Contraindications to time critical surgery; when not to proceed from the perspective of: The Physician A/Prof Peter Morley
|
|
|
- Charla Greene
- 5 years ago
- Views:
Transcription
1 Contraindications to time critical surgery; when not to proceed from the perspective of: The Physician A/Prof Peter Morley
2

3
4
5
6 British Journal of Surgery 2013; 100:
7
8 The risk of 30 day mortality increased with a surgical delay of more than 12h (odds ratio, 1.45; p = 0.02), more than 24h (odds ratio, 1.34; p = 0.02), and more than 48h (odds ratio, 1.56; p = 0.02); the risk of 90 day mortality increased with a surgical delay of more than 24h (odds ratio, 1.23; p = 0.04). An education level of the surgeon below that of an attending surgeon increased the risk of thirty-day mortality (odds ratio, 1.28; p = 0.035) and ninety-day mortality (odds ratio, 1.26; p = 0.016).

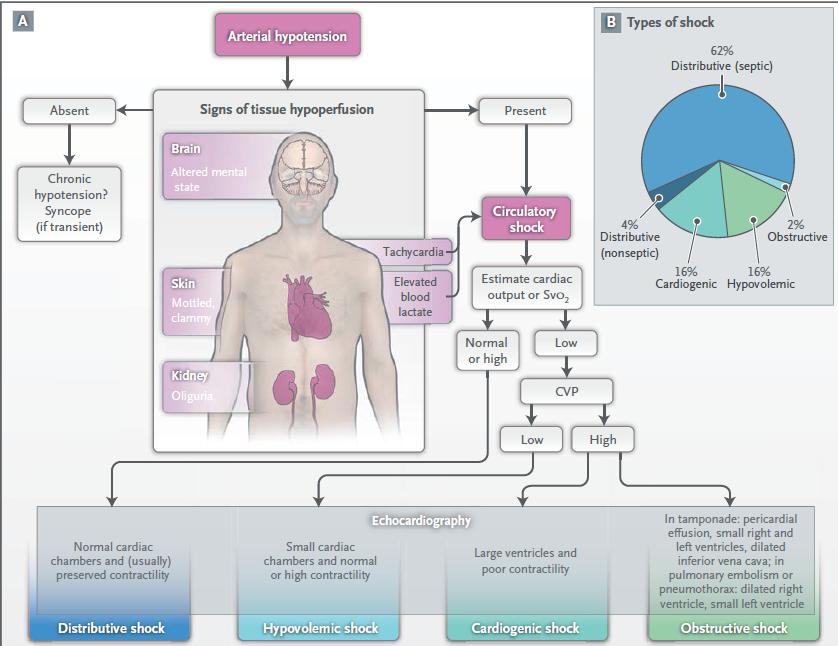
9 Physician input can be crucial Please avoid hypoxia and hypotension

10

11 Sometimes time is critical

12 Does a physician have a role?

13
14 14

15 There s really not much there...
16 Some will be covered in more detail later

17 Some will need to be comanaged by the physician, anaesthetist and surgeon
18 Three main areas Can I improve the problem in the time available? Should we operate at all? Recognise when you should not delay
19 Three main areas Can I improve the problem in the time available? Should we operate at all? Recognise when you should not delay
20 Can I improve the problem in the time available? Do I understand what the surgeon needs to do? Do I understand what the anaesthetist needs to do? Can I help them do their job better? All crucially dependent on what resources are available
21 Systematic approach Airway Breathing Circulation Disability Exposure

22 Airway management
23
24
25 Systematic approach Airway Breathing Circulation Disability Exposure

26
27 Ventilation tricks Improve mechanics and oxygenation APO CPAP, diuretics, venesection Bronchoconstriction Beta-agonists, steroids, magnesium, volatiles Collapsed lung CPAP, bronchoscopy, physiotherapy ARDS Recruitment, better ventilator?
28 Systematic approach Airway Breathing Circulation Disability Exposure
29
30
31

32 For patients of GI perforation with associated septic shock, time from admission to initiation of surgery for source control is a critical determinant, under the condition of being supported by hemodynamic stabilization. The target time for a favorable outcome may be within 6 hours from admission. We should not delay in initiating EGDT-assisted surgery if patients are complicated with septic shock.
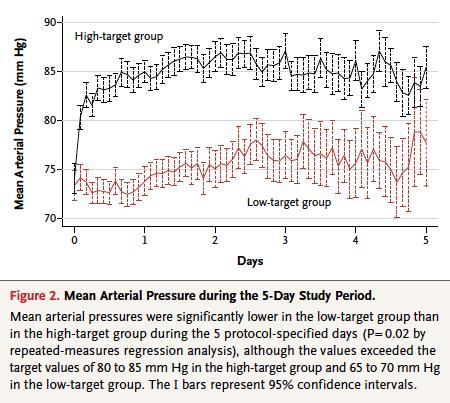
33 Azuhata et al. Critical Care 2014, 18:R87

34 British Journal of Surgery 2013; 100:

35 British Journal of Surgery 2013; 100:
36

37 An automated prediction tool identified at risk patients and prompted a bedside evaluation resulting in more timely sepsis care, improved documentation, and a suggestion of reduced mortality. Journal of Hospital Medicine 2015;10:26 31

38 Crit Care Med 2014; 42: ) The results of the analysis of this large population of patients with severe sepsis and septic shock demonstrate that delay in first antibiotic administration was associated with increased in-hospital mortality. In addition, there was a linear increase in the risk of mortality for each hour delay in antibiotic administration.

39 The administration of adequate antimicrobial therapy before ICU admission is decisive for the survival of patients with severe sepsis and septic shock.

