DENGUE EPIDEMIC: WHAT WE KNOW SO FAR TAN CHENG CHENG INTENSIVIST SULTANAH AMINAH JOHOR BAHRU
|
|
|
- Juniper Byron Baldwin
- 5 years ago
- Views:
Transcription

1 DENGUE EPIDEMIC: WHAT WE KNOW SO FAR TAN CHENG CHENG INTENSIVIST SULTANAH AMINAH JOHOR BAHRU
 and envelope protein (E) The non structural proteins: NS1, NS2A, NS2B, NS3, NS4A, NS4B and NS5 The proteins are involved in the various stages of the dengue viral replication The envelope")
2 2 Dengue Virus Genome A single stranded RNA Genome is about ribonucleotides, encoding 3 structural proteins and 7 non-structural proteins Structural proteins: capsid protein (C), membrane protein (M) and envelope protein (E) The non structural proteins: NS1, NS2A, NS2B, NS3, NS4A, NS4B and NS5 The proteins are involved in the various stages of the dengue viral replication The envelope protein (E) is involved in the initial attachment of the virus particles on host cells
, DenV 2 (6), DenV 3 (5) and DenV 4 (3) Malaysia hyperendemic as all serotypes could be isolated at any point of time")
3 3 Dengue Virus 4 serotypes, namely DenV 1, DenV 2, DenV 3 and DenV 4 Further Classification into genotypes is dependent on the geographically region where the virus was isolated The number of genotypes for each serotype are as follows: DenV 1 (5), DenV 2 (6), DenV 3 (5) and DenV 4 (3) Malaysia hyperendemic as all serotypes could be isolated at any point of time
4 4 DENGUE SEROTYPES YEAR 2013, 2014 AND : DENV : DENV : DENV : DENV : DENV3 70% 60% % 40% 30% 20% 10% 0% DENV1 DENV2 DENV3 DENV4
5 5 NO PREDICTABLE CYCLE FOR DEN V INFECTION Four-year cycle outbreaks: 1974, 1978, 1982, 1986, 1990 No predictable cycle from 1991 Three-year cycle outbreak from 2008 Yearly cycle outbreak from 2012 Usually an outbreak whenever there was a change in the dengue virus serotype as fewer people would be immune to the serotype after the change Each individual can have 4 times of Den V infection in his/her lifetime
6 Serological Profile 6

7 7 ADE: ANTIBODY-DEPENDENT ENHANCEMENT OF DENV INFECTION ADAPTED FROM TAKADA AND KAWAOKA, 2003 Virus bound to Ab, is able to enter macrophages via the Fc receptor This makes the infection of macrophages more efficient and leads to the infection of a large number of macrophages, leading in turn to a more severe clinical presentation According to this hypothesis, DHF/DSS should occur only when there is more than one serotype of DV circulating in a specific area
8 microbewiki.kenyon.edu 8
9 DENGUE INCIDENCE RATE & CASE FATALITY RATE FOR YEAR , MALAYSIA 9
 6543 14255 10146 7103 19429 16368 27381 19884 21900")
, MALAYSIA 120000 100000 80000 60000 40000 20000 0")
10 (till 18 July) Number of Cases DENGUE CASES (TILL 18 JULY), MALAYSIA Year
 Increase of cases 34% and deaths 91% CFR 0.")
11 11 DENGUE DEATHS (TILL 18 JULY) MALAYSIA Jan-18 July ,396 cases with 174 deaths (compared 48,845 cases with 91 deaths in 2014) Increase of cases 34% and deaths 91% CFR 0.26% (target < 0.2%)
12
")
13 DISTRIBUTION OF DENGUE CASES BY URBAN AND RURAL AREA ( ) 13
 Male")

14 DENGUE MORTALITY ANALYSIS 2014 (N = 197 DEATHS) Male 31% : 50 years old 50% : 25 to 49 years 19% : < 25 years old

15 DENGUE MORTALITY ANALYSIS 2014 (N = 197 DEATHS) Duration between disease onset and patients sought 1 st treatment Patients did seek early treatment: 62% within 48h after onset

16 DENGUE MORTALITY ANALYSIS 2014 (N = 197 DEATHS) Duration in days between admission & onset of disease 90% of patients admitted early to hospital within 5 days of onset
17 DENGUE MORTALITY ANALYSIS 2014 (N = 197 DEATHS) Duration between admission and death
18 18 ORGAN INVOLVED IN DENGUE DEATH Organ involved % 2012 % 2013 % 2014 CNS: Impaired consciousness Renal failure Hepatitis Multi-organ failure Heart
19 Dengue Infection 2010 n = 1643 Dengue Infection 2011 n = 798 Dengue Infection 2012 n = 906 Dengue Infection 2013 n=1550 Dengue Infection 2014 n=3261 Age, years median (IQR) 28.8 ( ) 29.5 ( ) 32.8 ( ) 31.3 ( ) 34.6 ( ) Interval from hospital to ICU admission, days median (IQR) Not available 0.5 ( ) 0.5 ( ) 0.5 ( ) 0.4 ( ) Length of ICU stay, days median (IQR) 1.9 ( ) 2.0 ( ) 1.9 ( ) 1.9 ( ) 2.8 ( ) Length of hospital stay, days median (IQR) Length of mechanical ventilation, days median (IQR) Total SAPS II score, mean +/-SD Median (IQR) 5.5 ( ) 3.8 ( ) 5.8 ( ) 3.6 ( ) 5.2 ( ) 4.2 ( ) 5.3 ( ) 2.9 ( ) 7.1 ( ) 5.0 ( ) ( ) % Invasive mechanical ventilation % 12.1 % Co-morbid diseases Main organ failure % Without organ failure Respiratory failure CVS failure Neurological failure Renal failure Hepatic failure Haematological failure SMR (95% CI) 0.75 ( ) ( ) 0.51 ( ) 0.50 ( ) 0.57 ( )
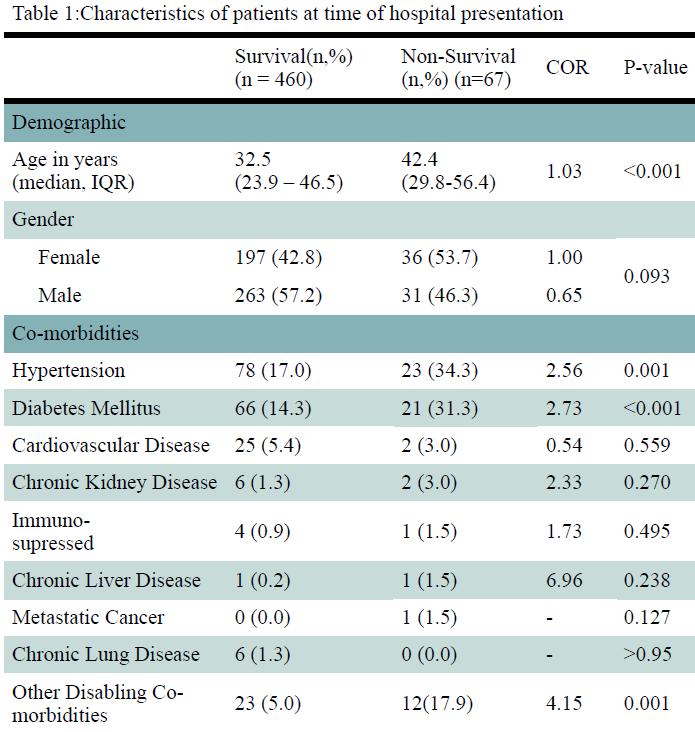
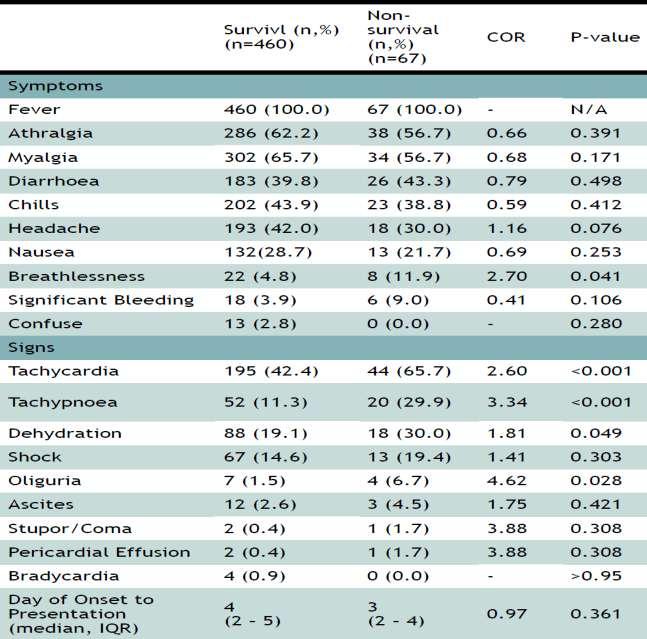
