003) 886 897 Review Aortic valve leaflet sparing and salvage surgery: evolution of techniques for aortic root reconstruction q Richard A. Hopkins* Brown
European Journal of Cardio-thoracic Surgery 24 (2003) 886 897 Review Aortic valve leaflet sparing and salvage surgery: evolution of techniques for aortic root reconstruction q Richard A. Hopkins* Brown
Transcatheter aortic valves in aortic regurgitation Gry Dahle Dept of Cardiothoracic- and vascular surgery Rikshospitalet, Oslo University Hospital,
 Transcatheter aortic valves in aortic regurgitation Gry Dahle Dept of Cardiothoracic- and vascular surgery Rikshospitalet, Oslo University Hospital, Oslo, Norway Aortic regurgitation Prevalence in Framingham
Transcatheter aortic valves in aortic regurgitation Gry Dahle Dept of Cardiothoracic- and vascular surgery Rikshospitalet, Oslo University Hospital, Oslo, Norway Aortic regurgitation Prevalence in Framingham
Pulmonary Valve Replacement
 Pulmonary Valve Replacement with Fascia Lata J. C. R. Lincoln, F.R.C.S., M. Geens, M.D., M. Schottenfeld, M.D., and D. N. Ross, F.R.C.S. ABSTRACT The purpose of this paper is to describe a technique of
Pulmonary Valve Replacement with Fascia Lata J. C. R. Lincoln, F.R.C.S., M. Geens, M.D., M. Schottenfeld, M.D., and D. N. Ross, F.R.C.S. ABSTRACT The purpose of this paper is to describe a technique of
Aortic Valve Resuspension in Ascending Aortic Aneurysm Repair With Aortic Insufficiency
 Aortic Valve Resuspension in Ascending Aortic Aneurysm Repair With Aortic Insufficiency Paul Simon, MD, Anton Mortiz, MD, Reinhard Moidl, MD, Natascha Kupilik, MD, Martin Grabenwoeger, MD, Marek Ehrlich,
Aortic Valve Resuspension in Ascending Aortic Aneurysm Repair With Aortic Insufficiency Paul Simon, MD, Anton Mortiz, MD, Reinhard Moidl, MD, Natascha Kupilik, MD, Martin Grabenwoeger, MD, Marek Ehrlich,
Late results of aortic root repair & replacement. John Pepper Imperial College and Royal Brompton Hospital, London, UK.
 Late results of aortic root repair & replacement John Pepper Imperial College and Royal Brompton Hospital, London, UK. REPLACEMENT OF ASCENDING AORTA AND ROOT Interposition graft Valve sparing VR + graft
Late results of aortic root repair & replacement John Pepper Imperial College and Royal Brompton Hospital, London, UK. REPLACEMENT OF ASCENDING AORTA AND ROOT Interposition graft Valve sparing VR + graft
Durability of Aortic Valve Preservation and Root Reconstruction in Acute Type A Aortic Dissection
 Durability of Aortic Valve Preservation and Root Reconstruction in Acute Type A Aortic Dissection Filip P. Casselman, MD, M. Erwin S. H. Tan, MD, Freddy E. E. Vermeulen, MD, Johannes C. Kelder, MD, Wim
Durability of Aortic Valve Preservation and Root Reconstruction in Acute Type A Aortic Dissection Filip P. Casselman, MD, M. Erwin S. H. Tan, MD, Freddy E. E. Vermeulen, MD, Johannes C. Kelder, MD, Wim
TSDA Boot Camp September 13-16, Introduction to Aortic Valve Surgery. George L. Hicks, Jr., MD
 TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
HURDLES FOR STARTING MINISTERNOTOMY AORTIC VALVE REPLACEMENT PROGRAM IN OUR INSTITUTE
 HURDLES FOR STARTING MINISTERNOTOMY AORTIC VALVE REPLACEMENT PROGRAM IN OUR INSTITUTE *Suraj Wasudeo Nagre Department of CVTS, Grant Medical College, Mumbai *Author for Correspondence ABSTRACT It s our
HURDLES FOR STARTING MINISTERNOTOMY AORTIC VALVE REPLACEMENT PROGRAM IN OUR INSTITUTE *Suraj Wasudeo Nagre Department of CVTS, Grant Medical College, Mumbai *Author for Correspondence ABSTRACT It s our
Interventional procedures guidance Published: 26 September 2014 nice.org.uk/guidance/ipg504
 Transcatheter valve-in-valve e implantation for aortic bioprosthetic valve dysfunction Interventional procedures guidance Published: 26 September 2014 nice.org.uk/guidance/ipg504 Your responsibility This
Transcatheter valve-in-valve e implantation for aortic bioprosthetic valve dysfunction Interventional procedures guidance Published: 26 September 2014 nice.org.uk/guidance/ipg504 Your responsibility This
Minimally invasive valve-sparing aortic root reimplantation
 Surgical Technique on Cardiac Surgery Page 1 of 5 Minimally invasive valve-sparing aortic root reimplantation Vishal N. Shah 1,2, Oleg I. Orlov 1,2, Cinthia Orlov 1,2, Serge Sicouri 1, Manabu Takebe 2,
