Cephalic Arch Stenosis: A unique entity
|
|
|
- Dylan Stafford
- 5 years ago
- Views:
Transcription







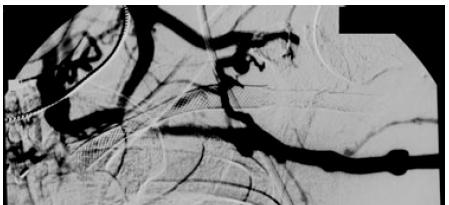
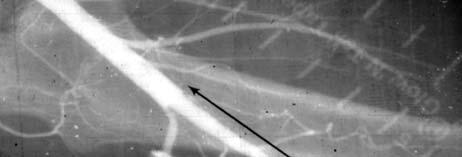
1 Cephalic Arch Stenosis: A unique entity Arif Asif, M.D. Professor of Medicine Director, Interventional Nephrology University of Miami, Miami, FL PUMP Kian K, Asif A: Semin Dial 2008 Prevalence of CAS 39% in brachiocephalic fistulae 2% in radiocephalic fistulae Cephalic Arch Stenosis: Etiology Hemodynaics (Turbulence) Valvular hypertrophy External compression External compression Minimum diameter required? Rajan et al: J Vasc Interv Radiol
2 Management Strategies PTA Stent Placement Patch Angioplasty Surgical Interventions Patency Rates Primary patency: 42% at 6 months and 23% at 1 year Primary assisted patency: 83% at 6 months and 75% at 1 year An average of 1.6 procedures a year was required to maintain patency Rajan et al: J Vasc Interv Radiol 2003 CAS and Stents CAS >50% within 3 months of successful PTA were randomized to have angioplasty and stenting with either a bare nitinol stent or a stent graft. Outcome was assessed by angiography 3 months later. Restenosis was defined as >50% narrowing of the stent lumen or of the vessel margin up to 0.5 cm adjacent to the stent. There were no exclusions. Shemesh et al: J Vasc Surg 2009 CAS and Stents At 3 months, three patients had died and one had undergone a renal transplant. The 21 patients who had angiography at 3 months had patent stents. Re-stenosis rates were seven of 10 (70%) in the bare stent group and two of 11 (18%) in the stent graft group (P =.024). Shemesh et al: J Vasc Surg 2009 CAS and Stents During a mean follow-up of 13.7 months Nine patients died Four in the bare stent group Five in the stent graft group Two patients in the stent graft group had received a renal transplant Bare metal=6 Stent-graft=4 CAS and Stents Shemesh et al: J Vasc Surg 2009 Shemesh et al: J Vasc Surg
.")


3 CAS and Stents Life-table analysis at 3 and 6 months showed that primary patency was 82% in the stent graft group and 39% in the bare stent group. One-year primary patency was 32% in the stent graft group and 0% in the bare stent group (P =.0023). Shemesh et al: J Vasc Surg 2009 CAS and Stents Restenosis rates in recurrent cephalic arch restenosis were significantly better for angioplasty using stent grafts compared with bare stents. This study altered our usage of stents for venous stenoses in AVA for hemodialysis by eliminating bare nitinol stents in favor of stent grafts. Shemesh et al: J Vasc Surg 2009 CAS and Stents We suggest that in patients where intimal hyperplasia is a possibility, stenting should be limited to the use of stents completely covered with PTFE, while paying careful attention to technical factors such as stent flexibility, stent length, and accurate deployment in relation to the position of the stenotic lesion. Shemesh et al: J Vasc Surg 2009 Recurrent CAS Stenosis 3





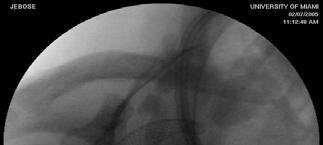
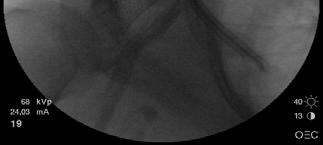
4 Recurrent CAS Stenosis 4





5 Conclusion No conclusive data in favor of stents PTA remains the mainstay of treatment Surgical intervention is an option Covered Stent at the Venous Anastomosis as the Primary Intervention Bart Dolmatch, MD Professor of Radiology Director of Vascular and Interventional Radiology University of Texas Southwestern Medical Center Dallas, TX 5

 VASA: Board of Directors")
 of AV Graft failures are caused by")

")

6 DISCLOSURE Information is consistent with FDA approval. Industry Relationships Bard Peripheral Vascular, Inc.: Royalties, Paid Consultant and Speaker Vital Access, Inc.: Medical Advisory Board Member (stock) VASA: Board of Directors Endovascular Forum: Medical Advisory Board Member (stock options) The vast majority (>75%) of AV Graft failures are caused by stenosis at and adjacent to the venous anastomosis. TOTAL = 77% VENOUS ANASTOMOTIC STENOSIS: DUE TO NEOINTIMAL HYPERPLASIA WHY? A V V G End-to-Side Anastomosis Shear forces (flow lines) Courtesy Tom Vesely HYPERPLASIA AT SITES OF GREATEST SHEAR FORCE 1 0 PATENCY OF AV GRAFTS 1 yr 1849 AVF s 1245 AVG s 60% Heel Graft Toe 40% AVF 1 AVG Vein Floor Huber et al. J Vasc Surg. 2003; 38: (meta-analysis of 34 series) 6

7 Angioplasty as a solution? Sept 22, mm PTA 3 mo post-pta Dec 22, 2006 Initial AVG VAS Post PTA 3 months ANGIOPLASTY of AV GRAFT VENOUS ANASTOMOTIC STENOSIS The Cutting Edge Trial 94 pts with Prospective 6-month follow-up* 40.9 % Access Circuit 6-mo.1 0 Patency (K-DOQI: At least 50% 6-mo. 1 0 Patency) *Vesely TM and Siegel JB. J Vasc Interv Radiol. 2005; WHY DOESN T PTA WORK VERY WELL FOR VENOUS ANASTOMOTIC STENOSIS? ELASTIC RECOIL Elastic Recoil Neointimal Hyperplastic Restenosis Post-PTA 7 mm 5 minutes post-pta elastic recoil of stenosis G Courtesy Tom Vesely, MD NEOINTIMAL HYPERPLASTIC RESTENOSIS STENT COVERED STENT OR STENT GRAFT VESSEL WALL GRAFT VESSEL WALL BLOOD STENT STENT 7


 Used for")





8 2 Coverings: PET and eptfe PET: Polyethylene Terephthalate (PET or POLYESTER DACRON ) Used for 50 years as an aortic bypass conduit eptfe: Expanded polytetrafluoroethylene Used for 20 years as a peripheral bypass conduit and AV graft conduit Dacron-covered stent: INFLAMMATORY!!! INFLAMMATION Stenosis was a problem!!! Dacron-covered Stents DEVELOPED IN-STENTGRAFT RESTENOSIS!!! 8










9 eptfe eptfe covered stent PET covered stent NODES FIBRILS eptfe COVERED STENTS PROTOTYPES Stent on inside of graft Stent on outside of graft Bare stent (control) LUMEN LUMEN LUMEN 9




10 eptfe Covered Stents The Flair: Stent embedded in eptfe Not inflammatory Subtle luminal neointima forms when stent is not on luminal surface Same material as most AV Grafts Porcine eptfe covered stent at 6wk C H The Delivery System A lot more stuff to deliver than a bare stent FLAIR ENDOVASCULAR STENT GRAFT CLINICAL TRIAL Ziv Haskal MD (PI), Samuel Mietling MD, Earl Schuman MD, Sanford Altman MD, Scott Berman MD, Gordon McLennon MD, Scott Trerotola MD, Clayton Trimmer DO, John Ross MD, Tom Vesely MD, Nilesh Patel MD, Richard Gray MD, Janet Durham MD, James Benenati MD, John Aruny MD, and Brett Wiechman MD 10



11 Study Design Multicenter Randomized Prospective PTA Flair Covered Stent versus optimal PTA, only Randomized 1:1 (PTA w/flair:pta only) Obligate clinical and angio f/u at 2 & 6 mo Core Lab assessment of all angiograms Designed to show non-inferiority VENOUS ANAST STENT GRAFT CONCEPT Prevents neointimal hyperplasia at PTA site Converts end-to-side to end-to-end Study Device: The Flair Covered Stent Flared and straight configuration Diameter 6, 7, 8, 9 mm Flare diameter is 4mm larger than body Lengths 30, 40, 50 mm PATIENTS INCLUDED 50% stenosis at the AV Graft venous anastomosis and at least one hemodynamic, functional, or clinical abnormality (per protocol) PATIENT 01-0A Venous Anastomotic Stenosis Total length of stenosis < 7cm During primary balloon angioplasty, full balloon could be achieved expansion of PTA with 7mm balloon 11
 in >20 criteria 7 mm x 50 mm flared device 84% of device patients received a flared Flair Demographics Graft age,")