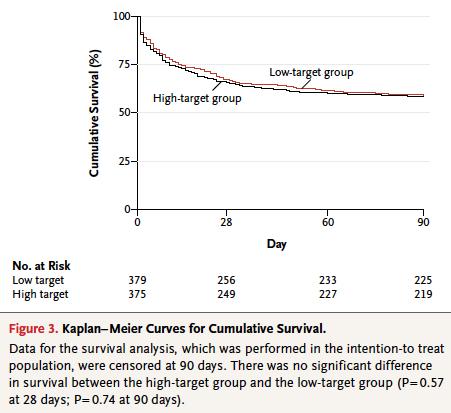
40 Targeting a mean arterial pressure of 80 to 85 mm Hg, as compared with 65 to 70 mm Hg, in patients with septic shock undergoing resuscitation did not result in significant differences in mortality at either 28 or 90 days.
41
 or when the level was 9 g per deciliter or less (higher threshold) during the")
42 In this multicenter, parallel-group trial, we randomly assigned patients in the intensive care unit (ICU) who had septic shock and a hemoglobin concentration of 9 g per deciliter or less to receive 1 unit of leukoreduced red cells when the hemoglobin level was 7 g per deciliter or less (lower threshold) or when the level was 9 g per deciliter or less (higher threshold) during the ICU stay.
43 N Engl J Med 2014;371:
44 N Engl J Med 2014;371:
45
46
47 NEJM 1994; 331:

48 Aggressive volume resuscitation of patients with raaas before proximal aortic control predicted an increased perioperative risk of death, which was independent of systolic blood pressure. Therefore, volume resuscitation should be delayed until surgical control of bleeding is achieved. J Vasc Surg 2013;57:
49
50
51
52 Cardiogenic issues Reversible rhythms Brady/asystole, tachy-dysrhythmias Pacing, electrolytes, anti-arrhythmics Ischaemia Revascularise? Cardiomypathy Inotropes? Tamponade Drain?
53 We could do with some more information
54
55
56 Anaesthesia 2012, 67, Prospective observational study investigated the effect of focused transthoracic echocardiography in 99 patients who had suspected cardiac disease or were 65 years old, and were scheduled for emergency noncardiac surgery. The treating anaesthetist completed a diagnosis and management plan before and after transthoracic echocardiography, which was performed by an independent operator. Clinical examination rated cardiac disease present in 75%; the remainder were asymptomatic. The cardiac diagnosis was changed in 67% and the management plan in 44% of patients after echocardiography. Cardiac disease was identified by echocardiography in 64% of patients, which led to a step-up of treatment in 36% (4% delay for cardiology referral, 2% altered surgery, 4% intensive care and 26% intra-operative haemodynamic management changes). Absence of cardiac disease in 36% resulted in a step-down of treatment in 8% (no referral 3%, intensive care 1% or haemodynamic treatment 4%).

57 Anaesthesia 2012, 67,
58
59 Obstructive shock Pulmonary embolus??? Tension pneumothorax Drain?
60 Systematic approach Airway Breathing Circulation Disability Exposure
61 Disability Reversible neurological state Seizure control? Drugs Antidotes? Don t Ever Forget Glucose Hypoglycemia, hyperglycemia?
62 Systematic approach Airway Breathing Circulation Disability Exposure
63
64
65 This meta-analysis supports ortho-geriatric collaboration to improve mortality after hip repair. Further study is needed to determine the best model of ortho-geriatric collaboration, and if these partnerships improve functional outcomes. J Orthop Trauma March ; 28(3): e49 e55
; the risk of 90 day mortality increased with a surgical delay of more than 24h (odds ratio, 1.23; p = 0.04).")
66 The risk of 30 day mortality increased with a surgical delay of more than 12h (odds ratio, 1.45; p = 0.02), more than 24h (odds ratio, 1.34; p = 0.02), and more than 48h (odds ratio, 1.56; p = 0.02); the risk of 90 day mortality increased with a surgical delay of more than 24h (odds ratio, 1.23; p = 0.04). An education level of the surgeon below that of an attending surgeon increased the risk of thirty-day mortality (odds ratio, 1.28; p = 0.035) and ninety-day mortality (odds ratio, 1.26; p = 0.016).

67 Older age, male gender, higher chronic comorbidity and higher severity measured by the Risk Mortality Index were associated with higher mortality, but the time to surgery was not.
68 Have a really good look Have we missed something? Drug effect/allergic reaction, anaphylaxis Metabolic/electrolyte/endocrine disturbance K, Mg, PO4, HCO3, etc Have we mis-diagnosed something? Fixation error? Anchoring bias? Recallability trap? Biliary pain is due to pneumonia Abdominal pain is due to myocardial ischaemia Should we be doing this Die with or without surgery Not what patient would want
69 Three main areas Can I improve the problem in the time available? Should we operate at all? Recognise when you should not delay

70
71
72 Should we operate at all? Futile? Are you sure? AVR in the 90s Is it what the patient would want? Previous expressed/documented wishes Able to consent, encompassing goals of care
73 Three main areas Can I improve the problem in the time available? Should we operate at all? Recognise when you should not delay
74

75 You may see things differently...
76 We know getting patients to ICU faster is good
77

: 1.")
78 There is a significant association between time to admission and survival rates. Each hour of waiting was independently associated with a 1.5% increased risk of ICU death (hazard ratio (HR): 1.015; 95% CI to 1.023; P = 0.001).

