Role of Sutureless Valves in the Surgeon s Armamentarium Prof. Dr Malakh Shrestha Vice Chair, Director of Aortic Surgery Cardiothoracic,
|
|
|
- Elfreda Boone
- 5 years ago
- Views:
Transcription





1 Role of Sutureless Valves in the Surgeon s Armamentarium Prof. Dr Malakh Shrestha Vice Chair, Director of Aortic Surgery Cardiothoracic, transplantation and Vascular Surgery Hannover Medical School, Germany
 Sutureless Valve (24th April 2007).")
2 Disclosure At present : none related to this presentation. First in man Implantation of Perceval (LivaNova) Sutureless Valve (24th April 2007). First in man Implantation of Elite Rapid Deployment Valve (Edwards) (20th Jan 2010) Cardio-thoracic, Transplantation and Vascular Surgery





3 Albert starr & Lowell Edwards August 25, 1960 H o l y G r a i l

4 The concept Simplifies the surgical procedure Reduction of implantation time Concomitant procedures possible Minimally invasive AVR easier. The McGovern Valve 1964 Native diseased aortic valve removed, Prosthesis not crimped: Better Durability


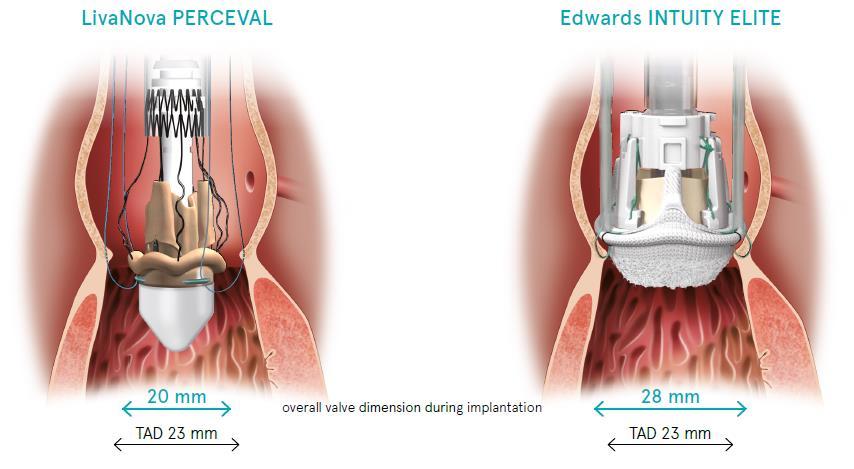
5 Rapid Deployment/Sutureless Valve Systems Sorin Perceval S Edwards Intuity Quick-connect System




6 Perceval first clinical implant (Pilot trial) Indications 1. Age 75 years 2. Aortic valve stenosis at high surgical risk and candidate for a standard surgical intervention of aortic valve replacement with biological prosthesis 3. NYHA functional class III and IV 4. Small and calcific aortic root/annulus Contra-indications: 1. Aneurysmal dilation or dissection of the ascending aorta requiring correction 2. Aortic annulus size (after decalcification) < 21 or > 23mm by direct intraoperative measurement MHH Hannover Male, 88 yrs, Logistic Euroscore 16.90% NYHA class III Perceval M and concomitant CABG X-clamp time: 53 min, CPB time: 83 min
 were operated on (Euro Score 17 [8-73]).")
7 OBJECTIVE: The purpose of this study was to assess a new sutureless aortic valve (Perceval Sorin). METHODS: Between April and September 2007, 16 high-risk patients (13 females, aged 81 [76-88]) were operated on (Euro Score 17 [8-73]). All patients had significant aortic valve disease and seven of these patients had concomitant coronary artery disease. RESULTS: One patient died during hospital stay for unknown reasons. Autopsy revealed no valve related pathologies. CPB time was 60 min (41-130), cross-clamping time was 36 (22-79) min. Intraoperative as well as postoperative echocardiography revealed neither aortic insufficiency nor paravalvular leakage in any of the patients. CONCLUSIONS: The new approach is a technically simple alternative to conventional aortic valve replacement in high-risk patients and offers the potential of less invasive approaches. It appears especially useful in patients with severe calcification of the aortic root. CPB and cross-clamping times were markedly reduced compared with patients who underwent conventional operations.


8 Minimally invasive AVR Technical Difficulties 1. Small Aortic Root: 2. Calcified Aortic Root 3. Calcified Ascending Aorta Sutureless valves make Minimally invasive AVR easier. For right mini-thoracotomy approach, this is technically speaking, the easiest valve prosthesis for implantation. Cardio-thoracic, Transplantation and Vascular Surgery





9 12/ , 35 Patients Sizes 21, Avg. Size = 22.1 Shrestha, M., et al., J Heart Valve Dis, (2): p


10 Perceval facilitates and standardizes MICS procedures 145 Perceval implanted via Mini J-Sternotomy Good clinical and hemodynamic results in the postoperative and at mid-term followup with no evidence of early prosthetic valve degeneration. mean implantation time of 7.8 minutes No PVL, 7.6% patients required PMI.


11 Clinical studies publications
12 40-months Survival Perceval vs. conventional AVR in RAT Freedom from Reoperation at follow-up Perceval vs. conventional AVR in RAT Aortic valve replacement through right anterior minithoracotomy: can sutureless technology improve clinical outcomes? Gilmanov D, Miceli A, Ferrarini M, Farneti P, Murzi M, Solinas M, Glauber M. - Ann Thorac Surg Nov;98(5):

13 First 100 Perceval implants!


14 AVR in small aortic annulus? Patient-Prosthesis Mismatch? No Suturing Ring: Perceval is stent-less Valve Perceval prosthesis himplantation is technically easy even in small aortic roots and has excellent gradients. Perceval implantation is easy to implant The gradients are excellent No PPM!! Patch enlargement of aortic annulus not necessary!


15 Features & Benefits: Collapsible UNIQUE COLLAPSIBLE DESIGN The valve diameter can be reduced prior to implantation, increasing visibility. Perceval Size M 11 mm 20 mm 14 mm


16 Features & Benefits: Collapsible ATRAUMATIC COLLAPSING The collapsing procedure does not affect the leaflets preventing any possible damage to the tissue Published Experience Lack of Evidence of Pericardial Injury Following Pre-implantation Collapse in the Sorin Perceval S Sutureless Prosthesis Mila Della Barbera, Cristina Basso, Marialuisa Valente, Gaetano Thiene Department of Medical and Diagnostic Sciences and Special Therapies, University of Padua Medical School, Padova, Italy CONCLUSIONS: Pre-implantation collapse and ballooning does not affect the structural integrity of the collagen network of the pericardial cusp tissue in LivaNova Perceval S Sutureless prosthesis.




17 Durability: Design Tests ISO5840 and FDA guidance require 200 million cycles for tissue valves Perceval valve was tested up to 600 million cycles (15 years equivalent) Before test After 600 Mcycles Testing performed in compliant chamber to mimic worst case in vivo condition Perceval over-achieved three times the FDA guidance

18 Facts: Perceval Worldwide First-in-Human performed in 2007 CE mark January 2011 FDA approval January 2016 Truly Global reach Robust body of Evidence
")




19 1,234 patients to be randomized (1:1) In countries where Perceval is approved International, multicenter controlled randomized trial Approximately 60 centers to be selected Follow up to 5 years




20 Odyssey (Elite) Valve and Delivery System Bovine pericardium Balloonexpandable stainless steel frame Designed to simplify and facilitate MIS Built upon proven valve technology Leverages innovation from transcatheter heart valves Balloon-expandable frame Sub-annular fixation Complete size range 19 mm to 27 mm

21 Edwards Rapid Deployment Valve (Elite) Three fixation sutures: No migration or dislodgment of valve!

22 Triton trial (CE Certification) Major Inclusion Criteria Patient is 18 years or older Aortic stenosis or stenosis insufficiency requiring planned replacement Planned aortic valve replacement with or without concomitant CABG Informed consent and patient agrees to all post procedure follow up Major Exclusion Criteria Pure aortic insufficiency Aneurysm of the aortic root or ascending aorta LVEF of < 25% Congenital bicuspid aortic valve Concomitant valve disease requiring repair or replacement Evidence of AMI 1 month before intended treatment In situ mitral, tricuspid, or pulmonic replacement valve or ring Non cardiac life expectancy < 12 months


