Articles in PresS. J Appl Physiol (September 29, 2005). doi: /japplphysiol
|
|
|
- Austin Kelley
- 5 years ago
- Views:
Transcription
1 Articles in PresS. J Appl Physiol (September 29, 2005). doi: /japplphysiol Assessment of Left Ventricular Diastolic Function by Early Diastolic Mitral Annulus Peak Acceleration Rate: Experimental Studies and Clinical Application Qinyun Ruan, MD, Liyun Rao, PhD, Katherine J Middleton, RCT, Dirar S Khoury, PhD, Sherif F. Nagueh, MD From the First Affiliated Hospital of Fujian Medical University, Fuzhou, China, from the Methodist Debakey Heart Center and from the Section of Cardiology, Department of Medicine, Baylor College of Medicine, Houston, Texas Correspondence and reprint requests Sherif F. Nagueh, MD Methodist DeBakey Heart Center 6550 Fannin Street, Suite-677 Houston, Texas Phone: snagueh@tmh.tmc.edu Copyright 2005 by the American Physiological Society.
2 2 Abstract We sought to examine the hemodynamic determinants and clinical application of the peak acceleration rate of early (Ea) diastolic velocity of the mitral annulus by tissue Doppler. Simultaneous LA and left ventricular (LV) catheterization and Doppler echocardiography (DE) were performed in 10 dogs. Preload was altered using volume infusion and caval occlusion, whereas myocardial lusitropic state was altered with dobutamine and esmolol. The clinical application was examined in 190 consecutive patients (control: 55, impaired relaxation: 41, pseudonormal: 46 and restrictive LV filling: 48). In addition, in 60 consecutive patients, we examined the relation between it and mean wedge pressure (PCWP) with simultaneous DE and right heart catheterization. In canine studies, a significant positive relation was present between peak Acc rate of Ea and transmitral pressure gradient only in the stages with normal or enhanced LV relaxation, but with no relation in the stages where was 50 ms. Its hemodynamic determinants were:, LV minimal pressure and transmitral pressure gradient. In clinical studies, peak Acc rate of Ea was significantly lower in patients with impaired LV relaxation irrespective of filling pressures (p<0.001), and with similar accuracy to peak Ea velocity (AUC for septal and lateral peak Acc rates: both 0.78) in identifying these patients. No significant relation was observed between peak Acc rate and PCWP. Peak acceleration rate of Ea appears to be a useful index of LV relaxation but not of filling pressures and can be applied to identify patients with impaired LV relaxation irrespective of their filling pressures.
3 3 Left ventricular (LV) diastolic function plays an important role in determining LV filling pressures and pulmonary congestion symptoms (14) in patients with and without depressed LV ejection fraction (EF). Novel non-invasive indices utilizing tissue Doppler imaging (TDI) have been recently applied for the evaluation of LV diastolic function and the prediction of filling pressures (3, 6, 9-10). Two of these indices include combined measurements of mitral inflow and TD signals of annular early diastolic excursion (3, 6, 9-10). The above methods have the disadvantage of multiple measurements from different cardiac cycles. A single measurement, if accurate, could be more applicable clinically. In this regard, a single measurement of the peak acceleration rate (P Acc) of early diastolic annular velocity (Ea) was shown in an animal model to provide a good assessment of left atrial pressure (4). Its clinical utility however, was not examined. We therefore sought to examine the hemodynamic determinants of the peak acceleration rate of Ea in experimental studies and to assess its clinical application in consecutive patients, including those referred for right heart catheterization. Methods Animal Preparation After the Baylor College of Medicine Animal Research Committee approved the study, 10 healthy adult mongrel dogs (weight: 19 to 28 kg) were anesthetized with sodium pentobarbital (30mg/kg), intubated, and mechanically ventilated with an external respirator. After a midline sternotomy, the heart was exposed and after calibration, a high fidelity 5-F pressure catheter (Millar Instruments, Houston, TX) was introduced into the left atrium (LA) through its appendage. Likewise, to measure LV pressures, a calibrated 5-F 12-electrode pressure catheter (Millar) was advanced into the LV by crossing the aortic valve (positioned along LV long axis). Surface electrocardiogram (lead II), atrial, and ventricular pressure signals were simultaneously acquired on
4 4 computer based data acquisition system and LA and LV pressures were digitized with recordings acquired at end expiration. The inferior vena cava (IVC) was dissected and a ring was placed around it to allow for gradual occlusion of the vein. Hemodynamic Measurements LV minimal pressure and LVEDP, maximal instantaneous diastolic transmitral pressure and LA mean pressure were noted. Also ascertained were the first derivatives of LV pressure in diastole (-dp/dt), and the time constant of LV relaxation (tau: ) (13). Echocardiography The animals were imaged from the epicardium using an ultrasound system equipped with TD imaging capability. In the apical 4-chamber view, PW Doppler was applied to record mitral inflow at the valve tips (intraobserver variability for measuring mitral peak E velocity: 3±1%). TD program was applied in PW Doppler to record mitral annular velocities at the septal and lateral areas (6). The peak velocity of Ea (intraobserver variability 5±2%) at above sites of the annulus was measured under the different loading conditions. The time interval between the peak of R wave and onset of mitral E velocity and between peak of R wave and onset of early diastolic velocity (Ea) at the 4 areas of the mitral annulus were measured. Subsequently the difference between these time intervals (T Ea E ) was calculated (10) for each of the 4 areas and an average value was derived (intraobserver variability 4±2%, interobserver variability 6±2%). The peak acceleration rate of Ea velocity was derived by the computer after the Ea velocity was traced. The computer algorithm used divided the time from the onset of Ea to its peak into 20 equal intervals and measured the change in velocity per unit of time in each interval and reported the highest value (interobserver variability 8±4%). In an attempt to simplify the measurement of acceleration rate of Ea, we also calculated
5 5 the mean acceleration rate as the Ea velocity divided by acceleration time. Interobserver variability was 6±3%. Experimental Protocols Initially LA pressure was increased with intravenous infusion of isotonic saline and decreased with inferior vena caval (IVC) external compression. Both the infusions and compressions were performed in a sequential manner with data acquired at predetermined increments and decrements of mean LA pressure. After achieving a stable hemodynamic state at each LA pressure level, the LA and the LV pressures and Doppler data, were acquired. After a stable hemodynamic state was achieved, to evaluate the influence of LV relaxation on Ea and its peak acceleration rate, dobutamine was administered at a dose of 5 ug/kg/min with Doppler and pressure data acquired. Dobutamine infusion was then terminated, and after the animals returned to their baseline state, esmolol with its negative lusitropic properties was administered (0.5 mg/kg intravenously) with subsequent reacquisition of data. To assess the possible interaction between atrial pressure and ventricular relaxation on the peak acceleration rate of Ea, fluid administration and IVC compression were repeated during dobutamine and esmolol infusion. Human Studies Study Group The institutional review board of Baylor College of Medicine approved the protocol and all patients provided written informed consent. The study sample was comprised of 190 consecutive patients referred for echocardiographic evaluation at our laboratory. Patients were divided according to the mitral inflow pattern, clinical data and echocardiographic examination into 4 groups (control, impaired relaxation or IR, pseudonormal or PN, and restrictive or Res.). Patients in the control group (n=55) had no history or evidence of cardiovascular disease with normal LV dimensions, wall
6 6 thickness, mass, normal PA systolic pressure and no evidence of significant valvular pathology on echocardiography. The IR group consisted of 41 patients with hypertension, coronary artery disease and/or LV hypertrophy, and a mitral inflow pattern with an early to late transmitral flow velocity (E/A) ratio <1.0. The PN group consisted of 46 patients with symptoms of pulmonary congestion and an E/A ratio 1.0. The Res. LV filling group consisted of 48 patients with symptoms of pulmonary congestion and an E/A ratio 2.0. An additional group of 60 consecutive patients who were undergoing right heart catheterization in the cardiac catheterization laboratory (n=25) or the intensive care unit (n=35) was included. All were in sinus rhythm ( beats/min) and with satisfactory Doppler and pressure recordings and no evidence of mitral stenosis, prosthetic mitral valve or severe mitral regurgitation. Patients had simultaneous echocardiographic and hemodynamic measurements. Echocardiographic studies: Patients were imaged in a supine position with an ultrasound system equipped with harmonic imaging, a multifrequency transducer and TD imaging capability. After acquiring parasternal and apical views, pulse-doppler was utilized to record transmitral and pulmonary venous flow in the apical 4-chamber view as previously described (8). TD imaging was applied in the PW mode to record the mitral annular velocities at the septal and lateral areas. Studies were recorded for later playback and analysis. Echocardiographic Analysis The analysis was performed offline without knowledge of hemodynamic data. LV EF and LA maximum volume were performed per the recommendations of the American Society of Echocardiography (12). All Doppler values represent the average of 3 beats. Pulmonary artery (PA) systolic pressure was estimated using the tricuspid regurgitation jet. Mitral inflow was analyzed for peak E, peak A velocities, E/A ratio and deceleration
7 7 (DT) time of E velocity. From the pulmonary vein flow velocities, the systolic filling fraction (SFF) and Ar A duration were computed (5, 11). Ea and Aa velocities at the 2 areas of the mitral annulus were measured (septal, and lateral). Peak and mean acceleration rates of Ea at septal and lateral sides of mitral annulus were also measured. In addition, the time interval between peak of R wave and onset of mitral E velocity as well as the time interval between peak of R wave and onset of Ea at the 4 areas of the mitral annulus were measured (10). Hemodynamic Measurements Hemodynamic data were collected by an investigator unaware of the echocardiographic measurements, at end expiration and represent the average of 5 cycles. PCWP (wedge verified by fluoroscopy, phasic changes in pressure waveforms and oxygen saturation) was determined using balanced transducers (0 level at mid-axillary line). Statistical Analysis Ea and its peak and mean acceleration rates were correlated with hemodynamic parameters using regression analysis. Stepwise regression was then used to determine the hemodynamic parameters that correlated best with the individual Doppler variables. The study was powered to detect a correlation coefficient of at least 0.4 between the transmitral pressure gradient and peak acceleration rate of Ea (power =80%, p =0.05). Repeated measures ANOVA with Bonferroni correction were used to compare Doppler and hemodynamic parameters at the different lusitropic states (baseline, dobutamine and esmolol) and loading conditions. ANOVA with Bonferroni correction was used to compare the control group with each of the other 3 groups (IR, PN and Res.). ROC curves were applied to examine the accuracy of TDI signals in identifying patients with increased LV filling pressures. Linear regression analysis was used to relate mean wedge pressure to Doppler measurements. Significance was set at a p value <0.05.