79 the summary 79
80 Summary Can I improve the problem in the time available? ABCDE Should we operate at all? Goals of Care, Advanced Care Planning Recognise when you should not delay

81
Maternal Collapse Guideline
 Maternal Collapse Guideline Guideline Number: 664 Supersedes: Classification Clinical Version No: Date of EqIA: Approved by: Date Approved: Date made active: Review Date: 1 Obstetric Written Documentation
Maternal Collapse Guideline Guideline Number: 664 Supersedes: Classification Clinical Version No: Date of EqIA: Approved by: Date Approved: Date made active: Review Date: 1 Obstetric Written Documentation
Blood transfusions in ICU: double-edged sword. Paul Hébert, MD MHSc(Epid) Physician-in-Chief, CHUM Professor, University of Montreal
 Physician-in-Chief, CHUM Professor, University of Montreal") Blood transfusions in ICU: double-edged sword Paul Hébert, MD MHSc(Epid) Physician-in-Chief, CHUM Professor, University of Montreal Canadian Critical Care Trials Group Collaborating for Impact Leading
Blood transfusions in ICU: double-edged sword Paul Hébert, MD MHSc(Epid) Physician-in-Chief, CHUM Professor, University of Montreal Canadian Critical Care Trials Group Collaborating for Impact Leading
University of Wisconsin - Madison Cardiovascular Medicine Fellowship Program UW CICU Rotation Goals and Objectives
 Background: The field of critical care cardiology has evolved considerably over the past 2 decades. Contemporary critical care cardiology is increasingly focused on the management of patients with advanced
Background: The field of critical care cardiology has evolved considerably over the past 2 decades. Contemporary critical care cardiology is increasingly focused on the management of patients with advanced
Case year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50
 Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
No conflicts of interest to disclose
 No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
Post-Cardiac Arrest Syndrome. MICU Lecture Series
 Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
Management of Post Cardiac Arrest Syndrome
 Management of Post Cardiac Arrest Syndrome Wilhelm Behringer Associated Professor of Emergency Medicine Medical University of Vienna, Austria Patients % What happens after ROSC? 35 30 25 20 15 10 5 ROSC
Management of Post Cardiac Arrest Syndrome Wilhelm Behringer Associated Professor of Emergency Medicine Medical University of Vienna, Austria Patients % What happens after ROSC? 35 30 25 20 15 10 5 ROSC
Major Points. The ED-ICU Interface. Chain of Survival. It usually starts here
 Major Points The ED-ICU Interface Robert M. Rodriguez, MD FAAEM Most ICU patients start in ED Chain of critical care starting in field and ED Collaborate, develop protocols (define roles), communicate
Major Points The ED-ICU Interface Robert M. Rodriguez, MD FAAEM Most ICU patients start in ED Chain of critical care starting in field and ED Collaborate, develop protocols (define roles), communicate
CCR Keywords Primary keywords
 CCR Keywords Primary keywords 1 Aboriginal health 2 Administration and health services 3 Allied health 4 Anaesthesia and intensive care 5 Biochemistry 6 Cardiology and cardiac surgery 7 Complementary medicine
CCR Keywords Primary keywords 1 Aboriginal health 2 Administration and health services 3 Allied health 4 Anaesthesia and intensive care 5 Biochemistry 6 Cardiology and cardiac surgery 7 Complementary medicine
In-hospital Care of the Post-Cardiac Arrest Patient. David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine
 In-hospital Care of the Post-Cardiac Arrest Patient David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine Disclosures I have no financial interest, arrangement,
In-hospital Care of the Post-Cardiac Arrest Patient David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine Disclosures I have no financial interest, arrangement,
Transfusion & Mortality. Philippe Van der Linden MD, PhD
 Transfusion & Mortality Philippe Van der Linden MD, PhD Conflict of Interest Disclosure In the past 5 years, I have received honoraria or travel support for consulting or lecturing from the following companies:
Transfusion & Mortality Philippe Van der Linden MD, PhD Conflict of Interest Disclosure In the past 5 years, I have received honoraria or travel support for consulting or lecturing from the following companies:
INTENSIVE CARE MEDICINE CPD EVENING. Dr Alastair Morgan Wednesday 13 th September 2017
 INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
LeMone & Burke Ch 30-32
 LeMone & Burke Ch 30-32 2 Right side- Low oxygenation Low pressure Light workload Goes toward the lungs Left side High oxygenation Thick walled high pressure Heavier workload Carries oxygenation blood
LeMone & Burke Ch 30-32 2 Right side- Low oxygenation Low pressure Light workload Goes toward the lungs Left side High oxygenation Thick walled high pressure Heavier workload Carries oxygenation blood
(Peripheral) Temperature and microcirculation
 Temperature and microcirculation") (Peripheral) Temperature and microcirculation Prof. Jan Bakker MD, PhD Chair dept Intensive Care Adults jan.bakker@erasmusmc.nl www.intensivecare.me Intensive Care Med (2005) 31:1316 1326 DOI 10.1007/s00134-005-2790-2
(Peripheral) Temperature and microcirculation Prof. Jan Bakker MD, PhD Chair dept Intensive Care Adults jan.bakker@erasmusmc.nl www.intensivecare.me Intensive Care Med (2005) 31:1316 1326 DOI 10.1007/s00134-005-2790-2
Unit 4 Problems of Cardiac Output and Tissue Perfusion
 Unit 4 Problems of Cardiac Output and Tissue Perfusion Lemone and Burke Ch 30-32 Objectives Review the anatomy and physiology of the cardiovascular system. Identify normal heart sounds and relate them
Unit 4 Problems of Cardiac Output and Tissue Perfusion Lemone and Burke Ch 30-32 Objectives Review the anatomy and physiology of the cardiovascular system. Identify normal heart sounds and relate them