 (Core Lab Analysis) PATENCY DEFINITIONS Treatment Area Primary Patency (TAPP) Index treatment area free from")
12 PATIENT 01-0A PATIENT DEMOGRAPHICS FLAIR VS PTA COHORTS No significant difference (p > 0.05) in >20 criteria 7 mm x 50 mm flared device 84% of device patients received a flared Flair Demographics Graft age, location, size, configuration Dysfunction criteria Presence of remote lesions Prior treatments Medications Anti-coagulation 37 Roll-In Patients 190 Randomized Patients STUDY ENROLLMENT ANGIOGRAPHIC SUCCESS FLAIR PTA <30% residual stenosis 94% 73% (p<0.001) (Core Lab Analysis) PATENCY DEFINITIONS Treatment Area Primary Patency (TAPP) Index treatment area free from reintervention AND NO access dysfunction Access Circuit Primary Patency (ACPP) Entire AV access circuit free from reintervention AND NO access dysfunction 12


 at 10 Months Restenosis of the Flair may occur High")


13 SURVIVAL FREE FROM ACCESS CIRCUIT PRIMARY PATENCY FAILURE PRE POST 6 MO 23 MO Vein Lesion raft Stent G Stent Graft S Synthetic Graft Log-Rank p=0.031 Wilcoxon p=0.044 ACPP lost at 35 mo February 2002: 60% 70% Due to intragraft 8mm Diameter stenosis FLAIR Endovascular Anastomotic Stenosis Stent Graft (Flared) at 10 Months Restenosis of the Flair may occur High venous pressure, 50% stenosis 8mm diameter flared Flair 16 mo: Recurrent dysfunction. Stenosis treated with PTA 3yr 9 mo: graft fully functional. Patient moved to another state. Treatment Area remains patent at 35 Months 35 months post placement of the FLAIR (Jan 2005) Courtesy of Scott Trerotola, M.D., Philadelphia, PN 13
 Larger (270 patients) Longer (12 months) Additional Endpoints (thrombosis, cum.")
14 In the final analysis Trial results now peer-reviewed and recently published in NEJM Doubling of circuit patency at 6 mos when a covered stent was used after PTA Only therapy proven to be better than PTA Ongoing post-approval study (RENOVA) Larger (270 patients) Longer (12 months) Additional Endpoints (thrombosis, cum. Patency) About half enrolled Initial AVG VAS Post PTA 1 0 Covered Stent Placement? Flair Doubles 6-mo AVG 1 0 Patency FDA Approval for primaryavg Use CMS Reimbursement: OPC or Hosp Peer-reviewed Level I Data (NEJM) Secondary Arteriovenous fistula (SAVF) Secondary AVF Creation: Be Careful What You Stent Rizwan A. Qazi, MD Assistant Professor of Internal Medicine/Nephrology Saint Louis University, School of Medicine Definition/Concept Types of SAVF (Type I & II) Timing of SAVF creation Sleeves up examination Judicious use of Endovascular stents in the AV dialysis shunts The use of Tunneled dialysis catheters (TDC) while transitioning from AVG to SAVF Summary

: When the outflow vein of a dysfunctional AV dialysis access (gr")


15 Concept of Secondary arteriovenous fistula (SAVF) A functional vascular access in the forearm (Graft or fistula) commonly results in dilatation of the veins of the upper arm. The increased flow and pressure causes maturation of the upper arm veins. These dilated veins can subsequently be used to create an AVF when the primary access starts to malfunction. Types of SAVF Type I (True SAVF): When the outflow vein of a dysfunctional AV dialysis access (graft or fistula) is used to create a secondary autogenous AVF e.g. creation of Brachiocephalic, Brachio basilic, Brachio brachial or Proximal radial artery to forearm veins fistula utilizing the arterialized part of the vein Type II: In the absence of a suitable outflow vein or presence of TDC an AV fistula is created anywhere in the ipsilateral or contralateral extremity by identifying vessels suitable for SAVF creation. OR Creation of a fistula anywhere in the body by identifying suitable vessels after the current dialysis access(tdc, AV graft or Fistula) starts to fail. Beathard GA (sem in Dialysis 2004) reported suitability of upper arm veins by angiographic examination in 62 patients with dysfunctional forearm AV grafts. 46(74%) ofthe outflowveins were deemed suitable for creation of SAVF drainage veins of a forearm AVG basilic v cephalic v AV Slide courtesy Aris G 15
 the cumulative patency was 87.5% at 2 years.")
16 G. Slayden et al (Sem in Dialysis 2008), reported Two surgeons experience with 160 AV fistula creations in a retrospective fashion. 38 patients with failing AVG underwent Type I SAVF creation. Type I SAVF cumulative 2 year patency was 97.4%. When both Type I and Type II were combined (142 patients) the cumulative patency was 87.5% at 2 years. Salman L, Asif A reported 62 patients with SAVF (type I, n=35;type II, n=27) in a prospective fashion. Cumulative 1 year patency was 100% for type I and 92% for type II. Cumulative 2 year patency was 83% for both type I and type II. Salman L et al. J Am Coll Surg July Asif et al in KI 2005 presented a prospective analysis of 86 patients consigned to TDCs, vascular mapping demonstrated that 94% of patients (64 of 66) with no prior arteriovenous accesses had suitable veins for arteriovenous access placement and 90% of patients (18 of 20) with previously failed arteriovenous accesses had suitable veins. Fistulas were created in 94% (68 of 72) of those patients. Seventy of the 72 accesses were functional with a mean follow up of 14.6 ±3.6 SD months. Indications for creating SAVF Failing grafts (recurrent angioplasty, clotting) Clotted forearm graft requiring jump grafting Steal syndrome with a functioning graft Graft erosions, infections, calcification Sleeves up examination Presence of a functional graft without complications or clinical or physical evidence of dysfunction is presently NOT an indication for conversion to SAVF. 95 Slide courtesy Aris 96 16
, TDC sometimes not required at all or required for short interval (1 4 weeks) Type II (TDC usually required) %age")

17 Brachio Brachial transposition AV fistulas Jennings WC et al. Journal of 97 10% were Type I SAVF. Cumulative patency 98 TDC transition for SAVF Type I (arterialized segment of vein), TDC sometimes not required at all or required for short interval (1 4 weeks) Type II (TDC usually required) %age of patients requiring TDC as a bridge during maturation/healing of SAVF was 60% in Type I SAVF and 100% in Type II SAVF as reported by Salman L et al in J Am Coll Surg Jul 2009 Yevzlin A et al. ACKD Sept Secondary AV fistula SAVF Stent Vs. SAVF Known and proven entity with 2 year cumulative patency of % Nephrologists should be Proactive with physical examination (Sleevesup exam) angiography or sonography Limit misguided intervention jump grafts, revisions, endovascular stents Timing Should be done before next failure episode



 fistula with resultant Radio Basilic fistula Son HJ et al in the J of")