8 8 Results Hemodynamics and Doppler measurements: Animal studies Table 1 summarizes the hemodynamic and TD data (average of the 2 annular sites shown in the table since similar observations were noted at each separate site) at the different experimental stages. Volume expansion resulted in an increase in LV filling pressures, annular Ea and its peak and mean acceleration rate. IVC occlusion resulted in significantly opposite changes in the above measurements. Dobutamine infusion resulted in shorter along with an increase in annular Ea and its peak and mean acceleration rate. Esmolol infusion resulted in significantly opposite changes in the above measurements. In all of the above interventions, only esmolol infusion resulted in a significant change in T E-Ea, prolonging it. Relation of TD signals to LV Hemodynamics: Animal studies In individual dogs, the correlation coefficient of Ea velocity, peak and mean acceleration rate of Ea with LA mean pressure ranged from 0.4 to 0.75 (p value range: 0.1 to 0.03). As for LV relaxation, peak Ea velocity (r=-0.76) and its mean (r=-0.73) and peak acceleration rates (r=-0.75) exhibited strong relations to (all p <0.001) and -dp/dt (r ranging from 0.65 to 0.79, all p <0.001) (Figure 1). Peak and mean acceleration rates of Ea were also significantly related to LV minimal pressure (r = and r=-0.65, respectively, both p<0.01). The relation of peak acceleration rate of Ea to the transmitral pressure gradient was evaluated in all the experimental stages where was 50 ms and in those where was <50 ms. There was no significant relation between peak acceleration rate of Ea and the pressure gradient in the stages where 50 ms, whereas a significant positive relation emerged in the stages where was <50 ms (Figure 2).
9 9 On multiple regression analysis (model R 2 =0.79, p <0.01), the predictors of peak acceleration rate of Ea velocity were:, LV minimal pressure and transmitral pressure gradient. Human studies Clinical characteristics and Doppler echocardiographic variables for the 190 patients, divided into 4 groups are listed in table 2. No significant differences were observed between the 4 groups in age, heart rate or blood pressure. The control, pseudonormal (PN) and restrictive (Res.) groups displayed a higher E velocity, E/A ratio, and a shorter deceleration time (DT) compared with the impaired relaxation (IR) group. Mitral inflow however, did not differentiate between normal and PN groups. However, as previously reported, LA volume, PA systolic pressure and pulmonary venous SFF, and Ar-A duration were useful in that regard (see table 2). As expected, septal and lateral Ea velocities were significantly lower in patients with PN and restrictive LV filling in comparison with controls, whereas T E-Ea was significantly longer in the patient groups (table 2). Similar to peak Ea velocity, peak and mean acceleration rate of Ea were significantly lower in patients with PN and Res. LV filling when compared to controls (ANOVA, p<0.001; Bonferroni t-test p<0.05 for control group versus each of the other 3 groups). Figure 3 illustrates examples of TDI signals in 4 representative cases. Table 3 summarizes the accuracy of peak Ea velocity and its acceleration rate in identifying patients with impaired LV relaxation despite elevated filling pressures (ROC curves shown in figure 4). Relation to mean PCWP The mean age of this group was 60±15 years. The mean arterial pressure was 81±15 mmhg, whereas the mean pulmonary artery pressure was 33±10 mmhg. Mitral inflow pattern was that of IR in 20 patients, PN filling in 25 patients and restrictive filling
10 10 in 15 patients. Mean PCWP was 20±10 (range: 5-45) mmhg. A non significant trend for an inverse relation was noted between mean PCWP and septal (and lateral) peak Acc rate (peak acceleration rate: r=-0.23, p=0.08, figure 5). However significant correlations were noted with mitral E/A ratio (r=0.5, p<0.05), E/Ea ratio (r=0.69, p<0.01), isovolumic relaxation time (r=-0.55, p<0.01), and SFF (r=-0.53, p<0.05). Discussion The animal experiments show that the hemodynamic determinants of peak acceleration rate of Ea are transmitral pressure gradient, LV minimal pressure and LV relaxation. The relation between peak acceleration rate of Ea and transmitral pressure gradient is a direct linear relation only in the presence of normal or enhanced LV relaxation, but no direct correlation was noted in the presence of impaired LV relaxation. The clinical studies confirm and extend these animal observations. The peak acceleration rate of Ea, at either side of the mitral annulus, in patients with impaired LV relaxation (IR, PN and Res. groups) was significantly lower than in the age matched control group. Overall its accuracy in identifying patients with impaired relaxation and elevated filling pressures was similar to peak Ea velocity. Furthermore, in the subgroup with simultaneous invasive measurements, no relation was noted between mean PCWP and peak acceleration rate of Ea. Animal studies We used the PW signal at each side of the mitral annulus to calculate the peak Acc. rate of Ea. PW -unlike color Doppler- has the major advantage of superior temporal resolution which suits well the need to calculate the peak acceleration rate given the very short time (frequently <50 ms) when acceleration of Ea is occurring. An additional advantage to our method lies in the higher sampling rate afforded by using 20 intervals
11 11 for deriving the peak Acc rate, making it much less likely to miss the highest acceleration rate when limiting the analysis to longer time intervals. In the previous study (4), the peak acceleration rate of the Ea velocity, particularly at the septal side of the mitral annulus, increased significantly with blood infusion but was not altered by dobutamine or metoprolol administration. Unlike these findings, we noted that changes in the myocardial lusitropic state with either dobutamine or esmolol were effective in producing significant changes in peak acceleration rate of Ea. The magnitude of change in Ea peak acceleration rate was comparable to the change in peak Ea velocity induced by these drugs. Furthermore, the peak acceleration rate of Ea had a significant inverse correlation with the invasive measurements of LV relaxation that was almost identical to those of Ea peak velocity. The relation between the peak acceleration rate of Ea and filling pressures is a complicated one, and overall very similar to that of the peak Ea velocity itself, as previously reported in animal (3, 6) and human studies (1, 2). The relation between LA pressure and peak acceleration rate of Ea in the presence of cardiac dysfunction is very important for the clinical application of Ea Acc rate in the clinical setting, since the assessment of LV filling pressures is frequently needed in patients with cardiac disease. The previous animal work was limited in that regard due to the occurrence of only small changes in LA pressure with beta-blockers. However, the peak acceleration rate of Ea can be used to predict LV filling pressures in normal subjects, given the direct relation between this Doppler measurement and preload in normal states. On the other hand, our animal study provides the pathophysiologic reasons for not applying the peak acceleration rate of Ea to the estimation of LV filling pressures, in the presence of impaired LV relaxation (figure 2). Similar to the acceleration rate of Ea, T E-Ea duration was altered by dobutamine and esmolol but unlike the acceleration rate, IVC occlusion and esmolol infusion had no significant effect on this time interval. Overall
12 12 these results are similar with the observations of Hasegawa et al (3) who noted that Ea was progressively delayed after LA to LV pressure crossover and was significantly related to tau in an animal model of pacing induced heart failure. Human Studies In the human studies, the mean and peak acceleration rate of Ea at either side of the mitral annulus were significantly lower in patients with impaired LV relaxation, irrespective of LV filling pressures. It is interesting that the relation between mean wedge pressure and peak acceleration rate of Ea, shown in figure 5, in patients with cardiac disease was very similar to that observed in the canine experiments between transmitral pressure gradient and peak acceleration rate of Ea when LV relaxation was impaired as shown in figure 2 (interrupted line and open circles). Our study also shows that the accuracy of peak acceleration rate of Ea at either side of the mitral annulus for identifying patients with impaired LV relaxation despite elevated filling pressures (PN and restrictive LV filling groups), is similar to that of the peak Ea velocity. There was no incremental information gained over peak Ea velocity by measuring its acceleration rate. Given the above findings and the complexity of its measurement, peak Ea velocity rather than its acceleration rate is more suitable for the daily application in the laboratory.
13 13 References 1-Firstenberg MS, Levine BD, Garcia MJ, Greenberg NL, Cardon L, Morehead AJ, Zuckerman J, Thomas JD. Relationship of echocardiographic indices to pulmonary capillary wedge pressures in healthy volunteers. J Am Coll Cardiol 36: , Graham RJ, Gelman JS, Donelan L, Mottram PM, Peverill RE. Effect of preload reduction by haemodialysis on new indices of diastolic function. Clin Sci (Lond). 105: , Hasegawa H, Little WC, Ohno M, Brucks S, Morimoto A, Cheng HJ, Cheng CP. Diastolic mitral annular velocity during the development of heart failure. J Am Coll Cardiol 41: , Hashimoto I, Bhat AH, Li X, Jones M, Davies CH, Swanson JC, Schindera ST, Sahn DJ. Tissue Doppler-derived myocardial acceleration for evaluation of left ventricular diastolic function. J Am Coll Cardiol 44: , Kuecherer HF, Muhiudeen IA, Kusumoto FM, Lee E, Moulinier LE, Cahalan MK, Schiller NB. Estimation of mean left atrial pressure from transesophageal pulsed Doppler echocardiography of pulmonary venous flow. Circulation 82: , Nagueh SF, Middleton KJ, Kopelen HA, Zoghbi WA, Quinones MA. Doppler tissue imaging :A noninvasive technique for evaluation of left ventricular relaxation and estimation of filling pressures. J Am Coll Cardiol 30: , Nagueh SF, Sun H, Kopelen HA, Middleton KJ, Khoury DS. Hemodynamic determinants of the mitral annulus diastolic velocities by tissue Doppler. J Am Coll Cardiol 37: , Nishimura RA, Tajik AJ. Evaluation of diastolic filling of left ventricle in health and disease: Doppler echocardiography is the clinician's Rosetta Stone. J Am Coll Cardiol
14 14 30:8-18, Ommen SR, Nishimura RA, Appleton CP, Miller FA, Oh JK, Redfield MM, Tajik AJ. Clinical utility of Doppler echocardiography and tissue Doppler imaging in the estimation of left ventricular filling pressures: A comparative simultaneous Doppler-catheterization study. Circulation 102: , Rivas-Gotz C, Khoury DS, Manolios M, Rao L, Kopelen HA, Nagueh SF. Time interval between onset of mitral inflow and onset of early diastolic velocity by tissue Doppler: a novel index of left ventricular relaxation: experimental studies and clinical application. J Am Coll Cardiol 42: , Rossvoll O, Hatle LK. Pulmonary venous flow velocities recorded by transthoracic Doppler ultrasound: relation to left ventricular diastolic pressures. J Am Coll Cardiol 21: , Schiller NB, Shah PM, Crawford MH, DeMaria A, Devereux R, Feigenbaum H, Gutgesell H, Reichek N, Sahn D, Schnittger I, et al. Recommendations for quantitation of the left ventricle by two-dimensional echocardiography: American Society of Echocardiography Committee on Standards, Subcommittee on quantitation of twodimensional echocardiograms. J Am Soc Echocardiog 2: , Weiss JL, Frederiksen JW, Weisfeldt ML. Hemodynamic determinants of the time-course of fall in canine left ventricular pressure. J Clin Invest 58: , Zile MR, Brutsaert DL. New concepts in diastolic dysfunction and diastolic heart failure: Part I: diagnosis, prognosis, and measurements of diastolic function. Circulation 105: , 2002.