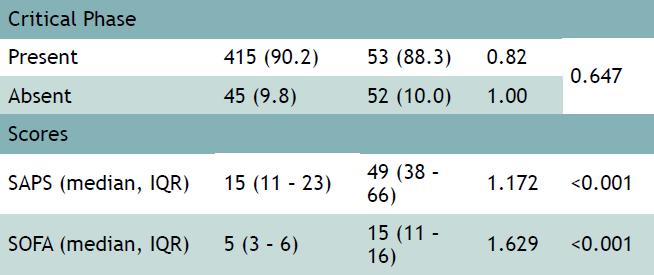
20 Severe Dengue in Intensive Care: Evaluation of Mortality Risk Factors Foong KW 1, Teoh SC 2, Woon YL 3, Lee HS 3, Abdul Rahim AH 4, Ismail NI 5, Kumarasamy S 6, Mohd Noor MR 7, Wan Ismail WN 8, Kamalul Bahrin LK 9, Tong MG 10, Vellayuthapillai S 2, Supramaniam P 3, Tan CC 11 Objective: To determine the demography of severe dengue cases in Intensive Care Unit (ICU) and identify the predictors of mortality Methods: Retrospective study of all adult dengue patients admitted to the 49 MOH ICUs in year 2013 Patients were identified via MRIC Medical records were reviewed by two intensivists independently to identify SD patients and determine its onset of critical phase Demographic, clinical and intervention data were extracted For patients with missing medical record, we assumed those who died were SD, and relevant data were extracted for mortality patients who appeared in both MRIC and National Dengue Mortality Enquiry Report
21 1531 cases coded as dengue identified from Malaysian Registry of Intensive Care (MRIC) 1436 patients medical record traced and screened by 2 intensivists independently 95 patients medical record missing 84 patients survived and excluded from analysis 916 excluded from analysis: -21 paediatric -188 not dengue -707 not severe dengue 520 severe dengue patients identified 11 patients died (data from MRIC) 4 patients not found in National Dengue Mortality Enquiry Report and excluded 7 patients with partial data from MRIC and National Dengue Mortality Enquiry Report 527 severe dengue cases analyzed The flow of patient selection / recruitment
22 1531 cases coded as dengue identified from Malaysian Registry of Intensive Care (MRIC) 1436 patients medical record traced and screened by 2 intensivists independently 95 patients medical record missing 84 patients survived and excluded from analysis 916 excluded from analysis: -21 paediatric -188 not dengue -707 not severe dengue 520 severe dengue patients identified 11 patients died (data from MRIC) 4 patients not found in National Dengue Mortality Enquiry Report and excluded 7 patients with partial data from MRIC and National Dengue Mortality Enquiry Report 527 severe dengue cases analyzed The flow of patient selection / recruitment 34.4% of all dengue admitted to ICU
23 1531 cases coded as dengue identified from Malaysian Registry of Intensive Care (MRIC) 1436 patients medical record traced and screened by 2 intensivists independently 95 patients medical record missing 84 patients survived and excluded from analysis 916 excluded from analysis: -21 paediatric -188 not dengue -707 not severe dengue 520 severe dengue patients identified 11 patients died (data from MRIC) 4 patients not found in National Dengue Mortality Enquiry Report and excluded 7 patients with partial data from MRIC and National Dengue Mortality Enquiry Report 12.7% ie 67 deaths 527 severe dengue cases analyzed The flow of patient selection / recruitment 34.4% of all dengue admitted to ICU
24
25
26

27

28 Table 4: Laboratory results at onset of critical phase / organ dysfunction*
29 Table 5 : Independent risk factors for predicting mortality in severe dengue identified by multivariate logistic regression model Variables* Estimate Adjusted OR 95% CI SAPS Tachycardia Lethargy Liver dysfunction Plasma leakage * The variables input in the models are diabetes mellitus, hypertension, breathlessness, dehydration, tachypnoe, oliguria, encephalitis, overbleeding, hematocrit on critical phase, platelet count on critical phase, SAPS II, tachycardia, lethargy, liver dysfunction and plasma leakage. The final model has a R-square of 0.658
30 Unusual Presentations of Severe Dengue Fever Encephalopathy Hepatic damage Cardiomyopathy Severe gastrointestinal hemorrhage
31 Unusual Presentations of Severe Dengue Fever Encephalopathy Hepatic damage Cardiomyopathy Severe gastrointestinal hemorrhage

32
33 Unusual Presentations of Severe Dengue Fever Encephalopathy Hepatic damage Cardiomyopathy Severe gastrointestinal hemorrhage

34

35 8 cases
36 Unusual Presentations of Severe Dengue Fever Encephalopathy Hepatic damage Cardiomyopathy Severe gastrointestinal hemorrhage
37 NATURE REVIEWS CARDIOLOGY REVIEW Cardiovascular manifestations of the emerging dengue pandemic Sophie Yacoub, Heiman Wertheim, Cameron P. Simmons, Gavin Screaton & Bridget Wills Nature Reviews Cardiology 11, (2014) doi: /nrcardio Published online 08 April 2014 Evidence is increasing that dengue can also cause myocardial impairment, arrhythmias and, occasionally, fulminant myocarditis. Defining the role of cardiac dysfunction in the haemodynamic compromise of severe dengue has potentially important management implications.