18 Summary: Superiority of AV Fistulas over an AV graft as a preferred vascular access for HD is an accepted fact. Interventional nephrologist should always consider SAVF when working on a dysfunctional AV graft. Before placing a Stent in an AV dialysis Shunt, always ask this question. Am I jeopardizing creation of a Type I or II SAVF? AV Grafts AV Fistula Catheters 103 In Hemodialysis patients always aim for the fistula. If you couldn t get it the first time around Keep trying 104 Forearm basilic vein transposition (FBVT) fistula with resultant Radio Basilic fistula Son HJ et al in the J of Vascular surgery 2010 reported creation of 461 AV access with ih34 FBVT fistula. Assisted primary patency of FBVT fistula was still better than AV graft 105 SonHJetalinthe Jof Forearm Basilic vein transposition with resultant Radio-Basilic Fistula and a potential Brachio- Basilic SAVF later on 106 DAV FBV F AVG T SonHJetalinthe Jof
COVERA Vascular Covered Stents in the Management of Dysfunctional AV Access
 COVERA Vascular Covered Stents in the Management of Dysfunctional AV Access Bart L. Dolmatch, M.D., FSIR Palo Alto Medical Foundation Mountain View, CA USA This presentation is being made on behalf of
COVERA Vascular Covered Stents in the Management of Dysfunctional AV Access Bart L. Dolmatch, M.D., FSIR Palo Alto Medical Foundation Mountain View, CA USA This presentation is being made on behalf of
Introduction to the Native Arteriovenous Fistula: A primer for medical students and radiology residents
 Introduction to the Native Arteriovenous Fistula: A primer for medical students and radiology residents Jesus Contreras, D.O. PGY-4 John Yasmer, D.O. Department of Radiology No Disclosures Objectives Introduce
Introduction to the Native Arteriovenous Fistula: A primer for medical students and radiology residents Jesus Contreras, D.O. PGY-4 John Yasmer, D.O. Department of Radiology No Disclosures Objectives Introduce
*PTA Failure: Recoil >30% stenosis or more than 2 PTA s within 3 mo. Bart Dolmatch, MD
 The views presented reflect those of the author/presenter and do not necessarily reflect those of ASDIN nor serve as an endorsement of safety, efficacy or applicability of said procedure. the Endovascular
The views presented reflect those of the author/presenter and do not necessarily reflect those of ASDIN nor serve as an endorsement of safety, efficacy or applicability of said procedure. the Endovascular
Prospective, randomized controlled study of paclitaxel-coated versus plain balloon angioplasty for the treatment of failing dialysis access
 Prospective, randomized controlled study of paclitaxel-coated versus plain balloon angioplasty for the treatment of failing dialysis access Disclosure Speaker name:... I have the following potential conflicts
Prospective, randomized controlled study of paclitaxel-coated versus plain balloon angioplasty for the treatment of failing dialysis access Disclosure Speaker name:... I have the following potential conflicts
Lutonix AV Clinical Trial
 Long Term Effects of LUTONIX 035 DCB Catheter Interim 24 Month Results Scott O. Trerotola, MD, for the Lutonix AV Investigators Stanley Baum Professor of Radiology Professor of Radiology in Surgery Associate
Long Term Effects of LUTONIX 035 DCB Catheter Interim 24 Month Results Scott O. Trerotola, MD, for the Lutonix AV Investigators Stanley Baum Professor of Radiology Professor of Radiology in Surgery Associate
All arteriovenous access circuits, whether native vein
 Summary of the Gore REVISE Clinical Study This nationwide study reports on the safety and effectiveness of the GORE VIHN Endoprosthesis for the treatment of stenoses and thrombotic occlusions involving
Summary of the Gore REVISE Clinical Study This nationwide study reports on the safety and effectiveness of the GORE VIHN Endoprosthesis for the treatment of stenoses and thrombotic occlusions involving
Disclosures. Consultant/Independent Contractor: B Braun, Teleflex, MedComp, Cook, Bard, WL Gore Royalty: Cook, Teleflex
 Disclosures Consultant/Independent Contractor: B Braun, Teleflex, MedComp, Cook, Bard, WL Gore Royalty: Cook, Teleflex DCB in Hemodialysis Access Scott Trerotola, MD 2016: 50 th birthday of the AVF History
Disclosures Consultant/Independent Contractor: B Braun, Teleflex, MedComp, Cook, Bard, WL Gore Royalty: Cook, Teleflex DCB in Hemodialysis Access Scott Trerotola, MD 2016: 50 th birthday of the AVF History
ASDIN 9th Annual Scientific Meeting
 Stent Graft Placement is Best for Cephalic Arch and Central Vein Stenosis Dheeraj K. Rajan MD, FRCPC, FSIR Head - Division of Vascular and Interventional Radiology University of Toronto University Health
Stent Graft Placement is Best for Cephalic Arch and Central Vein Stenosis Dheeraj K. Rajan MD, FRCPC, FSIR Head - Division of Vascular and Interventional Radiology University of Toronto University Health
COVERA Vascular Covered Stents Innovation in AV Access
 IL0118 Rev.0 1 COVERA Vascular Covered Stents Innovation in AV Access Dheeraj Rajan, MD, FRCPC, FSIR Head and Associate Professor, Division of Vascular & Interventional Radiology Department of Medical
IL0118 Rev.0 1 COVERA Vascular Covered Stents Innovation in AV Access Dheeraj Rajan, MD, FRCPC, FSIR Head and Associate Professor, Division of Vascular & Interventional Radiology Department of Medical
Proven Performance Through Innovative Design *
 Proven Performance Through Innovative Design * Deliver Our Next Generation AV Covered Stent Results The COVERA Vascular Covered Stent builds upon proven technologies from the category leader in AV Access.
Proven Performance Through Innovative Design * Deliver Our Next Generation AV Covered Stent Results The COVERA Vascular Covered Stent builds upon proven technologies from the category leader in AV Access.
IN.PACT AV Access IDE Study Full Baseline Data. Robert Lookstein, MD MHCDL New York, NY On Behalf of the IN.PACT AV ACCESS Investigators
 IN.PACT AV Access IDE Study Full Baseline Data Robert Lookstein, MD MHCDL New York, NY On Behalf of the IN.PACT AV ACCESS Investigators Disclosures Speaker name: Robert Lookstein, MD... I have the following
IN.PACT AV Access IDE Study Full Baseline Data Robert Lookstein, MD MHCDL New York, NY On Behalf of the IN.PACT AV ACCESS Investigators Disclosures Speaker name: Robert Lookstein, MD... I have the following
Jimmy Wei Hwa Tan, Surg, MD
 Jimmy Wei Hwa Tan, Surg, MD Director, Department of Surgery Chief, Department of Cardiovascular Surgery Tainan An-Nan Municipal Hospital, China Medical University, Taiwan Disclosure I have the following
Jimmy Wei Hwa Tan, Surg, MD Director, Department of Surgery Chief, Department of Cardiovascular Surgery Tainan An-Nan Municipal Hospital, China Medical University, Taiwan Disclosure I have the following
Role of Covered Stents and Drug Eluting Balloons In Dialysis Access
 Role of Covered Stents and Drug Eluting Balloons In Dialysis Access Joseph Habib, MD, FACS Assistant Professor Department of Surgery Division of Vascular and Endovascular Surgery University of Florida
Role of Covered Stents and Drug Eluting Balloons In Dialysis Access Joseph Habib, MD, FACS Assistant Professor Department of Surgery Division of Vascular and Endovascular Surgery University of Florida
Since the initiation of hemodialysis, multiple inventions
 Special Feature Stent Graft for Nephrologists: Concerns and Consensus Loay Salman and Arif Asif Division of Nephrology, Section of Interventional Nephrology, University of Miami Miller School of Medicine,
Special Feature Stent Graft for Nephrologists: Concerns and Consensus Loay Salman and Arif Asif Division of Nephrology, Section of Interventional Nephrology, University of Miami Miller School of Medicine,
COVERA covered stent to treat stenosis in arteriovenous fistula: 6-month results from the prospective, multi-center, randomized AVeNEW study
 COVERA covered stent to treat stenosis in arteriovenous fistula: 6-month results from the prospective, multi-center, randomized AVeNEW study Panagiotis Kitrou MD, MSc, PhD, EBIR Consultant Interventional
COVERA covered stent to treat stenosis in arteriovenous fistula: 6-month results from the prospective, multi-center, randomized AVeNEW study Panagiotis Kitrou MD, MSc, PhD, EBIR Consultant Interventional