15 15 Figure Legends Figure 1 Relation of versus septal peak Ea velocity (left), and its peak acceleration rate (right). Figure 2 Relation of peak acceleration rate of Ea versus transmitral pressure gradient. Solid line and circles correspond to the stages where was < 50ms. The interrupted line and open circles correspond to the stages where was 50 ms. In the presence of normal or enhanced relaxation, a direct significant relation was present (r=0.71, p<0.01), whereas with impaired relaxation, no relation was observed between peak acceleration rate of Ea and transmitral pressure gradient (p>0.3). Figure 3 Examples of mitral inflow and TDI at septal annulus from patients in each of the 4 groups. Note the reduced Ea velocity in patients with PN and Res. LV filling, despite increased LV filling pressures. Peak acceleration rate of Ea in the normal subject was 330 cm/s 2, whereas it was reduced to 140 cm/s 2 in the patient with IR pattern, to 138 cm/s 2 in the patient with PN pattern and to 160 cm/s 2 in the patient with Res. filling. Figure 4 ROC curves showing the accuracy of septal peak acceleration rate of Ea (left), and lateral peak acceleration rate of Ea (right) in identifying patients with impaired LV relaxation despite increased LV filling pressures (PN and Res. filling groups). Figure 5 Plot of mean PCWP versus septal Ea peak acceleration rate.
16 16 Table 1. Hemodynamics and TD Velocities During Volume Loading, IVC Occlusion, Dobutamine and Esmolol Infusions Hemodynamic Parameter Baseline Volume Loading Data: Mean±SD; p <0.05 vs volume loading, IVC occlusion, dobutamine and esmolol stages; p <0.05 vs IVC occlusion, dobutamine and esmolol stages; p <0.05 vs IVC occlusion and esmolol stages; p<0.05 vs dobutamine and esmolol stages, p< 0.05 vs baseline, volume loading and IVC occlusion stages, p <0.05 vs esmolol stage; p <0.05 vs baseline, volume infusion, IVC occlusion and esmolol, p <0.05 vs baseline, volume loading, IVC occlusion and dobutamine stages. IVC Occlusion Dobutamine Esmolol LV Stroke Volume (ml) 20±5 28±4 14±4 23±4.5 16±5.4 Heart rate (beats/min) 115±6 115±8 118±12 136±3 103±8 LVEDP (mmhg) 5±3 11±5 2.1± ± ±3 LA mean pressure (mmhg) 7±4 11±6.4 3±2 3.5±2.2 15±4 Tau (ms) 42±10 44±9 39±8 26±7 87±8 LV -dp/dt (mmhg/s) 1840± ± ± ± ±367 Ea (cm/s) 5.2±1 5.9± ±1 8.8±0.8 3±0.7 Ea mean acceleration rate (cm/s 2 ) 74±15 90±19 63±20 100±21 53±20 Ea peak acceleration rate (cm/s 2 ) 105±25 129±21 91±19 143±33 69±18 T E-Ea (ms) 1±5 0±5 1±3 0±3 23±4
17 17 Table 2. Clinical and Doppler findings in the 4 patient groups Control (n=55) IR (n=41) PN (n=46) Res. (n=48) Age (years) 61±15 62±15 61±15 67±12 Heart rate (/min) 73±12 75±13 75±13 70±13 Mean arterial pressure (mmhg) 90±14 97±19 94±16 87±19 LV EF (%) 65±3* 53±17 55±17 50±15 Left atrial volume (ml) 43±11* 73±28 81±26 89±22 PA systolic pressure (mmhg) 30±3 35±13 44± ±10 Mitral E/A ratio 1.1± ± ±0.29 3±0.9 Deceleration time (ms) 220±86 252±84 188±69 169±43 Pulmonary veins (SFF) 0.6± ± ± ±0.1 Ar A duration (ms) 0±8* 18±10 45±11 58±10 Septal Ea (cm/s) 9.3±3.2* 5.2± ± ±1.5 Septal mean acceleration rate (cm/s 2 ) 131±53* 77±41 84±43 74±32 Septal peak acceleration rate (cm/s 2 ) 259±99* 159±88 178±87 149±75 Lateral Ea (cm/s) 11.3±4.7* 7.5± ± ±3.2 Lateral mean acceleration rate (cm/s 2 ) 161±68* 98±38 134±49 100±48 Lateral peak acceleration rate (cm/s 2 ) 311±116* 185±79 210± ±112 T E-Ea (ms) 3±5* 29±5 33±3 40±3 *: p <0.05 versus IR, PN and Res. groups, : p <0.05 vs control, IR and PN groups, : p <0.05 vs control and PN groups, : p <0.05 vs PN and Res groups, : p<0.05 vs Res. group, : p <0.05 vs PN
18 18 Table 3 Accuracy of peak Ea velocity and acceleration rate of Ea in identifying patients with impaired LV relaxation despite elevated filling pressures Sensitivity (%) Specificity (%) Area under ROC curve Septal Ea (<5.6 cm/s) ( ) * Septal peak acceleration rate (<195.5 cm/s 2 ) ( ) * Lateral Ea (<8.6 cm/s) ( ) * Lateral peak acceleration rate (<252 cm/s 2 ) ( ) * *: p<0.0001, numbers between parenthesis refer to 5-95% confidence intervals.
19 19 Peak Ea velocity (cm/s) r = p< Peak Acceleration Rate of Ea (cm/s 2 ) r = p< (ms) 1 Figure 1
20 20 Peak Acceleration Rate of Ea (cm/s 2 ) Maximum Transmitral Pressure Gradient (mmhg) 2 Figure 2


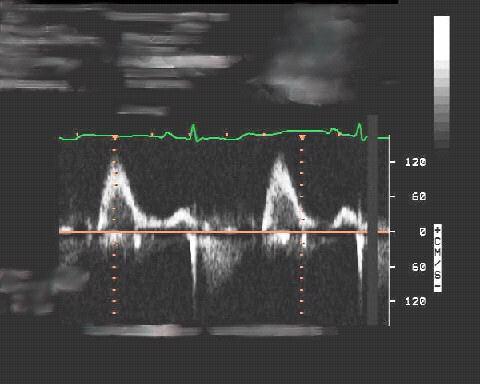


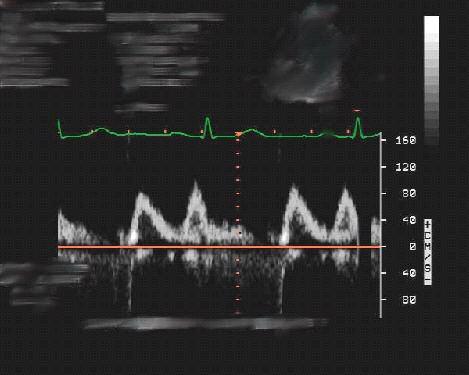
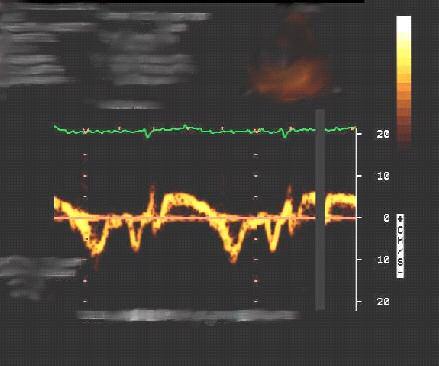
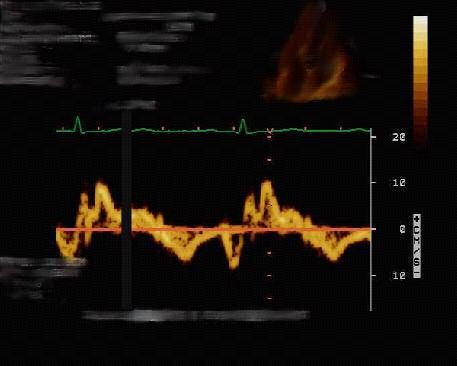
21 21 NL NL NL IR PN Res. E Ea Aa 3 Figure 3
22 22 ROC Curve for Septal Ea Pk Acc Rate ROC Curve for Lateral Ea Peak Acc Rate Figure 4
23 23 Peak Acc. Rate of Septal Ea (cm/s 2 ) Mean PCWP (mmhg) r = p = 0.08 Y = X 5 Figure 5
Effect of Heart Rate on Tissue Doppler Measures of E/E
 Cardiology Department of Bangkok Metropolitan Administration Medical College and Vajira Hospital, Bangkok, Thailand Abstract Background: Our aim was to study the independent effect of heart rate (HR) on
Cardiology Department of Bangkok Metropolitan Administration Medical College and Vajira Hospital, Bangkok, Thailand Abstract Background: Our aim was to study the independent effect of heart rate (HR) on
Rownak Jahan Tamanna 1, Rowshan Jahan 2, Abduz Zaher 3 and Abdul Kader Akhanda. 3 ORIGINAL ARTICLES
 University Heart Journal Vol. 4 No. 2 July 2008 ORIGINAL ARTICLES Correlation of Doppler echocardiography with cardiac catheterization in estimating pulmonary capillary wedge pressure: A tertiary level
University Heart Journal Vol. 4 No. 2 July 2008 ORIGINAL ARTICLES Correlation of Doppler echocardiography with cardiac catheterization in estimating pulmonary capillary wedge pressure: A tertiary level
An Integrated Approach to Study LV Diastolic Function
 An Integrated Approach to Study LV Diastolic Function Assoc. Prof. Adriana Ilieşiu, FESC University of Medicine Carol Davila Bucharest, Romania LV Diastolic Dysfunction impaired relaxation (early diastole)
An Integrated Approach to Study LV Diastolic Function Assoc. Prof. Adriana Ilieşiu, FESC University of Medicine Carol Davila Bucharest, Romania LV Diastolic Dysfunction impaired relaxation (early diastole)
Valvular Heart Disease. Doppler Estimation of Left Ventricular Filling Pressures in Patients With Mitral Valve Disease
 Valvular Heart Disease Doppler Estimation of Left Ventricular Filling Pressures in Patients With Mitral Valve Disease Abhvinav Diwan, MD; Marti McCulloch, RDCS; Gerald M. Lawrie, MD; Michael J. Reardon,
Valvular Heart Disease Doppler Estimation of Left Ventricular Filling Pressures in Patients With Mitral Valve Disease Abhvinav Diwan, MD; Marti McCulloch, RDCS; Gerald M. Lawrie, MD; Michael J. Reardon,
Noninvasive assessment of left ventricular (LV)
") Comparative Value of Tissue Doppler Imaging and M-Mode Color Doppler Mitral Flow Propagation Velocity for the Evaluation of Left Ventricular Filling Pressure* Michal Kidawa, MD; Lisa Coignard, MD; Gérard
