The Role of an Interventional Pulmonologist in Management of Complications of Thoracic Malignancies
|
|
|
- Hollie Dickerson
- 6 years ago
- Views:
Transcription

1 Canadian Association of General Practitioners in Oncology 2015 The Role of an Interventional Pulmonologist in Management of Complications of Thoracic Malignancies Kayvan Amjadi MD, FRCPC Director, Interventional Pulmonology October 2 nd, 2015
2 Disclosures Advisory Committee Carefusion PFM Medical Avantage
3 Objectives Discuss the role of an Interventional Respirologist in management of thoracic oncological emergencies Pleural Disease Parenchymal Disease Central Airway Disease

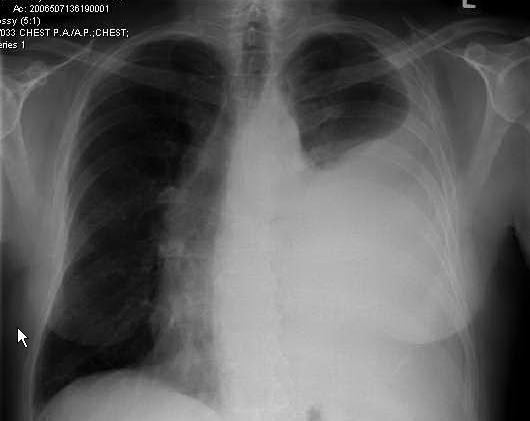
4 White-out of a hemithorax 70 y.o male with renal cancer Progressive SOBOE Now SOB at rest No infectious, cardiac issues No hemoptysis, hoarseness, pleuritic chest pain

5 Post Right Chronic Indwelling Catheter Insertion (7L)
6 Pleural Physiology Pleural Pressure Ppl Determined by the elastic properties of the lung and the chest wall FRC ( 3 to 5 cmh 2 O) TLC ( 30 cmh 2 O) Vertical pleural pressure gradient Pleural pressure decreases by 0.5 cmh 2 O per centimeter of vertical distance above the lung base (viscous flow theory) Higgins and Doelken Clin Chest Med 2006; 27:

7 When Pleural Fluid Enters Pleural Space There would be a gradual increase in intra pleural pressure Compresses the underlying lung Exerts pressure on chest wall Exerts pressure on the mediastinum Depresses the diaphragm Neuromechanichal dissociation
8 Pleural Physiology Improvement in respiratory status post drainage of the effusion depends on Re expansion of the lung Normalization of intra pleural pressure Functional capacity of the re expanded lung

9 Pleural Physiology Un expandable lung (40%) Endobronchial Obstruction Severe Parenchymal Fibrosis Lymphangitic ca Visceral Pleural Restriction Trapped lung Lung entrapment
10 Pleural Physiology As pleural fluid is drained, the drop in pleural pressure is dependent on whether the lung is Expandable (a/w clinical improvement) Un expandable (rarely improve)
11 Pleural pressure measurements Hepatic hydrothorax PEL 3.0 cm H 2 O/L Trapped lung with ve opening pressure and a steep slope. PEL 216 cm H 2 O/L Entrapped lung. PEL during first 1250 ml is normal, but then the elastance increases to 22 cm H 2 O/L Doelken et al., Chest 2004; 126:
12 Lung Entrapment

13 Entrapped Lung

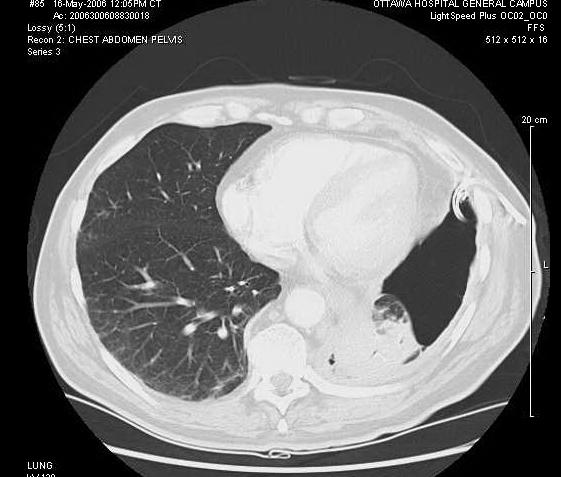
14 Case of Pleural Effusion 54 y.o male with Adeno ca Diffuse lymphangitic ca C/o progressive SOBOE and now requiring O 2 at rest. Referred for drainage of moderated R pleural effusion


15 CT chest post drainage of effusion
16 Drainage of effusion does not lead to improvement Patient denied any benefit from drainage of 1.2 L of effusion Within 24 hours Progressively more SOB Increased FiO 2 requirements (100% non rebreather) Hypotensive (89/52, HR=104/min, sinus)
17 Pleural Physiology Thoracentesis related complications Procedural Bleeding, nerve injury, infection, PTX Re expansion of the lung Cough Chest tightness Re perfusion of the lung Hypotension Re expansion pulmonary edema (RPE)

18 Re-expansion Pulmonary Edema
19 RPE Clinical syndrome characterized by Development of unilateral (non cardiogenic) pulmonary edema In a lung that has been re inflated rapidly After variable period of collapse Pleural effusion Pneumothorax Clinical picture varies Asymptomatic (radiographic) Variable degree of hypoxia May require mechanical ventilation or Death Pneumothorax (Lancet 1979; 1: )


20 Radiographic appearance of RPE (J Thorac Dis 2014;6: )


21 Radiographic appearance of RPE (J Thorac Dis 2014;6: )
22 RPE Pathophysiology Unclear May be related to Duration of lung collapse Application of excessive ve pleural pressure Miller et al, Am Rev Respir Dis 1973; 108: Pavlin and Cheney. J Appl Physiol 1979; 46: Size of the effusion Re perfusion injury Leaky vessels» Pavlin et al., Am Rev Respir Dis 1981; 124: » Pavlin DJ. Chest 1986; 89:2 3» Pavlin et al., J Appl Physiol 1987; 62: (FiO 2 0.4)» Jackson et al., Amm Rev Respir Dis 1988; 137: (Anti oxidants) Elevated levels of IL 8, leukotriene B4» Nakamura et al., Am J Respir Crit Care Med 1994; 149:
23 Therapy for RPE Therapy Supportive O 2, CPAP, mechanical ventilation? Benefit from Diuretics, albumin infusion

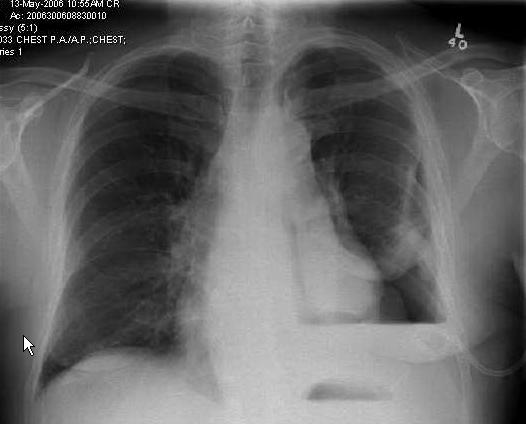
24 CXR 24 hours post catheter insertion


25 CT-PE ve for embolus
 Chemo/Rads 2005 RA Right hip replacement Recurrent chest infections since therapy October 16 th,")
26 Sudden Onset Dyspnea 57 year old male presents to Emergency Department Dec/1 st /06 sudden onset of shortness of breath after a coughing spell Past history of RUL NSCLC (SVCO) Chemo/Rads 2005 RA Right hip replacement Recurrent chest infections since therapy October 16 th, 2006

