MEET 2007: Evaluation and treatment of the stroke and TIA patient for the non-neurointerventionist. neurointerventionist
|
|
|
- Baldric Horn
- 5 years ago
- Views:
Transcription

1 MEET 2007: Evaluation and treatment of the stroke and TIA patient for the non-neurointerventionist neurointerventionist Steve Ramee, MD Ochsner Medical Center New Orleans
2 DISCLOSURE Nothing Nothing to disclose.

3 Percentage Breakdown of Deaths from Cardiovascular Diseases United States: 2001 Source: CDC/NCHS. p5
4 Age-Adjusted Death Rates for Coronary Heart Disease, Stroke, and Lung and Breast Cancer for White and Black Females United States: 2001 Source: CDC/NCHS. p7

5 Don t hurt my brain, its my second favorite organ. Woody Allen

6 Birth of a Neurointervention Program: 1994 Carotid bifurcation is causative in less than 1/3 of all TIA s and strokes! Other lesion locations do not have established surgical therapy: Aorto-ostial ostial stenosis Subclavian stenosis Vertebrobasilar disease Intracranial stenosis PFOPFO Atrial Atrial fibrillation These patients need treatment, too!
7 Each specialty has deficiencies Cardiologists lack a fund of knowledge. Neuroradiologists lack clinical skills. Neurologists lack angiographic skills. Neuroradiology FUND OF KNOWLEDGE Neurology or Neurosurgery ANGIO SKILLS CLINICAL SKILLS CARDIOLOGY
8 Ochsner Multidisciplinary Neurovascular Team Components Emergency Medicine Stroke Stroke Neurology Radiology Interventional Neuroradiology Non-invasive Cardiology Interventional Cardiology Internal Internal Medicine Vascular Vascular Surgery Physical Physical Medicine
9 What they do with Stroke and TIA patients ER Physicians Dx/triage TIA & stroke Stroke neurology Clinical evaluation/tcd Initiate stroke therapy Referral for intervention Radiology CFD/CT/MRI Neuroradiology Angiography Intracranial intervention Vascular Surgery Elective CEA Non-invasive cardiology Echocardiogram/TEE Critical care service Interventional cardiology Intracranial intervention Stroke intervention Carotid/veertebral stents PFO/ASD/LAA closure Internal Medicine Inpatient service Physical Medicine Rehabilitation


10 Major Types of Stroke Ischemic = 83% Hemorrhagic = 17%


11 What causes ischemic stroke? Different than MI. The intracranial vessels are usually normal. Embolic occlusion rather than intracranial plaque rupture Extracranial sources in 85%: Carotid plaque Cardioembolic Atrial appendage LV thrombus PFO Carotid dissection


12 Normal cerebral anatomy ACA: Lower extremity MCA: Upper extremity, speech Lenticulo-striate arteries ACA M1 M2 ICA Anterior Lateral

13 Normal Vertebral Artery Symptoms Dizziness Gait disturbances Blurred or double vision Syncope All brainstem functions Thalamoperforator a.
14 ANATOMY

15 Localization Simplified Cerbral cortex Nearly always Embolic Aphasia Neglect Visual Field Loss Hemiplegia Sensory Loss

16 Localization Simplified Lacunar cerebral Nearly always Thrombotic Pure Motor Hemiplegia Pure Sensory Mixed Motor Sensory Ataxic Hemiparesis No cortical signs

17 Localization Simplified Brainstem Embolic or Thrombotic Diplopia Nausea/Vomiting Crossed Findings Vertigo
18 We Aren t Doing Very Well: Managing Acute Stroke Patients 97% 97% of all stroke patients get NO therapy at all! 97% 97% of all stroke lawsuits are for non- treatment, NOT bad outcomes! 63% of stroke patients arrive at hospital > 24 hours after symptom onset! From Alberta, MJ et al. Stroke 1992;23:
19 In Our ER s: IV Lytics are ONLY effective if given within 3 hrs of symptom onset! Up to 90 min 2.8x better outcomes than placebo 90min - 3 hrs 1.5x better than placebo Over Over 3 hrs M 1 occlusion Multiple failed trials Poor outcome w/ i.v. lysis Marler et al. Neurology. 2000;55:
20 Or in Our Neuro-Intervention Suites: Intra-arterial Thrombolysis Prolyse in Acute Cerebral Thromboembolism (PROACT) II 180 patients with occlusion of middle cerebral artery within 6 hours of onset Recanalization Intraarterial Prourokinase (9mg) vs placebo Follow-up 3 months Pro-urokinase Placebo 66% 18% Hemorrhagic transformation 10% 2% Favorable outcome 40% 25%
21 Health Economics Hospital charges for Stroke Patients Stroke patients who receive a thrombolytic agent have significantly higher in-hospital charges but are currently small in number Of all discharges in DRGs 14 & 15 N (% of Total) LOS Mean Std. Charges Mean Patients receiving a thrombolytic identified by code ,452 (0.76%) 7.1 $31,765 99% get NO Rx! Patients not receiving a thrombolytic 321,757 (99.24%) 5.6 $16,400 Source: 2003 Medicare MedPAR data. Thrombolytic patients coded with ICD-9 code
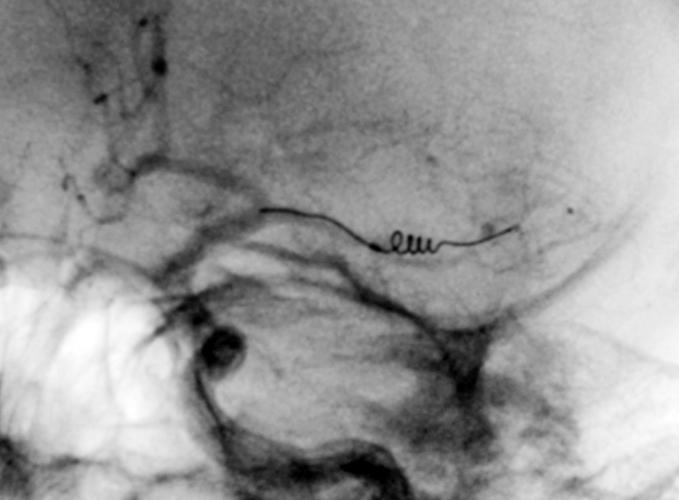
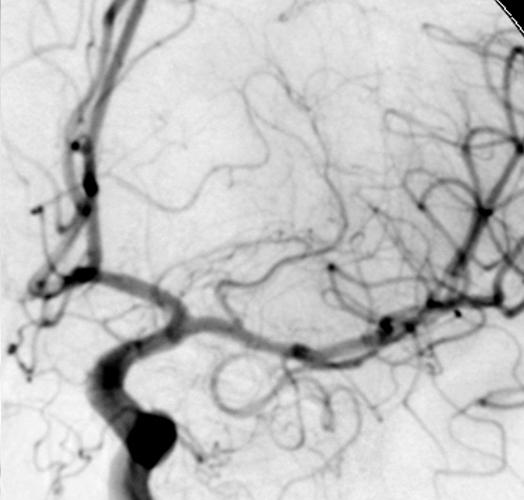
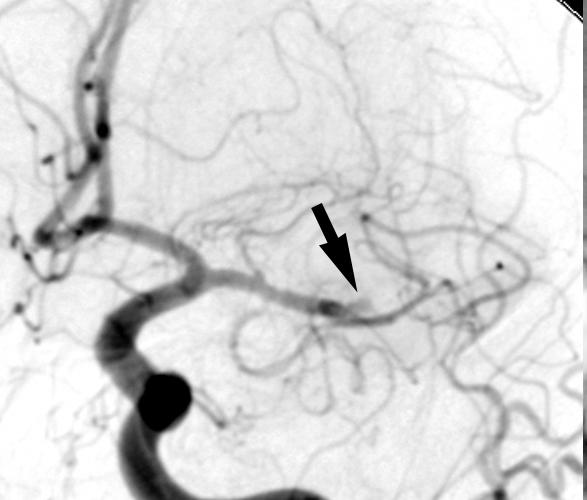
22 Technique of Stroke Intervention
23 Catheter-based approach Time Time is brain Target Target vessel angiography first Other vessels only if dx is in question Cross Cross lesion with hydrophilic wire If soft thrombus: Lysis, balloon, stent If hard thrombus: Merci, balloon, stent Remember: Primum non-nocere nocere!