Comparative Value of Tissue Doppler Imaging and M-Mode Color Doppler Mitral Flow Propagation Velocity for the Evaluation of Left Ventricular Filling Pressure* Michal Kidawa, MD; Lisa Coignard, MD; Gérard
The Patient with Atrial Fibrilation
 Assessment of Diastolic Function The Patient with Atrial Fibrilation Assoc. Prof. Adriana Ilieşiu, FESC University of Medicine Carol Davila Bucharest, Romania Associated Conditions with Atrial Fibrillation
Assessment of Diastolic Function The Patient with Atrial Fibrilation Assoc. Prof. Adriana Ilieşiu, FESC University of Medicine Carol Davila Bucharest, Romania Associated Conditions with Atrial Fibrillation
Left ventricular diastolic function and filling pressure in patients with dilated cardiomyopathy
 Left ventricular diastolic function and filling pressure in patients with dilated cardiomyopathy Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania My conflicts of interest: I have
Left ventricular diastolic function and filling pressure in patients with dilated cardiomyopathy Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania My conflicts of interest: I have
Jong-Won Ha*, Jeong-Ah Ahn, Jae-Yun Moon, Hye-Sun Suh, Seok-Min Kang, Se-Joong Rim, Yangsoo Jang, Namsik Chung, Won-Heum Shim, Seung-Yun Cho
 Eur J Echocardiography (2006) 7, 16e21 CLINICAL/ORIGINAL PAPERS Triphasic mitral inflow velocity with mid-diastolic flow: The presence of mid-diastolic mitral annular velocity indicates advanced diastolic
Eur J Echocardiography (2006) 7, 16e21 CLINICAL/ORIGINAL PAPERS Triphasic mitral inflow velocity with mid-diastolic flow: The presence of mid-diastolic mitral annular velocity indicates advanced diastolic
Journal of the American College of Cardiology Vol. 36, No. 5, by the American College of Cardiology ISSN /00/$20.
 Journal of the American College of Cardiology Vol. 36, No. 5, 2000 2000 by the American College of Cardiology ISSN 0735-1097/00/$20.00 Published by Elsevier Science Inc. PII S0735-1097(00)00909-8 Echocardiography
Journal of the American College of Cardiology Vol. 36, No. 5, 2000 2000 by the American College of Cardiology ISSN 0735-1097/00/$20.00 Published by Elsevier Science Inc. PII S0735-1097(00)00909-8 Echocardiography
Characteristics of Left Ventricular Diastolic Function in Patients with Systolic Heart Failure: A Doppler Tissue Imaging Study
 Characteristics of Left Ventricular Diastolic Function in Patients with Systolic Heart Failure: A Doppler Tissue Imaging Study Bassem A. Samad, MD, PhD, Jens M. Olson, MD, and Mahbubul Alam, MD, PhD, FESC,
Characteristics of Left Ventricular Diastolic Function in Patients with Systolic Heart Failure: A Doppler Tissue Imaging Study Bassem A. Samad, MD, PhD, Jens M. Olson, MD, and Mahbubul Alam, MD, PhD, FESC,
Evaluation of Left Ventricular Diastolic Dysfunction by Doppler and 2D Speckle-tracking Imaging in Patients with Primary Pulmonary Hypertension
 ESC Congress 2011.No 85975 Evaluation of Left Ventricular Diastolic Dysfunction by Doppler and 2D Speckle-tracking Imaging in Patients with Primary Pulmonary Hypertension Second Department of Internal
ESC Congress 2011.No 85975 Evaluation of Left Ventricular Diastolic Dysfunction by Doppler and 2D Speckle-tracking Imaging in Patients with Primary Pulmonary Hypertension Second Department of Internal
E/Ea is NOT an essential estimator of LV filling pressures
 Euroecho Kopenhagen Echo in Resynchronization in 2010 E/Ea is NOT an essential estimator of LV filling pressures Wilfried Mullens, MD, PhD December 10, 2010 Ziekenhuis Oost Limburg Genk University Hasselt
Euroecho Kopenhagen Echo in Resynchronization in 2010 E/Ea is NOT an essential estimator of LV filling pressures Wilfried Mullens, MD, PhD December 10, 2010 Ziekenhuis Oost Limburg Genk University Hasselt
Imaging. Global Diastolic Strain Rate for the Assessment of Left Ventricular Relaxation and Filling Pressures
 Imaging Global Diastolic Strain Rate for the Assessment of Left Ventricular Relaxation and Filling Pressures Jianwen Wang, PhD, MD; Dirar S. Khoury, PhD; Vinay Thohan, MD; Guillermo Torre-Amione, PhD,
Imaging Global Diastolic Strain Rate for the Assessment of Left Ventricular Relaxation and Filling Pressures Jianwen Wang, PhD, MD; Dirar S. Khoury, PhD; Vinay Thohan, MD; Guillermo Torre-Amione, PhD,
Diastology Disclosures: None. Dias2011:1
 Diastology 2011 James D. Thomas, M.D., F.A.C.C. Cardiovascular Imaging Center Department of Cardiology Cleveland Clinic Foundation Cleveland, Ohio, USA Disclosures: None Dias2011:1 Is EVERYBODY a member!?!
Diastology 2011 James D. Thomas, M.D., F.A.C.C. Cardiovascular Imaging Center Department of Cardiology Cleveland Clinic Foundation Cleveland, Ohio, USA Disclosures: None Dias2011:1 Is EVERYBODY a member!?!
Diastolic Function: What the Sonographer Needs to Know. Echocardiographic Assessment of Diastolic Function: Basic Concepts 2/8/2012
 Diastolic Function: What the Sonographer Needs to Know Pat Bailey, RDCS, FASE Technical Director Beaumont Health System Echocardiographic Assessment of Diastolic Function: Basic Concepts Practical Hints
Diastolic Function: What the Sonographer Needs to Know Pat Bailey, RDCS, FASE Technical Director Beaumont Health System Echocardiographic Assessment of Diastolic Function: Basic Concepts Practical Hints
DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES
 QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES") THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement
THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement
Left Atrial Deformation Predicts Pulmonary Capillary Wedge Pressure in Pediatric Heart Transplant Recipients
 DOI: 10.1111/echo.12679 2014, Wiley Periodicals, Inc. Echocardiography Left Atrial Deformation Predicts Pulmonary Capillary Wedge Pressure in Pediatric Heart Transplant Recipients Jay Yeh, M.D.,* Ranjit
DOI: 10.1111/echo.12679 2014, Wiley Periodicals, Inc. Echocardiography Left Atrial Deformation Predicts Pulmonary Capillary Wedge Pressure in Pediatric Heart Transplant Recipients Jay Yeh, M.D.,* Ranjit
Hemodynamic Assessment. Assessment of Systolic Function Doppler Hemodynamics
 Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
laboratory and animal investigations
 laboratory and animal investigations Influence of Alterations in Loading on Mitral Annular Velocity by Tissue Doppler Echocardiography and Its Associated Ability To Predict Filling Pressures* Didier C.
laboratory and animal investigations Influence of Alterations in Loading on Mitral Annular Velocity by Tissue Doppler Echocardiography and Its Associated Ability To Predict Filling Pressures* Didier C.
Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function
 Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function J A F E R A L I, M D U N I V E R S I T Y H O S P I T A L S C A S E M E D I C A L C E N T E R S T A F F C A R D I O T
Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function J A F E R A L I, M D U N I V E R S I T Y H O S P I T A L S C A S E M E D I C A L C E N T E R S T A F F C A R D I O T
How to Assess Diastolic Dysfunction?