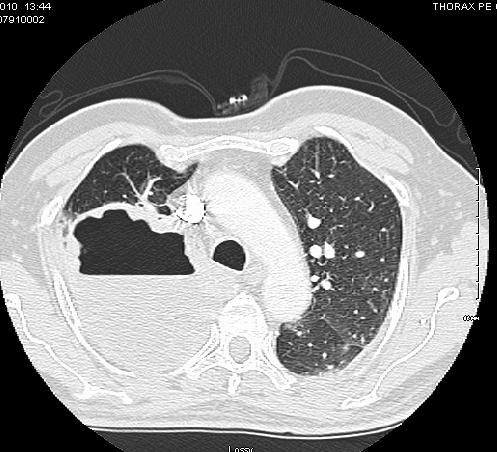
27 Dec 1 st, 2006

28 Post Chest Tube placement

29 Jan/25/2007 post pleurodesis x 3, 8 weeks of hospitalization and prior to d/c

30 Feb 2 nd, 2007 return to ED

31 Post Insertion of Pleurx Catheter and suction

32 Follow-up as outpatient, Intermittent drainage

33 May 22 nd, 2009 presents with fever, cough, SOB

34 May 25 th, 2009 progresses to ARDS
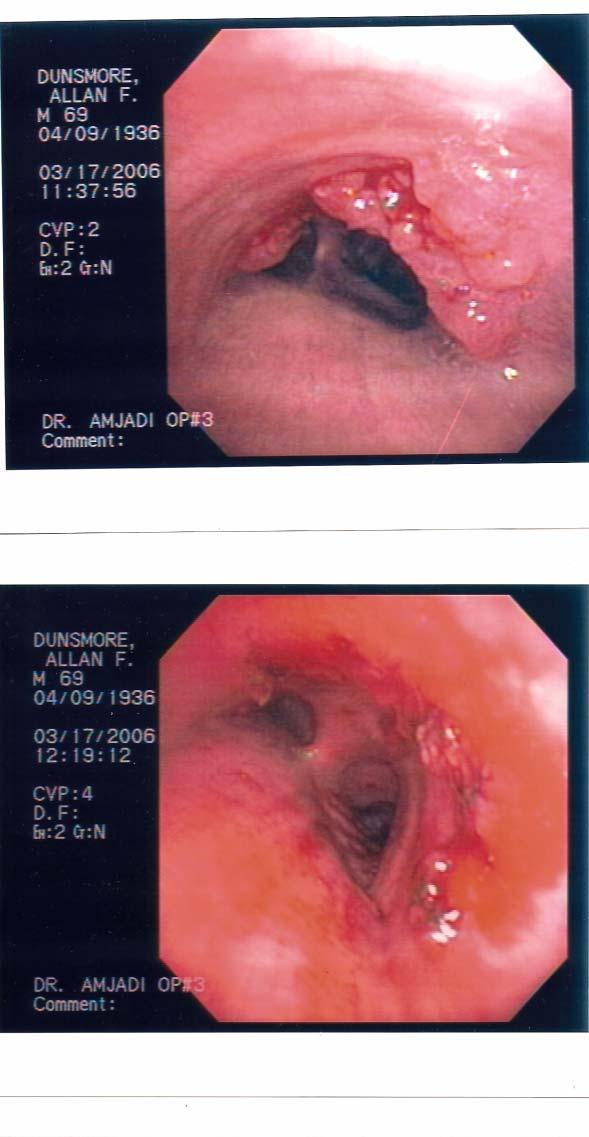
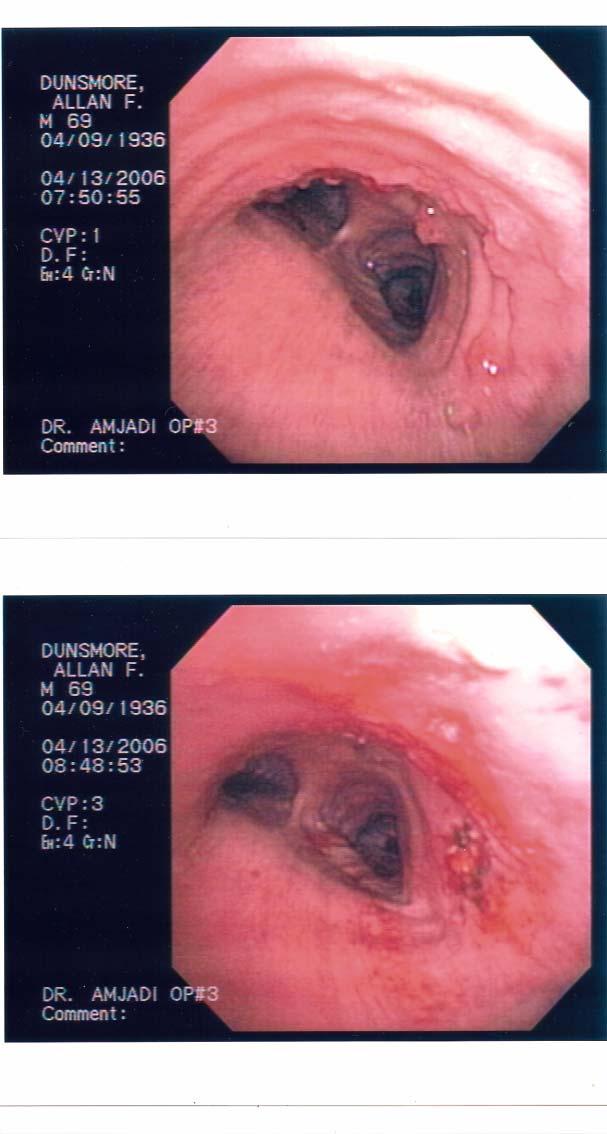
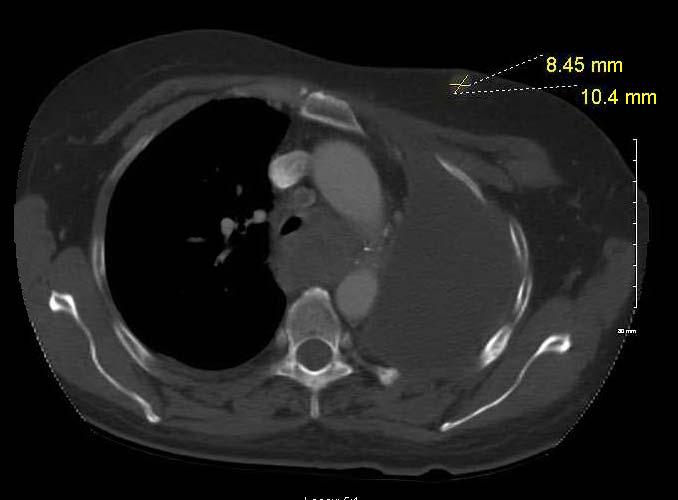
35 Persistent Fever and Hemoptysis 66 y.o male with metastatic Right NSCLC Completed palliative Radiation therapy 6/52 ago Persistent, productive, foul smelling cough, moderate hemoptysis, fever, 15 lb weight loss, elevated WBC, air fluid level in cavity despite 4/52 of IV Pip/Tazo Meropenem Clindamycin

36 Persistent Fever and Hemoptysis


37 Persistent Fever and Hemoptysis Patient continued to decline despite antibiotics Drainage of the infected cavity was requested Embolization of the feeding bronchial arteries to the RUL was organized Bronchoscopy was performed postembolization
38 Persistent Fever and Hemoptysis Bronchoscopy was performed with the aim to create an opening from the cavity into the central airways Using laser/cautery Facilitate emptying of the cavity Administer intra cavitary antibiotics or antifungal Left a catheter in the cavity Administered Intra cavitary Clindamycin Cultures from the cavity grew Stomatococcus Mucilaginosa No need for Ampho B


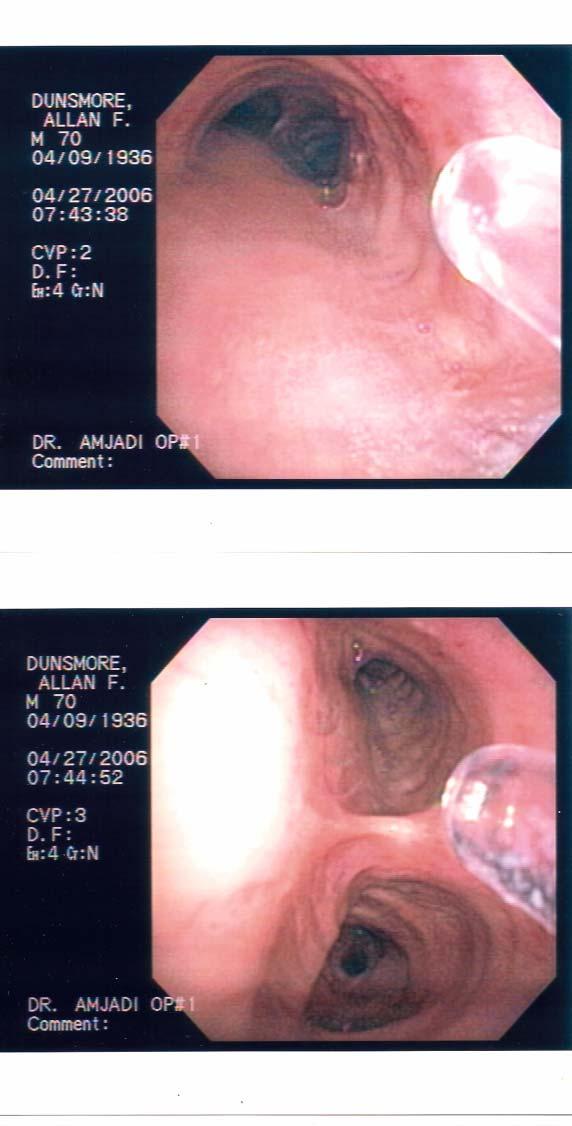
39 Post drainage of cavity


40 Drainage of cavity

41 Post Procedure Patient defervesced within 48 hours Was discharged home 4 days later Was able to start chemotherapy 4 months later, no obvious cavity