23
24 Case 1: 80 Year Old Female Symptomatic Severe Aortic Valve Prosthesis Stenosis (Gradient: 73/49 Hg mm, EOA: 0.73 cm²) EF:58% Past History: Aortic Valve Replacement (Sutureless Perceval Valve, 21mm) in ReDo Aortic Valve Replacement (Perceval Sutureless Valve, 21 mm)

25

26
 Ascending aortic replacement with a Dacron Graft (30mm Diameter) Post-op mean Gradient: 6mm mm")
27 Case 2: 56 Year Old Male Symptomatic Severe Aortic Valve Stenosis Aneurysm of the ascending Aorta X-ray, CTScan: Extreme Calcification in the aortic root and Myocardium Aortic Valve Replacement :(Edwards Elite Valve, 27 mm) Ascending aortic replacement with a Dacron Graft (30mm Diameter) Post-op mean Gradient: 6mm mm Hg

28

29


30


31

32 Perceval vs Intuity

33 The growing adoption of percutaneous AVR likely will compel more surgeons to explore minimal access approaches for isolated AVR, if it is not currently part of their surgical toolbox. Importantly, the learning curve for rapid deployment heart valves cannot be discounted, which highlights the importance of device-specific training, whether sponsored by industry or by the professional societies. Finally, although the early clinical outcomes seem satisfactory and comparable with conventional heart valves, the important issue of long-term valve durability remains unanswered. In expert hands, conventional and minimal access AVR is associated with low risk and outstanding long-term results that were unheard of even a decade ago. The transition from conventional surgical AVR to rapid deployment AVR by our specialty must be performed in a deliberate and methodical fashion so that the benefits accrued during the last 55 years will not be squandered.


34 To gain evidence-based consensus on the use of sutureless and rapid deployment valves in minimally invasive isolated aortic valve replacement To define the role of minimally invasive aortic valve replacement with sutureless and rapid deployment valves.
 ranges from")
 Not indicated in annular abscess or deconstruction due to")
35 Key recommendations regarding PATIENT INDICATIONS: Sutureless or rapid deployment: Use of sutureless and rapid deployment valves in minimally invasive approaches in patients candidates for AVR and not for TAVI Suitable annular size (after decalcification) ranges from 19 to 27 mm Not indicated for Bicuspid valve type 0 Can be implanted in bicuspid valves type 1 and 2 if: - Coronary ostia do not have 180 position - Rounded annulus - Uniform height of the commissures (in type 2) Not indicated in annular abscess or deconstruction due to endocarditis

