Dengue Case Discussion. When things can go wrong!
|
|
|
- Nathaniel Cook
- 5 years ago
- Views:
Transcription
1 Dengue Case Discussion When things can go wrong!
2 What the local experts say! 99.99% of walked in patients who come to hospital with dengue should walk out from hospital! Even those who come in Shock but without Prolonged Shock should have >99% survival Except very RARELY a walked in dengue patient should not need an ICU bed or ventilator support Is it a dream!!
3 Case Scenario 1 27 year Undergraduate from Colombo presented with fever, headache, severe bodyaches for 3 days He was asked to get admitted by his GP with a blood report of WBC 2300,PCV 38,Plat 118,000 Weight 68kg He was pyrexial 102⁰F,pulse 100,BP- 120/75 CRFT < 2sec, had good urine output at home
4 Case Scenario 1 What phase of illness Febrile Critical Recovery What is your management pyrexial 102⁰F pulse 100 BP- 120/75 CRFT < 2sec WBC 2300 PCV 38 Plat 118,000
5 Case Scenario 1 What phase of illness Febrile Critical Recovery What is your management
6 Case Scenario 1 Management Temp Chart 3 hourly observation chart Symptomatic management PCM/ No NSAIDs Maintenance fluids? Oral or IV FBC twice daily PCV 6hourly?
7 12/4/15 Epidemiology Unit, Ministry of Health
8 12/4/15 Epidemiology Unit, Ministry of Health UOP ml/hr
9 Case Scenario 1 Family is keen for laboratory confirmation? Dengue NS1 Ag?Dengue Ab IgM/IgG Day 3 pyrexial 102⁰F pulse 100 BP- 120/75 CRFT < 2sec WBC 2300 PCV 38 Plat 118,000
10 Laboratory diagnosis NS1 detection Fever IgM Viraemia IgG- 2ry IgG- 1ry /52 Days
11 Diagnostic options and sensitivity of NS1Ag % sensitivity Day of illness PCR IgM NS1 NS1- detection at admission 1. Sensitivity=67% 2. Specificity=100% 3. Positive predictive value=67% 4. Negative predictive value=75%
12 Immune Response to Dengue Infection Antibody Level Onset of Symptoms Onset of Symptoms IgG IgG Cutoff HAI 1:2560 Virus IgM Virus IgM IgM Cutoff Primary Infection Secondary Infection
13 Case Scenario 1 DAY 2 (Fever Day 4) Dengue NS1 Ag+ Fever continues Bodyaches,anorexia Stable 3 hourly observation FBC WBC ,PCV - 40 Plat- 84,000 On oral/iv maintenance Paracetamol SOS Day 1 pyrexial 102⁰F pulse 96 BP- 120/75 CRFT < 2sec WBC 2300 PCV 38 Plat 118,000
14 Case Scenario 1 Day 3 (Day 5 from onset) Apyrexial since previous evening Feeling faintish, abdominal pain, vomiting Pulse - 90,BP- 100/75,CRFT <2 UOP - 30ml/hr,PCV- 44 What phase of illness? Critical Recovery Day 2 pyrexial pulse 96 BP- 110/75 CRFT < 2sec WBC 3400 PCV 40 Plat 84,000
15 How do you detect onset of critical phase Clinical Hematology Radiology Biochemistry
16 Detection: onset of leakage 1.Clinical Potential leaker- Clinical deterioration when fever is settling Abdominal pain, vomitting Faintish on standing Enlarged tender liver Reduced UOP Confirmed leaker (late sign) Pleural effusions, free fluid in abdomen
17 Timing the onset of critical period- Haematology WBC platelets 260, , , , , , , , ,000 80,000 60,000 40,000 20, th 8 am 18 th 8 am 18 th 8 pm 19 th 8 am 19 th 8 pm 20 th 8 am 20 th 8 pm 21 st 8 am 21 st 8 pm 0
18 Haematocrit/PCV Base line haematocrit is important (if not known- adult male female 35-38) Rise towards 20% above baseline considered significant May be less than 20% - fluids taken in excess or overt bleeding (menstrual bleeding) Suspect when PCV rises > 10% If in shock due to leakage usually 30% rise is expected
19 Platelets- Importance to clinicians When count reaches close to during a febrile illness suspect Dengue When count drops to < start 3 hourly observation chart When count drops to < consider admission Patient usually never leaks > so look for evidence of leakage when it drops Expect leakage if there is a rapid drop of platelets The start of rise in platelets marks the end of peak of leakage
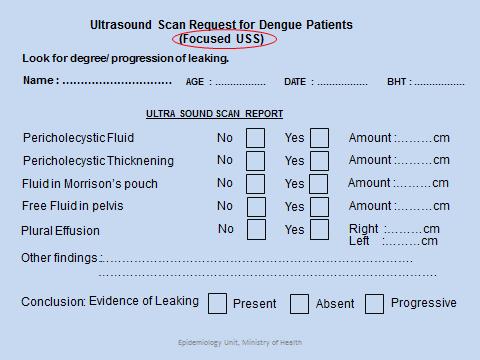
20 Radiological diagnosis Point of care Ultrasound scan Progressive accumulation of fluid in pleural or peritoneal cavities CXR- right lateral decubitus (rarely performed now)

21 R /Lateral decubitus film
22 Point of care sonography Galle bladder wall oedema Pericholycystic fluid Fluid in the pelvis Fluid in hepato renal pouch R /Pleural effusion

23 Point of care sonography Galle bladder wall oedema Pericholycystic fluid Fluid in the pelvis Fluid in hepato renal pouch R /Pleural effusion
24 Interpretation of USS DF D H F GB wall Oedema Pericholecystic fluid Plueral effusion usually unilateral Peritoneal cavity Significant (progressive) effusion Plueral cavity No fluid Peritoneal cavity Little/ no fluid in deep pelvis
25

26
27
28 What strategy to adopt to diagnose the onset of leakage Ward setting Clinical/Haematology/Radiology Emergency Unit Clinical/Radiology/Haematology
29 Case Scenario 1 Blood sent at 8am PCV - 44,Platelets 54,000 US done at 10am Fluid in the Hepato renal pouch What phase of illness? Critical Recovery How do you calculate the onset of leakage
30 How do you define the onset of critical phase Difficult at times! Time from the last fever spike Time when platelets dropped to <100,00 Time from the WBC started to rise Time from you first detected leakage on scan Do not wait for clinical detection of effusion/ascites You may change the onset time later considering the clinical response
31 Management of Critical Phase Where? What monitoring charts needed? What equipment needed?

32
33

34 How good is a multi para monitor Manual BP checks may be subjective Critical phase should be managed relying on a multi para monitor Saves time on the hourly chart Can we provide that facility to all leakers?

35 How often do we need to do PCV? Micro haematocrit centrifuge 3 hourly or more frequently if clinical condition changes
36 Management of Critical Phase Monitoring of hourly urine output needed Do we need an indwelling urinary catheter?
37 Critical Phase Monitoring In Summary Move the patient close to doctors/nurses bay Start Hourly Observation Chart Connect to Multi para monitor Easy access to Micro haematocrit centrifuge Indwelling urinary catheter Above all close vigilance!!