Lutonix AV Clinical Trial
 Long Term Effects of LUTONIX 035 DCB Catheter Interim 24 Month Results Ta-Wei Su MD Vascular surgery CGMH Taiwan Disclosure I have the following potential conflicts of interest to report: Consulting Employment
Long Term Effects of LUTONIX 035 DCB Catheter Interim 24 Month Results Ta-Wei Su MD Vascular surgery CGMH Taiwan Disclosure I have the following potential conflicts of interest to report: Consulting Employment
Technical Aspects for Treating AV Dialysis Fistulae with the IN.PACT DCB. Andrew Holden Auckland Hospital Auckland, New Zealand
 Technical Aspects for Treating AV Dialysis Fistulae with the IN.PACT DCB Andrew Holden Auckland Hospital Auckland, New Zealand LINC 2017 26 th January 2017 Disclosure Speaker name: Andrew Holden I have
Technical Aspects for Treating AV Dialysis Fistulae with the IN.PACT DCB Andrew Holden Auckland Hospital Auckland, New Zealand LINC 2017 26 th January 2017 Disclosure Speaker name: Andrew Holden I have
Why Can't I Cannulate This Fistula? Fistula Immaturity: The Simple But Critical Steps for a Functioning (Mature) AVF
 AVF") Why Can t I Cannulate This Access? Steven J. Bander M.D. Adjunct Professor of Nephrology St. Louis University Director, Vascular Access Center, St. Luke s Hospital Saint Louis, MO Why Can't I Cannulate
Why Can t I Cannulate This Access? Steven J. Bander M.D. Adjunct Professor of Nephrology St. Louis University Director, Vascular Access Center, St. Luke s Hospital Saint Louis, MO Why Can't I Cannulate
Bare Metal Stents vs Stent Grafts
 Bare Metal Stents vs Stent Grafts ASDIN 12th Annual Scientific Meeting Phoenix, AZ, February 20, 2016 Dirk Hentschel, MD Director, Interventional Nephrology Brigham and Women s Hospital Disclosure Consultant:
Bare Metal Stents vs Stent Grafts ASDIN 12th Annual Scientific Meeting Phoenix, AZ, February 20, 2016 Dirk Hentschel, MD Director, Interventional Nephrology Brigham and Women s Hospital Disclosure Consultant:
The Art of Angioplasty
 The Art of Angioplasty Achieving and Defining Success Thomas M. Vesely, MD Saint Louis, Missouri Dr. Vesely is a consultant for: W.L. Gore & Associates Lutonix Imaging the Vascular Access Circuit A well
The Art of Angioplasty Achieving and Defining Success Thomas M. Vesely, MD Saint Louis, Missouri Dr. Vesely is a consultant for: W.L. Gore & Associates Lutonix Imaging the Vascular Access Circuit A well
Lutonix in AV fistula and Early look AV IDE trial data
 Lutonix in AV fistula and Early look AV IDE trial data Jackie P Ho Dept of Cardiac, Thoracic & Vascular Surgery National University of Singapore NUHS, Singapore Lutonix in AV fistula and final AV IDE trial
Lutonix in AV fistula and Early look AV IDE trial data Jackie P Ho Dept of Cardiac, Thoracic & Vascular Surgery National University of Singapore NUHS, Singapore Lutonix in AV fistula and final AV IDE trial
2006 NKF-DOQI Guidelines Preferred Vascular Access Order 1. Radiocephalic (wrist) fistula 2. Brachiocephalic (elbow) fistula 3. Basilic vein transposi
 fistula 2. Brachiocephalic (elbow) fistula 3. Basilic vein transposi") Stage 5 Chronic Kidney Disease Assessing the Results of AV Access: Realistic Outcomes in 2009 Sean P. Roddy, MD Albany, NY Defined as a GFR
Stage 5 Chronic Kidney Disease Assessing the Results of AV Access: Realistic Outcomes in 2009 Sean P. Roddy, MD Albany, NY Defined as a GFR
First experience with DCB for treatment of dialysis access stenosis The Greek experience
 First experience with DCB for treatment of dialysis access stenosis The Greek experience D Karnabatidis Department of Interventional Radiology Patras University Hospital Patras, Greece Background Vessel
First experience with DCB for treatment of dialysis access stenosis The Greek experience D Karnabatidis Department of Interventional Radiology Patras University Hospital Patras, Greece Background Vessel
Interventions for AV-Shunt stenosis: What works best PTA, Stent or DCB?
 Interventions for AV-Shunt stenosis: What works best PTA, Stent or DCB? Martin Forlee Vascular Surgeon Cape Town Disclosure Speaker name: Martin Forlee I have the following potential conflicts of interest
Interventions for AV-Shunt stenosis: What works best PTA, Stent or DCB? Martin Forlee Vascular Surgeon Cape Town Disclosure Speaker name: Martin Forlee I have the following potential conflicts of interest
Angioplasty remains the most common method
 When AVF Angioplasty Fails Defining procedural success and overcoming common problems. By Thomas M. Vesely, MD Angioplasty remains the most common method of treating obstructive vascular stenoses associated
When AVF Angioplasty Fails Defining procedural success and overcoming common problems. By Thomas M. Vesely, MD Angioplasty remains the most common method of treating obstructive vascular stenoses associated
LUTONIX AV Clinical Trial
 LUTONIX AV Clinical Trial A Prospective, Global, Multicenter, Randomized, Controlled Study Comparing LUTONIX 035 AV Drug Coated Balloon PTA Catheter vs. Standard Balloon PTA Catheter for the Treatment
LUTONIX AV Clinical Trial A Prospective, Global, Multicenter, Randomized, Controlled Study Comparing LUTONIX 035 AV Drug Coated Balloon PTA Catheter vs. Standard Balloon PTA Catheter for the Treatment
ASDIN 7th Annual Scientific Meeting DISCLOSURES TECHNICAL CONSIDERATIONS TECHNICAL CONSIDERATIONS UTILITY OF ULTRASOUND IN EVALUATING ACCESS
 DISCLOSURES UTILITY OF ULTRASOUND IN EVALUATING ACCESS DYSFUNCTION None Vandana Dua Niyyar, MD Assistant Professor of Medicine, Division of Nephrology, Emory University UTILITY OF ULTRASOUND IN ACCESS
DISCLOSURES UTILITY OF ULTRASOUND IN EVALUATING ACCESS DYSFUNCTION None Vandana Dua Niyyar, MD Assistant Professor of Medicine, Division of Nephrology, Emory University UTILITY OF ULTRASOUND IN ACCESS
IN ARTERIOVENOUS FISTULA FAILURE
 DRUG ELUTING BALLOON ANGIOPLASTY IN ARTERIOVENOUS FISTULA FAILURE Nicola Troisi, MD GUIDELINES GUIDELINES VAS 2007 GUIDELINES VAS 2007 GUIDELINES VAS 2007 GUIDELINES VAS 2007 2007!!!!!!!!!! GUIDELINES
DRUG ELUTING BALLOON ANGIOPLASTY IN ARTERIOVENOUS FISTULA FAILURE Nicola Troisi, MD GUIDELINES GUIDELINES VAS 2007 GUIDELINES VAS 2007 GUIDELINES VAS 2007 GUIDELINES VAS 2007 2007!!!!!!!!!! GUIDELINES
Recurrent lesions in AV access & Initial DCB experience in India
 Recurrent lesions in AV access & Initial DCB experience in India Dr. Virender K Sheorain Consultant Interventional Radiologist Medanta-The Medicity Hospital Gurgaon, INDIA Disclosure Speaker name:... I
Recurrent lesions in AV access & Initial DCB experience in India Dr. Virender K Sheorain Consultant Interventional Radiologist Medanta-The Medicity Hospital Gurgaon, INDIA Disclosure Speaker name:... I
The recent United States Renal Data System
 Maintenance of Hemodialysis ccess With Stents and Covered Stents Hemodialysis access maintenance advances beyond angioplasty. Y RT L. DOLMTCH, MD The recent United States Renal Data System report 1 shows
Maintenance of Hemodialysis ccess With Stents and Covered Stents Hemodialysis access maintenance advances beyond angioplasty. Y RT L. DOLMTCH, MD The recent United States Renal Data System report 1 shows
4/29/2012. Management of Central Vein Stenoses. Central Venous Stenoses and Occlusions
 Central Venous Stenoses and Occlusions Management of Central Vein Stenoses Robert K. Kerlan Jr. M.D. Professor of Clinical Radiology and Surgery University of California San Francisco Key Questions What
Central Venous Stenoses and Occlusions Management of Central Vein Stenoses Robert K. Kerlan Jr. M.D. Professor of Clinical Radiology and Surgery University of California San Francisco Key Questions What
Supera for the Juxta-anastomotic AVF Stenosis
 Supera for the Juxta-anastomotic AVF Stenosis Dr Shannon D. Thomas Vascular Access Surgeon Conjoint Senior Lecturer University of New South Wales Sydney, Australia Disclosure Speaker name: Dr S. D. Thomas...
Supera for the Juxta-anastomotic AVF Stenosis Dr Shannon D. Thomas Vascular Access Surgeon Conjoint Senior Lecturer University of New South Wales Sydney, Australia Disclosure Speaker name: Dr S. D. Thomas...
Regardless of whether you are a vascular surgeon,