36 It is important to find the right balance in life!








37 AVR: we need the whole range of Armementarium!
38 Conclusion Rapid Deployment and Sutureless Valves are technically easier to implant and more reproducible even in Calcified/ small annulus. Min. Inv. AVR: Limited Exposure not a disadvantage Reduces of the X-clamp time and CPB time. No Suturing Ring: Perceval is stent-less Valve: No PPM! Safety: Good durability (Follow-up >10 year) Effectiveness: Hemodynamics are excellent! Re-do AVR: not a problem. Valve of choice for the geriatric Pt.s! Especially in combined AVR
REDUCING THE IMPACT OF SURGERY AND FACILITATING FASTER RECOVERY
 REDUCING THE IMPACT OF SURGERY AND FACILITATING FASTER RECOVERY AORTIC SOLUTIONS PERCEVAL VALVE PERCEVAL THE BIOLOGICAL VALVE OF CHOICE IN AVR 0914 RE0210195/A AORTIC SOLUTIONS PERCEVAL THE BIOLOGICAL
REDUCING THE IMPACT OF SURGERY AND FACILITATING FASTER RECOVERY AORTIC SOLUTIONS PERCEVAL VALVE PERCEVAL THE BIOLOGICAL VALVE OF CHOICE IN AVR 0914 RE0210195/A AORTIC SOLUTIONS PERCEVAL THE BIOLOGICAL
Management of Difficult Aortic Root, Old and New solutions
 Management of Difficult Aortic Root, Old and New solutions Hani K. Najm MD, Msc, FRCSC,, FACC, FESC Chairman, Pediatric and Congenital Heart Surgery Cleveland Clinic Conflict of Interest None Difficult
Management of Difficult Aortic Root, Old and New solutions Hani K. Najm MD, Msc, FRCSC,, FACC, FESC Chairman, Pediatric and Congenital Heart Surgery Cleveland Clinic Conflict of Interest None Difficult
TAVI Versus Suturless Valve In Intermediate Risk Patients
 TAVI Versus Suturless Valve In Intermediate Risk Patients Walid Abukhudair FRCSc President of Saudi Society for Cardiac Surgeons Head of Cardiac Surgery in KFAFH Background AS is the most frequent cardiac
TAVI Versus Suturless Valve In Intermediate Risk Patients Walid Abukhudair FRCSc President of Saudi Society for Cardiac Surgeons Head of Cardiac Surgery in KFAFH Background AS is the most frequent cardiac
AVR with Sutureless Valves State of the Art
 AVR with Sutureless Valves State of the Art T. Fischlein Department of Cardiac Surgery, Cardiovascular Center Klinikum Nürnberg Paracelsus Medical University Nuremberg, Germany Disclosures Consultant and
AVR with Sutureless Valves State of the Art T. Fischlein Department of Cardiac Surgery, Cardiovascular Center Klinikum Nürnberg Paracelsus Medical University Nuremberg, Germany Disclosures Consultant and
National Institute for Health and Care Excellence IP865/2 Sutureless Aortic Valve Replacement for aortic stenosis
 National Institute for Health and Care Excellence IP865/2 Sutureless Aortic Valve Replacement for aortic stenosis IPAC 14/06/18: 1 1 NHS professional 2 1 NHS professional ments 1.1 1.1 Current evidence
National Institute for Health and Care Excellence IP865/2 Sutureless Aortic Valve Replacement for aortic stenosis IPAC 14/06/18: 1 1 NHS professional 2 1 NHS professional ments 1.1 1.1 Current evidence
42yr Old Male with Severe AR Mild LV dysfunction s/p TOF -AV Replacement(tissue valve) or AoV plasty- Kyung-Hwan Kim
 or AoV plasty- Kyung-Hwan Kim") 42yr Old Male with Severe AR Mild LV dysfunction s/p TOF -AV Replacement(tissue valve) or AoV plasty- Kyung-Hwan Kim Current Guideline for AR s/p TOF Surgery is reasonable in adults with prior repair of
42yr Old Male with Severe AR Mild LV dysfunction s/p TOF -AV Replacement(tissue valve) or AoV plasty- Kyung-Hwan Kim Current Guideline for AR s/p TOF Surgery is reasonable in adults with prior repair of
Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated?
 Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated? RM Suri, V Sharma, JA Dearani, HM Burkhart, RC Daly, LD Joyce, HV Schaff Division of Cardiovascular Surgery, Mayo Clinic, Rochester,
Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated? RM Suri, V Sharma, JA Dearani, HM Burkhart, RC Daly, LD Joyce, HV Schaff Division of Cardiovascular Surgery, Mayo Clinic, Rochester,
Rapid deployment aortic valve replacement for the treatment of severe aortic stenosis in high risk patients. Β. Κόλλιας, Σ. Ματιάτου, Δ. Αγγουράς.
 Rapid deployment aortic valve replacement for the treatment of severe aortic stenosis in high risk patients. Οι βιοπροσθετικές αορτικές βαλβίδες ταχείας έκπτυξης στην αντιµετώπιση της σοβαρής αορτικής
Rapid deployment aortic valve replacement for the treatment of severe aortic stenosis in high risk patients. Οι βιοπροσθετικές αορτικές βαλβίδες ταχείας έκπτυξης στην αντιµετώπιση της σοβαρής αορτικής
How Do I Evaluate a Patient Being Considered for TAVR? Sunday, February 14, :00 11:25 PM 25 min
 2016 ASE State of the Art Echocardiography Course Tucson, AZ How Do I Evaluate a Patient Being Considered for TAVR? Sunday, February 14, 2016 11:00 11:25 PM 25 min 1 M U H A M E D S A R I Ć, M D, P H D
2016 ASE State of the Art Echocardiography Course Tucson, AZ How Do I Evaluate a Patient Being Considered for TAVR? Sunday, February 14, 2016 11:00 11:25 PM 25 min 1 M U H A M E D S A R I Ć, M D, P H D
Surgical AVR: Are there any contraindications? Pyowon Park Samsung Medical Center Seoul, Korea
 Surgical AVR: Are there any contraindications? Pyowon Park Samsung Medical Center Seoul, Korea Contents Decision making in surgical AVR in old age Clinical results of AVR with tissue valve Impact of 19mm
Surgical AVR: Are there any contraindications? Pyowon Park Samsung Medical Center Seoul, Korea Contents Decision making in surgical AVR in old age Clinical results of AVR with tissue valve Impact of 19mm
Kinsing Ko, Thom de Kroon, Najim Kaoui, Bart van Putte, Nabil Saouti. St. Antonius Hospital, Nieuwegein, The Netherlands
 Minimal Invasive Mitral Valve Surgery After Previous Sternotomy Without Aortic Clamping: Short- and Long Term Results of a Single Surgeon Single Institution Kinsing Ko, Thom de Kroon, Najim Kaoui, Bart
Minimal Invasive Mitral Valve Surgery After Previous Sternotomy Without Aortic Clamping: Short- and Long Term Results of a Single Surgeon Single Institution Kinsing Ko, Thom de Kroon, Najim Kaoui, Bart
MINIMALLY INVASIVE AVR
 MINIMALLY INVASIVE AVR MATTHEW S. PANAGIOTOU MD FETCS CARDIAC SURGEON MEDITERRANEAO HOSPITAL MINIMALLY INVASIVE AVR In cardiac surgery Minimally invasive has been defined as a small chest incision that
MINIMALLY INVASIVE AVR MATTHEW S. PANAGIOTOU MD FETCS CARDIAC SURGEON MEDITERRANEAO HOSPITAL MINIMALLY INVASIVE AVR In cardiac surgery Minimally invasive has been defined as a small chest incision that
Minimally invasive aortic valve surgery: new solutions to old problems.
 SCDU DI CARDIOCHIRURGIA Università degli Studi di Torino Ospedale S. Giovanni Battista Direttore: Prof. Mauro Rinaldi Minimally invasive aortic valve surgery: new solutions to old problems. Prof. Mauro
SCDU DI CARDIOCHIRURGIA Università degli Studi di Torino Ospedale S. Giovanni Battista Direttore: Prof. Mauro Rinaldi Minimally invasive aortic valve surgery: new solutions to old problems. Prof. Mauro
2/28/2010. Speakers s name: Paul Chiam. I have the following potential conflicts of interest to report: NONE. Antegrade transvenous transseptal route
 Transcatheter Aortic Valve Implantation Asian perspective Speakers s name: Paul Chiam Paul TL Chiam MBBS, MRCP, FACC I have the following potential conflicts of interest to report: NONE Consultant National
Transcatheter Aortic Valve Implantation Asian perspective Speakers s name: Paul Chiam Paul TL Chiam MBBS, MRCP, FACC I have the following potential conflicts of interest to report: NONE Consultant National
Percutaneous Valve Interventions. Percutaneous Valve Interventions
 Percutaneous Valve Interventions Stanton J. Rowe President, Percutaneous Valve Interventions Edwards is Best Positioned to Capitalize on Percutaneous Valve Opportunities #1 global valve replacement and
Percutaneous Valve Interventions Stanton J. Rowe President, Percutaneous Valve Interventions Edwards is Best Positioned to Capitalize on Percutaneous Valve Opportunities #1 global valve replacement and
