Fluids in Sepsis Less is more. Dr Anand Senthi Joondalup Health Campus ED MBBS, MAppFin, GradCertPubHlth,
|
|
|
- Francis Robinson
- 5 years ago
- Views:
Transcription
1 Fluids in Sepsis Less is more Dr Anand Senthi Joondalup Health Campus ED MBBS, MAppFin, GradCertPubHlth,
2 Summary Discussion of the evidence for/against fluid resuscitation in septic shock What s the alternative to aggressive fluid resuscitation?
3 I AM NOT AN EXPERT! Disclosures I have no financial conflicts to disclose
4 Evidence of benefit of fluid resuscitation
5 Carcillo, JAMA 1991 Observational analysis of 34 kids with septic shock who had pulmonary artery catheters placed divided into 3 groups based on fluid in 1 st hour: Group 1 <20ml/kg: 6/14 survived Group 2: 20-40ml/kg: 4/11 survived Group 3: >40ml/kg: 8/9 survived
6 Carcillo, JAMA 1991 Issues: 1. Tiny retrospective study 2. Only patients with pulmonary artery cath included 3. Not controlled for different use of pressors/vent 4. No dose response
7 EGDT, Rivers 2001 The primary source of the Surviving Sepsis Guidelines (SSG) on fluid resus EGDT 5 L v Standard care 3.5L in 1 st 6 hours High controversial questionable validity Financial conflicts (Rivers and SSG), high mortality, differential clinical expertise Questions regarding whether results were real 25 patients excluded post randomisation if included à no significant mortality reduction PROCESS and ARISE now have debunked EGDT
8 Anecdotal experience We give fluids and patients look better!

9 Evidence of Fluid Causing Harms Several observational studies 1 x Animal RCT 1 large human RCT
10 Observational Studies Lead Author Year Journal Patients Pros/Retro Alsous 2000 Chest 36 Retro Vincent 2006 Crit Care Med 1177 Pros Rosenberg 2009 J of Int Care Med 844 Pros + post hoc Boyd 2011 Crit Care Med 778 Retro Micek 2013 Crit Care 163 Retro
11 Key points Positive fluid balance (early & late) was a strong independent predictor of mortality Vincent 2006, SOAP study OR 1.1 increased mortality per litre excess fluid Rosenberg 2009 ARDS Net Cumulative negative fluid balance by day 4 OR 0.5 for reduced mortality
12 Limitations of Observational Studies Positive fluid balance fluid administration Potential confounders eg shock severity However in most studies, positive fluid balance was an independent risk factor after multivariate logistic regression so key known confounders accounted for Unknown or unmeasured confounders may still be relevant

13
14 Brandt, Crit Care 2009 RCT in Pigs 48 pigs randomised in 3 groups: 1. faecal peritonitis 2. endotoxin infusion 3. control Then randomised to 2 treatments: moderate volume (10ml/kg/hr) high volume (20ml/kg/hr)
15 RCT in Pigs Results: Improved haemodynamics in high vol group Improved CI, higher MAP, lower lactate BUT: Increased mortality in high vol group Peritonitis: 87% v s 50% Endotoxemia: 75% v 13% Controls: 13% v 0%

16
17 RCT in Humans

18
19 RCT in Humans FEAST Trial, Maitland, NEJM 2011 Large, well conducted RCT in Africa: 3141 patients Investigated the effect of fluids in children with septic shock Patients randomised into 3 groups Intervention 1: 20ml/kg normal saline bolus Intervention 2: 20ml/kg albumin bolus Control: no bolus Note all groups received maintenance fluids Excluded hypovolaemic conditions i.e gastroenteritis
20 Results Increased mortality in the fluid bolus group Increased RR mortality = 45% Albumin Saline Control 48hr 10.6% 10.5% 7.3% 4 week 12.2% 12.0% 8.7&
21
22 Sub-groups Results were consistent across every single subgroup including Severity of shock Presence of malaria or anaemia Coma Type of sepsis Acidosis Lactate level = LIKELY REAL FINDING
23 Criticismsà Refuted High malaria prevalence (57%) à Same findings with and without malaria High anaemia prevalence à Same findings with and without anaemia Clinical measures of shock may have overestimated the children with septic shock à Most severe shock cases had the greatest harm from fluid boluses: 10% v 3% mortality
