STROKE UPDATE ANTHEA PARRY MAY 2010
|
|
|
- Hannah Bennett
- 6 years ago
- Views:
Transcription
1 STROKE UPDATE ANTHEA PARRY MAY 2010
2 Delivery of stroke care Clinical presentations Management
3 Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services
4 Hyperacute stroke units All patients who are suspected of having a stroke Implementation will be complete by July 2010 Travel time<30mins LOS up to 72hours, then repatriated to local stroke unit depending on post code
5 Acute care. Principles that lie behind are the restoration of normal blood flow and salvage of the ischaemic penumbra. Thrombolysis Maintenance of normal physiological environment.
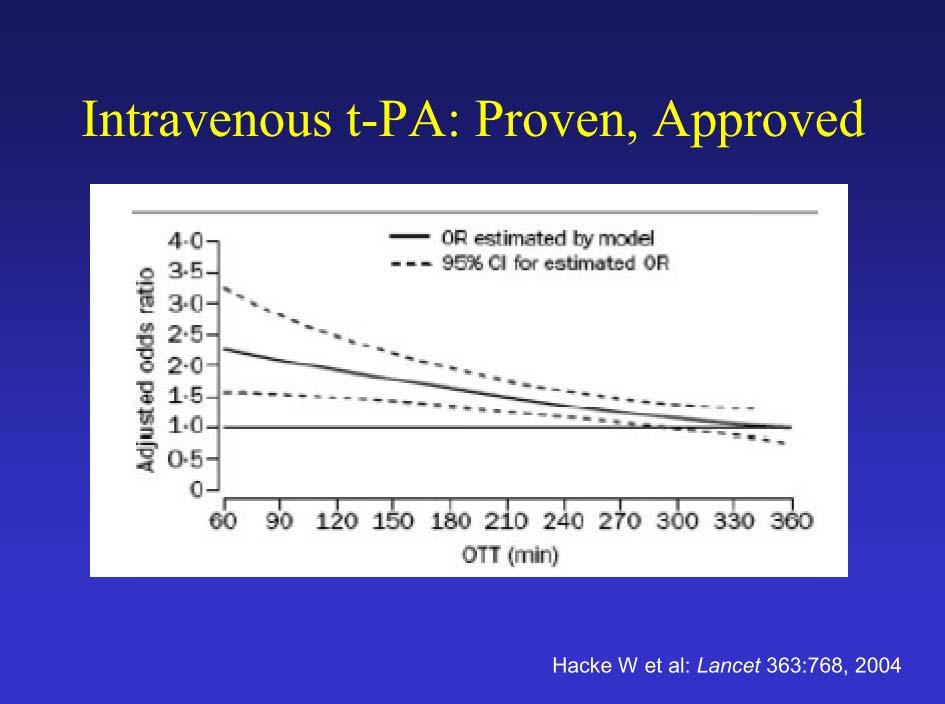
6 Acute stroke timeline Time of onset= last time seen normal Is this a stroke? Is this patient suitable for thrombolysis Thrombolysis can be given hours from onset of symptoms Send immediately to HASU
7 Intravenous TPA Pivotal NINDS trial (0-3hours) 30% increase in minimal or no disability at 90 days Symptomatic haem increased %, half were serious and fatal No change in mortality
8
9
10 WHO IS THROMBOLYSIS FOR? Ischaemic stroke with significant disability (only 80%) Rate in UK <1%( Sentinel Audit 2009) 2 in 10 patients who present with a FAST positive event will have a stroke mimic Significant number of exclusions
11 Impact of established treatments Treatment NNT Benefit/100 TPA 3 32 Stroke unit Aspirin 77 1
12 STROKE v TIA A stroke is a clinical syndrome of rapid onset of focal or sometimes global cerebral deficit with a vascular cause lasting more than 24hrs or leading to death. The distinction between TIA and stroke is an arbitrary one at 24 hours.