CIPG Transcatheter Aortic Valve Replacement- When Is Less, More?
 CIPG 2013 Transcatheter Aortic Valve Replacement- When Is Less, More? James D. Rossen, M.D. Professor of Medicine and Neurosurgery Director, Cardiac Catheterization Laboratory and Interventional Cardiology
CIPG 2013 Transcatheter Aortic Valve Replacement- When Is Less, More? James D. Rossen, M.D. Professor of Medicine and Neurosurgery Director, Cardiac Catheterization Laboratory and Interventional Cardiology
The Ross Procedure: Outcomes at 20 Years
 The Ross Procedure: Outcomes at 20 Years Tirone David Carolyn David Anna Woo Cedric Manlhiot University of Toronto Conflict of Interest None The Ross Procedure 1990 to 2004 212 patients: 66% 34% Mean age:
The Ross Procedure: Outcomes at 20 Years Tirone David Carolyn David Anna Woo Cedric Manlhiot University of Toronto Conflict of Interest None The Ross Procedure 1990 to 2004 212 patients: 66% 34% Mean age:
Aortic valve repair: When and how to employ this novel approach?
 Aortic valve repair: When and how to employ this novel approach? Konstadinos A Plestis, MD System Chief of Cardiac Thoracic and Vascular Surgery Main Line Health Care System Professor Sidney Kimmel Medical
Aortic valve repair: When and how to employ this novel approach? Konstadinos A Plestis, MD System Chief of Cardiac Thoracic and Vascular Surgery Main Line Health Care System Professor Sidney Kimmel Medical
Developments in Valve Surgery
 Developments in Valve Surgery Introduction Will discuss Aortic Valve and Mitral Valve surgery What is a mini valve operation? When do we do traditional valve surgery (SAVR, SMVR) vs. mini valve surgery
Developments in Valve Surgery Introduction Will discuss Aortic Valve and Mitral Valve surgery What is a mini valve operation? When do we do traditional valve surgery (SAVR, SMVR) vs. mini valve surgery
Bicuspid aortic root spared during ascending aorta surgery: an update of long-term results
 Short Communication Bicuspid aortic root spared during ascending aorta surgery: an update of long-term results Marco Russo, Guglielmo Saitto, Paolo Nardi, Fabio Bertoldo, Carlo Bassano, Antonio Scafuri,
Short Communication Bicuspid aortic root spared during ascending aorta surgery: an update of long-term results Marco Russo, Guglielmo Saitto, Paolo Nardi, Fabio Bertoldo, Carlo Bassano, Antonio Scafuri,
Experience with 500 Stentless Aortic Valve Replacements
 Experience with 500 Stentless Aortic Valve Replacements Dimitrios C. Iliopoulos, MD Cardiac Surgeon Ass. Professor of Surgery University of Athens, School of Medicine I declare no conflict of interest
Experience with 500 Stentless Aortic Valve Replacements Dimitrios C. Iliopoulos, MD Cardiac Surgeon Ass. Professor of Surgery University of Athens, School of Medicine I declare no conflict of interest
SOLO SMART. The smart way to return to life. Native-like performance now with stented-like implantability
 SOLO SMART TM The smart way to return to life Native-like performance now with stented-like implantability MANY PATIENTS NEED SUPERIOR HEMODYNAMIC PERFORMANCE TO RETURN TO THEIR NORMAL LIFESTYLE. 2 SOLO
SOLO SMART TM The smart way to return to life Native-like performance now with stented-like implantability MANY PATIENTS NEED SUPERIOR HEMODYNAMIC PERFORMANCE TO RETURN TO THEIR NORMAL LIFESTYLE. 2 SOLO
Hemodynamics Benefit of Supra-Annular Design in Failed Bio-Prosthetic Valves
 Hemodynamics Benefit of Supra-Annular Design in Failed Bio-Prosthetic Valves Speaker's name: I have the following potential conflicts of interest to report: Proctorship for Medtronic Agenda Failure modes
Hemodynamics Benefit of Supra-Annular Design in Failed Bio-Prosthetic Valves Speaker's name: I have the following potential conflicts of interest to report: Proctorship for Medtronic Agenda Failure modes
2017 Cardiovascular Symposium CARDIAC SURGERY UPDATE: SMALLER INCISIONS AND LESS COUMADIN DAVID L. SAINT, MD
 2017 Cardiovascular Symposium CARDIAC SURGERY UPDATE: SMALLER INCISIONS AND LESS COUMADIN DAVID L. SAINT, MD David L Saint M.D. Tallahassee Memorial Hospital Southern Medical Group Division of Cardiothoracic
2017 Cardiovascular Symposium CARDIAC SURGERY UPDATE: SMALLER INCISIONS AND LESS COUMADIN DAVID L. SAINT, MD David L Saint M.D. Tallahassee Memorial Hospital Southern Medical Group Division of Cardiothoracic
Joseph E. Bavaria, M.D. Roberts Measy Professor and Vice Chief CardioVascular Surgery Director: Thoracic Aortic Surgery Program University of
 Joseph E. Bavaria, M.D. Roberts Measy Professor and Vice Chief CardioVascular Surgery Director: Thoracic Aortic Surgery Program University of Pennsylvania, USA North American Valve Repair, Philadelphia
Joseph E. Bavaria, M.D. Roberts Measy Professor and Vice Chief CardioVascular Surgery Director: Thoracic Aortic Surgery Program University of Pennsylvania, USA North American Valve Repair, Philadelphia
When Should We Consider TAVI. (Surgeon s Viewpoint)? Pyowon Park Samsung Medical Center Seoul, Korea
? Pyowon Park Samsung Medical Center Seoul, Korea") When Should We Consider TAVI Procedure in Korea (Surgeon s Viewpoint)? Pyowon Park Samsung Medical Center Seoul, Korea Aortic Stenosis in Korea Rapidly increasing valve disease in Korea Still low incidence
When Should We Consider TAVI Procedure in Korea (Surgeon s Viewpoint)? Pyowon Park Samsung Medical Center Seoul, Korea Aortic Stenosis in Korea Rapidly increasing valve disease in Korea Still low incidence
Indications and Late Results of Aortic Valve Repair
 Indications and Late Results of Aortic Valve Repair Prof. Gebrine El Khoury Department of Cardiovascular and Thoracic Surgery Cliniques St. Luc Brussels, Belgium Aortic Valve Repair Question # 1 Can the
Indications and Late Results of Aortic Valve Repair Prof. Gebrine El Khoury Department of Cardiovascular and Thoracic Surgery Cliniques St. Luc Brussels, Belgium Aortic Valve Repair Question # 1 Can the
Dr Nikolaos Baikoussis
 Dr Nikolaos Baikoussis Cardiac Surgeon Evangelismos General Hospital of Athens, Greece STS database: any procedure not performed with a full sternotomy (FS) and cardiopulmonary bypass (CPB)..(TAVI) Schmitto
Dr Nikolaos Baikoussis Cardiac Surgeon Evangelismos General Hospital of Athens, Greece STS database: any procedure not performed with a full sternotomy (FS) and cardiopulmonary bypass (CPB)..(TAVI) Schmitto
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair?
 TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
Hani K. Najm MD, Msc, FRCSC FACC, FESC President Saudi Society for Cardiac Surgeons Associate Professor of Cardiothoracic Surgery King Abdulaziz
 Hani K. Najm MD, Msc, FRCSC FACC, FESC President Saudi Society for Cardiac Surgeons Associate Professor of Cardiothoracic Surgery King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia Decision process for
Hani K. Najm MD, Msc, FRCSC FACC, FESC President Saudi Society for Cardiac Surgeons Associate Professor of Cardiothoracic Surgery King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia Decision process for
TAVR for Valve-In-Valve. Brian O Neill Assistant Professor of Medicine Department of Medicine, Section of Cardiology
 TAVR for Valve-In-Valve Brian O Neill Assistant Professor of Medicine Department of Medicine, Section of Cardiology Temple Hearth and Vascular Institute Disclosures: Consultant: Cardiac Assist TAVR for
TAVR for Valve-In-Valve Brian O Neill Assistant Professor of Medicine Department of Medicine, Section of Cardiology Temple Hearth and Vascular Institute Disclosures: Consultant: Cardiac Assist TAVR for
Sotirios N. Prapas, M.D., Ph.D, F.E.C.T.S.
 CORONARY ARTERY REVASCULARIZATION WITH MILD AORTIC STENOSIS: STRATEGIES OF TREATMENT 9 th ANNUAL MEETING OF THE EAB SOCIETY, Pravets, Bulgaria, 2012 Sotirios N. Prapas, M.D., Ph.D, F.E.C.T.S. Director
CORONARY ARTERY REVASCULARIZATION WITH MILD AORTIC STENOSIS: STRATEGIES OF TREATMENT 9 th ANNUAL MEETING OF THE EAB SOCIETY, Pravets, Bulgaria, 2012 Sotirios N. Prapas, M.D., Ph.D, F.E.C.T.S. Director
