DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES
|
|
|
- Bridget Clarke
- 6 years ago
- Views:
Transcription

1 THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt
2 DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement (flow) - stroke volume (SV) - regurgitant volume/fraction (RV/RF) Valve orifice areas - stenotic orifice area (AVA, MVA) - (effective) regurgitant orifice area (EROA)
 =")
3 Quantification of pressure gradients Simplified Bernouilli equation: Pressure gradient (in mmhg) = 4(Vmax)²

4 Evaluation of RV Systolic Pressure RV systolic pressure = TR gradient + RA pressure Vmax TR gradient RV PA RA RAP 0

")

5 Assessing Hemodynamics RA pressure (using IVC size) Clinical: CVP RA pressure = 5 mmhg RA pressure > 15 mmhg
6 Tricuspid regurg. Patient # 1 This 40 yo man has a TR Vmax of 3 m/sec. 3 m/s IVC diameter 15 mm. Respiration change > 50%. What is his estimated RV pressure? mmhg mmhg mmhg mmhg 5. > 50 mmhg

7 Tricuspid regurg. Patient # 1 This 40 yo man has a TR Vmax of 3 m/s. 3 m/s 3x3x4 = 36mmHg IVC diameter 15 mm. Respiration change > 50%. What is his estimated RV pressure? mmhg mmhg mmhg mmhg 5. > 50 mmhg (Estimated RAP = 5 mmhg)
8 Evaluation of RV Diastolic Pressure In the absence of TS: RV diastolic pressure = RA pressure In the presence of TS: RV diastolic pressure = RA pressure - TS gradient

9 Evaluation of PA Systolic Pressure PA systolic pressure = TR gradient + RA pressure In the presence of PS: PA systolic pressure = RV systolic pressure - PS gradient 16 mmhg 2 m/s
")
10 Evaluation of PA end-diastolic pressure PA end-diastolic pressure = PR gradient + RA(V) end-diastolic pressure
11 CW Doppler of Pulmonic Valve Flow 2.5 m/sec The study suggests: 1. Severe PS 2. Right heart failure 3. Pulmonary hypertension 4. Constrictive Pericarditis
12 CW Doppler of Pulmonic Valve Flow 2.5 m/sec Answer: Pulmonary hypertension Note the end-diastolic gradient of 2.5 m/sec, indicating a gradient of 25 mmhg between the PA and RV
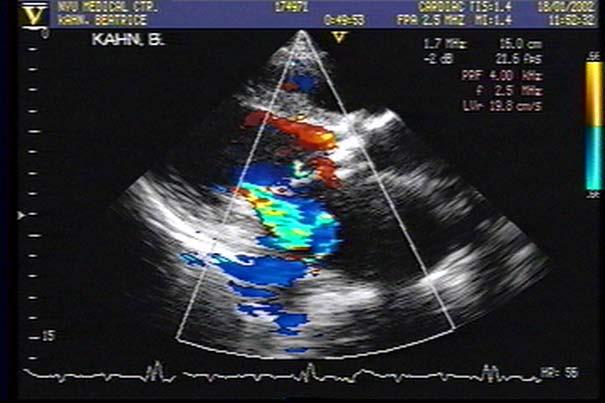
13 CW Doppler of MR Jet BP 120/80 mmhg. MR velocity is 7.7 m/sec The most likely diagnosis is: 1. Aortic stenosis 2. Aortic insufficiency 3. High cardiac output 4. Pulmonary hypertension

14 CW Doppler of MR Jet BP 120/80 mmhg. MR velocity is 7.7 m/sec Answer : Severe aortic stenosis

15 CW Doppler of MR Jet BP 120/80 mmhg. MR velocity is 7.7 m/sec Ao gradient LV Peak systolic LVP Peak systolic BP Ao LA The velocity of the MR jet indicates an LV-LA gradient of 237 mmhg; therefore the aortic gradient is at least 117 mmhg.
16 Evaluation of LV Systolic Pressure In pts without valve disease: LV systolic pressure = systolic BP In pts with AS or LVOT obstr.: LV systolic pressure = systolic BP + Peak-to-Peak gradient
17 Aortic Valve Gradients 1. Peak-to-Peak Gradient (PP) 2. Maximum Instantaneous Gradient (MIG) 3. Mean Gradient The PP gradient is 70% of the MIG In pts with AS or LVOT obstr.: LV systolic pressure = systolic BP + Peak-to-Peak gradient Ao In pts with AR: LV end-diastolic pressure = diastolic BP - AR gradient LV
18 CW Doppler of Aortic Valve Flow BP is 150/80 mmhg 4 m/sec 4 m/sec 4m/sec The LV pressure is: 1. 84/16 mmhg / / /16
19 CW Doppler of Aortic Valve Flow BP is 150/80 mmhg ANSWER: /16 mmhg LV (sys) = Sys. BP (150) + 70% Ao gradient (45) = 195 mmhg 4 m/sec Ao LV 4 m/sec LV (dias) = Dias. BP (80) - Ao dias. gradient (64) = 16 mmhg


20 Calculation of LA pressure e = 6 cm/sec LAP = E/e + 4 e E/e = 9.2 E 120cm/sec LAP= 55/6 + 4 = 13 mmhg E = 55 cm/sec E/e = 8: LA pressure nl E/e = 15: LA pressure high
21 Estimating LA Pressure by E/e may be inaccurate in: Mitral stenosis Mitral annular calcification Prosthetic MV Mitral regurgitation Diffuse severe LV dysfunction




22 Assessment of LA pressure in pts with MS LA diastolic pressure = LVDP + transmitral gradient MV gradient 16mmHg MV gradient 4mmHg
23 Noninvasive Hemodynamic Study 53-year-old male with dyspnea BP 100/65 HR 70, regular No JVD Apical diastolic rumble Basal systolic ejection murmur radiating to the neck 100/65
24
25 Normal IVC Size 1.6 cm >50% Respiratory Variation 100/65


26 Normal IVC Size 1.6 cm >50% Respiratory Variation 6 100/65 6 6
27 RV Pressures RV systolic = RA pressure (6) + TR gradient (40) = 46 mm Hg 6 100/ m/sec 6 46/6 In the absence of TS, RV diastolic pressure = RA pressure
 Diastolic = PR")

28 PA Pressure Systolic = RV systolic (46) Diastolic = PR gradient (20) + RA pressure (6) = 26 mmhg 6 100/65 46/ m/sec 46/6

 = 10 mmhg 6")

29 LVEDP = aortic diastolic pressure (65) AR gradient (55) = 10 mmhg 6 100/65 46/ m/sec 6 46/6 /10 (55 mmhg) 6 CP
 + 70% of")

30 LV systolic pressure = aortic systolic pressure (100) + 70% of AV gradient (64) = 164 mmhg 6 100/65 46/ m/sec (92mmHg) /6 164/10
 + MV mean")