24 Criticisms à Refuted No 1 st world ICU care à ICU care may have masked fluid harms but is no reason not to prevent the harm in the first place Could be an effect of saline in N/S and albumin à possible though see re-analysis In kids not adults à perhaps relevant if death by fluid overload see re-analysis
25 Re-analysis of FEAST Exploring mechanisms of excess mortality with early fluid resuscitation: insights from the FEAST trial Maitland et al, BMC Medicine 2013 Causes of death after fluid bolus resuscitation: new insights from FEAST Myburgh & Finfer, BMC Medicine 2013
26 Criticisms Refuted: Reanalysis Cause of death was not fluid overload! Cause of death that increased in the bolus group = cardiovascular collapse! This was despite the bolus group having an initial improvement in haemodynamics Doctors were shocked by the results Our anecdotal experience is no longer reassuring
27 Proposed mechanisms of harm from fluids Cardiovascular collapse Undermining sympathetic compensation Reperfusion injury Injury to the Endothelial Glycocalyx (EG) Shear forces on EG Atrial stretch releasing ANP and BNP which damage EG harm Net result is increasing vasodilation and capillary permeability à cardiovascular collapse chasing our tail with additional fluids
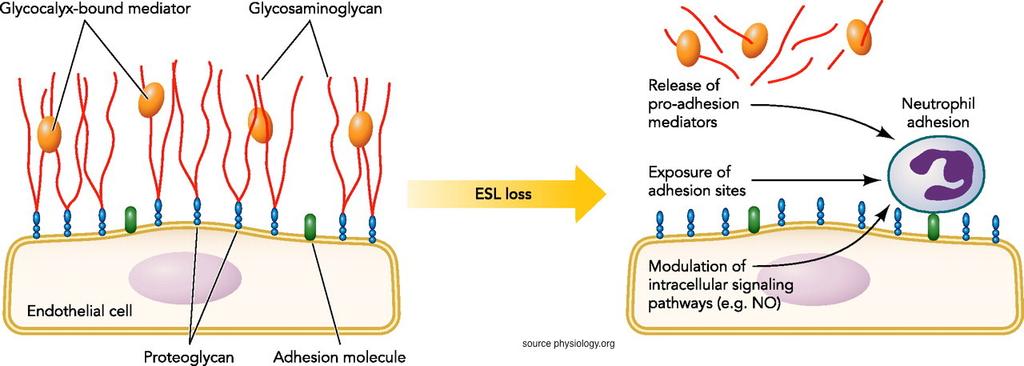
28 Endothelial Glycocalyx
29 Balance of fluid resus evidence? FOR: 1 observational study (10 pts per arm) + Rivers EGDT (260 pts) Vs AGAINST: PROMISE & ARISE debunking EGDT (3000 pts) Several observational studies (3000 pts) + 1 animal RCT (48 pigs) + 1 human RCT (3000 pts)
30 Resuscitation End Points in 1. Adequate MAP? 65mmHg Sepsis 2. Adequate tissue perfusion Relatively normal CR (<4 sec) Peripheral warmth Absence of skin mottling Lactate <2 Urine output > 0.5ml/kg/hr Assuming these targets are worthy endpoints: the journey may be as important as the destination
31 Choice of journey Aggressive fluid resus followed by late use of noradrenaline OR Conservative fluid resuscitation combined with early use of noradrenaline
32 Treatment of vasodilatory shock Anaphylaxis: Adrenaline, Adrenaline, Adrenaline Sepsis: Fluids, Fluids, Fluids then not in pulmonary oedema? give some more fluids then norad
33 Why don t we currently use noradrenaline early? 1. Requires a central line à Wrong Ricard et al, Critical Care Medicine 2013 Used up to 33mcg/min of vasopressors peripherally 2. Commits patients to an ICU/HDU à Excellent! 3. Could it be harmful?
34 Noradrenaline in septic shock Bellomo, Critical Care 2001 Hamzoui Critical Care 2007 Hamzoui Critical Care 2010 Perishini Critical Care Medicine, 2012
35 Hamzoui, Critical Care 2010 Observational study re early admin of norad 105 patients admitted to ICU for less than 6 hours ½ had norad started already à increased. Other ½ had norad started Median volume fluid administered prior was only 1L ( L)
36 Hamzoui, Critical Care 2010 Results: Early administration of norad increases preload, contractility and CO Finding was true regardless of LVEF unless: Patients had LVEF < 45% AND MAP > 75mmHg Who said you need to fill the tank before you tense it?
37 Noradrenaline Summary In hypotensive vasodilated septic shock patients noradrenaline increases: Preload CO Renal blood flow and function When MAP increases beyond 75mmHg this may not be the case in patients with poor LEVF
38 Date of download: 8/28/2014 Copyright American College of Chest Physicians. All rights reserved. From: Early Management of Severe SepsisManagement of Sepsis: Concepts and Controversies Chest. 2014;145(6): doi: /chest Figure Legend: Suggested initial approach to the management of patients with severe sepsis and septic shock. CI = cardiac index; ECHO = echocardiography; inc = increase; LR = Lactated Ringers solution; LV = left ventricle; MAP = mean arterial pressure; Max = maximal; PCT = procalcitonin; PLR = passive leg raising; SV = stroke volume.