TSDA Boot Camp September 13-16, Introduction to Aortic Valve Surgery. George L. Hicks, Jr., MD
 TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
TAVR or SAVR: Beyond the STS Score
 TAVR or SAVR: Beyond the STS Score Juan Crestanello, MD Division of Cardiac Surgery Lakshmi Prasad Dasi, PhD Department of Biomedical Engineering The Ohio State University Wexner Medical Center 1 Disclosures
TAVR or SAVR: Beyond the STS Score Juan Crestanello, MD Division of Cardiac Surgery Lakshmi Prasad Dasi, PhD Department of Biomedical Engineering The Ohio State University Wexner Medical Center 1 Disclosures
Transcatheter Aortic Valve Implantation. SSVQ November 23, 2012 Centre Mont-Royal 15:40
 Transcatheter Aortic Valve Implantation SSVQ November 23, 2012 Centre Mont-Royal 15:40 Nicolo Piazza MD, PhD, FRCPC, FESC, FACC McGill University Health Center German Heart Center Munich 1 First-in-Human
Transcatheter Aortic Valve Implantation SSVQ November 23, 2012 Centre Mont-Royal 15:40 Nicolo Piazza MD, PhD, FRCPC, FESC, FACC McGill University Health Center German Heart Center Munich 1 First-in-Human
Percutaneous Aortic Valve Implantation. Core-Valve and Cribier-Edwards Update
 Percutaneous Aortic Valve Implantation. Core-Valve and Cribier-Edwards Update T. Lefèvre Natural History of Aortic Stenosois 100 Latent period Survival (%) 80 60 40 20 Symptoms Average Age Death 0 40 50
Percutaneous Aortic Valve Implantation. Core-Valve and Cribier-Edwards Update T. Lefèvre Natural History of Aortic Stenosois 100 Latent period Survival (%) 80 60 40 20 Symptoms Average Age Death 0 40 50
Edwards Transcatheter AVR: Have the Outcomes Changed after CE Approval?
 Edwards Transcatheter AVR: Have the Outcomes Changed after CE Approval? Update from PARTNER EU and SOURCE Registries T. Lefèvre Disclosure Statement Cardiologist Interventional cardiologist 1 st PABV in
Edwards Transcatheter AVR: Have the Outcomes Changed after CE Approval? Update from PARTNER EU and SOURCE Registries T. Lefèvre Disclosure Statement Cardiologist Interventional cardiologist 1 st PABV in
PPM: How to fit a big valve in a small heart
 PPM: How to fit a big valve in a small heart Hani K. Najm MD, Msc, FRCSC, FRCS (Glasgow), FACC, FESC King Abdulaziz Cardiac Centre National Guard Health Affairs Riyadh, Saudi Arabia GHA meeting Muscat
PPM: How to fit a big valve in a small heart Hani K. Najm MD, Msc, FRCSC, FRCS (Glasgow), FACC, FESC King Abdulaziz Cardiac Centre National Guard Health Affairs Riyadh, Saudi Arabia GHA meeting Muscat
Is it a business for the cardiac surgeon?
 TAVI FOR LOW RISK PATIENTS Is it a business for the cardiac surgeon? Augusto D Onofrio Gino Gerosa Department of Cardiac, Thoracic and Vascular Sciences, University of Padua, Italy T A V I Cardiac surgery
TAVI FOR LOW RISK PATIENTS Is it a business for the cardiac surgeon? Augusto D Onofrio Gino Gerosa Department of Cardiac, Thoracic and Vascular Sciences, University of Padua, Italy T A V I Cardiac surgery
Late failure of transcatheter heart valves: An open question
 Late failure of transcatheter heart valves: An open question A comparison with surgically implanted bioprosthetic heart valves. A. Rashid The Cardiothoracic Centre Liverpool, UK. Conflict of Interest Statement
Late failure of transcatheter heart valves: An open question A comparison with surgically implanted bioprosthetic heart valves. A. Rashid The Cardiothoracic Centre Liverpool, UK. Conflict of Interest Statement
How to Avoid Prosthesis-Patient Mismatch
 How to Avoid Prosthesis-Patient Mismatch Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE, FESC Canada Research Chair in Valvular Heart Diseases INSTITUT UNIVERSITAIRE DE CARDIOLOGIE ET DE PNEUMOLOGIE DE QUÉBEC
How to Avoid Prosthesis-Patient Mismatch Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE, FESC Canada Research Chair in Valvular Heart Diseases INSTITUT UNIVERSITAIRE DE CARDIOLOGIE ET DE PNEUMOLOGIE DE QUÉBEC
Transcatheter aortic valves in aortic regurgitation Gry Dahle Dept of Cardiothoracic- and vascular surgery Rikshospitalet, Oslo University Hospital,
 Transcatheter aortic valves in aortic regurgitation Gry Dahle Dept of Cardiothoracic- and vascular surgery Rikshospitalet, Oslo University Hospital, Oslo, Norway Aortic regurgitation Prevalence in Framingham
Transcatheter aortic valves in aortic regurgitation Gry Dahle Dept of Cardiothoracic- and vascular surgery Rikshospitalet, Oslo University Hospital, Oslo, Norway Aortic regurgitation Prevalence in Framingham
TRANSCATHETER AORTIC VALVE IMPLANTATION: PSCC EXPERIENCE DR HUSSEIN ALAMRI PSCC RIYADH
 TRANSCATHETER AORTIC VALVE IMPLANTATION: PSCC EXPERIENCE DR HUSSEIN ALAMRI PSCC RIYADH Available systems: Edwards (TA and TF) and Core valve. INTRODUCTION 3 4% 0f > 65 y. 30 40% of elderly denied surgery,.
TRANSCATHETER AORTIC VALVE IMPLANTATION: PSCC EXPERIENCE DR HUSSEIN ALAMRI PSCC RIYADH Available systems: Edwards (TA and TF) and Core valve. INTRODUCTION 3 4% 0f > 65 y. 30 40% of elderly denied surgery,.
Valve Replacement without a Scalpel Transcatheter Aortic Valve Replacement (TAVR) Charles T. Klodell, M.D.
 Charles T. Klodell, M.D.") Valve Replacement without a Scalpel Transcatheter Aortic Valve Replacement (TAVR) Charles T. Klodell, M.D. Professor, Thoracic and Cardiovascular Surgery University of Florida klodell@surgery.ufl.edu Disclosures
Valve Replacement without a Scalpel Transcatheter Aortic Valve Replacement (TAVR) Charles T. Klodell, M.D. Professor, Thoracic and Cardiovascular Surgery University of Florida klodell@surgery.ufl.edu Disclosures
Incidence and Management of Early Implant Failure after Transcatheter Aortic Valve Implantation
 ESC Congress 2010 28 Aug 2010-01 Sep 2010 Stockholm - Sweden Incidence and Management of Early Implant Failure after Transcatheter Aortic Valve Implantation Gian Paolo Ussia, MD Director of Interventional
ESC Congress 2010 28 Aug 2010-01 Sep 2010 Stockholm - Sweden Incidence and Management of Early Implant Failure after Transcatheter Aortic Valve Implantation Gian Paolo Ussia, MD Director of Interventional
1-YEAR OUTCOMES FROM JOHN WEBB, MD
 1-YEAR OUTCOMES FROM JOHN WEBB, MD ON BEHALF OF THE SAPIEN 3 INVESTIGATORS UNIVERSITY OF BRITISH COLUMBIA VANCOUVER, CANADA Potential conflicts of interest Speaker's name: John Webb I have the following
1-YEAR OUTCOMES FROM JOHN WEBB, MD ON BEHALF OF THE SAPIEN 3 INVESTIGATORS UNIVERSITY OF BRITISH COLUMBIA VANCOUVER, CANADA Potential conflicts of interest Speaker's name: John Webb I have the following
Less Invasive Aortic Valve Surgery
 Less Invasive Aortic Valve Surgery SCTS Brighton 19th March 2013 Andrew Chukwuemeka MD FRCS Consultant Cardiothoracic Surgeon Hammersmith Hospital Imperial College Healthcare NHS Trust Less Invasive Aortic
Less Invasive Aortic Valve Surgery SCTS Brighton 19th March 2013 Andrew Chukwuemeka MD FRCS Consultant Cardiothoracic Surgeon Hammersmith Hospital Imperial College Healthcare NHS Trust Less Invasive Aortic
Thrombocytopenia in Moderate- to High-Risk Sutureless Aortic Valve Replacement
 Korean J Thorac Cardiovasc Surg 2018;51:172-179 ISSN: 2233-601X (Print) ISSN: 2093-6516 (Online) CLINICAL RESEARCH https://doi.org/10.5090/kjtcs.2018.51.3.172 Thrombocytopenia in Moderate- to High-Risk
Korean J Thorac Cardiovasc Surg 2018;51:172-179 ISSN: 2233-601X (Print) ISSN: 2093-6516 (Online) CLINICAL RESEARCH https://doi.org/10.5090/kjtcs.2018.51.3.172 Thrombocytopenia in Moderate- to High-Risk
Aortic valve repair: Techniques and Pitfalls. Allan Stewart, MD Columbia University Medical Center New York, NY
 Aortic valve repair: Techniques and Pitfalls Allan Stewart, MD Columbia University Medical Center New York, NY Take Away Points 1. Valve anatomy is essential to assess repair 2. Unique Decisions with Aneurysm/AI
Aortic valve repair: Techniques and Pitfalls Allan Stewart, MD Columbia University Medical Center New York, NY Take Away Points 1. Valve anatomy is essential to assess repair 2. Unique Decisions with Aneurysm/AI