13 TIA Most TIAs last only minutes (70% last less than 30 mins.) 25% of patients whose TIAS last >5 hours have infarcts on their CTscans Proportion of patients with MR-DWI abnormality ranged from 25-58%
14 SYMPTOMS TIA % Stroke % Diplopia 6 6 Ataxia Hemianopia 6 16 Speech Sensory Motor 50 81
15 LIKELY SYMPTOMS Acute Negative ie loss of function Vascular risk factors NB the clumsy hand
16 UNLIKELY SYMPTONS LOC DIZZINESS ( in isolation) CONFUSION ( distinguish from dysphasia)
17 Prevalence of Risk factors OCPS BP 50% Age<45 20% IHD 33% Smoker 27% 45% PVD 25% TIA 12% Diabetes 10% 11% 2%
18 THE BIG THREE Transient focal neurological deficit TIA Seizure Complicated migraine
19 START 300MG OF ASPIRIN IMMEDIATELY
20 TIA 15 % of strokes are preceded by a TIA OXVACS study showed the risk of recurrence was 7 days 10% 28 days 18% Highest rate of recurrence occurred in those with LAA (Rothwell Lancet2007)
21 MANAGEMENT No clinical way of differentiating which patients will go on to have a stroke. Risk stratification score Speed of treatment
22 ABCD 2 RISK STRATIFICATION SCORE Age> 60 1 Duration of symptoms.60mins 2 Bp >140/ <10 0 Clinical features Unilat weakness 2 Diabetes 1 Speech 1 Other 0
23 ABCD2 scoring system ABCD score is highly predictive of risk of stroke at 7 and 30 days ABCD score of 5 and 6 was an independent predictor of subsequent stroke (7/90day risk 30 and 35% respectively)
24 Risk of Stroke at 7 days by ABCD ABCD score % risk(95%ci) < (0-3.3) (4.2-20) (16-46)
25 Urgency of treatment Express study (Rothwell Lancet 2007) Early initiation of treatment was associated with an 80% reduction of stroke in the risk of early recurrence(90 days)
26 Express study Rapid access Same day referral Same day initiation of treatment if diagnosis confirmed Aspirin 300mg Simvastatin 40mg BP therapy, perindopril/indapamide
27 ABCD2 score and risk High risk 4 seen assessed and treated within 24 hours from first contact with doctor Low risk <4 Seen,assessed and treated within 7days from first contact with doctor
28 TIA SERVICE AT HILLINGDON Standardised referral form throughout NW London Fax /ring Stroke specialist nurse 3-4 clinics a week CT scan,carotid doppler and MRI same day access
29 HIGH RISK Refer directly to stroke specialist nurse Cathy Mason Bleep number 5447 Patient will be seen same day
30 HIGH RISK ABCD 4 Headache, neck pain prominent feature Age < 45 More than 2 TIA in a week On anticoagulation
31 Approach to stroke/tia treatment Anticoagulation Antiplatelets Modification of risk factors
32 Antiplatelets agents Aspirin 300mg-75mg DipyridamoleMR 200mg bd ESPS-2 and ESPRIT (Lancet 5/06) Clopidogrel 75mg MATCH (Lancet7/04) FASTER (Lancet neurol10/07)
33 PROFESS TRIAL(NEJM9/08) Randomised double blind trial of Dipyridamole v Clopidogrel 20,000 patients with ischaemic stroke Recurrent 4 yearly events D =C Composite of stroke, MI and vasc death 13.1% in each Major haem rates higher with dipyridamole
34 Anti platelet options If aspirin naive Aspirin If already on aspirin Add dipyridamole? Or single agent clopidogrel If on 2 agents or clop???
35 Approach to stroke/tia treatment Acute stroke therapy? Anticoagulation Antiplatelets Modification of risk factors
36 Indications for anticoagulation Atrial fibrillation Some cardioembolic sources Thrombus in the heart?ef<35% Vertebral and? carotid dissection Rare hypercoaguable states
37 Approach to stroke/tia treatment Acute stroke therapy? Anticoagulation Antiplatelets Modification of risk factors
38 Hypertension Number one risk factor, effects in both primary and secondary prevention. PROGRESS and LIFE trials show that stroke risk reduction is proportional to the degree of reduction and not absolute level. Some evidence that ACE inhibitors have added benefit..
39 Hypercholesterolemia HPS shows same affect for cholesterol and statins Statins for (almost ) all SPARCL (NEJM 8/06), 80mg atorvastatin in stroke TIA if LDL>100
40 Summary of Treatment Aspirin 300mg for2/52, then 75mg Dipyridamole in addition or clopidogrel Statin Blood pressure lowering Assessment of carotid and cardiac disease NO DRIVING FOR 1 MONTH
41 What treatment for TIA? Aggressive medical management Carotid Endartectomy Carotid stenting
42 Carotid Endarterectomy NASCET and ECAS trials showed that surgery is beneficial in symptomatic stenosis >70% Selected patients with 50-60%, male with events within last 2 weeks and specific plaque morphology
43 Case 5 61 year old man with hypertension comes to surgery with 5 min episode of right arm weakness and dysphasia which have resolved Bp 150/90 Not diabetic
44 Management ABCD 5 Ring SSN If overnight then admit needs to be investigated and treated within 24 hours
45 Case 6 42 year old man presents with episode of visual loss Smoker No vascular risk factors BP 130/80
46 Management ABCD 1 Start on aspirin 300mg Tell patient not to drive Refer TIA clinic Form/Stroke specialist nurse Low risk so needs to be seen within a week
47 Case 4 30 year old man presents with 15 mins of aphasia and R upper limb weakness All symptoms have resolved No vascular risk factors Examination is normal Patient reports history of neck pain after vomiting
48 CASE 7 60 year old man presents with an episode of collapse While getting out of the shower Wife thinks there may have been a facial droop Hypertensive on 3 medications ABCD2 2
49 Case 8 88 year old Lives in a nursing home Dementia Carer noticed that patient was not responsive. Vomited once No neurological signs
50 What is the diagnosis and what would you do? Unlikely TIA Given comorbidities GP should start aspirin No TIA referral
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know. Case 1 4/5/11. What treatment should you initiate?
 Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University
Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University
Pharmacy STROKE. Anne Kinnear Lead Pharmacist NHS Lothian. Educational Solutions for Workforce Development
 STROKE Anne Kinnear Lead Pharmacist NHS Lothian Aim To update pharmacists on Stroke: the disease and its management and explore ways to implement pharmaceutical care for this patient group as part of normal
STROKE Anne Kinnear Lead Pharmacist NHS Lothian Aim To update pharmacists on Stroke: the disease and its management and explore ways to implement pharmaceutical care for this patient group as part of normal
TIA: Updates and Management 2008
 TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Management of TIA. Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital
 Management of TIA Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital Objectives Definition TIA and stroke TIA: Diagnosis & mimics Risk assessment Referral and emergency management Secondary
Management of TIA Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital Objectives Definition TIA and stroke TIA: Diagnosis & mimics Risk assessment Referral and emergency management Secondary
TIA AND STROKE. Topics/Order of the day 1. Topics/Order of the day 2 01/08/2012
 Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
New Zealand Guideline for the Assessment and Management of Transient Ischaemic Attack (TIA) User Guide
 User Guide") New Zealand Guideline for the Assessment and Management of Transient Ischaemic Attack (TIA) User Guide Acknowledgements The generous voluntary contribution of time and expertise by writers, consumers and
New Zealand Guideline for the Assessment and Management of Transient Ischaemic Attack (TIA) User Guide Acknowledgements The generous voluntary contribution of time and expertise by writers, consumers and
Secondary Stroke Prevention
 Secondary Stroke Prevention Acute stroke conference, Sunnybrook Estates January 20, 2011 Rick Swartz HBSc, MD, PhD, FRCPC Assistant Professor, Department of Medicine, Divisions of Neurology and Obstetrical
Secondary Stroke Prevention Acute stroke conference, Sunnybrook Estates January 20, 2011 Rick Swartz HBSc, MD, PhD, FRCPC Assistant Professor, Department of Medicine, Divisions of Neurology and Obstetrical
2015 Update in Diagnosis and Management of Stroke
 2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
2014 Update in Diagnosis and Management of Stroke
 2014 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Acting Chairman, Department of Neurology
2014 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Acting Chairman, Department of Neurology
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
TIA Transient Ischaemic Attack?
 TIA Transient Ischaemic Attack? OR Transient loss of function (TLOF) Tal Anjum Consultant Stroke Physician, Morriston Hospital Training & education lead, WASP (Welsh Association of Stroke Physicians) Qs.
TIA Transient Ischaemic Attack? OR Transient loss of function (TLOF) Tal Anjum Consultant Stroke Physician, Morriston Hospital Training & education lead, WASP (Welsh Association of Stroke Physicians) Qs.
TIAs and posterior circulation problems
 TIAs and posterior circulation problems A/Professor Helen Dewey Head, Stroke Service Austin Health Austin Health How many strokes and TIAs are out there? depends on the definition! ~60,000 strokes in
TIAs and posterior circulation problems A/Professor Helen Dewey Head, Stroke Service Austin Health Austin Health How many strokes and TIAs are out there? depends on the definition! ~60,000 strokes in
Dr Ben Turner. Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital
 Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
Stroke in the ED. Dr. William Whiteley. Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian
 Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Appendix 2C - Stroke Services in Fife
 Appendix 2C - Stroke Services in Fife Stroke and TIA Management Guidance for GPs The aim of this document is to; Inform GPs of acute stroke services in Fife Summarise who to admit and describe acute management
Appendix 2C - Stroke Services in Fife Stroke and TIA Management Guidance for GPs The aim of this document is to; Inform GPs of acute stroke services in Fife Summarise who to admit and describe acute management
Guideline scope Stroke and transient ischaemic attack in over 16s: diagnosis and initial management (update)
") NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Stroke and transient ischaemic attack in over s: diagnosis and initial management (update) 0 0 This will update the NICE on stroke and
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Stroke and transient ischaemic attack in over s: diagnosis and initial management (update) 0 0 This will update the NICE on stroke and
Stroke/TIA. Tom Bedwell
 Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS. 73 year old NS right-handed male applicant for $1 Million life insurance
 MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
Stroke & the Emergency Department. Dr. Barry Moynihan, March 2 nd, 2012
 Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS. 73 year old NS right-handed male applicant for $1 Million Life Insurance
 MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
Disclosures. An Update on TIA and Minor Stroke. The Agenda PROGNOSIS PATHOPHYSIOLOGY GUIDELINES AND PROVEN MANAGEMENT STRATEGIES AGGRESSIVE TREATMENT
 Disclosures An Update on TIA and Minor Stroke Dr. Johnston is principal investigator for the POINT trial, sponsored by the NIH but with drug and placebo contributed by Sanofi-Aventis. S. Claiborne Johnston,
Disclosures An Update on TIA and Minor Stroke Dr. Johnston is principal investigator for the POINT trial, sponsored by the NIH but with drug and placebo contributed by Sanofi-Aventis. S. Claiborne Johnston,
Referral Guideline for Patients with TIA