38 Unusual Presentations of Severe Dengue Fever Encephalopathy Hepatic damage Cardiomyopathy Severe gastrointestinal hemorrhage

39
40 REVISED 2 ND EDITION OF 2010 CPG 2015 THE CHANGES Calculating weight Fluid management Electrolytes and acid-base balance ECG and ECHO monitoring Haemophagocytic syndrome
41 Non-obese and non-overweight patients Maintenance fluid can be calculated based on the following formula : ml/kg/hour Obese and overweight patients Maintenance fluid can be calculated based on adjusted body weight Adjusted bodyweight (ABW) can be calculated using this formula. o ABW = IBW + 0.4(actual weight - IBW)* o Ideal bodyweight (IBW) can be estimated based on the following 72, level III formula. Female: 45.5 kg (height ) cm Male: 50.0 kg (height ) cm *Adapted : GlobalRPH 2015, calculator adjusted body weight (available at
42 REVISED 2 ND EDITION OF 2010 CPG 2015 THE CHANGES Calculating weight Fluid management Electrolytes and acid-base balance ECG and ECHO monitoring Haemophagocytic syndrome
43 ALGORITHM A FLUID MANAGEMENT IN COMPENSATED SHOCK COMPENSATED SHOCK (systolic pressure maintained but has signs of reduced perfusion) Fluid resuscitation with isotonic crystalloid 5 10ml/kg/h over 1h FBC, HCT, before and after fluid resuscitation, BUSEC, LFT, RBS, PT/APTT, Lactate/HCO 3, GXM YES IV crystalloid 5 7ml/kg/h x 1 2h, then: IMPROVEMENT* Check HCT NO reduce to 3 5 ml/kg/h for 2 4h reduce to 2 3 ml/kg/h for 2 4h If patient continues to improve, fluid can be further reduced. Monitor HCT 4 6 hourly If the patient is not stable, act according to HCT levels: If HCT, consider bolus fluid administration or fluid administration If HCT decreases, consider transfusion with fresh whole blood Consider to stop IV fluid at 48h of plasma leakage / defervescence. HCT or high Administer 2 nd bolus of fluid (colloid)** ml/kg/h for 1h IMPROVEMENT* YES If patient improves, reduce to 7-10 ml/kg/h for 1 2h Then reduce further HCT Consider significant occult/over bleed Initiate transfusion with fresh blood 2 (whole blood/packed cell) NO * Reassess the patient s clinical condition, vital signs, pulse volume, capillary refill time, urine output and temperature of extremities. ** Colloid is preferable if the patient has already received previous boluses of crystalloid
44 ALGORITHM B FLUID MANAGEMENT IN DECOMPENSATED SHOCK Fluid resuscitation with 20 ml/kg/h colloid minutes Try to obtain a HCT level before fluid resuscitation FBC, HCT, before and after fluid resuscitation, BUSEC, LFT, RBS, PT/APTT, Lactate/HCO 3, GXM YES IMPROVEMENT* NO Review 1 st HCT Crystalloid/colloid 10ml/kg/hx1h, then continue with: HCT or high HCT HCT Unchanged IV crystalloid 5 7 ml/kg/h for 1 2h reduce to 3-5 ml/kg/h for 2 4h reduce to 2 3 ml/kg/h for 2 4h If patient continues to improve, fluid can be further reduced. Monitor HCT q4h or more frequent as indicated If the patient is not stable, act according to HCT levels : If HCT, consider bolus fluid administration or fluid administration If HCT decreases, consider transfusion with fresh whole blood Consider to stop IV fluid at 48h of plasma leakage / defervescence Administer 2 nd bolus of fluid (colloid)** 10 20ml/kg ½ to 1h YES Repeat 3rd HCT IMPROVEMENT* NO YES Consider significant occult/overt bleed Initiate transfusion with fresh blood 2 (whole blood/packed cell) HCT or high NO Repeat 2 nd HCT HCT Administer 3 rd bolus of fluid (colloid) ml/kg over 1h IMPROVEMENT* REFER ALGORITHM C * Reassess the patient s clinical condition, vital signs, pulse volume, capillary refill time, urine output and temperature of extremities. Colloid is preferable if the patient has already received previous boluses of crystalloid ** In absence of colloid, crystalloid can be used
45 ALGORITHM C FLUID MANAGEMENT IN DECOMPENSATED SHOCK (WITH PRESENCE OF BLEEDING & LEAKING AND OTHER CAUSES SHOCK) HAEMATOCRIT REMAIN UNCHANGED AFTER FIRST FLUID RESUSCITATION Consider other causes of shock Bleeding and leaking at same time Look for source of bleeding (eg.ogds) Evidence of leaking (USG) Correct coagulopathy Transfused blood and blood products Cardiac dysfunction Septic shock Vasodilated state Liver failure with severe metabolic acidosis from lactate accumulation Cytokine storm Low CO: Inotrope (eg. dobutamine) High CO: Vasodilated shock with myocardia; dysfunction Inotropes + vasopressor (eg. Noradrenaline + dobutamine) Noradrenaline titrated to MAP 65 mmhg Vasopressor + Supportive care + Continuous renal replacement therapy (CRRT) Noradrenaline and fluids All the above types of shocks need to be supported by echocardiography and non-invasive cardiac output monitoring and treatments tailor to each patient.
46 REVISED 2 ND EDITION OF 2010 CPG 2015 THE CHANGES Calculating weight Fluid management Electrolytes and acid-base balance ECG and ECHO monitoring Haemophagocytic syndrome
47 ELECTROLYTES AND ACID-BASE BALANCE Hyponatraemia common observation in severe dengue - a marker of disease severity - underlying mechanism not fully understood -? GI loss or? use of hypotonic solution Metabolic acidosis -? Leakage and shock - consider severe bleeding, liver failure, sepsis, or cardiac dysfunction
48 REVISED 2 ND EDITION OF 2010 CPG 2015 THE CHANGES Calculating weight Fluid management Electrolytes and acid-base balance ECG and ECHO monitoring Haemophagocytic syndrome

49 79 patients (adult and children) with dengue infection with 3 severity grades ECHO exam of intravascular volume + myocardial tissue Doppler Imaging preload independent of cardiac function parameters after immediate resus, at 24h and at hospital discharge Systolic and diastolic impairment with segmental wall abnormalities of the septum and right ventricular wall Least severe dengue transient More severe dengue more frequently to have
50 RECOMMENDATION All cases of severe dengue in shock should have Echocardiography to look for evidence of cardiac dysfunction and to guide in fluid management. Adequate fluid resuscitation is a pre-requisite before myocardial dysfunction can be diagnosed. Cautious volume resuscitation is required in those with myocardial dysfunction to avoid risk of iatrogenic fluid overload.
51 REVISED 2 ND EDITION OF 2010 CPG 2015 THE CHANGES Calculating weight Fluid management Electrolytes and acid-base balance ECG and ECHO monitoring Haemophagocytic syndrome
52 HEMOPHAGOCYTIC SYNDROME A potentially fatal hyperinflammatory condition caused by highly stimulated but dysregulated and often ineffective immune responses Cardinal features: fever, hepato-splenomegaly, pancytopenia, and widespread histiocytic tissue infiltration 2 major forms: i. primary (hereditary) form - in early childhood ii. secondary (reactive) form - at any age - may be related to infection, malignancy, or autoimmune disease Dengue associated haemophagocytic syndrome increasingly reported in case reports and case series in past few years in both primary and secondary dengue infections - South East Asia & among returned travelers from tropical countries. Often missed or delayed as its presentation mimics sepsis
 d. Hepatitis 3. And at least 1 of 4: a. Hemophagocytosis b. Ferritin c. sil2rα (age based) d. Absent or very decreased NK function 4.")
53 DIAGNOSIS OF HLH Table 2. Proposed HLH diagnostic criteria, Molecular diagnosis of hemophagocytic lymphohistiocytosis (HLH) or X-linked lymphoproliferative syndrome (XLP). 2. Or at least 3 of 4: a. Fever b. Splenomegaly c. Cytopenias (minimum 2 cell lines reduced) d. Hepatitis 3. And at least 1 of 4: a. Hemophagocytosis b. Ferritin c. sil2rα (age based) d. Absent or very decreased NK function 4. Other results supportive of HLH diagnosis: a. Hypertriglyceridemia b. Hypofibrinogenemia c. Hyponatremia

54

55 Limitation: Goodness of fit 0.93 aroc Retrospective sample selection bias medical records, results of bone marrow aspirate, ICD-10 classification Classification of patients 4 investigators, independent Goodness of fit 0.76 aroc 0.95 Small validation sample 27 patients compared to 312 patients in development sample Validated mainly among population with autoimmune diseases - used with caution in infection associated HS
56 MANAGEMENT OF HS Mainly supportive Not so severe cases can recover spontaneously Sometimes, short course dexamethasone (10mg/m2 BSA) could be adequate Due to the transient nature of HS in dengue, full HLH 2004 treatment protocol which includes chemotherapy is not necessary For severe cases, HS specific therapy i.e IV methylprednisolone + IV Ig to be tapered off rapidly as patients improve clinically and biochemically In patients with co-existing sepsis and/or GIT bleeding, risks and benefits on use of steroids need to be weighed
57 TAKE HOME MESSAGE Do not forget the basics ie history, physical examination, investigations and diagnosis Look at the BIG picture do not fix your mind on one or two parameter Make a diagnosis after knowing the parameters more fluids, less fluids, on the right track, other diagnosis, further investigations Monitor response and medical condition Remember if you are on the right track, patient should get better
58 TAKE HOME MESSAGE Do not forget the basics ie history, physical examination, investigations and diagnosis Look at the BIG picture do not fix your mind on one or two parameter/s Make a diagnosis after knowing the parameters more fluids, less fluids, on the right track, other diagnosis, further investigations Monitor response and medical condition Remember if you are on the right track, patient should get better