Key Points. Angus DC: Crit Care Med 29:1303, 2001
 Sepsis Key Points Sepsis is the combination of a known or suspected infection and an accompanying systemic inflammatory response (SIRS) Severe sepsis is sepsis with acute dysfunction of one or more organ
Sepsis Key Points Sepsis is the combination of a known or suspected infection and an accompanying systemic inflammatory response (SIRS) Severe sepsis is sepsis with acute dysfunction of one or more organ
Update on Sudden Cardiac Death and Resuscitation
 Update on Sudden Cardiac Death and Resuscitation Ashish R. Panchal, MD, PhD Medical Director Center for Emergency Medical Services Assistant Professor Clinical Department of Emergency Medicine The Ohio
Update on Sudden Cardiac Death and Resuscitation Ashish R. Panchal, MD, PhD Medical Director Center for Emergency Medical Services Assistant Professor Clinical Department of Emergency Medicine The Ohio
Fluid Resuscitation and Monitoring in Sepsis. Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS
 Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
The Management and Treatment of Ruptured Abdominal Aortic Aneurysm (RAAA)
") The Management and Treatment of Ruptured Abdominal Aortic Aneurysm (RAAA) Disclosure Speaker name: Ren Wei, Li Zhui, Li Fenghe, Zhao Yu Department of Vascular Surgery, The First Affiliated Hospital of
The Management and Treatment of Ruptured Abdominal Aortic Aneurysm (RAAA) Disclosure Speaker name: Ren Wei, Li Zhui, Li Fenghe, Zhao Yu Department of Vascular Surgery, The First Affiliated Hospital of
Sepsis overview. Dr. Tsang Hin Hung MBBS FHKCP FRCP
 Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Continuous monitoring of cardiac output: why and how
 33rd International Symposium of Intensive Care and Emergency Medicine, Brussels 19.03.-22.03.2013 UNIVERSITÄTSKLINIKUM Schleswig-Holstein Continuous monitoring of cardiac output: why and how Berthold Bein,
33rd International Symposium of Intensive Care and Emergency Medicine, Brussels 19.03.-22.03.2013 UNIVERSITÄTSKLINIKUM Schleswig-Holstein Continuous monitoring of cardiac output: why and how Berthold Bein,
Patient Blood Management: Enough is Enough
 Patient Blood Management: Enough is Enough Richard Benjamin, MBChB, PhD, FRCPath Professor of Pathology Georgetown University Medical Center Washington, D.C. Chief Medical Officer Cerus Corporation Concord,
Patient Blood Management: Enough is Enough Richard Benjamin, MBChB, PhD, FRCPath Professor of Pathology Georgetown University Medical Center Washington, D.C. Chief Medical Officer Cerus Corporation Concord,
Nothing to disclose 9/25/2017
 Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
3 papers from ED. counting sepsis sepsis 3 wet or dry?
 3 papers from ED counting sepsis sepsis 3 wet or dry? 5 million deaths/yr globally 24 billion USD annually in US system causes or contributes to half of US hospital deaths BP GCS RR From: The Third International
3 papers from ED counting sepsis sepsis 3 wet or dry? 5 million deaths/yr globally 24 billion USD annually in US system causes or contributes to half of US hospital deaths BP GCS RR From: The Third International
9/25/2017. Nothing to disclose
 Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Use of Blood Lactate Measurements in the Critical Care Setting
 Use of Blood Lactate Measurements in the Critical Care Setting John G Toffaletti, PhD Director of Blood Gas and Clinical Pediatric Labs Professor of Pathology Duke University Medical Center Chief, VAMC
Use of Blood Lactate Measurements in the Critical Care Setting John G Toffaletti, PhD Director of Blood Gas and Clinical Pediatric Labs Professor of Pathology Duke University Medical Center Chief, VAMC
Tailored Volume Resuscitation in the Critically Ill is Achievable. Objectives. Clinical Case 2/16/2018
 Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
The Blue Baby. Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin
 The Blue Baby Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin Session Structure Definitions and assessment of cyanosis Causes of blue baby Structured approach to assessing
The Blue Baby Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin Session Structure Definitions and assessment of cyanosis Causes of blue baby Structured approach to assessing
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Early-goal-directed therapy and protocolised treatment in septic shock
 CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
AllinaHealthSystem 1
 : Definition End-organ hypoperfusion secondary to cardiac failure Venoarterial ECMO: Patient Selection Michael A. Samara, MD FACC Advanced Heart Failure, Cardiac Transplant & Mechanical Circulatory Support
: Definition End-organ hypoperfusion secondary to cardiac failure Venoarterial ECMO: Patient Selection Michael A. Samara, MD FACC Advanced Heart Failure, Cardiac Transplant & Mechanical Circulatory Support
Early Goal-Directed Therapy
 Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Supplement Table 1. Definitions for Causes of Death
 Supplement Table 1. Definitions for Causes of Death 3. Cause of Death: To record the primary cause of death. Record only one answer. Classify cause of death as one of the following: 3.1 Cardiac: Death
Supplement Table 1. Definitions for Causes of Death 3. Cause of Death: To record the primary cause of death. Record only one answer. Classify cause of death as one of the following: 3.1 Cardiac: Death
SHOCK Susanna Hilda Hutajulu, MD, PhD
 SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
UPDATE IN HOSPITAL MEDICINE
 UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
IV fluid administration in sepsis. Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London
 IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
Stressed Out: Evaluating the Need for Stress Ulcer Prophylaxis in the ICU