 How to Assess Diastolic Dysfunction? Fausto J Pinto, MD, PhD, FESC, FACC, FASE Lisbon University Dyastolic Dysfunction Impaired relaxation Elevated filling pressures Ischemic heart disease Cardiomyopathies
How to Assess Diastolic Dysfunction? Fausto J Pinto, MD, PhD, FESC, FACC, FASE Lisbon University Dyastolic Dysfunction Impaired relaxation Elevated filling pressures Ischemic heart disease Cardiomyopathies
Evalua&on)of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on)
of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on)") Evalua&on)of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on) N.Koutsogiannis) Department)of)Cardiology) University)Hospital)of)Patras)! I have no conflicts of interest
Evalua&on)of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on) N.Koutsogiannis) Department)of)Cardiology) University)Hospital)of)Patras)! I have no conflicts of interest
PART II ECHOCARDIOGRAPHY LABORATORY OPERATIONS ADULT TRANSTHORACIC ECHOCARDIOGRAPHY TESTING
 PART II ECHOCARDIOGRAPHY LABORATORY OPERATIONS ADULT TRANSTHORACIC ECHOCARDIOGRAPHY TESTING STANDARD - Primary Instrumentation 1.1 Cardiac Ultrasound Systems SECTION 1 Instrumentation Ultrasound instruments
PART II ECHOCARDIOGRAPHY LABORATORY OPERATIONS ADULT TRANSTHORACIC ECHOCARDIOGRAPHY TESTING STANDARD - Primary Instrumentation 1.1 Cardiac Ultrasound Systems SECTION 1 Instrumentation Ultrasound instruments
Myocardial performance index, Tissue Doppler echocardiography
 Value of Measuring Myocardial Performance Index by Tissue Doppler Echocardiography in Normal and Diseased Heart Tarkan TEKTEN, 1 MD, Alper O. ONBASILI, 1 MD, Ceyhun CEYHAN, 1 MD, Selim ÜNAL, 1 MD, and
Value of Measuring Myocardial Performance Index by Tissue Doppler Echocardiography in Normal and Diseased Heart Tarkan TEKTEN, 1 MD, Alper O. ONBASILI, 1 MD, Ceyhun CEYHAN, 1 MD, Selim ÜNAL, 1 MD, and
The study of left ventricular diastolic function by Doppler echocardiography: the essential for the clinician
 Heart International / Vol. 3 no. 1-2, 2007 / pp. 42-50 Wichtig Editore, 2007 Review The study of left ventricular diastolic function by Doppler echocardiography: the essential for the clinician POMPILIO
Heart International / Vol. 3 no. 1-2, 2007 / pp. 42-50 Wichtig Editore, 2007 Review The study of left ventricular diastolic function by Doppler echocardiography: the essential for the clinician POMPILIO
Diastolic Function Assessment Practical Ways to Incorporate into Every Echo
 Diastolic Function Assessment Practical Ways to Incorporate into Every Echo Jae K. Oh, MD Echo Hawaii 2018 2018 MFMER 3712003-1 Learning Objectives My presentation will help you to Appreciate the importance
Diastolic Function Assessment Practical Ways to Incorporate into Every Echo Jae K. Oh, MD Echo Hawaii 2018 2018 MFMER 3712003-1 Learning Objectives My presentation will help you to Appreciate the importance
NEW GUIDELINES. A Guideline Protocol for the Echocardiographic assessment of Diastolic Dysfunction
 NEW GUIDELINES A Guideline Protocol for the Echocardiographic assessment of Diastolic Dysfunction Echocardiography plays a central role in the non-invasive evaluation of diastole and should be interpreted
NEW GUIDELINES A Guideline Protocol for the Echocardiographic assessment of Diastolic Dysfunction Echocardiography plays a central role in the non-invasive evaluation of diastole and should be interpreted
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Deceleration time of systolic pulmonary venous flow: a new clinical marker of left atrial pressure and compliance
 J Appl Physiol 100: 685 689, 2006. First published October 20, 2005; doi:10.1152/japplphysiol.00705.2005. Deceleration time of systolic pulmonary venous flow: a new clinical marker of left atrial pressure
J Appl Physiol 100: 685 689, 2006. First published October 20, 2005; doi:10.1152/japplphysiol.00705.2005. Deceleration time of systolic pulmonary venous flow: a new clinical marker of left atrial pressure
Diastolic Function Overview
 Diastolic Function Overview Richard Palma BS, RDCS, RCS, APS, FASE Director and Clinical Coordinator The Hoffman Heart and Vascular Institute School of Cardiac Ultrasound None Disclosures Learning Objectives
Diastolic Function Overview Richard Palma BS, RDCS, RCS, APS, FASE Director and Clinical Coordinator The Hoffman Heart and Vascular Institute School of Cardiac Ultrasound None Disclosures Learning Objectives
Journal of the American College of Cardiology Vol. 34, No. 4, by the American College of Cardiology ISSN /99/$20.
 Journal of the American College of Cardiology Vol. 34, No. 4, 1999 1999 by the American College of Cardiology ISSN 0735-1097/99/$20.00 Published by Elsevier Science Inc. PII S0735-1097(99)00341-1 Changes
Journal of the American College of Cardiology Vol. 34, No. 4, 1999 1999 by the American College of Cardiology ISSN 0735-1097/99/$20.00 Published by Elsevier Science Inc. PII S0735-1097(99)00341-1 Changes
Cardiac resynchronization therapy (CRT) is an
 is an") Cardiac Resynchronization Therapy Acutely Improves Diastolic Function Alan D. Waggoner, MHS, Mitchell N. Faddis, MD, PhD, Marye J. Gleva, MD, Lisa de Las Fuentes, MD, Judy Osborn, RN, Sharon Heuerman,
Cardiac Resynchronization Therapy Acutely Improves Diastolic Function Alan D. Waggoner, MHS, Mitchell N. Faddis, MD, PhD, Marye J. Gleva, MD, Lisa de Las Fuentes, MD, Judy Osborn, RN, Sharon Heuerman,
Journal of the American College of Cardiology Vol. 34, No. 2, by the American College of Cardiology ISSN /99/$20.
 Journal of the American College of Cardiology Vol. 34, No. 2, 1999 1999 by the American College of Cardiology ISSN 0735-1097/99/$20.00 Published by Elsevier Science Inc. PII S0735-1097(99)00230-2 Combined
Journal of the American College of Cardiology Vol. 34, No. 2, 1999 1999 by the American College of Cardiology ISSN 0735-1097/99/$20.00 Published by Elsevier Science Inc. PII S0735-1097(99)00230-2 Combined
Elevated LV filling pressure is a major determinant of cardiac symptoms and
 LEFT VENTRICULAR FILLING PRESSURE, DIASTOLIC FUNCTION, AND HEART RATE PATRIZIO LANCELLOTTI, MD, PhD, FESC PERSPECTIVES Author affiliations: University of Liège hospital, GIGA Cardiovascular Science, Heart
LEFT VENTRICULAR FILLING PRESSURE, DIASTOLIC FUNCTION, AND HEART RATE PATRIZIO LANCELLOTTI, MD, PhD, FESC PERSPECTIVES Author affiliations: University of Liège hospital, GIGA Cardiovascular Science, Heart
Introduction. In Jeong Cho, MD, Wook Bum Pyun, MD and Gil Ja Shin, MD ABSTRACT
 ORIGINAL ARTICLE DOI 10.4070 / kcj.2009.39.4.145 Print ISSN 1738-5520 / On-line ISSN 1738-5555 Copyright c 2009 The Korean Society of Cardiology The Influence of the Left Ventricular Geometry on the Left
ORIGINAL ARTICLE DOI 10.4070 / kcj.2009.39.4.145 Print ISSN 1738-5520 / On-line ISSN 1738-5555 Copyright c 2009 The Korean Society of Cardiology The Influence of the Left Ventricular Geometry on the Left
Hypertrophic cardiomyopathy (HCM) is a genetic disease
 is a genetic disease") Doppler Estimation of Left Ventricular Filling Pressures in Patients With Hypertrophic Cardiomyopathy Sherif F. Nagueh, MD; Nasser M. Lakkis, MD; Katherine J. Middleton, RCT; William H. Spencer III, MD;
Doppler Estimation of Left Ventricular Filling Pressures in Patients With Hypertrophic Cardiomyopathy Sherif F. Nagueh, MD; Nasser M. Lakkis, MD; Katherine J. Middleton, RCT; William H. Spencer III, MD;
P atients with heart disease frequently have abnormalities
 iii18 A clinical approach to the assessment of left ventricular diastolic function by Doppler echocardiography: update 2003 S R Ommen, R A Nishimura... P atients with heart disease frequently have abnormalities
iii18 A clinical approach to the assessment of left ventricular diastolic function by Doppler echocardiography: update 2003 S R Ommen, R A Nishimura... P atients with heart disease frequently have abnormalities
Diastolic Heart Function: Applying the New Guidelines Case Studies
 Diastolic Heart Function: Applying the New Guidelines Case Studies Mitral Regurgitation The New ASE William Guidelines: A. Zoghbi Role MD, of FASE, 2D/3D MACCand CMR Professor and Chairman, Department
Diastolic Heart Function: Applying the New Guidelines Case Studies Mitral Regurgitation The New ASE William Guidelines: A. Zoghbi Role MD, of FASE, 2D/3D MACCand CMR Professor and Chairman, Department
Tissue Doppler imaging (TDI) is. Original Research
 is. Original Research") Original Research Hellenic J Cardiol 2011; 52: 23-29 The Relationship Between the Time Interval Difference of Isovolumic Relaxation (T IVRT-IVRTa ) and Serum Levels of N-Terminal Pro-Brain Natriuretic
Original Research Hellenic J Cardiol 2011; 52: 23-29 The Relationship Between the Time Interval Difference of Isovolumic Relaxation (T IVRT-IVRTa ) and Serum Levels of N-Terminal Pro-Brain Natriuretic
Left atrial function. Aliakbar Arvandi MD
 In the clinic Left atrial function Abstract The left atrium (LA) is a left posterior cardiac chamber which is located adjacent to the esophagus. It is separated from the right atrium by the inter-atrial
In the clinic Left atrial function Abstract The left atrium (LA) is a left posterior cardiac chamber which is located adjacent to the esophagus. It is separated from the right atrium by the inter-atrial
Diastole is Not a Single Entity Four Components of Diastolic Dysfunction
 Physiology of Diastolic Function Made Easy James D. Thomas, MD, FACC, FASE Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg School of Medicine, Northwestern
Physiology of Diastolic Function Made Easy James D. Thomas, MD, FACC, FASE Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg School of Medicine, Northwestern
The Doppler Examination. Katie Twomley, MD Wake Forest Baptist Health - Lexington
 The Doppler Examination Katie Twomley, MD Wake Forest Baptist Health - Lexington OUTLINE Principles/Physics Use in valvular assessment Aortic stenosis (continuity equation) Aortic regurgitation (pressure
The Doppler Examination Katie Twomley, MD Wake Forest Baptist Health - Lexington OUTLINE Principles/Physics Use in valvular assessment Aortic stenosis (continuity equation) Aortic regurgitation (pressure
Clinical Investigations
 Clinical Investigations The Effect of Pulmonary Hypertension on Left Ventricular Diastolic Function in Chronic Obstructive Lung Disease: A Tissue Doppler Imaging and Right Cardiac Catheterization Study
Clinical Investigations The Effect of Pulmonary Hypertension on Left Ventricular Diastolic Function in Chronic Obstructive Lung Disease: A Tissue Doppler Imaging and Right Cardiac Catheterization Study
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital
 LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
The importance of left atrium in LV diastolic function
 II Baltic Heart Failure Meeting and Congress of Latvian Society of Cardiology The importance of left atrium in LV diastolic function Dr. Artem Kalinin Eastern Clinical University Hospital Riga 30.09.2010.
