PATENT FORAMEN OVALE: UPDATE IN MANAGEMENT OF RECURRENT STROKE KATRINE ZHIROFF, MD, FACC, FSCAI LOS ANGELES CARDIOLOGY ASSOCIATES
|
|
|
- Rafe Bishop
- 5 years ago
- Views:
Transcription

1 PATENT FORAMEN OVALE: UPDATE IN MANAGEMENT OF RECURRENT STROKE KATRINE ZHIROFF, MD, FACC, FSCAI LOS ANGELES CARDIOLOGY ASSOCIATES
2 OBJECTIVES Review social burden and epidemiology of stroke Gender disparities in stroke diagnosis and management Diagnosis of cryptogenic stroke Role of PFO and gender in pathophysiology of cryptogenic stroke Indications for PFO closure in secondary stroke prevention Review of date from clinical trials supporting PFO closure
3 STROKE STATISTICS Stroke kills about 140,000 Americans each year 1 out of every 20 deaths Every year, more than 795,000 people in the United States have a stroke About 610,000 of these are first or new strokes About 185,00 strokes nearly 1 of 4 87% of all strokes have ischemic etiology Projections by 2030, an additional 3.4 million US adults will have had a stroke 20.5% increase in prevalence from 2012 Highest increase (29%) is projected to be in Hispanic men
4 STROKE ECONOMIC BURDEN US cost estimated $34 billion each year Health care services, medicines to treat stroke, and missed days of work Between 2012 and 2030, total direct medical stroke-related costs are projected to triple $71.6 billion to $184.1 billion majority of the projected increase in costs arising from those 65 to 79 years of age
5 fields of cardiology and stroke medicine encompass the 2 most important vascular territories affected by disease, the heart and brain. the most important overlap between cardiology and stroke medicine involves ischemic heart disease and ischemic stroke. Commonalities between these 2 frequently encountered disorders include similar epidemiological bases and risk factors, overlapping pathophysiological mechanisms, and similar approaches to acute therapy and to primary and secondary prevention.

6
7 WOMEN AND STROKE Women have a higher lifetime risk of stroke than men Lifetime risk of stroke among 55 to 75 years of age was 1 in 5 for women (20% 21%) Lifetime risk of stroke among 55 to 75 years of age 1 in 6 for men (14% 17%) Age-specific incidence rates are substantially lower in women than men in younger and middle-age groups Differences narrow in the older age groups

8 RISK OF STROKE IN WOMEN: EFFECT OF AGE AND GENDER
. Emelia J. Benjamin et al.")

9 PREVALENCE OF STROKE BY AGE AND SEX (NHANES ). Emelia J. Benjamin et al. Circulation. 2017;135:e146-e603 Copyright American Heart Association, Inc. All rights reserved.
10 WOMEN AND STROKE Stroke is the 3 rd leading cause of death for women Stroke is the 5 th leading cause of death for men Each year 55,000 more women have a stroke than men. Stroke will have a more negative impact in women Live longer than men Live alone when they have a stroke Be more likely to live in a long term health care facility after a stroke Have a worse functional recovery after stroke

11 Probability of death within 1 year after first stroke. Emelia J. Benjamin et al. Circulation. 2017;135:e146-e603 Copyright American Heart Association, Inc. All rights reserved.
12 STROKE AND DISABILITY In 2003, among Medicare patients discharged from the hospital after stroke 45% returned directly home 32% used home healthcare services 24% were discharged to inpatient rehabilitation facilities 31% were discharged to skilled nursing facilities
13 WOMEN AND DISABILITY After stroke, women often have greater disability than men Women were half as likely to be independent in activities of daily living after stroke, after controlling for age, race, education, and marital status A meta-analysis of >25 studies found that women had worse functional recovery and greater long-term disability and handicap
14 STROKE AND DISABILITY

15 AWARENESS OF STROKE SYMPTOMS
16 PUBLIC AWARENESS Someone other than the patient decides to seek treatment in 66% of the cases A study was conducted of patients admitted to an ED with possible stroke to determine their knowledge of the signs, symptoms, and risk factors of stroke 39% did not know a single sign or symptom A study of patients with stroke 60.5% were able to accurately identify 1 stroke risk factor 55.3% were able to identify 1 stroke symptom Median delay time from onset of symptoms to admission in the ED was 16 hours and only 31.6% accessed the ED in <2 hours
17 ACUTE STROKE SYMPTOMS WOMEN VS MEN DISCOORDINATION/ATAXIA HEMIPARESIS APHASIA MENTAL STATUS CHANGE DIPLOPIA Analysis showed that the appearance of nonmotor symptoms as the primary symptom and nonuse of the system were significant predictors of delay >2 hours.
18 NONTRADITIONAL SYMPTOMS OF STROKE 51.8% women reported 1 nontraditional stroke/tia symptom compared to 43.9% of men (p=0.09). Most prevalent nontraditional symptom was mental status change (women, 23.2%; men, 15.2%; p=0.03). The odds of reporting at least 1 nontraditional stroke/tia symptom were 1.42 times (95% CI, ) greater in women than in men.
19 WOMEN AND STROKE SYMPTOMS Loss of consciousness or fainting General weakness Difficulty or shortness of breath Confusion, unresponsiveness or disorientation Sudden behavioral change Agitation Hallucination Nausea or vomiting Pain Seizures Hiccups
20 GENDER DISPARITIES IN TREATMENT OF STROKE Median time to arrival to ED longer by 1 hour Longer waiting times in ED 11% longer door-to-doctor times and 15% longer door-to-image times as men Less intensive treatment and therapeutic workup 71% males versus 62% females had carotid imaging 57% males versus 48% females had 2D ECho
21 WOMEN AND ACUTE STROKE CARE 10% less likely to be admitted within 3 hours of stroke 13% less likely to receive thrombolysis Discrepancies persist despite controlling for age, comorbidity, prestroke functional status, stroke severity OR 0.51 for women to receive tpa compared to men Several studies have demonstrated equal or superior effectiveness of tpa compared to men Lower Rankin scores and more substantial neurological recovery in women within 24 hours of IV tpa Worse functional outcomes in untreated women
22 % of patients IDENTIFICATION OF PERSONAL RISK FACTORS Hypertension 54 High Cholesterol Smoke ever Diabetes Angina/CAD Atrial Fibrillation Identified Risk Factor 7.9 Carotid Stenosis % Have % Identified
23 % of Subjects AWARENESS OF SYMPTOMS IN WOMEN Knowledge of Warning Signs Weakness/numbness Dizziness Headache Confusion Trouble talking 0 % of Subjects
24 STROKE RISK FACTORS UNIQUE TO WOMEN GENERAL RISK FACTORS Family history, high blood pressure, high cholesterol, atrial fibrillation, diabetes, smoking, lack of exercise, and being overweight ORAL CONTRACEPTIVES PREGNANCY HORMONE REPLACEMENT THERAPY (HRT) MIGRAINE HEADACHES WITH AURA
25 HORMONE THERAPY AND STROKE Menopausal state is associated with increased risk of stroke Women with natural menopause <42 yo had 2-fold increased ischemic stroke risk of women with natural menopause >42 yo Use of oral contraceptives increased prothrombotic state and increases risk of stroke Use of estrogen plus progestin, as well as estrogen alone, increases stroke risk in postmenopausal, generally healthy women Provides no protection for postmenopausal women with established and recent stroke or TIA
26 PREGNANCY AND STROKE The risk of ischemic stroke or intracranial hemorrhage during pregnancy and the first 6 weeks after giving birth was 2.4 times greater than for nonpregnant women of similar age and race Preeclampsia is a risk factor for ischemic stroke remote from pregnancy
27 MIGRAINE AND STROKE RISK Increase a woman's stroke risk two and a half times Most people in the U.S. who suffer migraines are women Migraine with aura is associated with ischemic stroke in younger women, particularly if they smoke or use oral contraceptives. The combination of Migraine+ OCP + Smoking all 3 factors increases the risk 9-fold compared with women without any of these factors
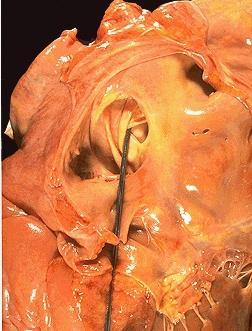
28 PATENT FORAMEN OVALE An anatomical interatrial communication with potential for right-to-left shunt Known since the time of Galen (130 AD-210 AD) In 1564, Leonardi Botali, an italian surgeon, was the first to describe the presence of foramen ovale at birth Function in utero was not known at that time In 1877, Cohnheim described paradoxical embolism relation to PFO
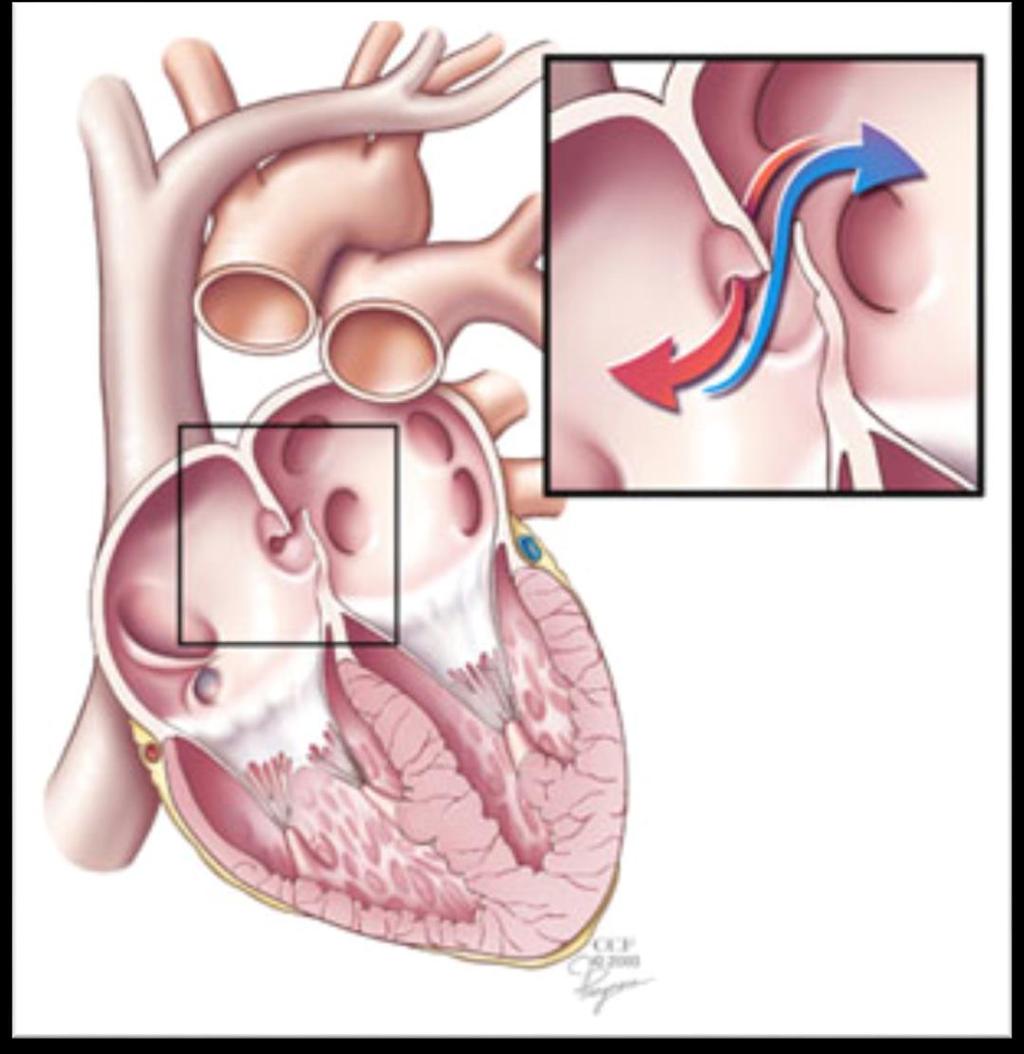
29 EPIDEMIOLOGY OF PFO Flaplike opening between the atrial septa primum and secundum at the location of the fossa ovalis that persists after age 1 year In utero, serves as a physiologic conduit for right-to-left shunting Once the pulmonary circulation is established after birth, left atrial pressure increases, allowing functional closure of the foramen ovale. Anatomical closure of the septum primum and septum secundum by the age of 1 year Detected in 10-15% of the population by contrast transthoracic echocardiography Autopsy studies show a 27% prevalence of probe-patent foramen ovale
30
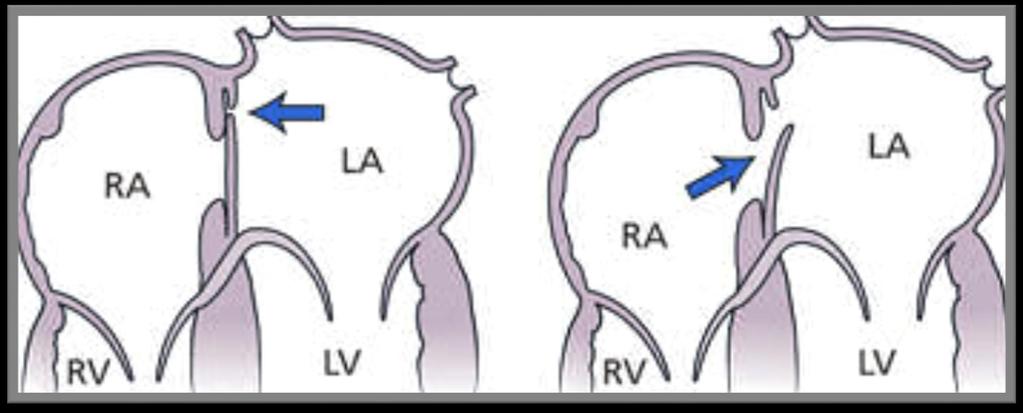
31 PATHOPHYSIOLOGY OF PFO The Mayo clinic autopsy study revealed that the size of a PFO increases from a mean of 3.4 mm in the first decade to 5.8 mm in the 10th decade of life, as the valve of fossa ovalis stretches with age Large enough to permit passage of emboli that may occlude MCA (~ 3 mm ) and major cortical branches (~1 mm) Any conditions that increase right atrial pressure more than left atrial pressure can induce paradoxical flow and may result in an embolic event Found in up to 50% of young adults with cryptogenic stroke
32 IS PFO A FAMILIAL TRAIT?
33
34 TOAST Classification Classification Of Stroke Subtypes LARGE-ARTERY ATHEROSCLEROSIS CARDIOEMBOLISM 14 to 30 % of ischemic strokes SMALL-VESSEL OCCLUSION STROKE OF OTHER DETERMINED ETIOLOGY STROKE OF UNDETERMINED ETIOLOGY CRYPTOGENIC STROKE No large vessel stenosis ( 50 percent) or occlusion in the territory of the infarct No evidence of occult atrial fibrillation and no other high-risk cardioembolic source No radiographic acute lacunar infarction and no clinical lacunar stroke syndrome if imaging shows no infarct
35 CRYPTOGENIC STROKE 20-30% of all strokes are qualified as cryptogenic Low overall rate of recurrence in patients yo with cryptogenic stroke treated with aspirin 1.9% in the first year of follow up 0.8% per year in years 2-4 of follow up Most are embolic in nature Sources include proximal arterial sources, heart and venous structure Topographic clues of etiology Infarcts in multiple territories suggest emboli from a proximal aortocardiac source Infarcts of different ages in a single territory suggest emboli of arterial origin Infarcts along the borders between brain artery territories suggest systemic hypotension or multiple emboli Small, deep infarct along with white-matter hyperintensities suggests intrinsic small-vessel disease Presenting history may point to clues for etiology Saver et al. NEJM 2016: 374;21