 Stressed Out: Evaluating the Need for Stress Ulcer Prophylaxis in the ICU Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds November 8, 2016 2016 MFMER slide-1 Objectives Identify the significance
Stressed Out: Evaluating the Need for Stress Ulcer Prophylaxis in the ICU Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds November 8, 2016 2016 MFMER slide-1 Objectives Identify the significance
STEMI and Cardiogenic Shock. The rules and solution. Dave Kettles St Dominics and Frere Hospitals East London ZA
 STEMI and Cardiogenic Shock. The rules and solution Dave Kettles St Dominics and Frere Hospitals East London ZA Definitions: Shock is a life threatening, but initially reversible state of cellular and
STEMI and Cardiogenic Shock. The rules and solution Dave Kettles St Dominics and Frere Hospitals East London ZA Definitions: Shock is a life threatening, but initially reversible state of cellular and
Impact of Fluids in Children with Acute Lung Injury
 Impact of Fluids in Children with Acute Lung Injury Canadian Critical Care Forum Toronto, Canada October 27 th, 2015 Adrienne G. Randolph, MD, MSc Critical Care Division, Department of Anesthesia, Perioperative
Impact of Fluids in Children with Acute Lung Injury Canadian Critical Care Forum Toronto, Canada October 27 th, 2015 Adrienne G. Randolph, MD, MSc Critical Care Division, Department of Anesthesia, Perioperative
Objectives. Design: Setting &Patients: Patients. Measurements and Main Results: Common. Adverse events VS Mortality
 ADVERSE EVENTS AND THEIR RELATION TO MORTALITY IN OUT-OF-HOSPITAL CARDIAC ARREST PATIENTS TREATED WITH THERAPEUTIC HYPOTHERMIA Reporter R1 吳志華 Supervisor VS 王瑞芳 100.04.02 Niklas Nielsen, MD, PhD; Kjetil
ADVERSE EVENTS AND THEIR RELATION TO MORTALITY IN OUT-OF-HOSPITAL CARDIAC ARREST PATIENTS TREATED WITH THERAPEUTIC HYPOTHERMIA Reporter R1 吳志華 Supervisor VS 王瑞芳 100.04.02 Niklas Nielsen, MD, PhD; Kjetil
Abdominal Aortic Aneurysm - Part 1. Learning Objectives. Disclosure. University of Toronto Division of Vascular Surgery
 University of Toronto Division of Vascular Surgery Abdominal Aortic Aneurysm - Part 1 Dr Mark Wheatcroft & Dr Elisa Greco Vascular Surgeon, St Michael s Hospital, Toronto & University of Toronto Disclosure
University of Toronto Division of Vascular Surgery Abdominal Aortic Aneurysm - Part 1 Dr Mark Wheatcroft & Dr Elisa Greco Vascular Surgeon, St Michael s Hospital, Toronto & University of Toronto Disclosure
Shock. Undifferentiated Shock: Beyond Blood Pressure. Shock. Epidemiology. Matthew Strehlow, MD Stanford University
 Shock Undifferentiated Shock: Beyond Blood Pressure Matthew Strehlow, MD Stanford University Shock Shock - The rude unhinging of the machinery of life -SD Gross 1872 Epidemiology Shock - inadequate tissue
Shock Undifferentiated Shock: Beyond Blood Pressure Matthew Strehlow, MD Stanford University Shock Shock - The rude unhinging of the machinery of life -SD Gross 1872 Epidemiology Shock - inadequate tissue
No conflicts of interest
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Date written: April 2014 Review date: April 2016 Related documents: Paediatric Sepsis 6
 Scottish Paediatric Retrieval Service (Edinburgh) www.paedsretrieval.com Clinical Guideline SEPSIS Date written: April 2014 Review date: April 2016 Related documents: Paediatric Sepsis 6 Author: Steve
Scottish Paediatric Retrieval Service (Edinburgh) www.paedsretrieval.com Clinical Guideline SEPSIS Date written: April 2014 Review date: April 2016 Related documents: Paediatric Sepsis 6 Author: Steve
Sleep Apnea and ifficulty in Extubation. Jean Louis BOURGAIN May 15, 2016
 Sleep Apnea and ifficulty in Extubation Jean Louis BOURGAIN May 15, 2016 Introduction Repetitive collapse of the upper airway > sleep fragmentation, > hypoxemia, hypercapnia, > marked variations in intrathoracic
Sleep Apnea and ifficulty in Extubation Jean Louis BOURGAIN May 15, 2016 Introduction Repetitive collapse of the upper airway > sleep fragmentation, > hypoxemia, hypercapnia, > marked variations in intrathoracic
Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine
 Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine Venous thromboembolism: pulmonary embolism (PE) deep vein thrombosis (DVT) 1% of all patients admitted to hospital 5% of in-hospital mortality
Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine Venous thromboembolism: pulmonary embolism (PE) deep vein thrombosis (DVT) 1% of all patients admitted to hospital 5% of in-hospital mortality
SAFE approach. Unresponsive? Shout or call for help. Open Airway. Not Breathing normally? 30 chest compressions. 2 rescue breaths
 Basic Life Support Dial 2222 Chin lift, head tilt jaw thrust Look, listen, feel For 10 seconds Rate 100/min *Lateral tilt* SAFE approach Unresponsive? Shout or call for help Open Airway Not Breathing normally?
Basic Life Support Dial 2222 Chin lift, head tilt jaw thrust Look, listen, feel For 10 seconds Rate 100/min *Lateral tilt* SAFE approach Unresponsive? Shout or call for help Open Airway Not Breathing normally?
Case Scenario 3: Shock and Sepsis
 Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
How to Address an Inappropriately high Mortality Rate? Joe Sharma, MD Associate Professor of Surgery NSQIP Surgical Champion
 How to Address an Inappropriately high Mortality Rate? Joe Sharma, MD Associate Professor of Surgery NSQIP Surgical Champion Disclosure Slide No COI and no disclosures. Hospital Mortality rate : is it
How to Address an Inappropriately high Mortality Rate? Joe Sharma, MD Associate Professor of Surgery NSQIP Surgical Champion Disclosure Slide No COI and no disclosures. Hospital Mortality rate : is it
Fluids and Lactate. A/Prof Peter Morley
 Fluids and Lactate A/Prof Peter Morley RCTs Other evidence 5 6 Plan Background information Crystalloids Which crystalloid? Colloids Crystalloids v colloids Once that s settled, how much fluid Plan Background