39
40 Fluids in ARISE ARISE gave 1960ml v 1710ml of fluid in EGDT v Controls in 1 st 6 hours Mortality rate = 19%
41 Take Home Messages 1. Target MAP and tissue perfusion goals but the journey maybe as important as the destination Our focus on short term haemodynamics may be misguided and misleading 2. Rapid fluid boluses and high cumulative volumes may increase mortality in septic shock Consider using smaller volumes/rates than usual practice 3. Consider early use of low dose noradrenaline (eg via good quality peripheral IVC)
42 Acknowledgements Prof John Myburgh Emcrit.org (Dr Scott Weingart) Dr Paul Marik
43 Emergucate.com Talk is posted here with references
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
towards early goal directed therapy
 Paediatric Septic Shock- towards early goal directed therapy Elliot Long Paediatric Acute Care 2011 Conference Outline Emergency Department Rivers Protocol (EGDT) ACCM Sepsis Protocol Evidence Barriers
Paediatric Septic Shock- towards early goal directed therapy Elliot Long Paediatric Acute Care 2011 Conference Outline Emergency Department Rivers Protocol (EGDT) ACCM Sepsis Protocol Evidence Barriers
EARLY GOAL DIRECTED THERAPY : seminaires iris. Etat des lieux en Daniel De Backer
 EARLY GOAL DIRECTED THERAPY : Etat des lieux en 2017 Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past-President European
EARLY GOAL DIRECTED THERAPY : Etat des lieux en 2017 Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past-President European
IV fluid administration in sepsis. Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London
 IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
Tailored Volume Resuscitation in the Critically Ill is Achievable. Objectives. Clinical Case 2/16/2018
 Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Sepsis care and the new core measures
 Sepsis care and the new core measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Sepsis care and the new core measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Sepsis Care and the New Core Measures. Daniel S. Hagg, MD January 15, 2016
 Sepsis Care and the New Core Measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Sepsis Care and the New Core Measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Sepsis Management Update 2014
 Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
SEPSIS: Seeing Through the. W. Graham Carlos MD, MSCR, ATSF, FACP
 SEPSIS: Seeing Through the W. Graham Carlos MD, MSCR, ATSF, FACP Objectives Forget everything you have known about sepsis Learn new things Objectives Define sepsis Explain why Early Goal Directed Therapy
SEPSIS: Seeing Through the W. Graham Carlos MD, MSCR, ATSF, FACP Objectives Forget everything you have known about sepsis Learn new things Objectives Define sepsis Explain why Early Goal Directed Therapy
Radboud University Nijmegen Medical Centre Why measure cardiac output in critically ill children?
 Radboud University Nijmegen Medical Centre Why measure cardiac output in critically ill children? J. Lemson Anesthesiologist/(pediatric)intensivist Case; Girl 2 years, 12 kg, severe meningococcal septic
Radboud University Nijmegen Medical Centre Why measure cardiac output in critically ill children? J. Lemson Anesthesiologist/(pediatric)intensivist Case; Girl 2 years, 12 kg, severe meningococcal septic
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP
 SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
Sepsis Management: Past, Present, and Future
 Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Actualités de la prise en charge hémodynamique initiale Daniel De Backer
 Actualités de la prise en charge hémodynamique initiale Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past- President European
Actualités de la prise en charge hémodynamique initiale Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past- President European
Fluid Treatments in Sepsis: Meta-Analyses
 Fluid Treatments in Sepsis: Recent Trials and Meta-Analyses Lauralyn McIntyre MD, FRCP(C), MSc Scientist, Ottawa Hospital Research Institute Assistant Professor, University of Ottawa Department of Epidemiology
Fluid Treatments in Sepsis: Recent Trials and Meta-Analyses Lauralyn McIntyre MD, FRCP(C), MSc Scientist, Ottawa Hospital Research Institute Assistant Professor, University of Ottawa Department of Epidemiology
FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL
 FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL COLLEGE NOVEMBER 10 TH 2017 TEXAS SCCM SYMPOSIUM Disclosures
FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL COLLEGE NOVEMBER 10 TH 2017 TEXAS SCCM SYMPOSIUM Disclosures
INTENSIVE CARE MEDICINE CPD EVENING. Dr Alastair Morgan Wednesday 13 th September 2017
 INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us?
 Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us? Mitchell M. Levy MD, FCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School
Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us? Mitchell M. Levy MD, FCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School
Sepsis Update: Focus on Early Recognition and Intervention. Disclosures
 Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
3/14/2017. Disclosures. None. Outline. Fluid Management and Hemodynamic Assessment Paul Marik, MD, FCCP, FCCM
 Fluid Management and Hemodynamic Assessment Paul Marik, MD, FCCP, FCCM Disclosures Stocks Advisory boards Grants Speakers Bureau None Outline Hemodynamic Goals Fluid Resuscitation Historical Perspective
Fluid Management and Hemodynamic Assessment Paul Marik, MD, FCCP, FCCM Disclosures Stocks Advisory boards Grants Speakers Bureau None Outline Hemodynamic Goals Fluid Resuscitation Historical Perspective
Presented by: Indah Dwi Pratiwi
 Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Fluid responsiveness and extravascular lung water
 Fluid responsiveness and extravascular lung water Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Conflicts of interest Member of the Medical Advisory Board of Maquet/Pulsion
Fluid responsiveness and extravascular lung water Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Conflicts of interest Member of the Medical Advisory Board of Maquet/Pulsion
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI)
") Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
Surviving Sepsis Campaign Guidelines 2012 & Update for David E. Tannehill, DO Critical Care Medicine Mercy Hospital St.
 Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Objectives. Epidemiology of Sepsis. Review Guidelines for Resuscitation. Tx: EGDT, timing/choice of abx, activated
 Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL
 resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL") Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL 65 Male, 60 kg D1 in ICU Admitted from OT intubated Diagnosis : septic shock secondary to necrotising fasciitis of the R lower limb
Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL 65 Male, 60 kg D1 in ICU Admitted from OT intubated Diagnosis : septic shock secondary to necrotising fasciitis of the R lower limb
What is the Role of Albumin in Sepsis? An Evidenced Based Affair. Justin Belsky MD PGY3 2/6/14
 What is the Role of Albumin in Sepsis? An Evidenced Based Affair Justin Belsky MD PGY3 2/6/14 Microcirculation https://www.youtube.com/watch?v=xao1gsyur7q Capillary Leak in Sepsis Asking the RIGHT Question
What is the Role of Albumin in Sepsis? An Evidenced Based Affair Justin Belsky MD PGY3 2/6/14 Microcirculation https://www.youtube.com/watch?v=xao1gsyur7q Capillary Leak in Sepsis Asking the RIGHT Question
Wet Lungs Dry lungs Impact on Outcome in ARDS. Charlie Phillips MD Division of PCCM OHSU 2009
 Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
Sepsis. From EMS to ER to ICU. What we need to be doing
 Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Modern fluid therapy. Anders Perner. Dept of Intensive Care, Rigshospitalet, University of Copenhagen
 Modern fluid therapy Anders Perner Dept of Intensive Care, Rigshospitalet, University of Copenhagen Scandinavian Critical Care Trials Group www.ssai.info/research/scctg Intensive Care Medicine www.icmjournal.esicm.org
Modern fluid therapy Anders Perner Dept of Intensive Care, Rigshospitalet, University of Copenhagen Scandinavian Critical Care Trials Group www.ssai.info/research/scctg Intensive Care Medicine www.icmjournal.esicm.org
The Ever Changing World of Sepsis Management. Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital
 The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Nurse Driven Fluid Optimization Using Dynamic Assessments
 Nurse Driven Fluid Optimization Using Dynamic Assessments 2016 1 WHAT WE BELIEVE We believe that clinicians make vital fluid and drug decisions every day with limited and inconclusive information Cheetah
Nurse Driven Fluid Optimization Using Dynamic Assessments 2016 1 WHAT WE BELIEVE We believe that clinicians make vital fluid and drug decisions every day with limited and inconclusive information Cheetah
Fluids in ICU. JMO teaching 5th July 2016
 Fluids in ICU JMO teaching 5th July 2016 Objectives Physiology of fluid infusion History of fluid resuscitation Physiology of fluid resuscitation Types of resuscitation fluid The ideal resuscitation fluid
Fluids in ICU JMO teaching 5th July 2016 Objectives Physiology of fluid infusion History of fluid resuscitation Physiology of fluid resuscitation Types of resuscitation fluid The ideal resuscitation fluid
Fluid resuscitation in specific patient populations: sepsis and traumatic brain injury
 Fluid resuscitation in specific patient populations: sepsis and traumatic brain injury John A Myburgh MBBCh PhD FCICM UNSW Professor of Critical Care Medicine The George Institute for Global Health University
Fluid resuscitation in specific patient populations: sepsis and traumatic brain injury John A Myburgh MBBCh PhD FCICM UNSW Professor of Critical Care Medicine The George Institute for Global Health University
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand
 2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
Case year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50
 Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
Fluid balance and clinically relevant outcomes
 Fluid balance and clinically relevant outcomes Rui Moreno, MD, PhD, Professor UCINC, Hospital de São José Centro Hospitalar de Lisboa Central, E.P.E. INSULT PRIMARY MODS SIRS SECONDARY MODS OUTCOME RECOVERY
Fluid balance and clinically relevant outcomes Rui Moreno, MD, PhD, Professor UCINC, Hospital de São José Centro Hospitalar de Lisboa Central, E.P.E. INSULT PRIMARY MODS SIRS SECONDARY MODS OUTCOME RECOVERY
Managing Patients with Sepsis
 Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
The syndrome formerly known as. Severe Sepsis. James Rooks MD. Coordinator of critical care education OU College of Medicine, Tulsa
 The syndrome formerly known as Severe Sepsis James Rooks MD Coordinator of critical care education OU College of Medicine, Tulsa Disclosures I have no actual or practical conflicts of interest in relation
The syndrome formerly known as Severe Sepsis James Rooks MD Coordinator of critical care education OU College of Medicine, Tulsa Disclosures I have no actual or practical conflicts of interest in relation
Early Goal-Directed Therapy
 Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Fluid Resuscitation and Monitoring in Sepsis. Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS
 Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
JOURNAL CLUB: THE FLUIDS DEBATE. Veronica Ueckermann
 JOURNAL CLUB: THE FLUIDS DEBATE Veronica Ueckermann INTRODUCTION The selection and use of resuscitation fluids should be based on physiological principles. However, historically, clinical practice has
JOURNAL CLUB: THE FLUIDS DEBATE Veronica Ueckermann INTRODUCTION The selection and use of resuscitation fluids should be based on physiological principles. However, historically, clinical practice has