38 LEAKAGE OF PLASMA in DHF 60% UOP

39 Rapid Moderate Slow F 0 Hr 24 Hr 48 Hr 6 Hr 36 Hr C R
40 When plasma leaks Intravascular volume drops Compensatory mechanisms start operating Peripheral vasoconstriction- > diastolic blood pressure goes up- > reduced pulse pressure Sinus tachycardia Urine out put drops (Compensated Shock) Compensation fails Systolic blood pressure drops (Decompensated/Refractory shock)
41 How do you decide the dynamics of leakage Time since onset of critical phase Pulse rate Pulse Pressure PCV CRFT UOP
42 Fluid Management Critical Phase Total fluid (48hrs) 1 st 10 kg 100ml/kg 2 nd 10kg 50ml/kg From 20-50kg 20ml/kg PLUS 5% deficit 50ml/kg max 50kg 65kg adult 4600ml/48hrs Fluids Oral +IV

43 Fluid Management Critical Phase How should we give this volume of fluid? 4600/48 95ml/hr Not at a uniform rate Start with 1.5-3/ml/kg/hr depending on patients clinical status Rate should match the dynamics of leakage
44 Your Treatment Goals Keep systolic blood pressure above 90mmHg Keep pulse rate below 100/min Keep pulse pressure above 30 mmhg Keep UOP above and around 25 ml/hour CRFT<2sec Maintain stable PCV 44
45 Monitoring parameters during Rx 1-24 hours after leakage hours after leakage SBP >90, Pulse <100,UOP >25ml/hr,PP >30,CRFT <2sec,stable PCV Hct bring down if high Narrow Pulse pressure or high PCV may be ignored
46 Case Scenario 1 Critical phase was managed according to National Guidelines Fluid intake was restricted to calculated quota Patient had uneventful critical phase Recovery was heralded by improvement of well being vitals and polyuria Patient was discharged on D6
47 LEARNING POINTS Monitoring during febrile phase Early detection of onset of critical phase Recommended monitoring during critical phase Treatment goals during critical phase
48 Case Scenario 2 34 year male, fever and body aches for 5 days Apyrexial since yesterday feeling faintish vomiting and reduced urine output Examination apyrexial pulse 106,BP- 90/70 CRFT 3,RHC tenderness,?r /Pleural effusion Body weight 65 kg What phase of illness
49 Febrile Phase Critical Phase DHF - I,II,III,IV Fluid Leakage Ascending limb Descending limb Peak (Equilibrium Phase) Recovery Phase Stage of illness
50 Case Scenario 2 Is he in shock Yes compensated shock What is the first bedside test you do/why PCV to define the cause of shock Apyrexial pulse 106 BP- 90/70 CRFT 3 sec What is the next important investigation Point of care Ultrasound
51 Management of Dengue shock Identify shock Look for the cause of shock Leakage - commonest Haemorrhage Leakage with haemorrhage SHOCK is NOT due to MYOCARDITIS!
52 Diagnosis of Dengue Shock Tachycardia >110 Pulse pressure <20 CRFT >2sec ± UOP <25ml/hr Cold peripheries with SBP<90
53 Look for the cause of shock 1. Leakage - commonest 2. Haemorrhage 3. Leakage with haemorrhage
54 LEAKING CAUSING SHOCK 60% UOP
55 BLEEDING CAUSING SHOCK 30% UOP
56 Leaking and Bleeding 40% UOP
57 How do you diagnose the cause of Shock Do bedside PCV Leaking Bleeding Leaking + Bleeding /
58 PCV - 50 Case Scenario 2 Catheterized - only 50cc of residual for last 3 hours Connected to multipara monitor What is your fluid management
59 Rate of IV Fluid in Dengue Shock Syndrome 10 Rate of IV ml/kg/hr ( ml/hr) 5 ml/kg/hr ( ml/hr) 3 ml/kg/hr ( ml/hr) 3-1 ml/kg/hr (40-80 ml/hr) 2 Rate Hours after shock Shock (Rate in adult)
60 Case Scenario 2 500cc of N Saline infused over 1 hour Patients vitals still remain unstable after 1 hr UOP 10ml previous hour What is your next step Repeat PCV 15min after the bolus Apyrexial pulse 106 BP- 90/70 CRFT 3 sec PCV - 50 What is the expected PCV change
61 Expected PCV changes after bolus infusion Crystalloid 10ml/kg drop of 5 Dextran 10ml/kg- drop of 10 Dextran 5ml/kg - drop of 5 Blood 5ml/kg - rise of 5
62 Repeat PCV 52 Case Scenario 2 Patients vitals still unstable What is your next step? Repeat 500ml N saline bolus over 60min Apyrexial pulse 106 BP- 90/70 CRFT 3 sec PCV - 50
63 Case Scenario 2 Pulse 110,BP- 90/70 CRFT 3,UOP- 15ml Repeat PCV 51 What to do next? Apyrexial pulse 106 BP- 90/70 CRFT 3 sec PCV - 52 UOP- 10ml/hr Dextran 500ml bolus
64 COLLOIDS? WHAT & WHEN Dextran 40 is the best Given mainly as 10ml/kg/hr bolus Patients who are in shock and not responding to two boluses of crystalloid Maximum amount is 3 boluses in 24hrs
65 Case Scenario 2 After the dextran patient stabilised pulse - 78,CRFT<2 sec,bp- 105/70,UOP- 50ml Repeat PCV after 15min - 42,Platelets 18,000 What is your next step in fluid management Start crystalloid Apyrexial pulse 106 BP- 90/70 CRFT 3 sec PCV - 51 UOP- 10ml/hr What is the rate of fluid administration Started with 1.5ml/hr
66 Rate of IV Fluid in Dengue Shock Syndrome 10 Rate of IV ml/kg/hr ( ml/hr) 5 ml/kg/hr ( ml/hr) 3 ml/kg/hr ( ml/hr) 3-1 ml/kg/hr (40-80 ml/hr) 2 Rate Hours after shock Shock (Rate in adult)
67 Case scenario 2 Patients vitals after 3 hours pulse - 96, BP 95/70 UOP- 20ml/hr,PCV 46 When a patient is not responding to boluses what else do you need to consider? pulse - 78, CRFT<2 sec, BP- 105/70 UOP- 50ml PCV- 42 ABCS in Dengue
68 Acidosis NOT RESPONDING TO BOLUSES HAEMODYNAMIC INSTABILITY - ABCS Bleeding Calcium Sugar
69 Acidosis Venous gas is recommended Due to profound shock and contributes to DIC Needs early correction When ph <7.35/ HCO3 <15mmol/L NaHCO3 1ml/kg, slow bolus diluted in equal volume of N. saline Refractory acidosis is an indication for blood transfusion
70 Calcium Calcium leaks out with proteins Hypocalcaemia needs be corrected. 10% calcium gluconate 10ml over 10min Given empirically in profound leakers since Calcium levels are not freely available.
71 Case scenario 2 Patients vitals after 3 hours pulse - 96, BP 95/70 UOP- 20ml/hr,PCV 46 No acidosis on VBG Calcium gluconate was given as a slow bolus pulse - 78, CRFT<2 sec, BP- 105/70 UOP- 50ml PCV- 42 What is your fluid management? Fluids stepped up to 5ml/kg/hr for 2 hours and later gradually tailed off from 3ml to 1.5ml/kg/hr
72 Rate of IV Fluid in Dengue Shock Syndrome 10 Rate of IV ml/kg/hr ( ml/hr) 5 ml/kg/hr ( ml/hr) 3 ml/kg/hr ( ml/hr) 3-1 ml/kg/hr (40-80 ml/hr) 2 Rate Hours after shock Shock (Rate in adult)
73 Monitoring parameters during Rx 1-12 hours after shock hours after shock * Hct bring down if high Narrow Pulse pressure or high PCV may be ignored
74 Case Scenario 2 24 hrs after admission Pulse 60,BP - 110/70,PCV - 48,UOP - 30ml/hr Oral maintenance continued Platelets are picking up slowly 6 hrs later vitals remain the same PCV still 48 What phase of illness? What is your management?