31 LA pressure = LV diastolic (10) + MV mean gradient (13) = 23 mmhg /65 46/ /10 46/6 6
32 6 100/65 46/ /10 46/6 6
33 How to measure dp/dt? 1. Optimize CW MR jet with clear initial slope (high-filter setting 2. Decrease velocity range to max envelope from baseline to 4 m/s 3. Increase sweep speed to 100 mm/s 4. Draw horizontal lines at 1 m/s and 3 m/s Draw vertical line from intercept at MR to these points 6. Measure time (ms) t
34 How to measure dp/dt? 1. Optimize CW MR jet with clear initial slope (high-filter setting 2. Decrease velocity range to max envelope from baseline to 4 m/s 3. Increase sweep speed to 100 mm/s 4. Draw horizontal lines at 1 m/s and 3 m/s Draw vertical line from intercept at MR to these points 6. Measure time (ms) t
35 How to measure dp/dt? 1. Optimize CW MR jet with clear initial slope (high-filter setting 2. Decrease velocity range to max envelope from baseline to 4 m/s 3. Increase sweep speed to 100 mm/s 4. Draw horizontal lines at 1 m/s and 3 m/s Draw vertical line from intercept at MR to these points 6. Measure time (ms) t
36 How to measure dp/dt? 1. Optimize CW MR jet with clear initial slope (high-filter setting 2. Decrease velocity range to max envelope from baseline to 4 m/s 3. Increase sweep speed to 100 mm/s 4. Draw horizontal lines at 1 m/s and 3 m/s 5. Draw vertical line from intercept at MR to these points t? Measure time (ms) t
37 Measurement of LV dp/dt from MR jet dp/dt mmhg/sec P mmhg x = t (msec) ECG 1 m/sec 3 m/sec MR jet 100 mm/sec = = = 4 (V 2 - V 2 ) x t (msec) 4 ( ) X t (msec) t (msec) t? Normal LV dp/dt = > 1000 mmhg/sec Normal t < 32 msec
38 Time to reach MR velocity from 1 to 3 m/sec is 25 msec. t = 25 msec dp/dt = msec = = 1200 mmhg/sec
39 Conclusions Normal and abnormal hemodynamics can be evaluated non-invasively by Doppler Echocardiography. Invasive evaluation may be needed for details not seen on echo, or when the clinical impression is not consistent with the echo-doppler findings
40