 C A S E R E P O R T The Versatility of the GORE VIABAHN Endoprosthesis Several case reports highlighting its unique design and why it is a valuable tool for the interventionist. BY PETER WAYNE, MD Regardless
C A S E R E P O R T The Versatility of the GORE VIABAHN Endoprosthesis Several case reports highlighting its unique design and why it is a valuable tool for the interventionist. BY PETER WAYNE, MD Regardless
Distal Hypoperfusion Ischemic Syndrome (DHIS)
") Pathophysiology Traditional View ( Steal Syndrome ) Distal Hypoperfusion Ischemic Syndrome (DHIS) Steven Wu, MD Director of Interventional Nephrology Massachusetts General Hospital Harvard Medical School
Pathophysiology Traditional View ( Steal Syndrome ) Distal Hypoperfusion Ischemic Syndrome (DHIS) Steven Wu, MD Director of Interventional Nephrology Massachusetts General Hospital Harvard Medical School
Current Status of DCB Experience with Non- Femoropopliteal Applications (Dialysis, Tibial, Venous)
") Current Status of DCB Experience with Non- Femoropopliteal Applications (Dialysis, Tibial, Venous) Saher Sabri, MD University of Virginia Health System Charlottesville, Virginia Dialysis vascular access
Current Status of DCB Experience with Non- Femoropopliteal Applications (Dialysis, Tibial, Venous) Saher Sabri, MD University of Virginia Health System Charlottesville, Virginia Dialysis vascular access
Juxta-anastomotic stenoses: angioplasty or surgery (or when/why should we wait)?
?") Juxta-anastomotic stenoses: angioplasty or surgery (or when/why should we wait)? Richard Shoenfeld MD, FSIR, FAHA The Access Center at West Orange West Orange, New Jersey USA SEDAV 2015 Madrid November
Juxta-anastomotic stenoses: angioplasty or surgery (or when/why should we wait)? Richard Shoenfeld MD, FSIR, FAHA The Access Center at West Orange West Orange, New Jersey USA SEDAV 2015 Madrid November
The Role of LUTONIX 035 DCB in AV Fistula Dysfunction Management in our Practice
 The Role of LUTONIX 035 DCB in AV Fistula Dysfunction Management in our Practice Dr Kate Steiner Consultant Interventional Radiologist East and North Hertfordshire NHS Trust Disclosure Speaker name: Dr
The Role of LUTONIX 035 DCB in AV Fistula Dysfunction Management in our Practice Dr Kate Steiner Consultant Interventional Radiologist East and North Hertfordshire NHS Trust Disclosure Speaker name: Dr
What s on the Horizon in Dialysis Access? Libby Watch, MD, FACS Miami Cardiac & Vascular Institute
 What s on the Horizon in Dialysis Access? Libby Watch, MD, FACS Miami Cardiac & Vascular Institute Disclosures No relevant disclosures Employee Advanced Access Care Dialysis Work 5 operating surgeons 3
What s on the Horizon in Dialysis Access? Libby Watch, MD, FACS Miami Cardiac & Vascular Institute Disclosures No relevant disclosures Employee Advanced Access Care Dialysis Work 5 operating surgeons 3
UPDATE IN VASCULAR ACCESS Mercedeh Kiaii MD FRCPC Rick Luscombe RN BSN CNeph(C) Elizabeth Lee MD FRCPC
 Elizabeth Lee MD FRCPC") UPDATE IN VASCULAR ACCESS Mercedeh Kiaii MD FRCPC Rick Luscombe RN BSN CNeph(C) Elizabeth Lee MD FRCPC Background Endovascular AVF Outline Data from FLEX and NEAT study SPH data Clinical experience Cannulation
UPDATE IN VASCULAR ACCESS Mercedeh Kiaii MD FRCPC Rick Luscombe RN BSN CNeph(C) Elizabeth Lee MD FRCPC Background Endovascular AVF Outline Data from FLEX and NEAT study SPH data Clinical experience Cannulation
AV Access Technology and Innovation DEVICES CHANGING HOW WE THINK ABOUT VASCULAR ACCESS
 AV Access Technology and Innovation DEVICES CHANGING HOW WE THINK ABOUT VASCULAR ACCESS Vascular Access New Technology What problem are you trying to solve for? Most common problem is inadequate outflow
AV Access Technology and Innovation DEVICES CHANGING HOW WE THINK ABOUT VASCULAR ACCESS Vascular Access New Technology What problem are you trying to solve for? Most common problem is inadequate outflow
ENDOVASCULAR TREATMENT OF MALFUNCTIONING HAEMODIALYSIS GRAFTS/FISTULAS. Dr R Uberoi Interventional Radiologist John Radcliffe hospital Oxford.
 ENDOVASCULAR TREATMENT OF MALFUNCTIONING HAEMODIALYSIS GRAFTS/FISTULAS Dr R Uberoi Interventional Radiologist John Radcliffe hospital Oxford. Stenosis Stenosis Native fistula/grafts. Radio-cephalic 55-75%
ENDOVASCULAR TREATMENT OF MALFUNCTIONING HAEMODIALYSIS GRAFTS/FISTULAS Dr R Uberoi Interventional Radiologist John Radcliffe hospital Oxford. Stenosis Stenosis Native fistula/grafts. Radio-cephalic 55-75%
Postoperative AV Fistula Evaluation. Postoperative examination protocol. Postoperative AVF Protocol. Hemodialysis Access Surveillance
 Hemodialysis Access Surveillance Postoperative AV Fistula Evaluation Failure of maturation Stenosis Perigraft mass/fluid collection Joseph L. Mills, Sr., M.D. Professor of Surgery Chief, Division of Vascular
Hemodialysis Access Surveillance Postoperative AV Fistula Evaluation Failure of maturation Stenosis Perigraft mass/fluid collection Joseph L. Mills, Sr., M.D. Professor of Surgery Chief, Division of Vascular
Salvaging prosthetic dialysis fistulas with stents: Forearm versus upper arm grafts
 From the Society for Clinical Vascular Surgery Salvaging prosthetic dialysis fistulas with stents: Forearm versus upper arm grafts Stephen Kolakowski, Jr, MD, Matthew J. Dougherty, MD, and Keith D. Calligaro,
From the Society for Clinical Vascular Surgery Salvaging prosthetic dialysis fistulas with stents: Forearm versus upper arm grafts Stephen Kolakowski, Jr, MD, Matthew J. Dougherty, MD, and Keith D. Calligaro,
Lutonix AV Clinical Trial
 Lutonix AV Clinical Trial Long Term Effects of LUTONIX 035 DCB Catheter 18 month Interim Results Scott O. Trerotola, MD Stanley Baum Professor of Radiology Professor of Surgery Associate Chair and Chief,
Lutonix AV Clinical Trial Long Term Effects of LUTONIX 035 DCB Catheter 18 month Interim Results Scott O. Trerotola, MD Stanley Baum Professor of Radiology Professor of Surgery Associate Chair and Chief,
Selection of Permanent Hemodialysis Vascular Access
 Selection of Permanent Hemodialysis Vascular Access TABLE OF CONTENTS 1.0 Scope...1 2.0 Recommendations & Rationale... 2 3.0 References... 3 4.0 Sponsors... 9 5.0 Effective Date... 10 Appendix 1: Key Elements
Selection of Permanent Hemodialysis Vascular Access TABLE OF CONTENTS 1.0 Scope...1 2.0 Recommendations & Rationale... 2 3.0 References... 3 4.0 Sponsors... 9 5.0 Effective Date... 10 Appendix 1: Key Elements
DCB in the treatment of av-accessa single center prospective study
 DCB in the treatment of av-accessa single center prospective study Dr. med. Tobias Steinke Schön Klinik Fachzentrum Gefäßchirurgie, Düsseldorf Disclosure Speaker name: Dr. med. Tobias Steinke I have the
DCB in the treatment of av-accessa single center prospective study Dr. med. Tobias Steinke Schön Klinik Fachzentrum Gefäßchirurgie, Düsseldorf Disclosure Speaker name: Dr. med. Tobias Steinke I have the
Few occlusive problems in arteriovenous access
 Treatment of VG Venous nastomotic Stenosis Clinical indicators and treatment techniques for this common cause of arteriovenous graft failure. y art L. Dolmatch, MD Few occlusive problems in arteriovenous
Treatment of VG Venous nastomotic Stenosis Clinical indicators and treatment techniques for this common cause of arteriovenous graft failure. y art L. Dolmatch, MD Few occlusive problems in arteriovenous
The HeRO Graft. Shawn M. Gage, PA Division of Vascular Surgery Duke University Medical Center
 The HeRO Graft Shawn M. Gage, PA Division of Vascular Surgery Duke University Medical Center Faculty Disclosure I disclose the following financial relationships: CryoLife/Hemosphere, Inc. & W.L. Gore and
The HeRO Graft Shawn M. Gage, PA Division of Vascular Surgery Duke University Medical Center Faculty Disclosure I disclose the following financial relationships: CryoLife/Hemosphere, Inc. & W.L. Gore and
UC SF. End Stage Renal Disease. National Kidney Foundation Dialysis Outcomes Quality Initiative (K/DOQI) BUT-- No Cephalic Vein What s Next
 BUT-- No Cephalic Vein What s Next") No Cephalic Vein What s Next End Stage Renal Disease Charles Eichler MD Clinical Professor of Surgery Division of Vascular Surgery UCSF April 5, 2014 Population of patients with ESRD growing rapidly -