75 Plasma leakage : Natural course in severe cases Shock Start Stop Equilibrium Reabsorption hours Plt < 100,000 cells/cumm Hct
76 Management of Equilibrium Phase Latter part or after end of leakage Do not try to correct PCV if the vitals are stable Close monitoring till the patient enters polyuric phase
77 Case Scenario 2 Patients vitals remained stable Patient became polyuric PCV gradually returned to baseline Discharged home 2 days later
78 Learning Points Diagnosis of Dengue shock Defining the cause of shock Management of Dengue shock due to leakage Use of colloids in Dengue ABCS in unstable dengue patients Stepping down the fluid regimen in critical phase Identification of Equilibrium phase in severe disease
79 Case Scenario 3 33 year old mother of 2 presented with a history of fever for 5 days,apyrexial since morning.she complaints of vomiting faintishness and reduced urine output. On examination she is apyrexial pulse BP- 98/70,CRFT 2sec Capillary PCV - 38, POC Ultrasound thin rim of fluid in Morrisons pouch with small R/Pleural effusion,little volume of residual urine in bladder.
80 What phase of illness Case Scenario 3 Critical phase What is the probable onset time of critical phase What is your fluid management Apyrexial 12hr Pulse BP- 98/70 CRFT 2sec PCV - 38 Leakage + 3ml/kg given for 2 hours
81 Case Scenario 3 after 2hrs What complication has occured Dengue shock What is the cause of shock Leakage/Bleeding Leakage + Bleeding Pulse 110 PCV 38 BP - 90/70 UOP- 10ml/hr What is your management Blood 5ml/kg
82 Leakage and bleeding 40% UOP
83 Case Scenario 3 Patients vitals improved marginally but a repeat 5ml/kg transfusion was given since the PCV didn t rise as expected With that the patient stabilised and the PCV and vitals remained stable Patient had uneventful recovery phase with adequate diuresis
84 Learning Points When to suspect concealed bleeding in dengue Leaking and bleeding can coexist in latter half of leakage If a patient is in shock PCV will help to define the aetiology
85 Case Scenario 4 18 year old schoolboy was transferred from a regional base hospital with worsening shortness of breath during management of the critical phase of dengue His weight is 56kg and has had 4800 ml of fluid into 40hrs of critical phase
86 Case Scenario 4 On arrival he has puffy eye lids RR - 36,Sat - 88% on room air pulse 112,CRFT >2 sec,bp- 90/70 clinical evidence of moderate R/ Pleural effusion UOP - 40ml for last 2 hours Inward PCV - 48 POC ultrasound confirms moderate pleural effusion and ascites
87 Case Scenario 4 What stage of illness Critical phase What complication/s has occurred Shock due to leakage Fluid Overload RR - 36, Sat - 88% Pulse 112 CRFT >2 sec BP- 90/70 UOP Mod effusion PCV- 48
88 Case Scenario 4 What is your fluid management Crystalloid/Colloid Colloid alone/colloid with frusemide Problems Fluid overload Fluid quota already finished Shock due to leakage
89 Fluid Overload in Dengue Usually second half/latter phase of leakage Only in profound leakers Excessive fluids during leakage Can be seen even with excessive oral intake Puffy eye lids, tacypnoea, tachycardia,low UOP Important to diagnose correctly
90 Case Scenario 4 Patient was given 250 ml Dextran within 30 minutes and Frusemide 10mg given midway Patient had a diuresis of 600 ml which relieved the respiratory distress PCV dropped to 44 from 48 Pulse - 96,BP - 100/70,RR- 26,Sat - 94%
91 Case Scenario 4 Patient had clinical evidence of pulmonary oedema PCV remained stable around 36 Patient was given 2 further doses of Frusemide 10mg 6 hrs apart Patient had good diuretic response and uncomplicated recovery phase
92 HALF BOLUS OF DEXTRAN 40 5ml/kg DEXTRAN 40 given over 30 minutes In practice the most useful and the commonest way of using Dextran Rising PCV where fluid quota is nearing completion In the descending limb of leakage/evidence of overloading given with Frusemide
93 Fluid over loaded patients UNSTABLE If in shock with High PCV 10ml/kg Dextran bolus over 1 hr with Frusemide 0.5mg/kg midway If in shock with Low PCV Blood transfusion with Frusemide midway STABLE If stable with High PCV Restrict fluids and observe If stable with Low PCV Restrict fluids & IV Frusemide 0.5mg/kg bolus check PCV after 1 hr
94 Learning Points Diagnosis of fluid overload in dengue Management of unstable fluid overload Management of stable fluid overload Clincal use of half Dextran with or without frusemide
95 What the local experts say! 99.99% of walked in patients who come to hospital with dengue should walk out from hospital! Even those who come in Shock but without Prolonged Shock should have >99% survival Except very RARELY a walked in dengue patient should not need an ICU bed or ventilator support It is achievable!!
Dengue Fever & Dengue Shock Syndrome. 07-May-18 PLES / SLCP 1
 Dengue Fever & Dengue Shock Syndrome 07-May-18 PLES / SLCP 1 Objectives Early diagnosis Pathophysiology of DHF Proper management How to avoid complications Case 07-May-18 PLES / SLCP 2 Febrile Phase High
Dengue Fever & Dengue Shock Syndrome 07-May-18 PLES / SLCP 1 Objectives Early diagnosis Pathophysiology of DHF Proper management How to avoid complications Case 07-May-18 PLES / SLCP 2 Febrile Phase High
MANAGEMENT OF DENGUE INFECTION IN ADULTS (Revised 2 nd Edition) QUICK REFERENCE FOR HEALTHCARE PROVIDERS
 QUICK REFERENCE FOR HEALTHCARE PROVIDERS") 1 KEY MESSAGES Dengue is a dynamic disease and presented in three phases - febrile phase, critical phase and recovery phase. Clinical deterioration often occurs in the critical phase and is marked by plasma
1 KEY MESSAGES Dengue is a dynamic disease and presented in three phases - febrile phase, critical phase and recovery phase. Clinical deterioration often occurs in the critical phase and is marked by plasma
1. Dengue An Overview. Dengue Expert Advisory Group
 1. Dengue An Overview Dengue Expert Advisory Group 1 Introduction Dengue Fever Dengue Hemorrhagic Fever Dengue Shock Syndrome 2 3 Dengue Virus Family : Flaviviridae Genus : Flavivirus Serotypes : DV1,
1. Dengue An Overview Dengue Expert Advisory Group 1 Introduction Dengue Fever Dengue Hemorrhagic Fever Dengue Shock Syndrome 2 3 Dengue Virus Family : Flaviviridae Genus : Flavivirus Serotypes : DV1,
KEY MESSAGES. There are three phases in dengue infection-febrile phase, critical phase and recovery (reabsorption) phase.