42 Sudden Onset of Dyspnea 70 y.o male History of metastatic colon ca Respiratory failure

43 Post thoracentesis consult was placed for management of pneumothorax



44

45 Post Tumor debulking and airway stent
46 Central Airway Obstruction Central airway obstruction (CAO), can result from a variety of disease processes and is a cause of significant morbidity and mortality It is estimated that 20 30% of patients with lung cancer will develop complications associated with airway obstruction Atelectasis Pneumonia Dyspnea Up to 40% of lung cancer deaths may be attributed to locoregional disease. Noppen et al., Acta Clin Belg 1997; 52:371
47 Therapeutic Procedures Laser Electrocautery Argon Plasma Coagulation (APC) Cryotherapy Brachytherapy Photodynamic Therapy (PDT) Airway Stents
48 Therapeutic Procedures The choice of intervention is dictated by Nature of the underlying problem Patient s stability Overall prognosis Patient s quality of life Particular expertise of the physician Available technology


49 Therapeutic Procedures: Endoluminal disease


50 Therapeutic Procedures: Extrinsic Compression
51 Therapeutic Procedures



52 Modified Y Stent


53 Training in Interventional Pulmnology

54 When you can t breath, nothing else matters (with permission from patient)
55 Study (N) Stent Results Dumon 1996 (1058) Wood 2003 (143) Saad 2003 (82) Noppen 1999 (46) Eisner 1999 (9) Bollinger 1996 (27) Bollinger 1993 (31) Silicone Silicone 87%, Metal 13% Metal Silicone Metal Metal Silicone 1574 stents, mean stenting 4 mo for malignant and 14 mo for benign, effective (migration) 95% clinical success, 41% required multiple procedures 14/16 (88%) of patients requiring mechanical ventilation were subsequently extubated More migration in benign disease. Effective Improvement (PFTs), 23 mo F/U 36 stents, significant improvement in Karnofsky Index Karnofsky Index improved in 90% of patients