36 Saver et al. NEJM 2016: 374;21
37 FEATURES THAT INCREASE LIKELIHOOD OF CAUSATION Younger age Valsalva at the onset of stroke symptoms Extended travel preceding stroke Concomitant VTE Coexisting venous hypercoagulable state Atrial septal aneurysm History of migraine with aura Cortical location, multiplicity and large size of cerebral infarcts Absence of hypertension, diabetes, smoking Saver et al. NEJM 2016: 374;21

38 Eleni Doufekias et al. JACC 2008;51: American College of Cardiology Foundation

39 RoPE SCORE CALCULATOR (Risk of Paradoxical Embolism) IS PFO AN INCIDENTAL FINDING OR CAUSE OF STROKE? PFO prevalence increased from 23% in those with 0 to 3 points to 73% in those with 9 or 10 points Kent et al. Neurology 2013; 81: 619
40 Kavinsky et al. CIT 2017; 11(3):47


41 Published July 27, 2016 in Neurology
42
43 CLOSURE OR MEDICAL THERAPY FOR CRYPTOGENIC STROKE WITH PATENT FORAMEN OVALE Furlan et al. For the CLOSURE I investigators N ENGL J MED 2012; 366: patients were enrolled Starflex septal closure system I 18 and 60 years of age with a cryptogenic stroke or transient ischemic attack (TIA) and PFO The primary end point was a composite of stroke or transient ischemic attack during 2 years of follow-up Closure with a device did not offer a greater benefit than medical therapy alone for the prevention of recurrent stroke or TIA.
44 CLOSURE OF PATENT FORAMEN OVALE VERSUS MEDICAL THERAPY AFTER CRYPTOGENIC STROKE John D. Carroll, M.D., et al. For the RESPECT investigators N= 980 patients (mean age, 45.9 years) at 69 sites Follow-up period of 2.6±2.0 years, a median of 2.1 years Amplatzer PFO occluder was implanted in 462 In the primary intention-to-treat analysis, there was no significant benefit associated with closure of a patent foramen ovale in adults who had had a cryptogenic ischemic stroke. Carroll et al. N Engl J Med 2013; 368:1092
45 PERCUTANEOUS CLOSURE OF PATENT FORAMEN OVALE IN CRYPTOGENIC EMBOLISM Bernhard Meier, M.D., et al. For the PC trial investigators * N Engl J Med 2013; 368: patients randomized 1:1 Mean duration of follow-up 4.1 yrs Amplatzer PFO Closer Closure of a patent foramen ovale for secondary prevention of cryptogenic embolism did not result in a significant reduction in the risk of recurrent embolic events or death as compared with medical therapy.
: 907 917 Among 2,303 patients, closure was not significantly associated with the primary composite outcome.")
46 DEVICE CLOSURE OF PATENT FORAMEN OVALE AFTER STROKE: POOLED ANALYSIS OF COMPLETED RANDOMIZED TRIALS Kent et al. J Am Coll Cardiol Mar 1; 67(8): Among 2,303 patients, closure was not significantly associated with the primary composite outcome. For the outcome of stroke, all comparisons were statistically significant HR.058