 phase.") MANAGEMENT OF DENGUE INFECTION IN ADULTS (2 nd Edition) QUICK REFERENCE FOR HEALTH CARE PROVIDERS KEY MESSAGES Dengue is a systemic and dynamic disease. There are three phases in dengue infection-febrile
MANAGEMENT OF DENGUE INFECTION IN ADULTS (2 nd Edition) QUICK REFERENCE FOR HEALTH CARE PROVIDERS KEY MESSAGES Dengue is a systemic and dynamic disease. There are three phases in dengue infection-febrile
Fluid Management in Dengue Fever and Dengue Haemorrhagic Fever
 Fluid Management in Dengue Fever and Dengue Haemorrhagic Fever Dengue infection Dr. A LakKumar Fernando, Consultant Paediatrician Dengue is a disease which is silently transmitted in the community. For
Fluid Management in Dengue Fever and Dengue Haemorrhagic Fever Dengue infection Dr. A LakKumar Fernando, Consultant Paediatrician Dengue is a disease which is silently transmitted in the community. For
Fluid balance in the critically ill child with dengue Too much too little? Professor Lucy Lum Universiti Malaya ASMIC Sept
 Fluid balance in the critically ill child with dengue Too much too little? Professor Lucy Lum Universiti Malaya ASMIC 2018 21-23 Sept CFR 0.22 in 2017 0.15 in 2018 2 Lecture Contents: Dynamic disease Self-limiting
Fluid balance in the critically ill child with dengue Too much too little? Professor Lucy Lum Universiti Malaya ASMIC 2018 21-23 Sept CFR 0.22 in 2017 0.15 in 2018 2 Lecture Contents: Dynamic disease Self-limiting
INTRODUCTION. Dengue is one of the ten leading. Globally 20 million cases/yr. 24,000 deaths/yr. It is important to know the typical and atypical
 DENGUE IN CHILDREN INTRODUCTION Dengue is one of the ten leading causes of hospitalization and death in children. Globally 20 million cases/yr. 24,000 deaths/yr. It is important to know the typical and
DENGUE IN CHILDREN INTRODUCTION Dengue is one of the ten leading causes of hospitalization and death in children. Globally 20 million cases/yr. 24,000 deaths/yr. It is important to know the typical and
Fine-tuning Management in Dengue Fever
 Fine-tuning Management in Dengue Fever Annual Scientific Meeting On Intensive Care 16 August 2014 Eg Kah Peng University of Malaya Medical Centre Rise In Dengue Infection New Straits Times 8 July 2014
Fine-tuning Management in Dengue Fever Annual Scientific Meeting On Intensive Care 16 August 2014 Eg Kah Peng University of Malaya Medical Centre Rise In Dengue Infection New Straits Times 8 July 2014
Case Study 6C. [TQ, 7-months-old infant girl] Dengue Clinical Management. Acknowledgements
![Case Study 6C. [TQ, 7-months-old infant girl] Dengue Clinical Management. Acknowledgements](/thumbs/77/74744886.jpg "Case Study 6C. [TQ, 7-months-old infant girl] Dengue Clinical Management. Acknowledgements") Case Study 6C [TQ, 7-months-old infant girl] Dengue Clinical Management Acknowledgements This curriculum was developed with technical assistance from the University of Malaya Medical Centre. Materials
Case Study 6C [TQ, 7-months-old infant girl] Dengue Clinical Management Acknowledgements This curriculum was developed with technical assistance from the University of Malaya Medical Centre. Materials
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Department of Pediatrics, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok 10700, Thailand.
 SIRIRAJ MEDICAL LIBRARY SpecialIssue Clinical Practice Guide for the Management of Dengue Hemorrhagic Fever (DHF), Siriraj Hospital Kulkanya Chokephaibulkit, M.D., Wanee Wisuthsarewong, M.D., Gavivann
SIRIRAJ MEDICAL LIBRARY SpecialIssue Clinical Practice Guide for the Management of Dengue Hemorrhagic Fever (DHF), Siriraj Hospital Kulkanya Chokephaibulkit, M.D., Wanee Wisuthsarewong, M.D., Gavivann
Guidelines. National. Guidelines on Management of Dengue Fever & Dengue Haemorrhagic Fever In Adults. Ministry of Health - Sri Lanka
 Ministry of Health - Sri Lanka National Guidelines Guidelines on Management of Dengue Fever & Dengue Haemorrhagic Fever In Adults In Collaboration with the Ceylon College of Physicians Revised and expanded
Ministry of Health - Sri Lanka National Guidelines Guidelines on Management of Dengue Fever & Dengue Haemorrhagic Fever In Adults In Collaboration with the Ceylon College of Physicians Revised and expanded
MODULE 8B: Management of Group B Dengue with Warning Signs or Dengue with Co-existing Conditions
 MODULE 8B: Management of Group B Dengue with Warning Signs or Dengue with Co-existing Conditions Dengue Clinical Management Acknowledgements This curriculum was developed with technical assistance from
MODULE 8B: Management of Group B Dengue with Warning Signs or Dengue with Co-existing Conditions Dengue Clinical Management Acknowledgements This curriculum was developed with technical assistance from
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
Care of the Critically Unwell Patient. fluids
 Care of the Critically Unwell Patient fluids Are we made of water? YES! Humans are like cucumbers Water content at least half of body weight in healty adults (60%) blood volume 7% bw males 6% bw females
Care of the Critically Unwell Patient fluids Are we made of water? YES! Humans are like cucumbers Water content at least half of body weight in healty adults (60%) blood volume 7% bw males 6% bw females
BREAK 11:10-11:
 1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
TACO CASE STUDIES RTC JUNE Kerry Dowling Blood Transfusion Laboratory Manager Jonathan Ricks Blood Transfusion Nurse Practitioner
 TACO CASE STUDIES RTC JUNE 2017 Kerry Dowling Blood Transfusion Laboratory Manager Jonathan Ricks Blood Transfusion Nurse Practitioner RISK FACTORS - TACO Age over 70 years although also seen in younger
TACO CASE STUDIES RTC JUNE 2017 Kerry Dowling Blood Transfusion Laboratory Manager Jonathan Ricks Blood Transfusion Nurse Practitioner RISK FACTORS - TACO Age over 70 years although also seen in younger
Clinical Management of Dengue Fever in Paediatric Patients
 Clinical Management of Dengue Fever in Paediatric Patients Dr. Mike Kwan Consultant Paediatrician Hospital Authority Infectious Disease Center Department of Paediatrics and Adolescent Medicine Princess
Clinical Management of Dengue Fever in Paediatric Patients Dr. Mike Kwan Consultant Paediatrician Hospital Authority Infectious Disease Center Department of Paediatrics and Adolescent Medicine Princess
INTRODUCTION CASE DEFINITION OF SUSPECTED DENGUE INFECTION. Review TMH Clinical Manifestations and Management of Dengue/DHF/DSS
 Tropical Medicine and Health Vol. 39 No. 4 Supplement, 2011, pp. 83-87 doi:10.2149/tmh.2011-s10 Copyright 2011 by The Japanese Society of Tropical Medicine 83 Review TMH Clinical Manifestations and Management
Tropical Medicine and Health Vol. 39 No. 4 Supplement, 2011, pp. 83-87 doi:10.2149/tmh.2011-s10 Copyright 2011 by The Japanese Society of Tropical Medicine 83 Review TMH Clinical Manifestations and Management
Ranjan Premaratna *, Erandi Liyanaarachchi, Mindu Weerasinghe, H Janaka de Silva. Abstract
 CASE REPORT Open Access Should colloid boluses be prioritized over crystalloid boluses for the management of dengue shock syndrome in the presence of ascites and pleural effusions? Ranjan Premaratna *,
CASE REPORT Open Access Should colloid boluses be prioritized over crystalloid boluses for the management of dengue shock syndrome in the presence of ascites and pleural effusions? Ranjan Premaratna *,
FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
 Manual: Section: Protocol #: Approval Date: Effective Date: Revision Due Date: 10/2019 LifeLine Patient Care Protocols Adult/Pediatrics AP1-011 10/2018 10/2018 FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
Manual: Section: Protocol #: Approval Date: Effective Date: Revision Due Date: 10/2019 LifeLine Patient Care Protocols Adult/Pediatrics AP1-011 10/2018 10/2018 FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
ISOVALERIC ACIDAEMIA -ACUTE DECOMPENSATION (standard version)
") Contact Details Name: Hospital Telephone: This protocol has 5 pages ISOVALERIC ACIDAEMIA -ACUTE DECOMPENSATION (standard version) Please read carefully. Meticulous treatment is very important as there
Contact Details Name: Hospital Telephone: This protocol has 5 pages ISOVALERIC ACIDAEMIA -ACUTE DECOMPENSATION (standard version) Please read carefully. Meticulous treatment is very important as there
COMPLICATED DKA SINDHU BHARATHI S STANLEY MEDICAL COLLEGE MD POST GRADUATE
 COMPLICATED DKA SINDHU BHARATHI S STANLEY MEDICAL COLLEGE MD POST GRADUATE Dr.Shanthi, Professor & Head, Dr. T.S. Ekambaranath Asst Professor, PICU, ISP, Stanley Medical College 9yrs male, previously normal
COMPLICATED DKA SINDHU BHARATHI S STANLEY MEDICAL COLLEGE MD POST GRADUATE Dr.Shanthi, Professor & Head, Dr. T.S. Ekambaranath Asst Professor, PICU, ISP, Stanley Medical College 9yrs male, previously normal
MATERIAL AND METHODS Study objective: To study the clinical profile and predictors of mortality in children with severe dengue.