II Baltic Heart Failure Meeting and Congress of Latvian Society of Cardiology The importance of left atrium in LV diastolic function Dr. Artem Kalinin Eastern Clinical University Hospital Riga 30.09.2010.
Tissue Doppler Imaging in Congenital Heart Disease
 Tissue Doppler Imaging in Congenital Heart Disease L. Youngmin Eun, M.D. Department of Pediatrics, Division of Pediatric Cardiology, Kwandong University College of Medicine The potential advantage of ultrasound
Tissue Doppler Imaging in Congenital Heart Disease L. Youngmin Eun, M.D. Department of Pediatrics, Division of Pediatric Cardiology, Kwandong University College of Medicine The potential advantage of ultrasound
Shape and Movement of the Interatrial Septum Predicts Change in Pulmonary Capillary Wedge Pressure
 Shape and Movement of the Interatrial Septum Predicts Change in Pulmonary Capillary Wedge Pressure Colin F. Royse, MBBS, MD, FANZCA, 1 Alistair G. Royse, MD, MBBS, FRACS, 2 Paul F. Soeding, MBBS, FANZCA,
Shape and Movement of the Interatrial Septum Predicts Change in Pulmonary Capillary Wedge Pressure Colin F. Royse, MBBS, MD, FANZCA, 1 Alistair G. Royse, MD, MBBS, FRACS, 2 Paul F. Soeding, MBBS, FANZCA,
Influence of Preload Reduction on Left Ventricular Diastolic Function in Hemodialysis Patients with Left Ventricular Hypertrophy
 93 Original Article St. Marianna Med. J. Vol. 35, pp. 93 99, 2007 Influence of Preload Reduction on Left Ventricular Diastolic Function in Hemodialysis Patients with Left Ventricular Hypertrophy Sachihiko
93 Original Article St. Marianna Med. J. Vol. 35, pp. 93 99, 2007 Influence of Preload Reduction on Left Ventricular Diastolic Function in Hemodialysis Patients with Left Ventricular Hypertrophy Sachihiko
Time Constants of Cardiac Function and Their Calculations
 168 The Open Cardiovascular Medicine Journal, 2010, 4, 168-172 Time Constants of Cardiac Function and Their Calculations Open Access Xufang Bai 1, * and Quan Wang 2 1 University of Ottawa Heart Institute,
168 The Open Cardiovascular Medicine Journal, 2010, 4, 168-172 Time Constants of Cardiac Function and Their Calculations Open Access Xufang Bai 1, * and Quan Wang 2 1 University of Ottawa Heart Institute,
Mitral annular Doppler tissue imaging (DTI) has
 has") CARDIAC SONOGRAPHERS COMMUNICATION Doppler Tissue Imaging for the Assessment of Left Ventricular Diastolic Function: A Systematic Approach for the Sonographer Jeffrey C. Hill, BS, RDCS, and Richie A. Palma,
CARDIAC SONOGRAPHERS COMMUNICATION Doppler Tissue Imaging for the Assessment of Left Ventricular Diastolic Function: A Systematic Approach for the Sonographer Jeffrey C. Hill, BS, RDCS, and Richie A. Palma,
Tissue Doppler-Derived Myocardial Acceleration for Evaluation of Left Ventricular Diastolic Function
 Journal of the American College of Cardiology Vol. 44, No. 7, 2004 2004 by the American College of Cardiology Foundation ISSN 0735-1097/04/$30.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2004.06.067
Journal of the American College of Cardiology Vol. 44, No. 7, 2004 2004 by the American College of Cardiology Foundation ISSN 0735-1097/04/$30.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2004.06.067
Methods. Circ J 2005; 69:
 Circ J 2005; 69: 432 438 Can Transthoracic Doppler Echocardiography Predict the Discrepancy Between Left Ventricular End-Diastolic Pressure and Mean Pulmonary Capillary Wedge Pressure in Patients With
Circ J 2005; 69: 432 438 Can Transthoracic Doppler Echocardiography Predict the Discrepancy Between Left Ventricular End-Diastolic Pressure and Mean Pulmonary Capillary Wedge Pressure in Patients With
In patients with aortic dissection, expansion of the false
 Left Ventricular Diastolic Dysfunction in Chronic Aortic Dissection Yasushige Shingu, MD, Norihiko Shiiya, MD, PhD, Taisei Mikami, MD, PhD, Kenji Matsuzaki, MD, Takashi Kunihara, MD, PhD, and Yoshiro Matsui,
Left Ventricular Diastolic Dysfunction in Chronic Aortic Dissection Yasushige Shingu, MD, Norihiko Shiiya, MD, PhD, Taisei Mikami, MD, PhD, Kenji Matsuzaki, MD, Takashi Kunihara, MD, PhD, and Yoshiro Matsui,
Echo-Doppler evaluation of left ventricular diastolic function. Michel Slama Amiens France
 Echo-Doppler evaluation of left ventricular diastolic function Michel Slama Amiens France Left ventricular pressure Pressure A wave [ LVEDP LVEDP préa Congestive cardiac failure with preserved systolic
Echo-Doppler evaluation of left ventricular diastolic function Michel Slama Amiens France Left ventricular pressure Pressure A wave [ LVEDP LVEDP préa Congestive cardiac failure with preserved systolic
Objectives. Diastology: What the Radiologist Needs to Know. LV Diastolic Function: Introduction. LV Diastolic Function: Introduction
 Objectives Diastology: What the Radiologist Needs to Know. Jacobo Kirsch, MD Cardiopulmonary Imaging, Section Head Division of Radiology Cleveland Clinic Florida Weston, FL To review the physiology and
Objectives Diastology: What the Radiologist Needs to Know. Jacobo Kirsch, MD Cardiopulmonary Imaging, Section Head Division of Radiology Cleveland Clinic Florida Weston, FL To review the physiology and
Diastolic function has been evaluated from the dynamics
 Restrictive Left Ventricular Filling Pattern Does Not Result From Increased Left Atrial Pressure Alone Satoshi Masutani, MD; William C. Little, MD; Hiroshi Hasegawa, MD, PhD; Heng-Jie Cheng, MD, PhD; Che-Ping
Restrictive Left Ventricular Filling Pattern Does Not Result From Increased Left Atrial Pressure Alone Satoshi Masutani, MD; William C. Little, MD; Hiroshi Hasegawa, MD, PhD; Heng-Jie Cheng, MD, PhD; Che-Ping
AIMI-HF PROCEDURE MANUAL TECHNICAL GUIDE FOR ECHOCARDIOGRAPHY. MHI Core Laboratory E. O Meara - J.C. Tardif J. Vincent, G. Grenier, C.
 AIMI-HF PROCEDURE MANUAL TECHNICAL GUIDE FOR ECHOCARDIOGRAPHY MHI Core Laboratory E. O Meara - J.C. Tardif J. Vincent, G. Grenier, C. Roy February 2016 Montreal Heart Institute HF Research Aude Turgeon,
AIMI-HF PROCEDURE MANUAL TECHNICAL GUIDE FOR ECHOCARDIOGRAPHY MHI Core Laboratory E. O Meara - J.C. Tardif J. Vincent, G. Grenier, C. Roy February 2016 Montreal Heart Institute HF Research Aude Turgeon,
Echocardiography as a diagnostic and management tool in medical emergencies
 Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
HEMODYNAMIC ASSESSMENT
 HEMODYNAMIC ASSESSMENT INTRODUCTION Conventionally hemodynamics were obtained by cardiac catheterization. It is possible to determine the same by echocardiography. Methods M-mode & 2D echo alone can provide
HEMODYNAMIC ASSESSMENT INTRODUCTION Conventionally hemodynamics were obtained by cardiac catheterization. It is possible to determine the same by echocardiography. Methods M-mode & 2D echo alone can provide
GENERAL PRINCIPLES FOR ECHO ASSESSMENT OF DIASTOLIC FUNCTION (For full recommendation refer to the Left Ventricular Diastolic Function Guideline)
") 1 THE AMERICAN SOCIETY OF ECHOCARDIOGRAPHY RECOMMENDATIONS FOR THE EVALUATION OF LEFT VENTRICULAR DIASTOLIC FUNCTION BY ECHOCARDIOGRAPHY: A QUICK REFERENCE GUIDE FROM THE ASE WORKFLOW AND LAB MANAGEMENT
1 THE AMERICAN SOCIETY OF ECHOCARDIOGRAPHY RECOMMENDATIONS FOR THE EVALUATION OF LEFT VENTRICULAR DIASTOLIC FUNCTION BY ECHOCARDIOGRAPHY: A QUICK REFERENCE GUIDE FROM THE ASE WORKFLOW AND LAB MANAGEMENT
Pericardial Diseases. Smonporn Boonyaratavej, MD. Division of Cardiology, Department of Medicine Chulalongkorn University
 Pericardial Diseases Smonporn Boonyaratavej, MD Division of Cardiology, Department of Medicine Chulalongkorn University Cardiac Center, King Chulalongkorn Memorial Hospital 21 AUGUST 2016 Pericardial
Pericardial Diseases Smonporn Boonyaratavej, MD Division of Cardiology, Department of Medicine Chulalongkorn University Cardiac Center, King Chulalongkorn Memorial Hospital 21 AUGUST 2016 Pericardial
The impact of hypertension on systolic and diastolic left ventricular function. A tissue Doppler echocardiographic study
 The impact of hypertension on systolic and diastolic left ventricular function. A tissue Doppler echocardiographic study Manolis Bountioukos, MD, PhD, a Arend F.L. Schinkel, MD, PhD, a Jeroen J. Bax, MD,
The impact of hypertension on systolic and diastolic left ventricular function. A tissue Doppler echocardiographic study Manolis Bountioukos, MD, PhD, a Arend F.L. Schinkel, MD, PhD, a Jeroen J. Bax, MD,
Diastolic Functions: Evaluation & Clinical Applications
 Special Articles Diastolic Functions: Evaluation & Clinical Applications Senior Consultant Cardiologist, Metro Heart Institute, Delhi Immediate Past President, Cardiological Society of India (Cardiovasc.