47 Kavinsky et al. CIT 2017; 11(3):47
48 WHY BE MORE AGGRESSIVE WITH PFO CLOSURE IN 2018? CLOSE REDUCE RESPECT
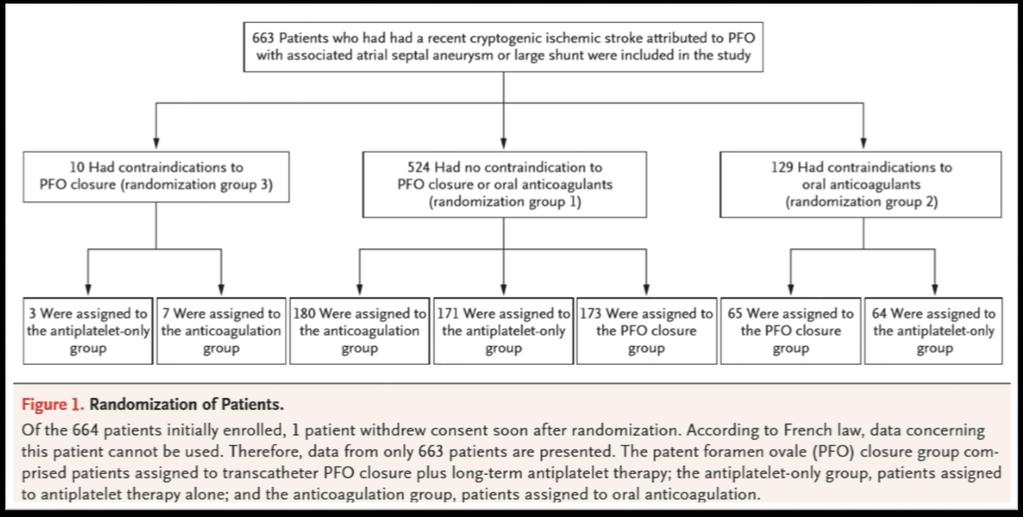
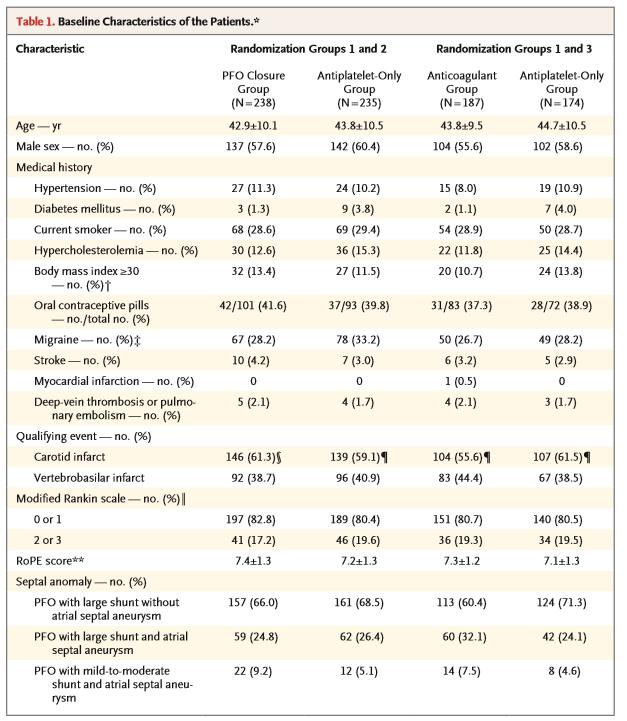
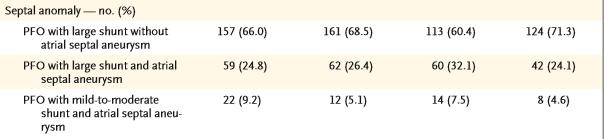
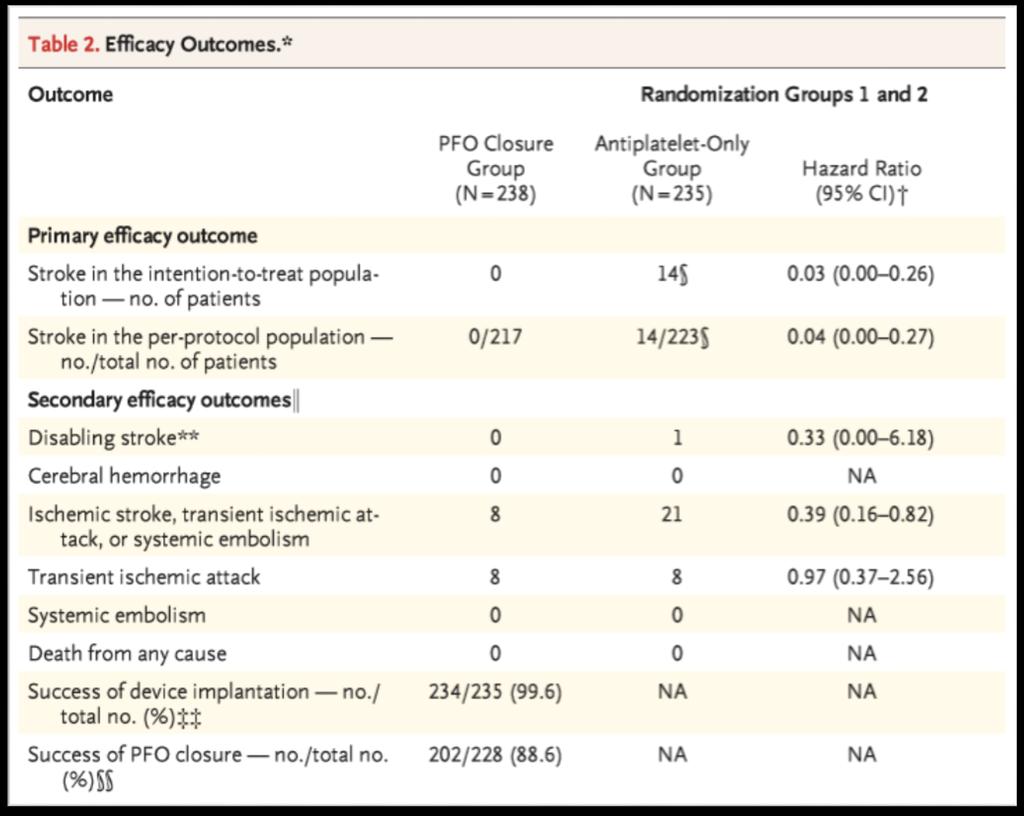
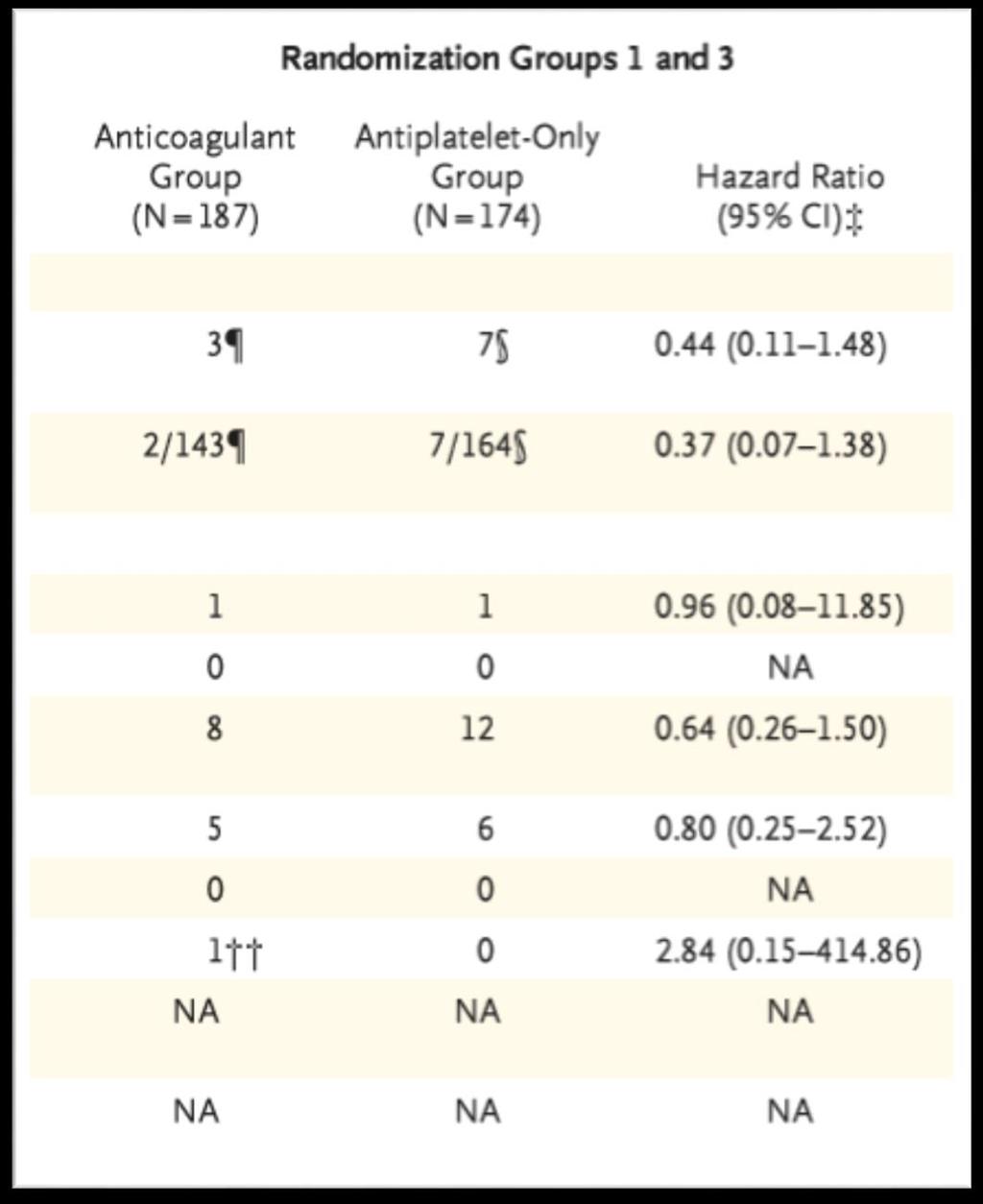
49 CLOSE PFO Closure vs Anticoagulation vs Antiplatelets After Stroke Multicenter, randomized, open-label trial; 1:1:1 randomization Patients 16 to 60 years of age who had had a recent stroke attributed to PFO, with an associated atrial septal aneurysm or large interatrial shunt Transcatheter PFO closure plus long-term antiplatelet therapy (PFO closure group) Antiplatelet therapy alone (antiplatelet-only group) or oral anticoagulation (anticoagulation group) (randomization group 1) Patients with contraindications to anticoagulants or to PFO closure were randomly assigned to the alternative noncontraindicated treatment or to antiplatelet therapy (randomization groups 2 and 3) The primary outcome was occurrence of stroke N=663 Study funded by the French Ministry of Health Derumeaux et al. NEJM ;11:1011
50
51