59 TAKE HOME MESSAGE Do not forget the basics ie history, physical examination, investigations and diagnosis Look at the BIG picture do not fix your mind on one or two parameter Make a diagnosis after knowing the parameters more fluids, less fluids, on the right track, other diagnosis, further investigations Monitor response and medical condition Remember if you are on the right track, patient should get better
60 TAKE HOME MESSAGE Do not forget the basics ie history, physical examination, investigations and diagnosis Look at the BIG picture do not fix your mind on one or two parameter Make a diagnosis after knowing the parameters more fluids, less fluids, on the right track, other diagnosis, further investigations Monitor response and medical condition Remember if you are on the right track, patient should get better
61 TAKE HOME MESSAGE Do not forget the basics ie history, physical examination, investigations and diagnosis Look at the BIG picture do not fix your mind on one or two parameter Make a diagnosis after knowing the parameters more fluids, less fluids, on the right track, other diagnosis, further investigations Monitor response and medical condition Remember if you are on the right track, patient should get better
62 ACKNOWLEDGEMENTS Dr Rose Nani Mudin Public Health Physician (Epidemiologist) Head of Vector Borne Disease Sector, Disease Control Division, Ministry of Health Malaysia Dr Shaharom Nor Azian Che Mat Pengarah, Makmal Kesihatan Awam Dr Shanthi Ratnam Consultant Intensivist, Hospital Sungai Buloh Dr Kan Foong Kee Consultant ID, Hospital Sultanah Aminah
63 THANKS
64 PEARLS ON SEVERE DENGUE INFECTION Patient will not have plasma leakage before 72h of fever. Rise in hematocrit likely means dehydration. Oral rehydration usually suffices Transition from febrile phase to critical phase could be as early as day 3 or as late as day 7 or 8 Critical phase usually 24-48h Total white cell count (instead of leukopenia) may increase in patients with severe disease at critical phase Liver enzymes are frequently elevated during the critical and recovery phases
65 PEARLS ON SEVERE DENGUE INFECTION Warning sign of severe abdominal pain can be mistaken as a surgical condition fever precedes pain, tender but not guarded, pain improves with fluid resuscitation Tense abdomen after IV fluid therapy - due to ascites + liver congestion can cause abdominal pain - consider fluid overload instead! If IV fluid therapy increases, this can cause acute pulmonary oedema
66 MANAGEMENT PEARLS OF SEVERE DENGUE INFECTION History: Ask open-ended questions 3 golden questions to ask: How much oral fluid intake: quantity and quality? How much urine output: frequency, volume and time of most recent voiding? What activities can the patient do during the febrile illness? Examination: 5-in-1 maneuver magic touch CCTV-R Investigations: NS1, IgM, IgG and or PCR Diagnosis, phase of disease and severity: Does the patient have dengue or other illnesses? Which phase of dengue (febrile/critical/recovery)? How severe the disease is? -hydration state? warning signs present? haemodynamic state? Best medical plan: monitoring
67 PEARLS ON IV FLUID THERAPY IV fluid therapy is a Careful Budget of in and out with only one priority ie to maintain tissue perfusion In outpatient setting, patient should drink enough fluids to pass urine about 4 to 6 times a day A patient with dengue shock should pass at least 0.5 ml/kg/h urine. If urine volume exceeds 0.5ml/kg/h, consider reducing IV fluid therapy Remember uncontrolled diabetes or hyperglycemia - shock becomes worse because of glycosuria Remember changes in haematocrit may be masked by IV fluid therapy
68 PEARLS ON MONITORING Monitoring CCTV-R + investigations Big picture Make a diagnosis after knowing the parameters more fluids, less fluids, on the right track, other diagnosis, further investigations Remember if you are on the right track, patient should get better For severe disease with multi-organ involvement, consider hemophagocytic syndrome
MANAGEMENT OF DENGUE INFECTION IN ADULTS (Revised 2 nd Edition) QUICK REFERENCE FOR HEALTHCARE PROVIDERS
 QUICK REFERENCE FOR HEALTHCARE PROVIDERS") 1 KEY MESSAGES Dengue is a dynamic disease and presented in three phases - febrile phase, critical phase and recovery phase. Clinical deterioration often occurs in the critical phase and is marked by plasma
1 KEY MESSAGES Dengue is a dynamic disease and presented in three phases - febrile phase, critical phase and recovery phase. Clinical deterioration often occurs in the critical phase and is marked by plasma
INTRODUCTION. Dengue is one of the ten leading. Globally 20 million cases/yr. 24,000 deaths/yr. It is important to know the typical and atypical
 DENGUE IN CHILDREN INTRODUCTION Dengue is one of the ten leading causes of hospitalization and death in children. Globally 20 million cases/yr. 24,000 deaths/yr. It is important to know the typical and
DENGUE IN CHILDREN INTRODUCTION Dengue is one of the ten leading causes of hospitalization and death in children. Globally 20 million cases/yr. 24,000 deaths/yr. It is important to know the typical and
MODULE 8B: Management of Group B Dengue with Warning Signs or Dengue with Co-existing Conditions
 MODULE 8B: Management of Group B Dengue with Warning Signs or Dengue with Co-existing Conditions Dengue Clinical Management Acknowledgements This curriculum was developed with technical assistance from
MODULE 8B: Management of Group B Dengue with Warning Signs or Dengue with Co-existing Conditions Dengue Clinical Management Acknowledgements This curriculum was developed with technical assistance from
KEY MESSAGES. There are three phases in dengue infection-febrile phase, critical phase and recovery (reabsorption) phase.
 phase.") MANAGEMENT OF DENGUE INFECTION IN ADULTS (2 nd Edition) QUICK REFERENCE FOR HEALTH CARE PROVIDERS KEY MESSAGES Dengue is a systemic and dynamic disease. There are three phases in dengue infection-febrile
MANAGEMENT OF DENGUE INFECTION IN ADULTS (2 nd Edition) QUICK REFERENCE FOR HEALTH CARE PROVIDERS KEY MESSAGES Dengue is a systemic and dynamic disease. There are three phases in dengue infection-febrile
Severe Dengue Infection in ICU. Shirish Prayag MD, FCCM Pune, India
 Severe Dengue Infection in ICU Shirish Prayag MD, FCCM Pune, India Greetings from India Declaration Honararia from MSD, Astra Zenecea, Fresenius Kabi, Pfizer, Intas, Glenmark for conducting lectures. No
Severe Dengue Infection in ICU Shirish Prayag MD, FCCM Pune, India Greetings from India Declaration Honararia from MSD, Astra Zenecea, Fresenius Kabi, Pfizer, Intas, Glenmark for conducting lectures. No
Fluid balance in the critically ill child with dengue Too much too little? Professor Lucy Lum Universiti Malaya ASMIC Sept
 Fluid balance in the critically ill child with dengue Too much too little? Professor Lucy Lum Universiti Malaya ASMIC 2018 21-23 Sept CFR 0.22 in 2017 0.15 in 2018 2 Lecture Contents: Dynamic disease Self-limiting
Fluid balance in the critically ill child with dengue Too much too little? Professor Lucy Lum Universiti Malaya ASMIC 2018 21-23 Sept CFR 0.22 in 2017 0.15 in 2018 2 Lecture Contents: Dynamic disease Self-limiting
1. Dengue An Overview. Dengue Expert Advisory Group
 1. Dengue An Overview Dengue Expert Advisory Group 1 Introduction Dengue Fever Dengue Hemorrhagic Fever Dengue Shock Syndrome 2 3 Dengue Virus Family : Flaviviridae Genus : Flavivirus Serotypes : DV1,
1. Dengue An Overview Dengue Expert Advisory Group 1 Introduction Dengue Fever Dengue Hemorrhagic Fever Dengue Shock Syndrome 2 3 Dengue Virus Family : Flaviviridae Genus : Flavivirus Serotypes : DV1,
Fluid Management in Dengue Fever and Dengue Haemorrhagic Fever
 Fluid Management in Dengue Fever and Dengue Haemorrhagic Fever Dengue infection Dr. A LakKumar Fernando, Consultant Paediatrician Dengue is a disease which is silently transmitted in the community. For
Fluid Management in Dengue Fever and Dengue Haemorrhagic Fever Dengue infection Dr. A LakKumar Fernando, Consultant Paediatrician Dengue is a disease which is silently transmitted in the community. For
Dengue Fever & Dengue Shock Syndrome. 07-May-18 PLES / SLCP 1
 Dengue Fever & Dengue Shock Syndrome 07-May-18 PLES / SLCP 1 Objectives Early diagnosis Pathophysiology of DHF Proper management How to avoid complications Case 07-May-18 PLES / SLCP 2 Febrile Phase High
Dengue Fever & Dengue Shock Syndrome 07-May-18 PLES / SLCP 1 Objectives Early diagnosis Pathophysiology of DHF Proper management How to avoid complications Case 07-May-18 PLES / SLCP 2 Febrile Phase High
MODULE 7: Outpatient Management
 MODULE 7: Outpatient Management Dengue Clinical Management Acknowledgements This curriculum was developed with technical assistance from the University of Malaya Medical Centre. Materials were contributed
MODULE 7: Outpatient Management Dengue Clinical Management Acknowledgements This curriculum was developed with technical assistance from the University of Malaya Medical Centre. Materials were contributed
NASRONUDIN 4/17/2013. DENVs of each type are grouped into several genotypes.