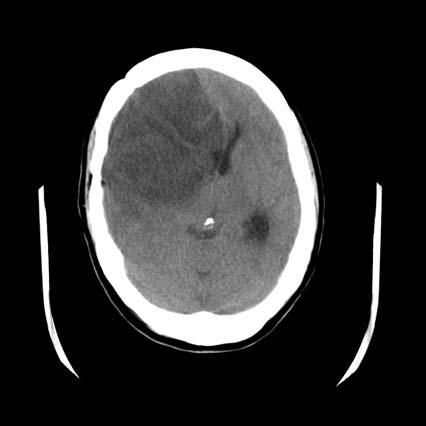
24 Acute Stroke Intervention 39 year old woman Mother of 4 yo boy Sudden collapse in shower at 5AM Dense R hemiplegia, aphasia CT showed MCA sign What would YOU do?

25

26
27
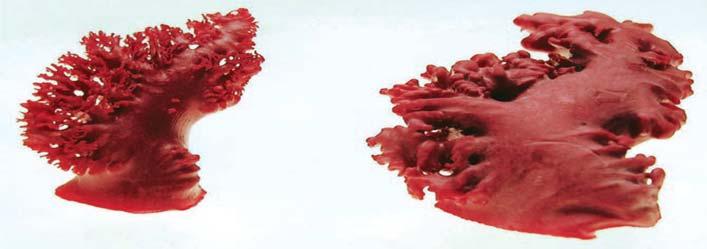
28 Four days later...


29 Concentric Retrieval System
30 12 RESULTS: NIH Stroke Scale 25 Patients with Acute Hemiplegic Stroke Ramee et al, Stroke, May 2004 Presentation versus 30 day outcome 13.3 P = Baseline 30 days
31 RESULTS: Modified Rankin Score 25 Patients with Acute Hemiplegic Stroke Ramee et al, Stroke, May 2004 Baseline versus 30 day outcome P = Baseline 30 days
32 What about Stroke Prevention?

33 What About Stroke Prevention? It s much easier than treatment! TIA is an ominous warning sign. Many patients have no warning TIA. Must treat underlying conditions that predispose to stroke.

34 The Heart and Aortic Arch as a Source of Preventable Ischemic Stroke Aortic arch and vertebral ostial stenosis ~25% ~15% Thrombotic IC cerebral and vertebral stenosis Cardioembolic Atrial fibrillation Akinetic segment Mitral stenosis Prosthetic valve Myxoma Cardiomyopathy ~25% ~30% Cryptogenic > 50-70% with PFO and ASD
35 IBNA\Folders\A\ATRITECH\BOLT\PPS\ 0210_0392_IBNA\main\ 0210_0392_IBNA_SCAtrial fibrillation source of stroke is a MAJOR Up to 25% of all ischemic strokes occur in patients with AF Percent of total strokes attributable to atrial fibrillation 35% 30% 25% 20% 15% 10% 5% 0% Source: Stroke, 1991, 22(8): Age group (years) Patients with AF have, on average, 5 to 6 times greater probability of having a stroke and 18 times greater probability of an embolic event 35% of patients with AF who are not treated with anticoagulants will have a stroke in their lifetime An estimated 55% of AF patients require anticoagulation therapy due to risk of stroke


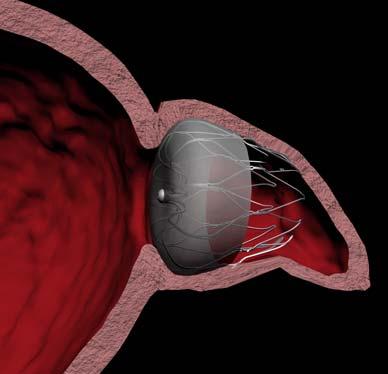
36 Atrial Fibrillation and Stroke WATCHMAN Device by Atritech RCT 300 PTS 2:1 Randomization Atritech vs.. Warfarin

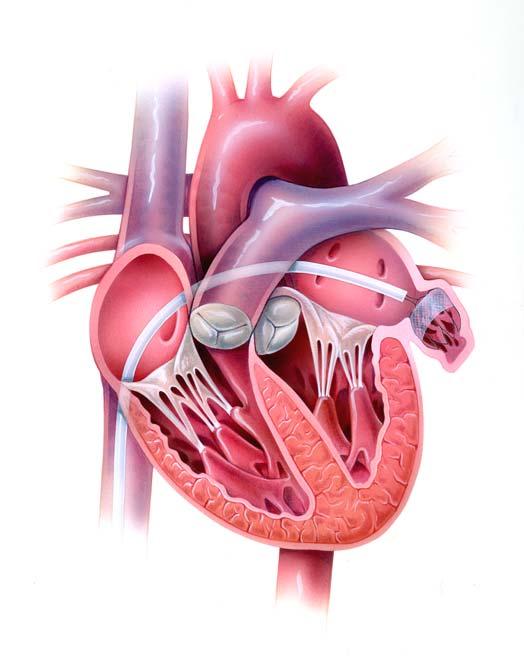
37 Frustration: Cryptogenic Stroke Antiquated historical term Pts with no carotid disease or afib 50-70% RA have a PFO! LA RA PRA Confirmed by TCD, TEE with bubble study LA PLA On Valsalva, PRA > PLA

38 Recurrence Rates on Medical Therapy in Cryptogenic Stroke 17% Stroke or 2 yr!! WARSS study NIH funded RCT 2606 patients randomized to ASA or Warfarin Excluded other sources of stroke (Afib, carotid dz.) Recurrent event = stroke or death at 2 years. Warfarin group 17.8% Aspirin group 16.0% Mohr et al, NEJM 2001, vol 345, 1444.
39 Remember our young mother with MCA occlusion?