56 Dyspnea Miyazawa et al., Chest 2000; 118:959
57 PFT Miyazawa et al., Chest 2000; 118:959
58 Quality of Life (QoL) EORTC was used for assessment of QoL 20 patients 7 days and 30 days post procedure Dyspnea scores improved in 85% of patients (p = 0.01) 65% of patients had improvement in overall QoL Significant improvement in dyspnea, insomnia, and fatigue scores 35% had stabilization or decline in QoL Significant decline in emotional, pain, and loss of appetite scores Need for multidisciplinary approach to patients with complications from thoracic malignancies Amjadi et al. Respiration 2008; 76:
59 Complications of Stenting Saad et al., Chest 2003; 124:1993 Complications Infection (15.9%) All treated with oral antibiotics, no hospitalizations In stent obstructive granulomas (14.6%) Laser, APC In stent obstructive disease recurrence (6.1%) Laser, APC, re stented Migration in (3.5%) Replaced with new stent Mild Hemoptysis (10%) No therapy required Bronchial perforation (1%) Covered stents No complications in 54%
60 Timely airway stenting improves survival in patients with malignant CAO 50 patients (10 stage III, 40 stage IV) received 72 airway stents Improvement in performance status was seen in 45/50 (90%) However, significant improvement in survival was observed in patients with intermediate performance (MRC < 4, ECOG < 3) compared to a matched group with poor performance status 8 months vs. 3 months; P<0.05 Conclusion Patients with CAO should be treated in timely fashion Razi et al. Ann Thorac Surg 2010; 90:
61 Stenting facilitates extubation 15 consecutive ICU patients with CAO who had multiple failed attempts at extubation Non surgical patients 14/15 (93%) were successfully extubated post stenting Noppen et al. Respiratory Medicine 2007; 101:
62 Conclusion Thoracic malignancies are often associated with unique complications impacting the Pleura Parenchyma Central Airways Endoscopic and minimally invasive modalities are available for patients with limited reserves Therapeutic and palliative options often need to be modified to accommodate patient s specific needs 1) Olden AM, Holloway R. J Palliat Med; 13:59 65.
ENDOBRONCHIAL ABLATIVE THERAPIES. Christopher Cortes, MD, FPCCP
 ENDOBRONCHIAL ABLATIVE THERAPIES Christopher Cortes, MD, FPCCP Choice of Ablative Therapy Size of the lesion Location of the lesion Characteristics of the lesion Availability of the different therapies
ENDOBRONCHIAL ABLATIVE THERAPIES Christopher Cortes, MD, FPCCP Choice of Ablative Therapy Size of the lesion Location of the lesion Characteristics of the lesion Availability of the different therapies
Interventional Pulmonology
 Interventional Pulmonology The Division of Thoracic Surgery Department of Cardiothoracic Surgery New York Presbyterian/Weill Cornell Medical College p: 212-746-6275 f: 212-746-8223 https://weillcornell.org/eshostak
Interventional Pulmonology The Division of Thoracic Surgery Department of Cardiothoracic Surgery New York Presbyterian/Weill Cornell Medical College p: 212-746-6275 f: 212-746-8223 https://weillcornell.org/eshostak
Therapeutic Bronchoscopy Etiology - Benign Stenosis Post - intubation Trauma Post - operative Inflammatory Idiopathic
 Endobronchial Palliation of Airway Disease Douglas E. Wood, MD Professor and Chief Division of Cardiothoracic Surgery Vice-Chair, Department of Surgery Endowed Chair in Lung Cancer Research University
Endobronchial Palliation of Airway Disease Douglas E. Wood, MD Professor and Chief Division of Cardiothoracic Surgery Vice-Chair, Department of Surgery Endowed Chair in Lung Cancer Research University
APPROACH TO PLEURAL EFFUSIONS. Raed Alalawi, MD, FCCP
 APPROACH TO PLEURAL EFFUSIONS Raed Alalawi, MD, FCCP CASE 65-year-old woman with H/O breast cancer presented with a 1 week H/O progressively worsening exersional dyspnea. Physical exam: Diminished breath
APPROACH TO PLEURAL EFFUSIONS Raed Alalawi, MD, FCCP CASE 65-year-old woman with H/O breast cancer presented with a 1 week H/O progressively worsening exersional dyspnea. Physical exam: Diminished breath
The Relationship of Pleural Pressure to Symptom Development During Therapeutic Thoracentesis*
 Original Research INTERVENTIONAL PULMONOLOGY The Relationship of Pleural Pressure to Symptom Development During Therapeutic Thoracentesis* David Feller-Kopman, MD, FCCP; Allan Walkey, MD; David Berkowitz,
Original Research INTERVENTIONAL PULMONOLOGY The Relationship of Pleural Pressure to Symptom Development During Therapeutic Thoracentesis* David Feller-Kopman, MD, FCCP; Allan Walkey, MD; David Berkowitz,
Interventional Pulmonary Case Based Discussions (ATS) Ali Imran Saeed, MD University of New Mexico
 Ali Imran Saeed, MD University of New Mexico") Interventional Pulmonary Case Based Discussions (ATS) Ali Imran Saeed, MD University of New Mexico Objectives Interventional Pulmonary in New Mexico Interventional Pulmonary and Advanced Diagnostic Cases
Interventional Pulmonary Case Based Discussions (ATS) Ali Imran Saeed, MD University of New Mexico Objectives Interventional Pulmonary in New Mexico Interventional Pulmonary and Advanced Diagnostic Cases
Restrictive Pulmonary Diseases
 Restrictive Pulmonary Diseases Causes: Acute alveolo-capillary sysfunction Interstitial disease Pleural disorders Chest wall disorders Neuromuscular disease Resistance Pathophysiology Reduced compliance
Restrictive Pulmonary Diseases Causes: Acute alveolo-capillary sysfunction Interstitial disease Pleural disorders Chest wall disorders Neuromuscular disease Resistance Pathophysiology Reduced compliance
Cystic Fibrosis Complications ANDRES ZIRLINGER, MD STANFORD UNIVERSITY MEDICAL CENTER MARCH 3, 2012
 Cystic Fibrosis Complications ANDRES ZIRLINGER, MD STANFORD UNIVERSITY MEDICAL CENTER MARCH 3, 2012 INTRODUCTION PNEUMOTHORAX HEMOPTYSIS RESPIRATORY FAILURE Cystic Fibrosis Autosomal Recessive Genetically
Cystic Fibrosis Complications ANDRES ZIRLINGER, MD STANFORD UNIVERSITY MEDICAL CENTER MARCH 3, 2012 INTRODUCTION PNEUMOTHORAX HEMOPTYSIS RESPIRATORY FAILURE Cystic Fibrosis Autosomal Recessive Genetically
Respiratory Diseases and Disorders
 Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Canadian Trauma Trials Collaborative. Occult Pneumothorax in Critical Care (OPTICC): Standardized Data Collection Sheet
: Standardized Data Collection Sheet") Canadian Trauma Trials Collaborative STUDY CENTRE: Institution: City / Province: / Occult Pneumothorax in Critical Care (OPTICC): Standardized Sheet PATIENT DEMOGRAPHICS: First Name: Health record number
Canadian Trauma Trials Collaborative STUDY CENTRE: Institution: City / Province: / Occult Pneumothorax in Critical Care (OPTICC): Standardized Sheet PATIENT DEMOGRAPHICS: First Name: Health record number
Case Study #2. Case Study #1 cont 9/28/2011. CAPA 2011 Christy Wilson PA C. LH is 78 yowf with PMHx of metz breast CA presents
 Case Study #1 CAPA 2011 Christy Wilson PA C 46 yo female presents with community acquired PNA (CAP). Her condition worsened and she was transferred to the ICU and placed on mechanical ventilation. Describe
Case Study #1 CAPA 2011 Christy Wilson PA C 46 yo female presents with community acquired PNA (CAP). Her condition worsened and she was transferred to the ICU and placed on mechanical ventilation. Describe
Problem Based Learning Session. Mr Robinson is a 67 year old man. He visits the GP as he has had a cough and fever for 5 days.
 Problem Based Learning Session Mr Robinson is a 67 year old man. He visits the GP as he has had a cough and fever for 5 days. The GP takes a history from him and examines his chest. Over the left base
Problem Based Learning Session Mr Robinson is a 67 year old man. He visits the GP as he has had a cough and fever for 5 days. The GP takes a history from him and examines his chest. Over the left base
Introduction to Interventional Pulmonology
 Introduction to Interventional Pulmonology Alexander Chen, M.D. Director, Interventional Pulmonology Assistant Professor of Medicine and Surgery Divisions of Pulmonary and Critical Care Medicine and Cardiothoracic
Introduction to Interventional Pulmonology Alexander Chen, M.D. Director, Interventional Pulmonology Assistant Professor of Medicine and Surgery Divisions of Pulmonary and Critical Care Medicine and Cardiothoracic
Introduction to Radiology for TB Nurses
 Introduction to Radiology for TB Nurses Juzar Ali, MD; FRCP(C); FCCP May 4, 2018 Essential Skills for the TB Nurse Case Manager Little Rock, AR May 3 4, 2017 Juzar Ali, MD; FRCP(C); FCCP has the following
Introduction to Radiology for TB Nurses Juzar Ali, MD; FRCP(C); FCCP May 4, 2018 Essential Skills for the TB Nurse Case Manager Little Rock, AR May 3 4, 2017 Juzar Ali, MD; FRCP(C); FCCP has the following
Breathlessness in advanced disease. February 2017
 Breathlessness in advanced disease February 2017 Breathlessness Managing breathlessness in primary care Chronic breathlessness Acute exacerbation of breathlessness Breathlessness at end of life Breathlessness
Breathlessness in advanced disease February 2017 Breathlessness Managing breathlessness in primary care Chronic breathlessness Acute exacerbation of breathlessness Breathlessness at end of life Breathlessness
ISPUB.COM. Rare Cases: Tracheal/bronchial Obstruction. O Wenker, L Moehn, C Portera, G Walsh HISTORY ADMISSION