Special Articles Diastolic Functions: Evaluation & Clinical Applications Senior Consultant Cardiologist, Metro Heart Institute, Delhi Immediate Past President, Cardiological Society of India (Cardiovasc.
Diastolic Heart Failure
 Chronic Heart Failure Prevalence overall = 2-3 % Diastolic Heart Failure Patrick Wouters University Hospital Ghent Belgium (Heart Failure + Asymptomatic Ventricular Dysfunction) Prevalence > 70 y = 10-20
Chronic Heart Failure Prevalence overall = 2-3 % Diastolic Heart Failure Patrick Wouters University Hospital Ghent Belgium (Heart Failure + Asymptomatic Ventricular Dysfunction) Prevalence > 70 y = 10-20
Systolic and Diastolic Dyssynchrony in Patients With Diastolic Heart Failure and the Effect of Medical Therapy
 Journal of the American College of Cardiology Vol. 49, No. 1, 2007 2007 by the American College of Cardiology Foundation ISSN 0735-1097/07/$32.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2006.10.023
Journal of the American College of Cardiology Vol. 49, No. 1, 2007 2007 by the American College of Cardiology Foundation ISSN 0735-1097/07/$32.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2006.10.023
Mechanisms of heart failure with normal EF Arterial stiffness and ventricular-arterial coupling. What is the pathophysiology at presentation?
 Mechanisms of heart failure with normal EF Arterial stiffness and ventricular-arterial coupling What is the pathophysiology at presentation? Ventricular-arterial coupling elastance Central arterial pressure
Mechanisms of heart failure with normal EF Arterial stiffness and ventricular-arterial coupling What is the pathophysiology at presentation? Ventricular-arterial coupling elastance Central arterial pressure
Thermal Therapy Improves Left Ventricular Diastolic Function in Patients With Congestive Heart Failure: A Tissue Doppler Echocardiographic
 J Cardiol 2007 Apr; 494: 187 191 Thermal Therapy Improves Left Ventricular Diastolic Function in Patients With Congestive Heart Failure: A Tissue Doppler Echocardiographic Study Akira Satoshi Takashi Yutaka
J Cardiol 2007 Apr; 494: 187 191 Thermal Therapy Improves Left Ventricular Diastolic Function in Patients With Congestive Heart Failure: A Tissue Doppler Echocardiographic Study Akira Satoshi Takashi Yutaka
Journal of the American College of Cardiology Vol. 37, No. 8, by the American College of Cardiology ISSN /01/$20.
 Journal of the American College of Cardiology Vol 37, No 8, 2001 2001 by the American College of Cardiology ISSN 0735-1097/01/$2000 Published by Elsevier Science Inc PII S0735-1097(01)01294-3 The Deceleration
Journal of the American College of Cardiology Vol 37, No 8, 2001 2001 by the American College of Cardiology ISSN 0735-1097/01/$2000 Published by Elsevier Science Inc PII S0735-1097(01)01294-3 The Deceleration
Disclosure Information : No conflict of interest
 Intravenous nicorandil improves symptoms and left ventricular diastolic function immediately in patients with acute heart failure : a randomized, controlled trial M. Shigekiyo, K. Harada, A. Okada, N.
Intravenous nicorandil improves symptoms and left ventricular diastolic function immediately in patients with acute heart failure : a randomized, controlled trial M. Shigekiyo, K. Harada, A. Okada, N.
Appendix II: ECHOCARDIOGRAPHY ANALYSIS
 Appendix II: ECHOCARDIOGRAPHY ANALYSIS Two-Dimensional (2D) imaging was performed using the Vivid 7 Advantage cardiovascular ultrasound system (GE Medical Systems, Milwaukee) with a frame rate of 400 frames
Appendix II: ECHOCARDIOGRAPHY ANALYSIS Two-Dimensional (2D) imaging was performed using the Vivid 7 Advantage cardiovascular ultrasound system (GE Medical Systems, Milwaukee) with a frame rate of 400 frames
Doppler Basic & Hemodynamic Calculations
 Doppler Basic & Hemodynamic Calculations August 19, 2017 Smonporn Boonyaratavej MD Division of Cardiology, Department of Medicine Chulalongkorn University Cardiac Center, King Chulalongkorn Memorial Hospital
Doppler Basic & Hemodynamic Calculations August 19, 2017 Smonporn Boonyaratavej MD Division of Cardiology, Department of Medicine Chulalongkorn University Cardiac Center, King Chulalongkorn Memorial Hospital
Strain/Untwisting/Diastolic Suction
 What Is Diastole and How to Assess It? Strain/Untwisting/Diastolic Suction James D. Thomas, M.D., F.A.C.C. Cardiovascular Imaging Center Department of Cardiology Cleveland Clinic Foundation Cleveland,
What Is Diastole and How to Assess It? Strain/Untwisting/Diastolic Suction James D. Thomas, M.D., F.A.C.C. Cardiovascular Imaging Center Department of Cardiology Cleveland Clinic Foundation Cleveland,
PROSTHETIC VALVE BOARD REVIEW
 PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
Right Heart Hemodynamics: Echo-Cath Discrepancies
 Department of cardiac, thoracic and vascular sciences University of Padua, School of Medicine Padua, Italy Right Heart Hemodynamics: Echo-Cath Discrepancies Luigi P. Badano, MD, PhD, FESC, FACC **Dr. Badano
Department of cardiac, thoracic and vascular sciences University of Padua, School of Medicine Padua, Italy Right Heart Hemodynamics: Echo-Cath Discrepancies Luigi P. Badano, MD, PhD, FESC, FACC **Dr. Badano
Ivana Nedeljkovic, M Ostojic, V Giga, V Stojanov, J Stepanovic, A Djordjevic Dikic, B Beleslin, M Nikolic, M Petrovic, D Popovic
 Combined cardiopulmonary exercise stress echocardiography test: New test for assessment of diastolic dysfunction in patients with hypertension Ivana Nedeljkovic, M Ostojic, V Giga, V Stojanov, J Stepanovic,
Combined cardiopulmonary exercise stress echocardiography test: New test for assessment of diastolic dysfunction in patients with hypertension Ivana Nedeljkovic, M Ostojic, V Giga, V Stojanov, J Stepanovic,
Adel Hasanin Ahmed 1
 Adel Hasanin Ahmed 1 PERICARDIAL DISEASE The pericardial effusion ends anteriorly to the descending aorta and is best visualised in the PLAX. PSAX is actually very useful sometimes for looking at posterior
Adel Hasanin Ahmed 1 PERICARDIAL DISEASE The pericardial effusion ends anteriorly to the descending aorta and is best visualised in the PLAX. PSAX is actually very useful sometimes for looking at posterior
M. Hajahmadi Poorrafsanjani 1 & B. Rahimi Darabad 1
 Global Journal of Health Science; Vol. 6, No. 7; 2014 ISSN 1916-9736 E-ISSN 1916-9744 Published by Canadian Center of Science and Education Evaluate the Sensitivity and Specificity Echocardiography in
Global Journal of Health Science; Vol. 6, No. 7; 2014 ISSN 1916-9736 E-ISSN 1916-9744 Published by Canadian Center of Science and Education Evaluate the Sensitivity and Specificity Echocardiography in
Patients with a Hypertensive Response to Exercise Have Impaired Left Ventricular Diastolic Function
 257 Original Article Hypertens Res Vol.31 (2008) No.2 p.257-263 Patients with a Hypertensive Response to Exercise Have Impaired Left Ventricular Diastolic Function Takeshi TAKAMURA 1), Katsuya ONISHI 2),
257 Original Article Hypertens Res Vol.31 (2008) No.2 p.257-263 Patients with a Hypertensive Response to Exercise Have Impaired Left Ventricular Diastolic Function Takeshi TAKAMURA 1), Katsuya ONISHI 2),
OPTIMIZING ECHO ACQUISTION FOR STRAIN AND DIASTOLOGY
 OPTIMIZING ECHO ACQUISTION FOR STRAIN AND DIASTOLOGY October 8, 2017 Deborah Agler, ACS, RDCS, FASE Coordinator of Education and Training Cleveland Clinic General Principles Diastology Clinical Data Heart
OPTIMIZING ECHO ACQUISTION FOR STRAIN AND DIASTOLOGY October 8, 2017 Deborah Agler, ACS, RDCS, FASE Coordinator of Education and Training Cleveland Clinic General Principles Diastology Clinical Data Heart
P = 4V 2. IVC Dimensions 10/20/2014. Comprehensive Hemodynamic Evaluation by Doppler Echocardiography. The Simplified Bernoulli Equation
 Comprehensive Hemodynamic Evaluation by Doppler Echocardiography Itzhak Kronzon, MD North Shore LIJ/ Lenox Hill Hospital New York, NY Disclosure: Philips Healthcare St. Jude Medical The Simplified Bernoulli
Comprehensive Hemodynamic Evaluation by Doppler Echocardiography Itzhak Kronzon, MD North Shore LIJ/ Lenox Hill Hospital New York, NY Disclosure: Philips Healthcare St. Jude Medical The Simplified Bernoulli
Echocardiography: Guidelines for Valve Quantification
 Echocardiography: Guidelines for Echocardiography: Guidelines for Chamber Quantification British Society of Echocardiography Education Committee Richard Steeds (Chair), Gill Wharton (Lead Author), Jane
Echocardiography: Guidelines for Echocardiography: Guidelines for Chamber Quantification British Society of Echocardiography Education Committee Richard Steeds (Chair), Gill Wharton (Lead Author), Jane
ONLINE DATA SUPPLEMENT. Impact of Obstructive Sleep Apnea on Left Ventricular Mass and. Diastolic Function
 ONLINE DATA SUPPLEMENT Impact of Obstructive Sleep Apnea on Left Ventricular Mass and Diastolic Function Mitra Niroumand Raffael Kuperstein Zion Sasson Patrick J. Hanly St. Michael s Hospital University
ONLINE DATA SUPPLEMENT Impact of Obstructive Sleep Apnea on Left Ventricular Mass and Diastolic Function Mitra Niroumand Raffael Kuperstein Zion Sasson Patrick J. Hanly St. Michael s Hospital University
Tissue Doppler Imaging
 Cronicon OPEN ACCESS Hesham Rashid* Tissue Doppler Imaging CARDIOLOGY Editorial Department of Cardiology, Benha University, Egypt *Corresponding Author: Hesham Rashid, Department of Cardiology, Benha University,
Cronicon OPEN ACCESS Hesham Rashid* Tissue Doppler Imaging CARDIOLOGY Editorial Department of Cardiology, Benha University, Egypt *Corresponding Author: Hesham Rashid, Department of Cardiology, Benha University,
Swan Song: Echocardiography as a Pulmonary Artery Catheter? Interdepartmental Division of Critical Care Medicine
 Swan Song: Echocardiography as a Pulmonary Artery Catheter? The swan is without spot, and it sings sweetly as it dies, that song ending its life Leonardo Da Vinci Curr Opin Anesthesiol 2016, 29:36 45 Circulation.