40 Four days later... One month later, PFO closure

41 What about symptomatic intracranial stenosis?
42 How effective is medical Rx? WASID Trial NEJM 2005;352,
43 WASID Trial Double blind, Multicenter RCT 569 patients with TIA or Stroke 50-99% stenosis by angiography Warfarin (INR 2-3) 2 vs.. ASA 1300mg Primary 2years: Ischemic Stroke Brain Hemorrhage Death (non-neurologic, neurologic, vascular) NEJM 2005;352,

44 Two Year Stoke and Death 22% NEJM 2005;352,

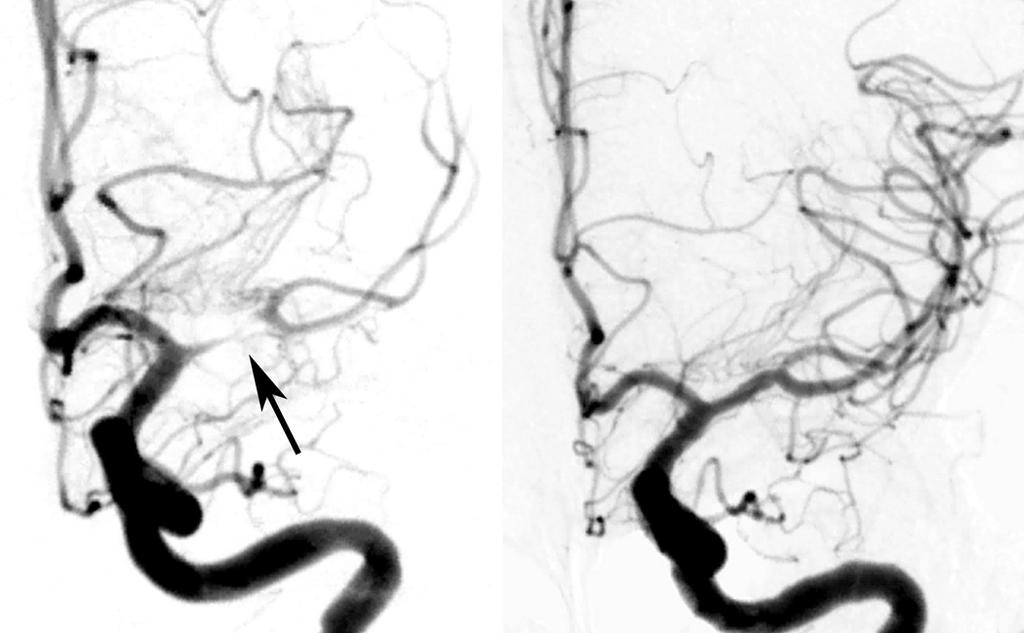
45 PTA result
46 Elective Intracranial Intervention Freedom from events at one year 100% 80% 60% 40% 20% N = 26 patients 100% Neurologic evaluation 100% 93% 0% TIA Stroke Ramee et al, CCI 52: , 467, 2001