41 Relation of E/E to PCWP Nagueh et al, 1997
42 Estimation of LV Filling Pressure MVF and PVF (Pozzoli et al., 1996) 1.85*DR 0.1*SF MVF and color M-mode 5.27*E/Pv (Garcia et al.,1997) MVF and TDI annulus (sinus tachycardia) 1.47*E/e MVF and TDI mitral annulus (atrial fibrillation) (Sohn et al.,1999) 0.82*(E/e ) (Nagueh et al.,1997)
43 Diastolic dysfunction and atrial fibrillation (Analyse bpm RR intervals) (Acceleration rate E wave) DT < 150 ms E/e ratio > 15 Color M-mode: Pv < 40 cm/sec
44 Evaluation of LV Diastolic Pressure In the absence of MS: LVDP = approx. LA pressure In pts with AR: LV end-diastolic pressure = diastolic BP - AR gradient Ao LV
P = 4V 2. IVC Dimensions 10/20/2014. Comprehensive Hemodynamic Evaluation by Doppler Echocardiography. The Simplified Bernoulli Equation
 Comprehensive Hemodynamic Evaluation by Doppler Echocardiography Itzhak Kronzon, MD North Shore LIJ/ Lenox Hill Hospital New York, NY Disclosure: Philips Healthcare St. Jude Medical The Simplified Bernoulli
Comprehensive Hemodynamic Evaluation by Doppler Echocardiography Itzhak Kronzon, MD North Shore LIJ/ Lenox Hill Hospital New York, NY Disclosure: Philips Healthcare St. Jude Medical The Simplified Bernoulli
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics.
 Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter.
 Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP North Shore HS, LIJ/Lenox Hill Hospital, New York
Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP North Shore HS, LIJ/Lenox Hill Hospital, New York
HEMODYNAMIC ASSESSMENT
 HEMODYNAMIC ASSESSMENT INTRODUCTION Conventionally hemodynamics were obtained by cardiac catheterization. It is possible to determine the same by echocardiography. Methods M-mode & 2D echo alone can provide
HEMODYNAMIC ASSESSMENT INTRODUCTION Conventionally hemodynamics were obtained by cardiac catheterization. It is possible to determine the same by echocardiography. Methods M-mode & 2D echo alone can provide
An Integrated Approach to Study LV Diastolic Function
 An Integrated Approach to Study LV Diastolic Function Assoc. Prof. Adriana Ilieşiu, FESC University of Medicine Carol Davila Bucharest, Romania LV Diastolic Dysfunction impaired relaxation (early diastole)
An Integrated Approach to Study LV Diastolic Function Assoc. Prof. Adriana Ilieşiu, FESC University of Medicine Carol Davila Bucharest, Romania LV Diastolic Dysfunction impaired relaxation (early diastole)
Hemodynamic Assessment. Assessment of Systolic Function Doppler Hemodynamics
 Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Choose the grading of diastolic function in 82 yo woman
 Question #1 Choose the grading of diastolic function in 82 yo woman E= 80 cm/s A= 70 cm/s LAVI < 34 ml/m 2 1= Grade 1 2= Grade 2 3= Grade 3 4= Normal 5= Indeterminate 2018 MFMER 3712003-1 Choose the grading
Question #1 Choose the grading of diastolic function in 82 yo woman E= 80 cm/s A= 70 cm/s LAVI < 34 ml/m 2 1= Grade 1 2= Grade 2 3= Grade 3 4= Normal 5= Indeterminate 2018 MFMER 3712003-1 Choose the grading
M-Mode Echocardiography Is it still Alive? Itzhak Kronzon, MD,FASE. Sampling Rate M-Mode: 1800 / sec 2D: 30 / sec
 M-Mode Echocardiography Is it still Alive? Itzhak Kronzon, MD,FASE Honoraria: Philips Classical M-mode Echocardiography M-Mode offers better time and image resolution. Sampling Rate M-Mode: 1800 / sec
M-Mode Echocardiography Is it still Alive? Itzhak Kronzon, MD,FASE Honoraria: Philips Classical M-mode Echocardiography M-Mode offers better time and image resolution. Sampling Rate M-Mode: 1800 / sec
Diastolic Heart Function: Applying the New Guidelines Case Studies
 Diastolic Heart Function: Applying the New Guidelines Case Studies Mitral Regurgitation The New ASE William Guidelines: A. Zoghbi Role MD, of FASE, 2D/3D MACCand CMR Professor and Chairman, Department
Diastolic Heart Function: Applying the New Guidelines Case Studies Mitral Regurgitation The New ASE William Guidelines: A. Zoghbi Role MD, of FASE, 2D/3D MACCand CMR Professor and Chairman, Department
Doppler Basic & Hemodynamic Calculations
 Doppler Basic & Hemodynamic Calculations August 19, 2017 Smonporn Boonyaratavej MD Division of Cardiology, Department of Medicine Chulalongkorn University Cardiac Center, King Chulalongkorn Memorial Hospital
Doppler Basic & Hemodynamic Calculations August 19, 2017 Smonporn Boonyaratavej MD Division of Cardiology, Department of Medicine Chulalongkorn University Cardiac Center, King Chulalongkorn Memorial Hospital
The Doppler Examination. Katie Twomley, MD Wake Forest Baptist Health - Lexington
 The Doppler Examination Katie Twomley, MD Wake Forest Baptist Health - Lexington OUTLINE Principles/Physics Use in valvular assessment Aortic stenosis (continuity equation) Aortic regurgitation (pressure
The Doppler Examination Katie Twomley, MD Wake Forest Baptist Health - Lexington OUTLINE Principles/Physics Use in valvular assessment Aortic stenosis (continuity equation) Aortic regurgitation (pressure
Diastolic Function Assessment Practical Ways to Incorporate into Every Echo
 Diastolic Function Assessment Practical Ways to Incorporate into Every Echo Jae K. Oh, MD Echo Hawaii 2018 2018 MFMER 3712003-1 Learning Objectives My presentation will help you to Appreciate the importance
Diastolic Function Assessment Practical Ways to Incorporate into Every Echo Jae K. Oh, MD Echo Hawaii 2018 2018 MFMER 3712003-1 Learning Objectives My presentation will help you to Appreciate the importance
E/Ea is NOT an essential estimator of LV filling pressures
 Euroecho Kopenhagen Echo in Resynchronization in 2010 E/Ea is NOT an essential estimator of LV filling pressures Wilfried Mullens, MD, PhD December 10, 2010 Ziekenhuis Oost Limburg Genk University Hasselt
Euroecho Kopenhagen Echo in Resynchronization in 2010 E/Ea is NOT an essential estimator of LV filling pressures Wilfried Mullens, MD, PhD December 10, 2010 Ziekenhuis Oost Limburg Genk University Hasselt
Diastolic Function Assessment New Guideline Update Practical Approach
 Mayo Clinic Department of Cardiovascular Diseases Mayo Clinic Echocardiography Review Course for Boards and Recertification Diastolic Function Assessment New Guideline Update Practical Approach Jae K.
Mayo Clinic Department of Cardiovascular Diseases Mayo Clinic Echocardiography Review Course for Boards and Recertification Diastolic Function Assessment New Guideline Update Practical Approach Jae K.
Quantification of Mitral Stenosis: Planimetry, pressure Half time, Continuity Common Errors
 Quantification of Mitral Stenosis: Planimetry, pressure Half time, Continuity Common Errors Christopher J Kramer RDCS Advanced Cardiovascular Services Aurora Health Care Milwaukee, WI No Disclosures Baumgartner,
Quantification of Mitral Stenosis: Planimetry, pressure Half time, Continuity Common Errors Christopher J Kramer RDCS Advanced Cardiovascular Services Aurora Health Care Milwaukee, WI No Disclosures Baumgartner,