Results of Aortic Valve Preservation and Repair
 Results of Aortic Valve Preservation and Repair Department of Cardiothoracic and Vascular Surgery Cliniques Universitaires St. Luc Brussels, Belgium Gebrine Elkhoury Institutional experience in AV preservation
Results of Aortic Valve Preservation and Repair Department of Cardiothoracic and Vascular Surgery Cliniques Universitaires St. Luc Brussels, Belgium Gebrine Elkhoury Institutional experience in AV preservation
The Bicuspid AV Surgical Conisiderations
 The Bicuspid AV Surgical Conisiderations Ehud Raanani, MD Cardiothoracic Surgery, Sheba Medical Center Sackler School of Medicine, Tel Aviv University MAY 15, 2014 Homburg BAV Repair Congenital variations
The Bicuspid AV Surgical Conisiderations Ehud Raanani, MD Cardiothoracic Surgery, Sheba Medical Center Sackler School of Medicine, Tel Aviv University MAY 15, 2014 Homburg BAV Repair Congenital variations
Joseph E. Bavaria, M.D. Roberts Measy Professor and Vice Chief CardioVascular Surgery Director: Thoracic Aortic Surgery Program University of
 Joseph E. Bavaria, M.D. Roberts Measy Professor and Vice Chief CardioVascular Surgery Director: Thoracic Aortic Surgery Program University of Pennsylvania, USA AVRS Philadelphia Sept 2016 Pictures courtesy
Joseph E. Bavaria, M.D. Roberts Measy Professor and Vice Chief CardioVascular Surgery Director: Thoracic Aortic Surgery Program University of Pennsylvania, USA AVRS Philadelphia Sept 2016 Pictures courtesy
Repair or Replacement
 Surgical intervention post MitraClip Device: Repair or Replacement Saudi Heart Association, February 21-24 Rüdiger Lange, MD, PhD Nicolo Piazza, MD, FRCPC, FESC German Heart Center, Munich, Germany Division
Surgical intervention post MitraClip Device: Repair or Replacement Saudi Heart Association, February 21-24 Rüdiger Lange, MD, PhD Nicolo Piazza, MD, FRCPC, FESC German Heart Center, Munich, Germany Division
MINIMALLY INVASIVE MITRAL VALVE SURGERY. Rohinton J. Morris, MD Chief, Cardiothoracic Surgery Jefferson University and Health Systems
 MINIMALLY INVASIVE MITRAL VALVE SURGERY Rohinton J. Morris, MD Chief, Cardiothoracic Surgery Jefferson University and Health Systems OVERVIEW History Anatomy Indications Techniques Variants Outcomes &
MINIMALLY INVASIVE MITRAL VALVE SURGERY Rohinton J. Morris, MD Chief, Cardiothoracic Surgery Jefferson University and Health Systems OVERVIEW History Anatomy Indications Techniques Variants Outcomes &
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV?
 Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Extension to medium and low risk patients? Friedrich Eckstein University Hospital Basel
 TAVI CON Extension to medium and low risk patients? Friedrich Eckstein University Hospital Basel Extension to medium and low risk patients? In octogenerians already reality in most of the swiss clinics!?
TAVI CON Extension to medium and low risk patients? Friedrich Eckstein University Hospital Basel Extension to medium and low risk patients? In octogenerians already reality in most of the swiss clinics!?
Prof. Dr. Thomas Walther. TAVI in ascending aorta / aortic root dilatation
 Prof. Dr. Thomas Walther TAVI in ascending aorta / aortic root dilatation nn AorticStenosis - Guidelines TAVI and aortic aneurysm? Few data published. EJCTS 2014;46:228-33 TAVI and aortic aneurysm? Few
Prof. Dr. Thomas Walther TAVI in ascending aorta / aortic root dilatation nn AorticStenosis - Guidelines TAVI and aortic aneurysm? Few data published. EJCTS 2014;46:228-33 TAVI and aortic aneurysm? Few
New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor. Cardiothoracic Radiology
 New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor Cardiothoracic Radiology Disclosure I have no disclosure pertinent to this presentation.
New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor Cardiothoracic Radiology Disclosure I have no disclosure pertinent to this presentation.
Long-term results (22 years) of the Ross Operation a single institutional experience
 of the Ross Operation a single institutional experience") Long-term results (22 years) of the Ross Operation a single institutional experience Authors: Costa FDA, Schnorr GM, Veloso M,Calixto A, Colatusso D, Balbi EM, Torres R, Ferreira ADA, Colatusso C Department
Long-term results (22 years) of the Ross Operation a single institutional experience Authors: Costa FDA, Schnorr GM, Veloso M,Calixto A, Colatusso D, Balbi EM, Torres R, Ferreira ADA, Colatusso C Department
Re-do aortic valve replacement after previous homograft aortic root replacement
 Re-do aortic valve replacement after previous homograft aortic root replacement Jullien Gaer, Toufan Bahrami, Fabio de Robertis, Ahmed Abdulsalam, John Pepper, NHS Foundation Trust, UK Professor Sir Magdi
Re-do aortic valve replacement after previous homograft aortic root replacement Jullien Gaer, Toufan Bahrami, Fabio de Robertis, Ahmed Abdulsalam, John Pepper, NHS Foundation Trust, UK Professor Sir Magdi
Hani K. Najm MD, Msc, FRCSC, FRCS (Glasgow), FACC, FESC President of Saudi Heart Association King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia.
, FACC, FESC President of Saudi Heart Association King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia.") Hani K. Najm MD, Msc, FRCSC, FRCS (Glasgow), FACC, FESC President of Saudi Heart Association King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia. Decision process for Management of any valve Timing Feasibility
Hani K. Najm MD, Msc, FRCSC, FRCS (Glasgow), FACC, FESC President of Saudi Heart Association King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia. Decision process for Management of any valve Timing Feasibility
Minimally invasive aortic valve surgery: state of the art and future directions
 Keynote Lecture Series Minimally invasive aortic valve surgery: state of the art and future directions Mattia Glauber, Matteo Ferrarini, Antonio Miceli Cardiac Surgery and Great Vessels Department, Istituto
Keynote Lecture Series Minimally invasive aortic valve surgery: state of the art and future directions Mattia Glauber, Matteo Ferrarini, Antonio Miceli Cardiac Surgery and Great Vessels Department, Istituto
TAVR SPRING 2017 The evolution of TAVR
 TAVR SPRING 2017 The evolution of TAVR Matthew Johnson, MD Disclosers None Evolution of the Balloon- Expandable Transcatheter Valves Cribier 2002 SAPIEN 2006 SAPIEN XT 2009 SAPIEN 3 2013 * Sheath compatibility
TAVR SPRING 2017 The evolution of TAVR Matthew Johnson, MD Disclosers None Evolution of the Balloon- Expandable Transcatheter Valves Cribier 2002 SAPIEN 2006 SAPIEN XT 2009 SAPIEN 3 2013 * Sheath compatibility
Aortic valve implantation using the femoral and apical access: a single center experience.
 Aortic valve implantation using the femoral and apical access: a single center experience. R. Hoffmann, K. Brehmer, R. Koos, R. Autschbach, N. Marx, G. Dohmen Rainer Hoffmann, University Aachen, Germany
Aortic valve implantation using the femoral and apical access: a single center experience. R. Hoffmann, K. Brehmer, R. Koos, R. Autschbach, N. Marx, G. Dohmen Rainer Hoffmann, University Aachen, Germany
CARDIOCHIRURGIA MINI-INVASIVA: INVASIVA: efficacia per il paziente efficienza per la sanita. Dott. Davide Ricci
 CARDIOCHIRURGIA MINI-INVASIVA: INVASIVA: efficacia per il paziente efficienza per la sanita Dott. Davide Ricci SC Cardiochirurgia U Universita degli Studi di Torino Minimally Invasive Surgical approaches
CARDIOCHIRURGIA MINI-INVASIVA: INVASIVA: efficacia per il paziente efficienza per la sanita Dott. Davide Ricci SC Cardiochirurgia U Universita degli Studi di Torino Minimally Invasive Surgical approaches
Results of Transapical Valves. A.P. Kappetein Dept Cardio-thoracic surgery
 Results of Transapical Valves A.P. Kappetein Dept Cardio-thoracic surgery Rotterda am, The Netherlands 2002 FIM 2003 2005 2006 2010 THV THV Cribier-Edwards Edwards Edwards Sapien Sapien XT Bovine pericardium