47 Who can prevent it? Neurologists Neuro-radiologists Neurosurgeons Cardiologists Radiologists Vascular Surgeons Internists TIA and Stroke It s up to All Of US at this meeting and our colleagues to prevent strokes They aren t referred to a neurologist until AFTER they have had one!
48 SUMMARY Stroke is a medical emergency. High morbidity, mortality, and cost Second only to CAD 85% of all strokes are embolic. 25% Atrial fibrillation 30% Cryptogenic 30% Atheroembolic Stroke patients are best managed by a multidisciplinary team. Interventional cardiologists are well suited to participate and provide stroke intervention. Stroke prevention much easier than stroke treatment and is our responsibility!
49 STROKE
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine
 Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Cryptogenic Strokes: Evaluation and Management
 Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
PFO Management update
 PFO Management update May 12, 2017 Peter Casterella, MD Swedish Heart and Vascular 1 PFO Update 2017: Objectives Review recently released late outcomes of RESPECT trial and subsequent FDA approval of PFO
PFO Management update May 12, 2017 Peter Casterella, MD Swedish Heart and Vascular 1 PFO Update 2017: Objectives Review recently released late outcomes of RESPECT trial and subsequent FDA approval of PFO
Cryptogenic Stroke: A logical approach to a common clinical problem
 Cryptogenic Stroke: A logical approach to a common clinical problem Alphonse M. Ambrosia, DO, FACC Interventional Cardiologist CardioVascular Associates of Mesa Mesa, Arizona Speakers Bureau Boston Scientific
Cryptogenic Stroke: A logical approach to a common clinical problem Alphonse M. Ambrosia, DO, FACC Interventional Cardiologist CardioVascular Associates of Mesa Mesa, Arizona Speakers Bureau Boston Scientific
Management and Investigation of Ischemic Stroke By Etiology
 Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
What the general cardiologist should know about arrhythmia Stroke prevention in AF" Peter Ammann Kantonsspital St. Gallen
 What the general cardiologist should know about arrhythmia Stroke prevention in AF" Peter Ammann Kantonsspital St. Gallen What the cardiologist should know about arrhythmia and stroke are there real low
What the general cardiologist should know about arrhythmia Stroke prevention in AF" Peter Ammann Kantonsspital St. Gallen What the cardiologist should know about arrhythmia and stroke are there real low
Disclosures. CREST Trial: Summary. Lecture Outline 4/16/2015. Cervical Atherosclerotic Disease
 Disclosures Your Patient Has Carotid Bulb Stenosis and a Tandem Intracranial Stenosis: How Do SAMMPRIS and Other Evidence Inform Your Treatment? UCSF Vascular Symposium 2015 Steven W. Hetts, MD Associate
Disclosures Your Patient Has Carotid Bulb Stenosis and a Tandem Intracranial Stenosis: How Do SAMMPRIS and Other Evidence Inform Your Treatment? UCSF Vascular Symposium 2015 Steven W. Hetts, MD Associate
Alex Abou-Chebl, MD Associate Professor of Neurology and Neurosurgery Director of Neurointerventional Services Director of Vascular and
 Alex Abou-Chebl, MD Associate Professor of Neurology and Neurosurgery Director of Neurointerventional Services Director of Vascular and Interventional Neurology Fellowships University of Louisville School
Alex Abou-Chebl, MD Associate Professor of Neurology and Neurosurgery Director of Neurointerventional Services Director of Vascular and Interventional Neurology Fellowships University of Louisville School
Practical Considerations in the Early Treatment of Acute Stroke
 Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Significant Relationships
 Opening Large Vessels During Acute Ischemic Stroke Significant Relationships Wade S Smith, MD, PhD Director UCSF Neurovascular Service Professor of Neurology Daryl R Gress Endowed Chair of Neurocritical
Opening Large Vessels During Acute Ischemic Stroke Significant Relationships Wade S Smith, MD, PhD Director UCSF Neurovascular Service Professor of Neurology Daryl R Gress Endowed Chair of Neurocritical
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval
 How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval Peter Howard MD FRCPC Disclosures No conflicts to disclose How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular
How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval Peter Howard MD FRCPC Disclosures No conflicts to disclose How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
Stroke/TIA. Tom Bedwell
 Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Acute Stroke Treatment: Current Trends 2010
 Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Stroke Topics. Advances in the Prevention and Treatment of Stroke. Non-Contrast Head CT. Patient 1-68 yo man
 Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
Patent Foramen Ovale and Cryptogenic Stroke: Do We Finally Have Closure? Christopher Streib, MD, MS
 Patent Foramen Ovale and Cryptogenic Stroke: Do We Finally Have Closure? Christopher Streib, MD, MS 11-8-18 Outline 1. Background 2. Anatomy of patent foramen ovale (PFO) 3. Relationship between PFO and
Patent Foramen Ovale and Cryptogenic Stroke: Do We Finally Have Closure? Christopher Streib, MD, MS 11-8-18 Outline 1. Background 2. Anatomy of patent foramen ovale (PFO) 3. Relationship between PFO and
Endovascular Neurointervention in Cerebral Ischemia
 Endovascular Neurointervention in Cerebral Ischemia Beyond Thrombolytics Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington 72 y/o female with a recent diagnosis
Endovascular Neurointervention in Cerebral Ischemia Beyond Thrombolytics Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington 72 y/o female with a recent diagnosis
ENDOVASCULAR THERAPIES FOR ACUTE STROKE
 ENDOVASCULAR THERAPIES FOR ACUTE STROKE Cerebral Arteriogram Cerebral Anatomy Cerebral Anatomy Brain Imaging Acute Ischemic Stroke (AIS) Therapy Main goal is to restore blood flow and improve perfusion
ENDOVASCULAR THERAPIES FOR ACUTE STROKE Cerebral Arteriogram Cerebral Anatomy Cerebral Anatomy Brain Imaging Acute Ischemic Stroke (AIS) Therapy Main goal is to restore blood flow and improve perfusion
 CLINICAL FEATURES THAT SUPPORT ATHEROSCLEROTIC STROKE 1. cerebral cortical impairment (aphasia, neglect, restricted motor involvement, etc.) or brain stem or cerebellar dysfunction 2. lacunar clinical
CLINICAL FEATURES THAT SUPPORT ATHEROSCLEROTIC STROKE 1. cerebral cortical impairment (aphasia, neglect, restricted motor involvement, etc.) or brain stem or cerebellar dysfunction 2. lacunar clinical
ACUTE ISCHEMIC STROKE. Current Treatment Approaches for Acute Ischemic Stroke
 ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
Carotid Artery Stenting
 Carotid Artery Stenting Natural history of the carotid stenosis Asymptomatic 80% carotid stenosis - 6% risk of stroke / year Symptomatic carotid stenosis have 10% risk of CVA at one year and 40% at 5 years
Carotid Artery Stenting Natural history of the carotid stenosis Asymptomatic 80% carotid stenosis - 6% risk of stroke / year Symptomatic carotid stenosis have 10% risk of CVA at one year and 40% at 5 years