Case Reviews: Hemodynamic Calculations in Valvular Regurgitation
 Case Reviews: Hemodynamic Calculations in Valvular Regurgitation Case 5 History: 69-year-old man with orthotopic heart transplant 15 years ago. Inferior MI several years ago. Recurrent CHF. Currently dyspneic
Case Reviews: Hemodynamic Calculations in Valvular Regurgitation Case 5 History: 69-year-old man with orthotopic heart transplant 15 years ago. Inferior MI several years ago. Recurrent CHF. Currently dyspneic
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital
 LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
The Patient with Atrial Fibrilation
 Assessment of Diastolic Function The Patient with Atrial Fibrilation Assoc. Prof. Adriana Ilieşiu, FESC University of Medicine Carol Davila Bucharest, Romania Associated Conditions with Atrial Fibrillation
Assessment of Diastolic Function The Patient with Atrial Fibrilation Assoc. Prof. Adriana Ilieşiu, FESC University of Medicine Carol Davila Bucharest, Romania Associated Conditions with Atrial Fibrillation
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants
 Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Evalua&on)of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on)
of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on)") Evalua&on)of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on) N.Koutsogiannis) Department)of)Cardiology) University)Hospital)of)Patras)! I have no conflicts of interest
Evalua&on)of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on) N.Koutsogiannis) Department)of)Cardiology) University)Hospital)of)Patras)! I have no conflicts of interest
Constriction vs Restriction Case-based Discussion
 Mayo Clinic Department of Cardiovascular Diseases Mayo Clinic Echocardiography Review Course for Boards and Recertification Constriction vs Restriction Case-based Discussion Jae K. Oh, MD Samsung Professor
Mayo Clinic Department of Cardiovascular Diseases Mayo Clinic Echocardiography Review Course for Boards and Recertification Constriction vs Restriction Case-based Discussion Jae K. Oh, MD Samsung Professor
Diastolic Function: What the Sonographer Needs to Know. Echocardiographic Assessment of Diastolic Function: Basic Concepts 2/8/2012
 Diastolic Function: What the Sonographer Needs to Know Pat Bailey, RDCS, FASE Technical Director Beaumont Health System Echocardiographic Assessment of Diastolic Function: Basic Concepts Practical Hints
Diastolic Function: What the Sonographer Needs to Know Pat Bailey, RDCS, FASE Technical Director Beaumont Health System Echocardiographic Assessment of Diastolic Function: Basic Concepts Practical Hints
MITRAL STENOSIS. Joanne Cusack
 MITRAL STENOSIS Joanne Cusack BSE Breakdown Recognition of rheumatic mitral stenosis Qualitative description of valve and sub-valve calcification and fibrosis Measurement of orifice area by planimetry
MITRAL STENOSIS Joanne Cusack BSE Breakdown Recognition of rheumatic mitral stenosis Qualitative description of valve and sub-valve calcification and fibrosis Measurement of orifice area by planimetry
좌심실수축기능평가 Cardiac Function
 Basic Echo Review Course 좌심실수축기능평가 Cardiac Function Seonghoon Choi Cardiology Hallym university LV systolic function Systolic function 좌심실수축기능 - 심근의수축으로심실에서혈액을대동맥으로박출하는기능 실제임상에서 LV function 의의미 1Diagnosis
Basic Echo Review Course 좌심실수축기능평가 Cardiac Function Seonghoon Choi Cardiology Hallym university LV systolic function Systolic function 좌심실수축기능 - 심근의수축으로심실에서혈액을대동맥으로박출하는기능 실제임상에서 LV function 의의미 1Diagnosis
OPTIMIZING ECHO ACQUISTION FOR STRAIN AND DIASTOLOGY
 OPTIMIZING ECHO ACQUISTION FOR STRAIN AND DIASTOLOGY October 8, 2017 Deborah Agler, ACS, RDCS, FASE Coordinator of Education and Training Cleveland Clinic General Principles Diastology Clinical Data Heart
OPTIMIZING ECHO ACQUISTION FOR STRAIN AND DIASTOLOGY October 8, 2017 Deborah Agler, ACS, RDCS, FASE Coordinator of Education and Training Cleveland Clinic General Principles Diastology Clinical Data Heart
Advanced Applica,on of Point- of- Care Echocardiography in Cri,cal Care. Dr. Mark Tutschka Dr. Rob ArnAield
 Advanced Applica,on of Point- of- Care Echocardiography in Cri,cal Care Dr. Mark Tutschka Dr. Rob ArnAield OBJECTIVES Provide an overview of common advanced echocardiographic techniques suitable for use
Advanced Applica,on of Point- of- Care Echocardiography in Cri,cal Care Dr. Mark Tutschka Dr. Rob ArnAield OBJECTIVES Provide an overview of common advanced echocardiographic techniques suitable for use
Congenital. Unicuspid Bicuspid Quadricuspid
 David Letterman s Top 10 Aortic Stenosis The victim can be anyone: Echo is the question and the answer!!!! Hilton Head Island Echocardiography Conference 2012 Timothy E. Paterick, MD, JD, MBA Christopher
David Letterman s Top 10 Aortic Stenosis The victim can be anyone: Echo is the question and the answer!!!! Hilton Head Island Echocardiography Conference 2012 Timothy E. Paterick, MD, JD, MBA Christopher
Swan Song: Echocardiography as a Pulmonary Artery Catheter? Interdepartmental Division of Critical Care Medicine
 Swan Song: Echocardiography as a Pulmonary Artery Catheter? The swan is without spot, and it sings sweetly as it dies, that song ending its life Leonardo Da Vinci Curr Opin Anesthesiol 2016, 29:36 45 Circulation.
Swan Song: Echocardiography as a Pulmonary Artery Catheter? The swan is without spot, and it sings sweetly as it dies, that song ending its life Leonardo Da Vinci Curr Opin Anesthesiol 2016, 29:36 45 Circulation.
Valvular Regurgitation: Can We Do Better Than Colour Doppler?
 Valvular Regurgitation: Can We Do Better Than Colour Doppler? A/Prof David Prior St Vincent s Hospital Melbourne Sports Cardiology Valvular Regurgitation Valve regurgitation volume loads the ventricles
Valvular Regurgitation: Can We Do Better Than Colour Doppler? A/Prof David Prior St Vincent s Hospital Melbourne Sports Cardiology Valvular Regurgitation Valve regurgitation volume loads the ventricles
Diastology Disclosures: None. Dias2011:1
 Diastology 2011 James D. Thomas, M.D., F.A.C.C. Cardiovascular Imaging Center Department of Cardiology Cleveland Clinic Foundation Cleveland, Ohio, USA Disclosures: None Dias2011:1 Is EVERYBODY a member!?!
Diastology 2011 James D. Thomas, M.D., F.A.C.C. Cardiovascular Imaging Center Department of Cardiology Cleveland Clinic Foundation Cleveland, Ohio, USA Disclosures: None Dias2011:1 Is EVERYBODY a member!?!
Appendix II: ECHOCARDIOGRAPHY ANALYSIS
 Appendix II: ECHOCARDIOGRAPHY ANALYSIS Two-Dimensional (2D) imaging was performed using the Vivid 7 Advantage cardiovascular ultrasound system (GE Medical Systems, Milwaukee) with a frame rate of 400 frames
Appendix II: ECHOCARDIOGRAPHY ANALYSIS Two-Dimensional (2D) imaging was performed using the Vivid 7 Advantage cardiovascular ultrasound system (GE Medical Systems, Milwaukee) with a frame rate of 400 frames
Tricuspid and Pulmonary Valve Disease
 Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Question 1 All of the following
Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Question 1 All of the following
What are the best diagnostic tools to quantify aortic regurgitation?
 What are the best diagnostic tools to quantify aortic regurgitation? Agnès Pasquet, MD, PhD Pôle de Recherche Cardiovasculaire Institut de Recherche Expérimentale et Clinique Université catholique de Louvain
What are the best diagnostic tools to quantify aortic regurgitation? Agnès Pasquet, MD, PhD Pôle de Recherche Cardiovasculaire Institut de Recherche Expérimentale et Clinique Université catholique de Louvain
MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS
 MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University
MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University
Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function
 Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function J A F E R A L I, M D U N I V E R S I T Y H O S P I T A L S C A S E M E D I C A L C E N T E R S T A F F C A R D I O T
Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function J A F E R A L I, M D U N I V E R S I T Y H O S P I T A L S C A S E M E D I C A L C E N T E R S T A F F C A R D I O T
Pericardial Disease: Case Examples. Echo Fiesta 2017
 Pericardial Disease: Case Examples Echo Fiesta 2017 2014 2014 MFMER MFMER 3346252-1 slide-1 Objectives Have a systematic approach to evaluation of constriction 2014 MFMER 3346252-2 CASE 1 2013 MFMER 3248567-3
Pericardial Disease: Case Examples Echo Fiesta 2017 2014 2014 MFMER MFMER 3346252-1 slide-1 Objectives Have a systematic approach to evaluation of constriction 2014 MFMER 3346252-2 CASE 1 2013 MFMER 3248567-3
Adel Hasanin Ahmed 1
 Adel Hasanin Ahmed 1 PERICARDIAL DISEASE The pericardial effusion ends anteriorly to the descending aorta and is best visualised in the PLAX. PSAX is actually very useful sometimes for looking at posterior
Adel Hasanin Ahmed 1 PERICARDIAL DISEASE The pericardial effusion ends anteriorly to the descending aorta and is best visualised in the PLAX. PSAX is actually very useful sometimes for looking at posterior
Prosthetic valve dysfunction: stenosis or regurgitation
 Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Right Heart Catheterization. Franz R. Eberli MD Chief of Cardiology Stadtspital Triemli, Zurich
 Right Heart Catheterization Franz R. Eberli MD Chief of Cardiology Stadtspital Triemli, Zurich Right Heart Catheterization Pressure measurements Oxygen saturation measurements Cardiac output, Vascular
Right Heart Catheterization Franz R. Eberli MD Chief of Cardiology Stadtspital Triemli, Zurich Right Heart Catheterization Pressure measurements Oxygen saturation measurements Cardiac output, Vascular
Right Ventricle Steven J. Lester MD, FACC, FRCP(C), FASE Mayo Clinic, Arizona
, FASE Mayo Clinic, Arizona") Right Ventricle Steven J. Lester MD, FACC, FRCP(C), FASE Mayo Clinic, Arizona 1. In which scenario will applying the simplified Bernoulli equation to the peak tricuspid regurgitation velocity and adding
Right Ventricle Steven J. Lester MD, FACC, FRCP(C), FASE Mayo Clinic, Arizona 1. In which scenario will applying the simplified Bernoulli equation to the peak tricuspid regurgitation velocity and adding
Echo in Pulmonary HTN
 Echo in Pulmonary HTN Steven A. Goldstein MD FACC FASE Professor of Medicine Georgetown University Medical Center MedStar Heart Institute Washington Hospital Center Monday, October 10, 2017 Pulmonary Artery
Echo in Pulmonary HTN Steven A. Goldstein MD FACC FASE Professor of Medicine Georgetown University Medical Center MedStar Heart Institute Washington Hospital Center Monday, October 10, 2017 Pulmonary Artery
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies
 Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
Diastolic Heart Failure
 Chronic Heart Failure Prevalence overall = 2-3 % Diastolic Heart Failure Patrick Wouters University Hospital Ghent Belgium (Heart Failure + Asymptomatic Ventricular Dysfunction) Prevalence > 70 y = 10-20
Chronic Heart Failure Prevalence overall = 2-3 % Diastolic Heart Failure Patrick Wouters University Hospital Ghent Belgium (Heart Failure + Asymptomatic Ventricular Dysfunction) Prevalence > 70 y = 10-20
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
British Society of Echocardiography
 British Society of Echocardiography Affiliated to the British Cardiac Society A Minimum Dataset for a Standard Adult Transthoracic Echocardiogram From the British Society of Echocardiography Education
British Society of Echocardiography Affiliated to the British Cardiac Society A Minimum Dataset for a Standard Adult Transthoracic Echocardiogram From the British Society of Echocardiography Education
ECHOCARDIOGRAPHY DATA REPORT FORM
 Patient ID Patient Study ID AVM - - Date of form completion / / 20 Initials of person completing the form mm dd yyyy Study period Preoperative Postoperative Operative 6-month f/u 1-year f/u 2-year f/u
Patient ID Patient Study ID AVM - - Date of form completion / / 20 Initials of person completing the form mm dd yyyy Study period Preoperative Postoperative Operative 6-month f/u 1-year f/u 2-year f/u
ASCeXAM / ReASCE. Practice Board Exam Questions Monday Morning
 ASCeXAM / ReASCE Practice Board Exam Questions Monday Morning Ultrasound Physics Artifacts Doppler Physics Imaging, Knobology, and Artifacts Echocardiographic Evaluation of the RV Tricuspid and Pulmonary
ASCeXAM / ReASCE Practice Board Exam Questions Monday Morning Ultrasound Physics Artifacts Doppler Physics Imaging, Knobology, and Artifacts Echocardiographic Evaluation of the RV Tricuspid and Pulmonary
Echo-Doppler evaluation of left ventricular diastolic function. Michel Slama Amiens France
 Echo-Doppler evaluation of left ventricular diastolic function Michel Slama Amiens France Left ventricular pressure Pressure A wave [ LVEDP LVEDP préa Congestive cardiac failure with preserved systolic
Echo-Doppler evaluation of left ventricular diastolic function Michel Slama Amiens France Left ventricular pressure Pressure A wave [ LVEDP LVEDP préa Congestive cardiac failure with preserved systolic
Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό
 Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό Diastolic HF DD: Diastolic Dysfunction DHF: Diastolic HF HFpEF: HF with preserved EF DD Pathophysiologic condition: impaired relaxation, LV compliance, LV filling
Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό Diastolic HF DD: Diastolic Dysfunction DHF: Diastolic HF HFpEF: HF with preserved EF DD Pathophysiologic condition: impaired relaxation, LV compliance, LV filling
Stage of Valvular AS. Outline 10/14/16. Low-flow and Other Challenges to the Assessment of Aortic Stenosis. Severe AS
 Low-flow and Other Challenges to the Assessment of Aortic Stenosis Nithima Ratanasit, MD, FACC, FASE Siriraj Hospital, Mahidol University Bangkok, Thailand Outline Types of low-flow aortic stenosis Assessment