 NASRONUDIN Institute of Tropical Disease, Airlangga University-Tropical and Infectious Diseases Division, Department of Internal Medicine Medical Faculty-Dr. Soetomo Hospital Disampaikan pada 14 th Jakarta
NASRONUDIN Institute of Tropical Disease, Airlangga University-Tropical and Infectious Diseases Division, Department of Internal Medicine Medical Faculty-Dr. Soetomo Hospital Disampaikan pada 14 th Jakarta
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Fine-tuning Management in Dengue Fever
 Fine-tuning Management in Dengue Fever Annual Scientific Meeting On Intensive Care 16 August 2014 Eg Kah Peng University of Malaya Medical Centre Rise In Dengue Infection New Straits Times 8 July 2014
Fine-tuning Management in Dengue Fever Annual Scientific Meeting On Intensive Care 16 August 2014 Eg Kah Peng University of Malaya Medical Centre Rise In Dengue Infection New Straits Times 8 July 2014
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Dengue Case Discussion. When things can go wrong!
 Dengue Case Discussion When things can go wrong! What the local experts say! 99.99% of walked in patients who come to hospital with dengue should walk out from hospital! Even those who come in Shock but
Dengue Case Discussion When things can go wrong! What the local experts say! 99.99% of walked in patients who come to hospital with dengue should walk out from hospital! Even those who come in Shock but
Department of Pediatrics, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok 10700, Thailand.
 SIRIRAJ MEDICAL LIBRARY SpecialIssue Clinical Practice Guide for the Management of Dengue Hemorrhagic Fever (DHF), Siriraj Hospital Kulkanya Chokephaibulkit, M.D., Wanee Wisuthsarewong, M.D., Gavivann
SIRIRAJ MEDICAL LIBRARY SpecialIssue Clinical Practice Guide for the Management of Dengue Hemorrhagic Fever (DHF), Siriraj Hospital Kulkanya Chokephaibulkit, M.D., Wanee Wisuthsarewong, M.D., Gavivann
MATERIAL AND METHODS Study objective: To study the clinical profile and predictors of mortality in children with severe dengue.
 INTERNATIONAL JOURNAL OF BIOASSAYS ISSN: 2278-778X CODEN: IJBNHY ORIGINAL RESEARCH ARTICLE OPEN ACCESS A PROSPECTIVE OBSERVATIONAL STUDY OF CLINICAL PREDICTORS OF OUTCOME IN DENGUE IN CHILDREN Sarada G,
INTERNATIONAL JOURNAL OF BIOASSAYS ISSN: 2278-778X CODEN: IJBNHY ORIGINAL RESEARCH ARTICLE OPEN ACCESS A PROSPECTIVE OBSERVATIONAL STUDY OF CLINICAL PREDICTORS OF OUTCOME IN DENGUE IN CHILDREN Sarada G,
Warm Autoantibodies in a Patient with Hemophagocytic Lymphohistiocytosis: A Case Report
 Warm Autoantibodies in a Patient with Hemophagocytic Lymphohistiocytosis: A Case Report Emily Coberly, MD Department of Pathology and Anatomical Sciences University of Missouri Columbia April 30, 2013
Warm Autoantibodies in a Patient with Hemophagocytic Lymphohistiocytosis: A Case Report Emily Coberly, MD Department of Pathology and Anatomical Sciences University of Missouri Columbia April 30, 2013
SEPSIS SYNDROME
 INTRODUCTION Sepsis has been defined as a life threatening condition that arises when the body s response to an infection injures its own tissues and organs. Sepsis may lead to shock, multiple organ failure
INTRODUCTION Sepsis has been defined as a life threatening condition that arises when the body s response to an infection injures its own tissues and organs. Sepsis may lead to shock, multiple organ failure
Sepsis Pathophysiology
 Sepsis Pathophysiology How Kids Differ From Adults Steve Standage Pediatric Critical Care Medicine Seattle Children's Hospital University of Washington School of Medicine Disclosures & Preamble No agenda,
Sepsis Pathophysiology How Kids Differ From Adults Steve Standage Pediatric Critical Care Medicine Seattle Children's Hospital University of Washington School of Medicine Disclosures & Preamble No agenda,
Initial Resuscitation of Sepsis & Septic Shock
 Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Sepsis Awareness and Education
 Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Clinical Management of Dengue Fever in Paediatric Patients
 Clinical Management of Dengue Fever in Paediatric Patients Dr. Mike Kwan Consultant Paediatrician Hospital Authority Infectious Disease Center Department of Paediatrics and Adolescent Medicine Princess
Clinical Management of Dengue Fever in Paediatric Patients Dr. Mike Kwan Consultant Paediatrician Hospital Authority Infectious Disease Center Department of Paediatrics and Adolescent Medicine Princess
Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL
 resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL") Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL 65 Male, 60 kg D1 in ICU Admitted from OT intubated Diagnosis : septic shock secondary to necrotising fasciitis of the R lower limb
Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL 65 Male, 60 kg D1 in ICU Admitted from OT intubated Diagnosis : septic shock secondary to necrotising fasciitis of the R lower limb
ISOVALERIC ACIDAEMIA -ACUTE DECOMPENSATION (standard version)
") Contact Details Name: Hospital Telephone: This protocol has 5 pages ISOVALERIC ACIDAEMIA -ACUTE DECOMPENSATION (standard version) Please read carefully. Meticulous treatment is very important as there
Contact Details Name: Hospital Telephone: This protocol has 5 pages ISOVALERIC ACIDAEMIA -ACUTE DECOMPENSATION (standard version) Please read carefully. Meticulous treatment is very important as there
Paediatric Shock. Dr Andrew Pittaway Department of Anaesthesia Bristol Royal Hospital for Children Bristol, UK
 Paediatric Shock Dr Andrew Pittaway Department of Anaesthesia Bristol Royal Hospital for Children Bristol, UK Self-assessment: 1. What is the definition of shock? 2. List the different pathophysiological
Paediatric Shock Dr Andrew Pittaway Department of Anaesthesia Bristol Royal Hospital for Children Bristol, UK Self-assessment: 1. What is the definition of shock? 2. List the different pathophysiological
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Sepsis Wave II Webinar Series. Sepsis Reassessment
 Sepsis Wave II Webinar Series Sepsis Reassessment Presenters Nova Panebianco, MD Todd Slesinger, MD Fluid Reassessment in Sepsis Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Residency Program Director
Sepsis Wave II Webinar Series Sepsis Reassessment Presenters Nova Panebianco, MD Todd Slesinger, MD Fluid Reassessment in Sepsis Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Residency Program Director
City Pediatric Meet-Dec 2011 SPECTRUM OF HLH. Spectrum of HLH. Dr.Revathi Raj s unit, Apollo Children s Hospital.