2/7/
 Disclosure Intracranial Atherosclerosis an update None Mai N. Nguyen-Huynh, MD, MAS Assistant Professor of Neurology UCSF Neurovascular Service February 7, 2009 Case #1 60 y.o. Chinese-speaking speaking
Disclosure Intracranial Atherosclerosis an update None Mai N. Nguyen-Huynh, MD, MAS Assistant Professor of Neurology UCSF Neurovascular Service February 7, 2009 Case #1 60 y.o. Chinese-speaking speaking
TIA AND STROKE. Topics/Order of the day 1. Topics/Order of the day 2 01/08/2012
 Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease
 Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease Christopher Koebbe, MD Endovascular Neurosurgeon Florida Spine Institute Director of Neurosciences Northside Hospital Overview
Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease Christopher Koebbe, MD Endovascular Neurosurgeon Florida Spine Institute Director of Neurosciences Northside Hospital Overview
Neuroanatomy of a Stroke. Joni Clark, MD Professor of Neurology Barrow Neurologic Institute
 Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
Carotid Artery Stenting
 Carotid Artery Stenting Woong Chol Kang M.D. Gil Medical Center, Gachon University of Medicine and Science, Incheon, Korea Carotid Stenosis and Stroke ~25% of stroke is due to carotid disease, the reminder
Carotid Artery Stenting Woong Chol Kang M.D. Gil Medical Center, Gachon University of Medicine and Science, Incheon, Korea Carotid Stenosis and Stroke ~25% of stroke is due to carotid disease, the reminder
Stroke & the Emergency Department. Dr. Barry Moynihan, March 2 nd, 2012
 Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
TIA: Updates and Management 2008
 TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
True cryptogenic stroke
 True cryptogenic stroke Arne Lindgren, MD, PhD Dept of Clinical Sciences Lund, Neurology, Lund University Dept of Neurology and Rehabilitation Medicine Skåne University Hospital Lund, Sweden Disclosures
True cryptogenic stroke Arne Lindgren, MD, PhD Dept of Clinical Sciences Lund, Neurology, Lund University Dept of Neurology and Rehabilitation Medicine Skåne University Hospital Lund, Sweden Disclosures
ACUTE CENTRAL PERIFERALEMBOLISM
 EAE TEACHING COURSE 2010 Belgrade, Serbia October 22-23, 2010 ACUTE CENTRAL and PERIFERALEMBOLISM Maria João Andrade Lisbon, PT BACKGROUND Stroke is a leading cause of mortality and long-term disability
EAE TEACHING COURSE 2010 Belgrade, Serbia October 22-23, 2010 ACUTE CENTRAL and PERIFERALEMBOLISM Maria João Andrade Lisbon, PT BACKGROUND Stroke is a leading cause of mortality and long-term disability
ACUTE STROKE INTERVENTION: THE ROLE OF THROMBECTOMY AND IA LYSIS
 Associate Professor of Neurology Director of Neurointerventional Services University of Louisville School of Medicine ACUTE STROKE INTERVENTION: THE ROLE OF THROMBECTOMY AND IA LYSIS Conflict of Interest
Associate Professor of Neurology Director of Neurointerventional Services University of Louisville School of Medicine ACUTE STROKE INTERVENTION: THE ROLE OF THROMBECTOMY AND IA LYSIS Conflict of Interest
Cryptogenic Stroke: What Don t We Know. Siddharth Sehgal, MD Medical Director, TMH Stroke Center Tallahassee Memorial Healthcare
 Cryptogenic Stroke: What Don t We Know Siddharth Sehgal, MD Medical Director, TMH Stroke Center Tallahassee Memorial Healthcare Financial Disclosures None Objectives Principles of diagnostic evaluation
Cryptogenic Stroke: What Don t We Know Siddharth Sehgal, MD Medical Director, TMH Stroke Center Tallahassee Memorial Healthcare Financial Disclosures None Objectives Principles of diagnostic evaluation
Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco
 Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco I have no financial disclosures 1 Hospital Management Thrombolytic and Thrombectomy Blood pressure Stroke in the Young
Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco I have no financial disclosures 1 Hospital Management Thrombolytic and Thrombectomy Blood pressure Stroke in the Young
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know. Case 1 4/5/11. What treatment should you initiate?
 Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University
Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University
Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices
 Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices Joey English MD, PhD Medical Director, Neurointerventional Services California Pacific Medical Center Hospitals, San Francisco,
Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices Joey English MD, PhD Medical Director, Neurointerventional Services California Pacific Medical Center Hospitals, San Francisco,
New Trials in Progress: ACT 1. Jon Matsumura, MD Cannes, France June 28, 2008
 New Trials in Progress: ACT 1 Jon Matsumura, MD Cannes, France June 28, 2008 Faculty Disclosure I disclose the following financial relationships: Consultant, CAS training director, and/or research grants
New Trials in Progress: ACT 1 Jon Matsumura, MD Cannes, France June 28, 2008 Faculty Disclosure I disclose the following financial relationships: Consultant, CAS training director, and/or research grants
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes. Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville
 Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
Stroke 101. Maine Cardiovascular Health Summit. Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013
 Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Watchman and Structural update..the next frontier. Ari Chanda, MD Cardiology Associates of Fredericksburg
 Watchman and Structural update..the next frontier Ari Chanda, MD Cardiology Associates of Fredericksburg Different Left Atrial Appendage (LAA) morphologies Watchman (the device) Fabric Anchors Device structure
Watchman and Structural update..the next frontier Ari Chanda, MD Cardiology Associates of Fredericksburg Different Left Atrial Appendage (LAA) morphologies Watchman (the device) Fabric Anchors Device structure
Cerebrovascular Disorders. Blood, Brain, and Energy. Blood Supply to the Brain 2/14/11
 Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Review of clinical carotid stent procedural & long-term outcomes in. symptomatic asymptomatic. patients
 Review of clinical carotid stent procedural & long-term outcomes in symptomatic asymptomatic patients 1 Conflict of Interest Statement Within the past 12 months, I or my spouse have had a financial interest/arrangement
Review of clinical carotid stent procedural & long-term outcomes in symptomatic asymptomatic patients 1 Conflict of Interest Statement Within the past 12 months, I or my spouse have had a financial interest/arrangement
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis
/intracranial atherosclerosis") Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
Peter A. Soukas, M.D., FACC, FSVM, FSCAI, RPVI
 Peter A. Soukas, M.D., FACC, FSVM, FSCAI, RPVI Director, Peripheral Vascular Interventional Laboratory Director, Vascular & Endovascular Medicine Fellowship Program Assistant Professor of Medicine The