Swan Song: Echocardiography as a Pulmonary Artery Catheter? The swan is without spot, and it sings sweetly as it dies, that song ending its life Leonardo Da Vinci Curr Opin Anesthesiol 2016, 29:36 45 Circulation.
Index. K Knobology, TTE artifact, image resolution, ultrasound, 14
 A Acute aortic regurgitation (AR), 124 128 Acute aortic syndrome (AAS) classic aortic dissection diagnosis, 251 263 evolutive patterns, 253 255 pathology, 250 251 classifications, 247 248 incomplete aortic
A Acute aortic regurgitation (AR), 124 128 Acute aortic syndrome (AAS) classic aortic dissection diagnosis, 251 263 evolutive patterns, 253 255 pathology, 250 251 classifications, 247 248 incomplete aortic
Journal of the American College of Cardiology Vol. 37, No. 7, by the American College of Cardiology ISSN /01/$20.
 Journal of the American College of Cardiology Vol. 37, No. 7, 2001 2001 by the American College of Cardiology ISSN 0735-1097/01/$20.00 Published by Elsevier Science Inc. PII S0735-1097(01)01271-2 Accurate
Journal of the American College of Cardiology Vol. 37, No. 7, 2001 2001 by the American College of Cardiology ISSN 0735-1097/01/$20.00 Published by Elsevier Science Inc. PII S0735-1097(01)01271-2 Accurate
Brief View of Calculation and Measurement of Cardiac Hemodynamics
 Cronicon OPEN ACCESS EC CARDIOLOGY Review Article Brief View of Calculation and Measurement of Cardiac Hemodynamics Samah Alasrawi* Pediatric Cardiologist, Al Jalila Children Heart Center, Dubai, UAE *
Cronicon OPEN ACCESS EC CARDIOLOGY Review Article Brief View of Calculation and Measurement of Cardiac Hemodynamics Samah Alasrawi* Pediatric Cardiologist, Al Jalila Children Heart Center, Dubai, UAE *
British Society of Echocardiography
 British Society of Echocardiography Affiliated to the British Cardiac Society A Minimum Dataset for a Standard Adult Transthoracic Echocardiogram From the British Society of Echocardiography Education
British Society of Echocardiography Affiliated to the British Cardiac Society A Minimum Dataset for a Standard Adult Transthoracic Echocardiogram From the British Society of Echocardiography Education
Pediatric Echocardiography Examination Content Outline
 Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Echocardiographic and Doppler Assessment of Cardiac Functions in Patients of Non-Insulin Dependent Diabetes Mellitus
 ORIGINAL ARTICLE JIACM 2002; 3(2): 164-8 Echocardiographic and Doppler Assessment of Cardiac Functions in Patients of Non-Insulin Dependent Diabetes Mellitus Rajesh Rajput*, Jagdish**, SB Siwach***, A
ORIGINAL ARTICLE JIACM 2002; 3(2): 164-8 Echocardiographic and Doppler Assessment of Cardiac Functions in Patients of Non-Insulin Dependent Diabetes Mellitus Rajesh Rajput*, Jagdish**, SB Siwach***, A
Journal of the American College of Cardiology Vol. 34, No. 1, by the American College of Cardiology ISSN /99/$20.
 Journal of the American College of Cardiology Vol. 34, No. 1, 1999 1999 by the American College of Cardiology ISSN 0735-1097/99/$20.00 Published by Elsevier Science Inc. PII S0735-1097(99)00191-6 Noninvasive
Journal of the American College of Cardiology Vol. 34, No. 1, 1999 1999 by the American College of Cardiology ISSN 0735-1097/99/$20.00 Published by Elsevier Science Inc. PII S0735-1097(99)00191-6 Noninvasive
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics.
 Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
JACC: CARDIOVASCULAR IMAGING VOL. 4, NO. 9, PUBLISHED BY ELSEVIER INC. DOI: /j.jcmg
 JACC: CARDIOVASCULAR IMAGING VOL. 4, NO. 9, 2011 2011 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 1936-878X/$36.00 PUBLISHED BY ELSEVIER INC. DOI:10.1016/j.jcmg.2011.07.004 ORIGINAL RESEARCH
JACC: CARDIOVASCULAR IMAGING VOL. 4, NO. 9, 2011 2011 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 1936-878X/$36.00 PUBLISHED BY ELSEVIER INC. DOI:10.1016/j.jcmg.2011.07.004 ORIGINAL RESEARCH
Tilburg University. Published in: American Heart Journal. Document version: Publisher's PDF, also known as Version of record. Publication date: 2007
 Tilburg University Improvement in diastolic function and left ventricular filling pressure induced by cardiac resynchronization therapy Jansen, A.H.M.; van Dantzig, J.M.; Bracke, F.; Peels, K.H.; Koolen,
Tilburg University Improvement in diastolic function and left ventricular filling pressure induced by cardiac resynchronization therapy Jansen, A.H.M.; van Dantzig, J.M.; Bracke, F.; Peels, K.H.; Koolen,
좌심실수축기능평가 Cardiac Function
 Basic Echo Review Course 좌심실수축기능평가 Cardiac Function Seonghoon Choi Cardiology Hallym university LV systolic function Systolic function 좌심실수축기능 - 심근의수축으로심실에서혈액을대동맥으로박출하는기능 실제임상에서 LV function 의의미 1Diagnosis
Basic Echo Review Course 좌심실수축기능평가 Cardiac Function Seonghoon Choi Cardiology Hallym university LV systolic function Systolic function 좌심실수축기능 - 심근의수축으로심실에서혈액을대동맥으로박출하는기능 실제임상에서 LV function 의의미 1Diagnosis
Diastolic Function Assessment New Guideline Update Practical Approach
 Mayo Clinic Department of Cardiovascular Diseases Mayo Clinic Echocardiography Review Course for Boards and Recertification Diastolic Function Assessment New Guideline Update Practical Approach Jae K.
Mayo Clinic Department of Cardiovascular Diseases Mayo Clinic Echocardiography Review Course for Boards and Recertification Diastolic Function Assessment New Guideline Update Practical Approach Jae K.
THE PATHOGENESIS OF ACUTE PULMONARY EDEMA ASSOCIATED WITH HYPERTENSION THE PATHOGENESIS OF ACUTE PULMONARY EDEMA ASSOCIATED WITH HYPERTENSION
 THE PATHOGENESIS OF ACUTE PULMONARY EDEMA ASSOCIATED WITH HYPERTENSION THE PATHOGENESIS OF ACUTE PULMONARY EDEMA ASSOCIATED WITH HYPERTENSION SANJAY K. GANDHI, M.D., JOHN C. POWERS, M.D., ABDEL-MOHSEN
THE PATHOGENESIS OF ACUTE PULMONARY EDEMA ASSOCIATED WITH HYPERTENSION THE PATHOGENESIS OF ACUTE PULMONARY EDEMA ASSOCIATED WITH HYPERTENSION SANJAY K. GANDHI, M.D., JOHN C. POWERS, M.D., ABDEL-MOHSEN
American Society of Echocardiography
 Page 1 American Society of Echocardiography Recommendations for Quantification of Doppler Echocardiography A Report from the Doppler Quantification Task Force of the Nomenclature and Standards Committee
Page 1 American Society of Echocardiography Recommendations for Quantification of Doppler Echocardiography A Report from the Doppler Quantification Task Force of the Nomenclature and Standards Committee
Peak Early Diastolic Mitral Annulus Velocity by Tissue Doppler Imaging Adds Independent and Incremental Prognostic Value
 Journal of the American College of Cardiology Vol. 41, No. 5, 2003 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00 Published by Elsevier Science Inc. doi:10.1016/s0735-1097(02)02921-2
Journal of the American College of Cardiology Vol. 41, No. 5, 2003 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00 Published by Elsevier Science Inc. doi:10.1016/s0735-1097(02)02921-2