52 NNT=20 To prevent one stroke
53

54 AF in PFO group detected within 1 month of the procedure No recurrence of AF in PFO group in the 4.4 years of follow up Effect on risk of stroke not known
55 CONCLUSIONS FROM CLOSE Among patients who had had a recent cryptogenic stroke attributed to PFO with an associated atrial septal aneurysm or large interatrial shunt, the rate of stroke recurrence was lower among those assigned to PFO closure combined with antiplatelet therapy than among those assigned to antiplatelet therapy alone. Patients in this trial were well selected for those with cryptogenic stroke 2/2 paradoxical embolism Observed rate of strokes was lower than anticipated based on historical data
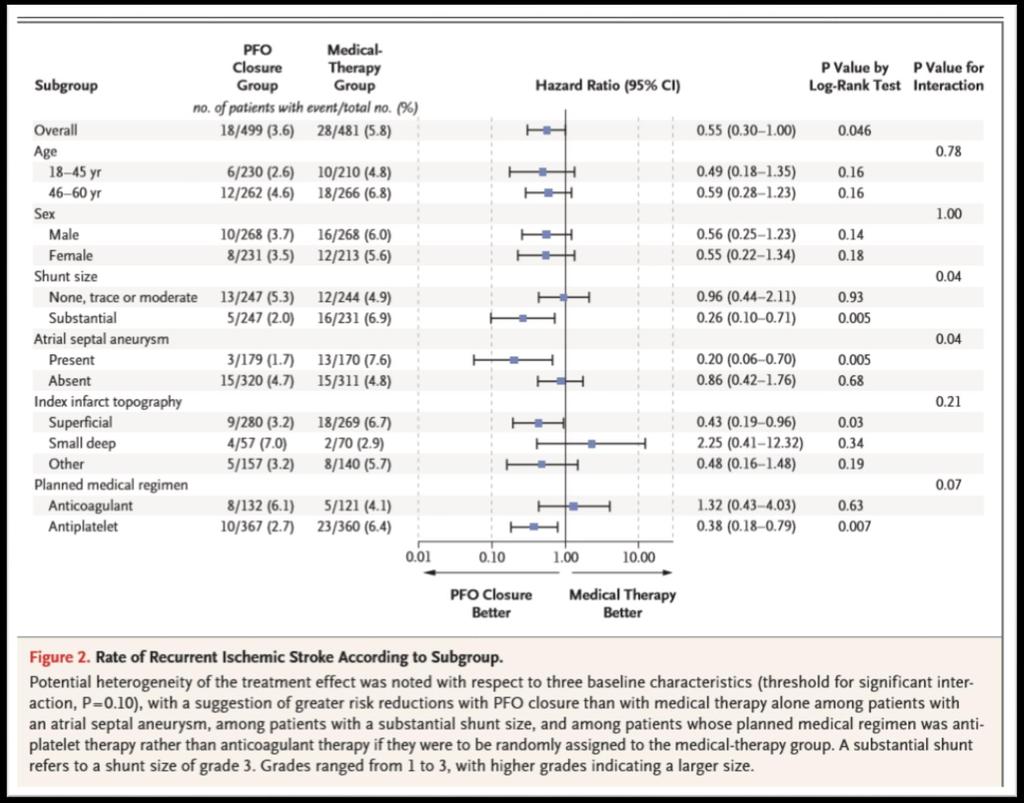
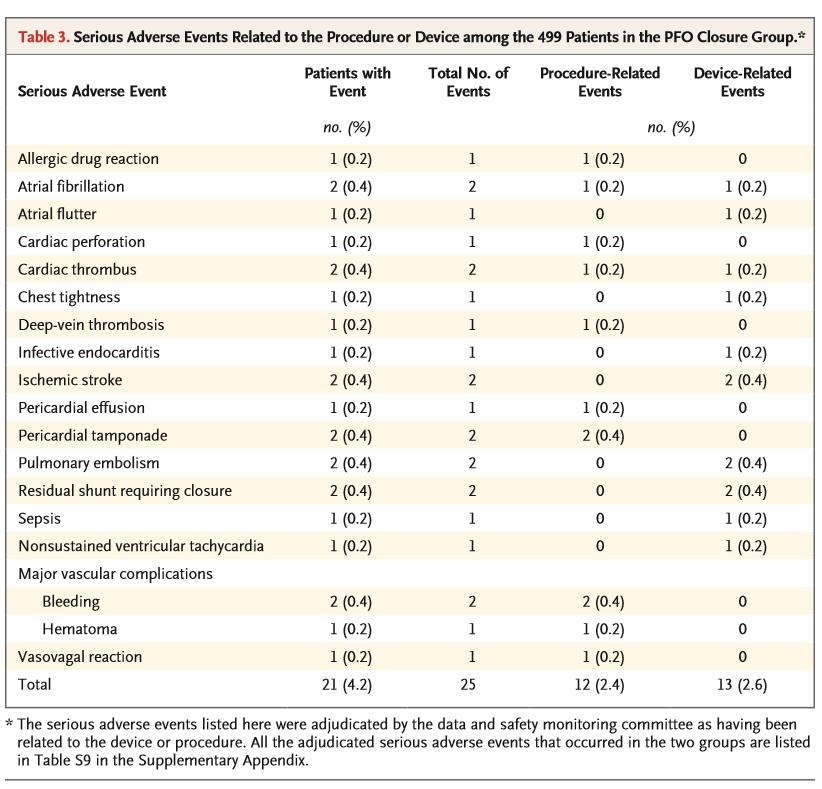
56 RESPECT Long Term Outcomes of Patent Foramen Ovale Closure or Medical Therapy after Stroke Multicenter, randomized, open label trial Patients 18 to 60 years of age who had a patent foramen ovale (PFO) and had had a cryptogenic ischemic stroke to undergo closure of the PFO or to receive medical therapy alone (aspirin, warfarin, clopidogrel, or aspirin combined with extended release dipyridamole at the discretion of physician). The primary efficacy end point was a composite of recurrent nonfatal ischemic stroke, fatal ischemic stroke, or early death after randomization. Saver et al. NEJM ;11:1022
57 PATIENT SELECTION 980 patients (mean age, 45.9 years) at 69 sites Follow up for a median of 5.9 years. Recurrent ischemic stroke of undetermined cause occurred in 10 patients in the PFO closure group and in 23 patients in the medical therapy group Hazard ratio, 0.38; P = 0.007
58
59
60
61 CONCLUSIONS FROM RESPECT PFO CLOSURE WITH THE USE OF AMPLATZER PFO OCCLUDER WAS ASSOCIATED WITH A LOWER RATE OF RECURRENT ISCHEMIC STROKES THAN MEDICAL THERAPY ALONE DURING EXTENDED FOLLOW UP PERIOD
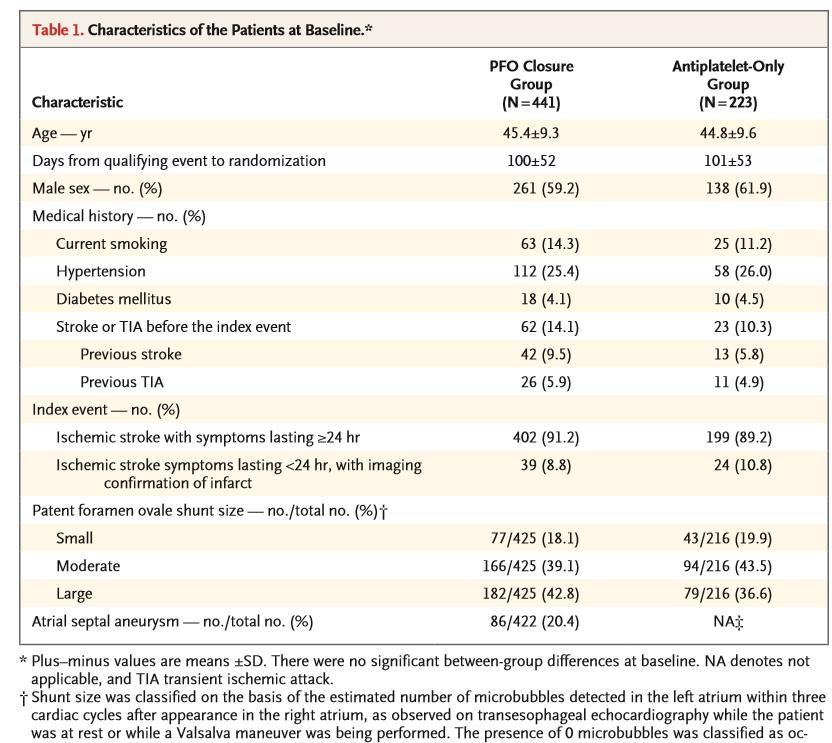
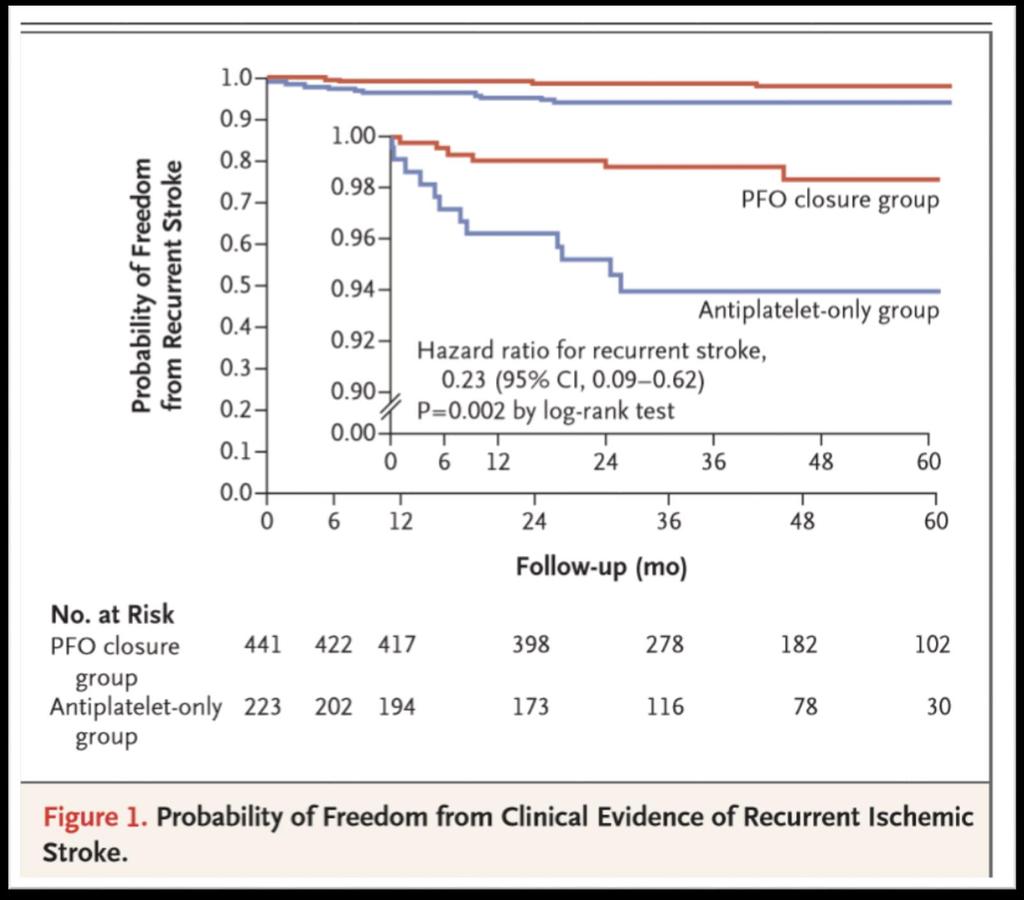
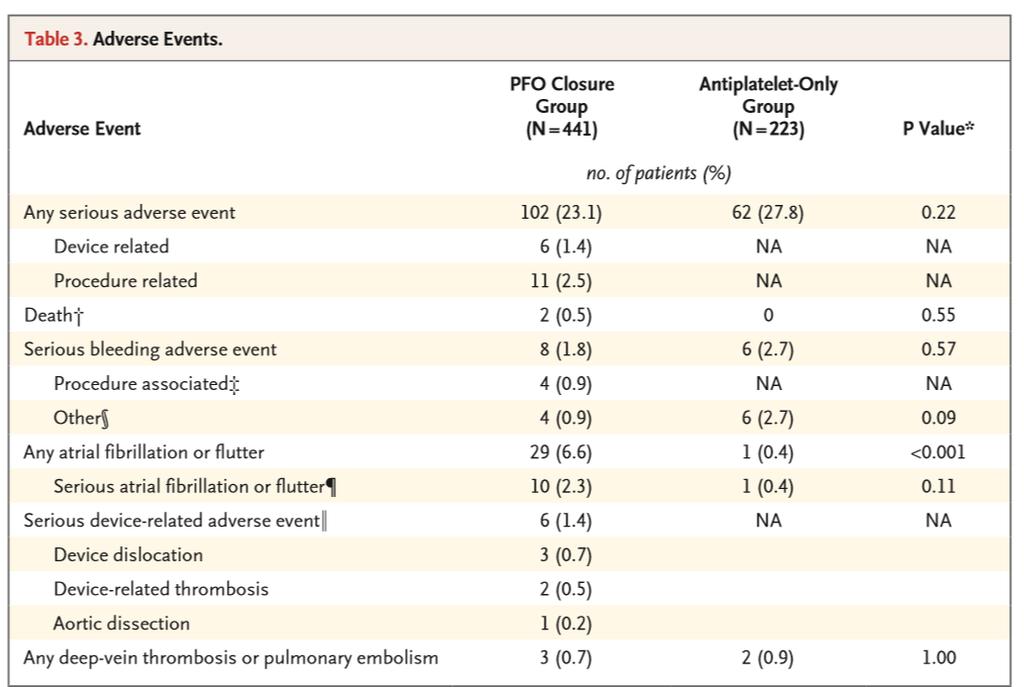
62 REDUCE Patent Foramen Ovale Closure or Antiplatelet Therapy for Cryptogenic Stroke Multinational, randomized trial using Gore Helex/ Gore Cardioform Device Randomly assigned patients, in a 2:1 ratio, to undergo PFO closure plus antiplatelet therapy (PFO closure group) or to receive antiplatelet therapy alone (antiplatelet-only group) Imaging of the brain was performed at the baseline screening and at 24 months 664 patients (mean age, 45.2 years) Median follow-up of 3.2 years (min 2 years and max 5 years) Coprimary end points were freedom from clinical evidence of ischemic and 24-month incidence of new brain infarction (composite clinical and silent with + imaging). Sondergaard et al. NEJM ; 11: 1033

63
64

65 Complete closure of PFO was achieved in 75% of patients by 12 months
66
67 CONCLUSIONS FROM REDUCE Among patients with a PFO who had had a cryptogenic stroke, the risk of subsequent ischemic stroke was lower among those assigned to PFO closure combined with antiplatelet therapy than among those assigned to antiplatelet therapy alone. PFO closure (with Helex device) was associated with higher rates of atrial fibrillation
68 WHY ARE THE RECENT TRIALS POSITIVE? Required more stringent inclusion/exclusion criteria Neuroimaging requirements Longer follow up In CLOSE, patients were required to have a large interatrial shunt at rest or an atrial septal aneurysm There were ZERO strokes in the PFO closure arm REDUCE allowed patients with moderate shunting Application of RoPE score for stratification of risk of paradoxical embolism Clinically useful tool: ensuring PFO is the cause of stroke and not just a dx of exclusion Of note, size/severity of shunting are not part of the score Ropper et al. NEJM ; 11: 1093