 INTERNATIONAL JOURNAL OF BIOASSAYS ISSN: 2278-778X CODEN: IJBNHY ORIGINAL RESEARCH ARTICLE OPEN ACCESS A PROSPECTIVE OBSERVATIONAL STUDY OF CLINICAL PREDICTORS OF OUTCOME IN DENGUE IN CHILDREN Sarada G,
INTERNATIONAL JOURNAL OF BIOASSAYS ISSN: 2278-778X CODEN: IJBNHY ORIGINAL RESEARCH ARTICLE OPEN ACCESS A PROSPECTIVE OBSERVATIONAL STUDY OF CLINICAL PREDICTORS OF OUTCOME IN DENGUE IN CHILDREN Sarada G,
SIMPLY. Fluids. Dr Will Dooley
 SIMPLY. Fluids Dr Will Dooley Plan Maintenance vs Resuscitation Prescribing Common Errors Calculations Drip rates Case 54 yo presents with severe diarrhoea and vomiting. How would you proceed? Assessment
SIMPLY. Fluids Dr Will Dooley Plan Maintenance vs Resuscitation Prescribing Common Errors Calculations Drip rates Case 54 yo presents with severe diarrhoea and vomiting. How would you proceed? Assessment
Fluids and electrolytes: the basics
 Fluids and electrolytes: the basics This document is based on the handout from the Surgery for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical
Fluids and electrolytes: the basics This document is based on the handout from the Surgery for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical
Data Collection Tool. Standard Study Questions: Admission Date: Admission Time: Age: Gender:
 Data Collection Tool Standard Study Questions: Admission Date: Admission Time: Age: Gender: Specifics of Injury: Time of Injury: Mechanism of Injury Blunt vs Penetrating? Injury Severity Score? Injuries:
Data Collection Tool Standard Study Questions: Admission Date: Admission Time: Age: Gender: Specifics of Injury: Time of Injury: Mechanism of Injury Blunt vs Penetrating? Injury Severity Score? Injuries:
Sepsis Awareness and Education
 Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
Acute Kidney Injury (AKI) Undergraduate nurse education
 Undergraduate nurse education") Acute Kidney Injury (AKI) Undergraduate nurse education Year Three Developed Summer 2017 Objectives Understand Acute Kidney Injury and its relevance to patient care. Brief revision of the Anatomy and physiology
Acute Kidney Injury (AKI) Undergraduate nurse education Year Three Developed Summer 2017 Objectives Understand Acute Kidney Injury and its relevance to patient care. Brief revision of the Anatomy and physiology
M3 Pros Revision 28/4/14 Renal
 M3 Pros Revision 28/4/14 Renal Q1. Mr Ravi is a 35- year old construction worker from India with no significant past medical history. He presents with a 3- day history of high fever (Tmax = 39.5), polyarthritis,
M3 Pros Revision 28/4/14 Renal Q1. Mr Ravi is a 35- year old construction worker from India with no significant past medical history. He presents with a 3- day history of high fever (Tmax = 39.5), polyarthritis,
Chapter 8 ADMINISTRATION OF BLOOD COMPONENTS
 Chapter 8 ADMINISTRATION OF BLOOD COMPONENTS PRACTICE POINTS Give the right blood product to the right patient at the right time. Failure to correctly check the patient or the pack can be fatal. At the
Chapter 8 ADMINISTRATION OF BLOOD COMPONENTS PRACTICE POINTS Give the right blood product to the right patient at the right time. Failure to correctly check the patient or the pack can be fatal. At the
ACUTE KIDNEY INJURY FOCUS ON OBSTETRICS DONNA HIGGINS, CLINICAL NURSE EDUCATOR, NORTHERN LINCOLNSHIRE HOSPITALS NHS FOUNDATION TRUST
 ACUTE KIDNEY INJURY FOCUS ON OBSTETRICS DONNA HIGGINS, CLINICAL NURSE EDUCATOR, NORTHERN LINCOLNSHIRE HOSPITALS NHS FOUNDATION TRUST AIMS & OBJECTIVES Review the functions of the kidney Identify renal
ACUTE KIDNEY INJURY FOCUS ON OBSTETRICS DONNA HIGGINS, CLINICAL NURSE EDUCATOR, NORTHERN LINCOLNSHIRE HOSPITALS NHS FOUNDATION TRUST AIMS & OBJECTIVES Review the functions of the kidney Identify renal
Transfusion Requirements and Management in Trauma RACHEL JACK
 Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
CARE PATHWAY FOR CHILDREN AND YOUNG PERSONS WITH FEBRILE NEUTROPENIA, NEUTROPENIC SEPSIS OR SUSPECTED CENTRAL VENOUS LINE INFECTIONS
 CARE PATHWAY FOR CHILDREN AND YOUNG PERSONS WITH FEBRILE NEUTROPENIA, NEUTROPENIC SEPSIS OR SUSPECTED CENTRAL VENOUS LINE INFECTIONS This Care Pathway has been developed by a multidisciplinary team. It
CARE PATHWAY FOR CHILDREN AND YOUNG PERSONS WITH FEBRILE NEUTROPENIA, NEUTROPENIC SEPSIS OR SUSPECTED CENTRAL VENOUS LINE INFECTIONS This Care Pathway has been developed by a multidisciplinary team. It
International Journal of Pharma and Bio Sciences A STUDY OF CLINCAL PROFILE IN DENGUE CASES ABSTRACT
 Research Article Microbiology International Journal of Pharma and Bio Sciences ISSN 0975-6299 A STUDY OF CLINCAL PROFILE IN DENGUE CASES DHANDAPANI E.* 1 AND SUDHA M 2 1 Formerly Professor of Medicine,
Research Article Microbiology International Journal of Pharma and Bio Sciences ISSN 0975-6299 A STUDY OF CLINCAL PROFILE IN DENGUE CASES DHANDAPANI E.* 1 AND SUDHA M 2 1 Formerly Professor of Medicine,
Guideline for Management of Severe or Fulminating Pre-Eclampsia
 Guideline for Management of Severe or Fulminating Pre-Eclampsia Originator: Labour Ward Forum, Maternity Services Date Approved: September 2011 Approved by: W&CH Quality & Safety Group Reviewed and ratified
Guideline for Management of Severe or Fulminating Pre-Eclampsia Originator: Labour Ward Forum, Maternity Services Date Approved: September 2011 Approved by: W&CH Quality & Safety Group Reviewed and ratified
PAEDIATRIC FLUIDS RCH DEHYDRATION
 PAEDIATRIC FLUIDS RCH DEHYDRATION AIMS Understand normal fluids electrolyte requirements/ maintenance Understand how to assess DEHYDRATION in children Understand the difference between DEHYDRATION and
PAEDIATRIC FLUIDS RCH DEHYDRATION AIMS Understand normal fluids electrolyte requirements/ maintenance Understand how to assess DEHYDRATION in children Understand the difference between DEHYDRATION and
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
DYSRHYTHMIAS. D. Assess whether or not it is the arrhythmia that is making the patient unstable or symptomatic
 DYSRHYTHMIAS GENERAL CONSIDERATIONS A. The 2015 American Heart Association Guidelines were referred to for this protocol development. Evidence-based science was implemented in those areas where the AHA
DYSRHYTHMIAS GENERAL CONSIDERATIONS A. The 2015 American Heart Association Guidelines were referred to for this protocol development. Evidence-based science was implemented in those areas where the AHA
Inpatient Quality Reporting Program
 SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part II Questions and Answers Moderator: Candace Jackson, RN Inpatient Quality Reporting (IQR) Program Lead Hospital Inpatient Value, Incentives,
SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part II Questions and Answers Moderator: Candace Jackson, RN Inpatient Quality Reporting (IQR) Program Lead Hospital Inpatient Value, Incentives,
ICU management and referral guidelines for severe hypoxic respiratory failure
 Aim: ICU management and referral guidelines for severe hypoxic respiratory failure 1) To provide a concise management plan Non ventilatory Ventilatory 2) Timeline for referring patient with refractory
Aim: ICU management and referral guidelines for severe hypoxic respiratory failure 1) To provide a concise management plan Non ventilatory Ventilatory 2) Timeline for referring patient with refractory
Nephrology. 3 rd Year Revision Session 06/05/17 Cathal Hannan