Sepsis Learning Collaborative: Evidence-based Approaches to Sepsis Resuscitation Sepsis Resuscitation in Medically Complex Patients
 Sepsis Learning Collaborative: Evidence-based Approaches to Sepsis Resuscitation Sepsis Resuscitation in Medically Complex Patients Presenters Dr. Nathan Shapiro Dr. Laurence Dubensky Evidence Based Approaches
Sepsis Learning Collaborative: Evidence-based Approaches to Sepsis Resuscitation Sepsis Resuscitation in Medically Complex Patients Presenters Dr. Nathan Shapiro Dr. Laurence Dubensky Evidence Based Approaches
Full Disclosure. The case for why it matters. Goal-directed Fluid Resuscitation
 Goal-directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco I own no stocks Full Disclosure The case for why
Goal-directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco I own no stocks Full Disclosure The case for why
Vasopressors for shock
 Vasopressors for shock Background Reviews and Observational Studies Holler 2015. Nontraumatic Hypotension and Shock in the Emergency Department and Prehospital Setting Prevalence, Etiology and Mortality:
Vasopressors for shock Background Reviews and Observational Studies Holler 2015. Nontraumatic Hypotension and Shock in the Emergency Department and Prehospital Setting Prevalence, Etiology and Mortality:
Nothing to disclose 9/25/2017
 Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Goal-directed vs Flow-guidedresponsive
 Goal-directed vs Flow-guidedresponsive therapy S Magder Department of Critical Care, McGill University Health Centre Flow-directed vs goal directed strategy for management of hemodynamics S Magder Curr
Goal-directed vs Flow-guidedresponsive therapy S Magder Department of Critical Care, McGill University Health Centre Flow-directed vs goal directed strategy for management of hemodynamics S Magder Curr
9/25/2017. Nothing to disclose
 Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill
 Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Vasopressors in septic shock
 Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia (Spain) Pulsion MAB
 Pulsion MAB") State of the Art Hemodynamic Monitoring III CO, preload, lung water and ScvO2 The winning combination! Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia
State of the Art Hemodynamic Monitoring III CO, preload, lung water and ScvO2 The winning combination! Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia
Sepsis is an important issue. Clinician s decision-making capability. Guideline recommendations
 Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Rationale for renal replacement therapy in ICU: indications, approaches and outcomes. Richard Beale
 Rationale for renal replacement therapy in ICU: indications, approaches and outcomes Richard Beale RIFLE classification (ADQI group) 2004 Outcome AKIN classification Definition: Abrupt (within 48 hrs)
Rationale for renal replacement therapy in ICU: indications, approaches and outcomes Richard Beale RIFLE classification (ADQI group) 2004 Outcome AKIN classification Definition: Abrupt (within 48 hrs)
Jarisch A. Kreislauffragen, Dünser et al. Critical Care 2013, 17:326 Sunday, March 30, 14
 It was fatal for the development of our understanding of circulation that blood flow is relatively difficult while blood pressure so easy to measure: This is the reason why the sphygmomanometer has gained
It was fatal for the development of our understanding of circulation that blood flow is relatively difficult while blood pressure so easy to measure: This is the reason why the sphygmomanometer has gained
Septic AKI in ICU patients
 Septic AKI in ICU patients Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum Berlin, Germany achim.joerres@charite.de Agenda Epidemiology
Septic AKI in ICU patients Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum Berlin, Germany achim.joerres@charite.de Agenda Epidemiology
Goal-directed resuscitation in sepsis; a case-based approach
 Goal-directed resuscitation in sepsis; a case-based approach Jorge A Guzman, MD, FCCM Head, Section Critical Care Medicine Respiratory Institute Cleveland Clinic Foundation The challenges to managing septic
Goal-directed resuscitation in sepsis; a case-based approach Jorge A Guzman, MD, FCCM Head, Section Critical Care Medicine Respiratory Institute Cleveland Clinic Foundation The challenges to managing septic
Prof. Dr. Iman Riad Mohamed Abdel Aal
 The Use of New Ultrasound Indices to Evaluate Volume Status and Fluid Responsiveness in Septic Shock Patients Thesis Submitted for partial fulfillment of MD degree in Anesthesiology, Surgical Intensive
The Use of New Ultrasound Indices to Evaluate Volume Status and Fluid Responsiveness in Septic Shock Patients Thesis Submitted for partial fulfillment of MD degree in Anesthesiology, Surgical Intensive
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014
 December 17, 2014") Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Early-goal-directed therapy and protocolised treatment in septic shock
 CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
Vasopressors in Septic Shock. Keith R. Walley, MD St. Paul s Hospital University of British Columbia Vancouver, Canada
 Vasopressors in Septic Shock Keith R. Walley, MD St. Paul s Hospital University of British Columbia Vancouver, Canada Echocardiogram: EF=25% 57 y.o. female, pneumonia, shock Echocardiogram: EF=25% 57 y.o.