Fluids and Lactate A/Prof Peter Morley RCTs Other evidence 5 6 Plan Background information Crystalloids Which crystalloid? Colloids Crystalloids v colloids Once that s settled, how much fluid Plan Background
New Strategies in the Management of Patients with Severe Sepsis
 New Strategies in the Management of Patients with Severe Sepsis Michael Zgoda, MD, MBA President, Medical Staff Medical Director, ICU CMC-University, Charlotte, NC Factors of increases in the dx. of severe
New Strategies in the Management of Patients with Severe Sepsis Michael Zgoda, MD, MBA President, Medical Staff Medical Director, ICU CMC-University, Charlotte, NC Factors of increases in the dx. of severe
ICU treatment of the trauma patient. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 ICU treatment of the trauma patient Intensive Care Training Program Radboud University Medical Centre Nijmegen Christian Kleber Surgical Intensive Care Unit - The trauma surgery Perspective Langenbecks
ICU treatment of the trauma patient Intensive Care Training Program Radboud University Medical Centre Nijmegen Christian Kleber Surgical Intensive Care Unit - The trauma surgery Perspective Langenbecks
Landmark articles on ventilation
 Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Transfusion Medicine Potpourri. BUMC - Phoenix Internal Medicine Residents September 29, 2015
 Transfusion Medicine Potpourri BUMC - Phoenix Internal Medicine Residents September 29, 2015 Clinical case A 24 year old female with sickle cell anemia has just moved to the area and presents as a new
Transfusion Medicine Potpourri BUMC - Phoenix Internal Medicine Residents September 29, 2015 Clinical case A 24 year old female with sickle cell anemia has just moved to the area and presents as a new
MICHIGAN. Table of Contents. State Protocols. Adult Treatment Protocols
 MICHIGAN State Protocols Protocol Number Protocol Name Adult Treatment Protocols Table of Contents 3.1 Altered Mental Status 3.2 Stroke/Suspected Stroke 3.3 Respiratory Distress 3.4 Seizures 3.5 Sepsis
MICHIGAN State Protocols Protocol Number Protocol Name Adult Treatment Protocols Table of Contents 3.1 Altered Mental Status 3.2 Stroke/Suspected Stroke 3.3 Respiratory Distress 3.4 Seizures 3.5 Sepsis
Resuscitation Symposium Resuscitation Literature Update. Abdullah Al Reesi, MD, MSc, FACEP, FRCPC Sr. Consultant and HoD SQUH
 Resuscitation Symposium Resuscitation Literature Update Abdullah Al Reesi, MD, MSc, FACEP, FRCPC Sr. Consultant and HoD SQUH Objectives Review recent articles in sepsis New sepsis definition High versus
Resuscitation Symposium Resuscitation Literature Update Abdullah Al Reesi, MD, MSc, FACEP, FRCPC Sr. Consultant and HoD SQUH Objectives Review recent articles in sepsis New sepsis definition High versus
Approach to type 2 Respiratory Failure
 Approach to type 2 Respiratory Failure Changing Nature of NIV Not longer just the traditional COPD patients Increasingly Obesity Neuromuscular Pneumonias 3 fold increase in patients with Ph 7.25 and below
Approach to type 2 Respiratory Failure Changing Nature of NIV Not longer just the traditional COPD patients Increasingly Obesity Neuromuscular Pneumonias 3 fold increase in patients with Ph 7.25 and below
SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY
 PS1070 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY TITLE: ADMISSION/DISCHARGE CRITERIA: CARDIOVASCULAR INTENSIVE Job Title of Reviewer: Director, CVICU EFFECTIVE DATE: REVIEWED/REVISED DATE: POLICY
PS1070 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY TITLE: ADMISSION/DISCHARGE CRITERIA: CARDIOVASCULAR INTENSIVE Job Title of Reviewer: Director, CVICU EFFECTIVE DATE: REVIEWED/REVISED DATE: POLICY
Evidence- Based Medicine Fluid Therapy
 Evidence- Based Medicine Fluid Therapy Ndidi Musa M.D. Assosciate Professor of Pediatrics Medical College of Wisconsin/ Children s Hospital of Wisconsin Disclosures A. I have no relevant financial relationships
Evidence- Based Medicine Fluid Therapy Ndidi Musa M.D. Assosciate Professor of Pediatrics Medical College of Wisconsin/ Children s Hospital of Wisconsin Disclosures A. I have no relevant financial relationships
Update on Sudden Cardiac Death and Resuscitation
 Update on Sudden Cardiac Death and Resuscitation Ashish R. Panchal, MD, PhD Medical Director Center for Emergency Medical Services Assistant Professor Clinical Department of Emergency Medicine The Ohio
Update on Sudden Cardiac Death and Resuscitation Ashish R. Panchal, MD, PhD Medical Director Center for Emergency Medical Services Assistant Professor Clinical Department of Emergency Medicine The Ohio
Perioperative TTE an under-utilised modality?
 Perioperative TTE an under-utilised modality? David Canty Senior Lecturer Department of Surgery, University of Melbourne Cardiothoracic Anaesthetist Disclosures Employed University of Melbourne POC workshops,
Perioperative TTE an under-utilised modality? David Canty Senior Lecturer Department of Surgery, University of Melbourne Cardiothoracic Anaesthetist Disclosures Employed University of Melbourne POC workshops,
SHOCK and the Trauma Victim. JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital.
 SHOCK and the Trauma Victim JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital. Classification of Shock Cardiogenic - Myopathic Arrythmic Mechanical Hypovolaemic - Haemorrhagic Non-haemorrhagic
SHOCK and the Trauma Victim JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital. Classification of Shock Cardiogenic - Myopathic Arrythmic Mechanical Hypovolaemic - Haemorrhagic Non-haemorrhagic
Adult Basic Life Support
 Adult Basic Life Support UNRESPONSIVE? Shout for help Open airway NOT BREATHING NORMALLY? Call 112* 30 chest compressions 2 rescue breaths 30 compressions *or national emergency number Fig 1.2_Adult BLS