Surgical Technique on Cardiac Surgery Page 1 of 5 Minimally invasive valve-sparing aortic root reimplantation Vishal N. Shah 1,2, Oleg I. Orlov 1,2, Cinthia Orlov 1,2, Serge Sicouri 1, Manabu Takebe 2,
Joseph E. Bavaria, MD
 EACTS Master Class on Aortic Valve Repair Joseph E. Bavaria, MD Director, Thoracic Aortic Surgery Program Roberts Measey Professor and Vice Chair of CV Surgery University of Pennsylvania Immediate-Past
EACTS Master Class on Aortic Valve Repair Joseph E. Bavaria, MD Director, Thoracic Aortic Surgery Program Roberts Measey Professor and Vice Chair of CV Surgery University of Pennsylvania Immediate-Past
Aortic valve insufficiency may be caused by abnormalities
 Reconstruction of the Ascending Aorta and Aortic Root: Experience in 45 Consecutive Patients Gebrine A. El Khoury, MD, Malcolm J. Underwood, MD, David Glineur, MD, David Derouck, MD, and Robert A. Dion,
Reconstruction of the Ascending Aorta and Aortic Root: Experience in 45 Consecutive Patients Gebrine A. El Khoury, MD, Malcolm J. Underwood, MD, David Glineur, MD, David Derouck, MD, and Robert A. Dion,
Kinsing Ko, Thom de Kroon, Najim Kaoui, Bart van Putte, Nabil Saouti. St. Antonius Hospital, Nieuwegein, The Netherlands
 Minimal Invasive Mitral Valve Surgery After Previous Sternotomy Without Aortic Clamping: Short- and Long Term Results of a Single Surgeon Single Institution Kinsing Ko, Thom de Kroon, Najim Kaoui, Bart
Minimal Invasive Mitral Valve Surgery After Previous Sternotomy Without Aortic Clamping: Short- and Long Term Results of a Single Surgeon Single Institution Kinsing Ko, Thom de Kroon, Najim Kaoui, Bart
The Bentall procedure: Is it the gold standard? A series of 597 consecutive cases
 The Bentall procedure: Is it the gold standard? A series of 597 consecutive cases Christian D. Etz, MD, PhD, Moritz S. Bischoff, MD, Carol Bodian, DrPH, Fabian Roder, MS, Robert Brenner, BS, Randall B.
The Bentall procedure: Is it the gold standard? A series of 597 consecutive cases Christian D. Etz, MD, PhD, Moritz S. Bischoff, MD, Carol Bodian, DrPH, Fabian Roder, MS, Robert Brenner, BS, Randall B.
PROVEN PLUS. Introducing the Avalus Aortic Valve by Medtronic.
 PROVEN PLUS. Introducing the Avalus Aortic Valve by Medtronic. With more than 40 years of heart valve innovations, we took proven valve design concepts and adapted them for excellent implantability for
PROVEN PLUS. Introducing the Avalus Aortic Valve by Medtronic. With more than 40 years of heart valve innovations, we took proven valve design concepts and adapted them for excellent implantability for
Aortic root aneurysm: Principles of repair and long-term follow-up
 Aortic Symposium 2010 David et al Aortic root aneurysm: Principles of repair and long-term follow-up Tirone E. David, MD, Manjula Maganti, MSc, and Susan Armstrong, MSc Objectives: This study was undertaken
Aortic Symposium 2010 David et al Aortic root aneurysm: Principles of repair and long-term follow-up Tirone E. David, MD, Manjula Maganti, MSc, and Susan Armstrong, MSc Objectives: This study was undertaken
Repair of the aortic valve in patients with insufficiency and aortic root aneurysm
 Surgery for Acquired Heart Disease Repair of the aortic valve in patients with insufficiency and aortic root aneurysm aortic Patients with aneurysms of the ascending aorta or aortic root frequently have
Surgery for Acquired Heart Disease Repair of the aortic valve in patients with insufficiency and aortic root aneurysm aortic Patients with aneurysms of the ascending aorta or aortic root frequently have
Functional anatomy of the aortic root. ΔΡΟΣΟΣ ΓΕΩΡΓΙΟΣ Διεσθσνηής Καρδιοθωρακοτειροσργικής Κλινικής Γ.Ν. «Γ. Παπανικολάοσ» Θεζζαλονίκη
 Functional anatomy of the aortic root ΔΡΟΣΟΣ ΓΕΩΡΓΙΟΣ Διεσθσνηής Καρδιοθωρακοτειροσργικής Κλινικής Γ.Ν. «Γ. Παπανικολάοσ» Θεζζαλονίκη What is the aortic root? represents the outflow tract from the LV provides
Functional anatomy of the aortic root ΔΡΟΣΟΣ ΓΕΩΡΓΙΟΣ Διεσθσνηής Καρδιοθωρακοτειροσργικής Κλινικής Γ.Ν. «Γ. Παπανικολάοσ» Θεζζαλονίκη What is the aortic root? represents the outflow tract from the LV provides