 Nephrology 3 rd Year Revision Session 06/05/17 Cathal Hannan Aims Acute Kidney Injury-recognition and management Sample OSCE Station Clinically relevant renal physiology Aetiology of Chronic Kidney Disease
Nephrology 3 rd Year Revision Session 06/05/17 Cathal Hannan Aims Acute Kidney Injury-recognition and management Sample OSCE Station Clinically relevant renal physiology Aetiology of Chronic Kidney Disease
Where Emergency Medicine Meets Critical Care: Next Level Resuscitation
 Where Emergency Medicine Meets Critical Care: Next Level Resuscitation Rob Green, BSc, MD, DABEM, FRCPC, FRCP(Edin) Professor, Dalhousie University Departments of Emergency Medicine,Critical Care Medicine
Where Emergency Medicine Meets Critical Care: Next Level Resuscitation Rob Green, BSc, MD, DABEM, FRCPC, FRCP(Edin) Professor, Dalhousie University Departments of Emergency Medicine,Critical Care Medicine
-Cardiogenic: shock state resulting from impairment or failure of myocardium
 Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL
 resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL") Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL 65 Male, 60 kg D1 in ICU Admitted from OT intubated Diagnosis : septic shock secondary to necrotising fasciitis of the R lower limb
Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL 65 Male, 60 kg D1 in ICU Admitted from OT intubated Diagnosis : septic shock secondary to necrotising fasciitis of the R lower limb
Paediatric Shock. Dr Andrew Pittaway Department of Anaesthesia Bristol Royal Hospital for Children Bristol, UK
 Paediatric Shock Dr Andrew Pittaway Department of Anaesthesia Bristol Royal Hospital for Children Bristol, UK Self-assessment: 1. What is the definition of shock? 2. List the different pathophysiological
Paediatric Shock Dr Andrew Pittaway Department of Anaesthesia Bristol Royal Hospital for Children Bristol, UK Self-assessment: 1. What is the definition of shock? 2. List the different pathophysiological
Outpatient dengue management
 Outpatient dengue management Dr David Lye FRACP, FAMS Senior consultant Institute of Infectious Diseases and Epidemiology, Communicable Diseases Centre, Tan Tock Seng Hospital Associate professor Yong
Outpatient dengue management Dr David Lye FRACP, FAMS Senior consultant Institute of Infectious Diseases and Epidemiology, Communicable Diseases Centre, Tan Tock Seng Hospital Associate professor Yong
PE Pathway. The charts are listed as follows:
 PE Pathway This document comprises 6 simple flow charts to assist clinicians in the investigation and treatment of suspected or confirmed Acute Pulmonary Emboli. The pathway has been put together using
PE Pathway This document comprises 6 simple flow charts to assist clinicians in the investigation and treatment of suspected or confirmed Acute Pulmonary Emboli. The pathway has been put together using
Top tips for surviving your first on call Dr Maleeha Rizvi
 Top tips for surviving your first on call Dr Maleeha Rizvi Specialist Registrar in Cardiology University Hospital Lewisham Overview Practical points The Bleep and prioritising on call Cardiac arrests Prescribing
Top tips for surviving your first on call Dr Maleeha Rizvi Specialist Registrar in Cardiology University Hospital Lewisham Overview Practical points The Bleep and prioritising on call Cardiac arrests Prescribing
Pediatric Diabetic Ketoacidosis (DKA) General Pediatrics Admission Order Set
 General Pediatrics Admission Order Set") Admitting MRP: Pediatrics: Dr. / Dr. on call to cover until 08:00 am Service: Medicine Team 1 Medicine Team 2 Medical subspecialty Diagnosis: Diabetic Ketoacidosis (DKA) Estimated length of stay Less than
Admitting MRP: Pediatrics: Dr. / Dr. on call to cover until 08:00 am Service: Medicine Team 1 Medicine Team 2 Medical subspecialty Diagnosis: Diabetic Ketoacidosis (DKA) Estimated length of stay Less than
the bleeding won t stop? Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital
 Royal Alexandra Hospital") What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
Initial Resuscitation of Sepsis & Septic Shock
 Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
INTRAVENOUS FLUIDS PRINCIPLES
 INTRAVENOUS FLUIDS PRINCIPLES Postnatal physiological weight loss is approximately 5-10% Postnatal diuresis is delayed in Respiratory Distress Syndrome (RDS) Preterm babies have limited capacity to excrete
INTRAVENOUS FLUIDS PRINCIPLES Postnatal physiological weight loss is approximately 5-10% Postnatal diuresis is delayed in Respiratory Distress Syndrome (RDS) Preterm babies have limited capacity to excrete
Management of Nephrotic Syndrome
 Management of Nephrotic Syndrome 1. Introduction Incidence 2-4/100,000. Boys > girls 3:2; age of onset 2-6 years 80% of cases in children is due to minimal change (MCD) of which 80% will respond to steroid
Management of Nephrotic Syndrome 1. Introduction Incidence 2-4/100,000. Boys > girls 3:2; age of onset 2-6 years 80% of cases in children is due to minimal change (MCD) of which 80% will respond to steroid
Transfusion-Related Acute Lung Injury (TRALI) and Strategies for Prevention. Khalid Abdulla Sharif, MD, MRCP (UK)*
 and Strategies for Prevention. Khalid Abdulla Sharif, MD, MRCP (UK)*") Bahrain Medical Bulletin, Vol. 29, No.4, December 2007 Transfusion-Related Acute Lung Injury (TRALI) and Strategies for Prevention Khalid Abdulla Sharif, MD, MRCP (UK)* Background: Transfusion-Related
Bahrain Medical Bulletin, Vol. 29, No.4, December 2007 Transfusion-Related Acute Lung Injury (TRALI) and Strategies for Prevention Khalid Abdulla Sharif, MD, MRCP (UK)* Background: Transfusion-Related
Resuscitation of the Critically ill Foal
 Resuscitation of the Critically ill Foal Sick Cell Syndrome Foal: Wishful Warm Blood filly DOB: March 25 1 AM Admission Date: March 25 11:25 AM 10 hours old Wishful History Born at 1 AM on March 25 Foal
Resuscitation of the Critically ill Foal Sick Cell Syndrome Foal: Wishful Warm Blood filly DOB: March 25 1 AM Admission Date: March 25 11:25 AM 10 hours old Wishful History Born at 1 AM on March 25 Foal
Case Scenario 3: Shock and Sepsis
 Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Guideline for the Management of Acute Chest Syndrome in Children with Sickle Cell Disease
 Guideline for the Management of Acute Chest Syndrome in Children with Sickle Cell Disease Definition Acute chest syndrome (ACS) is defined as an acute illness characterized by fever and/or respiratory
Guideline for the Management of Acute Chest Syndrome in Children with Sickle Cell Disease Definition Acute chest syndrome (ACS) is defined as an acute illness characterized by fever and/or respiratory
CASE SCENARIO EXERCISE
 påçííáëü=pìêîéáää~ååé=çñ=eé~äíüå~êé ^ëëçåá~íéç=fåñéåíáçå=mêçöê~ããé CASE SCENARIO EXERCISE CATHETER-ASSOCIATED URINARY TRACT INFECTION SURVEILLANCE SCOTTISH SURVEILLANCE OF HEALTHCARE ASSOCIATED INFECTION
påçííáëü=pìêîéáää~ååé=çñ=eé~äíüå~êé ^ëëçåá~íéç=fåñéåíáçå=mêçöê~ããé CASE SCENARIO EXERCISE CATHETER-ASSOCIATED URINARY TRACT INFECTION SURVEILLANCE SCOTTISH SURVEILLANCE OF HEALTHCARE ASSOCIATED INFECTION
Blood/Blood Component Utilization and Administration Annual Compliance Education
 Blood/Blood Component Utilization and Administration Annual Compliance Education This course contains annual compliance education necessary to meet compliance and regulatory requirements. Instructions:
Blood/Blood Component Utilization and Administration Annual Compliance Education This course contains annual compliance education necessary to meet compliance and regulatory requirements. Instructions:
UHSM ED Pathway ELDERLY FALL / COLLAPSE
 UHSM ED Pathway ELDERLY FALL / COLLAPSE Patient name / Pathway for patients who require assessment in ED after a fall or collapse Note: - It can be used if the patient has also sustained a minor head injury
UHSM ED Pathway ELDERLY FALL / COLLAPSE Patient name / Pathway for patients who require assessment in ED after a fall or collapse Note: - It can be used if the patient has also sustained a minor head injury
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP
 SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
INTRAVENOUS FLUID THERAPY
 INTRAVENOUS FLUID THERAPY PRINCIPLES Postnatal physiological weight loss is approximately 5 10% in first week of life Preterm neonates have more total body water and may lose 10 15% of their weight in
INTRAVENOUS FLUID THERAPY PRINCIPLES Postnatal physiological weight loss is approximately 5 10% in first week of life Preterm neonates have more total body water and may lose 10 15% of their weight in
Nitroglycerin and Heparin Drip Interfacility Protocols
 Nitroglycerin and Heparin Drip Interfacility Protocols EMS Protocol This protocol applies to nitroglycerin and Heparin drips that are initiated at the transferring facility prior to transport and are not
Nitroglycerin and Heparin Drip Interfacility Protocols EMS Protocol This protocol applies to nitroglycerin and Heparin drips that are initiated at the transferring facility prior to transport and are not
Damage Control Resuscitation. VGH Trauma Rounds 2018 Harvey Hawes
 Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
Example Clinician Educational Material for Providers of Immune Effector Cellular Therapy
 Example Clinician Educational Material for Providers of Immune Effector Cellular Therapy Disclaimer: This example is just one of many potential examples of clinician education material that can be provided
Example Clinician Educational Material for Providers of Immune Effector Cellular Therapy Disclaimer: This example is just one of many potential examples of clinician education material that can be provided
SIMPLY. Fluids. Dr William Dooley
 SIMPLY. Fluids Dr William Dooley Plan Fluid management Resuscitation Routine Maintenance Replacement Redistribution Reassessment Common Errors Calculations Assessment?ORAL vs. IVF History Limited intake
SIMPLY. Fluids Dr William Dooley Plan Fluid management Resuscitation Routine Maintenance Replacement Redistribution Reassessment Common Errors Calculations Assessment?ORAL vs. IVF History Limited intake
CRRT Fundamentals Pre-Test. AKI & CRRT 2017 Practice Based Learning in CRRT
 CRRT Fundamentals Pre-Test AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling at home. He
CRRT Fundamentals Pre-Test AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling at home. He
STORMY DENGUE with bloody problems. Anand M.Patil PICU MED/SURG TEAM Apollo Childrens Hospitals Chennai
 STORMY DENGUE with bloody problems Anand M.Patil PICU MED/SURG TEAM Apollo Childrens Hospitals Chennai 1 HISTORY 4 ½ years girl Day 1: Fever, Lethargy, Low urine output Hypotension, high PCV,low platelets
STORMY DENGUE with bloody problems Anand M.Patil PICU MED/SURG TEAM Apollo Childrens Hospitals Chennai 1 HISTORY 4 ½ years girl Day 1: Fever, Lethargy, Low urine output Hypotension, high PCV,low platelets
Chapter 3 MAKING THE DECISION TO TRANSFUSE
 Chapter 3 MAKING THE DECISION TO TRANSFUSE PRACTICE POINTS Determine the best treatment for the patient which may include transfusion. Treat the cause of cytopenia (anaemia or thrombocytopenia) or plasma
Chapter 3 MAKING THE DECISION TO TRANSFUSE PRACTICE POINTS Determine the best treatment for the patient which may include transfusion. Treat the cause of cytopenia (anaemia or thrombocytopenia) or plasma
Severe Dengue Infection in ICU. Shirish Prayag MD, FCCM Pune, India
 Severe Dengue Infection in ICU Shirish Prayag MD, FCCM Pune, India Greetings from India Declaration Honararia from MSD, Astra Zenecea, Fresenius Kabi, Pfizer, Intas, Glenmark for conducting lectures. No
Severe Dengue Infection in ICU Shirish Prayag MD, FCCM Pune, India Greetings from India Declaration Honararia from MSD, Astra Zenecea, Fresenius Kabi, Pfizer, Intas, Glenmark for conducting lectures. No
Evidence- Based Medicine Fluid Therapy
 Evidence- Based Medicine Fluid Therapy Ndidi Musa M.D. Assosciate Professor of Pediatrics Medical College of Wisconsin/ Children s Hospital of Wisconsin Disclosures A. I have no relevant financial relationships
Evidence- Based Medicine Fluid Therapy Ndidi Musa M.D. Assosciate Professor of Pediatrics Medical College of Wisconsin/ Children s Hospital of Wisconsin Disclosures A. I have no relevant financial relationships
SLCOA National Guidelines
 SLCOA National Guidelines Peri - operative Fluid & Electrolyte Management SLCOA National Guidelines Contents List of Contributors 92 Paediatric fasting guidelines for elective procedures 93 Guidelines
SLCOA National Guidelines Peri - operative Fluid & Electrolyte Management SLCOA National Guidelines Contents List of Contributors 92 Paediatric fasting guidelines for elective procedures 93 Guidelines
SHOCK Susanna Hilda Hutajulu, MD, PhD
 SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
With Dr. Sarah Reid and Dr. Sarah Curtis
 5. Headaches 6. Known diabetes 7. Specific high risk groups (ie. Teenagers, children on insulin pumps and those from lower socio-economic status). Episode 63 Pediatric Diabetic Ketoacidosis With Dr. Sarah
5. Headaches 6. Known diabetes 7. Specific high risk groups (ie. Teenagers, children on insulin pumps and those from lower socio-economic status). Episode 63 Pediatric Diabetic Ketoacidosis With Dr. Sarah
MODULE 7: Outpatient Management
 MODULE 7: Outpatient Management Dengue Clinical Management Acknowledgements This curriculum was developed with technical assistance from the University of Malaya Medical Centre. Materials were contributed
MODULE 7: Outpatient Management Dengue Clinical Management Acknowledgements This curriculum was developed with technical assistance from the University of Malaya Medical Centre. Materials were contributed
Sharing of HA Current Protocols on Dengue Fever (DF) Ms MY KONG, SNO, HA CICO office 31 August 2018
 Ms MY KONG, SNO, HA CICO office 31 August 2018") Sharing of HA Current Protocols on Dengue Fever (DF) Ms MY KONG, SNO, HA CICO office 31 August 2018 1 HA Preparedness for Dengue Fever Outbreak HA Operational Plan for Dengue Fever Outbreak http://ha.home/ho/cico/ha_operational_plan_dengue.pdf
Sharing of HA Current Protocols on Dengue Fever (DF) Ms MY KONG, SNO, HA CICO office 31 August 2018 1 HA Preparedness for Dengue Fever Outbreak HA Operational Plan for Dengue Fever Outbreak http://ha.home/ho/cico/ha_operational_plan_dengue.pdf
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
HEAT STROKE. Lindsay VaughLindsay Vaughn, DVM, DACVECCDVM, DACVECC
 HEAT STROKE Lindsay VaughLindsay Vaughn, DVM, DACVECCDVM, DACVECC Heat Stroke More Preventable Than Treatable Heat Stroke A form of hyperthermia associated with a systemic inflammatory response leading