 City Pediatric Meet-Dec 2011 SPECTRUM OF HLH Spectrum of HLH Dr.Revathi Raj s unit, Apollo Children s Hospital. Case 1 4 month male child /thriving well Fever - 5 days with cough O/E hepatospenomegaly
City Pediatric Meet-Dec 2011 SPECTRUM OF HLH Spectrum of HLH Dr.Revathi Raj s unit, Apollo Children s Hospital. Case 1 4 month male child /thriving well Fever - 5 days with cough O/E hepatospenomegaly
Fluids in Sepsis Less is more. Dr Anand Senthi Joondalup Health Campus ED MBBS, MAppFin, GradCertPubHlth,
 Fluids in Sepsis Less is more Dr Anand Senthi Joondalup Health Campus ED MBBS, MAppFin, GradCertPubHlth, FRACGP @drsenthi Summary Discussion of the evidence for/against fluid resuscitation in septic shock
Fluids in Sepsis Less is more Dr Anand Senthi Joondalup Health Campus ED MBBS, MAppFin, GradCertPubHlth, FRACGP @drsenthi Summary Discussion of the evidence for/against fluid resuscitation in septic shock
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
IV fluid administration in sepsis. Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London
 IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
Shock and hemodynamic monitorization. Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital
 Shock and hemodynamic monitorization Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital Shock Leading cause of morbidity and mortality Worldwide: dehydration and hypovolemic
Shock and hemodynamic monitorization Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital Shock Leading cause of morbidity and mortality Worldwide: dehydration and hypovolemic
Example Clinician Educational Material for Providers of Immune Effector Cellular Therapy
 Example Clinician Educational Material for Providers of Immune Effector Cellular Therapy Disclaimer: This example is just one of many potential examples of clinician education material that can be provided
Example Clinician Educational Material for Providers of Immune Effector Cellular Therapy Disclaimer: This example is just one of many potential examples of clinician education material that can be provided
IV Fluids. I.V. Fluid Osmolarity Composition 0.9% NaCL (Normal Saline Solution, NSS) Uses/Clinical Considerations
 Uses/Clinical Considerations") IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
Chapter 5: Sepsis Stephen Lo
 Chapter 5: Sepsis Stephen Lo Introduction Sepsis and its consequence are the bread and butter of intensive care medicine and management of it is time critical. This chapter will discuss the definitions,
Chapter 5: Sepsis Stephen Lo Introduction Sepsis and its consequence are the bread and butter of intensive care medicine and management of it is time critical. This chapter will discuss the definitions,
Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR
 Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR A very important aspect in paediatric intensive care and deserve more attention Basic principle is to
Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR A very important aspect in paediatric intensive care and deserve more attention Basic principle is to
Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency
 Application of ICG in Intensive Care and Emergency") Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency Aim of haemodynamic monitoring in ICU and ED Detection and therapy of insufficient organ perfusion Answers to common cardiovascular
Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency Aim of haemodynamic monitoring in ICU and ED Detection and therapy of insufficient organ perfusion Answers to common cardiovascular
Brief summary of the NICE guidelines December 2013
 Brief summary of the NICE guidelines December 2013 Intravenous fluid therapy in adults in hospital the relevance to Emergency Department Care Applicable to patients 16 years and older receiving i.v. fluids
Brief summary of the NICE guidelines December 2013 Intravenous fluid therapy in adults in hospital the relevance to Emergency Department Care Applicable to patients 16 years and older receiving i.v. fluids
Approach to Severe Sepsis. Jan Hau Lee, MBBS, MRCPCH. MCI Children s Intensive Care Unit KK Women s and Children's Hospital, Singapore
 Approach to Severe Sepsis Jan Hau Lee, MBBS, MRCPCH. MCI Children s Intensive Care Unit KK Women s and Children's Hospital, Singapore 1 2 No conflict of interest Overview Epidemiology of Pediatric Severe
Approach to Severe Sepsis Jan Hau Lee, MBBS, MRCPCH. MCI Children s Intensive Care Unit KK Women s and Children's Hospital, Singapore 1 2 No conflict of interest Overview Epidemiology of Pediatric Severe
International Journal of Pharma and Bio Sciences A STUDY OF CLINCAL PROFILE IN DENGUE CASES ABSTRACT
 Research Article Microbiology International Journal of Pharma and Bio Sciences ISSN 0975-6299 A STUDY OF CLINCAL PROFILE IN DENGUE CASES DHANDAPANI E.* 1 AND SUDHA M 2 1 Formerly Professor of Medicine,
Research Article Microbiology International Journal of Pharma and Bio Sciences ISSN 0975-6299 A STUDY OF CLINCAL PROFILE IN DENGUE CASES DHANDAPANI E.* 1 AND SUDHA M 2 1 Formerly Professor of Medicine,
Tailored Volume Resuscitation in the Critically Ill is Achievable. Objectives. Clinical Case 2/16/2018
 Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
INTRAVENOUS FLUID THERAPY. Tom Heaps Consultant Acute Physician
 INTRAVENOUS FLUID THERAPY Tom Heaps Consultant Acute Physician LEARNING OBJECTIVES 1. Crystalloids vs colloids 2. Balanced vs non-balanced solutions 3. Composition of various IV fluids 4. What is normal
INTRAVENOUS FLUID THERAPY Tom Heaps Consultant Acute Physician LEARNING OBJECTIVES 1. Crystalloids vs colloids 2. Balanced vs non-balanced solutions 3. Composition of various IV fluids 4. What is normal
International Journal of Pediatrics and Neonatal Health
 International Journal of Pediatrics and Neonatal Health Research Article ISSN 2572-4355 Reduction in Deaths due to Severe Pneumonia with all-inclusive Treatment Subhashchandra Daga *1, Bela Verma 2, Chhaya
International Journal of Pediatrics and Neonatal Health Research Article ISSN 2572-4355 Reduction in Deaths due to Severe Pneumonia with all-inclusive Treatment Subhashchandra Daga *1, Bela Verma 2, Chhaya
Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand
 Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand Vital signs Symptoms LAB BT > 38.3 or < 36 ๐ C HR > 90 bpm RR > 20 /min
Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand Vital signs Symptoms LAB BT > 38.3 or < 36 ๐ C HR > 90 bpm RR > 20 /min
Taking the shock factor out of shock
 Taking the shock factor out of shock Julie Antonellis, BS, LVT, VTS (ECC) Northern Virginia Regional Director for the VALVT Technician Supervisor VCA Animal Emergency Critical Care Business owner Antonellis
Taking the shock factor out of shock Julie Antonellis, BS, LVT, VTS (ECC) Northern Virginia Regional Director for the VALVT Technician Supervisor VCA Animal Emergency Critical Care Business owner Antonellis
Principles of Infusion Therapy: Fluids
 Principles of Infusion Therapy: Fluids Christie Heinzman, MSN, APRN-CNP Acute Care Pediatric Nurse Practitioner Cincinnati Children s Hospital Medical Center May 22, 2018 Conflict of Interest Disclosure
Principles of Infusion Therapy: Fluids Christie Heinzman, MSN, APRN-CNP Acute Care Pediatric Nurse Practitioner Cincinnati Children s Hospital Medical Center May 22, 2018 Conflict of Interest Disclosure
Evidence- Based Medicine Fluid Therapy
 Evidence- Based Medicine Fluid Therapy Ndidi Musa M.D. Assosciate Professor of Pediatrics Medical College of Wisconsin/ Children s Hospital of Wisconsin Disclosures A. I have no relevant financial relationships
Evidence- Based Medicine Fluid Therapy Ndidi Musa M.D. Assosciate Professor of Pediatrics Medical College of Wisconsin/ Children s Hospital of Wisconsin Disclosures A. I have no relevant financial relationships
Original Article. Vol. 28 No. 2 Thai Adult Dengue Hemorrhagic Fever:- Sorakhunpipitkul L, et al.