No Cephalic Vein What s Next End Stage Renal Disease Charles Eichler MD Clinical Professor of Surgery Division of Vascular Surgery UCSF April 5, 2014 Population of patients with ESRD growing rapidly -
Guidelines for Arteriovenous Access Intervention, Management and Abandonment, and for Removal of Pre- Study Dialysis Catheter
 Guidelines for Arteriovenous Access Intervention, Management and Abandonment, and for Removal of Pre- Study Dialysis Catheter The guidelines for arteriovenous access intervention, management and abandonment,
Guidelines for Arteriovenous Access Intervention, Management and Abandonment, and for Removal of Pre- Study Dialysis Catheter The guidelines for arteriovenous access intervention, management and abandonment,
CIRCUIT OPTIMIZING THE VASCULAR ACCESS. Bringing long-term value to AV access creation and intervention. Sponsored by Gore & Associates.
 Supplement to June 2018 OPTIMIZING THE VASCULAR ACCESS CIRCUIT Bringing long-term value to AV access creation and intervention TABLE OF 2 SUPPLEMENT TO ENDOVASCULAR TODAY JUNE 2018 VOL. 17, NO. 6 CONTENTS
Supplement to June 2018 OPTIMIZING THE VASCULAR ACCESS CIRCUIT Bringing long-term value to AV access creation and intervention TABLE OF 2 SUPPLEMENT TO ENDOVASCULAR TODAY JUNE 2018 VOL. 17, NO. 6 CONTENTS
CATHETER REDUCTION. Angelo N. Makris, M.D. Medical Director Chicago Access Care
 CATHETER REDUCTION Angelo N. Makris, M.D. Medical Director Chicago Access Care Objectives Discuss tools/techniques proven to improve AVF rates & decrease catheter rates Implement a change process in your
CATHETER REDUCTION Angelo N. Makris, M.D. Medical Director Chicago Access Care Objectives Discuss tools/techniques proven to improve AVF rates & decrease catheter rates Implement a change process in your
Hemodialysis Fistula Maturation Consortium
 Hemodialysis Fistula Maturation Consortium Rationale for Fistula Maturation Study Dialysis Access Consortium AVF study 60% of new AVFs were unusable for dialysis at 4-5 months post surgery No predictors
Hemodialysis Fistula Maturation Consortium Rationale for Fistula Maturation Study Dialysis Access Consortium AVF study 60% of new AVFs were unusable for dialysis at 4-5 months post surgery No predictors
A Practical Review of the Use of Stents for the Maintenance of Hemodialysis Access
 How I Do It 217 A Practical Review of the Use of Stents for the Maintenance of Hemodialysis Access Michael Ginsburg, MD 1 Jonathan M. Lorenz, MD 2 Sean P. Zivin, MD 3 Steven Zangan, MD 2 Don Martinez,
How I Do It 217 A Practical Review of the Use of Stents for the Maintenance of Hemodialysis Access Michael Ginsburg, MD 1 Jonathan M. Lorenz, MD 2 Sean P. Zivin, MD 3 Steven Zangan, MD 2 Don Martinez,
Clinical Study Endovascular Stent Placement for Hemodialysis Arteriovenous Access Stenosis
 International Vascular Medicine Volume 215, Article ID 97122, 7 pages http://dx.doi.org/1.1155/215/97122 Clinical Study Endovascular Stent Placement for Hemodialysis Arteriovenous Access Stenosis Brendon
International Vascular Medicine Volume 215, Article ID 97122, 7 pages http://dx.doi.org/1.1155/215/97122 Clinical Study Endovascular Stent Placement for Hemodialysis Arteriovenous Access Stenosis Brendon
Inflow stenosis in arteriovenous fistulas and grafts: A multicenter, prospective study
 Kidney International, Vol. 67 (2005), pp. 1986 1992 Inflow stenosis in arteriovenous fistulas and grafts: A multicenter, prospective study ARIFASIF, FLORIN N. GADALEAN, DONNA MERRILL, GAUTAM CHERLA, CRISTIAN
Kidney International, Vol. 67 (2005), pp. 1986 1992 Inflow stenosis in arteriovenous fistulas and grafts: A multicenter, prospective study ARIFASIF, FLORIN N. GADALEAN, DONNA MERRILL, GAUTAM CHERLA, CRISTIAN
Which Stent Is Best for Various Femoropopliteal Anatomy? 2018 Pacific Northwest Endovascular Conference June 15-26, 2018 Seattle, WA
 Which Stent Is Best for Various Femoropopliteal Anatomy? 2018 Pacific Northwest Endovascular Conference June 15-26, 2018 Seattle, WA Brian DeRubertis, MD, FACS Associate Professor of Surgery UCLA Division
Which Stent Is Best for Various Femoropopliteal Anatomy? 2018 Pacific Northwest Endovascular Conference June 15-26, 2018 Seattle, WA Brian DeRubertis, MD, FACS Associate Professor of Surgery UCLA Division
Thrombectomy, open, arteriovenous fistula without revision, autogenous or nonautogenous dialysis graft (separate procedure)
") Dialysis Vascular Access Coverage, Coding and Reimbursement Overview Hospital Outpatient 2019 Edition All Reimbursement Amounts are Listed at ational Unadjusted Medicare Rates and Do ot Include the 2%
Dialysis Vascular Access Coverage, Coding and Reimbursement Overview Hospital Outpatient 2019 Edition All Reimbursement Amounts are Listed at ational Unadjusted Medicare Rates and Do ot Include the 2%
Konstantinos Katsanos, MSc, MD, PhD, EBIR
 Konstantinos Katsanos, MSc, MD, PhD, EBIR Interventional Radiologist Patras University Hospital, Rion, Greece & Guy s and St. Thomas Hospitals, London, UK Honoraria from MEDTRONIC, BOSTON SCI Research
Konstantinos Katsanos, MSc, MD, PhD, EBIR Interventional Radiologist Patras University Hospital, Rion, Greece & Guy s and St. Thomas Hospitals, London, UK Honoraria from MEDTRONIC, BOSTON SCI Research
Case #1. Case #1- Possible codes. Unraveling the -59 modifier. Principles of Interventional. CASE 1: Simple angioplasty
 Unraveling the -59 modifier Principles of Interventional Coding Donald Schon, MD, FACP Debra Lawson, CPC, PCS Distinct or independent from other services performed on the same day Normally not reported
Unraveling the -59 modifier Principles of Interventional Coding Donald Schon, MD, FACP Debra Lawson, CPC, PCS Distinct or independent from other services performed on the same day Normally not reported
Stent Graft versus Balloon Angioplasty for Failing Dialysis-Access Grafts
 The new england journal of medicine original article Stent Graft versus Balloon Angioplasty for Failing Dialysis-Access Grafts Ziv J. Haskal, M.D., Scott Trerotola, M.D., Bart Dolmatch, M.D., Earl Schuman,
The new england journal of medicine original article Stent Graft versus Balloon Angioplasty for Failing Dialysis-Access Grafts Ziv J. Haskal, M.D., Scott Trerotola, M.D., Bart Dolmatch, M.D., Earl Schuman,
Angiographic Changes following the Use of a Purse-String Suture Hemostasis Device in Hemodialysis Access Interventions
 Angiographic Changes following the Use of a Purse-String Suture Hemostasis Device in Hemodialysis Access Interventions Timothy W.I. Clark, MD, Shawn Haji-Momenian, MD, Andrew Kwak, MD, Michael C. Soulen,
Angiographic Changes following the Use of a Purse-String Suture Hemostasis Device in Hemodialysis Access Interventions Timothy W.I. Clark, MD, Shawn Haji-Momenian, MD, Andrew Kwak, MD, Michael C. Soulen,
Percutaneous and Surgical Treatments
 AVG Pseudoaneurysms Percutaneous and Surgical Treatments Marius Florescu M.D. Feb. 2015 ASDIN DEFINITION AVG Pseudoaneurysm Formation Incidence AVG Pseudoaneurysm incidence rate ranges between 2% and 10%
AVG Pseudoaneurysms Percutaneous and Surgical Treatments Marius Florescu M.D. Feb. 2015 ASDIN DEFINITION AVG Pseudoaneurysm Formation Incidence AVG Pseudoaneurysm incidence rate ranges between 2% and 10%
Steal Syndrome: The Role of the Vascular Lab
 Steal Syndrome: The Role of the Vascular Lab Eighth Overlook Noninvasive Vascular Lab Symposium Larry A. Scher, M.D. Professor of Surgery Division of Vascular Surgery Montefiore Medical Center Albert Einstein
Steal Syndrome: The Role of the Vascular Lab Eighth Overlook Noninvasive Vascular Lab Symposium Larry A. Scher, M.D. Professor of Surgery Division of Vascular Surgery Montefiore Medical Center Albert Einstein
Disclosure Statement. Objectives. Novel Therapies for Vascular Access Dysfunction: OptiflowDevice, Gene Therapy, and Sirolimus Wrap 2/29/2012
 Novel Therapies for Vascular Access Dysfunction: OptiflowDevice, Gene Therapy, and Sirolimus Wrap Neointimal Hyperplasia Characteristic Lesion of Dialysis Access Dysfunction AVF Timmy Lee, M.D., M.S.P.H.,
Novel Therapies for Vascular Access Dysfunction: OptiflowDevice, Gene Therapy, and Sirolimus Wrap Neointimal Hyperplasia Characteristic Lesion of Dialysis Access Dysfunction AVF Timmy Lee, M.D., M.S.P.H.,