HEAT STROKE Lindsay VaughLindsay Vaughn, DVM, DACVECCDVM, DACVECC Heat Stroke More Preventable Than Treatable Heat Stroke A form of hyperthermia associated with a systemic inflammatory response leading
INTRAVENOUS FLUID THERAPY. Tom Heaps Consultant Acute Physician
 INTRAVENOUS FLUID THERAPY Tom Heaps Consultant Acute Physician LEARNING OBJECTIVES 1. Crystalloids vs colloids 2. Balanced vs non-balanced solutions 3. Composition of various IV fluids 4. What is normal
INTRAVENOUS FLUID THERAPY Tom Heaps Consultant Acute Physician LEARNING OBJECTIVES 1. Crystalloids vs colloids 2. Balanced vs non-balanced solutions 3. Composition of various IV fluids 4. What is normal
Right Iliac Fossa Pain
 Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Right Iliac Fossa Pain Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should
Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Right Iliac Fossa Pain Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should
Hyperglycaemic Emergencies GRI EDUCATION
 Hyperglycaemic Emergencies GRI EDUCATION LEARNING OUTCOMES Develop and describe your system of blood gas interpretation and recognise common patterns of acid-base abnormality. Describe the pathophysiology
Hyperglycaemic Emergencies GRI EDUCATION LEARNING OUTCOMES Develop and describe your system of blood gas interpretation and recognise common patterns of acid-base abnormality. Describe the pathophysiology
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 13 Resuscitation and Preparation for Anesthesia & Surgery Key Points 2 13.1 Management of Emergencies and Cardiopulmonary Resuscitation The emergency measures that
Surgical Care at the District Hospital 1 13 Resuscitation and Preparation for Anesthesia & Surgery Key Points 2 13.1 Management of Emergencies and Cardiopulmonary Resuscitation The emergency measures that
Medicine Dr. Dana Lecture 1 Acute Kidney Injury (AKI)
") Medicine Dr. Dana Lecture 1 Acute Kidney Injury (AKI) Renal function Kidney has many roles: 1. Excretory function 2. Osmolality regulation 3. Acid base balance 4. BP regulation through salt and water balance
Medicine Dr. Dana Lecture 1 Acute Kidney Injury (AKI) Renal function Kidney has many roles: 1. Excretory function 2. Osmolality regulation 3. Acid base balance 4. BP regulation through salt and water balance
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT
 PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
Acid Base Imbalance. 1. Prior to obtaining the ABG s an Allen s test should be performed. Explain the rationale for this.
 Acid Base Imbalance Case 1. An 18-year-old male arrives via EMS to the emergency department. He is experiencing Tachypnea, dizziness, numbness and paraesthesia. He is anxious, respirations are 28 per minute
Acid Base Imbalance Case 1. An 18-year-old male arrives via EMS to the emergency department. He is experiencing Tachypnea, dizziness, numbness and paraesthesia. He is anxious, respirations are 28 per minute
No Catheter, No CAUTI Scenario 1 Urinary catheter-trauma
 No Catheter, No CAUTI Scenario 1 Urinary catheter-trauma Course lead Colette Laws-Chapman Faculty Course / Curriculum Scenario name No Catheter, No catheter associated urine infection (CAUTI) Scenario
No Catheter, No CAUTI Scenario 1 Urinary catheter-trauma Course lead Colette Laws-Chapman Faculty Course / Curriculum Scenario name No Catheter, No catheter associated urine infection (CAUTI) Scenario
TBSA Burn Estimation Chart Adult Major Burn Clinical Practice Guideline
 TBSA Burn Estimation Chart Adult Major Burn Clinical Practice Guideline Patient Label Anatomical Subunit Percent Total Percent One Side Anterior Posterior Injury Subtotal 3.5% 2nd and 3rd degree burns
TBSA Burn Estimation Chart Adult Major Burn Clinical Practice Guideline Patient Label Anatomical Subunit Percent Total Percent One Side Anterior Posterior Injury Subtotal 3.5% 2nd and 3rd degree burns
Shock is defined as a state of cellular and tissue hypoxia due to : reduced oxygen delivery and/or increased oxygen consumption or inadequate oxygen
 Shock is defined as a state of cellular and tissue hypoxia due to : reduced oxygen delivery and/or increased oxygen consumption or inadequate oxygen utilization The effects of shock are initially reversible
Shock is defined as a state of cellular and tissue hypoxia due to : reduced oxygen delivery and/or increased oxygen consumption or inadequate oxygen utilization The effects of shock are initially reversible
Transfusion reactions. Jim Taylor Haematology SpR Sheffield
 Transfusion reactions Jim Taylor Haematology SpR Sheffield Pre questions 1. Platelet transfusions are more prone to bacterial contamination compared to red cells. T/F 2. Common causes of an acute transfusion
Transfusion reactions Jim Taylor Haematology SpR Sheffield Pre questions 1. Platelet transfusions are more prone to bacterial contamination compared to red cells. T/F 2. Common causes of an acute transfusion
A Care Pathway exists for the management of neutropenic fever. Copies of the care pathway document are available in EAU, A&E, Deanesly and CHU.
 Subject: Neutropenic Fever Guideline for Junior Doctors Date of Implementation: January 2010 Date of Review: January 2012 Director Responsible for Implementation and Review: Policy location: Consultant
Subject: Neutropenic Fever Guideline for Junior Doctors Date of Implementation: January 2010 Date of Review: January 2012 Director Responsible for Implementation and Review: Policy location: Consultant
Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018
 Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018") Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018 Objectives 1. To identify the symptom of severe sepsis and septic shock syndrome.
Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018 Objectives 1. To identify the symptom of severe sepsis and septic shock syndrome.
Presented by: Indah Dwi Pratiwi
 Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Acute changes in condition: Caring for a child with myocarditis. Looking at the first 48 hours of admission
 Acute changes in condition: Caring for a child with myocarditis Looking at the first 48 hours of admission Demographics introduction Nosi TB GIRL HIVUNEXPOSED 5 years old 15kg, well nourished 1 of 4 children
Acute changes in condition: Caring for a child with myocarditis Looking at the first 48 hours of admission Demographics introduction Nosi TB GIRL HIVUNEXPOSED 5 years old 15kg, well nourished 1 of 4 children
CHILDREN S SERVICES. Guidelines for the Management of Meningococcal Septicaemia
 1 CHILDREN S SERVICES Guidelines for the Management of Meningococcal Septicaemia Please note these are guidelines only and it will be the clinician s discretion to apply different treatment depending on
1 CHILDREN S SERVICES Guidelines for the Management of Meningococcal Septicaemia Please note these are guidelines only and it will be the clinician s discretion to apply different treatment depending on
Brief summary of the NICE guidelines December 2013
 Brief summary of the NICE guidelines December 2013 Intravenous fluid therapy in adults in hospital the relevance to Emergency Department Care Applicable to patients 16 years and older receiving i.v. fluids
Brief summary of the NICE guidelines December 2013 Intravenous fluid therapy in adults in hospital the relevance to Emergency Department Care Applicable to patients 16 years and older receiving i.v. fluids