Peter A. Soukas, M.D., FACC, FSVM, FSCAI, RPVI Director, Peripheral Vascular Interventional Laboratory Director, Vascular & Endovascular Medicine Fellowship Program Assistant Professor of Medicine The
Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington
 Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington Disclosures: SWIFT PRIME site (Medtronic) Physician Proctor
Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington Disclosures: SWIFT PRIME site (Medtronic) Physician Proctor
CAROTID DEBATE High-Grade Asymptomatic Disease Should Be Repaired Selectively; Medical Management is NOT Enough
 Todd W GenslerMD April 28, 2018 CAROTID DEBATE High-Grade Asymptomatic Disease Should Be Repaired Selectively; Medical Management is NOT Enough DISCLOSURES I have no financial disclosures Presenter name
Todd W GenslerMD April 28, 2018 CAROTID DEBATE High-Grade Asymptomatic Disease Should Be Repaired Selectively; Medical Management is NOT Enough DISCLOSURES I have no financial disclosures Presenter name
2018 Update in Diagnosis and Management of Stroke
 2018 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Chair, Department of Neurology Director,
2018 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Chair, Department of Neurology Director,
I, (Issam Moussa) DO NOT have a financial interest/arrangement t/ t or affiliation with one or more organizations that could be perceived as a real
 DO NOT have a financial interest/arrangement t/ t or affiliation with one or more organizations that could be perceived as a real") PFO Closure: Where We Are Going to after CLOSURE I Study? Issam D. Moussa, MD Professor of Medicine Chair, Division of Cardiovascular Diseases Mayo Clinic Jacksonville, Florida Disclosure Statement of
PFO Closure: Where We Are Going to after CLOSURE I Study? Issam D. Moussa, MD Professor of Medicine Chair, Division of Cardiovascular Diseases Mayo Clinic Jacksonville, Florida Disclosure Statement of
Carotid Artery Revascularization: Current Strategies. Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014
 Carotid Artery Revascularization: Current Strategies Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014 Disclosures None 1 Stroke in 2014 Stroke kills almost
Carotid Artery Revascularization: Current Strategies Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014 Disclosures None 1 Stroke in 2014 Stroke kills almost
EAE RECOMMENDATIONS FOR TRANSESOPHAGEAL ECHO. Cardiac Sources of Embolism. Luigi P. Badano, MD, FESC
 EAE RECOMMENDATIONS FOR TRANSESOPHAGEAL ECHO. Cardiac Sources of Embolism Luigi P. Badano, MD, FESC Background Stroke is the 3 cause of death in several industrial countries; Embolism accounts for 15-30%
EAE RECOMMENDATIONS FOR TRANSESOPHAGEAL ECHO. Cardiac Sources of Embolism Luigi P. Badano, MD, FESC Background Stroke is the 3 cause of death in several industrial countries; Embolism accounts for 15-30%
Brain Attack. Strategies in the Management of Acute Ischemic Stroke: Neuroscience Clerkship. Case Medical Center
 Brain Attack Strategies in the Management of Acute Ischemic Stroke: Neuroscience Clerkship Stroke is a common and devastating disorder Third leading antecedent of death in American men, and second among
Brain Attack Strategies in the Management of Acute Ischemic Stroke: Neuroscience Clerkship Stroke is a common and devastating disorder Third leading antecedent of death in American men, and second among
2015 Update in Diagnosis and Management of Stroke
 2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
Permanent foramen ovale: when to close?
 Permanent foramen ovale: when to close? Pierre Amarenco INSERM U-698 and Denis Diderot University - Paris VII Department of Neurology and Stroke Center Bichat hospital, Paris, France PFO - Pathology TEE
Permanent foramen ovale: when to close? Pierre Amarenco INSERM U-698 and Denis Diderot University - Paris VII Department of Neurology and Stroke Center Bichat hospital, Paris, France PFO - Pathology TEE
Index. interventional.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACAS (Asymptomatic Carotid Atherosclerosis Study), 65 66 ACST (Asymptomatic Carotid Surgery Trial), 6 7, 65, 75 Age factors, in carotid
Index Note: Page numbers of article titles are in boldface type. A ACAS (Asymptomatic Carotid Atherosclerosis Study), 65 66 ACST (Asymptomatic Carotid Surgery Trial), 6 7, 65, 75 Age factors, in carotid
Ischemic stroke: management, prevention and follow up. Amit Kansara MD Providence Stroke Center Providence Brain and Spine Institute
 Ischemic stroke: management, prevention and follow up Amit Kansara MD Providence Stroke Center Providence Brain and Spine Institute Quotes Benjamin Franklin: All would live long, but none would be old.
Ischemic stroke: management, prevention and follow up Amit Kansara MD Providence Stroke Center Providence Brain and Spine Institute Quotes Benjamin Franklin: All would live long, but none would be old.
Nicolas Bianchi M.D. May 15th, 2012
 Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Session Antiplatelet Therapy: How, Why and When? In patients with ischemic stroke/tia
 GROUPE HOSPITALIER BICHAT-CLAUDE BERNARD PARIS DIDEROT UNIVERSITY - PARIS 7 Session Antiplatelet Therapy: How, Why and When? In patients with ischemic stroke/tia Pierre Amarenco INSERM U-698 and Denis
GROUPE HOSPITALIER BICHAT-CLAUDE BERNARD PARIS DIDEROT UNIVERSITY - PARIS 7 Session Antiplatelet Therapy: How, Why and When? In patients with ischemic stroke/tia Pierre Amarenco INSERM U-698 and Denis
Case 1 5/26/2017 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE
 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
How Can We Properly Manage Patients With Stroke of Undetermined Origin?
 How Can We Properly Manage Patients With Stroke of Undetermined Origin? : Spotlight on Embolic Stroke of Undetermined Source (ESUS) MI SUN OH Department of Neurology, Hallym University Scared Heart Hospital,
How Can We Properly Manage Patients With Stroke of Undetermined Origin? : Spotlight on Embolic Stroke of Undetermined Source (ESUS) MI SUN OH Department of Neurology, Hallym University Scared Heart Hospital,
Dr Ben Turner. Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital
 Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
Symptoms of small vessel strokes. Small Vessel stroke. What is this? Treatment. Large Vessel stroke 6/1/2018
 Stroke Stroke Megan Stevens MD Vascular Neurology SUDDEN Maximal at onset Lateralized weakness, lateralized numbness, vision loss (one eye or portion of field in both eyes), double vision, slurred speech,
Stroke Stroke Megan Stevens MD Vascular Neurology SUDDEN Maximal at onset Lateralized weakness, lateralized numbness, vision loss (one eye or portion of field in both eyes), double vision, slurred speech,
Endovascular Treatment of Ischemic Stroke
 Endovascular Treatment of Ischemic Stroke William Thorell, MD Associate Professor Neurosurgery UNMC Co-Director Stroke and Neurovascular Center Nebraska Medicine Overview Definitions of terms Review basic
Endovascular Treatment of Ischemic Stroke William Thorell, MD Associate Professor Neurosurgery UNMC Co-Director Stroke and Neurovascular Center Nebraska Medicine Overview Definitions of terms Review basic