Vasopressors in Septic Shock Keith R. Walley, MD St. Paul s Hospital University of British Columbia Vancouver, Canada Echocardiogram: EF=25% 57 y.o. female, pneumonia, shock Echocardiogram: EF=25% 57 y.o.
Impact of Fluids in Children with Acute Lung Injury
 Impact of Fluids in Children with Acute Lung Injury Canadian Critical Care Forum Toronto, Canada October 27 th, 2015 Adrienne G. Randolph, MD, MSc Critical Care Division, Department of Anesthesia, Perioperative
Impact of Fluids in Children with Acute Lung Injury Canadian Critical Care Forum Toronto, Canada October 27 th, 2015 Adrienne G. Randolph, MD, MSc Critical Care Division, Department of Anesthesia, Perioperative
Obligatory joke. The case for why it matters. Sepsis: More is more. Goal-Directed Fluid Resuscitation 6/1/2013
 Obligatory joke Keep your eye on the food. Goal-Directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco The
Obligatory joke Keep your eye on the food. Goal-Directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco The
UTILITY of ScvO 2 and LACTATE
 UTILITY of ScvO 2 and LACTATE Professor Jeffrey Lipman Department of Intensive Care Medicine Royal Brisbane Hospital University of Queensland THIS TRIP SPONSORED AND PAID FOR BY STRUCTURE Physiology -
UTILITY of ScvO 2 and LACTATE Professor Jeffrey Lipman Department of Intensive Care Medicine Royal Brisbane Hospital University of Queensland THIS TRIP SPONSORED AND PAID FOR BY STRUCTURE Physiology -
Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency
 Application of ICG in Intensive Care and Emergency") Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency Aim of haemodynamic monitoring in ICU and ED Detection and therapy of insufficient organ perfusion Answers to common cardiovascular
Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency Aim of haemodynamic monitoring in ICU and ED Detection and therapy of insufficient organ perfusion Answers to common cardiovascular
OHSU. Update in Sepsis
 Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Evidence- Based Medicine Fluid Therapy
 Evidence- Based Medicine Fluid Therapy Ndidi Musa M.D. Assosciate Professor of Pediatrics Medical College of Wisconsin/ Children s Hospital of Wisconsin Disclosures A. I have no relevant financial relationships
Evidence- Based Medicine Fluid Therapy Ndidi Musa M.D. Assosciate Professor of Pediatrics Medical College of Wisconsin/ Children s Hospital of Wisconsin Disclosures A. I have no relevant financial relationships
Updates in Sepsis 2017
 Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Where did it all begin?
 EXPLORE Healthcare Summit Sepsis: Can We Finally Just Relax on the SOFA? Mark Keuchel, D.O. Background: 1. Sepsis is a wide-spectrum disease process that remains poorly understood 2. Early-goal directed
EXPLORE Healthcare Summit Sepsis: Can We Finally Just Relax on the SOFA? Mark Keuchel, D.O. Background: 1. Sepsis is a wide-spectrum disease process that remains poorly understood 2. Early-goal directed
Purist? or Pragmatist? Assessment & Management of ICU Volume Status
 Assessment & Management of ICU Volume Status 9 th Annual Rocky Mountain Hospital Medicine Symposium Denver, Colorado Paula Dennen, MD Assistant Professor of Medicine Nephrology and Critical Care Medicine
Assessment & Management of ICU Volume Status 9 th Annual Rocky Mountain Hospital Medicine Symposium Denver, Colorado Paula Dennen, MD Assistant Professor of Medicine Nephrology and Critical Care Medicine
Sepsis and septic shock Practical hemodynamic consequences. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 Sepsis and septic shock Practical hemodynamic consequences Intensive Care Training Program Radboud University Medical Centre Nijmegen Septic cardiomyopathy Present in > 50% and often masked by low vascular
Sepsis and septic shock Practical hemodynamic consequences Intensive Care Training Program Radboud University Medical Centre Nijmegen Septic cardiomyopathy Present in > 50% and often masked by low vascular
How and why I give IV fluid Disclosures SCA Fluids and public health 4/1/15. Andrew Shaw MB FRCA FCCM FFICM
 How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
9/13/2015. Laboratory. HPI and PE
 Critical Care HPI and PE 74 yo male confused SBP 90/20 MAP50, P 122, RR 34 Ox1 w/o nuchal rigidity S1S2 wo m RLL reduced breath sounds Skin warm dry Laboratory» WBC 15,600 Hgb 8.4 HCt 23%, Plts 95000,
Critical Care HPI and PE 74 yo male confused SBP 90/20 MAP50, P 122, RR 34 Ox1 w/o nuchal rigidity S1S2 wo m RLL reduced breath sounds Skin warm dry Laboratory» WBC 15,600 Hgb 8.4 HCt 23%, Plts 95000,
IN THE NAME OF GOD SHOCK MANAGMENT OMID MORADI MOGHADDAM,MD,FCCM IUMS ASSISTANT PROFESSOR
 IN THE NAME OF GOD SHOCK MANAGMENT OMID MORADI MOGHADDAM,MD,FCCM IUMS ASSISTANT PROFESSOR The ability to evaluate and manage a critically ill patient is one of the most important skills any intensivist
IN THE NAME OF GOD SHOCK MANAGMENT OMID MORADI MOGHADDAM,MD,FCCM IUMS ASSISTANT PROFESSOR The ability to evaluate and manage a critically ill patient is one of the most important skills any intensivist
What is the right fluid to use?