Qizhuang Jin. Renal Division, Department of Medicine, Peking University First Hospital, Peking University Institute of Nephrology, Beijing, China
 Safety and Efficacy of the Paclitaxel Releasing Peripheral Balloon Dilatation Catheter (APERTO OTW ) for Arteriovenous Fistulae Stenosis: a Prospective, Multicenter, Randomized Controlled Trial APERTO
Safety and Efficacy of the Paclitaxel Releasing Peripheral Balloon Dilatation Catheter (APERTO OTW ) for Arteriovenous Fistulae Stenosis: a Prospective, Multicenter, Randomized Controlled Trial APERTO
The word stent originates in the dentistry literature to
 In-Depth Review Stent Placement in Hemodialysis Access: Historical Lessons, the State of the Art and Future Directions Alexander Yevzlin* and Arif Asif *Department of Medicine, Section of Interventional
In-Depth Review Stent Placement in Hemodialysis Access: Historical Lessons, the State of the Art and Future Directions Alexander Yevzlin* and Arif Asif *Department of Medicine, Section of Interventional
PREVENTION AND TREATMENT OF ANEURYSMS OF AUTOGENOUS DIALYSIS ACCESSES STEPHEN L. HILL, M.D.,F.A.C.S
 PREVENTION AND TREATMENT OF ANEURYSMS OF AUTOGENOUS DIALYSIS ACCESSES STEPHEN L. HILL, M.D.,F.A.C.S THE INCREASE IN THE CONSTRUCTION OF AUTOGENOUS FISTULAE OVER THE PAST TEN YEARS HAS BROUGHT WITH IT 1.
PREVENTION AND TREATMENT OF ANEURYSMS OF AUTOGENOUS DIALYSIS ACCESSES STEPHEN L. HILL, M.D.,F.A.C.S THE INCREASE IN THE CONSTRUCTION OF AUTOGENOUS FISTULAE OVER THE PAST TEN YEARS HAS BROUGHT WITH IT 1.
Vascular Access creation in the US A surgical perspective. Surendra Shenoy M.D., Ph.D. Section of Transplantation Department of Surgery
 Vascular Access creation in the US A surgical perspective Surendra Shenoy M.D., Ph.D. Section of Transplantation Department of Surgery Disclosures No specific disclosures pertaining to the topic of presentation
Vascular Access creation in the US A surgical perspective Surendra Shenoy M.D., Ph.D. Section of Transplantation Department of Surgery Disclosures No specific disclosures pertaining to the topic of presentation
VIRTUS: Trial Design and Primary Endpoint Results
 VIRTUS: Trial Design and Primary Endpoint Results Mahmood K. Razavi, MD St. Joseph Cardiac and Vascular Center Orange, CA, USA IMPORTANT INFORMATION: These materials are intended to describe common clinical
VIRTUS: Trial Design and Primary Endpoint Results Mahmood K. Razavi, MD St. Joseph Cardiac and Vascular Center Orange, CA, USA IMPORTANT INFORMATION: These materials are intended to describe common clinical
Surgical Options in Thrombectomy for Non-Surgeons
 Surgical Options in Thrombectomy for Non-Surgeons Shouwen Wang, MD, PhD, FASDIN AKDHC Ambulatory Surgery Center Arizona Kidney Disease and Hypertension Center Phoenix, Arizona Disclosure No relevant financial
Surgical Options in Thrombectomy for Non-Surgeons Shouwen Wang, MD, PhD, FASDIN AKDHC Ambulatory Surgery Center Arizona Kidney Disease and Hypertension Center Phoenix, Arizona Disclosure No relevant financial
ASDIN 7th Annual Scientific Meeting
 Strategies for Decreasing the Use of Hemodialysis Catheters ASDIN 7 th Annual Scientific Meeting Outline Late referral Primary failure Why Not PD? Summary Micah Chan MD MPH FACP Assistant Professor of
Strategies for Decreasing the Use of Hemodialysis Catheters ASDIN 7 th Annual Scientific Meeting Outline Late referral Primary failure Why Not PD? Summary Micah Chan MD MPH FACP Assistant Professor of
Percutaneous transluminal angioplasty in the treatment of stenosis of hemodialysis arteriovenous fistulae: our experience
 Percutaneous transluminal angioplasty in the treatment of stenosis of hemodialysis arteriovenous fistulae: our experience Poster No.: C-3355 Congress: ECR 2010 Type: Scientific Exhibit Topic: Interventional
Percutaneous transluminal angioplasty in the treatment of stenosis of hemodialysis arteriovenous fistulae: our experience Poster No.: C-3355 Congress: ECR 2010 Type: Scientific Exhibit Topic: Interventional
Update from Korea on the Lutonix SFA registry 12 month data
 Update from Korea on the Lutonix SFA registry 12 month data Prospective, Multicenter, Post-Market Registy Assessing the Clinical Use and Safety of the Lutonix Drug Coated Balloon in Femoropopliteal Arteries
Update from Korea on the Lutonix SFA registry 12 month data Prospective, Multicenter, Post-Market Registy Assessing the Clinical Use and Safety of the Lutonix Drug Coated Balloon in Femoropopliteal Arteries
Drug Eluting Balloon for AVF Angioplasty : Does it work?
 Drug Eluting Balloon for AVF Angioplasty : Does it work? Dr Kiang Hiong TAY (MBBS, FRCR, FAMS, FSIR) Head & Senior Consultant, Dept of Diagnostic Radiology, Singapore General Hospital Director Interventional
Drug Eluting Balloon for AVF Angioplasty : Does it work? Dr Kiang Hiong TAY (MBBS, FRCR, FAMS, FSIR) Head & Senior Consultant, Dept of Diagnostic Radiology, Singapore General Hospital Director Interventional
John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division
 John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division John Campbell, MD For the 12 months preceding this CME activity,
John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division John Campbell, MD For the 12 months preceding this CME activity,
Medical Director/Surgeon as Partners WebEx February 11, 2010
 Medical Director/Surgeon as Partners WebEx February 11, 2010 Over 400,000 patients are treated yearly for ESRD in the USA; 60% of these patients receive some form of hemodialysis Despite major advances
Medical Director/Surgeon as Partners WebEx February 11, 2010 Over 400,000 patients are treated yearly for ESRD in the USA; 60% of these patients receive some form of hemodialysis Despite major advances
HD Scanning: Velocities and Volume Flow
 HD Scanning: Velocities and Volume Flow Non-Invasive Lab Symposium West Orange, NJ April 27, 2018 Volume Flow Cindy Sturt, MD, FACS, RVT 500,000 Americans on dialysis 20-25% annual mortality 65% 5 year
HD Scanning: Velocities and Volume Flow Non-Invasive Lab Symposium West Orange, NJ April 27, 2018 Volume Flow Cindy Sturt, MD, FACS, RVT 500,000 Americans on dialysis 20-25% annual mortality 65% 5 year
Thoughtful vs. Dogmatic
 Debate on Balloon Assisted Maturation The Biology is Wrong: BAM Won t Work BAM Dr. Rapp Debate BIVF Dr. Lawson Jeffrey H. Lawson, M.D., Ph.D. Departments of Surgery and Pathology Duke University Medical
Debate on Balloon Assisted Maturation The Biology is Wrong: BAM Won t Work BAM Dr. Rapp Debate BIVF Dr. Lawson Jeffrey H. Lawson, M.D., Ph.D. Departments of Surgery and Pathology Duke University Medical
AVF Prevalence. Local elastase to aid fistula maturation. I have nothing to disclose
 Local elastase to aid fistula maturation Warren Gasper MD UCSF Vascular Surgery Fellow 2013 UCSF Vascular Symposium I have nothing to disclose AVF Prevalence 60.6% (April 2012) Fistula First Initiative
Local elastase to aid fistula maturation Warren Gasper MD UCSF Vascular Surgery Fellow 2013 UCSF Vascular Symposium I have nothing to disclose AVF Prevalence 60.6% (April 2012) Fistula First Initiative
ASDIN 7th Annual Scientific Meeting
 Partial aneurysmectomy is effective in managing aneurysm-associated complications and preserving dialysis arteriovenous fistulae Ammar Almehmi, MD, MPH Shouwen Wang, MD, PhD University of Arizona and AKDHC-ASC
Partial aneurysmectomy is effective in managing aneurysm-associated complications and preserving dialysis arteriovenous fistulae Ammar Almehmi, MD, MPH Shouwen Wang, MD, PhD University of Arizona and AKDHC-ASC
Real-World Experience With Drug-Coated Balloons in AV Access
 GLOBAL ROUNDTABLE Real-World Experience With Drug-Coated Balloons in AV Access Experts discuss the current use of DCBs in AV fistulas and review how upcoming trials may influence progress in this space.
GLOBAL ROUNDTABLE Real-World Experience With Drug-Coated Balloons in AV Access Experts discuss the current use of DCBs in AV fistulas and review how upcoming trials may influence progress in this space.
The ZILVERPASS study a randomized study comparing ZILVER PTX stenting with Bypass in femoropopliteal lesions