CVA. Alison Atwater PA-C
 CVA Alison Atwater PA-C Types of CVAs Ischemic strokes 80% of strokes 2/3 are thrombotic 1/3 are embolic emboli from the heart or arteries feeding the brain such as carotids, vertebral and basilar etc
CVA Alison Atwater PA-C Types of CVAs Ischemic strokes 80% of strokes 2/3 are thrombotic 1/3 are embolic emboli from the heart or arteries feeding the brain such as carotids, vertebral and basilar etc
UPMC HAMOT CAROTID ARTERY DISEASE WHERE DO WE GO FROM HERE?
 UPMC HAMOT CAROTID ARTERY DISEASE WHERE DO WE GO FROM HERE? Richard W. Petrella M.D. FACP,FACC,FASCI DEPARTMENT CHAIRMAN CVM&S UPMC HAMOT MEDICAL CENTER 1 LEARNING OBJECTIVES REVIEW THE RISK FACTORS FOR
UPMC HAMOT CAROTID ARTERY DISEASE WHERE DO WE GO FROM HERE? Richard W. Petrella M.D. FACP,FACC,FASCI DEPARTMENT CHAIRMAN CVM&S UPMC HAMOT MEDICAL CENTER 1 LEARNING OBJECTIVES REVIEW THE RISK FACTORS FOR
Speakers. 2015, American Heart Association 1
 Speakers Lee Schwamm, MD, FAHA Executive Vice Chairman of Neurology, Massachusetts General Hospital Director, Stroke Service and Medical Director, MGH TeleHealth, Massachusetts General Hospital Director,
Speakers Lee Schwamm, MD, FAHA Executive Vice Chairman of Neurology, Massachusetts General Hospital Director, Stroke Service and Medical Director, MGH TeleHealth, Massachusetts General Hospital Director,
APPENDIX A NORTH AMERICAN SYMPTOMATIC CAROTID ENDARTERECTOMY TRIAL
 APPENDIX A Primary Findings From Selected Recent National Institute of Neurological Disorders and Stroke-Sponsored Clinical Trials That Have shaped Modern Stroke Prevention Philip B. Gorelick 178 NORTH
APPENDIX A Primary Findings From Selected Recent National Institute of Neurological Disorders and Stroke-Sponsored Clinical Trials That Have shaped Modern Stroke Prevention Philip B. Gorelick 178 NORTH
From interventional cardiology to cardio-neurology. A new subspeciality
 From interventional cardiology to cardio-neurology. A new subspeciality in the future? Prof. Andrejs Erglis, MD, PhD Pauls Stradins Clinical University Hospital University of Latvia Riga, LATVIA Disclosure
From interventional cardiology to cardio-neurology. A new subspeciality in the future? Prof. Andrejs Erglis, MD, PhD Pauls Stradins Clinical University Hospital University of Latvia Riga, LATVIA Disclosure
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
How to Evaluate Patients with Cryptogenic Stroke
 How to Evaluate Patients with Cryptogenic Stroke Jeffrey Saver, MD Professor of Neurology Director, How to Evaluate Patients with Cryptogenic Stroke Disclosure Scientific Consultant, Unpaid Trialist: AGA
How to Evaluate Patients with Cryptogenic Stroke Jeffrey Saver, MD Professor of Neurology Director, How to Evaluate Patients with Cryptogenic Stroke Disclosure Scientific Consultant, Unpaid Trialist: AGA
Michael Horowitz, MD Pittsburgh, PA
 Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
PATENT FORAMEN OVALE: UPDATE IN MANAGEMENT OF RECURRENT STROKE KATRINE ZHIROFF, MD, FACC, FSCAI LOS ANGELES CARDIOLOGY ASSOCIATES
 PATENT FORAMEN OVALE: UPDATE IN MANAGEMENT OF RECURRENT STROKE KATRINE ZHIROFF, MD, FACC, FSCAI LOS ANGELES CARDIOLOGY ASSOCIATES OBJECTIVES Review social burden and epidemiology of stroke Gender disparities
PATENT FORAMEN OVALE: UPDATE IN MANAGEMENT OF RECURRENT STROKE KATRINE ZHIROFF, MD, FACC, FSCAI LOS ANGELES CARDIOLOGY ASSOCIATES OBJECTIVES Review social burden and epidemiology of stroke Gender disparities
CVA Updates Karen Greenberg, DO, FACOEP. Director Neurologic Emergency Department Crozer Chester Medical Center
 CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
Sixth Annual Intensive Update in Neurology 9/15-16/2016. W Tom Kushner DO Swedish Stroke Clinic Neurohospitalist
 W Tom Kushner DO Swedish Stroke Clinic Neurohospitalist 1 One Strategy for cryptogenic stroke: ESUS Positively defined criteria FDA allows clinical trials NOACs have lower risk profile Another strategy
W Tom Kushner DO Swedish Stroke Clinic Neurohospitalist 1 One Strategy for cryptogenic stroke: ESUS Positively defined criteria FDA allows clinical trials NOACs have lower risk profile Another strategy
Advances in Neuro-Endovascular Care for Acute Stroke
 Advances in Neuro-Endovascular Care for Acute Stroke Ciarán J. Powers, MD, PhD, FAANS Associate Professor Program Director Department of Neurological Surgery Surgical Director Comprehensive Stroke Center
Advances in Neuro-Endovascular Care for Acute Stroke Ciarán J. Powers, MD, PhD, FAANS Associate Professor Program Director Department of Neurological Surgery Surgical Director Comprehensive Stroke Center
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Primary Care Atrial Fibrillation Update: Anticoagulation and Left Atrial Appendage Occlusion. Greg Francisco, MD, FACC
 Primary Care Atrial Fibrillation Update: Anticoagulation and Left Atrial Appendage Occlusion Greg Francisco, MD, FACC DISCLOSURES None to declare Estimated 33.5million have AF worldwide (6-7million in
Primary Care Atrial Fibrillation Update: Anticoagulation and Left Atrial Appendage Occlusion Greg Francisco, MD, FACC DISCLOSURES None to declare Estimated 33.5million have AF worldwide (6-7million in
Cryptogenic Stroke/PFO with Thrombophilia and VTE: Do We Know What To Do?
 Cryptogenic Stroke/PFO with Thrombophilia and VTE: Do We Know What To Do? Robert J. Sommer, MD Columbia University Medical Center New York, NY Disclosure Statement of Financial Interest Within the past
Cryptogenic Stroke/PFO with Thrombophilia and VTE: Do We Know What To Do? Robert J. Sommer, MD Columbia University Medical Center New York, NY Disclosure Statement of Financial Interest Within the past
Guiding Secondary Stroke Prevention through Evaluation of Ischemic Stroke Etiology
 Guiding Secondary Stroke Prevention through Evaluation of Ischemic Stroke Etiology Ann M. Leonhardt Caprio, MS, RN, ANP-BC Program Coordinator Comprehensive Stroke Center, Strong Memorial Hospital Clinical
Guiding Secondary Stroke Prevention through Evaluation of Ischemic Stroke Etiology Ann M. Leonhardt Caprio, MS, RN, ANP-BC Program Coordinator Comprehensive Stroke Center, Strong Memorial Hospital Clinical
About 700,000 Americans each year suffer a new or recurrent stroke. On average, a stroke occurs every 45 seconds
 UCLA Stroke Center Stroke Facts About 700,000 Americans each year suffer a new or recurrent stroke On average, a stroke occurs every 45 seconds Stroke kills more than 150,000 people a year (1 of every
UCLA Stroke Center Stroke Facts About 700,000 Americans each year suffer a new or recurrent stroke On average, a stroke occurs every 45 seconds Stroke kills more than 150,000 people a year (1 of every
2017 Bryan Health Primary Care Conference. Dale Hansen MD Bryan Heart 5/20/17
 2017 Bryan Health Primary Care Conference Dale Hansen MD Bryan Heart 5/20/17 I have no financial disclosures or conflicts of interest Bridging Anticoagulation Primum Non Nocere 67 y.o. male with mechanical
2017 Bryan Health Primary Care Conference Dale Hansen MD Bryan Heart 5/20/17 I have no financial disclosures or conflicts of interest Bridging Anticoagulation Primum Non Nocere 67 y.o. male with mechanical