 What is the right fluid to use? L McIntyre Associate Professor, University of Ottawa Senior Scientist, Ottawa Hospital Research Institute Centre for Transfusion Research CCCF, November 2, 2016 Disclosures
What is the right fluid to use? L McIntyre Associate Professor, University of Ottawa Senior Scientist, Ottawa Hospital Research Institute Centre for Transfusion Research CCCF, November 2, 2016 Disclosures
Sepsis or Severe Sepsis? Is there a right thing, and how do we do it?
 Sepsis or Severe Sepsis? Is there a right thing, and how do we do it? Steven Q Simpson, MD, FCCP, FACP Professor of Medicine Division of Pulmonary and Critical Care University of Kansas Disclosures No
Sepsis or Severe Sepsis? Is there a right thing, and how do we do it? Steven Q Simpson, MD, FCCP, FACP Professor of Medicine Division of Pulmonary and Critical Care University of Kansas Disclosures No
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
SEPSIS SYNDROME
 INTRODUCTION Sepsis has been defined as a life threatening condition that arises when the body s response to an infection injures its own tissues and organs. Sepsis may lead to shock, multiple organ failure
INTRODUCTION Sepsis has been defined as a life threatening condition that arises when the body s response to an infection injures its own tissues and organs. Sepsis may lead to shock, multiple organ failure
Pediatric Sepsis Treatment:
 Disclosures Pediatric Sepsis Treatment: (treat) Early & (reevaluate) Often None June 11, 2018 Leslie Dervan, MD MS Pacific Northwest Sepsis Conference 1 Agenda Sepsis: pathophysiology at-a-glance Pediatric
Disclosures Pediatric Sepsis Treatment: (treat) Early & (reevaluate) Often None June 11, 2018 Leslie Dervan, MD MS Pacific Northwest Sepsis Conference 1 Agenda Sepsis: pathophysiology at-a-glance Pediatric
Cardiovascular Management of Septic Shock
 Cardiovascular Management of Septic Shock R. Phillip Dellinger, MD Professor of Medicine Robert Wood Johnson Medical School/UMDNJ Director, Critical Care Medicine and Med/Surg ICU Cooper University Hospital
Cardiovascular Management of Septic Shock R. Phillip Dellinger, MD Professor of Medicine Robert Wood Johnson Medical School/UMDNJ Director, Critical Care Medicine and Med/Surg ICU Cooper University Hospital
L : Line and Tube อ นตรายป องก นได จากการให สารน า
 L : Line and Tube อ นตรายป องก นได จากการให สารน า รศ.นพ.กว ศ กด จ ตตว ฒนร ตน ภาคว ชาศ ลยศาสตร คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม 3 rd Mini Conference: ความปลอดภ ยในผ ป วย ร วมด วย ช วยได ท กคน ว นท 13-14
L : Line and Tube อ นตรายป องก นได จากการให สารน า รศ.นพ.กว ศ กด จ ตตว ฒนร ตน ภาคว ชาศ ลยศาสตร คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม 3 rd Mini Conference: ความปลอดภ ยในผ ป วย ร วมด วย ช วยได ท กคน ว นท 13-14
FLUIDS AND SOLUTIONS IN THE CRITICALLY ILL. Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium
 FLUIDS AND SOLUTIONS IN THE CRITICALLY ILL Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium Why do we want to administer fluids? To correct hypovolemia? To increase
FLUIDS AND SOLUTIONS IN THE CRITICALLY ILL Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium Why do we want to administer fluids? To correct hypovolemia? To increase
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Actualités sur le remplissage peropératoire. Philippe Van der Linden MD, PhD
 Actualités sur le remplissage peropératoire Philippe Van der Linden MD, PhD Fees for lectures, advisory board and consultancy: Fresenius Kabi GmbH B Braun Medical SA Perioperative Fluid Volume Administration
Actualités sur le remplissage peropératoire Philippe Van der Linden MD, PhD Fees for lectures, advisory board and consultancy: Fresenius Kabi GmbH B Braun Medical SA Perioperative Fluid Volume Administration
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Core Measures SEPSIS UPDATES
 Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Hemodynamic monitoring beyond cardiac output
 Hemodynamic monitoring beyond cardiac output Prof Xavier MONNET Medical Intensive Care Unit Bicêtre Hospital Assistance publique Hôpitaux de Paris FRANCE Conflicts of interest Lilly GlaxoSmithKline Pulsion
Hemodynamic monitoring beyond cardiac output Prof Xavier MONNET Medical Intensive Care Unit Bicêtre Hospital Assistance publique Hôpitaux de Paris FRANCE Conflicts of interest Lilly GlaxoSmithKline Pulsion
Sepsis and septic shock: can we win the battle against this hidden crisis?