69 FDA APPROVAL OF PFO CLOSURE DEVICE: AMPLATZER PFO OCCLUDER

: 55")
70 MacCarthy et al. CIT 2017; 11(3): 55
71 CONSIDERATION FOR EXCLUSIONS TO DEVICE CLOSURE VTE provoked by a known event or an identifiable transient risk factor treated with anticoagulation for 3 to 12 months PFO device closure can be postponed until anticoagulation is stopped May have an indication for chronic anticoagulation (e.g., unprovoked or recurrent deep venous thrombosis) Other considerations to percutaneous device closure include the presence of an inferior vena cava filter, elevated bleeding risk or coagulopathy, and vascular, cardiac, or PFO anatomy that is unsuitable for device placement.
72 CLINICAL PRACTICE UPDATE PFO closure is superior to medical therapy in patient <60 years of age presenting with embolic stroke secondary to PFO demonstrated by imaging and after extensive work up excluding other potential causes of ischemic stroke PFO closure is advised in addition to antiplatelet therapy for secondary stroke prevention
73 CONCLUSIONS Recent RCTs consistently demonstrate that device closure of a PFO plus antiplatelet therapy is more effective than antiplatelet therapy alone for preventing recurrent ischemic stroke Absolute risk reductions ranging from 2.2 to 6 %. Medical therapy alone is not adequate for secondary prevention of stroke Patient selection is critical RoPE score Device associated increase in post procedural AF in short term follow up that has unclear clinical significance
74 QUESTIONS?
Rahul Jhaveri, M.D. The Heart Group of Lancaster General Health
 Rahul Jhaveri, M.D. The Heart Group of Lancaster General Health INTRODUCTION Three recently published randomized controlled trials in The New England Journal of Medicine provide new information about closure
Rahul Jhaveri, M.D. The Heart Group of Lancaster General Health INTRODUCTION Three recently published randomized controlled trials in The New England Journal of Medicine provide new information about closure
PFO Management update
 PFO Management update May 12, 2017 Peter Casterella, MD Swedish Heart and Vascular 1 PFO Update 2017: Objectives Review recently released late outcomes of RESPECT trial and subsequent FDA approval of PFO
PFO Management update May 12, 2017 Peter Casterella, MD Swedish Heart and Vascular 1 PFO Update 2017: Objectives Review recently released late outcomes of RESPECT trial and subsequent FDA approval of PFO
Patent Foramen Ovale and Cryptogenic Stroke: Do We Finally Have Closure? Christopher Streib, MD, MS
 Patent Foramen Ovale and Cryptogenic Stroke: Do We Finally Have Closure? Christopher Streib, MD, MS 11-8-18 Outline 1. Background 2. Anatomy of patent foramen ovale (PFO) 3. Relationship between PFO and
Patent Foramen Ovale and Cryptogenic Stroke: Do We Finally Have Closure? Christopher Streib, MD, MS 11-8-18 Outline 1. Background 2. Anatomy of patent foramen ovale (PFO) 3. Relationship between PFO and
Percutaneous closure of a patent foramen ovale after cryptogenic stroke
 Neth Heart J (2018) 26:5 12 https://doi.org/10.1007/s12471-017-1063-3 POINT OF VIEW Percutaneous closure of a patent foramen ovale after cryptogenic stroke R. J. R. Snijder 1 M.J.Suttorp 1 J.M.tenBerg
Neth Heart J (2018) 26:5 12 https://doi.org/10.1007/s12471-017-1063-3 POINT OF VIEW Percutaneous closure of a patent foramen ovale after cryptogenic stroke R. J. R. Snijder 1 M.J.Suttorp 1 J.M.tenBerg
Why Treat Patent Forman Ovale
 Why Treat Patent Forman Ovale Clifford J Kavinsky, MD, PHD Professor of Medicine and pediatrics Associate Director, Center for Congenital and Structural Heart Disease Rush University Medical Center Conclusions
Why Treat Patent Forman Ovale Clifford J Kavinsky, MD, PHD Professor of Medicine and pediatrics Associate Director, Center for Congenital and Structural Heart Disease Rush University Medical Center Conclusions
CPAG Summary Report for Clinical Panel Patent Foramen Ovale Closure for Secondary Prevention of Cryptogenic Stroke
 MANAGEMENT IN CONFIDENCE CPAG Summary Report for Clinical Panel Patent Foramen Ovale Closure for Secondary Prevention of Cryptogenic Stroke The Benefits of the Proposition Percutaneous Patent Foramen Ovale
MANAGEMENT IN CONFIDENCE CPAG Summary Report for Clinical Panel Patent Foramen Ovale Closure for Secondary Prevention of Cryptogenic Stroke The Benefits of the Proposition Percutaneous Patent Foramen Ovale
CLOSE. Closure of Patent Foramen Ovale, Oral anticoagulants or Antiplatelet Therapy to Prevent Stroke Recurrence
 CLOSE Closure of Patent Foramen Ovale, Oral anticoagulants or Antiplatelet Therapy to Prevent Stroke Recurrence Guillaume TURC, MD, PhD Paris Descartes University Sainte-Anne hospital Paris, France On
CLOSE Closure of Patent Foramen Ovale, Oral anticoagulants or Antiplatelet Therapy to Prevent Stroke Recurrence Guillaume TURC, MD, PhD Paris Descartes University Sainte-Anne hospital Paris, France On
Patent Foramen Ovale: Diagnosis and Treatment
 Patent Foramen Ovale: Diagnosis and Treatment Anthony DeMaria Judy and Jack White Chair in Cardiology University of California, San Diego At one time or another a Grantee, Sponsored Speaker or Ad-hoc Consultant
Patent Foramen Ovale: Diagnosis and Treatment Anthony DeMaria Judy and Jack White Chair in Cardiology University of California, San Diego At one time or another a Grantee, Sponsored Speaker or Ad-hoc Consultant
I, (Issam Moussa) DO NOT have a financial interest/arrangement t/ t or affiliation with one or more organizations that could be perceived as a real
 DO NOT have a financial interest/arrangement t/ t or affiliation with one or more organizations that could be perceived as a real") PFO Closure: Where We Are Going to after CLOSURE I Study? Issam D. Moussa, MD Professor of Medicine Chair, Division of Cardiovascular Diseases Mayo Clinic Jacksonville, Florida Disclosure Statement of
PFO Closure: Where We Are Going to after CLOSURE I Study? Issam D. Moussa, MD Professor of Medicine Chair, Division of Cardiovascular Diseases Mayo Clinic Jacksonville, Florida Disclosure Statement of
Cryptogenic Stroke: What Don t We Know. Siddharth Sehgal, MD Medical Director, TMH Stroke Center Tallahassee Memorial Healthcare
 Cryptogenic Stroke: What Don t We Know Siddharth Sehgal, MD Medical Director, TMH Stroke Center Tallahassee Memorial Healthcare Financial Disclosures None Objectives Principles of diagnostic evaluation
Cryptogenic Stroke: What Don t We Know Siddharth Sehgal, MD Medical Director, TMH Stroke Center Tallahassee Memorial Healthcare Financial Disclosures None Objectives Principles of diagnostic evaluation
PFO closure group total no. PFO closure group no. of males
 Suppl Table. Characteristics of the five trials included in this meta-analysis. Trial name Device used for Definition of medical Primary Endpoint group total no. group no. of males group age (yrs) group
Suppl Table. Characteristics of the five trials included in this meta-analysis. Trial name Device used for Definition of medical Primary Endpoint group total no. group no. of males group age (yrs) group
Patent foramen ovale (PFO) is composed of
 is composed of") PFO Closure for Prevention of Recurrent Cryptogenic Stroke The evidence base is here. BY JOHN F. RHODES, JR, MD Patent foramen ovale (PFO) is composed of overlapping portions of septum primum and septum
PFO Closure for Prevention of Recurrent Cryptogenic Stroke The evidence base is here. BY JOHN F. RHODES, JR, MD Patent foramen ovale (PFO) is composed of overlapping portions of septum primum and septum
GERIATRICS CASE PRESENTATION
 GERIATRICS CASE PRESENTATION CASE 79 year old Patient X was admitted to hospital with SOB. He had a hx of sarcoidosis and asbestosis. Home oxygen requirement is 3-3.5litre. He was admitted, given ceftriaxone
GERIATRICS CASE PRESENTATION CASE 79 year old Patient X was admitted to hospital with SOB. He had a hx of sarcoidosis and asbestosis. Home oxygen requirement is 3-3.5litre. He was admitted, given ceftriaxone
DEBATE: PFO MANAGEMENT TO CLOSE OR NOT TO CLOSE. Matthew Starr, MD Stroke Attending
 DEBATE: PFO MANAGEMENT TO CLOSE OR NOT TO CLOSE Matthew Starr, MD Stroke Attending DISCLOSURES None DEBATE Should PFO be closed? * * Sometimes yes THE CASE AGAINST PFO CLOSURE 1. Did the PFO cause the
DEBATE: PFO MANAGEMENT TO CLOSE OR NOT TO CLOSE Matthew Starr, MD Stroke Attending DISCLOSURES None DEBATE Should PFO be closed? * * Sometimes yes THE CASE AGAINST PFO CLOSURE 1. Did the PFO cause the
PFO (Patent Foramen Ovale): Smoking Gun or an Innocent Bystander?
: Smoking Gun or an Innocent Bystander?") PFO (Patent Foramen Ovale): Smoking Gun or an Innocent Bystander? J Thompson Sullebarger, M.D. Florida Cardiovascular Institute University of South Florida Kris Letang Tedy Bruschi Bret Michaels The Atrial
PFO (Patent Foramen Ovale): Smoking Gun or an Innocent Bystander? J Thompson Sullebarger, M.D. Florida Cardiovascular Institute University of South Florida Kris Letang Tedy Bruschi Bret Michaels The Atrial
Transcatheter Closure of Septal Defects
 Transcatheter Closure of Septal Defects Policy Number: 2.02.09 Last Review: 11/2018 Origination: 3/2007 Next Review: 11/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage
Transcatheter Closure of Septal Defects Policy Number: 2.02.09 Last Review: 11/2018 Origination: 3/2007 Next Review: 11/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage
Cryptogenic Stroke/PFO with Thrombophilia and VTE: Do We Know What To Do?
 Cryptogenic Stroke/PFO with Thrombophilia and VTE: Do We Know What To Do? Robert J. Sommer, MD Columbia University Medical Center New York, NY Disclosure Statement of Financial Interest Within the past
Cryptogenic Stroke/PFO with Thrombophilia and VTE: Do We Know What To Do? Robert J. Sommer, MD Columbia University Medical Center New York, NY Disclosure Statement of Financial Interest Within the past
Cryptogenic Stroke: A logical approach to a common clinical problem
 Cryptogenic Stroke: A logical approach to a common clinical problem Alphonse M. Ambrosia, DO, FACC Interventional Cardiologist CardioVascular Associates of Mesa Mesa, Arizona Speakers Bureau Boston Scientific
Cryptogenic Stroke: A logical approach to a common clinical problem Alphonse M. Ambrosia, DO, FACC Interventional Cardiologist CardioVascular Associates of Mesa Mesa, Arizona Speakers Bureau Boston Scientific
Index. cardiology.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute ischemic stroke TOAST classification of, 270 Acute myocardial infarction (AMI) cardioembolic stroke following, 207 208 noncardioembolic
Index Note: Page numbers of article titles are in boldface type. A Acute ischemic stroke TOAST classification of, 270 Acute myocardial infarction (AMI) cardioembolic stroke following, 207 208 noncardioembolic
Fabien Praz, Andreas Wahl, Sophie Beney, Stephan Windecker, Heinrich P. Mattle*, Bernhard Meier