Cerebrovascular Disease
 Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
Oltre la terapia medica nelle dissezioni carotidee
 Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
MD SUBTYPE ADJUDICATION VARIABLE DEFINITIONS MANUAL The following is a list of variables and how to complete each one:
 MD SUBTYPE ADJUDICATION VARIABLE DEFINITIONS MANUAL 2014-15 The following is a list of variables and how to complete each one: (PHY-1) Case, per physician review: The most important task for the physicians
MD SUBTYPE ADJUDICATION VARIABLE DEFINITIONS MANUAL 2014-15 The following is a list of variables and how to complete each one: (PHY-1) Case, per physician review: The most important task for the physicians
Stroke Case Studies. Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow
 Stroke Case Studies Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow Case 1 64 year old female with dysphasia and right arm weakness 3 hours prior CT head: dense M1 sign. No established ischaemia
Stroke Case Studies Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow Case 1 64 year old female with dysphasia and right arm weakness 3 hours prior CT head: dense M1 sign. No established ischaemia
Why Should We Treat PFO?
 Why Should We Treat PFO? SCAI Interventional Cardiology Fellows Course December 7, 2012 Jonathan Tobis, MD Director of Interventional Cardiology UCLA Disclosures Jonathan Tobis, MD 1. A Principal Investigator
Why Should We Treat PFO? SCAI Interventional Cardiology Fellows Course December 7, 2012 Jonathan Tobis, MD Director of Interventional Cardiology UCLA Disclosures Jonathan Tobis, MD 1. A Principal Investigator
Interventional Neuroradiology. & Stroke INR PROCEDURES INR PROCEDURES. Dr Steve Chryssidis. 25-Sep-17. Interventional Neuroradiology
 Interventional Neuroradiology Interventional Neuroradiology & Stroke Dr Steve Chryssidis Interventional Neuroradiology (INR) is a subspecialty within Radiology INR -- broadly defined as treatment by endovascular
Interventional Neuroradiology Interventional Neuroradiology & Stroke Dr Steve Chryssidis Interventional Neuroradiology (INR) is a subspecialty within Radiology INR -- broadly defined as treatment by endovascular
Management of cervicocephalic arterial dissection. Ciro G. Randazzo, MD, MPH Thomas Jefferson University Hospital, Department of Neurosurgery
 Management of cervicocephalic arterial dissection Ciro G. Randazzo, MD, MPH Thomas Jefferson University Hospital, Department of Neurosurgery Definition Disruption of arterial wall, either at level of intima-media
Management of cervicocephalic arterial dissection Ciro G. Randazzo, MD, MPH Thomas Jefferson University Hospital, Department of Neurosurgery Definition Disruption of arterial wall, either at level of intima-media
Secondary Stroke Prevention: A Precautionary Tale
 Secondary Stroke Prevention: A Precautionary Tale Kirsten George-Phillips, BSP Clinical Practice Leader, AHS Clinical Pharmacist, AHS Owen Stroke Prevention Clinic Learning Objectives! Examine literature
Secondary Stroke Prevention: A Precautionary Tale Kirsten George-Phillips, BSP Clinical Practice Leader, AHS Clinical Pharmacist, AHS Owen Stroke Prevention Clinic Learning Objectives! Examine literature
Antithrombotic Summit Basel 2012 Basel, 26. April Peter T. Buser Klinik Kardiologie Unviersitätsspital Basel
 Antithrombotic Summit Basel 2012 Basel, 26. April 2012 Peter T. Buser Klinik Kardiologie Unviersitätsspital Basel Background stroke = third-leading cause of death among adults 1/5 of stroke survivors require
Antithrombotic Summit Basel 2012 Basel, 26. April 2012 Peter T. Buser Klinik Kardiologie Unviersitätsspital Basel Background stroke = third-leading cause of death among adults 1/5 of stroke survivors require
Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke
 Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke Alexander A. Khalessi MD MS Director of Endovascular Neurosurgery Surgical Director of NeuroCritical Care University
Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke Alexander A. Khalessi MD MS Director of Endovascular Neurosurgery Surgical Director of NeuroCritical Care University
Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre
 Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre Objectives To learn what s new in stroke care 2010-11 1) Acute stroke management Carotid artery stenting versus surgery for symptomatic
Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre Objectives To learn what s new in stroke care 2010-11 1) Acute stroke management Carotid artery stenting versus surgery for symptomatic
Alex Abou-Chebl, MD Medical Director, Stroke Baptist Health, Louisvile. Alex Abou-Chebl, MD
 Medical Director, Stroke Baptist Health, Louisvile No Conflicts or Disclosures Post SAMMPRIS Too many unanswered questions Is stenting too risky? What aspects of the procedure resulted in such a high-complication
Medical Director, Stroke Baptist Health, Louisvile No Conflicts or Disclosures Post SAMMPRIS Too many unanswered questions Is stenting too risky? What aspects of the procedure resulted in such a high-complication
Is Stroke Frequency Declining?
 Is Stroke Frequency Declining? Etiologic Factors Clinical, Anatomic, Technique-related, and Device-specific Samir Kapadia, MD Professor of Medicine Section head, Interventional Cardiology Director, Cardiac
Is Stroke Frequency Declining? Etiologic Factors Clinical, Anatomic, Technique-related, and Device-specific Samir Kapadia, MD Professor of Medicine Section head, Interventional Cardiology Director, Cardiac
Mark J. Alberts, MD, FAHA, FANA Vice-Chair, Dept of Neurology Professor of Neurology UT Southwestern Medical Center Dallas, TX
 Interventional Therapies for Cerebrovascular Diease: The Good, The Bad, The Needed, and The Few 1 Mark J. Alberts, MD, FAHA, FANA Vice-Chair, Dept of Neurology Professor of Neurology UT Southwestern Medical
Interventional Therapies for Cerebrovascular Diease: The Good, The Bad, The Needed, and The Few 1 Mark J. Alberts, MD, FAHA, FANA Vice-Chair, Dept of Neurology Professor of Neurology UT Southwestern Medical
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES
 TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
Carotid Artery Stenting
 Carotid Artery Stenting JESSICA MITCHELL, ACNP CENTRAL ILLINOIS RADIOLOGICAL ASSOCIATES External Carotid Artery (ECA) can easily be identified from Internal Carotid Artery (ICA) by noticing the branches.
Carotid Artery Stenting JESSICA MITCHELL, ACNP CENTRAL ILLINOIS RADIOLOGICAL ASSOCIATES External Carotid Artery (ECA) can easily be identified from Internal Carotid Artery (ICA) by noticing the branches.
Interventional Revolution in Treatment of Stroke
 TCT RUSSIA 2018 XX Moscow s International Course on Endovascular Therapies Moscow, Russia, May 18-20, 2018 Interventional Revolution in Treatment of Stroke Horst Sievert, Ilona Hofmann, Laura Vaskelyte,
TCT RUSSIA 2018 XX Moscow s International Course on Endovascular Therapies Moscow, Russia, May 18-20, 2018 Interventional Revolution in Treatment of Stroke Horst Sievert, Ilona Hofmann, Laura Vaskelyte,