 ISPUB.COM The Internet Journal of Radiology Volume 1 Number 1 O Wenker, L Moehn, C Portera, G Walsh Citation O Wenker, L Moehn, C Portera, G Walsh.. The Internet Journal of Radiology. 1999 Volume 1 Number
ISPUB.COM The Internet Journal of Radiology Volume 1 Number 1 O Wenker, L Moehn, C Portera, G Walsh Citation O Wenker, L Moehn, C Portera, G Walsh.. The Internet Journal of Radiology. 1999 Volume 1 Number
Thoracic Surgery; An Overview
 Thoracic Surgery What we see Thoracic Surgery; An Overview James P. Locher, Jr, MD Methodist Cardiovascular and Thoracic Surgery Lung cancer Mets Fungus and TB Lung abcess and empyema Pleural based disease
Thoracic Surgery What we see Thoracic Surgery; An Overview James P. Locher, Jr, MD Methodist Cardiovascular and Thoracic Surgery Lung cancer Mets Fungus and TB Lung abcess and empyema Pleural based disease
Dyspnea in the Cancer Patient 33 rd Annual PSONS Nursing Symposium April 1, 2011
 Dyspnea in the Cancer Patient 33 rd Annual PSONS Nursing Symposium April 1, 2011 Kathy Witmer, MN, ARNP Swedish Cancer Institute Thoracic Surgery - Oncology Dyspnea The word denotes disordered breathing
Dyspnea in the Cancer Patient 33 rd Annual PSONS Nursing Symposium April 1, 2011 Kathy Witmer, MN, ARNP Swedish Cancer Institute Thoracic Surgery - Oncology Dyspnea The word denotes disordered breathing
Stenting for Esophageal Cancer Technical Issues and Outcomes
 Stenting for Esophageal Cancer Technical Issues and Outcomes Moishe Liberman Director C.E.T.O.C. Division of Thoracic Surgery Centre Hospitalier de l Université de Montréal Disclosures Research and Educational
Stenting for Esophageal Cancer Technical Issues and Outcomes Moishe Liberman Director C.E.T.O.C. Division of Thoracic Surgery Centre Hospitalier de l Université de Montréal Disclosures Research and Educational
Lung Cancer - Suspected
 Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Part I Study Questions
 Part I Study Questions 1. A 59-year-old man with a history of pulmonary embolism diagnosed 2 years ago and treated with warfarin for 6 months is evaluated for progressive dyspnea and bilateral lower extremity
Part I Study Questions 1. A 59-year-old man with a history of pulmonary embolism diagnosed 2 years ago and treated with warfarin for 6 months is evaluated for progressive dyspnea and bilateral lower extremity
Indwelling Pleural Catheters in Malignant and Non-Malignant Disease
 Indwelling Catheters in Malignant and Non-Malignant Disease 20th Hellenic Conference November 2011 Najib Rahman Clinical Lecturer Oxford Centre for Respiratory Medicine University of Oxford, UK Najib.rahman@ndm.ox.ac.uk
Indwelling Catheters in Malignant and Non-Malignant Disease 20th Hellenic Conference November 2011 Najib Rahman Clinical Lecturer Oxford Centre for Respiratory Medicine University of Oxford, UK Najib.rahman@ndm.ox.ac.uk
Thoracic anaesthesia. Simon May
 Thoracic anaesthesia Simon May Contents Indications for lung isolation Ways of isolating lungs Placing a DLT Hypoxia on OLV Suitability for surgery Analgesia Key procedures Indications for lung isolation
Thoracic anaesthesia Simon May Contents Indications for lung isolation Ways of isolating lungs Placing a DLT Hypoxia on OLV Suitability for surgery Analgesia Key procedures Indications for lung isolation
Since central airway stenosis is often a lifethreatening. Double Y-stenting for tracheobronchial stenosis. Masahide Oki and Hideo Saka
 Eur Respir J 2012; 40: 1483 1488 DOI: 10.1183/09031936.00015012 CopyrightßERS 2012 Double Y-stenting for tracheobronchial stenosis Masahide Oki and Hideo Saka ABSTRACT: The purpose of the present study
Eur Respir J 2012; 40: 1483 1488 DOI: 10.1183/09031936.00015012 CopyrightßERS 2012 Double Y-stenting for tracheobronchial stenosis Masahide Oki and Hideo Saka ABSTRACT: The purpose of the present study
Respiratory Disease. Dr Amal Damrah consultant Neonatologist and Paediatrician
 Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
BELLWORK page 343. Apnea Dyspnea Hypoxia pneumo pulmonary Remember the structures of the respiratory system 1
 BELLWORK page 343 Apnea Dyspnea Hypoxia pneumo pulmonary respiratory system 1 STANDARDS 42) Review case studies that involve persons with respiratory disorders, diseases, or syndromes. Citing information
BELLWORK page 343 Apnea Dyspnea Hypoxia pneumo pulmonary respiratory system 1 STANDARDS 42) Review case studies that involve persons with respiratory disorders, diseases, or syndromes. Citing information
Case of the Day Chest
 Case of the Day Chest Darin White MDCM FRCPC Department of Radiology, Mayo Clinic 76 th Annual Scientific Meeting Canadian Association of Radiologists Montreal, QC April 26, 2013 2013 MFMER slide-1 Disclosures
Case of the Day Chest Darin White MDCM FRCPC Department of Radiology, Mayo Clinic 76 th Annual Scientific Meeting Canadian Association of Radiologists Montreal, QC April 26, 2013 2013 MFMER slide-1 Disclosures
Pneumothorax Ex-vacuo or trapped lung in the setting of hepatic hydrothorax
 Kim et al. BMC Pulmonary Medicine 2012, 12:78 CASE REPORT Open Access Pneumothorax Ex-vacuo or trapped lung in the setting of hepatic hydrothorax Yan S Kim 1*, Irawan Susanto 1, Catherine A Lazar 1, Ali
Kim et al. BMC Pulmonary Medicine 2012, 12:78 CASE REPORT Open Access Pneumothorax Ex-vacuo or trapped lung in the setting of hepatic hydrothorax Yan S Kim 1*, Irawan Susanto 1, Catherine A Lazar 1, Ali
BMC Pulmonary Medicine
 BMC Pulmonary Medicine This Provisional PDF corresponds to the article as it appeared upon acceptance. Fully formatted PDF and full text (HTML) versions will be made available soon. Pneumothorax Ex-vacuo
BMC Pulmonary Medicine This Provisional PDF corresponds to the article as it appeared upon acceptance. Fully formatted PDF and full text (HTML) versions will be made available soon. Pneumothorax Ex-vacuo
The use of metallic expandable tracheal stents in the management of inoperable malignant tracheal obstruction
 The use of metallic expandable tracheal stents in the management of inoperable malignant tracheal obstruction Alaa Gaafar-MD, Ahmed Youssef-MD, Mohamed Elhadidi-MD A l e x a n d r i a F a c u l t y o f
The use of metallic expandable tracheal stents in the management of inoperable malignant tracheal obstruction Alaa Gaafar-MD, Ahmed Youssef-MD, Mohamed Elhadidi-MD A l e x a n d r i a F a c u l t y o f
Malignant Effusions. Anantham Devanand Respiratory and Critical Care Medicine Singapore General Hospital
 Malignant Effusions Anantham Devanand Respiratory and Critical Care Medicine Singapore General Hospital Malignant Effusions Definition: Presence of malignant cells in the pleural space 75% are caused by
Malignant Effusions Anantham Devanand Respiratory and Critical Care Medicine Singapore General Hospital Malignant Effusions Definition: Presence of malignant cells in the pleural space 75% are caused by
Interpreting thoracic x-ray of the supine immobile patient: Syllabus
 Interpreting thoracic x-ray of the supine immobile patient: Syllabus Johannes Godt Dep. of Radiology and Nuclear Medicine Oslo University Hospital Ullevål NORDTER 2017, Helsinki Content - Why bedside chest
Interpreting thoracic x-ray of the supine immobile patient: Syllabus Johannes Godt Dep. of Radiology and Nuclear Medicine Oslo University Hospital Ullevål NORDTER 2017, Helsinki Content - Why bedside chest
Pneumothorax lecture no. 3
 Pneumothorax lecture no. 3 Is accumulation of air in a pleural space or accumulation of extra pulmonary air within the chest, Is uncommon during childhood, may result from external trauma, iatrogenic,
Pneumothorax lecture no. 3 Is accumulation of air in a pleural space or accumulation of extra pulmonary air within the chest, Is uncommon during childhood, may result from external trauma, iatrogenic,
Resident Case Review CHEST. Daria Manos CAR 2016
 Resident Case Review CHEST CAR 2016 Daria Manos Disclosure Speakers bureau, Roche CAR 2016 Daria Manos 1. Recognize common and critical chest radiograph and computed tomography signs and use these clues
Resident Case Review CHEST CAR 2016 Daria Manos Disclosure Speakers bureau, Roche CAR 2016 Daria Manos 1. Recognize common and critical chest radiograph and computed tomography signs and use these clues
Pleurodesis. What is a pleurodesis?
 2014 Pleurodesis Pleurodesis What is a pleurodesis? Pleurodesis is a procedure which involves a doctor or nurse practitioner putting a special solution in your chest. This solution is placed between the
2014 Pleurodesis Pleurodesis What is a pleurodesis? Pleurodesis is a procedure which involves a doctor or nurse practitioner putting a special solution in your chest. This solution is placed between the
Management of Dyspnea and Cough in Lung Cancer
 Management of Dyspnea and Cough in Lung Cancer Dr. Chris Ogaranko Lung Cancer Educational Event November 2013 Presenter Disclosure Faculty: Dr. Chris Ogaranko Relationships with commercial interests: Grants/Research
Management of Dyspnea and Cough in Lung Cancer Dr. Chris Ogaranko Lung Cancer Educational Event November 2013 Presenter Disclosure Faculty: Dr. Chris Ogaranko Relationships with commercial interests: Grants/Research
Chapter 8. Other Important Tests and Procedures. Mosby items and derived items 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