Low-flow and Other Challenges to the Assessment of Aortic Stenosis Nithima Ratanasit, MD, FACC, FASE Siriraj Hospital, Mahidol University Bangkok, Thailand Outline Types of low-flow aortic stenosis Assessment
Marti McCulloch, BS, MBA, RDCS, FASE Houston, Texas
 Marti McCulloch, BS, MBA, RDCS, FASE Houston, Texas Mitral Regurgitation What to Expect Review Specific Signs of Severity Supportive Signs of Severity Qualitative Parameters Structural Doppler Quantitative
Marti McCulloch, BS, MBA, RDCS, FASE Houston, Texas Mitral Regurgitation What to Expect Review Specific Signs of Severity Supportive Signs of Severity Qualitative Parameters Structural Doppler Quantitative
Usually we DON T need to go beyond the gradient
 Aortic Stenosis Going Beyond the Gradient James D. Thomas, MD, FACC, FASE Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg School of Medicine, Northwestern
Aortic Stenosis Going Beyond the Gradient James D. Thomas, MD, FACC, FASE Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg School of Medicine, Northwestern
10/1/2016. Constrictive Pericarditis Unique Hemodynamics. What s New in Pericardial Disease? Case-based Discussion
 Mayo Clinic Department of Cardiovascular Diseases Mayo Clinic Echocardiography Review Course for Boards and Recertification What s New in Pericardial Disease? Case-based Discussion Jae K. Oh, MD Samsung
Mayo Clinic Department of Cardiovascular Diseases Mayo Clinic Echocardiography Review Course for Boards and Recertification What s New in Pericardial Disease? Case-based Discussion Jae K. Oh, MD Samsung
Echocardiography. Guidelines for Valve and Chamber Quantification. In partnership with
 Echocardiography Guidelines for Valve and Chamber Quantification In partnership with Explanatory note & references These guidelines have been developed by the Education Committee of the British Society
Echocardiography Guidelines for Valve and Chamber Quantification In partnership with Explanatory note & references These guidelines have been developed by the Education Committee of the British Society
SONOGRAPHER & NURSE LED VALVE CLINICS
 SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
Left ventricular diastolic function and filling pressure in patients with dilated cardiomyopathy
 Left ventricular diastolic function and filling pressure in patients with dilated cardiomyopathy Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania My conflicts of interest: I have
Left ventricular diastolic function and filling pressure in patients with dilated cardiomyopathy Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania My conflicts of interest: I have
Evaluation of Left Ventricular Diastolic Dysfunction by Doppler and 2D Speckle-tracking Imaging in Patients with Primary Pulmonary Hypertension
 ESC Congress 2011.No 85975 Evaluation of Left Ventricular Diastolic Dysfunction by Doppler and 2D Speckle-tracking Imaging in Patients with Primary Pulmonary Hypertension Second Department of Internal
ESC Congress 2011.No 85975 Evaluation of Left Ventricular Diastolic Dysfunction by Doppler and 2D Speckle-tracking Imaging in Patients with Primary Pulmonary Hypertension Second Department of Internal
Echocardiographic evaluation of mitral stenosis
 Echocardiographic evaluation of mitral stenosis Euroecho 2011 Philippe Unger, MD, FESC Erasme Hospital, ULB, Brussels, Belgium I have nothing to declare EuroHeart Survey Etiology of single native left-sided
Echocardiographic evaluation of mitral stenosis Euroecho 2011 Philippe Unger, MD, FESC Erasme Hospital, ULB, Brussels, Belgium I have nothing to declare EuroHeart Survey Etiology of single native left-sided
Imaging in Heart Failure: A Multimodality Approach. Thomas Ryan, MD
 Imaging in Heart Failure: A Multimodality Approach Thomas Ryan, MD Heart Failure HFrEF HFpEF EF50% Lifetime risk 20% Prevalence 6M Americans Societal costs - $30B 50% 5-year survival 1 Systolic
Imaging in Heart Failure: A Multimodality Approach Thomas Ryan, MD Heart Failure HFrEF HFpEF EF50% Lifetime risk 20% Prevalence 6M Americans Societal costs - $30B 50% 5-year survival 1 Systolic
MR echo case. N.Koutsogiannis Department of Cardiology University Hospital Of Patras
 MR echo case N.Koutsogiannis Department of Cardiology University Hospital Of Patras Case A 35 years old male came to the echo lab for a third opinion for his valvulopathy. He reports a long standing MR
MR echo case N.Koutsogiannis Department of Cardiology University Hospital Of Patras Case A 35 years old male came to the echo lab for a third opinion for his valvulopathy. He reports a long standing MR
Quantification of Aortic Regurgitation
 Quantification of Aortic Regurgitation ASE Review 2018 Boston Susan E Wiegers, MD, FASE, FACC Professor of Medicine And thanks to Dr. Roberto Lang Disclosure None related to this presentation 1 Objectives
Quantification of Aortic Regurgitation ASE Review 2018 Boston Susan E Wiegers, MD, FASE, FACC Professor of Medicine And thanks to Dr. Roberto Lang Disclosure None related to this presentation 1 Objectives
TAVR: Echo Measurements Pre, Post And Intra Procedure
 2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
Constrictive Pericarditis
 Constrictive Pericarditis Never Confused with Anything Else Jae K. Oh, MD 2018 MFMER 3712003-1 ARS #1 CP Which of following patients has constrictive pericarditis? 1 2 3 Medial e 13 cm/s Medial e 3 cm/s
Constrictive Pericarditis Never Confused with Anything Else Jae K. Oh, MD 2018 MFMER 3712003-1 ARS #1 CP Which of following patients has constrictive pericarditis? 1 2 3 Medial e 13 cm/s Medial e 3 cm/s
Quantification of MR
 Valvular Regurgitation: Putting the New Guidelines into Practice James D. Thomas, MD, FACC, FASE, FESC Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg
Valvular Regurgitation: Putting the New Guidelines into Practice James D. Thomas, MD, FACC, FASE, FESC Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg
Doppler and Hemodynamics Muhamed Saric and Itzhak Kronzon
 LWBK739-C07_p77-119.qxd 9/1/10 11:50 PM Page 77 Aptara Doppler and Hemodynamics Muhamed Saric and Itzhak Kronzon CHAPTER 7 1. On echocardiography, the diameter of the inferior vena cava is measured at
LWBK739-C07_p77-119.qxd 9/1/10 11:50 PM Page 77 Aptara Doppler and Hemodynamics Muhamed Saric and Itzhak Kronzon CHAPTER 7 1. On echocardiography, the diameter of the inferior vena cava is measured at
ECHO HAWAII. Role of Stress Echo in Valvular Heart Disease. Not only ischemia! Cardiomyopathy. Prosthetic Valve. Diastolic Dysfunction
 Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Aortic Stenosis: LVOT Obstruction
 Aortic Stenosis: LVOT Obstruction Raymond Stainback, MD 7 th annual Houston Echo Review 2016: Boot Camp for the Echo Board Murmur: Additional heart or vascular sound due to normal or abnormal turbulent
Aortic Stenosis: LVOT Obstruction Raymond Stainback, MD 7 th annual Houston Echo Review 2016: Boot Camp for the Echo Board Murmur: Additional heart or vascular sound due to normal or abnormal turbulent
Tricuspid and Pulmonary Valve Disease
 Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Right Sided Failure Edema Gut congestion
Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Right Sided Failure Edema Gut congestion
Echocardiography: Guidelines for Valve Quantification
 Echocardiography: Guidelines for Echocardiography: Guidelines for Chamber Quantification British Society of Echocardiography Education Committee Richard Steeds (Chair), Gill Wharton (Lead Author), Jane
Echocardiography: Guidelines for Echocardiography: Guidelines for Chamber Quantification British Society of Echocardiography Education Committee Richard Steeds (Chair), Gill Wharton (Lead Author), Jane
RVOTO adult and post-op
 Right ventricular outflow tract obstruction in the adult: native and post-op Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center University of
Right ventricular outflow tract obstruction in the adult: native and post-op Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center University of
Diastology State of The Art Assessment
 Diastology State of The Art Assessment Dr. Mohammad AlGhamdi Assistant professor, KSAU-HS Consultant Cardiologist King AbdulAziz Cardiac Center Ministry of National Guard Health Affairs Diagnostic Clinical
Diastology State of The Art Assessment Dr. Mohammad AlGhamdi Assistant professor, KSAU-HS Consultant Cardiologist King AbdulAziz Cardiac Center Ministry of National Guard Health Affairs Diagnostic Clinical
Ref 1. Ref 2. Ref 3. Ref 4. See graph
 Ref 1 Ref 2 Ref 3 1. Ages 6-23 y/o 2. Significant LVM differences by gender 3. For males 95 th percentiles: a. LVM/BSA = 103 b. LVM/height = 100 4. For females 95 th percentiles: a. LVM/BSA = 84 b. LVM/height
Ref 1 Ref 2 Ref 3 1. Ages 6-23 y/o 2. Significant LVM differences by gender 3. For males 95 th percentiles: a. LVM/BSA = 103 b. LVM/height = 100 4. For females 95 th percentiles: a. LVM/BSA = 84 b. LVM/height
European Heart Journal - Cardiovascular Imaging Advance Access published July 18, 2016
 European Heart Journal - Cardiovascular Imaging Advance Access published July 18, 2016 European Heart Journal Cardiovascular Imaging doi:10.1093/ehjci/jew082 Recommendations for the Evaluation of Left
European Heart Journal - Cardiovascular Imaging Advance Access published July 18, 2016 European Heart Journal Cardiovascular Imaging doi:10.1093/ehjci/jew082 Recommendations for the Evaluation of Left
Diastole is Not a Single Entity Four Components of Diastolic Dysfunction
 Physiology of Diastolic Function Made Easy James D. Thomas, MD, FACC, FASE Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg School of Medicine, Northwestern
Physiology of Diastolic Function Made Easy James D. Thomas, MD, FACC, FASE Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg School of Medicine, Northwestern
Quantitation of Aortic Regurgitation ASCeXAM / ReASCE Review Course
 Quantitation of Aortic Regurgitation 2017 ASCeXAM / ReASCE Review Course David Adams, ACS, RCS, RDCS, FASE Duke University Medical Center May 1, 2017 Disclosures None 1 Exam based on: Zoghbi et al. JASE
Quantitation of Aortic Regurgitation 2017 ASCeXAM / ReASCE Review Course David Adams, ACS, RCS, RDCS, FASE Duke University Medical Center May 1, 2017 Disclosures None 1 Exam based on: Zoghbi et al. JASE
How to Assess Diastolic Dysfunction?
 How to Assess Diastolic Dysfunction? Fausto J Pinto, MD, PhD, FESC, FACC, FASE Lisbon University Dyastolic Dysfunction Impaired relaxation Elevated filling pressures Ischemic heart disease Cardiomyopathies
How to Assess Diastolic Dysfunction? Fausto J Pinto, MD, PhD, FESC, FACC, FASE Lisbon University Dyastolic Dysfunction Impaired relaxation Elevated filling pressures Ischemic heart disease Cardiomyopathies
Disclosures Rebecca T. Hahn, MD, FASE
 The New ASE Guidelines for Native Valvular Regurgitation Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR (With caveats and comments from R. Hahn) William A. Zoghbi MD, FASE, MACC Professor
The New ASE Guidelines for Native Valvular Regurgitation Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR (With caveats and comments from R. Hahn) William A. Zoghbi MD, FASE, MACC Professor
Right Heart Hemodynamics: Echo-Cath Discrepancies
 Department of cardiac, thoracic and vascular sciences University of Padua, School of Medicine Padua, Italy Right Heart Hemodynamics: Echo-Cath Discrepancies Luigi P. Badano, MD, PhD, FESC, FACC **Dr. Badano
Department of cardiac, thoracic and vascular sciences University of Padua, School of Medicine Padua, Italy Right Heart Hemodynamics: Echo-Cath Discrepancies Luigi P. Badano, MD, PhD, FESC, FACC **Dr. Badano
Indicator Mild Moderate Severe
 Indicator Mild Moderate Severe Jet velocity (m/s) 2.0-2.9 3.0-3.9 4.0 Mean gradient (mmhg) < 20 20-39 40 Valve area (cm 2 ) 1.0 Valve area index (cm 2 /m 2 ) 0.6 1 Abnormal AV with Reduced Systolic Opening
Indicator Mild Moderate Severe Jet velocity (m/s) 2.0-2.9 3.0-3.9 4.0 Mean gradient (mmhg) < 20 20-39 40 Valve area (cm 2 ) 1.0 Valve area index (cm 2 /m 2 ) 0.6 1 Abnormal AV with Reduced Systolic Opening
Bogdan A. Popescu. University of Medicine and Pharmacy Bucharest, Romania. EAE Course, Bucharest, April 2010
 Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania EAE Course, Bucharest, April 2010 This is how it started Mitral stenosis at a glance 2D echo narrow diastolic opening of MV leaflets
Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania EAE Course, Bucharest, April 2010 This is how it started Mitral stenosis at a glance 2D echo narrow diastolic opening of MV leaflets
NEW GUIDELINES. A Guideline Protocol for the Echocardiographic assessment of Diastolic Dysfunction
 NEW GUIDELINES A Guideline Protocol for the Echocardiographic assessment of Diastolic Dysfunction Echocardiography plays a central role in the non-invasive evaluation of diastole and should be interpreted
NEW GUIDELINES A Guideline Protocol for the Echocardiographic assessment of Diastolic Dysfunction Echocardiography plays a central role in the non-invasive evaluation of diastole and should be interpreted
Effect of Heart Rate on Tissue Doppler Measures of E/E
 Cardiology Department of Bangkok Metropolitan Administration Medical College and Vajira Hospital, Bangkok, Thailand Abstract Background: Our aim was to study the independent effect of heart rate (HR) on
Cardiology Department of Bangkok Metropolitan Administration Medical College and Vajira Hospital, Bangkok, Thailand Abstract Background: Our aim was to study the independent effect of heart rate (HR) on
Stress Testing in Valvular Disease
 2017 ASE Florida Orlando, FL October 10, 2017 2:40 2:50 PM 10 min Grand Harbor Ballroom South Stress Testing in Valvular Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida Orlando, FL October 10, 2017 2:40 2:50 PM 10 min Grand Harbor Ballroom South Stress Testing in Valvular Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
Diastolic Function Overview