Adult Basic Life Support UNRESPONSIVE? Shout for help Open airway NOT BREATHING NORMALLY? Call 112* 30 chest compressions 2 rescue breaths 30 compressions *or national emergency number Fig 1.2_Adult BLS
Objectives. Management of Septic Shock. Definitions Progression of sepsis. Epidemiology of severe sepsis. Major goals of therapy
 Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
TEACHING BASIC LIFE SUPPORT (& ALS)
") TEACHING BASIC LIFE SUPPORT (& ALS) Anton Koželj, R.N., B. Sc., lecturer Faculty of Health Sciences, University of Maribor Žitna ulica 15, 2000 Maribor, Slovenia Fact s To know-how to perform basic life
TEACHING BASIC LIFE SUPPORT (& ALS) Anton Koželj, R.N., B. Sc., lecturer Faculty of Health Sciences, University of Maribor Žitna ulica 15, 2000 Maribor, Slovenia Fact s To know-how to perform basic life
ICU Referral For Common Medical Disorders. Prof. M A Jalil Chowdhury
 ICU Referral For Common Medical Disorders Prof. M A Jalil Chowdhury Intensive Care Unit (ICU) An intensive care unit (ICU), also known as an critical care unit (CCU), is a special department of a hospital
ICU Referral For Common Medical Disorders Prof. M A Jalil Chowdhury Intensive Care Unit (ICU) An intensive care unit (ICU), also known as an critical care unit (CCU), is a special department of a hospital
SHOCK AETIOLOGY OF SHOCK (1) Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function
 Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function") SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
Bedside assessment of fluid status
 Bedside assessment of fluid status 2nd AKI Academy October 18 th 2014 David Treacher Guy s & St Thomas NHS Trust Assessing the circulation - the 3 key questions v Is my patient adequately filled? v What
Bedside assessment of fluid status 2nd AKI Academy October 18 th 2014 David Treacher Guy s & St Thomas NHS Trust Assessing the circulation - the 3 key questions v Is my patient adequately filled? v What
Acute Kidney Injury for the General Surgeon
 Acute Kidney Injury for the General Surgeon UCSF Postgraduate Course in General Surgery Maui, HI March 20, 2011 Epidemiology & Definition Pathophysiology Clinical Studies Management Summary Hobart W. Harris,
Acute Kidney Injury for the General Surgeon UCSF Postgraduate Course in General Surgery Maui, HI March 20, 2011 Epidemiology & Definition Pathophysiology Clinical Studies Management Summary Hobart W. Harris,
Point-of-Care Ultrasound Closer look at the Inferior Vena Cavae &
 Point-of-Care Ultrasound Closer look at the Inferior Vena Cavae & Brief Introduction to Gross Systolic Function Omar S. Darwish, MS, DO Certified in Point-of-Care Ultrasound Hospitalist University of California,
Point-of-Care Ultrasound Closer look at the Inferior Vena Cavae & Brief Introduction to Gross Systolic Function Omar S. Darwish, MS, DO Certified in Point-of-Care Ultrasound Hospitalist University of California,
Sepsis Pathophysiology
 Sepsis Pathophysiology How Kids Differ From Adults Steve Standage Pediatric Critical Care Medicine Seattle Children's Hospital University of Washington School of Medicine Disclosures & Preamble No agenda,
Sepsis Pathophysiology How Kids Differ From Adults Steve Standage Pediatric Critical Care Medicine Seattle Children's Hospital University of Washington School of Medicine Disclosures & Preamble No agenda,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Updates in Sepsis 2017
 Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Objectives. Health care significance of ARF 9/10/15 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION
 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
Sepsis Update: Focus on Early Recognition and Intervention. Disclosures
 Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Emergency Intraoperative Echocardiography
 Emergency Intraoperative Echocardiography Justiaan Swanevelder Department of Anaesthesia, Glenfield Hospital University Hospitals of Leicester NHS Trust, UK Carl Gustav Jung (1875-1961) Your vision will
Emergency Intraoperative Echocardiography Justiaan Swanevelder Department of Anaesthesia, Glenfield Hospital University Hospitals of Leicester NHS Trust, UK Carl Gustav Jung (1875-1961) Your vision will
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abdomen, and aorta, as causes of shock, point-of-care ultrasonography in assessment of, 915 917 Abdominal compartment syndrome, trauma patient
Note: Page numbers of article titles are in boldface type. A Abdomen, and aorta, as causes of shock, point-of-care ultrasonography in assessment of, 915 917 Abdominal compartment syndrome, trauma patient
Controversies in Hospital Medicine: Critical Care. Vasopressors, Steroids, and Insulin Therapy
 Controversies in Hospital Medicine: Critical Care Vasopressors, Steroids, and Insulin Therapy Douglas Fish, Pharm.D. Professor of Pharmacy, University of Colorado Denver Clinical Specialist in Critical
Controversies in Hospital Medicine: Critical Care Vasopressors, Steroids, and Insulin Therapy Douglas Fish, Pharm.D. Professor of Pharmacy, University of Colorado Denver Clinical Specialist in Critical
Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium
 Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium MARIA E. MANDICH MD Fairbanks Memorial Hospital Emergency Department Attending Physician Interior Region EMS Council Medical Director
Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium MARIA E. MANDICH MD Fairbanks Memorial Hospital Emergency Department Attending Physician Interior Region EMS Council Medical Director
PRE Operative Care of the High Risk Surgical Patient. Dr A T Dewhurst Consultant Anaesthetist St George s Hospital London
 PRE Operative Care of the High Risk Surgical Patient Dr A T Dewhurst Consultant Anaesthetist St George s Hospital London Perioperative Optimization Shoemaker oxygen delivery goal directed therapy ITS NOT