 Chapter 8 Other Important Tests and Procedures 1 Introduction Additional important diagnostic studies include: Sputum examination Skin tests Endoscopic examination Lung biopsy Thoracentesis Hematology,
Chapter 8 Other Important Tests and Procedures 1 Introduction Additional important diagnostic studies include: Sputum examination Skin tests Endoscopic examination Lung biopsy Thoracentesis Hematology,
The Respiratory System
 The Respiratory System Respiratory Anatomy Upper respiratory tract Nose Nasal passages Pharynx Larynx Respiratory Anatomy Functions of the upper respiratory tract: Provide entry for inhaled air Respiratory
The Respiratory System Respiratory Anatomy Upper respiratory tract Nose Nasal passages Pharynx Larynx Respiratory Anatomy Functions of the upper respiratory tract: Provide entry for inhaled air Respiratory
Tunneled pleural catheters for management of malignant pleural effusions: a 2-year review of outcomes at a high-volume center
 Original Article Page 1 of 8 Tunneled pleural catheters for management of malignant pleural effusions: a 2-year review of outcomes at a high-volume center Amit K. Mahajan 1,2, Devon T. Collins 1, Christiana
Original Article Page 1 of 8 Tunneled pleural catheters for management of malignant pleural effusions: a 2-year review of outcomes at a high-volume center Amit K. Mahajan 1,2, Devon T. Collins 1, Christiana
Double Y-stenting for tracheobronchial stenosis
 ERJ Express. Published on April 10, 2012 as doi: 10.1183/09031936.00015012 Double Y-stenting for tracheobronchial stenosis M. Oki and H. Saka AFFILIATIONS Dept of Respiratory Medicine, Nagoya Medical Center,
ERJ Express. Published on April 10, 2012 as doi: 10.1183/09031936.00015012 Double Y-stenting for tracheobronchial stenosis M. Oki and H. Saka AFFILIATIONS Dept of Respiratory Medicine, Nagoya Medical Center,
Paramedic Rounds. Pre-Hospital Continuous Positive Airway Pressure (CPAP)
") Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
TB Intensive Houston, Texas
 TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
Diagnostic Approach to Pleural Effusion
 Diagnostic Approach to Pleural Effusion Objectives Define the leading causes of pleural effusion Classify the type of effusion Identify procedures and tests associated with diagnosis 2 Agenda Basic anatomy
Diagnostic Approach to Pleural Effusion Objectives Define the leading causes of pleural effusion Classify the type of effusion Identify procedures and tests associated with diagnosis 2 Agenda Basic anatomy
Bronchial syndrome. Atelectasis Draining bronchus Bronchiectasis
 Bronchial syndrome Atelectasis Draining bronchus Bronchiectasis Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Atelectasis Consequence
Bronchial syndrome Atelectasis Draining bronchus Bronchiectasis Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Atelectasis Consequence
Specific Basic Standards for Osteopathic Fellowship Training in Pulmonary / Critical Care Medicine
 Specific Basic Standards for Osteopathic Fellowship Training in Pulmonary / Critical Care Medicine American Osteopathic Association and American College of Osteopathic Internists BOT Rev. 2/2011 These
Specific Basic Standards for Osteopathic Fellowship Training in Pulmonary / Critical Care Medicine American Osteopathic Association and American College of Osteopathic Internists BOT Rev. 2/2011 These
Reducing lung volume in emphysema Surgical Aspects
 Reducing lung volume in emphysema Surgical Aspects Simon Jordan Consultant Thoracic Surgeon Royal Brompton Hospital Thirteenth Cambridge Chest Meeting April 2015 Surgical aspects of LVR Why we should NOT
Reducing lung volume in emphysema Surgical Aspects Simon Jordan Consultant Thoracic Surgeon Royal Brompton Hospital Thirteenth Cambridge Chest Meeting April 2015 Surgical aspects of LVR Why we should NOT
Pneumothorax and Chest Tube Problems
 Pneumothorax and Chest Tube Problems Pneumothorax Definition Air accumulation in the pleural space with secondary lung collapse Sources Visceral pleura Ruptured esophagus Chest wall defect Gas-forming
Pneumothorax and Chest Tube Problems Pneumothorax Definition Air accumulation in the pleural space with secondary lung collapse Sources Visceral pleura Ruptured esophagus Chest wall defect Gas-forming
Medical Thoracoscopy When to Choose Over a General Anaesthetic VATS
 Medical Thoracoscopy When to Choose Over a General Anaesthetic VATS SpR Training Day 07.07.14 Dr Alex West Consultant Chest/Pleural Physician Guy s and St Thomas Hospital Medical Thoracoscopy? No Just
Medical Thoracoscopy When to Choose Over a General Anaesthetic VATS SpR Training Day 07.07.14 Dr Alex West Consultant Chest/Pleural Physician Guy s and St Thomas Hospital Medical Thoracoscopy? No Just
(SKILLS/HANDS-ON) Chest Tubes. Rebecca Carman, MSN, ACNP-BC. Amanda Shumway, PA-C. Thomas W. White, MD, FACS, CNSC
 Chest Tubes. Rebecca Carman, MSN, ACNP-BC. Amanda Shumway, PA-C. Thomas W. White, MD, FACS, CNSC") (SKILLS/HANDS-ON) Chest Tubes Rebecca Carman, MSN, ACNP-BC Nurse Practitioner, Trauma Services, Intermountain Medical Center, Intermountain Healthcare Amanda Shumway, PA-C APC Trauma and Critical Care
(SKILLS/HANDS-ON) Chest Tubes Rebecca Carman, MSN, ACNP-BC Nurse Practitioner, Trauma Services, Intermountain Medical Center, Intermountain Healthcare Amanda Shumway, PA-C APC Trauma and Critical Care
A comparison between two types of indwelling pleural catheters for management of malignant pleural effusions
 Original Article A comparison between two types of indwelling pleural catheters for management of malignant pleural effusions Sushilkumar Satish Gupta 1, Charalampos S. Floudas 2, Abhinav B. Chandra 3
Original Article A comparison between two types of indwelling pleural catheters for management of malignant pleural effusions Sushilkumar Satish Gupta 1, Charalampos S. Floudas 2, Abhinav B. Chandra 3
Chapter 10 Respiratory System J00-J99. Presented by: Jesicca Andrews
 Chapter 10 Respiratory System J00-J99 Presented by: Jesicca Andrews 1 Respiratory System 2 Respiratory Infections A respiratory infection cannot be assumed from a laboratory report alone; physician concurrence
Chapter 10 Respiratory System J00-J99 Presented by: Jesicca Andrews 1 Respiratory System 2 Respiratory Infections A respiratory infection cannot be assumed from a laboratory report alone; physician concurrence
Pulmonary Embolism. Thoracic radiologist Helena Lauri
 Pulmonary Embolism Thoracic radiologist Helena Lauri 8.5.2017 Statistics 1-2 out of 1000 adults annually are diagnosed with deep vein thrombosis (DVT) and/or pulmonary embolism (PE) About half of patients
Pulmonary Embolism Thoracic radiologist Helena Lauri 8.5.2017 Statistics 1-2 out of 1000 adults annually are diagnosed with deep vein thrombosis (DVT) and/or pulmonary embolism (PE) About half of patients
SURGERY FOR GIANT BULLOUS EMPHYSEMA
 SURGERY FOR GIANT BULLOUS EMPHYSEMA Dr. Carmine Simone Head, Division of Critical Care & Thoracic Surgeon Department of Surgery December 15, 2006 OVERVIEW Introduction Classification Patient selection
SURGERY FOR GIANT BULLOUS EMPHYSEMA Dr. Carmine Simone Head, Division of Critical Care & Thoracic Surgeon Department of Surgery December 15, 2006 OVERVIEW Introduction Classification Patient selection
Thoracoscopy for Lung Cancer
 Thoracoscopy for Lung Cancer Introduction The occurrence of lung cancer has increased dramatically over the last 50 years. Your doctor may have recommended an operation to remove your lung cancer. The
Thoracoscopy for Lung Cancer Introduction The occurrence of lung cancer has increased dramatically over the last 50 years. Your doctor may have recommended an operation to remove your lung cancer. The
MRSA pneumonia mucus plug burden and the difficult airway
 Case report Crit Care Shock (2016) 19:54-58 MRSA pneumonia mucus plug burden and the difficult airway Ann Tsung, Brian T. Wessman An 80-year-old female with a past medical history of chronic obstructive
Case report Crit Care Shock (2016) 19:54-58 MRSA pneumonia mucus plug burden and the difficult airway Ann Tsung, Brian T. Wessman An 80-year-old female with a past medical history of chronic obstructive
Pulmonary Pathophysiology
 Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Audra Fuller MD, Mark Sigler MD, Shrinivas Kambali MD, Raed Alalawi MD
 Clinical Series Successful treatment of post-intubation tracheal stenosis with balloon dilation, argon plasma coagulation, electrocautery and application of mitomycin C Audra Fuller MD, Mark Sigler MD,
Clinical Series Successful treatment of post-intubation tracheal stenosis with balloon dilation, argon plasma coagulation, electrocautery and application of mitomycin C Audra Fuller MD, Mark Sigler MD,
Bacterial pneumonia with associated pleural empyema pleural effusion
 EMPYEMA Synonyms : - Parapneumonic effusion - Empyema thoracis - Bacterial pneumonia - Pleural empyema, pleural effusion - Lung abscess - Complicated parapneumonic effusions (CPE) 1 Bacterial pneumonia
EMPYEMA Synonyms : - Parapneumonic effusion - Empyema thoracis - Bacterial pneumonia - Pleural empyema, pleural effusion - Lung abscess - Complicated parapneumonic effusions (CPE) 1 Bacterial pneumonia
Persistent Spontaneous Pneumothorax for Four Years: A Case Report