 Diastolic Function Overview Richard Palma BS, RDCS, RCS, APS, FASE Director and Clinical Coordinator The Hoffman Heart and Vascular Institute School of Cardiac Ultrasound None Disclosures Learning Objectives
Diastolic Function Overview Richard Palma BS, RDCS, RCS, APS, FASE Director and Clinical Coordinator The Hoffman Heart and Vascular Institute School of Cardiac Ultrasound None Disclosures Learning Objectives
25 different brand names >44 different models Sizes mm
 Types of Prosthetic Valves BIOLOGIC STENTED Porcine xenograft Pericardial xenograft STENTLESS Porcine xenograft Pericardial xenograft Homograft (allograft) Autograft PERCUTANEOUS MECHANICAL Bileaflet Single
Types of Prosthetic Valves BIOLOGIC STENTED Porcine xenograft Pericardial xenograft STENTLESS Porcine xenograft Pericardial xenograft Homograft (allograft) Autograft PERCUTANEOUS MECHANICAL Bileaflet Single
Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis?
 EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
Valve Disease Board Review Questions
 Valve Disease Board Review Questions Dennis A. Tighe, MD, FASE University of Massachusetts Medical School Worcester, MA Case 1 History A 61 year-old man Presents to hospital with worsening shortness of
Valve Disease Board Review Questions Dennis A. Tighe, MD, FASE University of Massachusetts Medical School Worcester, MA Case 1 History A 61 year-old man Presents to hospital with worsening shortness of
How to Assess and Treat Obstructive Lesions
 How to Assess and Treat Obstructive Lesions Erwin Oechslin, MD, FESC, FRCPC, Director, Congenital Cardiac Centre for Adults Peter Munk Cardiac Centre University Health Network/Toronto General Hospital
How to Assess and Treat Obstructive Lesions Erwin Oechslin, MD, FESC, FRCPC, Director, Congenital Cardiac Centre for Adults Peter Munk Cardiac Centre University Health Network/Toronto General Hospital
ICE: Echo Core Lab-CRF
 APPENDIX 1 ICE: Echo Core Lab-CRF Study #: - Pt Initials: 1. Date of study: / / D D M M M Y Y Y Y 2. Type of Study: TTE TEE 3. Quality of Study: Poor Moderate Excellent Ejection Fraction 4. Ejection Fraction
APPENDIX 1 ICE: Echo Core Lab-CRF Study #: - Pt Initials: 1. Date of study: / / D D M M M Y Y Y Y 2. Type of Study: TTE TEE 3. Quality of Study: Poor Moderate Excellent Ejection Fraction 4. Ejection Fraction
Imaging Assessment of Aortic Stenosis/Aortic Regurgitation
 Imaging Assessment of Aortic Stenosis/Aortic Regurgitation Craig E Fleishman, MD FACC FASE The Heart Center at Arnold Palmer Hospital for Children, Orlando SCAI Fall Fellows Course 2014 Las Vegas Disclosure
Imaging Assessment of Aortic Stenosis/Aortic Regurgitation Craig E Fleishman, MD FACC FASE The Heart Center at Arnold Palmer Hospital for Children, Orlando SCAI Fall Fellows Course 2014 Las Vegas Disclosure
Emergency Echo, Emergency Setting, ABCD Approach
 ECHO Alex Conference 2010 Emergency Echo, Emergency Setting, ABCD Approach Aleksandar N. Nešković Clinical Hospital Center Zemun Belgrade University School of Medicine Emergency Echocardiography Why ECHO
ECHO Alex Conference 2010 Emergency Echo, Emergency Setting, ABCD Approach Aleksandar N. Nešković Clinical Hospital Center Zemun Belgrade University School of Medicine Emergency Echocardiography Why ECHO
Quantitative Doppler echocardiography
 BJA Education, 16 (2): 46 52 (2016) doi: 10.1093/bjaceaccp/mkv015 Advance Access Publication Date: 10 June 2015 Matrix reference 1A03, 2A04, 3G00 Quantitative Doppler echocardiography P Harris MBChB FRCA
BJA Education, 16 (2): 46 52 (2016) doi: 10.1093/bjaceaccp/mkv015 Advance Access Publication Date: 10 June 2015 Matrix reference 1A03, 2A04, 3G00 Quantitative Doppler echocardiography P Harris MBChB FRCA
New murmur: acute valvular regurgitations. A.Pasquet, MD,PhD. UCL -Cliniques Saint Luc
 New murmur: acute valvular regurgitations. A.Pasquet, MD,PhD UCL -Cliniques Saint Luc Acute valvular regurgitation Clinical case Mr Dupont, a 53 y old men, without any particular medical history On Thursday
New murmur: acute valvular regurgitations. A.Pasquet, MD,PhD UCL -Cliniques Saint Luc Acute valvular regurgitation Clinical case Mr Dupont, a 53 y old men, without any particular medical history On Thursday
Comprehensive Echo Assessment of Aortic Stenosis
 Comprehensive Echo Assessment of Aortic Stenosis Smonporn Boonyaratavej, MD, MSc King Chulalongkorn Memorial Hospital Bangkok, Thailand Management of Valvular AS Medical and interventional approaches to
Comprehensive Echo Assessment of Aortic Stenosis Smonporn Boonyaratavej, MD, MSc King Chulalongkorn Memorial Hospital Bangkok, Thailand Management of Valvular AS Medical and interventional approaches to
Strain/Untwisting/Diastolic Suction
 What Is Diastole and How to Assess It? Strain/Untwisting/Diastolic Suction James D. Thomas, M.D., F.A.C.C. Cardiovascular Imaging Center Department of Cardiology Cleveland Clinic Foundation Cleveland,
What Is Diastole and How to Assess It? Strain/Untwisting/Diastolic Suction James D. Thomas, M.D., F.A.C.C. Cardiovascular Imaging Center Department of Cardiology Cleveland Clinic Foundation Cleveland,
The Fontan circulation. Folkert Meijboom
 The Fontan circulation Folkert Meijboom What to expect? Why a Fontan-circulation Indications How does it work Types of Fontan circulation Historical overview Role of echocardiography What to expect? Why
The Fontan circulation Folkert Meijboom What to expect? Why a Fontan-circulation Indications How does it work Types of Fontan circulation Historical overview Role of echocardiography What to expect? Why
Relevant Financial Relationship(s) Off Label Usage. None. None
 Off Label Usage. None. None") Different Variants Amr E Abbas, MD, FACC, FSCAI, FASE, FSVM Director, Interventional Cardiology Research Beaumont Health Associate Professor of Medicine, OU/WB School of Medicine ASCeXAM/ReASCeXAM 2018
Different Variants Amr E Abbas, MD, FACC, FSCAI, FASE, FSVM Director, Interventional Cardiology Research Beaumont Health Associate Professor of Medicine, OU/WB School of Medicine ASCeXAM/ReASCeXAM 2018
HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY?
 HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY? John D. Carroll, MD Professor, Director of Interventional Cardiology and Co-Medical Director of the Cardiac and Vascular Center, University of Colorado
HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY? John D. Carroll, MD Professor, Director of Interventional Cardiology and Co-Medical Director of the Cardiac and Vascular Center, University of Colorado
FUNDAMENTALS OF HEMODYNAMICS, VASOACTIVE DRUGS AND IABP IN THE FAILING HEART
 FUNDAMENTALS OF HEMODYNAMICS, VASOACTIVE DRUGS AND IABP IN THE FAILING HEART CINDY BITHER, MSN, ANP, ANP, AACC, CHFN CHIEF NP, ADV HF PROGRAM MEDSTAR WASHINGTON HOSPITAL CENTER CONFLICTS OF INTEREST NONE
FUNDAMENTALS OF HEMODYNAMICS, VASOACTIVE DRUGS AND IABP IN THE FAILING HEART CINDY BITHER, MSN, ANP, ANP, AACC, CHFN CHIEF NP, ADV HF PROGRAM MEDSTAR WASHINGTON HOSPITAL CENTER CONFLICTS OF INTEREST NONE