PRE Operative Care of the High Risk Surgical Patient Dr A T Dewhurst Consultant Anaesthetist St George s Hospital London Perioperative Optimization Shoemaker oxygen delivery goal directed therapy ITS NOT
Transfusion for the sickest ICU patients: Are there unanswered questions?
 Transfusion for the sickest ICU patients: Are there unanswered questions? Tim Walsh Professor of Critical Care Edinburgh University None Conflict of Interest Guidelines on the management of anaemia and
Transfusion for the sickest ICU patients: Are there unanswered questions? Tim Walsh Professor of Critical Care Edinburgh University None Conflict of Interest Guidelines on the management of anaemia and
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
Evaluation of Social Science Interventions. A/Prof Daryl Jones
 Evaluation of Social Science Interventions A/Prof Daryl Jones Conflict of interest ACQSHC - $AU $77k research grant Eastern Health - $ AU 5k consultancy fees Academic bias RRT Overview What are social
Evaluation of Social Science Interventions A/Prof Daryl Jones Conflict of interest ACQSHC - $AU $77k research grant Eastern Health - $ AU 5k consultancy fees Academic bias RRT Overview What are social
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
Prehospital Care Bundles
 Prehospital s The MLREMS Prehospital s have been created to provide a simple framework to help EMS providers identify the most critical elements when caring for a patient. These bundles do not replace
Prehospital s The MLREMS Prehospital s have been created to provide a simple framework to help EMS providers identify the most critical elements when caring for a patient. These bundles do not replace
Surgery Grand Rounds. Non-invasive Ventilation: A valuable tool. James Cromie, PGY 3 8/24/09
 Surgery Grand Rounds Non-invasive Ventilation: A valuable tool James Cromie, PGY 3 8/24/09 History of mechanical ventilation 1930 s: use of iron lung 1940 s: First NIV system (Bellevue Hospital) 1950 s:
Surgery Grand Rounds Non-invasive Ventilation: A valuable tool James Cromie, PGY 3 8/24/09 History of mechanical ventilation 1930 s: use of iron lung 1940 s: First NIV system (Bellevue Hospital) 1950 s:
Rounds in the ICU. Eran Segal, MD Director General ICU Sheba Medical Center
 Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
Intra-operative Echocardiography: When to Go Back on Pump
 Intra-operative Echocardiography: When to Go Back on Pump GREGORIO G. ROGELIO, MD., F.P.C.C. OUTLINE A. Indications for Intraoperative Echocardiography B. Role of Intraoperative Echocardiography C. Criteria
Intra-operative Echocardiography: When to Go Back on Pump GREGORIO G. ROGELIO, MD., F.P.C.C. OUTLINE A. Indications for Intraoperative Echocardiography B. Role of Intraoperative Echocardiography C. Criteria
CPR What Works, What Doesn t
 Resuscitation 2017 ECMO and ECLS April 1, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Circulation 2013;128:417-35
Resuscitation 2017 ECMO and ECLS April 1, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Circulation 2013;128:417-35
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI)
") Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
Response to questions at ACCA Webinar on Echocardiography in Critical Care
 Response to questions at ACCA Webinar on Echocardiography in Critical Care The participants in the Webinar were Bernard Cosyns [Professor of Cardiology at the Free University, Brussels, Belgium, and Chairman
Response to questions at ACCA Webinar on Echocardiography in Critical Care The participants in the Webinar were Bernard Cosyns [Professor of Cardiology at the Free University, Brussels, Belgium, and Chairman
Immunomodulation and Sepsis in Oncological Patients. Imad Haddad, M.D. Medical Director, PICU Banner Children s Hospital at BDMC
 Immunomodulation and Sepsis in Oncological Patients Imad Haddad, M.D. Medical Director, PICU Banner Children s Hospital at BDMC 1 Objectives Immune dys-regulation in oncological septic patients Implementation
Immunomodulation and Sepsis in Oncological Patients Imad Haddad, M.D. Medical Director, PICU Banner Children s Hospital at BDMC 1 Objectives Immune dys-regulation in oncological septic patients Implementation
IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING
 IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING Christopher Hunter, MD, PhD, FACEP Director, Health Services Department Associate Medical Director, Orange County EMS System Medical Director, Orlando Health
IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING Christopher Hunter, MD, PhD, FACEP Director, Health Services Department Associate Medical Director, Orange County EMS System Medical Director, Orlando Health
From Bench to Bedside: Reducing Sepsis Mortality
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/clinicians-roundtable/from-bench-to-bedside-reducing-sepsismortality/4009/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/clinicians-roundtable/from-bench-to-bedside-reducing-sepsismortality/4009/
University of Florida Department of Surgery. CardioThoracic Surgery VA Learning Objectives
 University of Florida Department of Surgery CardioThoracic Surgery VA Learning Objectives This service performs coronary revascularization, valve replacement and lung cancer resections. There are 2 faculty
University of Florida Department of Surgery CardioThoracic Surgery VA Learning Objectives This service performs coronary revascularization, valve replacement and lung cancer resections. There are 2 faculty
Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit
 Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit * Patient s name and age * Surgical procedure and type of anesthetic including drugs used * Other intraoperative
Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit * Patient s name and age * Surgical procedure and type of anesthetic including drugs used * Other intraoperative