 303) Persistent Spontaneous Pneumothorax for Four Years: A Case Report Mizuno Y., Iwata H., Shirahashi K., Matsui M., Takemura H. Department of General and Cardiothoracic Surgery, Graduate School of Medicine,
303) Persistent Spontaneous Pneumothorax for Four Years: A Case Report Mizuno Y., Iwata H., Shirahashi K., Matsui M., Takemura H. Department of General and Cardiothoracic Surgery, Graduate School of Medicine,
Interventional procedures guidance Published: 20 December 2017 nice.org.uk/guidance/ipg600
 Endobronchial valve insertion to reduce lung volume in emphysema Interventional procedures guidance Published: 20 December 2017 nice.org.uk/guidance/ipg600 Your responsibility This guidance represents
Endobronchial valve insertion to reduce lung volume in emphysema Interventional procedures guidance Published: 20 December 2017 nice.org.uk/guidance/ipg600 Your responsibility This guidance represents
Introduction to Chest CT Interpretation. Objectives 8/28/2017
 Introduction to Chest CT Interpretation Deborah Stein ACNP BC, CCRN NP Education Specialist Department of Anesthesia and Critical Care Medicine August 28, 2017 Objectives Basic Principles Thoracic Anatomy
Introduction to Chest CT Interpretation Deborah Stein ACNP BC, CCRN NP Education Specialist Department of Anesthesia and Critical Care Medicine August 28, 2017 Objectives Basic Principles Thoracic Anatomy
Management of Pleural Effusion
 Management of Pleural Effusion Development of Pleural Effusion pulmonary capillary pressure (CHF) capillary permeability (Pneumonia) intrapleural pressure (atelectasis) plasma oncotic pressure (hypoalbuminemia)
Management of Pleural Effusion Development of Pleural Effusion pulmonary capillary pressure (CHF) capillary permeability (Pneumonia) intrapleural pressure (atelectasis) plasma oncotic pressure (hypoalbuminemia)
Tests Your Pulmonologist Might Order. Center For Cardiac Fitness Pulmonary Rehab Program The Miriam Hospital
 Tests Your Pulmonologist Might Order Center For Cardiac Fitness Pulmonary Rehab Program The Miriam Hospital BASIC ANATOMY OF THE LUNGS Lobes of Lung 3 lobes on the Right lung 2 lobes on the Left Blood
Tests Your Pulmonologist Might Order Center For Cardiac Fitness Pulmonary Rehab Program The Miriam Hospital BASIC ANATOMY OF THE LUNGS Lobes of Lung 3 lobes on the Right lung 2 lobes on the Left Blood
HEMOPTYSIS. Prof. G. Zuliani
 HEMOPTYSIS Prof. G. Zuliani HEMOPTYSIS Hemoptysis is the expectoration of blood, that can range from blood-streaking of sputum (Hemoptoe) to the presence of gross blood in the absence of any accompanying
HEMOPTYSIS Prof. G. Zuliani HEMOPTYSIS Hemoptysis is the expectoration of blood, that can range from blood-streaking of sputum (Hemoptoe) to the presence of gross blood in the absence of any accompanying
Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine
 Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine Venous thromboembolism: pulmonary embolism (PE) deep vein thrombosis (DVT) 1% of all patients admitted to hospital 5% of in-hospital mortality
Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine Venous thromboembolism: pulmonary embolism (PE) deep vein thrombosis (DVT) 1% of all patients admitted to hospital 5% of in-hospital mortality
Is severe re-expansion pulmonary edema still a lethal complication of closed thoracostomy or thoracic surgery?
 Original Article Page 1 of 6 Is severe re-expansion pulmonary edema still a lethal complication of closed thoracostomy or thoracic surgery? Sang Kwon Lee 1, Jung Joo Hwang 2, Mi Hee Lim 1, Joo Hyung Son
Original Article Page 1 of 6 Is severe re-expansion pulmonary edema still a lethal complication of closed thoracostomy or thoracic surgery? Sang Kwon Lee 1, Jung Joo Hwang 2, Mi Hee Lim 1, Joo Hyung Son
Patient History 1. Patient History 2. Social History. The Role of Surgery in the Management of TB. Reynard McDonald, MD & Paul Bolanowski, MD
 Patient History 1 The Role of Surgery in the Management of TB Reynard McDonald, MD & Paul Bolanowski, MD September 16, 2010 42 y/o AA male was initially diagnosed with pansensitive pulmonary TB in 1986
Patient History 1 The Role of Surgery in the Management of TB Reynard McDonald, MD & Paul Bolanowski, MD September 16, 2010 42 y/o AA male was initially diagnosed with pansensitive pulmonary TB in 1986
INDEPENDENT LUNG VENTILATION
 INDEPENDENT LUNG VENTILATION Giuseppe A. Marraro, MD Director Anaesthesia and Intensive Care Department Paediatric Intensive Care Unit Fatebenefratelli and Ophthalmiatric Hospital Milan, Italy gmarraro@picu.it
INDEPENDENT LUNG VENTILATION Giuseppe A. Marraro, MD Director Anaesthesia and Intensive Care Department Paediatric Intensive Care Unit Fatebenefratelli and Ophthalmiatric Hospital Milan, Italy gmarraro@picu.it
Thoraxdrainage SGP Jahresversammlung 2016, Lausanne
 Thoraxdrainage SGP Jahresversammlung 2016, Lausanne Dr. med. Lukas Kern a bit of history (incomplete.) a bit of physiology (basic ) indication data guidelines a bit of history (incomplete.) a bit of physiology
Thoraxdrainage SGP Jahresversammlung 2016, Lausanne Dr. med. Lukas Kern a bit of history (incomplete.) a bit of physiology (basic ) indication data guidelines a bit of history (incomplete.) a bit of physiology
Chronic obstructive lung disease. Dr/Rehab F.Gwada
 Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
Emphysema. Endoscopic lung volume reduction. PhD. Chief, department of chest diseases and thoracic oncology. JM VERGNON M.D, PhD.
 Emphysema Endoscopic lung volume reduction JM VERGNON M.D, PhD. PhD. Chief, department of chest diseases and thoracic oncology Genève 2010 INSERM IFR 143 Physiological concepts EMPHYSEMA Slide of Ch H
Emphysema Endoscopic lung volume reduction JM VERGNON M.D, PhD. PhD. Chief, department of chest diseases and thoracic oncology Genève 2010 INSERM IFR 143 Physiological concepts EMPHYSEMA Slide of Ch H
Bronchogenic Carcinoma
 A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
FOREIGN BODY ASPIRATION in children. Dr. Xayyavong Bouathongthip, M.D Emergency department, children s hospital
 FOREIGN BODY ASPIRATION in children Dr. Xayyavong Bouathongthip, M.D Emergency department, children s hospital How common is choking? About 3,000 people die/year from choking Figure remained unchanged
FOREIGN BODY ASPIRATION in children Dr. Xayyavong Bouathongthip, M.D Emergency department, children s hospital How common is choking? About 3,000 people die/year from choking Figure remained unchanged
SCLERODERMA LUNG DISEASE: WHAT THE PATIENT SHOULD KNOW
 SCLERODERMA LUNG DISEASE: WHAT THE PATIENT SHOULD KNOW Lung disease can be a serious complication of scleroderma. The two most common types of lung disease in patients with scleroderma are interstitial
SCLERODERMA LUNG DISEASE: WHAT THE PATIENT SHOULD KNOW Lung disease can be a serious complication of scleroderma. The two most common types of lung disease in patients with scleroderma are interstitial
Lung Cancer Resection
 Lung Cancer Resection Introduction The occurrence of lung cancer has increased dramatically over the last 50 years. Your health care provider may have recommended an operation to remove your lung cancer.
Lung Cancer Resection Introduction The occurrence of lung cancer has increased dramatically over the last 50 years. Your health care provider may have recommended an operation to remove your lung cancer.
Acute presentations of lung cancer. Dr Prina Ruparelia Respiratory consultant Cambridge University Hospital
 Acute presentations of lung cancer Dr Prina Ruparelia Respiratory consultant Cambridge University Hospital The problem Incidence CADIAS report /NCIN Acute lung cancer presentations Future pathway developments
Acute presentations of lung cancer Dr Prina Ruparelia Respiratory consultant Cambridge University Hospital The problem Incidence CADIAS report /NCIN Acute lung cancer presentations Future pathway developments
Top Tips for Pleural Disease in 2012
 Top Tips for Pleural Disease in 2012 The unilateral pleural effusion on the Post Take Ward Round Pleural Effusion on CXR Bedside ultrasound + Pleural aspirate Empyema Nil evidence infection Admit IV antibiotics
Top Tips for Pleural Disease in 2012 The unilateral pleural effusion on the Post Take Ward Round Pleural Effusion on CXR Bedside ultrasound + Pleural aspirate Empyema Nil evidence infection Admit IV antibiotics
Common Confounding Consults In Pulmonary & Critical Care
 Common Confounding Consults In Pulmonary & Critical Care Lekshmi Santhosh, M.D. Assistant Professor, Pulm/Critical Care & Hosp Med Management of the Hospitalized Patient 10.20.2018 Disclosures None. 1
Common Confounding Consults In Pulmonary & Critical Care Lekshmi Santhosh, M.D. Assistant Professor, Pulm/Critical Care & Hosp Med Management of the Hospitalized Patient 10.20.2018 Disclosures None. 1
Identification and Treatment of the Patient with Sleep Related Hypoventilation
 Identification and Treatment of the Patient with Sleep Related Hypoventilation Hillary Loomis-King, MD Pulmonary and Critical Care of NW MI Munson Sleep Disorders Center X Conflict of Interest Disclosures
Identification and Treatment of the Patient with Sleep Related Hypoventilation Hillary Loomis-King, MD Pulmonary and Critical Care of NW MI Munson Sleep Disorders Center X Conflict of Interest Disclosures