 Procedural Outcome after Percutaneous Closure of Patent Foramen Ovale using the Amplatzer PFO Occluder Without Intra-Procedural Echocardiography in 1,000 Patients Fabien Praz, Andreas Wahl, Sophie Beney,
Procedural Outcome after Percutaneous Closure of Patent Foramen Ovale using the Amplatzer PFO Occluder Without Intra-Procedural Echocardiography in 1,000 Patients Fabien Praz, Andreas Wahl, Sophie Beney,
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Stroke and ASA / FO REBUTTAL
 REBUTTAL Definition of an ischemic stroke Definition of a PFO Evidence for a causal role of PFO in stroke Evidence against a role of PFO in stroke Stroke recurrencies in stroke (PFO) patients Medical treatment
REBUTTAL Definition of an ischemic stroke Definition of a PFO Evidence for a causal role of PFO in stroke Evidence against a role of PFO in stroke Stroke recurrencies in stroke (PFO) patients Medical treatment
Speakers. 2015, American Heart Association 1
 Speakers Lee Schwamm, MD, FAHA Executive Vice Chairman of Neurology, Massachusetts General Hospital Director, Stroke Service and Medical Director, MGH TeleHealth, Massachusetts General Hospital Director,
Speakers Lee Schwamm, MD, FAHA Executive Vice Chairman of Neurology, Massachusetts General Hospital Director, Stroke Service and Medical Director, MGH TeleHealth, Massachusetts General Hospital Director,
Effect of Having a PFO Occlusion Device in Place in the RESPECT PFO Closure Trial
 Effect of Having a PFO Occlusion Device in Place in the RESPECT PFO Closure Trial DAVID E. THALER, MD, PHD, JEFFREY L. SAVER, MD RICHARD W. SMALLING, MD, PHD, JOHN D. CARROLL, MD, SCOTT BERRY, PHD, LEE
Effect of Having a PFO Occlusion Device in Place in the RESPECT PFO Closure Trial DAVID E. THALER, MD, PHD, JEFFREY L. SAVER, MD RICHARD W. SMALLING, MD, PHD, JOHN D. CARROLL, MD, SCOTT BERRY, PHD, LEE
Current management aspects in adult congenital heart disease: non-surgical closure of patent foramen ovale
 Review Article Current management aspects in adult congenital heart disease: non-surgical closure of patent foramen ovale Kaivan Vaidya 1,2, Chinmay Khandkar 1,2, David Celermajer 1,2 1 Department of Cardiology,
Review Article Current management aspects in adult congenital heart disease: non-surgical closure of patent foramen ovale Kaivan Vaidya 1,2, Chinmay Khandkar 1,2, David Celermajer 1,2 1 Department of Cardiology,
Stroke Case Studies. Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow
 Stroke Case Studies Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow Case 1 64 year old female with dysphasia and right arm weakness 3 hours prior CT head: dense M1 sign. No established ischaemia
Stroke Case Studies Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow Case 1 64 year old female with dysphasia and right arm weakness 3 hours prior CT head: dense M1 sign. No established ischaemia
2017 Cardiovascular Symposium CRYPTOGENIC STROKE: A CARDIOVASCULAR PERSPECTIVE DR. WILLIAM DIXON AND DR. VENKATA BAVAKATI SOUTHERN MEDICAL GROUP, P.A.
 CRYPTOGENIC STROKE: 2017 Cardiovascular Symposium A CARDIOVASCULAR PERSPECTIVE DR. WILLIAM DIXON AND DR. VENKATA BAVAKATI SOUTHERN MEDICAL GROUP, P.A. CRYPTOGENIC STROKE CRYPTOGENIC: OF OBSCURE OR UNKNOWN
CRYPTOGENIC STROKE: 2017 Cardiovascular Symposium A CARDIOVASCULAR PERSPECTIVE DR. WILLIAM DIXON AND DR. VENKATA BAVAKATI SOUTHERN MEDICAL GROUP, P.A. CRYPTOGENIC STROKE CRYPTOGENIC: OF OBSCURE OR UNKNOWN
PFO- To Close for Comfort. By: Vincent J.Caracciolo, MD FACC
 PFO- To Close for Comfort By: Vincent J.Caracciolo, MD FACC PATENT FORAMEN OVALE PFO- congenital lesion that frequently persists into adulthood ( 25-30%)- autopsy and TEE studies. PFO prevalence higher
PFO- To Close for Comfort By: Vincent J.Caracciolo, MD FACC PATENT FORAMEN OVALE PFO- congenital lesion that frequently persists into adulthood ( 25-30%)- autopsy and TEE studies. PFO prevalence higher
Description. Page: 1 of 23. Closure Devices for Patent Foramen Ovale and Atrial Septal Defects. Last Review Status/Date: December 2014
 Last Review Status/Date: December 2014 Page: 1 of 23 Description Background Patent Foramen Ovale The foramen ovale, a component of fetal cardiovascular circulation, consists of a communication between
Last Review Status/Date: December 2014 Page: 1 of 23 Description Background Patent Foramen Ovale The foramen ovale, a component of fetal cardiovascular circulation, consists of a communication between
PERCUTANEOUS CLOSURE OF PATENT FORAMEN OVALE AND ATRIAL SEPTAL DEFECT: STATE OF THE ART AND A CRITICAL APPRAISAL
 PERCUTANEOUS CLOSURE OF PATENT FORAMEN OVALE AND ATRIAL SEPTAL DEFECT: STATE OF THE ART AND A CRITICAL APPRAISAL Carmelo Cernigliaro Clinica San Gaudenzio Novara Eco 2D e 3D Eco Transesofageo Large shunt
PERCUTANEOUS CLOSURE OF PATENT FORAMEN OVALE AND ATRIAL SEPTAL DEFECT: STATE OF THE ART AND A CRITICAL APPRAISAL Carmelo Cernigliaro Clinica San Gaudenzio Novara Eco 2D e 3D Eco Transesofageo Large shunt
Management and Investigation of Ischemic Stroke By Etiology
 Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
Cryptogenic Strokes: Evaluation and Management
 Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
Why Should We Treat PFO?
 Why Should We Treat PFO? SCAI Interventional Cardiology Fellows Course December 7, 2012 Jonathan Tobis, MD Director of Interventional Cardiology UCLA Disclosures Jonathan Tobis, MD 1. A Principal Investigator
Why Should We Treat PFO? SCAI Interventional Cardiology Fellows Course December 7, 2012 Jonathan Tobis, MD Director of Interventional Cardiology UCLA Disclosures Jonathan Tobis, MD 1. A Principal Investigator
Transcatheter Closure of Cardiovascular Defects
 Medical Coverage Policy Effective Date...11/15/2017 Next Review Date...11/15/2018 Coverage Policy Number... 0011 Transcatheter Closure of Cardiovascular Defects Table of Contents Related Coverage Resources
Medical Coverage Policy Effective Date...11/15/2017 Next Review Date...11/15/2018 Coverage Policy Number... 0011 Transcatheter Closure of Cardiovascular Defects Table of Contents Related Coverage Resources
RESPECT Safety Findings
 CO-1 SCAI Town Hall Meeting Monday, October 31, 2016 Washington, DC RESPECT Safety Findings John D. Carroll, M.D., MSCAI Professor of Medicine Cardiology University of Colorado School of Medicine University
CO-1 SCAI Town Hall Meeting Monday, October 31, 2016 Washington, DC RESPECT Safety Findings John D. Carroll, M.D., MSCAI Professor of Medicine Cardiology University of Colorado School of Medicine University
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
PFO Closure for the Management of Migraine and Stroke
 PFO Closure for the Management of Migraine and Stroke Sun U. Kwon Department of Neurology, Asan Medical Center, UUMC Contents PFO & Migraine PFO causes Migraine or Not? PFO closure for Migraine PFO & Stroke
PFO Closure for the Management of Migraine and Stroke Sun U. Kwon Department of Neurology, Asan Medical Center, UUMC Contents PFO & Migraine PFO causes Migraine or Not? PFO closure for Migraine PFO & Stroke
In October 2016, the US Food and Drug Administration
 The Approval of PFO Closure in the United States A look back at the long road to FDA approval and the implications on patient care options going forward. By Marie-France Poulin, MD, and Clifford J. Kavinsky,
The Approval of PFO Closure in the United States A look back at the long road to FDA approval and the implications on patient care options going forward. By Marie-France Poulin, MD, and Clifford J. Kavinsky,
Clinical Commissioning Policy Statement: Patent Foramen Ovale (PFO) Closure. April Reference: NHSCB/A09/PS/a
 Closure. April Reference: NHSCB/A09/PS/a") Clinical Commissioning Policy Statement: Patent Foramen Ovale (PFO) Closure April 2013 Reference: NHSCB/A09/PS/a NHS Commissioning Board Clinical Commissioning Policy Statement: Patent Foramen Ovale (PFO)
Clinical Commissioning Policy Statement: Patent Foramen Ovale (PFO) Closure April 2013 Reference: NHSCB/A09/PS/a NHS Commissioning Board Clinical Commissioning Policy Statement: Patent Foramen Ovale (PFO)
Devices for Stroke Prevention. Douglas Ebersole, MD Interventional Cardiology Watson Clinic LLP
 Devices for Stroke Prevention Douglas Ebersole, MD Interventional Cardiology Watson Clinic LLP Overview Left Atrial Appendage Closure FDA Approved Watchman Investigational Amulet PFO Closure Atrial Fibrillation
Devices for Stroke Prevention Douglas Ebersole, MD Interventional Cardiology Watson Clinic LLP Overview Left Atrial Appendage Closure FDA Approved Watchman Investigational Amulet PFO Closure Atrial Fibrillation
Transcatheter Closure of Septal Defects
 Transcatheter Closure of Septal Defects Policy Number: 2.02.09 Last Review: 11/2017 Origination: 3/2007 Next Review: 11/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage
Transcatheter Closure of Septal Defects Policy Number: 2.02.09 Last Review: 11/2017 Origination: 3/2007 Next Review: 11/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage
Stroke 101. Maine Cardiovascular Health Summit. Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013
 Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
What the general cardiologist should know about arrhythmia Stroke prevention in AF" Peter Ammann Kantonsspital St. Gallen
 What the general cardiologist should know about arrhythmia Stroke prevention in AF" Peter Ammann Kantonsspital St. Gallen What the cardiologist should know about arrhythmia and stroke are there real low
What the general cardiologist should know about arrhythmia Stroke prevention in AF" Peter Ammann Kantonsspital St. Gallen What the cardiologist should know about arrhythmia and stroke are there real low
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
AVC Criptogénico: Está na altura de alterar as guidelines? Claudia Jorge University Hospital of Santa Maria
 Está na altura de alterar as guidelines? Claudia Jorge University Hospital of Santa Maria Está na altura de alterar as guidelines? Está na altura de alterar as guidelines? ~25% of all ischemic strokes
Está na altura de alterar as guidelines? Claudia Jorge University Hospital of Santa Maria Está na altura de alterar as guidelines? Está na altura de alterar as guidelines? ~25% of all ischemic strokes
MEET 2007: Evaluation and treatment of the stroke and TIA patient for the non-neurointerventionist. neurointerventionist
 MEET 2007: Evaluation and treatment of the stroke and TIA patient for the non-neurointerventionist neurointerventionist Steve Ramee, MD Ochsner Medical Center New Orleans DISCLOSURE Nothing Nothing to
MEET 2007: Evaluation and treatment of the stroke and TIA patient for the non-neurointerventionist neurointerventionist Steve Ramee, MD Ochsner Medical Center New Orleans DISCLOSURE Nothing Nothing to
Transcatheter closure of patent foramen ovale using the internal jugular venous approach
 New methods in diagnosis and therapy Transcatheter closure of patent foramen ovale using the internal jugular venous approach Przemysław Węglarz 1,2, Ewa Konarska-Kuszewska 2, Tadeusz Zębik 2, Piotr Kuszewski