Results of Transapical Valves A.P. Kappetein Dept Cardio-thoracic surgery Rotterda am, The Netherlands 2002 FIM 2003 2005 2006 2010 THV THV Cribier-Edwards Edwards Edwards Sapien Sapien XT Bovine pericardium
Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data
 Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data Echo Florida 2013 Jonathan J. Passeri, M.D. Co-Director, Heart Valve Program Director,
Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data Echo Florida 2013 Jonathan J. Passeri, M.D. Co-Director, Heart Valve Program Director,
Aortic stenosis (AS) is the most common valvular heart
 is the most common valvular heart") REVIEW ARTICLE Current Clinical Evidence on Rapid Deployment Aortic Valve Replacement Sutureless Aortic Bioprostheses Glenn R. Barnhart, MD* and Malakh Lal Shrestha, MBBS, PhDÞ Abstract: Aortic stenosis
REVIEW ARTICLE Current Clinical Evidence on Rapid Deployment Aortic Valve Replacement Sutureless Aortic Bioprostheses Glenn R. Barnhart, MD* and Malakh Lal Shrestha, MBBS, PhDÞ Abstract: Aortic stenosis
TAVI IN BICUSPID AOV AND VALVE-IN-VALVE
 TAVI IN BICUSPID AOV AND VALVE-IN-VALVE Petros S. Dardas, MD, FESC St Lukes Hospital Thessaloniki, GREECE 6o ΣΥΝΕΔΡΙΟ ΔΙΑΚΑΘΕΤΗΡΙΑΚΗΣ ΘΕΡΑΠΕΙΑΣ ΚΑΡΔΙΑΚΩΝ ΒΑΛΒΙΔΟΠΑΘΕΙΩΝ ΑΘΗΝΑ 2017 BICUSPID AOV Surgical
TAVI IN BICUSPID AOV AND VALVE-IN-VALVE Petros S. Dardas, MD, FESC St Lukes Hospital Thessaloniki, GREECE 6o ΣΥΝΕΔΡΙΟ ΔΙΑΚΑΘΕΤΗΡΙΑΚΗΣ ΘΕΡΑΠΕΙΑΣ ΚΑΡΔΙΑΚΩΝ ΒΑΛΒΙΔΟΠΑΘΕΙΩΝ ΑΘΗΝΑ 2017 BICUSPID AOV Surgical
Transcatheter Mitral Valve Replacement How Close Are We?
 Transcatheter Mitral Valve Replacement How Close Are We? Gregory Pavlides, MD, PhD, FACC, FESC Professor of Medicine Miscia Chair of Interventional Cardiology Director, Cardiac Catheterization Laboratories,
Transcatheter Mitral Valve Replacement How Close Are We? Gregory Pavlides, MD, PhD, FACC, FESC Professor of Medicine Miscia Chair of Interventional Cardiology Director, Cardiac Catheterization Laboratories,
Transcatheter Aortic Valve Implantation Management of risks and complications
 Transcatheter Aortic Valve Implantation Management of risks and complications TAVI Summit, Seoul, Korea, Spetember 3rd, 2011 Alain Cribier University of Rouen, France Complications of TAVI Depending on
Transcatheter Aortic Valve Implantation Management of risks and complications TAVI Summit, Seoul, Korea, Spetember 3rd, 2011 Alain Cribier University of Rouen, France Complications of TAVI Depending on
Late secondary TR after left sided heart disease correction: is it predictibale and preventable
 Late secondary TR after left sided heart disease correction: is it predictibale and preventable Gilles D. Dreyfus Professor of Cardiothoracic surgery Nath J, et al. JACC 2004 PREDICT Incidence of secondary
Late secondary TR after left sided heart disease correction: is it predictibale and preventable Gilles D. Dreyfus Professor of Cardiothoracic surgery Nath J, et al. JACC 2004 PREDICT Incidence of secondary
Really Less-Invasive Trans-apical Beating Heart Mitral Valve Repair: Which Patients?
 Really Less-Invasive Trans-apical Beating Heart Mitral Valve Repair: Which Patients? David H. Adams, MD Cardiac Surgeon-in-Chief Mount Sinai Health System Marie Josée and Henry R. Kravis Professor and
Really Less-Invasive Trans-apical Beating Heart Mitral Valve Repair: Which Patients? David H. Adams, MD Cardiac Surgeon-in-Chief Mount Sinai Health System Marie Josée and Henry R. Kravis Professor and
Transcatheter aortic valve implantation for severe aortic valve stenosis with the ACURATE neo2 valve system: 30-day safety and performance outcomes
 All cited trademarks are the property of their respective owners. CAUTION: The law restricts these devices to sale by or on the order of a physician. Indications, contraindications, warnings and instructions
All cited trademarks are the property of their respective owners. CAUTION: The law restricts these devices to sale by or on the order of a physician. Indications, contraindications, warnings and instructions
Outcomes of Mitral Valve Repair for Mitral Regurgitation Due to Degenerative Disease
 Outcomes of Mitral Valve Repair for Mitral Regurgitation Due to Degenerative Disease TIRONE E. DAVID, MD ; SEMIN THORAC CARDIOVASC SURG 19:116-120c 2007 ELSEVIER INC. PRESENTED BY INTERN 許士盟 Mitral valve
Outcomes of Mitral Valve Repair for Mitral Regurgitation Due to Degenerative Disease TIRONE E. DAVID, MD ; SEMIN THORAC CARDIOVASC SURG 19:116-120c 2007 ELSEVIER INC. PRESENTED BY INTERN 許士盟 Mitral valve
Interventional procedures guidance Published: 26 July 2017 nice.org.uk/guidance/ipg586
 Transcatheter aortic valve implantation for aortic stenosis Interventional procedures guidance Published: 26 July 17 nice.org.uk/guidance/ipg586 Your responsibility This guidance represents the view of
Transcatheter aortic valve implantation for aortic stenosis Interventional procedures guidance Published: 26 July 17 nice.org.uk/guidance/ipg586 Your responsibility This guidance represents the view of
Aortic Stenosis Background and Breakthroughs in Treatment: TAVR Update
 Aortic Stenosis Background and Breakthroughs in Treatment: TAVR Update Howard J Broder MD Interventional Cardiology DaVita Medical Group/ Healthcare Partners Cardiology Disclosures for Howard J Broder
Aortic Stenosis Background and Breakthroughs in Treatment: TAVR Update Howard J Broder MD Interventional Cardiology DaVita Medical Group/ Healthcare Partners Cardiology Disclosures for Howard J Broder
Prince Sultan Cardiac Center Experience Riyadh, Saudi Arabia
 Transcatheter Transapical Aortic Valve Implantation Prince Sultan Cardiac Center Experience Riyadh, Saudi Arabia Ahmed Elwatidy, MD,PhD, FRCS S Kassab, MD,S Ahmari, MD, H Amri, MD, H Ismail, MD, A Calafiori,
Transcatheter Transapical Aortic Valve Implantation Prince Sultan Cardiac Center Experience Riyadh, Saudi Arabia Ahmed Elwatidy, MD,PhD, FRCS S Kassab, MD,S Ahmari, MD, H Amri, MD, H Ismail, MD, A Calafiori,
8. Nov, 2018 Athens Clossroad 2018, Athens GREEK
 8. Nov, 2018 Athens Clossroad 2018, Athens GREEK Stent Less Bio prosthesis Aortic Valve replacement with Minimally Invasive Approach ~ Indication for the 1 st Surgical Aortic Valve Treatment Considering
8. Nov, 2018 Athens Clossroad 2018, Athens GREEK Stent Less Bio prosthesis Aortic Valve replacement with Minimally Invasive Approach ~ Indication for the 1 st Surgical Aortic Valve Treatment Considering
Reconstruction of the Aortic Valve and Root A Practical approach Failures after aortic valve repair. Diana Aicher. September 16 th -18 th 2015
 Reconstruction of the Aortic Valve and Root A Practical approach Failures after aortic valve repair Diana Aicher September 16 th -18 th 2015 Classification of failures- root repair 51/810 acute/ intraoperative
Reconstruction of the Aortic Valve and Root A Practical approach Failures after aortic valve repair Diana Aicher September 16 th -18 th 2015 Classification of failures- root repair 51/810 acute/ intraoperative
Appropriate Use of TAVR - now and in the future. A Surgeon s Perspective. Neil Moat Royal Brompton Hospital, London, UK
 Appropriate Use of TAVR - now and in the future A Surgeon s Perspective Neil Moat Royal Brompton Hospital, London, UK Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner
Appropriate Use of TAVR - now and in the future A Surgeon s Perspective Neil Moat Royal Brompton Hospital, London, UK Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner
Aortic valve reconstruction using the Ozaki technique, when and in whom? Mr Cesare Quarto MD PhD Consultant Cardiac Surgeon Royal Brompton Hospital
 Aortic valve reconstruction using the Ozaki technique, when and in whom? Mr Cesare Quarto MD PhD Consultant Cardiac Surgeon Royal Brompton Hospital London Disclosure of Interest Cesare Quarto I have the
Aortic valve reconstruction using the Ozaki technique, when and in whom? Mr Cesare Quarto MD PhD Consultant Cardiac Surgeon Royal Brompton Hospital London Disclosure of Interest Cesare Quarto I have the