Handling Common Problems & Pitfalls During. Oxygen desaturation in patients receiving mechanical ventilation ACUTE SEVERE RESPIRATORY FAILURE
 Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
THORACIK RICK. Lungs. Outline and objectives Richard A. Malthaner MD MSc FRCSC FACS
 THORACIK RICK Outline and objectives Lungs Management of a solitary lung nodule Mediastinum Management of a mediastinal mass Pleura Management of a pleural fluid & pneumothorax Esophagus & Stomach Management
THORACIK RICK Outline and objectives Lungs Management of a solitary lung nodule Mediastinum Management of a mediastinal mass Pleura Management of a pleural fluid & pneumothorax Esophagus & Stomach Management
The diagnosis and management of pneumothorax
 Respiratory 131 The diagnosis and management of pneumothorax Pneumothorax is a relatively common presentation in patients under the age of 40 years (approximately, 85% of patients are younger than 40 years).
Respiratory 131 The diagnosis and management of pneumothorax Pneumothorax is a relatively common presentation in patients under the age of 40 years (approximately, 85% of patients are younger than 40 years).
Navigational Bronchoscopy with Transbronchial Radiofrequency Ablation
 Navigational Bronchoscopy with Transbronchial Radiofrequency Ablation Katie S. Nason, MD MPH AATS Focus on Thoracic: Mastering Surgical Innovation October 28, 2017 No disclosures Radiofrequency ablative
Navigational Bronchoscopy with Transbronchial Radiofrequency Ablation Katie S. Nason, MD MPH AATS Focus on Thoracic: Mastering Surgical Innovation October 28, 2017 No disclosures Radiofrequency ablative
CPAP. Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device. Charlottesville Albemarle Rescue Squad - CPAP
 CPAP Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device CPAP What Is It? C ontinuous P ositive A irway P ressure Anatomy Review Anatomy Review Anatomy Review Alveoli Anatomy Review Chest
CPAP Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device CPAP What Is It? C ontinuous P ositive A irway P ressure Anatomy Review Anatomy Review Anatomy Review Alveoli Anatomy Review Chest
EVALUATE DATA IN THE PATIENT RECORD
 EVALUATE DATA IN THE PATIENT RECORD Shawna Strickland, PhD, RRT-NPS, AE-C, FAARC Objectives At the end of this module, the learner will be able to identify the pertinent data from the patient chart for
EVALUATE DATA IN THE PATIENT RECORD Shawna Strickland, PhD, RRT-NPS, AE-C, FAARC Objectives At the end of this module, the learner will be able to identify the pertinent data from the patient chart for
Patient Management Code Blue in the CT Suite
 Patient Management Code Blue in the CT Suite David Stultz, MD November 28, 2001 Case Presentation A 53-year-old woman experienced acute respiratory distress during an IV contrast enhanced CT scan of the
Patient Management Code Blue in the CT Suite David Stultz, MD November 28, 2001 Case Presentation A 53-year-old woman experienced acute respiratory distress during an IV contrast enhanced CT scan of the
Department of Thoracic Medicine, Chang Gung Memorial Hospital, Lin-Kuo Branch, Chang Gung Medical Foundation; Abstract
 DOI 10.6314/JIMT.2017.28(4).07 2017 28 243-251 Impacts of Airway Self-expandable Metallic Stent on Ventilator Weaning and Survival of Mechanically Ventilated Patients with Esophageal Cancer and Cental
DOI 10.6314/JIMT.2017.28(4).07 2017 28 243-251 Impacts of Airway Self-expandable Metallic Stent on Ventilator Weaning and Survival of Mechanically Ventilated Patients with Esophageal Cancer and Cental
10/17/2016. Nuts and Bolts of Thoracic Radiology. Objectives. Techniques
 Nuts and Bolts of Thoracic Radiology October 20, 2016 Carleen Risaliti Objectives Understand the basics of chest radiograph Develop a system for interpreting chest radiographs Correctly identify thoracic
Nuts and Bolts of Thoracic Radiology October 20, 2016 Carleen Risaliti Objectives Understand the basics of chest radiograph Develop a system for interpreting chest radiographs Correctly identify thoracic
Surgical management of lung cancer
 Surgical management of lung cancer Nick Roubos FRACS Cardiothoracic Surgeon Box Hill Hospital, Epworth Eastern Thoracic Oncology Non Small Cell Lung Cancer (NSCLC) Small Cell Lung Cancer Mesothelioma Pulmonary
Surgical management of lung cancer Nick Roubos FRACS Cardiothoracic Surgeon Box Hill Hospital, Epworth Eastern Thoracic Oncology Non Small Cell Lung Cancer (NSCLC) Small Cell Lung Cancer Mesothelioma Pulmonary
Objectives. What is a Chest X Ray? CXR Workshop. Definition (diagnostic tool/internal PE) Types. Cost
 Types. Cost") Objectives CAPA 2011 Christy Wilson, PA C Georgia Lung Associates Identify the radiographic landmarks on a chest radiograph Recognize identifiers of poor quality on the chest radiograph Outline an approach
Objectives CAPA 2011 Christy Wilson, PA C Georgia Lung Associates Identify the radiographic landmarks on a chest radiograph Recognize identifiers of poor quality on the chest radiograph Outline an approach
Pleural Effusion. Exudative pleural effusion - Involve an increase in capillary permeability and impaired pleural fluid resorption
 Pleural Effusion Definition of pleural effusion Accumulation of fluid between the pleural layers Epidemiology of pleural effusion Estimated prevalence of pleural effusion is 320 cases per 100,000 people
Pleural Effusion Definition of pleural effusion Accumulation of fluid between the pleural layers Epidemiology of pleural effusion Estimated prevalence of pleural effusion is 320 cases per 100,000 people
ASSESSMENT OF LUNG PARENCHYMAL ABNORMALITIES
 2016 by the author Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as
2016 by the author Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as
Original Research. Mummadi, Srinivas; Pack, Sasheen; Hahn, Peter
 The Official Journal of the International Society of Pleural Diseases Original Research The Use of Bronchoscopic Oxygen Insufflation to Isolate Persistent Air Leaks in Secondary Pneumothorax Due to COPD
The Official Journal of the International Society of Pleural Diseases Original Research The Use of Bronchoscopic Oxygen Insufflation to Isolate Persistent Air Leaks in Secondary Pneumothorax Due to COPD
Contraindications to time critical surgery; when not to proceed from the perspective of: The Physician A/Prof Peter Morley
 Contraindications to time critical surgery; when not to proceed from the perspective of: The Physician A/Prof Peter Morley British Journal of Surgery 2013; 100: 1045 1049 The risk of 30 day mortality
Contraindications to time critical surgery; when not to proceed from the perspective of: The Physician A/Prof Peter Morley British Journal of Surgery 2013; 100: 1045 1049 The risk of 30 day mortality
Coexistence of confirmed obstruction in spirometry and restriction in body plethysmography, e.g.: COPD + pulmonary fibrosis
 Volumes: IRV inspiratory reserve volume Vt tidal volume ERV expiratory reserve volume RV residual volume Marcin Grabicki Department of Pulmonology, Allergology and Respiratory Oncology Poznań University
Volumes: IRV inspiratory reserve volume Vt tidal volume ERV expiratory reserve volume RV residual volume Marcin Grabicki Department of Pulmonology, Allergology and Respiratory Oncology Poznań University
Current Management of Postpneumonectomy Bronchopleural Fistula
 Current Management of Postpneumonectomy Bronchopleural Fistula Shaf Keshavjee MD MSc FRCSC FACS Surgeon-in-Chief, University Health Network James Wallace McCutcheon Chair in Surgery Professor, Division
Current Management of Postpneumonectomy Bronchopleural Fistula Shaf Keshavjee MD MSc FRCSC FACS Surgeon-in-Chief, University Health Network James Wallace McCutcheon Chair in Surgery Professor, Division
Surgical indications: Non-malignant pulmonary diseases. Punnarerk Thongcharoen
 Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
TAVR : Caring for your patients before and after TAVR
 TAVR : Caring for your patients before and after TAVR Zubair Ahmed MD FSCAI Interventional Cardiologist Washington Regional Medical Center / Walker Heart Institute What is Aortic Valve Stenosis? AVA ~4
TAVR : Caring for your patients before and after TAVR Zubair Ahmed MD FSCAI Interventional Cardiologist Washington Regional Medical Center / Walker Heart Institute What is Aortic Valve Stenosis? AVA ~4
4/17/2010 C ini n ca c l a Ev E a v l a ua u t a ion o n of o ILD U dat a e t e i n I LDs
 Update in ILDs Diagnosis 101: Clinical Evaluation April 17, 2010 Jay H. Ryu, MD Mayo Clinic, Rochester MN Clinical Evaluation of ILD Outline General aspects of ILDs Classification of ILDs Clinical evaluation
Update in ILDs Diagnosis 101: Clinical Evaluation April 17, 2010 Jay H. Ryu, MD Mayo Clinic, Rochester MN Clinical Evaluation of ILD Outline General aspects of ILDs Classification of ILDs Clinical evaluation
Lecture Notes. Chapter 9: Smoke Inhalation Injury and Burns
 Lecture Notes Chapter 9: Smoke Inhalation Injury and Burns Objectives List the factors that influence mortality rate Describe the nature of smoke inhalation and the fire environment Recognize the pulmonary
Lecture Notes Chapter 9: Smoke Inhalation Injury and Burns Objectives List the factors that influence mortality rate Describe the nature of smoke inhalation and the fire environment Recognize the pulmonary