 DERBYSHIRE COUNTY PCT & NHS DERBY CITY Clinical Effectiveness & Guidelines Group Referral Guideline for Patients with TIA Key Messages This is a revised guideline for patients referred to the TIA service
DERBYSHIRE COUNTY PCT & NHS DERBY CITY Clinical Effectiveness & Guidelines Group Referral Guideline for Patients with TIA Key Messages This is a revised guideline for patients referred to the TIA service
Neuroanatomy of a Stroke. Joni Clark, MD Professor of Neurology Barrow Neurologic Institute
 Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
Stroke secondary prevention. Gill Cluckie Stroke Nurse Consultant St. George s Hospital
 Stroke secondary prevention Gill Cluckie Stroke Nurse Consultant St. George s Hospital Stroke recurrence The risk of recurrent stroke is greatest after first stroke 2 3% of survivors of a first stroke
Stroke secondary prevention Gill Cluckie Stroke Nurse Consultant St. George s Hospital Stroke recurrence The risk of recurrent stroke is greatest after first stroke 2 3% of survivors of a first stroke
03/30/2016 DISCLOSURES TO OPERATE OR NOT THAT IS THE QUESTION CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE
 CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE Elizabeth L. Detschelt, M.D. Allegheny Health Network Vascular and Endovascular Symposium April 2, 2016 DISCLOSURES I have no
CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE Elizabeth L. Detschelt, M.D. Allegheny Health Network Vascular and Endovascular Symposium April 2, 2016 DISCLOSURES I have no
Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre
 Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre Objectives To learn what s new in stroke care 2010-11 1) Acute stroke management Carotid artery stenting versus surgery for symptomatic
Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre Objectives To learn what s new in stroke care 2010-11 1) Acute stroke management Carotid artery stenting versus surgery for symptomatic
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Pre-Hospital Stroke Care: Bringing It To The Street. by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center
 Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
ICSS Safety Results NOT for PUBLICATION. June 2009 ICSS ICSS ICSS ICSS. International Carotid Stenting Study: Main Inclusion Criteria
 Safety Results NOT for The following slides were presented to the Investigators Meeting on 22/05/09 and most of them were also presented at the European Stroke Conference on 27/05/09 They are NOT for in
Safety Results NOT for The following slides were presented to the Investigators Meeting on 22/05/09 and most of them were also presented at the European Stroke Conference on 27/05/09 They are NOT for in
Vague Neurological Conditions
 Vague Neurological Conditions Dr. John Lefebre, MD, FRCPC Chief Regional Medical Director Europe, India, South Africa, Middle East and Turkey Canada 2014 2 3 4 Agenda Dr. John Lefebre, M.D., FRCPC 1. TIA
Vague Neurological Conditions Dr. John Lefebre, MD, FRCPC Chief Regional Medical Director Europe, India, South Africa, Middle East and Turkey Canada 2014 2 3 4 Agenda Dr. John Lefebre, M.D., FRCPC 1. TIA
2018 Update in Diagnosis and Management of Stroke
 2018 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Chair, Department of Neurology Director,
2018 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Chair, Department of Neurology Director,
Critical Review Form Therapy
 Critical Review Form Therapy A transient ischaemic attack clinic with round-the-clock access (SOS-TIA): feasibility and effects, Lancet-Neurology 2007; 6: 953-960 Objectives: To evaluate the effect of
Critical Review Form Therapy A transient ischaemic attack clinic with round-the-clock access (SOS-TIA): feasibility and effects, Lancet-Neurology 2007; 6: 953-960 Objectives: To evaluate the effect of
CONCISE GUIDE National Clinical Guidelines for Stroke 2nd Edition
 CONCISE GUIDE 2004 National for Stroke 2nd Edition This concise guide summarises the recommendations, graded according to the evidence, from the National 2nd edition. As critical aspects of care are not
CONCISE GUIDE 2004 National for Stroke 2nd Edition This concise guide summarises the recommendations, graded according to the evidence, from the National 2nd edition. As critical aspects of care are not
Canadian Best Practice Recommendations for Stroke Care. (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management
 Section # 3 Section # 3 Hyperacute Stroke Management") Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
KEEPING YOUR PATIENT OUT OF THE HOSPITAL BY PREVENTING A SECOND STROKE
 KEEPING YOUR PATIENT OUT OF THE HOSPITAL BY PREVENTING A SECOND STROKE Dr. Grant Stotts Staff Neurologist, Ottawa Hospital Director, Ottawa Stroke Program Medical Director, Champlain Regional Stroke Program
KEEPING YOUR PATIENT OUT OF THE HOSPITAL BY PREVENTING A SECOND STROKE Dr. Grant Stotts Staff Neurologist, Ottawa Hospital Director, Ottawa Stroke Program Medical Director, Champlain Regional Stroke Program
Stroke Topics. Advances in the Prevention and Treatment of Stroke. Non-Contrast Head CT. Patient 1-68 yo man
 Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
Management and Investigation of Ischemic Stroke By Etiology
 Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
Stroke and TIA. Stephen Davis Melbourne Brain Centre Department of Neurology, Royal Melbourne Hospital University of Melbourne
 Stroke and TIA Stephen Davis Melbourne Brain Centre Department of Neurology, Royal Melbourne Hospital University of Melbourne Global burden of stroke 20 million strokes each year 2 nd leading cause of
Stroke and TIA Stephen Davis Melbourne Brain Centre Department of Neurology, Royal Melbourne Hospital University of Melbourne Global burden of stroke 20 million strokes each year 2 nd leading cause of
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis
/intracranial atherosclerosis") Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
5/2/2016. Outpatient Stroke Management Sheila Smith MD May 5, 2016
 Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Nicolas Bianchi M.D. May 15th, 2012
 Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
GOVERNANCE BOARD. 14th January Clinical Audit of Stroke Services. At Shrewsbury and Telford Hospitals NHS Trust
 GOVERNANCE BOARD 14th January 2014 Clinical Audit of Stroke Services At Shrewsbury and Telford Hospitals NHS Trust 1.0 Introduction A clinical review of cases recorded and coded as with a 0-1 day length
GOVERNANCE BOARD 14th January 2014 Clinical Audit of Stroke Services At Shrewsbury and Telford Hospitals NHS Trust 1.0 Introduction A clinical review of cases recorded and coded as with a 0-1 day length
Stroke 101. Maine Cardiovascular Health Summit. Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013
 Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine
 Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Treatment Considerations for Carotid Artery Stenosis. Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery
 Treatment Considerations for Carotid Artery Stenosis Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery 4.29.2016 There is no actual or potential conflict of interest in regards to this presentation
Treatment Considerations for Carotid Artery Stenosis Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery 4.29.2016 There is no actual or potential conflict of interest in regards to this presentation
Branko N Huisa M.D. Assistant Professor of Neurology UNM Stroke Center
 Branko N Huisa M.D. Assistant Professor of Neurology UNM Stroke Center THE END! CHANGABLE Blood pressure Diabetes Mellitus Hyperlipidemia Atrial fibrillation Nicotine Drug abuse Life style NOT CHANGABLE
Branko N Huisa M.D. Assistant Professor of Neurology UNM Stroke Center THE END! CHANGABLE Blood pressure Diabetes Mellitus Hyperlipidemia Atrial fibrillation Nicotine Drug abuse Life style NOT CHANGABLE
Slide 1. Slide 2 Conflict of Interest Disclosure. Slide 3 Stroke Facts. The Treatment of Intracranial Stenosis. Disclosure
 Slide 1 The Treatment of Intracranial Stenosis Helmi Lutsep, MD Vice Chair and Dixon Term Professor, Department of Neurology, Oregon Health & Science University Chief of Neurology, VA Portland Health Care
Slide 1 The Treatment of Intracranial Stenosis Helmi Lutsep, MD Vice Chair and Dixon Term Professor, Department of Neurology, Oregon Health & Science University Chief of Neurology, VA Portland Health Care
Stroke: What did we learn in the last year?
 Stroke: What did we learn in the last year? J. Claude Hemphill III, MD, MAS Associate Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director, Neurocritical
Stroke: What did we learn in the last year? J. Claude Hemphill III, MD, MAS Associate Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director, Neurocritical
TRANSIENT ISCHEMIC ATTACK (TIA)
") TRANSIENT ISCHEMIC ATTACK (TIA) AND MINOR STROKE Dr. Leanne K. Casaubon, MD MSc FRCPC Associate Professor, University of Toronto Director, TIA and Minor Stroke (TAMS) Unit University Health Network - Toronto
TRANSIENT ISCHEMIC ATTACK (TIA) AND MINOR STROKE Dr. Leanne K. Casaubon, MD MSc FRCPC Associate Professor, University of Toronto Director, TIA and Minor Stroke (TAMS) Unit University Health Network - Toronto
Clinical Decision Making: Hyperacute Management of Symptomatic Carotid Artery Disease
 Clinical Decision Making: Hyperacute Management of Symptomatic Carotid Artery Disease Tarvinder Singh, MS, MD Neurohospitalist Swedish Neuroscience Institute 1 Objectives Definition Why the urgency? Evidence/Guidelines
Clinical Decision Making: Hyperacute Management of Symptomatic Carotid Artery Disease Tarvinder Singh, MS, MD Neurohospitalist Swedish Neuroscience Institute 1 Objectives Definition Why the urgency? Evidence/Guidelines
Redgrave JN, Coutts SB, Schulz UG et al. Systematic review of associations between the presence of acute ischemic lesions on
 6. Imaging in TIA 6.1 What type of brain imaging should be used in suspected TIA? 6.2 Which patients with suspected TIA should be referred for urgent brain imaging? Evidence Tables IMAG1: After TIA/minor
6. Imaging in TIA 6.1 What type of brain imaging should be used in suspected TIA? 6.2 Which patients with suspected TIA should be referred for urgent brain imaging? Evidence Tables IMAG1: After TIA/minor
Michael Horowitz, MD Pittsburgh, PA
 Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
Reducing delays to outpatient assessment of strokes and TIAs
 Reducing delays to outpatient assessment of strokes and TIAs Prof Martin Dennis Stroke Physician (Lothian) Clinical lead for Scottish Stroke Care Audit The patient pathway Step 1 Possible TIA, minor stroke
Reducing delays to outpatient assessment of strokes and TIAs Prof Martin Dennis Stroke Physician (Lothian) Clinical lead for Scottish Stroke Care Audit The patient pathway Step 1 Possible TIA, minor stroke
David Strain, Diabetes and Vascular Research Centre University of Exeter Medical School, UK
 Risk Stratification in TIA/Stroke? David Strain, Diabetes and Vascular Research Centre University of Exeter Medical School, UK Disclaimer I would never allow a scientist to partake in my government Give
Risk Stratification in TIA/Stroke? David Strain, Diabetes and Vascular Research Centre University of Exeter Medical School, UK Disclaimer I would never allow a scientist to partake in my government Give
Dawn Matherne Meyer PhD,RN,FNP-C. Assistant Professor University of California San Diego
 Dawn Matherne Meyer PhD,RN,FNP-C Assistant Professor University of California San Diego Evidence Based Care of the Stroke Patient: A Focus on Acute Treatment, BP Management, & Antiplatelets TIME IS BRAIN
Dawn Matherne Meyer PhD,RN,FNP-C Assistant Professor University of California San Diego Evidence Based Care of the Stroke Patient: A Focus on Acute Treatment, BP Management, & Antiplatelets TIME IS BRAIN
Unclogging The Pipes. Zahraa Rabeeah MD Chief Resident February 9,2018
 Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
How do we assess risk in TIA?