Decellularization of Aortic Homografts: South American and European Current Experience
 Department of Cardiac Surgery Instituto de Neurologia e Cardiologia de Curitiba (INC-Cardio) Decellularization of Aortic Homografts: South American and European Current Experience Francisco Diniz Affonso
Department of Cardiac Surgery Instituto de Neurologia e Cardiologia de Curitiba (INC-Cardio) Decellularization of Aortic Homografts: South American and European Current Experience Francisco Diniz Affonso
Interventional procedures guidance Published: 26 September 2014 nice.org.uk/guidance/ipg504
 Transcatheter valve-in-valve e implantation for aortic bioprosthetic valve dysfunction Interventional procedures guidance Published: 26 September 2014 nice.org.uk/guidance/ipg504 Your responsibility This
Transcatheter valve-in-valve e implantation for aortic bioprosthetic valve dysfunction Interventional procedures guidance Published: 26 September 2014 nice.org.uk/guidance/ipg504 Your responsibility This
After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients?
 After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients? Vinod H. Thourani, MD Professor of Surgery and Medicine Emory University Disclosure Statement of Financial
After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients? Vinod H. Thourani, MD Professor of Surgery and Medicine Emory University Disclosure Statement of Financial
APOLLO TMVR Trial Update: Case Presentation
 APOLLO TMVR Trial Update: Case Presentation Anelechi Anyanwu, MD, MSc, FRCS-CTh Professor and Vice-Chairman Department of Cardiovascular Surgery Icahn School of Medicine at Mount Sinai New York, NY Disclosure
APOLLO TMVR Trial Update: Case Presentation Anelechi Anyanwu, MD, MSc, FRCS-CTh Professor and Vice-Chairman Department of Cardiovascular Surgery Icahn School of Medicine at Mount Sinai New York, NY Disclosure
Policy Specific Section: March 30, 2012 March 7, 2013
 Medical Policy Transcatheter Aortic Valve Replacement for Aortic Stenosis Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Surgery Original Policy Date: Effective Date:
Medical Policy Transcatheter Aortic Valve Replacement for Aortic Stenosis Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Surgery Original Policy Date: Effective Date:
Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM
 The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
Aortic valve replacement with sutureless and rapid deployment aortic valve prostheses
 Symposium: Transcatheter aortic valve implantation Guest Editor: Prof. Khalil Fattouch Journal of Geriatric Cardiology (2016) 13: 504 510 2016 JGC All rights reserved; www.jgc301.com Open Access Aortic
Symposium: Transcatheter aortic valve implantation Guest Editor: Prof. Khalil Fattouch Journal of Geriatric Cardiology (2016) 13: 504 510 2016 JGC All rights reserved; www.jgc301.com Open Access Aortic
Indication, Timing, Assessment and Update on TAVI
 Indication, Timing, Assessment and Update on TAVI Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Starr- Edwards Mechanical
Indication, Timing, Assessment and Update on TAVI Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Starr- Edwards Mechanical
Andrzej Ochala, MD Medical University of Silesia, Katowice, Poland
 Andrzej Ochala, MD Medical University of Silesia, Katowice, Poland Bicuspid aortic valve o Most common congenital heart disease in adults (1% - 2%) o AS is the most common complication of BAV o Patophysiology
Andrzej Ochala, MD Medical University of Silesia, Katowice, Poland Bicuspid aortic valve o Most common congenital heart disease in adults (1% - 2%) o AS is the most common complication of BAV o Patophysiology
Carpentier-Edwards Pericardial Valve in the Aortic Position: 25-Years Experience
 SURGERY: The Annals of Thoracic Surgery CME Program is located online at http://www.annalsthoracicsurgery.org/cme/ home. To take the CME activity related to this article, you must have either an STS member
SURGERY: The Annals of Thoracic Surgery CME Program is located online at http://www.annalsthoracicsurgery.org/cme/ home. To take the CME activity related to this article, you must have either an STS member
Dr.ssa Loredana Iannetta. Centro Cardiologico Monzino
 Dr.ssa Loredana Iannetta Centro Cardiologico Monzino Bicuspid aortic valve BAV is the most common congenital cardiac anomaly. Estimated incidence is 2% in general population. 4:1 male predominance. Frequency
Dr.ssa Loredana Iannetta Centro Cardiologico Monzino Bicuspid aortic valve BAV is the most common congenital cardiac anomaly. Estimated incidence is 2% in general population. 4:1 male predominance. Frequency
2017 ESC/EACTS Guidelines for the management of valvular heart disease
 2017 ESC/EACTS Guidelines for the management of valvular heart disease Prof. Fausto J. Pinto, FESC, FACC Immediate ESC Past President Head, Cardiology Dpt/ University Hospital Sta Maria-HPV University
2017 ESC/EACTS Guidelines for the management of valvular heart disease Prof. Fausto J. Pinto, FESC, FACC Immediate ESC Past President Head, Cardiology Dpt/ University Hospital Sta Maria-HPV University
TAVI: Transapical Procedures
 Cardiology Update Davos TAVI: Transapical Procedures Volkmar Falk, MD University Hospital Zürich TA-AVI: antegrade, simple, safe The front door approach! Transapical TAVI Technical advantages of TA approach
Cardiology Update Davos TAVI: Transapical Procedures Volkmar Falk, MD University Hospital Zürich TA-AVI: antegrade, simple, safe The front door approach! Transapical TAVI Technical advantages of TA approach
Ian T. Meredith AM. MBBS, PhD, FRACP, FCSANZ, FACC, FAPSIC. Monash HEART, Monash Health & Monash University Melbourne, Australia
 Two-Year Outcomes With the Fully Repositionable and Retrievable Lotus Transcatheter Aortic Replacement Valve in 120 High-Risk Surgical Patients With Severe Aortic Stenosis: Results From the REPRISE II
Two-Year Outcomes With the Fully Repositionable and Retrievable Lotus Transcatheter Aortic Replacement Valve in 120 High-Risk Surgical Patients With Severe Aortic Stenosis: Results From the REPRISE II
Transcatheter Aortic Valve Replacement with Evolut-R
 Transcatheter Aortic Valve Replacement with Evolut-R Department of Transcatheter Heart Valves and 2 nd Cardiothoracic Surgery Clinic K. Spargias, M.Chrissoheris, A.Halapas, I. Nikolaou, S.Pattakos Disclosures
Transcatheter Aortic Valve Replacement with Evolut-R Department of Transcatheter Heart Valves and 2 nd Cardiothoracic Surgery Clinic K. Spargias, M.Chrissoheris, A.Halapas, I. Nikolaou, S.Pattakos Disclosures
Lessons From The Computer Model and How We Do Root Replacement
 Lessons From The Computer Model and How We Do Root Replacement Ehud Raanani, MD Cardiac Surgery Leviev Cardiothoracic and Vascular Center Sheba Medical Center Sackler School of Medicine, Tel Aviv University
Lessons From The Computer Model and How We Do Root Replacement Ehud Raanani, MD Cardiac Surgery Leviev Cardiothoracic and Vascular Center Sheba Medical Center Sackler School of Medicine, Tel Aviv University
Transcatheter Aortic Valve Implantation Present Status and Perspectives
 Transcatheter Aortic Valve Implantation Present Status and Perspectives Angioplasty Summit TCTAP 2010 Alain Cribier, MD University of Rouen, France Transcatheter Aortic Valve Implantation has entered the
Transcatheter Aortic Valve Implantation Present Status and Perspectives Angioplasty Summit TCTAP 2010 Alain Cribier, MD University of Rouen, France Transcatheter Aortic Valve Implantation has entered the
The Bicuspid AV Surgical Considerations
 The Bicuspid AV Surgical Considerations Ehud Raanani, MD Cardiothoracic Surgery, Sheba Medical Center Sackler School of Medicine, Tel Aviv University September 12, 2014 Homburg BAV Repair Congenital variations
The Bicuspid AV Surgical Considerations Ehud Raanani, MD Cardiothoracic Surgery, Sheba Medical Center Sackler School of Medicine, Tel Aviv University September 12, 2014 Homburg BAV Repair Congenital variations