 REVIEW ARTICLE Sepsis and septic shock: can we win the battle against this hidden crisis? V.G. Dassanayake Department of Surgery, Faculty of Medicine, University of Colombo, Sri Lanka Key words : Sepsis;
REVIEW ARTICLE Sepsis and septic shock: can we win the battle against this hidden crisis? V.G. Dassanayake Department of Surgery, Faculty of Medicine, University of Colombo, Sri Lanka Key words : Sepsis;
JAMA. 2016;315(8): doi: /jama
: doi: /jama") JAMA. 2016;315(8):801-810. doi:10.1001/jama.2016.0287 SEPSIS 3 life-threatening organ dysfunction caused by a dysregulated host response to infection organ dysfunction: an increase in the SOFA
JAMA. 2016;315(8):801-810. doi:10.1001/jama.2016.0287 SEPSIS 3 life-threatening organ dysfunction caused by a dysregulated host response to infection organ dysfunction: an increase in the SOFA
4/5/2018. Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY. I have no financial disclosures
 Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
6/5/2014. Sepsis Management and Hemodynamics. 2004: International group of experts,
 Sepsis Management and Hemodynamics Javier Perez-Fernandez, M.D., F.C.C.P. Medical Director Critical Care Services, Baptist t Hospital of Miamii Medical Director Pulmonary Services, West Kendall Baptist
Sepsis Management and Hemodynamics Javier Perez-Fernandez, M.D., F.C.C.P. Medical Director Critical Care Services, Baptist t Hospital of Miamii Medical Director Pulmonary Services, West Kendall Baptist
Practical. Septic shock resuscitation ไชยร ตน เพ มพ ก ล พบ. ภาคว ชาอาย รศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล
 Practical Septic shock resuscitation ไ ไชยร ตน เพ มพ ก ล พบ. ภาคว ชาอาย รศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล ประช มว ชาการ 101 ป อาย รศาสตร ศ ร ราช 6 ก มภาพ นธ 2561 Early recognition Early resuscitation Early
Practical Septic shock resuscitation ไ ไชยร ตน เพ มพ ก ล พบ. ภาคว ชาอาย รศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล ประช มว ชาการ 101 ป อาย รศาสตร ศ ร ราช 6 ก มภาพ นธ 2561 Early recognition Early resuscitation Early
Sepsis & Beyond Guidelines & Goal-Directed Therapy
 Sepsis & Beyond Guidelines & Goal-Directed Therapy Canadian Association of Critical Care Nurses 2014 Quebec City Presented by: Nicole Kupchik RN, MN, CCNS, CCRN, PCCN Objectives Review the 2012 Surviving
Sepsis & Beyond Guidelines & Goal-Directed Therapy Canadian Association of Critical Care Nurses 2014 Quebec City Presented by: Nicole Kupchik RN, MN, CCNS, CCRN, PCCN Objectives Review the 2012 Surviving
Sepsis Story At Intermountain Healthcare Intensive Medicine Clinical Program
 Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Top Sepsis Studies
 A75M233/A75M529 Monday 08:00-09:15 Wednesday 14:45-16:00 Maureen A Seckel APRN, ACNS-BC, CCRN, CCNS, FCCM Critical Care CNS and Sepsis Leader Christiana Care Health Services, Newark, DE Top Sepsis Studies
A75M233/A75M529 Monday 08:00-09:15 Wednesday 14:45-16:00 Maureen A Seckel APRN, ACNS-BC, CCRN, CCNS, FCCM Critical Care CNS and Sepsis Leader Christiana Care Health Services, Newark, DE Top Sepsis Studies