 How do we assess risk in TIA? David Strain, Diabetes and Vascular Research Centre University of Exeter Medical School, UK Disclaimer I would never allow a scientist to partake in my government Give them
How do we assess risk in TIA? David Strain, Diabetes and Vascular Research Centre University of Exeter Medical School, UK Disclaimer I would never allow a scientist to partake in my government Give them
PFO Management update
 PFO Management update May 12, 2017 Peter Casterella, MD Swedish Heart and Vascular 1 PFO Update 2017: Objectives Review recently released late outcomes of RESPECT trial and subsequent FDA approval of PFO
PFO Management update May 12, 2017 Peter Casterella, MD Swedish Heart and Vascular 1 PFO Update 2017: Objectives Review recently released late outcomes of RESPECT trial and subsequent FDA approval of PFO
Neuro-vascular Intervention in Stroke. Will Adams Consultant Neuroradiologist Plymouth Hospitals NHS Trust
 Neuro-vascular Intervention in Stroke Will Adams Consultant Neuroradiologist Plymouth Hospitals NHS Trust Stroke before the mid 1990s Swelling Stroke extension Haemorrhagic transformation Intravenous thrombolysis
Neuro-vascular Intervention in Stroke Will Adams Consultant Neuroradiologist Plymouth Hospitals NHS Trust Stroke before the mid 1990s Swelling Stroke extension Haemorrhagic transformation Intravenous thrombolysis
2018 Early Management of Acute Ischemic Stroke Guidelines Update
 2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
Document Title: The Management of Acute Ischemic Stroke & TIA
 Project: Ghana Emergency Medicine Collaborative Document Title: The Management of Acute Ischemic Stroke & TIA Author(s): Rashmi U. Kothari, M.D. (KCMS/MSU), 2012 License: Unless otherwise noted, this material
Project: Ghana Emergency Medicine Collaborative Document Title: The Management of Acute Ischemic Stroke & TIA Author(s): Rashmi U. Kothari, M.D. (KCMS/MSU), 2012 License: Unless otherwise noted, this material
Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco
 Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco I have no financial disclosures 1 Hospital Management Thrombolytic and Thrombectomy Blood pressure Stroke in the Young
Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco I have no financial disclosures 1 Hospital Management Thrombolytic and Thrombectomy Blood pressure Stroke in the Young
Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE
 Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
Understanding transient ischaemic attack
 chemistanddruggist.co.uk/update UPDATE Module 1679 PREMIUM CPD CONTENT FOR 1 per week Buy UPDATEPLUS for 52+VAT Visit chemistanddruggist.co.uk/update-plus for full details This module covers: Causes, symptoms
chemistanddruggist.co.uk/update UPDATE Module 1679 PREMIUM CPD CONTENT FOR 1 per week Buy UPDATEPLUS for 52+VAT Visit chemistanddruggist.co.uk/update-plus for full details This module covers: Causes, symptoms
44TH ANNUAL RECENT ADVANCES IN NEUROLOGY
 Presenter Disclosure Information J. Donald Easton, MD Clinical Professor of Neurology February 17, 2011 44TH ANNUAL RECENT ADVANCES IN NEUROLOGY TIA: Definition, Evaluation, and Treatment J. Donald Easton,
Presenter Disclosure Information J. Donald Easton, MD Clinical Professor of Neurology February 17, 2011 44TH ANNUAL RECENT ADVANCES IN NEUROLOGY TIA: Definition, Evaluation, and Treatment J. Donald Easton,
Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO
 Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO Goal of treatment of carotid disease Identify those at risk of developing symptoms Prevent patients at risk from developing symptoms Prevent
Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO Goal of treatment of carotid disease Identify those at risk of developing symptoms Prevent patients at risk from developing symptoms Prevent
Advances in the treatment of posterior cerebral circulation symptomatic disease
 Advances in the treatment of posterior cerebral circulation symptomatic disease Athanasios D. Giannoukas MD, MSc(Lond.), PhD(Lond.), FEBVS Professor of Vascular Surgery Faculty of Medicine, School of Health
Advances in the treatment of posterior cerebral circulation symptomatic disease Athanasios D. Giannoukas MD, MSc(Lond.), PhD(Lond.), FEBVS Professor of Vascular Surgery Faculty of Medicine, School of Health
Stroke Mimics. Paul Guyler
 Stroke Mimics Paul Guyler Consultant Stroke Physician at Southend University Hospital Clinical Lead for Acute Stroke Essex Cardiac and Stroke Network Aims Why worry? Stroke Recognition Tools History, Examination
Stroke Mimics Paul Guyler Consultant Stroke Physician at Southend University Hospital Clinical Lead for Acute Stroke Essex Cardiac and Stroke Network Aims Why worry? Stroke Recognition Tools History, Examination