 Original Article Vol. 28 No. 2 Thai Adult Dengue Hemorrhagic Fever:- Sorakhunpipitkul L, et al. 99 Thai Adult Dengue Hemorrhagic Fever During 2008-2010: Seven Cases Presented with Severe Multiorgan Failure
Original Article Vol. 28 No. 2 Thai Adult Dengue Hemorrhagic Fever:- Sorakhunpipitkul L, et al. 99 Thai Adult Dengue Hemorrhagic Fever During 2008-2010: Seven Cases Presented with Severe Multiorgan Failure
SLCOA National Guidelines
 SLCOA National Guidelines Peri - operative Fluid & Electrolyte Management SLCOA National Guidelines Contents List of Contributors 92 Paediatric fasting guidelines for elective procedures 93 Guidelines
SLCOA National Guidelines Peri - operative Fluid & Electrolyte Management SLCOA National Guidelines Contents List of Contributors 92 Paediatric fasting guidelines for elective procedures 93 Guidelines
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
INTENSIVE CARE MEDICINE CPD EVENING. Dr Alastair Morgan Wednesday 13 th September 2017
 INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
Pediatric Sepsis Treatment:
 Disclosures Pediatric Sepsis Treatment: (treat) Early & (reevaluate) Often None June 11, 2018 Leslie Dervan, MD MS Pacific Northwest Sepsis Conference 1 Agenda Sepsis: pathophysiology at-a-glance Pediatric
Disclosures Pediatric Sepsis Treatment: (treat) Early & (reevaluate) Often None June 11, 2018 Leslie Dervan, MD MS Pacific Northwest Sepsis Conference 1 Agenda Sepsis: pathophysiology at-a-glance Pediatric
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients. Keliana O Mara, PharmD August 4, 2018
 The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
MODULE 5. Dengue. Edwin J. Asturias Associate Professor of Pediatrics Senior Investigator Director for Latin America
 MODULE 5 Dengue Edwin J. Asturias Associate Professor of Pediatrics Senior Investigator Director for Latin America Symptoms of Dengue Fever Dengue: Skin rashes DHF manifestations Hemorrhages Thrombocytopenia
MODULE 5 Dengue Edwin J. Asturias Associate Professor of Pediatrics Senior Investigator Director for Latin America Symptoms of Dengue Fever Dengue: Skin rashes DHF manifestations Hemorrhages Thrombocytopenia
ICU management and referral guidelines for severe hypoxic respiratory failure
 Aim: ICU management and referral guidelines for severe hypoxic respiratory failure 1) To provide a concise management plan Non ventilatory Ventilatory 2) Timeline for referring patient with refractory
Aim: ICU management and referral guidelines for severe hypoxic respiratory failure 1) To provide a concise management plan Non ventilatory Ventilatory 2) Timeline for referring patient with refractory
for determining dengue severity in Thai patients
 Comparison of the 1997 and 2009 WHO classifications for determining dengue severity in Thai patients Auchara Tangsathapornpong 1, Pornumpa Bunjoungmanee 1, Pimpare Pengpris 1 and Thana Khawcharoenporn
Comparison of the 1997 and 2009 WHO classifications for determining dengue severity in Thai patients Auchara Tangsathapornpong 1, Pornumpa Bunjoungmanee 1, Pimpare Pengpris 1 and Thana Khawcharoenporn
Physiologic Based Management of Circulatory Shock Kuwait 2018
 Physiologic Based Management of Circulatory Shock Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program Staff Neonatologist
Physiologic Based Management of Circulatory Shock Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program Staff Neonatologist
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
Immunomodulation and Sepsis in Oncological Patients. Imad Haddad, M.D. Medical Director, PICU Banner Children s Hospital at BDMC
 Immunomodulation and Sepsis in Oncological Patients Imad Haddad, M.D. Medical Director, PICU Banner Children s Hospital at BDMC 1 Objectives Immune dys-regulation in oncological septic patients Implementation
Immunomodulation and Sepsis in Oncological Patients Imad Haddad, M.D. Medical Director, PICU Banner Children s Hospital at BDMC 1 Objectives Immune dys-regulation in oncological septic patients Implementation
Dr Ben Edwards Consultant Anaesthetist Sheffield Teaching Hospitals
 Dr Ben Edwards Consultant Anaesthetist Sheffield Teaching Hospitals 70-75,000 #NOF per annum (costs 2 billion) 10% die within 1 month 33% die within 1 year Operative delays >48hs more than doubles risk
Dr Ben Edwards Consultant Anaesthetist Sheffield Teaching Hospitals 70-75,000 #NOF per annum (costs 2 billion) 10% die within 1 month 33% die within 1 year Operative delays >48hs more than doubles risk
UNIVERSITI TEKNOLOGI MARA COPY NUMBER VARIATION OF FCGR3B GENE AMONG SEVERE DENGUE PATIENT IN MALAYSIA
 UNIVERSITI TEKNOLOGI MARA COPY NUMBER VARIATION OF FCGR3B GENE AMONG SEVERE DENGUE PATIENT IN MALAYSIA UMI SHAKINA HARIDAN Thesis submitted in fulfilment of the requirements for the degree of Master of
UNIVERSITI TEKNOLOGI MARA COPY NUMBER VARIATION OF FCGR3B GENE AMONG SEVERE DENGUE PATIENT IN MALAYSIA UMI SHAKINA HARIDAN Thesis submitted in fulfilment of the requirements for the degree of Master of
SHOCK Susanna Hilda Hutajulu, MD, PhD
 SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
 Manual: Section: Protocol #: Approval Date: Effective Date: Revision Due Date: 10/2019 LifeLine Patient Care Protocols Adult/Pediatrics AP1-011 10/2018 10/2018 FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
Manual: Section: Protocol #: Approval Date: Effective Date: Revision Due Date: 10/2019 LifeLine Patient Care Protocols Adult/Pediatrics AP1-011 10/2018 10/2018 FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
Albumina nel paziente critico. Savona 18 aprile 2007
 Albumina nel paziente critico Savona 18 aprile 2007 What Is Unique About Critical Care RCTs patients eligibility is primarily defined by location of care in the ICU rather than by the presence of a specific
Albumina nel paziente critico Savona 18 aprile 2007 What Is Unique About Critical Care RCTs patients eligibility is primarily defined by location of care in the ICU rather than by the presence of a specific
Current State of Pediatric Sepsis. Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018
 Current State of Pediatric Sepsis Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018 Objectives Review the history of pediatric sepsis Review the current definition of pediatric sepsis Review triage
Current State of Pediatric Sepsis Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018 Objectives Review the history of pediatric sepsis Review the current definition of pediatric sepsis Review triage
SEPSIS: IT ALL BEGINS WITH INFECTION. Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft.
 SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
Impact of Fluids in Children with Acute Lung Injury
 Impact of Fluids in Children with Acute Lung Injury Canadian Critical Care Forum Toronto, Canada October 27 th, 2015 Adrienne G. Randolph, MD, MSc Critical Care Division, Department of Anesthesia, Perioperative
Impact of Fluids in Children with Acute Lung Injury Canadian Critical Care Forum Toronto, Canada October 27 th, 2015 Adrienne G. Randolph, MD, MSc Critical Care Division, Department of Anesthesia, Perioperative
Clinical Profile of the Dengue Infection in Children
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 3 Ver.7 March. (18), PP 01-05 www.iosrjournals.org Clinical Profile of the Dengue Infection
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 3 Ver.7 March. (18), PP 01-05 www.iosrjournals.org Clinical Profile of the Dengue Infection
Frank Sebat, MD - June 29, 2006
 Types of Shock Hypovolemic Shock Low blood volume decreasing cardiac output. AN INTEGRATED SYSTEM OF CARE FOR PATIENTS AT RISK SHOCK TEAM and RAPID RESPONSE TEAM Septic or Distributive Shock Decrease in
Types of Shock Hypovolemic Shock Low blood volume decreasing cardiac output. AN INTEGRATED SYSTEM OF CARE FOR PATIENTS AT RISK SHOCK TEAM and RAPID RESPONSE TEAM Septic or Distributive Shock Decrease in
Presented by: Indah Dwi Pratiwi
 Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Fluids in ICU. JMO teaching 5th July 2016
 Fluids in ICU JMO teaching 5th July 2016 Objectives Physiology of fluid infusion History of fluid resuscitation Physiology of fluid resuscitation Types of resuscitation fluid The ideal resuscitation fluid
Fluids in ICU JMO teaching 5th July 2016 Objectives Physiology of fluid infusion History of fluid resuscitation Physiology of fluid resuscitation Types of resuscitation fluid The ideal resuscitation fluid
Thrombocytopenia, fever, rash, hypotension. Alexander D. Hristov MD University of Wisconsin Hospital and Clinic Internal Medicine PGY 2
 Thrombocytopenia, fever, rash, hypotension Alexander D. Hristov MD University of Wisconsin Hospital and Clinic Internal Medicine PGY 2 Case Chief Complaint: Fever, diarrhea, bloody nose, rash HPI: 38 y/o
Thrombocytopenia, fever, rash, hypotension Alexander D. Hristov MD University of Wisconsin Hospital and Clinic Internal Medicine PGY 2 Case Chief Complaint: Fever, diarrhea, bloody nose, rash HPI: 38 y/o
Alister Jones Patient Blood Management Practitioner NHS Blood and Transplant
 Alister Jones Patient Blood Management Practitioner NHS Blood and Transplant All medical RCC transfusions (but only 1 in 3 haematology or oncology cases) in 3 x one week periods Medical specialties include:
Alister Jones Patient Blood Management Practitioner NHS Blood and Transplant All medical RCC transfusions (but only 1 in 3 haematology or oncology cases) in 3 x one week periods Medical specialties include:
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
FLUIDS AND SOLUTIONS IN THE CRITICALLY ILL. Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium
 FLUIDS AND SOLUTIONS IN THE CRITICALLY ILL Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium Why do we want to administer fluids? To correct hypovolemia? To increase
FLUIDS AND SOLUTIONS IN THE CRITICALLY ILL Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium Why do we want to administer fluids? To correct hypovolemia? To increase
Outpatient dengue management
 Outpatient dengue management Dr David Lye FRACP, FAMS Senior consultant Institute of Infectious Diseases and Epidemiology, Communicable Diseases Centre, Tan Tock Seng Hospital Associate professor Yong
Outpatient dengue management Dr David Lye FRACP, FAMS Senior consultant Institute of Infectious Diseases and Epidemiology, Communicable Diseases Centre, Tan Tock Seng Hospital Associate professor Yong
Early-goal-directed therapy and protocolised treatment in septic shock
 CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
Early Goal-Directed Therapy
 Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY
 & COOLING THERAPY") Background NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY A perinatal hypoxic-ischaemic insult may present with varying degrees of neonatal encephalopathy, neurological disorder and
Background NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY A perinatal hypoxic-ischaemic insult may present with varying degrees of neonatal encephalopathy, neurological disorder and
Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium
 Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium MARIA E. MANDICH MD Fairbanks Memorial Hospital Emergency Department Attending Physician Interior Region EMS Council Medical Director
Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium MARIA E. MANDICH MD Fairbanks Memorial Hospital Emergency Department Attending Physician Interior Region EMS Council Medical Director
Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines
 Updated Guidelines") Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines Margaret Oates, PharmD, BCPPS Pediatric Critical Care Specialist GSHP Summer Meeting July 16, 2016 Disclosures I have nothing to
Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines Margaret Oates, PharmD, BCPPS Pediatric Critical Care Specialist GSHP Summer Meeting July 16, 2016 Disclosures I have nothing to
SHOCK and the Trauma Victim. JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital.
 SHOCK and the Trauma Victim JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital. Classification of Shock Cardiogenic - Myopathic Arrythmic Mechanical Hypovolaemic - Haemorrhagic Non-haemorrhagic
SHOCK and the Trauma Victim JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital. Classification of Shock Cardiogenic - Myopathic Arrythmic Mechanical Hypovolaemic - Haemorrhagic Non-haemorrhagic
Sepsis Management: Past, Present, and Future
 Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis overview. Dr. Tsang Hin Hung MBBS FHKCP FRCP
 Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Management of Cardiogenic Shock. Dr Stephen Pettit, Consultant Cardiologist
 Dr Stephen Pettit, Consultant Cardiologist Cardiogenic shock Management of Cardiogenic Shock Outline Definition, INTERMACS classification Medical management of cardiogenic shock PA catheters and haemodynamic
Dr Stephen Pettit, Consultant Cardiologist Cardiogenic shock Management of Cardiogenic Shock Outline Definition, INTERMACS classification Medical management of cardiogenic shock PA catheters and haemodynamic
HYPOVOLEMIA AND HEMORRHAGE UPDATE ON VOLUME RESUSCITATION HEMORRHAGE AND HYPOVOLEMIA DISTRIBUTION OF BODY FLUIDS 11/7/2015
 UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
Septic Shock. Rontgene M. Solante, MD, FPCP,FPSMID
 Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Sepsis and septic shock: can we win the battle against this hidden crisis?
 REVIEW ARTICLE Sepsis and septic shock: can we win the battle against this hidden crisis? V.G. Dassanayake Department of Surgery, Faculty of Medicine, University of Colombo, Sri Lanka Key words : Sepsis;
REVIEW ARTICLE Sepsis and septic shock: can we win the battle against this hidden crisis? V.G. Dassanayake Department of Surgery, Faculty of Medicine, University of Colombo, Sri Lanka Key words : Sepsis;
Risk Evaluation and Mitigation Strategy (REMS): Cytokine release syndrome and neurological toxicities
: Cytokine release syndrome and neurological toxicities") Risk Evaluation and Mitigation Strategy (REMS): Cytokine release syndrome and neurological toxicities A REMS is a program required by the FDA to manage known or potential serious risks associated with
Risk Evaluation and Mitigation Strategy (REMS): Cytokine release syndrome and neurological toxicities A REMS is a program required by the FDA to manage known or potential serious risks associated with
Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018
 Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018") Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018 Objectives 1. To identify the symptom of severe sepsis and septic shock syndrome.
Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018 Objectives 1. To identify the symptom of severe sepsis and septic shock syndrome.
Fluid balance and clinically relevant outcomes
 Fluid balance and clinically relevant outcomes Rui Moreno, MD, PhD, Professor UCINC, Hospital de São José Centro Hospitalar de Lisboa Central, E.P.E. INSULT PRIMARY MODS SIRS SECONDARY MODS OUTCOME RECOVERY
Fluid balance and clinically relevant outcomes Rui Moreno, MD, PhD, Professor UCINC, Hospital de São José Centro Hospitalar de Lisboa Central, E.P.E. INSULT PRIMARY MODS SIRS SECONDARY MODS OUTCOME RECOVERY
Ranjan Premaratna *, Erandi Liyanaarachchi, Mindu Weerasinghe, H Janaka de Silva. Abstract
 CASE REPORT Open Access Should colloid boluses be prioritized over crystalloid boluses for the management of dengue shock syndrome in the presence of ascites and pleural effusions? Ranjan Premaratna *,
CASE REPORT Open Access Should colloid boluses be prioritized over crystalloid boluses for the management of dengue shock syndrome in the presence of ascites and pleural effusions? Ranjan Premaratna *,
SHOCK. May 12, 2011 Body and Disease
 SHOCK May 12, 2011 Body and Disease Shock Definition of shock Pathophysiology Types of shock Management of shock Shock Definition? Shock What the Duke Community would have experienced if Gordon Hayward
SHOCK May 12, 2011 Body and Disease Shock Definition of shock Pathophysiology Types of shock Management of shock Shock Definition? Shock What the Duke Community would have experienced if Gordon Hayward
How and why I give IV fluid Disclosures SCA Fluids and public health 4/1/15. Andrew Shaw MB FRCA FCCM FFICM
 How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
Acute heart failure: ECMO Cardiology & Vascular Medicine 2012
 Acute heart failure: ECMO Cardiology & Vascular Medicine 2012 Lucia Jewbali cardiologist-intensivist 14 beds/8 ICU beds Acute coronary syndromes Heart failure/ Cardiogenic shock Post cardiotomy Heart
Acute heart failure: ECMO Cardiology & Vascular Medicine 2012 Lucia Jewbali cardiologist-intensivist 14 beds/8 ICU beds Acute coronary syndromes Heart failure/ Cardiogenic shock Post cardiotomy Heart
Fluid Resuscitation and Monitoring in Sepsis. Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS
 Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
The right heart: the Cinderella of heart failure
 The right heart: the Cinderella of heart failure Piotr Ponikowski, MD, PhD, FESC Medical University, Centre for Heart Disease Clinical Military Hospital Wroclaw, Poland none Disclosure Look into the Heart
The right heart: the Cinderella of heart failure Piotr Ponikowski, MD, PhD, FESC Medical University, Centre for Heart Disease Clinical Military Hospital Wroclaw, Poland none Disclosure Look into the Heart