New methods in diagnosis and therapy Transcatheter closure of patent foramen ovale using the internal jugular venous approach Przemysław Węglarz 1,2, Ewa Konarska-Kuszewska 2, Tadeusz Zębik 2, Piotr Kuszewski
Update interventional Cardiology Hans Rickli St.Gallen
 Update interventional Cardiology 2012 Hans Rickli St.Gallen 26.11.2012 Review of Literature ESC-Highlights TCT/AHA-Highlights Update interventional cardiology 2012 Structural Heart Disease Transcatheter
Update interventional Cardiology 2012 Hans Rickli St.Gallen 26.11.2012 Review of Literature ESC-Highlights TCT/AHA-Highlights Update interventional cardiology 2012 Structural Heart Disease Transcatheter
Qualifying and Outcome Strokes in the RESPECT PFO Trial: Additional Evidence of Treatment Effect
 Qualifying and Outcome Strokes in the RESPECT PFO Trial: Additional Evidence of Treatment Effect JEFFREY L. SAVER, MD DAVID E. THALER, MD, PHD, RICHARD W. SMALLING, MD, PHD, JOHN D. CARROLL, MD, SCOTT
Qualifying and Outcome Strokes in the RESPECT PFO Trial: Additional Evidence of Treatment Effect JEFFREY L. SAVER, MD DAVID E. THALER, MD, PHD, RICHARD W. SMALLING, MD, PHD, JOHN D. CARROLL, MD, SCOTT
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Andrew Barreto, MD MS Associate Professor of Neurology Stroke Neurologist UTHealth. May 23, 2018
 Andrew Barreto, MD MS Associate Professor of Neurology Stroke Neurologist UTHealth May 23, 2018 Disclosure No personal financial relationships with any company. Presentation Outline Definitions, signs
Andrew Barreto, MD MS Associate Professor of Neurology Stroke Neurologist UTHealth May 23, 2018 Disclosure No personal financial relationships with any company. Presentation Outline Definitions, signs
INSTRUCTIONS FOR USE FOR:
 INSTRUCTIONS FOR USE FOR: en English bg INSTRUCTIONS FOR USE FOR: GORE CARDIOFORM SEPTAL OCCLUDER Carefully read all instructions prior to use. Observe all warnings and precautions noted throughout these
INSTRUCTIONS FOR USE FOR: en English bg INSTRUCTIONS FOR USE FOR: GORE CARDIOFORM SEPTAL OCCLUDER Carefully read all instructions prior to use. Observe all warnings and precautions noted throughout these
STROKE UPDATE ANTHEA PARRY MAY 2010
 STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
Occlusion de l'auricule gauche: Niche ou réel avenir? D Gras, MD, Nantes, France
 Occlusion de l'auricule gauche: Niche ou réel avenir? D Gras, MD, Nantes, France LAA Occlusion Is there a real future? Background Protect AF Trial Other Studies CAP, ASAP, Prevail Left Atrial Appendage
Occlusion de l'auricule gauche: Niche ou réel avenir? D Gras, MD, Nantes, France LAA Occlusion Is there a real future? Background Protect AF Trial Other Studies CAP, ASAP, Prevail Left Atrial Appendage
Is Stroke Frequency Declining?
 Is Stroke Frequency Declining? Etiologic Factors Clinical, Anatomic, Technique-related, and Device-specific Samir Kapadia, MD Professor of Medicine Section head, Interventional Cardiology Director, Cardiac
Is Stroke Frequency Declining? Etiologic Factors Clinical, Anatomic, Technique-related, and Device-specific Samir Kapadia, MD Professor of Medicine Section head, Interventional Cardiology Director, Cardiac
Clinical Policy: Transcatheter Closure of Patent Foramen Ovale Reference Number: CP.MP.151
 Clinical Policy: Reference Number: CP.MP.151 Effective Date: 12/17 Last Review Date: 12/17 See Important Reminder at the end of this policy for important regulatory and legal information. Coding Implications
Clinical Policy: Reference Number: CP.MP.151 Effective Date: 12/17 Last Review Date: 12/17 See Important Reminder at the end of this policy for important regulatory and legal information. Coding Implications
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase <48h)
") Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
ΣΥΓΚΛΕΙΣΗ ΑΝΟΙΚΤΟΥ ΩΟΕΙΔΟΥΣ ΤΡΗΜΑΤΟΣ ΠΕΣΡΟ. ΔΑΡΔΑ, MD, FESC 33 Ο Πανελλήνιο Καρδιολογικό Συνζδριο ΑΘΗΝΑ 2012
 ΣΥΓΚΛΕΙΣΗ ΑΝΟΙΚΤΟΥ ΩΟΕΙΔΟΥΣ ΤΡΗΜΑΤΟΣ 2012 ΠΕΣΡΟ. ΔΑΡΔΑ, MD, FESC 33 Ο Πανελλήνιο Καρδιολογικό Συνζδριο ΑΘΗΝΑ 2012 The Problem: Not All PFO in Patients With Cryptogenic Stroke is Pathogenic; No Definitive
ΣΥΓΚΛΕΙΣΗ ΑΝΟΙΚΤΟΥ ΩΟΕΙΔΟΥΣ ΤΡΗΜΑΤΟΣ 2012 ΠΕΣΡΟ. ΔΑΡΔΑ, MD, FESC 33 Ο Πανελλήνιο Καρδιολογικό Συνζδριο ΑΘΗΝΑ 2012 The Problem: Not All PFO in Patients With Cryptogenic Stroke is Pathogenic; No Definitive
Sex Differences in Stroke Risk and Quality of Life after Stroke
 Sex Differences in Stroke Risk and Quality of Life after Stroke Cheryl Bushnell, MD, MHS Associate Professor of Neurology Director, WFB Stroke Center Disclosures Research funding from: World Federation
Sex Differences in Stroke Risk and Quality of Life after Stroke Cheryl Bushnell, MD, MHS Associate Professor of Neurology Director, WFB Stroke Center Disclosures Research funding from: World Federation
APPENDIX A NORTH AMERICAN SYMPTOMATIC CAROTID ENDARTERECTOMY TRIAL
 APPENDIX A Primary Findings From Selected Recent National Institute of Neurological Disorders and Stroke-Sponsored Clinical Trials That Have shaped Modern Stroke Prevention Philip B. Gorelick 178 NORTH
APPENDIX A Primary Findings From Selected Recent National Institute of Neurological Disorders and Stroke-Sponsored Clinical Trials That Have shaped Modern Stroke Prevention Philip B. Gorelick 178 NORTH
True cryptogenic stroke
 True cryptogenic stroke Arne Lindgren, MD, PhD Dept of Clinical Sciences Lund, Neurology, Lund University Dept of Neurology and Rehabilitation Medicine Skåne University Hospital Lund, Sweden Disclosures
True cryptogenic stroke Arne Lindgren, MD, PhD Dept of Clinical Sciences Lund, Neurology, Lund University Dept of Neurology and Rehabilitation Medicine Skåne University Hospital Lund, Sweden Disclosures
The Epidemiology of Stroke and Vascular Risk Factors in Cognitive Aging
 The Epidemiology of Stroke and Vascular Risk Factors in Cognitive Aging REBECCA F. GOTTESMAN, MD PHD ASSOCIATE PROFESSOR OF NEUROLOGY AND EPIDEMIOLOGY JOHNS HOPKINS UNIVERSITY OCTOBER 20, 2014 Outline
The Epidemiology of Stroke and Vascular Risk Factors in Cognitive Aging REBECCA F. GOTTESMAN, MD PHD ASSOCIATE PROFESSOR OF NEUROLOGY AND EPIDEMIOLOGY JOHNS HOPKINS UNIVERSITY OCTOBER 20, 2014 Outline
11/27/2017 DISCLOSURE CRYPTOGENIC STROKE CLINICAL PATHWAYS. No Relevant Financial Disclosures Sub-Investigator LEARNING OBJECTIVES
 CRYPTOGENIC STROKE CLINICAL PATHWAYS Michelle Lee Kearney, ACNP-BC NP, Stroke Program St Thomas Health Nashville, TN DISCLOSURE No Relevant Financial Disclosures Sub-Investigator Stroke-AF Trial (Medtronic)
CRYPTOGENIC STROKE CLINICAL PATHWAYS Michelle Lee Kearney, ACNP-BC NP, Stroke Program St Thomas Health Nashville, TN DISCLOSURE No Relevant Financial Disclosures Sub-Investigator Stroke-AF Trial (Medtronic)
Evidence Based Stroke Update Ajay Bhalla Guy s and St Thomas Hospitals UK Stroke Forum
 Evidence Based Stroke Update 2017 Ajay Bhalla Guy s and St Thomas Hospitals UK Stroke Forum Future is hard to predict.. Future is hard to predict.. Future is hard to predict.. Future is hard to predict..
Evidence Based Stroke Update 2017 Ajay Bhalla Guy s and St Thomas Hospitals UK Stroke Forum Future is hard to predict.. Future is hard to predict.. Future is hard to predict.. Future is hard to predict..
Practical Considerations in the Early Treatment of Acute Stroke
 Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Antithrombotic Summit Basel 2012 Basel, 26. April Peter T. Buser Klinik Kardiologie Unviersitätsspital Basel
 Antithrombotic Summit Basel 2012 Basel, 26. April 2012 Peter T. Buser Klinik Kardiologie Unviersitätsspital Basel Background stroke = third-leading cause of death among adults 1/5 of stroke survivors require
Antithrombotic Summit Basel 2012 Basel, 26. April 2012 Peter T. Buser Klinik Kardiologie Unviersitätsspital Basel Background stroke = third-leading cause of death among adults 1/5 of stroke survivors require
ACUTE CENTRAL PERIFERALEMBOLISM
 EAE TEACHING COURSE 2010 Belgrade, Serbia October 22-23, 2010 ACUTE CENTRAL and PERIFERALEMBOLISM Maria João Andrade Lisbon, PT BACKGROUND Stroke is a leading cause of mortality and long-term disability
EAE TEACHING COURSE 2010 Belgrade, Serbia October 22-23, 2010 ACUTE CENTRAL and PERIFERALEMBOLISM Maria João Andrade Lisbon, PT BACKGROUND Stroke is a leading cause of mortality and long-term disability
Nearly 1/3 of men can t recognize even one stroke symptom so they can act FAST and help the women in their lives survive stroke.
 Nearly 1/3 of men can t recognize even one stroke symptom so they can act FAST and help the women in their lives survive stroke. Most people don t know that stroke kills twice as many women as breast cancer
Nearly 1/3 of men can t recognize even one stroke symptom so they can act FAST and help the women in their lives survive stroke. Most people don t know that stroke kills twice as many women as breast cancer
Atrial Septal Defect Closure. Stephen Brecker Director, Cardiac Catheterisation Labs
 Stephen Brecker Director, Cardiac Catheterisation Labs ADVANCED ANGIOPLASTY Incorporating The Left Main 5 Plus Course Conflicts of Interest The following companies have supported educational courses held
Stephen Brecker Director, Cardiac Catheterisation Labs ADVANCED ANGIOPLASTY Incorporating The Left Main 5 Plus Course Conflicts of Interest The following companies have supported educational courses held
2018 Update in Diagnosis and Management of Stroke
 2018 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Chair, Department of Neurology Director,
2018 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Chair, Department of Neurology Director,
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
TIA: Updates and Management 2008
 TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
Migraine and Patent Foramen Ovale (PFO)
") Migraine and Patent Foramen Ovale (PFO) Hans-Christoph Diener Senior Professor of Clinical Neurosciences Department of Neurology and Headache Center University Essen Topics Prevalence of PFO Is migraine
Migraine and Patent Foramen Ovale (PFO) Hans-Christoph Diener Senior Professor of Clinical Neurosciences Department of Neurology and Headache Center University Essen Topics Prevalence of PFO Is migraine
PFO CLOSURE: WHAT S NEW?
 PFO CLOSURE: WHAT S NEW? 1. AHA rescinds major sections of 2018 AHA/ASA Stroke Guidelines 2. PFO closure is cost effective 3. Now 12 meta-analyses of PFO/Stoke RCT confirm PFO closure superiority 4. FDA
PFO CLOSURE: WHAT S NEW? 1. AHA rescinds major sections of 2018 AHA/ASA Stroke Guidelines 2. PFO closure is cost effective 3. Now 12 meta-analyses of PFO/Stoke RCT confirm PFO closure superiority 4. FDA
The Patent Foramen Ovale A Preventable Stroke Etiology?! Brian Whisenant, M.D.
 The Patent Foramen Ovale A Preventable Stroke Etiology?! Brian Whisenant, M.D. Conflict of Interest Statement I have a financial interest in Coherex Medical. Heart Disease and Stroke Statistics 2008 Update:
The Patent Foramen Ovale A Preventable Stroke Etiology?! Brian Whisenant, M.D. Conflict of Interest Statement I have a financial interest in Coherex Medical. Heart Disease and Stroke Statistics 2008 Update:
Long-Term Outcomes of Patent Foramen Ovale Closure or Medical Therapy after Stroke
 The new england journal of medicine Original Article Long-Term Outcomes of Patent Foramen Ovale Closure or Medical Therapy after Stroke Jeffrey L. Saver, M.D., John D. Carroll, M.D., David E. Thaler, M.D.,
The new england journal of medicine Original Article Long-Term Outcomes of Patent Foramen Ovale Closure or Medical Therapy after Stroke Jeffrey L. Saver, M.D., John D. Carroll, M.D., David E. Thaler, M.D.,
Supplementary webappendix
 Supplementary webappendix This webappendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Hart RG, Diener H-C, Coutts SB, et al,
Supplementary webappendix This webappendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Hart RG, Diener H-C, Coutts SB, et al,
Reduce Your Risk of Stroke Starting Now
 Reduce Your Risk of Stroke Starting Now Take steps against recurrent stroke by making the necessary changes in your life. Stroke prevention tips for better health Prevent stroke. Live healthy. You can
Reduce Your Risk of Stroke Starting Now Take steps against recurrent stroke by making the necessary changes in your life. Stroke prevention tips for better health Prevent stroke. Live healthy. You can
Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre
 Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre Objectives To learn what s new in stroke care 2010-11 1) Acute stroke management Carotid artery stenting versus surgery for symptomatic
Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre Objectives To learn what s new in stroke care 2010-11 1) Acute stroke management Carotid artery stenting versus surgery for symptomatic
PFO Closure is a Therapy for Migraine PRO
 PFO Closure is a Therapy for Migraine PRO Andrew Charles, M.D. Professor Director, UCLA Goldberg Migraine Program Meyer and Renee Luskin Chair in Migraine and Headache Studies Director, Headache Research
PFO Closure is a Therapy for Migraine PRO Andrew Charles, M.D. Professor Director, UCLA Goldberg Migraine Program Meyer and Renee Luskin Chair in Migraine and Headache Studies Director, Headache Research
Secondary Stroke Prevention
 Secondary Stroke Prevention Acute stroke conference, Sunnybrook Estates January 20, 2011 Rick Swartz HBSc, MD, PhD, FRCPC Assistant Professor, Department of Medicine, Divisions of Neurology and Obstetrical
Secondary Stroke Prevention Acute stroke conference, Sunnybrook Estates January 20, 2011 Rick Swartz HBSc, MD, PhD, FRCPC Assistant Professor, Department of Medicine, Divisions of Neurology and Obstetrical
Corporate Medical Policy
 Corporate Medical Policy Congenital Heart Defect, Repair Devices File Name: Origination: Last CAP Review: Next CAP Review: Last Review: congenital_heart_defect_repair_devices 10/2000 6/2017 6/2018 6/2017
Corporate Medical Policy Congenital Heart Defect, Repair Devices File Name: Origination: Last CAP Review: Next CAP Review: Last Review: congenital_heart_defect_repair_devices 10/2000 6/2017 6/2018 6/2017
Ischemic Stroke in Critically Ill Patients with Malignancy
 Ischemic Stroke in Critically Ill Patients with Malignancy Jeong-Am Ryu 1, Oh Young Bang 2, Daesang Lee 1, Jinkyeong Park 1, Jeong Hoon Yang 1, Gee Young Suh 1, Joongbum Cho 1, Chi Ryang Chung 1, Chi-Min
Ischemic Stroke in Critically Ill Patients with Malignancy Jeong-Am Ryu 1, Oh Young Bang 2, Daesang Lee 1, Jinkyeong Park 1, Jeong Hoon Yang 1, Gee Young Suh 1, Joongbum Cho 1, Chi Ryang Chung 1, Chi-Min
Roles and Effective of Foramen Ovale Closure to Prevent Recurrent Stroke
 Roles and Effective of Foramen Ovale Closure to Prevent Recurrent Stroke 1 Saeed Abdulrahman Alghamdi, 2 Abdullah Abdulrahman Alghamdi, 3 Saeed Abdulaziz Alghamdi, 4 Eid Hussein Alshahrani, 5 Alwaleed
Roles and Effective of Foramen Ovale Closure to Prevent Recurrent Stroke 1 Saeed Abdulrahman Alghamdi, 2 Abdullah Abdulrahman Alghamdi, 3 Saeed Abdulaziz Alghamdi, 4 Eid Hussein Alshahrani, 5 Alwaleed
CVA Updates Karen Greenberg, DO, FACOEP. Director Neurologic Emergency Department Crozer Chester Medical Center
 CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
Patients selection criteria for LAA occlusion. Young Keun On, MD, PhD, FHRS Samsung Medical Center Sungkyunkwan University School of Medicine
 Patients selection criteria for LAA occlusion Young Keun On, MD, PhD, FHRS Samsung Medical Center Sungkyunkwan University School of Medicine Atrial Fibrillation The most common cardiac arrhythmia. Confers
Patients selection criteria for LAA occlusion Young Keun On, MD, PhD, FHRS Samsung Medical Center Sungkyunkwan University School of Medicine Atrial Fibrillation The most common cardiac arrhythmia. Confers
Sixth Annual Intensive Update in Neurology 9/15-16/2016. W Tom Kushner DO Swedish Stroke Clinic Neurohospitalist
 W Tom Kushner DO Swedish Stroke Clinic Neurohospitalist 1 One Strategy for cryptogenic stroke: ESUS Positively defined criteria FDA allows clinical trials NOACs have lower risk profile Another strategy
W Tom Kushner DO Swedish Stroke Clinic Neurohospitalist 1 One Strategy for cryptogenic stroke: ESUS Positively defined criteria FDA allows clinical trials NOACs have lower risk profile Another strategy
How to Evaluate Patients with Cryptogenic Stroke
 How to Evaluate Patients with Cryptogenic Stroke Jeffrey Saver, MD Professor of Neurology Director, How to Evaluate Patients with Cryptogenic Stroke Disclosure Scientific Consultant, Unpaid Trialist: AGA
How to Evaluate Patients with Cryptogenic Stroke Jeffrey Saver, MD Professor of Neurology Director, How to Evaluate Patients with Cryptogenic Stroke Disclosure Scientific Consultant, Unpaid Trialist: AGA
Patent Foramen Ovale Closure or Antiplatelet Therapy for Cryptogenic Stroke
 The new england journal of medicine Original Article Patent Foramen Ovale Closure or Antiplatelet Therapy for Cryptogenic Stroke Lars Søndergaard, M.D., Scott E. Kasner, M.D., John F. Rhodes, M.D., Grethe
The new england journal of medicine Original Article Patent Foramen Ovale Closure or Antiplatelet Therapy for Cryptogenic Stroke Lars Søndergaard, M.D., Scott E. Kasner, M.D., John F. Rhodes, M.D., Grethe
Supplementary Online Content
 Supplementary Online Content Inohara T, Xian Y, Liang L, et al. Association of intracerebral hemorrhage among patients taking non vitamin K antagonist vs vitamin K antagonist oral anticoagulants with in-hospital
Supplementary Online Content Inohara T, Xian Y, Liang L, et al. Association of intracerebral hemorrhage among patients taking non vitamin K antagonist vs vitamin K antagonist oral anticoagulants with in-hospital
Strokes , The Patient Education Institute, Inc. hp Last reviewed: 11/11/2017 1
 Strokes Introduction A stroke or a brain attack is a very serious condition that can result in death and significant disability. This disease is ranked as the third leading cause of death in the United
Strokes Introduction A stroke or a brain attack is a very serious condition that can result in death and significant disability. This disease is ranked as the third leading cause of death in the United
 CLINICAL FEATURES THAT SUPPORT ATHEROSCLEROTIC STROKE 1. cerebral cortical impairment (aphasia, neglect, restricted motor involvement, etc.) or brain stem or cerebellar dysfunction 2. lacunar clinical
CLINICAL FEATURES THAT SUPPORT ATHEROSCLEROTIC STROKE 1. cerebral cortical impairment (aphasia, neglect, restricted motor involvement, etc.) or brain stem or cerebellar dysfunction 2. lacunar clinical
Primary Stroke Center Quality & Performance Measures
 Primary Stroke Center Quality & Performance Measures This section of the manual contains information related to the quality performance of Primary Stroke Centers. Brain Attack Coalition Definitions Recognition
Primary Stroke Center Quality & Performance Measures This section of the manual contains information related to the quality performance of Primary Stroke Centers. Brain Attack Coalition Definitions Recognition
Permanent foramen ovale: when to close?
 Permanent foramen ovale: when to close? Pierre Amarenco INSERM U-698 and Denis Diderot University - Paris VII Department of Neurology and Stroke Center Bichat hospital, Paris, France PFO - Pathology TEE
Permanent foramen ovale: when to close? Pierre Amarenco INSERM U-698 and Denis Diderot University - Paris VII Department of Neurology and Stroke Center Bichat hospital, Paris, France PFO - Pathology TEE
EAE RECOMMENDATIONS FOR TRANSESOPHAGEAL ECHO. Cardiac Sources of Embolism. Luigi P. Badano, MD, FESC
 EAE RECOMMENDATIONS FOR TRANSESOPHAGEAL ECHO. Cardiac Sources of Embolism Luigi P. Badano, MD, FESC Background Stroke is the 3 cause of death in several industrial countries; Embolism accounts for 15-30%
EAE RECOMMENDATIONS FOR TRANSESOPHAGEAL ECHO. Cardiac Sources of Embolism Luigi P. Badano, MD, FESC Background Stroke is the 3 cause of death in several industrial countries; Embolism accounts for 15-30%
Atrial Fibrillaiton and Heart Failure: Anticoagulation therapy in all cases?
 Atrial Fibrillaiton and Heart Failure: Anticoagulation therapy in all cases? Nicolas Lellouche Fédération de Cardiologie Hôpital Henri Mondor Créteil Disclosure Statement of Financial Interest I currently
Atrial Fibrillaiton and Heart Failure: Anticoagulation therapy in all cases? Nicolas Lellouche Fédération de Cardiologie Hôpital Henri Mondor Créteil Disclosure Statement of Financial Interest I currently
Listen to Your Heart. What Everyone Needs To Know About Atrial Fibrillation & Stroke. The S-ICD System. The protection you need
 Listen to Your Heart The S-ICD System What Everyone Needs To Know About Atrial Fibrillation & Stroke The protection you need without Stroke. touching Are you your at heart risk? Increase your knowledge.
Listen to Your Heart The S-ICD System What Everyone Needs To Know About Atrial Fibrillation & Stroke The protection you need without Stroke. touching Are you your at heart risk? Increase your knowledge.
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Subject Expert. Michelle Whaley MSN, CNS, CCNS, ANVP-BC Swedish Medical Center Englewood, CO
 Stroke 101 Subject Expert Michelle Whaley MSN, CNS, CCNS, ANVP-BC Swedish Medical Center Englewood, CO 2 Objectives Types of strokes Stroke warning signs Stroke risk factors Medical test performed following
Stroke 101 Subject Expert Michelle Whaley MSN, CNS, CCNS, ANVP-BC Swedish Medical Center Englewood, CO 2 Objectives Types of strokes Stroke warning signs Stroke risk factors Medical test performed following
Stroke & the Emergency Department. Dr. Barry Moynihan, March 2 nd, 2012
 Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model