Andrew Barreto, MD MS Associate Professor of Neurology Stroke Neurologist UTHealth. May 23, 2018
 Andrew Barreto, MD MS Associate Professor of Neurology Stroke Neurologist UTHealth May 23, 2018 Disclosure No personal financial relationships with any company. Presentation Outline Definitions, signs
Andrew Barreto, MD MS Associate Professor of Neurology Stroke Neurologist UTHealth May 23, 2018 Disclosure No personal financial relationships with any company. Presentation Outline Definitions, signs
Acute stroke. Ischaemic stroke. Characteristics. Temporal classification. Clinical features. Interpretation of Emergency Head CT
 Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Carotid Artery Stenting
 Carotid Artery Stenting Woong Chol Kang M.D. Gil Medical Center, Gachon University of Medicine and Science, Incheon, Korea Carotid Stenosis and Stroke ~25% of stroke is due to carotid disease, the reminder
Carotid Artery Stenting Woong Chol Kang M.D. Gil Medical Center, Gachon University of Medicine and Science, Incheon, Korea Carotid Stenosis and Stroke ~25% of stroke is due to carotid disease, the reminder
Episode 117 TIA Update
 TIA Causes and Common Mimics Episode 117 TIA Update With Walter Himmel & David Dushenski Prepared by Shaun Mehta & Alex Hart, Nov 2018 Much has changed in recent years when it comes to TIA risk stratification,
TIA Causes and Common Mimics Episode 117 TIA Update With Walter Himmel & David Dushenski Prepared by Shaun Mehta & Alex Hart, Nov 2018 Much has changed in recent years when it comes to TIA risk stratification,
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase <48h)
") Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
Oltre la terapia medica nelle dissezioni carotidee
 Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
Subject Expert. Michelle Whaley MSN, CNS, CCNS, ANVP-BC Swedish Medical Center Englewood, CO
 Stroke 101 Subject Expert Michelle Whaley MSN, CNS, CCNS, ANVP-BC Swedish Medical Center Englewood, CO 2 Objectives Types of strokes Stroke warning signs Stroke risk factors Medical test performed following
Stroke 101 Subject Expert Michelle Whaley MSN, CNS, CCNS, ANVP-BC Swedish Medical Center Englewood, CO 2 Objectives Types of strokes Stroke warning signs Stroke risk factors Medical test performed following
Maximising Delivery of Thrombectomy
 Maximising Delivery of Thrombectomy Professor Gary Ford Chief Executive Officer, Oxford Academic Health Science Network Consultant Stroke Physician, Oxford University Hospitals Visiting Professor of Clinical
Maximising Delivery of Thrombectomy Professor Gary Ford Chief Executive Officer, Oxford Academic Health Science Network Consultant Stroke Physician, Oxford University Hospitals Visiting Professor of Clinical
NEW ZEALAND GUIDELINE FOR THE ASSESSMENT AND MANAGEMENT OF PEOPLE WITH RECENT TRANSIENT ISCHAEMIC ATTACK (TIA)
") NEW ZEALAND GUIDELINE FOR THE ASSESSMENT AND MANAGEMENT OF PEOPLE WITH RECENT TRANSIENT ISCHAEMIC ATTACK (TIA) Acknowledgements The generous voluntary contribution of time and expertise by writers, consumers
NEW ZEALAND GUIDELINE FOR THE ASSESSMENT AND MANAGEMENT OF PEOPLE WITH RECENT TRANSIENT ISCHAEMIC ATTACK (TIA) Acknowledgements The generous voluntary contribution of time and expertise by writers, consumers
Therapy for Acute Stroke. Systems of Care for TIA
 Therapy for Acute Stroke and Systems of Care for TIA Gregory W. Albers, MD Coyote Foundation Professor of Neurology and Neurological Sciences Director, Stanford Stroke Center Stanford University Medical
Therapy for Acute Stroke and Systems of Care for TIA Gregory W. Albers, MD Coyote Foundation Professor of Neurology and Neurological Sciences Director, Stanford Stroke Center Stanford University Medical
Patients who experience a stroke or transient ischemic
 REPORTS Therapeutic Interventions for Prevention of Recurrent Ischemic Stroke Howard S. Kirshner, MD Abstract Patients who suffer ischemic stroke or transient ischemic attack (TIA) are at increased risk
REPORTS Therapeutic Interventions for Prevention of Recurrent Ischemic Stroke Howard S. Kirshner, MD Abstract Patients who suffer ischemic stroke or transient ischemic attack (TIA) are at increased risk
It is the nature of a stroke to partly take away the use of a man s limbs and to throw him onto the parish if he had no children to look to
 It is the nature of a stroke to partly take away the use of a man s limbs and to throw him onto the parish if he had no children to look to George Eliot The Cripples (1949) All cerebrovascular events in
It is the nature of a stroke to partly take away the use of a man s limbs and to throw him onto the parish if he had no children to look to George Eliot The Cripples (1949) All cerebrovascular events in
Stroke: clinical presentations, symptoms and signs
 Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
Management of Acute Confusional State in Older People
 Management of Acute Confusional State in Older People BACKGROUND Acute confusional state or delirium occurs in 15-20% of all admissions to hospital. It is more likely to occur on a background of pre existing
Management of Acute Confusional State in Older People BACKGROUND Acute confusional state or delirium occurs in 15-20% of all admissions to hospital. It is more likely to occur on a background of pre existing
Carotid Revascularization
 Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Supplementary Online Content
 Supplementary Online Content Wolters FJ, Li L, Gutnikov SA, Mehta Z, Rothwell PM. Medical attention seeking after transient ischemic attack and minor stroke in relation to the UK Face, Arm, Speech, Time
Supplementary Online Content Wolters FJ, Li L, Gutnikov SA, Mehta Z, Rothwell PM. Medical attention seeking after transient ischemic attack and minor stroke in relation to the UK Face, Arm, Speech, Time
Appendix A: Summary of evidence from surveillance
 Appendix A: Summary of evidence from surveillance 8-year surveillance (2016) stroke and transient ischaemic attack in over 16s (2008) NICE guideline CG68 Summary of new evidence from surveillance... 1
Appendix A: Summary of evidence from surveillance 8-year surveillance (2016) stroke and transient ischaemic attack in over 16s (2008) NICE guideline CG68 Summary of new evidence from surveillance... 1
Carotid Artery Stenting
 Carotid Artery Stenting JESSICA MITCHELL, ACNP CENTRAL ILLINOIS RADIOLOGICAL ASSOCIATES External Carotid Artery (ECA) can easily be identified from Internal Carotid Artery (ICA) by noticing the branches.
Carotid Artery Stenting JESSICA MITCHELL, ACNP CENTRAL ILLINOIS RADIOLOGICAL ASSOCIATES External Carotid Artery (ECA) can easily be identified from Internal Carotid Artery (ICA) by noticing the branches.
Cryptogenic Stroke: A logical approach to a common clinical problem
 Cryptogenic Stroke: A logical approach to a common clinical problem Alphonse M. Ambrosia, DO, FACC Interventional Cardiologist CardioVascular Associates of Mesa Mesa, Arizona Speakers Bureau Boston Scientific
Cryptogenic Stroke: A logical approach to a common clinical problem Alphonse M. Ambrosia, DO, FACC Interventional Cardiologist CardioVascular Associates of Mesa Mesa, Arizona Speakers Bureau Boston Scientific
Restart or stop antithrombotics after intracerebral haemorrhage (ICH)?
?") Restart or stop antithrombotics after intracerebral haemorrhage (ICH)? Rustam Al-Shahi Salman professor of clinical neurology & honorary consultant neurologist www.rush.ed.ac.uk @BleedingStroke /bleedingstroke
Restart or stop antithrombotics after intracerebral haemorrhage (ICH)? Rustam Al-Shahi Salman professor of clinical neurology & honorary consultant neurologist www.rush.ed.ac.uk @BleedingStroke /bleedingstroke
TIA triage in Not all that glitters is gold
 TIA triage in 2016 Not all that glitters is gold Disclosures No industry related disclosures Expert witness work Overview Definition Implications Guidelines, secondary prevention Implementation of guidelines
TIA triage in 2016 Not all that glitters is gold Disclosures No industry related disclosures Expert witness work Overview Definition Implications Guidelines, secondary prevention Implementation of guidelines
Practical Considerations in the Early Treatment of Acute Stroke
 Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Game Strategy: High Intensity Statin in Stroke. K.M. Osei MD, MSc Cardiovascular Conference PARMC Feb 24, 2018
 Game Strategy: High Intensity Statin in Stroke K.M. Osei MD, MSc Cardiovascular Conference PARMC Feb 24, 2018 No Disclosures Are you Mind Full or Mindful? Objectives 1. Discuss the correlation between
Game Strategy: High Intensity Statin in Stroke K.M. Osei MD, MSc Cardiovascular Conference PARMC Feb 24, 2018 No Disclosures Are you Mind Full or Mindful? Objectives 1. Discuss the correlation between
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Journal Club. 1. Develop a PICO (Population, Intervention, Comparison, Outcome) question for this study
 question for this study") Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for
 Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Stroke Workshop. Pre-Workshop Handout. With Walter Himmel, Meeta Patel & Anton Helman
 2018 Stroke Workshop Pre-Workshop Handout With Walter Himmel, Meeta Patel & Anton Helman Instructions for Getting the Most Out of The EMU Stroke Workshop Handout This workshop has been designed around
2018 Stroke Workshop Pre-Workshop Handout With Walter Himmel, Meeta Patel & Anton Helman Instructions for Getting the Most Out of The EMU Stroke Workshop Handout This workshop has been designed around