 The ZILVERPASS study a randomized study comparing ZILVER PTX stenting with Bypass in femoropopliteal lesions Dr. Sven Bräunlich Department of Angiology University-Hospital Leipzig, Germany Disclosure Speaker
The ZILVERPASS study a randomized study comparing ZILVER PTX stenting with Bypass in femoropopliteal lesions Dr. Sven Bräunlich Department of Angiology University-Hospital Leipzig, Germany Disclosure Speaker
Decreased Incidence of Clotted AV Access in Hemodialysis Patients after the Implementation of Follow up Program
 Global Journal of Health Science; Vol. 8, No. 10; 2016 ISSN 1916-9736 E-ISSN 1916-9744 Published by Canadian Center of Science and Education Decreased Incidence of Clotted AV Access in Hemodialysis Patients
Global Journal of Health Science; Vol. 8, No. 10; 2016 ISSN 1916-9736 E-ISSN 1916-9744 Published by Canadian Center of Science and Education Decreased Incidence of Clotted AV Access in Hemodialysis Patients
Pitfalls in pushing fistulas ----
 Pitfalls in pushing fistulas ---- An argument for more grafts Marc Webb, MD, FACS Michigan Vascular Access, PC March 27 th, 2009 Vascular Access for Hemodialysis ------- Basic facts - the need for Access
Pitfalls in pushing fistulas ---- An argument for more grafts Marc Webb, MD, FACS Michigan Vascular Access, PC March 27 th, 2009 Vascular Access for Hemodialysis ------- Basic facts - the need for Access
The Role of Lithotripsy in Solving the Challenges of Vascular Calcium. Thomas Zeller, MD
 The Role of Lithotripsy in Solving the Challenges of Vascular Calcium Thomas Zeller, MD 1 1 Disclosure Speaker name: Thomas Zeller... I have the following potential conflicts of interest to report: X X
The Role of Lithotripsy in Solving the Challenges of Vascular Calcium Thomas Zeller, MD 1 1 Disclosure Speaker name: Thomas Zeller... I have the following potential conflicts of interest to report: X X
HeRO. Jeffrey H. Lawson, M.D., Ph.D. Departments of Surgery and Pathology Duke University Medical Center Durham, North Carolina
 HeRO Jeffrey H. Lawson, M.D., Ph.D. Departments of Surgery and Pathology Duke University Medical Center Durham, North Carolina Disclosures Consulting, Clinical Trials and Opinion Hemosphere Ark Therapeutics
HeRO Jeffrey H. Lawson, M.D., Ph.D. Departments of Surgery and Pathology Duke University Medical Center Durham, North Carolina Disclosures Consulting, Clinical Trials and Opinion Hemosphere Ark Therapeutics
Percutaneous AV Fistula Creation. Ellipsys EndoAVF System
 Percutaneous AV Fistula Creation Ellipsys EndoAVF System Presented by Forest Rawls Jr CHT,CCHT-A,FNKF No Disclosures Various Access Types Some old Some new Scribner Shunt OUR OLD DEPENDABLE FRIEND
Percutaneous AV Fistula Creation Ellipsys EndoAVF System Presented by Forest Rawls Jr CHT,CCHT-A,FNKF No Disclosures Various Access Types Some old Some new Scribner Shunt OUR OLD DEPENDABLE FRIEND
TheSensitivityandSpecificityofClinicalExaminationoftheHemodialysisArterialVenousFistulaAVFasComparedtoAngiography
 : F Diseases Volume 16 Issue 3 Version 1.0 Year 2016 Type: Double Blind Peer Reviewed International Research Journal Publisher: Global Journals Inc. (USA) Online ISSN: 2249-4618 & Print ISSN: 0975-5888
: F Diseases Volume 16 Issue 3 Version 1.0 Year 2016 Type: Double Blind Peer Reviewed International Research Journal Publisher: Global Journals Inc. (USA) Online ISSN: 2249-4618 & Print ISSN: 0975-5888
Sid Bhende MD Sentara Vascular Specialists April 28 th Dialysis Access Review: Understanding the Access Options our Patients Face
 Sid Bhende MD Sentara Vascular Specialists April 28 th 2018 Dialysis Access Review: Understanding the Access Options our Patients Face Disclosures Dialysis Background Why is it important? Outline National
Sid Bhende MD Sentara Vascular Specialists April 28 th 2018 Dialysis Access Review: Understanding the Access Options our Patients Face Disclosures Dialysis Background Why is it important? Outline National
Christian Wissgott MD, PhD Assistant Director, Radiology Westküstenkliniken Heide
 2-Year Results Of The Tack Optimized Balloon Angioplasty (TOBA) Trial For Fem- Pop Lesions Demonstrates Safety and Efficacy Of The Tack Endovascular System In Repairing Focal Post-PTA Dissections Christian
2-Year Results Of The Tack Optimized Balloon Angioplasty (TOBA) Trial For Fem- Pop Lesions Demonstrates Safety and Efficacy Of The Tack Endovascular System In Repairing Focal Post-PTA Dissections Christian
FLEXIBLE, BALOON EXPANDABLE
 EARLY RESULTS OF A CLINICAL TRIAL OF FLEXIBLE, BALOON EXPANDABLE COVERED STENT GRAFT IN ILIAC OCCLUSIVE DISEASE Chris LeCroy Coastal Vascular and Interventional Pensacola, Florida Clinical Trial WL GORE
EARLY RESULTS OF A CLINICAL TRIAL OF FLEXIBLE, BALOON EXPANDABLE COVERED STENT GRAFT IN ILIAC OCCLUSIVE DISEASE Chris LeCroy Coastal Vascular and Interventional Pensacola, Florida Clinical Trial WL GORE
Access More Patients. Customize Each Seal.
 Access More. Customize Each Seal. The Least Invasive Path Towards Proven Patency ULTRA LOW PROFILE TO EASE ADVANCEMENT The flexible, ultra-low 12F ID Ovation ix delivery system enables you to navigate
Access More. Customize Each Seal. The Least Invasive Path Towards Proven Patency ULTRA LOW PROFILE TO EASE ADVANCEMENT The flexible, ultra-low 12F ID Ovation ix delivery system enables you to navigate
Conversion of tunneled hemodialysis catheter consigned patients to arteriovenous fistula
 Kidney International, Vol. 67 (2005), pp. 2399 2406 Conversion of tunneled hemodialysis catheter consigned patients to arteriovenous fistula ARIFASIF, GAUTAM CHERLA, DONNA MERRILL, CRISTIAN D. CIPLEU,
Kidney International, Vol. 67 (2005), pp. 2399 2406 Conversion of tunneled hemodialysis catheter consigned patients to arteriovenous fistula ARIFASIF, GAUTAM CHERLA, DONNA MERRILL, CRISTIAN D. CIPLEU,
Chapter 2 Proximal Forearm Arteriovenous Fistula Creation
 Chapter 2 Proximal Forearm Arteriovenous Fistula Creation Venkat Kalapatapu and Andre Ramdon Introduction Worldwide greater than two million patients need renal replacement therapy. The aging population
Chapter 2 Proximal Forearm Arteriovenous Fistula Creation Venkat Kalapatapu and Andre Ramdon Introduction Worldwide greater than two million patients need renal replacement therapy. The aging population
Gerald Beathard Annual State of the Art Lecture Innovations in Vascular Access - Have We Moved Forward?
 Gerald Beathard Annual State of the Art Lecture Innovations in Vascular Access - Have We Moved Forward? Maurizio Gallieni Nephrology and Dialysis Unit Ospedale S. Carlo Borromeo, ASST Santi Paolo e Carlo,
Gerald Beathard Annual State of the Art Lecture Innovations in Vascular Access - Have We Moved Forward? Maurizio Gallieni Nephrology and Dialysis Unit Ospedale S. Carlo Borromeo, ASST Santi Paolo e Carlo,
Clinical hemodialysis experience with percutaneous arteriovenous fistulas created using the Ellipsys vascular access system
 Hemodialysis International 2019 Original Article Clinical hemodialysis experience with percutaneous arteriovenous fistulas created using the Ellipsys vascular access system Hedia HEBIBI, 1,2,3 Jedjiga
Hemodialysis International 2019 Original Article Clinical hemodialysis experience with percutaneous arteriovenous fistulas created using the Ellipsys vascular access system Hedia HEBIBI, 1,2,3 Jedjiga
Management of In-stent Restenosis after Lower Extremity Endovascular Procedures
 Management of In-stent Restenosis after Lower Extremity Endovascular Procedures Piotr Sobieszczyk, MD Associate Director, Cardiac Catheterization Laboratory Cardiovascular Division and Vascular Medicine
Management of In-stent Restenosis after Lower Extremity Endovascular Procedures Piotr Sobieszczyk, MD Associate Director, Cardiac Catheterization Laboratory Cardiovascular Division and Vascular Medicine
Endovascular and Hybrid Treatment of TASC C & D Aortoiliac Occlusive Disease
 Endovascular and Hybrid Treatment of TASC C & D Aortoiliac Occlusive Disease Arash Bornak, MD FACS Vascular & Endovascular Surgery University of Miami Miller School of Medicine No disclosure BACKGROUND
Endovascular and Hybrid Treatment of TASC C & D Aortoiliac Occlusive Disease Arash Bornak, MD FACS Vascular & Endovascular Surgery University of Miami Miller School of Medicine No disclosure BACKGROUND